Embed Size (px)
Citation preview

2/1/2017
1
WHAT ORAL ANTINEOPLASTIC AGENTS MEAN FOR YOUR PATIENTS, YOUR STAFF, AND YOUR PHARMACY: A REVIEW OF COMMON ORAL
AGENTS, PROPER HANDLING, AND
SUPPORTIVE CAREKelsey Mulverhill, PharmD and Ai Thi Nguyen, PharmD Oregon State Pharmacy AssociationPGY2 Oncology Pharmacy Residents Lane County Mid-Winter CE SeminarOregon Health & Science University February 19, 2017
Disclosure
� Kelsey Mulverhill and Ai Thi Nguyen have no actual or potential conflicts of interest in relation to this program.
2
Objectives
1. Identify common side effects for the oral oncolytic agents
that are presented.
2. Properly counsel patients on supportive therapies to
reduce complications from oral oncolytic agents.
3. Describe standard precautions every pharmacy staff
member must take when handling an oral oncolytic
medication.
4. Given a patient case, recommend at least two patient
counseling points on how an oncolytic medication should
be handled, stored, and administered by the patient
and/or caregiver.
5. Given a patient case, list at least two resources for references a pharmacist may use to determine if an
oncolytic agent may interact with a patient’s other
medications.
3

2/1/2017
2
Presentation outline4
Questions and
introduction
Common side effects
Supportive care
Standard handling
precautions
Pharmacy staff
resources
Break
Question #1
� When preparing agents for dispensing or when handling oral oncolytics, pharmacy staff should wash their hands, then don gloves. After the oral oncolytic agent is placed in its final container for
dispensing, staff should wash hands again and wash any material that touched the oral oncolytic agent.
a) True
b) False
5
Question #2
� A patient comes to your pharmacy to fill fluconazole 200 mg PO once daily for 7 days for completion of treatment for Candida albicans pyelonephritis. The patient is also taking imatinib 400 mg PO daily for
chronic myeloid leukemia. What resources would you use to determine if any drug interactions exist?
a) Lexi-Comp or other drug database
b) Imatinib package insert
c) Oncology pharmacist colleague
d) All of the above
6

2/1/2017
3
Question #3
� When educating patients/caregivers on oral oncolytic administration, which of the following general recommendations is INCORRECT?
a) Keep away from children and pets
b) Caregivers should wear gloves when handling
c) May be stored in pill boxes, but should be separate
from other medications
d) May chew, crush, cut, or dissolve
7
Question #4
� Which of the following is a possible side effect of anti-estrogen therapies for estrogen-receptor positive breast cancer?
a) Hot flashes
b) Hallucinations
c) Neutropenia
d) Arrhythmias
8
Question #5
� A patient comes to your pharmacy asking for your recommendation for GERD symptoms. They are currently taking dasatinib. What over-the-counter medication would you recommend?
a) Ranitidine
b) Omeprazole
c) An antacid, such as calcium carbonate
d) None of the above are recommended
9

2/1/2017
4
ORAL ONCOLYTICS:COMPLICATIONS AND MANAGEMENT
Introduction
10
Oral oncolytic drugs
Common classes of oral
oncolytics12
� Tyrosine kinase inhibitors (TKIs)
� Immunomodulatory drugs (IMiDs)
� Hormone therapy
� Selective estrogen receptor modulators (SERMs)
� Selective estrogen receptor down-regulators (SERDs)
� Aromatase inhibitors
� Non-steroidal anti-androgens

2/1/2017
5
Major oral oncolytic
complications13
� The most prevalent complications arising from cancer treatments are
� Cutaneous reactions
� Nausea & vomiting
� Gastrointestinal complaints
� Myelosuppression
CUTANEOUS REACTIONS
Major oral oncolytic complications
14
Cutaneous reactions15
� Common with TKIs
� Epidermal growth factor receptor (EGFR) TKIs� Afatinib (Giotrif®)
� Erlotinib (Tarceva®)
� Gefitinib (Iressa®)
� Bcr-Abl TKIs� First generation
� Imatinib (Gleevec®)
� Second generation
� Bosutinib (Bosulif®)
� Dasatinib (Sprycel®)
� Nilotinib (Tasigna®)
Drug Des Devel Ther 2008;2:215-219.

2/1/2017
6
Cutaneous reactions16
� TKIs for renal cell carcinoma
� Sorafenib (Nexavar®)
� Sunitinib (Sutent®)
� Immunomodulatory drugs
� Lenalidomide (Revlimid®)
� Thalidomide (Thalomid®)
� Antimetabolite
� Capecitabine (Xeloda®)
Drug Des Devel Ther 2008;2:215-219.Arch Dermatol 2006;142(10):1298-1302.
Cutaneous reactions17
� Rashes can present as acneiform, papulomacular, or pustular
� May affect any part of the body
� Bcr-Abl TKIs
� Milder cutaneous side effects compared to EGFR inhibitors
� Hand-foot syndrome (HFS) is a distinct cutaneous manifestation
� Associated with sorafenib, sunitinib, and
capecitabine
Drug Des Devel Ther 2008;2:215-219.Arch Dermatol 2006;142(10):1298-1302.
http://www.cancernetwork.com/s ites/default/f iles/cn_import/1913258.png
http://jgo.amegroups.com/article/viewFile/1285/html/7174
http://www.oncotherapynetwork.com/
Cutaneous reactions18
Grade NCI definition2 Management
1 Mild <10% BSA with or without
symptoms (e.g., pruritus, burning, tightness)
Oral antihistamines1,2,3
Topical antipruritics1
2 Moderate 10-30% BSA with or without
symptoms
Oral antihistamines1,2,3
Topical steroids1,2,3
3 Severe >30% BSA with or without
associated symptoms
Oral antihistamines1,2,3
Topical steroids1,2,3
Antibiotics1,2,3
4 Life-
threatening
Papules or pustules covering any
part of the body which are associated with extensive super-
infection
Discontinue therapy
Oral steroids3
Antibiotics1,2,3
5 Death Rash resulting in death -1European Society for Medical Oncology.2Curr Oncol 2011;18(3):126-138.3J Natl Compr Canc Netw 2009;7 Suppl 1:S5-21. BSA=body surface area

2/1/2017
7
Cutaneous reaction
management
� Oral antihistamines
� Topical antihistamines/ antipruritics
� Topical steroids
� Hydrocortisone 1-2.5%
� Beclometasone 0.025-
0.1%
� Clobetasol 0.05%
� Topical antibiotics
� Clindamycin 2%
� Antibiotics
� Doxycycline 100 mg PO BID
� Minocycline 100 mg
PO daily
� Tetracycline 500 mg
PO BID
19
Curr Oncol 2009;16(1):16–26.Drugs 2015;75(12):1335-48.
Cutaneous reaction
management20
Use alcohol-free, fragrance-free, hypoallergenic
moisturizer
Drink plenty of fluids (at least 2L
per day) and avoid caffeine
Apply PABA-free sunscreen of at
least SPF 30 and wear protective
clothing
Avoid hot showers, walking
barefoot, and tight-fitting footwear
Wear hypoallergenic
makeup
Use mild detergents and skin cleansers
Don’t use over-the-counter anti-acne medications
NAUSEA & VOMITING (N&V)
Major oral oncolytic complications
21

2/1/2017
8
Nausea & vomiting22
� Risk factors
� Female
� Younger age
� History of emesis during pregnancy
� Motion sickness
� High anxiety
� History of alcohol use is protective against chemotherapy-induced N&V
National Comprehensive Cancer Network. Antiemesis (Version 2.2016).
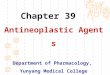
Nausea & vomiting: mechanism of action of neurotransmitters
23
Vomiting Center
Serotonin
Histamine
Acetyl-choline
Substance P
Dopamine
N Engl J Med 2008;358:2482-2494.N Engl J Med 2005;352:817-825.
Nausea & vomiting24
Anticipatory Acute Delayed
Chemotherapy
0-24 hours >24 hours
Psychological
Treatment
BehavioralLorazepam
SerotoninSubstance P
DopamineHistamine
Treatment
5-HT3 antagonistNK-1 receptor antagonist
DexamethasoneDopamine antagonist
Substance P
DopamineHistamine
Treatment
NK-1 receptor antagonistDopamine antagonist
Other receptors
National Comprehensive Cancer Network. Antiemesis (Version 2.2016).

2/1/2017
9
Nausea & vomiting: emetogenic potential of common agents
25
Emetogenic
potential
Emetogenic
risk
Examples
Minimal <10% � Most TKIs
� Thioguanine (Tabloid®)� Hydroxyurea (Hydrea®)
Low 10-30% � Some TKIs
� Lenalidomide (Revlimid®)� Thalidomide (Thalomid®)
Moderate 30-90% � Temozolomide
(Temodar®)� Vinorelbine (Navelbine®)
� Bexarotene (Targretin®)
� Lomustine (CeeNU®)
High >90% � Procarbazine (Matulane®)National Comprehensive Cancer Network. Antiemesis (Version 2.2016).
Nausea & vomiting prevention and treatment
26
Emetogenicity
Acute N&V prevention Breakthrough N&V
Minimal Treat only if symptoms are presentAdd one agent from a different class� Olanzapine� Lorazepam
� Cannabinoid� Haloperidol� Metoclopramide� Scopolamine� Phenothiazine� 5-HT3 antagonists� Steroids
LowDexamethasone, metoclopramide, prochlorperazine, or 5-HT3
antagonist
Moderate
5-HT3 antagonist� Dolasetron 100 mg IV days 1-3� Granisetron 2 mg or 1 mg IV/PO BID days 1-3� Ondansetron 16-24 mg PO days 1-3
� Palonosetron 0.25 mg IV onceAND
� Dexamethasone 12 mg IV/PO day 1, 8 mg IV/PO days 2-3WITH/WITHOUT NK-1 antagonist
High
5-HT3 antagonist as aboveANDNK-1 antagonist
� Aprepitant 125 mg PO day 1, 80 mg PO day 2-3
� Fosaprepitant 150 mg IV (Day 1 only)� Rolapitant 180 mg PO
AND� Dexamethasone 12 mg IV/PO day 1, 8 mg IV/PO days 2-4
Alternatives� Olanzapine 10 mg
PO days 1-3� Palonosetron 0.25
mg IV once� Dexamethasone 20
mg IV/PO once
National Comprehensive Cancer Network. Antiemesis (Version 2.2016).
EPS
Movement initiation without fine motor
tuning
Nausea & vomiting: antiemetic side effects
� Extrapyramidal symptoms (EPS) are a common side effect of several antiemetics
� Prochlorperazine
� Promethazine
� Chlorpromazine
� Haloperidol
� Droperidol
� Metoclopramide
27
National Comprehensive Cancer Network. Antiemesis (Version 2.2016).
� Treatment� Diphenhydramine 25-
50mg PO or IV q4-6h
� Benztropine 1-2mg IV
or IM x1, followed by 1-
2mg PO daily or BID

2/1/2017
10
GASTROINTESTINAL COMPLICATIONS
Major oral oncolytic complications
28
Gastrointestinal complications: diarrhea
29
� Multifaceted and complex pathophysiology
� Impaired absorptive and secretory capacity
� Due to chemotherapy-induced damage to rapidly
dividing crypt cells throughout the intestinal epithelium
� Common offending oral agents
� EGFR inhibitors
� Capecitabine (Xeloda®)
J Clin Oncol 2004;22(14):2918-2926.
Gastrointestinal complications: diarrhea
30
� Rule out Clostridium difficile associated diarrhea (CDAD), other infections, and other etiologies
� Carcinoid syndrome
� Irritable bowel disease (IBD)
� Malabsorption
� NCCN and MASCC lack guidelines for the management of diarrhea associated with cancer
treatment
� ASCO published guidelines in 2004
J Clin Oncol 2004;22(14):2918-2926.
ASCO=American Society of Clinical Oncology, MASCC=Multinational Association of Supportive Care in Cancer, NCCN=National Comprehensive
Cancer Network

2/1/2017
11
Gastrointestinal complications: diarrhea
31
� Management
� Hold chemotherapy
� Replace fluids and electrolytes
� Anti-diarrheals
� Reduce chemotherapy dose
� Associated with a decreased overall and disease-free survival
J Clin Oncol 2004;22(14):2918-2926.
Gastrointestinal complications: diarrhea
32
J Clin Oncol 2004;22(14):2918-2926.
Agent Mechanism of action Dose
Loperamide(Imodium®)
Opioid agonist: decreases intestinal
motility
4 mg PO x1, then 2 mg PO q2-4h
� No maximum daily dose
Diphenoxylate/atropine (Lomotil®)
Opioid agonist/ anticholinergic:
decreases intestinal motility
2.5 mg/0.025 mg: 2 tablets PO q6h
� Max daily dose = 20 mg
Tincture of opium Opioid agonist: decreases intestinal
motility
10 mg/mL: 0.6 mL PO q6h
Octreotide (SandoSTATIN®)
Synthetic somatostatin analog: decreases
secretion of vasoactive intestinal peptide (VIP),
prolongs intestinal transit time, and
100-150 mcg subcutaneously TID
Gastrointestinal complications: constipation
33
� Common offending oral agents
� Hormonal agents� Anastrozole (Arimidex®)
� Letrozole (Femara®)
� Exemestane (Aromasin®)
� Bicalutamide (Casodex®)
� TKIs� Sorafenib (Nexavar®)
� Sunitinib (Sutent®)
� Immunomodulatory Drugs (IMiDs)
� Supportive therapy� Ondansetron (Zofran®)

2/1/2017
12
Gastrointestinal complications: constipation
34
MYELOSUPPRESSION
Major oral oncolytic complications
35
Common offending agents
� Antimetabolites
� Capecitabine (Xeloda®)
� 6-mercaptopurine
(Purinethol®)
� Methotrexate (Trexall®)
� Thioguanine (Tabloid®)
� EGFR TKIs
� Bcr-Abl TKIs
� Immunomodulatory drugs (IMiDs)
� Everolimus (Afintor®)
� Hydroxyurea (Hydrea®)
� Idelalisib (Zydelig®)
� Temozolomide(Temodar®)
36

2/1/2017
13
Myelosuppression37
� Anemia
� Occurs in 30-90% of patients with cancer
� Pathophysiology
� Bone marrow infiltration
� Iron sequestration secondary to upregulation of cytokines
� Chronic blood loss at tumor site
� Chemotherapy-induced depression of erythropoietin
production through the kidneys
� Chemotherapy-induced myelosuppression
National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016)
Myelosuppression38
� Anemia
� Erythropoiesis-stimulating agents (ESAs)
� Epoetin Alfa (Procrit®)
� 150 units/kg subcutaneously three times weekly
� 40,000 units subcutaneously once weekly
� Darbepoetin Alfa (Aranesp®)
� 300 mcg subcutaneously once weekly
National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016)
Myelosuppression39
� Anemia
� Iron supplementation
� Ferrous sulfate 325 mg PO TID
� Ferric carboxymaltose (Injectafer®) 750 mg IV x2 doses q7days
� Iron dextran (INFeD®) 100 mg/day IV (usually until 1000 mg
total dose is reached)
� Iron sucrose (Venofer®) 100-400 mg IV (usually until 1000 mg
total dose is reached)
� Sodium ferric gluconate (Ferrlecit®) 125 mg/dose IV
National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016)

2/1/2017
14
Myelosuppression40
� Febrile neutropenia
� Temperature >38.3oC (101oF) or >38oC (100.3oF) for
more than one hour
AND
� Absolute neutrophil count (ANC) <500 cells/mcL
OR
� ANC <1000 cells/mcL with expected drop to <500
cells/mcL within 48 hours
National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016)
Myelosuppression41
Multinational Association of Supportive Care in Cancer (MASCC)
Severity of illness� No symptoms or mild symptoms
� Moderate symptoms
5
3
No hypotension 5
No chronic obstructive pulmonary disease
4
Solid tumor or no fungal infection 4
No dehydration 3
Outpatient at onset of fever 3
Age <60 years old 2
National Comprehensive Cancer Network. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016)
� MASCC score >21 indicates low risk of acute bacterial infection
Myelosuppression42
� Low risk patients can be treated on an outpatient basis:
� Amoxicillin/clavulanate 875 mg PO BID and ciprofloxacin
500 mg PO BID
� Clindamycin 300 mg PO q6h is substituted for penicillin
allergy
� If febrile neutropenia is treated on an outpatient basis:
� Counsel patients that they need to have daily follow-up
and will need to contact their provider immediately if
their condition worsens
� Do not advise patients to go to the ED unless directed
by their provider

2/1/2017
15
OTHER UNIQUE COMPLICATIONS WITH ORAL ONCOLYTICS
Major oral oncolytic complications
43
Venous thromboembolism44
� Risk factors
� Active cancer
� Post-surgical patients
� Indwelling catheters
� Smoking
� Obesity
� Common offending agents
� TKIs
� IMiDs in combination with dexamethasone
� Selective Estrogen Receptor Modulators (SERMs)
National Comprehensive Cancer Network. Cancer-Associated Venous Thromboembolic Disease. (Version 1.2016).
Venous thromboembolism45
National Comprehensive Cancer Network. Cancer-Associated Venous Thromboembolic Disease. (Version 1.2016).
� Mechanical prophylaxis
� Intermittent pneumatic compression (IPC) devices
� Graduated compression stockings (GCS)
Agent Standard dosing Dosing in obesity (BMI ≥40 kg/m2)
Dalteparin 5000 units SC daily Consider 7500 units SC daily
Enoxaparin 40 mg SC daily Consider 40 mg SC q12h
Fondaparinux 2.5 mg SC daily Consider 5 mg SC daily
Unfractionatedheparin
5000 units SC q8-12h Consider 7500 units SC q8h
Aspirin 81-325 mg daily
Warfarin Adjusted to INR 2-3
SC=subcutaneously

2/1/2017
16
Hormonal agents46
� Selective Estrogen Receptor Modulator (SERMs)
� Tamoxifen citrate (Soltamox®)
� Raloxifene (Evista®)
� Toremifene citrate (Fareston®)
� Selective Estrogen Receptor Down-Regulators (SERDs)
� Fulvestrant (Faslodex®)
� Aromatase inhibitors
� Anastrozole (Arimidex®)
� Letrozole (Femara®)
� Exemestane (Aromasin®)
Lexi-Comp OnlineTM; Accessed January 27, 2017.
Estrogen47
� Primarily produced by the ovaries
� Adrenal glands produce androgens that are converted to estrogen through aromatase
� Aromatase is located in the ovarian tissue, adipose
and skin fibroblasts, bone, and the brain
� Types of Estrogen
� Estradiol: predominant form in premenopausal women
� Estrone: precursor to estradiol, predominant form in
postmenopausal women
� Estriol: estrogen secreted by placenta during pregnancy
FASEB J 2008;22(9):3328-3336.
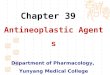
Estrogen48
FASEB J 2008;22(9):3328-3336.
LH
ACTH
EstradiolAndrostenedione
Estrone
Estradiol
Testosterone
Xaromatase inhibitors

2/1/2017
17
Estrogen deprivation side
effects49
� Menopausal symptoms
� Hot flashes
� Night sweats
� Changes in mood
� Arthralgia
� Osteoporosis
� Hypertension
Lexi-Comp OnlineTM; Accessed January 27, 2017.
Menopausal-like symptom management
50
� Hot flashes and night sweats
� Dress in layers, temperature control, and avoid triggers
� Regular exercise
� SSRIs/SNRIs or gabapentin
� No hormone replacement therapy
� Arthalgias
� Exercise and/or acupuncture
� Switch to another aromatase inhibitor or SERM if able
� NSAIDs – consider patient’s comorbidities
� Supplement vitamin D if low
Lexi-Comp OnlineTM. Accessed January 27, 2017.Mayo Clin Proc 2010;85(6):560-566.Curr Oncol 2010;17(1):81-86.
NSAID=non-steroidal anti-inflammatory drug, SERM=selective estrogen receptor modulator,
SSRI=selective serotonin reuptake inhibitor, SNRI=serotonin-norepinephrine reuptake inhibitor
Bone health management51
� Cancer causes � bone metastases
� Majority of cancers have the potential to metastasize to
bones
� Most common: prostate, lung, and breast cancers
� Drug causes � treatment-induced bone loss
� Hormone therapy
� Steroid use for more than 6 months
Ann Oncol 2014;25 Suppl 3:iii124-137.

2/1/2017
18
Bone health management52
� Bisphosphonates� Zoledronic acid (Zometa®)
� 4 mg IV every 3-6 months depending on cancer type and chemotherapy
� Pamidronate (Aredia®)� 90 mg IV every month if used for bone metastases
� 60 mg IV every 3 months if used for prevention of androgen deprivation-induced osteoporosis
� Denosumab (Xgeva®, Prolia®)� Bone metastases from solid tumors: 120 mg
subcutaneously every 4 weeks
� Treatment-induced bone loss in breast and prostate cancer: 60 mg subcutaneously every 6 months
� Calcium 1000 mg PO daily + vitamin D 1000-2000 units PO daily
Ann Oncol 2014;25 Suppl 3:iii124-137.
References53
1. Huang X, Patel S, Ahmed N, et al. Severe toxicity of skin rash, fever and diarrhea associated with imatinib: case report and review of skin toxicities associated with tyrosine kinase inhibitors. Drug Des Devel Ther 2008;2:215-219.
2. Sviggum HP, Davis MD, Rajkumar SV, et al. Dermatologic adverse effects of lenalidomide therapy for amyloidosis and multiple myeloma. Arch Dermatol 2006;142(10):1298-1302.
3. Burtness B, Anadkat M, Basti S, et al. NCCN Task Force Report: management of dermatologic and other toxicities associated with EGFR inhibition in patients with cancer. J Natl Compr Canc Netw 2009;7(Suppl 1):S5-21.
4. Hirsh V. Managing treatment-related adverse events associated with EGFRtyrosine kinase inhibitors in advanced non-small-cell lung cancer. Curr Oncol 2011;18(3):126-138.
5. Melosky B, Anderson H, Burkes RL. Pan Canadian rash trial: a randomized phase III trial evaluating the impact of a prophylactic skin treatment regimen on epidermal growth factor receptor-tyrosine kinase inhibitor-induced skin toxicities in patients with metastatic lung cancer. J Clin Oncol 2016;34(8):810-815.
6. Benson AB, Ajani JA, Catalano RB, et al. Recommended guidelines for the treatment of cancer treatment-induced diarrhea. J Clin Oncol 2004;22(14):2918-2926.
7. Antiemesis (Version 2.2016). In: National Comprehensive Cancer Network. Accessed May 2016.8. Cancer- and Chemotherapy-Induced Anemia (Version 2.2016). In: National Comprehensive Cancer
Network. Accessed May 2016.9. Prevention and Treatment of Cancer-Related Infections (Version 1.2016). In: National Comprehensive Cancer
Network. Accessed January 2016.10. Watson CS, Jeng Y, Kochukov M. Nongenomic actions of estradiol compared with estrone and estriol in pituitary
tumor cell signaling and proliferation. FASEB J 2008;22(9):3328-3336.11. Gralow JR, Biermann JS, Farooki A, et al. NCCN Task Force report: bone health in cancer care. J Natl Compr
Canc Netw 2013;11(Suppl 3):S1-50.12. Lexicomp Online®, Lexi-Drugs®, Hudson, Ohio: Lexi-Comp, Inc.; Accessed January 27, 2017.13. Coleman R, Body JJ, Aapro M, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines. Ann
Oncol 2014;25(Suppl 3):iii124-137. 14. Files JA, Ko MG, Pruthi S. Managing aromatase inhibitors in breast cancer survivors. Mayo Clin Proc
2010;85(6):560-566.
Questions and a short break54

2/1/2017
19
Oral oncolytics55
� Why do we care about oral oncolytics?
� 25% of the chemo agents in the research pipeline are
oral
� >30 new oral oncolytics approved since 1998
� 80% of patients would prefer oral oncolytics over other
routes
� How many oral oncolytic agents are available?
� A lot!
J Oncol Pract 2014;doi.10.1200/ JOP.2013.001183.
Introduction: oral oncolytics
� Advantages?
� Convenience
� Non-invasive
� Less complex
� Improved quality of life
� Disadvantages?
� Cost
� Detailed counseling
� Decreased follow up
� Unknown adherence
56
Pharmacy Times website. Updated August 15, 2009. Accessed December 23, 2016.
HANDLING AND STORAGE OF ORAL ONCOLYTICS
Standard precautions
57

2/1/2017
20
Standard precautions58
� The healthcare setting has the largest and most diverse mix of chemicals that are hazardous to humans
� Exposure can arise from
� Surface contamination
� Inhalation
� Ingestion via hand-to-mouth contact
� Injection
The main vector of exposure is dermal contact with drugs/drug packaging and through indirect contact by contaminated surfaces
The Oncology Nurse 2014;7(4):1-17.
Standard precautions59
� A 2003 study documented the presence of drugs and metabolites in the urine of exposed healthcare workers
� Even in those not directly involved in compounding
� Associations have been shown between
� Surface contamination presence of drugs in urine
� Exposure genotoxicity
The Oncology Nurse 2014;7(4):1-17.Int Arch Occup Environ Health 2003;76(1):5-10.
Standard precautions60
� Significance
� Guidelines for safe and appropriate handling are
imperative
� Accidental exposure to oral oncolytics can occur at
various stages during handling
Transport Unpacking Storage Handling Dispensing Administration Disposal
J Oncol Practice 2011;7(1):7-12.

2/1/2017
21
Standard precautions61
� United States Pharmacopeia (USP) Chapter <800>
� Proposed by Compounding Expert Committee and
Compounding with Hazardous Drugs Expert Panel
� Created to identify requirements for hazardous drugs
� Aim to protect
USP website. Accessed January 22, 2017.
Receipt StorageMixing, preparing,
compoundingDispensing Administration
PatientsHealthcare personnel
The environment
Standard precautions62
� USP <800> unpacking and storage
Designate separate areas for unpacking and handling
Hazardous drug (HD) storage
areas and containers should
be labeled as such
Unless in final unit dose
package, store HDs separately
from other inventory
Store, unpack, compound, or manipulate in
negative pressure areas
Do not store HDs on the floor
USP website. Accessed January 22, 2017.
Unpacking may also occur in neutral pressure
areas
Standard precautions63
� USP <800> handling and personal protective equipment (PPE)
Activity Gloves Gown Hair, face, and shoe covers
Eye and face protection
Respiratoryprotection
Receiving intact supplies
+
Transportingintact supplies
+
Stocking +
Non-sterile compounding
+ + +
Spills + + + + +
Receiving brokensupplies
+ + + + +
+=required
USP website. Accessed January 22, 2017.

2/1/2017
22
Standard precautions64
� USP <800> handling and personal protective equipment (PPE)
� Gloves
� Disposal of PPE
USP website. Accessed January 22, 2017.MMWR 2002;51(No. RR-16):1-48.
Powder-free
Perform hand hygiene before donning gloves
AND after removing gloves
Two pairs when compounding, disposing, or
managing a spill
Incinerate at regulated medical waste incinerator
Do NOT place in red bag or sharps
container
Standard precautions65
� USP <800> dispensing
� HDs not requiring alteration before delivery to the patient
may be dispensed without requirements for containment
unless required by manufacturer
Unit of use or unit dose packaging
Transfer from manufacturer’s
package to prescription container
Count HDs carefully, using dedicated, clean
equipment
Do NOT useautomated counting
machines
Counting coated tablets or capsules
does not require compounding hoods or
isolators as long as they are not altered or
brokenUSP website. Accessed January 22, 2017.
Standard precautions66
� USP <800> deactivation, decontamination, cleaning, and disinfection
� Should be appropriate for the type of HD, location, and
surface material
USP website. Accessed January 22, 2017.
Cleaning step Purpose Agents
Deactivation Render compound inert or inactive As listed in HD labelingIf none listed, sodium hypochlorite or EPA-registered oxidizer
Decontamination
Remove inactivated residue Sterile alcohol, sterile water, peroxide, or sodium hypochlorite
Cleaning Remove organic and inorganic material
Germicidal detergent and sterile water
Disinfection Destroy microorganisms Sterile alcohol or EPA-registereddisinfectant
EPA=Environmental Protection Agency

2/1/2017
23
Standard precautions67
� USP <800> disposal
� Comply with all applicable federal and state regulations
� Train all staff who perform routine custodial waste
removal and cleaning activities appropriately
USP website. Accessed January 22, 2017.
Goal = protect staff and the environment to prevent contamination
ORAL ONCOLYTICS
Caregiver and patient counseling
68
Caregiver and patient
counseling69
� Important for providers to
� Components of pharmacist counseling
J Oncol Practice 2011;7(1):7-12.
Review all current medications with the
patient and/or caregiver
Provide clear dosing instructions
Include what to do when a dose is skipped
or if vomiting/spillage occurs
Reassess and discuss medication and food interactions during prescription refill
Provide information on required monitoring, disposal, and side effect management
Provide access to written protocol and
treatment plan from the institution where
treatment was initiated
May come from ambulatory clinic pharmacists or oncologists
Obtain patient consent for oral oncolytics
Consult and assess patient ability to take
oral therapy and comply with their treatment plan

2/1/2017
24
Caregiver and patient counseling: Do’s for oral oncolytics
70
� Review package label, checking medication name and dosage
� Ensure you understand when and how to take the medication
� Administer the medication as instructed
� Transport and store medications as instructed on the label
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.
Caregiver and patient counseling: Do’s for oral oncolytics
71
� Consider pill boxes
� Use separate boxes for oncolytic and non-oncolytic
medications
� Report all medications and dietary requirements to
healthcare providers
� Inform other healthcare providers that you are on an oral
oncolytic
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.
Caregiver and patient counseling: Do’s for oral oncolytics
72
� Use gloves if possible and wash hands thoroughly before and after glove application
� If no gloves, tip tablets and capsules from
container/blister pack directly in disposable medicine
cup
� Caregivers should wear gloves at all times while
handling oral oncolytics and potentially contaminated
items to minimize exposure
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.

2/1/2017
25
Caregiver and patient counseling: Do’s for oral oncolytics
73
� Keep a journal of side effects
� Make a list of side effects for which healthcare providers
have to be contacted immediately
� Report any overdosing immediately
� Return wet, damaged, unused, discontinued, or expired medications to the pharmacist or hospital for disposal
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.
Caregiver and patient counseling: Do’s for oral oncolytics
74
� Keep information ready for necessary action in events of accidental exposure (ex. vomiting or accidental ingestion)
� Minimize number of people who come in contact
with oral oncolytics
� Double-flush the toilet during use of and for 4-7 days after stopping oral oncolytics
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.
Caregiver and patient counseling: Don’ts for oral oncolytics
75
� Leave in open areas, near water, direct sunlight, or in easy access by children or pets
� Store in areas where food or drinks are stored or consumed
� Crush, break, or chew
� Discard down the toilet or in the garbage
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.

2/1/2017
26
Caregiver and patient counseling: Don’ts for oral oncolytics
76
� Double-up on doses, unless instructed by healthcare provider
� Skip doses unless instructed by healthcare provider
� Share medications
� Assume that oral is safer than intravenous chemotherapy
J Oncol Practice 2011;7(1):7-12.US Pharm 2014;39(8):4-7.
General patient and caregiver resources
77
� American Cancer Society
� http://www.cancer.org/treatment/treatments-and-side-
effects/treatment-types/chemotherapy/oral-chemotherapy.html
� Dana-Farber Cancer Institute
� http://www.dana-farber.org/Health-Library/Oral-chemotherapy-
fact-sheet.aspx
� OncoLink
� https://www.oncolink.org/cancer-treatment/chemotherapy/ chemotherapy-safety/taking-oral-anti-cancer-medications-at-
home
� Michigan Society of Hematology & Oncology
� http://www.msho.org/aws/MSHO/asset_manager/get_file/45157
FOOD AND DRUG INTERACTIONS
Pharmacy staff resources
78

2/1/2017
27
Drug or food interaction identification
79
1• Is the oral oncolytic agent new to the patient?
2• Has the patient recently started or stopped any new medications?
3• What medications is the patient taking, including prescription, over the counter,
supplements, herbals, or alternative therapies?
4
• Does any medication induce or inhibit CYP enzymes or P-glycoprotein, interfere with GI absorption, affect immune system function or blood counts, or inhibit the conversion to the active drug?
5
• If unsure of any question above, consult a drug database (Natural Medicines, Lexi-Comp, Micromedex, etc.), primary literature, package insert, and/or oncology pharmacist colleague.
Select interaction: TKIs and CYP inhibitors
80
� Strong inhibitors of CYP3A4 decrease the clearance of all TKIs
� Monitor for increased TKI side effects when CYP
inhibitors are used concomitantly
� Anemia, neutropenia, acneiform rash, nausea, vomiting,
and diarrhea may be increased
� Decreased TKI exposure by CYP enzyme induction may cause clinically relevant ineffectiveness of treatment
Lancet Oncol 2014;15:e315-326. TKI=tyrosine kinase inhibitor
Select interaction: TKIs and other QTc-prolonging medications
81
EKG=electrocardiogram, SSRI=selective serotonin reuptake inhibitor, SNRI=serotonin-norepinephrine
reuptake inhibitor, TCA=tricyclic antidepressant, TKI=tyrosine kinase inhibitor
Blood 2010;doi.org/10.1182/blood-2010-07-294330.
� TKIs commonly cause QTc interval prolongation on EKGs
� Review the patient’s medication list for
� Fluoroquinolones
� Macrolides
� Amiodarone and digoxin
� Metoclopramide
� Azole antifungals
� SSRIs, SNRIs, TCAs, and antipsychotics

2/1/2017
28
Select interaction: tamoxifen and antidepressants
82
� Tamoxifen is converted to it’s active metabolite, endoxifen, by CYP2D6
� SSRIs/SNRIs are inhibitors of CYP2D6
� However, weak inhibitors of CYP2D6 have minimal
effects on the conversion to endoxifen
� For hot flashes associated with tamoxifen
� Recommended venlafaxine, escitalopram, or citalopram
� Weak inhibitors of CYP2D6
BMJ 2010;doi:10.1136/bmj.c693.
SSRI=selective serotonin reuptake inhibitor, SNRI=serotonin-norepinephrine reuptake
inhibitor
Select interaction: TKIs and acid suppressants
83
� Most TKIs require an acidic environment for absorption
� Package inserts and drug databases indicate that
TKIs should not be given with
� PPIs and H2RAs – drug levels may be decreased
� Antacids – okay if given 2 hours before or after the TKI
Lexi-Comp OnlineTM. Accessed January 22, 2017.Lancet Oncol 2014;15:e315-326.
H2RA=histamine-2 receptor antagonist, PPI=proton pump inhibitor, TKI=tyrosine kinase
inhibitor
Increased stomach pH can reduce TKI solubility,
bioavailability, and exposure to the TKI
May result in decreased oncolytic efficacy
In clinical practice, H2RAs may be
given 2 hours after or 10 hours before
TKIs
Food interactions
� As with acid suppressants, the intake of food may alter the pH of the
stomach
� Oral oncolytics have
narrow therapeutic
indices
� Changes in absorption
may lead to harmful
levels or result in
decreased efficacy
84
J Oncol Pract 2014;doi:10.1200/JOP.2013.001183.
Take with food Take on an empty stomach
AltretamineBexaroteneBosutinibCapecitabine
CyclophosphamideExemestaneRegorafenibVorinostat
AbirateroneAfatinibCabozantinibChlorambucil
DabrafenibErlotinibEstramustineLapatinibLomustineMelphalan
MercaptopurineNilotinibPazopanibPomalidomideSorafenibTemozolomide
ThalidomideTrametinibIt is always okay to consult a drug reference
for the most up to date recommendations

2/1/2017
29
Herbals and alternative
medicines85
� May use Natural Medicines database or aboutherbs.com for drug interaction identification
� Consider if any unwanted side effects may exist
Be extremely cautious when recommending herbal medications to patients being treated for cancer
Increased bleeding risk
� Dong quai
� Echinacea
� Fenugreek
� Fish oil
� Garlic
� Ginger
� Ginkgo biloba
� Ginseng
� Green tea
� St. John’s wort
� Valerian
� Vitamin E
� Willow bark
86
Recent Pat Food Nutr Agric 2010;2(1):12-55.
Anticoagulant and
antiplatelet effects
Patients may already be
anemic
Antioxidant activity87
� Cat’s claw
� Coenzyme Q10
� Devil’s claw
� Gingko biloba
� Green tea
� Melatonin
Recent Pat Food Nutr Agric 2010;2(1):12-55.
May counteract chemotherapy
oxidizing effects

2/1/2017
30
Immune stimulating effects88
� Bee pollen
� Bitter melon
� Blue-green algae
� Cat’s claw
� Echinacea
� Ginseng
� Spirulina
Recent Pat Food Nutr Agric 2010;2(1):12-55.
Especially important to avoid in
hematologic malignancies
References89
1. Segal EM, Flood MR, Mancini RS, et al. Oral chemotherapy food and drug interactions: a comprehensive review of the literature. J Oncol Pract 2014;doi:10.1200/JOP.2013.001183.
2. Mahay H. Oral chemotherapy: patient advantages and challenges. Pharmacy Times website: http://www.pharmacytimes.com/publications/issue/2009/august2009/counselingchemotherapy-0809. Updated August 15, 2009. Accessed December 23, 2016.
3. Weingart SN, Brown E, Bach PB, et al. NCCN task force report: oral chemotherapy. JNCCN 2008;6[Suppl 3]:S1-S14.
4. Goodin S, Griffith N, Chen B, et al. Safe handling of oral chemotherapeutic agents in clinical practice: recommendations from an international pharmacy panel. J Oncol Practice 2011;7(1):7-12.
5. Patel S. Safe handling of chemotherapy for pharmacists. US Pharm 2014;39(8):4-7.6. The United States Pharmacopeial Convention. Briefing: <800> Hazardous drugs–handling in healthcare
settings. USP website: http://www.usp.org/sites/default/files/usp_pdf/EN/m7808_pre-post.pdf. Accessed January 22, 2017.
7. Centers for Disease Control and Prevention. Guideline for hand hygiene in health-care settings: recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR 2002;51(No. RR-16):1-48.
8. Roussel C, Connor TH. Chemotherapy: current and emerging issues in safe handling of antineoplastic and other hazardous drugs. The Oncology Nurse 2014;7(4):1-17.
9. Pethran A, Schierl R, Hauff K, Grimm CH, Boos KS, Nowak D. Uptake of antineoplastic agents in pharmacy and hospital personnel. Part I: monitoring of urinary concentrations. Int Arch Occup Environ Health 2003;76(1):5-10.
10. van Leeuwen RWF, van Gelder T, Mathijssen RHJ, Jansman FGA. Drug-drug interactions with tyrosine kinase inhibitors: a clinical perspective. Lancet Oncol 2014;15:e315-e326.
11. Haouala A, Widmer N, Duchosal MA, Montemurro M, Buclin T, Decosterd LA. Drug interactions with the tyrosine kinase inhibitors imatinib, dasatinib, and nilotinib. Blood 2010;doi.org/10.1182/blood-2010-07-294330.
12. Kelly CM, Juurlink DN, Gomes T, et al. Selective serotonin reuptake inhibitors and breast cancer mortality in women receiving tamoxifen: a population based cohort study. BMJ 2010;doi:10.1136/bmj.c693.
13. Yap KY, See CS, Chan A. Clinically relevant chemotherapy interactions with complementary and alternative medicines in patients with cancer. Recent Pat Food Nutr Agric 2010;2(1):12-55.
[email protected]@ohsu.edu