Embed Size (px)
Citation preview

lable at ScienceDirect
Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e7
Contents lists avai
Journal of Cranio-Maxillo-Facial Surgery
journal homepage: www.jcmfs.com
What patients consider important: Temporal variations by earlyand late stage oral, oropharyngeal and laryngeal subsites
Christopher W. Metcalfe, Derek Lowe, Simon N. Rogers*
Regional Head and Neck Unit, University Hospital Aintree, Lower Lane, Liverpool L9 7AL, United Kingdom
a r t i c l e i n f o
Article history:Paper received 4 May 2013Accepted 13 September 2013
Keywords:Health related quality of lifeUW-QOLHead and neck cancerQuestionnairesPatient reported outcomesImportance
* Corresponding author.E-mail addresses: [email protected]
[email protected] (S.N. Rogers).
1010-5182/$ e see front matter � 2013 European Asshttp://dx.doi.org/10.1016/j.jcms.2013.09.008
Please cite this article in press as: Metcalfeoropharyngeal and laryngeal subsites, Journ
a b s t r a c t
Functional outcomes are of high priority to cancer patients and are relevant when considering treatmentstrategies. This study aimed to collate and analyse importance rankings of UW-QOL over time for patientstreated with curative intent for primary head and neck squamous cell carcinoma between 2000 and2010, and to compare early and late stage oral, oropharyngeal and laryngeal subsites. There were 1614patients comprising oral cavity 47% (751), oropharyngeal 24% (382), laryngeal 20% (320) and other HNClocations 10% (161). Items of importance remained relatively stable within clinical groups but there werenotable differences between groups. For patients with early oral tumours no domain was especiallydominant, whereas for late oral tumours swallowing, chewing, speech and saliva were selected moreoften. Swallowing and saliva were more important in oropharyngeal tumours, as was taste with moreadvanced oropharyngeal tumours. Speech and activity were important for those with early laryngealtumours, as were swallowing and speech for more advanced laryngeal tumours. Swallowing and salivawere more important in advanced tumours for all sites. This data confirms the priority patients place onswallowing, chewing, speech, and saliva, therefore curative treatments should optimise these functionswherever possible and provide access to post-treatment interventions as required.
� 2013 European Association for Cranio-Maxillo-Facial Surgery. Published by Elsevier Ltd. All rightsreserved.
1. Introduction
Health related quality of life (HRQOL) is a concept that has risento prominence in recent years, and now has a major role in patientreported outcome assessment following head and neck (H&N)cancer (Rogers et al., 2007). HRQOL outcomes vary with clinicalcharacteristics such as age, gender, cancer type, cancer site, treat-ment methods and time since diagnosis (Rogers et al., 1999, 2010).It is pertinent to include the HRQOL perspective to help planoptimal treatment strategies, gain appreciation of post-treatmentdysfunction, augment patient information around what to expectand assist in the identification of patient concerns. Longitudinalchanges in HRQOL give insight into the variations in patient re-sponses over time and long-term outcomes.
Patient self-completed HRQOL questionnaires can gauge theimpact of disease process and treatment from a number of differentperspectives, including physical, social and emotional aspects(Aaronson et al., 1988). There are a number of questionnaires
ool.ac.uk (C.W. Metcalfe),
ociation for Cranio-Maxillo-Facial
CW, et al., What patients coal of Cranio-Maxillo-Facial Su
currently used for the assessment of HRQOL in head and neckcancer (Kanatas and Rogers, 2008). The University of WashingtonQuality of Life scale (UW-QOL) is widely used and is notable for itsinclusion of patient chosen importance ratings. This unique aspectallows importance to be used in conjunction with the individualscore for each domain and enhances the opportunity for thequestionnaire to be used as a screening tool to help identify pa-tients most in need of support (Rogers and Lowe, 2009). Consid-eration of importance has the potential to increase the sensitivity ofUW-QOL as evenmild dysfunctionmight require intervention if thepatient regards it as important.
Although the UW-QOL has been used in many studies (Larawayand Rogers, 2012) relatively little specific to the domain importanceratings has been published. Rogers et al. (2002a) showed using anearlier version of the UW-QOL (version 2) that patients tended torank speech, swallowing and chewing highly in terms of impor-tance. This 2002 paper focused mainly on oral cancer with a verymodest sample size and longitudinal evaluation only to 1-year. Theaim of this current study was to collate and analyse UW-QOL(version 4) data over time for patients treated with curativeintent for primary head and neck squamous cell carcinoma be-tween 2000 and 2010, and in particular to note importance in earlyand late stage oral, oropharyngeal and laryngeal subsites. Items of
Surgery. Published by Elsevier Ltd. All rights reserved.
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008

C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e72
importance can serve to emphasise key areas of concern reflectedby the questionnaire and inform discussion around strategies tomodify treatments and support to help optimise HRQOL.
2. Material and methods
Patients treated with curative intent for primary head and necksquamous cell carcinoma between 1 January 2000 and 31 Decemer2010were identified from the University Hospital Aintree Head andNeck Cancer database. Patients aged 85 years or older at time ofprimary diagnosis or operation were excluded as were patientswith cutaneous and salivary glandmalignancy or who lived abroad.Mortality status was tracked via the Office of National Statistics(ONS) to 1 September 2012.
The UW-QOL questionnaire is well established (Kanatas andRogers, 2008; Rogers et al., 2007) and from 2000 we used version4, mainly in annual postal surveys. The 12 UW-QOL domains areeach a single question about the past seven days with possibleresponses scaled from 0 (worst) to 100 (best). The UW-QOL alsoasks “Which issues have been themost important to you during thepast 7 days? “, and from a list of the 12 domains the patient is askedto tick up to three that were most important. Earlier work derivedalgorithm criteria by combining domain scores with domainimportance to define cut-off levels beyond which patients could beregarded as having a ‘significant problem’ (Rogers and Lowe, 2009).Reference UW-QOL data from patients routinely attending GDPs isavailable (Rogers et al., 2006a). UW-QOL questionnaires were notknowingly sent to patients with current recurrence or on-goingdisease.
2.1. Statistical analysis
We used all available UW-QOL version 4 data from 2000 to 2012for eligible patients and analysed data within time windows fromprimary diagnosis/operation, namely 3e11 months (first year), 12e23 months (second year), 24e47 months (thirdefourth years) and�48 months (fifth year and beyond). Where patients completedmore than one questionnaire in a time period their results wereaveraged and the average taken forward into the overall calcula-tions which were patient-based. Results were also analysed withinclinical groups defined by tumour site (oral, oropharyngeal, laryn-geal, other H&N) and overall clinical stage (early disease stages 0e2,late disease stages 3e4) based on the clinical tumour, node, andmetastases (TNM) classification (Sobin and Wittekind, 2002). Thechi-squared test compared these clinical groups in other charac-teristics at the time of primary diagnosis/surgery. KaplaneMeierestimates of survival were performed, with the log-rank test usedto compare survival curves. Patient and clinical characteristics wereconsidered jointly in binary regressionmodelling to predict domainimportance, with separate regressions run for each domain and allfactors included in each model. Risk ratios (i.e. relating to the ‘risk’of a patient selecting a domain as ‘important’) were obtained usingthe ‘binreg’ procedure within STATA software v11. Robust estimatesof standard error enabled an adjustment for patient clustering ofdata to be made to the P values associated with the risk ratios. A‘pseudo’ R2 statistic ranging between 0 and 1 was also obtainedusing the ‘logistic’ procedurewithin STATA to give some estimate ofhow much variability in importance was explained by the ‘pre-dictor’ factors in the model. This statistic is more helpful forinterpreting a model relative to another model (as is done in thispaper) rather than in terms of its absolute value per se. More basicstatistical analyses were performed using SPSS software v19.Missing data are reflected by changes in denominator. The hospitalClinical Audit Department approved the collection of the UW-QOLoutcomes as part of audit and service evaluation.
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
3. Results
There were 1614 patients in the 2000e2010 primary and cura-tive treatment cohort, with mean (SD) age of 62 (11) years and 70%(1133) male. Tumour site was oral cavity for 47% (751), oropha-ryngeal 24% (382), laryngeal 20% (320) and other HNC locations 10%(161). Overall clinical staging was advanced stage 3e4 for 52% (830/1587). Primary treatment was surgery alone for 44% (716), surgerywith adjuvant radiotherapy (RT) for 32% (514) and (chemo) RTalone for 24% (384). Of those treated with surgery 42% (502/1188)had free-flaps (338 soft, 164 composite). KaplaneMeier estimatesfor all-causes survival were 85% (SE 1%) at 12months, 75% (SE 1%) at24 months and 59% (SE 1%) at 60 months. Patient and clinicalcharacteristics of the 7 clinical subgroups inherent to this report aresummarised in Table 1. Missing data meant that 1.4% (23) of the1614 could not be placed into one of these subgroups.
Two-thirds (1081/1614) of patients completed 3975 UW-QOLquestionnaires during their cancer journeys; 219 (278 question-naires) were <3 months from diagnosis or operation mainlybaseline, 520 (699) were within 3e11 months, 666 (821) within12e23 months, 646 (1095) within 24e47 months, and 389 (1082)were�48months. Adjusting for follow-up under 24 and 48monthsand for overall survival rates at 0, 3, 12, 24 and 48 months then thepercentage of patients with QOL data within each time period wasestimated at 14%, 33%, 48%, 56% and 54% respectively. There were398 patients with QOL data in one time period only, 232 in two, 267in three, 143 in 4 and 41 in all five. The percentage with any QOLdata was notably lower than the overall 67% in certain subgroups eelderly patients 75e84 years at 58%, non-surgically treated patientsat 48% and patients with late laryngeal tumours at 49%. Domainimportance was known for 3934 questionnaires.
UW-QOL importance by domain over time is summarisedwithin clinical group in Table 2. There was a general lack of trendover time in that importance remained relatively stable within eachclinical group. However there were notable differences betweenclinical groups. For patients with early oral tumours no domainwasespecially dominant, whereas for late oral tumours swallowing,chewing, speech and saliva were selected more often than otherissues. Swallowing and saliva were more important domains forthose with oropharynx tumours, as was taste with more advancedoropharynx tumours. Speech was the dominant issue for thosewith early tumours of the larynx, along with activity, whilst formore advanced laryngeal tumours swallowing and speech werenotably important. For each tumour site, patients with later stagedtumours regarded swallowing and saliva as more important thanpatients with earlier tumours.
Domain importance over time is shown for all patients in Table 3including baseline data. Other than a decrease in the importance ofpain and anxiety and an increase regarding saliva during theearliest months of follow-up, there was, across all domains fromabout 12 months into the cancer journey, a general flatness orstability of the whole group in regard to domain importance. Thiswas seen also for the 184 patients with data in 4 or all 5 timewindows (results not shown). The GDP reference data provides acomparison with patients routinely attending 10 high street dentalpractices. H&N cancer patients regarded issues of oral function andshoulder function as more important than other domains whencompared to the non-cancer GDP group, whilst other issues of pain,appearance, activity, recreation, mood and anxiety were viewed asless important.
For 904 patients with UW-QOL data (2940 questionnaires) atleast 12 months into follow-up, binary regression was used tomodel importance (Yes/No) of each domain in relation to theclinical and patient factors of Tables 1 and 2. Patient and clinicalfactors were considered jointly in the regression model to predict
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008

Table 1Clinical group characteristics relating to primary treatment.
Tumour location Oral Oral Oropharynx Oropharynx Larynx Larynx Othersa
Overall clinical stage Early 0e2 Late 3e4 Early 0e2 Late 3e4 Early 0e2 Late 3e4
No. of patients 409 335 109 271 218 94 155Male 56% (230) 66% (220) 59% (64) 79% (214) 89% (193) 81% (76) 75% (117)Mean (SD) Age 63 (12) 63 (11) 60 (10) 58 (10) 66 (10) 63 (9) 60 (10)65e84 years 42% (173) 41% (138) 30% (33) 26% (70) 53% (115) 40% (38) 31% (48)Primary treatmentSurgery & RT 15% (62) 54% (181) 26% (28) 42% (113) 9% (19) 46% (43) 43% (66)Surgery alone 81% (330) 30% (99) 56% (61) 17% (46) 50% (110) 22% (21) 23% (35)Chemo/RT alone 4% (17) 16% (55) 18% (20) 41% (112) 41% (89) 32% (30) 35% (54)Free-flap (if surgery)No free-flap 67% (260) 14% (39) 60% (52) 54% (82) 97% (121) 88% (53) 75% (71)Soft 29% (113) 39% (106) 36% (31) 41% (62) 2% (3) 10% (6) 16% (15)Composite 4% (14) 47% (129) 3% (3) 5% (7) 1% (1) 2% (1) 9% (9)% Survival (SE) at 12 months 92% (1%) 69% (3%) 92% (3%) 86% (2%) 94% (2%) 83% (4%) 88% (3%)% Survival (SE) at 24 months 85% (2%) 55% (3%) 85% (3%) 74% (3%) 88% (2%) 66% (5%) 75% (4%)% Survival (SE) at 60 months 70% (3%) 40% (3%) 67% (5%) 61% (3%) 69% (4%) 49% (6%) 59% (5%)
The Chi-squared test compared the 7 groups, apart from the log-rank test which compared survival curves. All tests were P < 0.001.a 21 of the 155 were stage 0e2, 134 were stage 3e4. Others (155) included pyriform fossa (46), metastatic lymph nodese primary unknown (26), hypopharynx (16), necke
occult primary (15), epiglottis (9), maxillary sinus (8), nasopharynx (8).
C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e7 3
importance. Risk ratio estimates for each factor were computedafter adjusting for other factors in the model (Table 4). Risk ratioswere also computed relative to a reference category for each factor;e.g. females were less likely to regard activity as important thanmales (the reference category), risk ratio 0.68, P < 0.01 all otherfactors remaining unchanged. Age was thus an important predictorfor several domains but with the direction of association varying bydomain. For pain, shoulder function, mood and anxiety the olderthe patient the less important the domain, whilst for activity,chewing and taste the older the patient the more important thedomain. For swallowing and saliva, where there was no notableassociation with age there was increased importance after treat-ment by radiotherapy relative to using surgery alone. Swallowingwas of increased importance with oropharyngeal and late laryngealtumours (relative to early oral tumours), as was speech withlaryngeal tumours. Also notable from Table 4 is the lack of associ-ation with time after 12 months.
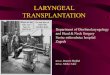
Binary regressionwas also used to model domain importance inrelation to domain score (Table 5). All available UW-QOL data wereincluded. Risk ratios were computed relative to the best possibledomain scores of 100; e.g. patients scoring ‘75’ for pain were 5.5times more likely to regard pain as important as patients scoring‘100’, patients scoring ‘50’ were 17.8 times more likely, and so on.These risk ratios were often large reflecting big absolute differencesin importance between domain scores. The ‘pseudo’ R2 statisticfrom the regression modelling (see last row of Table 5) gives arough idea of how much variability in domain importance wasexplained by knowing the domain score. These can be comparedwith similar statistics in the last row of Table 4. What theydemonstrate is the much stronger relationship between domainscore and domain importance for pain, swallowing, chewing,shoulder and saliva than for other domains. With the exception ofactivity and recreation the association between domain score anddomain importance is stronger than the association seen betweenthe combined clinical factors and domain importance.
Descriptive results by domain score are shown in Table 6. It wasthe relationship between domain score and importance that droveearlier work (Rogers and Lowe, 2009) to define algorithm criteria tohighlight patients with clinically ‘significant’ problems. Coupledwith scrutiny of the wording of domain questions the intentionwasto create cut-offs in the data to identify the worst affected 10e20%of patients. Table 6 shows that this original purpose has beenmaintained over a much larger number of questionnaires.
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
4. Discussion
This is a detailed evaluation of UW-QOLv4 domain importanceranking in head and neck cancer. The use of questionnaires over aten-year period provided a substantial sample size, which allowedfor meaningful comparisons across subsite and stage of cancer. Themain method of data collection was an annual survey which hasresulted in a relatively smaller percentage of patients with data atless than 12 months. Response rates beyond one-year were morereasonable. In contrast to previous work (Rogers et al., 2002a) thisstudy used version 4 of the UW-QOL throughout so, rather thanscale each item 1e5 in terms of importance (UW-QOL version 2),patients are asked to select up to 3 items which have beenimportant in the past 7 days. UW-QOLv4 includes mood and anx-iety domains (Rogers et al., 2002b); 2 items which were lacking inUW-QOLv2, and this allows a comparison of how psychological andphysical domains, such as speech and swallowing, are ranked interms of importance. The interpretation of the data presented inthis paper needs to be considered with some caution as the samplecomprised patients treated at one H&N cancer centre only andalthough treatment methods are consistent across subsites andstage based on MDT protocols, they may not be reflective of otherunits. Some units might have a much higher proportion beingmanaged by a non-surgical approach (chemoradiotherapy). Theassessment of importance is also limited to the 12 domains of theUW-QOL. Patients can only flag up to 3 of these items as importantwhichmeans there could have been additional domains consideredimportant by the patient that were not recorded. This may be anadvantageous feature as, by forcing the patient to choose only 3items, it makes them focus on the 3 items which really are the mostimportant to them. Also, the concept of importance is limited by theUW-QOL construct as the literature suggests that priority is givenby patients to survival and cure, rather than the physical aspects ofdisease included in UW-QOL (Sharp et al., 1999; List et al., 2000; Gillet al., 2011).
There are variations in which items patients consider impor-tant over time but this is only exhibited in the earliest months offollow-up; beyond 12 months domain importance remains fairlystable across the whole group. The importance of swallowing,chewing and speech remain persistently high after treatment. Forswallowing and saliva there was no notable association with agebut there was increased importance after treatment by radio-therapy compared to surgery alone. This strengthens the case
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008

Table 2UW-QOL importance (%) by clinical group by time along the cancer journey.
Time period Clinical group (tumour location/overall clinical stage)
Oral Oral Oropharynx Oropharynx Larynx Larynx Others
Early 0e2 Late 3e4 Early 0e2 Late 3e4 Early 0e2 Late 3e4
N of patients with UW-QOL questionnairesin time period (adjusted response %)
3e11m 187 (46%) 124 (40%) 37 (35%) 84 (32%) 48 (22%) 8 (9%) 30 (20%)12e23m 234 (62%) 116 (50%) 51 (51%) 113 (49%) 76 (37%) 23 (29%) 48 (35%)24e47m 217 (65%) 116 (64%) 49 (56%) 106 (57%) 77 (43%) 20 (33%) 58 (54%)48mþ 127 (56%) 70 (60%) 26 (49%) 60 (54%) 49 (46%) 19 (62%) 35 (57%)
N of UW-QOL questionnairesin time period (median time in months)
3e11m 286 (7m) 172 (7m) 48 (8m) 100 (8m) 48 (8m) 10 (9m) 33 (9m)12e23m 305 (17m) 157 (18m) 69 (18m) 132 (18m) 77 (18m) 24 (17m) 52 (18m)24e47m 408 (34m) 201 (34m) 91 (34m) 174 (34m) 110 (33m) 29 (33m) 78 (32m)48mþ 402 (69m) 222 (71m) 69 (71m) 176 (69m) 100 (69m) 39 (66m) 68 (66m)
% ImportantPain 3e11m 18 21 22 24 6 25 22
12e23m 13 14 22 12 4 33 2224e47m 15 19 29 19 12 25 2148mþ 15 14 17 15 8 8 24
Appearance 3e11m 16 21 14 12 10 17 1712e23m 14 21 19 8 8 13 2324e47m 16 28 16 10 15 23 2548mþ 16 29 5 9 16 18 28
Activity 3e11m 14 10 12 10 31 38 3812e23m 16 16 14 15 27 17 2324e47m 18 10 17 14 25 18 2748mþ 17 12 6 11 35 35 29
Recreation 3e11m 6 8 4 4 15 0 1012e23m 5 6 11 6 20 0 1524e47m 10 6 10 7 21 10 1448mþ 10 6 2 2 26 3 16
Swallowing 3e11m 20 39 45 64 13 75 3812e23m 17 34 42 48 16 61 5024e47m 19 37 40 54 20 47 3648mþ 21 35 34 50 13 54 35
Chewing 3e11m 24 37 23 17 8 21 1912e23m 22 30 19 21 5 20 724e47m 20 27 22 24 8 10 948mþ 13 30 26 18 3 12 15
Speech 3e11m 21 29 34 16 38 29 2112e23m 22 31 20 12 38 30 1924e47m 21 30 14 13 38 38 1448mþ 17 23 16 19 25 41 19
Shoulder 3e11m 12 13 18 24 6 21 2812e23m 16 12 17 14 11 13 1824e47m 12 9 16 18 9 12 1648mþ 18 9 22 21 10 27 20
Taste 3e11m 13 20 16 34 6 13 312e23m 13 10 19 30 7 9 924e47m 13 18 10 21 13 10 1148mþ 10 13 17 16 10 7 11
Saliva 3e11m 26 38 36 54 25 13 4812e23m 21 40 37 60 14 30 3824e47m 24 41 41 66 19 38 4248mþ 29 33 41 70 16 23 34
Mood 3e11m 15 17 7 5 19 38 712e23m 17 12 15 13 19 26 1224e47m 16 12 15 9 16 25 1948mþ 11 11 12 7 13 22 17
Anxiety 3e11m 19 20 14 16 13 13 2112e23m 14 16 19 9 23 17 1724e47m 15 17 19 5 12 15 1348mþ 12 16 22 7 12 8 12
C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e74
for withholding adjuvant radiotherapy when considering treat-ment in patient groups with an intermediate risk of recurrence(Bekiroglu et al., 2011) and for the use of Intensity-ModulationRadiation Therapy (IMRT) (Rathod et al., 2013) in thoserequiring radiotherapy, in order to preserve saliva function.Overall the least important of the 12 items across the wholesample was recreation, whilst the two most important wereswallowing and saliva with the rest similarly ranked in between.For mood and anxiety it has already been demonstrated thatpsychological distress in H&N cancer patients can be picked up
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
with both UW-QOL (Rogers et al., 2006b) and PCI (Kanatas et al.,2012). There were subtle difference in what items patients rankedas important by gender and age. Risk ratios suggest that femaleswere less likely to regard activity as important than males. Forpain, shoulder function, mood and anxiety the older the patientthe less important the domain, whilst for activity, chewing andtaste the older the patient the more important the domain. Whenthese data are contrasted with data from GDPs (Table 3) it can beseen that the priorities of head and neck cancer patients are oftenfunctional (swallowing, chewing, saliva) rather than related to
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008

Table 3UW-QOL importance by time along the cancer journey, with GDP reference datafrom patients routinely attending high street dentists.
<3m 3e11m 12e23m 24e47m 48þm GDPreference
No. of UW-QOLquestionnaires
278 699 821 1095 1082 349
No. of patients 219 520 666 646 389 349% ImportantPain 34 19 14 18 15 35Appearance 16 16 14 18 18 30Activity 15 16 18 18 19 35Recreation 4 7 8 10 10 23Swallowing 27 34 31 32 30 5Chewing 28 24 20 19 16 11Speech 18 25 24 22 21 17Shoulder 10 15 14 13 17 7Taste 11 17 15 15 12 6Saliva 12 35 33 37 35 5Mood 18 13 15 14 12 26Anxiety 29 18 15 13 12 24
C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e7 5
appearance, activity and pain which is perhaps secondary tocoping strategies related to their disease.
Consideration of findings by cancer subsite (Tables 1 and 2)exhibited a number of variations in importance ratings. Early oralcancer was treated primarily by surgery alone and advanced oralcancer treated by surgery with or without adjuvant radiotherapy.Both early and late oral showed many similarities in importanceacross the domains except swallowing, chewing, speech and salivawhich were considered more important in advanced cancers; anobservation which probably reflects the use of radiotherapy in latestage tumours. Chewing in late oral cancer was identified asimportant more often than both oropharyngeal and laryngealsubsites which is reflective both of the site, and the use of radio-therapy. After having adjusted for other factors such as age and
Table 4Risk ratios for patient and clinical factors in relation to UW-QOL domain importance,modelling, 904 patients with 2904 UW-QOL questionnaires.
Pain Appearance Activity Recreation
Gender Male 1.00 1.00 1.00 1.00Female 1.07 1.35 0.68 0.67
Age <55 1.00 1.00 1.00 1.0055e64 0.67 0.79 1.05 0.8965e74 0.57 0.58 1.30 1.3275e84 0.27 1.08 1.78 1.14
Primary treatment Surgery alone 1.00 1.00 1.00 1.00Surgery & RT 1.04 1.01 0.85 0.81Chemo/RT alone 0.90 0.63 0.54 0.71
Free-flap (if surgery) No free-flap 1.00 1.00 1.00 1.00Soft 0.93 0.60 0.54 0.66Composite 0.99 0.71 0.53 0.68
Clinical groupbased on tumoursite and overallclinical grade
Oral Early 0e2 1.00 1.00 1.00 1.00Oral Late 3e4 1.48 1.23 0.61 0.64OropharynxEarly 0e2
1.56 0.74 0.87 1.04
OropharynxLate 3e4
1.01 0.69 0.85 0.62
Larynx Early 0e2 0.98 1.01 1.43 2.41Larynx Late 3e4 1.74 1.27 1.67 0.73Other H&N 1.81 1.54 1.76 1.94
Time from primarydiagnosisor operation
12e23m 1.00 1.00 1.00 1.0024e47m 1.19 0.72 0.89 0.8748þm 1.45 0.96 0.89 1.00PseudoRSQUARED
0.0361 0.0397 0.0389 0.0578
Risk ratios at P < 0.01 are highlighted; risk ratios at P < 0.001 are highlighted and undeRisk ratios are computed relative to a reference category for each factor: i.e. males, <55 ythe table with the reference category having the value 1.00 assigned to it.
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
treatment differences only pain was significantly more importantin late oral cancer (Table 4).
For early oropharyngeal cancer there was a tendency to usesurgery alone whilst treatment of late stage usually involved sur-gery with adjuvant radiotherapy or radiotherapy/chemo-radiotherapy alone. Saliva was considered extremely important forthis subsite in both early and late stages, which perhaps relates tothe large proportion of patients receiving radiotherapy. The swal-lowing domain in oropharyngeal cancer was also identified asimportant in both early and late stages after adjustment for otherpredictors.
Treatment for early laryngeal cancer involved either surgeryalone or radiotherapy/chemoradiotherapy, whilst for late laryngealcancer treatment was more evenly distributed across the threestrategies. Higher importance was observed for recreation in earlylaryngeal cancer when compared to other subsites. For the swal-lowing domain a notable difference was observed between earlyand late stage larynx and remained significantly higher in advanceddisease after adjustment for other factors. Speech was identified asmore important in both early and late stages after adjustment forother factors.
Domain score was related to importance as patients withdysfunction tended to rate the item as important, particularly withregards to pain, swallowing, chewing, shoulder and saliva (Table 5).The domain score was more likely to reflect patient ranking ofimportance than clinical characteristics. This is shown dramaticallyin Table 6, where for example pain was flagged as important in 85%when scoring ’I have severe pain, not controlled by medication’,progressively dropping to only 2% when scoring ‘I have no pain’.These data also reinforce the domain algorithms (Rogers and Lowe,2009), whereby domain score and importance are combined toreflect significant disability.
Importance rating can be use to facilitate screening for sig-nificant problems following H&N cancer (Rogers and Lowe, 2009).
from 12 months on along the cancer journey, as obtained from binary regression
Swallowing Chewing Speech Shoulder Taste Saliva Mood Anxiety
1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.001.00 0.77 0.92 0.76 0.80 0.95 1.19 1.351.00 1.00 1.00 1.00 1.00 1.00 1.00 1.001.13 1.46 1.34 0.79 1.45 1.03 0.70 0.581.08 1.69 1.24 0.61 2.07 1.13 0.36 0.311.10 1.80 1.03 0.63 2.23 0.81 0.32 0.371.00 1.00 1.00 1.00 1.00 1.00 1.00 1.001.81 1.00 1.31 0.80 1.18 1.49 0.78 0.651.88 1.22 0.45 0.85 1.05 1.90 0.51 1.091.00 1.00 1.00 1.00 1.00 1.00 1.00 1.000.97 0.70 0.64 1.73 0.80 0.98 0.82 1.111.18 1.16 0.94 1.94 0.66 1.02 0.68 1.061.00 1.00 1.00 1.00 1.00 1.00 1.00 1.001.26 1.34 0.96 0.79 0.88 1.12 0.87 1.541.77 1.34 0.82 1.31 1.05 1.38 0.78 1.29
1.69 0.99 0.86 1.20 1.60 1.64 0.69 0.54
0.74 0.29 1.97 0.88 0.69 0.47 1.50 1.412.01 0.97 2.10 1.22 0.68 0.82 1.49 0.951.31 0.54 0.83 1.53 0.72 0.89 1.31 0.991.00 1.00 1.00 1.00 1.00 1.00 1.00 1.001.07 1.29 0.97 0.90 1.28 0.91 1.31 1.351.05 1.27 0.94 0.81 1.25 0.95 1.21 1.110.0849 0.0573 0.0469 0.0360 0.0355 0.0943 0.0399 0.0560
rlined.ears, surgery alone, No free-flap, Oral Early 0e2, 12e23m for the predictor factors in
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008
Table 5Risk ratios for UW-QOL domain importance by UW-QOL domain importance, using all available UW-QOL data along the cancer journey, as obtained from binary regressionmodelling, from 1081 patients with 3975 UW-QOL questionnaires.
Pain Appearance Activity Recreation Swallowing Chewing Speech Shoulder Taste Saliva Mood Anxiety
Domainscore
100 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.0075 5.50 1.78 1.24 1.07 2.6370 7.03 6.58 48.6 3.01 5.50 7.4450 17.8 4.29 1.72 0.66 7.48 4.2130 10.1 10.44 80.4 5.78 10.03 15.725 33.3 4.95 1.70 1.38 8.030 38.7 1.85 1.90 0.30 10.0 5.88 8.09 99.4 7.05 10.27 8.47 23.1
PseudoRSQUARED
0.3170 0.0776 0.0114 0.0063 0.2275 0.1341 0.1643 0.3519 0.0978 0.2411 0.1099 0.1646
Risk ratios at P < 0.01 are highlighted; risk ratios at P < 0.001 are highlighted and underlined.Risk ratios are computed relative to a reference category e a domain score of ‘100’ e this reference category having the value 1.00 assigned to it.
Table 6Domain importance (%) in relation to UW-QOL domain score, using all available UW-QOL data along the cancer journey, as obtained from binary regression modelling, 1081patients with 3975 UW-QOL questionnaires.
Possible UW-QOL scores for UW-QOL domains Algorithm criteriaa for‘significant’ problem
% with‘significant’problem
0 25 30 50 70 75 100
Pain 85% (34/40) 73%(170/233)
39% (324/830) 12%(102/845)
2% (43/1960) 0, 25, 50 if important 15% (597/3908)
Appearance 16% (3/19) 42%(58/137)
37% (242/659) 15%(261/1714)
9% (119/1391) 0, 25, 50 if important 10% (398/3920)
Activity 23% (14/62) 20%(19/94)
20% (298/1460) 15%(166/1125)
12% (140/1177) 0, 25, 50 if important 12% (454/3918)
Recreation 2% (1/42) 11%(25/226)
5% (36/684) 9%(146/1698)
8% (101/1261) 0, 25, 50 if important 8% (304/3911)
Swallowing 65% (112/171) 66% (281/424) 46%(711/1544)
7% (116/1771) 0, 30 15% (595/3910)
Chewing 27% (130/485) 34% (599/1756) 5% (74/1622) 0 13% (485/3863)Speech 42% (14/33) 55% (155/283) 35%
(619/1793)5% (93/1773) 0, 30 8% (316/3882)
Shoulder 56% (102/183) 45% (228/506) 27%(232/851)
1% (13/2318) 0, 30 if important 11% (411/3858)
Taste 32% (78/244) 26% (191/729) 14%(157/1151)
5% (80/1764) 0, 30 if important 11% (435/3888)
Saliva 69% (221/321) 67% (518/770) 37%(446/1220)
7% (104/1551) 0, 30 if important 22% (839/3862)
Mood 40% (32/80) 38%(167/440)
20% (72/362) 12%(186/1499)
5% (72/1524) 0, 25, 50 if important 15% (592/3905)
Anxiety 54% (92/171) 37% (165/450) 17%(307/1772)
2% (35/1503) 0, 30 16% (621/3896)
a Derived from earlier work (Rogers and Lowe, 2009). Also see related text and Methods.
C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e76
This can be further enhanced by the use of the Patient ConcernsInventory (PCI) in routine clinical practice (Rogers et al., 2009;Kanatas et al., 2012, 2013). Ghazali et al. took this a step furtherwith the introduction of a BettereStableeWorse question aftereach domain of the UW-QOL which was shown to add littlequestionnaire burden and allow more effective identification ofissues for discussion during outpatient clinics (Ghazali et al.,2012).
Other validated questionnaires are available for the assessmentof QOL in H&N cancer however UW-QOL is unique in its inclusion ofimportance. Other head and neck specific questionnaires includeEORTC Quality of Life Head and Neck 35 (Bjordal and Kaasa, 1992),Functional Assessment of Cancer Therapy e Head and Neck Sub-scale (List et al., 1990) and H&N Oncology Health Status Assessment(Funk et al., 2003); whilst other patient related outcome measuresnot specific to H&N cancer, such as the Hospital Anxiety andDepression Scale (HAD) are also useful in QOL assessment (Snaithand Zigmond, 1986). EORTC QLQ-H&N35 in particular is a vali-dated and widely used tool which has been implemented over timeto show areas of dysfunction in H&N cancer patients. López-Jornetet al. (2012) reported on QOL using QLQ-H&N35 for 94 patients over
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
3 years and reinforced findings from this study showing that bothage and sex have implications for patient reported QOL. Abovefindings relating to saliva problems in oropharyngeal cancertreated by radiotherapy have also been identified with EORTC QLQ-H&N35 (Broglie et al., 2013). The large sample size of this paper isadvantageous, allowing extensive comparison of subsites andstages and exploration of variations over time.
5. Conclusion
In summary, results from this study have underlined the value ofincluding domain importance ratings in the UW-QOL to betterunderstand the impact of treatment for patients. Dysfunction re-lates strongly to importance across all three subsites (oral,oropharyngeal, laryngeal) and therefore the aim of treatmentshould focus on strategies to minimise functional deficits whilstmaintaining survival.
Conflict of interestThe authors have no conflict of interest to declare.
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008

C.W. Metcalfe et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e7 7
References
Aaronson NK, Bullinger M, Ahmedzai S: A modular approach to quality-of-lifeassessment in cancer clinical trials. Recent Results Cancer Res 111: 231e249,1988
Bekiroglu F, Ghazali N, Laycock R, Katre C, Lowe D, Rogers SN: Adjuvant radio-therapy and health-related quality of life of patients at intermediate risk ofrecurrence following primary surgery for oral squamous cell carcinoma. OralOncol 47(10): 967e973, 2011
Bjordal K, Kaasa S: Psychometric validation of the EORTC Core Quality of LifeQuestionnaire, 30-item version and a diagnosis-specific module for head andneck cancer patients. Acta Oncol 31: 311e321, 1992
Broglie MA, Soltermann A, Haile SR, Röösli C, Huber GF, Schmid S, et al: Quality oflife of oropharyngeal cancer patients with respect to treatment strategy andp16-positivity. Laryngoscope 123(1): 164e170, 2013
Funk GF, Karnell LH, Christensen AJ, Moran PJ, Ricks J: Comprehensive head andneck oncology health status assessment. Head Neck 25: 561e575, 2003
Ghazali N, Lowe D, Rogers SN: Enhanced patient reported outcome measurementsuitable for head and neck cancer follow-up clinics. Head Neck Oncol 4: 32,2012
Gill SS, Frew J, Fry A, Adam J, Paleri V, Dobrowsky W, et al: Priorities for the headand neck cancer patient, their companion and members of the multidisci-plinary team and decision regret. Clin Oncol (R Coll Radiol) 23(8): 518e524,2011
Kanatas AN, Rogers SN: A guide of the questionnaires used in the measurement ofhealth-related quality of life in head and neck oncology. Tumori 94(5): 724e731, 2008
Kanatas A, Ghazali N, Lowe D, Rogers SN: The identification of mood and anxietyconcerns using the patients concerns inventory following head and neck cancer.Int J Oral Maxillofac Surg 41(4): 429e436, 2012
Kanatas A, Ghazali N, Lowe D, Udberg M, Heseltine J, O’Mahony E, et al: Issuespatients would like to discuss at their review consultation: variation by earlyand late stage oral, oropharyngeal and laryngeal subsites. Eur Arch Oto-rhinolaryngol 270(3): 1067e1074, 2013
Laraway DC, Rogers SN: A structured review of journal articles reporting outcomesusing the University of Washington Quality of Life Scale. Br J Oral MaxillofacSurg 50: 122e131, 2012
List MA, Ritter-Sterr C, Lansky SB: A performance status scale for head and neckcancer patients. Cancer 66: 564e569, 1990
List MA, Stracks J, Colangelo L, Butler P, Ganzenko N, Lundy D, et al: How do headand neck cancer patients prioritize treatment outcomes before initiatingtreatment? J Clin Oncol 18(4): 877e884, 2000
López-Jornet P, Camacho-Alonso F, López-Tortosa J, Palazon Tovar T, Rodríguez-Gonzales MA: Assessing quality of life in patients with head and neck cancer in
Please cite this article in press as: Metcalfe CW, et al., What patients cooropharyngeal and laryngeal subsites, Journal of Cranio-Maxillo-Facial Su
Spain by means of EORTC QLQ-C30 and QLQ-H&N35. J Craniomaxillofac Surg40(7): 614e620, 2012
Rathod S, Gupta T, Ghosh-Laskar S, Murthy V, Budrukkar A, Agarwal J: Quality-of-life (QOL) outcomes in patients with head and neck squamous cell carcinoma(HNSCC) treated with intensity-modulated radiation therapy (IMRT) comparedto three-dimensional conformal radiotherapy (3D-CRT): evidence from a pro-spective randomized study. Oral Oncol, 2013 pii: S1368-8375(13)00060-202.013
Rogers SN, Hannah L, Lowe D, Magennis P: Quality of life 5e10 years after primarysurgery for oral and oro-pharyngeal cancer. J Craniomaxillofac Surg 27(3): 187e191, 1999
Rogers SN, Laher S, Overend L, Lowe D: Domain importance-rating using the UW-QOL questionnaire in patients treated by primary surgery for oral andoropharyngeal cancer. J Craniomaxillofac Surg 30(2): 125e132, 2002a
Rogers SN, Gwane S, Lowe D, Humphris G, Yueh B, Weymuller EA: The addition ofmood and anxiety domains to the University of Washington Quality of LifeScale. Head Neck 24: 521e529, 2002b
Rogers SN, O’Donnell JP, Williams- Hewitt S, Christensen J, Lowe D: Health-relatedquality of life measured by the UWQOL e reference values from a generaldental practice. Oral Oncol 42(3): 281e287, 2006a
Rogers SN, Rajlawat B, Goru J, Lowe D, Humphris GM: Comparison of the domains ofanxiety and mood of the University of Washington Head and Neck CancerQuestionnaire (UW-QOL V4) with the CES-D and HADS. Head Neck 28(8): 697e704, 2006b
Rogers SN, Ahad SA, Murphy AP: A structured review and theme analysis of paperspublished on ‘quality of life’ in head and neck Cancer: 2000 to 2005. Oral Oncol43(9): 843e868, 2007
Rogers S, Lowe D: Screening for dysfunction to promote multidisciplinary inter-vention by using the University of Washington Quality of Life Questionnaire.Arch Otolaryngol Head Neck Surg 135(4): 369e375, 2009
Rogers SN, El-Sheikha J, Lowe D: The development of a Patients Concerns Inventory(PCI) to help reveal patients concerns in the head and neck clinic. Oral Oncol45(7): 555e561, 2009
Rogers SN, Lowe D, Yueh B, Weymuller Jr EA: The physical function and social-emotional function subscales of the University of Washington Quality of LifeQuestionnaire. Arch Otolaryngol Head Neck Surg 136(4): 352e357, 2010
Sharp HM, List M, MacCracken E, Stenson K, Stocking C, Siegler M: Patients’ pri-orities among treatment effects in head and neck cancer: evaluation of a newassessment tool. Head Neck 21(6): 538e546, 1999
Snaith RP, Zigmond AS: The hospital anxiety and depression scale. Br Med J (ClinRes Ed) 292: 344, 1986
Sobin L, Wittekind Ch (eds), TNM classification of malignant tumours, 6th edn. NewYork: Wiley-Liss, 99e103, 2002
nsider important: Temporal variations by early and late stage oral,rgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.09.008