Embed Size (px)
Citation preview
10262015
1
- -
What Why How about
Dry Eye Disease
Management
Paul M Karpecki OD FAAO
Director of the OSD Center at KVG
Lexington KY
- -
Paul M Karpecki OD FAAO Financial Disclosures
iCare USA
Imprimis
JampJ
Konan Medical
MacuLogix
Oculus
Beaver Visitech
OM Solutions
Ocular Solutions
Reichert
Shire Pharmaceuticals
Science Based Health
TearLab
TearFilm Innovations
TLC Vision
Topcon
Vmax
AMO
Alcon Labs
Allergan Inc
Akorn
Arctic Dx
Bausch amp Lomb Inc
BioTissue
Bruder Healthcare
Ocusoft
Essilor
SightRisk
Focus Laboratories
Nicox
Rigel Pharma
Eleven BioTherapeutics
Freedom Meditech
- -
Ocular Surface Disease
ndash 20 years since starting my first dry eye clinic
ndash 14 of those years werehellip frustrating
Dry Eye Disease Understanding has Changed
- -
Predisposing factors
bull Age
bull Gender
bull Environment
bull Anterior
Segment
Disease
bull Medications
bull CL Wear
bull Refractive or
cataract surgery
bull Systemic Disease
- -
Gender
bull Sjogrenrsquos Dry eye is characterized by a triad
of dry eye dry mouth and associated auto-
immune disorders
bull Prevalence
ndash 04
ndash 85 women
- -
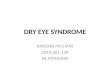
Prevalence of Dry Eye (continued)
Prevalence by Age and Gender ndash WHS
Study
0
2
4
6
8
9
11
13
15
55-59 60-64 65-69 70-74 75+
Pre
vale
nce o
f D
ry E
ye (
)
Age Group (years)
Women
Men
10262015
2
- -
Environment
bull Air conditioners or heaters
bull Airline travel
bull Winter months allergy season
bull Ceiling fan
bull Exogenous irritants (smoking)
bull Reading time
bull Digital device use
- -
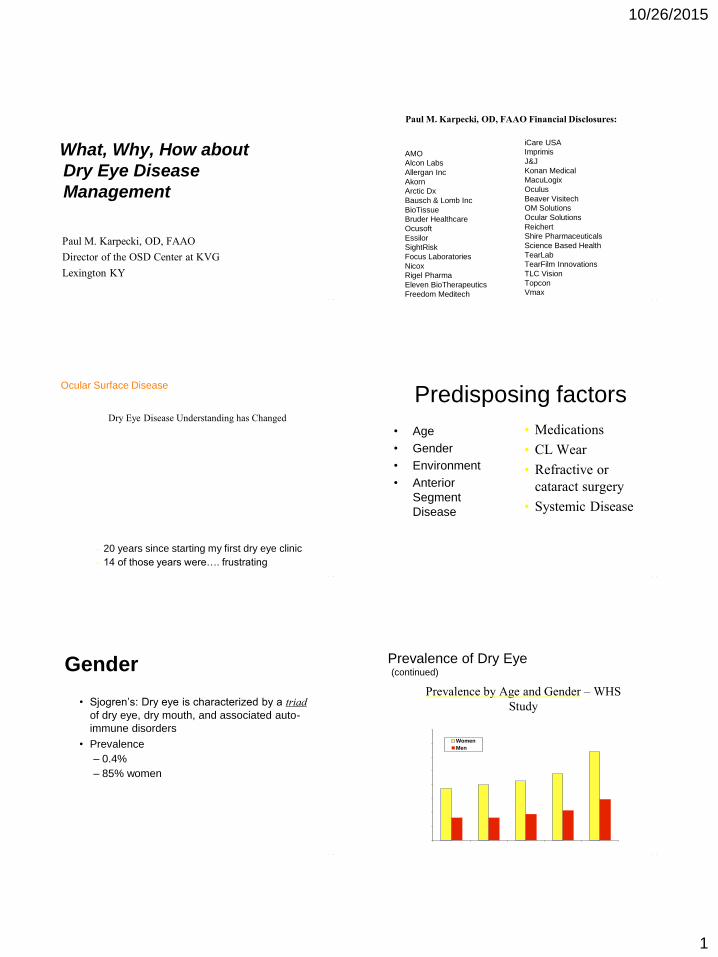
DTS Clinical Categories in 2006
bull Most common presentation ldquoNo lid margin diseaserdquo
bull Treatment decision based on severity level
Dysfunctional Tear Syndrome
Lid Margin
Disease
Altered Tear
Distribution
No Lid Margin
Disease
Behrens et al submitted
- -
Anterior Blepharitis
- -
Anterior Blepharitis
- -
OcuSoft Tea Tree Kit
bull Contains Tea Tree Oil + Buckthorn seed oil
bull Bland Ung QHS
bull OcuSoft Lid Scrub Plus
- -
BlephEx Treatment
10262015
3
- -
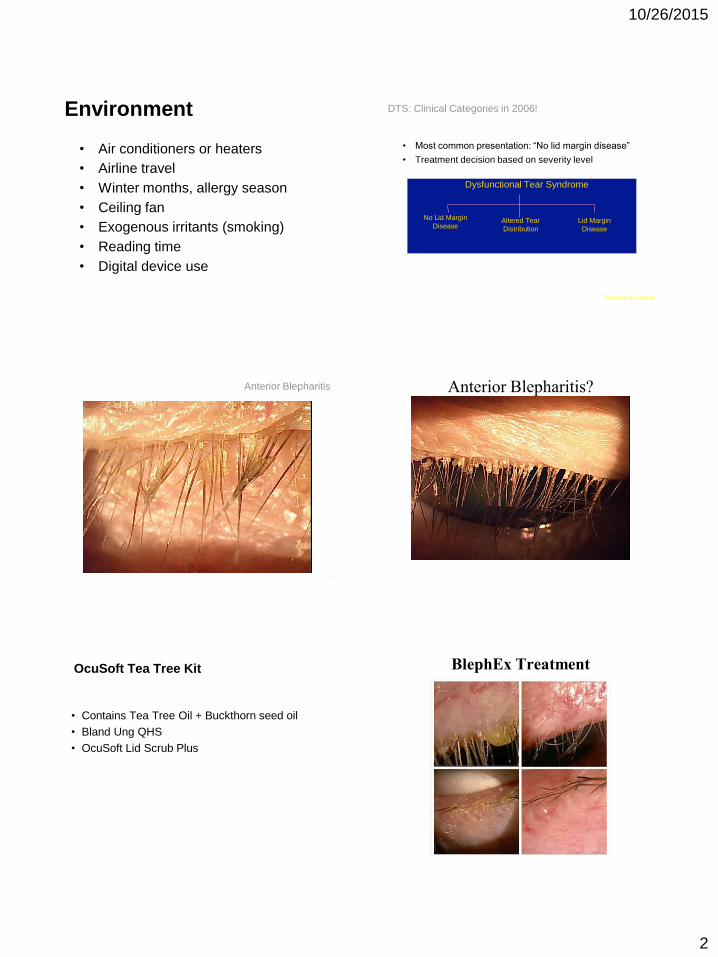
Frothy Foamy Tears = MGD
38
Key Components to MGD
bull Obstruction
bull Inflammation
bull Biofilm development
bull Tear film alterationsinstability
14
Not present in all cases
38
Obstruction
bull Lid margin debridementscaling
bull Commercial WC (eg Bruder
TranquilEyes etc)
bull Cold or manual expression
bull Mechanical thermal pulsation
15
Obstruction Debridement-Scaling
bull Debridement-scaling of the line of Marx and keratinized lid margin improves MG function and reducing symptoms
bull Korb DR1 Blackie CA Debridement-scaling a new procedure that increases Meibomian gland function and reduces dry eye symptoms Cornea 2013 Dec32(12)1554-7
bull Ong BL Hodson SA Wigham T et al Evidence for keratin proteins in normal and abnormal human meibomian fluids Curr Eye Res 1991 Dec10(12)1113-9
16 14
7
Warm Compress Effectiveness
bull Olson MC1 Korb DR Greiner JV Increase in tear film lipid layer thickness following treatment with warm compresses in patients with meibomian gland dysfunction Eye Contact Lens 2003 Apr29(2)96-9
bull Romero JM Biser SA Perry HD et al Conservative treatment of meibomian gland dysfunction Eye Contact Lens 2004 Jan30(1)14-9
bull Effective Requires continuous heat and temperature
bull Commercial compresses (eg Bruder) favored especially if they can provide hydration
17 14
7
Bruder Eye Hydrating Compress
18
10262015
4
Thermal Pulsation LipiFlow
bull Greiner JV A single LipiFlowreg Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 monthsCurr Eye Res 201237272-278 3
bull Conclusion Single 12 minute procedure statistically improved MG secretions TFBUT and OSDI at 9 months
19 14
7
20
The device applies controlled heat to
the inner upper and lower palpebral
conjunctival surfaces and lid margins
while simultaneously applying
pulsating pressure over the upper and
lower (outer) eyelids
THERMODYNAMIC TX TO EXPRESS AND EVACUATE MGs
THE LIPIFLOW (TearScience Inc Morrisville NC)
A new thermodynamic treatment to express amp evacuate the MGs
Heat applied to both inner lid surfaces
Pulsatile pressure applied to outer lids
FDA approved LipiFlow July 2011
Thermal Pulsation LipiFlow
bull Blackie CA Carlson AN Korb DR Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation a review Curr Opin Ophthalmol 2015 Jul26(4)306-13
bull Review of 31 peer-reviewed reports on vectored thermal pulsation therapy at the time of the search (eight manuscripts and 23 meeting abstracts)
bull Effective Optimal temperature for entire time back surface simultaneous expression
21 14
7
38
BioFilm Development
bull Lid hygiene products (eg Ocusoft Lid
scrub plus or Sterilid etc)
bull Canister options seem to work well
bull Surfactant and hypochlorus acid
versions
bull Mechanical with surfactant cleaner (eg
Blephex)
22
Inflammation and MGD
bull Suzuki T Teramukai S Konoshita S Meibomian Glands and Ocular Surface Inflammation Ocul Surf 2015 Apr13(2)133-149
bull Baudouin C Revisiting meibomian gland dysfunctionJ Fr Ophtalmol 2014 Dec37(10)757-62
bull Aragona P Aguennouz M2 Rania L et al Matrix metalloproteinase 9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease Ophthalmology 2015 Jan122(1)62-71
bull Enriacutequez-de-Salamanca A1 Castellanos et al Tear cytokine and chemokine analysis and clinical correlations in evaporative-type dry eye disease Mol Vis 2010 May 1916862-73
23 14
7
The Cycle of Inflammation
Sym
pto
ms I
ncre
ase
Potential Long-term Damage Inflammation
Stasis inspissation and obstruction of the Meibomian Glands
Meibomian Gland Dysfunction (MGD)
Tissue Changes
Decrease in Meibomian secretions
Decrease in tear film stability increased aqueous tearing1
Increase in evaporative stress
Ocular surface exposure (between blinks) amp Micro-trauma (during blinking)
24
1 Arita R et al Increased Tear Fluid Production as a Compensatory Response to
Meibomian Gland Loss A Multicenter Cross-sectional Study Ophthalmology 2015
Jan 24 pii S0161-6420(14)01195-6 doi 101016jophtha201412018 [Epub
ahead of print]
10262015
5
38
Inflammation in MGD
bull Combination agents amp steroid agents
bull Topical AzaSite
bull Cyclosporine (Restasis)
bull Omega fatty acids
bull PO doxycycline or azithromycin
25
Clinical Reseach on Corticosteroids in MGD
Aragona P1 Aguennouz M2 Rania L3 et al Ophthalmology Matrix metalloproteinase-9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease 2015 Jan122(1)62-71 2014 Sep 18 Akyol-Salman I1 Azizi S Mumcu UY et al J Ocul Pharmacol Ther Comparison of the efficacy of topical N-acetyl-cysteine and a topical steroid-antibiotic combination therapy in the treatment of meibomian gland dysfunction 2012 Feb28(1)49-52
26
Clinical Research on Cyclosporine and MGD
bull Prabhasawat P Tesavibul N Mahawong W A randomized double-masked study of 005 cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction Cornea 2012 Dec31(12)1386-93
bull Conclusions OSDI TFBUT lid margin inflammation meibomian gland expressibility and tarsal injection showed significant improvement from baseline in group A (Plt001 Plt001 Plt0001 Plt005 and Plt0001 respectively) In group B only the OSDI improved significantly from baseline at 3 months (P=0003)
27
Clinical Research on Cyclosporine and MGD
bull International Workshop on MGD Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Gerd Geerling Joseph Tauber Christophe Baudouin et al
bull Reviewed MGD and cyclosporine data in MGD as favorable
bull Perry H Doshi-Carnevale S Donnenfeld E et al Efficacy of Commercially Available Topical Cyclosporine A 005 in the Treatment of Meibomian Gland Dysfunction Cornea 200625171ndash175
bull At the 3-month visit statistical improvements (plt 005) in lid margin vascular injection tarsal telangiectasis and NaFl staining Most significant finding (P = 0001) was the greater decrease in the number of meibomian gland inclusions in the tCsA group compared with the placebo group
28
Clinical Research on Cyclosporine and MGD
bull Rubin M Rao S Efficacy Topical Cyclosporine 005 in the Treatment of Posterior Blepharitis Ocular Pharmacology and Therapeutics Nov 2006 22 (1)
bull Conclusions Comparison of Cyclosporine to Tobradex for MGD after 12 weeks greater improvements in Schirmers scores (P lt 0001) and TBUT(P = 0018) than tobramycindexamethasone
bull Mean improvement in meibomian gland secretion quality was significantly greater with cyclosporin (P = 0015)
bull Higher percentage of patients in the cyclosporin treatment group had improvements in symptoms of blurred vision burning and itching and more cyclosporin-treated patients experienced resolution of lid telangiectasia
29
Clinical Research on Cyclosporine and MGD
bull Schechter BA Katz RS Friedman L Efficacy of Topical Cyclosporine for the Treatment of Ocular Rosacea Adv Ther (2009) 26(6)651-659
bull Conclusions Statistical improvement in Schirmer (with anesthesia)(Plt0001) meant TFBUT corneal staining scores (Plt0001) OSDI (P=0022) compared to artificial tears at 3 months
30
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
10262015
2
- -
Environment
bull Air conditioners or heaters
bull Airline travel
bull Winter months allergy season
bull Ceiling fan
bull Exogenous irritants (smoking)
bull Reading time
bull Digital device use
- -
DTS Clinical Categories in 2006
bull Most common presentation ldquoNo lid margin diseaserdquo
bull Treatment decision based on severity level
Dysfunctional Tear Syndrome
Lid Margin
Disease
Altered Tear
Distribution
No Lid Margin
Disease
Behrens et al submitted
- -
Anterior Blepharitis
- -
Anterior Blepharitis
- -
OcuSoft Tea Tree Kit
bull Contains Tea Tree Oil + Buckthorn seed oil
bull Bland Ung QHS
bull OcuSoft Lid Scrub Plus
- -
BlephEx Treatment
10262015
3
- -
Frothy Foamy Tears = MGD
38
Key Components to MGD
bull Obstruction
bull Inflammation
bull Biofilm development
bull Tear film alterationsinstability
14
Not present in all cases
38
Obstruction
bull Lid margin debridementscaling
bull Commercial WC (eg Bruder
TranquilEyes etc)
bull Cold or manual expression
bull Mechanical thermal pulsation
15
Obstruction Debridement-Scaling
bull Debridement-scaling of the line of Marx and keratinized lid margin improves MG function and reducing symptoms
bull Korb DR1 Blackie CA Debridement-scaling a new procedure that increases Meibomian gland function and reduces dry eye symptoms Cornea 2013 Dec32(12)1554-7
bull Ong BL Hodson SA Wigham T et al Evidence for keratin proteins in normal and abnormal human meibomian fluids Curr Eye Res 1991 Dec10(12)1113-9
16 14
7
Warm Compress Effectiveness
bull Olson MC1 Korb DR Greiner JV Increase in tear film lipid layer thickness following treatment with warm compresses in patients with meibomian gland dysfunction Eye Contact Lens 2003 Apr29(2)96-9
bull Romero JM Biser SA Perry HD et al Conservative treatment of meibomian gland dysfunction Eye Contact Lens 2004 Jan30(1)14-9
bull Effective Requires continuous heat and temperature
bull Commercial compresses (eg Bruder) favored especially if they can provide hydration
17 14
7
Bruder Eye Hydrating Compress
18
10262015
4
Thermal Pulsation LipiFlow
bull Greiner JV A single LipiFlowreg Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 monthsCurr Eye Res 201237272-278 3
bull Conclusion Single 12 minute procedure statistically improved MG secretions TFBUT and OSDI at 9 months
19 14
7
20
The device applies controlled heat to
the inner upper and lower palpebral
conjunctival surfaces and lid margins
while simultaneously applying
pulsating pressure over the upper and
lower (outer) eyelids
THERMODYNAMIC TX TO EXPRESS AND EVACUATE MGs
THE LIPIFLOW (TearScience Inc Morrisville NC)
A new thermodynamic treatment to express amp evacuate the MGs
Heat applied to both inner lid surfaces
Pulsatile pressure applied to outer lids
FDA approved LipiFlow July 2011
Thermal Pulsation LipiFlow
bull Blackie CA Carlson AN Korb DR Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation a review Curr Opin Ophthalmol 2015 Jul26(4)306-13
bull Review of 31 peer-reviewed reports on vectored thermal pulsation therapy at the time of the search (eight manuscripts and 23 meeting abstracts)
bull Effective Optimal temperature for entire time back surface simultaneous expression
21 14
7
38
BioFilm Development
bull Lid hygiene products (eg Ocusoft Lid
scrub plus or Sterilid etc)
bull Canister options seem to work well
bull Surfactant and hypochlorus acid
versions
bull Mechanical with surfactant cleaner (eg
Blephex)
22
Inflammation and MGD
bull Suzuki T Teramukai S Konoshita S Meibomian Glands and Ocular Surface Inflammation Ocul Surf 2015 Apr13(2)133-149
bull Baudouin C Revisiting meibomian gland dysfunctionJ Fr Ophtalmol 2014 Dec37(10)757-62
bull Aragona P Aguennouz M2 Rania L et al Matrix metalloproteinase 9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease Ophthalmology 2015 Jan122(1)62-71
bull Enriacutequez-de-Salamanca A1 Castellanos et al Tear cytokine and chemokine analysis and clinical correlations in evaporative-type dry eye disease Mol Vis 2010 May 1916862-73
23 14
7
The Cycle of Inflammation
Sym
pto
ms I
ncre
ase
Potential Long-term Damage Inflammation
Stasis inspissation and obstruction of the Meibomian Glands
Meibomian Gland Dysfunction (MGD)
Tissue Changes
Decrease in Meibomian secretions
Decrease in tear film stability increased aqueous tearing1
Increase in evaporative stress
Ocular surface exposure (between blinks) amp Micro-trauma (during blinking)
24
1 Arita R et al Increased Tear Fluid Production as a Compensatory Response to
Meibomian Gland Loss A Multicenter Cross-sectional Study Ophthalmology 2015
Jan 24 pii S0161-6420(14)01195-6 doi 101016jophtha201412018 [Epub
ahead of print]
10262015
5
38
Inflammation in MGD
bull Combination agents amp steroid agents
bull Topical AzaSite
bull Cyclosporine (Restasis)
bull Omega fatty acids
bull PO doxycycline or azithromycin
25
Clinical Reseach on Corticosteroids in MGD
Aragona P1 Aguennouz M2 Rania L3 et al Ophthalmology Matrix metalloproteinase-9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease 2015 Jan122(1)62-71 2014 Sep 18 Akyol-Salman I1 Azizi S Mumcu UY et al J Ocul Pharmacol Ther Comparison of the efficacy of topical N-acetyl-cysteine and a topical steroid-antibiotic combination therapy in the treatment of meibomian gland dysfunction 2012 Feb28(1)49-52
26
Clinical Research on Cyclosporine and MGD
bull Prabhasawat P Tesavibul N Mahawong W A randomized double-masked study of 005 cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction Cornea 2012 Dec31(12)1386-93
bull Conclusions OSDI TFBUT lid margin inflammation meibomian gland expressibility and tarsal injection showed significant improvement from baseline in group A (Plt001 Plt001 Plt0001 Plt005 and Plt0001 respectively) In group B only the OSDI improved significantly from baseline at 3 months (P=0003)
27
Clinical Research on Cyclosporine and MGD
bull International Workshop on MGD Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Gerd Geerling Joseph Tauber Christophe Baudouin et al
bull Reviewed MGD and cyclosporine data in MGD as favorable
bull Perry H Doshi-Carnevale S Donnenfeld E et al Efficacy of Commercially Available Topical Cyclosporine A 005 in the Treatment of Meibomian Gland Dysfunction Cornea 200625171ndash175
bull At the 3-month visit statistical improvements (plt 005) in lid margin vascular injection tarsal telangiectasis and NaFl staining Most significant finding (P = 0001) was the greater decrease in the number of meibomian gland inclusions in the tCsA group compared with the placebo group
28
Clinical Research on Cyclosporine and MGD
bull Rubin M Rao S Efficacy Topical Cyclosporine 005 in the Treatment of Posterior Blepharitis Ocular Pharmacology and Therapeutics Nov 2006 22 (1)
bull Conclusions Comparison of Cyclosporine to Tobradex for MGD after 12 weeks greater improvements in Schirmers scores (P lt 0001) and TBUT(P = 0018) than tobramycindexamethasone
bull Mean improvement in meibomian gland secretion quality was significantly greater with cyclosporin (P = 0015)
bull Higher percentage of patients in the cyclosporin treatment group had improvements in symptoms of blurred vision burning and itching and more cyclosporin-treated patients experienced resolution of lid telangiectasia
29
Clinical Research on Cyclosporine and MGD
bull Schechter BA Katz RS Friedman L Efficacy of Topical Cyclosporine for the Treatment of Ocular Rosacea Adv Ther (2009) 26(6)651-659
bull Conclusions Statistical improvement in Schirmer (with anesthesia)(Plt0001) meant TFBUT corneal staining scores (Plt0001) OSDI (P=0022) compared to artificial tears at 3 months
30
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
10262015
3
- -
Frothy Foamy Tears = MGD
38
Key Components to MGD
bull Obstruction
bull Inflammation
bull Biofilm development
bull Tear film alterationsinstability
14
Not present in all cases
38
Obstruction
bull Lid margin debridementscaling
bull Commercial WC (eg Bruder
TranquilEyes etc)
bull Cold or manual expression
bull Mechanical thermal pulsation
15
Obstruction Debridement-Scaling
bull Debridement-scaling of the line of Marx and keratinized lid margin improves MG function and reducing symptoms
bull Korb DR1 Blackie CA Debridement-scaling a new procedure that increases Meibomian gland function and reduces dry eye symptoms Cornea 2013 Dec32(12)1554-7
bull Ong BL Hodson SA Wigham T et al Evidence for keratin proteins in normal and abnormal human meibomian fluids Curr Eye Res 1991 Dec10(12)1113-9
16 14
7
Warm Compress Effectiveness
bull Olson MC1 Korb DR Greiner JV Increase in tear film lipid layer thickness following treatment with warm compresses in patients with meibomian gland dysfunction Eye Contact Lens 2003 Apr29(2)96-9
bull Romero JM Biser SA Perry HD et al Conservative treatment of meibomian gland dysfunction Eye Contact Lens 2004 Jan30(1)14-9
bull Effective Requires continuous heat and temperature
bull Commercial compresses (eg Bruder) favored especially if they can provide hydration
17 14
7
Bruder Eye Hydrating Compress
18
10262015
4
Thermal Pulsation LipiFlow
bull Greiner JV A single LipiFlowreg Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 monthsCurr Eye Res 201237272-278 3
bull Conclusion Single 12 minute procedure statistically improved MG secretions TFBUT and OSDI at 9 months
19 14
7
20
The device applies controlled heat to
the inner upper and lower palpebral
conjunctival surfaces and lid margins
while simultaneously applying
pulsating pressure over the upper and
lower (outer) eyelids
THERMODYNAMIC TX TO EXPRESS AND EVACUATE MGs
THE LIPIFLOW (TearScience Inc Morrisville NC)
A new thermodynamic treatment to express amp evacuate the MGs
Heat applied to both inner lid surfaces
Pulsatile pressure applied to outer lids
FDA approved LipiFlow July 2011
Thermal Pulsation LipiFlow
bull Blackie CA Carlson AN Korb DR Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation a review Curr Opin Ophthalmol 2015 Jul26(4)306-13
bull Review of 31 peer-reviewed reports on vectored thermal pulsation therapy at the time of the search (eight manuscripts and 23 meeting abstracts)
bull Effective Optimal temperature for entire time back surface simultaneous expression
21 14
7
38
BioFilm Development
bull Lid hygiene products (eg Ocusoft Lid
scrub plus or Sterilid etc)
bull Canister options seem to work well
bull Surfactant and hypochlorus acid
versions
bull Mechanical with surfactant cleaner (eg
Blephex)
22
Inflammation and MGD
bull Suzuki T Teramukai S Konoshita S Meibomian Glands and Ocular Surface Inflammation Ocul Surf 2015 Apr13(2)133-149
bull Baudouin C Revisiting meibomian gland dysfunctionJ Fr Ophtalmol 2014 Dec37(10)757-62
bull Aragona P Aguennouz M2 Rania L et al Matrix metalloproteinase 9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease Ophthalmology 2015 Jan122(1)62-71
bull Enriacutequez-de-Salamanca A1 Castellanos et al Tear cytokine and chemokine analysis and clinical correlations in evaporative-type dry eye disease Mol Vis 2010 May 1916862-73
23 14
7
The Cycle of Inflammation
Sym
pto
ms I
ncre
ase
Potential Long-term Damage Inflammation
Stasis inspissation and obstruction of the Meibomian Glands
Meibomian Gland Dysfunction (MGD)
Tissue Changes
Decrease in Meibomian secretions
Decrease in tear film stability increased aqueous tearing1
Increase in evaporative stress
Ocular surface exposure (between blinks) amp Micro-trauma (during blinking)
24
1 Arita R et al Increased Tear Fluid Production as a Compensatory Response to
Meibomian Gland Loss A Multicenter Cross-sectional Study Ophthalmology 2015
Jan 24 pii S0161-6420(14)01195-6 doi 101016jophtha201412018 [Epub
ahead of print]
10262015
5
38
Inflammation in MGD
bull Combination agents amp steroid agents
bull Topical AzaSite
bull Cyclosporine (Restasis)
bull Omega fatty acids
bull PO doxycycline or azithromycin
25
Clinical Reseach on Corticosteroids in MGD
Aragona P1 Aguennouz M2 Rania L3 et al Ophthalmology Matrix metalloproteinase-9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease 2015 Jan122(1)62-71 2014 Sep 18 Akyol-Salman I1 Azizi S Mumcu UY et al J Ocul Pharmacol Ther Comparison of the efficacy of topical N-acetyl-cysteine and a topical steroid-antibiotic combination therapy in the treatment of meibomian gland dysfunction 2012 Feb28(1)49-52
26
Clinical Research on Cyclosporine and MGD
bull Prabhasawat P Tesavibul N Mahawong W A randomized double-masked study of 005 cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction Cornea 2012 Dec31(12)1386-93
bull Conclusions OSDI TFBUT lid margin inflammation meibomian gland expressibility and tarsal injection showed significant improvement from baseline in group A (Plt001 Plt001 Plt0001 Plt005 and Plt0001 respectively) In group B only the OSDI improved significantly from baseline at 3 months (P=0003)
27
Clinical Research on Cyclosporine and MGD
bull International Workshop on MGD Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Gerd Geerling Joseph Tauber Christophe Baudouin et al
bull Reviewed MGD and cyclosporine data in MGD as favorable
bull Perry H Doshi-Carnevale S Donnenfeld E et al Efficacy of Commercially Available Topical Cyclosporine A 005 in the Treatment of Meibomian Gland Dysfunction Cornea 200625171ndash175
bull At the 3-month visit statistical improvements (plt 005) in lid margin vascular injection tarsal telangiectasis and NaFl staining Most significant finding (P = 0001) was the greater decrease in the number of meibomian gland inclusions in the tCsA group compared with the placebo group
28
Clinical Research on Cyclosporine and MGD
bull Rubin M Rao S Efficacy Topical Cyclosporine 005 in the Treatment of Posterior Blepharitis Ocular Pharmacology and Therapeutics Nov 2006 22 (1)
bull Conclusions Comparison of Cyclosporine to Tobradex for MGD after 12 weeks greater improvements in Schirmers scores (P lt 0001) and TBUT(P = 0018) than tobramycindexamethasone
bull Mean improvement in meibomian gland secretion quality was significantly greater with cyclosporin (P = 0015)
bull Higher percentage of patients in the cyclosporin treatment group had improvements in symptoms of blurred vision burning and itching and more cyclosporin-treated patients experienced resolution of lid telangiectasia
29
Clinical Research on Cyclosporine and MGD
bull Schechter BA Katz RS Friedman L Efficacy of Topical Cyclosporine for the Treatment of Ocular Rosacea Adv Ther (2009) 26(6)651-659
bull Conclusions Statistical improvement in Schirmer (with anesthesia)(Plt0001) meant TFBUT corneal staining scores (Plt0001) OSDI (P=0022) compared to artificial tears at 3 months
30
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
4
Thermal Pulsation LipiFlow
bull Greiner JV A single LipiFlowreg Thermal Pulsation System treatment improves meibomian gland function and reduces dry eye symptoms for 9 monthsCurr Eye Res 201237272-278 3
bull Conclusion Single 12 minute procedure statistically improved MG secretions TFBUT and OSDI at 9 months
19 14
7
20
The device applies controlled heat to
the inner upper and lower palpebral
conjunctival surfaces and lid margins
while simultaneously applying
pulsating pressure over the upper and
lower (outer) eyelids
THERMODYNAMIC TX TO EXPRESS AND EVACUATE MGs
THE LIPIFLOW (TearScience Inc Morrisville NC)
A new thermodynamic treatment to express amp evacuate the MGs
Heat applied to both inner lid surfaces
Pulsatile pressure applied to outer lids
FDA approved LipiFlow July 2011
Thermal Pulsation LipiFlow
bull Blackie CA Carlson AN Korb DR Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation a review Curr Opin Ophthalmol 2015 Jul26(4)306-13
bull Review of 31 peer-reviewed reports on vectored thermal pulsation therapy at the time of the search (eight manuscripts and 23 meeting abstracts)
bull Effective Optimal temperature for entire time back surface simultaneous expression
21 14
7
38
BioFilm Development
bull Lid hygiene products (eg Ocusoft Lid
scrub plus or Sterilid etc)
bull Canister options seem to work well
bull Surfactant and hypochlorus acid
versions
bull Mechanical with surfactant cleaner (eg
Blephex)
22
Inflammation and MGD
bull Suzuki T Teramukai S Konoshita S Meibomian Glands and Ocular Surface Inflammation Ocul Surf 2015 Apr13(2)133-149
bull Baudouin C Revisiting meibomian gland dysfunctionJ Fr Ophtalmol 2014 Dec37(10)757-62
bull Aragona P Aguennouz M2 Rania L et al Matrix metalloproteinase 9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease Ophthalmology 2015 Jan122(1)62-71
bull Enriacutequez-de-Salamanca A1 Castellanos et al Tear cytokine and chemokine analysis and clinical correlations in evaporative-type dry eye disease Mol Vis 2010 May 1916862-73
23 14
7
The Cycle of Inflammation
Sym
pto
ms I
ncre
ase
Potential Long-term Damage Inflammation
Stasis inspissation and obstruction of the Meibomian Glands
Meibomian Gland Dysfunction (MGD)
Tissue Changes
Decrease in Meibomian secretions
Decrease in tear film stability increased aqueous tearing1
Increase in evaporative stress
Ocular surface exposure (between blinks) amp Micro-trauma (during blinking)
24
1 Arita R et al Increased Tear Fluid Production as a Compensatory Response to
Meibomian Gland Loss A Multicenter Cross-sectional Study Ophthalmology 2015
Jan 24 pii S0161-6420(14)01195-6 doi 101016jophtha201412018 [Epub
ahead of print]
10262015
5
38
Inflammation in MGD
bull Combination agents amp steroid agents
bull Topical AzaSite
bull Cyclosporine (Restasis)
bull Omega fatty acids
bull PO doxycycline or azithromycin
25
Clinical Reseach on Corticosteroids in MGD
Aragona P1 Aguennouz M2 Rania L3 et al Ophthalmology Matrix metalloproteinase-9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease 2015 Jan122(1)62-71 2014 Sep 18 Akyol-Salman I1 Azizi S Mumcu UY et al J Ocul Pharmacol Ther Comparison of the efficacy of topical N-acetyl-cysteine and a topical steroid-antibiotic combination therapy in the treatment of meibomian gland dysfunction 2012 Feb28(1)49-52
26
Clinical Research on Cyclosporine and MGD
bull Prabhasawat P Tesavibul N Mahawong W A randomized double-masked study of 005 cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction Cornea 2012 Dec31(12)1386-93
bull Conclusions OSDI TFBUT lid margin inflammation meibomian gland expressibility and tarsal injection showed significant improvement from baseline in group A (Plt001 Plt001 Plt0001 Plt005 and Plt0001 respectively) In group B only the OSDI improved significantly from baseline at 3 months (P=0003)
27
Clinical Research on Cyclosporine and MGD
bull International Workshop on MGD Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Gerd Geerling Joseph Tauber Christophe Baudouin et al
bull Reviewed MGD and cyclosporine data in MGD as favorable
bull Perry H Doshi-Carnevale S Donnenfeld E et al Efficacy of Commercially Available Topical Cyclosporine A 005 in the Treatment of Meibomian Gland Dysfunction Cornea 200625171ndash175
bull At the 3-month visit statistical improvements (plt 005) in lid margin vascular injection tarsal telangiectasis and NaFl staining Most significant finding (P = 0001) was the greater decrease in the number of meibomian gland inclusions in the tCsA group compared with the placebo group
28
Clinical Research on Cyclosporine and MGD
bull Rubin M Rao S Efficacy Topical Cyclosporine 005 in the Treatment of Posterior Blepharitis Ocular Pharmacology and Therapeutics Nov 2006 22 (1)
bull Conclusions Comparison of Cyclosporine to Tobradex for MGD after 12 weeks greater improvements in Schirmers scores (P lt 0001) and TBUT(P = 0018) than tobramycindexamethasone
bull Mean improvement in meibomian gland secretion quality was significantly greater with cyclosporin (P = 0015)
bull Higher percentage of patients in the cyclosporin treatment group had improvements in symptoms of blurred vision burning and itching and more cyclosporin-treated patients experienced resolution of lid telangiectasia
29
Clinical Research on Cyclosporine and MGD
bull Schechter BA Katz RS Friedman L Efficacy of Topical Cyclosporine for the Treatment of Ocular Rosacea Adv Ther (2009) 26(6)651-659
bull Conclusions Statistical improvement in Schirmer (with anesthesia)(Plt0001) meant TFBUT corneal staining scores (Plt0001) OSDI (P=0022) compared to artificial tears at 3 months
30
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
5
38
Inflammation in MGD
bull Combination agents amp steroid agents
bull Topical AzaSite
bull Cyclosporine (Restasis)
bull Omega fatty acids
bull PO doxycycline or azithromycin
25
Clinical Reseach on Corticosteroids in MGD
Aragona P1 Aguennouz M2 Rania L3 et al Ophthalmology Matrix metalloproteinase-9 and transglutaminase 2 expression at the ocular surface in patients with different forms of dry eye disease 2015 Jan122(1)62-71 2014 Sep 18 Akyol-Salman I1 Azizi S Mumcu UY et al J Ocul Pharmacol Ther Comparison of the efficacy of topical N-acetyl-cysteine and a topical steroid-antibiotic combination therapy in the treatment of meibomian gland dysfunction 2012 Feb28(1)49-52
26
Clinical Research on Cyclosporine and MGD
bull Prabhasawat P Tesavibul N Mahawong W A randomized double-masked study of 005 cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction Cornea 2012 Dec31(12)1386-93
bull Conclusions OSDI TFBUT lid margin inflammation meibomian gland expressibility and tarsal injection showed significant improvement from baseline in group A (Plt001 Plt001 Plt0001 Plt005 and Plt0001 respectively) In group B only the OSDI improved significantly from baseline at 3 months (P=0003)
27
Clinical Research on Cyclosporine and MGD
bull International Workshop on MGD Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction Gerd Geerling Joseph Tauber Christophe Baudouin et al
bull Reviewed MGD and cyclosporine data in MGD as favorable
bull Perry H Doshi-Carnevale S Donnenfeld E et al Efficacy of Commercially Available Topical Cyclosporine A 005 in the Treatment of Meibomian Gland Dysfunction Cornea 200625171ndash175
bull At the 3-month visit statistical improvements (plt 005) in lid margin vascular injection tarsal telangiectasis and NaFl staining Most significant finding (P = 0001) was the greater decrease in the number of meibomian gland inclusions in the tCsA group compared with the placebo group
28
Clinical Research on Cyclosporine and MGD
bull Rubin M Rao S Efficacy Topical Cyclosporine 005 in the Treatment of Posterior Blepharitis Ocular Pharmacology and Therapeutics Nov 2006 22 (1)
bull Conclusions Comparison of Cyclosporine to Tobradex for MGD after 12 weeks greater improvements in Schirmers scores (P lt 0001) and TBUT(P = 0018) than tobramycindexamethasone
bull Mean improvement in meibomian gland secretion quality was significantly greater with cyclosporin (P = 0015)
bull Higher percentage of patients in the cyclosporin treatment group had improvements in symptoms of blurred vision burning and itching and more cyclosporin-treated patients experienced resolution of lid telangiectasia
29
Clinical Research on Cyclosporine and MGD
bull Schechter BA Katz RS Friedman L Efficacy of Topical Cyclosporine for the Treatment of Ocular Rosacea Adv Ther (2009) 26(6)651-659
bull Conclusions Statistical improvement in Schirmer (with anesthesia)(Plt0001) meant TFBUT corneal staining scores (Plt0001) OSDI (P=0022) compared to artificial tears at 3 months
30
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
10262015
6
- -
Mild MGD
bull HotWarm compresses
bull Lid hygiene
bull Lipid based tears-mildmoderate
bull Osmolarity lowering drops in
moderatesevere
- -
ModerateAcute
bull Tobradex ST
bull Zylet
bull AzaSite
bull Tobradex generic
bull Steroid drops or ung bull (loteprednol preservative-free ung
QhS)
- -
Long Term
bull Pulse dose medications
periodically
bull Restasis bid
bull Essential fatty acids
ndash EPA
ndash DHA
ndash GLA
- -
Moderatesevere or not improving
bull Add PO tetracycline
bull Recommendation
bull Doxycycline 50mg bid x 4-12 weeks then taper to qd
bull Doxycycline 20 mg bid x 4-12 weeks then taper to qd (periostat concern $$$)
- -
Tetracyclines
bull Antibiotics inhibit
bacterial protein
synthesis by binding 30S ribosome
bull Anti-inflammatory properties
ndash decreases IL-1 TNF-
ndash decreases NO production
ndash decreases HLA Class II antigen expression
ndash decreases metalloproteinase production and
activation
bull Decrease symptoms and joint destruction in RA
- -
Contraindications
bull Pregnant or child bearing age
bull Children
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
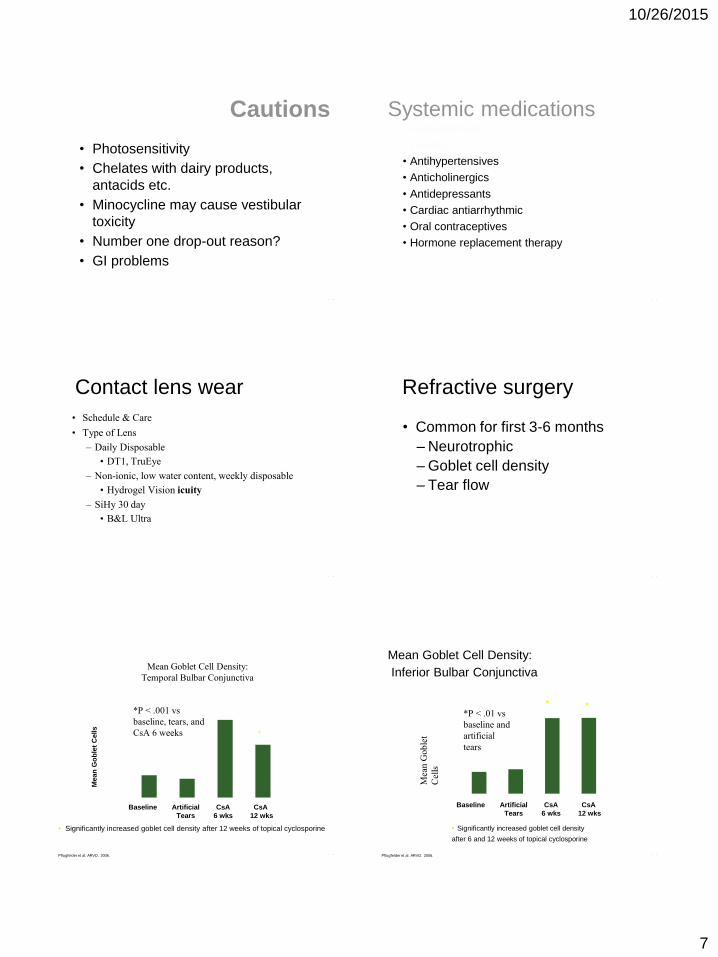
10262015
7
- -
Cautions
bull Photosensitivity
bull Chelates with dairy products
antacids etc
bull Minocycline may cause vestibular
toxicity
bull Number one drop-out reason
bull GI problems
- -
Systemic medications bull Antihistamines
bull Diuretics
bull Antihypertensives
bull Anticholinergics
bull Antidepressants
bull Cardiac antiarrhythmic
bull Oral contraceptives
bull Hormone replacement therapy
- -
Contact lens wear
bull Schedule amp Care
bull Type of Lens
ndash Daily Disposable
bull DT1 TruEye
ndash Non-ionic low water content weekly disposable
bull Hydrogel Vision icuity
ndash SiHy 30 day
bull BampL Ultra
- -
Refractive surgery
bull Common for first 3-6 months
ndash Neurotrophic
ndash Goblet cell density
ndash Tear flow
- - Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mean
Go
ble
t C
ells
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 001 vs
baseline tears and
CsA 6 weeks
Mean Goblet Cell Density
Temporal Bulbar Conjunctiva
bull Significantly increased goblet cell density after 12 weeks of topical cyclosporine
- -
Mean Goblet Cell Density
Inferior Bulbar Conjunctiva
Pflugfelder et al ARVO 2006
000
450
900
1350
1800
2250
Mea
n G
ob
let
Cel
ls
Baseline Artificial
Tears
CsA
6 wks
CsA
12 wks
P lt 01 vs
baseline and
artificial
tears
bull Significantly increased goblet cell density
after 6 and 12 weeks of topical cyclosporine
10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
8
- -
Systemic Disease
bull Diabetes
bull Rheumatoid Arthritis
ndash Sjogrenrsquos syndrome
bull Thyroid Disease
bull Dermatological eg rosacea
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 04 prevalence
bull Women gt Men (younger
women)
bull Much lower androgen counts
bull Treat underlying immune
disorder
- -
Which of these conditions are Sjogrenrsquos patients 46x
more likely to develop
A Leukemia
C Diabetes
B Lymphoma
D Cardiac Arrythmia
- -
Sjogrenrsquos Syndrome
bull Lymphocytic infiltration of
lacrimal and salivary glands
bull 5-8 incidence of B-cell non-
Hodgkins Lymphoma
bull 463x more often
ndash Moutsopoulos HM et all
- -
Sjogrenrsquos Syndrome
bull Medical Treatments Secretagogues ndash Salagen 5 mg
bull Pilocarpine tablets
bull Avoid in asthma patients GI ulcer acute iritis or narrow angles
ndash Evoxac 30 mg TIDndash saliva stimulating drug bull Very effective with a lot less side effects
- -
Symptoms of Dry Eye
bull Burning
bull Stinging
bull Transient blur
bull Dryness
bull Photophobia
bull Epiphora
bull Blurred vision
bull Contact lens intolerance
bull Injection
bull Foreign body sensation
bull Grittiness
bull Increased blink rate
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
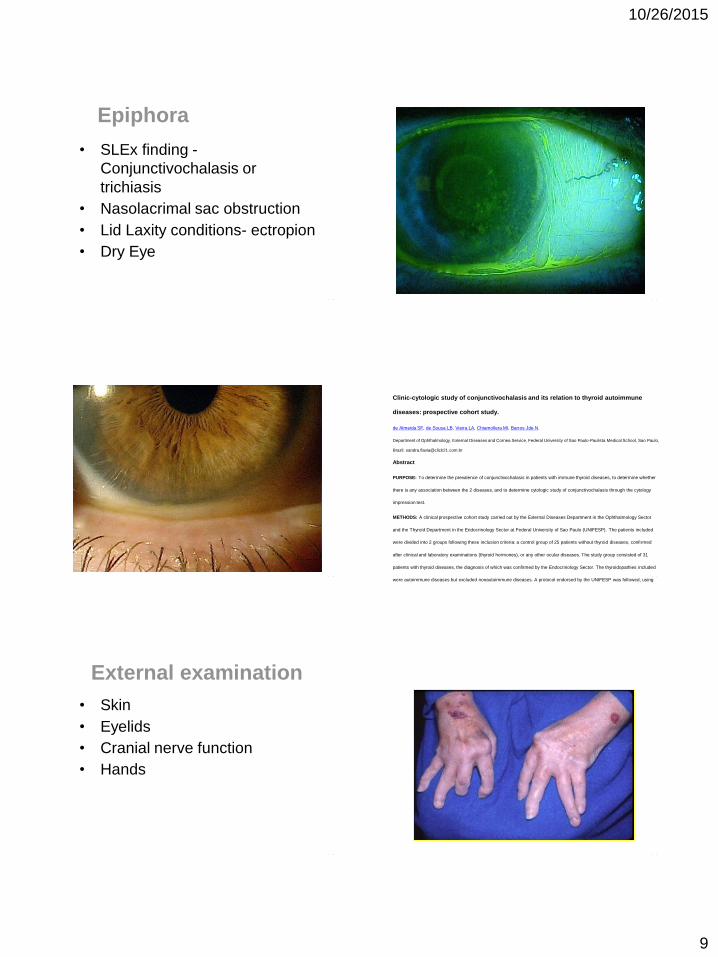
10262015
9
- -
Epiphora
bull SLEx finding -
Conjunctivochalasis or
trichiasis
bull Nasolacrimal sac obstruction
bull Lid Laxity conditions- ectropion
bull Dry Eye
- -
- -
- -
Clinic-cytologic study of conjunctivochalasis and its relation to thyroid autoimmune
diseases prospective cohort study
de Almeida SF de Sousa LB Vieira LA Chiamollera MI Barros Jde N
Department of Ophthalmology External Diseases and Cornea Service Federal University of Sao Paulo-Paulista Medical School Sao Paulo
Brazil sandraflaviaclick21combr
Abstract
PURPOSE To determine the prevalence of conjunctivochalasis in patients with immune thyroid diseases to determine whether
there is any association between the 2 diseases and to determine cytologic study of conjunctivochalasis through the cytology
impression test
METHODS A clinical prospective cohort study carried out by the External Diseases Department in the Ophthalmology Sector
and the Thyroid Department in the Endocrinology Sector at Federal University of Sao Paulo (UNIFESP) The patients included
were divided into 2 groups following these inclusion criteria a control group of 25 patients without thyroid diseases confirmed
after clinical and laboratory examinations (thyroid hormones) or any other ocular diseases The study group consisted of 31
patients with thyroid diseases the diagnosis of which was confirmed by the Endocrinology Sector The thyroidopathies included
were autoimmune diseases but excluded nonautoimmune diseases A protocol endorsed by the UNIFESP was followed using
clinical and ophthalmological history biomicroscopy and impression cytology
RESULTS Fifty-two percent of patients without thyroid diseases and 88 of patients with thyroid diseases presented with
conjunctivochalasis The risk ratio was 1705 (Pr gt chi(2) = 00038) indicating that there is an association between them For the
impression cytology in inferior bulbar conjunctiva there was an association between the result of the impression cytology and
conjunctivochalasis (Pearson chi(2) = 101190 Pr = 0006)
CONCLUSION The prevalence of conjunctivochalasis in patients with autoimmune thyroid diseases was 88 Patients with
autoimmune thyroidopathy presented higher percentages of conjunctivochalasis than the control group confirming the
association between them The cytologic study showed the highest prevalence of abnormal surface features in eyes with
conjunctivochalasis
- -
External examination
bull Skin
bull Eyelids
bull Cranial nerve function
bull Hands
- -
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
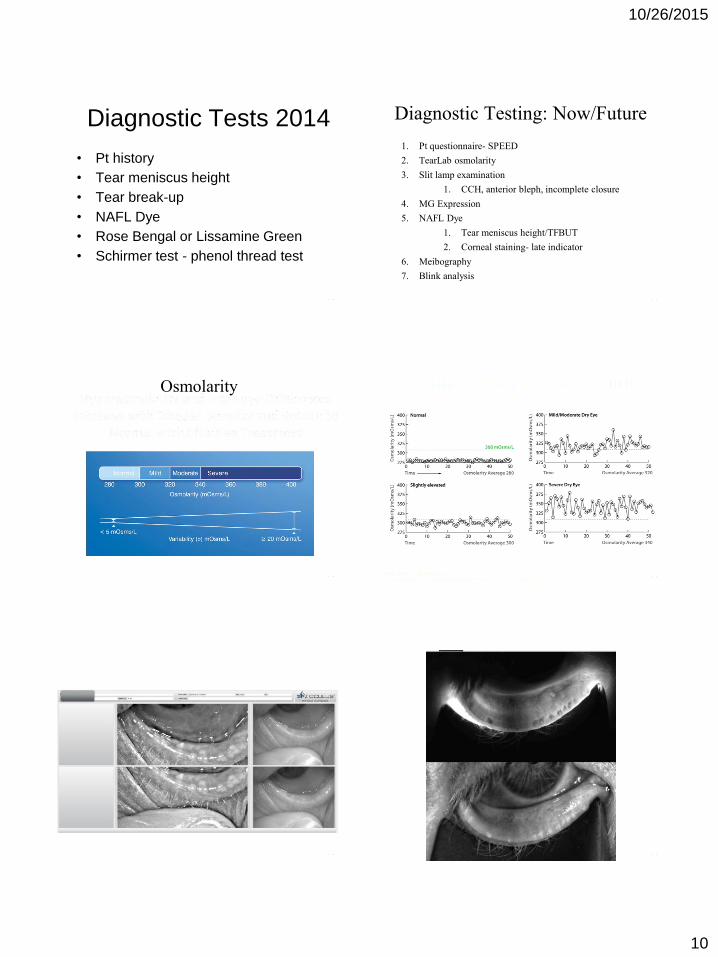
10262015
10
- -
Diagnostic Tests 2014
bull Pt history
bull Tear meniscus height
bull Tear break-up
bull NAFL Dye
bull Rose Bengal or Lissamine Green
bull Schirmer test - phenol thread test
- -
Diagnostic Testing NowFuture
1 Pt questionnaire- SPEED
2 TearLab osmolarity
3 Slit lamp examination
1 CCH anterior bleph incomplete closure
4 MG Expression
5 NAFL Dye
1 Tear meniscus heightTFBUT
2 Corneal staining- late indicator
6 Meibography
7 Blink analysis
- -
Osmolarity
- -
- -
- -
10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
11
- -
Other Diagnostic Tests of Value
bull Light Seal Test -Transilluminate
bull Bink analysis
- -
Dr i-Coach
A patented sensor and software package that can help users develop and maintain proper
computer habits
- -
Features Include
bull Eye Fatigue Monitor (Blink Rate)
bull User Distance Monitor
bull Timer
bull Seated Height Detector
bull Environmental Light Detector
- -
Eye Fatigue Monitor (Blink Rate) ala Fitbit
bull Dr i-Coach can efficiently track the eye region detecting and
counting userrsquos blinks
bull Blink rate data will be available in an easy to read chart for the
use of the patient and their eye care professional
bull The Dr i-Coachreg software monitors and records the users
viewing time when there is any computer activity
bull After a viewing time between twenty to sixty minutes (pre-
selected by the user) the program alerts the viewer and reminds
them to take a break
- -
bull Based on distance head-track localization and screen tilt measured by an embedded gyroscope Dr i-Coach is able to determine if the user is seated at the proper height and reminds them to adjust accordingly
- -
Treatment
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
10262015
12
- -
Symptoms of DED but normal
osmolarity minimal other signs
bull DED that is well controlled
bull CL solutions related -PATH
bull Mild allergic conjunctivitis
bull EBMD- MDF dystrophy
bull Pinguecula amp early Pterygium
bull Infection - eg conjunctivitis
bull Anterior blepharitis
ndash Demodex
bull GPC
bull Asthenopia - vertical CI etc
bull Salzmannrsquos Nodular
Degeneration
bull Mildmod conjunctivochalasis
Patient with epiphora will actually
have osmolarity readings below
normal or very low (ie lt 280)
- -
Treatment
bull Emphasis chronic nature of the
condition
bull Eliminate exacerbating factors
ndash smoking air conditioner meds
bull Drink 4-6 glasses of water per day
bull Tear replacements
- -
Role of ATrsquos bull Osmolarity lowering
ndash Blink Tears amp TheraTears
bull EBMDcorneal staining ndash FreshKote
bull Lipid Deficient ndash Systane Balance Soothe XP Retaine MGD
Refresh Optive Advanced
bull Aqueous deficient ndash OptiveRefresh Systane Ultra
bull Severe ------gt SystaneGenteal gel or ung
- -
Nutritional Supplements
Essential fatty acids
bull Omega fatty acids
bull ALA- eg Flaxseed oil
bull EPA-DHA ndash eg Fish oils
bull GLA
ndash Black Currant Seed Oil etc
- -
HydroEye (HE) Clinical
Purpose Evaluate HE in
postmenopausal women with
moderate-severe KCS amp tear
dysfunction
Dual Sites Virginia Eye Consultants
amp Baylor University
Type Double-blind placebo-
controlled randomized
Duration 6 months
- -
Key Findings Symptoms
HydroEyereg therapy significantly decreased
the mean OSDI score over the treatment
period (p=0004) while the OSDI score
was essentially unchanged in the placebo
group
At the end of 24 weeks OSDI scores were
significantly reduced in the HydroEyereg
group compared to placebo (p=005)
10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
13
- -
Primary Sign Improvement
- -
Primary Sign Improvement
- -
Targeted Treatments are KEY
bull Treatments aimed at local inflammatory
processes
ndash Topical corticosteroids (Lotemax)
bull Effective anti-inflammatory agents
bull Site specific Steroids
ndash Cyclosporin A (Restasis)
- -
Dry Eye DiseasemdashA Real Condition That Needs
More Than a Palliative Solution
bull ldquoDry eye is a disorder of the tear film due to tear deficiency
or excessive tear evaporation which can cause damage to
the interpalpebral ocular surfacerdquo1
bull Artificial tears provide temporary palliative relief2
ldquoArtificial tears are inadequate
because they failhellipto prevent
progression of Dry Eye diseaserdquo3
J Daniel Nelson MD
Corneal Specialist
University of Minnesota
1 Lemp CLAO J 1995
2 Stern et al Cornea 1998
3 Nelson et al Adv Ther 2000
- -
Corticosteroids
bull Bind to nuclear receptors that bind
DNA and regulate gene expression
bull Interfere with transcription regulators
[eg AP-1 amp NF-kB]
bull most inflammatory pathways
ndash cytokine production
ndash lipid mediators (PGs)
ndash cell adhesion molecules
ndash lymphocyte trafficking
ndash vascular permeability
bull Ring modifications alter potency
and membrane stabilizing effects
- -
Steroids and Dry Eye
Symptomatic improvement in irritation
symptoms in 83 and objective
improvement ( redness dye staining and
tarsal papillae FTC) in 80
of 70 patients treated for 2 weeks with non-
preserved methylprednisolone
Prabhasawat amp Tseng BJO 1998
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
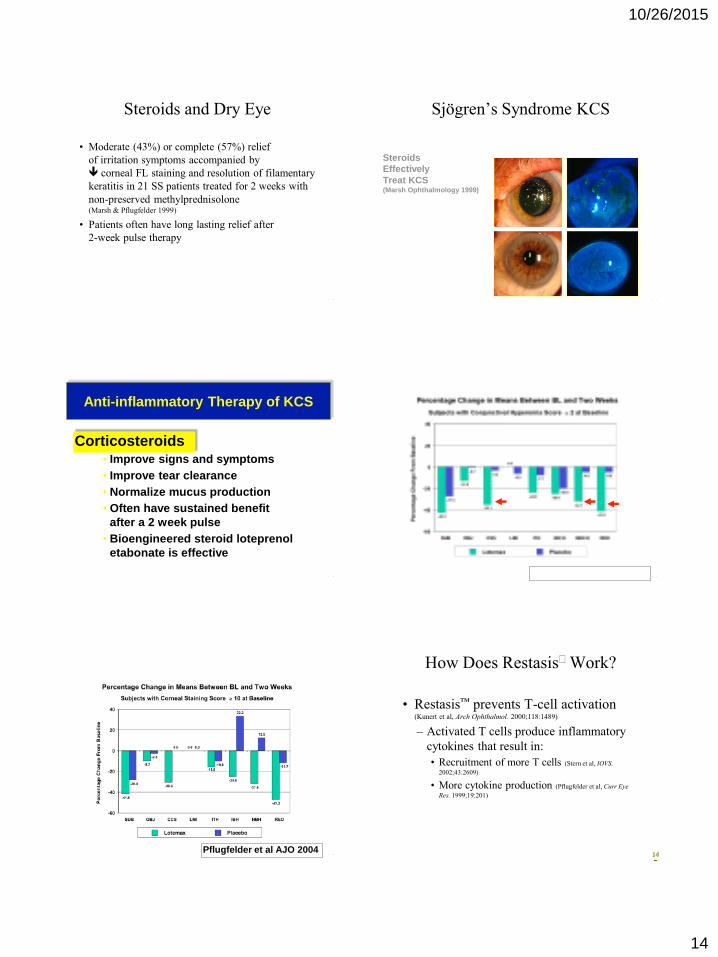
10262015
14
- -
Steroids and Dry Eye
bull Moderate (43) or complete (57) relief
of irritation symptoms accompanied by
corneal FL staining and resolution of filamentary
keratitis in 21 SS patients treated for 2 weeks with
non-preserved methylprednisolone (Marsh amp Pflugfelder 1999)
bull Patients often have long lasting relief after
2-week pulse therapy
- -
Pre-Steroid
Post-Steroid
Steroids
Effectively
Treat KCS (Marsh Ophthalmology 1999)
Sjoumlgrenrsquos Syndrome KCS
- -
Anti-inflammatory Therapy of KCS
Corticosteroids bull Improve signs and symptoms
bull Improve tear clearance
bull Normalize mucus production
bull Often have sustained benefit
after a 2 week pulse
bull Bioengineered steroid loteprenol
etabonate is effective
- -
Pflugfelder et al AJO 2004
- - Pflugfelder et al AJO 2004
- -
How Does Restasis Work
bull Restasistrade prevents T-cell activation (Kunert et al Arch Ophthalmol 20001181489)
ndash Activated T cells produce inflammatory
cytokines that result in
bull Recruitment of more T cells (Stern et al IOVS
2002432609)
bull More cytokine production (Pflugfelder et al Curr Eye
Res 199919201)
14
7
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
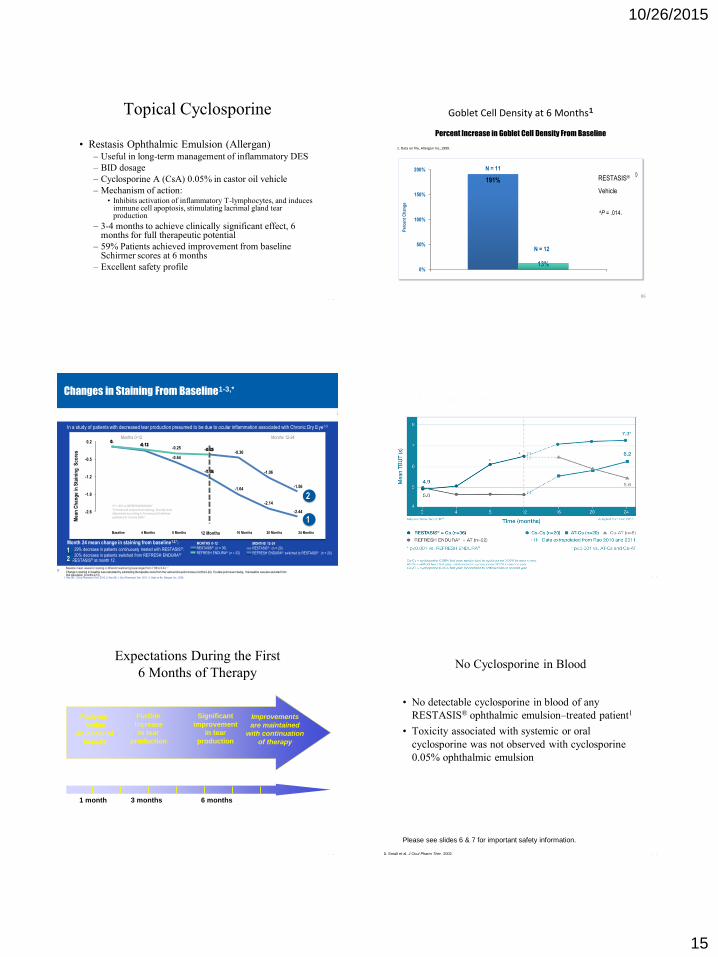
10262015
15
- -
Topical Cyclosporine
bull Restasis Ophthalmic Emulsion (Allergan) ndash Useful in long-term management of inflammatory DES
ndash BID dosage
ndash Cyclosporine A (CsA) 005 in castor oil vehicle
ndash Mechanism of action bull Inhibits activation of inflammatory T-lymphocytes and induces
immune cell apoptosis stimulating lacrimal gland tear production
ndash 3-4 months to achieve clinically significant effect 6 months for full therapeutic potential
ndash 59 Patients achieved improvement from baseline Schirmer scores at 6 months
ndash Excellent safety profile
Goblet Cell Density at 6 Months1
1 Data on file Allergan Inc1999
86
191
13 0
50
100
150
200RESTASISreg
Vehicle
N = 11
N = 12
aP = 014
RESTASISreg
Vehicle
Per
cen
t C
han
ge
Percent Increase in Goblet Cell Density From Baseline
In a study of patients with decreased tear production presumed to be due to ocular inflammation associated with Chronic Dry Eye1-3
Months 0-12
Me
an
Ch
ang
e in
Sta
inin
g S
co
res
Months 12-24
MONTHS 12-24 RESTASISreg (n = 20)
REFRESH ENDURAreg switched to RESTASISreg (n = 20)
-104
-164
-214
-244
-026 -036
-106
-156
0 -013
-064
-119
0 -012
-025 -032
-26
-19
-12
-05
02
87
Changes in Staining From Baseline1-3
1 Rao SN J Ocul Pharmacol Ther 2010 2 Rao SN J Ocul Pharmacol Ther 2011 3 Data on file Allergan Inc 2009
Month 24 mean change in staining from baseline12 29 decrease in patients continuously treated with RESTASISreg
20 decrease in patients switched from REFRESH ENDURAreg
to RESTASISreg at month 12
1
Baseline 8 Months 4 Months 12 Months 24 Months 16 Months 20 Months
Baseline mean values for staining in different treatment groups ranged from 786 to 8441
2
1
2
MONTHS 0-12 RESTASISreg (n = 36)
REFRESH ENDURAreg (n = 22)
Change in staining in baseline was calculated by subtracting the baseline score from the various time point scores (months 0-24) If a data point was missing the baseline was also excluded from that calculation (months 0-12)
aP lt 007 vs REFRESH ENDURAreg
Corneal and conjunctival staining Severity level determined according to Consensus Guidelines
published in Cornea 20062
- -
- -
Expectations During the First
6 Months of Therapy
Patients
notice
an onset of
benefit
Further
increase
in tear
production
Significant
improvement
in tear
production
Improvements
are maintained
with continuation
of therapy
1 month 3 months 6 months
- - 1 Small et al J Ocul Pharm Ther 2002
No Cyclosporine in Blood
bull No detectable cyclosporine in blood of any
RESTASISreg ophthalmic emulsionndashtreated patient1
bull Toxicity associated with systemic or oral
cyclosporine was not observed with cyclosporine
005 ophthalmic emulsion
Please see slides 6 amp 7 for important safety information
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
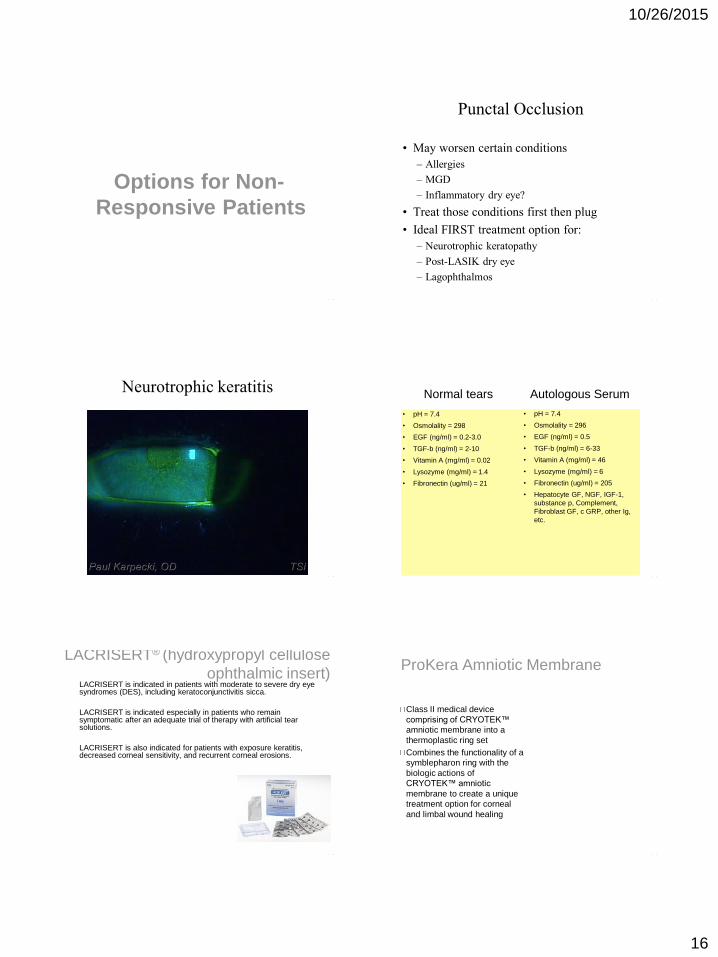
10262015
16
- -
Options for Non-
Responsive Patients
- -
Punctal Occlusion
bull May worsen certain conditions
ndash Allergies
ndash MGD
ndash Inflammatory dry eye
bull Treat those conditions first then plug
bull Ideal FIRST treatment option for
ndash Neurotrophic keratopathy
ndash Post-LASIK dry eye
ndash Lagophthalmos
- -
Neurotrophic keratitis
- -
Normal tears Autologous Serum
bull pH = 74
bull Osmolality = 298
bull EGF (ngml) = 02-30
bull TGF-b (ngml) = 2-10
bull Vitamin A (mgml) = 002
bull Lysozyme (mgml) = 14
bull Fibronectin (ugml) = 21
bull pH = 74
bull Osmolality = 296
bull EGF (ngml) = 05
bull TGF-b (ngml) = 6-33
bull Vitamin A (mgml) = 46
bull Lysozyme (mgml) = 6
bull Fibronectin (ugml) = 205
bull Hepatocyte GF NGF IGF-1
substance p Complement
Fibroblast GF c GRP other Ig
etc
- -
LACRISERTreg (hydroxypropyl cellulose
ophthalmic insert) LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
ProKera Amniotic Membrane
Class II medical device
comprising of CRYOTEKtrade
amniotic membrane into a
thermoplastic ring set
Combines the functionality of a
symblepharon ring with the
biologic actions of
CRYOTEKtrade amniotic
membrane to create a unique
treatment option for corneal
and limbal wound healing
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom
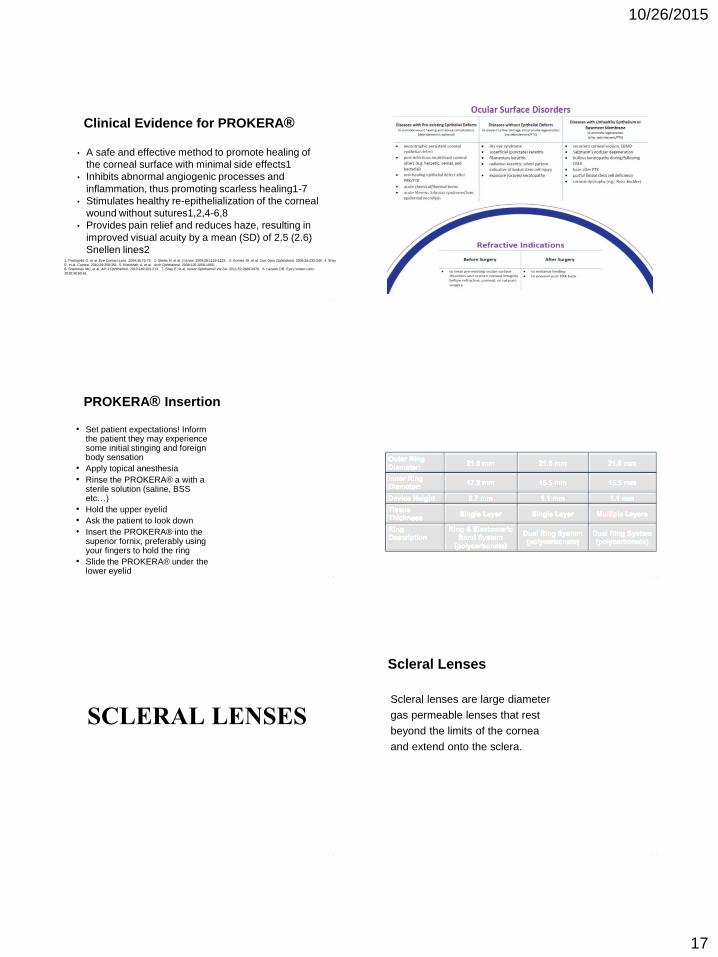
10262015
17
- -
Clinical Evidence for PROKERAreg
bull A safe and effective method to promote healing of
the corneal surface with minimal side effects1
bull Inhibits abnormal angiogenic processes and
inflammation thus promoting scarless healing1-7
bull Stimulates healthy re-epithelialization of the corneal
wound without sutures124-68
bull Provides pain relief and reduces haze resulting in
improved visual acuity by a mean (SD) of 25 (26)
Snellen lines2 1 Pachigolla G et al Eye Contact Lens 20093572-75 2 Sheha H et al Cornea 2009281118-1123 3 Gomes JA et al Curr Opin Ophthalmol 200516233-240 4 Shay
E et al Cornea 201029359-361 5 Kheirkhah A et al Arch Ophthalmol 20081261059-1066
6 Shammas MC et al Am J Ophthalmol 2010149203-213 7 Shay E et al Invest Ophthalmol Vis Sci 2011522669-2678 8 Lazarro DR Eye Contact Lens
20103660-61
- -
SCLERAL LENSES
LACRISERT is indicated in patients with moderate to severe dry eye syndromes (DES) including keratoconjunctivitis sicca
LACRISERT is indicated especially in patients who remain symptomatic after an adequate trial of therapy with artificial tear solutions
LACRISERT is also indicated for patients with exposure keratitis decreased corneal sensitivity and recurrent corneal erosions
- -
PROKERAreg Insertion
bull Set patient expectations Inform the patient they may experience some initial stinging and foreign body sensation
bull Apply topical anesthesia
bull Rinse the PROKERAreg a with a sterile solution (saline BSS etchellip)
bull Hold the upper eyelid
bull Ask the patient to look down
bull Insert the PROKERAreg into the superior fornix preferably using your fingers to hold the ring
bull Slide the PROKERAreg under the lower eyelid
- -
- -
SCLERAL LENSES
- -
Scleral Lenses
Scleral lenses are large diameter
gas permeable lenses that rest
beyond the limits of the cornea
and extend onto the sclera
10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom

10262015
18
- -
GLAUCOMA SIMILARITY
bull Look at the structure and functioning of the
MGs and ocular surface
bull Multiple testing
ndash IOP = osmolarity
ndash VF testing = corneal staining
ndash OCT = meibomographyLipiView
ndash MG expression = ONH examination
- -
FUTURE DENTAL MODEL
bull Tooth Brush amp Floss = Hydrating compress
and lid hygiene products
bull Scaling = Scalingdebridement of keratin
bull Dental cleaning = mechanical pulsation or
cleaning ie LipiFlow Blephex etc
bull Dental X-rays = MeibographyLipiview
Dry Eye Disease Conclusion
bull Understand the ramifications of not
treating this disease
bull The eyelids are key
bull Be aggressive in your treatment and then
reduce medications
bull The single largest medical eyecare
opportunity now and in the future
105 - -
ndash `
paulkarpeckicom
wwwophthalmicresourcescom