Embed Size (px)
Citation preview
What’s New in Helicobacter
Pylori Therapy
Waqar Qureshi, MD,Professor of Medicine,
Clinical Chief of Gastroenterology,Baylor College of
Medicine,Houston, Texas
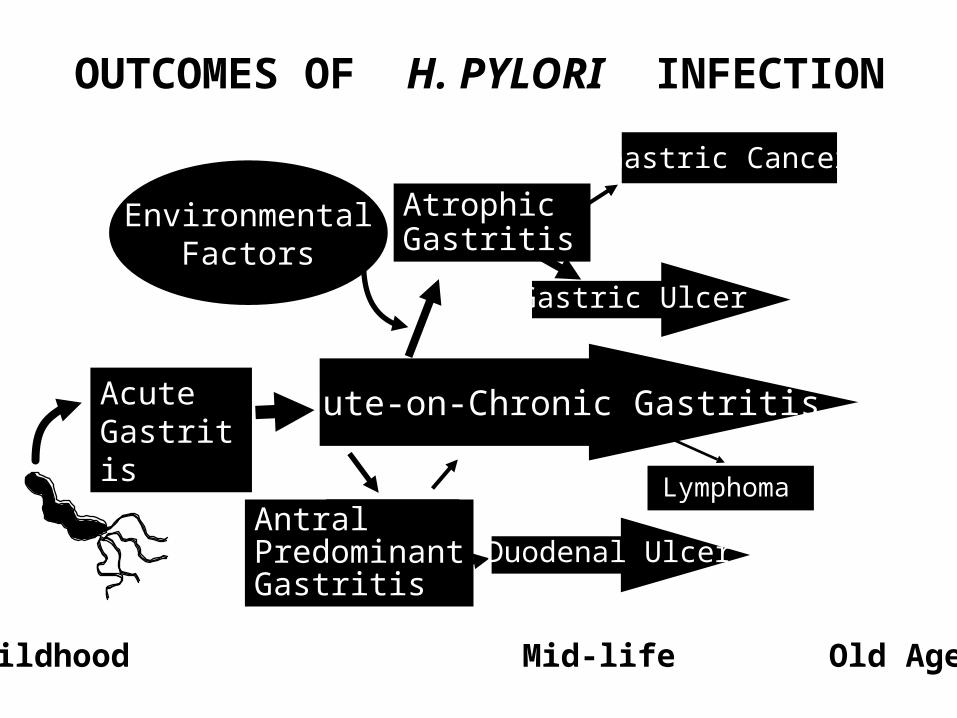
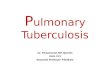
Acute-on-Chronic Gastritis
AntralPredominantGastritis
AtrophicGastritis
EnvironmentalFactors
Childhood Mid-life Old Age
Gastric Cancer
Lymphoma
Gastric Ulcer
AcuteGastritis
OUTCOMES OF H. PYLORI INFECTION
Duodenal Ulcer
H. pylori CausesPeptic ulcer disease (1 in 6)Gastric cancer (1 to 19%)Progressive gastric damage
- Iron deficiency- B12 deficiency- Reduced absorption of drugs requiring an acid stomach such as L-dopa & thyroxine
Helicobacter pyloriH. pylori is a serious chronic
transmissible infectious disease that causes damage to gastric structure and function and is a major cause of morbidity and mortality worldwide.
The prevalence of H. pylori is inversely related to the general health and well being of a society.
It should be eradicated
WHOM TO TEST
Dyspepsia (symptomatic Hp?)Ulcer Disease
-Present or past history-1st degree relatives
Gastric cancer-Family history gastric cancer-After endoscopic resection of gastric cancer
Plan to start therapy-Chronic NSAID therapy-Chronic PPI therapy (eg, GERD)
Evaluate Hp eradicationFamily members of infectedPatient desires to be tested
WHOM TO TEST
Whom to Treat for Hp
All with active Hp infection unless there is a compelling reason not to
STEPS IN THERAPY OF Hp
Diagnosis Therapy Confirm cure
Hp is an Infectious Disease
Hp therapies either succeed or fail- There is no partial success
Primary causes of failure- Resistance to one or more antibiotics- Adherence with drug regimen
Scoring “Effective” Treatment Regimens
Excellent: >95% Good: >90% Borderline: 85-89%Unacceptable <84%
Outcome Success*
* Per Protocol: reliably with susceptible strains.
The Present• No new therapies approved for more
than a decade• Old therapies have become relatively
ineffective (eg, 70% cure rates)• Overall prevalence decreasing but
still high in subpopulations (31% in VA population), 70%+ in Hispanic and Asian immigrants.
Current Therapies
• Clarithromycin based therapy• Bismuth based therapy• PPI, amox, metronidazole• Fluoroqunilone based• Rifabutin based TripleQuadruple7, 10 or 14 days duration
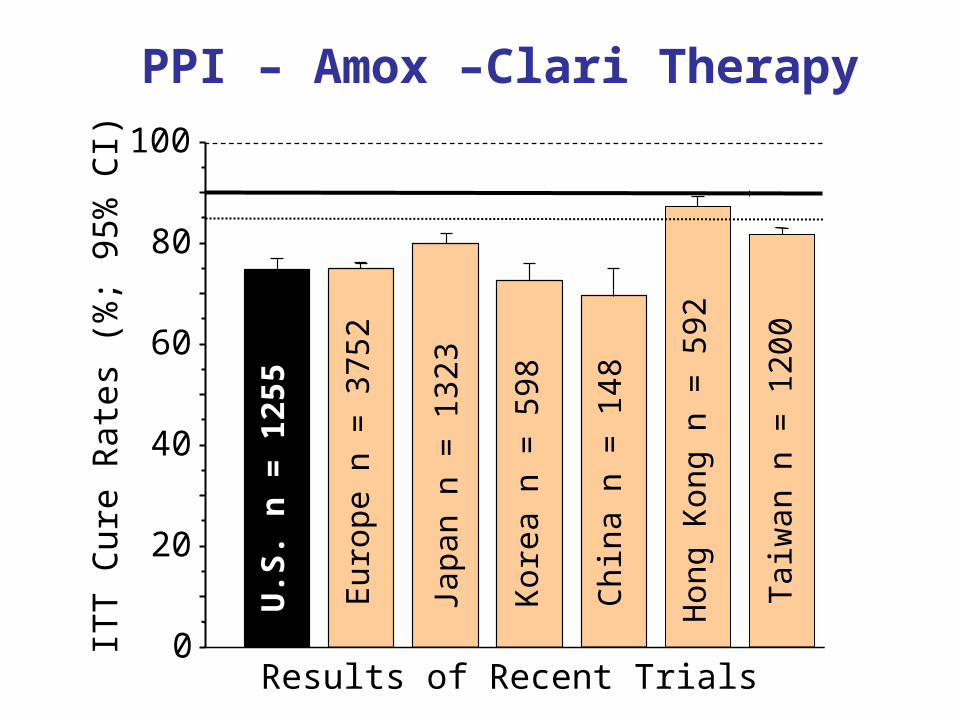
Results of Recent Trials
ITT C
ure
Rate
s (%
; 9
5%
CI)
0
20
40
60
80
100
U.S
. n
= 1
255
Eu
rope n
= 3
75
2
Kore
a n
= 5
98
Chin
a n
= 1
48
Jap
an n
= 1
32
3
Hon
g K
on
g n
= 5
92
Taiw
an n
= 1
20
0
PPI – Amox –Clari Therapy
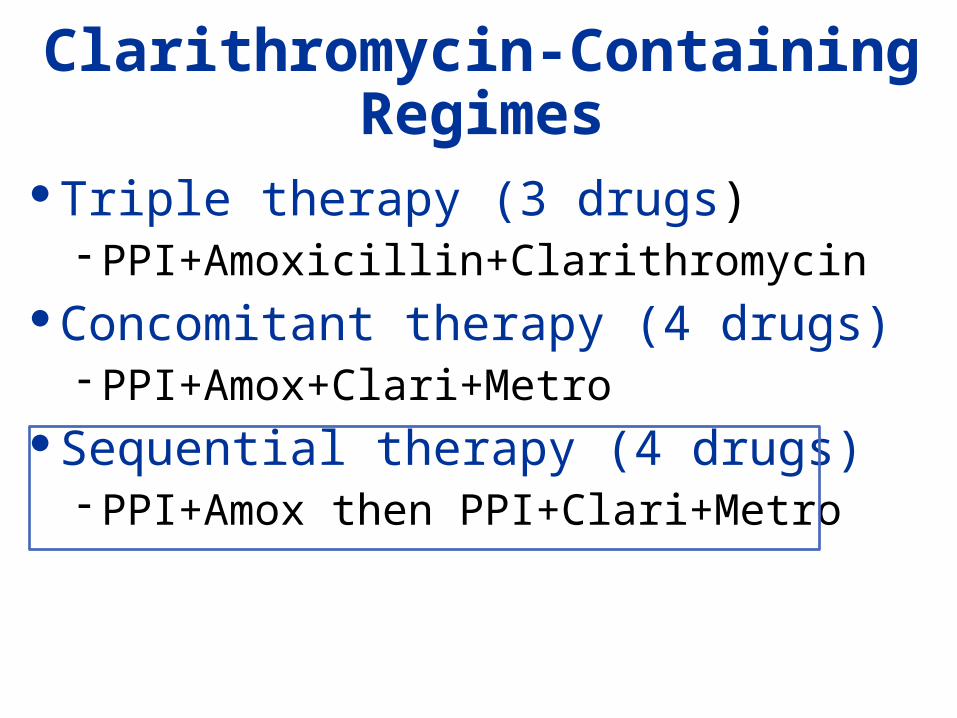
Clarithromycin-Containing Regimes
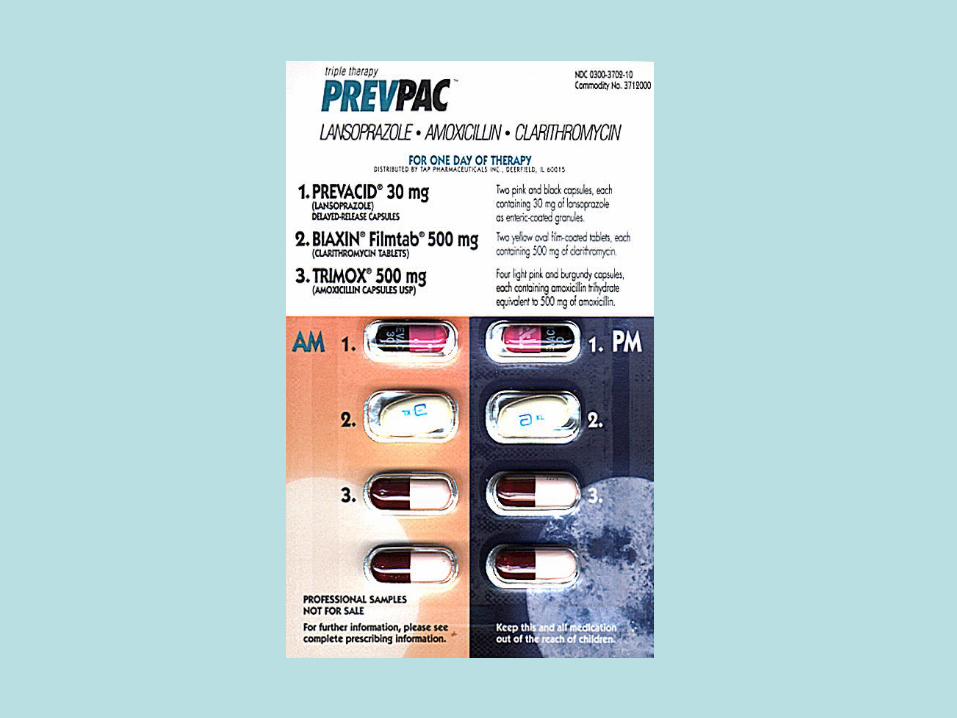
Triple therapy (3 drugs)- PPI+Amoxicillin+Clarithromycin
Concomitant therapy (4 drugs)- PPI+Amox+Clari+Metro
Sequential therapy (4 drugs)- PPI+Amox then PPI+Clari+Metro
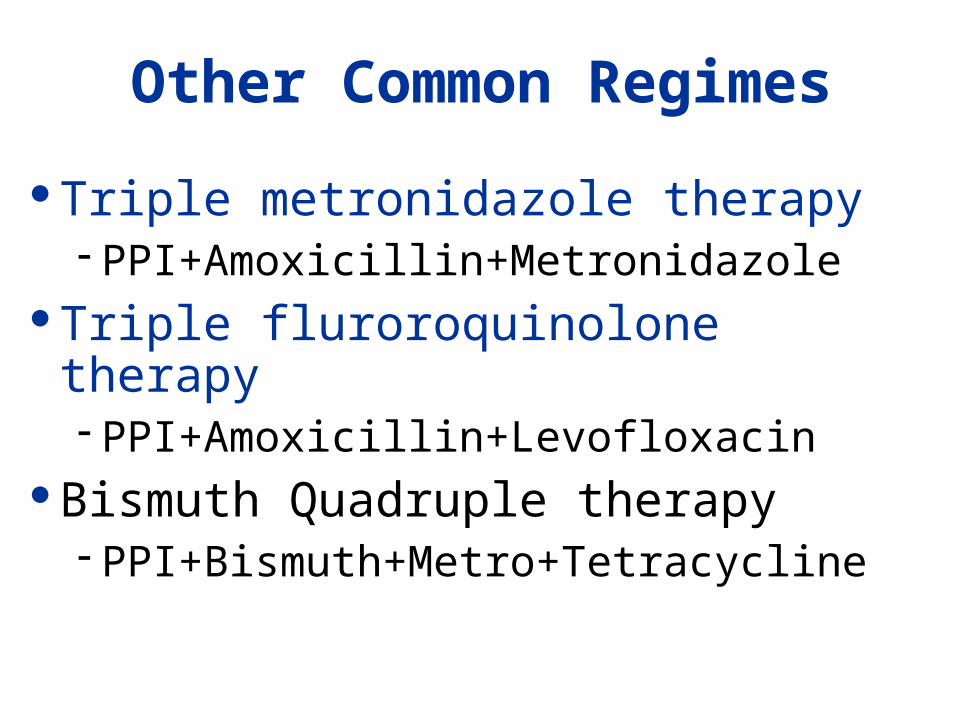
Other Common Regimes
Triple metronidazole therapy- PPI+Amoxicillin+Metronidazole
Triple fluroroquinolone therapy- PPI+Amoxicillin+Levofloxacin
Bismuth Quadruple therapy- PPI+Bismuth+Metro+Tetracycline
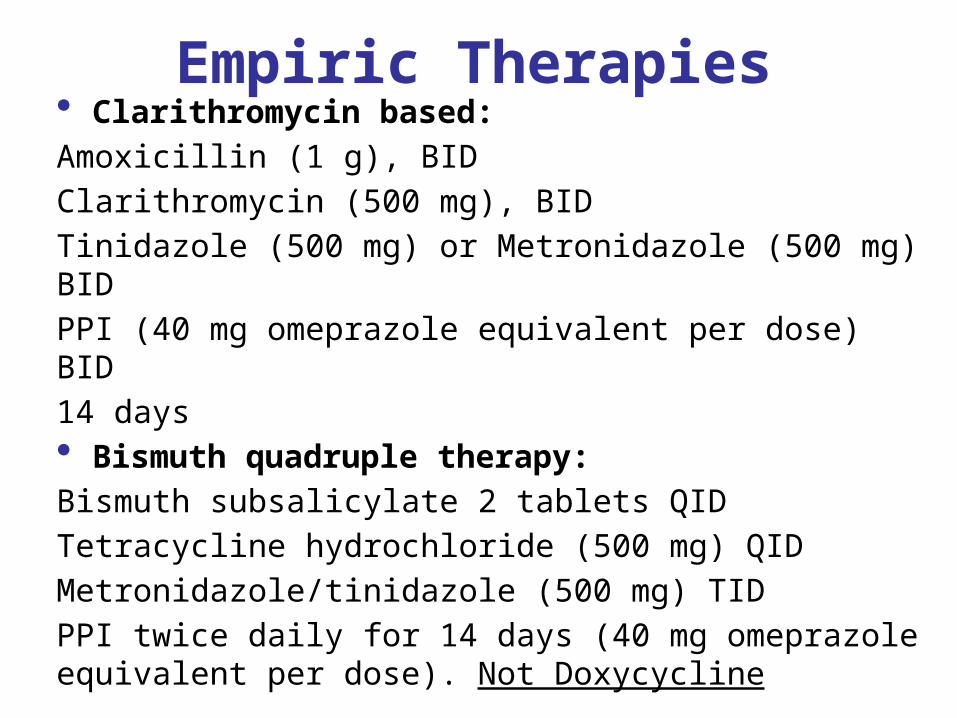
Empiric Therapies• Clarithromycin based:Amoxicillin (1 g), BIDClarithromycin (500 mg), BIDTinidazole (500 mg) or Metronidazole (500 mg) BIDPPI (40 mg omeprazole equivalent per dose) BID14 days• Bismuth quadruple therapy:Bismuth subsalicylate 2 tablets QIDTetracycline hydrochloride (500 mg) QID Metronidazole/tinidazole (500 mg) TID PPI twice daily for 14 days (40 mg omeprazole equivalent per dose). Not Doxycycline
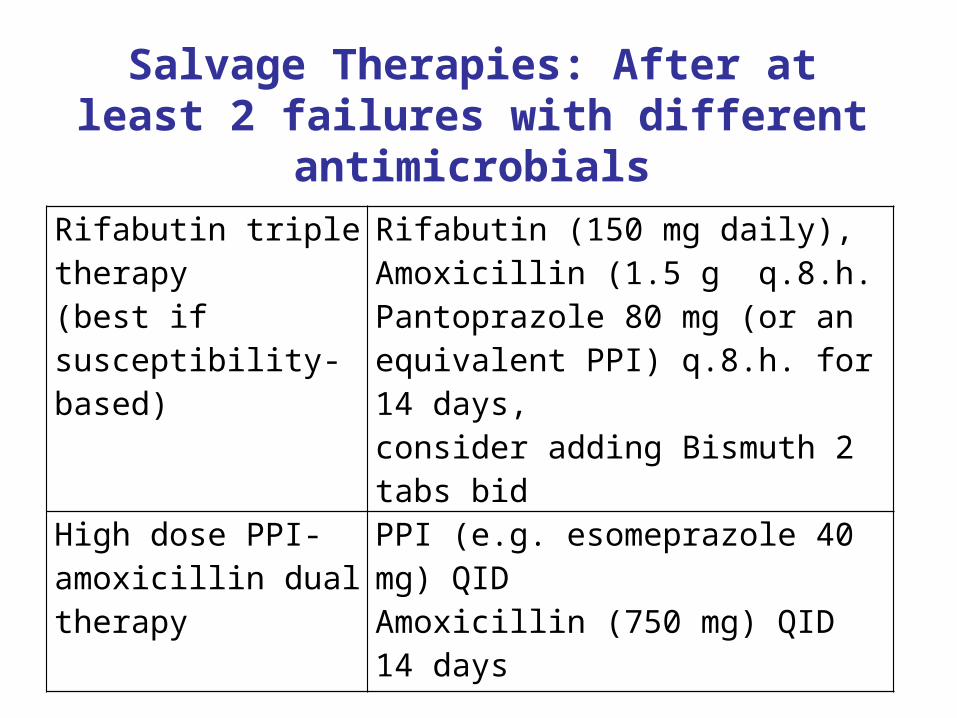
Salvage Therapies: After at least 2 failures with different antimicrobials
Rifabutin triple therapy(best if susceptibility-based)
Rifabutin (150 mg daily), Amoxicillin (1.5 g q.8.h.Pantoprazole 80 mg (or an equivalent PPI) q.8.h. for 14 days, consider adding Bismuth 2 tabs bid
High dose PPI-amoxicillin dual therapy
PPI (e.g. esomeprazole 40 mg) QID Amoxicillin (750 mg) QID14 days
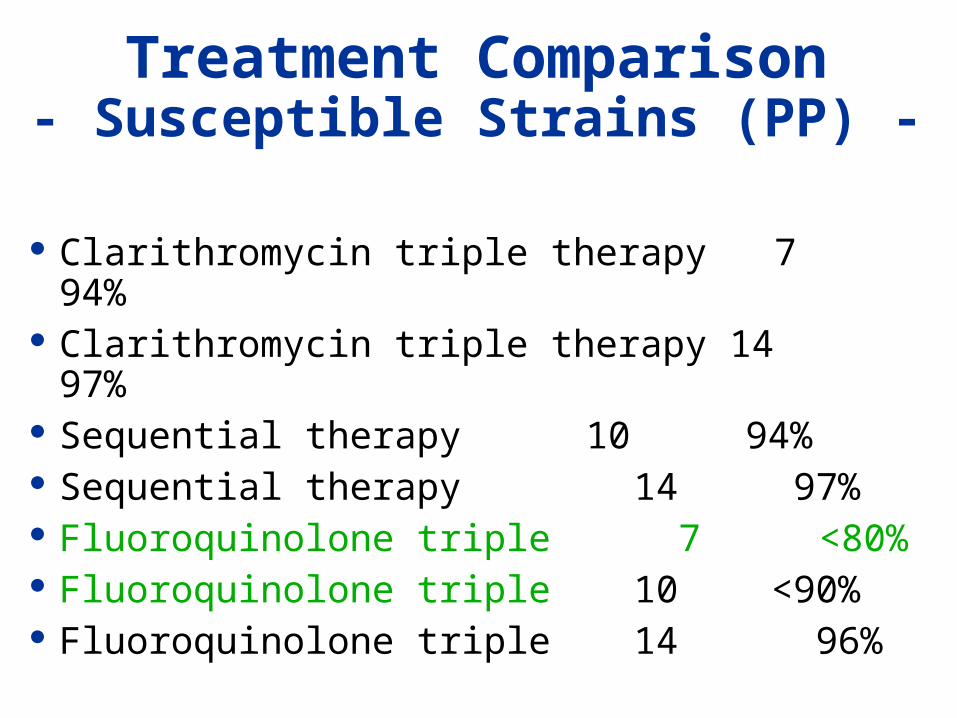
Treatment Comparison- Susceptible Strains (PP) -
Clarithromycin triple therapy 7 94% Clarithromycin triple therapy 14 97% Sequential therapy 10 94% Sequential therapy 14 97% Fluoroquinolone triple 7 <80% Fluoroquinolone triple 10 <90% Fluoroquinolone triple 14 96%
Therapy Days Success
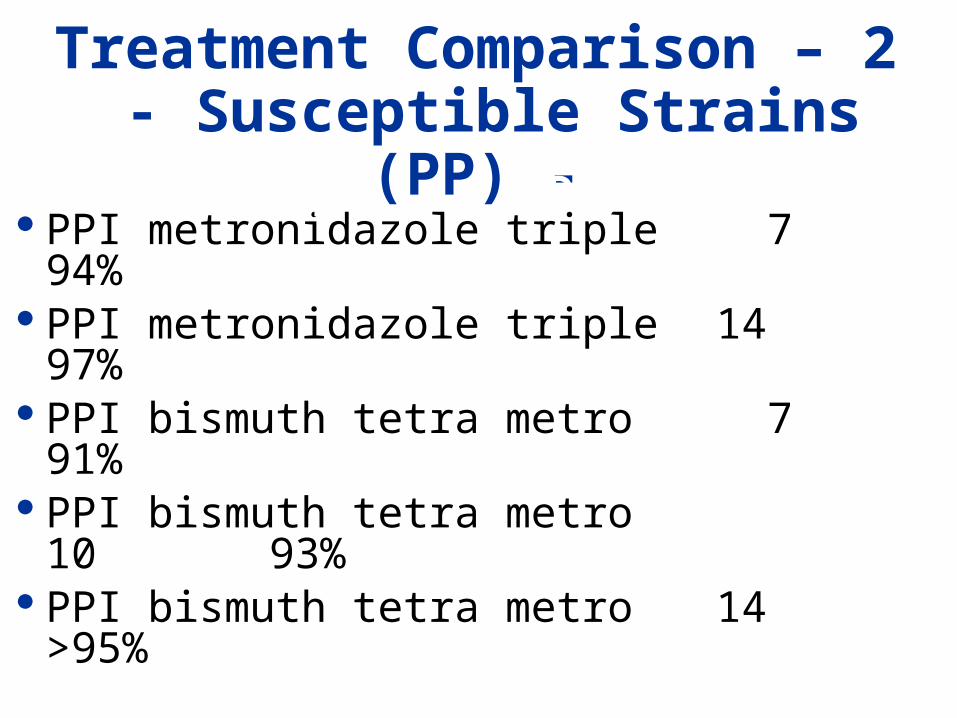
PPI metronidazole triple 7 94%
PPI metronidazole triple 14 97%
PPI bismuth tetra metro 7 91%
PPI bismuth tetra metro 10 93%
PPI bismuth tetra metro 14 >95%
Treatment Comparison – 2 - Susceptible Strains (PP) -
Therapy Days Success
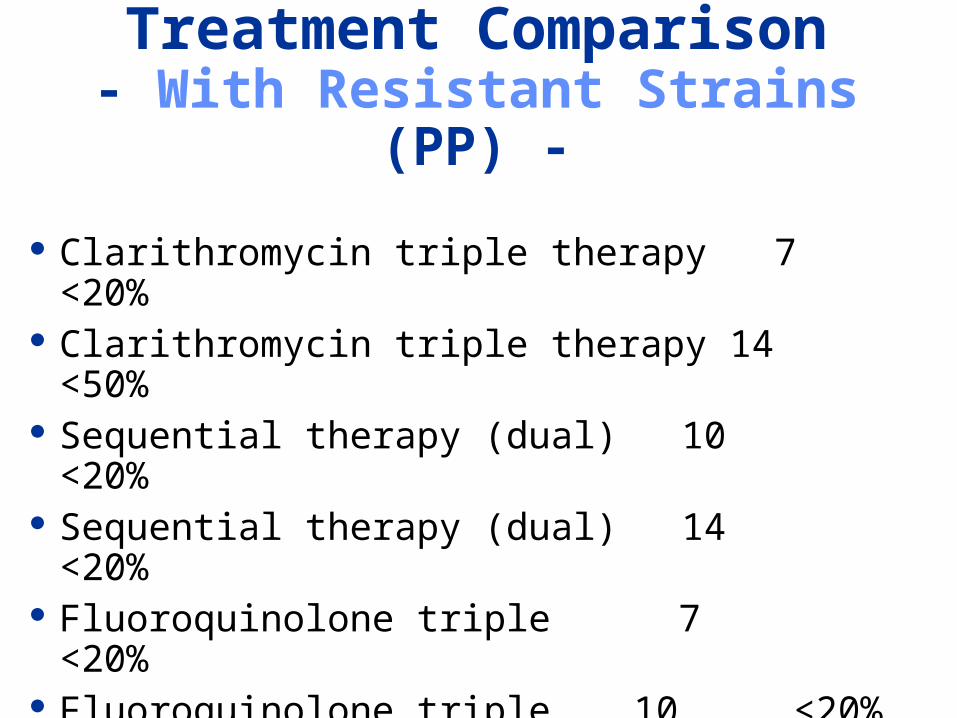
Treatment Comparison- With Resistant Strains (PP) -
Clarithromycin triple therapy 7 <20% Clarithromycin triple therapy 14 <50% Sequential therapy (dual) 10 <20% Sequential therapy (dual) 14 <20% Fluoroquinolone triple 7 <20% Fluoroquinolone triple 10 <20% Fluoroquinolone triple 14 <50%
Therapy Days Success
Triple Rx Dual (PPI +A)
Tre
atm
ent
Suc
cess
(%
)
0
20
40
60
80
100
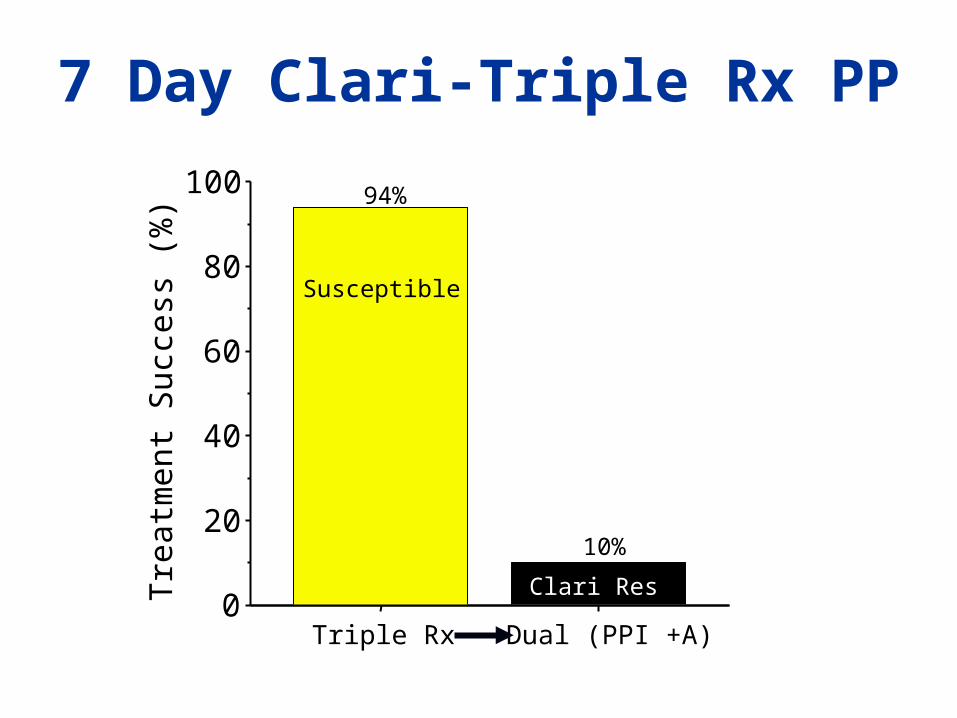
Susceptible
Clari Res
94%
10%
7 Day Clari-Triple Rx PP
98+%
95%
97%
94%
DualResistant
MetroResistan
t
ClariResista
nt
All Susce
pt7 day Clari Triple
Regimen
14 day Clari Triple
10 day Sequential
14 day Sequential
97+%
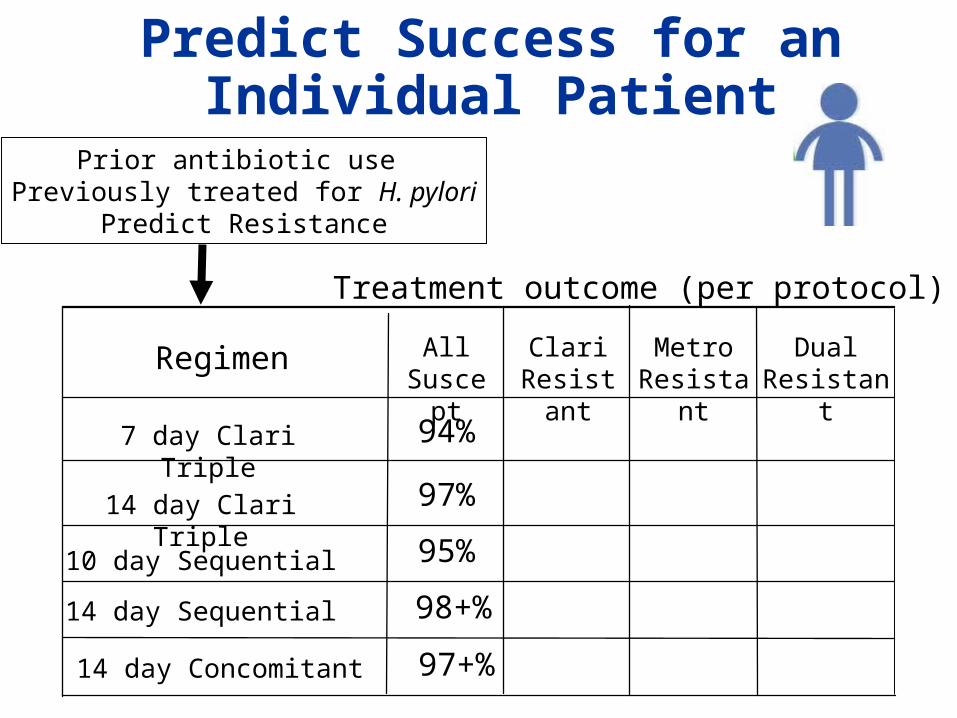
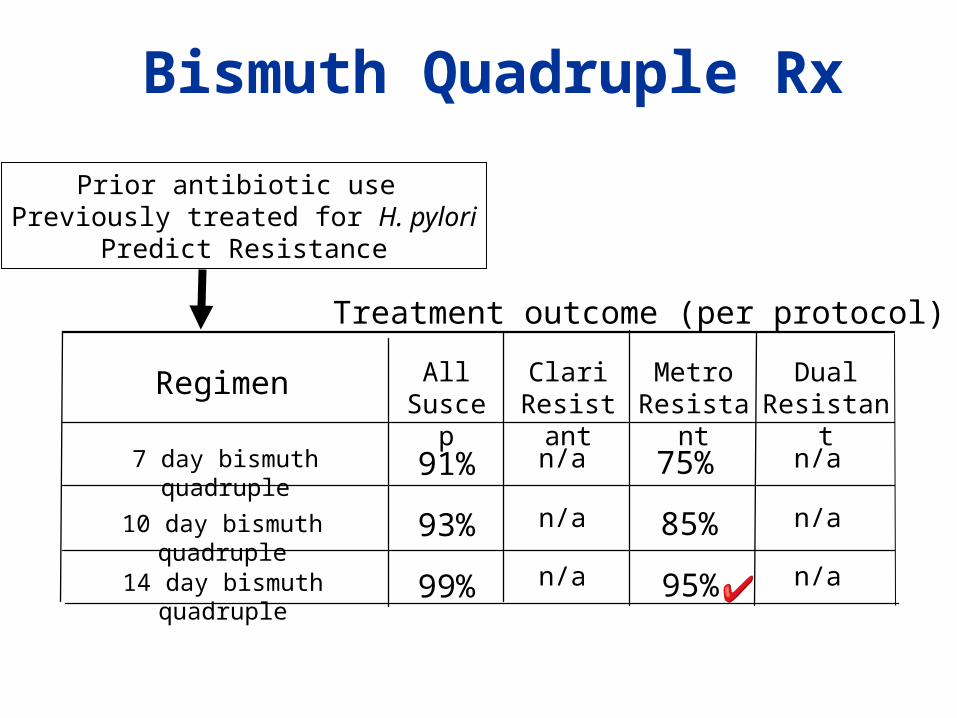
Prior antibiotic use Previously treated for H. pylori
Predict Resistance
Treatment outcome (per protocol)
Predict Success for an Individual Patient
14 day Concomitant
88%98+%
80%95%
<50%97%
<20%94%
DualResistant
MetroResistan
t
ClariResista
nt
All Susce
pt7 day Clari Triple
Regimen
14 day Clari Triple
10 day Sequential
14 day Sequential
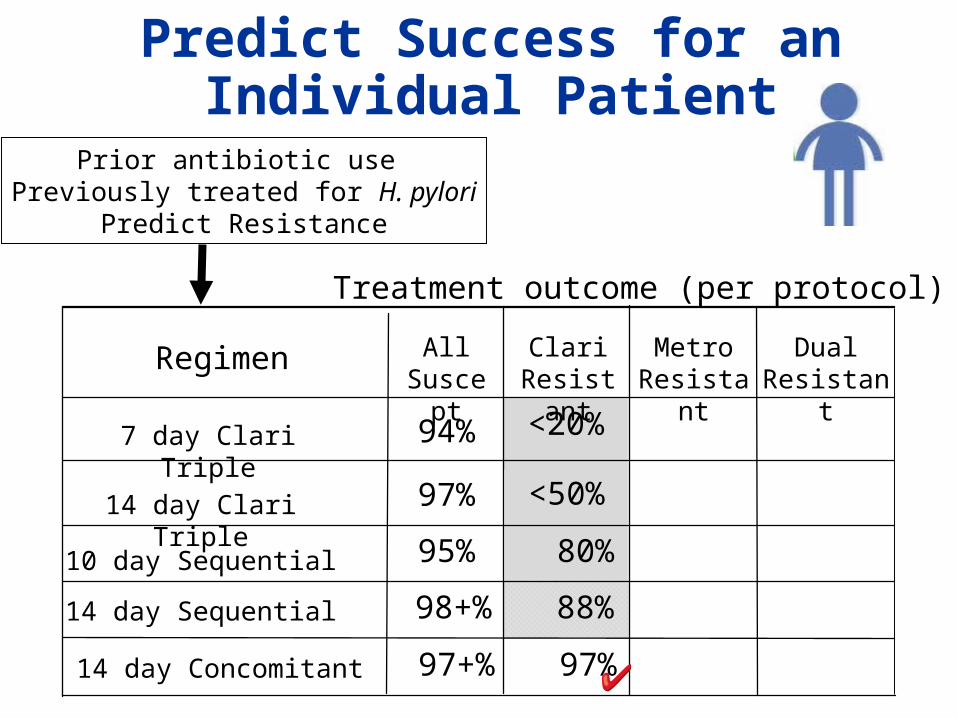
97%97+%
Prior antibiotic use Previously treated for H. pylori
Predict Resistance
Treatment outcome (per protocol)
Predict Success for an Individual Patient
14 day Concomitant
75% 88%98+%
75% 80%95%
97%<50%97%
94%<20%94%
DualResistant
MetroResistan
t
ClariResista
nt
All Susce
pt7 day Clari Triple
Regimen
14 day Clari Triple
10 day Sequential
14 day Sequential
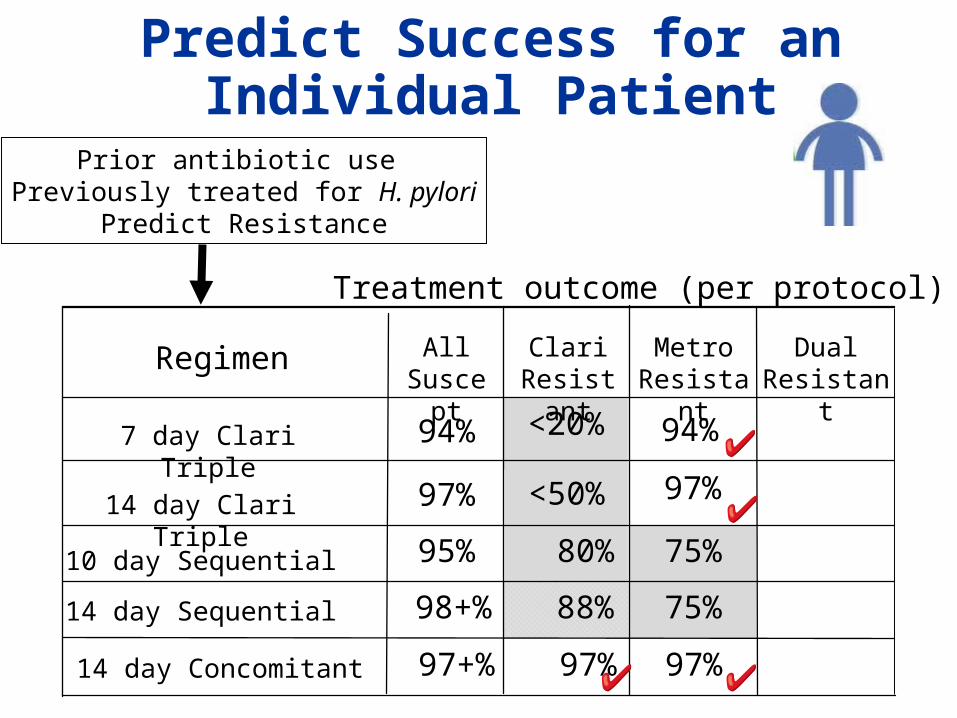
97% 97%97+%
14 day Concomitant
Prior antibiotic use Previously treated for H. pylori
Predict Resistance
Treatment outcome (per protocol)
Predict Success for an Individual Patient
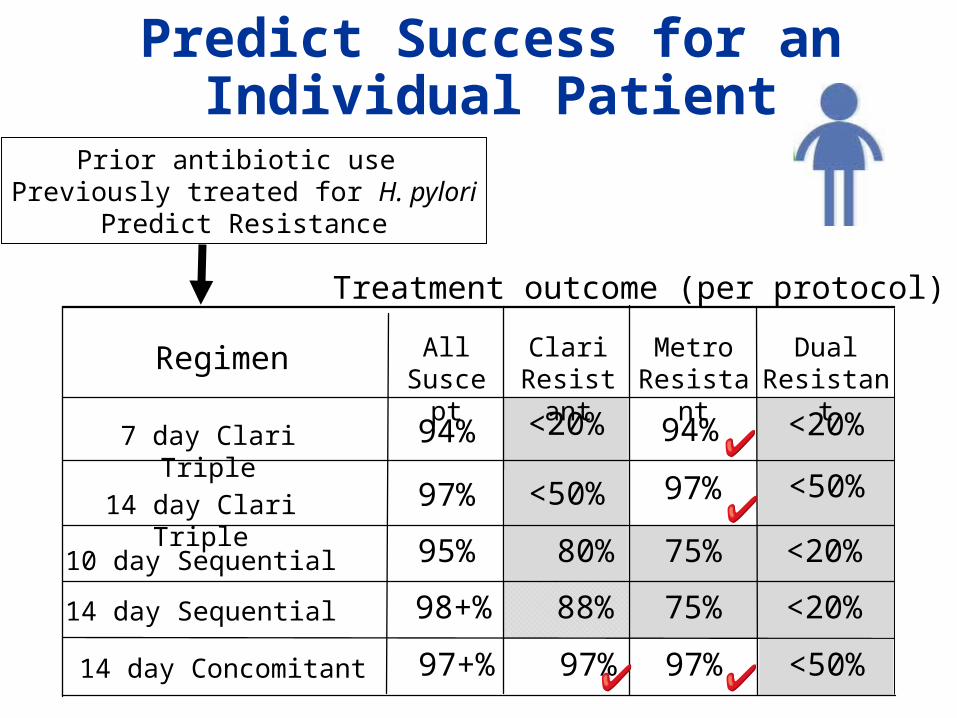
<20%75% 88%98+%
<20%75% 80%95%
<50%97%<50%97%
<20%94%<20%94%
DualResistant
MetroResistan
t
ClariResista
nt
All Susce
pt7 day Clari Triple
Regimen
14 day Clari Triple
10 day Sequential
14 day Sequential
<50%97% 97%97+%
Prior antibiotic use Previously treated for H. pylori
Predict Resistance
Treatment outcome (per protocol)
Predict Success for an Individual Patient
14 day Concomitant
DualResistant
MetroResistan
t
ClariResista
nt
All Susce
p7 day bismuth
quadruple
Regimen
Prior antibiotic use Previously treated for H. pylori
Predict Resistance
Treatment outcome (per protocol)
10 day bismuth quadruple
14 day bismuth quadruple
91%
93%
99%
75%
85%
95%
n/a
n/a
n/a
n/a
n/a
n/a
Bismuth Quadruple Rx
Bismuth Quadruple
Bismuth subsalicylate 2 tablets QID Tetracycline hydrochloride (500 mg) QID Metronidazole (500 mg) TID PPI BID 14 days.
Tetracycline is difficult to obtain Doxycycline is not a useful substitute! Helidac (not currently available)
Amoxicillin 1gm BID
“Modified”
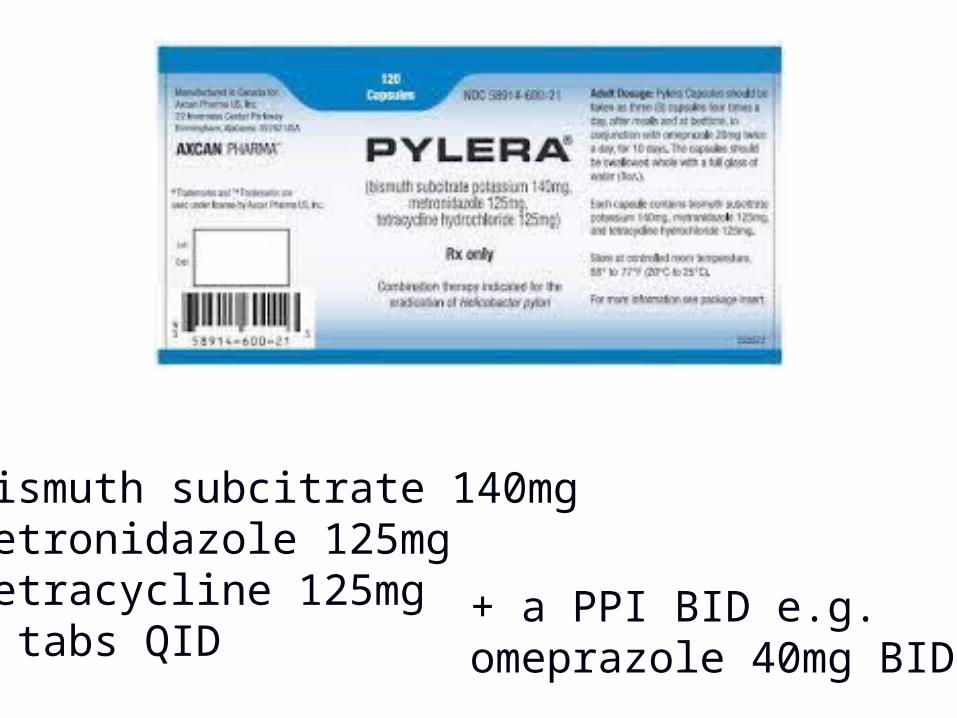
+ a PPI BID e.g. omeprazole 40mg BID
Bismuth subcitrate 140mgMetronidazole 125mgTetracycline 125mg3 tabs QID
Recommended Empiric Regimens (14 days)
Concomitant therapyBismuth quadruple therapy
- Currently only Pylera available (give for 14 days) + PPI - Do not use doxycycline
PPI: always use 40 mg omeprazole or equivalent b.i.d.
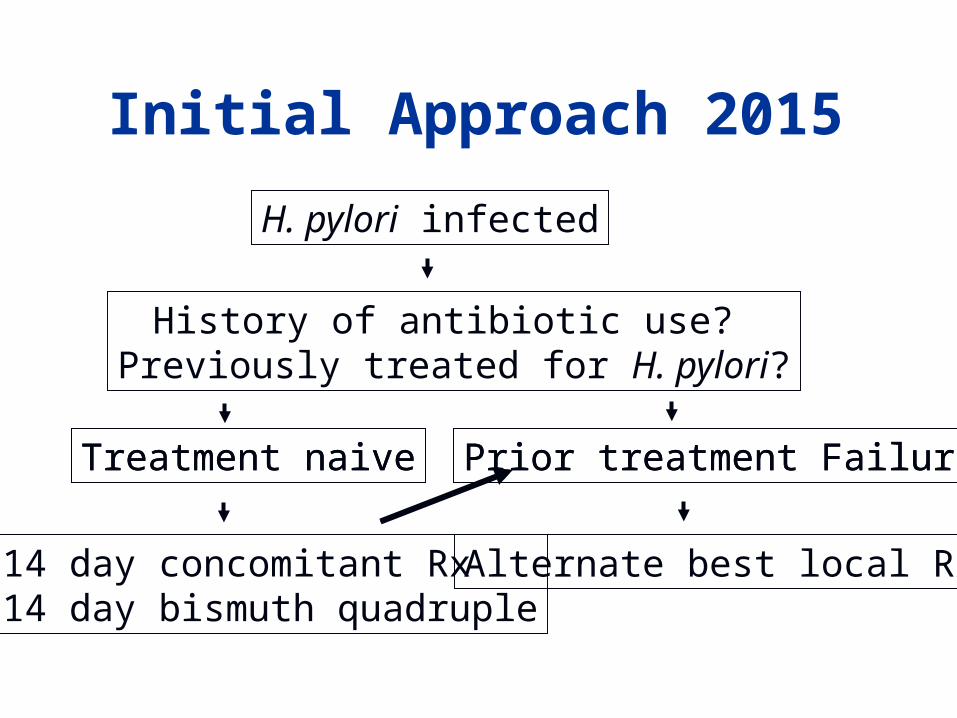
Initial Approach 2015
H. pylori infected
History of antibiotic use? Previously treated for H. pylori?
Treatment naive Prior treatment Failure
14 day concomitant Rx14 day bismuth quadruple
Treatment naive
Alternate best local Rx
Prior treatment Failure
Ensure complianceAvoid antibiotics used before (history)- Fluoroquinolones- Rifabutin- PPI – Amoxicillin high dose
Susceptibility based: Culture for antimicrobial sensitivities
Treatment Failures
In particular, don’t use these again
ClarithromycinFluoroquinolones (eg, levofloxacin)
Rifabutin
PPI + clarithromycin + amoxicillin becomes PPI + amoxicillin
14 day Fluoroquinolone
Amoxicillin 1 gram b.i.d.Levo 500 or Moxi 400 once a day PPI b.i.d.14 days (7 and 10 day = poor results)
Can not be used if a fluoroquinolone has been used in the pastBest if based on culture and susceptibility testing
Miehlke: Helicobacter 2011:16:420
Rifabutin Triple Rx
Rifabutin 150 mg once daily (b.i.d.?)
Amoxicillin 1.5 g t.i.d. Pantoprazole 80 mg t.i.d. (or
equivalent) (Consider adding bismuth 2 tabs b.i.d.)
- All for 14 days
Borody: Aliment Pharmacol Ther 2006;23:481.
* We need more studies and confirmation
High Dose PPI-Amox
PPI (eg, 40 mg esomeprazole) plus Amoxicillin 750 mg every 6 hours for 14 days.
Choice for a Population
Depends on resistance patterns - 14 day triple (only when all susceptible)
- 14 day concomitant - 14 day bismuth quadruple (dual
resistance)
Should yield >90% eradication
Clari-Containing Regimens- Conclusions -
High prevalence of clari AND met resistance (high dual resistance)- No clari-containing regimen is useful when the is a high prevalence of dual resistance
Keys to Success
Use what is effective locally- Use it exactly (dose, duration, etc)
In treatment failures, base therapy on measured susceptibility testing (Tailored therapy)
Confirm cure in all (UBT or Stool)
References