Embed Size (px)
Citation preview

When Addiction Hurts:
Managing Acute Pain in Patients on Medications for Opioid Use Disorder(MOUD)
Michelle Meyer, PharmD, BCPS, BCNSP Andrea Wetshtein, PharmD, MHSA, BCPS, CPE
OhioHealth Grant Medical Center

Conflict of Interest Disclosure
• Author’s conflicts of interest:
• Michelle Meyer, no conflict of interest
• Andrea Wetshtein, no conflict of interest

Objectives
• Review the pharmacology of currently available MOUD options
• Discuss options for treating acute pain with opioids in patients on MOUD
• Describe non-opioid options and dosing for treating pain in patients on MOUD

Medications for Opioid Use Disorder (MOUD)
• The use of medications in COMBINATION with counseling and behavioral therapies for the treatment of substance use disorders
• Three current medications approved for use as MOUD
1. Methadone
2. Buprenorphine
3. Naltrexone

Methadone
• Brand names:
– Dolophine, Methadose
• Class:
– Full Mu agonist and NMDA antagonist
• Use:
– To reduce cravings and withdrawal symptoms from opioids
• Dosage Forms:
– PO Tablets
– PO Solution
– IV Solution

Methadone
• Advantages:
– Slows brain uptake and reduces euphoria in oral dosing
– Beneficial in patients finding no response to other MOUD medications
• Disadvantages:
– Only available through outpatient treatment programs which MOST patients must visit daily
• Clinical Pearls:
– Start at no more than 30 mg total daily dose
– QTc prolonging agent– watch for drug interactions
– Use with caution in patients with liver dysfunction

Buprenorphine
• Brand Names:
– Subutex, Suboxone, Zubsolv, Sublocade
• Class:
– Partial Mu agonist
• Use:
– To reduce cravings and withdrawal symptoms from opioids
• Dosage Forms:
– Sublingual film
– Sublingual tablet
– Subcutaneous injection
– Topical patch (for pain management only)

Buprenorphine
• Advantages:
– Wider availability than methadone, patients can take at home
• Disadvantages:
– Plain buprenorphine product has high abuse potential
– High $$$ to patients
• Clinical Pearls:
– Use plain buprenorphine product in pregnant women
– Takes up to 20 min for sublingual tablet to dissolve
– Depot injection can remain in the plasma for > 12 months after reaching steady state

Naltrexone
• Brand Names:
– ReVia, Vivitrol
• Class:
– Full Mu antagonist
• Use:
– To diminish the reinforcing effects of opioids
• Dosage Forms:
– PO tablets
– Depot Injection

Naltrexone
• Advantages:
– Does not result in physical dependence
– Non-sedating
• Disadvantages:
– Poor patient compliance (with PO tabs)
– Management of acute pain crisis can pose a challenge
• Clinical Pearls:
– Initiation requires prolonged abstinence – 7 days
– Must stop PO naltrexone 48 to 72H before surgery in order for opioids to be effective
– Within the first 14 days of depot injection, unable to overcome the mu receptor blockade for pain control

Availability of MOUDMethadone = clinic
– Dosed in clinic
– Take home bottles
– Do not submit data to PMP
Buprenorphine= DATA2000 waiver (XDEA)
– Can be filled in multiple day prescription
– Dosing can be verified in state PMP
Naltrexone (REMS)
– No prescriptive restrictions
– Increasing court mandated use
– May not show up on ESI as frequently given in the office setting

Clinical Pearls for patients on MOUD
• Include the patient in the plan
• Utilize multi-modal analgesia for pain
• Require opioid tolerant doses to be effective

Patient with SUD AND Pain
Long-Acting
Opioids
Short Acting
Opioids
Symptomatic Medications

UNDER TREATMENT OF PAIN IN OPIOID USE DISORDER PATIENTS
INCREASES INCIDENCE OF RELAPSE

Approaches to Acute Pain Crisis

Approaches to Pain Crisis in Patients on MOUD
• General Considerations
– Maximize non-opioid therapies
– Patients on MOUD typically require higher doses of opioids to compensate for tolerance and/or effect of their MOUD therapy
– Try to avoid morphine as it is undistinguishable from heroin on a UDS
– Transition to oral opioids as soon as clinically appropriate
• IF patient has nausea consider utilizing sublingual opioids
– Identify and avoid a patient’s previous drug of abuse and avoid as this may aggravate their addiction disorder
ALWAYS include the patient on their pain crisis plan

Pain Crisis: Sublingual/Buccal Buprenorphine
• Buprenorphine products are not required to be stopped prior to surgery
• SL films have greater bioavailability than buccal tablets– Monitor for over or under dosing when switching between products
• Approaches for pain management for SL buprenorphine products:1) Maintain outpatient dose of Buprenorphine
OR Buprenorphine/Naloxone and split home
regimen into divided doses given every 4 -6
Hours +/- an opioid at a tolerant dose
--OR--2) Maintain outpatient dose schedule of Buprenorphine
OR Buprenorphine/Naloxone +/- an opioid at a tolerant dose
--OR--3) Discontinue Buprenorphine/Naloxone and add an opioid at a tolerant dose

Pain Crisis: Subcutaneous Buprenorphine
• The depot can be “cut out” within 14 days of administration if necessary
• Approaches for pain management for subcutaneousbuprenorphine:
– Maximize non-opioid therapy
– Add opioids at tolerant dosing if non-opioids ineffective
• Patients will require opioid tolerant dosing for pain control if they have received an injection within the past 6 months

Pain Crisis: Methadone
• Confirm home dose and when last dose given with methadone clinic
• Approaches to pain management with methadone:
– Split home dose of methadone Q8H
• Duration of analgesia of methadone is 6-8H
--OR--– Continue home DAILY dose of methadone
– May consider adding opioids at a tolerant dose for either approach
• NOTE: If patient is enrolled in a methadone clinic, they will have to provide evidence of continued administration of methadone during their hospitalization in able to remain enrolled in the outpatient program

Pain Crisis: ORAL Naltrexone
• Stop/Suspend use of oral naltrexone
– Recommend to stop 72 hours prior to any PLANNED procedures
• Add opioids at an opioid tolerant dose
Other Considerations:
– Regional anesthetic techniques
– Ketamine
• Typically dosed @ 0.1mg/kg/hr
• NOTE: A 7-10 day opioid free period is recommended before naltrexone can be resumed

Pain Crisis: DEPOT Naltrexone
• Determine when the last naltrexone injection was administered
• 0 to 14 days
– Maximize adjuvant therapies
– Regional anesthetic techniques
– Continuous ketamine infusion at 0.1mg/kg/hr
– Opioids are ineffective during this time frame
• 15 to 28 days:
– All recommendations for 0-14 days +/- opioids at a tolerant dose
• NOTE: Coordination with naltrexone provider is key

Multimodal Therapies to the Rescue!

Rational Polypharmacy
23
Brain
Spinal Cord
PNS
Descending Inhibition(NE, 5HT)
Central Sensitization(Ca2+ channels, NMDA receptors)
Peripheral Sensitization (Na+ channels)
NSAIDsOpioidsTCALidocaine
TCAGabapentinOpioidsKetamine
TCA SNRITramadolOpioids
Mechanism-Specific TreatmentMultiple targets…

Multimodal Therapies
• Inpatient titration of anti-epileptic drugs can be more aggressive with balancing of sedation-caution if renal impairment
• Schedule adjunct meds to maximize effects
• Pre-operative cocktails could include APAP, anti-epileptic, NSAID, epidural or local block
• Non-pharmacological treatments-heat/ice, massage, healing touch, physical therapy
24

IV Acetaminophen
• Higher plasma concentrations of APAP when given IV vs oral
• Levels quickly become equivalent to oral administration
• Dose oral APAP 1 hr prior to surgery
25

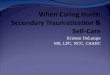
IV APAP Literature Recap
Am J Health Syst Pharm. 2018 Mar 15;75(6):367-375.
Hickman et. al.IV (n = 241)
PO (n = 245)
P-value
Median opioid use first 24hr* 21.7 mg 21.7 mg 0.60
Median time to first pain med 41 mins 38 mins 0.90
Median time to ambulation 18.8 hrs 18.5 hrs 0.54
Median PACU LOS 2.1 hrs 2.2 hrs 0.17
Median hospital LOS 58.5 hrs 58 hrs 0.63
Post-op nausea 21.2 % 21.6 % 0.91
Post-op vomiting 7.9 % 6.9 % 0.73
*Opioid use in morphine mg equivalents. PACU=post-op anesthesia care unit, LOS=length of stay

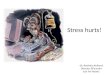
Liposomal Bupivacaine (Exparel®)
00.5
11.5
22.5
33.5
4
Mean Pain Score POD3
0
20
40
60
80
100
120
Opioid Use
0
0.5
1
1.5
2
2.5
LOS
Knee. 2012 Oct;19(5):530-6; J Arthroplasty. 2016 Sep;31(9 Suppl):22-5; J Arthroplasty. 2014 Apr 4. pii: S0883-5403(14)00222-8.

Value Based Analgesia
• IV Acetaminophen
– No published trials demonstrating outcome differences when compared to oral APAP
– Cost of 975mg oral APAP=$0.06 vs IV 1000mg APAP=$48.18
• Liposomal Bupivacaine
– Published data shows no significant difference in outcomes when compared to active comparators
– Cost of bupivacaine 0.5% with epinephrine=$1.77 vs liposomal bupivacaine $301.49
28
Choose your patients thoughtfully with high cost/low value adding medications

Ketamine
• Mechanism of Analgesia: NMDA antagonism
– Some effects on μ-opioid receptors, muscarinic receptors, monoaminergic receptors, γ-aminobutyric acid receptors, and several others
• Analgesic, anti-inflammatory, and anti-hyperalgesic effects
Dosing For Pain Dosing For Anesthesia Intravenous
0.3–0.5 mg/kg bolus 0.1–0.2 mg/kg/hour
Intravenous 1–4.5 mg/kg bolus0.5–4.5 mg/kg/hour
Oral10 mg PO TID
1 mg/kg divided in equal doses Q8H

Ketamine
• Who can benefit?– Surgical patients with expected SEVERE post-operative pain
– Opioid tolerant or dependent patients with exacerbation of a chronic condition or requiring surgery
– Patients at increased risk for opioid-related respiratory depression
• Contraindications– Poorly controlled cardiovascular disease
– Severe hepatic dysfunction
– Poorly controlled psychiatric conditions with psychosis

Lidocaine Infusion
• Mechanism of Analgesia
– Attenuates nociceptive sensitization via sodium channel blocking
– Decreases the NMDA receptor mediated post-synaptic depolarization
– Proposed that ischemic nerves are more affected than non-stimulated nerves
• Analgesic, anti-inflammatory, and anti-hyperalgesic effects
• Dosing regimens vary
– 1-2mg/kg bolus followed by 0.5-3mg/kg/hr
– 2-5mg/kg(150mg) IVPB x 1 over 2 hours

Lidocaine Infusion
• Who makes a good candidate?
– Opioid-refractory nociceptive pain
– Central and peripheral neuropathic pain
– Increasing opioid requirements
• Relative contraindications
– History of arrhythmia, ischemic disease, syncope
– 1st and 2nd degree heart block
– Use of alpha agonists or beta blockers
– Congestive heart failure
32

Lidocaine Infusion
• Monitoring
– 1st order kinetics, level proportional to infusion dose
– Efficacy measured by patient reported and any decrease in MME
– Side effects and early signs of toxicity via patient report
• Concern for toxicity in patients, especially renal or cardiac failure
– CNS symptoms tongue numbness->metallic taste->light-headedness->visual changes->mental status changes->coma->respiratory arrest
– Continuous cardiac monitoring recommended with this patient population

Putting It All TogetherApply what you’ve learned

Patient Case-Methadone
• 38 yo female presents with fever, severe L arm pain secondary to multiple abscesses. Her abscesses are going to require I&D and she is concerned with her pain control and is extremely fearful of withdrawal. She has a history of OUD, but has been in remission for the past 2 years and is being managed by the local methadone clinic. Her current MOUD is methadone 120 mg PO Qday. She usually will take acetaminophen as needed for any minor aches and pain. She requests not to be started on oxycodone, as she reports this was her drug of choice when she was using.
• What recommendations would you make to the hospitalist to control this patient’s pain?

Patient Case: Buprenorphine
• 57 y.o. male presented to your hospital for a TKA. He has a history of HTN, DM2 and substance use disorder. His SUD is currently being managed with buprenorphine-naloxone sublingual tablets 8-2mg SL twice daily. He is anxious about controlling his pain after surgery.
• What recommendations would you make to the surgery team in order to control this patient’s pain?

Patient Case: Naltrexone
• 43 yo male presents as a level 2 trauma after an MVC. He has multiple rib fractures, a sternal fracture, and a L humerus fracture. In the trauma bay he continuously rates his pain as 10/10 and has not responded to IV hydromorphone 1mg.
• A nurse finds a medication alert necklace which shows the patient is on naltrexone. He then reports that he recently received a dose of depot naltrexone 18 days ago
• What recommendations would you provide the trauma team for the management of this patient’s pain?

Patient Case: Naltrexone
• 37 yo male admitted s/p GSW to the head. He was administered one dose of depot naltrexone 7 days prior to admission. The patient’s family would like to transition to comfort measures only due to the nature of his injuries but are worried about maintaining the patient’s comfort due to his naltrexone injection.
• What are your concerns with the date of his last naltrexone injection?
• What recommendations do you have for the team to control the patient’s pain for comfort care?

Patient Case: Naltrexone
• Limited options to manage pain and end-of-life symptoms
– Typically rely on opioids in patients not receiving naltrexone
– Patient is still experiencing complete mu-receptor blockage as the injection was only one week prior to admission
– Attending teams uncomfortable with the amount of opioids theoretically required to overcome blockade
– Management of dyspnea was also difficult due to mu-receptor blockade
• Ketamine infusion was started at 0.1 mg/kg/hr
– What are some concerns/cautions with use of ketamine?
– What is the maximum recommended dose for pain management?
– Can nurses push ketamine for pain management?

Patient Case: Naltrexone
• Ketamine was titrated up to 0.4 mg/kg/hr for comfort
– Symptoms were well controlled
– Patient respirations were easy
– Patient passed away peacefully
• What if we didn’t know the last date of naltrexone administration? How would this have changed our therapy plan?
• What if the patient had received naltrexone 20 days prior to admission? What alternatives could be considered?

References
• Prunty LM, Prunty JJ. Acute opioid withdrawal: identification and treatment strategies. US Pharm. 2016;41(11):HS2-HS6. • Baron D, Garbely J, Boyd RL. Evaluation and management of substance abuse emergencies. Primary Psychiatry. 2009. 16(9). • Connery HS. Medication-assisted treatment of opioid use disorder: review of the evidence and future directions. Harv Rev Psychiatry. 2015 Mar; 23(2):63-
75.• Thomas CP, Fullerton CA, Kim M, Delphin-Rittmon ME, et al. Medication-assisted treatment with buprenorphine: assessing the evidence. Psychiatr Serv.
2014 Feb; 65(2):158-70.• Fullerton CA, Kim M, Thomas CP, Delphin-Rittmon ME, et al. Medication-assisted treatment with methadone: assessing the evidence. Psychiatr Serv.
2014 Feb; 65(2):146-57.• Volkow ND, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies- tackling the opioid-overdose epidemic. N Engl J Med. 2014
May;3780(22):2063-66. • Sin B, Ternas T, Motov SM. The use of subdissociative-dose ketamine for acute pain in the emergency department. Acad Emerg Med. 2015 Mar;
22(3):251-7.• Persson J. Ketamine in pain management. CNS Neurosci Ther. 2013 Jun; 19(6):396-402. • Schwenk ES, Viscusi ER, Buvanedran A, Hurley RW, Wasan AD, Narouze S, Bhatia A, Davis FN, Hooten WM, Cohen SP. Consensus guidleines on the
use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Scoeity of Anesthesiologists. Regional Anesthesia and Acute Pain. 2018 July; 43(5):1-11.
• CDC. Opioid Data Analysis. Feb 9, 2017. Retrieved from https://www.cdc.gov/drugoverdose/data/analysis.html.• Ohio Dept of Health, 2015 Ohio Dru Overdose Data at a Glance. Aug 25, 2016. Retrieved from http://www.odh.ohio.gov/en/health/vipp/drug/dpoison.• Salehi, M., Khierabadi, G., et al. Importance of Gabapentin Dose in Treatment of Opioid Withdrawal. J of Clin Psychopharm. 2011 October; 31(5):593-596• “Clinical Opiate Withdrawal Scale Induction Flowsheet”, National Alliance of Advocates for Buprenorphine Treatment.
https://www.naabt.org/documents/COWS_induction_flow_sheet.pdf, Accessed 22 March 2018• Lachiewicz, PF. The role of intravenous acetaminophen in multimodal pain protocols for perioperative patients. Orthopedics. 2013; 36 (2): 15-19• Hickman, S. et al. Randomized trial of oral versus intravenous acetaminophen for postoperative pain control. Am J Health Syst Pharm. 2018 Mar
15;75(6):367-375.• Yu, Z, Yang, Z, Yao, L. Effectivenss of liposome bupivacaine for postoperative pain control in total knee arthroplasty. A PRISMA-compliant meta-analysis
of randomized controlled trials. Knee. 2012 Oct;19(5):530-6; J Arthroplasty. 2016 Sep;31(9 Suppl):22-5; J Arthroplasty. 2014 Apr 4.• Noviasky, J et al. Bupivacaine Liposomal vs Bupivacaine: Comparative Review. Hosp Pharm. 2014 June; 49(6): 539-543

When Addiction Hurts:
Managing Acute Pain in Patients on Medications for Opioid Use Disorder (MOUD)
Michelle Meyer, PharmD, BCPS, BCNSP Andrea Wetshtein, PharmD, MHSA, BCPS, CPE
OhioHealth Grant Medical Center

PCSS Mentoring Program
� PCSS Mentor Program is designed to offer general information to clinicians about evidence-based clinical practices in prescribing medications for opioid addiction.
� PCSS Mentors are a national network of providers with expertise in addictions, pain, evidence-based treatment including medication-
assisted treatment.
• 3-tiered approach allows every mentor/mentee relationship to be unique and catered to the specific needs of the mentee.
• No cost.
For more information visit:
pcssnow.org/mentoring

PCSS Discussion Forum
Have a clinical question?

American Academy of Family Physicians American Psychiatric Association
American Academy of Neurology American Society of Addiction Medicine
Addiction Technology Transfer Center American Society of Pain Management Nursing
American Academy of Pain Medicine Association for Medical Education and Research in Substance Abuse
American Academy of Pediatrics International Nurses Society on Addictions
American College of Emergency Physicians American Psychiatric Nurses Association
American College of Physicians National Association of Community Health Centers
American Dental Association National Association of Drug Court Professionals
American Medical Association Southeastern Consortium for Substance Abuse Training
American Osteopathic Academy of Addiction Medicine
PCSS is a collaborative effort led by the American Academy of Addiction Psychiatry (AAAP) in partnership with:

Educate. Train. Mentor
www.pcssNOW.org
@PCSSProjects
www.facebook.com/pcssprojects/
Funding for this initiative was made possible (in part) by grant nos. 5U79TI026556-02 and 3U79TI026556-02S1 from SAMHSA. The views expressed in
written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department of Health
and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government.