Embed Size (px)
Citation preview

Treatment of Endocarditis
Judgment Calls
When to Replace vs. Spare the Aortic
Valve and Root
Tirone E. David
University of Toronto

Conflict of Interest
None

AV Endocarditis
When to Replace vs. Spare the AV & Root
• Infection limited to the aortic cusps
Valve replacement
Valve repair

Localized vegetation excision patch repair
AV Endocarditis

CORMATRIX
Extracellular matrix from porcine jejunal mucosa

AV Endocarditis
When to Replace vs. Spare the AV & Root
• Infection limited to the aortic cusps
Valve replacement
Valve repair
• Infection involving valve annulus and surrounding
tissues with abscess formation:
Radical resection and reconstruction

Anatomy of the Base of Heart
AV
TV
PV
IVFB

Aorto-Mitral Continuity

Aorto-Mitral Continuity

Abscess in the Intervalvular Fibrous Body





Case Study
79 y.o.♂ with known asymptomatic aortic stenosis
developed signs and symptoms of acute sepsis.
Blood culture grew Staphylococcus aureus. He was
started on appropriate antibiotics but remained
febrile after 4 days of treatment. He was transferred
for surgical treatment. Coronary angiography showed
75% stenosis of the LAD.













Case study:
53 year-old man had AVR with a bioprosthetic
valve for bicuspid aortic valve stenosis. Three years
later he developed endocarditis due to Staphylococcus
aureus. Treatment with antibiotics failed and he
developed an extensive aortic root abscess surrounding
the left main coronary artery and dominant circumflex.
He was transferred to Toronto General Hospital for
surgery.

TEE: Extensive Aortic Root Abscess

TEE: Extensive Aortic Root Abscess

TEE: Abscess Involves Circumflex Artery

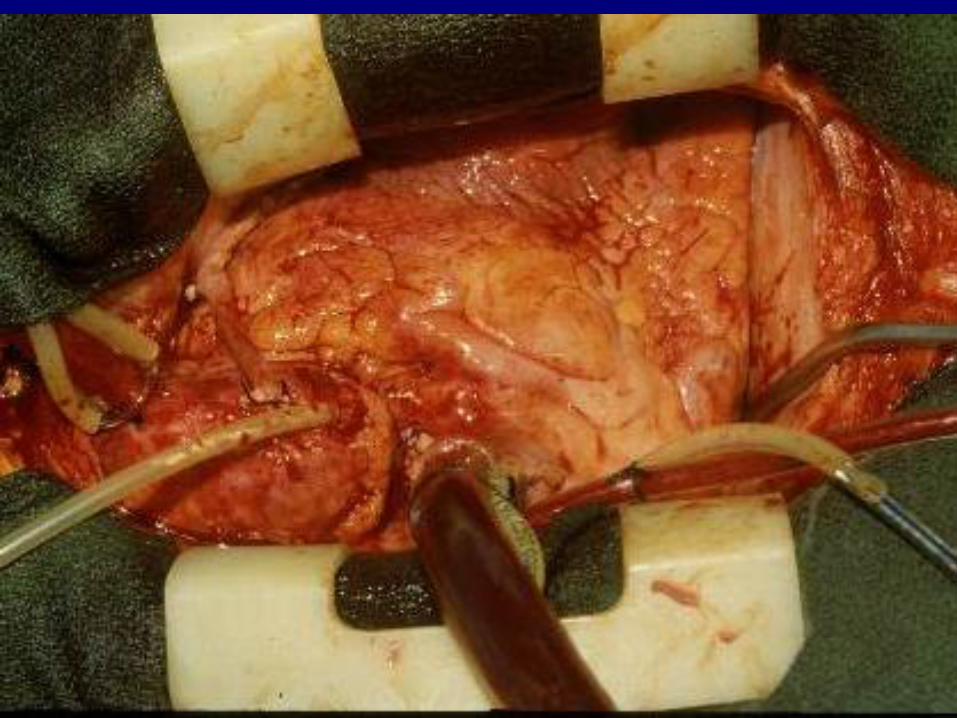
Extensive Aortic Root Abscess


TEE: Postoperative Aortic Homograft

TEE: Postoperative LV Function
383 patients
Mean age: 51±16 years
Mean follow-up: 6.1±5.2 years
84% in NYHA class IV
14% in cardiogenic/septic shock
31% paravalvular abscess

Surgery for Infective Endocarditis David et al. JTCVS 2007;133:144-9
Native valve: 266 94 – AV
77 – MV
74 – AV + MV
9 – AV + other
12 – Other
Prosthetic valve: 117 66 – AV
32 – MV
15 – AV + MV
1 – PV
Surgery for Infective Endocarditis David et al. JTCVS 2007;133:144-9
Microorganisms:
23% - S. Aureus
10% - S. Epidermidis
18% - S. Viridans
5% - Enterococcus

Surgery for Infective Endocarditis David et al. JTCVS 2007;133:144-9
PVE, shock, abscess and S.aureus = independent predictors

Surgery for Infective Endocarditis David et al. JTCVS 2007;133:144-9
Patients’ survival

Surgery for Infective Endocarditis David et al. JTCVS 2007;133:144-9
Freedom from recurrent infective endocarditis

David TE et al.
Surgical treatment of paravalvular abscess: Long-term results.
Eur J Cardiothorac Surg 2007:31:43-8
135 patients
Sex: 68% men
Mean age: 51 ± 16 years
NYHA functional classes I - III = 13%
IV = 87%
ECG: Sinus - 72%
AF - 21%
CHB - 7%

Clinical Profile of Patients
• Native valve endocarditis: 51%
• Prosthetic valve endocarditis: 49%
• Cardiogenic/septic shock: 17%
• Preoperative renal failure: 12%
• Recent stroke (<30 days): 24%
• Timing of surgery:
Same hospitalization - 37%
Urgent/emergent - 65%
David et al. EJCTS 2007

Clinical Profile of Patients
Microorganisms:
• 34% - Staphylococcus aureus
• 19% - Staphylococcus epidermidis
• 16% - Streptococcus viridans
• 4% - Enterococcus faecalis
• 14% - Streptococci - other
• 8% - Other bacteria
• 4% - Culture negative
53%

Surgical Pathology
• Location of abscess:
54% - limited to aortic annulus
20% - limited to mitral annulus
21% - aortic annulus + mitral annulus
3% - aortic annulus + mitral + tricuspid
2% - aortic annulus + tricuspid +/- pulmonary

Operations Performed
• Reconstruction of LVOFT 75%
• Reconstruction of posterior MA 16%
• Recons. LVOFT and posterior MA 5%
• Bentall 21%
• Replacement of the ascending aorta 4%
• Repair of congenital VSD 4%
• CABG 17%

Operations Performed
• AVR 43%
• AVR + MVR 26%
• AVR + MVR + TV repair 4%
• AVR + MV repair 9%
• MVR 6%
• AVR + PVR 1%
• AVR + TVR + PVR 1%

Operations Performed
• Patches used:
Fresh autologous pericardium 40%
Bovine pericardium 53%
Dacron graft 3%
MV leaflet of aortic homograft 4%
• Heart valve used for replacement:
Mechanical 49%
Bioprosthetic 41%
Aortic homograft 10%
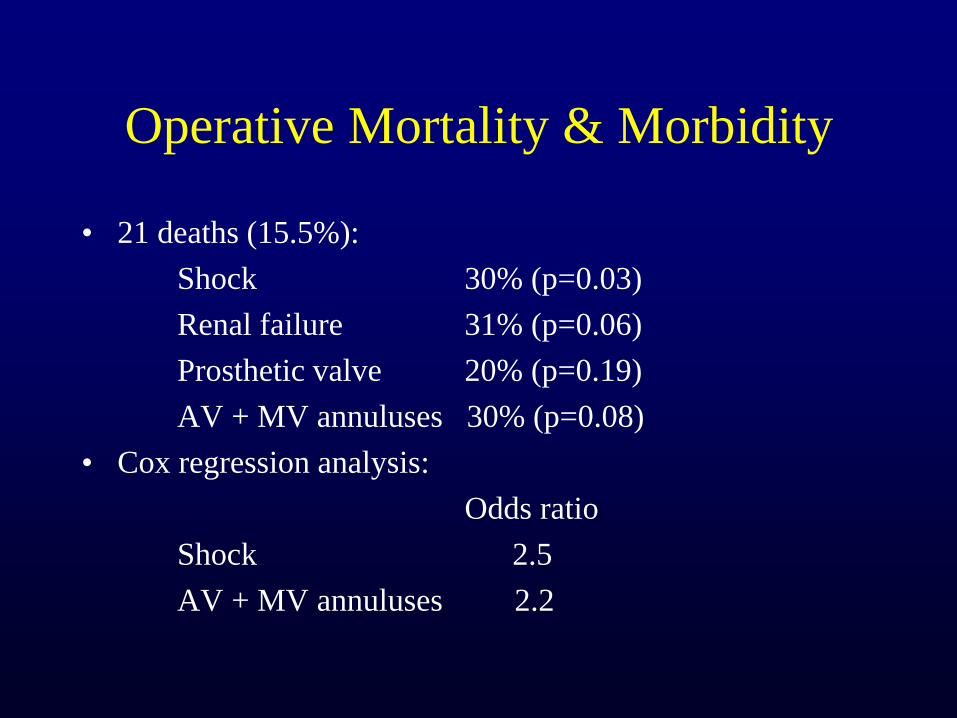
Operative Mortality & Morbidity
• 21 deaths (15.5%):
Shock 30% (p=0.03)
Renal failure 31% (p=0.06)
Prosthetic valve 20% (p=0.19)
AV + MV annuluses 30% (p=0.08)
• Cox regression analysis:
Odds ratio
Shock 2.5
AV + MV annuluses 2.2

Follow-up
• Mean follow-up: 6.2±5.2 years
• 100% complete
• 34 late deaths
• 16 bouts of recurrent endocarditis in 15 patients
• 15 reoperations in 14 patients
• 4 primary tissue failure
• 7 paravalvular leakage

Patients’ Survival
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Percen
t li
vin
g
Pts at risk
104 72 31 10
5 yr = 71 ± 4%
10 yr = 57 ± 5%
15 yr = 43 ± 6%
8 – CHF
8 – Endo
3 – AMI
2 – Stroke
2 – Valve

Surgery for Active Infective Endocarditis
Survival: Valve vs. Abscess
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Per
cen
t li
vin
g
abscess valve
1 year 15 year
Valve 87% 50%
Abscess 81% 43%
David TE et al. J Thorac Cardiovasc Surg 2007:133:144-9

Freedom from Recurrent Endocarditis
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Per
cen
t fr
ee
Pts at risk
104 72 31 10
1 yr = 96 ± 2%
5 yr = 88 ± 3%
10 yr = 82 ± 4%
15 yr = 82 ± 4%
15 patients had 16 episodes
of recurrent endocarditis

Freedom from Reoperation
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Per
cen
t fr
ee
Pts at risk
104 72 31 10
5 yr = 96 ± 2%
10 yr = 84 ± 5%
15 yr = 72 ± 9%
15 reoperations: 5 – patch/valve dehiscence
3 – primary tissue failure
5 – endocarditis
2 – new mitral regurgitation

Review of the literature

Kang DH et al.
Early surgery versus conventional treatment for infective
endocarditis
N Engl J Med. 2012 Jun 28;366:2466-73
CONCLUSIONS:
As compared with conventional treatment, early surgery in
patients with infective endocarditis and large vegetations
significantly reduced the composite end point of death
from any cause and embolic events by effectively
decreasing the risk of systemic embolism.

Conclusions
• Surgery for endocarditis of the aortic valve
remains challenging and it is associated
with high operative mortality and morbidity
• Infection of the cusps can be safely treated
with AV replacement and occasionally
repair. Infections involving the aortic
annulus and surrounding structures require
extensive resection and sometimes complex
reconstruction of the LVOF

Conclusions
• The type of valve implanted is probably less
important than the surgeon’s ability to
extirpate all infected tissues
• Patients who had one bout of endocarditis
are more likely to have a second bout than
patients who never had endocarditis

Thank you






























