Embed Size (px)
Citation preview

Which Patients for Subcutaneous Immunotherapy?
Harold S. Nelson. MD
Professor of Medicine
National Jewish Heath
University of Colorado Denver School of Medicine
Denver, Colorado, USA

Which Patients for Immunotherapy?
Appropriate clinical manifestations. Demonstrated IgE-mediated sensitivity to
relevant aeroallergen(s) Significant exposure to the relevant allergen(s) Availability of high quality extract for the
relevant allergen(s). Asthma, if present, adequately controlled.

Present Status of Immunotherapy with Inhalant Allergens:
Common to SCIT & SLIT Effective in allergic rhinitis, allergic asthma and
selected patients with atopic dermatitis Defined mechanisms Demonstrated prevention of:
- New sensitization in monosensitized subjects- Progression from rhinitis to asthma
Established duration required for:Persistence of efficacy after stopping
Therefore should not be limited to those failing symptomatic treatment.

SCIT versus SLITAdvantages of Each
Favoring SLIT:- Relative safety in subjects with allergic rhinitis and controlled asthma. - Home administration
Favoring SCIT:- Optimal dosing has been determined for many allergens - Efficacy of treatment with mixes of multiple unrelated allergens verified.- Efficacy, at least in the first year, may be greater.

Effective Doses in Double-Blind Studies (Major Allergen)
Allergen Extract Major Allergen Effective Doses Less or Ineffective doses
Ragweed Amb a 1 4 to 24 mcg 0.6 & 2 mcg
Timothy Phl p 5 15 to 20 mcg 2 mcg
D pteronyssinus Der p 1 7 & 12 mcg 0.7 mcg
D farinae Der f 1 10 mcg Not determined
Cat Fel d 1 11-17 mcg 0.6 & 3.0 mcg
Dog Can f 1 15 mcg 0.6 & 3.0 mcg
Birch Bet v 1 3.28 & 12 mcg Not determined
Alternaria Alt a 1 1.6 & 8 mcg Not determined

Studies of the Use of ≥ 2 Allergens in Immunotherapy
Reviewed English & non-English literature 1961-2007:
4 studies with 2-allergen mixes (SCIT & SLIT):Results > placebo and = to single allergen when reported.
6 studies with > 2 allergen mixes (all SCIT):4 showed clinical efficacy (2 asthma, 2 rhinitis.2 failed to show clinical efficacy.
HS Nelson. J Allergy Clin Immunol 2009;123:763-0

Evidence for Effectiveness of Immunotherapy Employing
Multiple AllergensJohnstone included all allergens to which the child was
skin test positive. He demonstrated a dose dependent improvement in asthma. Pediatrics 1968;l42:793-802
Lowell & Franklin removed or reduced only ragweed in patients’ multi-allergen mixture and demonstrated increased symptoms during the ragweed pollen season. N. Engl J Med1965;273:675-9; JAMA 1967;201:915-7
Reid added only grass or placebo to multiple allergen mixes and showed significant reduction in asthma symptoms during the grass pollen season.
J Allergy Clin Immunol 1986;78:590-600

The Value of Hyposensitization Therapy for Bronchial Asthma in Children - A 14-year Study
“Free of Asthma” After 4 years- placebo and lowest dose 18%- 1/5,000 w/v 58%- 1/250 w/v 81%
“Free of Asthma” at end of study (age 16 yr)- placebo and lowest dose 22%- 1/5,000 w/v 66%- 1/250 w/v 78%
DE Johnstone, A Dutton Pediatrics 1968l42:793-802

Evidence for Effectiveness of Immunotherapy Employing
Multiple AllergensJohnstone included all allergens to which the child was
skin test positive. He demonstrated a dose dependent improvement in asthma. Pediatrics 1968;l42:793-802
Lowell & Franklin removed or reduced only ragweed in patients’ multi-allergen mixture and demonstrated increased symptoms during the ragweed pollen season.
N. Engl J Med1965;273:675-9; JAMA 1967;201:915-7
Reid added only grass or placebo to multiple allergen mixes and showed significant reduction in asthma symptoms during the grass pollen season.
J Allergy Clin Immunol 1986;78:590-600

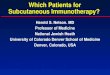
Effectiveness and Specificity of Ragweed Immunotherapy
1200
800
400
0
19 26 2 9 16 23 30 7 14 21 28* * ** * * *
Aug. Sept. Oct.
treated untreated median mean
1963
To
tal
Sco
re
Lowell & Franklin NEJM 1965

Evidence for Effectiveness of Immunotherapy Employing
Multiple AllergensJohnstone included all allergens to which the child was
skin test positive. He demonstrated a dose dependent improvement in asthma. Pediatrics 1968;l42:793-802
Lowell & Franklin removed or reduced only ragweed in patients’ multi-allergen mixture and demonstrated increased symptoms during the ragweed pollen season. N. Engl J Med1965;273:675-9; JAMA 1967;201:915-7
Reid added only grass or placebo to multiple allergen mixes and showed significant reduction in asthma symptoms during the grass pollen season.
J Allergy Clin Immunol 1986;78:590-600

8
6
4
2
0
1985ASTHMA
ME
AN
SM
S
Grass treatedNon-grass treated
25
20
15
10
0
RHINITISM
EA
N S
MS
Grass treatedNon-grass treated
300
200
100
0
CO
UN
TS
/cm
2
Grass pollen count
APRIL MAY JUNE
MONTHS
5
Response to Grass Subcutaneous I.T.
P < 0.05
P = 0.11
MJ Reid, et al. J Allergy Clin Immunol 1986;78:590-600
N = 9
N = 9

Sheila M. Amar, MD, Ronald J. Harbeck, PhD, Michael Sills, BS, Lori J. Silveira, MS, Holly
O’Brien, RN, Harold S. Nelson, MD National Jewish Health,
J Allergy Clin Immunol 2009;121:

Single-center, randomized, double-blind, placebo-controlled
SLIT for 10 months, 56 subjects randomized to 3 arms- SLIT with timothy pollen extract alone (17
mcg Phl p 5 daily)- SLIT with same dose of timothy extract + 9
additional pollen extracts- SLIT placebo

TM Group, Allergen Extract
Amount
Timothy 1.0 mL
Diluent 9.0 mL
Caramelized Sugar
Placebo Group Amount
Diluent 10 mL
Caramelized Sugar
*Amount added to 10 ml vial for 1 month of treatment
*CMD : Timothy approximately 30x SCIT dose (17 mcg Phl p 5 qday), other allergens 15-20x SCIT dose
MAT Group, Allergen Extract
Amount
Timothy 1.0 mL
Maple, Box-Elder 1.0 mL
Ash, White 1.0 mL
Juniper, Western 1.0 mL
Elm, American 1.0 mL
Cottonwood, Common 1.0 mL
Firebush (Kochia) 1.0 mL
Ragweed, Western 1.0 mL
Sagebrush, Common 1.0 mL
Russian Thistle 1.0 mL

Multi-allergen Sublingual Immunotherapy:Results
Only 3 “ of rain fell in Denver the first 6 months of 2008
Accordingly there was little grass pollen, few symptoms and no difference in symptom scores or medication use among the three treatment groups.
There were, however, significant differences in several clinically relevant outcomes.

p=0.03

p=0.001
p=0.04

p=0.005

Evidence for Effectiveness of Immunotherapy Employing
Multiple Allergens: Conclusions
Four studies support the clinical effectiveness of subcutaneous immunotherapy employing multiple allergens.
The only study of multiple allergen sublingual immunotherapy raises questions regarding its effectiveness.

14
12
10
8
6
4
2
SY
MP
TO
M S
CO
RE
PO
LL
EN
CO
UN
T
2800
2400
2000
1600
1200
800
400
TreatedUntreated
Pollen Count
16 20 24 28 1062 14 18 22 30 426AUGUST SEPTEMBER OCTOBER
1971
Norman & Lichtenstein JACI 1978;61:370
Pre-seasonal Immunotherapy

Sublingual Immunotherapy for allergic Rhinitis: Systematic Review and Meta-Analysis
21 trials involving 959 patients were included, all were DBPC parallel design.
Overall standard mean reduction in- Symptoms - 0.42 (p = 0.002) - Medications: - 0.43 (p = 0.00003)
Insufficient data to analyze for dose.
DR Wilson, M Torres Lima, SR Durham Allergy 2005;60:4-12

Sublingual immunotherapy for allergic rhinitis: systematic review and meta- analysis. DR Wilson, M Torres Lima, SR
Durham. Allergy 2005:60:4-12.
SMD -0.43

Symptom scores
Cochrane Database Syst Rev 2007; (1):CD001936.
SMD -0.73
Allergen Injection Immunotherapy for Seasonal Allergic Rhinitis
Calderon MA, Alves B, Jacobson M, Hurwitz B, Sheikh A, Durham S

Clinical Efficacy of Sublingual and Subcutaneous Birch Pollen Allergen-Specific Immunotherapy: A Randomized, Placebo-Controlled,Double-Blind,
Double-Dummy Study
Subcutaneous maintenance dose contained 3.28 mg Bet v 1 once monthly.
Sublingual maintenance dose contained 49.2 mg Bet v 1 every other day (cumulative dose 225 times SC).
5 cases of grade 3 or 4 systemic reactions in the s.c. group, two treated with adrenalin. No grade 3 or 4 reactions with SLIC
MS Khinchi, et al. Allergy 2004;59:45-53

SLIT versus SCITTreatment Symptoms Medication*
Placebo + .02 + 1.35
SLIT - .36 + .29
SCIT - .75 No change
SLIT & SCIT significantly better than placebo, no difference between active treatments.
* Pollen counts higher second year
MS Khinchi, et al. Allergy 2004;59:45-53

SLIT vs SCIT Comparative Study First Treatment Season
SCIT SLIT Placebo
Symptom Scores Medication Scores
The hatched areas indicate the daily birch pollen count. The rectangles indicate the defined pollen season.
Khinchi MS, et al. Allergy. 2004;59:45-53.
Mean Weekly Rhinoconjunctivitis Symptom and Medication Scores

Considerations Favoring the Use of Subcutaneous Rather Than Sublingual Immunotherapy
Well-defined effective and ineffective doses have been determined for more allergens.
Multiple-allergen mixes have been shown to be effective in multiple studies.
Where comparisons are available, they suggest greater efficacy for SCIT, at least in the first year.