Embed Size (px)
Citation preview
1
Which Treatments for Uterine Fibroids Have the Best Results?Investigators:
Duke University Medical Center
Evan Myers, MD
Walter M. Thomas Distinguished Professor
Division of Clinical and Epidemiological Research, Department of Obstetrics & Gynecology
2301 Erwin Rd
Durham, NC 27710 USA
Phone: +1 919 684 8111
Center for Medical Technology Policy
Donna A. Messner, PhD
Vice President, Senior Research Director
World Trade Center Baltimore
401 East Pratt Street, Suite 631
Baltimore, MD 21202 USA
Phone: +1 410 547 2687 ext. 102
QuintilesIMS
Priscilla Velentgas, PhD
Senior Director, Epidemiology
Real‐World Insights
201 Broadway
Cambridge, MA 01945 USA
Phone: +1 617 621 1600
Original Project Title: Comparing Patient-centered Outcomes after Treatment for Uterine FibroidsPCORI Project ID: CE‐12‐11‐4430 HSRProj ID: 20143198Clinicaltrials.gov ID: NCT02819609
_______________________________
To cite this document, please use: Myers E, Messner D, Velentgas P, et al. 2018. Which Treatments for Uterine Fibroids Have the Best Results?. Washington, DC: Patient‐Centered Outcomes Research
Institute (PCORI). https://doi.org/10.25302/5.2018.CE.12114430
2
Table of Contents
ABSTRACT ........................................................................................................................ 3
1. BACKGROUND ................................................................................................................. 4
2. METHODS ........................................................................................................................ 6 2.1 Retrospective Cohort Study ............................................................................................................................... 6 2.1.1 Study Design .................................................................................................................................................... 6 2.1.2 Subjects ........................................................................................................................................................... 7 2.1.3 Variables .......................................................................................................................................................... 8 2.1.4 Statistical Methods ........................................................................................................................................ 10 2.2 Stakeholder Engagement ................................................................................................................................ 11 2.2.1 Study Design .................................................................................................................................................. 11 2.2.2 Subjects ......................................................................................................................................................... 12 2.2.3 Analysis Methods .......................................................................................................................................... 12
3. RESULTS ......................................................................................................................... 12 3.1 Retrospective Cohort Study ............................................................................................................................. 12 3.1.1 Descriptive Data ............................................................................................................................................ 12 3.1.2 Main Results .................................................................................................................................................. 17 3.1.3 Sensitivity Analyses ....................................................................................................................................... 28 3.2 Stakeholder Engagement ................................................................................................................................ 29 3.2.1 Main Results .................................................................................................................................................. 29
4. DISCUSSION ................................................................................................................... 31 4.1 Retrospective Cohort Study ...................................................................................................................... 31 4.1.1 Key Results ..................................................................................................................................................... 31 4.1.2 Biases and Limitations ................................................................................................................................... 32 4.2 Stakeholder Engagement ................................................................................................................................ 34
5. CONCLUSION ................................................................................................................. 35 5.1 Retrospective Cohort Study .............................................................................................................................. 35 5.2 Stakeholder Engagement ................................................................................................................................. 36
6. REFERENCES.................................................................................................................... 37
7. APPENDICES ................................................................................................................... 39

3
ABSTRACT
Background
Uterine fibroids are one of the leading causes of morbidity in reproductive-aged women. Because treatment options for symptomatic fibroids involve significant trade-offs, the lack of evidence on treatment effectiveness limits the ability of patients and their physicians to make informed treatment decisions.
Objectives
The first objective of this study was to compare the durability of symptom relief after uterus-conserving treatments for symptomatic fibroids in terms of incidence of, and time to, new or recurrent symptoms and subsequent procedures. The second objective of this study was to evaluate the effect stakeholder participation had on the research process.
Methods
This was a retrospective database study of patients with uterine fibroids. The study used 2 data sources: Quintiles Electronic Medical Record System (Q-EMR) linked to Truven MarketScan claims and the COMparative effectiveness and PAtient Safety and Surveillance (COMPASS) Research Network. The study included patients with uterine fibroids having 1 of the procedures of interest occurring from January 1, 2005, to December 31, 2011, with the first instance being designated as the index procedure. The study then followed patients for a minimum of 2 years in the electronic medical record and claims data to look for new or recurrent symptoms and subsequent procedures. We created a Stakeholder Participation Council (SPC) with 17 diverse stakeholders (e.g., patients/patient advocates, physicians, payers) to provide continuous input on the research process and interpretation and dissemination of the study findings.
Results
The study included a total of 8687 patients in Q-EMR and 3547 patients in COMPASS. Due to the relatively small sample size of the COMPASS data, we based the comparative analyses on the Q-EMR data only. Endometrial ablation was the most common index procedure in Q-EMR. Patients who had uterine artery embolization as their index procedure had a lower risk of new or recurrent symptoms after the index procedure and a lower risk of having a subsequent procedure during the study period compared with patients who underwent endometrial ablation. Myomectomy patients had a lower risk of having a subsequent procedure than patients who received endometrial ablation.
Conclusions
This research provides additional evidence about expectations for the durability of symptom relief and time to subsequent procedures among women with uterine fibroids that may be helpful to women and their health care providers when making treatment choices. Overall, the SPC provided critical input that shaped the study design, data analysis, and dissemination plan for key findings.
4
1. BACKGROUND
Uterine leiomyomata, commonly referred to as fibroids, are one of the leading causes of morbidity in reproductive-aged women. These benign tumors of uterine smooth muscle and extracellular matrix have a cumulative incidence (based on imaging) by age 50 of almost 70% for white women and more than 80% for African American women.1
Although most fibroids are asymptomatic, a substantial proportion cause symptoms. The most common symptoms are heavy menstrual bleeding and/or pain, with a peak incidence for symptoms between ages 35 and 45.2 Studies using both global and disease-specific measures of health-related quality of life (HRQOL) show substantial impairment in HRQOL in women with fibroids.3,4
Symptomatic fibroids are by far the most common cause of hospitalization for benign gynecologic conditions in the United States.5 Fibroids may also contribute to adverse reproductive outcomes. Fibroids are associated with some cases of infertility,6,7 although this may be due in part to referral bias.8 Fibroids are common in pregnancy, with approximately 10% of women having detectable fibroids in the first trimester of pregnancy.9 They are also associated with such adverse pregnancy outcomes as miscarriage, preterm birth, and an increased risk of cesarean delivery,2,10,11 although, again, there is uncertainty about whether this association is causal.
Approximately 200 000 hysterectomies, 30 000 myomectomies, and thousands of selective uterine artery embolizations and high-intensity focused ultrasound procedures are performed annually in the United States to remove or destroy uterine fibroids, with the annual economic burden of these tumors estimated to be between $5.9 billion and $34.4 billion.12 Symptoms related to fibroids affect patients’ ability to work and result in substantial out-of-pocket costs. Employed women with symptomatic fibroids report significantly decreased work productivity.13 Nonmedical costs directly incurred by patients with uterine bleeding include not only those associated with lost work due to symptoms and medical visits, but also medications and supplies such as sanitary pads, which in 1 2008 study averaged more than $300 per year.14
Despite the high burden of disease associated with fibroids, the quality of the evidence on optimal management is poor. A systematic review conducted in 2002 for the Agency for Healthcare Research and Quality (AHRQ) found almost no high-quality evidence for the comparative effectiveness of different treatment options for symptomatic fibroids.2 An update conducted in 2007 found no substantive changes in the state of the evidence and concluded, “The dearth of high-quality evidence supporting the effectiveness of most interventions for uterine fibroids is remarkable, given how common this problem is. The current state of the literature does not permit definitive conclusions about benefit, harm, or relative costs to help guide women’s choices. Significant research gaps include well-conducted trials in US populations that directly compare interventions on short- and, especially, long-term outcomes, studies on therapeutics for medical management, and information on treatment decisions for women who desire a pregnancy.”15
5
Treatment options for symptomatic fibroids involve significant trade-offs, including decisions about relative rates of short-term side effects, and, in the case of procedures, complications and recovery time, the likelihood of cure versus recurrent symptoms, and the effect on future childbearing potential. These trade-offs, coupled with the lack of evidence on outcomes of treatment, limit the ability of patients to make informed treatment decisions. There is considerable uncertainty about all of these outcomes for available treatments for fibroids. Additional research, particularly research on the relative effectiveness of available treatments, is needed.
In addition, significant disparities exist in disease burden and short-term treatment outcomes among fibroid patient subgroups. African American women consistently develop symptomatic fibroids at younger ages, have more severe disease (larger uterine size and number of fibroids at presentation), are more likely to have significant anemia compared with white women, and, in some but not all studies, were found to have more severe symptoms.1,2,9,16–18 African American women with uterine fibroids also tend to experience greater degrees of work impairment, presumably due to more severe symptoms.13 Hysterectomy for any indication is more common among reproductive-aged African American women compared with white women,19 as is myomectomy.2 These factors, along with higher prevalence of such comorbid conditions as obesity and hypertension, make surgical treatment more difficult and contribute to higher rates of complications in African American women for both hysterectomy and myomectomy.20–22
The premise that underlies comparative effectiveness research and patient-centered outcomes research is that research guided by patients and other stakeholders will substantively improve the quality and relevance of clinical research, such that it is more informative to patients and other decision makers. This concept is particularly important for uterine fibroids, for which patient preferences strongly influence treatment decisions. Retrospective observational studies represent 1 approach to studying the effectiveness of treatment options for uterine fibroids. However, little is known about the degree to which stakeholder participation will markedly change the study design or analysis plan for these types of studies.
The long-term objective of this research study is to help patients and care providers make informed decisions about which treatment options for uterine fibroids are most likely to result in the outcomes that are of greatest importance to each patient. To help achieve this long-term objective, this study has the following specific aims, taking advantage of unique data resources that combine administrative and electronic medical record (EMR) data:
To compare the durability of symptom relief after uterus-conserving treatments (myomectomy, endometrial ablation, uterine artery embolization, magnetic resonance imaging [MRI]-guided focused ultrasound ablation) for symptomatic fibroids in terms of:
• incidence of subsequent procedures (including hysterectomy) after the initial treatment, adjusting for such factors as symptom type (e.g., bleeding, pain, pressure) and patient characteristics (e.g., age, race/ethnicity); and
• time to subsequent procedure, also adjusting for relevant patient characteristics.
6
To compare the durability of symptom relief after uterus-conserving treatments for symptomatic fibroids in terms of:
• incidence of recurrent symptoms (based on diagnosis codes, prescriptions, and medical records) after initial treatment, adjusting for symptom type, and patient characteristics; and
• time to recurrent symptoms, again adjusting for relevant patient characteristics.
To evaluate the effect of stakeholder participation in the research process in terms of qualitative and semiquantitative evaluation of the process by investigators and stakeholders.
2. METHODS
This observational study includes 2 components: (1) a retrospective cohort study of 2 independent data sources to study the effectiveness of treatment options for uterine fibroids; and (2) a stakeholder engagement plan to evaluate the contributions of a stakeholder committee in influencing the analysis and dissemination plans for this study.
In accordance with the Patient-Centered Outcomes Research Institute’s (PCORI’s) authorizing legislation, all funded research should be assessed for adherence to PCORI’s Methodology Standards27 as part of the peer review process. The investigators hereby identify the following Methodology Standards applicable to the research and confirm the research is adherent to these standards: RQ1 through RQ6; PC1 through PC4; IR1 through IR3, IR5 and IR6; MD1 through MD5; DR1 through DR3; and DN1 and DN2.
2.1 Retrospective Cohort Study
2.1.1 Study Design
This was a retrospective cohort study of uterine fibroid patients to compare the durability of symptom relief following 4 uterus-conserving procedures of interest, including myomectomy, endometrial ablation, uterine artery embolization, and MRI-guided focused ultrasound ablation. The study separately analyzed two independent data sources: Quintiles Electronic Medical Records (Q-EMR) linked with Truven MarketScan claims, and the COMparative effectiveness and PAtient Safety and Surveillance (COMPASS) Research Network. Both data sources include geographically and demographically diverse patient populations and are described in detail below. Use of 2 independent sources of data (Q-EMR and COMPASS) was planned to serve as a validation of the findings from each source, with similar results in the 2 data sources (if observed), strengthening the conclusions and suggesting some generalizability of the findings across health systems and data sources.
Q-EMR is a national network of outpatient offices whose providers allow their deidentified patient-level data to be made available for research. The study captured clinical data from more than 525-member institutions and more than 30 000 providers. The study then linked the Q-EMR data to the Truven MarketScan claims data using an algorithm based on specific data elements (gender, month/year of birth, and 3-digit area codes) and health care service dates.23
The COMPASS Research Network is a network of integrated delivery networks (IDNs) organized to support the conduct of research using EMRs and other linked data sources. Data from these IDNs can be
7
extracted and harmonized using a post hoc common data model to better understand characteristics of and differences between patient populations and changes in treatment over time, and to draw comparisons between geographic regions.
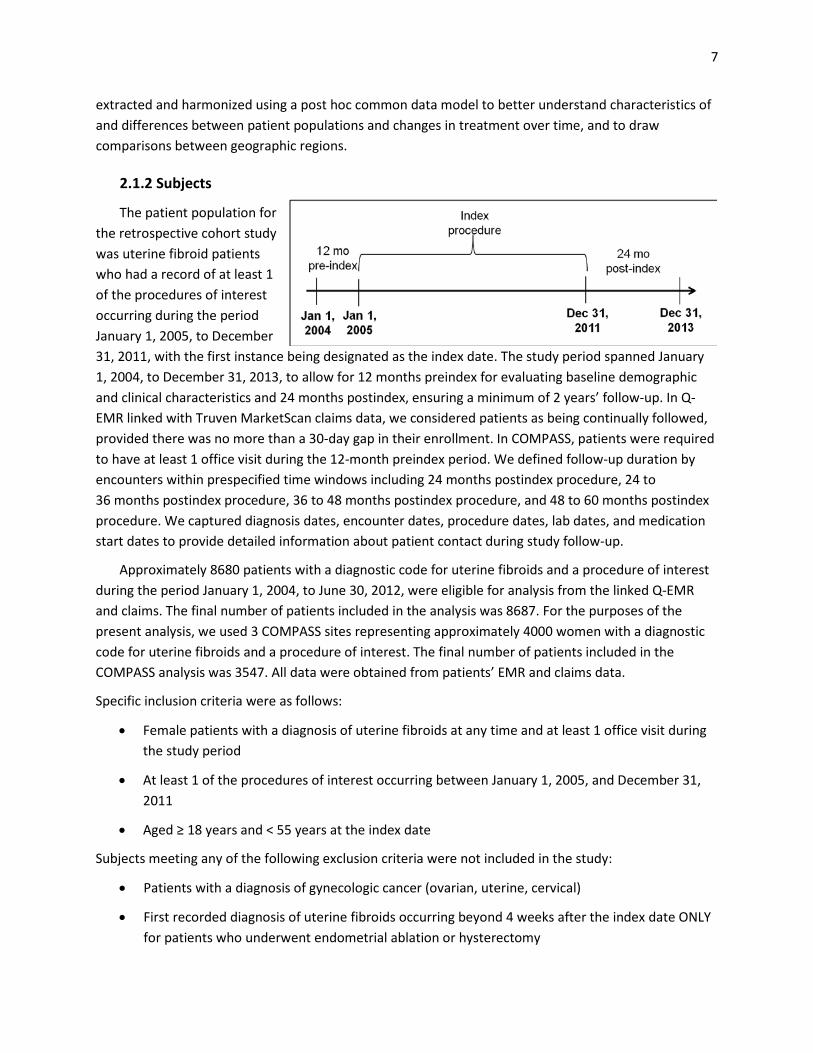
2.1.2 Subjects
The patient population for the retrospective cohort study was uterine fibroid patients who had a record of at least 1 of the procedures of interest occurring during the period January 1, 2005, to December 31, 2011, with the first instance being designated as the index date. The study period spanned January 1, 2004, to December 31, 2013, to allow for 12 months preindex for evaluating baseline demographic and clinical characteristics and 24 months postindex, ensuring a minimum of 2 years’ follow-up. In Q-EMR linked with Truven MarketScan claims data, we considered patients as being continually followed, provided there was no more than a 30-day gap in their enrollment. In COMPASS, patients were required to have at least 1 office visit during the 12-month preindex period. We defined follow-up duration by encounters within prespecified time windows including 24 months postindex procedure, 24 to 36 months postindex procedure, 36 to 48 months postindex procedure, and 48 to 60 months postindex procedure. We captured diagnosis dates, encounter dates, procedure dates, lab dates, and medication start dates to provide detailed information about patient contact during study follow-up.
Approximately 8680 patients with a diagnostic code for uterine fibroids and a procedure of interest during the period January 1, 2004, to June 30, 2012, were eligible for analysis from the linked Q-EMR and claims. The final number of patients included in the analysis was 8687. For the purposes of the present analysis, we used 3 COMPASS sites representing approximately 4000 women with a diagnostic code for uterine fibroids and a procedure of interest. The final number of patients included in the COMPASS analysis was 3547. All data were obtained from patients’ EMR and claims data.
Specific inclusion criteria were as follows:
• Female patients with a diagnosis of uterine fibroids at any time and at least 1 office visit during the study period
• At least 1 of the procedures of interest occurring between January 1, 2005, and December 31, 2011
• Aged ≥ 18 years and < 55 years at the index date
Subjects meeting any of the following exclusion criteria were not included in the study:
• Patients with a diagnosis of gynecologic cancer (ovarian, uterine, cervical)
• First recorded diagnosis of uterine fibroids occurring beyond 4 weeks after the index date ONLY for patients who underwent endometrial ablation or hysterectomy
8
• Patients with a record of any procedures of interest occurring before January 1, 2005
2.1.3 Variables
2.1.3.1 Descriptive measures
We extracted and used patient demographics and relevant medical history available in the linked Q-EMR and claims and COMPASS data to create 2 separate cohorts to describe patient characteristics and durability of symptom relief after procedures of interest. We obtained data from structured fields in the EMR and claims, using ICD9 codes for symptoms and diagnoses and HCPC and ICD9 for procedures. We evaluated potential predictors of outcomes including patient demographics (i.e., age, race/ethnicity, region), comorbid medical conditions, and symptoms (i.e., bleeding, pain) at the time of the index procedure. Note that coding definitions for the comorbid medical conditions and symptoms, as well as the medical procedures, can be found in Appendix A.
Descriptive measures computed as described include the following:
• Baseline patient characteristics
o Age
o Race (white, black, other)
o Region (Northeast, Midwest, Southeast, West)
• Comorbid conditions
o Hypertension
o Type 2 diabetes
o Disorders of lipid metabolism
o Obesity
o Coronary artery disease
o Heart failure
o Myocardial infarction (MI)
o Stroke
o Cardiac dysrhythmias
• Symptoms that may be related to uterine fibroids
o Menorrhagia/anemia
o Dysmenorrhea
o Pelvic pain not related to menstrual cycle
o Other vaginal/pelvic symptoms (leucorrhea, vaginal discharge, dyspareunia)
9
o Urinary symptoms (dysuria, urinary retention, hydronephrosis)
o Bowel symptoms (constipation, diarrhea)
o Other symptoms (leg pain, back pain, shortness of breath)
• Qualifying procedure of interest
o Myomectomy
o Endometrial ablation
o Uterine artery embolization
o MRI-guided focused ultrasound ablation
o Hysterectomy
2.1.3.2 Exposure definition and measures
The main exposure of interest was a uterus-sparing procedure for uterine fibroid treatment as an index procedure including myomectomy, endometrial ablation, uterine artery embolization, or MRI-guided focused ultrasound. We did not include hysterectomy as an index procedure in comparative analyses across procedures as symptoms because uterine fibroids and subsequent procedures for uterine fibroids cannot be experienced/occur posthysterectomy.
2.1.3.3 Outcome definition and measures
We evaluated durability of symptom relief after uterus-conserving treatments (myomectomy, endometrial ablation, and uterine artery embolization) for symptomatic fibroids using several endpoints described below. New or recurrent symptoms included only those recorded later than 60 days postprocedure, to eliminate those that may have been postoperative. Subsequent procedures also excluded new procedures recorded less than 60 days after the index procedure, to eliminate what may have been duplicate coding of the index procedure or other misleading coding, with the exception of hysterectomy as a subsequent procedure, based on input from the Stakeholder Partnership Council (SPC).
The following are the specific outcomes assessed in this study:
• Incidence of any new or recurrent symptoms later than 60 days through 2 years after initial procedure (yes/no)
• Time to first new or recurrent symptom(s), excluding symptoms recorded less than 60 days after initial procedure
• Incidence of any subsequent procedures (including hysterectomy) after initial procedure, excluding procedures (except hysterectomy) recorded less than 60 days after initial procedure
• Time to subsequent procedure (including hysterectomy) after initial procedure, excluding procedures (except hysterectomy) recorded less than 60 days after initial procedure
10
2.1.4 Statistical Methods
We maintained and analyzed data obtained from linked Q-EMR and claims and COMPASS separately in SAS®.
2.1.4.1 Main summary measures
We described demographic and other baseline characteristics of the 2 cohorts as counts and percentages for categorical variables and measures of central tendency (mean, standard deviation, median, interquartile range) for continuous variables.
2.1.4.2 Main statistical measures
We used multivariable logistic regression models to (1) compare the incidence of recurrent or new symptoms, and (2) compare the incidence of subsequent procedures following myomectomy, endometrial ablation, and uterine artery embolization, and (3) to calculate the odds ratios (OR), controlling for potential confounding variables (race, region, index procedure, symptoms at baseline, comorbidities at baseline, and age) as covariates in the multivariable models. We used Cox proportional hazard models to compare time to new or recurrent symptoms and time to subsequent procedures following the myomectomy, endometrial ablation, and uterine artery embolization, and to calculate the hazard ratios (HRs), controlling for potential confounding variables (race, region, index procedure, symptoms at baseline, comorbidities at baseline, and age) as covariates in the multivariable models. We created Kaplan-Meier curves to graphically present time to first new or recurrent symptom or first subsequent procedure.
To ensure equal follow-up time for study patients, we included only 2 years of follow-up after the index procedure in the logistic regression modeling, regardless of the total follow-up time available for individual patients. We included all available follow-up data in the time-to-event analyses, namely the Cox proportional hazards modeling.
For analyses examining the incidence and time to subsequent procedures, we excluded procedures coded as having occurred within 60 days of the index procedure (except for hysterectomy, which was included regardless of when the procedure occurred). We assumed that these procedures were likely related to coding issues because, clinically, we would not expect to see a subsequent procedure (with the exception of hysterectomy) occurring so soon after the index treatment. Similarly, for analyses examining the incidence and time to new or recurrent symptoms, we did not include symptoms coded as having occurred within 60 days of the index procedure, because many of these symptoms immediately following the index procedure were presumed to be due to the procedure itself (e.g., postoperative pain and discomfort) and less likely to be reflective of symptomatic uterine fibroids.
We included the following variables (with referent group asterisked) in the multivariate models (i.e., logistic and Cox proportional hazard models):
• Race (white*, African American, other) • Region (Northeast*, Midwest, Southeast, West) • Index procedure (endometrial ablation*, myomectomy, uterine artery embolization)
11
• Symptoms at baseline (none*, symptoms in 1 group, symptoms in 2–3 groups) o Symptoms groups included
anemia and menorrhagia; pelvic pain and dysmenorrhea; and other (urinary retention, leucorrhea, shortness of breath, dyspareunia,
constipation, diarrhea, back pain, leg pain, dysuria). • Comorbidities at baseline (none*, any high risk, obesity and non–high risk, any other non–high
risk, obesity only) o Comorbidity groups included
obesity; non–high risk (hypertension, type 2 diabetes, disorders of lipid metabolism);
and high risk (coronary artery disease, heart failure, MI, stroke, cardiac dysthymias).
• Age in years
2.2 Stakeholder Engagement
We assembled an SPC made up of 17 individuals representing stakeholders including patients and consumers, clinicians, insurers and/or payers, federal agencies, and researchers. We invited stakeholders to participate as members of the SPC based on their experience as experts in the clinical management and/or epidemiology of uterine fibroids, their experience as a uterine fibroids patient and/or their previous patient advocacy activities, or their experience as a stakeholder in 1 of the other areas mentioned.
The specific aims of stakeholder engagement for this project were 4-fold:
• To refine the protocol to ensure that:
o the outcomes being measured are relevant to decision makers o the patient population includes important subpopulations of interest to decision makers o the comparators and their definitions are of importance to decision makers, and o other factors relevant to the analysis or interpretation of the data are considered
• To leverage the perspectives of the various stakeholders in interpreting the results
• To develop a dissemination strategy tailored to the information needs and usual sources of information specific to 3 target audiences—patients, clinicians, and policymakers
• To evaluate the “success” of stakeholder engagement in the context of this project
2.2.1 Study Design
We engaged the SPC in a series of discussions to gather its feedback on this study. We asked the SPC to provide input on the key research questions that should be addressed by the study and the details of the implementation of the research, such as which variables should be included and how they should be defined, which subpopulations would be of interest, how to define meaningful measures that reflect
12
clinical management of uterine fibroids based on EMR and claims data, how to interpret the study results, what findings would be the most meaningful to different stakeholders, and what means would be appropriate to disseminate the results.
We asked stakeholders to provide informed consent prior to participating in the research activities, given that their participation included a research component of evaluating the effectiveness of stakeholder input and the process of obtaining it. We sent the informed consent form to stakeholders by email prior to the first face-to-face meeting. Stakeholders had the option to withdraw their consent and discontinue participation in the SPC at any time. However, no stakeholders withdrew consent.
In accordance with these specific aims for stakeholder engagement, the first face-to-face meeting in June 2014 focused on obtaining stakeholder input to revise a draft version of the study protocol. Subsequent Web meetings and teleconferences provided additional opportunities for the stakeholders to review and help the research team interpret interim results. Stakeholders were able to review preliminary output from the analysis of the first available data source 6 months into the project; they were then asked to provide further input into the refinement of the study protocol before we began our analysis of the second data source. At the second face-to-face meeting in July 2015, the stakeholder group assisted with framing messages that are important to patients, providers, and policymakers, based on the study results and planning dissemination strategies, to ensure information was presented in sources and formats accessible to these decision makers.
A final 2-hour teleconference meeting of stakeholders in November 2015 was devoted to an evaluation of stakeholder experience. In addition to presenting the formal evaluation of the impact of stakeholder refinement on the project’s protocol and the outcomes, we requested that participants complete an online evaluation form and provide more detailed individual feedback through comment forms, which we discussed at this meeting.
2.2.2 Subjects
As previously described, the SPC consisted of 17 individuals. Each stakeholder’s affiliations and areas of representation are summarized in Appendix B.
2.2.3 Analysis Methods
We qualitatively evaluated the effect of stakeholder participation in the research for the 4 aims: effect on the protocol, analyses, dissemination strategy, and overall “success” of engagement as evaluated via stakeholder interview. Stakeholder comments on both the protocol and the analyses are summarized in this report, along with stakeholder recommendations for dissemination. Finally, key findings from the interviews with SPC members are also described below.
13
3. RESULTS
3.1 Retrospective Cohort Study
3.1.1 Descriptive Data
Index Procedure
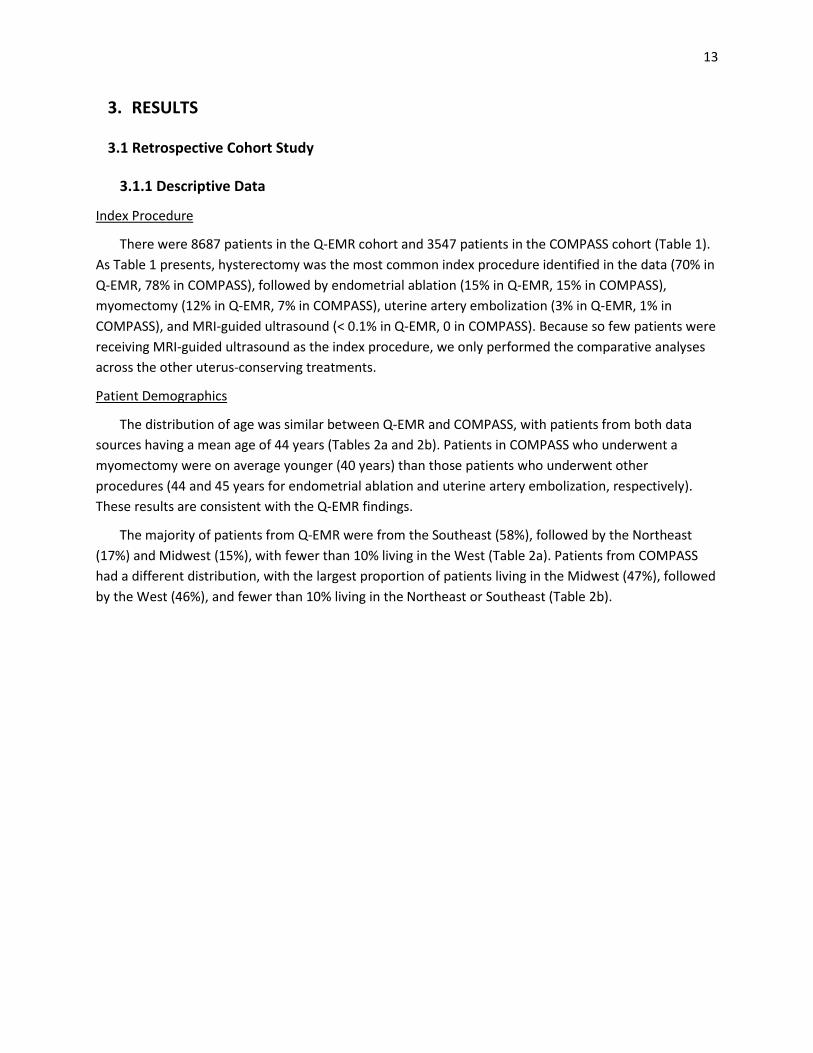
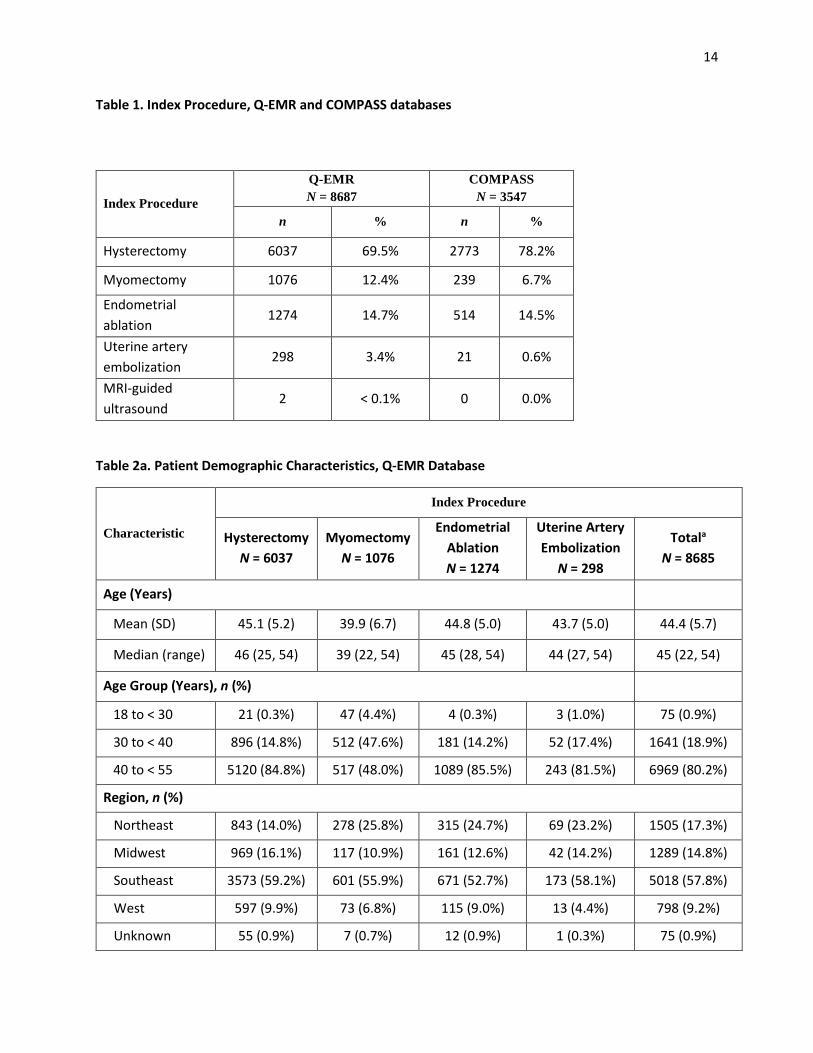
There were 8687 patients in the Q-EMR cohort and 3547 patients in the COMPASS cohort (Table 1). As Table 1 presents, hysterectomy was the most common index procedure identified in the data (70% in Q-EMR, 78% in COMPASS), followed by endometrial ablation (15% in Q-EMR, 15% in COMPASS), myomectomy (12% in Q-EMR, 7% in COMPASS), uterine artery embolization (3% in Q-EMR, 1% in COMPASS), and MRI-guided ultrasound (< 0.1% in Q-EMR, 0 in COMPASS). Because so few patients were receiving MRI-guided ultrasound as the index procedure, we only performed the comparative analyses across the other uterus-conserving treatments.
Patient Demographics
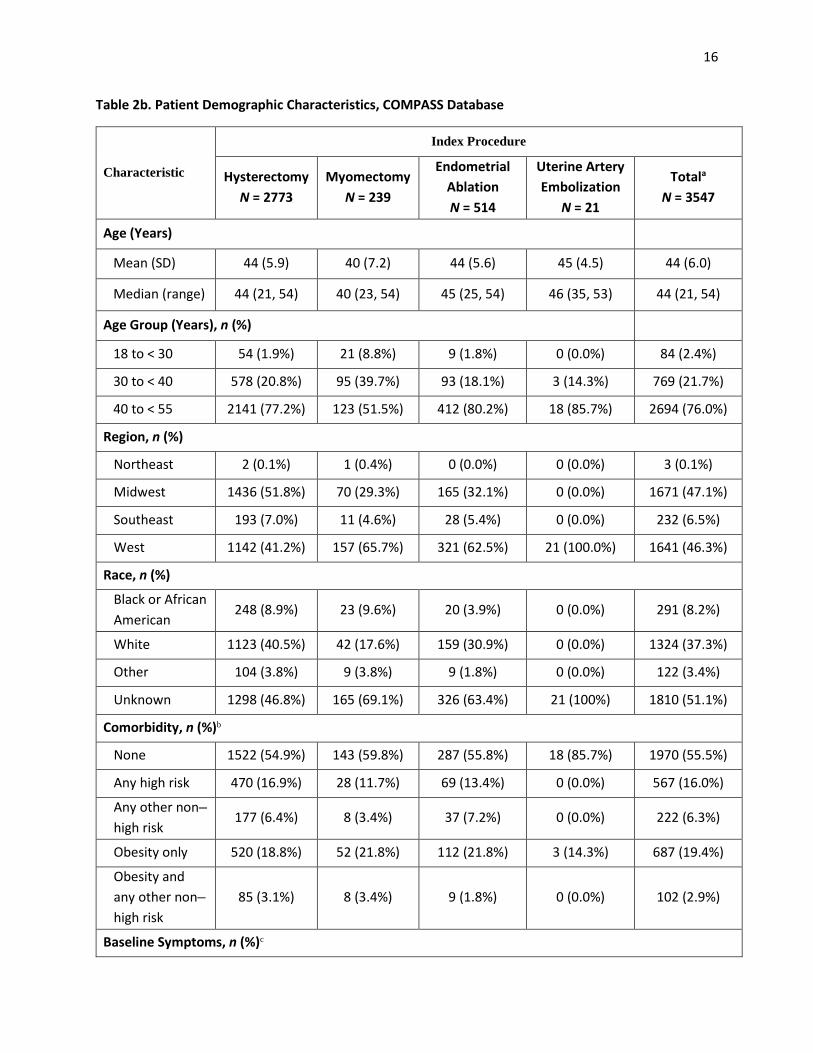
The distribution of age was similar between Q-EMR and COMPASS, with patients from both data sources having a mean age of 44 years (Tables 2a and 2b). Patients in COMPASS who underwent a myomectomy were on average younger (40 years) than those patients who underwent other procedures (44 and 45 years for endometrial ablation and uterine artery embolization, respectively). These results are consistent with the Q-EMR findings.
The majority of patients from Q-EMR were from the Southeast (58%), followed by the Northeast (17%) and Midwest (15%), with fewer than 10% living in the West (Table 2a). Patients from COMPASS had a different distribution, with the largest proportion of patients living in the Midwest (47%), followed by the West (46%), and fewer than 10% living in the Northeast or Southeast (Table 2b).
14
Table 1. Index Procedure, Q-EMR and COMPASS databases
Table 2a. Patient Demographic Characteristics, Q-EMR Database
Characteristic
Index Procedure
Hysterectomy N = 6037
Myomectomy N = 1076
Endometrial Ablation N = 1274
Uterine Artery Embolization
N = 298
Totala
N = 8685
Age (Years)
Mean (SD) 45.1 (5.2) 39.9 (6.7) 44.8 (5.0) 43.7 (5.0) 44.4 (5.7)
Median (range) 46 (25, 54) 39 (22, 54) 45 (28, 54) 44 (27, 54) 45 (22, 54)
Age Group (Years), n (%)
18 to < 30 21 (0.3%) 47 (4.4%) 4 (0.3%) 3 (1.0%) 75 (0.9%)
30 to < 40 896 (14.8%) 512 (47.6%) 181 (14.2%) 52 (17.4%) 1641 (18.9%)
40 to < 55 5120 (84.8%) 517 (48.0%) 1089 (85.5%) 243 (81.5%) 6969 (80.2%)
Region, n (%)
Northeast 843 (14.0%) 278 (25.8%) 315 (24.7%) 69 (23.2%) 1505 (17.3%)
Midwest 969 (16.1%) 117 (10.9%) 161 (12.6%) 42 (14.2%) 1289 (14.8%)
Southeast 3573 (59.2%) 601 (55.9%) 671 (52.7%) 173 (58.1%) 5018 (57.8%)
West 597 (9.9%) 73 (6.8%) 115 (9.0%) 13 (4.4%) 798 (9.2%)
Unknown 55 (0.9%) 7 (0.7%) 12 (0.9%) 1 (0.3%) 75 (0.9%)
Index Procedure
Q-EMR N = 8687
COMPASS N = 3547
n % n %
Hysterectomy 6037 69.5% 2773 78.2%
Myomectomy 1076 12.4% 239 6.7%
Endometrial ablation
1274 14.7% 514 14.5%
Uterine artery embolization
298 3.4% 21 0.6%
MRI-guided ultrasound
2 < 0.1% 0 0.0%
15
Race, n (%)
Black or African American
1121 (18.6%) 314 (29.2%) 203 (15.9%) 132 (44.3%) 1770 (20.4%)
White 3079 (51.0%) 375 (34.9%) 672 (52.8%) 79 (26.5%) 4205 (48.4%)
Other 222 (3.7%) 54 (5.0%) 43 (3.4%) 11 (3.7%) 330 (3.8%)
Unknown 1615 (26.8%) 333 (31.0%) 356 (27.9%) 76 (25.5%) 2380 (27.4%)
Comorbidity, n (%)b
None 365 (6.1%) 39 (3.6%) 72 (5.7%) 10 (3.4%) 486 (5.6%)
Any high risk 1767 (29.3%) 229 (21.3%) 328 (25.8%) 72 (24.2%) 2396 (27.6%)
Any other non–high risk
2765 (45.8%) 645 (59.9%) 623 (48.9%) 159 (53.4%) 4192 (48.3%)
Obesity only 659 (10.9%) 77 (7.2%) 153 (12.0%) 37 (12.4%) 926 (10.7%)
Obesity and any other non–high risk
481 (8.0%) 86 (8.0%) 98 (7.7%) 20 (6.7%) 685 (7.9%)
Baseline Symptoms, n (%)c
None 572 (9.5%) 201 (18.7%) 53 (4.2%) 56 (18.8%) 882 (10.2%)
1 group 2358 (39.1%) 430 (40.0%) 554 (43.5%) 121 (40.6%) 3463 (39.9%)
2–3 groups 3107 (51.5%) 445 (41.4%) 667 (52.4%) 121 (40.6%) 4340 (50.0%)
a Two women had MRI-guided focused ultrasound as their index procedure; these patients were not included in the descriptive tables due to small sample size. b Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias.
c Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
16
Table 2b. Patient Demographic Characteristics, COMPASS Database
Characteristic
Index Procedure
Hysterectomy N = 2773
Myomectomy N = 239
Endometrial Ablation N = 514
Uterine Artery Embolization
N = 21
Totala N = 3547
Age (Years)
Mean (SD) 44 (5.9) 40 (7.2) 44 (5.6) 45 (4.5) 44 (6.0)
Median (range) 44 (21, 54) 40 (23, 54) 45 (25, 54) 46 (35, 53) 44 (21, 54)
Age Group (Years), n (%)
18 to < 30 54 (1.9%) 21 (8.8%) 9 (1.8%) 0 (0.0%) 84 (2.4%)
30 to < 40 578 (20.8%) 95 (39.7%) 93 (18.1%) 3 (14.3%) 769 (21.7%)
40 to < 55 2141 (77.2%) 123 (51.5%) 412 (80.2%) 18 (85.7%) 2694 (76.0%)
Region, n (%)
Northeast 2 (0.1%) 1 (0.4%) 0 (0.0%) 0 (0.0%) 3 (0.1%)
Midwest 1436 (51.8%) 70 (29.3%) 165 (32.1%) 0 (0.0%) 1671 (47.1%)
Southeast 193 (7.0%) 11 (4.6%) 28 (5.4%) 0 (0.0%) 232 (6.5%)
West 1142 (41.2%) 157 (65.7%) 321 (62.5%) 21 (100.0%) 1641 (46.3%)
Race, n (%)
Black or African American
248 (8.9%) 23 (9.6%) 20 (3.9%) 0 (0.0%) 291 (8.2%)
White 1123 (40.5%) 42 (17.6%) 159 (30.9%) 0 (0.0%) 1324 (37.3%)
Other 104 (3.8%) 9 (3.8%) 9 (1.8%) 0 (0.0%) 122 (3.4%)
Unknown 1298 (46.8%) 165 (69.1%) 326 (63.4%) 21 (100%) 1810 (51.1%)
Comorbidity, n (%)b
None 1522 (54.9%) 143 (59.8%) 287 (55.8%) 18 (85.7%) 1970 (55.5%)
Any high risk 470 (16.9%) 28 (11.7%) 69 (13.4%) 0 (0.0%) 567 (16.0%)
Any other non–high risk
177 (6.4%) 8 (3.4%) 37 (7.2%) 0 (0.0%) 222 (6.3%)
Obesity only 520 (18.8%) 52 (21.8%) 112 (21.8%) 3 (14.3%) 687 (19.4%)
Obesity and any other non–high risk
85 (3.1%) 8 (3.4%) 9 (1.8%) 0 (0.0%) 102 (2.9%)
Baseline Symptoms, n (%)c
17
None 383 (13.8%) 54 (22.6%) 33 (6.4%) 1 (4.8%) 471 (13.3%)
1 group 1022 (36.8%) 99 (41.4%) 219 (42.6%) 4 (19.1%) 1344 (37.9%)
2–3 groups 1369 (49.4%) 86 (36.0%) 262 (51.0%) 16 (76.2%) 1733 (48.8%)
a Two women had MRI-guided focused ultrasound as their index procedure; these patients were not included in the descriptive tables due to small sample size. b Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias.
c Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
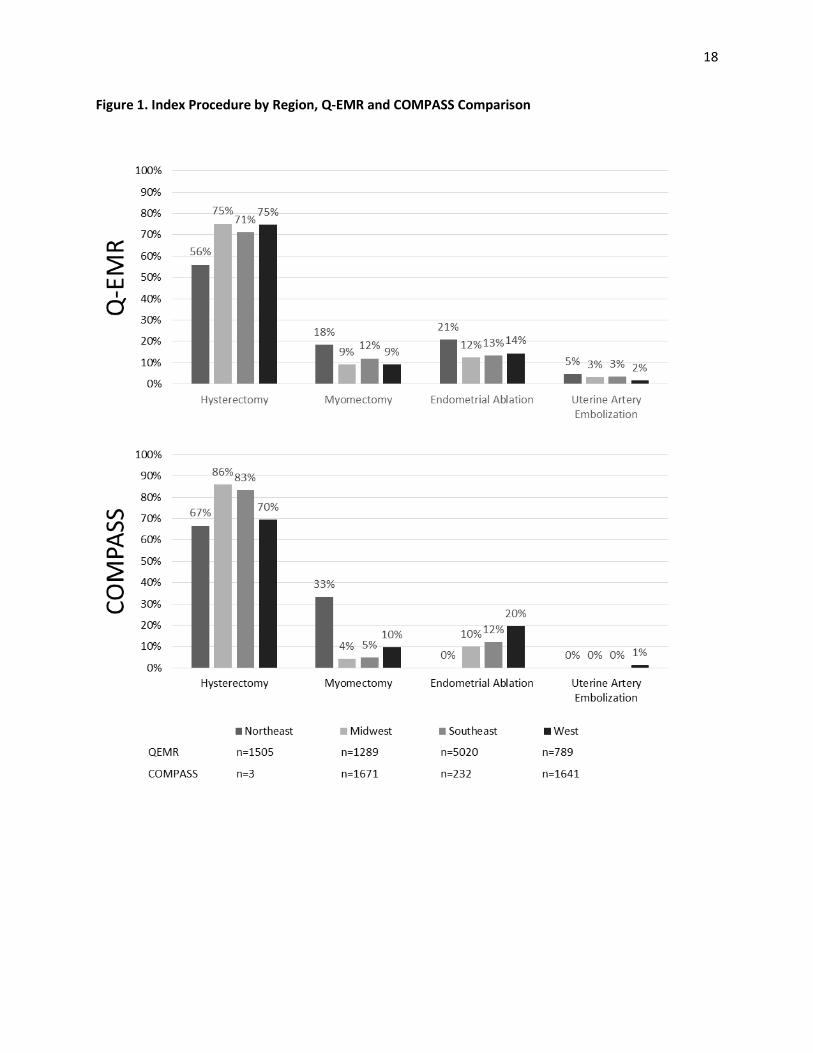
The distribution of procedures across geographic regions was similar between the 2 data sets (see Tables 2a and 2b). In both data sets, hysterectomy represented the most common index procedure, particularly in the Midwest region in COMPASS (86%; see Figure 1).
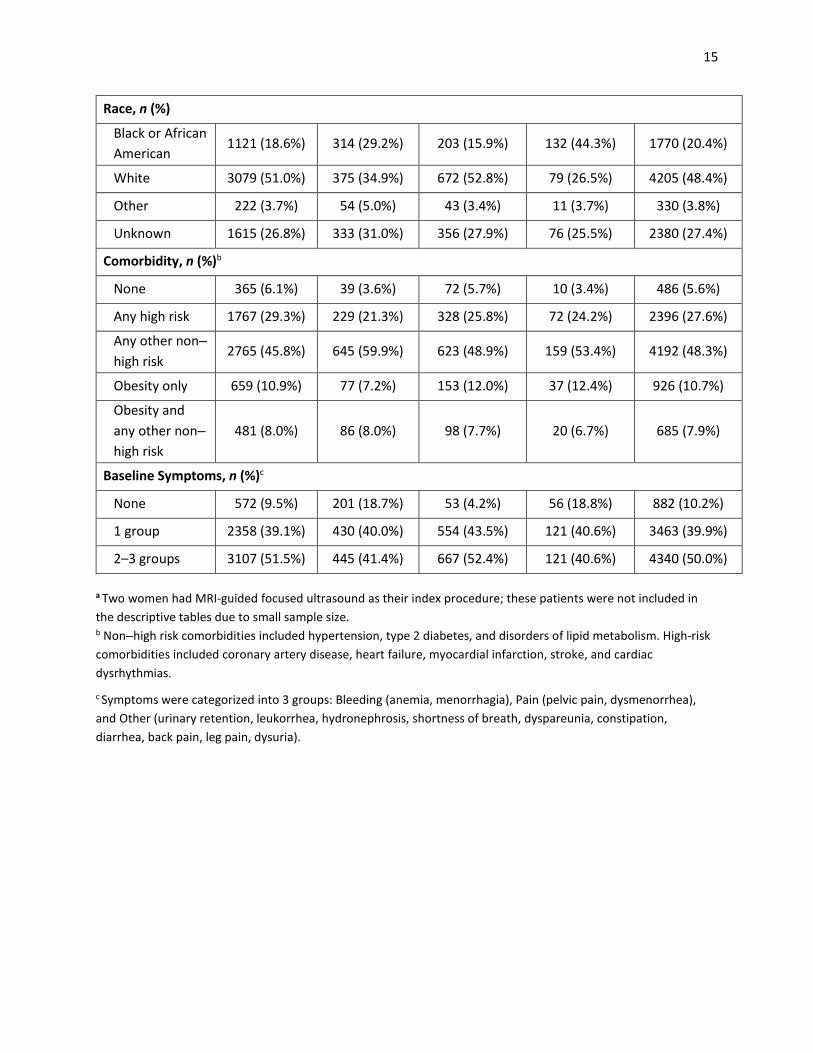
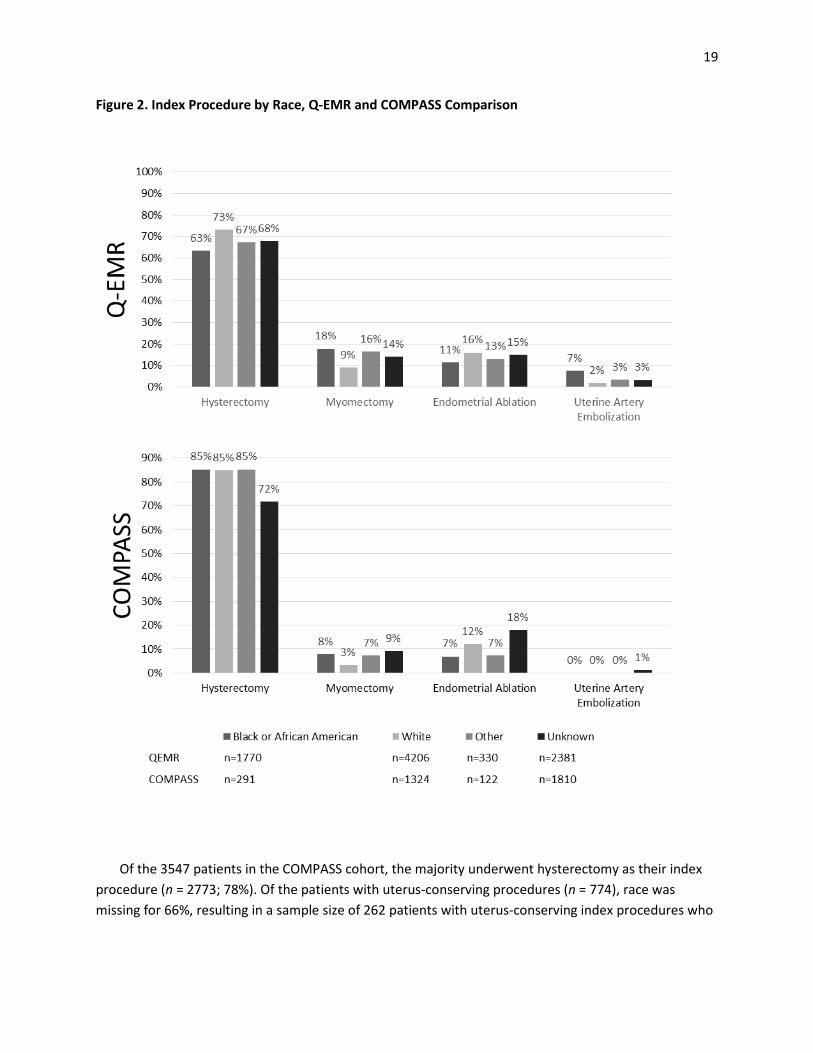
Race was missing for 27% of patients in Q-EMR and 51% of patients in COMPASS, as is often observed in EMR and claims data sources. Among those patients with known race, the majority were white (Q-EMR: 67%; COMPASS: 76%), followed by black or African American (Q-EMR: 28%; COMPASS: 17%; see Tables 2a and 2b). Figure 2 illustrates findings across both data sets with respect to race. White women were more likely than African American women to undergo endometrial ablation in both data sources.
3.1.2 Main Results
After the initial descriptive analysis of the 2 data sets, we performed further analyses using only the Q-EMR data owing to the substantially larger sample size available and on the consensus recommendation of the SPC. All patients were required to have a minimum of 2 years of follow-up data. Among patients in the Q-EMR cohort included in the analysis, the mean and median follow-up time was 53 months and 48 months, respectively (minimum: 24 months; maximum: 111 months). For both study outcomes, the sample size of patients with complete data for race and other covariates for the logistic regression analyses and Cox proportional hazards analyses in Q-EMR was 1869.
18
Figure 1. Index Procedure by Region, Q-EMR and COMPASS Comparison
19
Figure 2. Index Procedure by Race, Q-EMR and COMPASS Comparison
Of the 3547 patients in the COMPASS cohort, the majority underwent hysterectomy as their index procedure (n = 2773; 78%). Of the patients with uterus-conserving procedures (n = 774), race was missing for 66%, resulting in a sample size of 262 patients with uterus-conserving index procedures who
20
had complete data for all covariates. Due to this small sample size, we did not perform regression analyses for COMPASS patients.
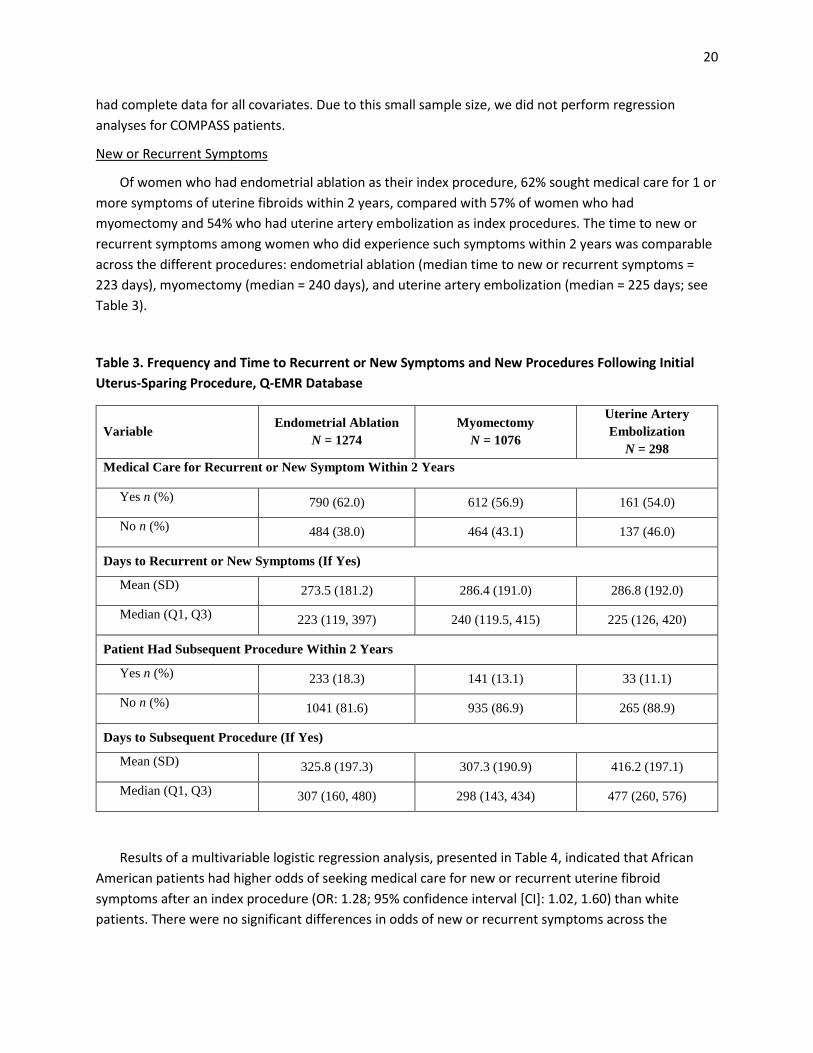
New or Recurrent Symptoms
Of women who had endometrial ablation as their index procedure, 62% sought medical care for 1 or more symptoms of uterine fibroids within 2 years, compared with 57% of women who had myomectomy and 54% who had uterine artery embolization as index procedures. The time to new or recurrent symptoms among women who did experience such symptoms within 2 years was comparable across the different procedures: endometrial ablation (median time to new or recurrent symptoms = 223 days), myomectomy (median = 240 days), and uterine artery embolization (median = 225 days; see Table 3).
Table 3. Frequency and Time to Recurrent or New Symptoms and New Procedures Following Initial Uterus-Sparing Procedure, Q-EMR Database
Variable Endometrial Ablation
N = 1274 Myomectomy
N = 1076
Uterine Artery Embolization
N = 298 Medical Care for Recurrent or New Symptom Within 2 Years
Yes n (%) 790 (62.0) 612 (56.9) 161 (54.0)
No n (%) 484 (38.0) 464 (43.1) 137 (46.0)
Days to Recurrent or New Symptoms (If Yes)
Mean (SD) 273.5 (181.2) 286.4 (191.0) 286.8 (192.0)
Median (Q1, Q3) 223 (119, 397) 240 (119.5, 415) 225 (126, 420)
Patient Had Subsequent Procedure Within 2 Years
Yes n (%) 233 (18.3) 141 (13.1) 33 (11.1)
No n (%) 1041 (81.6) 935 (86.9) 265 (88.9)
Days to Subsequent Procedure (If Yes)
Mean (SD) 325.8 (197.3) 307.3 (190.9) 416.2 (197.1)
Median (Q1, Q3) 307 (160, 480) 298 (143, 434) 477 (260, 576)
Results of a multivariable logistic regression analysis, presented in Table 4, indicated that African American patients had higher odds of seeking medical care for new or recurrent uterine fibroid symptoms after an index procedure (OR: 1.28; 95% confidence interval [CI]: 1.02, 1.60) than white patients. There were no significant differences in odds of new or recurrent symptoms across the
21
procedure groups (myomectomy versus endometrial ablation, OR: 1.03; 95% CI: 0.82, 1.30; uterine artery embolization versus endometrial ablation, OR: 0.90; 95% CI: 0.66, 1.24).
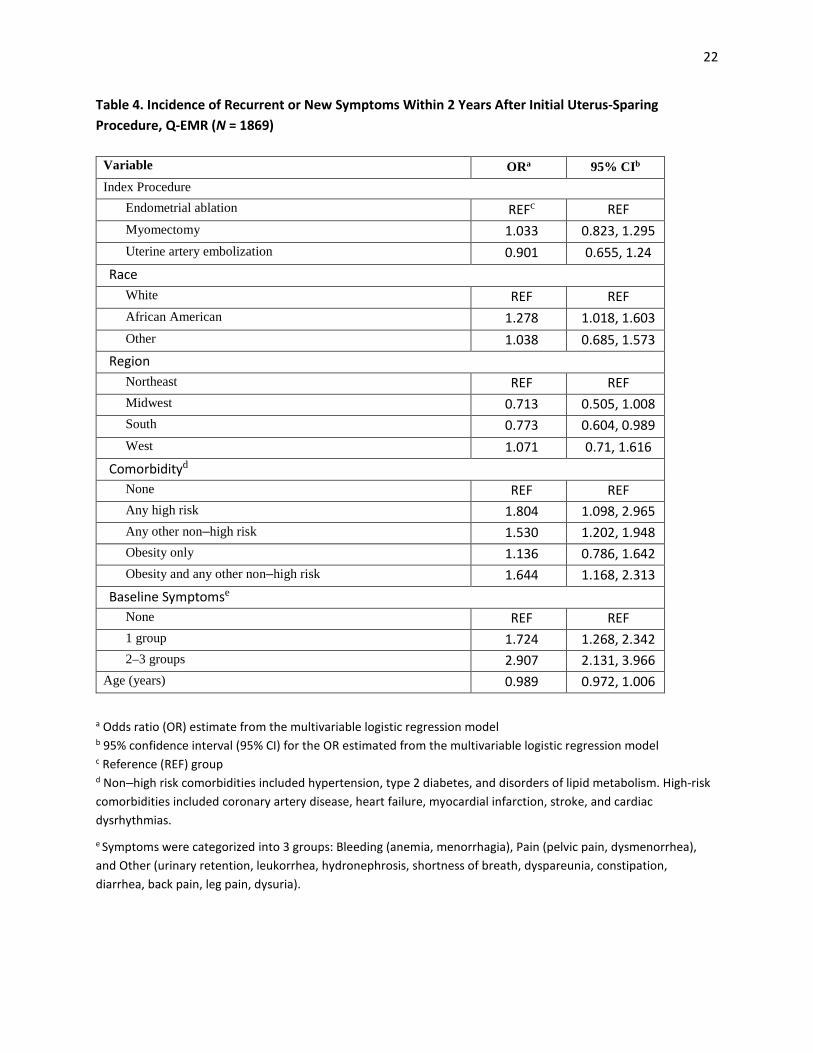
Patients with any high-risk comorbidity (OR: 1.80; 95% CI: 1.10, 2.97), any other non–high risk comorbidity (OR: 1.53; 95% CI: 1.20, 1.95), or both obesity and any other non–high risk comorbidity (OR: 1.64; 95% CI: 1.17, 2.31) had higher incidence of new or recurrent symptoms compared with patients with no symptoms reported after the index procedure (Table 4). Patients with symptoms in 1 symptom group (OR: 1.72; 95% CI: 1.27, 2.34) or 2 or 3 symptom groups at study entry (OR: 2.91; 95% CI: 2.13, 3.97) also had higher incidence of new or recurrent symptoms when compared with patients with no recorded symptoms for which they sought medical care at study entry (Table 4).
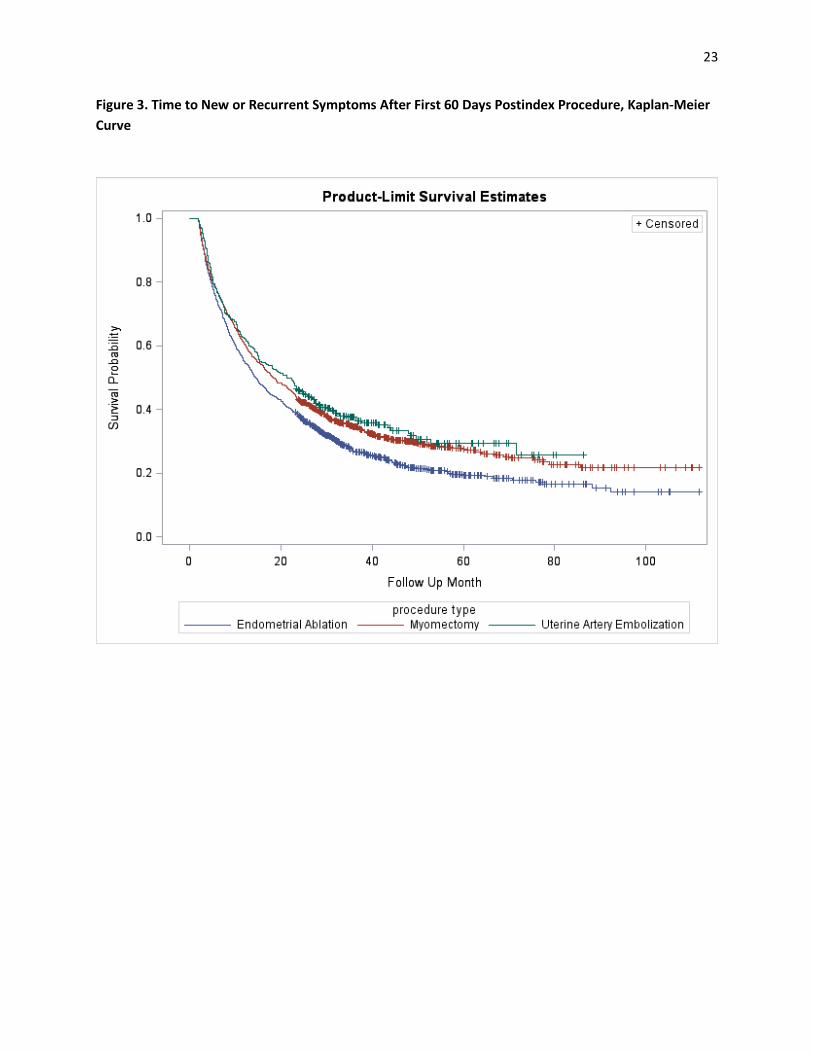
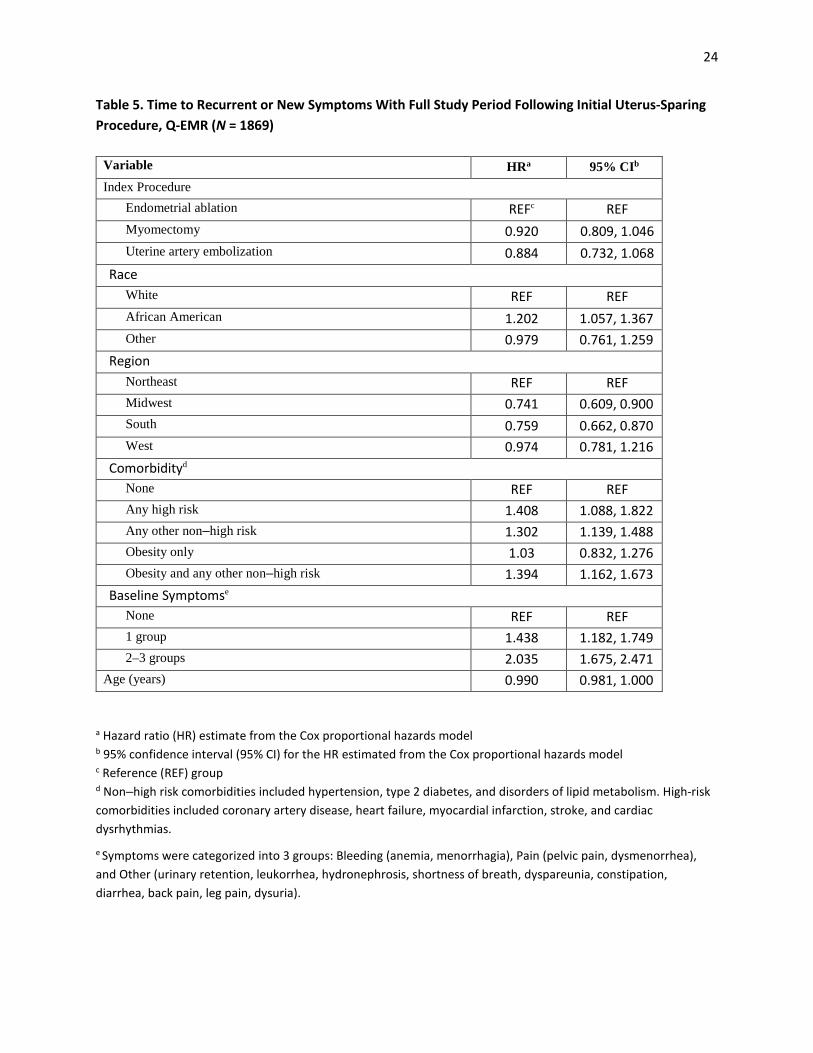
Results of multivariable Cox proportional hazards regression analysis, presented in Table 5 and Figure 3, showed that African American patients had a higher risk of seeking medical care for uterine fibroid symptoms (HR: 1.20; 95% CI: 1.06, 1.37) than white patients. There was no statistically significant difference in risk of seeking medical care for new or recurrent symptoms between myomectomy patients (HR: 0.92; 95% CI: 0.81, 1.05) or uterine artery embolization patients (HR: 0.88; 95% CI: 0.73, 1.07) and endometrial ablation patients.
Patients with any high-risk comorbidity (HR: 1.41; 95% CI: 1.09, 1.82), any other non–high risk comorbidity (HR: 1.30; 95% CI: 1.14, 1.49), or both obesity and any other non–high risk comorbidity (HR: 1.39; 95% CI: 1.16, 1.67) had a higher risk of new or recurrent symptoms compared with patients with no recorded symptoms for which they sought medical care at study entry. Patients with symptoms in 1 baseline group (HR: 1.44; 95% CI: 1.18, 1.75) or 2 or 3 symptom groups at study entry (HR: 2.04; 95% CI: 1.68, 2.47) were at a higher risk for recurrent or new symptoms compared with patients with no recorded symptoms at study entry. Patients in the Midwest (HR: 0.74; 95% CI: 0.61, 0.90) and Southeast (HR: 0.76; 95% CI: 0.66, 0.87) had a lower risk of new or recurrent symptoms compared with patients in the Northeast. Those who underwent a uterine artery embolization or myomectomy as the index procedure had lower risk, albeit not significant, than patients who had endometrial ablation as the index procedure (HR: 0.88; 95% CI: 0.73, 1.07 and HR: 0.92; 95% CI: 0.81, 1.05, respectively).
22
Table 4. Incidence of Recurrent or New Symptoms Within 2 Years After Initial Uterus-Sparing Procedure, Q-EMR (N = 1869)
a Odds ratio (OR) estimate from the multivariable logistic regression model b 95% confidence interval (95% CI) for the OR estimated from the multivariable logistic regression model c Reference (REF) group d Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias.
e Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
Variable ORa 95% CIb
Index Procedure Endometrial ablation REFc REF Myomectomy 1.033 0.823, 1.295 Uterine artery embolization 0.901 0.655, 1.24
Race White REF REF African American 1.278 1.018, 1.603 Other 1.038 0.685, 1.573
Region Northeast REF REF Midwest 0.713 0.505, 1.008 South 0.773 0.604, 0.989 West 1.071 0.71, 1.616
Comorbidityd None REF REF Any high risk 1.804 1.098, 2.965 Any other non–high risk 1.530 1.202, 1.948 Obesity only 1.136 0.786, 1.642 Obesity and any other non–high risk 1.644 1.168, 2.313
Baseline Symptomse None REF REF 1 group 1.724 1.268, 2.342 2–3 groups 2.907 2.131, 3.966
Age (years) 0.989 0.972, 1.006
23
Figure 3. Time to New or Recurrent Symptoms After First 60 Days Postindex Procedure, Kaplan-Meier Curve
24
Table 5. Time to Recurrent or New Symptoms With Full Study Period Following Initial Uterus-Sparing Procedure, Q-EMR (N = 1869)
a Hazard ratio (HR) estimate from the Cox proportional hazards model b 95% confidence interval (95% CI) for the HR estimated from the Cox proportional hazards model c Reference (REF) group d Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias.
e Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
Variable HRa 95% CIb
Index Procedure Endometrial ablation REFc REF Myomectomy 0.920 0.809, 1.046 Uterine artery embolization 0.884 0.732, 1.068
Race White REF REF African American 1.202 1.057, 1.367 Other 0.979 0.761, 1.259
Region Northeast REF REF Midwest 0.741 0.609, 0.900 South 0.759 0.662, 0.870 West 0.974 0.781, 1.216
Comorbidityd None REF REF Any high risk 1.408 1.088, 1.822 Any other non–high risk 1.302 1.139, 1.488 Obesity only 1.03 0.832, 1.276 Obesity and any other non–high risk 1.394 1.162, 1.673
Baseline Symptomse None REF REF 1 group 1.438 1.182, 1.749 2–3 groups 2.035 1.675, 2.471
Age (years) 0.990 0.981, 1.000

25
Subsequent Procedure
Of women who had an endometrial ablation as the index procedure, 18% had a subsequent procedure for treatment of uterine fibroid disease within 2 years of the initial procedure, compared with 13% of women who had myomectomy and 11% who had uterine artery embolization as index procedures. When comparing all available follow-up time, the median and mean times to subsequent procedure were shorter among women who had a myomectomy (mean 307 days, median 298 days) compared with women who underwent uterine artery embolization (mean 416 days, median 477 days) and with those who underwent endometrial ablation (mean 326 days, median 307 days; see Table 3).
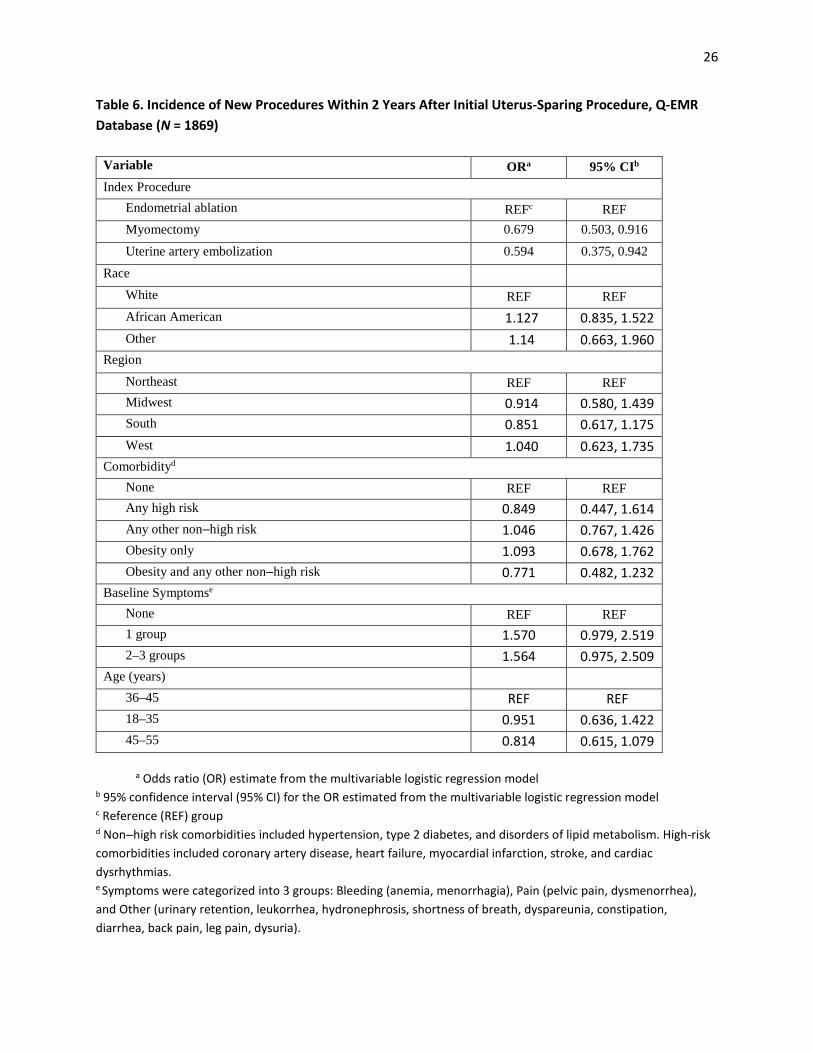
Results of a multivariable logistic regression analysis indicated that African American and white patients had similar rates of subsequent procedures within 2 years following their index procedure (OR: 1.13; 95% CI: 0.84, 1.52; see Table 6). Patients with myomectomy as the index procedure (OR: 0.68; 95% CI: 0.50, 0.92), and patients with uterine artery embolization as the index procedure (OR: 0.59; 95% CI: 0.38, 0.94) had lower odds of having a subsequent procedure within 2 years of their index procedure than those with endometrial ablation. Patients with symptoms in 1 symptom group (OR: 1.57; 95% CI: 0.98, 2.52) or 2 or 3 symptom groups at study entry (OR: 1.56; 95% CI: 0.98, 2.51) had higher odds of having a subsequent procedure within 2 years compared with those with no recorded symptoms for which they sought medical care at study entry, although these results were not statistically significant (Table 6).
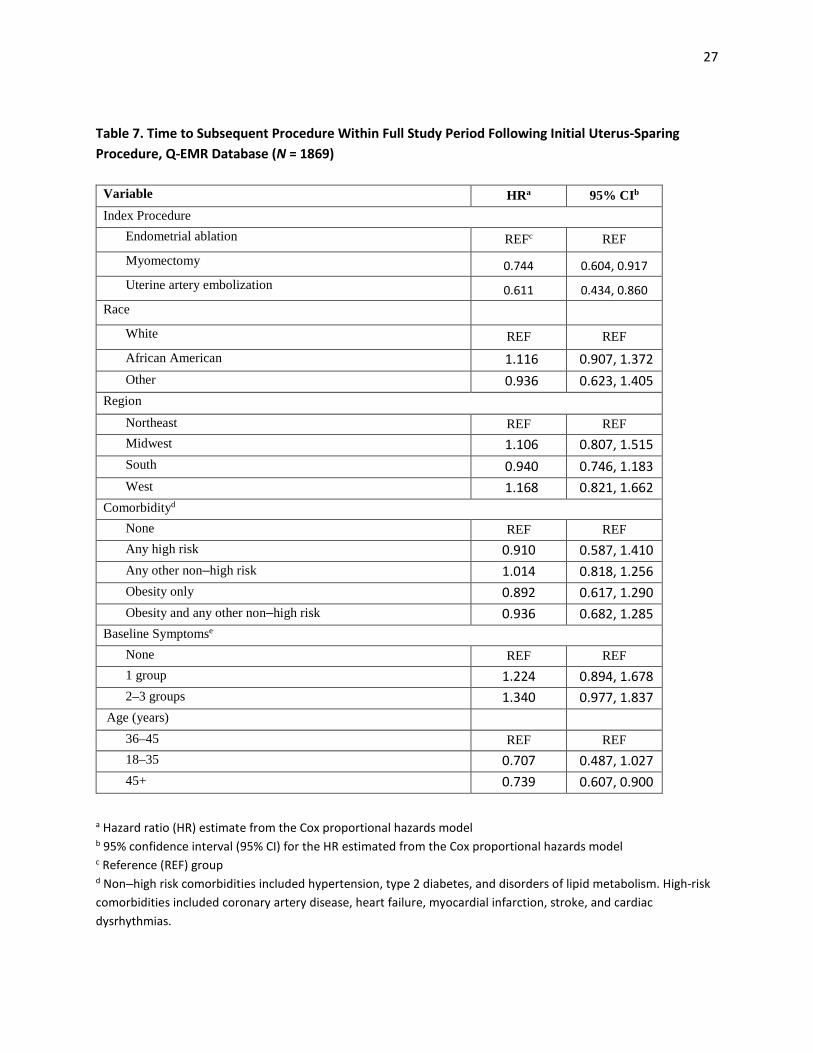
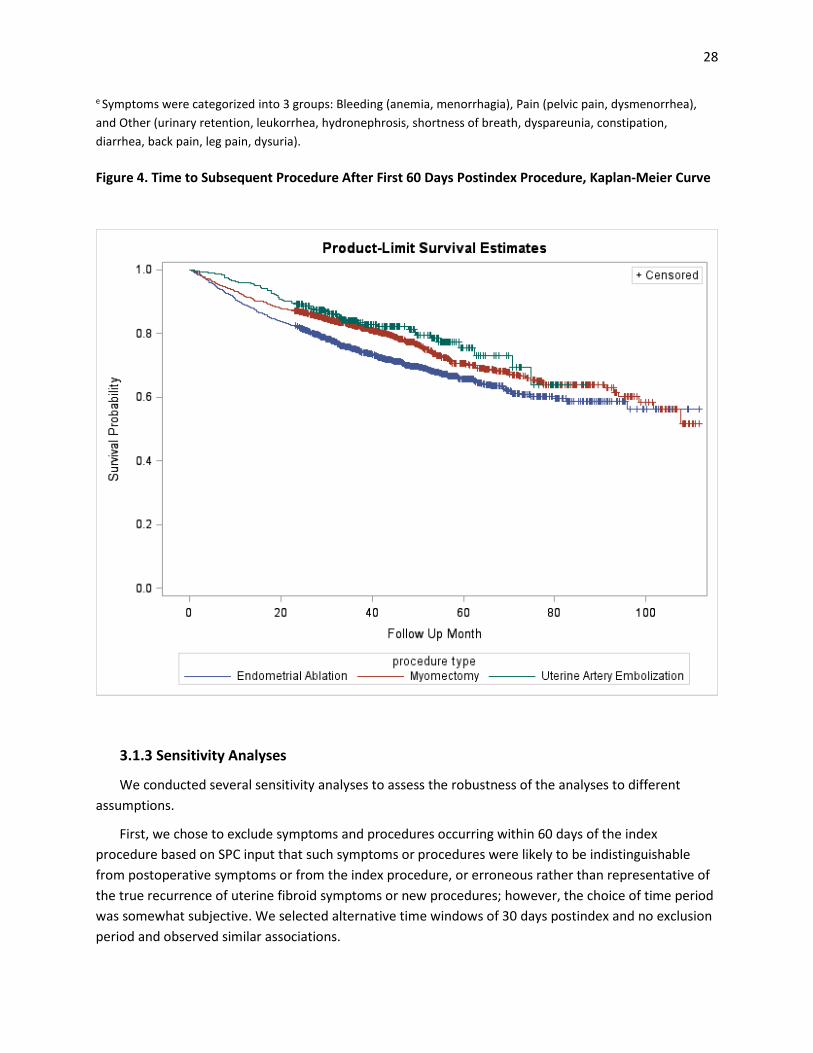
Results of a multivariable Cox proportional hazards regression analysis indicated that African American patients underwent subsequent procedures during the study period about as often as white patients (HR: 1.12; 95% CI: 0.91, 1.37; see Table 7). Patients who underwent either a myomectomy (HR: 0.74; 95% CI: 0.60, 0.92) or uterine artery embolization (HR: 0.61; 95% CI: 0.43, 0.86) as their index procedure were at reduced risk of having a subsequent procedure during the study period compared with patients who had endometrial ablation (Table 7, Figure 4).
26
Table 6. Incidence of New Procedures Within 2 Years After Initial Uterus-Sparing Procedure, Q-EMR Database (N = 1869)
a Odds ratio (OR) estimate from the multivariable logistic regression model b 95% confidence interval (95% CI) for the OR estimated from the multivariable logistic regression model c Reference (REF) group d Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias. e Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
Variable ORa 95% CIb
Index Procedure Endometrial ablation REFc REF Myomectomy 0.679 0.503, 0.916
Uterine artery embolization 0.594 0.375, 0.942
Race White REF REF African American 1.127 0.835, 1.522 Other 1.14 0.663, 1.960
Region
Northeast REF REF Midwest 0.914 0.580, 1.439 South 0.851 0.617, 1.175 West 1.040 0.623, 1.735
Comorbidityd None REF REF Any high risk 0.849 0.447, 1.614 Any other non–high risk 1.046 0.767, 1.426 Obesity only 1.093 0.678, 1.762 Obesity and any other non–high risk 0.771 0.482, 1.232
Baseline Symptomse None REF REF 1 group 1.570 0.979, 2.519 2–3 groups 1.564 0.975, 2.509
Age (years) 36–45 REF REF 18–35 0.951 0.636, 1.422 45–55 0.814 0.615, 1.079
27
Table 7. Time to Subsequent Procedure Within Full Study Period Following Initial Uterus-Sparing Procedure, Q-EMR Database (N = 1869)
a Hazard ratio (HR) estimate from the Cox proportional hazards model b 95% confidence interval (95% CI) for the HR estimated from the Cox proportional hazards model c Reference (REF) group d Non–high risk comorbidities included hypertension, type 2 diabetes, and disorders of lipid metabolism. High-risk comorbidities included coronary artery disease, heart failure, myocardial infarction, stroke, and cardiac dysrhythmias.
Variable HRa 95% CIb
Index Procedure Endometrial ablation REFc REF Myomectomy 0.744 0.604, 0.917 Uterine artery embolization 0.611 0.434, 0.860
Race White REF REF African American 1.116 0.907, 1.372 Other 0.936 0.623, 1.405
Region
Northeast REF REF Midwest 1.106 0.807, 1.515 South 0.940 0.746, 1.183 West 1.168 0.821, 1.662
Comorbidityd None REF REF Any high risk 0.910 0.587, 1.410 Any other non–high risk 1.014 0.818, 1.256 Obesity only 0.892 0.617, 1.290 Obesity and any other non–high risk 0.936 0.682, 1.285
Baseline Symptomse None REF REF 1 group 1.224 0.894, 1.678 2–3 groups 1.340 0.977, 1.837
Age (years) 36–45 REF REF 18–35 0.707 0.487, 1.027 45+ 0.739 0.607, 0.900
28
e Symptoms were categorized into 3 groups: Bleeding (anemia, menorrhagia), Pain (pelvic pain, dysmenorrhea), and Other (urinary retention, leukorrhea, hydronephrosis, shortness of breath, dyspareunia, constipation, diarrhea, back pain, leg pain, dysuria).
Figure 4. Time to Subsequent Procedure After First 60 Days Postindex Procedure, Kaplan-Meier Curve
3.1.3 Sensitivity Analyses
We conducted several sensitivity analyses to assess the robustness of the analyses to different assumptions.
First, we chose to exclude symptoms and procedures occurring within 60 days of the index procedure based on SPC input that such symptoms or procedures were likely to be indistinguishable from postoperative symptoms or from the index procedure, or erroneous rather than representative of the true recurrence of uterine fibroid symptoms or new procedures; however, the choice of time period was somewhat subjective. We selected alternative time windows of 30 days postindex and no exclusion period and observed similar associations.

29
Second, we assessed multiple endpoints related to durability of uterine fibroid treatments, including onset of new or recurrent symptoms and subsequent procedures, both of which we examined over different time frames (2 years of follow-up and the full available follow-up period extending as far as 9 years), using different analytic approaches (unadjusted comparisons of the proportion of patients in each treatment group with the endpoint of interest, comparison of Kaplan-Meier curves, multivariate logistic regression and Cox regression analyses). We saw similar direction of effect with regard to treatment benefit in each analysis favoring uterine artery embolization compared with endometrial ablation, with myomectomy in most cases appearing to be superior to endometrial ablation, although the magnitude of effect varied across analyses.
3.2 Stakeholder Engagement
3.2.1 Main Results
Protocol
After review of the protocol developed by the investigators, the SPC recommended 15 changes, including 1 on duration of follow-up, 3 on inclusion and exclusion criteria, 7 on patient characteristics, 2 on comparators, 1 on outcomes, and 1 on subgroup analyses. Of the 15 recommended changes, 10 were feasible for implementation in the protocol given the proposed study design (see summary in Table 8 and full list of recommendations in Appendix C). The Investigators considered the remaining 5 recommendations but deemed them either not feasible due to limitations with existing data or beyond the scope and focus of the current study.
30
Table 8. Number of Suggestions from the Stakeholder Partnership Council Adopted for Protocol
Area Number of Suggestions
Number Able to Be Implemented
Duration of follow-up 1 1
Inclusion and exclusion criteria 3 2
Patient characteristics 7 3
Comparators 2 0
Outcomes 1 1
Subgroup analyses 1 0
Total 15 7
Analysis
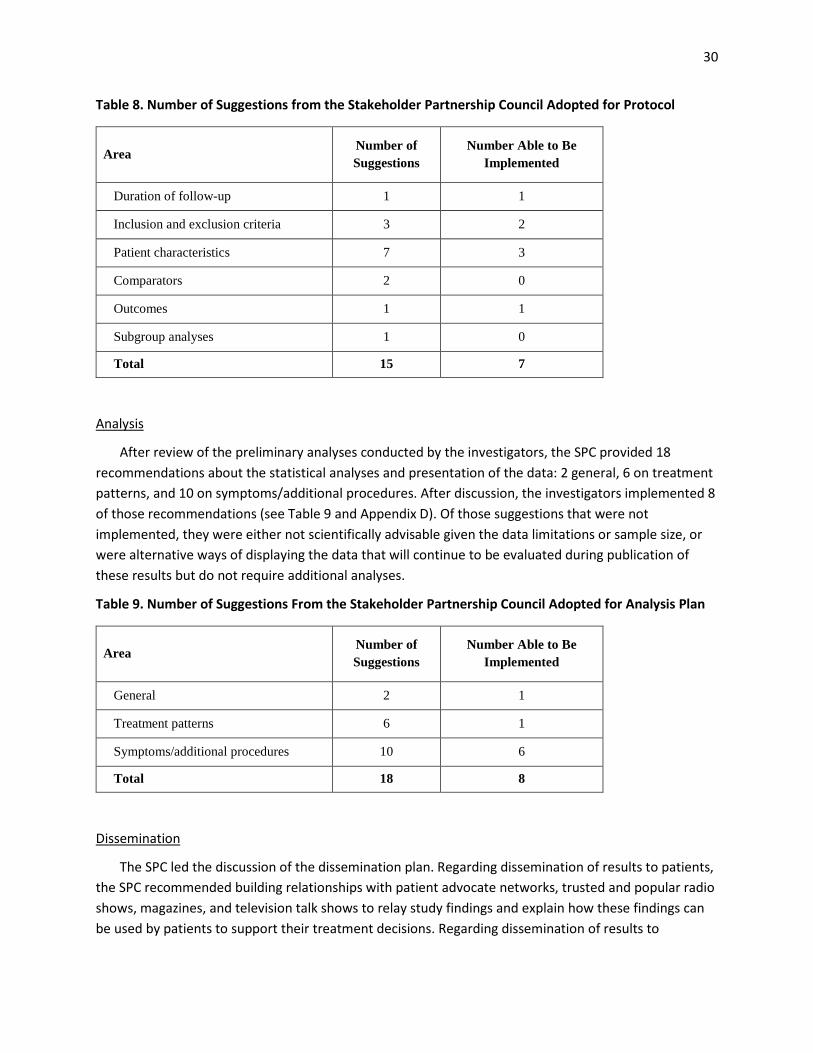
After review of the preliminary analyses conducted by the investigators, the SPC provided 18 recommendations about the statistical analyses and presentation of the data: 2 general, 6 on treatment patterns, and 10 on symptoms/additional procedures. After discussion, the investigators implemented 8 of those recommendations (see Table 9 and Appendix D). Of those suggestions that were not implemented, they were either not scientifically advisable given the data limitations or sample size, or were alternative ways of displaying the data that will continue to be evaluated during publication of these results but do not require additional analyses.
Table 9. Number of Suggestions From the Stakeholder Partnership Council Adopted for Analysis Plan
Area Number of Suggestions
Number Able to Be Implemented
General 2 1
Treatment patterns 6 1
Symptoms/additional procedures 10 6
Total 18 8
Dissemination
The SPC led the discussion of the dissemination plan. Regarding dissemination of results to patients, the SPC recommended building relationships with patient advocate networks, trusted and popular radio shows, magazines, and television talk shows to relay study findings and explain how these findings can be used by patients to support their treatment decisions. Regarding dissemination of results to
31
clinicians, the SPC recommended connecting with clinicians at conferences and through peer reviewed journals.
Stakeholder Evaluation
There was general agreement that a sincere and good effort was made to engage and be responsive to the SPC members’ perspectives. Stakeholders were in unanimous agreement about the value of patient advocate involvement, and 1 person remarked on the benefit of engaging multiple patient advocates. Stakeholders also appreciated the diversity of categories represented within the SPC, and the opportunities to work with and learn from one another. Some of the participants expressed that they would have appreciated more opportunity to interact with the core research team. Many of the stakeholders noted the limitation of the retrospective data; they felt that important questions could not be addressed in the context of this study design.
4. DISCUSSION
4.1 Retrospective Cohort Study
4.1.1 Key Results
Treatment Patterns
The majority of patients underwent hysterectomy as their index procedures in both Q-EMR and COMPASS, while endometrial ablation was the most common uterus-conserving index procedure. Overall, distribution of index procedures was similar across both data sources.
When we analyzed treatment patterns by race, as recommended by the SPC, we found that overall, African American women underwent myomectomy more frequently than white women. When we considered both race and region—another SPC recommendation—we found the percentage of women undergoing myomectomies and endometrial ablation differed slightly by region, with a higher proportion of white women undergoing endometrial ablation in the Midwest, and more African American women undergoing endometrial ablation in the Southeast than white women (data not shown).
New or Recurrent Symptoms
African American women had a 20% greater risk of seeking medical care for new or recurrent uterine fibroid symptoms during the study period than white women. Regarding index procedure, women who underwent myomectomy had an 8% lower risk, though not statistically significant, of seeking medical care for new or recurrent symptoms during the entire study period than those who underwent endometrial ablation, as did women who underwent uterine artery embolization (12% lower, not statistically significant). Factors statistically significantly associated with risk of new or recurrent symptoms postindex procedure included a history of at least 1 comorbidity and having more symptoms recorded in the medical record at study entry. For the most part, logistic regression analyses that examined the likelihood of having any symptoms within 2 years of index procedure and Cox
32
regression analyses that examined the time to seeking medical care for any symptoms during the full study follow-up period yielded similar results.
Subsequent Procedure
Women who underwent a myomectomy or uterine artery embolization had 26% and 39% reduction, respectively, in risk of subsequent procedure during the study period compared with those who underwent endometrial ablation. The risk of subsequent procedure within 2 years of the index procedure was not statistically different between African American and white patients (13% higher risk among African American patients, although, again, not statistically significant). Having more uterine fibroid symptoms recorded in the medical record preprocedure was associated with a 57% increase in odds of having a subsequent procedure within 2 years and a 22% increase during the full study period compared with women without any preprocedure symptoms; however, this association was not statistically significant.
4.1.2 Biases and Limitations
We designed and analyzed the study in a manner to minimize the likelihood that bias would be an alternative explanation for the observed results. However, there are inherent limitations to using EMR and administrative data. Potential sources of bias are described below.
4.1.2.1 Information bias
In this study we analyzed secondary data, which were not collected for research purposes. This may have introduced information bias due to inconsistencies in coding practices, as well as coding that reflected “rule out” diagnoses or “upcoding” practice related to maximizing reimbursement. Also, substantial data were missing for key variables of interest, especially race (a common problem encountered in analyses of EMR and claims data sources), which may or may not be missing at random. As it is not anticipated that missing race or possible “upcoding” of diagnoses would be related to which specific uterine-sparing procedure patients received at baseline, the direction of impact of this bias on the observed associations would be expected to be toward the null; however, this cannot be directly verified.
The underlying cause of symptoms identified in this study could not be determined in either Q-EMR or COMPASS, as would be typical of most EMR data. This may have resulted in inclusion of some symptoms assumed to be uterine fibroid related but that are due to other causes. Also, only symptoms reported to and entered by the health care provider in the EMR were captured in this study. Thus, a patient was likely to have experienced additional symptoms that were not captured in the EMR. Misclassification of symptoms at baseline as well as subsequent symptoms as an outcome would not be expected to be associated with initial procedure, and thus would most likely be expected to bias associations involving either the baseline symptoms measure or the subsequent symptoms outcome measure toward the null.
33
4.1.2.2 Confounding
Some important potential confounders, including such markers for disease severity as number, size, location of fibroids, knowledge of a woman’s childbearing goals, and other reasons for choosing one procedure over another for treatment of uterine fibroids were not available within the EMRs. This unmeasured confounding may have led to overestimates or underestimates of the true associations of specific uterine-sparing procedures with onset of new symptoms and time to subsequent procedures, if reasons underlying the choice of initial procedure also influenced willingness to undergo an additional procedure, or if specific procedures were more likely to be used in women with more severe disease burden who also had a greater need to consider undergoing subsequent procedures (confounding by indication).
We used statistical methods including multivariable regression methods to account for measured confounders in analyses that compared different treatments for uterine fibroids. We had originally planned to perform subgroup analyses defined by race and other important designations (e.g., age), in part to account for potential confounding but also to explore the comparative benefits of the different procedures within these subgroups. However, the sample sizes for the subgroups were relatively small and not sufficient for performing multivariable regression analyses within subgroups. Tests of interaction with race also would have been underpowered due to the small size of the subgroups. This is particularly true for race given the missing data for this variable. Although we did not conduct subgroup analyses, we included race and other important demographic and clinical covariates in the regression models and we provided discussion about differences observed among the groups for these variables (e.g., differences found among the racial groups).
We encourage researchers in future studies with sufficient sample size to explore the comparative effectiveness of uterine fibroid therapies in clinically meaningful subgroups.
4.1.2.3 Generalizability
While the study made specific efforts to ensure regional representativeness and racial diversity through selection of the linked Q-EMR and claims and COMPASS data sources, the patterns of care, including frequency of specific procedures for treatment of uterine fibroids and characteristics of the patient population within these networks may not be fully generalizable to the US population. In addition, only patients who sought medical treatment for their uterine fibroids were reflected in these data sources and only commercially insured patients were available in the linked Q-EMR and claims data. Finally, we focused solely on surgical interventions for uterine fibroids; we did not consider medicinal treatments. Future studies involving comparative analyses of both surgical and medicinal treatments for this condition would clearly be of value.
Use of COMPASS as a second independent data source served as some additional validation of the findings from the Q-EMR data source, but it also identified some additional variation that may reflect regional care patterns. For example, while overall distribution of procedures for treatment of uterine fibroids was relatively similar between the 2 data sources, Q-EMR data reflected a higher prevalence of myomectomy and uterine artery embolization, potentially due to differences in the underlying populations as Q-EMR data focus primarily on outpatient care while COMPASS data also include
34
inpatient data. Further, Q-EMR data include more family practices and fewer obstetrics and gynecology practices than COMPASS, which may underlie the different frequencies of specific procedures. Finally, Q-EMR data include those primarily insured through the commercial market, while COMPASS data also include those insured by Medicaid and those not insured.
4.1.2.4 Missing data Missing information is a common issue with EMR data, especially for certain variables (e.g., race) that are not consistently collected by health care providers. Most of the missing information in the present study (for both data sources) related to race. While imputation strategies are reasonable for handling missingness among certain types of variables (e.g., clinical outcomes), this is not necessarily the case when the missing information is a variable such as race. We excluded patients from the multivariable analysis who were missing race (n = 765 in Q-EMR) and other covariates or who had less than 2 years of follow-up in the EMR system (n = 14 missing other covariates or with less than 2 years of follow-up in Q-EMR). We recognize that, to the extent those with missing race information may differ from the rest of the sample, the external validity of the findings from the regression models may have been affected. However, the underlying mechanism (i.e., missing completely at random, missing at random, missing not at random) of missing race in these databases, especially the Q-EMR database that was used for the multivariable analyses, is uncertain. Moreover, the optimal method for managing missing data for similar databases is unclear.24,25 Missing outcome data due to loss to follow-up is not anticipated because of the requirement that patients have at least 2 years of follow-up from the time of their index procedure. We performed some analyses that capped the follow-up for patients at 2 years, thus adjusting for differential follow-up times across patients. We also performed time-to-event analyses using all follow-up data and censoring patients who were lost to follow-up.
4.2 Stakeholder Engagement
The SPC provided valuable feedback on both the protocol and the analyses of the data. These recommendations were discussed during face-to-face meetings and webinars and the investigators implemented the majority of recommendations that were feasible within the study design and scope. These recommendations were critical in shaping the study design and analyses. The SPC provided numerous recommendations of potential avenues for dissemination of study findings. At the end of the study, the stakeholder engagement evaluation interview assessed the stakeholders’ perspective of their involvement in the study. Overall, there was unanimous agreement about the value of patient advocate involvement, appreciation for the diversity of categories represented within the SPC, and appreciation for the opportunities to work with and learn from one another. Some of the participants expressed that they would have appreciated more opportunity to interact with the core research team. The limitation of the retrospective data source was noted by many of the stakeholders, who felt that important questions could not be addressed in the context of this study design.

35
5. CONCLUSION
5.1 Retrospective Cohort Study
This research provides additional new evidence about expectations for the durability of symptom relief and time to subsequent procedures among women with uterine fibroids that may be helpful to women and their health care providers when making treatment choices. Also, the broad agreement between descriptive results from both Q-EMR and COMPASS provides additional evidence to support the descriptive trends identified in this report.
In this analysis of linked Q-EMR and claims data, women who had uterine artery embolization as an index procedure were somewhat less likely to seek medical care for recurrent symptoms and were substantially less likely to have a subsequent procedure during the study period than women who had endometrial ablation, with women who had myomectomy falling in between. African American race was associated with a 20% greater risk of seeking medical care for recurrent symptoms of uterine fibroids, but it was not statistically significantly associated with an increased risk of subsequent procedures compared with white women.
There are multiple possible explanations for the observed associations of measures of treatment durability with specific uterine-sparing procedures. In addition to the possibility of true underlying differences in effectiveness of symptom relief between the procedures, confounding by indication, in which specific procedures were most commonly selected for women with more severe uterine fibroid disease who were also likely to require additional treatment sooner than women with less severe uterine fibroid disease, should also be considered. Other explanations include more complex relationships between the choice of procedure, desire to preserve fertility, and desire to postpone subsequent procedures. For example, endometrial ablation destroys the uterine lining and is used as a treatment for heavy menstrual bleeding due to multiple etiologies; because the treatment does not physically affect fibroids, recurrence of symptoms, or appearance of symptoms unrelated to bleeding, is not unusual. In randomized trials of endometrial ablation compared with hysterectomy for bleeding for all causes, recurrence rates are high.26 As was discussed at an in-person SPC meeting for this study, it is often understood when choosing uterus-conserving procedures that they are not a permanent or curative treatment but will improve symptoms and quality of life in the short term while preserving fertility or postponing the option of a hysterectomy for other reasons. Thus, it is expected that a subsequent procedure will likely be required in the future and without the initial procedure being considered a treatment “failure.” Future studies, namely prospective studies, should collect data on quality-of-life measures, as well as patient preferences and rationale behind treatment selection for uterine fibroids.
In addition to providing additional information that can inform patient and provider treatment decisions, some of the current study findings can also be applied to inform development of the new COMPARE-UF study, a large prospective patient registry of women with uterine fibroids, which will not share the same limitations of this study related to retrospective analysis of existing EMR and claims data.

36
5.2 Stakeholder Engagement
Overall, the stakeholders provided critical input that shaped the study design, data analysis, and dissemination of key findings. After self-assessment of their involvement, the stakeholders agreed with the value of a diverse stakeholder committee, particularly for eliciting patient perspectives.
37
6. REFERENCES
1. Baird D, Dunson DB, Hill MC, et al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;(188):100-107.
2. Myers ER, Barber MD, Gustilo-Ashby T, et al. Management of uterine leiomyomata: what do we really know? Obstet Gynecol. 2002;(100):8-17.
3. Williams VS, Jones G, Mauskopf J, et al. Uterine fibroids: a review of health-related quality of life assessment. J Womens Health (Larchmt). 2006;(15):818-829.
4. Kuppermann M, Learman LA, Schembri M, et al. Effect of noncancerous pelvic problems on health-related quality of life and sexual functioning. Obstet Gynecol. 2007;(110):633-642.
5. Whiteman MK, Kuklina E, Jamieson DJ, et al. Inpatient hospitalization for gynecologic disorders in the United States. Am J Obstet Gynecol. 2010;(202):541.e1-541.e6.
6. Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009;(91):1215-1223.
7. Sunkara SK, Khairy M, El-Toukhy T, et al. The effect of intramural fibroids without uterine cavity involvement on the outcome of IVF treatment: a systematic review and meta-analysis. Hum Reprod. 2010;(25):418-429.
8. Johnson G, MacLehose RF, Baird DD, et al. Uterine leiomyomata and fecundability in the Right From the Start study. Hum Reprod. 2012;(27):2991-2997.
9. Laughlin SK, Baird DD, Savitz DA, et al. Prevalence of uterine leiomyomas in the first trimester of pregnancy: an ultrasound-screening study. Obstet Gynecol. 2009;113:630-635.
10. Klatsky PC, Tran ND, Caughey AB, et al. Fibroids and reproductive outcomes: a systematic literature review from conception to delivery. Am J Obstet Gynecol. 2008;198:357-366.
11. Lai J, Caughey AB, Qidwai GI, et al. Neonatal outcomes in women with sonographically identified uterine leiomyomata. J Matern Fetal Neonatal Med. 2012;(25):710-713.
12. Bulun SE. Uterine fibroids. N Engl J Med. 2013;369(14):1344-1355. 13. Lerner D, Mirza F, Chang H, et al. Impaired work performance among women with symptomatic
uterine fibroids. J Occup Environ Med. 2008;(50):1149-1157. 14. Frick KD, Clark MA, Steinwachs DM, et al. Financial and quality-of-life burden of dysfunctional
uterine bleeding among women agreeing to obtain surgical treatment. Womens Health Issues. 2009;(19):70-78.
15. Viswanathan M, Hartmann K, McKoy N, et al. Management of uterine fibroids: an update of the evidence. Evid Rep Technol Assess (Full Rep). 2007(154):1-122.
16. Myers ER, Goodwin S, Landow W, et al. Prospective data collection of a new procedure by a specialty society: the FIBROID registry. Obstet Gynecol. 2005;(106):44-51.
17. Moorman PG, Schildkraut JM, Myers ER, et al. Reported symptoms before and one year after hysterectomy in African American and white women. J Womens Health (Larchmt). 2011;(20):1035-1042.
38
18. Moorman PG, Leppert P, Myers ER, et al. Comparison of characteristics of fibroids in African American and white women undergoing premenopausal hysterectomy. Fertil Steril. 2013;99(3):768-776.
19. Bower JK, Schreiner PJ, Sternfeld B, et al. Black–white differences in hysterectomy prevalence: the CARDIA study. Am J Public Health. 2009;(99):300-307.
20. Kjerulff KH, Guzinski GM, Langenberg PW, et al. Hysterectomy and race. Obstet Gynecol. 1993;(82):757-764.
21. Roth TM, Gustilo-Ashby T, Barber MD, et al. Effects of race and clinical factors on short-term outcomes of abdominal myomectomy. Obstet Gynecol. 2003;(101):881-884.
22. Hakim RB, Benedict MB, Merrick NJ. Quality of care for women undergoing a hysterectomy: effects of insurance and race/ethnicity. Am J Public Health. 2004;(94):1399-1405.
23. Huse DM. (2013, May). Expanding the evidence base in outcomes research: linking electronic medical records and claims data. Presented at the 2013 Truven Health Advantage Conference, Scottsdale, AZ. Available at: https://www.ispor.org/meetings/neworleans0513/releasedpresentations/W26-Durden.pdf.
24. Henry AJ, Hevelone ND, Lipsitz, S, Nguyen LL. Comparative methods for handling missing data in large databases. J Vasc Surg. 2013;58(5):1353-1359.
25. Meghani SH, Wiedemer NL, Harden P, et al. (2008, Feb). Missing race/ethnicity data in the VA longitudinal online research database: implications for health disparities researchers. Presented at the 2008 Health Services Research and Development National Meeting in Baltimore, MD. Available at: https://www.hsrd.research.va.gov/meetings/2008/display_abstract.cfm?RecordID=45
26. Fergusson RJ, Lethaby A, Shepperd S, et al. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev. 2013;11. Art. No.: CD000329.
27. PCORI Methodology Committee. The PCORI Methodology Report. Patient-Centered Outcomes Research Institute; 2013. Available from http://www.pcori.org/research-we-support/research-methodology-standards.
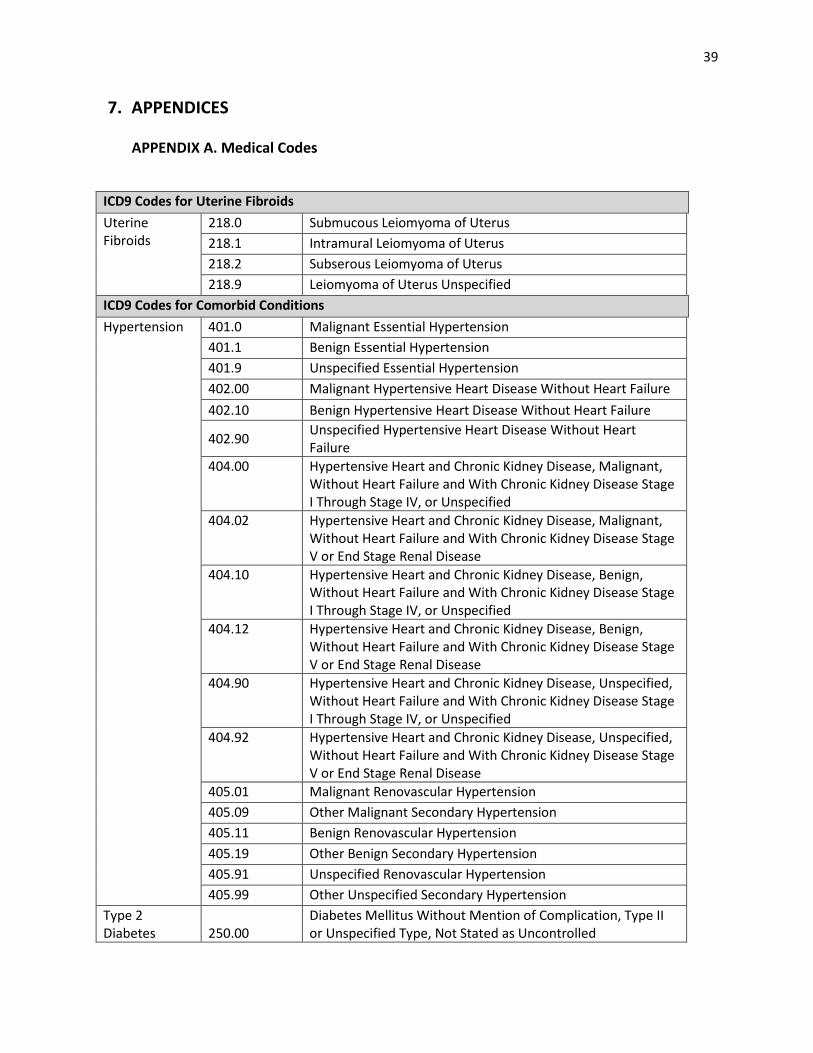
39
7. APPENDICES
APPENDIX A. Medical Codes
ICD9 Codes for Uterine Fibroids Uterine Fibroids
218.0 Submucous Leiomyoma of Uterus 218.1 Intramural Leiomyoma of Uterus 218.2 Subserous Leiomyoma of Uterus 218.9 Leiomyoma of Uterus Unspecified
ICD9 Codes for Comorbid Conditions Hypertension 401.0 Malignant Essential Hypertension
401.1 Benign Essential Hypertension 401.9 Unspecified Essential Hypertension 402.00 Malignant Hypertensive Heart Disease Without Heart Failure 402.10 Benign Hypertensive Heart Disease Without Heart Failure
402.90
Unspecified Hypertensive Heart Disease Without Heart Failure
404.00 Hypertensive Heart and Chronic Kidney Disease, Malignant, Without Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.02 Hypertensive Heart and Chronic Kidney Disease, Malignant, Without Heart Failure and With Chronic Kidney Disease Stage V or End Stage Renal Disease
404.10 Hypertensive Heart and Chronic Kidney Disease, Benign, Without Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.12 Hypertensive Heart and Chronic Kidney Disease, Benign, Without Heart Failure and With Chronic Kidney Disease Stage V or End Stage Renal Disease
404.90 Hypertensive Heart and Chronic Kidney Disease, Unspecified, Without Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.92 Hypertensive Heart and Chronic Kidney Disease, Unspecified, Without Heart Failure and With Chronic Kidney Disease Stage V or End Stage Renal Disease
405.01 Malignant Renovascular Hypertension 405.09 Other Malignant Secondary Hypertension 405.11 Benign Renovascular Hypertension 405.19 Other Benign Secondary Hypertension 405.91 Unspecified Renovascular Hypertension 405.99 Other Unspecified Secondary Hypertension
Type 2 Diabetes 250.00
Diabetes Mellitus Without Mention of Complication, Type II or Unspecified Type, Not Stated as Uncontrolled
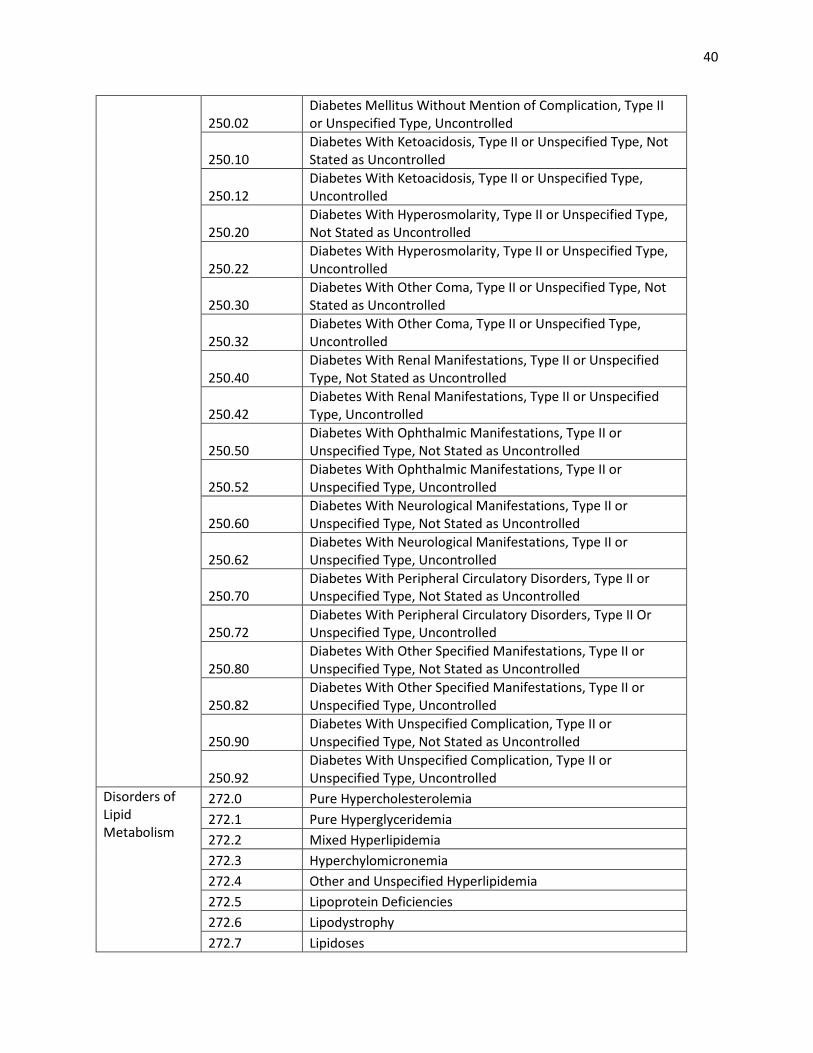
40
250.02 Diabetes Mellitus Without Mention of Complication, Type II or Unspecified Type, Uncontrolled
250.10 Diabetes With Ketoacidosis, Type II or Unspecified Type, Not Stated as Uncontrolled
250.12 Diabetes With Ketoacidosis, Type II or Unspecified Type, Uncontrolled
250.20 Diabetes With Hyperosmolarity, Type II or Unspecified Type, Not Stated as Uncontrolled
250.22 Diabetes With Hyperosmolarity, Type II or Unspecified Type, Uncontrolled
250.30 Diabetes With Other Coma, Type II or Unspecified Type, Not Stated as Uncontrolled
250.32 Diabetes With Other Coma, Type II or Unspecified Type, Uncontrolled
250.40 Diabetes With Renal Manifestations, Type II or Unspecified Type, Not Stated as Uncontrolled
250.42 Diabetes With Renal Manifestations, Type II or Unspecified Type, Uncontrolled
250.50 Diabetes With Ophthalmic Manifestations, Type II or Unspecified Type, Not Stated as Uncontrolled
250.52 Diabetes With Ophthalmic Manifestations, Type II or Unspecified Type, Uncontrolled
250.60 Diabetes With Neurological Manifestations, Type II or Unspecified Type, Not Stated as Uncontrolled
250.62 Diabetes With Neurological Manifestations, Type II or Unspecified Type, Uncontrolled
250.70 Diabetes With Peripheral Circulatory Disorders, Type II or Unspecified Type, Not Stated as Uncontrolled
250.72 Diabetes With Peripheral Circulatory Disorders, Type II Or Unspecified Type, Uncontrolled
250.80 Diabetes With Other Specified Manifestations, Type II or Unspecified Type, Not Stated as Uncontrolled
250.82 Diabetes With Other Specified Manifestations, Type II or Unspecified Type, Uncontrolled
250.90 Diabetes With Unspecified Complication, Type II or Unspecified Type, Not Stated as Uncontrolled
250.92 Diabetes With Unspecified Complication, Type II or Unspecified Type, Uncontrolled
Disorders of Lipid Metabolism
272.0 Pure Hypercholesterolemia 272.1 Pure Hyperglyceridemia 272.2 Mixed Hyperlipidemia 272.3 Hyperchylomicronemia 272.4 Other and Unspecified Hyperlipidemia 272.5 Lipoprotein Deficiencies 272.6 Lipodystrophy 272.7 Lipidoses
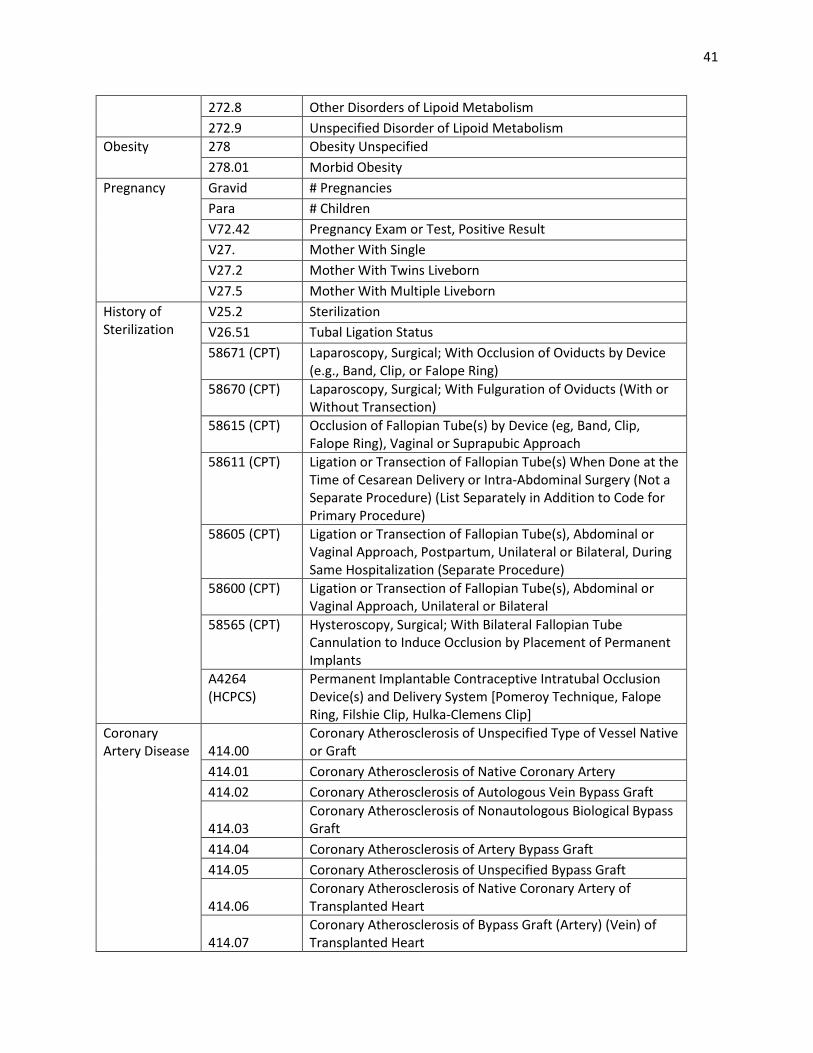
41
272.8 Other Disorders of Lipoid Metabolism 272.9 Unspecified Disorder of Lipoid Metabolism
Obesity 278 Obesity Unspecified 278.01 Morbid Obesity
Pregnancy Gravid # Pregnancies Para # Children V72.42 Pregnancy Exam or Test, Positive Result V27. Mother With Single V27.2 Mother With Twins Liveborn V27.5 Mother With Multiple Liveborn
History of Sterilization
V25.2 Sterilization V26.51 Tubal Ligation Status 58671 (CPT) Laparoscopy, Surgical; With Occlusion of Oviducts by Device
(e.g., Band, Clip, or Falope Ring) 58670 (CPT) Laparoscopy, Surgical; With Fulguration of Oviducts (With or
Without Transection) 58615 (CPT) Occlusion of Fallopian Tube(s) by Device (eg, Band, Clip,
Falope Ring), Vaginal or Suprapubic Approach 58611 (CPT) Ligation or Transection of Fallopian Tube(s) When Done at the
Time of Cesarean Delivery or Intra-Abdominal Surgery (Not a Separate Procedure) (List Separately in Addition to Code for Primary Procedure)
58605 (CPT) Ligation or Transection of Fallopian Tube(s), Abdominal or Vaginal Approach, Postpartum, Unilateral or Bilateral, During Same Hospitalization (Separate Procedure)
58600 (CPT) Ligation or Transection of Fallopian Tube(s), Abdominal or Vaginal Approach, Unilateral or Bilateral
58565 (CPT) Hysteroscopy, Surgical; With Bilateral Fallopian Tube Cannulation to Induce Occlusion by Placement of Permanent Implants
A4264 (HCPCS)
Permanent Implantable Contraceptive Intratubal Occlusion Device(s) and Delivery System [Pomeroy Technique, Falope Ring, Filshie Clip, Hulka-Clemens Clip]
Coronary Artery Disease 414.00
Coronary Atherosclerosis of Unspecified Type of Vessel Native or Graft
414.01 Coronary Atherosclerosis of Native Coronary Artery 414.02 Coronary Atherosclerosis of Autologous Vein Bypass Graft
414.03 Coronary Atherosclerosis of Nonautologous Biological Bypass Graft
414.04 Coronary Atherosclerosis of Artery Bypass Graft 414.05 Coronary Atherosclerosis of Unspecified Bypass Graft
414.06 Coronary Atherosclerosis of Native Coronary Artery of Transplanted Heart
414.07 Coronary Atherosclerosis of Bypass Graft (Artery) (Vein) of Transplanted Heart
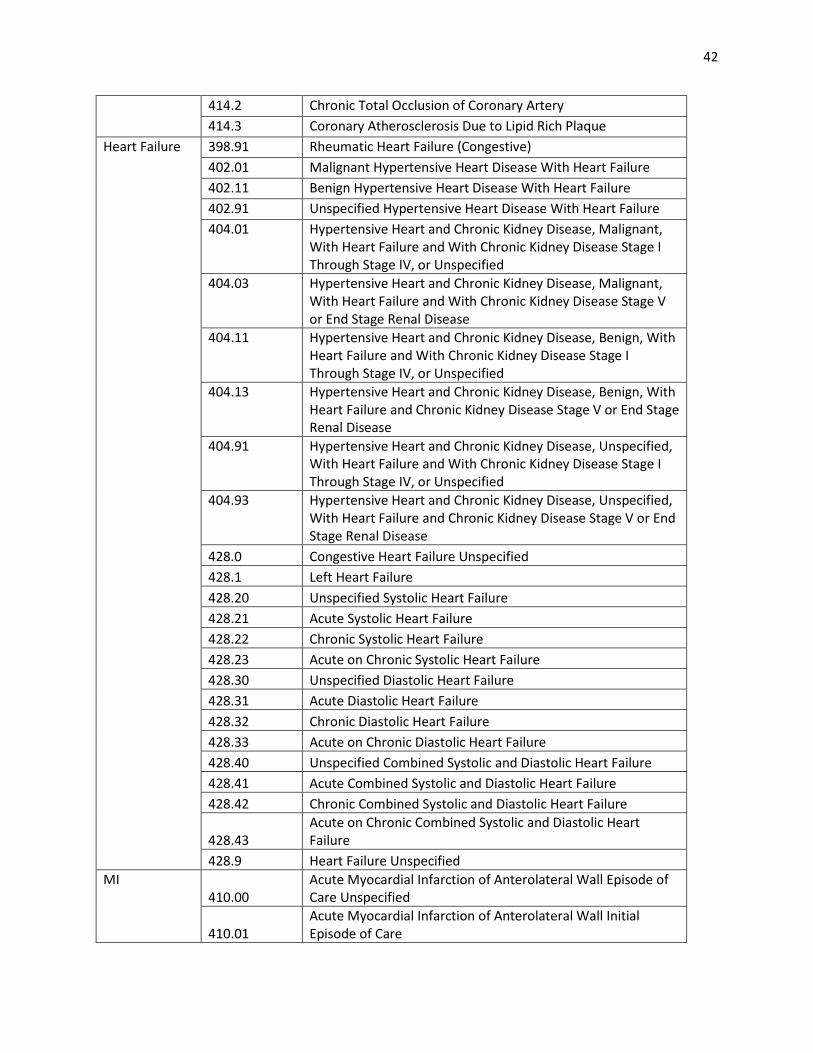
42
414.2 Chronic Total Occlusion of Coronary Artery 414.3 Coronary Atherosclerosis Due to Lipid Rich Plaque
Heart Failure 398.91 Rheumatic Heart Failure (Congestive) 402.01 Malignant Hypertensive Heart Disease With Heart Failure 402.11 Benign Hypertensive Heart Disease With Heart Failure 402.91 Unspecified Hypertensive Heart Disease With Heart Failure 404.01 Hypertensive Heart and Chronic Kidney Disease, Malignant,
With Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.03 Hypertensive Heart and Chronic Kidney Disease, Malignant, With Heart Failure and With Chronic Kidney Disease Stage V or End Stage Renal Disease
404.11 Hypertensive Heart and Chronic Kidney Disease, Benign, With Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.13 Hypertensive Heart and Chronic Kidney Disease, Benign, With Heart Failure and Chronic Kidney Disease Stage V or End Stage Renal Disease
404.91 Hypertensive Heart and Chronic Kidney Disease, Unspecified, With Heart Failure and With Chronic Kidney Disease Stage I Through Stage IV, or Unspecified
404.93 Hypertensive Heart and Chronic Kidney Disease, Unspecified, With Heart Failure and Chronic Kidney Disease Stage V or End Stage Renal Disease
428.0 Congestive Heart Failure Unspecified 428.1 Left Heart Failure 428.20 Unspecified Systolic Heart Failure 428.21 Acute Systolic Heart Failure 428.22 Chronic Systolic Heart Failure 428.23 Acute on Chronic Systolic Heart Failure 428.30 Unspecified Diastolic Heart Failure 428.31 Acute Diastolic Heart Failure 428.32 Chronic Diastolic Heart Failure 428.33 Acute on Chronic Diastolic Heart Failure 428.40 Unspecified Combined Systolic and Diastolic Heart Failure 428.41 Acute Combined Systolic and Diastolic Heart Failure 428.42 Chronic Combined Systolic and Diastolic Heart Failure
428.43 Acute on Chronic Combined Systolic and Diastolic Heart Failure
428.9 Heart Failure Unspecified MI
410.00 Acute Myocardial Infarction of Anterolateral Wall Episode of Care Unspecified
410.01 Acute Myocardial Infarction of Anterolateral Wall Initial Episode of Care
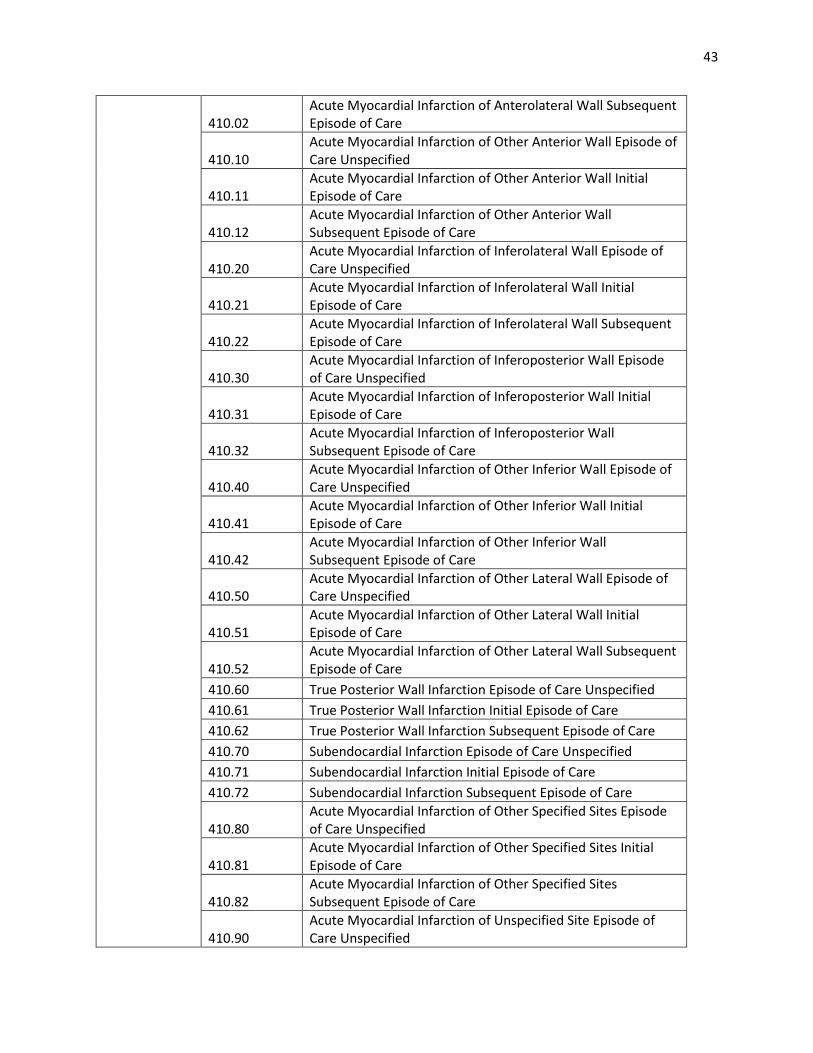
43
410.02 Acute Myocardial Infarction of Anterolateral Wall Subsequent Episode of Care
410.10 Acute Myocardial Infarction of Other Anterior Wall Episode of Care Unspecified
410.11 Acute Myocardial Infarction of Other Anterior Wall Initial Episode of Care
410.12 Acute Myocardial Infarction of Other Anterior Wall Subsequent Episode of Care
410.20 Acute Myocardial Infarction of Inferolateral Wall Episode of Care Unspecified
410.21 Acute Myocardial Infarction of Inferolateral Wall Initial Episode of Care
410.22 Acute Myocardial Infarction of Inferolateral Wall Subsequent Episode of Care
410.30 Acute Myocardial Infarction of Inferoposterior Wall Episode of Care Unspecified
410.31 Acute Myocardial Infarction of Inferoposterior Wall Initial Episode of Care
410.32 Acute Myocardial Infarction of Inferoposterior Wall Subsequent Episode of Care
410.40 Acute Myocardial Infarction of Other Inferior Wall Episode of Care Unspecified
410.41 Acute Myocardial Infarction of Other Inferior Wall Initial Episode of Care
410.42 Acute Myocardial Infarction of Other Inferior Wall Subsequent Episode of Care
410.50 Acute Myocardial Infarction of Other Lateral Wall Episode of Care Unspecified
410.51 Acute Myocardial Infarction of Other Lateral Wall Initial Episode of Care
410.52 Acute Myocardial Infarction of Other Lateral Wall Subsequent Episode of Care
410.60 True Posterior Wall Infarction Episode of Care Unspecified 410.61 True Posterior Wall Infarction Initial Episode of Care 410.62 True Posterior Wall Infarction Subsequent Episode of Care 410.70 Subendocardial Infarction Episode of Care Unspecified 410.71 Subendocardial Infarction Initial Episode of Care 410.72 Subendocardial Infarction Subsequent Episode of Care
410.80 Acute Myocardial Infarction of Other Specified Sites Episode of Care Unspecified
410.81 Acute Myocardial Infarction of Other Specified Sites Initial Episode of Care
410.82 Acute Myocardial Infarction of Other Specified Sites Subsequent Episode of Care
410.90 Acute Myocardial Infarction of Unspecified Site Episode of Care Unspecified
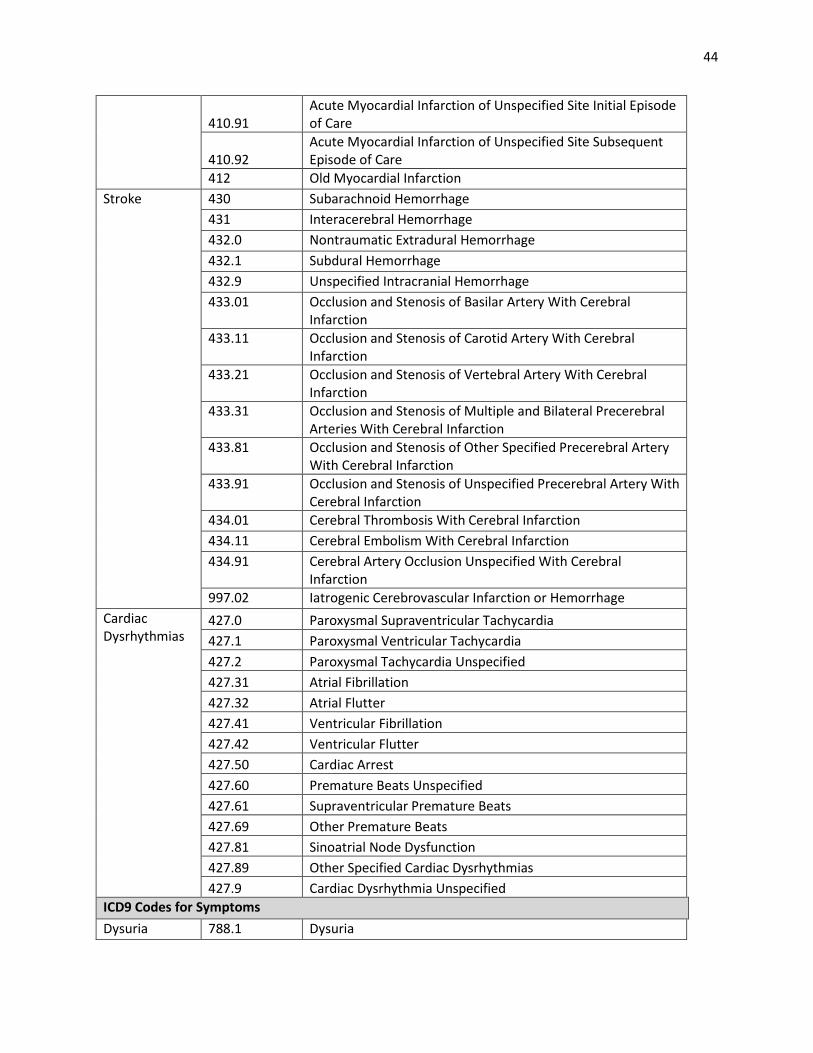
44
410.91 Acute Myocardial Infarction of Unspecified Site Initial Episode of Care
410.92 Acute Myocardial Infarction of Unspecified Site Subsequent Episode of Care
412 Old Myocardial Infarction Stroke 430 Subarachnoid Hemorrhage
431 Interacerebral Hemorrhage 432.0 Nontraumatic Extradural Hemorrhage 432.1 Subdural Hemorrhage 432.9 Unspecified Intracranial Hemorrhage 433.01 Occlusion and Stenosis of Basilar Artery With Cerebral
Infarction 433.11 Occlusion and Stenosis of Carotid Artery With Cerebral
Infarction 433.21 Occlusion and Stenosis of Vertebral Artery With Cerebral
Infarction 433.31 Occlusion and Stenosis of Multiple and Bilateral Precerebral
Arteries With Cerebral Infarction 433.81 Occlusion and Stenosis of Other Specified Precerebral Artery
With Cerebral Infarction 433.91 Occlusion and Stenosis of Unspecified Precerebral Artery With
Cerebral Infarction 434.01 Cerebral Thrombosis With Cerebral Infarction 434.11 Cerebral Embolism With Cerebral Infarction 434.91 Cerebral Artery Occlusion Unspecified With Cerebral
Infarction 997.02 Iatrogenic Cerebrovascular Infarction or Hemorrhage
Cardiac Dysrhythmias
427.0 Paroxysmal Supraventricular Tachycardia 427.1 Paroxysmal Ventricular Tachycardia 427.2 Paroxysmal Tachycardia Unspecified 427.31 Atrial Fibrillation 427.32 Atrial Flutter 427.41 Ventricular Fibrillation 427.42 Ventricular Flutter 427.50 Cardiac Arrest 427.60 Premature Beats Unspecified 427.61 Supraventricular Premature Beats 427.69 Other Premature Beats 427.81 Sinoatrial Node Dysfunction 427.89 Other Specified Cardiac Dysrhythmias 427.9 Cardiac Dysrhythmia Unspecified
ICD9 Codes for Symptoms Dysuria 788.1 Dysuria
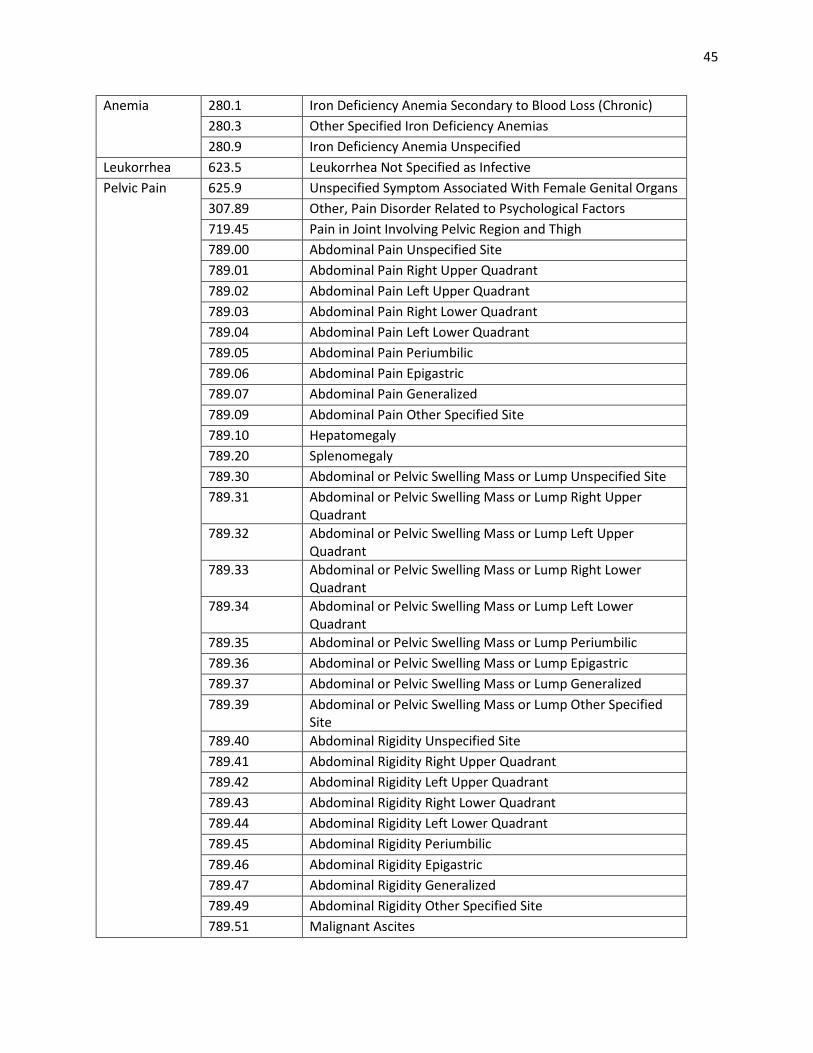
45
Anemia 280.1 Iron Deficiency Anemia Secondary to Blood Loss (Chronic) 280.3 Other Specified Iron Deficiency Anemias 280.9 Iron Deficiency Anemia Unspecified
Leukorrhea 623.5 Leukorrhea Not Specified as Infective Pelvic Pain 625.9 Unspecified Symptom Associated With Female Genital Organs
307.89 Other, Pain Disorder Related to Psychological Factors 719.45 Pain in Joint Involving Pelvic Region and Thigh 789.00 Abdominal Pain Unspecified Site 789.01 Abdominal Pain Right Upper Quadrant 789.02 Abdominal Pain Left Upper Quadrant 789.03 Abdominal Pain Right Lower Quadrant 789.04 Abdominal Pain Left Lower Quadrant 789.05 Abdominal Pain Periumbilic 789.06 Abdominal Pain Epigastric 789.07 Abdominal Pain Generalized 789.09 Abdominal Pain Other Specified Site 789.10 Hepatomegaly 789.20 Splenomegaly 789.30 Abdominal or Pelvic Swelling Mass or Lump Unspecified Site 789.31 Abdominal or Pelvic Swelling Mass or Lump Right Upper
Quadrant 789.32 Abdominal or Pelvic Swelling Mass or Lump Left Upper
Quadrant 789.33 Abdominal or Pelvic Swelling Mass or Lump Right Lower
Quadrant 789.34 Abdominal or Pelvic Swelling Mass or Lump Left Lower
Quadrant 789.35 Abdominal or Pelvic Swelling Mass or Lump Periumbilic 789.36 Abdominal or Pelvic Swelling Mass or Lump Epigastric 789.37 Abdominal or Pelvic Swelling Mass or Lump Generalized 789.39 Abdominal or Pelvic Swelling Mass or Lump Other Specified
Site 789.40 Abdominal Rigidity Unspecified Site 789.41 Abdominal Rigidity Right Upper Quadrant 789.42 Abdominal Rigidity Left Upper Quadrant 789.43 Abdominal Rigidity Right Lower Quadrant 789.44 Abdominal Rigidity Left Lower Quadrant 789.45 Abdominal Rigidity Periumbilic 789.46 Abdominal Rigidity Epigastric 789.47 Abdominal Rigidity Generalized 789.49 Abdominal Rigidity Other Specified Site 789.51 Malignant Ascites
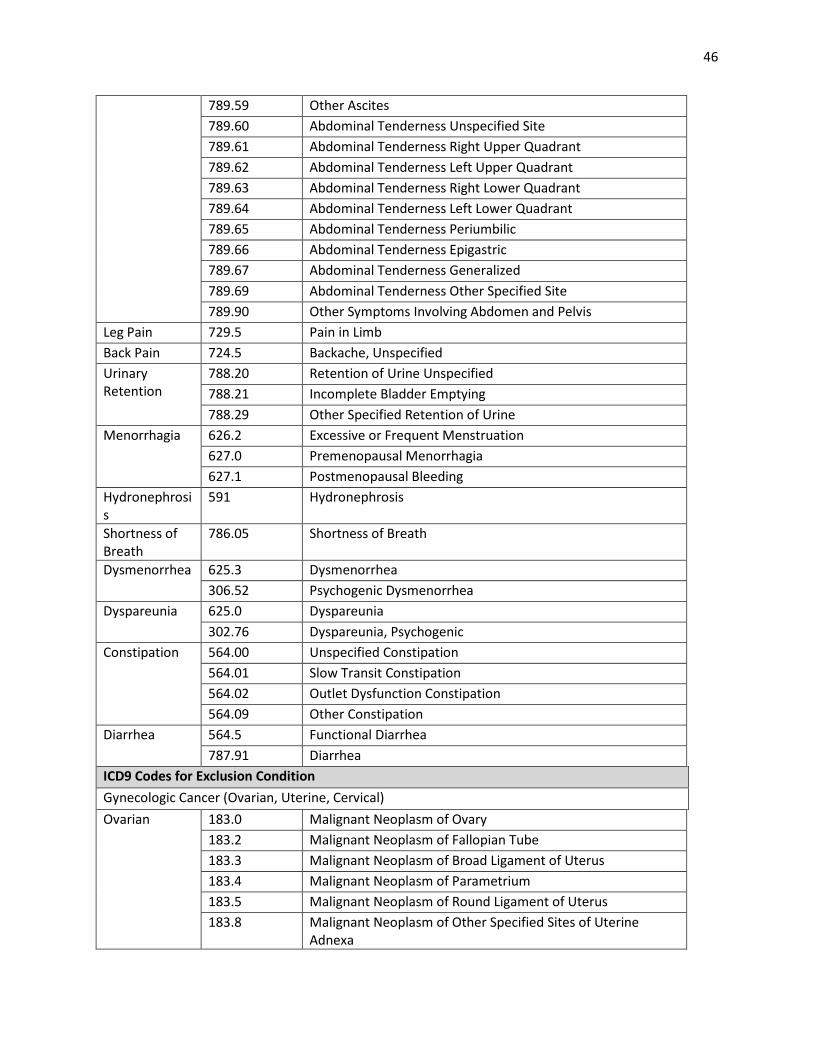
46
789.59 Other Ascites 789.60 Abdominal Tenderness Unspecified Site 789.61 Abdominal Tenderness Right Upper Quadrant 789.62 Abdominal Tenderness Left Upper Quadrant 789.63 Abdominal Tenderness Right Lower Quadrant 789.64 Abdominal Tenderness Left Lower Quadrant 789.65 Abdominal Tenderness Periumbilic 789.66 Abdominal Tenderness Epigastric 789.67 Abdominal Tenderness Generalized 789.69 Abdominal Tenderness Other Specified Site 789.90 Other Symptoms Involving Abdomen and Pelvis
Leg Pain 729.5 Pain in Limb Back Pain 724.5 Backache, Unspecified Urinary Retention
788.20 Retention of Urine Unspecified 788.21 Incomplete Bladder Emptying 788.29 Other Specified Retention of Urine
Menorrhagia 626.2 Excessive or Frequent Menstruation 627.0 Premenopausal Menorrhagia 627.1 Postmenopausal Bleeding
Hydronephrosis
591 Hydronephrosis
Shortness of Breath
786.05 Shortness of Breath
Dysmenorrhea 625.3 Dysmenorrhea 306.52 Psychogenic Dysmenorrhea
Dyspareunia 625.0 Dyspareunia 302.76 Dyspareunia, Psychogenic
Constipation 564.00 Unspecified Constipation 564.01 Slow Transit Constipation 564.02 Outlet Dysfunction Constipation 564.09 Other Constipation
Diarrhea 564.5 Functional Diarrhea 787.91 Diarrhea
ICD9 Codes for Exclusion Condition Gynecologic Cancer (Ovarian, Uterine, Cervical) Ovarian 183.0 Malignant Neoplasm of Ovary
183.2 Malignant Neoplasm of Fallopian Tube 183.3 Malignant Neoplasm of Broad Ligament of Uterus 183.4 Malignant Neoplasm of Parametrium 183.5 Malignant Neoplasm of Round Ligament of Uterus 183.8 Malignant Neoplasm of Other Specified Sites of Uterine
Adnexa
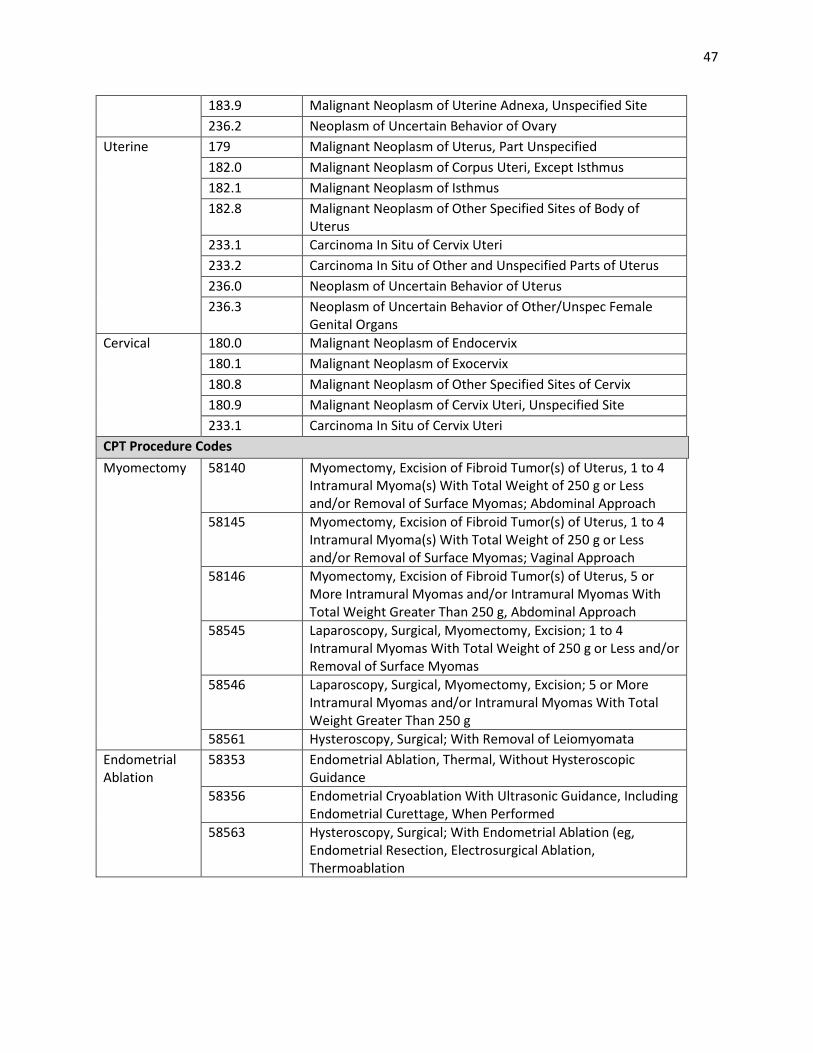
47
183.9 Malignant Neoplasm of Uterine Adnexa, Unspecified Site 236.2 Neoplasm of Uncertain Behavior of Ovary
Uterine 179 Malignant Neoplasm of Uterus, Part Unspecified 182.0 Malignant Neoplasm of Corpus Uteri, Except Isthmus 182.1 Malignant Neoplasm of Isthmus 182.8 Malignant Neoplasm of Other Specified Sites of Body of
Uterus 233.1 Carcinoma In Situ of Cervix Uteri 233.2 Carcinoma In Situ of Other and Unspecified Parts of Uterus 236.0 Neoplasm of Uncertain Behavior of Uterus 236.3 Neoplasm of Uncertain Behavior of Other/Unspec Female
Genital Organs Cervical 180.0 Malignant Neoplasm of Endocervix
180.1 Malignant Neoplasm of Exocervix 180.8 Malignant Neoplasm of Other Specified Sites of Cervix 180.9 Malignant Neoplasm of Cervix Uteri, Unspecified Site 233.1 Carcinoma In Situ of Cervix Uteri
CPT Procedure Codes Myomectomy 58140 Myomectomy, Excision of Fibroid Tumor(s) of Uterus, 1 to 4
Intramural Myoma(s) With Total Weight of 250 g or Less and/or Removal of Surface Myomas; Abdominal Approach
58145 Myomectomy, Excision of Fibroid Tumor(s) of Uterus, 1 to 4 Intramural Myoma(s) With Total Weight of 250 g or Less and/or Removal of Surface Myomas; Vaginal Approach
58146 Myomectomy, Excision of Fibroid Tumor(s) of Uterus, 5 or More Intramural Myomas and/or Intramural Myomas With Total Weight Greater Than 250 g, Abdominal Approach
58545 Laparoscopy, Surgical, Myomectomy, Excision; 1 to 4 Intramural Myomas With Total Weight of 250 g or Less and/or Removal of Surface Myomas
58546 Laparoscopy, Surgical, Myomectomy, Excision; 5 or More Intramural Myomas and/or Intramural Myomas With Total Weight Greater Than 250 g
58561 Hysteroscopy, Surgical; With Removal of Leiomyomata Endometrial Ablation
58353 Endometrial Ablation, Thermal, Without Hysteroscopic Guidance
58356 Endometrial Cryoablation With Ultrasonic Guidance, Including Endometrial Curettage, When Performed
58563 Hysteroscopy, Surgical; With Endometrial Ablation (eg, Endometrial Resection, Electrosurgical Ablation, Thermoablation
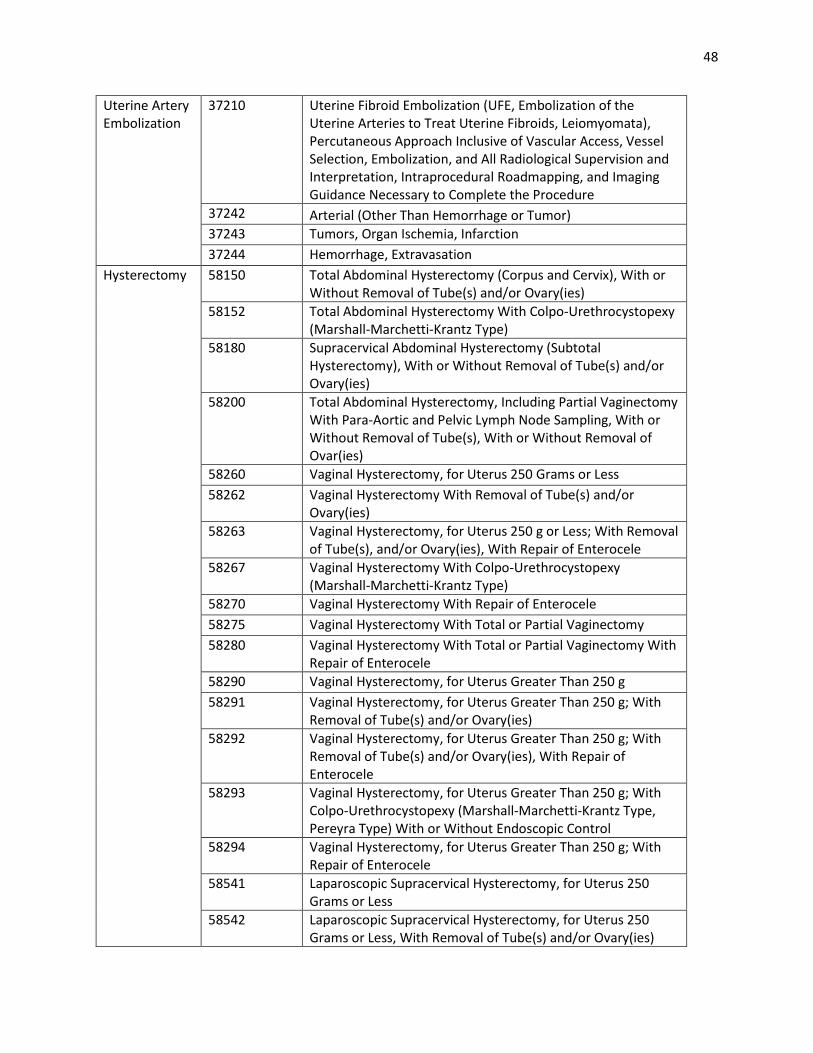
48
Uterine Artery Embolization
37210 Uterine Fibroid Embolization (UFE, Embolization of the Uterine Arteries to Treat Uterine Fibroids, Leiomyomata), Percutaneous Approach Inclusive of Vascular Access, Vessel Selection, Embolization, and All Radiological Supervision and Interpretation, Intraprocedural Roadmapping, and Imaging Guidance Necessary to Complete the Procedure
37242 Arterial (Other Than Hemorrhage or Tumor) 37243 Tumors, Organ Ischemia, Infarction 37244 Hemorrhage, Extravasation
Hysterectomy 58150 Total Abdominal Hysterectomy (Corpus and Cervix), With or Without Removal of Tube(s) and/or Ovary(ies)
58152 Total Abdominal Hysterectomy With Colpo-Urethrocystopexy (Marshall-Marchetti-Krantz Type)
58180 Supracervical Abdominal Hysterectomy (Subtotal Hysterectomy), With or Without Removal of Tube(s) and/or Ovary(ies)
58200 Total Abdominal Hysterectomy, Including Partial Vaginectomy With Para-Aortic and Pelvic Lymph Node Sampling, With or Without Removal of Tube(s), With or Without Removal of Ovar(ies)
58260 Vaginal Hysterectomy, for Uterus 250 Grams or Less 58262 Vaginal Hysterectomy With Removal of Tube(s) and/or
Ovary(ies) 58263 Vaginal Hysterectomy, for Uterus 250 g or Less; With Removal
of Tube(s), and/or Ovary(ies), With Repair of Enterocele 58267 Vaginal Hysterectomy With Colpo-Urethrocystopexy
(Marshall-Marchetti-Krantz Type) 58270 Vaginal Hysterectomy With Repair of Enterocele 58275 Vaginal Hysterectomy With Total or Partial Vaginectomy 58280 Vaginal Hysterectomy With Total or Partial Vaginectomy With
Repair of Enterocele 58290 Vaginal Hysterectomy, for Uterus Greater Than 250 g 58291 Vaginal Hysterectomy, for Uterus Greater Than 250 g; With
Removal of Tube(s) and/or Ovary(ies) 58292 Vaginal Hysterectomy, for Uterus Greater Than 250 g; With
Removal of Tube(s) and/or Ovary(ies), With Repair of Enterocele
58293 Vaginal Hysterectomy, for Uterus Greater Than 250 g; With Colpo-Urethrocystopexy (Marshall-Marchetti-Krantz Type, Pereyra Type) With or Without Endoscopic Control
58294 Vaginal Hysterectomy, for Uterus Greater Than 250 g; With Repair of Enterocele
58541 Laparoscopic Supracervical Hysterectomy, for Uterus 250 Grams or Less
58542 Laparoscopic Supracervical Hysterectomy, for Uterus 250 Grams or Less, With Removal of Tube(s) and/or Ovary(ies)
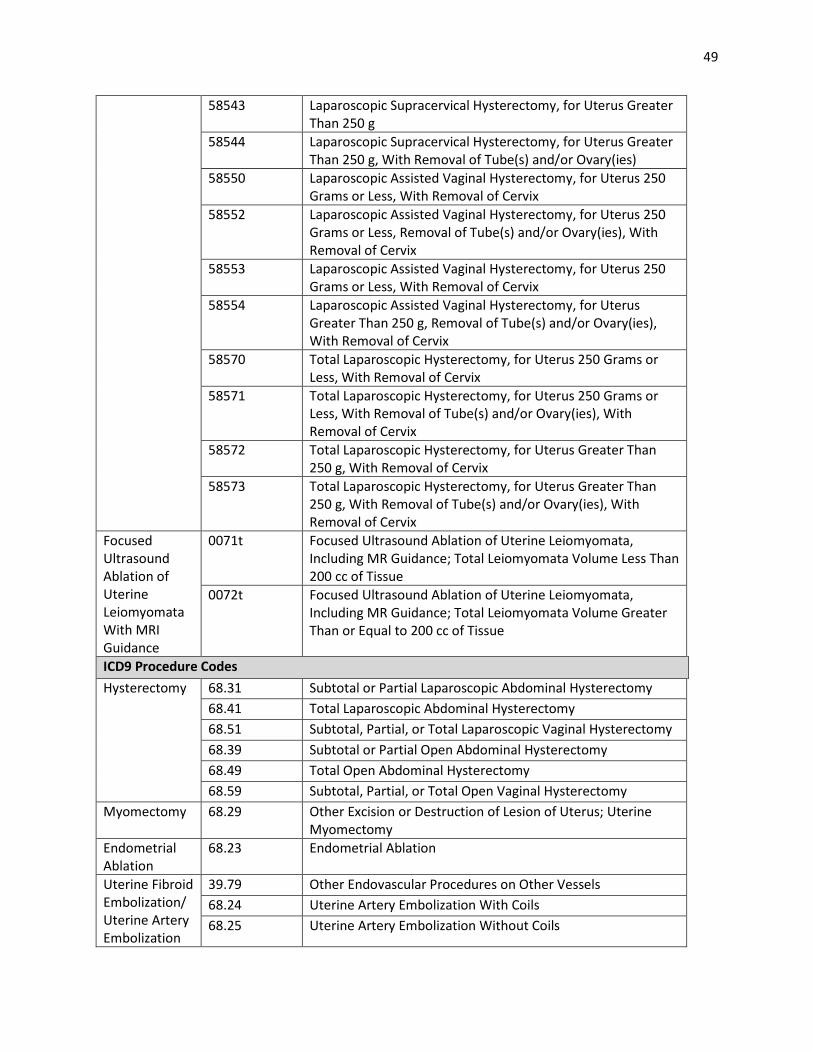
49
58543 Laparoscopic Supracervical Hysterectomy, for Uterus Greater Than 250 g
58544 Laparoscopic Supracervical Hysterectomy, for Uterus Greater Than 250 g, With Removal of Tube(s) and/or Ovary(ies)
58550 Laparoscopic Assisted Vaginal Hysterectomy, for Uterus 250 Grams or Less, With Removal of Cervix
58552 Laparoscopic Assisted Vaginal Hysterectomy, for Uterus 250 Grams or Less, Removal of Tube(s) and/or Ovary(ies), With Removal of Cervix
58553 Laparoscopic Assisted Vaginal Hysterectomy, for Uterus 250 Grams or Less, With Removal of Cervix
58554 Laparoscopic Assisted Vaginal Hysterectomy, for Uterus Greater Than 250 g, Removal of Tube(s) and/or Ovary(ies), With Removal of Cervix
58570 Total Laparoscopic Hysterectomy, for Uterus 250 Grams or Less, With Removal of Cervix
58571 Total Laparoscopic Hysterectomy, for Uterus 250 Grams or Less, With Removal of Tube(s) and/or Ovary(ies), With Removal of Cervix
58572 Total Laparoscopic Hysterectomy, for Uterus Greater Than 250 g, With Removal of Cervix
58573 Total Laparoscopic Hysterectomy, for Uterus Greater Than 250 g, With Removal of Tube(s) and/or Ovary(ies), With Removal of Cervix
Focused Ultrasound Ablation of Uterine Leiomyomata With MRI Guidance
0071t Focused Ultrasound Ablation of Uterine Leiomyomata, Including MR Guidance; Total Leiomyomata Volume Less Than 200 cc of Tissue
0072t Focused Ultrasound Ablation of Uterine Leiomyomata, Including MR Guidance; Total Leiomyomata Volume Greater Than or Equal to 200 cc of Tissue
ICD9 Procedure Codes Hysterectomy 68.31 Subtotal or Partial Laparoscopic Abdominal Hysterectomy
68.41 Total Laparoscopic Abdominal Hysterectomy 68.51 Subtotal, Partial, or Total Laparoscopic Vaginal Hysterectomy 68.39 Subtotal or Partial Open Abdominal Hysterectomy 68.49 Total Open Abdominal Hysterectomy 68.59 Subtotal, Partial, or Total Open Vaginal Hysterectomy
Myomectomy 68.29 Other Excision or Destruction of Lesion of Uterus; Uterine Myomectomy
Endometrial Ablation
68.23 Endometrial Ablation
Uterine Fibroid Embolization/ Uterine Artery Embolization
39.79 Other Endovascular Procedures on Other Vessels 68.24 Uterine Artery Embolization With Coils 68.25 Uterine Artery Embolization Without Coils
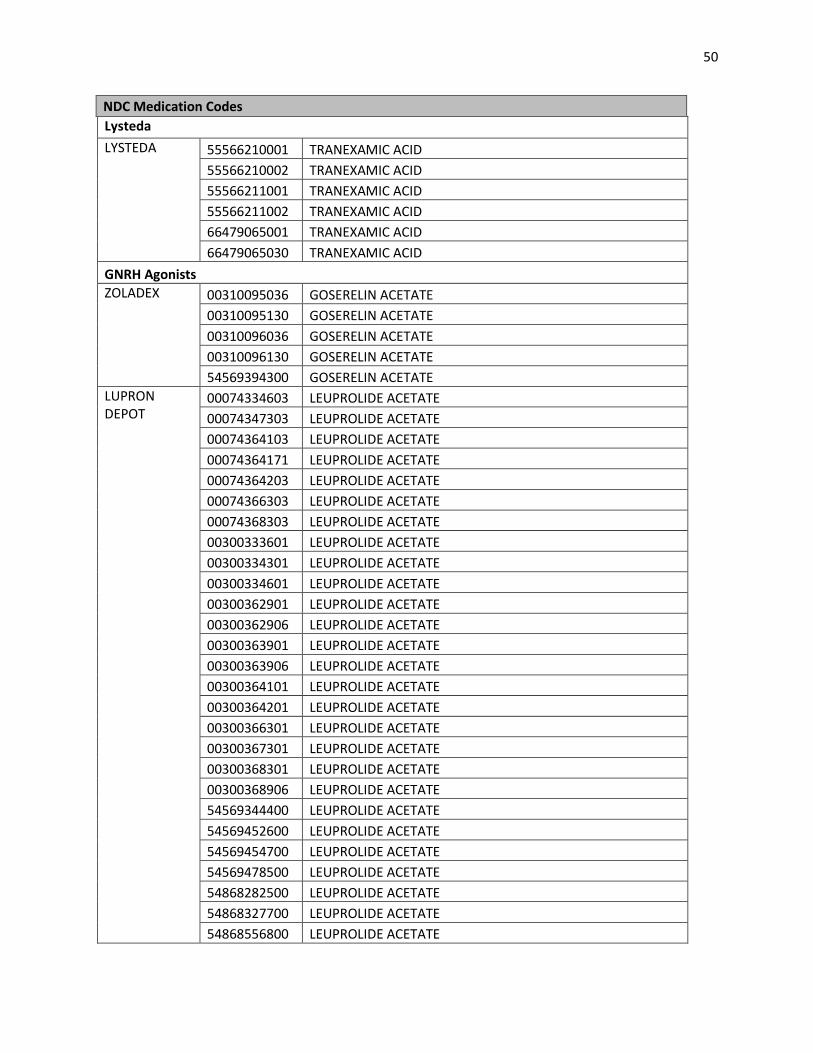
50
NDC Medication Codes Lysteda LYSTEDA 55566210001 TRANEXAMIC ACID
55566210002 TRANEXAMIC ACID 55566211001 TRANEXAMIC ACID 55566211002 TRANEXAMIC ACID 66479065001 TRANEXAMIC ACID 66479065030 TRANEXAMIC ACID
GNRH Agonists ZOLADEX 00310095036 GOSERELIN ACETATE
00310095130 GOSERELIN ACETATE 00310096036 GOSERELIN ACETATE 00310096130 GOSERELIN ACETATE 54569394300 GOSERELIN ACETATE
LUPRON DEPOT
00074334603 LEUPROLIDE ACETATE 00074347303 LEUPROLIDE ACETATE 00074364103 LEUPROLIDE ACETATE 00074364171 LEUPROLIDE ACETATE 00074364203 LEUPROLIDE ACETATE 00074366303 LEUPROLIDE ACETATE 00074368303 LEUPROLIDE ACETATE 00300333601 LEUPROLIDE ACETATE 00300334301 LEUPROLIDE ACETATE 00300334601 LEUPROLIDE ACETATE 00300362901 LEUPROLIDE ACETATE 00300362906 LEUPROLIDE ACETATE 00300363901 LEUPROLIDE ACETATE 00300363906 LEUPROLIDE ACETATE 00300364101 LEUPROLIDE ACETATE 00300364201 LEUPROLIDE ACETATE 00300366301 LEUPROLIDE ACETATE 00300367301 LEUPROLIDE ACETATE 00300368301 LEUPROLIDE ACETATE 00300368906 LEUPROLIDE ACETATE 54569344400 LEUPROLIDE ACETATE 54569452600 LEUPROLIDE ACETATE 54569454700 LEUPROLIDE ACETATE 54569478500 LEUPROLIDE ACETATE 54868282500 LEUPROLIDE ACETATE 54868327700 LEUPROLIDE ACETATE 54868556800 LEUPROLIDE ACETATE
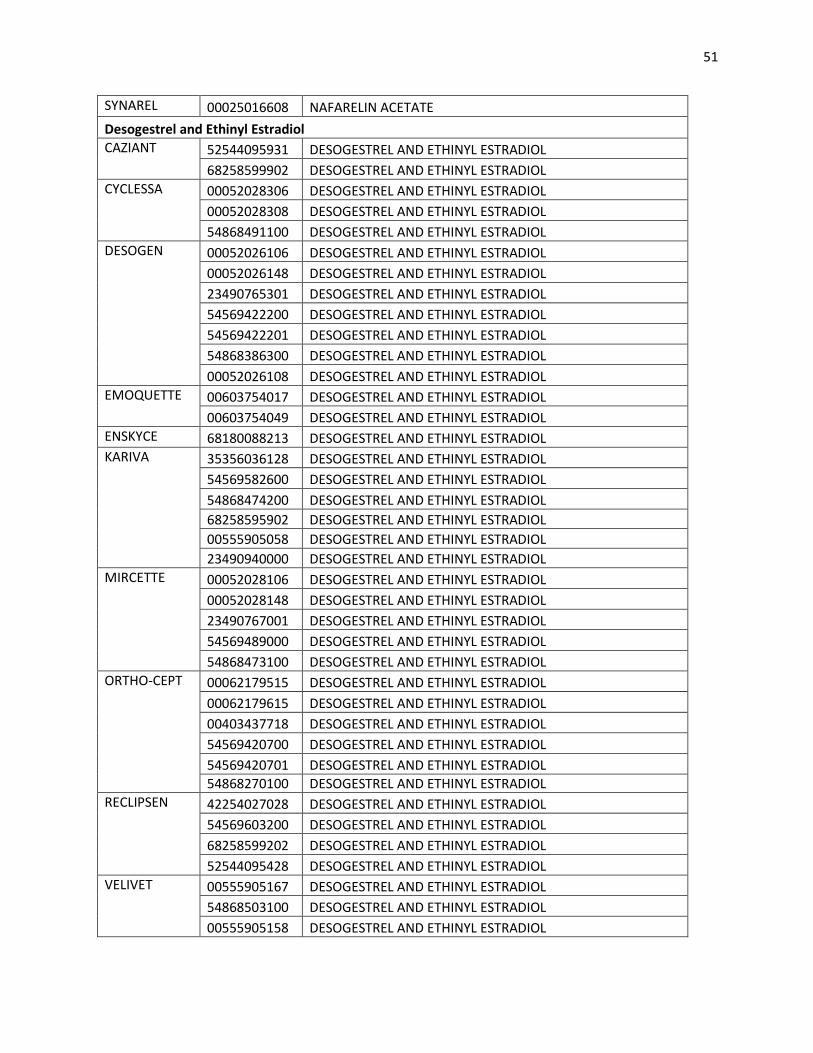
51
SYNAREL 00025016608 NAFARELIN ACETATE Desogestrel and Ethinyl Estradiol CAZIANT 52544095931 DESOGESTREL AND ETHINYL ESTRADIOL
68258599902 DESOGESTREL AND ETHINYL ESTRADIOL CYCLESSA 00052028306 DESOGESTREL AND ETHINYL ESTRADIOL
00052028308 DESOGESTREL AND ETHINYL ESTRADIOL 54868491100 DESOGESTREL AND ETHINYL ESTRADIOL
DESOGEN 00052026106 DESOGESTREL AND ETHINYL ESTRADIOL 00052026148 DESOGESTREL AND ETHINYL ESTRADIOL 23490765301 DESOGESTREL AND ETHINYL ESTRADIOL 54569422200 DESOGESTREL AND ETHINYL ESTRADIOL 54569422201 DESOGESTREL AND ETHINYL ESTRADIOL 54868386300 DESOGESTREL AND ETHINYL ESTRADIOL 00052026108 DESOGESTREL AND ETHINYL ESTRADIOL
EMOQUETTE 00603754017 DESOGESTREL AND ETHINYL ESTRADIOL 00603754049 DESOGESTREL AND ETHINYL ESTRADIOL
ENSKYCE 68180088213 DESOGESTREL AND ETHINYL ESTRADIOL KARIVA 35356036128 DESOGESTREL AND ETHINYL ESTRADIOL
54569582600 DESOGESTREL AND ETHINYL ESTRADIOL 54868474200 DESOGESTREL AND ETHINYL ESTRADIOL 68258595902 DESOGESTREL AND ETHINYL ESTRADIOL 00555905058 DESOGESTREL AND ETHINYL ESTRADIOL 23490940000 DESOGESTREL AND ETHINYL ESTRADIOL
MIRCETTE 00052028106 DESOGESTREL AND ETHINYL ESTRADIOL 00052028148 DESOGESTREL AND ETHINYL ESTRADIOL 23490767001 DESOGESTREL AND ETHINYL ESTRADIOL 54569489000 DESOGESTREL AND ETHINYL ESTRADIOL 54868473100 DESOGESTREL AND ETHINYL ESTRADIOL
ORTHO-CEPT 00062179515 DESOGESTREL AND ETHINYL ESTRADIOL 00062179615 DESOGESTREL AND ETHINYL ESTRADIOL 00403437718 DESOGESTREL AND ETHINYL ESTRADIOL 54569420700 DESOGESTREL AND ETHINYL ESTRADIOL 54569420701 DESOGESTREL AND ETHINYL ESTRADIOL 54868270100 DESOGESTREL AND ETHINYL ESTRADIOL
RECLIPSEN 42254027028 DESOGESTREL AND ETHINYL ESTRADIOL 54569603200 DESOGESTREL AND ETHINYL ESTRADIOL 68258599202 DESOGESTREL AND ETHINYL ESTRADIOL 52544095428 DESOGESTREL AND ETHINYL ESTRADIOL
VELIVET 00555905167 DESOGESTREL AND ETHINYL ESTRADIOL 54868503100 DESOGESTREL AND ETHINYL ESTRADIOL 00555905158 DESOGESTREL AND ETHINYL ESTRADIOL
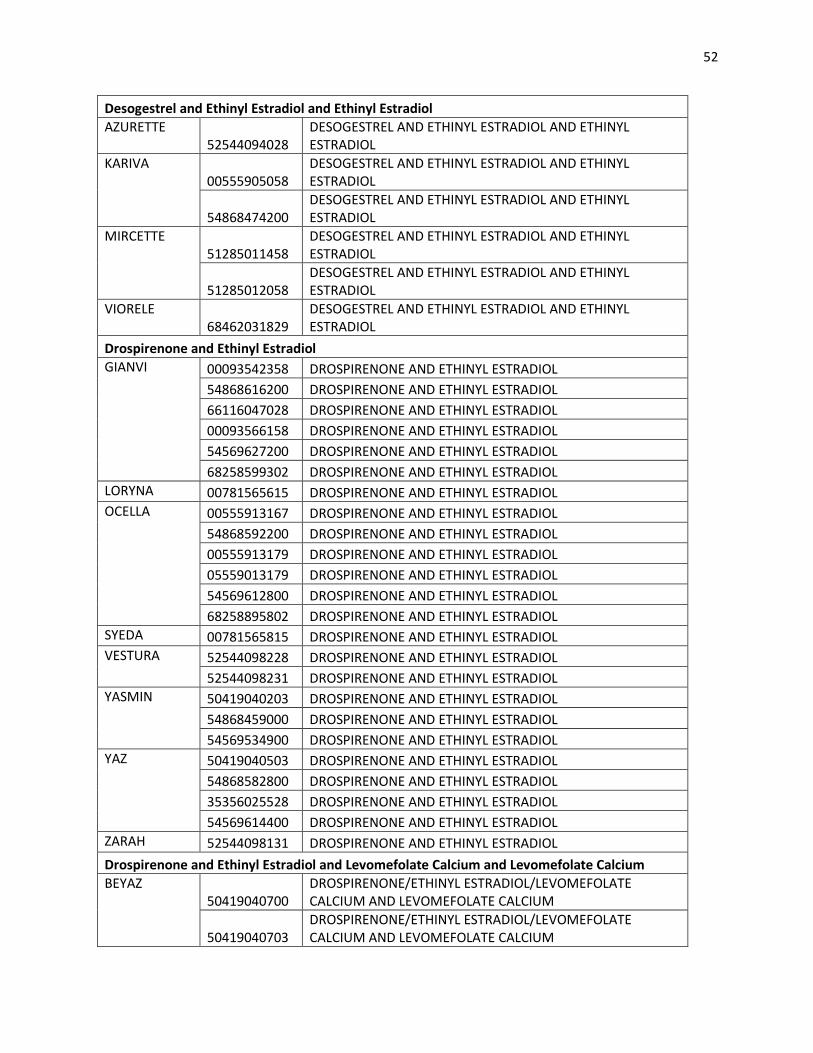
52
Desogestrel and Ethinyl Estradiol and Ethinyl Estradiol AZURETTE
52544094028 DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
KARIVA 00555905058
DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
54868474200 DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
MIRCETTE 51285011458
DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
51285012058 DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
VIORELE 68462031829
DESOGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
Drospirenone and Ethinyl Estradiol GIANVI 00093542358 DROSPIRENONE AND ETHINYL ESTRADIOL
54868616200 DROSPIRENONE AND ETHINYL ESTRADIOL 66116047028 DROSPIRENONE AND ETHINYL ESTRADIOL 00093566158 DROSPIRENONE AND ETHINYL ESTRADIOL 54569627200 DROSPIRENONE AND ETHINYL ESTRADIOL 68258599302 DROSPIRENONE AND ETHINYL ESTRADIOL
LORYNA 00781565615 DROSPIRENONE AND ETHINYL ESTRADIOL OCELLA 00555913167 DROSPIRENONE AND ETHINYL ESTRADIOL
54868592200 DROSPIRENONE AND ETHINYL ESTRADIOL 00555913179 DROSPIRENONE AND ETHINYL ESTRADIOL 05559013179 DROSPIRENONE AND ETHINYL ESTRADIOL 54569612800 DROSPIRENONE AND ETHINYL ESTRADIOL 68258895802 DROSPIRENONE AND ETHINYL ESTRADIOL
SYEDA 00781565815 DROSPIRENONE AND ETHINYL ESTRADIOL VESTURA 52544098228 DROSPIRENONE AND ETHINYL ESTRADIOL
52544098231 DROSPIRENONE AND ETHINYL ESTRADIOL YASMIN 50419040203 DROSPIRENONE AND ETHINYL ESTRADIOL
54868459000 DROSPIRENONE AND ETHINYL ESTRADIOL 54569534900 DROSPIRENONE AND ETHINYL ESTRADIOL
YAZ 50419040503 DROSPIRENONE AND ETHINYL ESTRADIOL 54868582800 DROSPIRENONE AND ETHINYL ESTRADIOL 35356025528 DROSPIRENONE AND ETHINYL ESTRADIOL 54569614400 DROSPIRENONE AND ETHINYL ESTRADIOL
ZARAH 52544098131 DROSPIRENONE AND ETHINYL ESTRADIOL Drospirenone and Ethinyl Estradiol and Levomefolate Calcium and Levomefolate Calcium BEYAZ
50419040700 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
50419040703 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
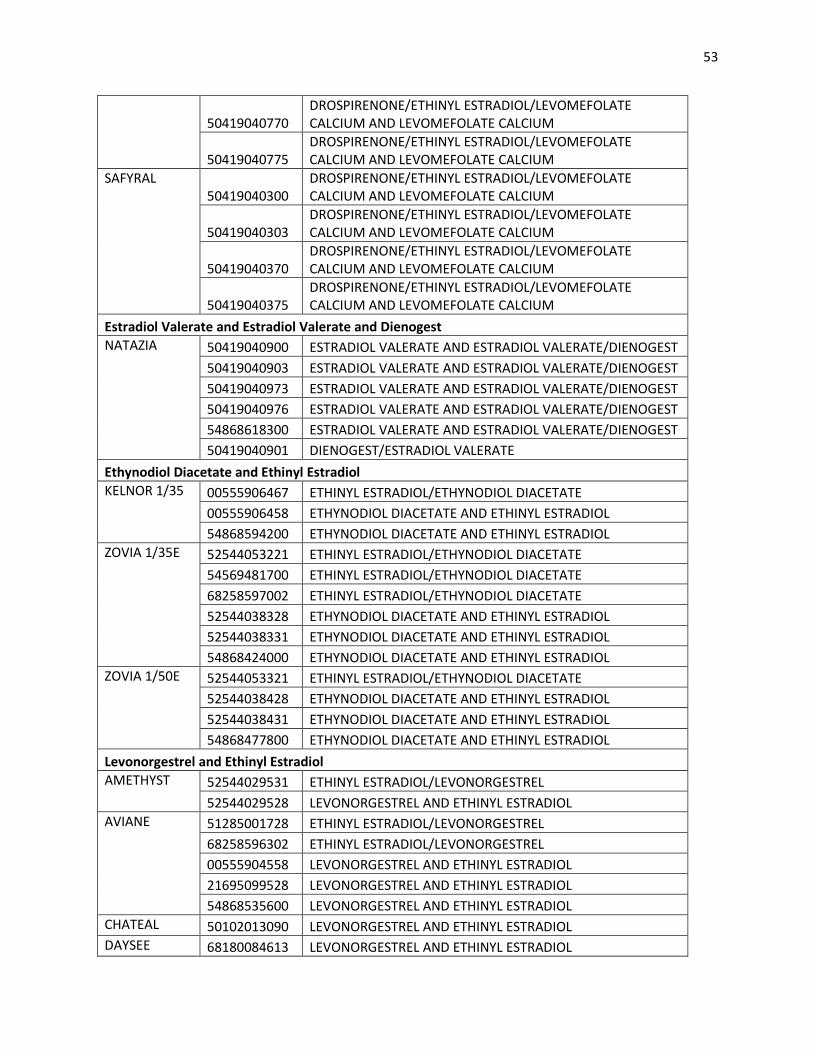
53
50419040770 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
50419040775 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
SAFYRAL 50419040300
DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
50419040303 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
50419040370 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
50419040375 DROSPIRENONE/ETHINYL ESTRADIOL/LEVOMEFOLATE CALCIUM AND LEVOMEFOLATE CALCIUM
Estradiol Valerate and Estradiol Valerate and Dienogest NATAZIA 50419040900 ESTRADIOL VALERATE AND ESTRADIOL VALERATE/DIENOGEST
50419040903 ESTRADIOL VALERATE AND ESTRADIOL VALERATE/DIENOGEST 50419040973 ESTRADIOL VALERATE AND ESTRADIOL VALERATE/DIENOGEST 50419040976 ESTRADIOL VALERATE AND ESTRADIOL VALERATE/DIENOGEST 54868618300 ESTRADIOL VALERATE AND ESTRADIOL VALERATE/DIENOGEST 50419040901 DIENOGEST/ESTRADIOL VALERATE
Ethynodiol Diacetate and Ethinyl Estradiol KELNOR 1/35 00555906467 ETHINYL ESTRADIOL/ETHYNODIOL DIACETATE
00555906458 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL 54868594200 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL
ZOVIA 1/35E 52544053221 ETHINYL ESTRADIOL/ETHYNODIOL DIACETATE 54569481700 ETHINYL ESTRADIOL/ETHYNODIOL DIACETATE 68258597002 ETHINYL ESTRADIOL/ETHYNODIOL DIACETATE 52544038328 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL 52544038331 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL 54868424000 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL
ZOVIA 1/50E 52544053321 ETHINYL ESTRADIOL/ETHYNODIOL DIACETATE 52544038428 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL 52544038431 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL 54868477800 ETHYNODIOL DIACETATE AND ETHINYL ESTRADIOL
Levonorgestrel and Ethinyl Estradiol AMETHYST 52544029531 ETHINYL ESTRADIOL/LEVONORGESTREL
52544029528 LEVONORGESTREL AND ETHINYL ESTRADIOL AVIANE 51285001728 ETHINYL ESTRADIOL/LEVONORGESTREL
68258596302 ETHINYL ESTRADIOL/LEVONORGESTREL 00555904558 LEVONORGESTREL AND ETHINYL ESTRADIOL 21695099528 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868535600 LEVONORGESTREL AND ETHINYL ESTRADIOL
CHATEAL 50102013090 LEVONORGESTREL AND ETHINYL ESTRADIOL DAYSEE 68180084613 LEVONORGESTREL AND ETHINYL ESTRADIOL
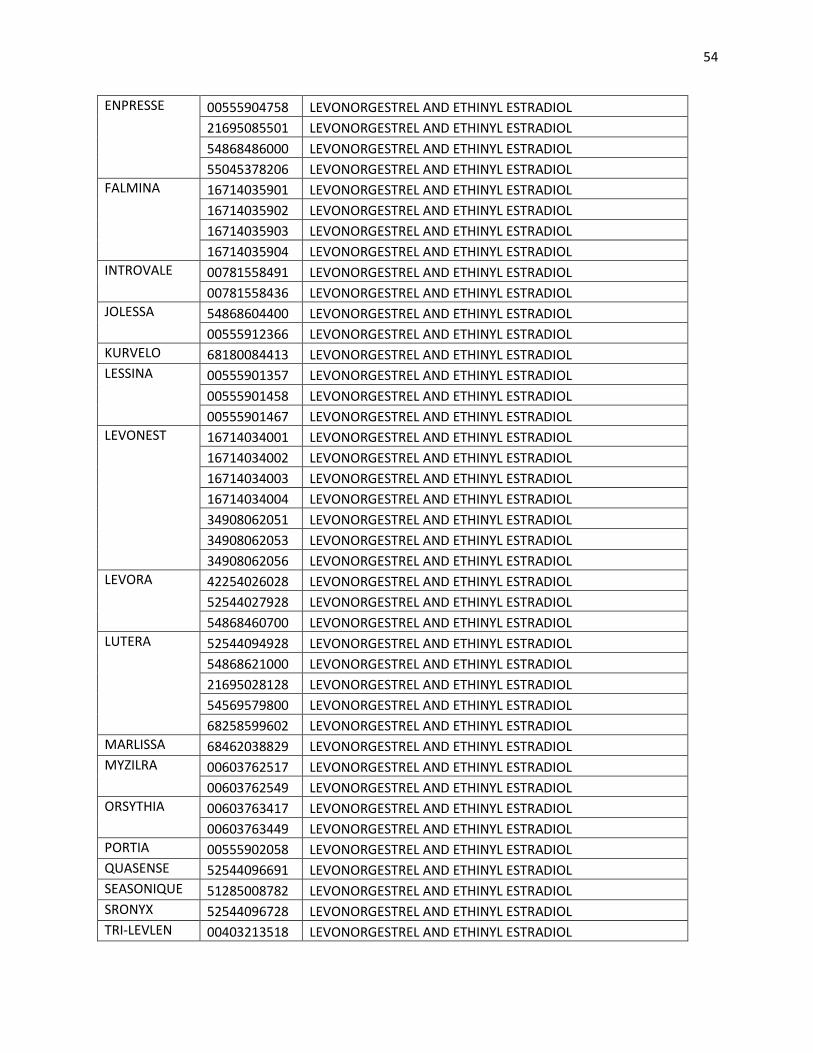
54
ENPRESSE 00555904758 LEVONORGESTREL AND ETHINYL ESTRADIOL 21695085501 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868486000 LEVONORGESTREL AND ETHINYL ESTRADIOL 55045378206 LEVONORGESTREL AND ETHINYL ESTRADIOL
FALMINA 16714035901 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714035902 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714035903 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714035904 LEVONORGESTREL AND ETHINYL ESTRADIOL
INTROVALE 00781558491 LEVONORGESTREL AND ETHINYL ESTRADIOL 00781558436 LEVONORGESTREL AND ETHINYL ESTRADIOL
JOLESSA 54868604400 LEVONORGESTREL AND ETHINYL ESTRADIOL 00555912366 LEVONORGESTREL AND ETHINYL ESTRADIOL
KURVELO 68180084413 LEVONORGESTREL AND ETHINYL ESTRADIOL LESSINA 00555901357 LEVONORGESTREL AND ETHINYL ESTRADIOL
00555901458 LEVONORGESTREL AND ETHINYL ESTRADIOL 00555901467 LEVONORGESTREL AND ETHINYL ESTRADIOL
LEVONEST 16714034001 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714034002 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714034003 LEVONORGESTREL AND ETHINYL ESTRADIOL 16714034004 LEVONORGESTREL AND ETHINYL ESTRADIOL 34908062051 LEVONORGESTREL AND ETHINYL ESTRADIOL 34908062053 LEVONORGESTREL AND ETHINYL ESTRADIOL 34908062056 LEVONORGESTREL AND ETHINYL ESTRADIOL
LEVORA 42254026028 LEVONORGESTREL AND ETHINYL ESTRADIOL 52544027928 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868460700 LEVONORGESTREL AND ETHINYL ESTRADIOL
LUTERA 52544094928 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868621000 LEVONORGESTREL AND ETHINYL ESTRADIOL 21695028128 LEVONORGESTREL AND ETHINYL ESTRADIOL 54569579800 LEVONORGESTREL AND ETHINYL ESTRADIOL 68258599602 LEVONORGESTREL AND ETHINYL ESTRADIOL
MARLISSA 68462038829 LEVONORGESTREL AND ETHINYL ESTRADIOL MYZILRA 00603762517 LEVONORGESTREL AND ETHINYL ESTRADIOL
00603762549 LEVONORGESTREL AND ETHINYL ESTRADIOL ORSYTHIA 00603763417 LEVONORGESTREL AND ETHINYL ESTRADIOL
00603763449 LEVONORGESTREL AND ETHINYL ESTRADIOL PORTIA 00555902058 LEVONORGESTREL AND ETHINYL ESTRADIOL QUASENSE 52544096691 LEVONORGESTREL AND ETHINYL ESTRADIOL SEASONIQUE 51285008782 LEVONORGESTREL AND ETHINYL ESTRADIOL SRONYX 52544096728 LEVONORGESTREL AND ETHINYL ESTRADIOL TRI-LEVLEN 00403213518 LEVONORGESTREL AND ETHINYL ESTRADIOL
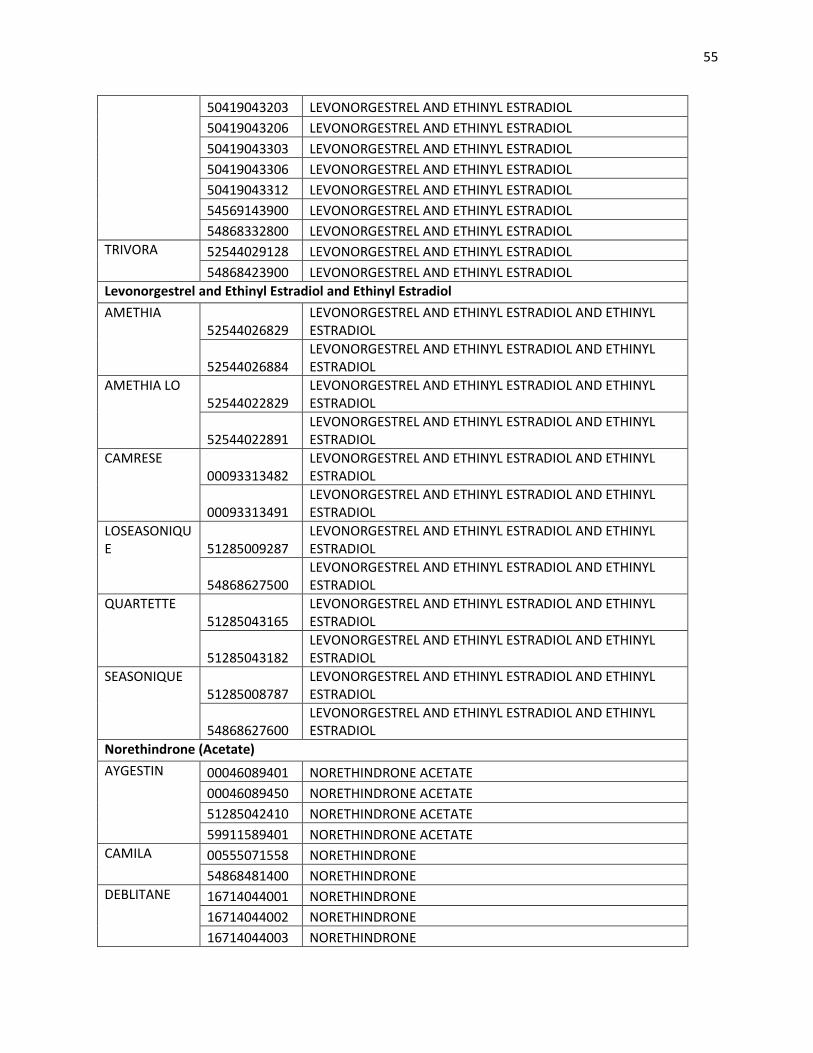
55
50419043203 LEVONORGESTREL AND ETHINYL ESTRADIOL 50419043206 LEVONORGESTREL AND ETHINYL ESTRADIOL 50419043303 LEVONORGESTREL AND ETHINYL ESTRADIOL 50419043306 LEVONORGESTREL AND ETHINYL ESTRADIOL 50419043312 LEVONORGESTREL AND ETHINYL ESTRADIOL 54569143900 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868332800 LEVONORGESTREL AND ETHINYL ESTRADIOL
TRIVORA 52544029128 LEVONORGESTREL AND ETHINYL ESTRADIOL 54868423900 LEVONORGESTREL AND ETHINYL ESTRADIOL
Levonorgestrel and Ethinyl Estradiol and Ethinyl Estradiol AMETHIA
52544026829 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
52544026884 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
AMETHIA LO 52544022829
LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
52544022891 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
CAMRESE 00093313482
LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
00093313491 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
LOSEASONIQUE 51285009287
LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
54868627500 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
QUARTETTE 51285043165
LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
51285043182 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
SEASONIQUE 51285008787
LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
54868627600 LEVONORGESTREL AND ETHINYL ESTRADIOL AND ETHINYL ESTRADIOL
Norethindrone (Acetate) AYGESTIN 00046089401 NORETHINDRONE ACETATE
00046089450 NORETHINDRONE ACETATE 51285042410 NORETHINDRONE ACETATE 59911589401 NORETHINDRONE ACETATE
CAMILA 00555071558 NORETHINDRONE 54868481400 NORETHINDRONE
DEBLITANE 16714044001 NORETHINDRONE 16714044002 NORETHINDRONE 16714044003 NORETHINDRONE
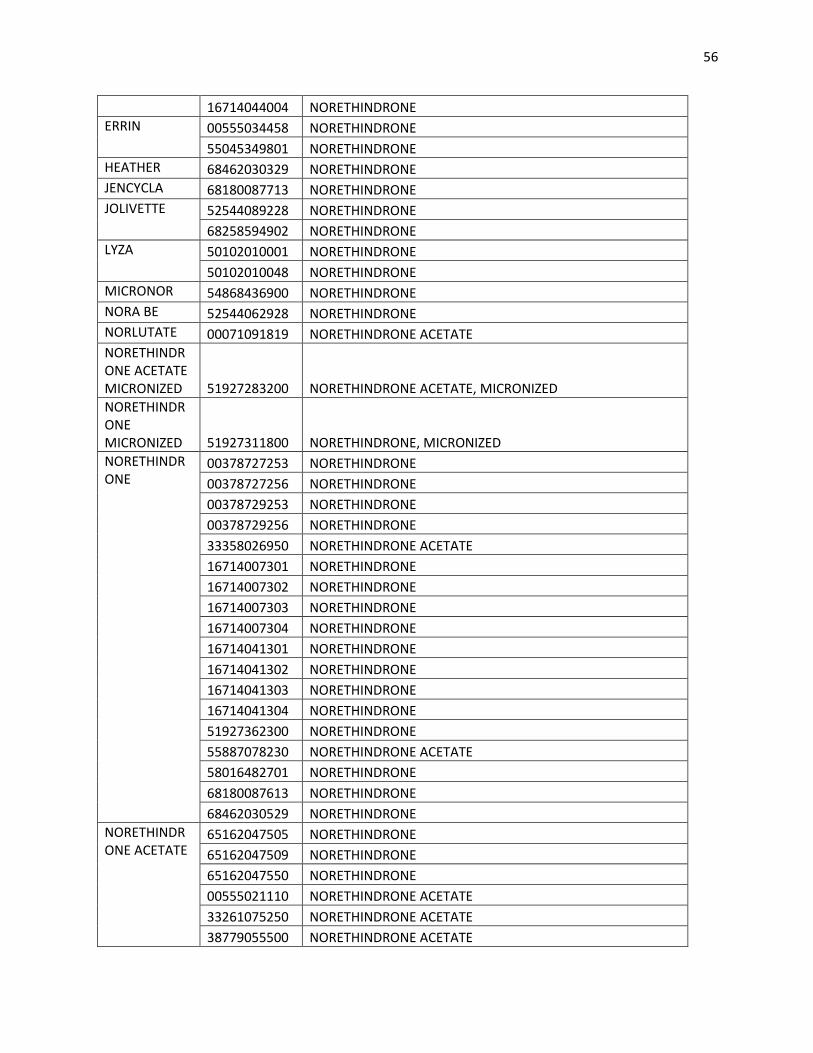
56
16714044004 NORETHINDRONE ERRIN 00555034458 NORETHINDRONE
55045349801 NORETHINDRONE HEATHER 68462030329 NORETHINDRONE JENCYCLA 68180087713 NORETHINDRONE JOLIVETTE 52544089228 NORETHINDRONE
68258594902 NORETHINDRONE LYZA 50102010001 NORETHINDRONE
50102010048 NORETHINDRONE MICRONOR 54868436900 NORETHINDRONE NORA BE 52544062928 NORETHINDRONE NORLUTATE 00071091819 NORETHINDRONE ACETATE NORETHINDRONE ACETATE MICRONIZED 51927283200 NORETHINDRONE ACETATE, MICRONIZED NORETHINDRONE MICRONIZED 51927311800 NORETHINDRONE, MICRONIZED NORETHINDRONE
00378727253 NORETHINDRONE 00378727256 NORETHINDRONE 00378729253 NORETHINDRONE 00378729256 NORETHINDRONE 33358026950 NORETHINDRONE ACETATE 16714007301 NORETHINDRONE 16714007302 NORETHINDRONE 16714007303 NORETHINDRONE 16714007304 NORETHINDRONE 16714041301 NORETHINDRONE 16714041302 NORETHINDRONE 16714041303 NORETHINDRONE 16714041304 NORETHINDRONE 51927362300 NORETHINDRONE 55887078230 NORETHINDRONE ACETATE 58016482701 NORETHINDRONE 68180087613 NORETHINDRONE 68462030529 NORETHINDRONE
NORETHINDRONE ACETATE
65162047505 NORETHINDRONE 65162047509 NORETHINDRONE 65162047550 NORETHINDRONE 00555021110 NORETHINDRONE ACETATE 33261075250 NORETHINDRONE ACETATE 38779055500 NORETHINDRONE ACETATE
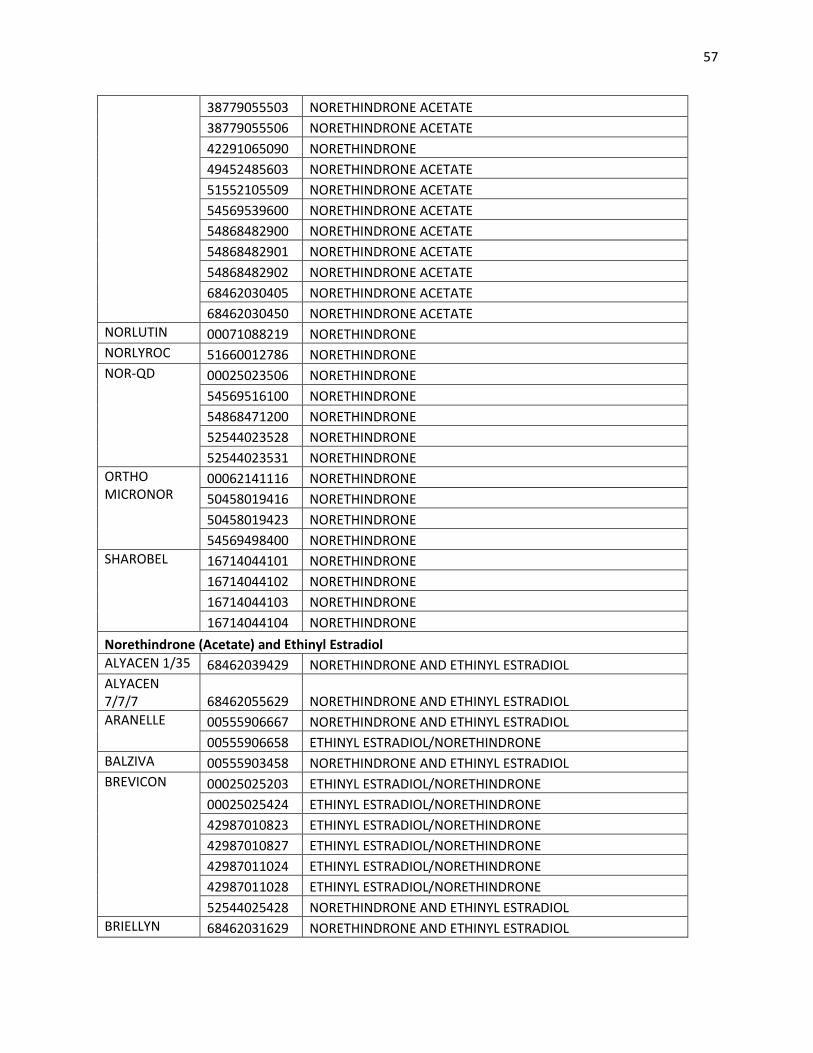
57
38779055503 NORETHINDRONE ACETATE 38779055506 NORETHINDRONE ACETATE 42291065090 NORETHINDRONE 49452485603 NORETHINDRONE ACETATE 51552105509 NORETHINDRONE ACETATE 54569539600 NORETHINDRONE ACETATE 54868482900 NORETHINDRONE ACETATE 54868482901 NORETHINDRONE ACETATE 54868482902 NORETHINDRONE ACETATE 68462030405 NORETHINDRONE ACETATE 68462030450 NORETHINDRONE ACETATE
NORLUTIN 00071088219 NORETHINDRONE NORLYROC 51660012786 NORETHINDRONE NOR-QD 00025023506 NORETHINDRONE
54569516100 NORETHINDRONE 54868471200 NORETHINDRONE 52544023528 NORETHINDRONE 52544023531 NORETHINDRONE
ORTHO MICRONOR
00062141116 NORETHINDRONE 50458019416 NORETHINDRONE 50458019423 NORETHINDRONE 54569498400 NORETHINDRONE
SHAROBEL 16714044101 NORETHINDRONE 16714044102 NORETHINDRONE 16714044103 NORETHINDRONE 16714044104 NORETHINDRONE
Norethindrone (Acetate) and Ethinyl Estradiol ALYACEN 1/35 68462039429 NORETHINDRONE AND ETHINYL ESTRADIOL ALYACEN 7/7/7 68462055629 NORETHINDRONE AND ETHINYL ESTRADIOL ARANELLE 00555906667 NORETHINDRONE AND ETHINYL ESTRADIOL
00555906658 ETHINYL ESTRADIOL/NORETHINDRONE BALZIVA 00555903458 NORETHINDRONE AND ETHINYL ESTRADIOL BREVICON 00025025203 ETHINYL ESTRADIOL/NORETHINDRONE
00025025424 ETHINYL ESTRADIOL/NORETHINDRONE 42987010823 ETHINYL ESTRADIOL/NORETHINDRONE 42987010827 ETHINYL ESTRADIOL/NORETHINDRONE 42987011024 ETHINYL ESTRADIOL/NORETHINDRONE 42987011028 ETHINYL ESTRADIOL/NORETHINDRONE 52544025428 NORETHINDRONE AND ETHINYL ESTRADIOL
BRIELLYN 68462031629 NORETHINDRONE AND ETHINYL ESTRADIOL
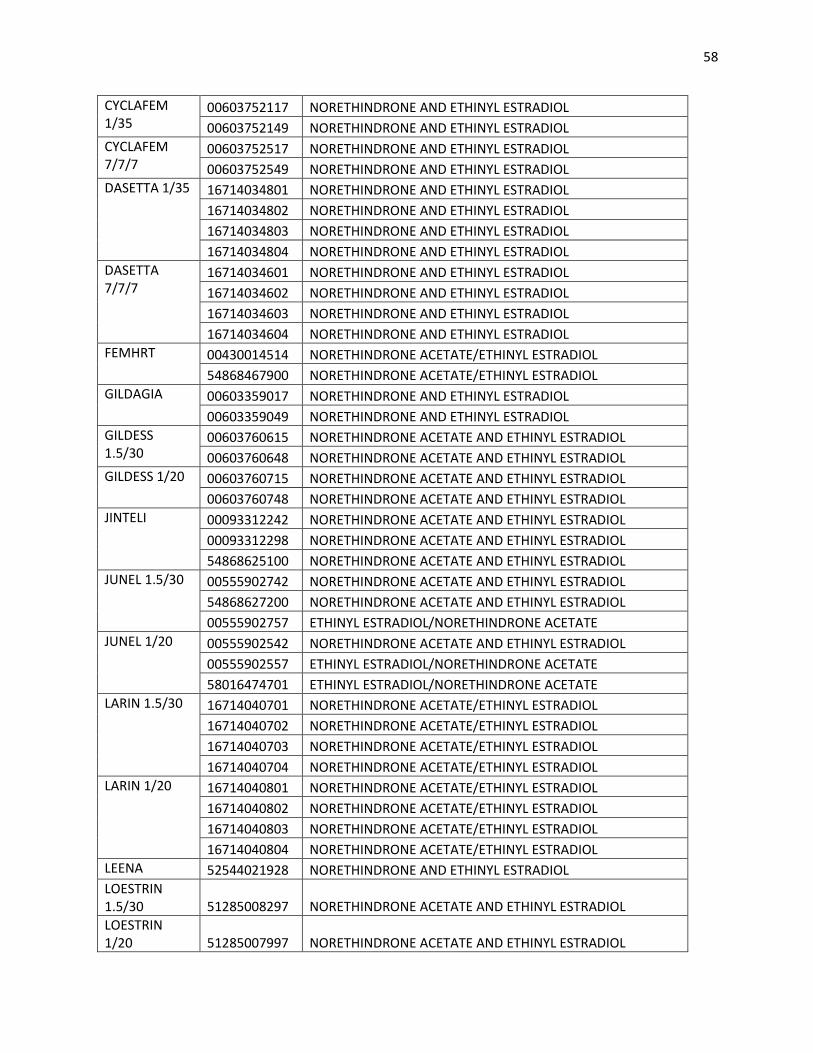
58
CYCLAFEM 1/35
00603752117 NORETHINDRONE AND ETHINYL ESTRADIOL 00603752149 NORETHINDRONE AND ETHINYL ESTRADIOL
CYCLAFEM 7/7/7
00603752517 NORETHINDRONE AND ETHINYL ESTRADIOL 00603752549 NORETHINDRONE AND ETHINYL ESTRADIOL
DASETTA 1/35 16714034801 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034802 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034803 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034804 NORETHINDRONE AND ETHINYL ESTRADIOL
DASETTA 7/7/7
16714034601 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034602 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034603 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034604 NORETHINDRONE AND ETHINYL ESTRADIOL
FEMHRT 00430014514 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 54868467900 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL
GILDAGIA 00603359017 NORETHINDRONE AND ETHINYL ESTRADIOL 00603359049 NORETHINDRONE AND ETHINYL ESTRADIOL
GILDESS 1.5/30
00603760615 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00603760648 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
GILDESS 1/20 00603760715 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00603760748 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
JINTELI 00093312242 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00093312298 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 54868625100 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
JUNEL 1.5/30 00555902742 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 54868627200 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00555902757 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE
JUNEL 1/20 00555902542 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00555902557 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE 58016474701 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE
LARIN 1.5/30 16714040701 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040702 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040703 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040704 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL
LARIN 1/20 16714040801 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040802 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040803 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 16714040804 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL
LEENA 52544021928 NORETHINDRONE AND ETHINYL ESTRADIOL LOESTRIN 1.5/30 51285008297 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL LOESTRIN 1/20 51285007997 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
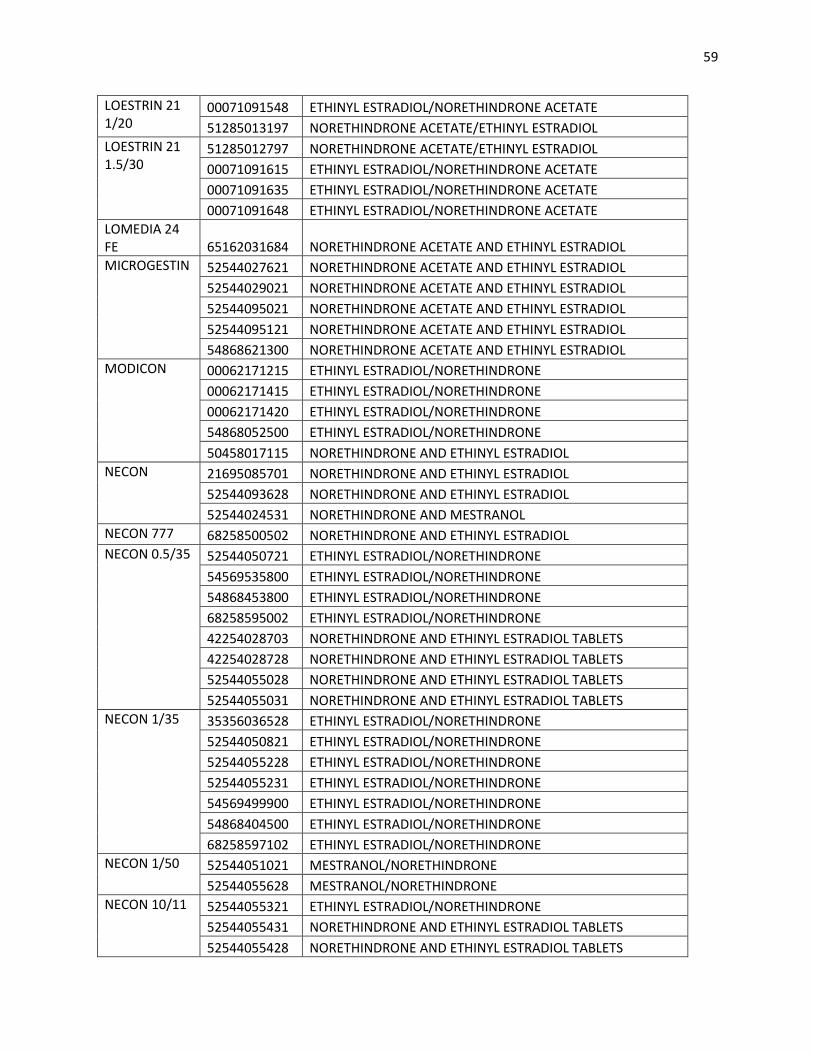
59
LOESTRIN 21 1/20
00071091548 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE 51285013197 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL
LOESTRIN 21 1.5/30
51285012797 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL 00071091615 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE 00071091635 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE 00071091648 ETHINYL ESTRADIOL/NORETHINDRONE ACETATE
LOMEDIA 24 FE 65162031684 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL MICROGESTIN 52544027621 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
52544029021 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 52544095021 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 52544095121 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 54868621300 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
MODICON 00062171215 ETHINYL ESTRADIOL/NORETHINDRONE 00062171415 ETHINYL ESTRADIOL/NORETHINDRONE 00062171420 ETHINYL ESTRADIOL/NORETHINDRONE 54868052500 ETHINYL ESTRADIOL/NORETHINDRONE 50458017115 NORETHINDRONE AND ETHINYL ESTRADIOL
NECON 21695085701 NORETHINDRONE AND ETHINYL ESTRADIOL 52544093628 NORETHINDRONE AND ETHINYL ESTRADIOL 52544024531 NORETHINDRONE AND MESTRANOL
NECON 777 68258500502 NORETHINDRONE AND ETHINYL ESTRADIOL NECON 0.5/35 52544050721 ETHINYL ESTRADIOL/NORETHINDRONE
54569535800 ETHINYL ESTRADIOL/NORETHINDRONE 54868453800 ETHINYL ESTRADIOL/NORETHINDRONE 68258595002 ETHINYL ESTRADIOL/NORETHINDRONE 42254028703 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS 42254028728 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS 52544055028 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS 52544055031 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS
NECON 1/35 35356036528 ETHINYL ESTRADIOL/NORETHINDRONE 52544050821 ETHINYL ESTRADIOL/NORETHINDRONE 52544055228 ETHINYL ESTRADIOL/NORETHINDRONE 52544055231 ETHINYL ESTRADIOL/NORETHINDRONE 54569499900 ETHINYL ESTRADIOL/NORETHINDRONE 54868404500 ETHINYL ESTRADIOL/NORETHINDRONE 68258597102 ETHINYL ESTRADIOL/NORETHINDRONE
NECON 1/50 52544051021 MESTRANOL/NORETHINDRONE 52544055628 MESTRANOL/NORETHINDRONE
NECON 10/11 52544055321 ETHINYL ESTRADIOL/NORETHINDRONE 52544055431 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS 52544055428 NORETHINDRONE AND ETHINYL ESTRADIOL TABLETS
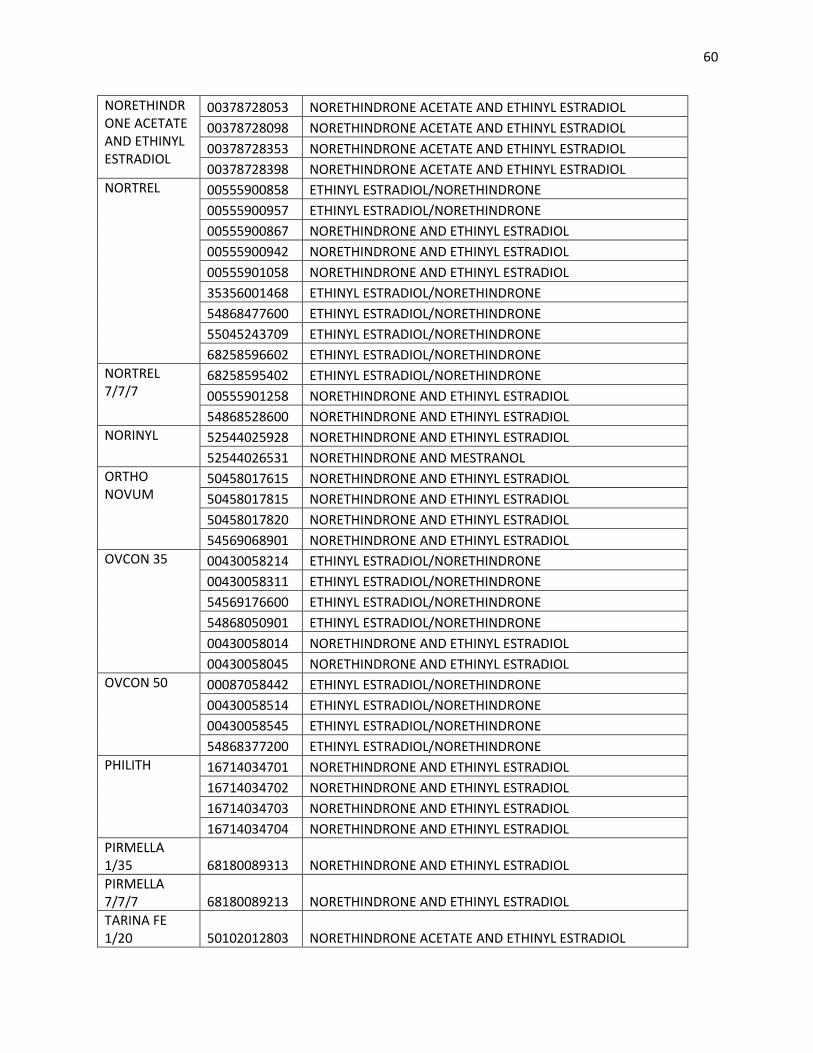
60
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
00378728053 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00378728098 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00378728353 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 00378728398 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
NORTREL 00555900858 ETHINYL ESTRADIOL/NORETHINDRONE 00555900957 ETHINYL ESTRADIOL/NORETHINDRONE 00555900867 NORETHINDRONE AND ETHINYL ESTRADIOL 00555900942 NORETHINDRONE AND ETHINYL ESTRADIOL 00555901058 NORETHINDRONE AND ETHINYL ESTRADIOL 35356001468 ETHINYL ESTRADIOL/NORETHINDRONE 54868477600 ETHINYL ESTRADIOL/NORETHINDRONE 55045243709 ETHINYL ESTRADIOL/NORETHINDRONE 68258596602 ETHINYL ESTRADIOL/NORETHINDRONE
NORTREL 7/7/7
68258595402 ETHINYL ESTRADIOL/NORETHINDRONE 00555901258 NORETHINDRONE AND ETHINYL ESTRADIOL 54868528600 NORETHINDRONE AND ETHINYL ESTRADIOL
NORINYL 52544025928 NORETHINDRONE AND ETHINYL ESTRADIOL 52544026531 NORETHINDRONE AND MESTRANOL
ORTHO NOVUM
50458017615 NORETHINDRONE AND ETHINYL ESTRADIOL 50458017815 NORETHINDRONE AND ETHINYL ESTRADIOL 50458017820 NORETHINDRONE AND ETHINYL ESTRADIOL 54569068901 NORETHINDRONE AND ETHINYL ESTRADIOL
OVCON 35 00430058214 ETHINYL ESTRADIOL/NORETHINDRONE 00430058311 ETHINYL ESTRADIOL/NORETHINDRONE 54569176600 ETHINYL ESTRADIOL/NORETHINDRONE 54868050901 ETHINYL ESTRADIOL/NORETHINDRONE 00430058014 NORETHINDRONE AND ETHINYL ESTRADIOL 00430058045 NORETHINDRONE AND ETHINYL ESTRADIOL
OVCON 50 00087058442 ETHINYL ESTRADIOL/NORETHINDRONE 00430058514 ETHINYL ESTRADIOL/NORETHINDRONE 00430058545 ETHINYL ESTRADIOL/NORETHINDRONE 54868377200 ETHINYL ESTRADIOL/NORETHINDRONE
PHILITH 16714034701 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034702 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034703 NORETHINDRONE AND ETHINYL ESTRADIOL 16714034704 NORETHINDRONE AND ETHINYL ESTRADIOL
PIRMELLA 1/35 68180089313 NORETHINDRONE AND ETHINYL ESTRADIOL PIRMELLA 7/7/7 68180089213 NORETHINDRONE AND ETHINYL ESTRADIOL TARINA FE 1/20 50102012803 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
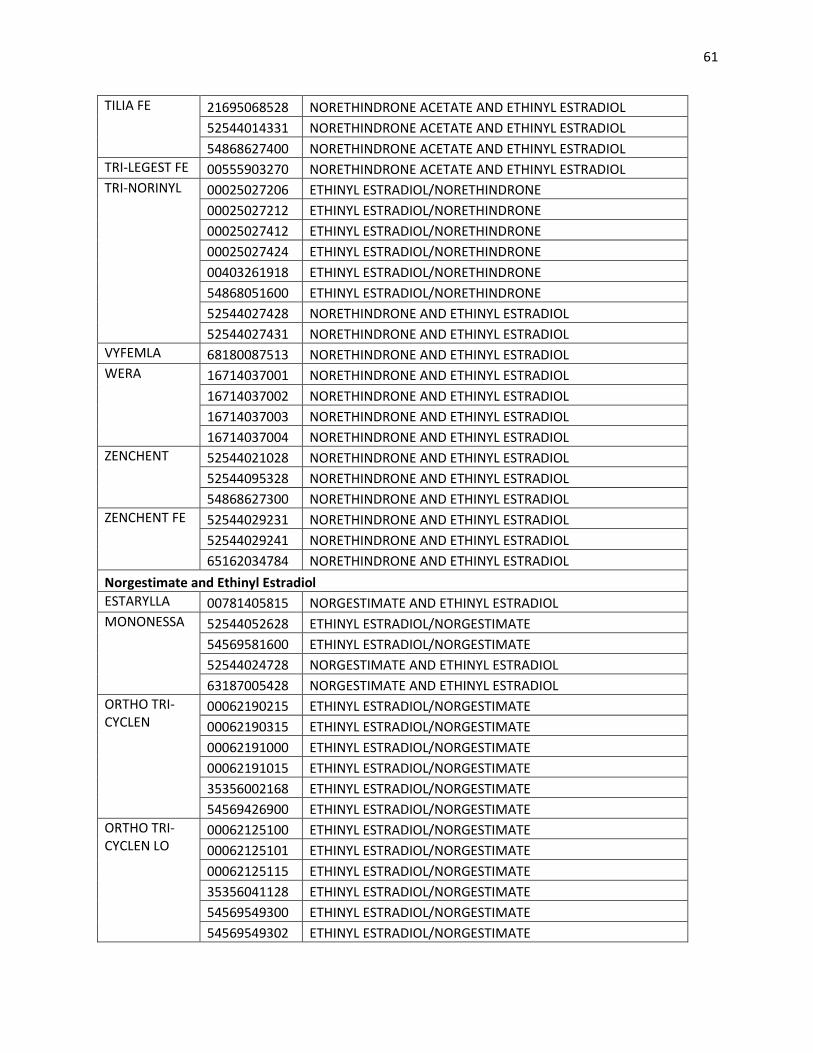
61
TILIA FE 21695068528 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 52544014331 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL 54868627400 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL
TRI-LEGEST FE 00555903270 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL TRI-NORINYL 00025027206 ETHINYL ESTRADIOL/NORETHINDRONE
00025027212 ETHINYL ESTRADIOL/NORETHINDRONE 00025027412 ETHINYL ESTRADIOL/NORETHINDRONE 00025027424 ETHINYL ESTRADIOL/NORETHINDRONE 00403261918 ETHINYL ESTRADIOL/NORETHINDRONE 54868051600 ETHINYL ESTRADIOL/NORETHINDRONE 52544027428 NORETHINDRONE AND ETHINYL ESTRADIOL 52544027431 NORETHINDRONE AND ETHINYL ESTRADIOL
VYFEMLA 68180087513 NORETHINDRONE AND ETHINYL ESTRADIOL WERA 16714037001 NORETHINDRONE AND ETHINYL ESTRADIOL
16714037002 NORETHINDRONE AND ETHINYL ESTRADIOL 16714037003 NORETHINDRONE AND ETHINYL ESTRADIOL 16714037004 NORETHINDRONE AND ETHINYL ESTRADIOL
ZENCHENT 52544021028 NORETHINDRONE AND ETHINYL ESTRADIOL 52544095328 NORETHINDRONE AND ETHINYL ESTRADIOL 54868627300 NORETHINDRONE AND ETHINYL ESTRADIOL
ZENCHENT FE 52544029231 NORETHINDRONE AND ETHINYL ESTRADIOL 52544029241 NORETHINDRONE AND ETHINYL ESTRADIOL 65162034784 NORETHINDRONE AND ETHINYL ESTRADIOL
Norgestimate and Ethinyl Estradiol ESTARYLLA 00781405815 NORGESTIMATE AND ETHINYL ESTRADIOL MONONESSA 52544052628 ETHINYL ESTRADIOL/NORGESTIMATE
54569581600 ETHINYL ESTRADIOL/NORGESTIMATE 52544024728 NORGESTIMATE AND ETHINYL ESTRADIOL 63187005428 NORGESTIMATE AND ETHINYL ESTRADIOL
ORTHO TRI-CYCLEN
00062190215 ETHINYL ESTRADIOL/NORGESTIMATE 00062190315 ETHINYL ESTRADIOL/NORGESTIMATE 00062191000 ETHINYL ESTRADIOL/NORGESTIMATE 00062191015 ETHINYL ESTRADIOL/NORGESTIMATE 35356002168 ETHINYL ESTRADIOL/NORGESTIMATE 54569426900 ETHINYL ESTRADIOL/NORGESTIMATE
ORTHO TRI-CYCLEN LO
00062125100 ETHINYL ESTRADIOL/NORGESTIMATE 00062125101 ETHINYL ESTRADIOL/NORGESTIMATE 00062125115 ETHINYL ESTRADIOL/NORGESTIMATE 35356041128 ETHINYL ESTRADIOL/NORGESTIMATE 54569549300 ETHINYL ESTRADIOL/NORGESTIMATE 54569549302 ETHINYL ESTRADIOL/NORGESTIMATE
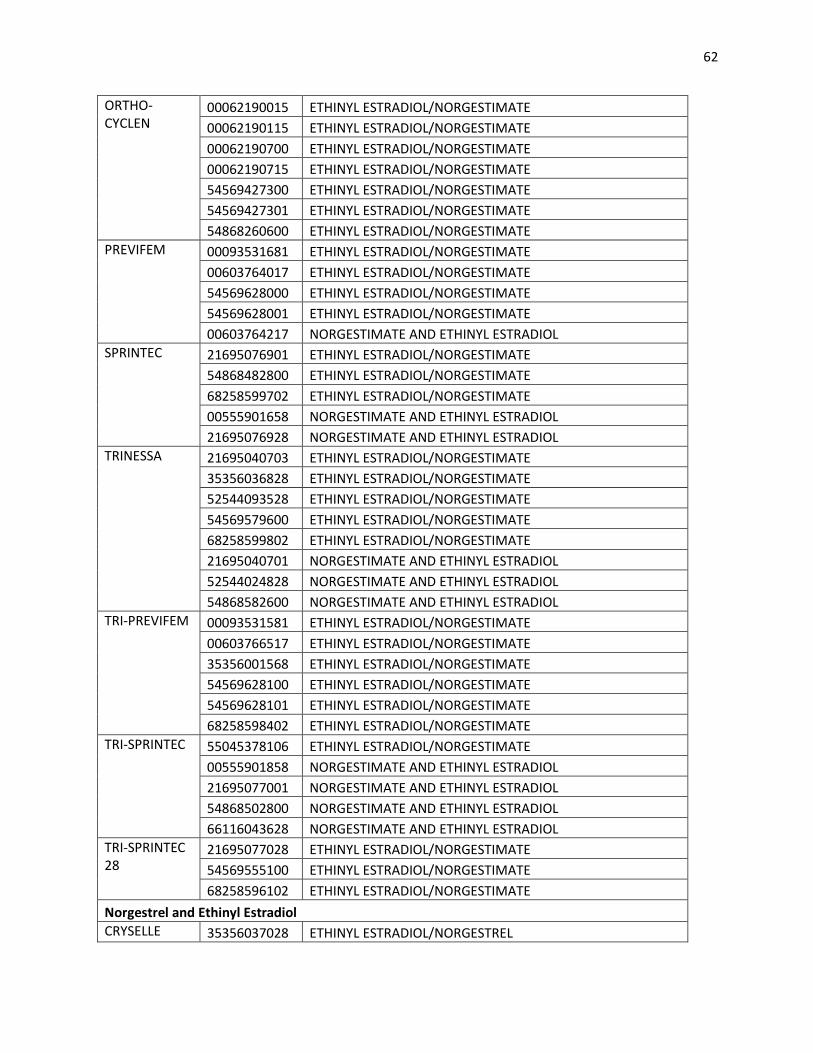
62
ORTHO-CYCLEN
00062190015 ETHINYL ESTRADIOL/NORGESTIMATE 00062190115 ETHINYL ESTRADIOL/NORGESTIMATE 00062190700 ETHINYL ESTRADIOL/NORGESTIMATE 00062190715 ETHINYL ESTRADIOL/NORGESTIMATE 54569427300 ETHINYL ESTRADIOL/NORGESTIMATE 54569427301 ETHINYL ESTRADIOL/NORGESTIMATE 54868260600 ETHINYL ESTRADIOL/NORGESTIMATE
PREVIFEM 00093531681 ETHINYL ESTRADIOL/NORGESTIMATE 00603764017 ETHINYL ESTRADIOL/NORGESTIMATE 54569628000 ETHINYL ESTRADIOL/NORGESTIMATE 54569628001 ETHINYL ESTRADIOL/NORGESTIMATE 00603764217 NORGESTIMATE AND ETHINYL ESTRADIOL
SPRINTEC 21695076901 ETHINYL ESTRADIOL/NORGESTIMATE 54868482800 ETHINYL ESTRADIOL/NORGESTIMATE 68258599702 ETHINYL ESTRADIOL/NORGESTIMATE 00555901658 NORGESTIMATE AND ETHINYL ESTRADIOL 21695076928 NORGESTIMATE AND ETHINYL ESTRADIOL
TRINESSA 21695040703 ETHINYL ESTRADIOL/NORGESTIMATE 35356036828 ETHINYL ESTRADIOL/NORGESTIMATE 52544093528 ETHINYL ESTRADIOL/NORGESTIMATE 54569579600 ETHINYL ESTRADIOL/NORGESTIMATE 68258599802 ETHINYL ESTRADIOL/NORGESTIMATE 21695040701 NORGESTIMATE AND ETHINYL ESTRADIOL 52544024828 NORGESTIMATE AND ETHINYL ESTRADIOL 54868582600 NORGESTIMATE AND ETHINYL ESTRADIOL
TRI-PREVIFEM 00093531581 ETHINYL ESTRADIOL/NORGESTIMATE 00603766517 ETHINYL ESTRADIOL/NORGESTIMATE 35356001568 ETHINYL ESTRADIOL/NORGESTIMATE 54569628100 ETHINYL ESTRADIOL/NORGESTIMATE 54569628101 ETHINYL ESTRADIOL/NORGESTIMATE 68258598402 ETHINYL ESTRADIOL/NORGESTIMATE
TRI-SPRINTEC 55045378106 ETHINYL ESTRADIOL/NORGESTIMATE 00555901858 NORGESTIMATE AND ETHINYL ESTRADIOL 21695077001 NORGESTIMATE AND ETHINYL ESTRADIOL 54868502800 NORGESTIMATE AND ETHINYL ESTRADIOL 66116043628 NORGESTIMATE AND ETHINYL ESTRADIOL
TRI-SPRINTEC 28
21695077028 ETHINYL ESTRADIOL/NORGESTIMATE 54569555100 ETHINYL ESTRADIOL/NORGESTIMATE 68258596102 ETHINYL ESTRADIOL/NORGESTIMATE
Norgestrel and Ethinyl Estradiol CRYSELLE 35356037028 ETHINYL ESTRADIOL/NORGESTREL
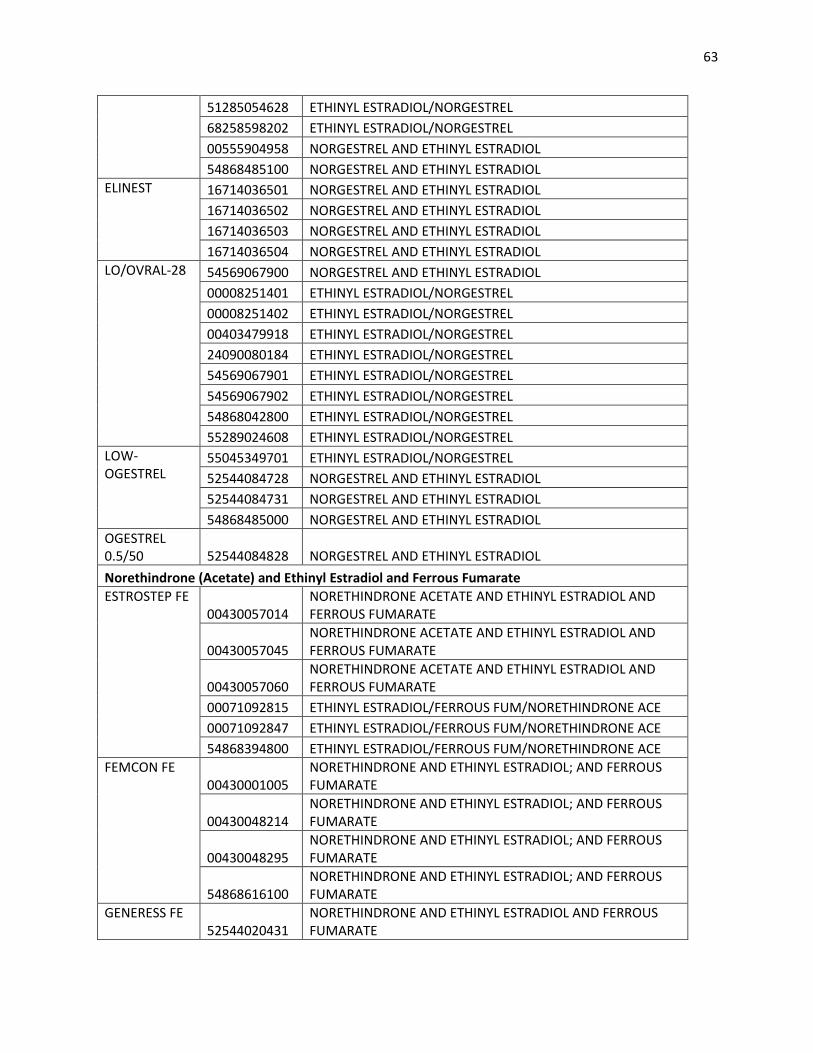
63
51285054628 ETHINYL ESTRADIOL/NORGESTREL 68258598202 ETHINYL ESTRADIOL/NORGESTREL 00555904958 NORGESTREL AND ETHINYL ESTRADIOL 54868485100 NORGESTREL AND ETHINYL ESTRADIOL
ELINEST 16714036501 NORGESTREL AND ETHINYL ESTRADIOL 16714036502 NORGESTREL AND ETHINYL ESTRADIOL 16714036503 NORGESTREL AND ETHINYL ESTRADIOL 16714036504 NORGESTREL AND ETHINYL ESTRADIOL
LO/OVRAL-28 54569067900 NORGESTREL AND ETHINYL ESTRADIOL 00008251401 ETHINYL ESTRADIOL/NORGESTREL 00008251402 ETHINYL ESTRADIOL/NORGESTREL 00403479918 ETHINYL ESTRADIOL/NORGESTREL 24090080184 ETHINYL ESTRADIOL/NORGESTREL 54569067901 ETHINYL ESTRADIOL/NORGESTREL 54569067902 ETHINYL ESTRADIOL/NORGESTREL 54868042800 ETHINYL ESTRADIOL/NORGESTREL 55289024608 ETHINYL ESTRADIOL/NORGESTREL
LOW-OGESTREL
55045349701 ETHINYL ESTRADIOL/NORGESTREL 52544084728 NORGESTREL AND ETHINYL ESTRADIOL 52544084731 NORGESTREL AND ETHINYL ESTRADIOL 54868485000 NORGESTREL AND ETHINYL ESTRADIOL
OGESTREL 0.5/50 52544084828 NORGESTREL AND ETHINYL ESTRADIOL Norethindrone (Acetate) and Ethinyl Estradiol and Ferrous Fumarate ESTROSTEP FE
00430057014 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
00430057045 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
00430057060 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
00071092815 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00071092847 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54868394800 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
FEMCON FE 00430001005
NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
00430048214 NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
00430048295 NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
54868616100 NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
GENERESS FE 52544020431
NORETHINDRONE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
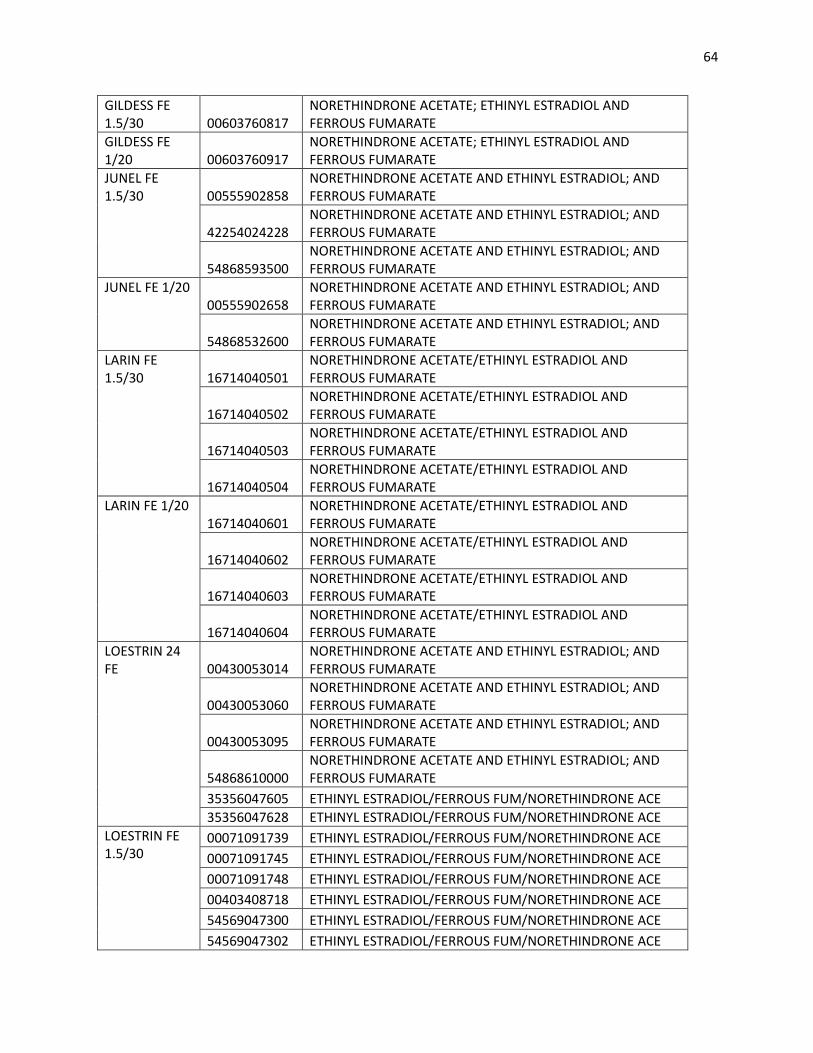
64
GILDESS FE 1.5/30 00603760817
NORETHINDRONE ACETATE; ETHINYL ESTRADIOL AND FERROUS FUMARATE
GILDESS FE 1/20 00603760917
NORETHINDRONE ACETATE; ETHINYL ESTRADIOL AND FERROUS FUMARATE
JUNEL FE 1.5/30 00555902858
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
42254024228 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
54868593500 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
JUNEL FE 1/20 00555902658
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
54868532600 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
LARIN FE 1.5/30 16714040501
NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040502 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040503 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040504 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
LARIN FE 1/20 16714040601
NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040602 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040603 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
16714040604 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
LOESTRIN 24 FE 00430053014
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
00430053060 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
00430053095 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
54868610000 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
35356047605 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 35356047628 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
LOESTRIN FE 1.5/30
00071091739 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00071091745 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00071091748 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00403408718 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54569047300 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54569047302 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
65
54868050200 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
51285008370 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
51285008498 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
51285012870 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
51285012998 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
LOESTRIN FE 1/20 51285012570
NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
51285012698 NORETHINDRONE ACETATE/ETHINYL ESTRADIOL AND FERROUS FUMARATE
00071091338 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00071091345 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00071091348 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 00403052918 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 35356036328 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54569325401 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54868151200 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
51285008070 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
51285008198 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
LO LOESTRIN FE 00430042014
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; ETHINYL ESTRADIOL AND FERROUS FUMARATE
00430042060 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; ETHINYL ESTRADIOL AND FERROUS FUMARATE
00430042095 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; ETHINYL ESTRADIOL AND FERROUS FUMARATE
LO MINASTRIN FE 00430053750
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; ETHINYL ESTRADIOL AND FERROUS FUMARATE
00430053795 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; ETHINYL ESTRADIOL AND FERROUS FUMARATE
MICROGESTIN 52544023328
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
52544024928 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
MICROGESTIN FE 52544063028
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
52544063031 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
52544063128 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
52544063131 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
66
54868474400 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE
MICROGESTIN FE 1.5/30
54868474500 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 68258598602 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
MICROGESTIN FE 1/20
21695085601 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 54569579700 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE 68258597602 ETHINYL ESTRADIOL/FERROUS FUM/NORETHINDRONE ACE
MINASTRIN 24 FE 00430054050
NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL CHEWABLE TABLETS AND FERROUS FUMARATE TABLETS
00430053550 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
00430053595 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
NORETHINDRONE AND ETHINYL ESTRADIOL AND FERROUS FUMARATE 68180089713 NORETHINDRONE AND ETHINYL ESTRADIOL OVCON 35 FE 00430058114 ETHINYL ESTRADIOL/FERROUS FUMARATE/NORETHINDRONE TILIA FE
52544017572 NORETHINDRONE ACETATE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
WYMZYA FE 68180089813
NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
ZEOSA 00093209058
NORETHINDRONE AND ETHINYL ESTRADIOL; AND FERROUS FUMARATE
Injectable Hormone Contraceptives AMEN 00086004905 MEDROXYPROGESTERONE ACETATE
00086004910 MEDROXYPROGESTERONE ACETATE 00086004990 MEDROXYPROGESTERONE ACETATE
CURRETAB 00032100742 MEDROXYPROGESTERONE ACETATE CYCRIN 00046089610 MEDROXYPROGESTERONE ACETATE
00046089681 MEDROXYPROGESTERONE ACETATE 00403458830 MEDROXYPROGESTERONE ACETATE 59911589601 MEDROXYPROGESTERONE ACETATE 59911589603 MEDROXYPROGESTERONE ACETATE 59911589701 MEDROXYPROGESTERONE ACETATE 59911589703 MEDROXYPROGESTERONE ACETATE 59911589801 MEDROXYPROGESTERONE ACETATE 59911589803 MEDROXYPROGESTERONE ACETATE
DEPO-PROVERA
00009062601 MEDROXYPROGESTERONE ACETATE 00009062602 MEDROXYPROGESTERONE ACETATE 00009074630 MEDROXYPROGESTERONE ACETATE 00009074635 MEDROXYPROGESTERONE ACETATE
67
00009737607 MEDROXYPROGESTERONE ACETATE 00009737611 MEDROXYPROGESTERONE ACETATE 54569370100 MEDROXYPROGESTERONE ACETATE 54569395700 MEDROXYPROGESTERONE ACETATE 54569395800 MEDROXYPROGESTERONE ACETATE 54569490400 MEDROXYPROGESTERONE ACETATE 54868334801 MEDROXYPROGESTERONE ACETATE
DEPO-PROVERA CONTRACEPTIVE
00009074631 MEDROXYPROGESTERONE ACETATE 00009074634 MEDROXYPROGESTERONE ACETATE 00009737601 MEDROXYPROGESTERONE ACETATE 00009737602 MEDROXYPROGESTERONE ACETATE 00009737603 MEDROXYPROGESTERONE ACETATE 00009737604 MEDROXYPROGESTERONE ACETATE 00403504318 MEDROXYPROGESTERONE ACETATE 54569552700 MEDROXYPROGESTERONE ACETATE 54868361300 MEDROXYPROGESTERONE ACETATE 54868410000 MEDROXYPROGESTERONE ACETATE 54868410001 MEDROXYPROGESTERONE ACETATE 55045350501 MEDROXYPROGESTERONE ACETATE
DEPO-SUBQ PROVERA 00009470913 MEDROXYPROGESTERONE ACETATE DEPO-SUBQ PROVERA 104
00009470901 MEDROXYPROGESTERONE ACETATE 54569621900 MEDROXYPROGESTERONE ACETATE
MEDROXYPROGESTERONE
55887047210 MEDROXYPROGESTERONE ACETATE 55887047230 MEDROXYPROGESTERONE ACETATE 55887047290 MEDROXYPROGESTERONE ACETATE
MEDROXYPROGESTERONE ACETATE
00047026524 MEDROXYPROGESTERONE ACETATE 00047026624 MEDROXYPROGESTERONE ACETATE 00047087419 MEDROXYPROGESTERONE ACETATE 00047087424 MEDROXYPROGESTERONE ACETATE 00047087429 MEDROXYPROGESTERONE ACETATE 00182119602 MEDROXYPROGESTERONE ACETATE 00182119619 MEDROXYPROGESTERONE ACETATE 00302395025 MEDROXYPROGESTERONE ACETATE 00302395048 MEDROXYPROGESTERONE ACETATE 00339585112 MEDROXYPROGESTERONE ACETATE 00349230901 MEDROXYPROGESTERONE ACETATE 00349230905 MEDROXYPROGESTERONE ACETATE 00349230925 MEDROXYPROGESTERONE ACETATE 00349230950 MEDROXYPROGESTERONE ACETATE 00364052104 MEDROXYPROGESTERONE ACETATE 00364052150 MEDROXYPROGESTERONE ACETATE
68
00403178010 MEDROXYPROGESTERONE ACETATE 00405461804 MEDROXYPROGESTERONE ACETATE 00405461850 MEDROXYPROGESTERONE ACETATE 00536399502 MEDROXYPROGESTERONE ACETATE 00536399506 MEDROXYPROGESTERONE ACETATE 00536590501 MEDROXYPROGESTERONE ACETATE 00536590601 MEDROXYPROGESTERONE ACETATE 00536590701 MEDROXYPROGESTERONE ACETATE 00555077902 MEDROXYPROGESTERONE ACETATE 00555077904 MEDROXYPROGESTERONE ACETATE 00555087202 MEDROXYPROGESTERONE ACETATE 00555087204 MEDROXYPROGESTERONE ACETATE 00555087302 MEDROXYPROGESTERONE ACETATE 00555087304 MEDROXYPROGESTERONE ACETATE 00603436521 MEDROXYPROGESTERONE ACETATE 00603436621 MEDROXYPROGESTERONE ACETATE 00603436721 MEDROXYPROGESTERONE ACETATE 00603436819 MEDROXYPROGESTERONE ACETATE 00603436824 MEDROXYPROGESTERONE ACETATE 00665400106 MEDROXYPROGESTERONE ACETATE 00665400107 MEDROXYPROGESTERONE ACETATE 00665400142 MEDROXYPROGESTERONE ACETATE 00677080301 MEDROXYPROGESTERONE ACETATE 00677080302 MEDROXYPROGESTERONE ACETATE 00677080303 MEDROXYPROGESTERONE ACETATE 00677161701 MEDROXYPROGESTERONE ACETATE 00677161801 MEDROXYPROGESTERONE ACETATE 00677161901 MEDROXYPROGESTERONE ACETATE 00703680101 MEDROXYPROGESTERONE ACETATE 00703680104 MEDROXYPROGESTERONE ACETATE 00703681121 MEDROXYPROGESTERONE ACETATE 00781168025 MEDROXYPROGESTERONE ACETATE 00781168050 MEDROXYPROGESTERONE ACETATE 00814466008 MEDROXYPROGESTERONE ACETATE 00814466022 MEDROXYPROGESTERONE ACETATE 00832008700 MEDROXYPROGESTERONE ACETATE 00832008725 MEDROXYPROGESTERONE ACETATE 00832008726 MEDROXYPROGESTERONE ACETATE 00832008750 MEDROXYPROGESTERONE ACETATE 00839661004 MEDROXYPROGESTERONE ACETATE 00839661006 MEDROXYPROGESTERONE ACETATE
69
00839661009 MEDROXYPROGESTERONE ACETATE 00904269040 MEDROXYPROGESTERONE ACETATE 00904269051 MEDROXYPROGESTERONE ACETATE 00904269060 MEDROXYPROGESTERONE ACETATE 00904269070 MEDROXYPROGESTERONE ACETATE 00904522740 MEDROXYPROGESTERONE ACETATE 00904522760 MEDROXYPROGESTERONE ACETATE 00904522840 MEDROXYPROGESTERONE ACETATE 00904522860 MEDROXYPROGESTERONE ACETATE 10544000130 MEDROXYPROGESTERONE ACETATE 10544006210 MEDROXYPROGESTERONE ACETATE 11845034102 MEDROXYPROGESTERONE ACETATE 21695089610 MEDROXYPROGESTERONE ACETATE 21695089620 MEDROXYPROGESTERONE ACETATE 21695089630 MEDROXYPROGESTERONE ACETATE 23490585300 MEDROXYPROGESTERONE ACETATE 23490585302 MEDROXYPROGESTERONE ACETATE 23490585401 MEDROXYPROGESTERONE ACETATE 23490585503 MEDROXYPROGESTERONE ACETATE 23490585701 MEDROXYPROGESTERONE ACETATE 33261053405 MEDROXYPROGESTERONE ACETATE 33261053410 MEDROXYPROGESTERONE ACETATE 33261053414 MEDROXYPROGESTERONE ACETATE 33261053430 MEDROXYPROGESTERONE ACETATE 33261053460 MEDROXYPROGESTERONE ACETATE 33261053490 MEDROXYPROGESTERONE ACETATE 33261060930 MEDROXYPROGESTERONE ACETATE 33261074020 MEDROXYPROGESTERONE ACETATE 33261074028 MEDROXYPROGESTERONE ACETATE 33261074030 MEDROXYPROGESTERONE ACETATE 35356036414 MEDROXYPROGESTERONE ACETATE 38779142203 MEDROXYPROGESTERONE ACETATE 38779142204 MEDROXYPROGESTERONE ACETATE 38779142205 MEDROXYPROGESTERONE ACETATE 38779142206 MEDROXYPROGESTERONE ACETATE 38779142208 MEDROXYPROGESTERONE ACETATE 38779142209 MEDROXYPROGESTERONE ACETATE 43063043805 MEDROXYPROGESTERONE ACETATE 43063043807 MEDROXYPROGESTERONE ACETATE 43063043810 MEDROXYPROGESTERONE ACETATE 43063043813 MEDROXYPROGESTERONE ACETATE
70
43063043830 MEDROXYPROGESTERONE ACETATE 43063043840 MEDROXYPROGESTERONE ACETATE 43063043842 MEDROXYPROGESTERONE ACETATE 43063043850 MEDROXYPROGESTERONE ACETATE 49349028702 MEDROXYPROGESTERONE ACETATE 49452463801 MEDROXYPROGESTERONE ACETATE 49452463802 MEDROXYPROGESTERONE ACETATE 49452463803 MEDROXYPROGESTERONE ACETATE 49999009205 MEDROXYPROGESTERONE ACETATE 49999009210 MEDROXYPROGESTERONE ACETATE 49999049410 MEDROXYPROGESTERONE ACETATE 51285054002 MEDROXYPROGESTERONE ACETATE 51285054004 MEDROXYPROGESTERONE ACETATE 51285054102 MEDROXYPROGESTERONE ACETATE 51285054104 MEDROXYPROGESTERONE ACETATE 51285054202 MEDROXYPROGESTERONE ACETATE 51285054204 MEDROXYPROGESTERONE ACETATE 51432026701 MEDROXYPROGESTERONE ACETATE 51432026704 MEDROXYPROGESTERONE ACETATE 51927149000 MEDROXYPROGESTERONE ACETATE 52125056208 MEDROXYPROGESTERONE ACETATE 52125064001 MEDROXYPROGESTERONE ACETATE 52125080308 MEDROXYPROGESTERONE ACETATE 52555046300 MEDROXYPROGESTERONE ACETATE 52555046302 MEDROXYPROGESTERONE ACETATE 52959042030 MEDROXYPROGESTERONE ACETATE 52959094310 MEDROXYPROGESTERONE ACETATE 54569080900 MEDROXYPROGESTERONE ACETATE 54569080901 MEDROXYPROGESTERONE ACETATE 54569080902 MEDROXYPROGESTERONE ACETATE 54569080903 MEDROXYPROGESTERONE ACETATE 54569080904 MEDROXYPROGESTERONE ACETATE 54569080905 MEDROXYPROGESTERONE ACETATE 54569080906 MEDROXYPROGESTERONE ACETATE 54569080907 MEDROXYPROGESTERONE ACETATE 54569080908 MEDROXYPROGESTERONE ACETATE 54569380600 MEDROXYPROGESTERONE ACETATE 54569380601 MEDROXYPROGESTERONE ACETATE 54569380602 MEDROXYPROGESTERONE ACETATE 54569380700 MEDROXYPROGESTERONE ACETATE 54569380701 MEDROXYPROGESTERONE ACETATE
71
54569561600 MEDROXYPROGESTERONE ACETATE 54569561600 MEDROXYPROGESTERONE ACETATE 54569857000 MEDROXYPROGESTERONE ACETATE 54569857001 MEDROXYPROGESTERONE ACETATE 54569857100 MEDROXYPROGESTERONE ACETATE 54569857200 MEDROXYPROGESTERONE ACETATE 54807055001 MEDROXYPROGESTERONE ACETATE 54868010900 MEDROXYPROGESTERONE ACETATE 54868010901 MEDROXYPROGESTERONE ACETATE 54868010902 MEDROXYPROGESTERONE ACETATE 54868010903 MEDROXYPROGESTERONE ACETATE 54868010905 MEDROXYPROGESTERONE ACETATE 54868010906 MEDROXYPROGESTERONE ACETATE 54868010907 MEDROXYPROGESTERONE ACETATE 54868010908 MEDROXYPROGESTERONE ACETATE 54868298400 MEDROXYPROGESTERONE ACETATE 54868298402 MEDROXYPROGESTERONE ACETATE 54868298403 MEDROXYPROGESTERONE ACETATE 54868298500 MEDROXYPROGESTERONE ACETATE 54868298501 MEDROXYPROGESTERONE ACETATE 54868298502 MEDROXYPROGESTERONE ACETATE 54868298503 MEDROXYPROGESTERONE ACETATE 54868525700 MEDROXYPROGESTERONE ACETATE 55045198908 MEDROXYPROGESTERONE ACETATE 55045394001 MEDROXYPROGESTERONE ACETATE 55154053300 MEDROXYPROGESTERONE ACETATE 55154053304 MEDROXYPROGESTERONE ACETATE 55175033301 MEDROXYPROGESTERONE ACETATE 55175033303 MEDROXYPROGESTERONE ACETATE 55175033401 MEDROXYPROGESTERONE ACETATE 55175033402 MEDROXYPROGESTERONE ACETATE 55175033403 MEDROXYPROGESTERONE ACETATE 55175033404 MEDROXYPROGESTERONE ACETATE 55175033405 MEDROXYPROGESTERONE ACETATE 55175033406 MEDROXYPROGESTERONE ACETATE 55289016005 MEDROXYPROGESTERONE ACETATE 55289016007 MEDROXYPROGESTERONE ACETATE 55289016010 MEDROXYPROGESTERONE ACETATE 55289016013 MEDROXYPROGESTERONE ACETATE 55289016030 MEDROXYPROGESTERONE ACETATE 55289016040 MEDROXYPROGESTERONE ACETATE
72
55289016042 MEDROXYPROGESTERONE ACETATE 55289016050 MEDROXYPROGESTERONE ACETATE 55289081630 MEDROXYPROGESTERONE ACETATE 55289090830 MEDROXYPROGESTERONE ACETATE 55289090842 MEDROXYPROGESTERONE ACETATE 55829035610 MEDROXYPROGESTERONE ACETATE 55887029110 MEDROXYPROGESTERONE ACETATE 55887029130 MEDROXYPROGESTERONE ACETATE 55887029160 MEDROXYPROGESTERONE ACETATE 55887029190 MEDROXYPROGESTERONE ACETATE 55887047260 MEDROXYPROGESTERONE ACETATE 56126048011 MEDROXYPROGESTERONE ACETATE 58016092600 MEDROXYPROGESTERONE ACETATE 58016092610 MEDROXYPROGESTERONE ACETATE 58016092614 MEDROXYPROGESTERONE ACETATE 58016092615 MEDROXYPROGESTERONE ACETATE 58016092620 MEDROXYPROGESTERONE ACETATE 58016092630 MEDROXYPROGESTERONE ACETATE 58016092640 MEDROXYPROGESTERONE ACETATE 58016092650 MEDROXYPROGESTERONE ACETATE 58469039953 MEDROXYPROGESTERONE ACETATE 58864074415 MEDROXYPROGESTERONE ACETATE 58864074430 MEDROXYPROGESTERONE ACETATE 59762374001 MEDROXYPROGESTERONE ACETATE 59762374004 MEDROXYPROGESTERONE ACETATE 59762374005 MEDROXYPROGESTERONE ACETATE 59762374101 MEDROXYPROGESTERONE ACETATE 59762374104 MEDROXYPROGESTERONE ACETATE 59762374201 MEDROXYPROGESTERONE ACETATE 59762374202 MEDROXYPROGESTERONE ACETATE 59762374203 MEDROXYPROGESTERONE ACETATE 59762374206 MEDROXYPROGESTERONE ACETATE 59762374207 MEDROXYPROGESTERONE ACETATE 59762374208 MEDROXYPROGESTERONE ACETATE 59762453701 MEDROXYPROGESTERONE ACETATE 59762453702 MEDROXYPROGESTERONE ACETATE 59762453801 MEDROXYPROGESTERONE ACETATE 59762453802 MEDROXYPROGESTERONE ACETATE 59762453809 MEDROXYPROGESTERONE ACETATE 60346021330 MEDROXYPROGESTERONE ACETATE 60346057105 MEDROXYPROGESTERONE ACETATE
73
60346057107 MEDROXYPROGESTERONE ACETATE 60346057110 MEDROXYPROGESTERONE ACETATE 60346057120 MEDROXYPROGESTERONE ACETATE 60346057130 MEDROXYPROGESTERONE ACETATE 60346057140 MEDROXYPROGESTERONE ACETATE 60346057148 MEDROXYPROGESTERONE ACETATE 62682500503 MEDROXYPROGESTERONE ACETATE 63629261201 MEDROXYPROGESTERONE ACETATE 63629261202 MEDROXYPROGESTERONE ACETATE 63629261203 MEDROXYPROGESTERONE ACETATE 63629261204 MEDROXYPROGESTERONE ACETATE 63629261205 MEDROXYPROGESTERONE ACETATE 63629261206 MEDROXYPROGESTERONE ACETATE 63629261301 MEDROXYPROGESTERONE ACETATE 63629261302 MEDROXYPROGESTERONE ACETATE 63629261303 MEDROXYPROGESTERONE ACETATE 63629261401 MEDROXYPROGESTERONE ACETATE 64205007710 MEDROXYPROGESTERONE ACETATE 64205008730 MEDROXYPROGESTERONE ACETATE 64205008790 MEDROXYPROGESTERONE ACETATE 66116028830 MEDROXYPROGESTERONE ACETATE 66267014010 MEDROXYPROGESTERONE ACETATE 66267014130 MEDROXYPROGESTERONE ACETATE 66336021330 MEDROXYPROGESTERONE ACETATE 66336060320 MEDROXYPROGESTERONE ACETATE 66336060330 MEDROXYPROGESTERONE ACETATE 66336062210 MEDROXYPROGESTERONE ACETATE 66336062230 MEDROXYPROGESTERONE ACETATE 68084055321 MEDROXYPROGESTERONE ACETATE 68115022510 MEDROXYPROGESTERONE ACETATE 68115022530 MEDROXYPROGESTERONE ACETATE 68788923301 MEDROXYPROGESTERONE ACETATE 68788989901 MEDROXYPROGESTERONE ACETATE 68788989903 MEDROXYPROGESTERONE ACETATE
PROVERA 00009005002 MEDROXYPROGESTERONE ACETATE 00009005009 MEDROXYPROGESTERONE ACETATE 00009005011 MEDROXYPROGESTERONE ACETATE 00009005027 MEDROXYPROGESTERONE ACETATE 00009006404 MEDROXYPROGESTERONE ACETATE 00009006406 MEDROXYPROGESTERONE ACETATE 00009006412 MEDROXYPROGESTERONE ACETATE
74
00009028603 MEDROXYPROGESTERONE ACETATE 00009028632 MEDROXYPROGESTERONE ACETATE 00009028642 MEDROXYPROGESTERONE ACETATE 00403177901 MEDROXYPROGESTERONE ACETATE 00403177910 MEDROXYPROGESTERONE ACETATE 00403324101 MEDROXYPROGESTERONE ACETATE 49999027201 MEDROXYPROGESTERONE ACETATE 49999027230 MEDROXYPROGESTERONE ACETATE 54569081600 MEDROXYPROGESTERONE ACETATE 54569081604 MEDROXYPROGESTERONE ACETATE 54569081605 MEDROXYPROGESTERONE ACETATE 54569081606 MEDROXYPROGESTERONE ACETATE 54569177900 MEDROXYPROGESTERONE ACETATE 54569177903 MEDROXYPROGESTERONE ACETATE 54569184901 MEDROXYPROGESTERONE ACETATE 54569184903 MEDROXYPROGESTERONE ACETATE 54569184904 MEDROXYPROGESTERONE ACETATE 54569184905 MEDROXYPROGESTERONE ACETATE 54569851600 MEDROXYPROGESTERONE ACETATE 54569851602 MEDROXYPROGESTERONE ACETATE 54569852400 MEDROXYPROGESTERONE ACETATE 54569852401 MEDROXYPROGESTERONE ACETATE 54868029000 MEDROXYPROGESTERONE ACETATE 54868029002 MEDROXYPROGESTERONE ACETATE 54868029003 MEDROXYPROGESTERONE ACETATE 54868029004 MEDROXYPROGESTERONE ACETATE 54868101001 MEDROXYPROGESTERONE ACETATE 54868101003 MEDROXYPROGESTERONE ACETATE 55289003410 MEDROXYPROGESTERONE ACETATE 55289012130 MEDROXYPROGESTERONE ACETATE 58016096900 MEDROXYPROGESTERONE ACETATE 58016096930 MEDROXYPROGESTERONE ACETATE 58016096960 MEDROXYPROGESTERONE ACETATE 58016096990 MEDROXYPROGESTERONE ACETATE 60346060330 MEDROXYPROGESTERONE ACETATE 60346060348 MEDROXYPROGESTERONE ACETATE 60346084830 MEDROXYPROGESTERONE ACETATE 60346084890 MEDROXYPROGESTERONE ACETATE
Intrauterine Devices—Nonhormonal PARAGARD T 380A
51285020401 COPPER 51285020402 COPPER
75
50907038006 INTRAUTERINE DEVICE, CONTRACEPTIVE & INTRODUCER 50907038007 INTRAUTERINE DEVICE, CONTRACEPTIVE & INTRODUCER 51285020402 INTRAUTERINE DEVICE, CONTRACEPTIVE & INTRODUCER 54765038001 INTRAUTERINE DEVICE, CONTRACEPTIVE & INTRODUCER 54765038005 INTRAUTERINE DEVICE, CONTRACEPTIVE & INTRODUCER
Intrauterine Devices—Hormonal MIRENA 50419042101 LEVONORGESTREL
50419042301 LEVONORGESTREL SKYLA 50419042201 LEVONORGESTREL
50419042208 LEVONORGESTREL 50419042271 LEVONORGESTREL
Implantable Hormones IMPLANON 00052027201 ETONOGESTREL NEXPLANON 00052027401 ETONOGESTREL
00052027480 ETONOGESTREL 00052433001 ETONOGESTREL
Hormonal Patch ORTHO EVRA 00062192001 NORELGESTROMIN AND ETHINYL ESTRADIOL
00062192015 NORELGESTROMIN AND ETHINYL ESTRADIOL 54569541300 NORELGESTROMIN AND ETHINYL ESTRADIOL 54868467000 NORELGESTROMIN AND ETHINYL ESTRADIOL 68258599403 NORELGESTROMIN AND ETHINYL ESTRADIOL 50458019201 NORELGESTROMIN AND ETHINYL ESTRADIOL 50458019215 NORELGESTROMIN AND ETHINYL ESTRADIOL 50458019224 NORELGESTROMIN AND ETHINYL ESTRADIOL
XULANE 00378334053 NORELGESTROMIN AND ETHINYL ESTRADIOL Vaginal Ring NUVARING 00052027301 ETHINYL ESTRADIOL/ETONOGESTREL
35356041003 ETHINYL ESTRADIOL/ETONOGESTREL 54569586500 ETHINYL ESTRADIOL/ETONOGESTREL 54868483200 ETHINYL ESTRADIOL/ETONOGESTREL 55887075401 ETHINYL ESTRADIOL/ETONOGESTREL 00052027303 ETONOGESTREL AND ETHINYL ESTRADIOL 00052027385 ETONOGESTREL AND ETHINYL ESTRADIOL 54868483201 ETONOGESTREL AND ETHINYL ESTRADIOL
76
APPENDIX B. Stakeholder Partnership Council Membership List
PATIENTS and CONSUMERS Shilpa Amin, MD, MBSc Fairfax County Health Department, until Summer 2014 **Former AHRQ Medical Officer for DEcIDE-CMTP Uterine Fibroid Project, 2009–11 Email: [email protected]
John Santa, MD, MPH Medical Director Consumer’s Union Email: [email protected]
Carla Dionne Founder and Executive Director National Uterine Fibroid Foundation Email: [email protected]
Sateria Venable Founder The Fibroid Foundation Email: [email protected]
Paula Gwynn Grant Vice President of Communications and Community Development Housing Authority of DeKalb County, Georgia Email: [email protected]
CLINICIANS Michael Brunner, MD Diagnostic & Interventional Radiologist Society for Interventional Radiologists Email: [email protected]
William Catherino, MD, PhD Associate Professor, Department of Obstetrics and Gynecology Veterans Administration/Department of Defense Email: [email protected]
Linda Bradley, MD Professor of Surgery, Vice Chairman of Obstetrics, Gynecology and Women’s Health Institute Director, Center for Menstrual Disorders, Fibroids & Hysteroscopic Services Email: [email protected]
RESEARCHERS James Spies, MD Chairman and Professor, Department of Radiology Georgetown University Medical Center Email: [email protected]
Elizabeth (Ebbie) Stewart, MD Professor of Obstetrics and Gynecology Chair, Division of Reproductive Endocrinology Mayo Clinic College of Medicine Email: [email protected]
PAYERS
77
Tina Groat, MD, MBA National Medical Director, Women’s Health UnitedHealthcare Email: [email protected]
Tina Raine-Bennett, MD, MPH Research Director, Women’s Health Research Institute Kaiser Permanente Email: [email protected]
FEDERAL FUNDING AGENCY REPRESENTATIVES and POLICY EXPERTS Donna Baird, PhD Principal Investigator, Epidemiology National Institute of Environmental Health Sciences, Women’s Health Group Email: [email protected]
Estella Parrott, MD, MPH Medical Officer Eunice Kennedy Shriver National Institute of Child Health and Human Development, Gynecologic Health and Disease Branch Email: [email protected]
Lisa Begg, DrPH, RN Senior Scientist Department of Health and Human Services Office on Women’s Health Email: [email protected]
Jim Segars, MD Investigator National Institute of Child Health and Human Development, Unit on Reproductive Endocrinology and Infertility Email: [email protected]
Elise Berliner, PhD Director, Technology Assessment Program Agency for Healthcare Quality and Research Email: [email protected]
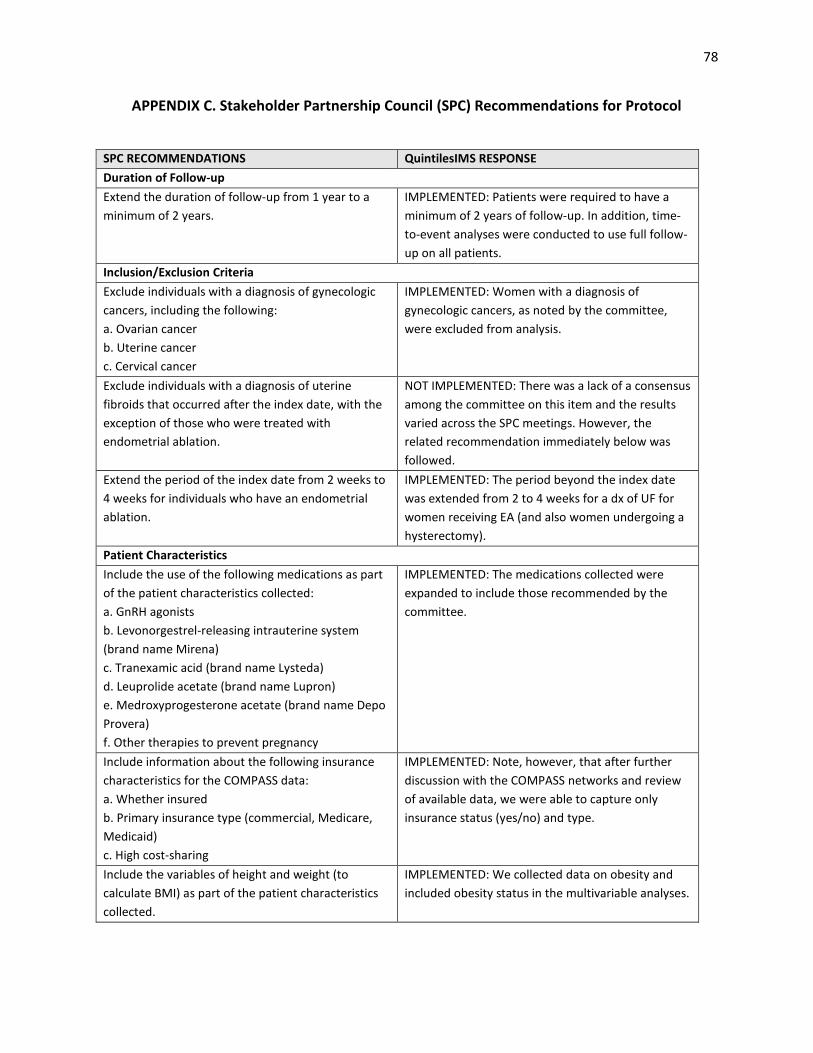
78
APPENDIX C. Stakeholder Partnership Council (SPC) Recommendations for Protocol
SPC RECOMMENDATIONS QuintilesIMS RESPONSE Duration of Follow-up Extend the duration of follow-up from 1 year to a minimum of 2 years.
IMPLEMENTED: Patients were required to have a minimum of 2 years of follow-up. In addition, time-to-event analyses were conducted to use full follow-up on all patients.
Inclusion/Exclusion Criteria Exclude individuals with a diagnosis of gynecologic cancers, including the following: a. Ovarian cancer b. Uterine cancer c. Cervical cancer
IMPLEMENTED: Women with a diagnosis of gynecologic cancers, as noted by the committee, were excluded from analysis.
Exclude individuals with a diagnosis of uterine fibroids that occurred after the index date, with the exception of those who were treated with endometrial ablation.
NOT IMPLEMENTED: There was a lack of a consensus among the committee on this item and the results varied across the SPC meetings. However, the related recommendation immediately below was followed.
Extend the period of the index date from 2 weeks to 4 weeks for individuals who have an endometrial ablation.
IMPLEMENTED: The period beyond the index date was extended from 2 to 4 weeks for a dx of UF for women receiving EA (and also women undergoing a hysterectomy).
Patient Characteristics Include the use of the following medications as part of the patient characteristics collected: a. GnRH agonists b. Levonorgestrel-releasing intrauterine system (brand name Mirena) c. Tranexamic acid (brand name Lysteda) d. Leuprolide acetate (brand name Lupron) e. Medroxyprogesterone acetate (brand name Depo Provera) f. Other therapies to prevent pregnancy
IMPLEMENTED: The medications collected were expanded to include those recommended by the committee.
Include information about the following insurance characteristics for the COMPASS data: a. Whether insured b. Primary insurance type (commercial, Medicare, Medicaid) c. High cost-sharing
IMPLEMENTED: Note, however, that after further discussion with the COMPASS networks and review of available data, we were able to capture only insurance status (yes/no) and type.
Include the variables of height and weight (to calculate BMI) as part of the patient characteristics collected.
IMPLEMENTED: We collected data on obesity and included obesity status in the multivariable analyses.
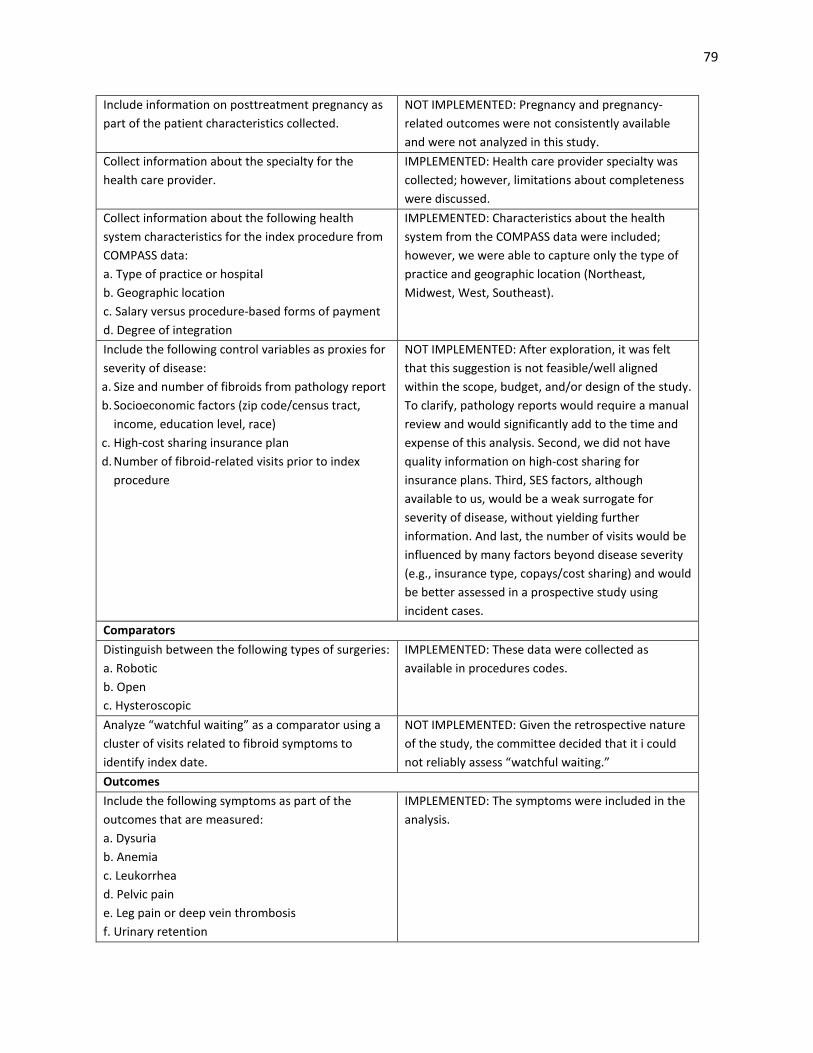
79
Include information on posttreatment pregnancy as part of the patient characteristics collected.
NOT IMPLEMENTED: Pregnancy and pregnancy-related outcomes were not consistently available and were not analyzed in this study.
Collect information about the specialty for the health care provider.
IMPLEMENTED: Health care provider specialty was collected; however, limitations about completeness were discussed.
Collect information about the following health system characteristics for the index procedure from COMPASS data: a. Type of practice or hospital b. Geographic location c. Salary versus procedure-based forms of payment d. Degree of integration
IMPLEMENTED: Characteristics about the health system from the COMPASS data were included; however, we were able to capture only the type of practice and geographic location (Northeast, Midwest, West, Southeast).
Include the following control variables as proxies for severity of disease: a. Size and number of fibroids from pathology report b. Socioeconomic factors (zip code/census tract,
income, education level, race) c. High-cost sharing insurance plan d. Number of fibroid-related visits prior to index
procedure
NOT IMPLEMENTED: After exploration, it was felt that this suggestion is not feasible/well aligned within the scope, budget, and/or design of the study. To clarify, pathology reports would require a manual review and would significantly add to the time and expense of this analysis. Second, we did not have quality information on high-cost sharing for insurance plans. Third, SES factors, although available to us, would be a weak surrogate for severity of disease, without yielding further information. And last, the number of visits would be influenced by many factors beyond disease severity (e.g., insurance type, copays/cost sharing) and would be better assessed in a prospective study using incident cases.
Comparators Distinguish between the following types of surgeries: a. Robotic b. Open c. Hysteroscopic
IMPLEMENTED: These data were collected as available in procedures codes.
Analyze “watchful waiting” as a comparator using a cluster of visits related to fibroid symptoms to identify index date.
NOT IMPLEMENTED: Given the retrospective nature of the study, the committee decided that it i could not reliably assess “watchful waiting.”
Outcomes Include the following symptoms as part of the outcomes that are measured: a. Dysuria b. Anemia c. Leukorrhea d. Pelvic pain e. Leg pain or deep vein thrombosis f. Urinary retention
IMPLEMENTED: The symptoms were included in the analysis.
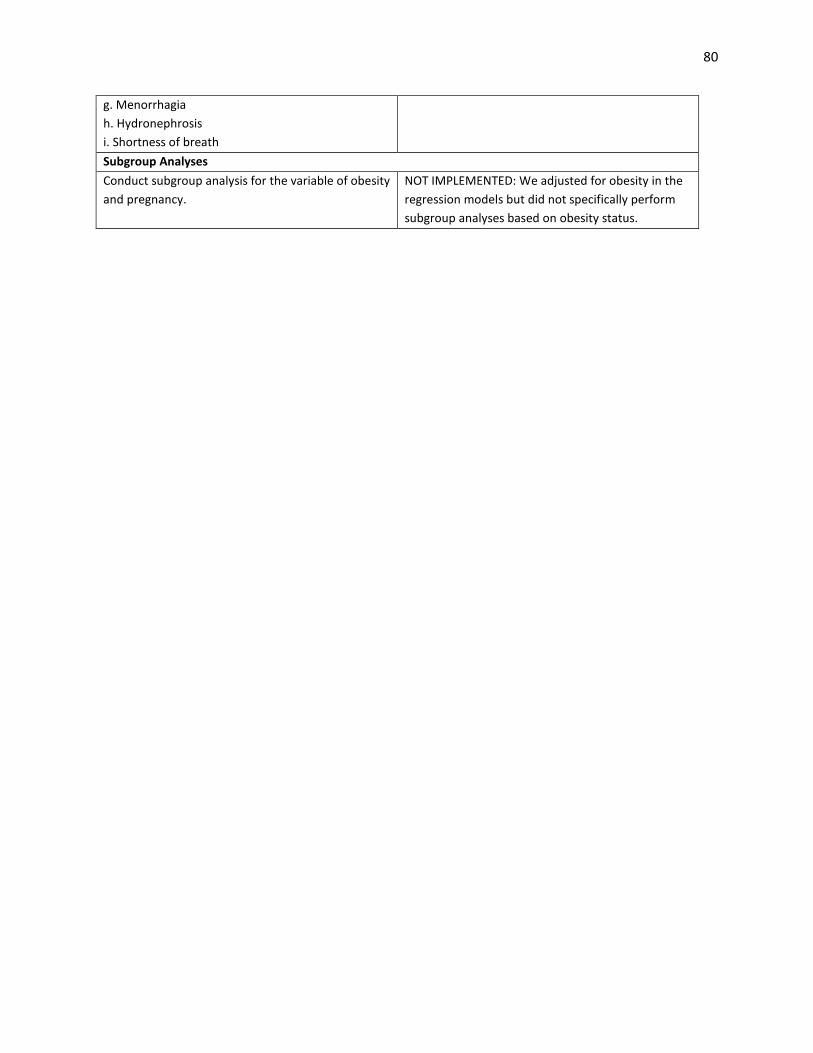
80
g. Menorrhagia h. Hydronephrosis i. Shortness of breath Subgroup Analyses Conduct subgroup analysis for the variable of obesity and pregnancy.
NOT IMPLEMENTED: We adjusted for obesity in the regression models but did not specifically perform subgroup analyses based on obesity status.
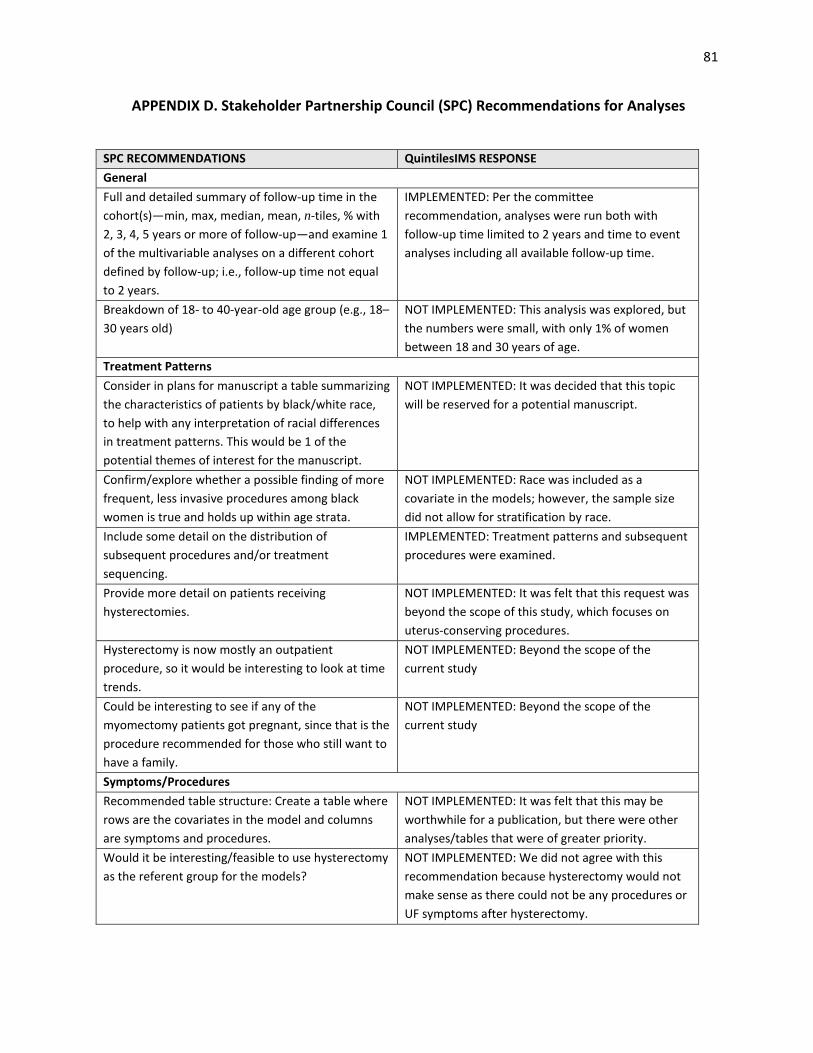
81
APPENDIX D. Stakeholder Partnership Council (SPC) Recommendations for Analyses
SPC RECOMMENDATIONS QuintilesIMS RESPONSE General Full and detailed summary of follow-up time in the cohort(s)—min, max, median, mean, n-tiles, % with 2, 3, 4, 5 years or more of follow-up—and examine 1 of the multivariable analyses on a different cohort defined by follow-up; i.e., follow-up time not equal to 2 years.
IMPLEMENTED: Per the committee recommendation, analyses were run both with follow-up time limited to 2 years and time to event analyses including all available follow-up time.
Breakdown of 18- to 40-year-old age group (e.g., 18–30 years old)
NOT IMPLEMENTED: This analysis was explored, but the numbers were small, with only 1% of women between 18 and 30 years of age.
Treatment Patterns Consider in plans for manuscript a table summarizing the characteristics of patients by black/white race, to help with any interpretation of racial differences in treatment patterns. This would be 1 of the potential themes of interest for the manuscript.
NOT IMPLEMENTED: It was decided that this topic will be reserved for a potential manuscript.
Confirm/explore whether a possible finding of more frequent, less invasive procedures among black women is true and holds up within age strata.
NOT IMPLEMENTED: Race was included as a covariate in the models; however, the sample size did not allow for stratification by race.
Include some detail on the distribution of subsequent procedures and/or treatment sequencing.
IMPLEMENTED: Treatment patterns and subsequent procedures were examined.
Provide more detail on patients receiving hysterectomies.
NOT IMPLEMENTED: It was felt that this request was beyond the scope of this study, which focuses on uterus-conserving procedures.
Hysterectomy is now mostly an outpatient procedure, so it would be interesting to look at time trends.
NOT IMPLEMENTED: Beyond the scope of the current study
Could be interesting to see if any of the myomectomy patients got pregnant, since that is the procedure recommended for those who still want to have a family.
NOT IMPLEMENTED: Beyond the scope of the current study
Symptoms/Procedures Recommended table structure: Create a table where rows are the covariates in the model and columns are symptoms and procedures.
NOT IMPLEMENTED: It was felt that this may be worthwhile for a publication, but there were other analyses/tables that were of greater priority.
Would it be interesting/feasible to use hysterectomy as the referent group for the models?
NOT IMPLEMENTED: We did not agree with this recommendation because hysterectomy would not make sense as there could not be any procedures or UF symptoms after hysterectomy.
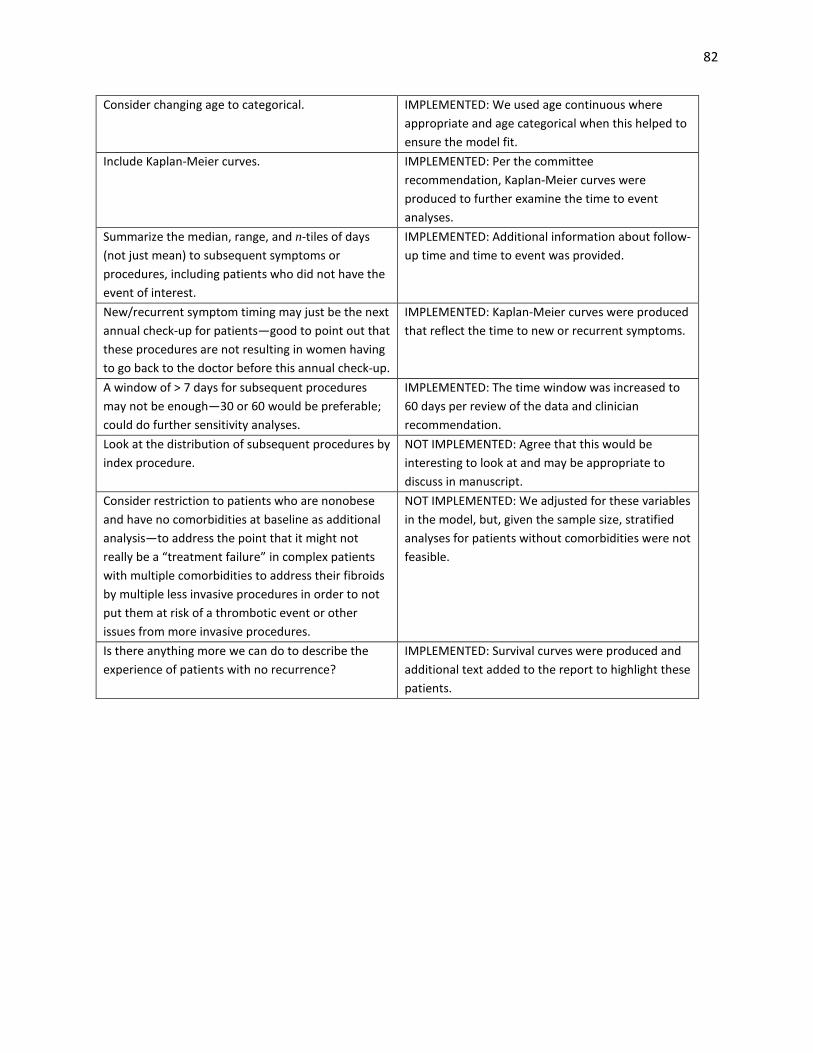
82
Consider changing age to categorical. IMPLEMENTED: We used age continuous where appropriate and age categorical when this helped to ensure the model fit.
Include Kaplan-Meier curves. IMPLEMENTED: Per the committee recommendation, Kaplan-Meier curves were produced to further examine the time to event analyses.
Summarize the median, range, and n-tiles of days (not just mean) to subsequent symptoms or procedures, including patients who did not have the event of interest.
IMPLEMENTED: Additional information about follow-up time and time to event was provided.
New/recurrent symptom timing may just be the next annual check-up for patients—good to point out that these procedures are not resulting in women having to go back to the doctor before this annual check-up.
IMPLEMENTED: Kaplan-Meier curves were produced that reflect the time to new or recurrent symptoms.
A window of > 7 days for subsequent procedures may not be enough—30 or 60 would be preferable; could do further sensitivity analyses.
IMPLEMENTED: The time window was increased to 60 days per review of the data and clinician recommendation.
Look at the distribution of subsequent procedures by index procedure.
NOT IMPLEMENTED: Agree that this would be interesting to look at and may be appropriate to discuss in manuscript.
Consider restriction to patients who are nonobese and have no comorbidities at baseline as additional analysis—to address the point that it might not really be a “treatment failure” in complex patients with multiple comorbidities to address their fibroids by multiple less invasive procedures in order to not put them at risk of a thrombotic event or other issues from more invasive procedures.
NOT IMPLEMENTED: We adjusted for these variables in the model, but, given the sample size, stratified analyses for patients without comorbidities were not feasible.
Is there anything more we can do to describe the experience of patients with no recurrence?
IMPLEMENTED: Survival curves were produced and additional text added to the report to highlight these patients.

83
Disclaimer:
The [views, statements, opinions] presented in this report are solely the responsibility of the author(s) and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute® (PCORI®), its Board of Governors or Methodology
Committee.
Acknowledgement:
Research reported in this report was [partially] funded through a Patient-Centered Outcomes Research Institute® (PCORI®) Award (CE-12-11-4430). Further information available at: https://www.pcori.org/research-results/2013/which-treatments-uterine-fibroids-
have-best-results