Embed Size (px)
Citation preview

THE COUNCIL FOR HEALTH
SERVICEACCREDITATION
OF SOUTHERNAFRICA
insi
de
�North WestProvince QualitySummit
�New Chief OperationsManager
�QI evolution in Free State Hospitals
� Injection safety
COHSASA HAS been working inthe field of quality improvement inSouth African healthcare facilitiesfor over 10 years. Part of theProudly South African movement,COHSASA has achieved globalrecognition and is one of only ahandful of internationally accreditedaccrediting bodies recognised bythe International Society for Qualityin Health Care (ISQua).
Since its inception, COHSASA hasfocused on providing South Africansolutions for South African problems.This has resulted in the developmentof facilitated accreditationprogrammes for South Africanhealthcare facilities that enablespecific identification of areas ofstrength and deficiency. Through aprocess of ongoing training,monitoring and evaluation, skillstransfer to local staff enables facilitiesto become accredited as centres ofexcellence for healthcare provision.
Because of the legacies of the past,many facilities in South Africa facesignificant obstacles in provision ofhealth care, including problems withfinance, physical infrastructure,medication and consumables supply,as well as staffing shortages. Toassist facilities to overcome thesedeficiencies and acting in responseto local needs, COHSASA developedthe graded accreditation process –unique in the world – that allows allfacilities in the country to accessworld-class accreditation processes
that are tailored to their specificrequirements. Responses to
these programmes over thelast decade have repeatedly
demonstrated the value of this localapproach in improving the delivery ofquality health care to all our citizens.
In the past ten years of operation,with COHSASA’s work in 595facilities in both the public andprivate sector, the followingmilestones have been reached:
� In 1994, the Pilot AccreditationProgramme for South AfricanHealth Services was launched as aresearch and developmentprogramme in the Faculty ofMedicine at the University ofStellenbosch under thedirectorship of Dr StuartWhittaker. The programme grewrapidly and, in October 1995,COHSASA was registered as anot-for-gain organisation.
� The first hospital to be accreditedin South Africa – the Medi-ClinicGroup’s Louis Leipoldt Hospital inBellville – was issued with a two-year COHSASA accreditationcertificate on June 1, 1995.
� The first public sector hospitalto be accredited – AddingtonHospital in Durban – was awardeda two-year accreditation onNovember 21, 1997.
� COHSASA signed the first majorcontract to accredit 29 publicsector hospitals in KwaZulu-Natalon November 12, 1998.
� In May 2002, COHSASA’sstandards were recognised by theInternational Society for Quality inHealth Care (ISQua) as meeting itsprinciples.
� In September 2002 COHSASAwas accredited by ISQua for fouryears. This is formal, worldwide
recognition that COHSASA meetsagreed international standardsspecifically developed and testedfor healthcare external evaluationbodies.
� In August 2004 COHSASAbecame the first organisation inthe world to undertake thedevelopment of standards for theevaluation and management of HIVand AIDS within a district andacross the continuum of care – fromprevention and VCT to terminal care.
(Continued on page 2)
While COHSASA’s 10 years have been marked
by triumphs and setbacks, it’s moments like these
when Wentworth Hospital in Durban celebrated itsaccreditation at the start
of the new millennium that linger forever…
We’ve come a long way
Mr Albert N Ramukumba,B.Dent.Ther (Hons), AMP(Manchester), PDH (UCT),
PG Dip. in HIV/AIDS(Medunsa), formerly Chief
Executive Officer of theHospital Association of South Africa (HASA),
has been appointed asChairperson of the
COHSASA Board of Directors.
Speaking soon after hiselection, Mr Ramukumba
said he believes in teamworkand aims to encourage fullparticipation from Board
members to carry COHSASAinto the future. �
May 2006
New Chairmanfor COHSASA
Coh
sasa
Bul
letin
In December 2005,windblown staffcelebrated COHSASA’s10th birthday in Cape Town.
2
North West Province
Quality SummitSENIOR OFFICIALS and hospital staff of the North West Province assembled at a hotel near Rustenbergduring the November 2005 Quality Month to take stock of service provision in their facilities.
The province has just completed its first contract with COHSASA. Eight of its hospitals earned ProgressAwards, seven received Entry Awards and one achieved an Intermediate Award. Klerksdorp/TshepongHospital was awarded a three-year accreditation and Witrand Psychiatric Hospital was accredited for twoyears.
The aims of the summit – Restoring Dignity through Quality Health Service – were to create a commonunderstanding and awareness of quality and quality assurance and to gain clarification of the role of qualityassurance and its relationship to other programmes initiated in the province. The rationale was to giveimpetus to QA activities and mark Quality Month in South Africa. COHSASA was invited to attend and gavefeedback on the status of the hospitals in the province participating in its programmes, and encouraged theinstitutions to continue with the process of quality improvement.
In his presentation, Dr Stuart Whittaker, CEO of COHSASA, said his organisation could assist the province toimprove the quality of health services provided to the public, but that the programmes were not a ‘magicbullet’. He said quality improvement is an investment over time and that if standards are to be fullymaintained and become ingrained in everyday hospital practice, the hospitals needed to make a long-termcommitment. �
FROM TOP� The two-day summit was hosted by Connie
Masiangoaka of the Quality Assurance Unit of theNorth West Province
� Enjoying a tea break were (from left to right):Salvation Baloyi, Matipi Kgaje, Esther Viljoen andEunice Abrams
� Participants broke into smaller groups to discussaspects of quality care
� Attentive audience in the main hall� Grissel Ncedana from COHSASA making friends� Key players at the Quality Summit
In 2005, the Council for Health Service Accreditation of Southern Africa celebrated a decade of involvementin quality improvement for healthcare facilities. A special dinner was held at a city restaurant afterCOHSASA’s Board meeting in November.
Those who attended this historic event were, from left (back row): Magda van Wyk from the Board of Healthcare Funders,Professor GJ van Zyl, Head of the School of Medicine in the Faculty of Health Sciences at the University of the Free State,Dr Shadrack Mazaza, member of the QUALSA Board of Directors (Clinical Governance Executive and Chairman of theClinical Governance Exco), Dr Louis Claassens, Director: Quality Assurance for the National Department of Health and FanieMaritz, COHSASA’s auditor.
Front row: Dr Helene Visser, Manager of Quality Assurance and Training for City Health in Cape Town, Professor MarieMuller, Dean of the Department of Nursing and Education at Johannesburg University, Dr Jill Hurst, Hospital Manager ofAddington, Mr Albert Ramukumba (Chairman), Dr Stuart Whittaker (CEO) and Dr Deon Moulder (Deputy Chairman).
Absent: Tevern Japhta from the South African Quality Institute.
COHSASA celebrates 10 years
� On December 17, 2004 COHSASA became an accredited member of the Proudly South Africancampaign.
� In January 2005 COHSASA assisted the World Health Organisation (WHO) to launch its WorldAlliance for Patient Safety in Durban, which aims to conduct studies around the world to determine thenature and the extent of adverse events in developing countries.
� In 10 years COHSASA has provided valuable input for global health bodies: it formed part of the JointCommission on Accreditation of Healthcare Organizations task team to develop healthcare standards;is part of the editorial team of the ISQua Journal; and regularly provides input for the World HealthOrganisation on issues of patient safety, quality assurance and accreditation. �
We’ve come a long way (Continued from first page)

3
FROM THE OFFICE OF THE CEO
IT IS DIFFICULT to fully comprehendthat a decade has gone by since theCouncil for Health ServiceAccreditation of Southern Africa firstregistered as a not-for-profitorganisation in 1995.
COHSASA has enjoyed its share ofboth success and disappointmentover the past 10 years and like allpioneers heading out on that rough,rocky road due West, there havebeen a number of obstacles alongthe way. Uncertainty has been partof this journey, but it has also beenthe reason why – at least it can nowbe said – that COHSASA does knowwhat works and what doesn’t, andbecause of the wisdom gained andimplemented, has made adifference to the quality of healthcare in Southern Africa.
Health facilities in COHSASA’squality improvement programme arenow beginning to meet internationalprofessional standards. In the publicsector, this has proved to be moredifficult than first thought. However,it is now known that with enabledand committed management inplace, it is possible for any facility(even those with poor resourcebases) to achieve accreditation.
To meet these specific challenges,two compensatory systems havebeen pioneered: facilitatedaccreditation and the gradedsystem of recognition. Instead ofleaving hospitals to their owndevices, COHSASA sends teams toassist with understanding andimplementing the standards andprovide training (in infection control,leadership, resuscitation, qualityassurance) in identified areas.
The graded system of accreditationmeans that instead of hospitals andclinics becoming despondent aboutnot meeting the standards first timeround, they are awarded certificatesat defined levels of progress (Entryand Intermediate) that encouragefurther participation until thequality assurance process becomesinstitutionalised and endemic, ratherthan viewed as an add-on at the endof a long day.
In this decade, it has becomeextremely clear that accreditation ismerely the “cherry on the top” andthat the most important componentof the COHSASA programme is thequality improvement process itself
and the maintenance of standards. Ithas become crucial to viewparticipation in an accreditationprogramme not as a “one-off” hitwith a magic bullet, but rather as along-term investment that pays hugedividends in terms of patient safety,credibility, avoidance of waste andminimisation of costly lawsuits.
In ten years, COHSASA haspositioned itself as only one of fourhealth accrediting bodies in theworld to be recognised as meetingthe competency requirements of theInternational Society for Quality inHealth Care Inc. (ISQua). COHSASA’sprofessional standards – derivedfrom the collective wisdom of 41countries around the world – havebeen gleaned and honed by localrepresentative bodies, tested locally,and have been officially recognisedas meeting the principles of ISQua.
COHSASA is a member of theProudly South African movementand has been invited to share what itknows about improving the qualityof health in the developing world onmany international podiums aroundthe globe. Our experience over timeon a wide range of issues thatimpact on accreditation and qualityassurance processes in our countryhas become a valuable asset.
Operations have increased ingeographical impact too, withCOHSASA now working in six of thenine provinces in South Africa, aswell as having contracts in Namibia,Botswana and Rwanda. The workhas taken place in 595 differentfacilities of all kinds in both theprivate and the public sector. Sets ofstandards have been developed forhospitals, clinics, and psychiatrichospitals, rehabilitation centres;sub-acute care centres andemergency services.
COHSASA has developed one of thehealth accreditation industry’s mostsophisticated computerised systemsto keep clients informed aboutprogress. The system providesfeedback which comprehensivelyoutlines and prioritises deficiencies,maps progress and tracks clientcommitment to the process ofimproving health care.
Reports generated are a valuablemanagement tool for facilities andoverseeing authorities because theyisolate and identify individual and
endemic weaknesses, trends thatendanger patient safety andpatterns of poor administration thatresult in waste and duplication.
After an intense and extensiveprocess, COHSASA has notched upa world first: the first set of standardsthat evaluate how effectively HIVdisease is being managed across adistrict with its component networkof hospitals, clinics, hospices andcommunity services. The HIV andAIDS District Evaluation Tool (HIV-DET) systematically evaluates thequality of HIV care provided to patientsin a geographically defined district.
Over the years COHSASA haspartnered with both local andinternational organisations toconduct research. These links havebecome the firm foundation leadingto further collaboration with majorplayers in global health such as theWorld Health Organisation.
COHSASA will soon be embarkingon a major infection controlimprovement programme with aninternational partner and thedevelopment of an adverse eventreporting system to improve patientsafety. These initiatives are part ofan international movement toimprove the current status of patientsafety throughout the world.
I am extremely grateful to all thosewho have participated in COHSASA’sfirst 10 years. Some of ourachievements have been quiteremarkable.
I would like to extend a thank you toall those who have believed – andcontributed to – the vision ofensuring that all Southern Africansreceive equitable and qualityhealthcare. The journey continues …
– Dr Stuart Whittaker
TERVERN JAPHTHA, actingCEO of the South AfricanQuality Institute in Pretoria, hasbeen formally appointed as aCOHSASA Board member. MrJaphta brings to the COHSASAboard business skills he learntwhile studying for a B.Admindegree (Public Administrationand Business Management) atthe University of Pretoria and aDiploma (Quality ManagementTechnician) from the College ofProduction Technology.
He has been with the SouthAfrican Quality Institutesince 2000, serving inseveral capacities includingmarketing, strategy, financialand personnel management,and corporate governance. Heis a member of the Boards ofDirectors of the South AfricanAuditors and TrainingCertification Association(SAATCA), the South AfricanExcellence Foundation and theUlwazi Ubuntu CC. Wewelcome him to COHSASA. �
New Board memberCOHSASA has madea difference to the
quality of health care inSouthern Africa
The CEO of COHSASA, Dr Stuart Whittaker

4
COHSASA appoints new Chief Operations ManagerJACQUI STEWART, a recognisedexpert in leadership at the mostsenior levels in the UK’s NationalHealth Service (NHS), has joinedCOHSASA as Chief OperationsManager.
Her return to this country (shegraduated as a nurse from theVictoria Hospital in Wynberg, CapeTown, in 1978, receiving the Awardfor Outstanding Achievement)constitutes a determined swimagainst the tide: coming back toinvest her global knowledge in adeveloping country when so manyother health professionals areleaving our shores.
“I have returned to South Africabecause there is a worthwhile jobthat needs doing and I hope I cancontribute something.The corporateethos I have found in COHSASAmakes me believe I have found theright organisation in which topractise those values I believe in –honesty, integrity, and doing thebest I possibly can with that which isavailable,” she says.
In February and April 2005Ms Stewart visited Mpumalangawith a team from the UK. Her briefwas to provide leadership andmanagement input into theCOHSASA Health ExecutiveDevelopment Programme for CEOsand medical, nursing andadministrative managers. The teamwent on a reconnaissance trip to theRob Ferreira and Shongwe hospitalsbefore conducting the training atregional centres.
These on-site visits are part ofMs Stewart’s firm belief that onecannot develop people withoutunderstanding the context theywork in and the challenges that gowith it. For example, when she waswith the East Kent Health Authorityshe took the trouble to go into thefield for home visits with the doctorsin the early hours of the morning onthe Sunday of a Bank Holidayweekend. In this way she couldunderstand the conditions theywork under and match it with thenecessary support and, wherepossible, resources.
A substantial part of the trainingmethod used in Mpumalanga wasparticipation and using actualexperiences to bring theory to life.This was a deliberate course of
action because her observations ledher to conclude that mostparticipants were used to lecturesand conferences only.
“We needed to get people to take anactive interest in their own learningprocess and asked them to submitevaluations on what they had learnt.It was extremely rewarding for mewhen one particularly pessimisticindividual sent back an evaluationsaying that while he had notanticipated learning much from theexercise, he had indeed learnt agreat deal to take with him into thenext phase of his career,” she says.“We also asked the leaders to take asingle COHSASA standard andwork as a team on a project toimprove that standard within theirhospital. The results were great witha tangible enthusiasm to share whatthey had done.”
Before returning to SA, Ms Stewartwas the Programme Director(Director of Career Developmentand Succession Planning) at theLeadership Centre of the NHSModernisation Agency.
She has occupied many keypositions in NHS organisations overthe years, including Senior Nurse inthe Harefield Hospital TransplantUnit, Director of Primary CareDevelopment for East Kent FamilyHealth Services, PerformanceDirector for the East Kent HealthAuthority, Project Director for theKent and Medway HealthAuthority, as well as organisational
development andleadership lead forthe Directorate ofHealth and SocialCare in the Midlandsand the east ofEngland.
Currently studyingfor her Doctorate inProfessional HealthStudies at Middlesex
University, Ms Stewart believes thathealth management should ensurethat people have what they need todo the job. They also need tounderstand the value one brings as amanager to support those givingdirect patient care.
“I enjoy developing the capacity andcapability of people, finding thetalent and watching it grow. Here inSouth Africa, it will be about sharingmy knowledge with COHSASA staffand helping health managers whohave gone through the COHSASAprogramme to manage and lead,reach their goals and grow,” shesays.
She will also be helping to trainfacilitators and extending the HealthExecutive Development Programmein the provinces where COHSASAworks. Her ultimate and ideal goal,however, will be to “work herself outof a job” in the sense that capacityand capability will have increased toan extent where developingleadership will be on everyone’sagenda.
With an outlook fired by a healthybalance between idealism andrealism, Ms Stewart has a strongbelief in the human ability totranscend the limits of educationand environment.
“I do not believe all leaders are born.I believe they can be developed. Weneed leaders in all spheres of anorganisation, not just at the top. Trueleadership is having vision and the
skills to motivate others. A leaderwill guide people to a goal and givethem enough space to achieve it ontheir own,” she says.
She will also take over the day-to-day operations of COHSASA fromCEO Dr Stuart Whittaker so that hewill be able to spend more time onplanning, strategy and researchprojects.
Who else – in the space of onemonth – could change jobs, changecountries, become part of thesenior management team of anorganisation, return to the countryshe has just left (the UK) for awedding, skip across to America,move house, get a banking accountin SA and host a family forChristmas … all with the tranquildemeanour of Mona Lisa on Valium?
Obviously someone very special. �
The corporate ethos I have found in COHSASAmakes me believe I have found the rightorganisation in which to practise those values I believe in – honesty, integrity, and doing the best I possibly can with that which is available
Jacqui Stewart, the new Chief Operations Manager
"Quality in health care can be defined asmeeting agreedstandards thatdefine theexpectations ofhealth careprofessionals,patients andthe community"Dr Stuart Whittaker, 2005
5
THE COUNCIL FOR Health Service Accreditation of Southern Africa wasfounded in 1995 with the mission to empower Southern African healthcarefacilities to deliver quality, cost effective and compassionate care through anintegrated quality improvement and accreditation approach.
Accreditation is a formal process by which a recognised organisation assessesand certifies that a healthcare facility meets applicable, predetermined,published standards. These standards are regarded as optimal andachievable. They are also designed to encourage continuous improvement ofpatient care. Accreditation is a voluntary process in which healthcare facilitieschoose to participate rather than be coerced by legislation.
ISQua (the International Society for Quality in Health Care) in 2002recognised the COHSASA standards as complying with internationalprinciples. There are 45 countries that have healthcare accreditationorganisations, of which only four have current international accreditation.
1. South Africa – COHSASA 2. Australia – ACHS 3. New Zealand – NZCHS4. Canada – CCHSA
Health care funders and consumers are applying pressure on healthcareproviders to prove that they deliver quality patient care. Hospital performancemeasures and quality improvement methods are complex interventions andnot easy to evaluate.
COHSASA standards provide a mechanism for healthcare facilities to structureand implement quality improvement methodology. Avedis Donabedian, thefounder of healthcare quality assurance, defined the following categories thatshould be assessed to evaluate and improve patient care:
1. Structure: Resources to deliver care and equipment - Credentials of doctors- Infrastructure- Standard procedures
2. Process: The care itself- How the diagnosis is made- Which procedures are performed- What medication is used
3. Outcomes: The valued results of care- Life enhancement- Relief of suffering- Satisfied consumers
The accreditation standards provide thefoundation to develop a structure that can beapplied to the whole hospital, i.e. non-clinicalas well as clinical services. This must be seenas a holistic approach to enable management,administration and patient care professionalsworking as a multi-disciplinary team toproduce good patient and businessoutcomes.
An organisation cannot be successful incontinuous improvement without laying thefoundation of the quality system, i.e. structure.Business and clinical process will be effective ifthe structure is sound and this will result in thedesired outcomes.
It is for this reason that COHSASA hasbecome an essential part of qualityassurance in the healthcare business. �
– DW Moulder, Acting Chairman of the Board of COHSASA, November 2005
A DELEGATION OF COHSASA senior staff visited the DeputyMinister of Health, Ms Nozizwe Madlala-Routledge, at heroffices in Parliament to present a review of COHSASA’s work inSouthern Africa to date. The presentation outlined commonproblems encountered in public sector hospitals and howstandards have been developed to manage HIV within all servicepoints in a district.
From left, Dr Morris Mathebula, programme manager of the HIVand AIDS District Evaluation Tool (HIV-DET), Dr Stuart Whittaker,CEO of COHSASA, Ms Nizizwe Madlala-Routledge, Mr GerardLocke, healthcare technology management consultant forCOHSASA, and Ms Grissel Ncedana, Chief Facilitator ofCOHSASA. �
COHSASAvisits Deputy Minister of Health
MESSAGE FROM THE ACTING CHAIRMAN AT 10-YEAR CELEBRATION
Dr Deon Moulder, the Acting Chairman,pictured at COHSASA’s10th birthday. He is also a director ofthe Medi-Clinic PrivateHealth Care Group.

6
Representatives of Addington Hospital crowded into the auditorium in 2002 tohear what they were letting themselves in for the second time around.
ADDINGTON HOSPITAL IN Durban, KwaZulu-Natal, has beenaccredited by COHSASA for a second time.
Attending the ceremony to present the certificate, Dr Stuart Whittaker,CEO of COHSASA, said the occasion affirmed a cherished notion forhim that, “given sufficient support and encouragement, health care inSouth Africa’s public sector can be transformed to meet the increasingdemands of a society having to grapple with serious public healthconcerns: the AIDS pandemic, TB, malaria and many other chronicillnesses.”
He said he found the professional level of Addington’s participation inthe accreditation very encouraging, as they have a firm grasp of thequality improvement concept.
“It means that this hospital has reached – and I hope will continue toreach – quality standards approved not only by all the relevantprofessional bodies in South Africa but also by ISQua – theInternational Society for Quality in Health Care – an organisation thatrepresents some 30 countries around the world,” said Whittaker.
On its journey to quality, Addington Hospital has brought about manyimpressive improvements. At ground level, several programmes are inplace that have won awards, including a patients’ complaint andcompliments audit; an in-house preventative maintenanceprogramme; a 24-hour rotating equipment pool and a preventativeprogramme for occupational exposure to HIV.
On November 21, 1997 Addington Hospital became the first publicsector hospital to receive a COHSASA accreditation certificate,remaining accredited for two years until 1999. There was a time lapsebetween programmes, and the hospital re-entered the accreditationprogramme in October 2002. Addington has now received a secondaccreditation award, valid until March 2007, making it one of the firstpublic sector hospitals to receive a second COHSASA accreditation onre-entry into the programme.
In 2000 and 2001 the hospital won a silver medal in the Premier’sand Price Waterhouse Coopers Awards for Good Governance. In2001, it achieved the Best Practice award for a needle-stick injuriescontribution to a preventive programme for occupational exposure toAIDS, and in 2002 scooped the Gold Medal for the Premier’s andPrice Waterhouse Coopers Good Governance Award. �
Addington Hospitalcelebrates its second COHSASAaccreditation
WHEN I WAS appointed as Clinical Manager for Witrand Hospital in theNorth West Province, one of my first observations was the high epilepsy rateat the facility. This obviously carried the potential for serious adverse eventsgiven the disease profile of the inpatient population.
Witrand Hospital is a 1152-bed mental health institution rendering servicesto three broad disease groups treated in a 60-bed psychiatric unit, a 15-bedphysical medicine and rehabilitation unit and 1077 beds for mentallyretarded patients.
It was clear that in trying to address the problem of an unacceptably highseizure rate (specifically in the mentally retarded section), a few qualityimprovement processes would have to be used to identify the root cause orcauses. Through a series of corrective measures we hoped to achieve adecrease in the rate of seizures.
These processes included development of a Quality ImprovementProgramme (QIP), an analysis of patient profiles regarding the diagnosis ofepilepsy as part of their mental retardation, as well as the daily data ofepileptic seizures.
This data needed to be evaluated against best practice epilepsy diagnosisand management policy (clinical audit) with root causes identified andaddressed. These root causes include incorrect doses or non-administrationof anti-epileptic drugs, mentally retarded patients not swallowing their drugsand co- morbidity of other diseases.
It was necessary to undertake in-service training for all stakeholders toensure a common understanding of the diagnostic features and treatmentregimes of different epileptic syndromes. Furthermore, all staff received in-service training regarding the diagnosis and management of epilepsy andbest practice guidelines.
Theuns Oosthuizen - Clinical Manager at Witrand Hospital
in the North West Province
QIPresults in lowerepilepsy rateBy Dr Theuns Oosthuizen, ClinicalManager at Witrand Hospital
Delegates have a tea break

IN A DEVELOPMENT that may have a considerable impact on the quality of health care delivered to the people of theEastern Cape, the province’s Department of Health has entered 23 facilities into the COHSASA quality improvementand accreditation programme.
Among these facilities – which include four major hospital complexes, psychiatric hospitals and district hospitals – arehospitals that are part of the National Department of Health’s revitalisation programme.
Under the supervision of Dr BN Mjamba-Matshoba, Chief Director of the Quality Health Care Assurance SystemsDirectorate of the Eastern Cape, the province joins several other regions across the country in a drive to meet basicbest practices and improved standards of health care as envisioned in the National Department of Health’s keystrategic objectives.
“In our experience, a long-term investment in continuous quality improvement and accreditation leads to improvedpatient care. The COHSASA programme has proved to be an appropriate management tool that – if picked up andused – empowers health facilities to provide a safer and better service to its patients,” says Dr Stuart Whittaker, CEOof COHSASA. �
7
� The first step was to captureelectronic data of all 850inpatients, identify epileptic patientnumbers and the frequency ofseizures. This revealed that 33% ofpatients at Witrand Hospital wereepileptic and that the initialepilepsy rate was 19,1%.
� The second step was to develop abest practice guideline for thediagnosis and management ofepilepsy. Available best practiceguidelines were researched on theInternet from worldwide sourcesand a guideline was developed.
� A clinical audit form was thendesigned and completed for everypatient who had an epilepticattack. This was analysed by theClinical Manager’s office againstthe best practice guideline and aroot cause identified.
� A number of causes emerged,ranging from systems failures topatient co-morbidity factors andstaff error. These were addressedin order of priority.
� At the time, the institution usedseparate medication prescriptionand administration systems,which resulted in nurses having totranscribe scripts to administerprescribed medication. Thissystem could lead to errors.
� Doctors customarily would onlyprescribe chronic treatment onceevery three months. To ensure thatprescriptions were not outdated,all 850 chronic medication scriptswere captured electronically andthe format changed to aprescription as well as 31-dayadministration format. This wasprinted monthly, checked by
doctors and re-signed or adaptedif applicable. Copies were handedover to dispensary.
� It was then identified that stockissued in bulk to the wards ledto incorrect administration(evidenced by clinical audit andrepeated blood levels of anti-epileptic drugs making no sense).This systems-related problem wassubsequently corrected throughimplementation of a pre-packeddosette dispensing system via thepharmacy. Wards with the highestnumber of epileptic patients weregiven first priority.
� Other causes for the patient to havefits, i.e. the possible side effects ofanti-epileptic drugs and thedevelopment of hyponatremiaassociated with the syndrome ofinappropriate antidiuretic hormonesecretion (SIADH) with electrolytedisturbances, were identified via fullblood counts and electrolyte tests.In certain patients the choice of ananti-epileptic drug was changed.
� Night duty staff allocations wereadjusted to create higher levels ofsupervision and decrease theworkload of the professional nurseswho rotated through the wards in aneffort to administer all medication.
The above-mentioned actionsresulted in a drop in the epilepsyseizure rate from 19,1% of all epilepticpatients at the start of the qualityimprovement programme to only1,5% of patients for the third quarterof the 2005/2006 financial year.
It definitely had other positiveoutputs regarding the quality of lifefor some patients: a decrease in the
number of after-hour consultationsfor epileptic fits and a decrease inmedication for the treatment ofacute seizures.
It was a learning experience for theteam who developed andimplemented the QIP. They did nothave all the knowledge in thebeginning but by implementing anumber of quality improvementprocesses after identifying aproblem and its cause, they realisedthat systems are often the culprit.
Systems in health need people toimplement them and thusmotivation and continuing in-service training is a daily task. Weused a multi-professional teamapproach and it resulted in anoverall organisational achievement.
This QIP is an example of the qualityimprovement spiral that works tothis day. We focused on the patient,implemented quality improvementthrough teamwork, understoodsystems and processes and re-organised them where necessary,used the best available information,did not ignore the human element,and now we can celebrate becausewe see the effect of this QIP inpatient care daily.
To ensure sustainability, all epilepticfits are monitored daily. Root causesfound are addressed with warddoctors and staff. It has become aningrained part of the ward round. Mysincere thanks go to all my colleaguesand staff who were part of this QIPand who sustain it to this day. �
Eastern Cape implements anational imperative
Eastern Cape enters the COHSASA
PROGRAMME
The following hospitals in theEastern Cape have enteredinto the COHSASA FacilitatedAccreditation Programme:
�All Saints Hospital �Bedford Orthopaedic Hospital�Bisho Hospital �Cecilia Makiwane Hospital �Dora Nginza Hospital �Fort England Hospital �Frere Hospital �Frontier Hospital �Grey Hospital �Komani Hospital �Livingstone Hospital �Madwaleni Hospital �Nelson Mandela AcademicHospital �PE Provincial Hospital �Rietvlei Hospital �St Barnabas Hospital �St Elizabeth's Hospital �St Lucy's Hospital �St Patrick's Hospital �Taylor Bequest Hospital �Umtata General Hospital �Umzimkulu Hospital �Zithulele Hospital
Once accredited, each of thehospitals will receive twomaintenance visits (one peryear) to ensure that standardsare sustained. The audits willfocus on high-risk areas withinthe hospitals identified duringthe implementation of theFacilitated AccreditationProgramme and a randomisedassessment of all areas todetermine the degree to whichthe standards have beenmaintained and/or improved.
8
COHSASA’s uniqueassets�COHSASA has spent the past ten years researching and developing quality
improvement and accreditation programmes specifically designed forSouth African healthcare facilities.
�COHSASA is the only healthcare-accrediting organisation in South Africaaccredited by the International Society for Quality in Health Care (ISQua).
�COHSASA has developed standards in collaboration with local professionalbodies to ensure they constitute a blueprint for excellence.
�Our 6th edition of Hospital Standards is recognised by the InternationalSociety for Quality in Health Care as meeting its principles.
�COHSASA has a unique computerised information system to ensure anobjective, scientific scoring of standards compliance within hospitaldepartments, in hospitals overall and across hospitals within specificdistricts and regions.
�COHSASA has developed a multi-tiered reporting system that providesvaluable information for hospitals and regional, provincial and nationalmanagers.
�Quality Improvement Programmes are developed in response to customerneeds.
�We are a Proudly South African NGO committed to capacity building andempowerment.
�We are affiliated to the South African Quality Institute as its only healthcarepartner.
�COHSASA has wide national and international networks and works closelywith the World Health Organisation, the Joint Commission on Accreditationof Healthcare Organisations, the International Society for Quality in HealthCare and the German Society for Technical Co-operation – Die DeutscheGesellschaft für Technische Zusammenarbeit (GTZ) GmbH.
�We have multi-disciplinary standards, revised every two years, for hospitals,clinics, step-down facilities and HIV district management that are ablueprint for excellent practice and the optimal use of resources.
�The COHSASA system is a valuable management tool for hospitals,provincial services and national services.
�The COHSASA programme can be used by the National Department ofHealth, provincial health services and private hospital groups as asurveillance tool (we can monitor a whole discipline, e.g. infection controlor resuscitation).
�Ours is a scientifically validated quality improvement training programme.
�We can call on a trained team of medical and academic experts.
�Over the last 10 years, we have developed world-class instruments andtools specifically tailored for the South African environment.
MissionTo empower Southern African healthcare facilities to deliverquality, cost-effective and compassionate care through anintegrated quality improvement and accreditation approach
VisionTo enable all Southern Africans to receive equitable andquality health care
IT IS PART OF the uplifting history of the Free State that five of the firstbatch of 12 hospitals that entered into the COHSASA programme in2001 achieved accreditation awards – this represented the highestpercentage accreditation score achieved by any province in the country.
The hospitals that did not achieve accreditation were given either Entryor Intermediate pre-accreditation awards from the portfolio ofCOHSASA’s Graded Recognition programme and the drive for qualityhas been continuing ever since.
Mr Shadrack Shuping, ExecutiveManager of the Free StateDepartment of Health, has saidthat the subsequent decision bythe Department to enrol all 31hospitals in the COHSASAprocess was inspired by itsdesire to maintain a sustainablelevel of quality hospital servicesin the province.
“Quality services for usmeans improved patientsafety, comprehensive riskmanagement, the cost-effectiveuse of resources and clientsatisfaction. We are excitedthat we are achieving the resultswe are: they are the sweet fruitsof hard labour.”
Henna van Zyl, Manager of theQuality Assurance Directoratefor the Free State ProvincialHealth Department, says thedecision was taken some timeago to take action to addressthe quality of public healthcarein the province. After examiningseveral options, the departmentchose to go the internationallyaccepted accreditation route.
“We now have policies and structures in place that are key tomaintaining high standards of quality healthcare,” says van Zyl. “Duringthe accreditation process, a lot of team building has taken place. Therehas also been a lot of development in the hospitals and among thepersonnel, which has not been restricted to management andmanagement processes, but is reflected across all categories of staff.”
Dr Stuart Whittaker, CEO of COHSASA, says that the Free Stateprovincial government has clearly demonstrated a commitment todeliver the highest possible standards of quality healthcare to membersof the public.
He pointed out, however, that some of the hospitals’ accreditationcertificates have lapsed and that it was “really important” that thesehospitals re-enter the programme. “Without ongoing external vigilancethat inspires staff to meet and maintain standards there is a humantendency to let things slip. Facilities need to be motivated by theknowledge that external audits take place regularly. Part of COHSASA’sstrength is that it helps hospitals to maintain standards over time. It isimportant to build on improvements that have been built up over timeand to sustain the momentum.”
The accreditation certificates of two of the five hospitals - BonganiRegional in Welkom and Nala District in Bothaville have recentlyexpired but the Free State Psychiatric Complex, Universitas Academicin Bloemfontein (previously accredited from 1997 to 1999) and theMafube District in Frankfort hold their accreditation certificates untilNovember this year.�
All roads lead to ...This is one of the mostfrequent signs that COHSASAfacilitators see when theytravel on the dusty bywaysand back roads of SouthAfrica. Dirkie van Jaarsveld,one of our facilitators whooften finds herself in remoteparts of the country, capturedthis one with a graffiti qualityimprovement solution: Fix it.
QI evolution in Free State Hospitals

9
COHSASA HELD AN executivetraining course for MpumalangaDepartment of Health hospitalmanagers and administrators at WhiteRiver in the last quarter of 2005 – thethird of similar workshops held thisyear. Aspects of the training courseincluded an outline of various qualityimprovement concepts, the difficultiesinvolved in implementing suchprogrammes, guidance onestablishing infection control and riskassessment programmes, and areas ofconcern about health and safety andhealthcare technology management.
CEO of COHSASA, Dr StuartWhittaker, outlined progress frombaselines in the Mpumalangahospitals and the areas that needfurther attention. Participants wereasked to outline why some hospitalsdo better than others, why hospitalsfind it difficult to meet the standardsand what can be done to improvethe current situation. The interactivesession resulted in valuablefeedback: including the fact thathospitals that do well in theCOHSASA programme havecommitted, motivated managerswho build team spirit.
Reasons given for the difficultiesexperienced by some hospitals inmeeting the standards included lackof understanding of the programmeby both managers and staff or thewrong attitude or approach towardsthe programme. Many staff felt thatit increased their workload and that
it was difficult to replace deep-seated, bad habits with new ones.Some of the solutions offeredincluded the notion of identifying“champions” of quality andappointing quality co-ordinatorsat facility level to drive the processforward. There were alsosuggestions that special time slotsshould be assigned for staff todedicate to the programme and thatstaff should be sensitised to useCOHSASA standards as part of theireveryday duties.
A presentation on the preventionand control of infection by LynRayment, head of COHSASA’sStandards Development andTraining, was followed by anothergroup session in which theparticipants were asked to identifyareas of potential infection risks intheir institutions. Delegates werecharged to return to their institutionsand undertake risk assessmentsbefore documenting comprehensiveinfection control programmes fortheir hospitals.
Gerard Locke, COHSASA’s clinicalengineer, presented areas of generalconcern about health and safety andhealthcare technology management.This was followed by another groupsession where participants wereasked to identify deficiencies withintheir institutions that could presentproblems with regard to health andsafety in general, deficiencies thatcould be in direct contravention ofany of the relevant Acts of Parliamentor other regulations, standards,guidelines, etc and any otherproblems that could present risks tothe patients, staff and visitors or tothe institutions themselves.
Evaluation results revealed thatparticipants’ perception of theworkshop was very positive. Threefurther workshops for hospitalmanagers and Mpumalanga districthealth staff are set for the future.
Presenters were: Dr StuartWhittaker (CEO of COHSASA), MrsLyn Rayment, head of StandardsDevelopment and Training, MrGerard Locke, COHSASA’s ClinicalEngineer and Ms G Ncedana,COHSASA’s Chief Facilitator. �
COHSASA trains health executives in Mpumalanga
COHSASA Standards Developer, Mrs Lyn Rayment, has a well-earned cup of teaduring the training of Mpumalanga health managers.
FULL-TIME AND part-timefacilitators attended a stafftraining session at the COHSASAhead office in December 2005.In addition to training sessionsheld in August and April, this two-day training workshop includeddiscussions on challenges facedin the field, new sets of standardsand amendments to existingones.
Also up for review were thespecial requirements forCOHSASA standards thatevaluate management of HIVacross the spectrum of care (HIVDistrict Evaluation Tool), anintroduction to the NDOH HealthCharter, and reviews of staffpolicies as well as the processesthat apply to facilitators’operations. These included anupdate on the refinements todatabase reports that will helpfacilitators to monitor the degreeof an institution’s performanceand commitment to theprogramme, and the consistentapplication of criteria scores.
Dr Stuart Whittaker, CEO ofCOHSASA, said that thefacilitators’ workshops weresignificant events in thecompany’s annual activitiesbecause they gave all staff – boththose based at head office andthose in the field – the opportunityto review their activities andconsider improvements wherethey might apply.
“We deal with issues facilitatorsexperience in the field and findsolutions. We are not justconsultants. We prioritisedeficiencies for our clients so theycan use our programme as amanagement tool,” he said.“Armed with the information wegive them, hospitals areempowered to makeimprovements inthe best possibleorder and therebyachieve maximumeffect.” �
FROM TOP LEFTPart of the facilitator training programmefeatures a healthy debate aboutreaching consensus as to whether acriterion is compliant or not.
A group of COHSASA facilitators provideinput into the Charter of the Public andPrivate Health Sectors for the NationalDepartment of Health.
FACILITATOR TRAINING
a central operationat COHSASA

10
Is the Mpumalanga Department of Health
turning a corner?
Last month, the nursing sister incharge of infection control atWitbank Hospital, Ms Nkobo Kobeli,discovered three positive cases ofKlebisiella infection. She pickedthese up during regular surveillanceof laboratory results and bymonitoring trends in woundinfection as required by COHSASA’sstandards. She immediately beganan intensive ‘manhunt’ for the culprit– an organism that was causing adisturbing rate of wound sepsis andspiking temperatures amongC-section patients in the post-natalwards.
Backing her all the way andencouraging her efforts was theCEO of the complex of threeMpumalanga hospitals (Witbank,Bernice Samuel and Impungwe),Dr Juliet Mannya.
Using an infection preventionapproach as defined in COHSASA’sstandards, Miss Kobeli isolated theaffected patients and took throatand nasal swabs from a sample ofthe staff and patients. She tookenvironmental swabs from thedarker corners of the hospital andfrom theatre instruments andcleaning cupboards – all the placesthat featured in her risk assessment
as to where the Klebsiella was likelyto be colonising.
She closed down the affected wardand set up an intense systemisedcleaning programme – a difficulttask given the perennial problem ofstaff shortages.
New patients were admitted to aclean, isolated ward while the post-natal ward was being scrubbed out.She then broadened her search toinclude the neonatal wards, the babyroom and the labour wards. Shechecked the theatres for rats,although she did not find any. Sheexamined the records of all patientswith septic wounds to establish anincidence rate. She created separateareas for wound dressings, wherenew patients were treated from adressing room and infected patientswere treated at their bedsides.
After a long, hard search – andwhen she had found one personwhose hands contained thebacteria – she immediately beganher battle plan. She galvanised keystaff to oversee a hand-washingcampaign in all suspect areas of thepost-natal wards, the labour wards,the CSSD and the operating theatre.Then she embarked on a drive toensure that all professional, cleaning
staff and visitors wore the correctprotective clothing such as gowns,head covers, gloves and masks.
She rallied her ‘link’ infection controlnurses (manning every ward andrecently trained in infection control) toensure that stocks for hand washing –soap, clean towels and sparklinghand basins – were available. Thenshe monitored the results.
By mid-February, although she wasstill hunting for the actual source ofthe Klebsiella bacteria, the number ofseptic cases had dropped from 90%of post-natal caesarean cases to20% and, arguably, lives had beensaved.
Dr Juliet Mannya, overseeing CEOof the Witbank, Impungwe and theBernice Samuel hospitals said,“COHSASA came into our liveswhen we needed it most. What thisorganisation brings is work that weshould be doing already: thesequality improvement processes andthe actions that flow from them
should be an integral part of ourdaily routine. The drive to improvequality brings with it the opportunityto document our difficulties,prioritise our actions and then dosomething about it,” said DrMannya. “Too often we hear theplaintive comment that our staffhave a ‘low morale’. It is true that ourstaff feel overwhelmed at times, butusing the quality improvementmethodology we can do things right– the first time, the right way. It istime to meet the challenge head onand to move ahead. COHSASA hasgot the toolbox that will assist us todo so”. �
AFTER A SPATE of negative publicity, the Mpumalanga Department of Health may be turning a corner: some ofthe hospitals have set up quality improvement projects that are delivering positive results for patients and savingtaxpayers’ money.
The changes in these hospitals – known as quality improvement projects – have come about because ofrequirements for compliance with professional standards in the programme administered by the Council forHealth Service Accreditation of Southern Africa (COHSASA).
Dr Keith Michael, Chief Director of Hospital Services for theMpumalanga Province, says that from his perspective at the provinciallevel, the greatest advantage of the COHSASA programme is its poweras an objective monitoring instrument.
“Although we knew that some hospitals were performing better thanothers, we had no way of monitoring progress or decline, objectively,”he said. “The programme has clearly identified those hospitals thatrequire special attention and support from district and/or provincialoffice level.”
The Mpumalanga Department of Health has entered 26 hospitals intothe COHSASA Facilitated Accreditation Programme. The full extent ofthe hospitals’ achievements and progress will be known in the nearfuture when they undergo an evaluation survey to establish what levelsof compliance they have reached with professional standards.
Champions of Quality in Mpumalanga… (from left): Dr Juliet Mannya, CEO of theWitbank, Impungwe and Bernice Samuel Complex, Josh Motlhamme, Director ofNkangala District Health, Andre Hansen, Principal Pharmacist at Bernice SamuelHospital and Miss Nkobo Kobeli, sister in charge of Infection Control at WitbankHospital.
WITBANK HOSPITAL reports ...
11
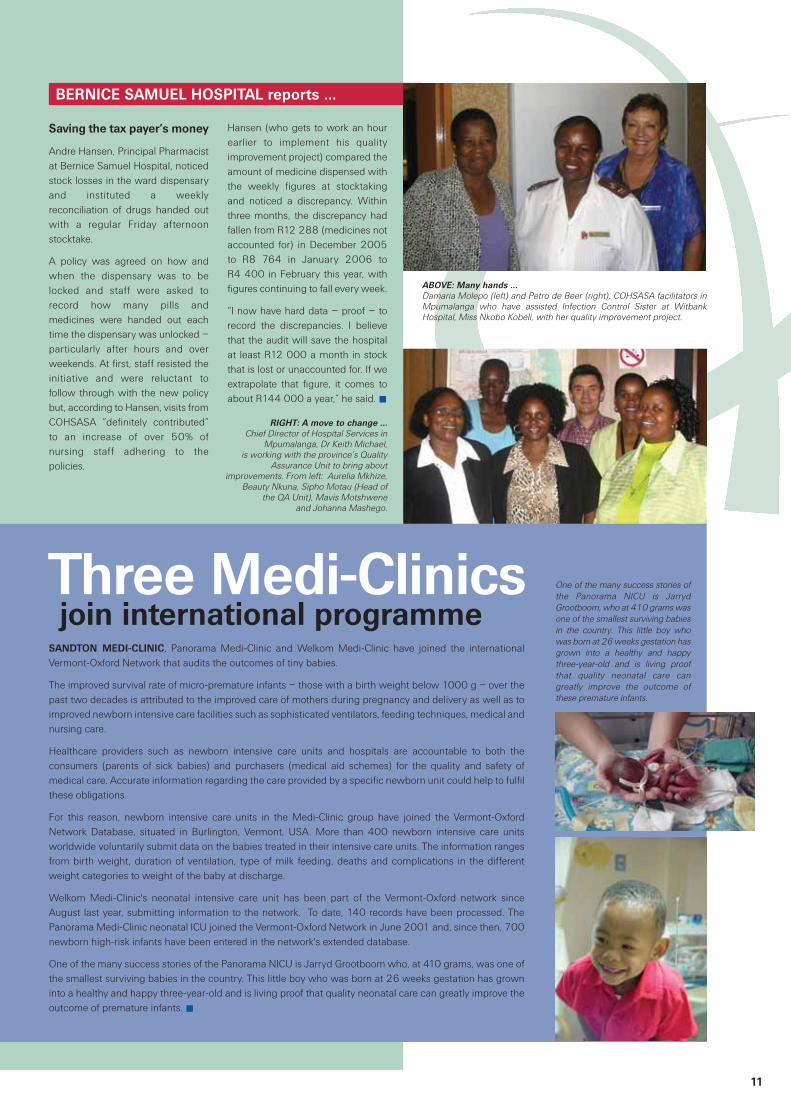
join international programmeThree Medi-ClinicsSANDTON MEDI-CLINIC, Panorama Medi-Clinic and Welkom Medi-Clinic have joined the internationalVermont-Oxford Network that audits the outcomes of tiny babies.
The improved survival rate of micro-premature infants – those with a birth weight below 1000 g – over thepast two decades is attributed to the improved care of mothers during pregnancy and delivery as well as toimproved newborn intensive care facilities such as sophisticated ventilators, feeding techniques, medical andnursing care.
Healthcare providers such as newborn intensive care units and hospitals are accountable to both theconsumers (parents of sick babies) and purchasers (medical aid schemes) for the quality and safety ofmedical care. Accurate information regarding the care provided by a specific newborn unit could help to fulfilthese obligations.
For this reason, newborn intensive care units in the Medi-Clinic group have joined the Vermont-OxfordNetwork Database, situated in Burlington, Vermont, USA. More than 400 newborn intensive care unitsworldwide voluntarily submit data on the babies treated in their intensive care units. The information rangesfrom birth weight, duration of ventilation, type of milk feeding, deaths and complications in the differentweight categories to weight of the baby at discharge.
Welkom Medi-Clinic's neonatal intensive care unit has been part of the Vermont-Oxford network sinceAugust last year, submitting information to the network. To date, 140 records have been processed. ThePanorama Medi-Clinic neonatal ICU joined the Vermont-Oxford Network in June 2001 and, since then, 700newborn high-risk infants have been entered in the network's extended database.
One of the many success stories of the Panorama NICU is Jarryd Grootboom who, at 410 grams, was one ofthe smallest surviving babies in the country. This little boy who was born at 26 weeks gestation has growninto a healthy and happy three-year-old and is living proof that quality neonatal care can greatly improve theoutcome of premature infants. �
One of the many success stories ofthe Panorama NICU is JarrydGrootboom, who at 410 grams wasone of the smallest surviving babiesin the country. This little boy whowas born at 26 weeks gestation hasgrown into a healthy and happythree-year-old and is living proofthat quality neonatal care cangreatly improve the outcome ofthese premature infants.
Saving the tax payer’s money
Andre Hansen, Principal Pharmacistat Bernice Samuel Hospital, noticedstock losses in the ward dispensaryand instituted a weeklyreconciliation of drugs handed outwith a regular Friday afternoonstocktake.
A policy was agreed on how andwhen the dispensary was to belocked and staff were asked torecord how many pills andmedicines were handed out eachtime the dispensary was unlocked –particularly after hours and overweekends. At first, staff resisted theinitiative and were reluctant tofollow through with the new policybut, according to Hansen, visits fromCOHSASA “definitely contributed”to an increase of over 50% ofnursing staff adhering to thepolicies.
Hansen (who gets to work an hourearlier to implement his qualityimprovement project) compared theamount of medicine dispensed withthe weekly figures at stocktakingand noticed a discrepancy. Withinthree months, the discrepancy hadfallen from R12 288 (medicines notaccounted for) in December 2005to R8 764 in January 2006 toR4 400 in February this year, withfigures continuing to fall every week.
“I now have hard data – proof – torecord the discrepancies. I believethat the audit will save the hospitalat least R12 000 a month in stockthat is lost or unaccounted for. If weextrapolate that figure, it comes toabout R144 000 a year,” he said. �
BERNICE SAMUEL HOSPITAL reports ...
ABOVE: Many hands …Damaria Molepo (left) and Petro de Beer (right), COHSASA facilitators inMpumalanga who have assisted Infection Control Sister at WitbankHospital, Miss Nkobo Kobeli, with her quality improvement project.
RIGHT: A move to change …Chief Director of Hospital Services in
Mpumalanga, Dr Keith Michael, is working with the province’s Quality
Assurance Unit to bring aboutimprovements. From left: Aurelia Mkhize,
Beauty Nkuna, Sipho Motau (Head of the QA Unit), Mavis Motshwene
and Johanna Mashego.

12
Dr RoseMulumba,
Country Directorof the JSI
Research andTraining Institute,
who has beenvisiting
COHSASA
COHSASA teams up to improveinjection safety
The COHSASA BULLETIN is designed to obtain feedback from ourclients, the public and other stakeholders on information in thisnewsletter, as well as to find out what you would like to read about.
While it is principally an information source on the work that COHSASA is doing in sub-Saharan Africa toimprove health care in both the public and private sectors, your thoughts and views on issues of qualityimprovement, accreditation and the subjects at hand are welcome.
If you wish to subscribe to the COHSASA BULLETIN, kindly access the subscription order form on our websiteat www.cohsasa.co.za
Address all other comments, complaints, letters and feedback to [email protected] Tel: +27 21 531 4225
EDITOR: Marilyn Keegan SUB-EDITOR: Carol BalchinPROOF READER: Paddy O’Leary
COHSASA WAS INVITED to attenda signing ceremony to mark a newpartnership between the MMISproject and the Mindset Network,with signal carrier Sentech. This willbring health education to hospitalsand health facilities in nineprovinces, as well as an additional80 facilities. The partnership hasthe support of the NationalDepartment of Health (NDOH) andwill enable healthcare workers andthe public in both urban and ruralareas to access training andinformation through satellitetransmission.
With support from MMIS, a JohnSnow Research and TrainingInstitute project funded by the USPresident’s Emergency Plan for AIDSRelief (PEPFAR) through the Centersfor Disease Control and Prevention(Department of Health and HumanServices), the Mindset HealthChannel will enable staff to access
on-demand information on criticalhealth topics such as injection safety,healthcare waste management, andinfection prevention and control.Healthcare providers and workerswaiting for services will be able toview videos on infection control andinjection safety.
The goal of the partnership is toimprove the infrastructure currentlyavailable to educate healthcareworkers and patients on key healthtopics and to create an environmentthat supports positive healthbehaviour changes. This willincrease the success of – andimprove the service delivery of –prevention, care, management andtreatment programmes of majordiseases, including HIV and AIDS.Inequalities in health education andcommunication will also beaddressed by using technology toreach rural areas.
Making Medical Injections Safer (MMIS) and Mindset Health Channel bring health education to urban and rural areas vianew technology
We’d like your views
COHSASA HAS TEAMED up with John Snow Inc Research and TrainingInstitute of Boston, USA, to conduct a preliminary pilot study to test aquestionnaire for their Making Medical Injections Safer (MMIS) project.
The MMIS project is designed to assist hospitals in improving theadministration of injections. The exploratory group will be looking at thesafe administration of injections, waste management of used syringesand needles, the prevention of needle-stick injuries and other infections,as well as stock control.
Poor injection and sharp waste disposal practices for preventive andcurative services pose an avoidable risk of transmission of deadlydiseases such as HIV/AIDS, hepatitis B and hepatitis C to consumers,healthcare providers, and communities. In 2004, as part of thePresident’s Emergency Plan for AIDS Relief (PEPFAR) focusing oncountries with high HIV prevalence, JSI Research and Training Institute,Inc, and its subcontractors – Program for Appropriate Technology inHealth (PATH), Academy for Educational Development (AED) and theManoff Group – were awarded funds through the Centers for DiseaseControl and Prevention (CDC) and the US Agency for InternationalDevelopment (USAID) to implement ‘Rapid Interventions to DecreaseUnsafe Injections’ in 11 countries. The project is commonly known asMaking Medical Injections Safer (MMIS). In 2009, at the end of the five-year project, MMIS and national counterparts will establish anenvironment where patients, health care workers and the community arebetter protected from the medical transmission of HIV and other blood-borne pathogens.
Pilot studies to test the JSI questionnaire have been conducted in theNorth West Province and, subject to peer research and ethical clearance,may soon go nationwide. �