Embed Size (px)
Citation preview

Page 1 of 63
An application to include blood pressure lowering drug fixed dose combinations to the model list of essential medicines lists for the
treatment of essential hypertension in adults Author Organization Abdul Salam The George Institute for Global Health India Raju Kanukula The George Institute for Global Health India Hariprasad Esam The George Institute for Global Health India Ehete Bahiru Abhishek Sharma
Northwestern University Feinberg School of Medicine Boston University School of Public Health, and Precision Health Economics
David Heller Arnhold Institute for Global Health Mark Huffman Northwestern University Feinberg School of Medicine Rajesh Vedanthan Icahn School of Medicine at Mount Sinai Anubha Agarwal Duke University and NIH Fogarty Global Health Fellow Marc G. Jaffe Resolve to Save Lives, Vital Strategies, and Kaiser Permanente
Northern California Tom Frieden Resolve to Save Lives, Vital Strategies Sandeep P. Kishore
Arnhold Institute for Global Health & Young Professionals Chronic Disease Network
Anthony Rodgers The George Institute for Global Health Coordinated and Submitted by: Sandeep P. Kishore, Arnhold Institute for Global Health & Young Professionals Chronic Disease Network Anthony Rodgers, The George Institute for Global Health Marc G. Jaffe, Resolve to Save Lives, Vital Strategies, and Kaiser Permanente Northern California Tom Frieden, Resolve to Save Lives, Vital Strategies Contact: Cherian Varghese, Coordinator, Management of NCDs, WHO Department for Management of Noncommunicable Diseases, Disability, Violence and Injury Prevention

Page 2 of 63
Table of Contents
General items ....................................................................................................... 5
1. Summary statement of the proposal for inclusion, change or deletion. ..................... 5
Rationale for inclusion ......................................................................................... 5
Hypertension guidelines recommendations for use of two BP lowering drugs and FDCs 5
2. Name of the WHO technical department and focal point supporting the application (where relevant) ................................................................................................... 7
3. Name of organization(s) consulted and/or supporting the application. ...................... 7
4. International Nonproprietary Name (INN) and Anatomical Therapeutic Chemical (ATC) code of the medicine. ............................................................................................ 7
5. Formulation(s) and strength(s) proposed for inclusion; including adult and paediatric (if appropriate). ........................................................................................................ 7
6. Whether listing is requested as an individual medicine or as representative of a pharmacological class. ........................................................................................... 8
7. Treatment details (requirements for diagnosis, treatment and monitoring) .............. 10
Diagnosis and monitoring of hypertension ............................................................. 10
Treatment strategy with dual BP combinations ...................................................... 11
8. Information supporting the public health relevance. ............................................. 12
Epidemiological information on disease burden and treatment gaps ......................... 12
Comparing Fixed-dose combinations vs. separate pills ............................................ 13
Target population(s) ........................................................................................... 14
Likely impact of treatment on the disease ............................................................. 14
9. Review of benefits: summary of comparative effectiveness in a variety of clinical settings. ............................................................................................................. 14
Review of BP lowering efficacy of dual vs mono ..................................................... 14
Review of effects of combination therapy vs. placebo/no treatment on cardiovascular events .............................................................................................................. 15
Review of clinical trials assessing BP lowering efficacy of FDC combinations .............. 16
Review of clinical trials assessing BP lowering efficacy of lisinopril/HCTZ ................... 17
Lisinopril/HCTZ vs. placebo ............................................................................... 17
Lisinopril/HCTZ vs. monotherapy ....................................................................... 17
Lisinopril/HCTZ vs. other dual combination therapies ........................................... 17
Review of clinical trials assessing BP lowering efficacy of telmisartan/amlodipine combination ...................................................................................................... 18
Telmisartan/amlodipine vs. placebo ................................................................... 18
Telmisartan-amlodipine vs. monotherapy............................................................ 18
Telmisartan-amlodipine vs. other dual therapies .................................................. 19

Page 3 of 63
Telmisartan/amlodipine as initial therapy ............................................................ 19
Review of clinical trials assessing BP lowering efficacy of telmisartan/HCTZ combinations ....................................................................................................................... 19
Telmisartan/HCTZ vs. placebo ........................................................................... 19
Telmisartan/HCTZ vs. monotherapy ................................................................... 19
Telmisartan/HCTZ vs. dual therapy .................................................................... 20
Four trials51,55–57 reported data for this comparison. ............................................. 20
Review of clinical trials assessing BP lowering efficacy of lisinopril/amlodipine combination ....................................................................................................................... 20
10. Review of harms and toxicity: summary of evidence on safety. ........................... 21
Safety data for Lisinopril/HCTZ ............................................................................ 21
Safety data for Telmisartan/Amlodipine ................................................................ 24
Safety data for lisinopril/amlodipine ..................................................................... 25
Safety data for Telmisartan/HCTZ ........................................................................ 27
11. Summary of available data on comparative cost and cost-effectiveness within the pharmacological class or therapeutic group. ............................................................ 28
Current price insights with respect to global use .................................................... 28
Procurement prices: fixed dose combinations versus single pills ............................ 29
Retail prices of proposed FDCs .......................................................................... 30
Evergreening strategies and FDC price points ...................................................... 30
Implications on cost of FDC for hypertension if added to WHO EML ........................ 31
12. Summary of regulatory status of the medicine ................................................... 32
13. Availability of pharmacopoeial standards (British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia, European Pharmacopeia). ................... 33
14. References .................................................................................................... 34
Appendix 1: Gender-specific hypertension awareness, treatment, and control in 2010 in countries with data by world region ................................................................ 40
Appendix 2: Summary of characteristics of RCTs that assessed the effects of combination therapy of BP lowering drugs compared to placebo/no treatment on CV outcomes ....................................................................................................... 43
Appendix 3: Lisinopril + Hctz search strategy, PRISMA and summary of characteristics of included trials .............................................................................................. 45
Appendix 4: Lisinopril + HCTZ PRISMA flow chart ................................................ 46
Appendix 5: Summary of characteristics of included trials for assessing lisinopril + HCTZ ..................................................................................................................... 47
Appendix 6: Telmisartan + Amlodipine search strategy, PRISMA and Summary of characteristics of included trials ......................................................................... 48
Appendix 7: Telmisartan + Amlodipine PRISMA flow chart .................................... 49
Appendix 8: Summary of characteristics of included trials for assessing telmisartan + amlodipine ...................................................................................................... 50

Page 4 of 63
Appendix 9: Telmisartan + Hydrochlorothiazide search strategy, PRISMA and summary of characteristics of included trials ..................................................................... 52
Appendix 10: Telmisartan + HCTZ PRISMA flow chart .......................................... 53
Appendix 11: Summary of characteristics of included trials for assessing telmisartan + HCTZ ............................................................................................................. 54
Appendix 12: Lisinopril + Amlodipine search strategy, PRISMA and Summary of included trials ................................................................................................. 56
Appendix 13: Lisinopril + amlodipine PRISMA flow chart ....................................... 57
Appendix 14: Manufacturers of proposed combinations in EU, USA and India .......... 58
Appendix 15: Summary of characteristics of included trials for assessing lisinopril + amlodipine ...................................................................................................... 61
Appendix 16: Standard doses of component drugs of the proposed combinations .... 62

Page 5 of 63
General items
1. Summary statement of the proposal for inclusion, change or deletion.
Rationale for inclusion
Cardiovascular disease (CVD) is the world’s leading cause of death, driving 18 million deaths annually.1 High blood pressure (BP) – hypertension – is the leading cause of CVD and the greatest cause of preventable morbidity and mortality globally, driving 10 million deaths.1 Worldwide, 1.4 billion people have hypertension, defined as SBP >140 mmHg or DBP >90 mmHg, but less than 15% have BP controlled to less than 140/90.2 Hypertension can be most effectively treated with low-cost, generic, safe, once daily regimens. However, most patients currently receive a single BP lowering drug (monotherapy), with the largest global survey indicating monotherapy was used for 60% of regimens3; while the evidence suggests that the vast majority of patients require two or more drugs to achieve optimal and sustained BP control.4,5 In low- and middle- income countries, more than 70% of people treated for hypertension have uncontrolled BP, with one major reason for low levels of control being that most only receive monotherapy.1 Major international clinical practice guidelines recommend addition of a second BP lowering drug when desired BP control is not achieved with monotherapy. These guidelines also recommend treatment initiation with two drugs for at least selected patients, such as those with markedly elevated BP.4–8 Among patients requiring treatment with more than one BP lowering drug, use of a fixed dose combination (FDC, also known as single-pill combination) is recommended instead of separate drugs (Table 1). For example, the 2017 ACC/AHA guidelines recommend prescribers to “utilize fixed-dose combination agents when available and simplify drug regimens” and the 2013 ESH/ESC Guidelines “favour the use of combinations of two antihypertensive drugs at fixed doses in a single tablet, because reducing the number of pills to be taken daily improves adherence, which is unfortunately low in hypertension, and increases the rate of BP control”. A systematic review of dual combination vs. monotherapy as initial therapy in hypertension was completed for this application, including 27 trials with more than 10,000 participants in total. The results showed a clear improvement in efficacy with similar tolerability. The size of benefit was clinically important: an overall 26% increase in the rate of achieving BP control among patients receiving dual combination therapy. FDCs have substantial advantages for patients and healthcare programs, including improved adherence, simpler dose schedules, decreased pill burden, simplified logistics leading to fewer drug stock-outs, greater ease of task sharing, training, and supervision. This proposal therefore recommends the inclusion of four dual combinations which would collectively support the implementation of the recommended WHO HEARTS hypertension treatment protocols. Globally, approximately 320 million (37%) of the 510 million people treated for hypertension are not controlled.1 Improving control rates by 25% would therefore increase by 80 million the number of people with successfully controlled hypertension, which would in turn avert many hundreds of thousands of fatal or disabling cardiovascular events annually.
Hypertension guidelines recommendations for use of two BP lowering drugs and FDCs
Guidelines from Europe, India, China, the United States as well as the WHO HEARTS program endorse the use of combination therapy for BP reduction. The 2017 guidelines from the American College of Cardiology and American Heart Association recommend combination therapy for BP above 140/90 with ACE inhibitors (ACEI) or Angiotensin

Page 6 of 63
Receptor Blockers (ARB), calcium channel blockers (CCB) and thiazide /thiazide like diuretics.8
Table 1: Selected hypertension guideline recommendations on dual combination and FDCs
ACC/AHA
20178 ESC/ESH
20139 India
201310 China 201011
Thailand 201512
WHO HEARTS13
Recommendations when to use two BP lowering drugs
Not controlled on monotherapy Yes Yes Yes Yes Yes Yes
Initial treatment for selected patients e.g. >20/10mmHg from goal* and/or high CV risk
Yes Yes Yes Yes Yes Yes
Recommendations when to use single pill combinations Recommended to substitute for separate pills to improve adherence
Yes Yes Yes Yes NR NR
* Some referred to this as stage II HTN or marked BP elevation, NR=Not reported
Addressing concerns raised by 2017 application for a dual BP lowering combination In 2017, the WHO Expert Panel reviewed a petition requesting the addition of an FDC for high BP (lisinopril and hydrochlorothiazide). The petition received favorable, publicly available, peer reviews; one reviewer suggested an amendment to the dose of diuretic; and another suggested a different combination to be included in the petition (in specific: amlodopine + benazepril). The previous petition, in part, prompted the WHO Expert Committee to formally recognize the benefits of cardiovascular FDC in the 2017 WHO EML:
“Fixed-dose combinations for non-communicable diseases may have advantages over the single medicines given concomitantly, including increased adherence and reduced pill
burden. The potential value of fixed-dose combinations of currently listed essential medicines, with regulatory approval and demonstrated bioavailability for the
management of chronic non-communicable diseases, is recognized.”
We note that a wide range of dual FDCs are available, and there is clinical and public health utility in having a selection available to guide national approaches, since some patients may have contraindications to one class of BP lowering drugs. For example, a significant number of patients, especially from in Asia and Africa, are susceptible to cough and other adverse effects from ACEI and so there is value in having an ARB combination. In this petition, we review possible FDCs to guide the WHO Expert Committee regarding formal inclusion on the EML. Given national and international scale-up opportunities for hypertension control, and substantial benefits of lowering BP well below 140 mmHg systolic14,15; and evidence that dual combination therapy reduces BP and cardiovascular events substantially more than monotherapy16,17 we recommend four two-drug FDC each qualified with a square box additions to the WHO EML to improve competition over available alternative options. The recommendation for multiple dose options and four different combinations will directly address the issues raised in 2017 with the proposal for a single FDC: “that listing a single FDC of cardiovascular medicines would limit choice from the variety of combinations, components and dosages available.” These recommendations are based on worldwide availability and affordability and best available evidence:
Page 7 of 63
Class Drug combinations (as representative) ACEI/Diuretic lisinopril/hydrochlorothiazide (HCTZ) ARB/CCB telmisartan/amlodipine ACEI/CCB lisinopril/amlodipine ARB/Diuretic telmisartan/HCTZ
The square box indication ensures that the pharmacological class therapeutic equivalence is endorsed to provide choice to nations. The approach herein addresses the key bases of rational, practical, affordable, generic, once daily combinations of the four classes of medication currently considered first line in leading national and international guidelines.
2. Name of the WHO technical department and focal point supporting the application (where relevant)
Cherian Varghese, Coordinator, Management of NCDs, WHO Department for Management of Noncommunicable Diseases, Disability, Violence and Injury Prevention
3. Name of organization(s) consulted and/or supporting the application.
Please see supporting letters.
4. International Nonproprietary Name (INN) and Anatomical Therapeutic Chemical (ATC) code of the medicine.
INN ATC code lisinopril/HCTZ C09BA03 telmisartan/amlodipine C09DB04 lisinopril/amlodipine C09BB03 telmisartan/HCTZ C09DA07
5. Formulation(s) and strength(s) proposed for inclusion; including adult and pediatric (if appropriate).
These are summarized in the Table below.

Page 8 of 63
Combinations Strength(s) Formulation lisinopril/HCTZ 10/12.5 Tablet 20/12.5 Tablet 20/25 Tablet
telmisartan/amlodipine 40/5 Tablet 80/5 Tablet 80/10 Tablet
lisinopril/amlodipine 10/5 Tablet 20/5 Tablet 20/10 Tablet telmisartan/HCTZ 40/12.5 Tablet 80/12.5 Tablet 80/25 Tablet
The provision of a selection of FDCs and of doses within each FDC addresses the WHO EML 2017 Committee concern about providing choice and flexibility. At the same time, not all possible dose combinations are recommended, in order to reduce complexity of purchase and supply for countries. Also of relevance of the FDA statement that “Over the last decade, the Agency has actively discouraged antihypertensive monotherapy and combination doses with effects that were very close together, considering them a nuisance to physicians seeking to get patients to goal.”18 All of the recommended hypertension algorithms in the WHO HEARTS package would be supported by the provision of these FDCs, which would be utilised in the 1st and/or 2nd step of each protocol (with the exception of the CCB+diuretic as first line protocol – this is not included in this submission given the lack of widely available CCB-diuretic FDCs). The safety and efficacy of the proposed FDCs have not been established in paediatrics, and the prevalence of hypertension is far lower than in adults; hence, their use in children is not recommended.19–23
6. Whether listing is requested as an individual medicine or as representative of a pharmacological class.
This application requests four ‘square box’ inclusions, taken as representative of the classes. Specifically of: • FDC of lisinopril/HCTZ as a square box representing two-drug FDC BP lowering therapy
of the pharmacological class ACEI/thiazide diuretic. The combination of lisinopril/HCTZ was chosen as it is one of the most commonly used, widely available and affordable BP combinations globally. Given the fact that all or almost all of the benefits of BP lowering drugs are due to the amount of BP lowering per se15,17,24, much the same clinical benefits can be expected from other ACEI-diuretic combinations (and indeed from other dual BP lowering combinations). An additional benefit of this combination is the balancing of the effects on serum potassium of ACEIs, which increase serum potassium, and diuretics, most of which decrease serum potassium. Although this

Page 9 of 63
does not preclude the desirability of laboratory monitoring, it is likely to increase the safety of diuretics, particularly in environments where management of serum potassium may be difficult. Alternatives include: Benazepril/HCTZ enalapril/HCTZ fosinopril/HCTZ moexipril/HCTZ quinapril/HCTZ perindopril/indapamide
• FDC of telmisartan/amlodipine as a square box representing two-drug FDC BP lowering therapy of the pharmacological class of ARB/CCB. Telmisartan is a long-acting ARB with longer duration of action compared to losartan; and is now available as a generic. Amlodopine is widely used in low and middle-income countries and is widely available in the class of CCB. Other daily long-acting DHP CCB could be considered. Amlodopine is effective for all races, and reduces need for laboratory testing for electrolytes and renal function. The concommitant use of ARB or ACEI with amlodipine, as in the proposed FDCs in this application, reduces the incidence of pedal oedema, which is the most common adverse effect encountered with use of amlodipine.13
Alternatives include: Valsartan/amlodipine olmesartan medoxomil/amlodipine irbesartan/amlodipine losartan/amlodipine candesartan/amlodipine valsartan/lercanidipine telmisartan/nifedipine SR
• FDC of telmisartan/HCTZ as a square box representing two-drug BP lowering therapy
of the pharmacological class of ARB + thiazide diuretic. Alternatives include: azilsartan medoxomil/chlorthalidone* candesartan/HCTZ eprosartan/HCTZ fimasartan/HCTZ irbesartan/HCTZ losartan/HCTZ olmesartan medoxomil/ HCTZ valsartan/HCTZ
*This formulation is the only widely marketed chlorthalidone combination with ACE or ARB

Page 10 of 63
• FDC of lisinopril/amlodipine as a square box representing two-drug BP lowering therapy of the pharmacological class of ACEI/CCB. Alternatives include:
delapril/manidipine enalapril/lercanidipine enalapril/amlodipine perindopril/amlodipine ramipril/felodipine ramipril/amlodipine trandolapril/verapamil
In general, for currently available and future FDCs, substitutions between the components of the proposed FDCs is advised based on national preference. Acceptable alternatives: • switch telmisartan to other once daily generic ARB, such as valsartan • switch lisinopril to other once daily generic ACEi, such as ramipril • switch amlodipine to other once-daily CCB such as felodipine • switch HCTZ to other once daily generic thiazide or thiazide-like diuretic such as
chlorthalidone, indapamide, indapamide SR. Treatment details, public health relevance and evidence appraisal and synthesis
7. Treatment details (requirements for diagnosis, treatment and monitoring)
Diagnosis and monitoring of hypertension
We reference the WHO HEARTS approach for diagnosis, treatment and monitoring of hypertension for the purposes of this application: Measuring BP is the only way to diagnose hypertension, as most people with raised BP have no symptoms. Accurate BP measurements should be conducted on adults during routine visits to primary health care facilities, including all adults at first presentation to the facility, and, if normal, periodically thereafter (e.g., every 1 to 5 years). The diagnosis of hypertension should be based on an average of two or more blood pressure readings obtained on two or more occasions or current treatment with antihypertensive drug therapy. Every patient with elevated BP readings requires immediate follow-up, according to the following protocol. Effective treatment algorithms for hypertension are dependent on accurate BP measurement. The following advice should be followed for measuring BP (1): Use the appropriate cuff size, noting the lines on the cuff to ensure that it is positioned correctly on the arm. (If the arm circumference is >32 cm, use large cuff.) • Although at the initial evaluation it is preferable to measure BP in both arms and use
the arm with the higher reading thereafter, this may not be practical in a busy health care environment.
• The patient should be sitting with back supported, legs uncrossed, empty bladder, relaxed for 5 minutes and not talking.

Page 11 of 63
• For persons who are getting their BP measured for the first time, it is preferable to take at least two readings and to use the second reading, or three readings and take an average of the last two readings.
• BP can be measured either by a conventional sphygmomanometer, using a stethoscope, or by an automated electronic device. The electronic device, if available, is preferred because it provides more reproducible results and is not influenced by variations in technique or by the bias of the observers.
• If the health care facility has electricity or regular access to batteries, then consider an automated validated BP device with a digital reading. If the health care facility has no electricity or batteries, then a manual BP cuff will have to be used with a stethoscope.
The diagnosis of hypertension should be confirmed at an additional patient visit, usually 1 to 4 weeks after the first measurement. In general, hypertension is diagnosed if, on two visits on different days: systolic BP on both days is ≥140 mmHg and/or diastolic BP on both days is ≥90 mmHg. Patients with an initial reading of ≥160 mmHg systolic and/or diastolic BP ≥100 mmHg are often recommended to be initiated on treatment the same day.
Treatment strategy with dual BP combinations
Several major international guidelines now recommend initial combination therapy for selected patients, as noted in Table 1. For example, the ESH/ESC 2013 guidelines25 note that this strategy will achieve “a prompter response in a larger number of patients (potentially beneficial in high-risk patients), a greater probability of achieving the target BP in patients with higher BP values and a lower probability of discouraging patient adherence with many treatment changes.” The AHA/ACC guidelines8 indicate FDC for stage II hypertension (>140/90mmHg) and a BP 20/10mmHg above target. Per guidelines in Table 1, an FDC may be used for initial therapy where local guidelines recommend such treatment, such as for people who are >20/10mmHg from goal. The FDCs are not indicated for the treatment of renovascular hypertension. Treatment with an FDC requires considerations of recent BP lowering drug treatment and the magnitude of baseline BP elevation. Adjustment of the existing BP lowering treatment may be needed. The FDC should be taken at about the same time every day as advised by the treating physician. In patients receiving diuretic therapy electrolyte abnormalities, orthostatic hypotension or dizziness may occur following the initial dose of an FDC, particularly due to volume/salt depletion with diuretic therapy. In the elderly, although reported BP responses were similar to that in younger patients, it is recommended that the proposed FDC should be used after considering BP response and renal function. Dose should be selected cautiously, preferably starting with the low dose of FDC. Any dose versions of the proposed FDC are not recommended in patients with severe renal impairment. In patients with mild-to-moderate renal impairment the FDC can be used after titration of the component drugs.

Page 12 of 63
8. Information supporting the public health relevance.
Epidemiological information on disease burden and treatment gaps Figure 1: Worldwide levels of raised blood pressure1
Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation 2016;134: 441–50. The benefits of BP lowering in reducing cardiovascular (CV) events are well established,24 and there is clear evidence that greater BP reduction confers larger reduction in CV events.15,17,26 However, control of high BP is poor with only one in three on treatment achieving BP targets of under 140/90 mmHg.3 Overall, control is reported at 13.% globally and as low as 7.7% in low and middle income countries.1 While 88% of people who are aware of hypertension received some pharmacological treatment, only 34% of those treated were controlled.3 There are substantial disparities: high-income countries had almost double the proportions of awareness (67.0% versus 37.9%) and treatment (55.6% versus 29.0%) and 4 times the proportion of control among patients with hypertension (28.4% versus 7.7%) in comparison with low- and middle income countries in 2010.1 This is in large part due to the fact that most treated patients only receive monotherapy,3 despite guidelines recognizing that the large majority of patients require combination therapy for BP control. The recommended use of dual BP lowering in major hypertension management guidelines recommend is outlined in Table 1. Guidelines also recommend one or more of the proposed combinations among the preferred combinations.4–7,10,27,28 Finally, guidelines recommend use of FDC as a means of simplifying treatment regimen which could potentially improve adherence to prescribed drugs and be cost-effective.4,5,10,27

Page 13 of 63
Table 2: Gender-specific hypertension awareness, treatment and control by income level in 2000 and 2010
Awareness Treatment Control* Control† 2000 2010 2000 2010 2000 2010 2000 2010
Global Overall 41.4
(34.3–48.5)
46.5 (41.9–51.1)
31.8 (25.6–37.9)
36.9 (33.8–40.0)
33.9 (26.5–41.3)
37.1 (33.6–40.5)
11.7 (7.1–16.2)
13.8 (11.4–16.3)
Men 36.1 (25.9–46.2)
40.2 (34.0–46.5)
26.8 (18.4–35.2)
30.3 (26.1–34.5)
34.2 (24.1–44.2)
35.8 (30.8–40.7)
10.0 (4.0–15.9)
10.9 (7.7–14.2)
Women 46.6 (36.7–56.5)
52.9 (46.1–59.6)
36.7 (27.7–45.7)
43.6 (39.1–48.1)
33.7 (23.2–44.2)
38.0 (33.2–42.8)
13.4 (6.5–20.2)
16.8 (13.1–20.5)
High-income countries Overall 58.2
(42.2–74.3)
67.0 (58.1–75.9)
44.5 (31.1–58.0)
55.6 (49.8–61.4)
38.6 (25.5–51.6)
50.4 (44.4–56.4)
17.9 (7.7–28.0)
28.4 (22.3–34.5)
Men 52.4 (29.0–75.8)
61.8 (48.0–75.7)
38.3 (19.7–56.9)
49.4 (40.8–58.1)
38.6 (21.1–56.0)
49.1 (40.7–57.4)
15.5 (2.3–28.7)
24.6 (16.0–33.2)
Women 64.1 (42.1–86.0)
72.2 (60.9–83.4)
50.9 (31.6–70.3)
61.7 (54.1–69.3)
38.6 (19.8–57.4)
51.5 (43.1–59.9)
20.3 (4.8–35.8)
32.2 (23.6–40.8)
Low- and middle-income countries Overall 32.3
(25.7–38.9)
37.9 (32.5–43.2)
24.9 (18.7–31.0)
29.0 (25.4–32.7)
29.4 (22.1–36.7)
26.3 (22.3–30.3)
8.4 (4.0–12.7)
7.7 (5.3–10.1)
Men 27.0 (18.0–36.0)
31.2 (24.5–38.0)
20.4 (12.4–28.4)
22.3 (17.6–27.0)
29.5 (19.9–39.2)
23.4 (17.9–28.9)
6.9 (1.3–12.6)
5.2 (2.3–8.1)
Women 37.4 (27.8–47.1)
44.7 (36.3–53.0)
29.2 (20.0–38.4)
35.9 (30.3–41.5)
29.2 (18.9–39.6)
28.1 (22.6–33.7)
9.7 (3.2–16.3)
10.2 (6.4–14.0)
From Kelley et al 2018.2 Values are percentages and 95% confidence intervals. Awareness is defined as self-reported previous diagnosis of hypertension among those with hypertension. Treatment is defined as self-reported antihypertensive medication use among those with hypertension. Control is defined as systolic blood pressure <140 mmHg and diastolic blood pressure <90 mmHg. *Among those self-reporting treatment. †Among all participants with hypertension.
Comparing Fixed-dose combinations vs. separate pills
Previous reviews of the 2017 FDC petition summarized trials that compared FDC vs the monocomponents taken as separate pills over short periods, often 4-12 weeks.29 However, these trials were conducted in tightly controlled settings in which adherence has been optimized in order to assess pharmacological equivalence and hence support a “substitution” indication. Such trials are not informative regarding the role of FDCs in overcoming treatment inertia and long-term adherence in real clinical practice. FDC therapy improves adherence to prescribed drugs and reduces treatment inertia.30

Page 14 of 63
Target population(s)
• Patients with uncontrolled BP despite treatment with one of the component drug in the proposed FDC.
• Initial treatment where indicated by local guidelines. • Patients currently receiving treatment with the both component drugs separately
at the dose as in FDC.
Likely impact of treatment on the disease
The proposed FDC has the potential to significantly improve BP control in a large number of hypertensives. The impact is expected to be substantially higher in low- and middle-income countries where the majority of the patients receive monotherapy and have uncontrolled BP. Per numbers needed to treat calculations,31 with current projections, it is estimated that 1 in 125 would have prevented death, 1 in 67 would have prevented stroke and 1 in 100 prevented heart attack (fatal and non-fatal myocardial infarction and sudden/rapid cardiac death).
9. Review of benefits: summary of comparative effectiveness in a variety of clinical settings.
In support of the application, an overview of all dual BP combinations, in terms of efficacy in lowering BP and reducing cardiovascular events, was undertaken.
Review of BP lowering efficacy of dual vs mono
Law et al32 performed meta-analysis of 42 factorial trials (10,968 participants) and showed that combining drugs from the four classes, ACEIs, Beta-blockers, thiazide and calcium channel blockers, produced additive BP lowering effects, also the effect was approximately five times greater compared to doubling the dose of monotherapy. A systematic review of dual vs monotherapy as initial treatment (among patients who were untreated or had washout of previous BP lowering therapy for ≥4 weeks), was completed for this application. The review included 27 randomised, double-blind trials with more than 10,000 participants in total. The results showed a clear improvement in efficacy with no increases in withdrawals due to adverse events. The size of benefits was clinically important, with a 26% increase in the rate of achieving BP control among patients receiving dual combination therapy.
Figure 2: Dual therapy vs standard-dose monotherapy – effects on mean BP reduction and hypertension control rates
<1+<1=dual low dose; 1+<1= standard and low dose; 1+1= dual standard dose. WDAE= withdrawal due to adverse event

Page 15 of 63
Two other trials33,34 have compared strategies for initial treatment of hypertension of dual-combination therapy vs monotherapy based care, each showing improved efficacy in patients receiving combination therapy. In the Simplified Treatment Intervention to Control Hypertension (STITCH) trial conducted in primary care practices in Canada, a simplified algorithm starting with ACE inhibitor-diuretic combination gave better BP control than a stepped care titration schedule at 6 months (65% vs 53%, p=0.03).33 In the STRATHE trial among patients with uncomplicated hypertension in France, a low dose combination ACE inhibitor-thiazide gave superior BP control without side effects compared to both sequential monotherapy and a stepped care regimen.34 Finally, the PATHWAYS-135 trial recently demonstrated the superiority of dual combination therapy vs monotherapy, without an increase in clinically important side effects and with no subgroup identified in whom dual therapy was not superior to monotherapy.
Review of effects of combination therapy vs. placebo/no treatment on cardiovascular events
A systematic review of RCTs was conducted to assess the effects of combination therapy of BP lowering drugs compared to no treatment on coronary heart disease (CHD), stroke, heart failure and death, based on previously published systematic reviews.15,17 One additional recently published trial36 was included. Eleven trials involving 35208 patients were included in the analysis. Mean age across patient groups was 64 years, and baseline BP was 148/84 mmHg (Appendix 1).
The effects on cardiovascular events are shown in Table 3. Given the pivotal role of the extent of BP reduction, the trials are divided into those which achieved a BP separation of more than or less than 6 mmHg SBP. In short-term trials, for which adherence will have been high, among people with hypertension dual combination BP lowering therapy has been shown to reduce BP by around 15/9 mmHg.16 The trials achieving a large BP separation were mostly conducted among patients with hypertension and did not have background treatment. Among these trials, there was a 25% reduction in CHD, a 39% reduction in stroke, a 52% reduction in heart failure and a 19% reduction in mortality (all p<0.001). The two trials with <6 mmHg SBP reduction were conducted among patients with a wide range of BP levels, a relatively low mean starting BP level, and a high number of patients already receiving background treatment. In these two trials there were lesser and non-significant reductions in major cardiovascular events. However, there was still a reduction in total mortality (p=0.05).

Page 16 of 63
Table 3: Effects of combination therapy vs. placebo on CHD, stroke, heart failure and death
Studies Intervention Control RR (95% CI) events/participants events/participants
Studies with >6 mm Hg reduction in SBP CHD 11 175/5585 240/5694 0.75 (0.62-0.91) Stroke 11 310/5669 518/5694 0.61 (0.53-0.69) Heart failure 8 66/3172 157/3879 0.48 (0.36-0.63) Death 11 499/5596 627/5694 0.81 (0.72-0.90) Studies with ≤6 mm Hg reduction in SBP CHD 2 317/11925 356/11920 0.90 (0.77-1.03) Stroke 2 290/11925 312/11920 0.93 (0.80-1.10) Heart failure 1 21/6356 29 / 6349 0.72 (0.41-1.27) Death 2 750/11925 820/11920 0.91 (0.83-1.00) All studies CHD 13 492/17510 596/17614 0.84 (0.74-0.94) Stroke 13 600/17594 830/17614 0.73 (0.66-0.80) Heart failure 9 87/9528 186/10228 0.52 (0.40-0.67) Death 13 1249/17521 1447/17614 0.87 (0.80-0.93)
Effects of combination therapy of BP lowering drugs compared to placebo on CHD, stroke and death in major patient groups are reported in Figure 2.
Figure 3: Effects of combination therapy of BP lowering drugs compared to placebo on coronary heart disease, stroke and death in major patient groups.
Review of clinical trials assessing BP lowering efficacy of FDC combinations
MEDLINE, Embase, and Cochrane Register of Controlled Trials, were searched, until March 2018, for RCTs of dual combinations compared to placebo, monotherapy or other dual combinations, published in English language. Included RCTs were double-blind that enrolled patients with hypertension, and had treatment with fixed-doses of drugs for at least four weeks. Trial of secondary hypertension were excluded. Detailed literature search strategy, PRISMA flow chart and summary of characteristics of included trials are reported in Appendices.

Page 17 of 63
Review of clinical trials assessing BP lowering efficacy of lisinopril/HCTZ
Lisinopril/HCTZ vs. placebo Two RCTs 37,38 reported data for this comparison (Figure 4).
Figure 4: Change from baseline BP with lisinopril/HCTZ compared to placebo
L = Lisinopril, H = Hydrochlorothiazide Lisinopril/HCTZ vs. monotherapy One RCT37 compared two strengths of dual combination to respective monotherpies of component drugs (Figure 5).
Figure 5: Change from baseline DBP with lisinopril/HCTZ compared to monotherapy components
L = Lisinopril, H = Hydrochlorothiazide Lisinopril/HCTZ vs. other dual combination therapies Two RCTs38,39 reported data for this comparison (Figure 6).
Figure 6: Change from baseline BP with lisinopril/HCTZ compared to other dual combinations
ared to other dual combinations
A = Amlodipine, C = Chlorthalidone, C = Candesartan, L = Lisinopril, H = Hydrochlorothiazide, V = Verapamil
Page 18 of 63
Review of clinical trials assessing BP lowering efficacy of telmisartan/amlodipine combination
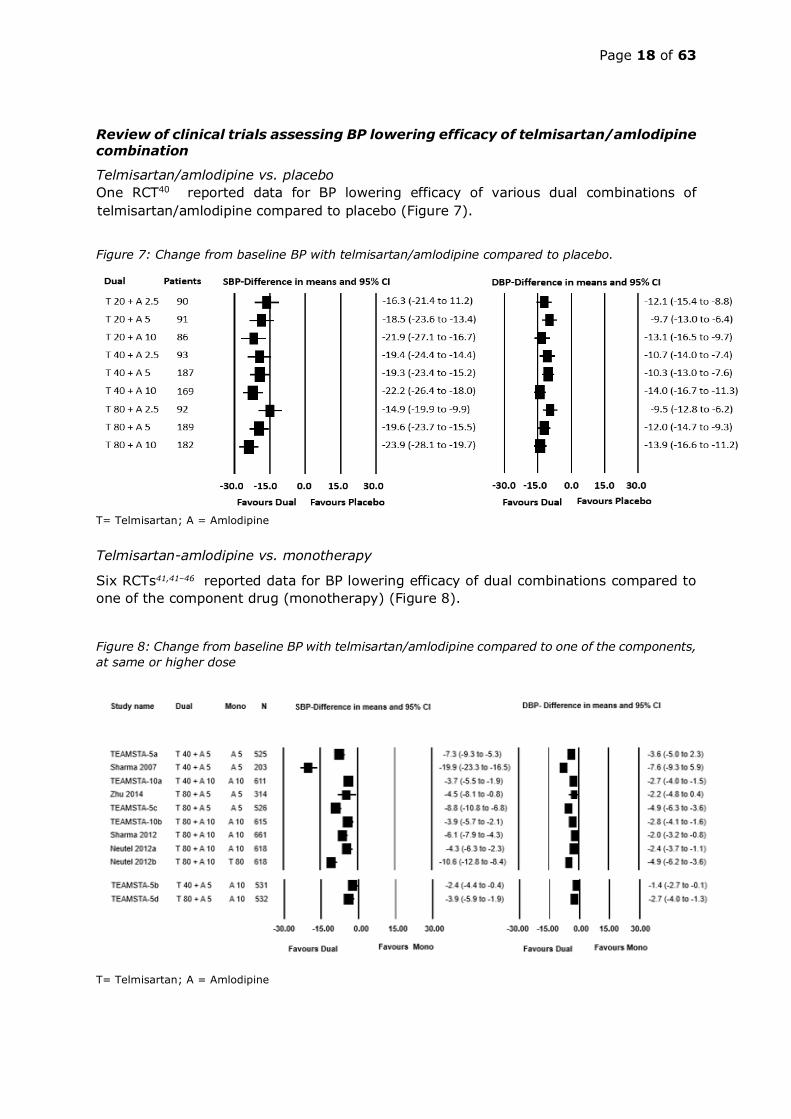
Telmisartan/amlodipine vs. placebo One RCT40 reported data for BP lowering efficacy of various dual combinations of telmisartan/amlodipine compared to placebo (Figure 7).
Figure 7: Change from baseline BP with telmisartan/amlodipine compared to placebo.
T= Telmisartan; A = Amlodipine Telmisartan-amlodipine vs. monotherapy
Six RCTs41,41–46 reported data for BP lowering efficacy of dual combinations compared to one of the component drug (monotherapy) (Figure 8).
Figure 8: Change from baseline BP with telmisartan/amlodipine compared to one of the components, at same or higher dose
T= Telmisartan; A = Amlodipine

Page 19 of 63
Telmisartan-amlodipine vs. other dual therapies One RCT47 (n=481) assessed the effects of telmisartan 80mg/amlodipine 5mg compared to olmesartan 40 mg/hydrochlorothiazide 12.5 mg in 481 hypertensive patients. Both the dual combinations were equally efficacious (BP reduction 12.7/9.1 vs. 12.8/10). Telmisartan/amlodipine as initial therapy Neldam et. al48 analysed patient-level data for three double-blind RCTs, conducted by Boehringer Ingelheim, to assess BP lowering efficacy of telmisartan/amlodipine combination therapy with respective monotherapies at week(s) 1, 2 and 4. Among patients initiated on combination therapy, greater reduction in BP and improvement in BP control was achieved with combination compared to monotherapies at these earlier time-points during the treatment period. The BP lowering effect of telmisartan and amlodipine combination does not differ substantially between blacks and whites (Table 4).
Table 4: Telmisartan (T) and amlodipine (A) reduction in DBP (mmHg), by race49 T80+A10 T40+A10 T80+A5 T40+A5
Black 17.2 20.9 16.7 13.7
Caucasian 20.6 20.3 15.6 17.0
Review of clinical trials assessing BP lowering efficacy of telmisartan/HCTZ combinations
Telmisartan/HCTZ vs. placebo Two RCTs50,51 reported data for this comparison (Figure 9).
Figure 9: Change from baseline in SBP & DBP with telmisartan/hydrochlorothiazide compared to placebo
T= Telmisartan; H = hydrochlorothiazide Telmisartan/HCTZ vs. monotherapy Three RCTs52–54 reported data for this comparison (Figure 10).

Page 20 of 63
Figure 10: Change from baseline in SBP & DBP with telmisartan/hydrochlorothiazide compared to monotherapy
T= Telmisartan; H = hydrochlorothiazide Telmisartan/HCTZ vs. dual therapy Four trials51,55–57 reported data for this comparison.
Figure 11: Change from baseline in SBP & DBP with telmisartan/hydrochlorothiazide compared to same dual combination at different dose or different dual combinations
T= Telmisartan; H = hydrochlorothiazide
Review of clinical trials assessing BP lowering efficacy of lisinopril/amlodipine combination
Only one small crossover RCT58 (n=15) assessed efficacy of lisinopril 10mg/amlodipine 5mg was compared with lisinopril 10mg, and amlodipine 5mg, for 1 month. SBP reduction with combination therapy was significantly higher with combination compared to respective monotherapies (13.3 [95% CI 9.9-17.2] vs. 5.5 [-1.1-12.0] vs. 8.6 [3.7-13.4], mmHg). Similar pattern was seen with DBP.

Page 21 of 63
10. Review of harms and toxicity: summary of evidence on safety.
Figure 12: Incidence of WDAEs and dizziness with initial dual combination vs. standard-dose monotherapy
Safety data for Lisinopril/HCTZ
Lisinopril/HCTZ vs. placebo In Chrysant et al.37, there was insignificantly higher incidence of pharyngitis and cough with lisinopril/HCTZ compared with placebo. In Leeuw et al38, incidence of adverse events did not differ significantly between treatments. Lisinopril/HCTZ vs. monotherapy In Chrysant et al.37, there was insignificantly higher incidence of pharyngitis and cough with lisinopril/HCTZ compared with monotherapy. Lisinopril/HCTZ vs. other dual combinations Of the two studies in this comparison, Leeuw et al.38 reported no difference in tolerability between the treatments that were compared. In McInnes et al.39 both the FDCs were well tolerated; however, significantly more patients in lisinopril/HCTZ group experienced adverse events, predominantly cough. Safety data from the marked products monographs/labels of the lisinopril/HCTZ FDC.
Table 5: Adverse experiences occurring in >1% of patients treated with lisinopril/HCTZ in controlled clinical trials59 lisinopril/HCTZ
(n=930) Incidence (discontinuation)
Placebo (n=207)
Incidence Dizziness 7.5 1.9 Headache 5.2 1.9 Cough 3.9 1.0 Fatigue 3.7 1.0 Orthostatic Effects 3.2 1.0 Diarrhea 2.5 2.4 Nausea 2.2 2.4 Upper Respiratory Infection
2.2 0.0
Muscle Cramps 2.0 0.5

Page 22 of 63
Asthenia 1.8 1.0 Paresthesia 1.5 0.0 Hypotension 1.4 0.5 Vomiting 1.4 0.5 Dyspepsia 1.3 0.0 Rash 1.2 0.5 Impotence 1.2 0.0
Table 6: Incidence of adverse reactions in patients receiving lisinopril/HCTZ in controlled trials.19 lisinopril/HCTZ
(n = 930) % lisinopril
(n = 2633) % Body as a whole Fatigue 3.7 - Asthenia 1.8 2.7 Impotence 1.2 0.7 Decreased libido 1.0 0.2 Fever 0.5 0.3 Gout 0.2 0.2 Cardiovascular Orthostatic effects 3.2 0.9 Hypotension 1.9 0.8 Chest pain 1.0 1.1 Palpitation 0.9 0.8 Syncope 0.8 0.2 Chest discomfort 0.6 - Edema 0.1 0.6 Rhythm disturbances 0.1 0.5 Angina 0.1 0.3 Digestive Diarrhea 2.5 1.8 Nausea 2.2 1.9 Vomiting 1.4 1.1 Dyspepsia 1.3 0.5 Abdominal pain 0.9 1.4 Constipation 0.3 0.2 Dry mouth 0.2 0.5 Anorexia 0.2 0.4 Flatulence 0.2 0.3 Dermatologic Rash 1.2 1.0 Flushing 0.8 0.3 Pruritis 0.4 0.5 Angioedema -* 0.1 Musculoskeletal Muscle cramps 2.0 0.5 Back pain 0.8 0.5

Page 23 of 63
Shoulder pain 0.5 0.2 Nervous/Psychiatric Dizziness 7.5 4.4 Headache 5.2 5.6 Paresthesia 1.5 0.5 Vertigo 0.9 0.2 Depression 0.5 0.7 Somnolence 0.4 0.8 Insomnia 0.2 0.3 Respiratory Cough 3.9 3.0 Upper respiratory infection 2.2 2.1 Dyspnea 0.4 0.4
* Marketing Experience Only Safety profile in elderly patients (age >65 years)59 Clinical studies did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy. This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection. Evaluation of the hypertensive patient should always include assessment of renal function. The FDC is contraindicated in selected clinical situations and so safety issues may arise in health system, and patient factors affect the ability to detect such situations.19,20,59
• In patients with history of previous hypersensitivity to the ingredients, ACEI, sulfonamide-derived drugs.
• Women who are pregnant, intend to become pregnant, or of child bearing potential who are not using adequate contraception.
• Nursing women. • In patients with anuria or sever hepatic impairment or severe renal impairment. • In patients with a history of hereditary and/or idiopathic angioedema or
angioedema associated with previous ACEI treatment. Black patients reported higher incidence of angioedema with ACEIs compared to non-blacks.
• Contraindicated in combination with a neprilysin inhibitor (e.g., sacubitril). • Do not administer within 36 hours of switching to or from sacubitril/valsartan, a
neprilysin inhibitor. • Do not co-administer with aliskiren or ARB in patients with diabetes or renal
impairment or hyperkalemia or congestive heart failure who are hypotensive.

Page 24 of 63
Safety data for Telmisartan/Amlodipine
Figure 13: Withdrawals due to AEs with telmisartan/amlodipine compared to one of the component, and compared to higher dose of one of the component.
T= Telmisartan; H = hydrochlorothiazide The FDA labelling for telmisartan/amlodipine21 reported that the concomitant use of these drugs has been evaluated for safety in more than 3700 patients with hypertension; approximately 1900 of these patients were exposed for at least 6 months and over 160 of these patients were exposed for at least one year. Adverse reactions have generally been mild and transient in nature and have only infrequently required discontinuation of therapy. In the placebo-controlled factorial design study40 the population treated with a telmisartan and amlodipine combination had a mean age of 53 years and included approximately 50% males, 79% were Caucasian, 17% Blacks, and 4% Asians. Patients received doses ranging from 20/2.5 mg to 80/10 mg orally, once daily. The frequency of adverse reactions was not related to gender, age, or race. The adverse reactions that occurred in the placebo-controlled factorial design trial in ≥2% of patients treated with TWYNSTA and at a higher incidence in TWYNSTA-treated patients (n=789) than placebo-treated patients (n=46) were peripheral edema (4.8% vs 0%), dizziness (3.0% vs 2.2%), and back pain (2.2% vs 0%). Edema (other than peripheral edema), hypotension, and syncope were reported in <2% of patients treated with TWYNSTA tablets. In the placebo-controlled factorial design trial, discontinuation due to adverse events occurred in 2.2% of all treatment cells of patients in the telmisartan/amlodipine treated patients and in 4.3% in the placebo-treated group. The most common reasons for

Page 25 of 63
discontinuation of therapy with TWYNSTA tablets were peripheral edema, dizziness, and hypotension (each ≤0.5%). Peripheral edema is a known, dose-dependent adverse reaction of amlodipine, but not of telmisartan. In the factorial design study, the incidence of peripheral edema during the 8 week, randomized, double-blind treatment period was highest with amlodipine 10 mg monotherapy. The incidence was notably lower when telmisartan was used in combination with amlodipine 10 mg.
Table 7: Incidence of peripheral edema during the 8-week treatment period21 Telmisartan
Placebo 40 mg 80 mg
Am
lod
ipin
e Placebo 0% 0.80% 0.70%
5 mg 0.70% 1.40% 2.10%
10 mg 17.80% 6.20% 11.30%
Safety profile in elderly patients (age >65 years)21 Of the total number of 3282 hypertensive patients receiving a telmisartan/amlodipine combination in clinical studies, 605 (18%) patients were 65 years of age or older and of these, 88 (3%) patients were 75 years and older. No overall differences in efficacy or safety were observed in this patient population. Since patients age 75 and older have decreased clearance of amlodipine, start amlodipine or add amlodipine 2.5 mg to telmisartan. The lowest dose of 40/5 mg; therefore, initial therapy is not recommended in patients 75 years of age and older. Since patients with hepatic impairment have decreased clearance of amlodipine, start amlodipine or add amlodipine 2.5 mg to telmisartan. The lowest dose of is 40/5 mg; therefore, initial therapy is not recommended in hepatically impaired patients The FDC is contraindicated in selected clinical situations and so safety issues may arise in health system, and patient factors affect the ability to detect such situations:21,60
• Known hypersensitivity (e.g., anaphylaxis or angioedema) to ingredients or ARBs or dihydropyridine derivatives.
• Patients with biliary obstructive disorders or sever hepatic impairment or cardiogenic shock.
• During pregnancy or breastfeeding. • Do not use with other ACEI or aliskiren in patients with diabetes or renal
impairment or hyperkalemia. • Patients with the rare hereditary condition of fructose intolerance (e.g. products
containing sorbitol).
Safety data for lisinopril/amlodipine
Page 26 of 63
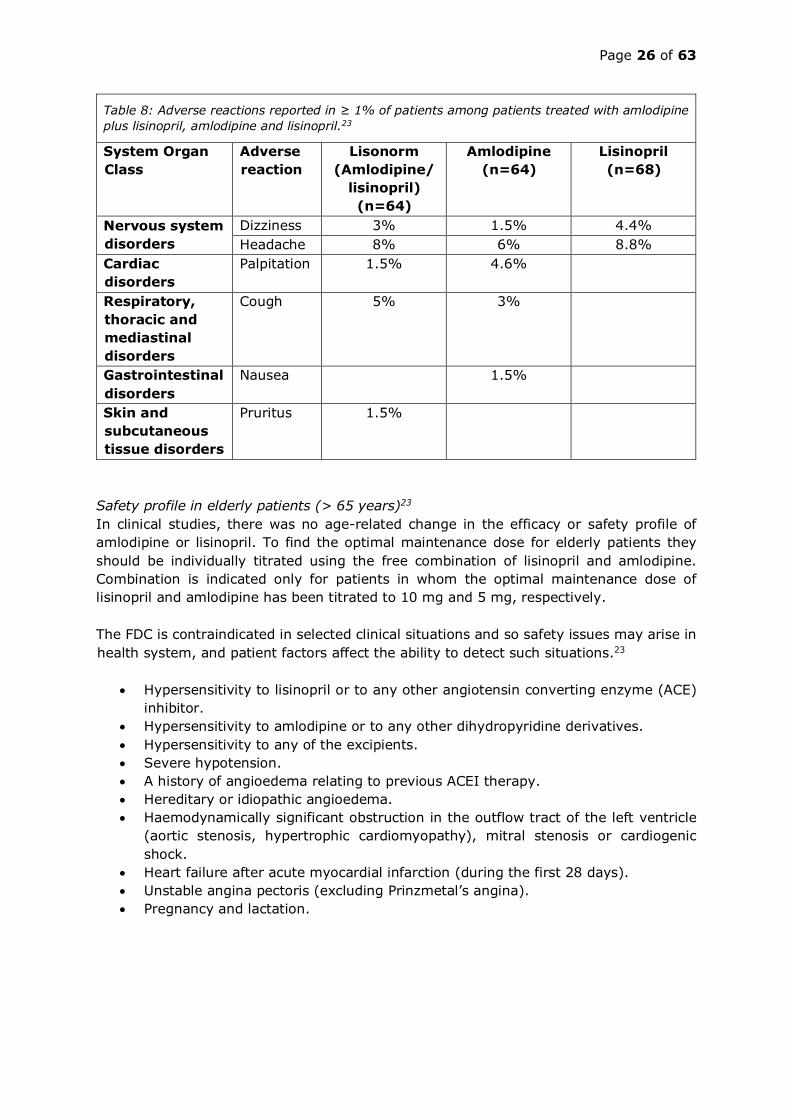
Table 8: Adverse reactions reported in ≥ 1% of patients among patients treated with amlodipine plus lisinopril, amlodipine and lisinopril.23
System Organ Class
Adverse reaction
Lisonorm (Amlodipine/
lisinopril) (n=64)
Amlodipine (n=64)
Lisinopril (n=68)
Nervous system disorders
Dizziness 3% 1.5% 4.4% Headache 8% 6% 8.8%
Cardiac disorders
Palpitation 1.5% 4.6%
Respiratory, thoracic and mediastinal disorders
Cough 5% 3%
Gastrointestinal disorders
Nausea 1.5%
Skin and subcutaneous tissue disorders
Pruritus 1.5%
Safety profile in elderly patients (> 65 years)23 In clinical studies, there was no age-related change in the efficacy or safety profile of amlodipine or lisinopril. To find the optimal maintenance dose for elderly patients they should be individually titrated using the free combination of lisinopril and amlodipine. Combination is indicated only for patients in whom the optimal maintenance dose of lisinopril and amlodipine has been titrated to 10 mg and 5 mg, respectively. The FDC is contraindicated in selected clinical situations and so safety issues may arise in health system, and patient factors affect the ability to detect such situations.23
• Hypersensitivity to lisinopril or to any other angiotensin converting enzyme (ACE) inhibitor.
• Hypersensitivity to amlodipine or to any other dihydropyridine derivatives. • Hypersensitivity to any of the excipients. • Severe hypotension. • A history of angioedema relating to previous ACEI therapy. • Hereditary or idiopathic angioedema. • Haemodynamically significant obstruction in the outflow tract of the left ventricle
(aortic stenosis, hypertrophic cardiomyopathy), mitral stenosis or cardiogenic shock.
• Heart failure after acute myocardial infarction (during the first 28 days). • Unstable angina pectoris (excluding Prinzmetal’s angina). • Pregnancy and lactation.
Page 27 of 63
Safety data for Telmisartan/HCTZ
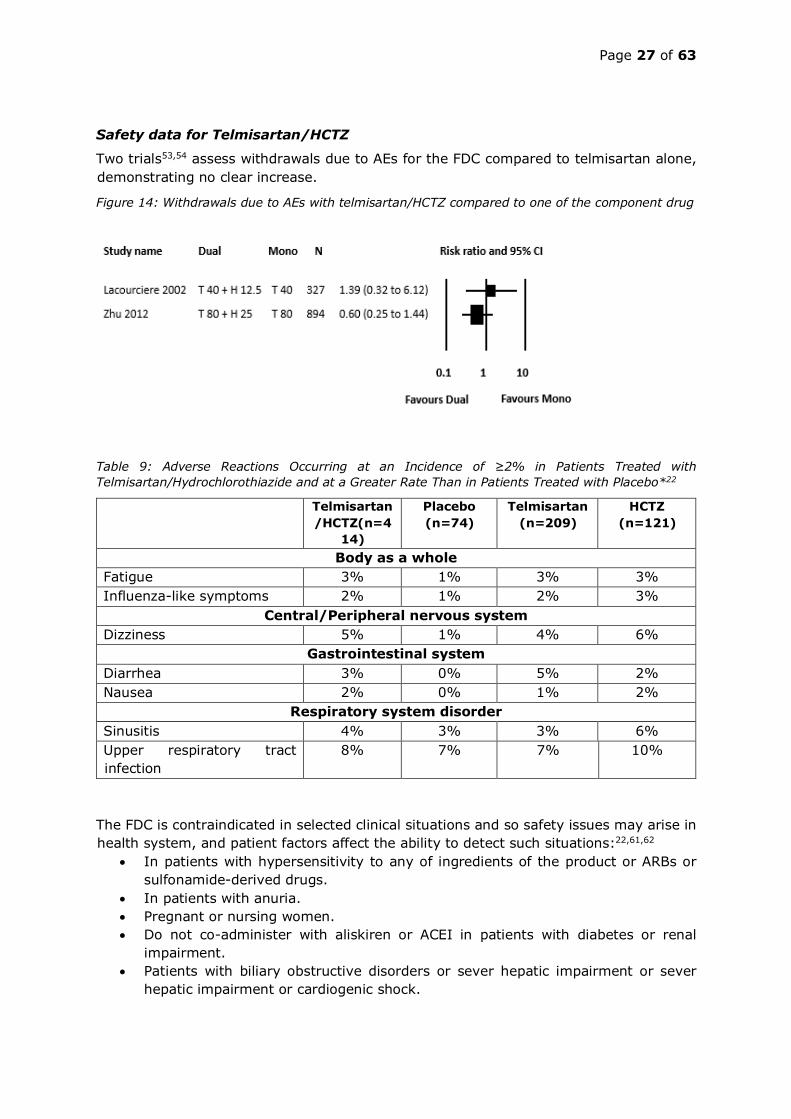
Two trials53,54 assess withdrawals due to AEs for the FDC compared to telmisartan alone, demonstrating no clear increase.
Figure 14: Withdrawals due to AEs with telmisartan/HCTZ compared to one of the component drug
Table 9: Adverse Reactions Occurring at an Incidence of ≥2% in Patients Treated with Telmisartan/Hydrochlorothiazide and at a Greater Rate Than in Patients Treated with Placebo*22
Telmisartan/HCTZ(n=4
14)
Placebo (n=74)
Telmisartan (n=209)
HCTZ (n=121)
Body as a whole Fatigue 3% 1% 3% 3% Influenza-like symptoms 2% 1% 2% 3%
Central/Peripheral nervous system Dizziness 5% 1% 4% 6%
Gastrointestinal system Diarrhea 3% 0% 5% 2% Nausea 2% 0% 1% 2%
Respiratory system disorder Sinusitis 4% 3% 3% 6% Upper respiratory tract infection
8% 7% 7% 10%
The FDC is contraindicated in selected clinical situations and so safety issues may arise in health system, and patient factors affect the ability to detect such situations:22,61,62
• In patients with hypersensitivity to any of ingredients of the product or ARBs or sulfonamide-derived drugs.
• In patients with anuria. • Pregnant or nursing women. • Do not co-administer with aliskiren or ACEI in patients with diabetes or renal
impairment. • Patients with biliary obstructive disorders or sever hepatic impairment or sever
hepatic impairment or cardiogenic shock.

Page 28 of 63
• Patients with the rare hereditary condition of fructose or galactose intolerance (e.g. products containing sorbitol or Lactose).
11. Summary of available data on comparative price of medicines within the pharmacological class or therapeutic group.
Current price insights with respect to global use
We utilized Quintiles IMS (http://www.imshealth.com/) data on 2015-16 medicine sales – by volume and value - in 73 countries globally (North America, 12 countries in South and Central America, 25 countries from Europe and 29 elsewhere). During these years, Lisinopril-HCTZ was the most commonly prescribed ACE-diuretic combination and had the lowest unit price. See table 10. Table 10: Quintiles IMS sales of ACE-diuretic combinations in 2015 and 2016
2015 2016* Stock units sold
(Millions) Average price per pill (Euro)
Stock units sold (Millions)
Average price per pill (Euro)
Lisinopril + HCTZ 7,153 0.08 7,162 0.07 Perindopril + indapamide 5,528 0.24 6,022 0.23 Ramipril + HCTZ 5,089 0.11 5,048 0.11
Enalapril + HCTZ 4,670 0.11 4,553 0.11 Quinapril + HCTZ 825 0.20 747 0.19 Captopril + HCTZ 766 0.12 702 0.11 Zofenopril + HCTZ 504 0.31 518 0.27 Benazepril + HCTZ 485 0.62 467 0.43
Fosinopril + HCTZ 456 0.20 444 0.18 Cilazapril + HCTZ 328 0.16 305 0.16 * Projections made based on Q2 sales
In 11 countries, we utilized Quintles IMS data on 2013-2014 sales of CCB + ARB combinations. See Table 11 for number of medicine units (pills) sold and the average unit price (i.e. price per pill) during these years. Across studied countries, the median of price per pill was 0.19 and 0.17 Euros in years 2013 and 2014, respectively. The USA had the highest unit price, about 170 times the lowest unit price that was from India.
Table 11: CCB+ARB sales in 11 countries 2013 2014 Medicine units
(pills) sold (in Millions)
Average Median price per pill (Euro)
Medicine units (pills) sold (in
Millions)
Average price per pill (Euro)
Australia 1,245,306 0.12 1,557,842 0.11 Brazil 4,214,477 0.16 4,570,294 0.15 China 6,413,435 0.06 9,577,657 0.06 France 3,730,504 0.26 3,844,684 0.27 Germany 2,339,436 0.52 2,484,979 0.51 India 61,204,872 0.01 69,116,835 0.01

Page 29 of 63
Italy 1,820,286 0.19 2,311,639 0.17 Mexico 908,476 0.29 1,029,660 0.31 Turkey 2,853,299 0.04 3,244,745 0.04 UK 77,594 0.26 79,040 0.26 USA 4,540,755 1.50 4,169,954 1.73
Median of average price per pill 0.19 0.17 Procurement prices of proposed FDCs versus single pills: case study from India To understand how the public-sector procurement prices of FDCs compare to that of monotherapy single pills, we conducted online searches to obtain publicly available data from India. Comparison was performed for a sample of FDCs proposed in this petition, for which procurement price data were available for both FDCs and constituent monotherapy pills. We found that procurement prices of combination therapies were similar to the sum of procurement prices of constituting monotherapies. For instance, median procurement price of single pill of FDC Telmisartan 40 mg + Amlodipine 5 mg was Euro 0.0084 (INR 0.673) compared to Euro 0.007 (INR 0.557) for two monotherapy pills. FDC Telmisartan 40 mg + Hydrochlorothiazide 12.5 mg was procured at Euro 0.011 (INR 0.8550) that was comparable to sum of price for two monotherapy pills (Euro 00.009/INR 0.694). See Exhibit A Tab ‘Price compare-procurement’ for detailed procurement price comparisons.
Table 12: Procurement prices of fixed dose combinations versus single pills in India
Procurement prices (FDC) Price per tablet (Euros)
• Telmisartan/HCTZ Telmisartan 40mg/ HCTZ 12.5mg 0.007-0.015 Source: Jan-Aushadi/BPPI (India)
• Lisinopril/Amlodopine Lisinopril 5mg / Amlodopine 5mg 0.004-0.023 Source: Rajasthan/J &K state (India)
• Telmisartan/Amlodopine Telmisartan 40mg / Amlodopine 5mg 0.008–0.014 Source: Central government/ESIC (India) In addition, we obtained procurement prices of various classes of monotherapies from several procurement agencies globally such as UNWRA, Organization of Eastern Caribbean States, Telangana Health and Family Welfare Department, and Thailand Ministry of Public Health. See Table 13 for mean procurement prices for classes of monotherapies. Table 13: Mean procurement prices of various medicine classes from 15 international procurement agencies Medicine class Procurement price (Euro) Mean Min Max CCB 0.011 0.0003 0.27 ARB 0.036 0.026 0.043 ACEi 0.036 0.0032 0.11

Page 30 of 63
HCTZ 0.038 0.0042 0089 Retail prices of proposed FDCs versus single pills: case study from India We conducted systematic searches in MedInd and MIMS-India databases to obtain private-sector retail prices of various FDC brands marketed in India. We also obtained prices of the respective constituent single pills/monotherapies. Table 14 summarizes the unit prices comparisons for various combination medicines and respective constituent monotherapy. We found that retail prices of FDCs were similar if not lower compared to the price of constituent monotherapies. For detailed calculations, see tab ‘Price compare-Retail’ in Exhibit A.
Table 14: Private-sector retail unit price (in INR) in India: FDC versus monotherapy
Fixed dose combination Median (range) unit price
per pill (2018, Euros) Lisinopril 5 mg + Hydrochlorothiazide 12.5 mg 0.060 (0.013 – 0.087) Constituent monotherapy pills Lisinopril 5 mg 0.045 (0.031-0.130) Hydrochlorothiazide 12.5 mg 0.013 (0.008-0.026) Sum of median prices of two monotherapy pills 0.059 Fixed dose combination Telmisartan 40mg + Amlodipine 5 mg 0.090 (0.004-0.120) Constituent monotherapy pills Telmisartan 40mg 0.079 (0.038-0.100) Amlodipine 5 mg 0.026 (0.013-0.053) Sum of median prices of two monotherapy pills 0.11 Fixed dose combination Telmisartan 40 mg + Hydrochlorothiazide 12.5 mg 0.09 (0.004-0.190) Constituent monotherapy pills Telmisartan 40 mg 0.088 (0.038-0.100) Hydrochlorothiazide 12.5 mg 0.013 (0.008-0.026) Sum of median prices of two monotherapy pills 0.093 Note: A full listing of retail and procurement prices is provided (Exhibit A) and manufacturers (Exhibit B) for one country (India)
Evergreening strategies and FDC price points FDCs have in numerous instances been used as ‘evergreening’ strategies, in efforts by originator companies to reduce price erosion once a molecule comes off patent. However, now monotherapy constituents of different dual combination drugs are now off-patent; one reason that various GDCs are available at low cost. Furthermore, we note that dual combination drugs can be more affordable than the same medications as separate pills (see table 14: example of Lisinopril-HCTZ 5-12.5 mg that has a large share in India’s pharmaceutical market).63

Page 31 of 63
Once established on the market, there is often a cost saving from use of dual combination therapy compared to the cost of both the separate products, both from direct medication costs and reduced script fees from a dual combination. However, when combinations first come to a market or are scarce, they attract a price premium. The retail drug prices need to be contextualized within the potential cost-savings from improved hypertension control due to improved compliance,29,30,64 reduced need for repeat visits to achieve BP control and with the use of FDC in settings where individuals requiring more than one BP lowering drug may have limited access to multiple drug classes.65,66 In a meta-analysis67 published in 2011, the annual total health care costs from 44,336 patients in all included observational studies (n = 7) were lower for patients treated with FDC compared to individual monotherapy for hypertension (mean pooled difference -1357.01 USD; 95% CI -1935.49 USD, -778.53 USD). An analysis using data from the 2004 Medical Expenditure Panel Survey in the United States demonstrated that total monthly prescription expenditures were lower for 23 of 27 FDC medications examined compared to the separate individual drugs68 (mean decrease in monthly total costs $20.89, 95% CI $20.10, $21.68). Using pharmacy claims data in Japan, a study demonstrated transitioning to FDC therapy from separate drugs was associated with an annual saving of $112 for patients.69 The cost savings of FDC therapy for patients also translate to the larger health system. In Canada, 60-100% of patients receiving two separate drugs transitioning to FDC therapy would lead to an estimated yearly cost-saving of $27 to $45 million.70 Implications on cost of FDC for hypertension if added to WHO EML Given the large and growing global burden of hypertension and the increasing and political attention to non-communicable diseases, addition of FDCs for hypertension as a WHO essential medicines prompt other nations to follow, thereby reducing overall healthcare and societal costs for patients and governments – while allowing more people to be treated. In discussing implications of EML listing, Magrini et al71 indicated that: “Previous expert committees have recognized the message that comes with identifying a medicine as essential. In some cases, medicines have been included in the core list to underscore their importance, for example, antiretrovirals in 2002.72 In other cases, the model list has been used to stimulate the entry of new manufacturers for products that are not widely available, such as with zinc sulfate in 2005 and rectal artesunate in 2009. Inclusion of effective but expensive medicines in the model list may also focus the attention of all stakeholders on the need to increase affordability and access to essential medicines.” The addition of FDC for hypertension to the WHO EML is an example, in our view, where reduced costs will be a consequence, not a precondition, to listing. Listing of FDC for hypertension could stimulate new manufacturers of products and sharpen attention on FDC costs, as seen for FDC for tuberculosis and HIV/AIDS.63

Page 32 of 63
12. Summary of regulatory status of the medicine
Availability of the proposed FDCs is outlined in the Table below, indicating widespread availability. However, numerous countries do not have all four options, which supports the rationale for a square box listing for each FDC, since alternative acceptable options are widely available.
Table 15: Availability of various formulations of proposed FDCs in the United States, Europe, Canada and other countries.
Country Lisinopril /HCTZ
Telmisartan-/amlodipine
Lisinopril /amlodipine
Telmisartan /HCTZ
Canada
10mg/12.5mg 20 mg/12.5mg 20mg/25mg
40mg/5mg 40mg/10mg 80mg/5mg 80mg/10mg n/a
80mg/12.5mg 80mg/25mg
Australia n/a
40mg/5mg 40mg/10mg 80mg/5mg 80mg/10mg n/a
40mg/12.5mg 80mg/12.5 mg 80mg/25 mg
China n/a n/a n/a 80mg/12.5mg 40mg/12.5mg
Ethiopia 10mg/12.5mg n/a n/a
Europe
10mg/12.5mg 20mg/12.5mg 20mg/25mg
40mg/5mg 40mg/10mg 80mg/5mg 80mg/10mg
10mg/5mg 20mg/5mg 20mg/10mg
40mg/12.5mg 80mg/12.5mg 80mg/25mg
India
2.5mg/12.5mg 5mg/12.5mg 5mg/25mg 10mg/12.5mg
40mg/5mg 80mg/5mg
2.5mg/2.5mg 5mg/5mg
40mg/12.5mg 80mg/12.5mg
Russia 10mg/12.5mg 20mg/12.5mg
40mg/5mg 40mg/10mg 80mg/5mg 80mg/10mg
10mg/5mg 20mg/10mg
40mg/12.5mg 80mg/12.5mg
Thailand n/a
40mg/5mg 40mg/10mg 80mg/5mg 80mg/10mg n/a
40mg/12.5mg 80mg/12.5mg
Turkey
12.5mg/10mg 12.5mg/20mg 20mg/12.5mg 20mg/25mg
80mg/5mg 80mg/10mg n/a
80mg/12.5m 80mg/25mg
United Kingdom 10mg/12.5mg 20mg/12.5mg NA
10mg/5mg 20mg/5mg 20mg/10mg
40mg/12.5mg 80mg/12.5mg 80mg/25mg

Page 33 of 63
Unites States
10mg/12.5mg 20mg/12.5mg 20mg/25mg
40mg/5mg 40mg/10mg 80mg/5mg 80m/10mg n/a
40mg/12.5mg 80mg/12.5ng 80mg/25mg
n/a=Not available. A listing of manufacturers for selected regions is provided in Appendix 14. Note: A full list of manufacturers and date of approvals in the United States (FDA) and Europe (European Medicine Association) is provided in Exhibit C.
13. Availability of pharmacopoeial standards (British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia, European Pharmacopeia).
These are summarised in the following table: Pharmacopoeia Lisinopril
/HCTZ Telmisartan-/amlodipine
Lisinopril /amlodipine
Telmisartan /HCTZ
British Pharmacopoeia
Both drugs are available as separate substances
Both drugs are available as separate substances
Both drugs are available as separate substances
Both drugs available as separate substances
The International Pharmacopoeia
Only HCTZ is available
neither of the two drugs are available
neither of the two drugs are available
Only HCTZ is available
The United States Pharmacopoeia
Both drugs are available as separate substances
Both drugs are available as separate substances
Both drugs are available as separate substances
Available
The European Pharmacopoeia
Both drugs are available as separate substances
Both drugs are available as separate substances
Both drugs are available as separate substances
Both drugs are available as separate substances

Page 34 of 63
14. References
1 Mills KT, Bundy JD, Kelly TN, et al. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation 2016; 134: 441–50. doi:10.1161/CIRCULATIONAHA.115.018912.
2 Mohammad H. Forouzanfar P, Patrick Liu BS, Gregory A. Roth MD, Marie Ng P, Stan Biryukov BS, Laurie Marczak P. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990-2015 2017; 317: 165–82.
3 Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013; 310: 959–68. doi:10.1001/jama.2013.184182.
4 Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension (Dallas, Tex. : 1979) 2003; 42: 1206–52. doi:10.1161/01.HYP.0000107251.49515.c2.
5 Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Journal of hypertension 2013; 31: 1281–357. doi:10.1097/01.hjh.0000431740.32696.cc.
6 Hackam DG, Khan NA, Hemmelgarn BR, et al. The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 - therapy. The Canadian journal of cardiology 2010; 26: 249–58.
7 Krause T, Lovibond K, Caulfield M, McCormack T, Williams B. Management of hypertension: summary of NICE guidance. BMJ (Clinical research ed.) 2011; 343: d4891. doi:10.1136/bmj.d4891.
8 Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology 2017: 24430.
9 Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Journal of hypertension 2013; 31: 1281–357. doi:10.1097/01.hjh.0000431740.32696.cc.
10 Indian guidelines on hypertension (I.G.H.) - III. 2013. The Journal of the Association of Physicians of India 2013; 61: 6–36.
11 Liu L-S. 2010 Chinese guidelines for the management of hypertension. Zhonghua xin xue guan bing za zhi 2011; 39: 579–615.
12 Peera Buranakitjaroen., Surapun Sitthisook., Tuangsit Wataganara., et al. 2015 Thai Hypertension Guideline. http://www.thaihypertension.org/files/2015%20Thai%20Hypertension%20Guideline.pdf.
13 HEARTS Technical package for cardiovascular disease management in primary health care: evidence-based treatment protocols. Geneva: World Health Organization; 2018 (WHO/NMH/NVI/18.2). Licence: CC BY-NC-SA 3.0 IGO.

Page 35 of 63
14 Wright JT, JR, Williamson JD, Whelton PK, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. The New England journal of medicine 2015; 373: 2103–16. doi:10.1056/NEJMoa1511939.
15 Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death. A systematic review and meta-analysis. The Lancet 2016; 387: 957–67. doi:10.1016/S0140-6736(15)01225-8.
16 Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. The American journal of medicine 2009; 122: 290–300. doi:10.1016/j.amjmed.2008.09.038.
17 Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ (Clinical research ed.) 2009; 338: b1665. doi:10.1136/bmj.b1665.
18 FDA Briefing Document. Cardiovascular and Renal Drugs Advisory Committee Meeting September 10, 2014 To discuss the potential clinical utility of fixed combination prescription drugs composed of an antihypertensive drug, aspirin, and a statin administered to reduce the risk of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke in patients with a history of cardiovascular disease. 2014.
19 AstraZeneca Canada Inc. ZESTORETIC Product monograph. Health Canada. http://www.hc-sc.gc.ca/dhp-mps/prodpharma/databasdon/index-eng.php (accessed Apr 24, 2018).
20 AstraZeneca UK Limited. ZESTORETIC Summary of product charecteristics. MHRA (accessed Apr 24, 2018).
21 Boehringer Ingelheim Pharmaceuticals I. TWYNSTA Prescribing information. Health Canada. https://pdf.hres.ca/dpd_pm/00033456.PDF (accessed Apr 24, 2018).
22 Boehringer Ingelheim Pharmaceuticals I. MICARDIS plus Public assessment report. MHRA. http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con677930.pdf (accessed Apr 24, 2018).
23 Lisonorm and associated products. Summary of Product Characteristics. EMEA. http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_document/Lisonorm_29/WC500007804.pdf (accessed Apr 24, 2018).
24 Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet (London, England) 2003; 362: 1527–35.
25 Council ESH, Redon J, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension. European Heart Journal 2013; 34: 2159–219.
26 Xie X, Atkins E, Lv J, et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta-analysis. Lancet (London, England) 2016; 387: 435–43. doi:10.1016/S0140-6736(15)00805-3.
27 Seedat YK, Rayner BL, Veriava Y. South African hypertension practice guideline 2014. Cardiovascular journal of Africa 2014; 25: 288–94. doi:10.5830/CVJA-2014-062.
28 National Heart Foundation of Australia. Guideline for the diagnosis and management of hypertension in adults - 2016. (accessed Dec 19, 2016).
29 Mallat SG, Tanios BY, Itani HS, Lotfi T, Akl EA. Free versus Fixed Combination Antihypertensive Therapy for Essential Arterial Hypertension: A Systematic Review and Meta-Analysis. PloS one 2016; 11: e0161285. doi:10.1371/journal.pone.0161285.

Page 36 of 63
30 Gupta AK, Arshad S, Poulter NR. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: a meta-analysis. Hypertension (Dallas, Tex. : 1979) 2010; 55: 399–407. doi:10.1161/HYPERTENSIONAHA.109.139816.
31 James McCormack. Blood Pressure Medicines for Five Years to Prevent Death, Heart Attacks, and Strokes. http://www.thennt.com/nnt/anti-hypertensives-to-prevent-death-heart-attacks-and-strokes/ (accessed Apr 19, 2018).
32 Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination Therapy Versus Monotherapy in Reducing Blood Pressure: Meta-analysis on 11,000 Participants from 42 Trials. The American journal of medicine 2009; 122: 290–300. doi:10.1016/j.amjmed.2008.09.038.
33 Feldman RD, Zou GY, Vandervoort MK, Wong CJ, Nelson SAE, Feagan BG. A simplified approach to the treatment of uncomplicated hypertension. A cluster randomized, controlled trial. Hypertension (Dallas, Tex. : 1979) 2009; 53: 646–53. doi:10.1161/HYPERTENSIONAHA.108.123455.
34 Mourad J-J, Waeber B, Zannad F, Laville M, Duru G, Andréjak M. Comparison of different therapeutic strategies in hypertension. A low-dose combination of perindopril/indapamide versus a sequential monotherapy or a stepped-care approach. Journal of hypertension 2004; 22: 2379–86.
35 MacDonald TM, Williams B, Webb DJ, et al. Combination Therapy Is Superior to Sequential Monotherapy for the Initial Treatment of Hypertension. A Double-Blind Randomized Controlled Trial. Journal of the American Heart Association 2017; 6. doi:10.1161/JAHA.117.006986.
36 Lonn EM, Bosch J, Lopez-Jaramillo P, et al. Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease. The New England journal of medicine 2016; 374: 2009–20. doi:10.1056/NEJMoa1600175.
37 Chrysant SG. Antihypertensive Effectiveness of Low-Dose Lisinopril-Hydrochlorothiazide Combination. Arch Intern Med 1994; 154: 737. doi:10.1001/archinte.1994.00420070047005.
38 Leeuw PW de, Notter T, Zilles P. Comparison of different fixed antihypertensive combination drugs: a double-blind, placebo-controlled parallel group study. Journal of hypertension 1997; 15: 87–91.
39 McInnes GT, O'Kane KP, Istad H, Keinanen-Kiukaanniemi S, van Mierlo HF. Comparison of the AT1-receptor blocker, candesartan cilexetil, and the ACE inhibitor, lisinopril, in fixed combination with low dose hydrochlorothiazide in hypertensive patients. Journal of human hypertension 2000; 14: 263–69.
40 Littlejohn TW, Majul CR, Olvera R, et al. Results of treatment with telmisartan-amlodipine in hypertensive patients. Journal of clinical hypertension (Greenwich, Conn.) 2009; 11: 207–13. doi:10.1111/j.1751-7176.2009.00098.x.
41 Zhu D, Gao P, Holtbruegge W, Huang C. A randomized, double-blind study to evaluate the efficacy and safety of a single-pill combination of telmisartan 80 mg/amlodipine 5 mg versus amlodipine 5 mg in hypertensive Asian patients. The Journal of international medical research 2014; 42: 52–66. doi:10.1177/0300060513503756.
42 Neutel JM, Mancia G, Black HR, et al. Single-pill combination of telmisartan/amlodipine in patients with severe hypertension. Results from the TEAMSTA severe HTN study. Journal of clinical hypertension (Greenwich, Conn.) 2012; 14: 206–15. doi:10.1111/j.1751-7176.2012.00595.x.
43 Sharma AM, Bakris G, Neutel JM, et al. Single-pill combination of telmisartan/amlodipine versus amlodipine monotherapy in diabetic hypertensive patients. An 8-week randomized, parallel-group, double-blind trial. Clinical therapeutics 2012; 34: 537–51. doi:10.1016/j.clinthera.2012.02.004.

Page 37 of 63
44 Neldam S, Edwards C, Jones R. Switching patients with uncontrolled hypertension on amlodipine 10 mg to single-pill combinations of telmisartan and amlodipine. Results of the TEAMSTA-10 study. Current medical research and opinion 2011; 27: 2145–53. doi:10.1185/03007995.2011.624089.
45 Neldam S, Lang M, Jones R. Telmisartan and amlodipine single-pill combinations vs amlodipine monotherapy for superior blood pressure lowering and improved tolerability in patients with uncontrolled hypertension. Results of the TEAMSTA-5 study. Journal of clinical hypertension (Greenwich, Conn.) 2011; 13: 459–66. doi:10.1111/j.1751-7176.2011.00468.x.
46 Sharma A, Bagchi A, Kinagi SB, Sharma YK, Baliga VP, Bollmall C. Results of a comparative, phase III, 12-week, multicenter, prospective, randomized, double-blind assessment of the efficacy and tolerability of a fixed-dose combination of telmisartan and amlodipine versus amlodipine monotherapy in Indian adults with stage II hypertension. Clinical therapeutics 2007; 29: 2667–76. doi:10.1016/j.clinthera.2007.12.017.
47 Jagodzinski A, Neumann JT, Ojeda F, et al. Cardiovascular Biomarkers in Hypertensive Patients with Medical Treatment-Results from the Randomized TEAMSTA Protect I Trial. Clinical chemistry 2017; 63: 1877–85. doi:10.1373/clinchem.2017.275289.
48 Neldam S, Dahlöf B, Oigman W, Schumacher H. Early combination therapy with telmisartan plus amlodipine for rapid achievement of blood pressure goals. International journal of clinical practice 2013; 67: 843–52. doi:10.1111/ijcp.12180.
49 Center for Drug Evaluation and Research. Clinical and Statistical Review - application number 022401. Twynsta - telmisartan-amlodipine 2009. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022401_twynsta_toc.cfm (accessed Apr 11, 2018).
50 McGill JB, Reilly PA. Telmisartan plus hydrochlorothiazide versus telmisartan or hydrochlorothiazide monotherapy in patients with mild to moderate hypertension. A multicenter, randomized, double-blind, placebo-controlled, parallel-group trial. Clinical therapeutics 2001; 23: 833–50.
51 White WB, Punzi HA, Murwin D, Koval SE, Davidai G, Neutel JM. Effects of the angiotensin II receptor blockers telmisartan vs valsartan in combination with hydrochlorothiazide 25 mg once daily for the treatment of hypertension. J Clin Hypertension 2006; 8: 626–33.
52 Lacourcière Y, Tytus R, O'Keefe D, Lenis J, Orchard R, Martin K. Efficacy and tolerability of a fixed-dose combination of telmisartan plus hydrochlorothiazide in patients uncontrolled with telmisartan monotherapy. J Hum Hypertens 2001; 15: 763–70. doi:10.1038/sj.jhh.1001267.
53 Lacourcière Y, Martin K. Comparison of a fixed-dose combination of 40 mg telmisartan plus 12.5 mg hydrochlorothiazide with 40 mg telmisartan in the control of mild to moderate hypertension. American journal of therapeutics 2002; 9: 111–17.
54 Zhu DL, Bays H, Gao P, Mattheus M, Voelker B, Ruilope LM. Efficacy and tolerability of initial therapy with single-pill combination telmisartan/hydrochlorothiazide 80/25 mg in patients with grade 2 or 3 hypertension. A multinational, randomized, double-blind, active-controlled trial. Clinical therapeutics 2012; 34: 1613–24. doi:10.1016/j.clinthera.2012.05.007.
55 Neldam S, Edwards C. Results of increasing doses of hydrochlorothiazide in combination with an angiotensin receptor blocker in patients with uncontrolled hypertension. J Clin Hypertension 2008; 10: 612–18.
56 Derosa G, Querci F, Franzetti I, Dario Ragonesi P, D'Angelo A, Maffioli P. Comparison of the effects of barnidipine+losartan compared with telmisartan+hydrochlorothiazide

Page 38 of 63
on several parameters of insulin sensitivity in patients with hypertension and type 2 diabetes mellitus. Hypertension research : official journal of the Japanese Society of Hypertension 2015; 38: 690–94. doi:10.1038/hr.2015.57.
57 White WB, Murwin D, Chrysant SG, Koval SE, Davidai G, Guthrie R. Effects of the angiotensin II receptor blockers telmisartan versus valsartan in combination with hydrochlorothiazide. A large, confirmatory trial. Blood pressure monitoring 2008; 13: 21–27. doi:10.1097/MBP.0b013e3282f3859d.
58 Cappuccio FP, Markandu ND, Singer DR, MacGregor GA. Amlodipine and lisinopril in combination for the treatment of essential hypertension. Efficacy and predictors of response. Journal of hypertension 1993; 11: 839–47.
59 Alvogen Malta. ZESTORETIC Prescribing information. FDA. http://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=BasicSearch.process (accessed Apr 24, 2018).
60 Boehringer Ingelheim Pharmaceuticals I. TWYNSTA Prescribing information. FDA. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022401s019lbl.pdf (accessed Apr 24, 2018).
61 Boehringer Ingelheim Pharmaceuticals I. MICARDIS HCT Prescribing information. FDA. https://www.accessdata.fda.gov/drugsatfda_docs/label/2000/21162lbl.pdf (accessed Apr 24, 2018).
62 Boehringer Ingelheim Pharmaceuticals I. MICARDIS plus Product Monograph. Health Canada. https://pdf.hres.ca/dpd_pm/00038160.PDF (accessed Apr 24, 2018).
63 Hoen E’t, Berger J, Calmy A, Moon S. Driving a decade of change. HIV/AIDS, patents and access to medicines for all. Journal of the International AIDS Society 2011; 14: 15.
64 Bangalore S, Kamalakkannan G, Parkar S, Messerli FH. Fixed-dose combinations improve medication compliance. A meta-analysis. The American journal of medicine 2007; 120: 713–19. doi:10.1016/j.amjmed.2006.08.033.
65 Attaei MW, Khatib R, McKee M, et al. Availability and affordability of blood pressure-lowering medicines and the effect on blood pressure control in high-income, middle-income, and low-income countries. An analysis of the PURE study data. The Lancet Public Health 2017; 2: e411-e419. doi:10.1016/S2468-2667(17)30141-X.
66 Khatib R, McKee M, Shannon H, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries. An analysis of the PURE study data. The Lancet 2016; 387: 61–69. doi:10.1016/S0140-6736(15)00469-9.
67 Sherrill B, Halpern M, Khan S, Zhang J, Panjabi S. Single-pill vs free-equivalent combination therapies for hypertension. A meta-analysis of health care costs and adherence. Journal of clinical hypertension (Greenwich, Conn.) 2011; 13: 898–909. doi:10.1111/j.1751-7176.2011.00550.x.
68 Rabbani A, Alexander GC. Out-of-pocket and total costs of fixed-dose combination antihypertensives and their components. American journal of hypertension 2008; 21: 509–13. doi:10.1038/ajh.2008.31.
69 Akazawa M, Fukuoka K. Economic impact of switching to fixed-dose combination therapy for Japanese hypertensive patients. A retrospective cost analysis. BMC health services research 2013; 13: 124. doi:10.1186/1472-6963-13-124.
70 Stankus V, Hemmelgarn B, Campbell NRC, Chen G, McAlister FA, Tsuyuki RT. Reducing costs and improving hypertension management. The Canadian journal of clinical pharmacology = Journal canadien de pharmacologie clinique 2009; 16: e151-5.
71 Magrini N, Robertson J, Forte G, et al. Tough decisions on essential medicines in 2015. Bulletin of the World Health Organization 2015; 93: 283–84.

Page 39 of 63
72 The selection and use of essential medicines: report of the WHO Expert Committee, 2013 [WHO technical report series No. 985]. Geneva: World Health Organization; 2014.
73 Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. The New England journal of medicine 2008; 358: 2560–72. doi:10.1056/NEJMoa0802987.
74 Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. The Lancet 2001; 358: 1033–41. doi:10.1016/S0140-6736(01)06178-5.
75 Hypertension-Stroke Cooperative Study Group. Effect of Antihypertensive Treatment on Stroke Recurrence: Hypertension-Stroke Cooperative Study Group.
76 A. Barham Carter. Hypotensive therapy in stroke survivors. 77 Dahlöf B, Hansson L, Lindholm LH, Scherstén B, Ekbom T, Wester P-O. Morbidity and
mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). The Lancet 1991; 338: 1281–85. doi:10.1016/0140-6736(91)92589-T.
78 Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. British medical journal (Clinical research ed.) 1986; 293: 1145–51.
79 Bulpitt CJ, Beckett NS, Peters R, et al. Blood pressure control in the Hypertension in the Very Elderly Trial (HYVET). Journal of human hypertension 2012; 26: 157–63. doi:10.1038/jhh.2011.10.
80 Smith WM. Treatment of mild hypertension: results of a ten-year intervention trial. Circulation research 1977; 40: I98-105.
81 Effects of treatment on morbidity in hypertension. II. Results in patients with diastolic blood pressure averaging 90 through 114 mm Hg. JAMA 1970; 213: 1143–52.
82 Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg. JAMA 1967; 202: 1028–34.

Page 40 of 63
Appendix 1: Gender-specific hypertension awareness, treatment, and control in 2010 in countries with data by world region
Country Awareness Treatment Control (among treated) Control (among
hypertension) Men Women Men Women Men Women Men Women
High Income Economies Australia -- -- 52.5 59.1 58.7 55.8 30.8 33.0 Chile 55.2 75.6 25.8 49.5 33.8 50.1 8.7 24.8 Czech Republic 68.4 71.4 58.2 58.9 41.9 42.2 24.4 24.9 Finland 63.3 72.7 31.3 39.9 33.8 39.9 10.6 15.9 France 46.9 58.8 41.0 62.0 41.7 58.4 17.1 36.2 Germany 77.9 86.6 -- -- -- -- -- -- Ireland -- -- 30.4 45.2 27.8 40.7 8.5 18.4 Japan -- -- 47.1 51.4 32.5 41.6 36.9 49.4 Korea, Rep. 58.5 76.1 51.7 71.3 70.5 68.4 15.3 21.4 Luxembourg 38.5 42.4 -- -- -- -- -- -- Puerto Rico 82.9 80.7 71.4 76.5 -- -- -- -- Russian Federation
53.3 64.9 42.4 54.2 14.3 22.5 6.1 12.2
Saudi Arabia 35.6 52.0 33.1 42.7 32.0 41.1 7.5 13.6 Singapore 70.8 77.2 -- -- -- -- -- -- Spain 50.9 64.6 -- -- -- -- -- -- Sweden -- -- 45.6 55.7 50.3 46.2 22.9 25.7 Switzerland 60.0 65.0 46.0 52.0 45.0 50.0 21.0 26.0 United Kingdom 61.0 66.0 52.4 58.2 61.8 59.8 32.4 34.8 United States 78.1 84.4 69.3 79.2 69.6 68.1 48.3 54.1 Uruguay 54.8 82.0 43.3 68.3 36.8 52.9 15.9 36.1
East Asia and Pacific China 30.4 36.7 20.6 27.7 17.0 15.5 3.5 4.3 Mongolia 25.7 51.3 28.1 54.1 26.7 39.6 7.5 21.4 Thailand 39.5 59.4 30.3 51.3 -- -- -- --

Page 41 of 63
Country Awareness Treatment Control (among treated) Control (among
hypertension) Men Women Men Women Men Women Men Women
Vietnam 37.9 53.2 22.1 36.7 28.0 40.3 3.8 9.9 Europe and Central Asia
Albania 14.4 29.9 6.1 16.7 19.7 17.9 1.2 3.0 Armenia 25.8 25.7 10.3 19.1 23.1 36.6 2.4 7.0 Azerbaijan 17.6 53.0 12.0 46.2 36.2 47.6 4.4 22.0 Bosnia 40.2 57.2 35.5 54.2 25.4 41.0 9.0 22.2 Romania 62.2 75.6 49.7 66.9 27.4 23.6 13.6 15.8 Serbia 48.6 66.5 56.2 63.2 18.8 22.1 10.6 14.0 Turkey 36.9 55.7 23.6 38.9 -- -- -- -- Ukraine 31.9 64.6 16.8 57.4 21.9 20.9 3.7 12.0
Latin America and the Caribbean Argentina 46.7 64.6 32.6 52.1 31.6 37.4 10.3 19.5 Brazil -- -- 44.0 73.0 30.3 47.7 13.3 34.9 Cuba 54.8 76.0 44.1 67.9 46.2 49.4 20.3 33.5 Jamaica 30.6 69.6 21.0 57.8 31.2 44.9 6.6 26.0 Mexico 24.8 41.0 17.4 33.8 17.4 24.9 3.0 8.4 Panama 53.1 73.6 51.9 71.9 35.3 50.9 17.9 34.6 Peru 45.4 50.5 35.7 43.4 34.7 36.2 12.4 15.7
Middle East and North Africa Algeria -- -- 22.2 39.6 20.5 24.3 4.5 9.6 Egypt 55.7 79.7 33.9 48.5 50.7 55.7 17.2 27.0 Iran, Islamic Rep. 22.5 44.7 16.1 33.1 25.7 23.5 4.1 7.7
Jordan 54.7 56.7 36.7 35.1 42.9 38.2 15.6 13.5 Tunisia 28.8 44.8 24.6 37.9 27.5 22.8 6.5 8.6 Yemen 40.7 47.6 36.5 43.6 17.2 28.8 6.3 12.5
South Asia India 20.4 36.7 14.2 19.2 51.4 40.8 7.3 7.8

Page 42 of 63
Country Awareness Treatment Control (among treated) Control (among
hypertension) Men Women Men Women Men Women Men Women
Sub-Saharan Africa Angola 15.3 27.5 -- -- -- -- -- -- Ghana 12.8 17.7 9.6 10.6 20.6 12.8 2.0 1.4 Kenya 26.5 57.6 16.2 39.4 9.1 26.9 1.5 10.6 Mozambique 10.6 18.4 3.5 11.2 28.7 42.9 1.0 4.8 Senegal 21.2 50.3 14.3 36.5 17.9 27.7 2.6 10.1 South Africa 12.1 25.1 10.1 22.3 20.1 19.3 2.0 4.3

Page 43 of 63
Appendix 2: Summary of characteristics of RCTs that assessed the effects of combination therapy of BP lowering drugs compared to placebo/no treatment on CV outcomes
Study Design participants BP Eligibility Sample size Females (%) Mean age,
years Interventions Follow
up years
Baseline SBP/DBP
Achieved red. in
SBP/DBP
ADVANCE73 DB, PC, PB, MC
DM2, High Risk for CVD
No BP criteria
11140 4735 (43) 66 perindopril + indapamide
4.3 145/81 -5.6/-2.2
PROGRESS74 DB, PC, PG, MC
Stroke / TIA ± HTN
No BP criteria
3544 1852 (30) 64 perindopril + indapamide
3.9 147/86 -9/-4
HSCSG75 DB, PC, PG, MC
HTN, Stroke/TIA
SBP 140-220, DBP 90-116
452 187 (41)
59 Methyclothiazide + deserpidine
3 164/100 -25/-12
Carter76 OL, PG, SC Stroke, HTN SBP <160 or DBP>110
99 43 (44)
64 methyldopa + bethanidine/debrisoquine
4 >160/>110 -17/-9
STOP77 DB, PC, PG, MC
HTN SBP 160-219, DBP< 90
1627 1019 (63) 76
HCTZ/ amiloride/ atenolol/metoprolol/pindolol ± beta-blocker/diuretic
2.1 170/77 -19.5/-8.1
HEP78 OL, PC, PG, MC
Elderly, HTN SBP 170-280, DBP 105-120
884 611 (69)
69 atenolol ± bendrofluazide
4.4 196/99 -18/-11
HYVET79 DB, PC, PB, MC
Elderly (≥80 yrs), HTN
SBP160-199 3845 2326 (60) 84 indapamide ± perindopril
2.1 173/90.8 -15/-6.1
USPHS80 PG, MC HTN DBP 90-115 389 78 (20)
44 chlorthalidone + rauwolfia
7 147/99 -15.9/-10
VA-281 DB, PC, PG, MC
HTN DBP 90-114 380 0 (0)
51 HCTZ + reserpine + hydralazine
18 164/104 -31.4/-18.4

Page 44 of 63
DB=Double Blind, PC=Placebo Controlled, PG=Parallel Group, MC=Multicenter, HTN=Hypertension, CVD=Cardiovascular
VA-182 DB, PC, PG, MC
HTN DBP 115-129
143 0 (0)
51 HCTZ + reserpine + hydralazine
1.5 186/121 -39.4/-26.8
HOPE 336 DB, PC, PG, MC
Intermediate CV risk, no CVD
No BP criteria
12705 5874 (46) 66 candesartan + HCTZ
5.6 138/82 -6/-3
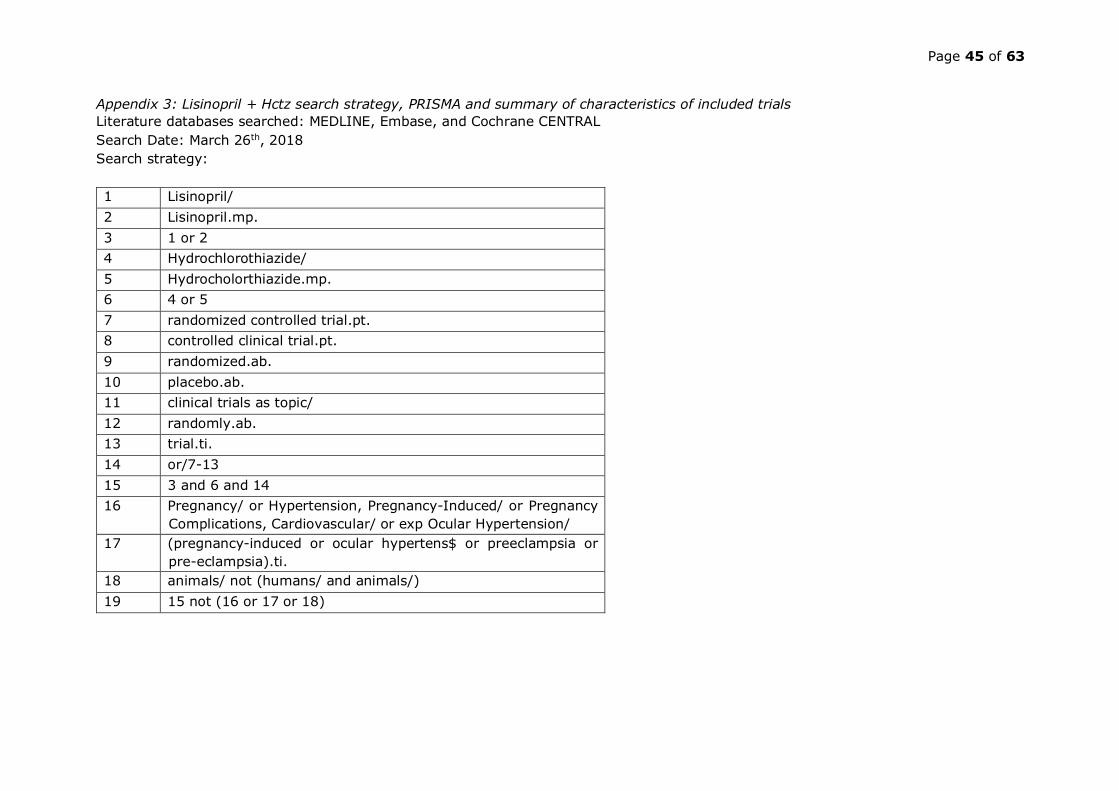
Page 45 of 63
Appendix 3: Lisinopril + Hctz search strategy, PRISMA and summary of characteristics of included trials Literature databases searched: MEDLINE, Embase, and Cochrane CENTRAL Search Date: March 26th, 2018 Search strategy: 1 Lisinopril/ 2 Lisinopril.mp. 3 1 or 2 4 Hydrochlorothiazide/ 5 Hydrocholorthiazide.mp. 6 4 or 5 7 randomized controlled trial.pt. 8 controlled clinical trial.pt. 9 randomized.ab. 10 placebo.ab. 11 clinical trials as topic/ 12 randomly.ab. 13 trial.ti. 14 or/7-13 15 3 and 6 and 14 16 Pregnancy/ or Hypertension, Pregnancy-Induced/ or Pregnancy
Complications, Cardiovascular/ or exp Ocular Hypertension/ 17 (pregnancy-induced or ocular hypertens$ or preeclampsia or
pre-eclampsia).ti. 18 animals/ not (humans/ and animals/) 19 15 not (16 or 17 or 18)

Page 46 of 63
Appendix 4: Lisinopril + HCTZ PRISMA flow chart

Page 47 of 63
Appendix 5: Summary of characteristics of included trials for assessing lisinopril + HCTZ
Author/Study Year Design Eligibility Sample size
BP measure for
outcome assessment
Males, %
Mean age, years
SBP, mmHg
DBP, mmHg
Interventions, dose in mg/day Treatment duration,
weeks
Chrysant37 1994 DB, PC, PG, MC
seDBP 100 to 114
505 seated 62 53 154.0 104 lisinopril 10 + HCTZ 25 vs. lisinopril 10 + HCTZ 12.5 vs. lisinopril 10 vs. HCTZ 25 vs. HCTZ 12.5 vs. placebo
12
Leeuw38 1996 DB, PC, PG, MC
suDBP 101-114 after 4 weeks on Placebo washout
215 seated 53.2 55 169.8 106.8 lisinopril 20 + HCTZ 12.5 vs. atenolol 100 + chlorthalidone 25 vs. verapamil 180 + trandolapril 2 vs. placebo
8
Mcinnes39 2000 DB, PG, MC
seDBP 95–114 after 2 weeks on any monotherapy
353 seated 55 57 166.3 102.4 lisinopril 10 + HCTZ 12.5 vs. candesartan 8 + HCTZ 12.5
26
DB=double blind, MC=multicentre, AC=active controlled, PG=parallel group, se=seated, su=supine, HCTZ=hydrochlorothiazide, NR=not reported

Page 48 of 63
Appendix 6: Telmisartan + Amlodipine search strategy, PRISMA and Summary of characteristics of included trials Literature databases searched: MEDLINE, Embase, and Cochrane CENTRAL Search Date: April 3rd, 2018 Search strategy: 1 Telmisartan.tw. 2 Telmisartan.mp. 3 1 or 2 4 Amlodipine/ 5 Amlodipine.mp. 6 4 or 5 7 randomized controlled trial.pt. 8 controlled clinical trial.pt. 9 randomized.ab. 10 placebo.ab. 11 clinical trials as topic/ 12 randomly.ab. 13 trial.ti. 14 or/7-13 15 3 and 6 and 14 16 Pregnancy/ or Hypertension, Pregnancy-Induced/ or Pregnancy
Complications, Cardiovascular/ or exp Ocular Hypertension/ 17 (pregnancy-induced or ocular hypertens$ or preeclampsia or pre-
eclampsia).ti. 18 animals/ not (humans/ and animals/) 19 15 not (16 or 17 or 18)

Page 49 of 63
Appendix 7: Telmisartan + Amlodipine PRISMA flow chart

Page 50 of 63
Appendix 8: Summary of characteristics of included trials for assessing telmisartan + amlodipine
Author Design Eligibility N Male,
%
Mean age, years
SBP, mmHg
*
DBP, mmHg
*
Interventions, dose in mg/day
Treatment duration,
weeks
Littlejohn 2009
DB, DD, PC, PG, factorial
Stage 1 or 2 HTN (DBP: ≥95 and ≤ 119) 1461 52 53 155 104
Placebo vs T20 to T80 vs A2.5 to 10 vs T20-80/A2.5 to A10
8
Neldam 2011
TEAMSTA-5
DB, PG, MC
HTN (DBP: ≥95 on AHT; ≥ 100 treatment naïve)* 1098 62 54 148 97 T40/A5 vs T80/A5 8
Jagodzinski 2017 DB,SC
Treated controlled or uncontrolled HTN and treatment naïve with 3 ≥ CV risk factors (such as metabolic syndrome and/or DM, and/or end-organ damage)
577 69 61 135 85 T80/A5 vs O40/H12.5 26
Zhu 2014 DB, DD, MC
HTN (DBP: ≥95 on AHT; ≥ 100 treatment naïve)*
324 53 52 155 103 T80/A5 vs A5 8
Sharma 2012
DB, PG, MC
T2DM and stage 1 or 2 HTN (SBP: > 150)*
706 52 61 161 91 T80/A10 vs A10 8
Sharma 2007 DB, MC
Stage II HTN (SBP: 160 – 179; DBP: 100 - 109) 210 68 51 174 100 T40/A5 vs A5 12
Neutel 2012
DB, PG, MC
SBP ≥180 and DBP ≥95 1315 52 58 185 103 T80/A10 vs T80 vs A10
8
Neldam 2011
TEAMSTA-10
DB, PG, MC
HTN, uncontrolled after 6 weeks run-in treatment with A10 (DBP: ≥95 on AHT; ≥ 100 treatment naïve)*
949 56 56 148 96 T40/A10 vs T80/A10 vs A10 8

Page 51 of 63
* = Blood pressure measured at seated position, A = Amlodipine, AHT = anti-hypertensives, BP = Blood pressure, DB = Double blind, DBP = Diastolic blood pressure, DD = Double dummy, H = Hydrochlorthiazide, HTN = Hypertension, MC = Multi centre, N = Sample Size, O = Olmesartan, PG = Parallel group, SBP = Systolic blood pressure, SC = Single centre, T = Telmisartan; all BP values in mmHg

Page 52 of 63
Appendix 9: Telmisartan + Hydrochlorothiazide search strategy, PRISMA and summary of characteristics of included trials Literature databases searched: MEDLINE, Embase, and Cochrane CENTRAL Search Date: April 5th, 2018 Search strategy:
1 Telmisartan.tw. 2 Telmisartan.mp. 3 1 or 2 4 hydrochlorothiazide/ 5 hydrochlorothiazide.mp. 6 4 or 5 7 randomized controlled trial.pt. 8 controlled clinical trial.pt. 9 randomized.ab. 10 placebo.ab. 11 clinical trials as topic/ 12 randomly.ab. 13 trial.ti. 14 or/7-13 15 3 and 6 and 14 16 Pregnancy/ or Hypertension, Pregnancy-Induced/ or Pregnancy
Complications, Cardiovascular/ or exp Ocular Hypertension/ 17 (pregnancy-induced or ocular hypertens$ or preeclampsia or pre-
eclampsia).ti. 18 animals/ not (humans/ and animals/) 19 15 not (16 or 17 or 18)

Page 53 of 63
Appendix 10: Telmisartan + HCTZ PRISMA flow chart

Page 54 of 63
Appendix 11: Summary of characteristics of included trials for assessing telmisartan + HCTZ
Author Design Eligibility N
Position of BP measure
Males, %
Mean age, years
SBP, mmHg
DBP, mmHg
Interventions, dose in mg/day
Treatment duration, weeks
Lacourciere 2001
DD, PG, MC
DBP >90 after 8 weeks of telmisartan 491
Seated, standing 63 55 149 97
T80/H12.5 vs T80 8
Lacourciere 2002 DB, PG
DBP >90 after 4 weeks of 40 mg telmisartan 327 Seated 54 58 147 96
T40/H12.5 vs T40 8
Neldam 2008 DB, DD
DBP: ≥95 on 1 current AHT or DBP ≥90 on 2 or 3 current AHT 713
Seated, standing 57 57 148 95
T80/H12.5 vs T80/H25 8
McGill 2001
DB, PC, PG, MC
suDBP: 95 to 114 at 2 weeks of the 4-week, single-blind, placebo run-in period 818
Supine, standing 60 53 154 101
T20-160 vs H6.25-25 vs T20-160/H6.25-25 vs Placebo 8
McGill b 2001
DB, DD, PC, PG
Black, suDBP: 95 to 114, suSBP: 140 to 200 222 Supine 51 48 155 104
T20-160 vs H6.25-25 vs T20-160/H6.25-25 vs Placebo 8
Derosa 2015 DB, MC
SBP≥140 ≤180 DBP≥90); controlled T2DM (HbA1c ≤7.5%) 148 Seated 50 60 152 97
B10/L100 vs T80/H12.5 26
Zhu 2012 DB, AC, PG, MC SBP≥160, DBP≥100 894
seated, trough 54 57 172.3 104.3
T80/H25 vs T80 7

Page 55 of 63
White 2006
DB, PC, PG, MC DBP≥95 after 4 w placebo
1109
seated, trough 58 53.5 155 102
T80/H25 vs V160/H25 8
White 2008
DB, PC, PG, MC
DBP 95-119 after 2-3 week placebo
1185
seated, trough 55 53 155 102
T80/H25 vs V160/H25 8
AHT = Antihypertensive therapy, B = Barnidipine, BP = Blood pressure, DB = Double blind, DBP = Diastolic blood pressure, DD = Double dummy, HbA1c = Glycated haemoglobin, H = Hydrochlorthiazide, L = Lisinopril, MC = Multi centre, N = Sample Size, O = Olmesartan, PG = Parallel group, SBP = Systolic blood pressure, su = supine, T = Telmisartan, T2DM = Type 2 diabetes mellitus, V = Valsartan
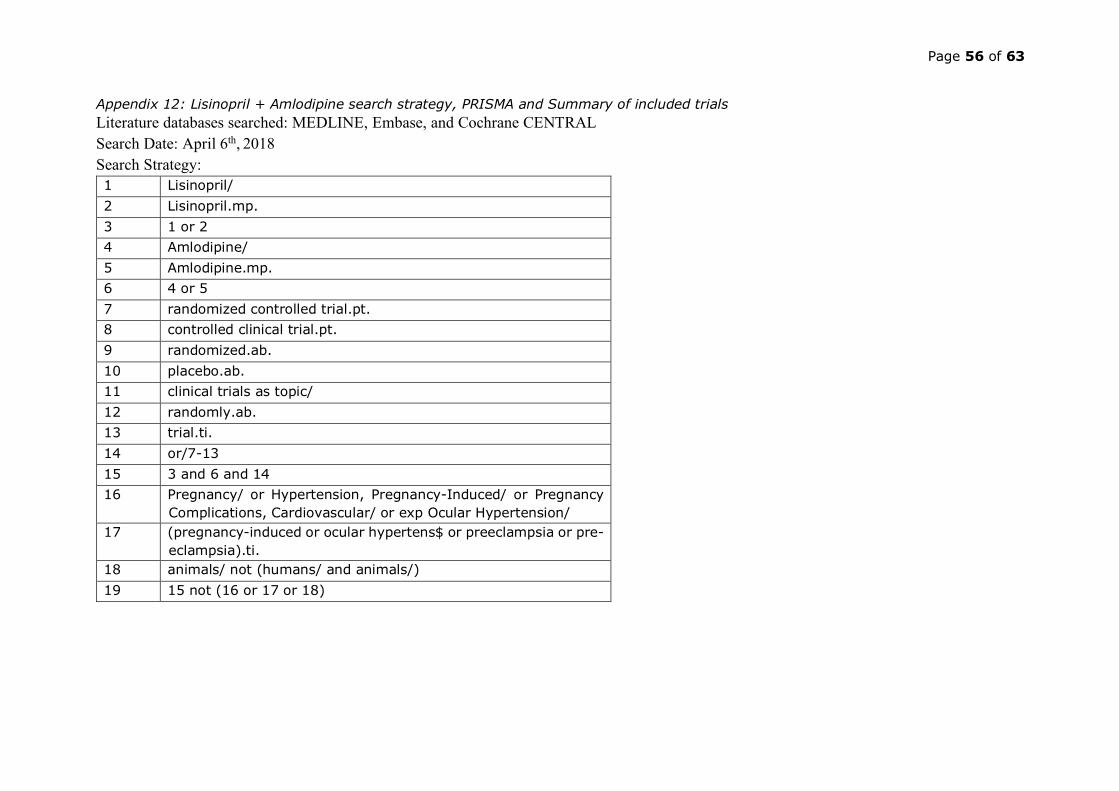
Page 56 of 63
Appendix 12: Lisinopril + Amlodipine search strategy, PRISMA and Summary of included trials Literature databases searched: MEDLINE, Embase, and Cochrane CENTRAL Search Date: April 6th, 2018 Search Strategy: 1 Lisinopril/ 2 Lisinopril.mp. 3 1 or 2 4 Amlodipine/ 5 Amlodipine.mp. 6 4 or 5 7 randomized controlled trial.pt. 8 controlled clinical trial.pt. 9 randomized.ab. 10 placebo.ab. 11 clinical trials as topic/ 12 randomly.ab. 13 trial.ti. 14 or/7-13 15 3 and 6 and 14 16 Pregnancy/ or Hypertension, Pregnancy-Induced/ or Pregnancy
Complications, Cardiovascular/ or exp Ocular Hypertension/ 17 (pregnancy-induced or ocular hypertens$ or preeclampsia or pre-
eclampsia).ti. 18 animals/ not (humans/ and animals/) 19 15 not (16 or 17 or 18)

Page 57 of 63
Appendix 13: Lisinopril + amlodipine PRISMA flow chart
Page 58 of 63
Appendix 14: Manufacturers of proposed combinations in EU, USA and India

Page 59 of 63
Combinations India USA EU lisinopril/HCTZ Registered (Aug 7, 2016)
*ramipril registered Apotex Aurobindo Hikma Invagen Ivax Lupin Mylan Prinston Sandoz Sun Watson labs
Teva Gedeon Richter Jenson Pharmaceutical Services Limited Heumann Pharma GmbH & Co Generica KG Hexal DOC Generici
telmisartan/amlodipine Registered (Jul 7, 2015) Alembic Lupin Mylan Torrent Boehringer ingelheim
Zentiva KRKA BOEHRINGER INGELHEIM

Page 60 of 63
telmisartan/HCTZ Registered (July 16, 2015) Boehringer ingelheim Alembic Aurobindo Lupin Macleods Mylan Prinston Torrent Zydus
DOC Generici Gedeon Richter EGIS Pharmaceuticals Teva Adamed Billev Pharma Sandoz HEXAL Zentiva Laboratorios LICONSA Chemo Ibérica axunio Pharma Apotex Europe Alvogen Ferrer Internacional, S.A. Stada Arzneimittel AG Sigillata Ltd. Mylan S.p.A. Glenmark Generics (Europe) Limited PharmaSwiss Medana Pharma Accord Healthcare Micro Labs GmbH
lisinopril/amlodipine Registered (July 7, 2015) Gedeon Richter

Page 61 of 63
Appendix 15: Summary of characteristics of included trials for assessing lisinopril + amlodipine
Author Design Eligibility N Male,
%
Mean age, years
SBP, mmHg
DBP, mmHg
Interventions, dose in mg/day
Treatment duration,
weeks Cappuccio
1993 DB, CO
Supine DBP ≥95 after 4 weeks on placebo
15 53 53 165 99 L10+A5 vs A5 vs L10
4
A=Amlodipine, CO=Crossover, DB = Double blind, DBP = Diastolic blood pressure, L=Losartan

Page 62 of 63
Appendix 16: Standard doses of component drugs of the proposed combinations Medication WHO BNF Martindale MIMS online DECISION ON
STANDARD DOSE
Amlodipine 5 5 -10 5-10 2.5-10 5 Hydrochlorothiazide 25 - 25-50 - 25 Lisinopril 10 20 20 10-20 20 Telmisartan 40 40 20-80 40 40

Page 63 of 63





























