Embed Size (px)
Citation preview

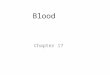
Whole Blood Processed within
8 hours )
Packed red blood cellsFresh frozen plasma Platelets

Component preparationComponent preparation Principle - Differential Principle - Differential
centrifugationcentrifugation Red cellsRed cells
Packed cellsPacked cells Red cells + additiveRed cells + additive
PlasmaPlasma Bank plasmaBank plasma Fresh frozenFresh frozen Cryo supernateCryo supernate
PlateletsPlatelets Platelet rich Platelet rich
concentrateconcentrate Platelet rich plasmaPlatelet rich plasma
CryoprecipitateCryoprecipitate
Plasma + Platelets
BuffyRBC
Whole blood

DEFINITIONSDEFINITIONS
BLOOD PRODUCTBLOOD PRODUCT = Any therapeutic substance = Any therapeutic substance prepared from human bloodprepared from human blood
WHOLE BLOODWHOLE BLOOD = Unseparated blood collected = Unseparated blood collected into an approved container containing an into an approved container containing an anticoagulant preservative solutionanticoagulant preservative solution
BLOOD COMPONENTBLOOD COMPONENT = 1. A constituent of blood = 1. A constituent of blood , separated from whole blood such as, separated from whole blood such as
• Red cell concentrateRed cell concentrate• PlasmaPlasma• Platelet concentratesPlatelet concentrates2. Plasma or platelets collected by apheresis2. Plasma or platelets collected by apheresis3. Cryoprecipitate prepared from fresh frozen 3. Cryoprecipitate prepared from fresh frozen
plasma plasma

Blood ComponentsBlood Components
THE THE PRBCPRBC StorageStorage - 2 – 6 - 2 – 6 OO C C Unit of issueUnit of issue - 1 donation ( unit or pack )- 1 donation ( unit or pack ) AdministrationAdministration - ABO & Rh compatible- ABO & Rh compatible - Never add medication to a unit- Never add medication to a unit - Complete transfusion within 4 hrs of - Complete transfusion within 4 hrs of
commencementcommencement
1Member

Dosage & Administration
Dosage - 1 unit/10 kg body wtAdult dose is 4-8 units
Administration - Preferably ABO & Rh group specific but not essentialOther groups can be used

PLATELETSPLATELETS
Platelet units can be eitherPlatelet units can be either Random donor unitsRandom donor units Apheresis unitsApheresis units
1 random donor unit contains 55 1 random donor unit contains 55 x10x109 platelets9 platelets
1 apheresis unit contains 240x101 apheresis unit contains 240x1099

Guidelines for Platelet Tx.
Mild - 50,000-1,00,000/µlTx - usually not required
Moderate - 20,000-50,000/µlTx-if symptomatic or has to undergo surgery/trauma
Severe - < 20,000/µlRisk of bleeding - highProphylactic Tx

Indications for platelet Indications for platelet transfusiontransfusion
BLEEDINGBLEEDING due to due to thrombocytopaeniathrombocytopaenia
Due to platelet dysfunctionDue to platelet dysfunction
Prevention of spontaneous bleeding Prevention of spontaneous bleeding with counts < 20,000with counts < 20,000

IMPORTANT IMPORTANT PRECAUTIONSPRECAUTIONS
Stored at 20-24 Degree celcius.Stored at 20-24 Degree celcius. Constantly agitatedConstantly agitated Only last for 5 daysOnly last for 5 days Infused in 30 minsInfused in 30 mins

Fresh Frozen plasmaFresh Frozen plasma
Fresh frozen plasmaFresh frozen plasma – labile & – labile & nonlabile clotting factors, nonlabile clotting factors, albumin and immunoglobulin. albumin and immunoglobulin. Factor VIII ( 8 ) level at least 70 Factor VIII ( 8 ) level at least 70 % of normal fresh plasma level% of normal fresh plasma level
StorageStorage - 20 C for 1 yr, - 65 C for 7 yrs.- 20 C for 1 yr, - 65 C for 7 yrs.- Before use thawed at 37 Before use thawed at 37 oo C C

Fresh frozen plasmaFresh frozen plasma
IndicationsIndications
- Replacement of multiple coagulation - Replacement of multiple coagulation factor deficiencies egfactor deficiencies eg
• Liver diseaseLiver disease• Anticoagulant overdoseAnticoagulant overdose• Depletion of coagulation factors in pts Depletion of coagulation factors in pts
receiving large volume transfusionsreceiving large volume transfusions- DIC (disseminated intravascular DIC (disseminated intravascular
coagulation)coagulation)

FRESHFRESH FROZEN PLASMAFROZEN PLASMA
IndicationIndication Clinically significant deficiency of Clinically significant deficiency of
Factors II, V, X, XI Factors II, V, X, XI Replacement of multiple coagulationReplacement of multiple coagulation
factor deficiencies :-factor deficiencies :- liver disease , warfarin treatment, liver disease , warfarin treatment, dilutional and consumption coagulopathydilutional and consumption coagulopathy
ContraindicationContraindication Volume expansionVolume expansion Immunoglobulin replacementImmunoglobulin replacement
Nutritional Nutritional supportsupport Wound healingWound healing
12

FRESH FROZEN PLASMAFRESH FROZEN PLASMAPrecautionPrecaution
Acute allergic reaction are common Acute allergic reaction are common Anaphylactic reaction may occurAnaphylactic reaction may occur Hypovolemia alone is not an indication forHypovolemia alone is not an indication for
useuse
Dosage - Initial dose of 15 - 20 ml / kgDosage - Initial dose of 15 - 20 ml / kgAdministrationAdministration
Must be ABO compatible, Rh not Must be ABO compatible, Rh not requiredrequired Infuse as soon as possible after thawing Infuse as soon as possible after thawing
( within 6 hrs )( within 6 hrs ) using standard blood administration setusing standard blood administration set
30/11/49 MD-3-4913

FFPFFP
Fresh Frozen PlasmaFresh Frozen Plasma
Plasma collected from single donor Plasma collected from single donor units or by apheresis units or by apheresis
Frozen within 8 hours of collectionFrozen within 8 hours of collection
-40-40o o CC
Can last for a yearCan last for a year

Dosage & Administration for FFP
Dosage - 10-15 ml/Kg(Approx 2-3 bags for an adult)
Administration - Thawed at +37o C before transfusionABO compatibleGroup AB plasma can be used for all patient

Do`s and Dont`sDo`s and Dont`sIn Blood and In Blood and
Blood Blood ComponentsComponents

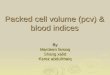
Risk Benefit Analysis
benefit > risk
risk > benefit
Hb gm/dl 4 5 6 7 8 9 10 11 12 13 14
why nottransfuse
why transfuse
individual patient factorsdecide transfusion trigger

18
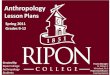
Blood/ Start infusion Complete infusionblood product
Whole blood/ within 30 min. of within 4 hourred cells removing pack (less in high from ambient temperature)
refrigerator
Platelet immediately within 20 minconcentrates
FFP within 30 min within 20 min
Time Limits for InfusionTime Limits for Infusion

TRANSFUSION TRANSFUSION REACTIONSREACTIONS
@RBC’s !@RBC’s ! Nonhemolytic Nonhemolytic 1-5 % transfusions 1-5 % transfusions Causes -Causes -Physical or chemical destruction ofPhysical or chemical destruction of
blood: freezing, blood: freezing, heating, hemolytic drug heating, hemolytic drug -solution added to blood-solution added to blood -Bacterial contamination-Bacterial contamination
: fever, chills, urticaria: fever, chills, urticaria Slow transfusion, diphenhydramine , antipyretic for feverSlow transfusion, diphenhydramine , antipyretic for fever
HemolyticHemolytic ImmediateImmediate: ABO incompatibility : ABO incompatibility (1/ 12-33,000) with (1/ 12-33,000) with
fatality (1/ 500-800,000)fatality (1/ 500-800,000)
Majority are group O patients receiving type A, B Majority are group O patients receiving type A, B or AB blood or AB blood
Complement activation, RBC lysis, free Hb (+ direct Complement activation, RBC lysis, free Hb (+ direct Coombs Ab test)Coombs Ab test)

Signs and Symptoms of Signs and Symptoms of AHTRAHTR
Chills , feverChills , fever Facial flushingFacial flushing HypotensionHypotension Renal failureRenal failure DICDIC Chest painChest pain DyspneaDyspnea Generalized Generalized
bleedingbleeding
HemoglobinemiaHemoglobinemia HemoglobinuriaHemoglobinuria ShockShock NauseaNausea VomittingVomitting Back painBack pain Pain along infusion Pain along infusion
veinvein

Anesthesia: hypotension, urticaria, Anesthesia: hypotension, urticaria, abnormal bleedingabnormal bleeding
Stop infusion, blood and urine to blood Stop infusion, blood and urine to blood bank, coagulation screen (urine/plasma Hb, bank, coagulation screen (urine/plasma Hb, haptoglobin)haptoglobin)
Fluid therapy and osmotic diuresisFluid therapy and osmotic diuresis Alkalinization of urine (increase solubility Alkalinization of urine (increase solubility
of Hb degradation products)of Hb degradation products) Correct bleeding, Rx. DIC Correct bleeding, Rx. DIC

@WBC’s!@WBC’s! Europe: All products leukodepletedEurope: All products leukodepleted USA: Initial FDA recommendation now reversed pending USA: Initial FDA recommendation now reversed pending
objective data (NOT objective data (NOT length of stay for length of stay for expense) expense)
Febrile reactionsFebrile reactions Recipient Ab reacts with donor Ag, Recipient Ab reacts with donor Ag,
stimulates pyrogens (1-2 % stimulates pyrogens (1-2 % transfusions) transfusions)
20 - 30% of platelet transfusions20 - 30% of platelet transfusions Slow transfusion, antipyretic, Slow transfusion, antipyretic,
meperidine for shiveringmeperidine for shivering

TRALI (TRALI (Transfusion related acute lung injury)Transfusion related acute lung injury) Donor Ab reacts with recipient Ag Donor Ab reacts with recipient Ag (1/ (1/
10,000)10,000) noncardiogenic pulmonary edemanoncardiogenic pulmonary edema Supportive therapySupportive therapy

Transfusion-related Acute Lung Transfusion-related Acute Lung Injury Injury (TRALI)(TRALI)
Acute and severe type of transfusion reactionAcute and severe type of transfusion reaction
Symptoms and signsSymptoms and signs FeverFever HypotensionHypotension TachypneaTachypnea DyspneaDyspnea Diffuse pulmonary infiltration on X-raysDiffuse pulmonary infiltration on X-rays Clinical of noncardiogenic pumonary Clinical of noncardiogenic pumonary
edemaedema

Transfusion-related Acute Transfusion-related Acute Lung InjuryLung Injury (TRALI)(TRALI)
Therapy and PreventionTherapy and Prevention Adequate respiratory and hemodynamic Adequate respiratory and hemodynamic
supportive treatmentsupportive treatment If TRALI is caused by pt. Ab If TRALI is caused by pt. Ab use LPB use LPB If TRALI is caused by donor Ab If TRALI is caused by donor Ab no no
special blood componentsspecial blood components

Transfusion-associated Graft-versus-Transfusion-associated Graft-versus-HostHost Disease ( TA-GVHD)Disease ( TA-GVHD)
Rare: immunocompromised patients Rare: immunocompromised patients Suggestion that more common with Suggestion that more common with
designated donorsdesignated donors BMT, LBW neonates, Hodgkin's disease, BMT, LBW neonates, Hodgkin's disease,
exchange Tx in neonatesexchange Tx in neonates

Graft-versus-Host ReactionGraft-versus-Host Reaction
Signs & SymptomsSigns & Symptoms
Onset ~ 3 to 30 days after transfusion Clinical significant – pancytopenia Other effects include fever, liver enzyme, copious watery diarrhea, erythematous skin erythroderma and desquamation

@Platelets!@Platelets!
AlloimmunizationAlloimmunization 50 % of repeated platelet transfusions50 % of repeated platelet transfusions Ab-dependent elimination of platelets with lack of Ab-dependent elimination of platelets with lack of
responseresponse Use single donor apheresis Use single donor apheresis Signs & SymptomsSigns & Symptoms
mild mild slight fever and Hb slight fever and Hb severe severe platelet refractoriness with bleeding platelet refractoriness with bleeding
Post-transfusion purpuraPost-transfusion purpura Recipient Ab leads to sudden destruction of Recipient Ab leads to sudden destruction of
platelets 1-2 weeks after transfusion (sudden platelets 1-2 weeks after transfusion (sudden onset)onset)
Rare complicationRare complication

INFECTIOUS INFECTIOUS COMPLICATIONSCOMPLICATIONS
I. I. Viral Viral (Hepatitis 88% of per unit viral (Hepatitis 88% of per unit viral risk)risk)
Hepatitis B Hepatitis B Risk 1/ 200,000 due to HBsAg, antiHBc Risk 1/ 200,000 due to HBsAg, antiHBc
screening (7-17 % of PTH) screening (7-17 % of PTH) Per unit risk 1/63-66,000Per unit risk 1/63-66,000 0.002% residual HBV remains in ‘negative’ 0.002% residual HBV remains in ‘negative’
donors (window 2-16 weeks)donors (window 2-16 weeks) Anti-HBc testing retained as surrogate marker Anti-HBc testing retained as surrogate marker
for HIV for HIV

NANB and Hepatitis CNANB and Hepatitis C
Risk now 1/ 103,000 (NEJM 96) with Risk now 1/ 103,000 (NEJM 96) with 2nd/ 1/ 125,000 with 3rd generation 2nd/ 1/ 125,000 with 3rd generation HCV Ab/ HVC RNA tests HCV Ab/ HVC RNA tests
Window 4 weeksWindow 4 weeks 70 % patients become chronic carriers, 70 % patients become chronic carriers,
10-20 % develop cirrhosis10-20 % develop cirrhosis

HIVHIV
Current risk 1/ 450- 660,000 (95) Current risk 1/ 450- 660,000 (95) With current screening (Abs to With current screening (Abs to
HIV I, II and p24 Ag), window 6-HIV I, II and p24 Ag), window 6-8 weeks (third generation ELISA 8 weeks (third generation ELISA tests in Europe)tests in Europe)
sero -ve window to < 16 dayssero -ve window to < 16 days

HTLV I, IIHTLV I, II
Only in cellular components (not FFP, Only in cellular components (not FFP, cryo)cryo)
Risk 1/ 641,000 (window period unknown)Risk 1/ 641,000 (window period unknown) Screening for antibody I may not pick up Screening for antibody I may not pick up
II II
CJD (and variant CJD)CJD (and variant CJD)

II. BacterialII. Bacterial Contamination unlikely in products stored for Contamination unlikely in products stored for
> 72 hours at 1-6 > 72 hours at 1-6 0 0 C C gram –ve, gram +ve bacteriagram –ve, gram +ve bacteria most frequentmost frequent – – Yersinia enterocolitica Yersinia enterocolitica
Produced Produced endotoxinendotoxin Platelets stored at room temperature for 5 Platelets stored at room temperature for 5
days, with infection rate of 0.25% days, with infection rate of 0.25%
III. ProtozoalIII. Protozoal Trypanosoma cruzi (Chaga’s disease) Trypanosoma cruzi (Chaga’s disease) MalariaMalaria ToxoplasmosisToxoplasmosis LeishmaniasisLeishmaniasis

Serological TestingSerological Testingfor Infectious markersfor Infectious markers
HIV – AgHIV – Ag Anti – HIVAnti – HIV HBsAgHBsAg Anti – HCVAnti – HCV Test for syphilisTest for syphilis

METABOLIC METABOLIC COMPLICATIONSCOMPLICATIONS
Citrate toxicityCitrate toxicity Citrate (3G/ unit WB) binds CaCitrate (3G/ unit WB) binds Ca2+ 2+ // MgMg++
Metabolized liver, mobilization bone storesMetabolized liver, mobilization bone stores Hypocalcemia ONLY if > 1 unit/ 5 min or Hypocalcemia ONLY if > 1 unit/ 5 min or
hepatic dysfunctionhepatic dysfunction Hypotension more likely due to Hypotension more likely due to cardiac cardiac
output/ perfusion than output/ perfusion than calcium (except calcium (except neonates) neonates)
Worse with hypothermia/ hepatic Worse with hypothermia/ hepatic dysfunctiondysfunction