Embed Size (px)
Citation preview

(—THIS SIDEBAR DOES NOT PRINT—)
DESIGN GUIDE
This PowerPoint 2007 template produces a 48”x72”
presentation poster. You can use it to create your research
poster and save valuable time placing titles, subtitles, text,
and graphics.
We provide a series of online answer your poster production
questions. To view our template tutorials, go online to
PosterPresentations.com and click on HELP DESK.
When you are ready to print your poster, go online to
PosterPresentations.com
Need assistance? Call us at 1.510.649.3001
QUICK START
Zoom in and out As you work on your poster zoom in and out to the level that is
more comfortable to you. Go to VIEW > ZOOM.
Title, Authors, and Affiliations Start designing your poster by adding the title, the names of the
authors, and the affiliated institutions. You can type or paste text
into the provided boxes. The template will automatically adjust the
size of your text to fit the title box. You can manually override this
feature and change the size of your text.
TIP: The font size of your title should be bigger than your name(s)
and institution name(s).
Adding Logos / Seals Most often, logos are added on each side of the title. You can insert
a logo by dragging and dropping it from your desktop, copy and
paste or by going to INSERT > PICTURES. Logos taken from web sites
are likely to be low quality when printed. Zoom it at 100% to see
what the logo will look like on the final poster and make any
necessary adjustments.
TIP: See if your company’s logo is available on our free poster
templates page.
Photographs / Graphics You can add images by dragging and dropping from your desktop,
copy and paste, or by going to INSERT > PICTURES. Resize images
proportionally by holding down the SHIFT key and dragging one of
the corner handles. For a professional-looking poster, do not distort
your images by enlarging them disproportionally.
Image Quality Check Zoom in and look at your images at 100% magnification. If they look
good they will print well.
ORIGINAL DISTORTED
Corner handles
Go
od
pri
nti
ng
qu
alit
y
Bad
pri
nti
ng
qu
alit
y
QUICK START (cont.)
How to change the template color theme You can easily change the color theme of your poster by going
to the DESIGN menu, click on COLORS, and choose the color
theme of your choice. You can also create your own color
theme.
You can also manually change the color of your background by
going to VIEW > SLIDE MASTER. After you finish working on
the master be sure to go to VIEW > NORMAL to continue
working on your poster.
How to add Text The template comes with a number of pre-formatted
placeholders for headers and text blocks. You can add more
blocks by copying and pasting the existing ones or by adding a
text box from the HOME menu.
Text size Adjust the size of your text based on how much content you
have to present. The default template text offers a good
starting point. Follow the conference requirements.
How to add Tables To add a table from scratch go to the INSERT menu
and click on TABLE. A drop-down box will help you
select rows and columns.
You can also copy and a paste a table from Word or another
PowerPoint document. A pasted table may need to be re-
formatted by RIGHT-CLICK > FORMAT SHAPE, TEXT BOX,
Margins.
Graphs / Charts You can simply copy and paste charts and graphs from Excel
or Word. Some reformatting may be required depending on
how the original document has been created.
How to change the column configuration RIGHT-CLICK on the poster background and select LAYOUT to
see the column options available for this template. The
poster columns can also be customized on the Master. VIEW >
MASTER.
How to remove the info bars If you are working in PowerPoint for Windows and have
finished your poster, save as PDF and the bars will not be
included. You can also delete them by going to VIEW >
MASTER. On the Mac adjust the Page-Setup to match the
Page-Setup in PowerPoint before you create a PDF. You can
also delete them from the Slide Master.
Save your work Save your template as a PowerPoint document. For printing,
save as PowerPoint or “Print-quality” PDF.
Student discounts are available on our Facebook page.
Go to PosterPresentations.com and click on the FB icon.
© 2015 PosterPresentations.com 2117 Fourth Street , Unit C Berkeley CA 94710 [email protected]
RESEARCH POSTER PRESENTATION DESIGN © 2015
www.PosterPresentations.com
Merosin-deficient congenital muscular dystrophy (CMD) belongs to a diverse
group of rare hereditary muscle diseases distinguished by specific phenotypes.
They are characterized by progressive joint contractures of all extremities and
spine. Subcategories of CMD besides other genetic muscle diseases should be
considered in the differential their diagnosis. MRI plays an expanding role in
diagnosis and disease tracking of various genetic muscle diseases. The goal is
to analyze the pattern of muscle involvement in a series of children with
clinically and genetically-determined merosin-deficient CMD employing
whole-body MRI. The specific objective is to establish contextual connections
with the children's clinical neuro-orthopedic and molecular profiles.
OBJECTIVES RESULTS Continued
Nagia Fahmy, MD1 Tamer A. EL-Sobky, MD2 Nermine S. Elsayed, MD3 Hossam M. Sakr, MD4 Amr M. Saadawy, MD4
1 Department of Neurology, 2 Department of Orthopedics, 3 Department of Genetics, 4 Department of Radiology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Whole-body Muscle Magnetic Resonance Imaging Characteristics of Children with Merosin-deficient Congenital Muscular Dystrophy
MATERIALS & METHODS
In this cross-sectional study nine children with merosin-deficient CMD (age
range 3y-14y, 2 boys, 7 girls) received a detailed neuro-orthopedic
examination, brain MRI, muscle biopsy with immunostaining, and serum
CPK to confirm the diagnosis. Children received a molecular study which
identified two homozygous pathogenic mutations in the LAMA2 gene in all
but one child with a compound heterozygous mutation. Children received
whole-body muscle MRI (including axial T1WI, T2WI & STIR) to detail the
pattern of muscle involvement in all extremities and trunk. We categorized
muscle fatty infiltration and atrophy. We used an age and sex-matched
control group of other hereditary muscle diseases.
RESULTS
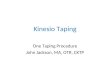
Figure 1: Orthopedic manifestations of index cases. Note the
characteristic fixed flexion deformity of elbows (A), massive
dorsolumbar scoliosis (B), excessive internal femoral torsion,
flexion deformity of hips, and compensatory lumbar lordosis
(C,D,E) respectively. Mark the hip dysplasia and dislocation
(F). Intraoperative images show a massive fatty infiltration of
the vastus lateralis (G). Note the retracted ends of the iliotibial
band (horizontal arrows) & retracted ends of vastus lateralis
sheath (vertical arrows), whole body MRI images of two
patients showing severe (H) & milder (I) deformities.
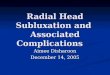
Figure 2: Axial FLAIR (A,C)
and T2WI (B,D) of two different
merosine deficiency patients
showing white matter
demyelination changes.
RESULTS Continued
Clinical Neuro-orthopedic Evaluation
Patient No
(Age /Sex)
Ambulatory
status
Symmetric
pattern Upper limb contractures Lower limb contractures Spine contractures
Immuno-
histochemistry
1.
(9Y/F)
(-) (+) all
limbs
Flexion of elbows 50°, shoulder
and wrists spared
Hip & knee flexion of 95° & 70° respectively, internal femoral torsion with posterior hip subluxation. Semi-rigid
dorsolumbar
lordoscoliosis
Partial merosin
deficiency
2.
(5.5Y/M)
(-)
(+) all
limbs
Elbow flexion 20°, shoulder and
wrists spared
Dislocatable hips with audible click & flexion of 35°, & mild adduction. Right and left knee flexion of 15° &
5° respectively & gastrocnemius-soleus induced ankle equinus.
Supple lumbar
lordosis
Merosin deficiency
3.
(9Y/F)
(-) (-) overall
asymmetric
(Left>
right)
Right and left elbow flexion 5° &
45° respectively.
Right and left knee flexion of 15° & 45° respectively, gastrocnemius-soleus induced ankle equinus with supple
varus feet.
Rigid moderate
dorsolumbar scoliosis
Merosin deficiency
4.1
(14Y/F)
(-) (+)
especially
in upper
limbs
Elbow flexion 80°, shoulder
spared, & moderate flexion of
wrist and digits.
Marked pelvic obliquity. Otherwise no contractures but flaccidity and wasting. Rigid massive
dorsolumbar scoliosis
-
4.2
(12Y/F)
sister
(-) (+)
especially
in upper
limbs
Elbow flexion 70°, shoulder
spared, ulnar deviation of wrist
& digital flexion .
Dislocatable left hip with audible click, femoral shortening & bilateral internal femoral torsion. Flexion of
knees 10°, asymmetric gastrocnemius-soleus induced ankle equinus (right> left) & supple varus of right foot.
None Merosin deficiency
5.
(11yYF)
(-) (+) In all
limbs
Elbow flexion contracture of
moderate degree.
Internal femoral torsion and external tibial torsion Supple lumbar
lordosis
Merosin deficiency
6.1
(9Y/F)
(-) (+) In all
limbs
Elbow flexion 60°, internal
rotation of left shoulder,
extension of wrists with digital
flexion including thumbs
Dislocated right, subluxed left hip with audible click, internal femoral torsion & hypermobile hip rotation.
Hip & knee flexion of 35° & 5° respectively & supple varus feet.
Semi-rigid
dorsolumbar
lordoscoliosis.
Merosin deficiency
6.2
(3Y/F)
sister
(-) (+) In all
limbs
Elbow flexion 20°, spared
shoulders and wrists.
Hip & knee flexion of 50° & 10° respectively. Dislocated left, subluxed right hip with audible click &
hypermobile hip rotation. Ankle equinus (gastrocnemius induced on right & gastrocnemius-soleus on left)
Supple lumbar
lordosis
-
7.
(10Y/M)
(-)
(+) In all
limbs
Flexion of elbows 10°, mild
flexion contracture of wrists and
digits, spared shoulders
Flexion of both hips 80° & knees 95°, internal femoral torsion with posterior hip subluxation. Hypermobile
hips. Symmetric gastrocnemius-soleus induced ankle equinus with semi-rigid varus feet.
Supple lumbar
lordosis
Merosin deficiency
Muscle MRI Findings
Fig. 3: Axial T1WI in merosin-deficient CMD showing bilateral nearly
symmetrical pattern of fatty degeneration more pronounced in the
subscapularis (A), para spinal (B), gluteus medius & minimus (C), all
components of quadriceps, anterior half of the gracilis (D) & superficial
posterior compartment of calf i.e. gastrocnemius-soleus and peroneal
muscles (E).
Fig. 4: Axial T1WI of the shoulder region in three patients with
merosin-deficient CMD (A,B,C) showing predominant affection of
subscapularis and to a lesser degree infra-spinatous muscles, with
relative sparing of the deltoid muscles. Contrastingly, patients of the
control group (D: Collagen 6 deficiency, E: Titinopathy, F:
Sarcoglyconopathy) exhibit a different pattern.
Fig. 5: Axial T1WI of the upper arm in three patients with
merosin-deficient CMD, (A,B,C) showing predominant
affection of anterior compartment muscles with relative
sparing of the triceps/posterior compartment.
Contrastingly, the control group (D: Collagen 6 deficiency,
E: Titinopathy, F: Sarcoglyconopathy) exhibit a different
pattern.
Fig. 6: Axial T1WI of the forearm in three patients with merosin-
deficient CMD (A,B,C) showing a homogenous pattern of
affection of anterior and posterior compartments forearm
muscles. Contrastingly, the control group (D: Collagen 6
deficiency, E: Titinopathy, F: Sarcoglyconopathy) exhibit a
different pattern.
Fig. 7: Selected Axial T1WI of the paraspinal muscles in
three merosin-deficient CMD patients (A,B,C) show
various grades of fatty degeneration of erector spinae
muscle. Contrastingly, the control group (D: Collagen 6
deficiency, E: Titinopathy, F: Sarcoglyconopathy) exhibit a
different pattern.
Fig. 8: Axial T1WI of the gluteal region in three merosin-
deficient CMD patients (A,B,C) showing severe fatty
infiltration of gluteal muscles. Contrastingly, the control
group (D: Collagen 6 Deficiency, E: Titinopathy, F:
Sarcoglyconopathy) exhibit a different pattern.
Muscle Biopsy
Muscle biopsy of patient 2 with Merosin faint
staining
Muscle biopsy of patient 1 with Merosin
negative staining
DISCUSSION & SIGNIFICANCE
All patients had myopathic faces with bilateral lesions. Patients 1, 3, 4,.5 were
originally ambulatory while the remaining patients were non- ambulatory
from the start. The neuro-orthopedic manifestations are presented (Table 1).
We documented a fairly characteristic neuro-orthopedic pattern of
involvement which correlated with the whole-body muscle MRI pattern in
some anatomic regions. Index patients showed a fairly consistent pattern of
muscle involvement in contrast to the control group e.g. shoulder regions
showed affection of the subscapularis & to a lesser degree infra spinatus
muscles with relative sparing of the deltoid muscle (Fig. 4). The arms showed
a specific predilection to involve the anterior compartment with relative
sparing of the triceps (Figs. 5&6). The trunk showed specific predilection to
involve the para spinal & gluteal musculature especially the gluteus medius &
minimus (Figs. 7&8). A consistent pattern was demonstrated in the rectus
femoris, hamstring & leg muscles(Figs. 9&10). Although some findings were
unique to merosin-deficient CMD, others were sensitive i.e, shared by other
subtypes of CMD such as the geographic pattern of the rectus femoris and
vastus lateralis previously thought to be specific to collagen 6 deficiency.
There is emerging evidence to suggest that whole-body muscle MRI can
become a useful contributor to the differential diagnosis of merosin-
deficient CMD. The presence of a fairly characteristic whole-body muscle
MRI and neuro-orthopedic pattern of involvement was documented. Both
sensitive and specific muscle MRI findings have been documented. The
whole-body muscle MRI findings should be interpreted with reference to the
clinical and molecular context to improve diagnostic accuracy. The strength
of this study is that it demonstrates a diversification of disease severities and
clinical profiles. Larger and longitudinal studies may yet have positive
implications for disease tracking and for phenotype-genotype correlations.
Fig. 11: Axial T1WI of the shoulder (A), forearm (B), paraspinal (C), gluteal (D) & calf regions
(E) (columns) in three different merosine-deficienct CMD patients aged 6,9 & 12 years (1,2,3)
(rows) showing different degrees of affection of the same muscles in different patients with
various ages.
A B C D E
1
2
3
Fig. 9: Axial T1WI of the thigh in three
merosin-deficient CMD patients (A,B,C)
showing predominant hamstrings affection
with relative sparing of gracilis & sartorius.
Contrastingly, patients of the control group
(D: Collagen 6 deficiency, E: Titinopathy, F:
Sarcoglyconopathy) exhibit a different pattern.
The geographic pattern of rectus femoris is
shared by both index and collagen 6 patients.
Fig. 10: Axial T1WI of the calf in three merosin-
deficient CMD patients (A,B,C) showing severe
involvement of gastrocnemius-soleus &
peroneal muscles with relatively spared deep
posterior and extensor compartment of leg.
Contrastingly, the control group (D: Collagen 6
deficiency, E: Titinopathy, F: Sarcoglycanopathy)
exhibit a different pattern.
Corresponding authors: Tamer EL-Sobky [email protected], Hossam Sakr