Embed Size (px)
Citation preview

APLAR Journal of Rheumatology 2004; 7: 83–89
©Asia Pacific League of Associations for Rheumatology
Blackwell Publishing, Ltd.LECTUREPathogenesis of SLE
Who’s afraid of the big bad wolf? Fifth Tay Chong Hai Lecture of the National Arthritis Foundation of SingaporeC. S. LAU
Division of Rheumatology and Clinical Immunology, Department of Medicine, The University of Hong Kong, Hong Kong
It gives me great pleasure to receive the honour as theFifth Tay Chong Hai Lecturer of the National ArthritisFoundation of Singapore. Dr Tay is the founder ofrheumatology in Singapore and has contributed signi-ficantly to the development of this subspecialty inSingapore, as well as Asia. A lot of his work has beenon systemic lupus erythematosus (SLE), a not uncom-mon multisystem autoimmune disease seen in Asia. Topay tribute to Dr Tay and his work, this lecture focuseson lupus research from Hong Kong, which in manyways has been inspired by Dr Tay, Professor P.H. Fengand their many colleagues.
Research in rheumatology, particularly lupus, inHong Kong has evolved slowly in the past two decades.Initial work in the ’70s focused on the development ofautoantibody assays and complement profiles, whileimmunogenetic and clinical studies were set up in themid-’80s. In the last 10 years or so, we have also extendedour scope to study the immunopathogenesis of SLE. Inthis lecture ‘Who’s afraid of the big bad wolf ’, studiesin this area that have been carried out in Hong Kong inthe past few years are reported.
The work reported in this paper is the fruition ofa lot of hard work of a number of people includingDr C.T.K. Ho, Dr M.Y. Mok and Dr Raymond Wong ofour unit, and Dr K.W. Lee and Dr C.C. Mok who usedto work in Queen Mary Hospital but have now movedelsewhere to establish their own units. Dr C.C. Mok,in particular, has contributed a significant amount ofwork in lupus research in Hong Kong. Other colleagueswho have made significant contributions includeMr Albert Chan, Dr David Chan, Dr J. Ou, Dr Y. Ren,
Dr K.K. Tong and Mr Joseph Yeung who used to workor are still working in my laboratory. Thanks are alsodue to Dr Eric Chan of the Department of Pathology,Queen Mary Hospital, and Dr S.Y. Chan, Dr Eddie Ipand Professor Y.L. Lau of the Department of Paediatricsand Adolescent Medicine, The University of Hong Kong.
AN OVERVIEW OF THE IMMUNOPATHOGENESIS OF SLE
Systemic lupus erythematosis is characterized by multi-organ manifestations secondary to a generalized immuneaberration. Pathologically, there is autoantibody (auto-ab) formation and immune complex (IC) deposition.Failure to regulate the production and clearance of auto-ab and IC results in tissue damage.
Any attempts to explain the pathogenesis of SLEmust address the following observations:1 SLE is found in all races, however, some ethnic groups
are more susceptible to develop this condition thanothers, suggesting a genetic basis for this disease. Forexample, SLE is uncommon in Caucasians but relat-ively common among Afro-Americans and Asians.1
Additionally, the presentation and course of SLE arehighly variable between patients of different ethnicorigins. Afro-Americans and Asians are believed tohave a more severe disease than Caucasian whites.Interestingly, however, Afro-Americans rarely developthis condition. This observation indicates changes inthe environment may alter the presentation or mani-festation of SLE.
2 SLE predominantly affects females of reproductiveage. The disease is uncommon among males and theelderly.2,3 Further, activity of the disease may fluctu-ate during certain physiological situations such aspregnancy and lactation where there are changesin sex hormone levels. Additionally, the use of oral
Correspondence: CS Lau, Division of Rheumatology and Clinical Immunology, Department of Medicine, The University of Hong Kong, Hong Kong SAR, China. Email: [email protected]
C. S. Lau
84 APLAR Journal of Rheumatology 2004; 7: 83–89
contraceptive pills has been suggested as being asso-ciated with an increased incidence and exacerbationof SLE.
3 The cause of excessive autoantibody production,the hallmark of SLE, is not clearly known. However,recent studies have suggested this is auto-antigendriven, the source of which includes the tissues thathave been damaged by auto-Ab as well as the resultof abnormal apoptosis. Factors that determine therate of apoptosis and the clearance of apoptotic cellsmay influence the development of SLE.In this lecture, work done from our unit on some
of the genetic determinants, the role of sex hormones,abnormal apoptosis and defective handling of apop-totic cells in the pathogenesis of SLE is presented.
SOME GENETIC DETERMINANTS OF SLE
Evidence that has been accrued so far suggests that SLEis a polygenic disease although in a small percentage
(< 5%) of patients, a single gene may be responsible– individuals who are homozygous for deficiencies ofearly components of the complement pathway. Othercandidate genetic loci that have been associated withSLE include the major histocompatibility complex(MHC) class II alleles, other complement-related pro-teins including mannose binding lectin (MBL), Ro/SSA,CR1, immunoglobulin Gm and Km allotypes, T-cellreceptors, several cytokines, Fcγ receptors, heat shockprotein (HSP)-70, and candidate regions in which theresponsible genes have yet to be mapped.
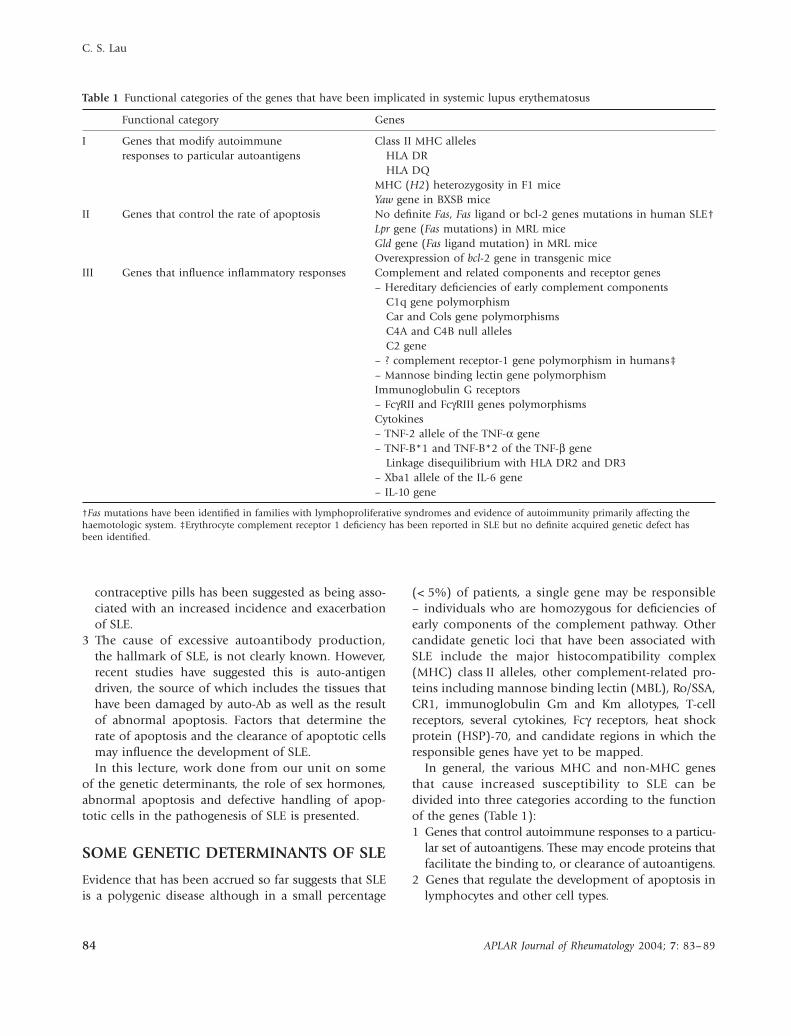
In general, the various MHC and non-MHC genesthat cause increased susceptibility to SLE can bedivided into three categories according to the functionof the genes (Table 1):1 Genes that control autoimmune responses to a particu-
lar set of autoantigens. These may encode proteins thatfacilitate the binding to, or clearance of autoantigens.
2 Genes that regulate the development of apoptosis inlymphocytes and other cell types.
Table 1 Functional categories of the genes that have been implicated in systemic lupus erythematosus
Functional category Genes
I Genes that modify autoimmune responses to particular autoantigens
Class II MHC allelesHLA DRHLA DQ
MHC (H2) heterozygosity in F1 miceYaw gene in BXSB mice
II Genes that control the rate of apoptosis No definite Fas, Fas ligand or bcl-2 genes mutations in human SLE†Lpr gene (Fas mutations) in MRL miceGld gene (Fas ligand mutation) in MRL miceOverexpression of bcl-2 gene in transgenic mice
III Genes that influence inflammatory responses Complement and related components and receptor genes– Hereditary deficiencies of early complement components
C1q gene polymorphismCar and Cols gene polymorphismsC4A and C4B null allelesC2 gene
– ? complement receptor-1 gene polymorphism in humans‡– Mannose binding lectin gene polymorphismImmunoglobulin G receptors– FcγRII and FcγRIII genes polymorphismsCytokines– TNF-2 allele of the TNF-α gene– TNF-B*1 and TNF-B*2 of the TNF-β gene
Linkage disequilibrium with HLA DR2 and DR3– Xba1 allele of the IL-6 gene– IL-10 gene
†Fas mutations have been identified in families with lymphoproliferative syndromes and evidence of autoimmunity primarily affecting the haemotologic system. ‡Erythrocyte complement receptor 1 deficiency has been reported in SLE but no definite acquired genetic defect has been identified.

Pathogenesis of SLE
APLAR Journal of Rheumatology 2004; 7: 83–89 85
3 Genes that influence the handling of immune com-plexes and the expression of inflammatory disease inparticular organs.
MBL gene and SLEMannose binding lectin is a c-type lectin which is syn-thesized by the liver as an acute phase protein. Man-nose binding lectin has been shown to be an importantcomponent of the innate immune system. It recognizesand binds to a wide spectrum of oligosaccharides onthe outer wall of microorganisms, and enables opsoni-zation and facilitates phagocytosis of the pathogen.Mannose binding lectin may also be considered as partof the complement family through its ability to activatethe classical complement pathway through an antibodyand C1q-independent mechanism – the lectin path-way.4 Deficiency in MBL may be secondary to one ofthree point mutations (codon 52, 54 and 57 of exon 1)found in the MBL gene, and/or promoter gene poly-morphisms. Individuals who are deficient in MBL aresusceptible to recurrent infections. Recent studies by usand others have also shown MBL insufficiency is asso-ciated with the development of SLE.5–9
Studies on MBL in SLE were initiated in light of theassociation of complement deficiency and SLE10 andthat MBL is now considered a member of the comple-ment family of proteins. Low serum levels of MBL havebeen found to be associated with SLE. The lower thelevel of MBL, the higher the risk for developing SLE.In our study, an MBL level of < 250 ng/mL gave anodds ratio for that individual to have SLE of 5.32.6
Subsequently, the frequency of the dysfunctional allelecaused by a mutation in codon 54 of the MBL gene wasfound to be significantly increased. Interestingly, how-ever, even taking into account structural mutations ofthe MBL gene, serum levels of MBL were still signi-ficantly lower in patients with SLE when compared withcontrols (Table 2). Serial measurements of MBL levelsin SLE patients without codon 54 mutation, but withlow MBL levels, were persistently low and did not seemto correlate with disease activity.
As serum levels of MBL may also be determined bypromoter polymorphisms of the MBL gene, analysisof the promoter haplotypes H/L and X/Y was laterperformed.11,12 The LX haplotype, which is the lowestMBL producing haplotype was found to be significantlyassociated with SLE. On the other hand, the HY haplo-type, which is the highest MBL producing haplotype,was negatively associated with the disease.
It is probable that MBL insufficiency predisposes tothe development of SLE through defective handling ofimmune complexes. Alternatively, since MBL is knownto interact with viral envelopes containing high man-nose concentrations, such as human immunodeficiencyvirus, it is possible that MBL deficiency predisposes tothe development of SLE by causing defective handlingof a triggering virus or other relevant microbes (reviewedby Lau et al.13).
IL-10 gene polymorphisms and SLEThe cytokine profile of SLE has been extensivelystudied. Over-expression of certain Th2 cytokines thatsuppress the Th1 response in lupus T-cells is a particularlyattractive theory. The recent discovery of a role playedby IL-10 in the pathogenesis of SLE sheds some light onthis issue. IL-10 is a Th2 type of cytokine that acts as apotent stimulator of B-cell proliferation and differenti-ation, and thereby a potential mediator of polyclonalB-cell activation in SLE. Indeed, recent studies haveshown that spontaneous production of IL-10 from SLEperipheral blood B-cells and monocytes is significantlyhigher than that of controls.14 Expression of IL-10 tran-scripts is significantly increased in non-T-cell popula-tion of peripheral blood mononuclear cells (PBMCs)from patients with SLE compared to controls.15 More-over, serum IL-10 levels are higher in lupus patients thancontrols and are correlated with clinical and serologicaldisease activity and anti-DNA titres.16 Further, an increasedratio of IL-10 : IFNγ -secreting cells in PBMCs of SLEpatients correlates with disease activity.17
The IL-10 gene contains two dinucleotide polymor-phisms (IL-10.G and IL-10.R) in its promoter region at
Table 2 MBL levels in patients with SLE
Whole* group Without** codon 54 mutation With*** codon 54 mutation
n Median n Median n Median
SLE patients 111 680 74 1083 37 211controls 123 1644 95 2174 28 370
*P < 0.0001, for median levels in SLE patients vs controls, by Mann–Whitney test. **P < 0.0001, for median levels in SLE patients vs controls. By Mann–Whitney test. ***P = 0.29, for median levels in SLE patients vs controls, by Mann–Whitney test.

C. S. Lau
86 APLAR Journal of Rheumatology 2004; 7: 83–89
about −4 Kb. A significant difference in the distributionof the IL-10.G alleles has previously been reported inCaucasian whites.18 Furthermore, the presence of renalinvolvement and autoantibody expression was asso-ciated with certain IL-10.G microsatellite alleles. We havealso recently studied the relationship between IL-10promoter polymorphisms and SLE susceptibility in acohort of Chinese patients with SLE.19
In our study, we investigated the three known biallelicIL-10 gene promoter polymorphisms – at positions–1087, –824, and –597 from the transcription initi-ation site and their possible clinical associations. A sig-nificant difference exists in the distribution of variousgenotypes and haplotypes for the IL-10 promoter poly-morphic sites between UK whites and our patients,suggesting that this could be a useful anthropologicgenetic marker. However, we were unable to demon-strate a role of these polymorphisms in the predisposi-tion of individuals to the development of SLE. Thissuggests either that they play no role in disease suscep-tibility per se or that genetic heterogeneity exists in thepatient group and the role of the IL-10 polymorphismmay be apparent only when it is examined in thecontext of the interaction of other polymorphic genes.Having said this, however, among our SLE patients, weshowed that the promoter polymorphisms at positions–824 and –597 were significantly associated with glo-merulonephritis. This is consistent with the hypothesisthat patients who are more capable of producing IL-10have a higher risk of renal disease, because IL-10promotes autoantibody production, and thus, immunecomplex formation and deposition in the kidneys.Although the functional significance of the promoterpolymorphisms has not been tested in our subjects, wesuggest that there may exist inter-ethnic variations inthe genetic control of IL-10 production by differentalleles in the IL-10 promoter.
INFLUENCE OF GENDER AND SEX HORMONES ON SLE
Previous studies in both humans and animals havedemonstrated that females express enhanced levels ofimmunoreactivity compared to their male counterpart.While this gender difference in the immune capabilitiesmay provide females with increased resistance to manytypes of infection and hence survival advantage, it hasalso been hypothesized that this may increase the sus-ceptibility of women to various autoimmune diseasessuch as thyroiditis, Graves’ disease, primary biliary cir-rhosis, insulin dependent diabetes mellitus, rheumatoid
arthritis, primary Sjögren’s syndrome, scleroderma,multiple sclerosis and SLE when compared to men.
There are several possible explanations for the highersusceptibility of females to autoimmune diseases. Apartfrom a possible difference in genes encoded in thesex chromosomes, the influence of the sex hormoneson the immune system plays an important role in thisaspect. Sex hormones such as estrogens, progesterone,androgens and prolactin have been shown to exert pro-found effects on the functions of the various cell typesof the immune system. The difference in the hormonalmilieu and the hormonal–immune interaction betweenthe two sexes may account, at least in part, for thegender difference in the susceptibility of autoimmunedisorders.
While animal studies and in vitro human studieshave shown evidence for a role for sex hormones in thepathogenesis of SLE, it is important to confirm thesefindings in clinical observation studies.
Sex hormone profile in male SLE patientsOne way of assessing the significance of male andfemale sex hormones in SLE is to study their profilein male lupus patients, and evaluate their correlationwith disease manifestations and activity. In a study con-ducted earlier, we investigated the serum sex hormonelevels – luteinizing hormone, follicular stimulatinghormone, total unconjugated testosterone, estradial,and prolactin – in 35 male SLE patients, and comparedthe results with age-matched healthy controls.20 Ourresults showed that serum levels of testosterone, estra-diol and the ratio of estradiol to testosterone were notsignificantly different between patients and age-matchedcontrols. However, the levels of gonadotrophins weresignificantly higher in the SLE patients and a certainproportion of patients had evidence of hypoandrogen-ism with low testosterone and high LH levels (Table 3).
Table 3 Number of patients and controls with abnormal hormonal levels
Plasma levelsControls (n = 33)
Male SLE (n = 35)
FSH > 7 IU/L 6 (18%) 19 (54%)LH > 8 IU/L 3 (9%) 12 (34%)T < 12 nmol/L 5 (15%) 6 (17%)E2 > 161 pmol/L 3 (9%) 2 (6%)High LH + Low T 0 (0%) 5 (14%)High FSH & LH + Low T 0 (0%) 4 (11%)E2/T > 12 2 (6%) 5 (14%)
Normal ranges for adult males – FSH: 1–7 IU/L; LH: 1–8 IU/L; T: 12–35 nmol/L; E2: 22–161 pmol/L.

Pathogenesis of SLE
APLAR Journal of Rheumatology 2004; 7: 83–89 87
These patients did not have overt clinical features ofhypogonadism but had a higher prevalence of centralnervous system disease and serositis than those withnormal androgen levels. On the other hand, active lupuswas associated with a lower level of testosterone but thedifference was not statistically significant. Althoughprolactin and total testosterone levels were not differ-ent between patients and controls, the ratio of pro-lactin to testosterone was significantly higher in the SLEpatients and correlated with disease activity scores.
It should be noted, however, that despite the factthat a high incidence of sex hormone abnormalities isdemonstrated in our male SLE patients, whether this isintrinsic to SLE or the result of any non-specific chronicillnesses cannot be distinguished from our data.
Ovarian failure and flares of SLEAnother way to evaluate the role of female sex hor-mones in SLE is to study what happen to the patient’sdisease after they have developed ovarian failure. Onewould expect these patients who are hypo-estrogenemicto have a lower frequency of disease flares.
In this study, premenopausal patients with SLE under45 years who had severe organ manifestations andrequired the use of oral cyclophosphamide (CYC) fordisease control were recruited for analysis.21 All patientshad similar disease severity at the time of CYC treatmentand had received the same cumulative dose of CYC forthe same length of time. The rates of severe and mild/moderate disease flares within the first 5 years ofCYC therapy were obtained and comparison was madebetween patients who developed documented CYC-induced ovarian failure and those who did not.
Of 44 patients studied, 14 developed documentedovarian failure with hypo-estrogenemia within 2 yearsafter CYC treatment. Compared with the menstruatinggroup of patients, those who developed ovarian failurewere significantly older at the time of CYC therapy(mean 37.9 vs 25.5 years; P < 0.001), but otherwise nosignificant differences in organ manifestations and auto-antibody profiles between the two groups were observed.Both the ovarian failure group and menstruating groupof patients had similar SLE Disease Activity Indexscores at the time of CYC treatment, and had compar-able treatment durations and cumulative doses of CYC.Flares of SLE were uncommon during the first year fol-lowing CYC administration. However, during the 5-yearfollow-up period, patients who developed CYC-inducedovarian failure had significantly fewer severe flares andsmaller total number of flares when compared withthose who were still menstruating (Table 4).
Results obtained from this study provide evidence thata hypo-estrogenemic state is protective against lupusflares.
ABNORMAL APOPTOSIS AND DEFECTIVE HANDLING OF APOPTOTIC CELLS IN THE PATHOGENESIS OF SLE
Apoptosis, or programmed cell death, is an energy-dependent process that occurs in various physiologicalstates including withdrawal of growth factors or cellularinsults by factors including hypopoxia, irradiation orchemicals like corticosteroids and alkylating agents.Increased apoptosis or defective removal of apoptoticcells leads to the breakdown of tolerance.
Table 4 Ovarian failure and lupus flares
Ovarian failure(n = 14)
Menstruating(n = 40)
Age at CYC administration (years) 37.9 (1.8) 25.5 (1.2)SLEDAI at CYC treatment 15.6 (1.2) 17.7 (0.8)Duration of CYC treatment (months) 8.2 (0.8) 7.8 (0.5)Daily dose of CYC (mg) 85.6 (3.9) 77.8 (3.4)Year 1 post-treatment: no. of severe flares/patient 0.00 0.00Total no. of flares/patient 0.00 0.050 (0.03)Year 2 post-treatment: no. of severe flares/patient 0.00 0.025 (0.03)Total no. of flares/patient 0.071 (0.07) 0.250 (0.08)Years 3–5 post-treatment: no. of severe flares/patient years 0.024 (0.02)† 0.117 (0.03)Total no. of flares/patient years 0.191 (0.06) 0.317 (0.05)Overall 5 year post-treatment: no. of severe flares/patient years 0.014 (0.01)† 0.074 (0.02)Total no. of flares/patient years 0.128 (0.04)† 0.250 (0.03)
CYC, cyclophosphamide; SLEDAI, systemic lupus erythematosis disease activity index; †compared with menstruating patients, P < 0.05.

C. S. Lau
88 APLAR Journal of Rheumatology 2004; 7: 83–89
Defects in apoptosis have been implicated in theonset of SLE. A possible association between SLE andFas-mediated apoptosis and the failure of cell tolerancewas suggested when Chu et al.22 reported a defect inFas messenger-RNA expression in MRL lpr mice. Thishypothesis was later supported by the identification ofthe gld gene, which was phenotypically similar to lpr,as a non-functional Fas ligand gene.23 In human SLE,increased spontaneous in vitro apoptosis in culturedPBMCs has been described.6 Indeed, the famous LEcell, which has only recently been removed from theACR criteria for SLE, is itself a neutrophil that hasphagocytosed apoptotic bodies.
It is prudent that apoptotic bodies are effectivelycleared to avoid release of intracellular contents thatmay be immunogenic, which may induce T- and B-cellautoreactivity.24 Impairment, if any, in phagocytic cellclearance of apoptotic bodies may therefore have apathogenic role in SLE. Recently, we studied the rate ofapoptosis of polymorphonuclear neutrophils (PMNs)and macrophages and the macrophage ability to removeapoptotic cells in patients with SLE and controls.25
In this study, we observed that the rate of in vitroapoptosis of PMNs and macrophages was increasedin patients with SLE when compared with controls.Patients with active disease had higher rates of in vitroapoptosis than did patients with inactive disease.Interestingly also, our results showed that serum frompatients with active SLE accelerated in vitro apoptosis inPMNs, while serum from control subjects failed to pre-vent cells from SLE patients from undergoing apopto-sis. These results suggest that both genetic and serumfactors that regulate PMN apoptosis may be abnormalin SLE.
Another important finding of this study was thatmacrophages from patients with SLE were less capableof ingesting apoptotic PMNs when compared withmacrophages from control subjects. Further, the ability
of macrophages to phagocytose apoptotic cells is inverselycorrelated with biochemical and serologic markers oflupus disease activity and the overall SLEDAI score. Thesefindings confirmed that impaired macrophage phago-cytosis has a contributory role in the pathogenesis ofSLE.
The underlying mechanism of defective macro-phage phagocytosis in SLE has not been fully evalu-ated. In our study, serum obtained from patients withactive SLE impaired the phagocytic ability of healthycontrol macrophages. Conversely, serum from controlsubjects restored the phagocytic ability of macro-phages from patients with SLE (Table 5). These datasuggest that in patients with SLE, the impaired abilityof macrophages to phagocytose apoptotic PMNs issecondary to the presence or absence of certain serumfactor(s) rather than being attributable to an intrinsicdefect of the macrophage or its binding to apoptoticPMNs.
CONCLUSION
In conclusion, SLE is a heterogeneous disease entitywith a multifactorial aetiology. Asia probably has thelargest number of lupus patients. Research in thiscondition in the Asia-Pacific region has gathered pace inthe past two decades. We in Hong Kong, have followedthe footsteps of our neighbours in this area of research.Although our contribution might have been limited,our studies have added evidence of a complex inter-action between genetic and environmental factors indetermining the susceptibility and manifestation ofSLE. We will continue to be inspired by Dr Tay and hiscolleagues and work toward the endeavour that oneday the whole network of the immuno-etiology of SLEwill be uncovered and specific treatment can be offeredto our patients to reduce disease-related complicationsand mortality to the minimum.
Table 5 Macrophage phagocytosis of apoptotic neutrophils expressed as percentage macrophage ingesting apoptotic neutrophils from healthy subjects and patients with SLE
Cultured with autologous serum
Cultured with active SLE serum
Cultured with healthy serum
Healthy subjects 38.7 ± 5.2% 13.2 ± 2.1%All SLE patients 23.2 ± 4.1%Active SLE patients 16.0 ± 4.0% 50.6 ± 7.4%Inactive SLE patients 27.5 ± 5.1%
Patients with active disease had a systemic lupus erythematosis disease activity index (SLEDAI) score = 5 at the time of study. Patients were classified as having inactive disease if the SLEDAI score was persistently = 4 for at least 4 months prior to study. Results are expressed as mean ± standard error of mean.

Pathogenesis of SLE
APLAR Journal of Rheumatology 2004; 7: 83–89 89
REFERENCES
1 Lau CS, Mok MY (1998) Lupus in Asia. JAMA (SEA) 14,5–7.
2 Mok CC, Lau CS, Chan TM, Wong RWS (1999) Clinicalcharacteristics and outcome of southern Chinese maleswith systemic lupus erythematosus. Lupus 8, 188–96.
3 Ho CTK, Mok CC, Lau CS, Wong RWS (1998) Late-onsetlupus eyrthematosus in southern Chinese. Ann Rheum Dis57, 437–40.
4 Turner MW (1998) Mannose-binding lectin (MBL) inhealth and disease. Immunobiology 199, 327–39.
5 Senaldi G, Davies ET, Peakman M, Vergani D, Lu J, Reid KB(1995) Frequency of mannose-binding protein deficiencyin patients with systemic lupus erythematosus (letter;comment). Arthritis Rheum 38, 1713–4.
6 Lau YL, Lau CS, Chan SY, Karlberg J, Turner MW (1996)Mannose-binding protein in Chinese patients with systemiclupus erythematosus. Arthritis Rheum 39, 706–8.
7 Davies EJ, Snowden N, Hillarby MC et al. (1995)Mannose-binding protein gene polymorphism in systemiclupus erythematosus (see comments). Arthritis Rheum 38,110–4.
8 Davies EJ, Teh LS, Ordi-Ros J et al. (1997) A dysfunctionalallele of the mannose binding protein gene associates withsystemic lupus erythematosus in a Spanish population. JRheumatol 24, 485–8.
9 Carthy D, Hajeer A, Ollier B et al. (1997) Mannose-binding lectin gene polymorphism in Greek systemiclupus erythematosus patients (letter). Br J Rheumatol 36,1238–9.
10 Walport MJ (1993) The Roche Rheumatology Prize Lecture.Complement deficiency and disease. Br J Rheumatol 32,269–73.
11 Sullivan KE, Wooten C, Goldman D, Petri M (1996)Mannose-binding protein genetic polymorphisms in blackpatients with systemic lupus erythematosus. Arthritis Rheum39, 2046–51.
12 Ip EWK, Chan SY, Lau CS, Lau YL (1998) Association ofsystemic lupus erythematosus with promoter polymor-phisms of the mannose-binding lectin gene. Arthritis Rheum41, 1663–8.
13 Lau CS, Ip EWK, Ip Mok CC et al. (2000) Mannose bind-ing lectin and autoimmune disease. APLAR J Rheumatol 4,17–20.
14 Llorente L, Richaud-Patin Y, Wijdenes J et al. (1993)Spontaneous production of interleukin-10 by B lym-phocytes and monocytes in systemic lupus erythematosus.Eur Cytokine Netw 4, 421–7.
15 Csiszar A, Nagy G, Gergely P, Pozsonyi T, Pocsik E (2000)Increased interferon-gamma (IFN-gamma), IL-10 anddecreased IL-4 mRNA expression in peripheral bloodmononuclear cells (PBMC) from patients with systemiclupus erythematosus (SLE). Clin Exp Immunol 122, 464–70.
16 Grondal G, Gunnarsson I, Ronnelid J, Rogberg S,Klareskog L, Lundberg I (2000) Cytokine production,serum levels and disease activity in systemic lupus ery-thematosus. Clin Exp Rheumatol 18, 565–70.
17 Hagiwara E, Gourley MF, Lee S, Klinman DK (1996) Dis-ease severity in patients with systemic lupus erythemato-sus correlates with an increased ratio of interleukin-10:interferon-gamma-secreting cells in the peripheral blood.Arthritis Rheum 39, 379–85.
18 Eskdale J, Wordsworth P, Bowman S, Field M, Gallagher G(1997) Association between polymorphisms at the humanIL-10 locus and systemic lupus erythematosus. Tissue-Antigens 49, 635–9.
19 Mok CC, Lanchbury JS, Chan DW, Lau CS (1998)Interleukin-10 promoter polymorphisms in southernChinese patients with systemic lupus erythematosus.Arthritis Rheum 41, 1090–5.
20 Mok CC, Lau CS (2000) Profile of sex hormones in malepatients with systemic lupus erythematosus. Lupus 9, 252–7.
21 Mok CC, Wong RWS, Lau CS (1999) Ovarian failure andflares of systemic lupus erythematosus. Arthritis Rheum 42,1274–80.
22 Chu JL, Drappa J, Parnassa A, Elkon KB (1993) The defectin Fas mRNA expression in MRL/lpr mice is associatedwith insertion of the retrotransposon, ETn. J Exp Med 178,723–30.
23 Takahashi T, Tanaka M, Brannan CI et al. (1994) General-ised lymphoproliferative disease in mice, caused by apoint mutation in the Fas ligand. Cell 76, 969–76.
24 Ren Y, Savill J (1998) Apoptosis: the importance of beingeaten. Cell Death Differ 5, 563–8.
25 Ren Y, Tang J, Mok MY, Chan AWK, Wu A, Lau CS (2003)Increased apoptotic neutrophils and macrophages andimpaired macrophage phagocytic clearance of apoptoticneutrophils in systemic lupus erythematosus. ArthritisRheum 48, 2888–97.