Embed Size (px)
Citation preview

Why all HIV+ Women on Antiretroviral Therapy Should
Breastfeed in both Low and High Resource Settings
Natella Rakhmanina, MD, PhD Professor of Pediatrics
The George Washington UniversityDirector, Special Immunology Program
Children's National Health SystemSenior Technical Advisor
Elizabeth Glaser Pediatric AIDS Foundation
HIV and Women WorkshopSeattle, 2017

Facing Lynne……is toughSamuel J. Heyman Service to America Medals honoring outstanding federal employees for service to their communities and for making a
difference

But Being Russian Helps….

Breastfeeding in the Resource Rich Settings
• 81.1% started to breastfeed in 2013 in the USA and 51.8% were breastfeeding at 6 months (2016 Breastfeeding Report Card, CDC)
• 83% initiated breastfeeding in the UK in 2010, exclusive breastfeeding at six months was 34% (UNICEF, UK, 2012)
• 89% off mother in Canada breastfed in 2011–2012, with 26% breastfeeding exclusively for six months (Statistics Canada)

Essential Women’s Right

Maternal Benefits of Breastfeeding
• Improved postpartum recovery• Decreased postpartum depression • Improved long term bone health• Decreased maternal cardiovascular
diseases• Diminished risk of cancer (breast and
ovarian)
AAP Policy Statement, 2012


Rights of the Child
Per Convention on the Rights of the Child, children have a right to the best start in life
with the best chance for health including higher intelligence, better growth,
protection against immediate and chronic diseases

Benefits of Breastfeeding for Children
• Decreased allergic diseases• Improved neurodevelopmental outcomes• Reduced obesity and other factors related to
heart disease • Reduced early childhood infections and
gastrointestinal disease (IBD, celiac disease)• Reduced diabetes rates and childhood
cancers• Improved outcomes in prematurity and LBW
AAP Policy Statement, 2012

Prenatal HIV Exposure and Prematurity
Uthman et al.Lancet HIV. 2017 Jan;4(1):e21-e30

See for yourself……
This is good…….. But this is better………

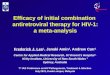
PROMISE Results

Among HIV-infected women who do not meet criteria for initiation of HAART for their own health, what is the optimal intervention to prevent transmission of HIV to infants during breastfeeding?
R
2,431 mother-infant pairs
Maternal ART during
breastfeeding
Infant daily NVP during
breastfeeding
n=1,220 n=1,211
PROMISE Postpartum Component: Maternal ART vs Infant NVP for Preventing PP MTCT
Taha T et al. IAS 2016 Durban S Africa, Abs. LBPE013
13 sites Africa, 1 site IndiaEnrolled June 2011-October 2014
Medianduration
BF15 mos
Infant: Median GA: 39 wkMedian BW: 2.9 kg
Mother: Median CD4: 68697% WHO Stage IMedian age: 26 yr

At 6 months of age, estimate 0.3%
(95% CI, 0.1-0.6)
At 9 months of age, estimate 0.5%
(95% CI, 0.2-0.8)
At 12 months of age, estimate 0.6%(95% CI, 0.4-1.1)
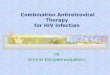
PROMISE Postpartum Component: Maternal ART vs Infant NVP for Preventing PP MTCT
Taha T et al. IAS 2016 Durban S Africa, Abs. LBPE013
No statistically significant difference in probability of MTCT of HIV by study arm (in both primary and sensitivity analyses).

Infant 12-month survival rate was extremely high (98.9%)
and did not differ significantly by study arm
PROMISE Postpartum Component: Maternal ART vs Infant NVP for Preventing PP MTCT
Taha T et al. IAS 2016 Durban S Africa, Abs. LBPE013
Infant Survival

NIH Statement, July 2016
“Maternal antiretroviral therapy safely minimizes the threat of HIV transmission
through breast milk while preserving the health advantages of breastfeeding, as the high infant
survival in this study underscores.”Anthony Fauci

Number of Children 0-14 Years Living with HIV Globally, 1990-2015: 2015 vs 2016 Estimates, UNAIDS 2016
Revision SPECTRUM model based on 2016 review of available data: PMTCT with ART more effective than prior estimates Median age children starting ART older than prior estimates Lead to mortality in children higher than prior estimates Result: ↓ children LWH than previous due to ↓ incidence & ↑ mortality
1.8 M
2.6 M
WHO, 2009

Number of Children 0-14 Years Newly Infected with HIV Globally, 1990-2015: 2015 vs 2016 Estimates, UNAIDS 2016
Revision SPECTRUM model based on 2016 review of data: MTCT with incident infection estimates lower than earlier PMTCT with ART more effective than prior estimates Results in fewer children than prior estimates due to ↓
incidence
160,000
220,000
27% lower
WHO, 2009

Compared to Low Resource Settings, we have:
• Less pressure for mixed feeding methods • Ample maternal VL monitoring and
repeat infant testing • Better and easier to take maternal ART
regimens with multiple choices • Better monitoring of short and long-term
toxicity

We get it….
In high resource settings PreP comes first

How to do it right?
“For to be free is not merely to cast off one's chains, but to live in a way that respects and enhances the freedom of
others” Nelson Mandela

How to do it right?• Initiating counseling before pregnancy and early
in pregnancy • Providing education on breastfeeding and
expectations for mother/child• Discussing all available options including donor
breast milk (wet nurse, banked breast milk)• Supporting mother in her decision and helping
hers and infant ART adherence • Repeating HIV testing in mother and the child

Seattle votes!
Seattle votes!

BAN or NO BAN?
• WHO recommends breastfeeding - NO BAN!• USA does not recommend breastfeeding- BAN!• Canada does not recommend breastfeeding -
BAN!• UK does not recommend, but understands –
BREXIT!• Europe – it depends…..• Your answer????