Embed Size (px)
Citation preview

Why Did They Close All Those Beds in the 1990s?!
Amy Diane Short, Lee Ann Liska and Ann Schlinkert
2/2/2006© 2005 The University Hospital , Cincinnati
2
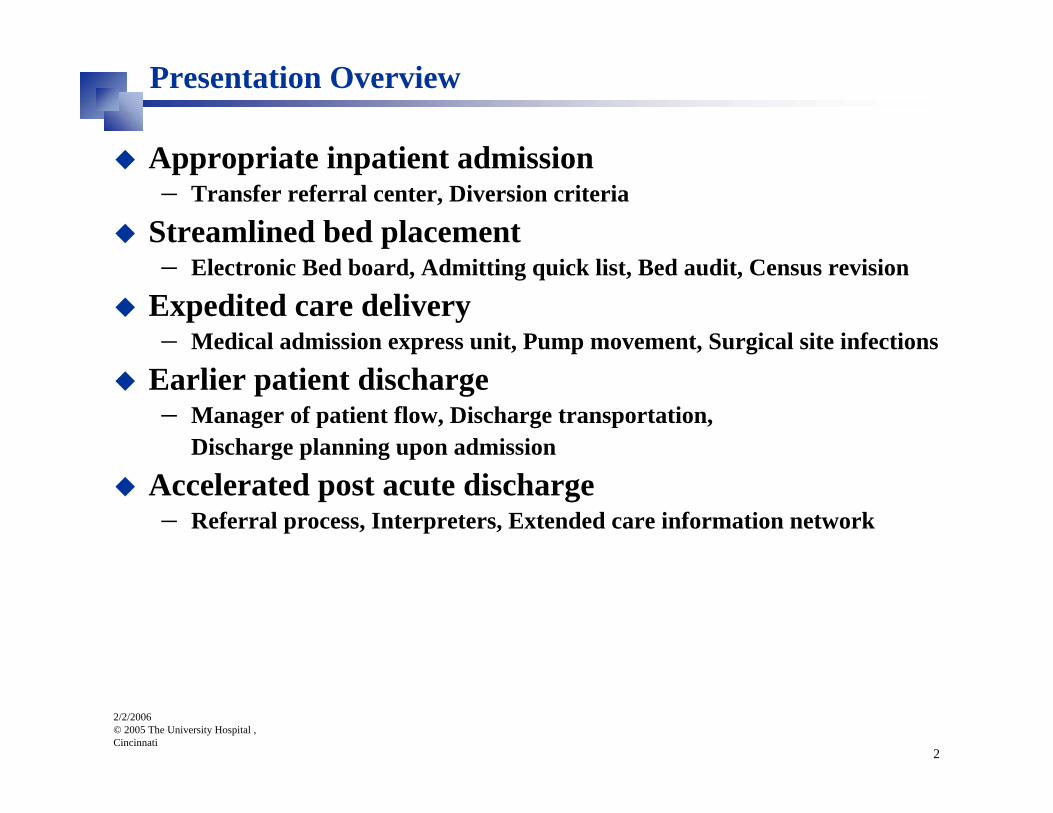
Presentation Overview
Appropriate inpatient admission– Transfer referral center, Diversion criteria
Streamlined bed placement– Electronic Bed board, Admitting quick list, Bed audit, Census revision
Expedited care delivery– Medical admission express unit, Pump movement, Surgical site infections
Earlier patient discharge– Manager of patient flow, Discharge transportation,
Discharge planning upon admission
Accelerated post acute discharge– Referral process, Interpreters, Extended care information network

2/2/2006© 2005 The University Hospital , Cincinnati
3
Capacity Constraints: National Dilemma
Gone are the days of having too many bedsEmergency rooms are at risk of diversionPACUs struggle to keep the operating rooms productiveCath labs must compete for inpatient bedsTransfers-in from other hospitals compete for limited inpatient space Direct admits face long delaysEvery bed is in use
2/2/2006© 2005 The University Hospital , Cincinnati
4
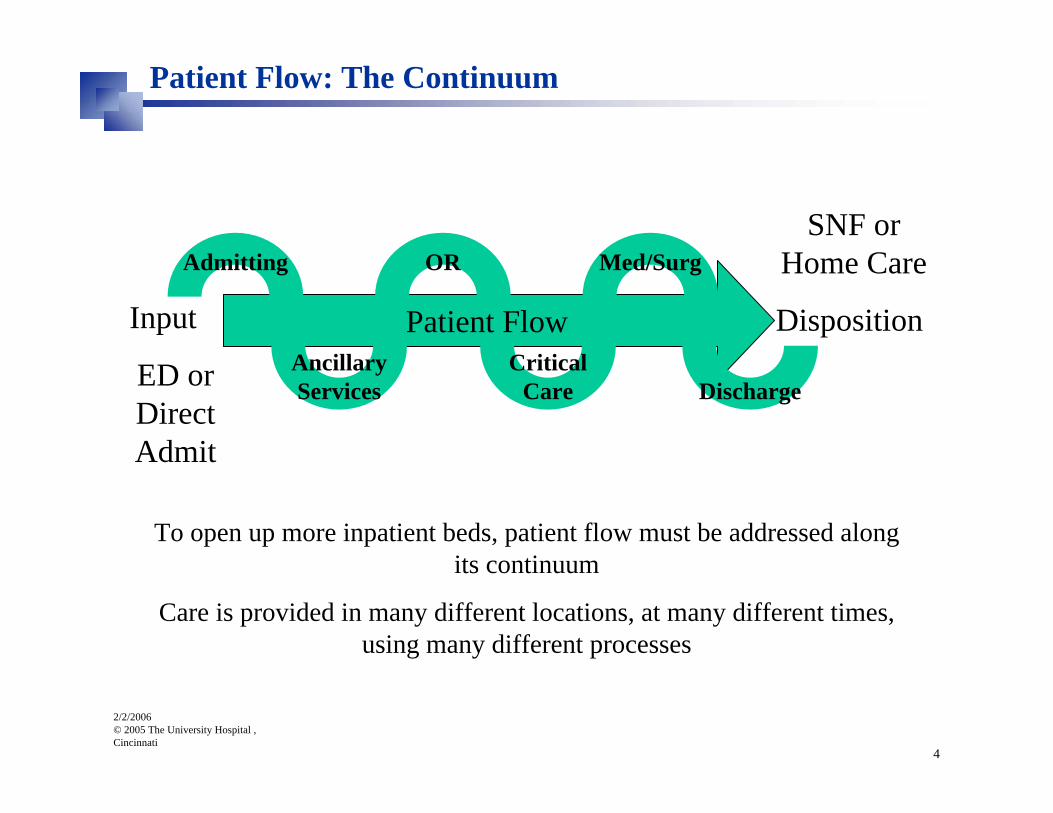
Input
ED or Direct Admit
SNF or Home Care
DispositionPatient FlowAncillaryServices
Admitting OR
CriticalCare
Med/Surg
Discharge
To open up more inpatient beds, patient flow must be addressed along its continuum
Care is provided in many different locations, at many different times, using many different processes
Patient Flow: The Continuum

2/2/2006© 2005 The University Hospital , Cincinnati
5
Patient Flow: The Solution
Key areas to address:– Appropriate inpatient admission– Streamlined bed placement– Expedited care delivery– Earlier patient discharge– Accelerated post acute discharge

2/2/2006© 2005 The University Hospital , Cincinnati
6
Patient Flow Project Structure: Old
Patient Flow Steering TeamLee Ann Liska (Chair)
Mavis BechtleAndrea Stewart
Patient Flow Action TeamLee Ann Liska (Chair)
Steering Team Mark Schroer, MDGreg Fermann, MD
Tim Pritts, MDMgt Point Persons (per below)
OE/BB Support (per below)Meeting frequency: bi-weekly
Appropriate Inpatient Admission
Michael GrodiAmy Short (BB)
Streamlined Bed Placement
Ann SchlinkertTerry Dunn (BB)
Expedited Care DeliveryRene Fischer
Yvette Kauffman (BB)
Earlier Patient DischargeDenise Jackson
Hewley Hinds (BB)
Accelerated Post-Acute Transfer
Peggy SogarBeth Solomon (BB)
Other Analytical ProjectsAmy Short
Trish Zapanta
Coordination with other TUH Projects
Lee Ann Liska
Coordination with other Alliance Throughput
ProjectsAndrea Stewart
Structure active from May to August 2005

2/2/2006© 2005 The University Hospital , Cincinnati
7
TUH Patient Flow Project Structure: Current
Patient Flow Action TeamLee Ann Liska (Chair)
Mavis BechtleAmy Diane ShortAnn Schlinkert
Ruby Crawford-HemphillRene Fischer
Denise JacksonMark Schroer, MDJohn Deledda, MD
Tim Pritts, MD
Meeting frequency: monthly
Other Analytical ProjectsLinda Flesch
Trish Zapanta
Coordination with other TUH Projects
Lee Ann Liska
Structure active from September 2005 to present

2/2/2006© 2005 The University Hospital , Cincinnati
8
Patient Flow: Metrics
MetricHCAB
BenchmarkTUH
Baseline JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV +/-
ALOS (Days) 4.6 4.9* 5.0 5.0 4.8 4.8 4.8 4.9 4.9 4.7 4.9 4.9 4.8 (0.2)
Hours on Diversion 0 44** 104 31 16 66 0 71 51 82.0 36.0 15.0 0.0 (15.0)Avg Wait Time for IP Beds -PACU (Mins) <= 60 146* 132 145 112 114 126 139 140 135 121 132 89 (43.0)
Avg Wait Time for IP Beds -ED (Mins) <= 60 434*** 457 457 455 410 288 396 377 330 392 300 272 (28.0)
Avg Wait Time for IP Beds -TRANSFERS-IN New Process (Mins)
<= 60 142**** NA NA NA 43 58 156 184 163 234 206 79 (127.6)
Avg Wait Time for IP Beds -TRANSFERS-IN Old Process (Mins)
<= 60 142**** 215 202 170 247 164 274 461 272 465 221 167 (54.7)
Modal Discharge Times (Time) 11:00am 14:00* 14:00 14:00 14:00 14:00 14:00 14:00 14:00 14:00 14:00 14:00 14:00 0.0
Transport Average TAT (Mins) 35 37** 36 35 39 39 40 40 39 46 42 36 34 (1.2)
Room Turn TAT - Regular (Mins) TBD 98** 88 92 102 101 107 110 107 115 112 118 119 1.0
Room Turn TAT - STAT (Mins) TBD 67** 67 65 67 69 67 66 67 71 70 73 76 3.0

Appropriate Inpatient Admission

2/2/2006© 2005 The University Hospital , Cincinnati
10
Transfer Referral Center: Concerns
Referring physicians– Passed around on phone to other TUH physicians– Took too long to get connected to a TUH physician– Uninformed about length of time for bed– Takes too long to get a bed
Accepting physicians– Unaware of the bed situation– ED physicians concerned about direct transfers to the ED

2/2/2006© 2005 The University Hospital , Cincinnati
11
Transfer Referral Center: Solutions
Give transfers-in more priority– Met with Nursing Supervisors– Asked that acuity be the criteria– Bed updates involve the Nursing Supervisors
Get Transfer Center staff access to better on-call information– Same information that operators use
Develop a paging escalation policy– Five minutes to return a page– Next pages escalate to a higher level
Transfer Center staff stays on the phone– Can facilitate the call
– Keeps tabs on the transfers’ progress– Provides regular updates on bed status

2/2/2006© 2005 The University Hospital , Cincinnati
12
Transfer Referral Center: Solutions
Hire a Physician Referral SpecialistDevelop scripts– Standardize the process
Create new forms for the Transfer Center– Capture more data
Record and QA calls– Error proof the process– Train and educate– Maintain a respectful organization
Get insurance pre-certificationsDevelop an ED admitting policy– Set the clear expectations
Transfer Center staff screen for the ED physicians– One of the benefits of staying on-line

2/2/2006© 2005 The University Hospital , Cincinnati
13
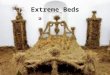
Transfer Referral Center
Percentage Successful Transfers-in
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
Week
Perc
enta
ge % SuccessfulBaseline 90%Target 97%
Process Change at Week 18
Week 29 dipped because of ED diversion and transfer referral center staff vacations

2/2/2006© 2005 The University Hospital , Cincinnati
14
Diversion Criteria Setting Project
Worked with the Greater Cincinnati Health Council to develop citywide “at capacity” guidelinesSet up 24/7 methods of diversion communication to key TUH stake holdersRolling out “Throughput Action Plan” (TAP)Posting “Bed Alert” signsDeveloping “Peak Census Plan” for each unit

2/2/2006© 2005 The University Hospital , Cincinnati
15
Diversion Criteria Setting Project
Hours on Diversion10
431
66
0
51
36
44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44
8272
16
0
15
020406080
100120
Janu
aryFeb
ruary
March
April
MayJu
ne July
Augus
tSep
tembe
rOcto
ber
Novembe
rDece
mber
Janu
aryFeb
ruary
March
April
May
Month
Hour
s DiversionBaseline
Streamlined Bed Placement
2/2/2006© 2005 The University Hospital , Cincinnati
17
Maximized Use of the Electronic Bed board: Phase I
The manual bed board:– Difficult to see the big picture of bed activity– Many phone calls to get a bed– No easy way to check the status of a dirty room.– Inconsistent communication about bed assignment
Teletracking’s electronic bed board solution– Implemented Phase I in March 2005– Rolled out five units

2/2/2006© 2005 The University Hospital , Cincinnati
18
Maximized Use of the Electronic Bed board: Phase II
The electronic bed board:– Units can see their bed activity (pending, admissions, discharges and
transfers)– No phone calls for bed placement (except ICU)– Real-time feed back on room clean status by pager– Real-time notification of bed assignment by pager– Nursing supervisors can see the bed big picture on their computers

2/2/2006© 2005 The University Hospital , Cincinnati
19
Throughput team prioritized phase II as a key projectPhase II rolled out 17 more units– Implemented August 2005
Users trained on-site by vendorEnhancement on-going:– Already upgraded system– Monthly user group meeting– Meeting users’ needs
Maximized Use of the Electronic Bed board: Phase II

2/2/2006© 2005 The University Hospital , Cincinnati
20
Maximized Use of the Electronic Bed board: Phase II

2/2/2006© 2005 The University Hospital , Cincinnati
21
Emergency Department “Quick List”
Forms and related documentation– Puts monitoring requirements, infectious disease concerns, and downgrade
information all in one place– Facilitates getting the right patient in the right bed and prevents delays– Keeps patient from returning to the ED
The University Hospital Emergency Department Admission Form* Date: _______________________ Time: _______________________ Diagnosis: _______________________________ Condition: Good Fair Serious Critical Monitoring Requirements (Check all that apply): None General
Telemetry: O2 sat & HR only
9 CCP 4 N/E 5 N/W/E MPCU 8CCP (FMCU)
Dysrhythmia Telemetry (Dysrhythmia Care per RNs)
6S 6/N/W CSD 7NW –no r/o MI
Patient Safety Monitor/Sitter **
Reason:
Infectious Disease Concerns (All transmission based precautions need a private room):
VRE Precautions ** Airborne Precautions (Negative Airflow Room) **
Droplet Precautions **
Contact Precautions **
Other – Describe**:
Other:
AKA (Protected Patient)*
Police Hold w/ Guard **
Peritoneal Dialysis with Cycler 7NW (CMCU), MPCU, MICU
Immuno-Deficient** Other - Describe:
Downgrade: Time of Request: _____________________
Admitting Attending Approved? : Yes No
Time of Response:__________________
Please Name Any Continuous IV Medications for This Patient: ______________________________________________________________________ Type of Bed Requested : ____________________________________
Medication Nursing Units Maximum Dose Special Considerations
Amiodorone CSD, 6S 1 MG/MIN
Ativan CSD, NPCU, MPCU 10 MG/HRMay remain in stepdown if dose has not been adjusted within 6 hours
Diltiazem CSD, NPCU, 6S 5-20 MG/HR
Dobutamine CSD, NPCU, 6S 20 MCG/KG/MIN Maintanance dose or weaning to off
Dopamine CSD, NPCU, MPCU, 6S, 6NW 5 MCG/KG/MIN Maintanance dose or weaning to off
Esmolol CSD 300 MCG/KG/MIN Must be weaning to off
Insulin CSD, NPCU, MPCU 0.1 UNITS/KG/HR Higher dose must be transferred to ICU
Milrinone CSD, 6S 0.75 MCG/KG/MIN
Nitroglycerin CSD, NPCU, Patient must have telemetry monitoring
Contact Isolations Airborne Isolation Non-Orders
Room Type: Private Room Negative Airflow Room (These orders do NOT exist)
● VRE ● Rule Out TB ● Respiratory● Clostridium difficile ● Active TB ● Reverse Isolation
● Lice/Scabies● Herpes Zoster (varicella-zoster) Chickenpox ● Neutropenic Precautions
● All draining wounds not contained by a dressing ● SARS ***
● All mulit-drug resistant organisims ● Smallpox ***● Monkeypox ***● Vaccinia Reactions or disease ***● Viral hemorrhagic viruses ***● Shingles ††
Turned in as: “…with contact precautions” “…with airborne isolation” (These orders do NOT exist)
For the HUC:Enter “Contact Precautions” in the
comments sectionEnter “Airborne Isolation” in the comments
section (These orders do NOT exist)
Questions?
(General) Telemetry
Either or both:
● Heart Rate
● O2 saturation
Dysrhythmia Telemetry
Cardiac Dysrhythmia monitoring plus either or both:
● Heart Rate
● O2 saturation
Patient Needs:
TELEMETRY MONITORING CAPABILITIES
The University Hospital
Bed Assignment Reference (BAR)
Dial the Operator and page the on-call Infection Control Practitioner.
Diagnosis:
Hospital Infection Control Policy II-334 Standard Precautions/Transmission Based Precautions
Notes:
This policy is a complete listing of diseases and conditions, with the isolation precautions they require. A current copy is available on the Health Alliance Intranet
Additional Reference:
INFECTION CONTROL REQUIREMENTS
● Pertussis (whooping cough)
● Pneumonia (until diagnosed)
● All undiagnosed respiratory illnesses
● Cystic Fibrosis (with contact precautions)
● Influenza
● Meningococcal Meningitis (Neisseria)
MEDICATION LIMITS
*** For these conditions PAGE INFECTION CONTROL IMMEDIATELY via hospital operator!
†† ONLY if Disseminated (varicella-zoster) or in a immuno-compromised patient.
“…with droplet precautions”
Enter “Droplet Precautions” in the comments section
Droplet Precautions
Private Room
● Mycoplasma Pneumonia
DRAFT DRAFT

2/2/2006© 2005 The University Hospital , Cincinnati
22
Conducted physical bed audit– Counted how many beds are currently in use– Counted how many head walls that could be immediately used if needed– Detailed renovation opportunities to expand bed count
Revising daily census report– Creating a tool that communicates, on a daily basis, the number of potential
beds, number of beds open for use, and the number of beds actually occupied by both inpatients and observation patients
Streamlined Bed Placement: Other Key Projects

Expedited Care Delivery

2/2/2006© 2005 The University Hospital , Cincinnati
24
Medicine Admission Express Unit (MAEU)
Purpose:– Facilitate admission of medicine patients from the ED, clinics, and outlying
hospitals– Increase documentation– Improve quality outcomes– Improve throughput
What is it?– Six bed inpatient unit– Telemetry capabilities– Staff completes admission paperwork and teaching – Staff documents core measures

2/2/2006© 2005 The University Hospital , Cincinnati
25
Medicine Admission Express Unit (MAEU)
Medical Admission Express Unit (MAEU)
Fina
l Uni
tM
AE
UA
dmitt
ing
CE
C AOD decides toadmit patient.
Medical teamassigned andorder written.
HUC requestsMAEU bed in the
EBB, documentingpreferred final unit.
Is a final bedavailable?1
Admitting assignspatient to MAEU
Admitting waitsuntil final bed is
ready.
Are thereavailable bedsin the MAEU?
Admitting assignspatient directly to
final bed.
Yes
No
Yes
CEC gets pagedfor ready bed.
Patient going toMAEU?
Patient Arrivesfrom CEC.
Patient arrivesfrom CEC.
Admissionpaperwork and
teachingcompleted.
JCAHO coremeasures
documented.
Social needsdocumented.
PharmacyInsurancecoverage
documented.
Normal place RXfilled documented.
Admitting assignsfinal bed.
Patient transportedto final room.
PharmacyInsurancecoverage
documented.
Social needsdocumented.
Normal place RXfilled documented.
JCAHO coremeasures
documented.
Admissionpaperwork and
teachingcompleted.
A
A
B
Yes
BNo
-
No
Footnotes:
1. Final bed may not be thepreferred bed but may reflect use ofbed placement algorithm for 2ndand 3rd choices
Last Revised: 9/23/05
Pending transfer tofinal bed
requested in EBB.
Actual transfer isrequested in Last
Word

2/2/2006© 2005 The University Hospital , Cincinnati
26
Medicine Admission Express Unit (MAEU)
Barriers for transfer to final unit:– Bed not available (need M/F bed)– Inpatient beds at capacity– Discharge process not facilitated on admission– Bed not clean (in MAEU/or Receiving Unit)– Floor too busy to take report/shift change– Progressive Care acuity (no beds)– No orders for patient/delay in return call MD (primarily direct admits)

2/2/2006© 2005 The University Hospital , Cincinnati
27
45.037.530.022.515.07.50.0
Median
Mean
987654
A nderson-Darling Normality Test
V ariance 53.1605Skewness 2.30098Kurtosis 7.63890N 165
Minimum 0.3333
A -Squared
1st Q uartile 3.2750Median 5.15003rd Q uartile 9.9333Maximum 50.7833
95% C onfidence Interv al for Mean
6.7195
11.09
8.9611
95% C onfidence Interv al for Median
4.4633 5.9626
95% C onfidence Interv al for StDev
6.5802 8.1756
P-V alue < 0.005
Mean 7.8403StDev 7.2911
95% Confidence Intervals
Summary for TAT
TUH Medicine Admissions Express Unit (MAEU)
Median TAT:
5 Hours
Data Period: 11/1 – 11/30

2/2/2006© 2005 The University Hospital , Cincinnati
28
Expedited Care Delivery: Other Key Projects
Reduce non-value added movement of pumps– Pumps no longer have to go back to Central Services for cleaning– Each floor will have a room that will have enough clean IV and PCA pumps
to serve all of its units for 24 hours– Estimated go live is the end of November
OR surgical site infection– Six Sigma project found that pre-op antibiotics were twice as likely to be
given in the appropriate therapeutic time frame if there were pre-op orders

Earlier Patient Discharge

2/2/2006© 2005 The University Hospital , Cincinnati
30
Nursing’s Role in Patient Flow
Manager of Patient Flow, Ann Schlinkert– Oversight of nursing supervisors, flow nurses, float nursing staff and
discharge lounge– Runs daily am logistic meeting
Flow Nurses– These registered nurses expedite discharges for all units, facilitate internal
transfers, and pull admissions into the inpatient units– Their analysis in the 3rd Qtr 05 identified key discharge bottle necks– They have been key players in rolling out better processes for planning for
discharge at admission

2/2/2006© 2005 The University Hospital , Cincinnati
31
Keeping “All Beds Open”
All beds are open at all times– Beds can only be “closed” through a formal process– Requires administrative approval– Nursing supervisors are on the front line
Requires teamwork between the sending units, the receiving units, Admitting, and the Nurse Supervisors– All channels of communication must be open– All hands must be on deck to provide support
Daily am logistics meeting– Provides forum for senders, receivers, and support services to address daily patient
flow operational needs– Engenders real time process improvement and monitoring– Provides transparency about the need for beds across the house

2/2/2006© 2005 The University Hospital , Cincinnati
32
Discharge Transportation Improvements
Simplified discharge transportation request proceduresGoal of 15 minute transportation response time (average)
Month # Discharge Transports
January-05 210February-05 270
March-05 347April-05 321May-05 376
June-05 305July-05 349
August-05 348September-05 335
October-05 347November-05 652

2/2/2006© 2005 The University Hospital , Cincinnati
33
Discharge Transportation Improvements
Bed ID Date/Time Time Bed ID Date/Time Time622502 7/3/2005 11:11 11:11 622201 7/7/2005 00:15 0:15623202 7/3/2005 11:23 11:23 623202 7/7/2005 06:23 6:23623101 7/3/2005 11:58 11:58 622502 7/7/2005 11:17 11:17621801 7/3/2005 14:24 14:24 622601 7/7/2005 12:26 12:26623301 7/3/2005 14:26 14:26 623101 7/7/2005 13:00 13:00622601 7/3/2005 18:27 18:27 623101 7/7/2005 13:00 13:00623101 7/4/2005 07:25 7:25 622401 7/7/2005 20:11 20:11623101 7/4/2005 07:25 7:25 622901 7/7/2005 20:12 20:12622502 7/4/2005 12:59 12:59 622502 7/7/2005 23:51 23:51622602 7/4/2005 13:30 13:30 623202 7/7/2005 23:51 23:51621802 7/4/2005 16:11 16:11 623202 7/8/2005 06:28 6:28622901 7/4/2005 22:22 22:22 622501 7/8/2005 13:54 13:54622902 7/5/2005 02:09 2:09 622602 7/8/2005 14:42 14:42621802 7/5/2005 11:38 11:38 622402 7/8/2005 15:30 15:30622901 7/5/2005 11:38 11:38 623001 7/8/2005 19:03 19:03622902 7/5/2005 11:38 11:38 623101 7/8/2005 19:03 19:03622501 7/5/2005 12:09 12:09 623301 7/8/2005 19:05 19:05622401 7/5/2005 13:44 13:44 623301 7/8/2005 19:39 19:39622502 7/5/2005 15:10 15:10 621802 7/8/2005 20:48 20:48621801 7/5/2005 17:18 17:18 622001 7/8/2005 22:43 22:43623001 7/5/2005 17:32 17:32 622201 7/8/2005 23:34 23:34622301 7/5/2005 17:46 17:46 622901 7/9/2005 11:57 11:57623001 7/5/2005 19:13 19:13 622602 7/9/2005 12:16 12:16622001 7/5/2005 21:00 21:00 622302 7/9/2005 12:44 12:44622001 7/6/2005 02:25 2:25 622502 7/9/2005 12:44 12:44622201 7/6/2005 05:31 5:31 622501 7/9/2005 12:57 12:57623001 7/6/2005 10:20 10:20 622001 7/9/2005 16:41 16:41622501 7/6/2005 15:51 15:51 622301 7/9/2005 16:52 16:52622901 7/6/2005 15:56 15:56 623301 7/9/2005 18:47 18:47622301 7/6/2005 19:26 19:26623301 7/6/2005 19:26 19:26622302 7/6/2005 20:38 20:38622902 7/6/2005 22:07 22:07622901 7/6/2005 22:31 22:31
Reviewing “clustering” of EVS & transportation
requests

2/2/2006© 2005 The University Hospital , Cincinnati
34
Discharge Planning on Admission
Improve the timeliness of discharge by:– Making earlier referrals to allied services– Changing discharge RX processes– Making better use of the discharge lounge– Using transportation for discharge transports
MD writes RX
MD hands RXstraight to the
patient
Unit Nurse tubesthe RX to the DL
RX goesstraight into
chart?
Pt hands DL NurseRX
DL Nurse goesinto LW and
checks patient'sfinancial class and
Act Doc.
Pt any otherfinancial class thanself pay who has
not seen by afinancial counselor
(FC)?
Is the patient inthe DL?
DL Nurse informsFC office who willsend a FC to the
pt's bed side.
DL Nurse sends ptto FC office for aSTAT financial
analysis
Pt's financialclass otherthan privateinsurance orMedicaid?
Prescription couldbe filled here.
Pt choose tohave RX filled
here?
RX filled off-site atanother pharmacy.
DL Nurse tubesRX to OutpatientPharmacy (OP)
with otheridentifying
paperwork andlogs it on the DL
RX log.
A
A RX received byOP
OP logs RX'spertinent data,
included whetheror not RX is a
controlledsubstance.
Insurance doublechecked.
Appropriate forOP to fill?
OP processes perusual procedurefor DL RX and
logged out
OP calls DL andthen sends RX
back to thedischarge lounge
Are items toolarge to fit in
the tube?
Items tubedregular or secure
as needed.
OP tech calls DLNurse
Does DL Nursedecide to pickitems up fromPharmacy?
Transportation, oradmitting staff pick
up items
DL Nurse walks toOP to get items
and brings back toDL.
In the DLPrescriptions are
processed,logged, pt signs
sticker which is puton the DL
pharmacy log.
B
B
DL Nursedispenses
medicines andother items to pt.
DL Nurse collectsthe co-pay
Is the patient intheDL?
DL Nurse explainsthat pt needs toget the RX filled
elsewhere.
DL Nurse informsfloor nurse of
situation
floor Nurseexplains that ptneeds to get the
RX filledelsewhere.
RX filled off-site atanother pharmacy.
Cash, Credit, andchecks secure
tubed to OP to beprocessed
Is the patientstill on the
unit?
After a call to Unit,Pt, Family
member, or unitstaff bring co-payto DL and pick up
items. Cashier'sOffice Open?
OP tubes receiptback to DL
(happens twice forcredit cards)
Cash, credit, andchecks processedthrough cashier's
office.
Original receiptgoes to pt, copy
tubed to OP
RX transactioncomplete.
RX transactioncomplete.
No No
No
Yes
Yes
RX filled off-site atanother pharmacy.
No
Yes
No
Yes
No
Yes
Yes
No
Yes
No No
Yes
No
Yes
Yes
No
Nurse sendspatient and RX to
the DL
No
Yes
Nurse tubesRX straight to
DischargeLounge? (DL)
Yes
Rumor is we still fill OHMedicaid, but not KY or IN
Notes:1. Logs in DL maintained forlegal reasons.
2. What about Psych andTransplant?
3. After hours?
Current State:
All this to get a discharge RX filled –OUCH!

2/2/2006© 2005 The University Hospital , Cincinnati
35
Discharge Planning on Admission: Tools
All patients who have been discharged and:
…..Need to wait for transportation home
People who:
…..Have poor behavior/mental status – as decided by Nursing Supervisor…..Are with guards…..Are actively Incontinent- as decided by Nursing Supervisor…..Cannot transfer independently or cannot transfer with one
Mission: The Discharge Lounge will serve as a comfortable place where discharged patients may wait for transportation home. The Discharge Lounge, partnering with the TUH Financial
Counselors, will also facilitate the use of the Outpatient Pharmacy
The University Hospital Discharge Lounge
…..People who don't know where they get their prescriptions filled
People who are:
Which discharged patients can wait for their Outpatient Pharmacy prescriptions in the Discharge Lounge?
People who qualify to have their prescriptions filled by the Outpatient Pharmacy and:
Opens at 9:00 am
.….People who typically get their prescriptions filled at the Outpatient Pharmacy
…..The final eligibility determination is made by the Financial Counselor
…..Qualify to have their prescriptions filled by the Outpatient Pharmacy (See above qualifications)
Which discharged patients are potentially eligible to have their prescriptions filled by the Outpatient Pharmacy?
Which discharged patients should go to the Discharge Lounge?
Which discharged patients should NOT use the Discharge Lounge?
Vision: The Discharge Lounge will serve our discharged patients by addressing their needs one
individual at a time
Date :Unit:Pt Room # :
1. If no help is needed check "N/A".2. If help is needed check "Needs" and sign with initials.
4. Document your actions on the IPOC.5. Person who resolves the problem checks "Resolved" and signs with initials.
Needs (Initial) Referral Made Resolved (Initial) N/AExample: X AC X AC X ADS
Social Work1.Transportation home2. Safe/accessible place to go3. Something to wear home
Interpreter4. Needs interpreter
Home Health5. Home Health evaluation6. Has home oxygen
PT/OT7. PT/OT evaluation
Pharmacist8. Needs Fragmin education
Diabetes Educator9. Diabetic teaching
Unit and/or Flow Nurse10. Smoking cessation education11. Other teaching/needs**
Where are prescriptionstypically filled?
**Details & other comments:
Things this patient needs for a timely discharge
Discharge Needs Assessment (DNA)
Community Pharmacy Name:TUH Outpatient Pharmacy
3. If help will be provided by Social Work, Interpreter, Home Health, PT/OT, Unit-based Pharmacist, or the Diabetes Educator page a referral immediately. Then check "Referral Made".
CSD’s Role in The Discharge Lounge Process
DNA_______________
DNA_______________
Unit nurse checkschart for direction
as to where ptshould have RX
filled
Unit nurse handspatient the RX
Patient stops byFinancial
Counselor Officeon the way out
Script Script
Appropriate tofill RX at OP?
Patient has RXfilled elsewhere
No
Yes
Patient's socialneeds are
assessed (Willthey have a ridehome, et al) and
documented
Patient is admitted
Patient's typicalpharmaceutical
provider isidentified anddocumented
Patient's stayelapses
Transportation andpharmacy needs
evaluated and arepart of discharge
planning anddocumented in
chart
MD places thedischarge RX in
chart
A
A
If the patient goes to a community pharmacy the answer is NO.
If the patient goes to the Outpatient Pharmacy or doesn’t know, the answer is YES.
If the discharged patient needs to wait for a ride, send them to the discharge lounge regardless of medication needs.
Physicians should not hand prescriptions directly to patients.
Criteria
Discharge Upon Admission
Unit Processes

2/2/2006© 2005 The University Hospital , Cincinnati
36
Discharge Planning on Admission: Data
•Number of RX’s tubed to straight to the DL since implementation of new processes were significantly lower than number before implementation
Number of Discharge Prescriptions Tubed from Six South
13
402468
101214
October 2005 November 2005
Rolled Out 10/3/05Number of Discharge Prescriptions Tubed from
CSD
1
9
0
2
4
6
8
10
October 2005 November 2005
Rolled Out 10/24/05
Number of Discharge Prescriptions Tubed from Seven NorthWest
6
19
0
5
10
15
20
October 2005 November 2005
Rolled Out 11/2/05

2/2/2006© 2005 The University Hospital , Cincinnati
37
Discharge Planning on Admission: Data
Six South
(Pre= September 2005, Post = October and November 2005)
Data Consists of Monday - Friday Disposition Home Only
Two-Sample T-Test and CI: Time Converted, Status
Two-sample T for Time converted
Status N Mean StDev SE Mean
Post 198 14:42 0.118 0.0084
Pre 107 15:25 0.118 0.011
T-Test of difference = 0 (vs not =): T-Value = -2.11
P-Value = 0.036
DF = 216
43 Minutes Earlier!

2/2/2006© 2005 The University Hospital , Cincinnati
38
Discharge Planning on Admission: Data
38 Minutes Earlier!
Seven North West
(Pre= September and October 2005, Post =November 2005)
Data Consists of Monday - Friday Disposition Home Only
Two-Sample T-Test and CI: Time Converted, Status
Two-sample T for Time converted
Status N Mean StDev SE Mean
Post 142 14:34 0.117 0.0098
Pre 204 15:12 0.118 0.0083
T-Test of difference = 0 (vs not =): T-Value = -2.09
P-Value = 0.038
DF = 305

Accelerated Post Acute Discharge

2/2/2006© 2005 The University Hospital , Cincinnati
40
Accelerated Post Acute Transfer: Key Projects
Smoothed process for Drake referrals– Improved referral process and communication– In-serviced medical social work staff and rehab regarding admission criteria and
procedures
Improve referrals to interpreter services– Referrals for pre-scheduling have improved – now receive 80% advance notice on
requests for interpreter– Additional interpreters have been added to the department due to grant with the Health
Foundation of Greater Cincinnati
Extended Care Information Network - ECIN– Signed contract for software to allow electronic transfer of patient information between
long term care facilities, homecare agencies, community resources and TUH.– Implementation scheduled for March 1st.

2/2/2006© 2005 The University Hospital , Cincinnati
41
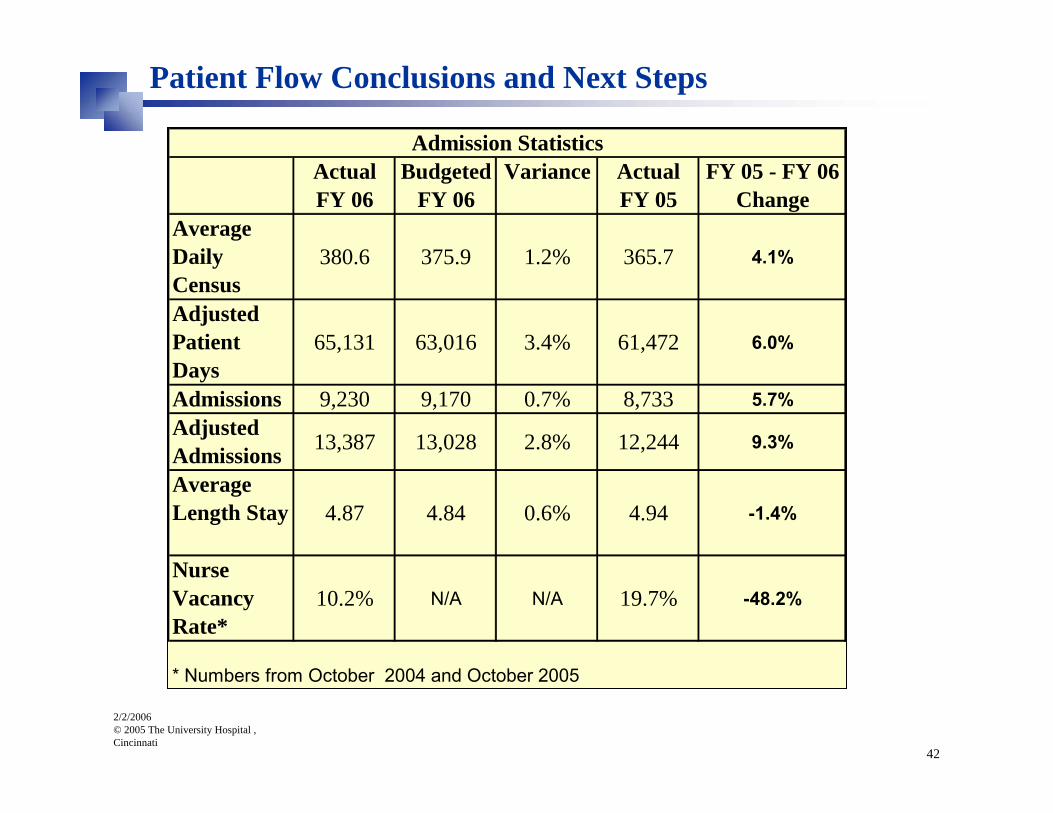
Patient Flow Conclusions and Next Steps
Hard to feel the impactHolding steady during a time of increased volume
2/2/2006© 2005 The University Hospital , Cincinnati
42
Patient Flow Conclusions and Next Steps
ActualFY 06
Budgeted FY 06
Variance ActualFY 05
FY 05 - FY 06Change
Average Daily Census
380.6 375.9 1.2% 365.7 4.1%
Adjusted Patient Days
65,131 63,016 3.4% 61,472 6.0%
Admissions 9,230 9,170 0.7% 8,733 5.7%Adjusted Admissions 13,387 13,028 2.8% 12,244 9.3%
Average Length Stay 4.87 4.84 0.6% 4.94 -1.4%
Nurse Vacancy Rate*
10.2% N/A N/A 19.7% -48.2%
* Numbers from October 2004 and October 2005
Admission Statistics

2/2/2006© 2005 The University Hospital , Cincinnati
43
Patient Flow Conclusions and Next Steps
Capacity11/1/2005
Medicine Svcs 7NW
32 35 3 NA NA 3
Medicine Svcs MAEU
0 6 6 NA NA 6
Surgical Svcs5 STSurgical SvcsSICUTotal 17 23
11/14/2005 4
18 24 6 28 2/6/2005 10
16 18 2 20
Increased Bed CapacityUnit Capacity
7/1/2005Net Bed Capacity Gain To
Date
Planned Capacity
Date of Planned Increase
Net Bed Capacity
Gain Future
Gained17
Beds!
Gained17
Beds!

2/2/2006© 2005 The University Hospital , Cincinnati
44
Beds Blocked/ Patient Holds Tracking
Ongoing data collection to monitor the number of patients waiting for inpatient beds (“holds”) as well as the number of inpatient beds being blocked

2/2/2006© 2005 The University Hospital , Cincinnati
45
Patient Holds TrackingCensus
356358360362364366368370372374
CY 2004 November 2005
Admits
70717273747576777879
CY 2004 November 2005
Total Holds
0
2
4
6
8
10
12
CY 2004 November 2005
ED Holds
012345678
CY 2004 November 2005
Diversion Hours
0
0.5
1
1.5
2
2.5
CY 2004 November 2005
372 78
2 2
0