Embed Size (px)
Citation preview

i
iTotalwhyCLINICAL RATIONALE FOR A PATIENT-SPECIFIC CRUCIATE-RETAINING KNEE REPLACEMENT SYSTEM
®
?

1
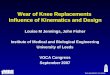
1 in 5 patients are
not satisfied with the results of their total knee replacement.1
iTotal G2CRUCIATE-RETAINING
Patient dissatisfaction50%
40%
30%
10%
20%
0%
Ander
son (
1996
) 2
% p
atie
nts
not
sat
isfie
d
clinical reference
11%
Heck (
1998
) 3
12%
Wyld
e (20
07) 7
15%
Hawke
r (199
8) 4
15%
Bour
ne (2
010)
1
19%
Noble
(2006
) 6
25%
Bulle
ns (2
001) 5
27%
Suda
(201
0) 8
39%

2
Over 5 million people are living with total knee replacements.9 Therefore, millions are likely dissatisfied with their knee replacement. This number continues to grow as over 1.2 million knee replacement procedures are done every year worldwide.10
Leading Causes of Patient Dissatisfaction
Residual Pain
• Fit: Data suggests that 27% of clinically significant knee pain is attributable to femoral implant overhang.11
• Rotation: Internal rotational errors, particularly of the tibial component, are a major cause of pain and functional deficit after TKA.12
Functional Limitations
• Poor Function: Patients who have a TKR experience substantial functional impairment compared to their peers without a TKR.13
• Unnatural Feel: 46% of dissatisfied patients state their knee does not feel normal. Even amongst satisfied TKR patients, 20% state their knee does not feel normal.6
Early Implant Failure
• 50% of early revision TKA are related to instability, malalignment and failure of fixation.14
iTotal Off-the-shelf

3
iTotal G2CRUCIATE-RETAINING
Residual pain: Improper fit
Off-the-shelf total knees force compromises between sizing and coverage. Variations in anatomy make it virtually impossible for off-the-shelf designs to fit the femur.
• In a series of 437 TKR femoral components, 68% of women and 40% of men had overhang of * 3mm. Overhang was correlated with a 1.9x increase in the risk of pain.11
• Impingement of the femoral component can cause a snapping of the popliteus tendon which may be painful or disconcerting to the patient.15
Implant overhang causes residual pain and dissatisfaction
increase in the risk of pain with overhang12
1.9x
iTotal G2 is uniquely qualified to address the wide variation in patient anatomy that lead to overhang and undercoverage. The individualized design is so precise that it virtually eliminates sizing compromises common with off-the-shelf knee replacements.
The iTotal G2 Solution: Individualized Fit
Popliteus tendon relief
Precise femoral and tibial fit

4
Rotational errors
• Proper tibial rotation based on pre-operative CT scan.
• Patient-specific shape matched to profile of resected proximal tibia.
The iTotal G2 Solution: Pre-navigated tibial rotation
Anatomic tibialaxis alignment
Patient-specific tibial profile
• Among painful knees, 44% were found to have significant rotational errors of the tibial tray.16
• Off-the-shelf tibial component designs maximize coverage at the expense of proper rotational alignment. One study of 120 tibial components found that only 30% were aligned within ±5° of proper rotation.17
• In a study of anterior knee pain, patients with excess internal component rotation were more than 5x as likely to experience knee pain versus a control group.18
Component malrotation is a leading cause of residual pain
to experience knee pain if excess internal component rotation is present18
5x as likely
There is a direct correlation between combined internal component rotation with the severity of patellofemoral complications.12
6
5
4
3
1
2
deg
ree
of r
otat
ion
7
8
9
Lateral Track Subluxation Dislocation Prosthesis Failure
0

5
• According to published data, 2 to 3 times as many patients with TKA report some degree of difficulty with activities relative to a similar control group.13
• Off-the-shelf total knee implants, including single radius designs, have been shown to alter kinematics.19
Unnatural feel and poor kinematics lead to patient dissatisfaction
iTotal G2CRUCIATE-RETAINING
Poor kinematics and mid-flexion instability
• Studies of early implant failures have shown that instability accounts for as much as 27% of revision surgeries.20
• Joint line movement of over 5mm has been shown to result in mid-flexion instability.21
Instability leads to patient dissatisfaction
increase in the risk of implant failure with ligament instability22
3.7x
Functional limitations:
In one study, dissatisfied patients reported that their knee did not feel normal at
more than twice the rate of satisfied patients.6
% r
epor
ting
no
diffi
cult
y
100%
80%
60%
20%
40%
turning/cutting golf dancing racquet sports0%
TKR subjects Age-matched control subjects
Functional limitations13

6
Poor kinematics and mid-flexion instability
• iTotal more closely approximated each patient’s normal femoral rollback throughout ROM, an important feature of healthy kinematics.
• iTotal resulted in varus-valgus laxity, as measured by adduction/ abduction, that was significantly closer to the normal knee.23
In a study comparing iTotal G2 to an off-the-shelf TKR, iTotal restored natural kinematics:
iTotal G2 is intended to restore each patient’s natural articulating geometry by:
• Using the patient’s natural medial, lateral and patellofemoral J-curves, corrected for deformity, as the basis for femoral implant design.
• Facilitating proper balancing of offset femur and joint line with femur-matched offset polys.
• Reducing lateral constraint to facilitate rollback.
The iTotal G2 Solution: Patient-specific J-curves
Patient’s natural J-curves
Dual inserts respect each patient’s joint line
25
20
15
5
0
Fem
oral
Rol
lba
ck (
mm
)
Flexion (deg)
0 10 20 30 40 50 60 70 80 90 100 110 120
10
Normal Off-the-shelf
Normal iTotal
25
20
15
5
0
Fem
oral
Rol
lba
ck (
mm
)
Flexion (deg)
0 10 20 30 40 50 60 70 80 90 100 110 120
10
Average femoral rollback for iTotal G2 and off-the-shelf TKR
iTotal G2 Off-the-shelf
500
400
300
200
600
100
0
Cu
mu
lati
ve D
ata
Su
m 700
800
900
Varus/valgus laxity, post implantation
Active Adduction
p = 0.036*
Passive Adduction Abduction
p = 0.016*

7
iTotal G2 is intended to achieve neutral mechanical alignment:
• iFit® image-to-implant™ technology virtually aligns to mechanical axis using anatomic landmarks (center of hip, femur, tibia and ankle).
• Patient imaging data is used to create a 3D representation of the patient’s anatomy to design accurate patient-specific implants and iJig® instrumentation with built-in neutral mechanical alignment.
The iTotal G2 Solution: Mechanical axis alignment
• Studies have shown that varus tibial malalignment (<90°) was associated with a 10.6x greater risk of failure, while >8° valgus femoral malalignment was associated with a 5.1x greater risk of failure.24
Cause of early implant failure: Poor overall alignment
iTotal G2CRUCIATE-RETAINING
Early implant failure: Poor alignment
Failure rate according to overall alignment in degrees24
3.0%
2.5%
2.0%
1.5%
.5%
1.0%
0.0%
failu
re r
ate
post operative alignment
3.5%9.1
-2 and below
1.8
-1-0
1.0
1-2
0.7
3-4
0.9
5
0.4
6-7
1.5
8-9
1.2
10 and above
Varus n=1044alignment below 2.5°
Fail rate=1.5%p=.0081
Neutral n=4310alignment 2.5° thru 7.4°
Fail rate=0.6%p<.0001
Valgus n=716alignment above 7.4°
Fail rate=1.4%p=.0053

8
• Due to its broad coronal radius, iTotal G2 allows for high contact area with low constraint.
• The coronal radius on the femur interfaces with the poly throughout the range of motion.
The iTotal G2 Solution: Engineered for low contact stress
• Significant polyethylene wear was observed in 25% of revision surgeries, making it the most prevalent mechanism of implant failure.14
Cause of implant failure: Polyethylene wear
Polyethylene wear
Overall causes of revision surgery14 Percentage
Polyethylene wear
Loosening
Instability
Infection
Arthrofibrosis
Malalignment or malpositioned
25.0
24.1
21.2
17.5
14.6
11.8
Contact area (mm2) at 0°, 60° and 90° of flexion
iTotal G225 Sigma26 (fixed bearing)
400
300
200
100
192 186270
116 123
0
0º Flexion 60º Flexion 90º Flexion
cont
act a
rea
(mm
2) 338
270

9
So, whyiTotal?
Designed with features to address the leading causes of patient dissatisfaction, iTotal G2 is the only individualized total knee system on the market today.
FIT • Individualized fit that virtually eliminates overhang and
sizing compromises
• Designed to follow the contour of each patient’s anatomy
• Tibial tray designed for maximized coverage and proper rotational alignment
SHAPE • Individualized medial, lateral and patellofemoral J-curves with
matching offset poly inserts
• Designed for optimal bone preservation
• Wear optimized by matching femur and tibial inserts for maximized surface contact area
SIMPLE SURGICAL TECHNIQUE • Reduced number of intra-operative decisions such as implant
sizing and rotation
• Mechanical and rotational alignment are pre-determined in the individualized iJig instrumentation
• iView surgical planning images for proper iJig placement and detailed resection values
OR EFFICIENCIES • Simplified set-up and tear down
• Minimal instrumentation required
• Disposable system delivered in a single pre-sterilized box
• Reduced sterilization and inventory costs
iTotal G2CRUCIATE-RETAINING

10
1. Bourne, et al; Patient Satisfaction after Total Knee Arthroplasty. Who is Satisfied and Who is Not? Clinical Orthopaedics and Related Research; 2010, 468: 57-63
2. Anderson, et al; Functional Outcome and Patient Satisfaction in Total Knee Patients Over the Age of 75. Journal of Arthroplasty; 1996, 11 # 7: 831-840
3. Heck, et al; Patient Outcomes After Knee Replacement. Clinical Orthopaedics and Related Research; 1998, 356: 93-110
4. Hawker, et al; Health-Related Quality of Life after Knee Replacement. Journal of Bone and Joint Surgery; 1998, 80-A #2: 163-173
5. Bullens, et al; Patient Satisfaction After Total Knee Arthroplasty. Journal of Arthroplasty; 2001, 16 #6: 740-747
6. Noble, et al; Patient Expectations Affect Satisfaction with Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 2006, 452: 35-43
7. Wylde, et al; Total knee replacement: Is it really an effective procedure for all? The Knee; 2007, 14: 417-423
8. Suda, et al; Are Patients’ Expectations of Hip and Knee Arthroplasty Fulfilled? A Prospective Study of 130 Patients. Orthopedics; 2010, 33 #2: 76-80
9. Thornhill, et al; How Many Americans are Currently Living with Total Knee Replacements? Abstract from AAOS Annual Meeting: 2012
10. Millennium Research Group; US/EU Markets for Large-Joint Reconstructive Implants 2007
11. Mahoney, et al; Overhang of the Femoral Component in Total Knee Arthroplasty: Risk Factors and Clinical Consequences. The Journal of Bone and Joint Surgery; 2010, 92: 1115-1121
12. Berger, et al; Malrotation Causing Patellofemoral Complications after Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 1998, 356: 144-153
13. Noble, et al; Does Total Knee Replacement Restore Normal Knee Function? Clinical Orthopaedics and Related Research; 2005, 431: 157-165
14. Sharkey, et al; Why Are Total Knee Arthroplasties Failing Today? Clinical Orthopaedics and Related Research; 2002, 404: 7-13
references
15. Barnes, et al; Popliteus Tendon Dysfunction Following Total Knee Arthroplasty. The Journal of Arthroplasty; 1995, 10: 543-545
16. Nicoll, et al; Internal Rotational Error of the Tibial Component is a Major Cause of Pain after Total Knee Replacement. The Journal of Bone and Joint Surgery; 2010, 92: 1238-1244
17. Martin, et al; Optimizing Tibial Coverage is Detrimental to Proper Rotational Alignment. Poster from AAHKS Annual Meeting: 2012
18. Barrack, et al; Component Rotation and Anterior Knee Pain after Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 2001, 392: 46-55
19. Bull, et al; Changes in Knee Kinematics Reflect the Articular Geometry after Arthroplasty. Clinical Orthopaedics and Related Research; 2008, 466: 2491-2499
20. Fehring, et al; Early Failures in Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 2001, 392: 315-318
21. Whiteside, et al; The Influence of Joint Line Position on Knee Stability After Condylar Knee Arthroplasty. Clinical Orthopaedics and Related Research; 1990, 259: 146-156
22. Fang, et al; Coronal Alignment in Post-operative TKA: Just how important is it? Journal of Arthroplasty; 2009, 24 #2: 39-43
23. Patil, et al; Patient-Specific Implants and Cutting Guides Better Approximate Natural Kinematics than Standard Total Knee Arthroplasty. ORS Annual Meeting 2013, Vol.38. Abstract # 0965
24. Ritter, et al; The Effect of Alignment and BMI on Failure of Total Knee Replacement. Journal of Bone and Joint Surgery; 2011, 93: 1588-1596
25. Data on file
26. DePuy Orthopedics, Inc. marketing literature. Data for Sigma fixed bearing is at 15° flexion as 0° flexion was not reported.

ii
ConforMIS, Inc. 28 Crosby Dr., Bedford, MA 01730 Phone: 781.345.9001 | Fax: 781.345.0147
www.conformis.com
Authorized Representative: Medical Device Safety Service, GMBH • Schiffgraben 41, 30175 Hannover, Germany P: +49 (511) 6262.8630 • F: +49 (511) 6262.86333
Copyright © by ConforMIS, Inc. All rights reserved. iDuo and ConforMIS are registered trademarks of ConforMIS.
CAUTION: USA federal law restricts this device to sale by or on the order of a physician. The ConforMIS Cruciate Retaining Total Knee Replacement System (iTotal G2) is intended for use only by fully trained physicians. Prior to use of a ConforMIS device, please review the instructions for use and surgical technique for a complete listing of indications, contraindications, warnings, precautions, and directions for use. MK-02797-AB 7/130086




















![Knee Osteoarthritis: A Review of Pathogenesis and State-Of ......with knee and hip joint replacements as the majority of that cost [9,12]. Furthermore, after low-back Furthermore,](https://img.pdfslide.net/doc/110x75/6086506fb492ce60b97ff111/knee-osteoarthritis-a-review-of-pathogenesis-and-state-of-with-knee-and.jpg)



![Hip and Knee Replacements · 2 | [footer text here] 3 Outline The Basics of Hip and Knee Replacement What’s changed over the last decade - Longevity - Pain Management - Hospital](https://img.pdfslide.net/doc/110x75/603e5ddc1246d57e120683de/hip-and-knee-2-footer-text-here-3-outline-the-basics-of-hip-and-knee-replacement.jpg)