Embed Size (px)
Citation preview
Why we need a practicaldisaster epidemiology
Why we need a practicaldisaster epidemiology
David AlexanderUniversity College London

Analysis
• registered• archived• forgotten• ignored
Vulnerabilitymaintained-
• utilised• adopted• learned
Disasterriskreduced
+
Lesson
s
Pastevent
s
The process ofdisaster riskreduction(DRR)
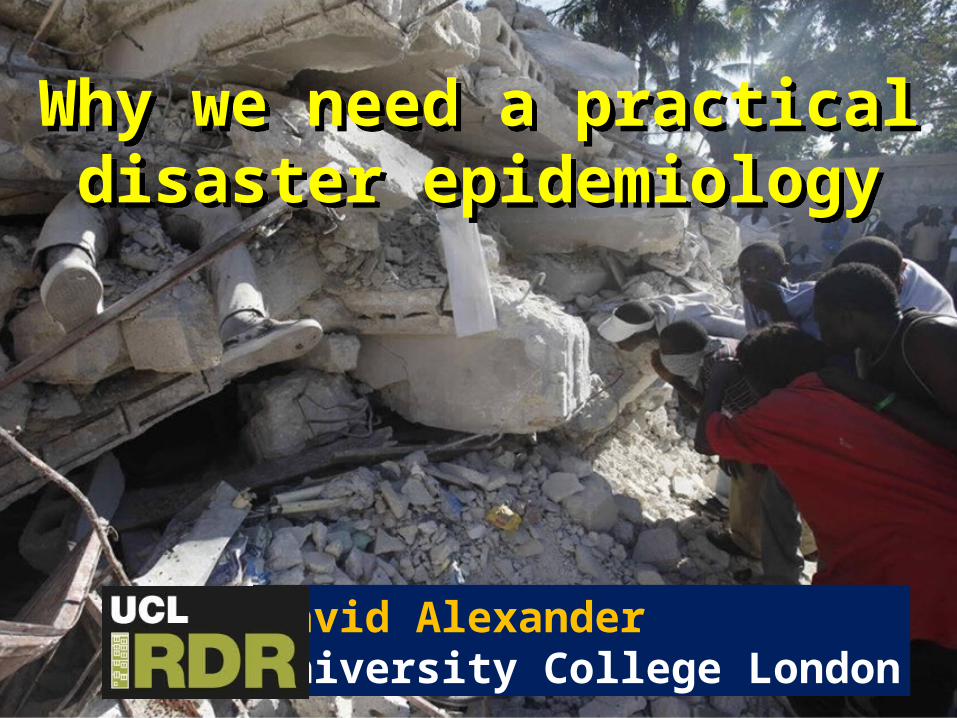
Learningprocesses
Improved
safety
Lessonlearned
Change andinnovation
Experienceand theory
Recognition andcomprehension
Lesson tobe
learned
• Unexpected event
• New circumstance
• Error• New
practice
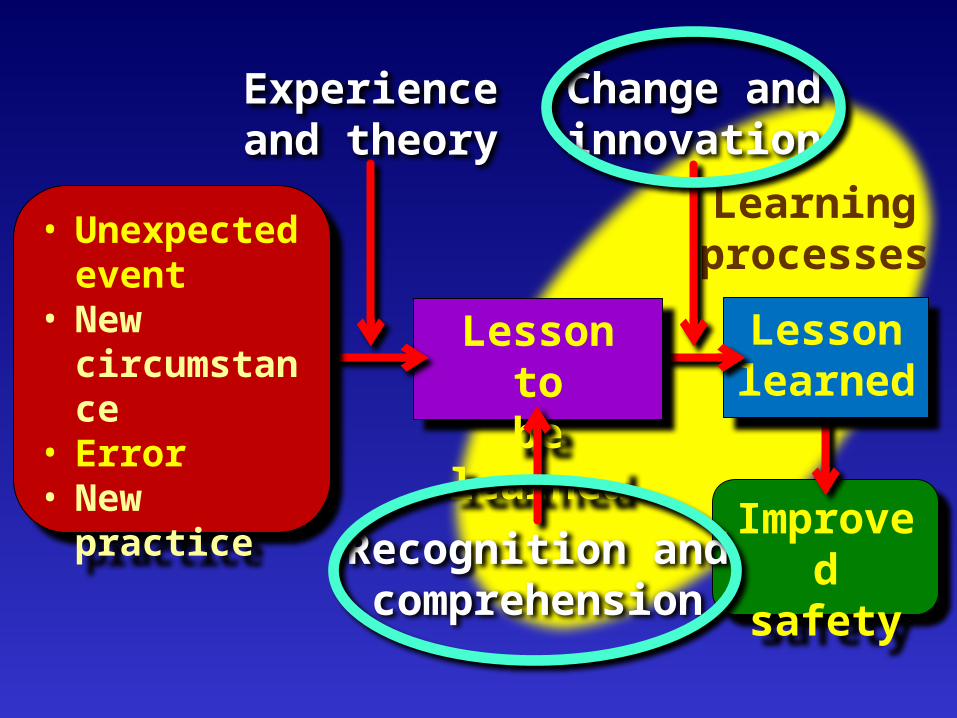
Self-protectivebehaviour
Hospitalmass-casualty
response
Urban searchand rescue
(USAR)
A practical disaster epidemiology
Focus Potential benefit to...
How, whereand why
people died;who they were;
how theyreacted to
the disaster
Sendai Framework for DisasterRisk Reduction, para. 24(1), 33(n)Promote the collection, analysis,
management and use of relevant dataand practical information. Ensure its
dissemination...
Establish a mechanism of case registryand a database of mortality caused by
disaster in order to improve theprevention of morbidity and mortality;
Physical injury (physical trauma):-• short-term condition• long-term injury or disease• fatal injury• premature death.
Psychological impairment:-• depression• anxiety• post-traumatic stress (including long-term).
Disaster injury epidemiology
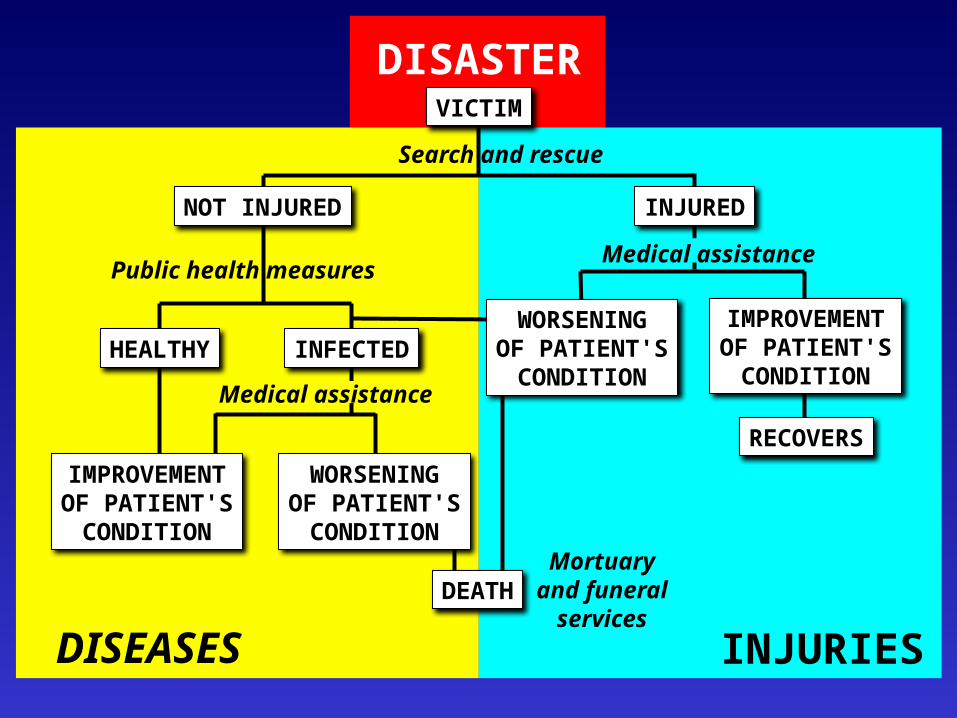
DISASTERVICTIM
NOT INJURED INJURED
HEALTHY INFECTEDWORSENINGOF PATIENT'SCONDITION
IMPROVEMENTOF PATIENT'SCONDITION
RECOVERS
IMPROVEMENTOF PATIENT'SCONDITION
DISEASES INJURIES
Public health measures
Search and rescue
Mortuaryand funeral
services
WORSENINGOF PATIENT'SCONDITION
DEATH
Medical assistance
Medical assistance

• failure to collect data [systematically]
• post-event data collection is not reliable enough
• few epidemiological researchers are specialists in this field
• most research consists of isolated clinical studies
• patient confidentiality issues.
Constraints on progress
Earthquakes as archetypicalsudden-impact disasters: toward
an evidence-based approachto earthquake epidemiology

After more than 30 years of study,
the causes and patterns ofinjury are still poorly
understood.

Magnitude Location Date Deaths Injuries D/I
6.7 Northridge, California
17.01.1994 57-72 8,700
0.0007
7.3 Kobe, Japan17.01.199
5 6,434 14,678 0.44
7.4-7.5 İzmit, Turkey17.08.199
917,127-45,000 43,959 0.39
9.1-9.3(*tsuna
mi)
Indonesia, Indian Ocean*
26.12.2004
184,167-
276,025125,000 2.21
7.6 Kashmir, Pakistan
08.10.2005 74,702 106,280 0.70
7.9 Wenchuan, China
12.05.2008 69,180 374,176 0.19
7.9 Padang, Indonesia
30.09.2009 1,115 2,902 0.38
7.0 Haiti12.01.201
046,000-316,000
uncounted --
6.3 Christchurch, New Zealand
11.02.2011 185 6,800 0.03
9.0 Eastern Japan*
11.03.2011 19,009 26,992 0.70
• no standard definitions (regarding incidence and prevalence)
• lack of comparability and compatibility of existing data
• regularities exist but are poorly known
• to what extent is injury predictable?.
What is an earthquake-related injury?
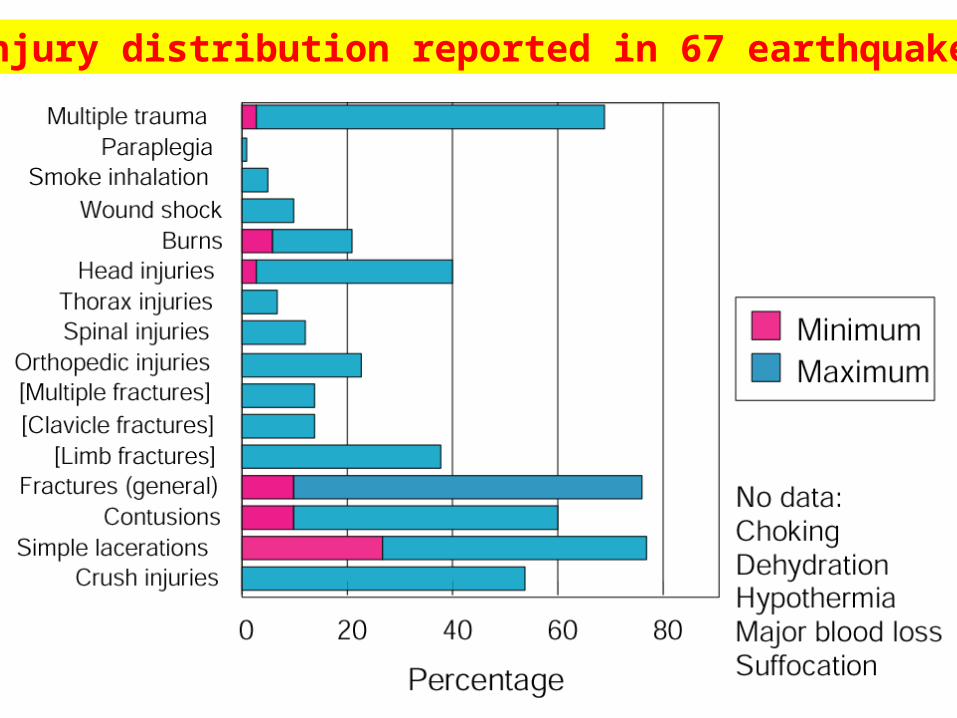
Injury distribution reported in 67 earthquakes
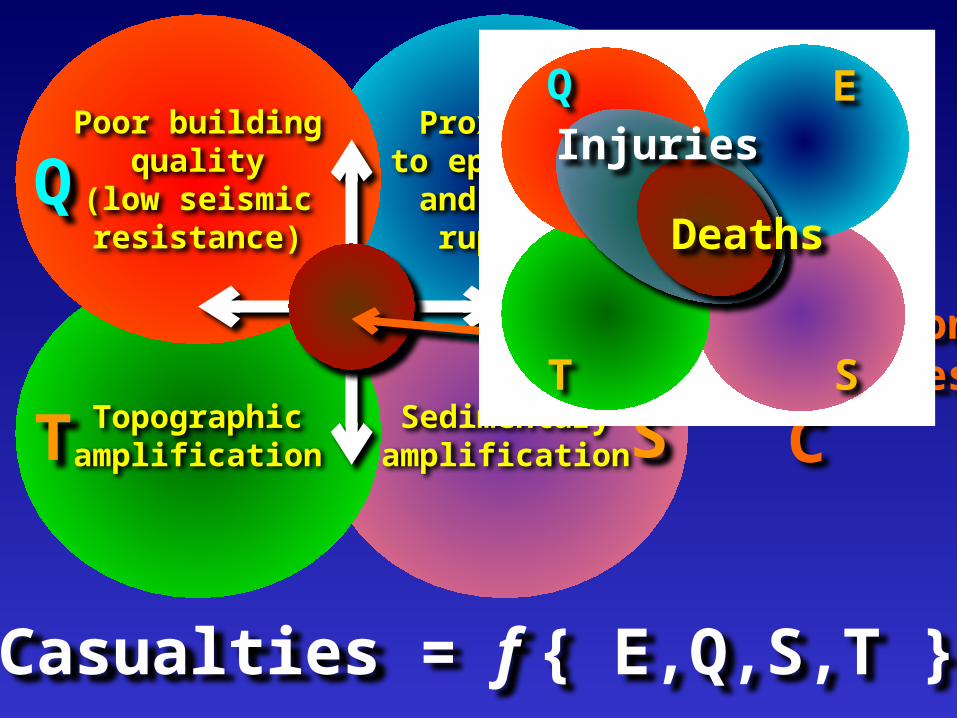
Poor buildingquality
(low seismicresistance)
Proximityto epicentre
and faultrupture
Topographicamplification
Sedimentaryamplification
Q E
T S
Concentrationof casualties
C
Casualties = f { E,Q,S,T }
Deaths
InjuriesQ E
T S
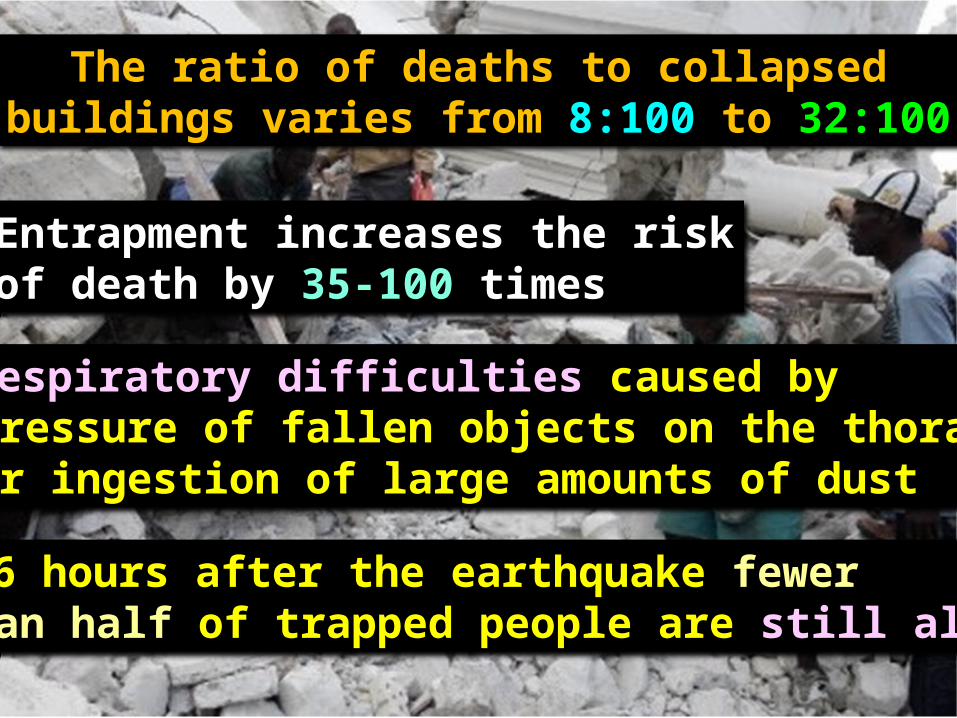
The ratio of deaths to collapsedbuildings varies from 8:100 to 32:100
Entrapment increases the riskof death by 35-100 times
• respiratory difficulties caused by pressure of fallen objects on the thorax or ingestion of large amounts of dust
• 2-6 hours after the earthquake fewer than half of trapped people are still alive.
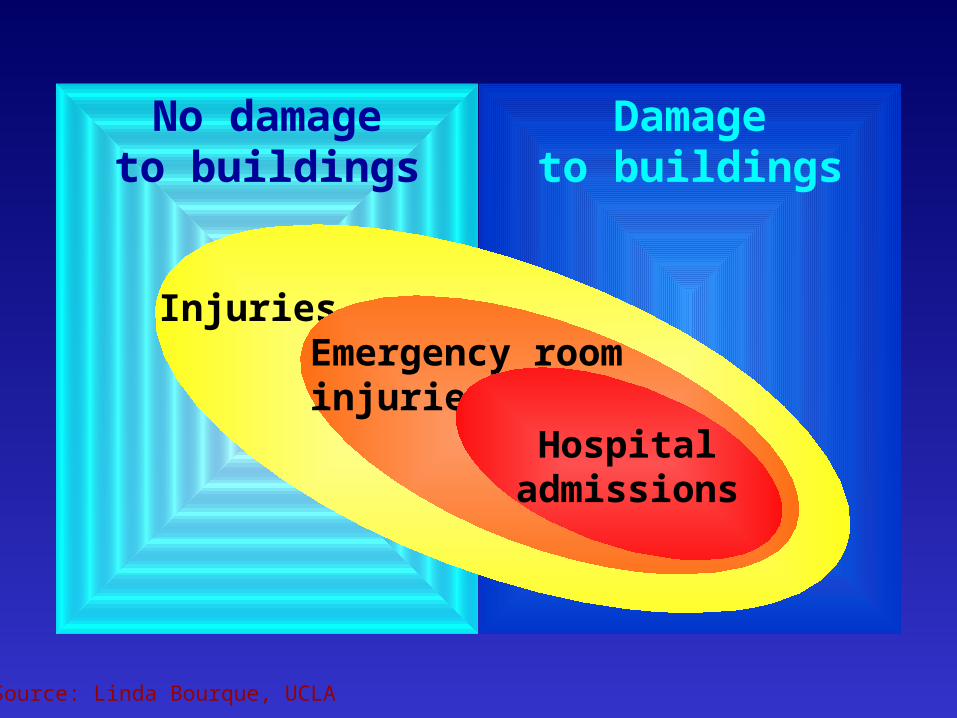
No damageto buildings
Damageto buildings
InjuriesEmergency roominjuries
Hospitaladmissions
Source: Linda Bourque, UCLA

Axiom: building collapse(structural failure) is the main
source of damage in earthquakes
What impact does self-protectivebehaviour have on injury rates? .

Behaviour
Vulnerability of thebuilt environment
Interaction
Force majeure:the earthquake
Perception
Knowledge, habit,custom and training
Active behaviour:• journey to and from work• recreational activities, etc.• family life at home
Active behaviour:• journey to and from work• recreational activities, etc.• family life at home
Passive behaviour:• sleeping at night• role, efficiency and rapidity of search and rescue and medical assistance after the earthquake.
Passive behaviour:• sleeping at night• role, efficiency and rapidity of search and rescue and medical assistance after the earthquake.
Behavioural influence on casualties
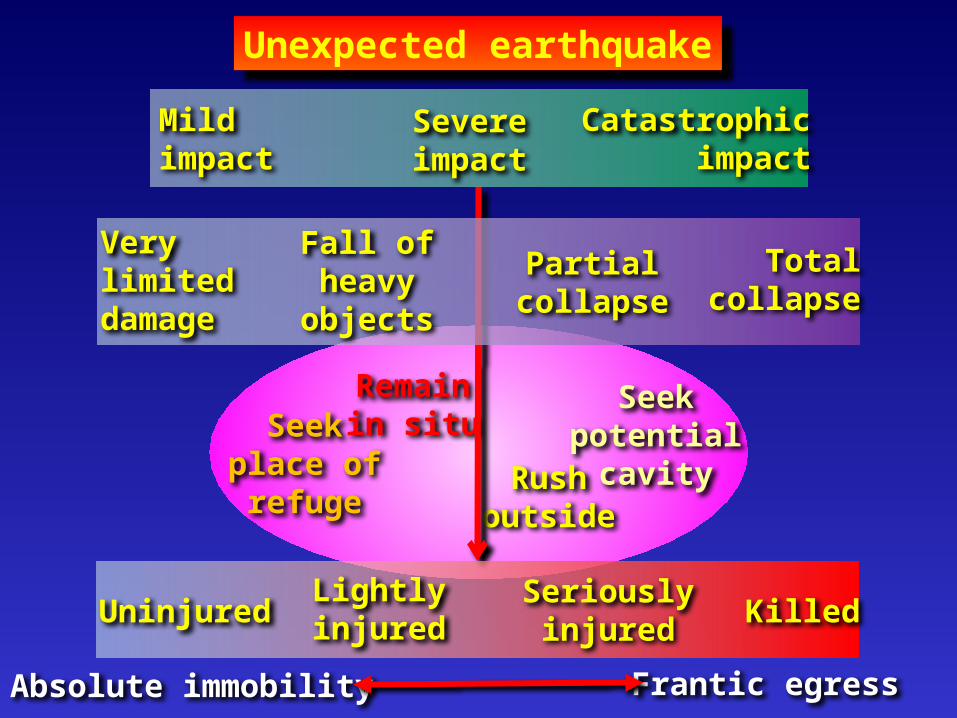
Seekplace ofrefuge
Remainin situ
Seekpotential
cavityRushoutside
Unexpected earthquake
Mildimpact
Severeimpact
Catastrophicimpact
Verylimiteddamage
Fall ofheavy
objects
Partialcollapse
Totalcollapse
Absolute immobility Frantic egress
UninjuredLightlyinjured
Seriouslyinjured Killed
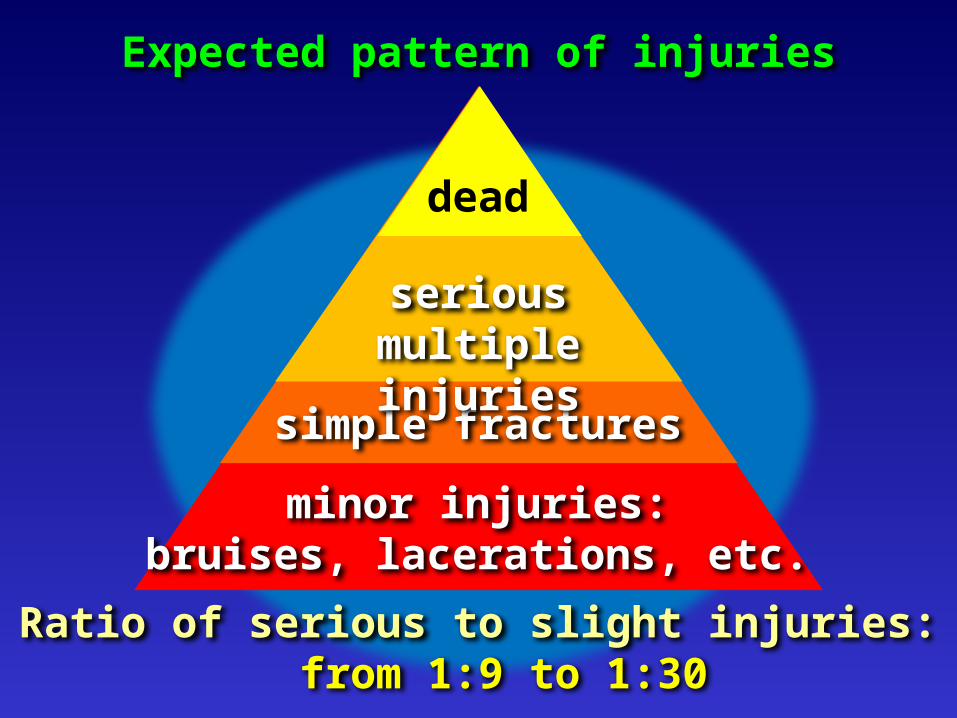
Expected pattern of injuries
minor injuries:bruises, lacerations, etc.
simple fractures
seriousmultiple injuries
Ratio of serious to slight injuries: from 1:9 to 1:30
dead

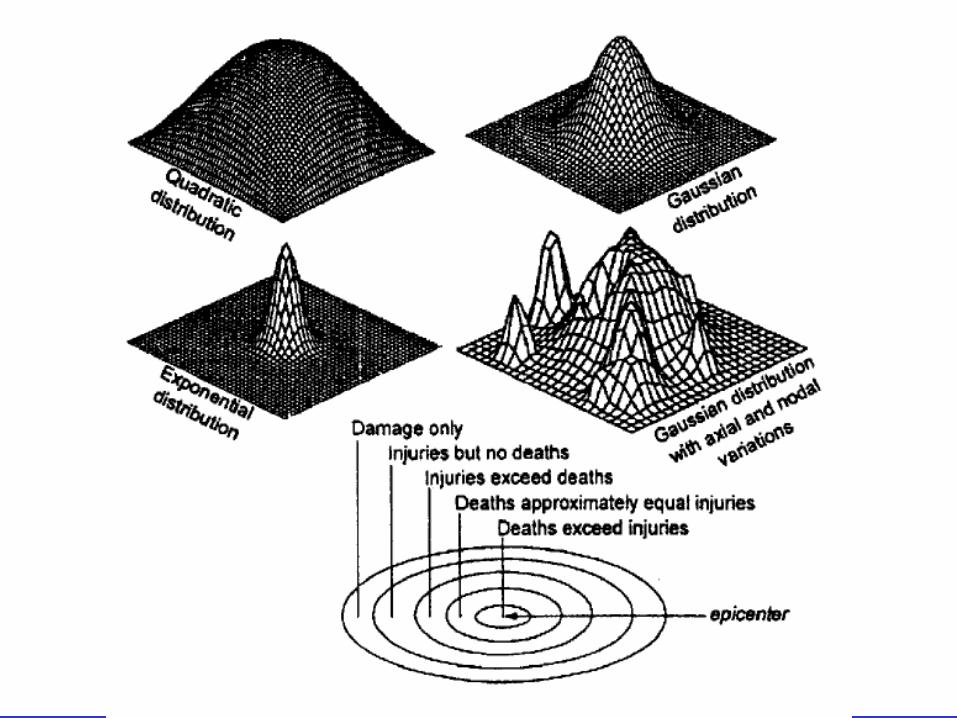
Spatial model of deathsand injuries in earthquakes
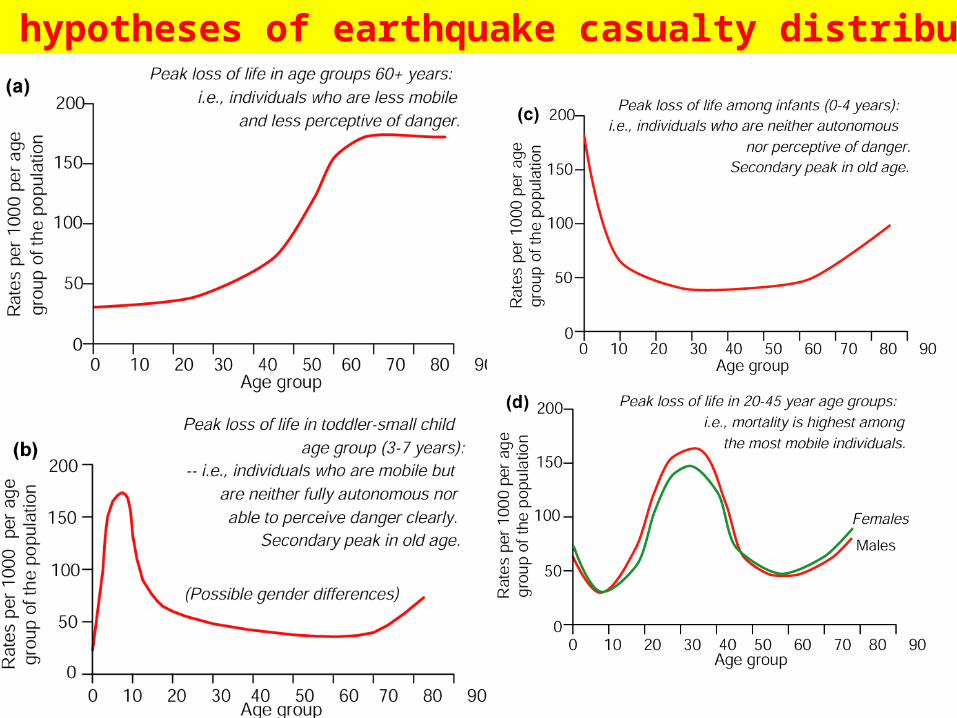
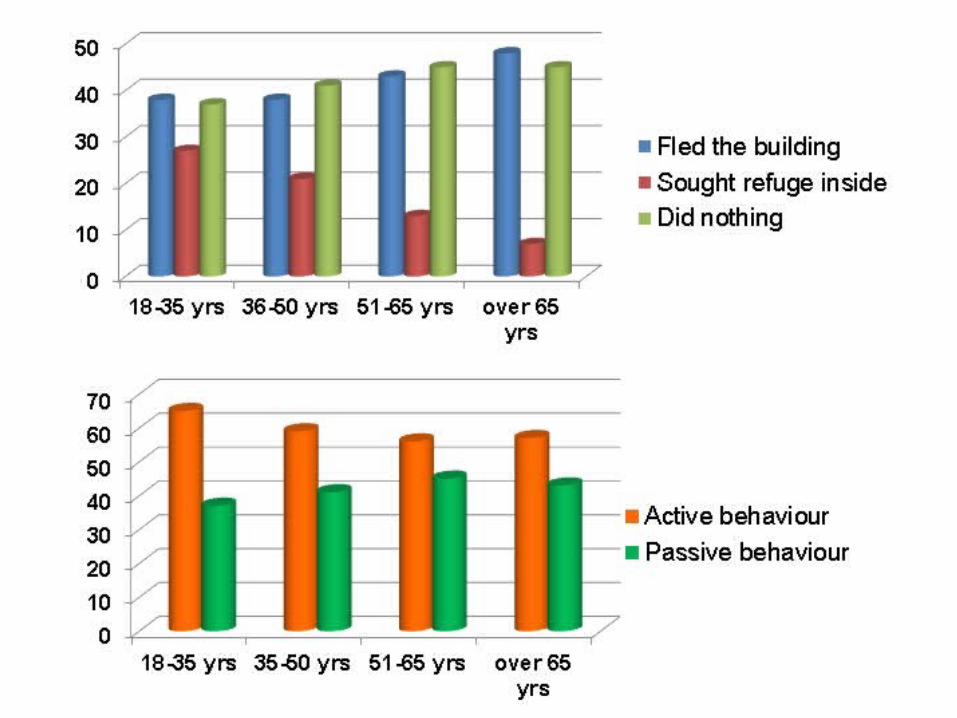
Four hypotheses of earthquake casualty distribution
• differences in exposure to risk, perception and behaviour
• social constraints on self-protection
• higher psychological burden
• demographic preponderance in old age.
Why are women and girls moreat risk than men and boys?
• ability to prepare for incidence of particular injuries
• need for mass-fatality planning
• social benefits of behavioural modification to avoid injury
• bolster arguments for investing in stronger buildings.
Better death and injury data
Dead bodies do not cause epidemics.
Hasty mass burial is not a goodresponse to a mass fatality situation
This simple observation has taken decadesto establish and is still not known
or accepted by all decision-makers.

Thank you foryour
attention!
david.alexander@ucl.ac.ukemergency-planning.blogspot.comwww.slideshare.net/dealexander