Embed Size (px)
Citation preview
Centre for Endocrinology,
Diabetes and Metabolism
Endocrinology in the time of COVID-19
Management of Adrenal Insufficiency
Wiebke Arlt
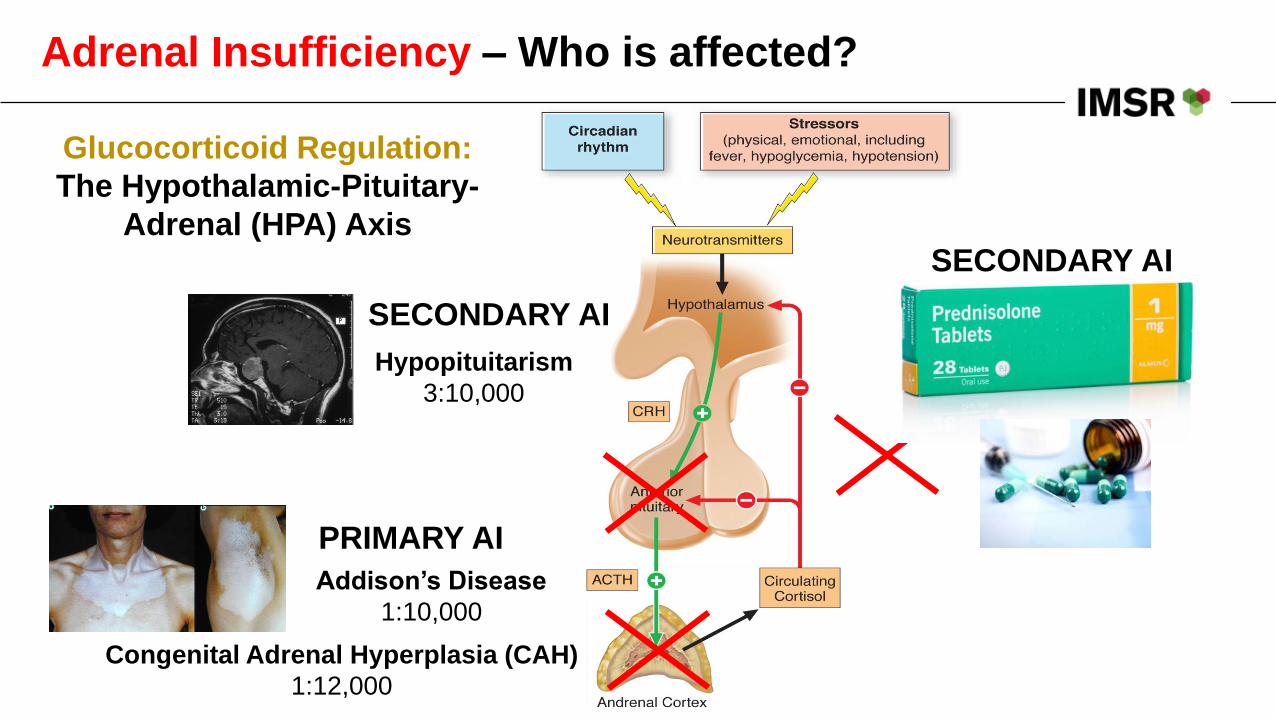
Adrenal Insufficiency – Who is affected?
Glucocorticoid Regulation:
The Hypothalamic-Pituitary-
Adrenal (HPA) Axis
Addison’s Disease
1:10,000
Hypopituitarism
3:10,000
Congenital Adrenal Hyperplasia (CAH)
1:12,000
PRIMARY AI
SECONDARY AI
SECONDARY AI
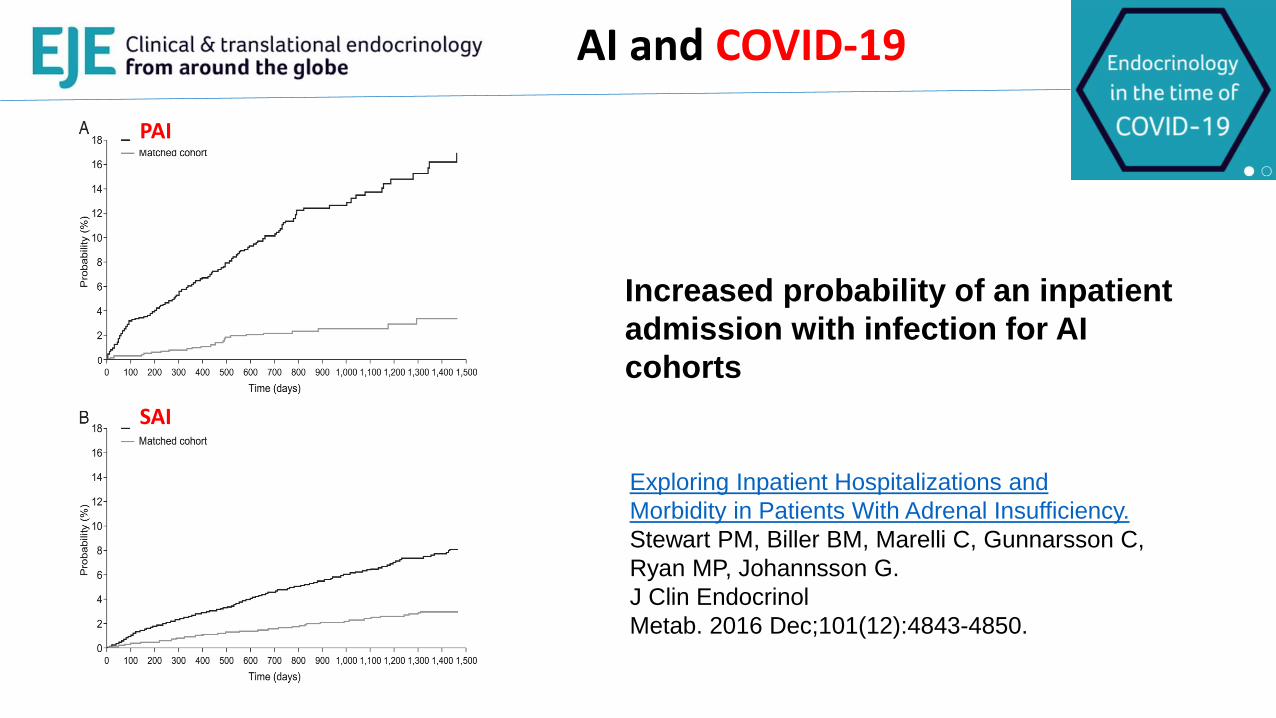
AI and COVID-19
Increased probability of an inpatient
admission with infection for AI
cohorts
Exploring Inpatient Hospitalizations and
Morbidity in Patients With Adrenal Insufficiency.
Stewart PM, Biller BM, Marelli C, Gunnarsson C,
Ryan MP, Johannsson G.
J Clin Endocrinol
Metab. 2016 Dec;101(12):4843-4850.
PAI
SAI
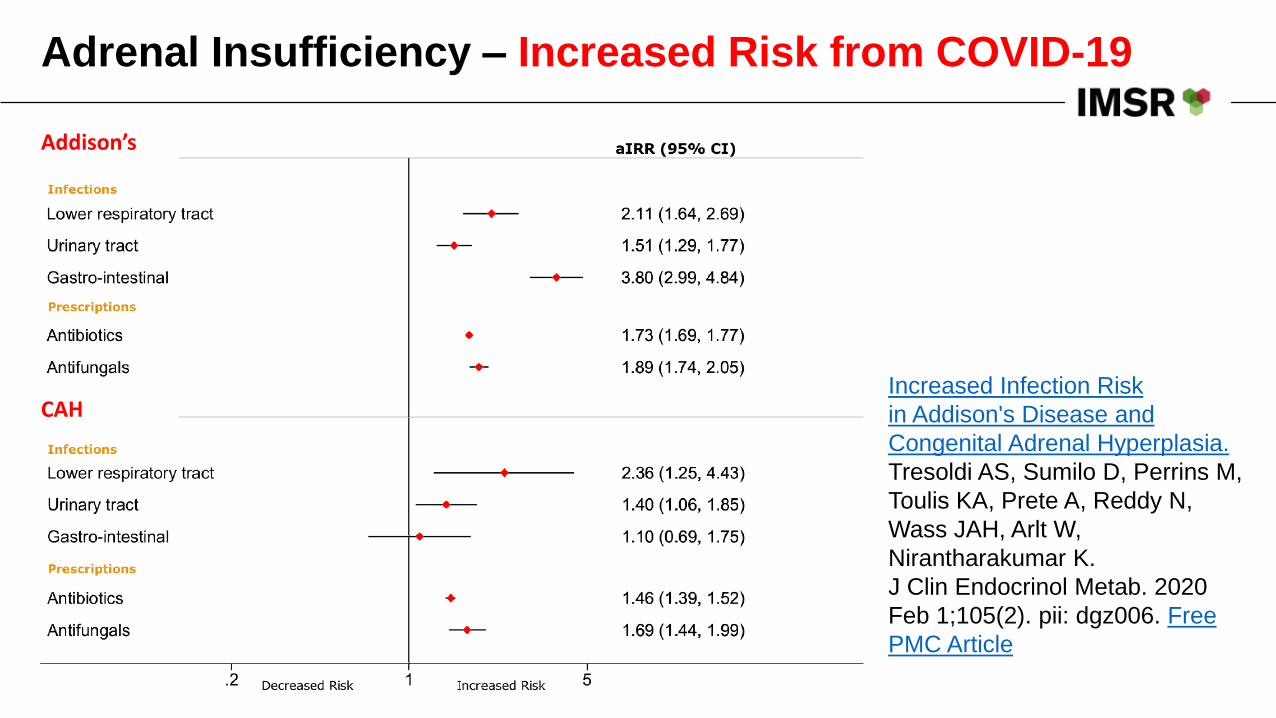
Adrenal Insufficiency – Increased Risk from COVID-19
Increased Infection Risk
in Addison's Disease and
Congenital Adrenal Hyperplasia.
Tresoldi AS, Sumilo D, Perrins M,
Toulis KA, Prete A, Reddy N,
Wass JAH, Arlt W,
Nirantharakumar K.
J Clin Endocrinol Metab. 2020
Feb 1;105(2). pii: dgz006. Free
PMC Article
Addison’s
CAH
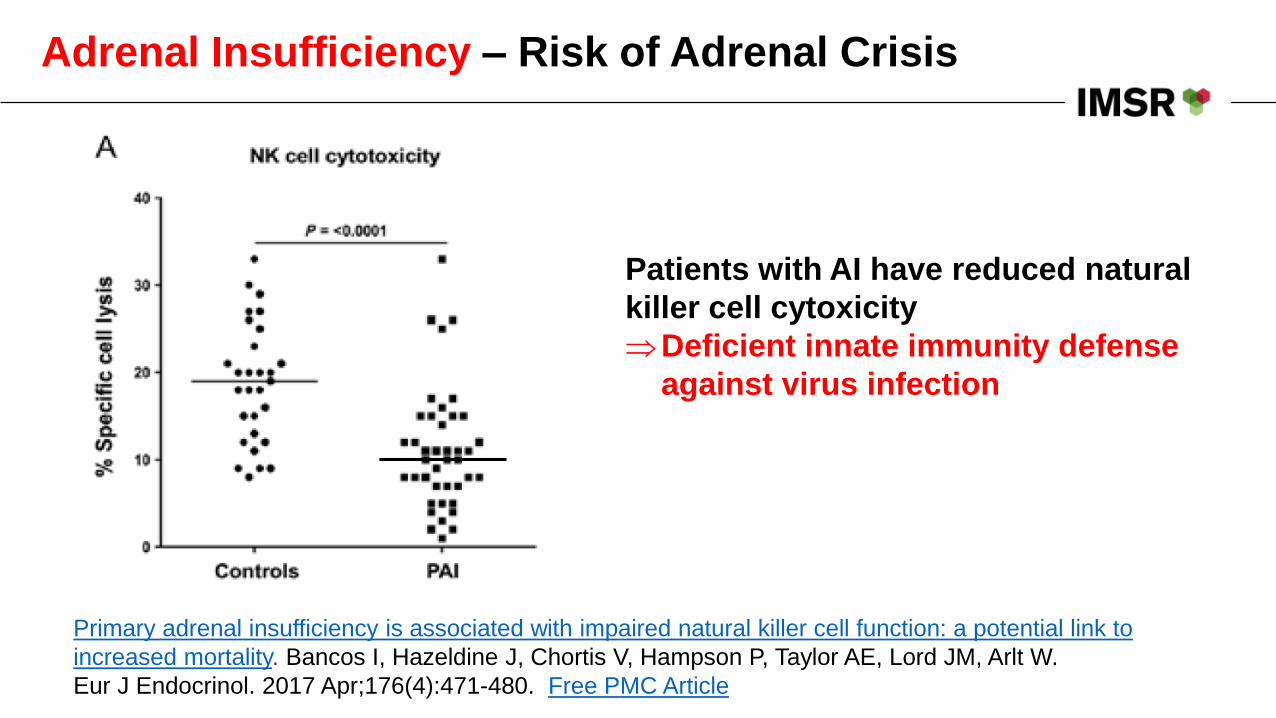
Adrenal Insufficiency – Risk of Adrenal Crisis
Primary adrenal insufficiency is associated with impaired natural killer cell function: a potential link to
increased mortality. Bancos I, Hazeldine J, Chortis V, Hampson P, Taylor AE, Lord JM, Arlt W.
Eur J Endocrinol. 2017 Apr;176(4):471-480. Free PMC Article
Patients with AI have reduced natural
killer cell cytoxicity
Deficient innate immunity defense
against virus infection
AI and COVID-19
Increased Risk to catch COVID-19 in patients with AI:
• Increased risk of infection including risk of respiratory infections and viral infections
• No evidence at present that COVID-19 has a more severe course in AI
Increased Risk from COVID-19 in patients with AI:
• Patients with AI experiencing major inflammation and fever are at risk of life-threatening adrenal crisis
Endocrinology in the time of COVID-19: Management of adrenal insufficiency.
Arlt W, Baldeweg SE, Pearce SHS, Simpson HL.
Eur J Endocrinol. 2020 Apr 1. pii: EJE-20-0361. doi: 10.1530/EJE-20-0361. [Epub ahead of print]
AI and COVID-19
Endocrinology in the time of COVID-19: Management of adrenal insufficiency.
Arlt W, Baldeweg SE, Pearce SHS, Simpson HL.
Eur J Endocrinol. 2020 Apr 1. pii: EJE-20-0361. doi: 10.1530/EJE-20-0361. [Epub ahead of print]
Educate• General Sick Day Rules, Special COVID-19 Sick Day Rules• Observe stringent social distancing
Equip• Provide with sufficient hydrocortisone supplies• Up-to-date hydrocortisone emergency self-injection kit
Empower• Provide with Hydrocortisone Steroid Emergency Card
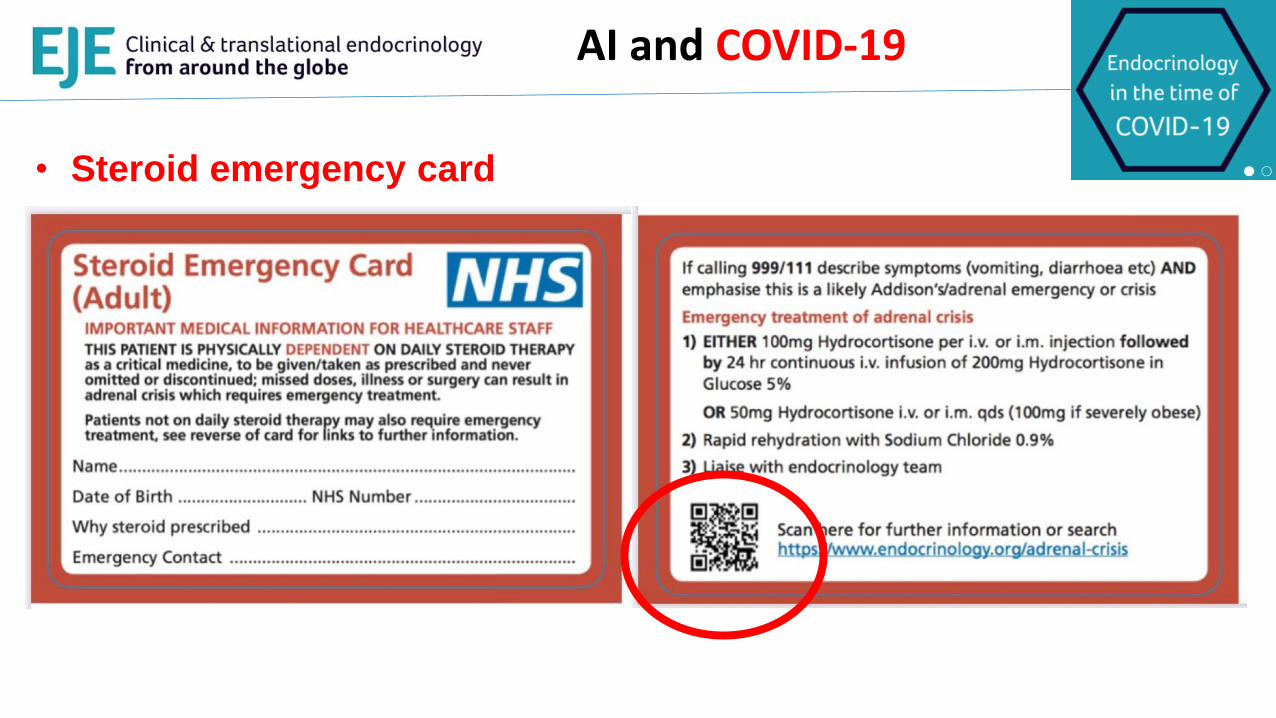
• Steroid emergency card
AI and COVID-19
https://www.endocrinology.org/adrenal-crisis
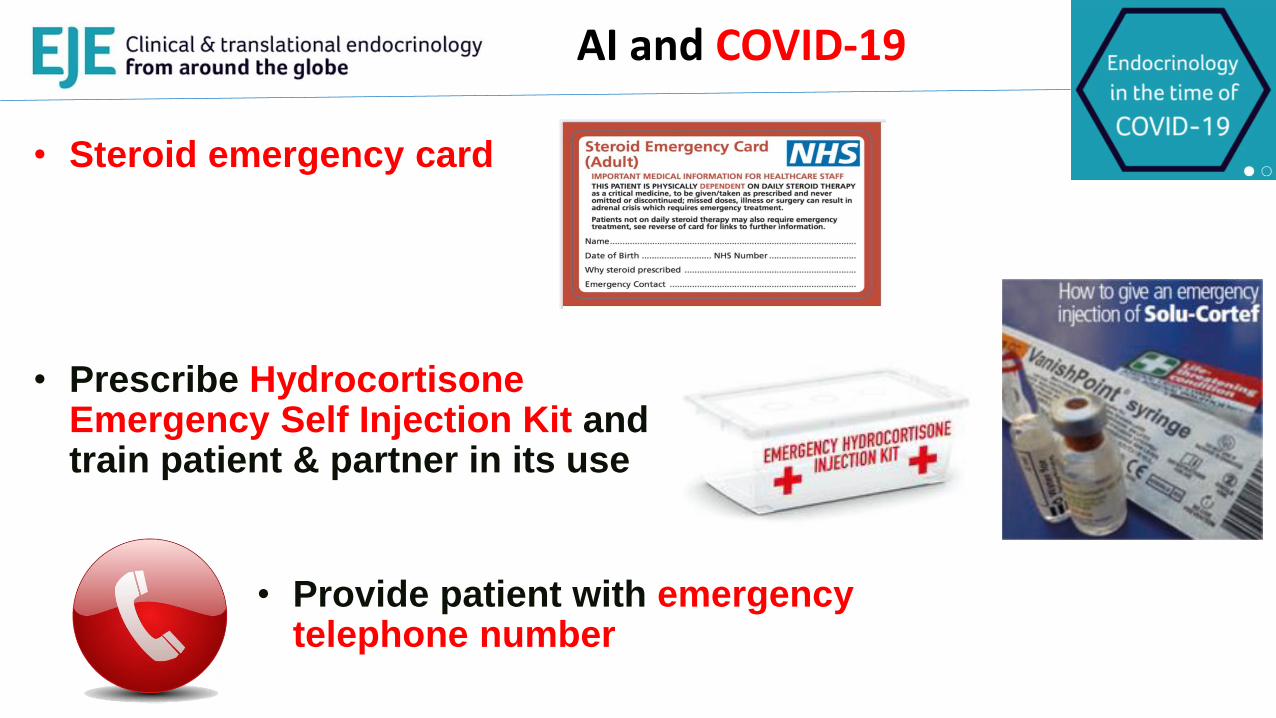
• Steroid emergency card
• Prescribe Hydrocortisone Emergency Self Injection Kit and train patient & partner in its use
AI and COVID-19
• Provide patient with emergency telephone number
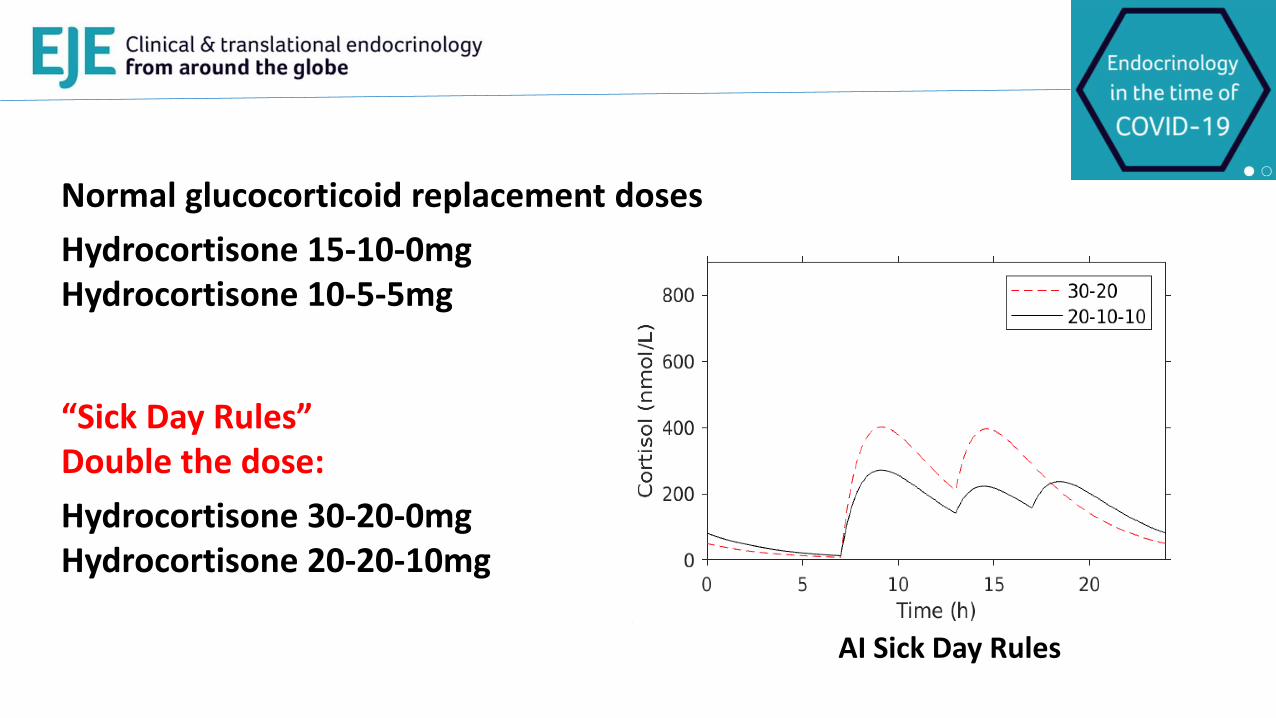
AI Sick Day Rules
Normal glucocorticoid replacement doses
Hydrocortisone 15-10-0mgHydrocortisone 10-5-5mg
“Sick Day Rules”Double the dose:
Hydrocortisone 30-20-0mgHydrocortisone 20-20-10mg
AI and COVID-19
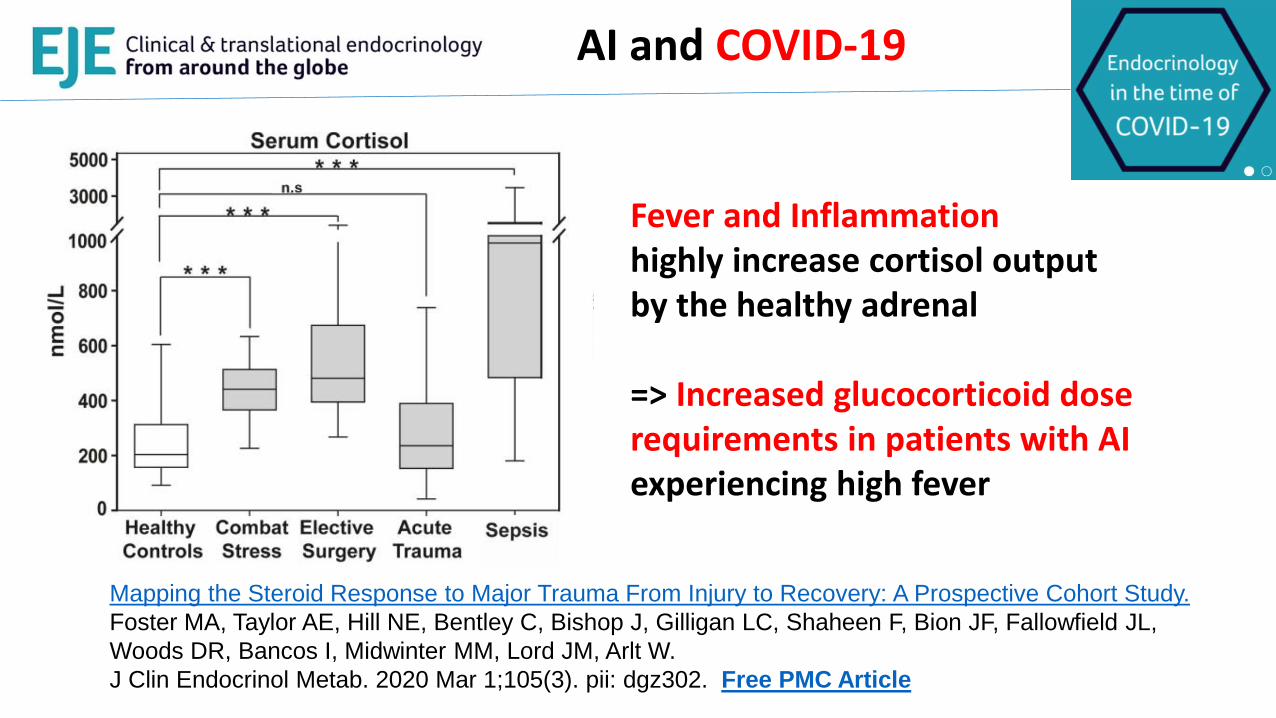
Fever and Inflammation highly increase cortisol output by the healthy adrenal
=> Increased glucocorticoid dose requirements in patients with AI experiencing high fever
Mapping the Steroid Response to Major Trauma From Injury to Recovery: A Prospective Cohort Study.
Foster MA, Taylor AE, Hill NE, Bentley C, Bishop J, Gilligan LC, Shaheen F, Bion JF, Fallowfield JL,
Woods DR, Bancos I, Midwinter MM, Lord JM, Arlt W.
J Clin Endocrinol Metab. 2020 Mar 1;105(3). pii: dgz302. Free PMC Article
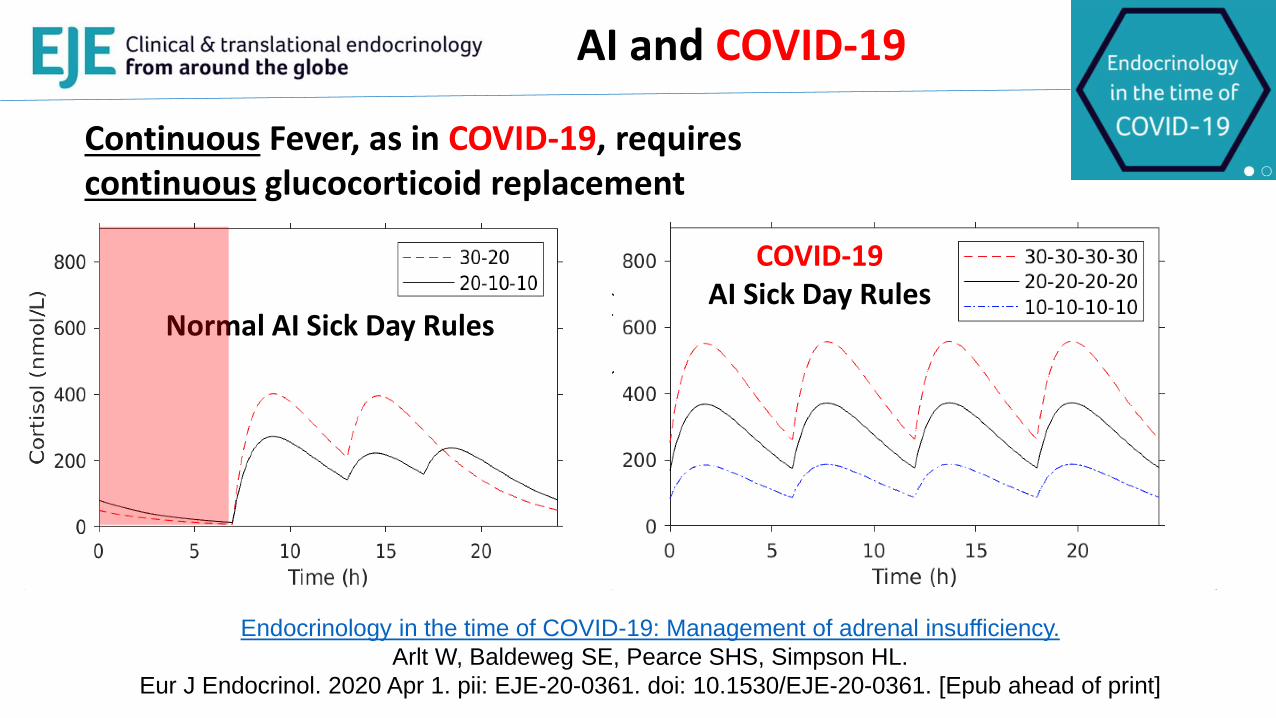
Normal AI Sick Day Rules
COVID-19 AI Sick Day Rules
Continuous Fever, as in COVID-19, requires continuous glucocorticoid replacement
AI and COVID-19
Endocrinology in the time of COVID-19: Management of adrenal insufficiency.
Arlt W, Baldeweg SE, Pearce SHS, Simpson HL.
Eur J Endocrinol. 2020 Apr 1. pii: EJE-20-0361. doi: 10.1530/EJE-20-0361. [Epub ahead of print]
AI and COVID-19
Endocrinology in the time of COVID-19: Management of adrenal insufficiency.
Arlt W, Baldeweg SE, Pearce SHS, Simpson HL.
Eur J Endocrinol. 2020 Apr 1. pii: EJE-20-0361. doi: 10.1530/EJE-20-0361. [Epub ahead of print]
Onset of signs and symptoms suggestive of COVID-19 (fever >38°C (>100 F), a new or continuous dry cough, sore throat, loss of sense of smell or taste, aches and pains, fatigue)
20 mg hydrocortisone orally every 6 hours Patients on modified release hydrocortisone should switch to immediate release hydrocortisone and take 20 mg
orally every 6 hours
Patients on 5-15 mg prednisolone daily should take 10 mg prednisolone every 12 hours; patients on oral
prednisolone >15 mg should continue their usual dose but take it split into two equal doses of at least 10 mg each.
Take paracetamol 1000 mg every 6 hours for fever
Rest, drink regularly throughout day and night and monitor whether passing urine
regularly
Request medical advice on the suspected COVID-19 infection
AI and COVID-19
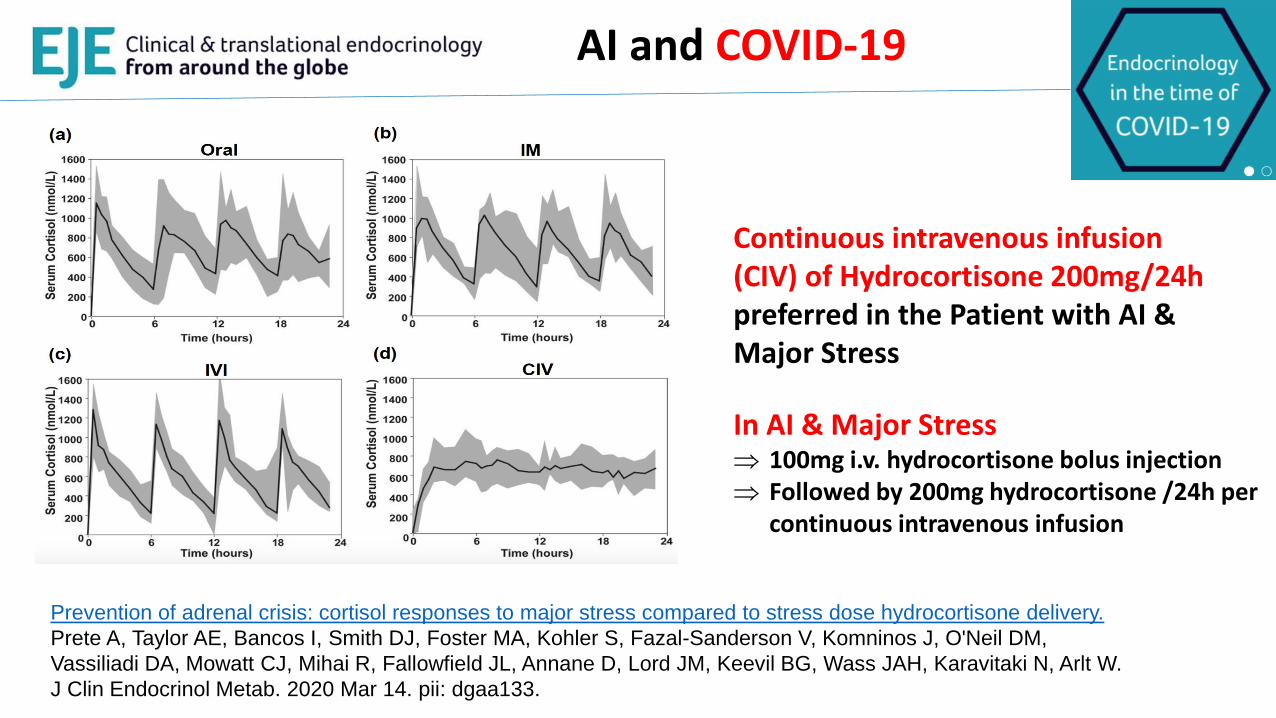
Prevention of adrenal crisis: cortisol responses to major stress compared to stress dose hydrocortisone delivery.
Prete A, Taylor AE, Bancos I, Smith DJ, Foster MA, Kohler S, Fazal-Sanderson V, Komninos J, O'Neil DM,
Vassiliadi DA, Mowatt CJ, Mihai R, Fallowfield JL, Annane D, Lord JM, Keevil BG, Wass JAH, Karavitaki N, Arlt W.
J Clin Endocrinol Metab. 2020 Mar 14. pii: dgaa133.
Continuous intravenous infusion (CIV) of Hydrocortisone 200mg/24hpreferred in the Patient with AI & Major Stress
In AI & Major Stress 100mg i.v. hydrocortisone bolus injection Followed by 200mg hydrocortisone /24h per
continuous intravenous infusion
AI and COVID-19
Endocrinology in the time of COVID-19: Management of adrenal insufficiency.
Arlt W, Baldeweg SE, Pearce SHS, Simpson HL.
Eur J Endocrinol. 2020 Apr 1. pii: EJE-20-0361. doi: 10.1530/EJE-20-0361. [Epub ahead of print]
Onset of signs and symptoms of clinical deterioration (dizziness; intense thirst; shaking uncontrollably; drowsiness, confusion, lethargy; vomiting; severe diarrhoea; increasing shortness of breath, respiratory rate >24/min , difficulty speaking
Immediately inject (patient or carer) 100 mg hydrocortisone per i.m. injection
Call for emergency medical attention for treatment and transfer to hospital, consider
making their own way to hospital
Present steroid card to medical emergency staff
In Hospital: Inject 100mg hydrocortisone i.v., followed by continuous i.v. infusion of
200mg hydrocortisone (alternative 6-hourly 50mg hydrocortisone i.m. or i.v.
injections)

Centre for Endocrinology,
Diabetes and MetabolismAdrenal Team
• Wiebke Arlt• Miriam Asia• Sherwin Criseno• Yasir Elhassan• Chona Feliciano• Helena Gleeson• Alessandro Prete• Cristina Ronchi
Stephanie BaldewegSimon PearceHelen Simpson
David J. Smith