Embed Size (px)
Citation preview

William G. Wierda, Prof., M.D., Ph.D.
Current position:
• Professor and Center Medical Director, Department of
Leukemia, Division of Cancer Medicine, The University of Texas
MD Anderson Cancer Center, Houston, TX
• Director of clinical core and clinical research at CLL
Consortium (CRC, multicenter P01 project)
Focus of work:
• Directing clinical and translational efforts in CLL and low-
grade lymphoproliferative diseases also as part of his role in
the CRC
• NCCN guidelines: CLL treatment recommendations
Specific expertise / current research interest:
• Prognostic factors and developing prognostic models in CLL
• Immune and Gene therapies for patients with CLL
• Developing Chemoimmunotherapy regimens and treatment
strategies for relapsed and refractory patients with CLL

Chronic Lymphocytic Leukemia:
Individualizing Therapy
26 January 2017
William G. Wierda M.D.,Ph.D.
Professor of Medicine
Department of Leukemia
Division of Cancer Medicine
U.T. M.D. Anderson Cancer Center
Houston, TX USA

Chronic Lymphocytic Leukemia

Chronic Lymphocytic Leukemia• Most common adult leukemia (~ 15,000 cases per year)
– 30% of adult leukemias
• Median age at diagnosis 72 years
• Median survival 9 yrs– Causes ~ 4400 deaths per year
• Absolute survival has increased over last 2 decades
• Advanced CLL has increased morbidity and mortality related to infections
American Cancer Society. Cancer Facts & Figures 2008; Rai K, et al. Blood. 1975;46:219-234;
Brenner H, et al. Blood. 2008;111:4916-4921.
1980-1984 2000-2004 P
5-year 54.2% 60.2% < .0001
10-year 27.8% 34.8% < .0001

CLL Diagnosis
ALC: > 5,000 /L – mature appearing lymphocytes
PLL = > 55% prolymphocytes or > 15,000 /L
Immunophenotype:
CD5+ / CD19+ / CD23+ / surface Ig light chain restricted ( or )
BM Bx: not required for diagnosis
> 30% lymphocytes on aspirate
Additional testing for prognosis:
Cytogenetics, FISH, CD38, ZAP70, IgVH mutations, serum B2M

Clinical Course of CLL
• Asymptomatic at diagnosis and for prolonged periods
• Diagnosis often incidental
• Initial symptoms: lymph node / anemia
• Progression: bone marrow impairment, susceptibility to infection
• Progressive hypogammaglobulinemia with advancing disease
• Long-term complications:autoimmune phenomena, Richter’s transformation

“Clinical and Classical” Prognostic Factors Associated With Inferior Survival in CLL
Advanced stage
Short lymphocyte doubling time
Diffuse pattern of bone marrow infiltration
Advanced age / male
-2 microglobulin and circulating CD23

Newer Prognostic Factors Associated With Inferior Survival in CLL
FISH cytogenetic abnormalities
17p deletion
11q deletion
Complex abnormalities
Unmutated (<2% homology with germline) immunoglobulin heavy chain variable gene (IGHV)
Expression of ZAP-70 ( 20% positive)
Expression of CD38 ( 30% positive)

Genomic Aberrations in CLLInterphase FISH Results—82% Abnormal
Abnormality No. Patients (%)
13q deletion 178 (55)
11q deletion 58 (18)
trisomy 12 53 (16)
17p deletion 23 (7)
6q deletion 21 (6)
Dohner et al. N Engl J Med. 2000;343:1910.

Dohner et al. N Engl J Med. 2000;343:1910-1916.
Probability of Survival100
80
60
40
20
00 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180
Pa
tie
nts
Su
rviv
ing
(%
)
Months
17p deletion
11q deletion
12q trisomy
Normal
13q deletion as
sole abnormality

Su
rviv
ing
(%
)
Survival of CLL Patients With Mutated vs Unmutated IgVH Gene
All patients (N=84)Stage-A CLL patients
(n=62)
Su
rviv
ing
(%
)
0 50100 150 200 250 3000
20
40
60
80
100
Months
P=0.0008
Months
P=0.001
0 50 100 150 200 250 3000
20
40
60
80
100
Mutated
UnmutatedUnmutated
Mutated
Hamblin TJ et al. Blood. 1999;94:1848-1854.

Hallek et al Blood 2008;111:5446-5456
IWCLL-NCI: Indications to
Initiate Treatment for CLL• Constitutional symptoms referable to CLL
• Progressive marrow failure
• Autoimmune anemia +/- thrombocytopenia poorly
responsive to steroids or other
• Massive (>6 cm) or progressive splenomegaly
• Massive (>10 cm) or progressive lymphadenopathy
• Progressive lymphocytosis, >50% increase over 2 months
or LDT < 6 months
• NO EARLY TREATMENT, EVEN FOR HIGH-RISK

1960s
1970s
Alkylating agents
- Chlorambucil
- Cyclophosphamide
2000s
Chemoimmunotherapy (FCR)
Alemtuzumab
CD20 mAbs
Bendamustine
1990s
Combination
chemotherapy
First-line Treatments for CLLTreatment Evolution
1980s
Purine nucleosides
- Fludarabine
- Pentostatin
- Cladribine
2010s
Small molecule
inhibitors
- BCR pathway
- Bcl-2

CLL Patient Populations and Community “Standards of Care”
Untreated, high-risk - watch and wait
First-line therapyDel(17p) - Ibrutinib
“Elderly” – chlorambucil+CD20 mAb
Fit CIT-eligible – FCR / BR
Salvage treatments for active disease, incl del(17p)BTK-inhibitor (ibrutinib)
PI3-K-inhibitor (idelalisib) + rituximab
Rel / Ref del(17p) - venetoclax
Richter’s transformation – intensive CIT the allo-SCT
ibrutinib

Treatment comparisons
R
A
N
D
O
M
I
Z
E
2:1:2
G-Clb vs. Clb
Obinutuzumab + chlorambucilx 6 cycles
R-Clb vs. Clb
Rituximab + chlorambucilx 6 cycles
Chlorambucil x 6 cycles (control arm)
R
A
N
D
O
M
I
Z
E
2:1:2
Chlorambucil x 6 cycles (control arm)
G-Clb vs. R-Clb
Obinutuzumab + chlorambucilx 6 cycles
Rituximab + chlorambucilx 6 cycles Goede V et al. ASH 2013; Plenary Abstract 6;
Goede V et al. N Engl J Med 2014;370:1101-1111

Median observation time: G-Clb, 18.8 months; R-Clb, 18.6 months
Type 1 error controlled through closed test procedure; P value of the global test was <0.0001
Independent Review Committee-assessed progression-free survival (PFS) was consistent with investigator-assessed PFS
0 3 6 9 12 15 18 21 24 27 30 33 36 39
330 317 309 259 163 114 72 49 31 14 5 2 0 0
330 307 302 278 213 156 122 93 60 34 12 4 1 0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Pro
gre
ssio
n-f
ree
su
rviv
al
Time (months)
G-Clb:
R-Clb:
No. at risk
Progression-free survival (Head-to-Head)
Goede V et al. ASH 2013; Plenary Abstract 6; Goede V et al. N Engl J Med 2014;370:1101-1111
Currently no significant difference in overall survival

Median observation time: G-Clb, 23.2 months; Clb, 20.4 months
No multiplicity adjustment was done for secondary endpoints
Total number of deaths: G-Clb, 22 (9%); Clb, 24 (20%)
0 3 6 9 12 15 18 21 24 27 30 33 36 39
118 109 105 103 102 94 70 56 44 29 15 5 0 0
238 226 223 221 215 211 170 144 115 71 34 14 2 0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Ove
rall
su
rviv
al
Time (months)
G-Clb:
Clb:
No. at risk
Overall survival (Obinutuzumab)
Goede V et al. ASH 2013; Plenary Abstract 6; Goede V et al. N Engl J Med 2014;370:1101-1111

ran
do
mis
e 1
:1
Minimum 3 cycles, until best response or PD , maximum 12 cycles
- No cross over allowed -
Ofatumumab +
Chlorambucil (O+CHL)
Chlorambucil (CHL)
Follow up:
1 Month post
last dose,
Month 3, q3mo
thereafter
COMPLEMENT 1: Study Design
O: cycle 1 d1 300 mg, d8 1000 mg, Cycle 2-12 d1 1000 mg every 28 days
CHL: 10 mg/m2 d1-7 every 28 days
Dose rationale: evidence of highest ORR and longest PFS with low toxicity
compared to any other CHL monotherapy regimen
Patients with
previously
untreated CLL
• considered
inappropriate for
F-based therapy
• Active disease (NCI-WG IWCLL 2008)
• ≥18 years
• ECOG ≤ 2
• N=444 (planned)
Hillmen et al. ASH 2013, Abstract 528.

Subjects at risk
C 226 173 130 92 67 52 33 17 6 1 1
O+CHL 221 192 169 148 125 104 70 46 28 15 9 3 1
Progression-free Survivalas assessed by an Independent Review Committee
(median [months])
CHL
mPFS: 13.1(95% CI: 10.6,13.8)
O+CHL
mPFS: 22.4(95% CI: 19.0,25.2)
HR 0.57, p<0.001
Pro
ba
bil
ity o
f P
rog
res
sio
n-f
ree S
urv
iva
l
Median follow-up: 28.9 months
Time since randomization (months)
Hillmen et al. ASH 2013, Abstract 528. Currently no difference in overall survival

CLL8 STUDY: FCR VS FC IN FRONTLINE
Rationale
Fischer K et al.
ASH 2012
FCR 69.4% alive
Median not reached
FC 62.3% alive
Median 86 months
HR 0.68,
95% CI 0.535-0.858
p=0.001

FCR300: PFS by IGHV Mutation Status
Thompson PA, et al. Blood 2016; 127:303–309
P<0.0001Perc
en
tag
e P
rog
ressio
n-f
ree
Time (Years)
0
25
50
75
100
0 1 2 3 4 8 9 105 6 7 11 12 13 14 15 16
N Prog-free
IGHV mutated 88 49
IGHV unmutated 126 12

CLL10 STUDY: FCR VS BR IN FRONT-LINE
Design
Non-Inferiority of BR in comparison to FCR for PFS:
HR (λ BR/FCR) less than 1.388
Randomization
Patients with untreated, active CLL without del(17p) and good physical fitness
(CIRS ≤ 6, creatinine clearance ≥ 70 ml/min)
FCR Fludarabine 25 mg/m² i.v., days 1-3
Cyclophosphamide 250 mg/m², days 1-3,
Rituximab 375 mg/ m2 i.v. day 0, cycle 1
Rituximab 500 mg/m² i.v. day 1, cycle 2-6
BR
Bendamustine 90mg/m² day 1-2
Rituximab 375 mg/m² day 0, cycle 1
Rituximab 500 mg/m² day 1, cycle 2-6
Eichhorst et al., ASH 2014, Abstract 19

CLL10 STUDY: FCR VS BR IN FRONT-LINE
PFS in IGHV matched population (n=398: FCR= 201; BR =197)
P = 0.005
HR = 1.565 =
> 1.388
Median PFS
FCR NR
BR 43.1 months
Eichhorst et al., ASH 2014, Abstract 19
NO difference in overall survival

CLL10 STUDY: FCR VS BR IN FRONT-LINE
Progression-free survival by age group
Patients ≤ 65 years: P < 0.001
FCR 53.6 months BR 38.5 months
Patients > 65 years: P = 0.170
FCR not reached BR 48.5 months
Eichhorst et al., ASH 2014, Abstract 19

CLL10 STUDY: FCR VS BR IN FRONT-LINE
Infections CTC 3-4 in detail
Adverse event FCR
(% of pt)
BR
(% of pt)
p value
All Infections 39.1 26.8 <0.001
Infections during therapy
only
22.6 17.3 0.1
Infections during first 5
months after therapy
11.8 3.6 <0.001
All infections in patients ≤ 65years
35.2 27.5 0.1
All infections in patients > 65years
47.7 20.6 <0.001
Eichhorst et al., ASH 2014, Abstract 19

Targeting of BCR signaling in CLL
• BCR-associated kinases are targets of new drugs in clinical development
• Btk (Bruton’s tyrosine kinase) inhibitors: Ibrutinib, CC-292, ACP-196
• PI3 kinase inhibitors: Isoform-Selective Inhibitor of PI3-Kinases1, Idelalisib, IPI-145, TGR-1202
• Syk (spleen tyrosine kinase) inhibitors: GS-9973, Fostamatinib, PRT-20702
1 Niedermeier M, et al. Blood 113(22):5549-57, 5/20092 Quiroga MP, et al. Blood 114(5):1029-37, 07/2009From: Nat Rev Immunol 2:945

RESONATE-2 (PCYC-1115/1116) Study Design
Patients (N=269)• Treatment-naïve CLL/SLL
with active disease• Age ≥65 years• For patients 65-69 years,
comorbidity that may preclude FCR
• del17p excluded
ibrutinib 420 mg once daily until progression
chlorambucil 0.5 mg/kg (to maximum 0.8 mg/kg) days 1 and 15 of 28-day cycle up to
12 cycles
CLL progression or
1115 study closure
PCYC-1116 Extension
Study*
In clb arm, n=55 crossed
over to ibrutinib
following PD
Stratification factors• ECOG status (0-1 vs. 2)• Rai stage (III-IV vs. ≤II)
RANDOMIZE
1:1
Efficacy (PFS, OS, ORR) determined by investigator-assessment.
*Patients could enroll in separate extension study PCYC-1116 after independent review committee-confirmed PD or at study PCYC-1115 closure for continuing treatment and follow-up.
Barr et al. ASH 2016, Abstract 234

RESONATE-2: Ibrutinib Prolonged PFS Over Chlorambucil
88% reduction in the risk of progression or death for patients randomized to ibrutinib Subgroup analysis of PFS revealed benefit was observed across all sub-groups
(n=136)
(n=133)
Median PFS not reached
Median PFS 15 mo
Barr et al. ASH 2016, Abstract 234

RESONATE-2: Ibrutinib Significantly Improved PFS in Patients with Del11q
In del11q subgroup, Ibrutinib led to 99% reduction in risk of progression or death and 82% reduction in those without del11q, compared to chemotherapy
(n=101)
(n=29)
(n=96)
(n=25)
(n=101)
(n=29)
(n=96)
(n=25)
ibrutinibdel11q yes (n=29)
del11q no (n=101)
del11q yes (n=25)
chlorambucil del11q no (n=96)
Barr et al. ASH 2016, Abstract 234

RESONATE-2: Ibrutinib Significantly Improved PFS in Patients Regardless of IGHV Status
Ibrutinib led to 83% and 92% reduction in the risk of progression or death in patients with mutated and unmutated IGHV, respectively, compared to chemotherapy
(n=40)
(n=58)
(n=42)
(n=60)
Barr et al. ASH 2016, Abstract 234

RESONATE-2: Ibrutinib Continues to Demonstrate OS Benefit Over Chlorambucil With Longer Follow-Up and Cross-Over
(n=136)
(n=133)
Barr et al. ASH 2016, Abstract 234

RESONATE-2: ORR in the Ibrutinib* Arm
Ibrutinib CR rates continue to improve over time: increasing from 7% at 12 months to 15% at 24 months to 18% with median follow-up of 29 months.
CR, complete response; CRi, CR with incomplete blood count recovery.
71%86%
67% 74%65%
18%
14%
20%21%
20%
0%10%20%30%40%50%60%70%80%90%
100%
All Patients(N=136)
With Del11q(n=29)
Without Del11q(n=101)
Unmutated IGHV(n=58)
Mutated IGHV(n=40)
PR-L PR nPR CR/CRi
1%
1%
1%
2%
3%
95%88%
100%92% 90%
0
6070
9080
100
40302010
50
Be
st R
esp
on
se (
%)
*Response rates with chlorambucil are the same as in the original report (Burger NEJM 2015)
Barr et al. ASH 2016, Abstract 234

Emerging Concepts in
First-line Therapy for CLL
del(17p) = no chemo
Older adults = move away from chemo
Mutated IGHV = role for FCR
MRD-negative = longer PFS, OS
Combination approaches

MDACC First-line Therapy
Individualizing treatment
Younger, fit, IGHV-M – 20% Ibrutinib + FC + Obinutuzumab (GA101) (iFCG) (2015-0281)
IGHV-UM, del(11q), ≥65yr – 75% Ibrutinib + Venetoclax (2015-0860)
Del(17p) – 5% Ibrutinib + Venetoclax (2015-0860)

FCR300: PFS by IGHV Mutation Status
Thompson PA, et al. Blood 2016; 127:303–309
P<0.0001Perc
en
tag
e P
rog
ressio
n-f
ree
Time (Years)
0
25
50
75
100
0 1 2 3 4 8 9 105 6 7 11 12 13 14 15 16
N Prog-free
IGHV mutated 88 49
IGHV unmutated 126 12

iFCG Regimen
2015-0281
•Obinutuzumab: more effective CD20 mAb than rituximab
•Addition of ibrutinib to CIT may be synergistic
•Reducing chemotherapy exposure may reduce risk of secondary MDS/AML
•Higher MRD-negativity will result in better PFS, OS

iFCG
First-line, Fit, IGHV-M
2015-0281
Courses 1-3Course 1 Course 2-3
D1 D2 D3 D4 D8 D15 D1 D2 D3
Obinutuzumab (mg) 100 900 - - 1000 1000 1000 - -
Fludarabine (mg/m2) - 25 25 25 - - 25 25 25
Cyclophosphamide
(mg/m2)- 250 250 250 - - 250 250 250
Ibrutinib 420 mg once daily continuous

iFCG
2015-0281
Treatment Schema
Ibrutinib
CR, MRD-negative @ C3
Ibrutinib+obinutuzumab
<CR or MRD-positive @ C3
iFCG iFCG iFCG
C3 Response
CT
BM
iG iG iG
C6 Response
CT
BM
C12 Response
CT
BM
MRD-positive
@ 1yr
Continue
Ibrutinib

Statistical Considerations
•Primary endpoint: CR/CRi and bone marrow MRD-negativity after 3 courses of iFCG
For mutated IGHV, the bone marrow MRD(-) rate was 26% (16/62) after 3 courses of FCR
Strati et al. Blood 2014
Simon’s optimal two-stage design
Null hypothesis 26%; target response rate 45%
Sample size = 45

Clinical Responses
n=18 BM MRD n=18 BM MRD
ORR 18/18 14/18 neg 18/18 16/18 neg
CR/CRi
PR
6
12
6/6 neg
8/12 neg
7
11
7/7 neg
9/11 neg
78% (14/18) BM MRD neg at 3 mos
Comparison: FCR 3 cycles, 26% marrow MRD-
3 mos Best
• 31 consented
• 24 started treatment

BCR vs. BCL-2 Inhibitors
B-cell Receptor Inhibitors
(Ibrutinib, Idelalisib)
Bcl-2
Antagonists
(ABT-199)
Response Blood +++
LN +++
Marrow +
Blood +++
LN ++
Marrow +++
Lymphocytosis +++ -
Complete Responses CR <10% CR 20-25%
S/E profile Ibrutinib (A. fib, bleeding)
Idelalisib (colitis, pneumonitis)
TLS

Ibrutinib + Venetoclax (2015-0860)
• Investigator-initiated Phase II trial
•Rationale
Non-overlapping mechanism of action
Non-overlapping toxicity profile
Synergy in preclinical models (Dr. Gandhi, MDACC)
• Cervantes-Gomez et al. Clin Cancer Res. 2015;21(16):3705-15.

5-Year Experience With Ibrutinib MonotherapyPCYC-1102/1103 Phase 2 Study Design
Patients with CLL/SLL treated with
oral, once-daily ibrutinib (420 or 840 mg/day)
Long-Term Follow-Up
≥SD
*R/R includes patients with high-risk CLL/SLL, defined as progression of disease <24 months after initiation of a chemoimmunotherapy regimen or failure to respond
Relapsed/Refractory*
(R/R)n=101
Treatment Naïve (TN) ≥65 years
n=31
Phase 2 (PCYC-1102)N=132
Extension Study (PCYC-1103)
O’Brien et al. ASH 2016, Abstract 233

5-Year Experience With Ibrutinib MonotherapyBaseline Characteristics
CharacteristicTN
(n=31)R/R
(n=101)
Cytogenetic abnormalitiesDel17pDel11qTrisomy 12Del13qComplex karyotype
Unmutated IGHV
6%3%
26%55%13%
48%
34%35%12%47%37%
78%
Median lines of prior therapies, n (range)1–23≥4
———
4 (1–12)27%14%59%
O’Brien et al. ASH 2016, Abstract 233

DispositionTN
(n=31)R/R
(n=101)
Median time on study, months (range)62
(1–67)49
(1–67)
Duration of study treatment, n (%)≤1 year>1–2 years>2–3 years>3–4 years≥4 years
5 (16%)0
1 (3%)1 (3%)
24 (77%)
24 (24%)14 (14%)
9 (9%)19 (19%)35 (35%)
Patients remaining on ibrutinib therapy, n (%) 20 (65%) 30 (30%)
Primary reason for discontinuation, n (%)Progressive diseaseAdverse eventConsent withdrawalInvestigator decisionLost to follow-up
1 (3%)6 (19%)3 (10%)
01 (3%)
33 (33%)21 (21%)
5 (5%)11 (11%)
1 (1%)
Ibrutinib Treatment Continued in 65% of TN and 30% of R/R Patients
• After ~5 years of follow-up, 65% of TN and 30% of R/R patients continue treatment on study.
O’Brien et al. ASH 2016, Abstract 233

3% 3% 3%
55%
76% 71%
29%
10% 14%
0%
20%
40%
60%
80%
100%
5-Year Experience With Ibrutinib MonotherapyBest Response
47
87% 89% 89%
Median DOR, months (range)
NR (0.0+ to 65.5+) 56.8 (0.0+ to 65.5+) NR (0.0+ to 65.5+)
Median follow-up, months (range)
62 (1–67) 49 (1+–67) 56 (1+–67)
CR
PRPR-L
TN (n=31) R/R (n=101) Total (N=132)
O’Brien et al. ASH 2016, Abstract 233

5-Year Experience With Ibrutinib MonotherapySurvival Outcomes: Overall Population
Median PFS 5-year PFS
TN (n=31) NR 92%R/R (n=101) 52 mo 43%
Progression-Free Survival Overall Survival
Median OS 5-year OS
TN (n=31) NR 92%R/R (n=101) NR 57%
O’Brien et al. ASH 2016, Abstract 233

5-Year Experience With Ibrutinib MonotherapySurvival by IGHV-MS in R/R Patients*
*Only 2 patients in the TN group showed disease progression. Subgroup analyses, therefore, focused on the R/R population.
Progression-Free Survival Overall Survival
Median OS 5-year OS
Mutated IGHV (n=16) 63 mo 66%
Unmutated IGHV (n=79) NR 55%
Median PFS 5-year PFS
Mutated IGHV (n=16) 63 mo 53%
Unmutated IGHV (n=79) 43 mo 38%
O’Brien et al. ASH 2016, Abstract 233

5-Year Experience With Ibrutinib MonotherapySurvival by FISH in R/R Patients*
**No del17p, del11q, del13q, or trisomy 12; in hierarchical order for del17p, and then del11q.
Progression-Free Survival Overall Survival
*Only 2 patients in the TN group showed PD or death. Subgroup analyses, therefore, focused on the R/R population.
Median OS 5-year OS
Del17p (n=34) 57 mo 32%
Del11q (n=28) NR 61%
Trisomy 12 (n=5) NR 80%
Del13q (n=13) NR 91%
No abnormality** (n=16) NR 83%
Median PFS 5-year PFS
Del17p (n=34) 26 mo 19%
Del11q (n=28) 55 mo 33%
Trisomy 12 (n=5) NR 80%
Del13q (n=13) NR 91%
No abnormality** (n=16) NR 66%
O’Brien et al. ASH 2016, Abstract 233

5-Year Experience With Ibrutinib MonotherapySurvival by Complex Karyotype
Progression-Free Survival Overall Survival
• The majority (90%) of patients with complex karyotype had R/R disease (median 4 prior therapies).
Median PFS
5-year PFS
Complex karyotype (n=41) 33 mo 36%
No complex karyotype (n=71) NR 69%
Median OS
5-year OS
Complex karyotype (n=41) 57 mo 46%
No complex karyotype (n=71) NR 84%
O’Brien et al. ASH 2016, Abstract 233

Factors considered
Del17p
Del11q
Trisomy 12
Del13q
Lines of prior therapy (1-2, 3, and ≥4 lines vs 0 lines)
Bulky disease (≥5cm vs <5 cm)
IGHV mutation status
Complex karyotype
Del17p was identified as a significant predictor of PFS and OS
5-Year Experience With Ibrutinib MonotherapyMultivariate Analysis* for PFS and OS
*Multivariate regression analysis using Cox Proportional Hazard model and stepwise selection. There might be confounding effectsbetween covariates considered.
O’Brien et al. ASH 2016, Abstract 233

Ibrutinib Refractory/Intolerant:Cumulative Incidence of Discontinuation
Woyach et al. ASH 2016, Abstract 55

Ibrutinib Refractory/Intolerant:Baseline Characteristics Associated with IbrutinibDiscontinuationVariable Transformation CLL Progression Other Event
HR (95% CI) P HR (95% CI) P HR (95% CI) P
Complex Karyotype
(y vs. n)
5.00
(1.51-16.52)0.008
2.81
(1.34-5.88)0.006 --- ---
MYC abnormality
(y vs. n)
2.15
(1.00-4.65)0.051 --- --- --- ---
Del(17p13.1) on FISH (y
vs n) --- ---2.14
(1.15-3.96)0.016 --- ---
Age, years
(≥65 vs <65) --- ---0.49
(0.27-0.91)0.023
2.02
(1.25-3.28) 0.004
Prior therapies >3 (yes
vs no) --- ---
1.99
(1.23-3.23) 0.005
All models adjusted for monotherapy with ibrutinib versus combination therapy with ibrutinib and ofatumumab, regardless of
statistical significance.
Woyach et al. ASH 2016, Abstract 55

Ion Torrent for BTK and PLCγ2 performed on blood or marrow on 46 patients
87% have mutations in BTK or PLCG2 acquired at relapse
31 had BTK C481 as sole mutations
3 had PLCG2 hotspot mutations only
6 have both BTK C481S and PLCG2 hotspot mutations
6 have neither mutation
Association of CLL Progression with BTK and PLCγ2 Mutations
Woyach et al. ASH 2016, Abstract 55

Woyach et al. ASH 2016, Abstract 55
Ibrutinib Refractory/Intolerant:Resistance Mutations Appear Over Time

Ibrutinib Refractory/Intolerant:Resistance Mutations Persist After Salvage Therapy
Venetoclax Therapy Non-Venetoclax Therapy
Woyach et al. ASH 2016, Abstract 55

Ibrutinib FDA approved: relapsed CLL; first-line; del(17p)
Monotherapy @ 420 mg once daily-continuous
Lymphocytosis on start, resolves with Tx
Potent LN shrinkage, most responses partial,
residual disease in blood and marrow
GI toxicity most common; <5% a. fib. / bleeding
90% prog-free @30 mo (non-del(17p)-del(11q)
Median PFS for relapsed CLL with del(17p) is
32 months
Improved OS vs. ofatumumab in relapsed CLL

Class IPI3K Isoform
Cell TypeMouse embryonic
fibroblasts
Mouse embryonic
fibroblastsHuman basophils
Human
basophils
Cell-Based
Activity
PDGF-induced
pAKT
LPA-induced
pAKT
fMLP-induced
CD63+
FceR1-induced
CD63+
EC50 (nM) >20,000 1,900 3,000 8
a g d
Idelalisib/
GS-1101
Idelalisib: Potent and Selective Inhibitor of PI3Kd
Lannutti, et al. Blood, 2011
• Selectivity relative to Class I PI3K isoforms involved in insulin signaling and other physiological functions
• No off-target activity against Class II or III PI3K, mTOR, or DNA-PK
• No off-target activity seen in screen of >350 protein kinases (Ambit KINOMEscan™)

Idelalisib
FDA approved for relapsed CLL appropriate for
rituximab monotherapy
Twice daily dosing, continuous + rituximab
Toxicities: elevated LFTs, GI / diarrhea;
less common colitis and pulmonary
Most responses are partial, residual disease
Median PFS was 19.4 months
Efficacy in relapsed CLL with del(17p) & del(11q)
Improved OS vs. rituximab + placebo
Infection concerns in first-line

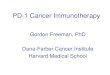
Venetoclax is a BCL-2 Selective Inhibitor
BCL-2 overexpression allows cancer cells to evade apoptosis by
sequestering pro-apoptotic proteins
Venetoclax binds selectively to BCL-2, freeing pro-apoptotic proteins that initiate
programmed cell death (apoptosis)
Cancer Cell DeathCancer Cell Survival
Restoration of apoptosis through BCL-2 inhibition
Pro-apoptoticprotein
BCL-2
Activation of caspases
Venetoclax
Apoptosis initiation
Pro-apoptoticprotein
BCL-2
BIM
BAX
BAK
BAX
Cytochrome c

Venetoclax oral once daily continuous dosing
Step-wise weekly ramp-up with risk-based prophylaxis to mitigate against tumor
lysis syndrome (TLS)
Response assessment (per iwCLL 2008 criteria):
• Monthly physical exam and blood counts
• CT scan
– To confirm clinical response
– Prespecified at week 36
• Bone marrow biopsy to confirm CR
Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Dosing Schedule and Assessments
*20mg dose for 1 week in patients with electrolyte abnormalities after first dose
Venetoclax 20 mg test 50 mg 100 mg 200 mg 400 mg
Week 1
D1
Week 1
D2-7
Week 2 Week 3 Week 4 and following*
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

N=107a n (%)
Median age (years), range 67, 37–85
Male 70 (65)
Prior therapies: median, range 2, 1–10
Prior bendamustine / refractory 54 (50) / 38 (70)
Prior fludarabine / refractory 78 (73) / 34 (44)
Prior CD20 mAb 90 (84)
ECOG grade 1/2 56 (52) / 9 (8)
One or more nodes ≥ 5 cm 57 (53)
ALC ≥25 x 109/L 54 (51)
TLS risk category
Low 19 (18)
Medium 43 (40)
High 45 (42)
Rai stage III or IV 51(48)
IGHV unmutated 30 (81)aIncludes 1 patient without 17p–; bLow defined as ALC<25 and nodes <5cm, medium defined as ALC>20 OR nodes
≥5 and < 10cm), high defined as (ALC>25 nodes ≥5 and < 10cm OR nodes > 10cm
Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Baseline Characteristics
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

IRC,
n (%)
Investigator, n
(%)
Overall Response 85 (79.4) 79 (73.8)
CR or CRi 8 (7.5) 17 (15.9)
nPR 3 (2.8) 4 (3.7)
PR 74 (69.2) 58 (54.2)
No response 22 (20.6) 28 (26.2)
Stable disease NA 24 (22.4)
Disease progression NA 2 (1.9)
Incomplete data NA 2 (1.9)
• 25 of 48 patients with no CLL in the bone marrow
• 18 of 45 patients assessed were MRD-negative in PB
Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Best Response
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

Of 45 patients tested, 18 achieved
MRD-negativity in peripheral blood
MRD-Negativity
Median time-to-first response: 0.8
months (0.1–8.1)
Median time to CR/CRi:
8.2 months (3.0–16.3)
Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Cumulative Incidence of Response
iwCLL Response
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Durability of Venetoclax Activity
PFS and OS (N=107)Duration of Response (N=85)
• 12-month estimates (95% CI):
– PFS: 72.0% (61.8, 79.8)
– OS: 86.7% (78.6, 91.9)
• 12-month estimates:
– All responders: 84.7%
– CR/CRi/nPR: 100%
– MRD-negative: 94.4%
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

Venetoclax (ABT-199) for Rel / Ref del(17p) CLL
Treatment-Emergent Adverse Events
Any grade
n (%)a
Grade 3/4
n (%)
Any treatment-emergent adverse event 103 (96) 81 (76)
Neutropenia 46 (43) 43 (40)
Diarrhea 31 (29) 0
Nausea 31 (29) 1 (1)
Anemia 29 (27) 19 (18)
Fatigue 23 (22) 0
Pyrexia 21 (20) 1 (1)
Thrombocytopenia 20 (19) 16 (15)
Hyperphosphatemia 17 (16) 1 (1)
Vomiting 16 (15) 1 (1)
Upper respiratory tract infectionb 16 (15) 2 (2)
aTable shows all-grade events occurring in 15% of patients or more; bInfections occurred in a total of 77 (72%) patients
Stilgenbauer et al. ASH 2015, Abstract LBA-6.

M14-032: Efficacy
Arm A
n=43
Arm B
n=21
Best response, n
(%)
Assessed by Assessed by
IRC Investigator IRC Investigator
ORR 30 (70) 29 (67) 13 (62) 12 (57)
CR/CRi 0/1 (2) 2 (5)/1 (2) 0/0 2 (10)/1 (5)
nPR 0 2 (5) 0 0
PR 29 (67) 24 (56) 13 (62) 9 (43)
Non-responder*
SD
PD
D/C‡
13 (30)
–
–
–
14 (23)
9 (21)
1† (2)
4 (9)
8 (38)
–
–
–
9 (43)
8 (38)
1† (5)
0*Non-responder category for IRC includes both SD or PD, which were not identified as separate categories
per IRC.†CLL progression and discontinued due to progression.‡D/C, patient discontinued the study prior to assessment.
Data as of 10June2016Jones et al. ASH 2016, Abstract 637

Median DoR, PFS, and OS had not been reached after 11.8 months of follow up
Estimated 12 month PFS for all patients: 80% (95% CI: 67%, 89%)
M14-032: Efficacy Per Independent Review
0 2 4 6 8 1 0 1 2 1 4
0
2 5
5 0
7 5
1 0 0
D u ra tio n o f R e s p o n s e
M o n th s s in c e f irs t d o s e
Pa
tie
nts
wit
h R
es
po
ns
e (
%)
N o . a t r is k 3 0 2 9 2 3 1 8 1 0 1
1 0 8 6 5 2
4 0 3 7 2 9 2 3 1 2 1
A rm A (R /R ib ru t in ib )
A rm B (R /R id e la l is ib )
A ll p a t ie n ts
0 2 4 6 8 1 0 1 2 1 4
0
2 5
5 0
7 5
1 0 0
P ro g re s s io n -F re e S u rv iv a l
M o n th s s in c e f irs t d o s e
Pro
gre
ss
ion
-fre
e s
urv
iva
l (%
)
4 3 3 7 3 6 2 8 2 7 1 5 3
2 1 1 7 1 5 6 5 2
6 4 5 4 5 1 3 4 3 2 1 7 3
A rm A (R /R ib ru t in ib )
A rm B (R /R id e la l is ib )
A ll p a t ie n ts
Data as of 10June2016Jones et al. ASH 2016, Abstract 637

Multivariate Analysis of R/R CLL/SLL in Phase 1 Studies of
Venetoclax ± Rituximab - Design
Final Escalation Strategy:
100 mg
Month 7 and ongoing
Cohort DoseCohort Dose200 mg
50 mg20 mg
Cohort Dose
Months 2 – 6Month 1Week 4Week 3
Week 2Week 1D2 – 7
Week 1D1 Venetoclax monotherapy
Rituximab: D1375 mg/m2
D1 of Months 2 - 6500 mg/m2
Dose escalation phase: 200, 300, 400, 500, 600mg/day cohorts (n = 41)
Safety expansion phase: 400mg/day cohort (n = 8)
Data pooled for these safety and efficacy analyses
Protocol-defined option to stop venetoclax after achieving CR or MRD-negative PR
Ma et al. ASH 2015, Abstract 830

Multivariate Analysis of R/R CLL/SLL in Phase 1 Studies of Venetoclax ± Rituximab – Baseline and Disposition
71
Characteristics Ven + R (n=49) Ven (n=116)
Median age, (range) 68 (50-88) 66 (36-86)
Male, n (%) 30 (61) 89 (77)
CLL, n (%)SLL, n (%)
48 (98)1 (2)
102 (88)14 (12)
ALC > 5 × 109/L, n (%)Median (range)*
32 (65)58 (5-207)
66 (57)28 (5-260)
Node size, n (%)>5 cm>10 cm
22 (25)1 (2)
67 (58)22 (19)
Prior therapies, median (range) 2 (1-5) 3 (1-11)
Del17p, n/N (%) 9/47 (19) 31/102 (30)
Del11q, n/N (%) 20/46 (44) 28/102 (28)
Unmutated IGHV, n/N (%) 19/27 (70) 46/63 (73)
Disposition Ven + R (n=49) Ven (n=116)
Months on venetoclax, median (range) 22 (<1-42) 17 (<1-44)
Discontinuation, n (%)Disease progressionAE/toxicityWithdrew consentManagement of comorbiditiesAllogeneic SCT
15 (31)9 (18)3 (6)3 (6)
00
65 (56)41 (35)13 (11)
2 (2)2 (2)7 (6)
*For patients with ALC > 5 × 109/L
Roberts et al. EHA 2016. Abstract P209

Multivariate Analysis of R/R CLL/SLL in Phase 1 Studies of Venetoclax ± Rituximab – Outcomes
72
Response, n/N (%)
ORR CR/CRi
Ven + R Ven Ven + R Ven
Best objective response 42/49 (86) 92/116 (79) 25/49 (51) 23/116 (20)
SubgroupsPrior therapies ≥3Lymph node size >5 cmDel17pDel11qAge ≥70 yearsDose ≥400 mg
16/21 (76)18/22 (82)
8/9 (89)17/20 (85)17/22 (77)28/33 (85)
52/72 (72)52/67 (78)22/31 (77)23/28 (82)24/34 (71)72/87 (83)
9/21 (43)9/22 (41)6/9 (67)
5/20 (25)11/22 (50)18/33 (55)
13/72 (18)5/70 (7)
5/31 (16)3/28 (11)7/34 (21)
18/87 (21)
Multivariate Analysis
ORR Odds Ratio* (95% CI); P Value
(n=157)
CR Odds Ratio†
(95% CI); P Value (n=129)
DOR HR for Relapse (95% CI); P Value (n=105)
Ven + R vs. Ven 1.14 (.43-3.02); .796.13 (2.44-15.44);
.0001.37 (.15-.89); .03
Prior therapies <3 vs ≥3 4.58 (1.62-12.91); .004 NS NS
Lymph node size ≤5 cm vs >5 cm NS 3.50 (1.39-8.84); .008 .36 (.15-.84); .02
11q, not deleted vs deleted NS 2.96 (1.04-8.43); .04 NS
17p, not deleted vs deleted NS NS .42 (.18-.95); .04
Age, continuous variable NS NS NS
Dose of Ven, >400 mg vs 400 mg NS NS 1.72 (.62-4.76); .29*Responders vs non-responders; †CR/CRi vs all other patients.
Roberts et al. EHA 2016. Abstract P209

Phase Ib - IBR+VEN+OBIN:Treatment Schema
C1 C2 C3 C4 C5 C6 C7 C8 C9 C10 C11 C12 C13 C14
Obinutuzumab 1000 mg IV
Ibrutinib 420 mg daily PO
Venetoclax (cohort dose) mg daily PO
Response assessed (CT + BMBx) –After Cycle 8– 2 months beyond end Cycle 14
Drugs initiated sequentially to limit risk for tumor lysis syndrome (TLS) All patients discontinue treatment after Cycle 14 Sequential cohorts of 3 underwent dose escalation to target venetoclax dose in Cycle 3 to
establish MTD of venetoclax in combination
Cycle = 28 days
Jones et al. ASH 2016, Abstract 639

Phase Ib - IBR+VEN+OBIN:Cycle 9 Treatment Response (N=12)
Patient ID Cycle 9 Response† Peripheral Blood MRDⱡ (%) Bone Marrow MRDⱡ (%)
Dose Level 1(venetoclax 100)
PR 0.00 0.40
PR 0.00 0.00
PR 1.70 0.50
Dose Level 2(venetoclax 200)
PR 1.00 8.00
PR 0.00 4.00
CR 0.00 0.20
Dose Level 3(venetoclax 400)
PR 0.00 0.00
PR 0.00 0.00
CR 0.10 0.05
PR 0.00 0.00
NR* -- --
NR* -- --
†IWCLL (2008) response; PR = partial response; CR = complete response; NR = not reachedⱡMeasured by four-color flow cytometry, reported as percentage (%) of events*All remain on therapy but had not yet completed 9 cycles of therapy
Jones et al. ASH 2016, Abstract 639

Venetoclax (ABT-199)
FDA approved: relapsed del(17p) CLL
Oral Bcl-2 inhibitor, potent monotherapy activity
Complete remissions in rel/ref CLL
MRD-negative CRs
Active in high-risk CLL: rel/ref CLL with del(17p) &
fludarabine-refractory CLL
TLS and neutropenia AE’s to monitor
Safely combined with rituximab and obinutuzumab
Phase III trial initiated in first-line

Management for “High-risk” Rel / Ref CLL
BTK-I-refractory / BTK/PLCG2-Mut / complex karyotypeVenetoclax (± CD20 mAb)
PI3K-inhibitor
Chemoimmunotherapy to de-bulk [non-del(17p)]
Allo-SCT
Del(17p) / TP53-Mut (BTK-I first-line)Venetoclax (± CD20 mAb)
Alternative BCR-inhibitor
Allo-SCT
BTK-inhibitor- or PI3K-inhibitor-intolerantAlternative BCR-inhibitor
Venetoclax (± CD20 mAb)

New Agents Changing Treatment for Patients with CLL
Agent Development Phase Sponsor
BTK inhibitorsIbrutinibONO-4059ACP-196BGB-3111
ApprovedPhase I
Phase IIIPhase I
AbbVieGilead / Ono
AcertaBeiGene
PI3KΥ/δ inhibitorsIdelalisibIPI-145AMG/ACP-319TGR-1202SAR245408 (XL147)
ApprovedRegistration Phase III
Phase IPhase IIIPhase I
Gilead SciencesInfinity Pharmaceuticals
AcertaTG Therapeutics
Sanofi
Syk inhibitorsEntospletinibFostamatinibPRT-2070
Phase IIPhase I/IIPhase I
Gilead SciencesRigel Pharmaceuticals
Portola
BCL-2 inhibitorVenetoclax (ABT-199) Approved AbbVie/Roche

CLL Treatment Directions
Untreated, high-risk – early intervention
First-line therapy
Fit CIT-eligible – IGHV-MutatedFCR-based with maintenance or Tx for MRD
Fit-IGHV-Unmutated & ElderlyBCR- / Bcl-2-inhibitor – sequencing and combinations
Second-line Therapy for active disease
Treatment (consolidation) for persistent disease on BTK-inhibitor (1st and later)
Richter’s transformation work-up and “novel treatments” program

THANK YOU!