Embed Size (px)
Citation preview

The Artificial Lung: Can It Be Realized?
William J. Federspiel, PhD
Whiteford Professor of Bioengineering
Professor of Critical Care Medicine
Director, Medical Devices Laboratory
McGowan Institute of Regenerative Medicine
University of Pittsburgh

Disclosure
William J. Federspiel, PhD
WJF is Co-Founder and Head of the SAB of Alung Technologies, in which he also holds equity. Portions of this talk cover the Hemolung ® Respiratory Assist System (RAS) and other technologies licensed or optioned by Alung from the University of Pittsburgh and invented in part by WJF.

Conclusion: It can be realized but …
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
We are about 20-30 years behind VAD technology
VADs Artificial Lungs
Implantable working unit
YesNo
Extracorporeal
Reliability Years Days-Months
Destination Therapy
YesNoICU
HemocompatibilityVery Good
~ cm2 contact area
Challenge~ m2 contact area
Technology Platform
Mostly Perfected In Infancy

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Vs
A ~ 140 m2
A/V ~ 2900 cm-1
~ 1 m VO2 ~ 210 - 3200 ml/min
A ~ 2.5 m2
A/V ~ 28 cm-1
~ 10-30 m VO2 ~ 150 - 250 ml/min
The Natural Lung Versus an Artificial Lung
The natural lung is a remarkable organ for gas exchange
Nature’s Technology “Our” Technology
Hollow Fiber Membrane Modules
Alveolar-Capillary
Microvascular Units

Current Artificial Lungs: ECMO Devices
Medical Devices Laboratory McGowan Institute of Regenerative Medicine

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Active rehabilitation / ambulation during pre-transplant respiratory support can improve post-transplant outcomes.
Where We Are Headed with Next Generation Devices
Focus has shifted towards new generation of respiratory assist devices that allow for easier ambulation.
Fully integrated and compact blood pump/gas exchange devices
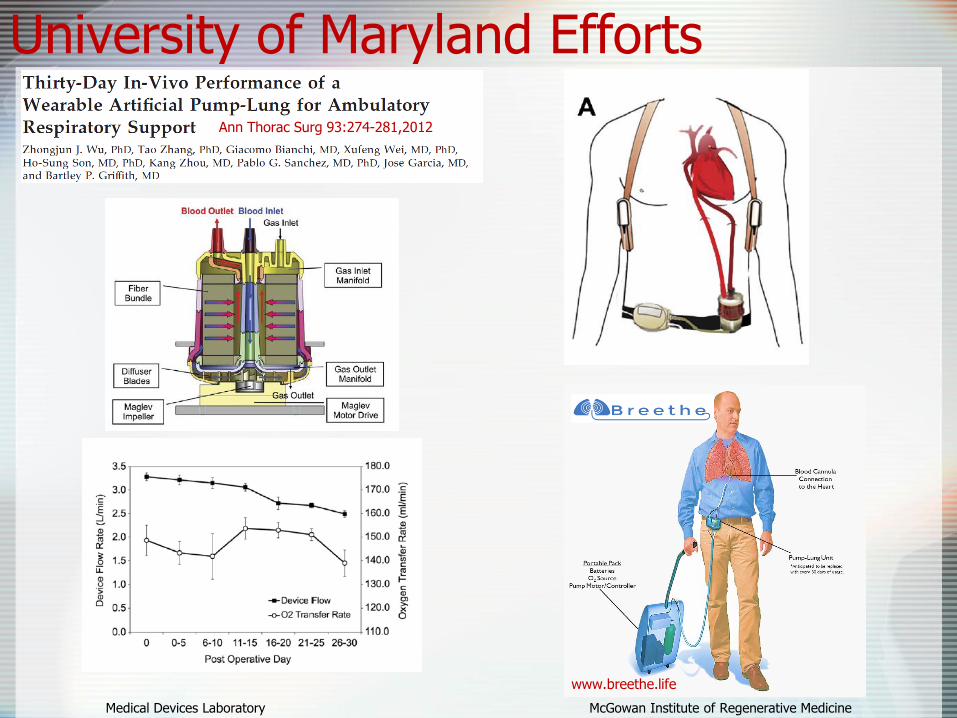
University of Maryland Efforts
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Ann Thorac Surg 93:274-281,2012
www.breethe.life

University of Michigan & CMU
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
ASAIO J,2017
• Uses right ventricle as pump
• PA to LA connection
• Compliance reduces load on RV
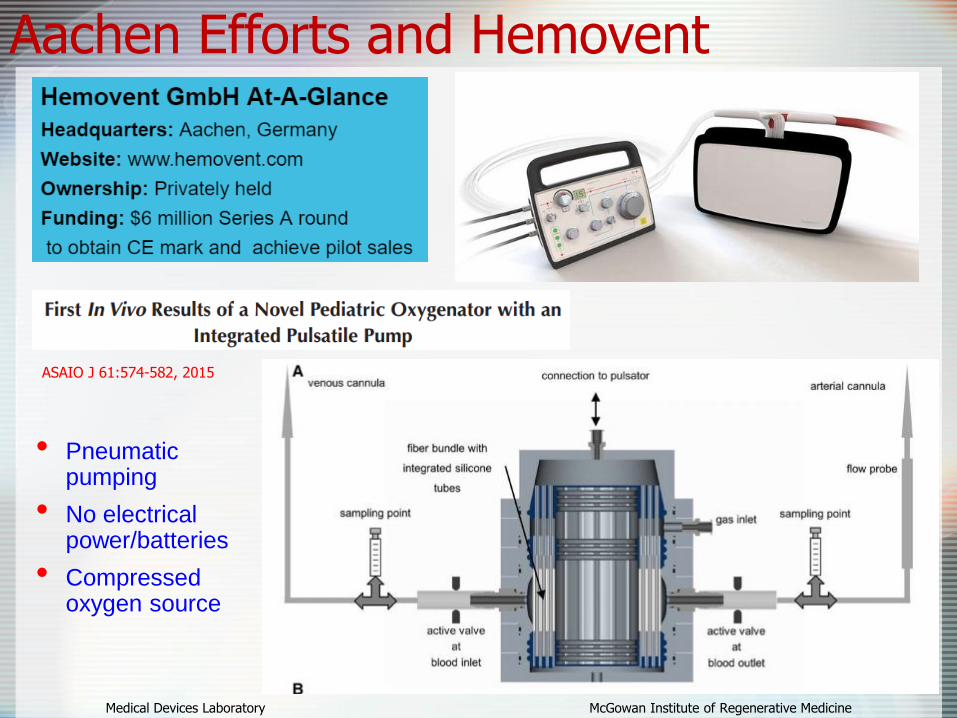
Aachen Efforts and Hemovent
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
ASAIO J 61:574-582, 2015
• Pneumatic pumping
• No electrical power/batteries
• Compressed oxygen source
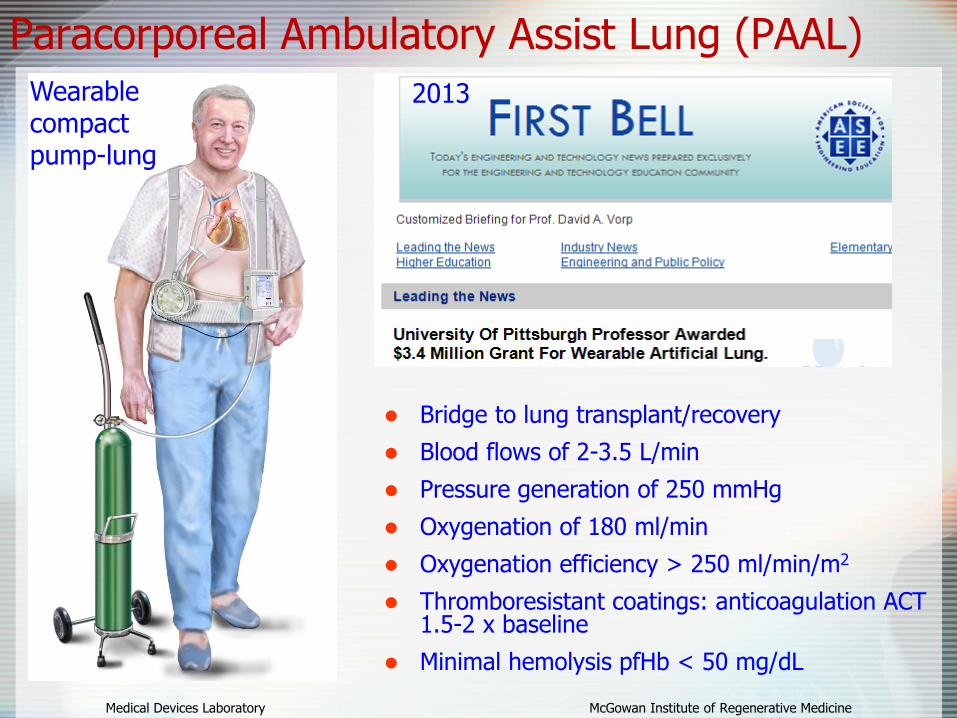
Paracorporeal Ambulatory Assist Lung (PAAL)
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Bridge to lung transplant/recovery
Blood flows of 2-3.5 L/min
Pressure generation of 250 mmHg
Oxygenation of 180 ml/min
Oxygenation efficiency > 250 ml/min/m2
Thromboresistant coatings: anticoagulation ACT 1.5-2 x baseline
Minimal hemolysis pfHb < 50 mg/dL
Wearable compact pump-lung
2013

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Basic Features of the PAAL System 27 Fr Avalon DLC
compatibility
PMP fiber with 0.65 m2
area; single step potting; bundle fabrication amenable to complete automation
Low gas flow resistance: uses positive pressure; no gas purge required
Pivot-bearing, CFD optimized pump
Controller Drive System
PAAL
UHMWPE Bearing
Ceramic Pivots
Inlet
Impeller
Fiber Bundle
Blood Outlet
Blood InletGas
Inlet
Gas Outlet
PumpImpeller
FiberBundleExit

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
PAAL In-Vivo Chronic Studies
Chronic 5-day studies in sheep
Oxygenation rates 105-155ml/min
Hemolysis < 20 mg/dL with no change from baseline
ASAIO J 2018

CO2 removal, rather than O2 delivery, can be the primary issue in therapy for acute respiratory failure
Chronic obstructive pulmonary disease
(COPD)
Acute respiratory distress syndrome
(ARDS)
• O2 requirements via non-invasive positive pressure ventilation
• Intubation & MV often necessary due to refractory hypercapnia
• Low tidal volume MV improves mortality (ARDSNet)
• Significant risk of hypercapnia and subsequent respiratory acidosis
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Avoid intubation and MV in aeCOPD (200-300K patients/year)
Protective ventilation in ARDS (100-150K patients/year)
Clinical Potential
ECCO2R: Extracorporeal CO2 Removal
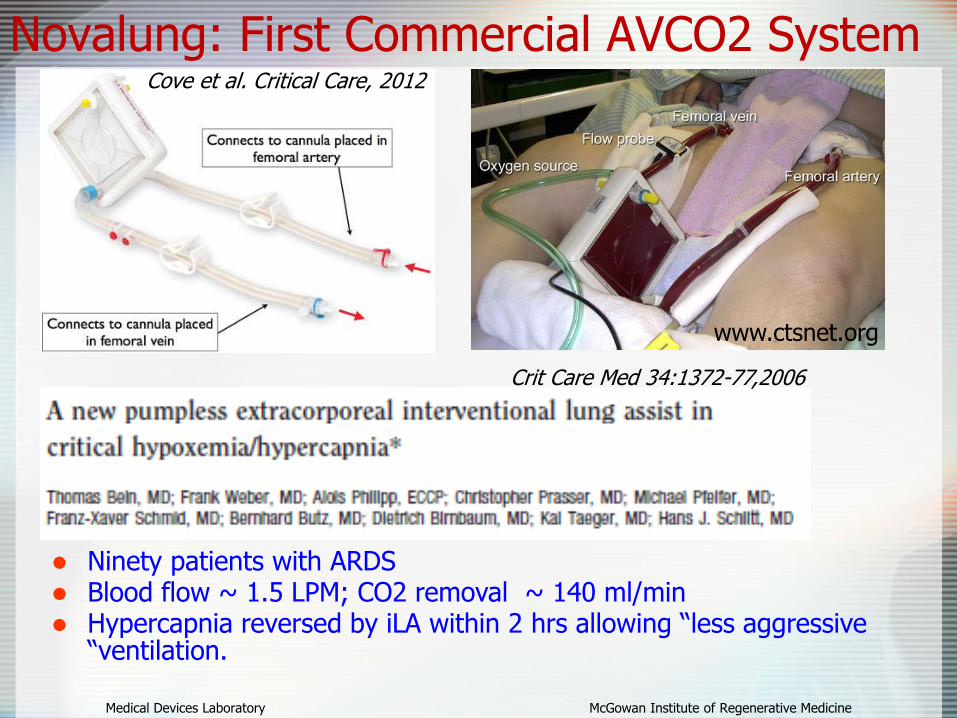
Novalung: First Commercial AVCO2 System
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Crit Care Med 34:1372-77,2006
Ninety patients with ARDS Blood flow ~ 1.5 LPM; CO2 removal ~ 140 ml/min Hypercapnia reversed by iLA within 2 hrs allowing “less aggressive
“ventilation.
www.ctsnet.org
Cove et al. Critical Care, 2012

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Compact, efficient hollow fiber module worn/placed externally
Small dual-lumen cannula (14-16 Fr) inserted in the venous circulation for blood flow
Blood flows of 250-500 ml/min for respiratory support (targeting 40-60% of CO2 production)
Rotating hollow fiber bundle for enhanced gas exchange
Self-pumping driven by rotating fiber bundle
Paracorporeal Respiratory Assist Lung (PRAL)*
“Respiratory Dialysis”
PRAL as envisioned in ~ 2002
*Pitt ECCO2R Efforts: ECCO2R to the Next Level
ASAIO J 51:773-780, 2005

Pittsburgh Start-Up: Alung Technologies
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Hemolung RAS(CE Mark 2013)
Hemolung Beginning US Clinical Trial
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Prospective, multi-center, open-label, randomized, controlled, 2-arm
Each arm will enroll patients with AE-COPD: 1) Failing NIV 2) Intubated and failing weaning
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
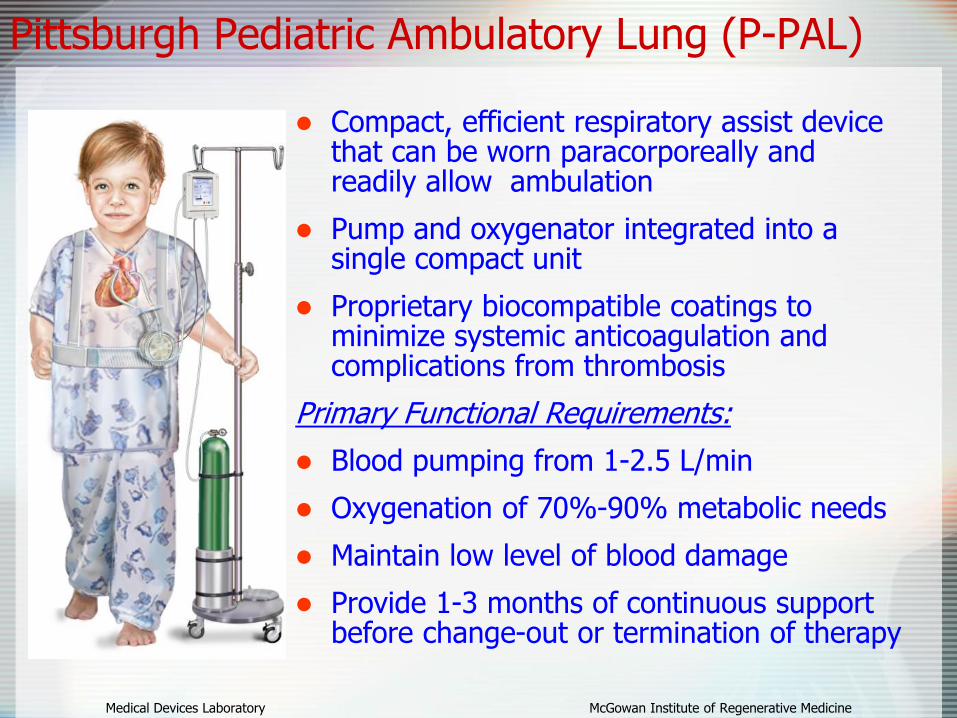
Compact, efficient respiratory assist device that can be worn paracorporeally and readily allow ambulation
Pump and oxygenator integrated into a single compact unit
Proprietary biocompatible coatings to minimize systemic anticoagulation and complications from thrombosis
Primary Functional Requirements:
Blood pumping from 1-2.5 L/min
Oxygenation of 70%-90% metabolic needs
Maintain low level of blood damage
Provide 1-3 months of continuous support before change-out or termination of therapy
Pittsburgh Pediatric Ambulatory Lung (P-PAL)

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Adult Vs. Pediatric Ambulatory Assist Lungs
P-PAL and adult PAAL pump-lungs utilize same/similar internal geometry and components.
Successful in vivo 5-day and on-going 30-day studies of PAAL; Acutein vivo studies of the P-PAL.
Pete Wearden: “If the P-PAL can have an important adult application, commercializing it will be much easier”

A Comprehensive Solution: ModELAS*
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
*Modular Extracorporeal Lung Assist System:“wearable” lung assist for adults and children
PediatricModELAS
(P-ModELAS)
AdultModELAS
A-ModELASFunction
Blood
FlowrateClinical Goal
Clinical Market
(NA/EU)
P-ModELAS
Pediatric O2
supply and CO2
removal
1-2.5
Liters/min
Bridge to recovery
(acute) or transplant
(chronic)
200-500
A-ModELASAdult O2 supply
and CO2 removal
2-3.5
Liters/min
Bridge to recovery
(severe ARDS) or
transplant (chronic)
20,000-50,000
A,P-
ModELAS
ECCO2R
Minimally
invasive CO2
removal
(respiratory
dialysis)
200-500
mL/min
Bridge to recovery
(ARDS, AE-COPD)
300,000-
500,000

Conclusion: Artificial lungs can be realized but …
Medical Devices Laboratory McGowan Institute of Regenerative Medicine
We are about 20-30 years behind VAD technology
VADs Artificial Lungs
Implantable working unit
YesNo
Extracorporeal
Reliability Years Days-Months
Destination Therapy
YesNoICU
HemocompatibilityVery Good
~ cm2 contact area
Challenge~ m2 contact area
Technology Platform
Mostly Perfected In Infancy

Medical Devices Laboratory McGowan Institute of Regenerative Medicine
Acknowledgments and Disclosure
• ALung Technologies is a Pittsburgh based medical start-up company.
• License agreement with the University of Pittsburgh covering portions of the technologies discussed today.
• Commercializing the Hemolung Respiratory Assist System
WJF is Founder, Consultant (Head of SAB) and Stockholder of:
• Medical Devices Laboratory: B. Frankowski, S. Madhani, R. Orizondo, A. May, R. Svitek
• U. Pitt.: J. D’Cunha, P. Wearden, W. Wagner
• Alung: S. Morley, L. Lund, J. Kimmel
• National Institutes of Health: Heart, Lung and Blood Institute • Commonwealth of Pennsylvania• National Tissue Engineering Center (NTEC)• McGowan Institute for Regenerative Medicine
People:
Funding:

The End…..





























