Embed Size (px)
Citation preview

Address of CorrespondenceDr. Fessy Louis T. Editor KFOG Journal , CIMAR COCHIN, Thykavu Stop, NH 17, Cheranalloor, Edappally,
Kochi -682 034, Kerala, INDIA Mob: 09846055224 E-mail: [email protected]
President:Dr.V.P.Paily
E-mail: [email protected]
Immediate Past president Dr.Narayanan T.Vice President Dr. NeenaThomas
Vice President Elect Dr.Ajith SJoint Secretary Dr. Sangeetha Menon
Treasurer Dr.Rajalakshmi JanardhananJournal Editor Dr. Fessy Louis
Committee Chair personsMaternal & Foetal Medicine Chair Dr.Ambujam
Academic chair Dr. V. Rajasekharan NairElect Dr. P.K.Syamala Devi
Adoloscent Chair Dr.V.K.ChellammaElect Dr.Kunjamma Roy
Reproductive Health Chair Dr.K.K.GopinathanElect Dr.Philip Abraham
Oncology Chair Dr.Sumangala DeviElect Dr.Chithra Thara
Reasearch Chair Dr.P.K.SekharanElect Dr.Nirmala .C
Laison Officer Dr. V. Rajasekharan Nair
Secretary GeneralDr. T. Jayandhi RaghavanE-mail: [email protected]
KFOG
OFF
ICE
BEAR
ERS
FOR
THE
YEA
R 20
11-12
Vol: 5 No: 3 December 2011
Web:www.kfogkerala.com
CONT
ENTS
The worst way to miss someone is to have them sitting right next to you & you nevernotice it. Knowledge is simillar, the worst is to miss it when there are lot of chances toaquire it all around you. We should realise it and strive to achieve it through the perusalof journals, books, internet etc .There are lots of people willing to share their knowledgeand experience by contributing articles and publishing their studies. I earnestly solicityour cooperation in contributing articles so that we may all benefit from your knowledgeand experience. Looking forward to receiving them at the earliest.
Wishing you happy readingand prosperous New year 2012
Design: Smritidesign Printing: Anaswara Offset
President’s Message 02
Secretary’s Message 02
ADOLESCENT OVARIAN TUMOURS
Dr. Chellamma V K 03
PREMENSTRUAL SYNDROME-
AN UPDATE ON
Dr. Roza Olyai 06
EVALUATION OF
THE INCONTINENT WOMAN
Dr.Karthik Gunasekaran 11
HOW TO START
LAPAROSCOPY PRACTICE…
Dr. Biju. P 12
INTRAUTERINE TRANSFUSION –
THE PROCEDURE SIMPLIFIED
Dr. Bijoy Balakrishnan 14
Dr. Fessy Louis T

2 www.kfogkerala.com
Secretary’s Message
President’sMessage
Cont. page-3
Message from the PresidentDear colleagues,
Greetings from KFOG.As 2011 is coming to a close, it is time to review
what we had been doing and plan for the next year. Nodoubt 2011 had been a busy year for us. We focused onvarious issues topical and relevant to our practice oftenbrought to lime light by the media. The escalatingcesarean section rate in our state is a matter of concernfor all of us. An initiative to address this issue andpromote safe vaginal deliveries was launched on 16th
Oct 2011 at Ernakulam. We partnered with NRHM anddiscussed various steps that can increase the vaginaldelivery rate. However, it is obvious that high CS ratescannot be controlled by obstetricians alone. The mostimportant step is to bring about attitudinal changeamong the public. The administrators(in private as wellas government hospitals) have to be convinced thatunless facilities for doing CS are provided round theclock, the obstetrician will be forced to do cesareansection during the regular working hours when thesefacilities are available rather than give a full trial forvaginal delivery which may extend into the night.
There are other trends in our specialty which needtimely intervention. Hysterectomy is under the limelight. There is no doubt that indications and route ofhysterectomy need to be under constant monitoring.With the advent of levonorgestrel intra uterine system,the need for hysterectomy for dysfunctional uterinebleeding has drastically come down. However, fibroidsand adenomyosis still remain valid indications. Afterthe euphoria for keyhole hysterectomy has settled down,it is time to review the no hole(or natural orifice)hysterectomy (vaginal hysterectomy). KFOG hadalways supported vaginal route for hysterectomy andhas scheduled workshops to promote nondescentvaginal hysterectomy. Such workshops are coming upin the near future at Kollam and Ernakulam. The annualvaginal surgery workshop at Mother hospital (V Surge)is scheduled for 22nd January 2012.
Very best wishes from KFOG secretariat! It gives me great pleasure in addressing ouresteemed members in this third issue of journal forthe year 2011. After a dynamic and busy schedule ofactivities we are towards the fag end of the year . Lotof achievements is there to feather the cap of KFOGduring this year. KFOG has succeeded to form a teamof trainers for the EMOCAL programme includingeminents from all parts of Kerala - the 2nd step toupgrade the standards of Obstetric Care, after ourPrestigious CHC Obstetric up gradation Project,Kerala 2010 and Nursing assistant trainingprogrammes. The forthcoming training programs onEMOCAL in different centers are aimed to improveour ability to manage any obstetric condition in anysituation and anywhere in Kerala. Thus the dream toreduce the Maternal mortality rate and Infant mortalityrate at par with the developed countries could beachieved in near future.
Further to fulfill these dreams, the Ambulanceservice in the whole state also should improve. Weshould appreciate our state Government and NRHMimplementing the emergency ambulance service inKerala which was implemented on May 19th 2010 andthe results of this facility has started coming. Firstimplemented in Thiruvananthapuram, and expandingto other parts of Kerala, could achieve a lot and savedmany lives. The team behind this programme is veryenthusiastic and sincere. KFOG take this opportunityto congratulate the officials behind this programmeand staff working in the Call center at Techno Park,TVM for coordinating the service effectively. TheMalayalam title – “AYUSSINTE KAVALKAR” reallysuites to them and wish “108” will be easily accessibleto all citizens of our state. They have provedthemselves that such efficient facility at par withwestern countries is not a dream for our populationbut possible if there is a will and sincerity.
Let us work together and achieve the best possible inour OBG specialty services.
Jai KFOGDr. T. Jayandhi Raghavan
Secretary General

3www.kfogkerala.com
Cont. from page-2
3www.kfogkerala.com
IntroductionOvarian tumours are relatively rare in adolescent
age group. Most ovarian tumours in adolescents arebenign but possibility of malignancy is high. 1%of all neoplasm occurs below 17 years and of these3% are ovarian neoplasms (Young & Miller 1975).65% of ovarian tumours in adolescents are benignand 35% having malignant features . According to astudy of incidence of ovarian tumours below 20 yearsin IMCH, Medical College Calicut showed 76%benign tumours , 35% germ cell tumours and 47%epithelial tumours (Simi 2002). Management ofovarian tumours in young age group is a challengefor gynaecologists as the incidence of malignancyis high and the need for preservation of fertility
Pathology of ovarian tumours in adolescents
These may be functional cysts, epithelialtumours, germ cell tumours or sex cord stromaltumours. Benign neoplasm or functional are the mostcommon ovarian masses in this age group.Functional cysts can present as follicular cyst,corpus luteal cyst , and theca lutein cysts. Functionalcysts are benign, unilocular, usually will resolve within 4-8 weeks. But rarely complications likespontaneous rupture, haemorrhage, or torsion mayoccur which may need intervention.Ultrasonographyshould be done to differentiate from ectopicpregnancy, endometriosis and neoplasms.
Benign ovarian tumours
Mature cystic teratomas (dermoid cyst) are the
Auditing Maternal Mortality had been our missionsince the inception of KFOG. In fact I am jotting downthese notes on the way to Trivandrum to discuss the issuewith the Director of Health Services and District MedicalOfficers at their monthly meeting. Whenever a maternaldeath occurs, the reporting form A&B and photo copiesof anonymised case records have to be sent to the Statecoordinator at the address:
Dr.V P Paily, Vakkanal House, East Fort, Thrissur-5,680 005
Tel No 0487 2336222.The next edition of “Why Mothers Die” covering the
years 2006,07,08,09 is to be published shortly. Similarly,
Dr.Rajasekharan Nair is working on the next edition ofprotocol book.
The next all Kerala Conference at Kottayam on Feb10,11, and 12th will be the occasion to meet once againand exchange views and experiences.
Please give us your suggestions and comments so thatKFOG can continue to help you in professionaldevelopment.
Jai KFOGV P PailyPresident
Dr. Chellamma V. K, Professor of O&GIMCH, Medical College, Calicut
Adolescentovarian tumours

4 www.kfogkerala.com
most common in adolescents which maycontain tissue derived from all three germcell layers, with ectodermal derivatives such as teethand hair. Patients with mature cystic teratomas areusually asymptomatic unless complications such astorsion or rupture occur. Malignant transformationoccurs in 0.17% to 2% of benign teratomas.Functional teratomas occur in 5% to 20% of benignteratoma and most commonly presence of thyroidtissue. Struma ovarii with thyroid tissue is seen inmore than 20% of benign teratomas with signs andsymptoms of thyrotoxicosis. The others are epithelialtumours like serous cystadenoma and mucinouscystadenoma. The incidence may be 28 % at 15-17 age group and they are usually of low malignantpotential. For stromal tumors, fibromas are commonin children and adolescent, account for 0.5% to2% of all ovarian tumor in this age group .Endometriosis also may occur in adolescents girlspresenting with severe dysmenorrhoea who do notrespond to simple NSAIDS and OCPs
Malignant ovarian tumors
Ovarian cancer, specific to children and adolescentpatients include germ cell tumours and juvenilegranulose cell tumors. 65% of ovarian cancers inadolescents present with acute or sub-acute painassociated with torsion or rupture of cyst.Malignant germ cell tumor exhibits an extremelyrapid growth pattern.
Germ cell tumours
Malignant germ cell tumors includedysgerminomas, endodermal sinus tumors,embryonal carcinomas, mixed germ cell tumors,chroriocarcinomas, and immature teratomas.Dysgerminoma are the most common malignanttumour in adolescents and bilateral in 10-15% ofcases. Dysgerminomas can be associated withgonadal dysgenesis and androgen insensitivity.Therefore, premenarchal patients should be identifiedfor karyotype. Immature teratomas are the secondmost common malignancy and account for 20% oftumors in the first two decades of life. These tumors
are normally unilateral but are oftenassociated with a mature cystic teratoma in
the contralateral of ovary and 30% deaths occur withthese tumours. Endodermal sinus tumour is thethird most common malignancy which is higlymalignant and often unilateral. It is also called Yolksac tumour. There is rapid growth and spread andpatient dies with in 2 years in advanced cases (Ayhan2005) Pure ovarian choriocarcinoma is extremelyrare in adolescents. Embryonal carcinomas are anextremely rare, generally large (10-15 cm), unilateralmasses and occur at mean age of 14 years.
Sex cord stromal tumours
Malignant stromal tumours include granulosacell tumour and Sertoli-Leydig cell tumour.Granulosa cell tumour accounts for < 7% of allovarian tumours with low grade malignancy andsecretes estrogen and hence presents symptoms andsigns of precocious puberty in 80% of patientsSertoli-Leydig cell tumour produces androgenscausing virilization in 70-80% of cases. Deepenedvoice, hirsutism, clitoromegaly, breast atrophy, andacne are common signs and symptoms.
Tumour markers
Tumor markers are extremely useful in thedifferential diagnosis, follow up, the patient’sresponse to therapy and to monitor for recurrence ofdisease. CA-125 was the first widely availablemonoclonal antibody against epithelial ovariancancer. The specificity of CA-125 is poor. Alphafetoprotein is the reliable marker for endodermalsinus tumors, embryonal tumors, mixed germ celltumors, and rarely by immature teratomas.Similarly, human chorionic gonadotrophin (hCG) isproduced by embryonal tumors andchoriocarcinomas. Inhibin is a reliable tumor markerfor granulosa cell tumors. Lactic dehydrogenase(LDH) level is elevated in many cases ofdysgerminoma

5www.kfogkerala.com
Clinical presentation
Patient may be asymptomatic or may present withabdominal discomfort & pain, abdominal swellingand hormonal effects Abdominal and per rectalexamination may reveal ascitis or the mass.
Diagnosis
The most important diagnostic method is USGalong with doppler study for exact size, location,nature of the tumour like cystic, solid or complex,presence of ascitis and metastasis. The othermethods are CT/MRI for metastasis to lymph node,liver, kidney, brain etc, abdominal and chest X rayand tumour markers like Ca 125, AFP, HCG, CEA.
Management
Functional cysts may be observed and ifpersisting, treatment with OC pills will be sufficient.
For benign ovarian neoplasms, conservativesurgery is the choice like cystectomy, ovariotomyor salpingo oophporectomy. For malignant tumours,staging laparotomy should be done after proper pre-operative evaluation .The surgical approach shouldaim to preserve fertility and ovarian function.
Surgical management of germ cell tumour
Stage 1
• Unilateral salpingo-oophorectomy
• Biopsy or wedge resection of contra lateralovary not required
• Complete staging
• Follow up
Stage 2
• TH with BSO
• Young patient- USO
• Adjuvant chemotherapy
Stage 3 and 4
• TH with BSO with removal of gross tumour
• Extensive tumor chemotherapy beforedebulking surgery
• Young patient- USO and chemotherapy
Chemotherapy
Chemotherapy for malignant germ cell tumorsshould be with combination chemotherapy withbleomycin, etoposide, and cisplatin. For malignantsex cord stromal tumors, cisplatin-basedchemotherapy may be required in those withmetastasis or recurrent disease.
Pregnancy and germ cell tumours
Ovarian tumours may coexist with pregnancyas it occurs in young patients. If present dermoidcysts are common and dysgerminomas may be seenin 1-2% of patients. Management is by surgicalstaging . Stage 1 tumour is removed intact andpregnancy is allowed to continue. In advanced casescontinuation depends on gestational age.Chemotherapy can be given in the same dosagewithout detriment to fetus
Conclusion
Although ovarian tumors are rare inchildhood and adolescence, the detection of theselesions is worrisome to patients, her families, andphysicians as the incidence of malignancy is higher.Early, and correct diagnosis could be reached byphysical examination, imaging, tumor marker,pathologic examination (including frozen section)and should be followed by individual therapy.However, preservation of fertility with conservativesurgery is essential part in the management.

6 www.kfogkerala.com
Premenstrual syndrome (PMS) can be defined asa condition which causes distressing physical,behavioral and psychological symptoms, in theabsence of organic or underlying psychiatric disease,which regularly recurs during the luteal phase of eachmenstrual cycle and which disappears or significantlyregresses by the end of menstruation. Almost 95 percent of women will experience mild physiologicalsymptoms prior to menstruation, however around fiveto eight per cent experience severe symptoms suchthat they cause considerable disruption to their lives.Severe PMS is also termed Premenstrual DysphoricDisorder (PMDD) by the American PsychiatricAssociation in the DSM-IV classification and hasstrict diagnostic criteria.
The aetiology of PMS remains poorly understood.The absence of PMS before puberty, duringpregnancy and after the menopause highlights the roleof cyclical ovarian activity in its pathogenesis.Women with PMS appear to produce the same levelsof gonadal hormones as women without PMS andtherefore it has been suggested that PMS may be dueto a differential sensitivity to circulating hormonemetabolites rather than abnormal hormone levels. Theneurotransmitters serotonin and gaba-aminobutyricacid (GABA) have also been implicated as potentialpathways through which abnormal responses tohormone levels may occur.
Assessment and diagnosisAccurate diagnosis of PMS is essential. A careful
history should be sought, specifically for a cyclical
nature of the symptoms. Premenstrual symptoms maycommence up to two weeks prior to menstruation andresolve by the end of menstruation. To make thediagnosis there should be a symptom free intervalprior to ovulation however this may often becomplicated by physical or psychiatric co-morbidities.
PMS can cause a wide range of psychological,behavioral and physical symptoms (see table 1). Insevere PMS some form of functional impairment,such as an inability to interact socially orprofessionally, will be evident.
Any underlying conditions as suggested by thehistory should be excluded and managedappropriately. Common conditions which may causediagnostic confusion include depression, generalizedanxiety disorder, stress, polycystic ovarian syndrome,hypothyroidism, and alcohol or drug abuse.
Table 1. Symptoms associated with PMS
Psychological Behavioral Physical
Mood swings Withdrawal Bloating
Tearfulness Lack of control Pelvic pain
Irritability Reduced concentration/ Breast tenderness
Depression cognitive ability Headaches
Anxiety Poor sleep Food cravings
Lethargy
Weight gain
PREMENSTRUALSYNDROME-
an update on managementDR. ROZA OLYAI
Chairperson Adolescent Health Committee FOGSI
Director Olyai Hospital, Gwalior MP

7www.kfogkerala.com
ManagementOnce the diagnosis has been confirmed,
several management options are available, many ofwhich can be used in the primary care setting.Treatments used are often unlicensed however theiruse is justified when they are of proven efficacy andsafety.
A potential treatment strategy for PMS is shownin box 1.
All women should be given dietary and lifestyleadvice on measures which may help reducesymptoms. The prevalence of PMS is increased inobese women and those who take less exercise.Weight loss and exercise have been shown to reducePMS symptoms and therefore should berecommended. Stress reduction and low glycaemicindex diets are also likely to be beneficial althoughno studies have examined these measures directly.Cognitive behavioral therapy has been shown toimprove PMS symptoms and should be consideredin all women.
Serotonin has been implicated in the pathogenesisof PMS and is thought to be associated withsymptoms such as irritability and low mood. Selectiveserotonin reuptake inhibitors (SSRIs) have been usedfor many years in the management of PMS. A recentmeta- analysis has shown SSRIs (fluoxetine,paroxetine, sertraline, citalopram) are effective inreducing premenstrual symptoms in moderate orsevere PMS. They have been shown to reducephysical, functional and behavioral premenstrualsymptoms and improve quality of life. SSRIs can begiven either continuously or in the luteal phase only(i.e. days 15-28); both regimens appear to be ofsimilar efficacy. The advantages of luteal phasetreatment include avoidance of dependency and thatthe regimen is often more acceptable to womenconcerned about the stigma of using treatmentsusually associated with psychiatric conditions. Somedata exists to the support the use of the SNRIvenlafaxine however further large scale studies areneeded.
Hormonal treatmentHormonal treatment aims to suppress ovulation
and stabilize hormonal fluctuations throughout themenstrual cycle.
· COCPThere is increasing evidence that new
generation COCPs are effective at reducing PMSsymptoms. The progesterone component of the COCPhas been held responsible for the failure of olderCOCPs to improve PMS as a common side effect ofprogestogens is PMS-like symptoms. The newprogestogen drospironone, contained in thepreparation Yasmin, has anti-mineralocorticoid andanti-androgenic properties, which may help avoidprogestogenic side effects such as bloating andirritability. The benefit of Yasmin over placebo hasbeen demonstrated for PMS symptoms in a smallrandomized trial however convincing, large scale datais lacking.
A further advance has been the development ofYaz, which also contains drospironone, but in a 24/4regimen, in contrast to the traditional 21/7 regimens.The shorter hormone free interval is associated withmore profound follicular suppression and more stablehormone levels. Two prospective randomized placebocontrolled trials have demonstrated the efficacy ofYaz in PMS and it is now licensed in USA fortreatment of PMDD. This drug is also available nowin India.
·Estrogen and progestogen therapyPercutaneous hormone replacement therapy in the
form of estradiol implants or the transdermal patchhas been shown suppress ovarian activity andimprove PMS symptoms. Suppression of ovulationusually requires the use of higher doses of estradiolthan is used in post-menopausal HRT, for example,100mcg estradiol patch.
In non-hysterectomised women, estradiol shouldbe given in combination with a progestogen. Cyclicalprogestogenic opposition (10-12 days per cycle) isrequired to protect against endometrial hyperplasia.Unfortunately however, progestogens commonlyresult in worsening of PMS symptoms and thereforecareful consideration should be given to this elementof HRT. Fewer side effects are seen with bioidenticalprogestogens (eg Utrogestan), the LNG-IUS orvaginal preparations such as cyclogest pessaries orcrinone vaginal gel.

8 www.kfogkerala.com
Dr Lola felicitating Dr Revathy Janakiram & Dr Vidya Thobbi during CMEon perimenopausal bleeding at Thrissur.
Health Education Project for youths at Calicut
Inauguration of TOGSICON by Medical UniversityVice Chanceller Dr.Mohandas at Thrissur
Annual, CME at Kollam
Dr. V.P. Paily (President) addressing theKFOG Exce. Committee Meeting at Alleppy
Book on carcinoma cervix edited by Dr Chitrathara released byDelhi health minister Dr A K Walia during AOGD
Dist Panchayath President Mr Eldo Kunnappally, with Dist collector Sri Sheikh Pareeth inaugurating the SLP at Cochin
cancer detection camp conducted in collaboration with Malabar cancersociety at all women’s co-operative society GAICOS at Kannur

9www.kfogkerala.com

10 www.kfogkerala.com
There is no evidence to support theuse of synthetic or naturalprogestogens alone in themanagement of PMS.
·GnRH analoguesSome women will not respond to
the above measures and at this stagereferral to specialist services shouldbe made. Inadequate response totreatment may be due to dueincomplete cycle suppression. GnRHanalogues may be considered the nextline treatment and can be used tocompletely suppress the ovarianactivity and are of proven efficacy inthe treatment of severe PMS. If GnRHanalogues are used for longer than sixmonths they must be used incombination with ‘add-back’ estrogenand progestogen HRT to avoidsymptoms of estrogen deficiency andits detrimental effects on bone density.Although the addition of add-backHRT has not been shown to reducethe efficacy of GnRHa in a smallproportion of women it may lead torecurrence of their cyclical symptoms,in which case continuous tibolone isan alternative option. For long termGnRH use, yearly assessment of bonedensity should be undertaken.
· Surgical optionsFor women with severe PMS
hysterectomy and bilateraloophorectomy will obviously providepermanent cycle suppression. Forthose with severe PMS who havecompleted their families it can be alife changing procedure. It is notwithout its risks and should only be
considered in women who have demonstrated a response to GnRHanalogues. Following the procedure, HRT should be given in womenbelow the age of 50 to avoid the effects of estrogen deficiency.Estradiol can be administered via implant, orally or transdermally.Consideration should also be given to testosterone replacement,especially if suffering from symptoms of lethargy and low libido.
ConclusionsSevere PMS can cause significant impairment to daily
functioning and is often poorly identified and managed. Althoughthe underlying aetiology is not well understood a number oftreatments with demonstrated efficacy exist. Lifestyle andcomplementary therapies have an important role, often incombination with psychological or hormonal treatments. Despiteadvances in treatment options, a small percentage of women willstill benefit greatly from surgery management.
Fig. 1 Management strategy for PMS

11www.kfogkerala.com
IntroductionUrinary Incontinence (UI) is a highly distressingsocial problem affecting mainly women. The mostcommon types of Incontinence are Stress , Urge,Mixed , Functional and Neurogenic. Fistulas andectopic ureters can be causes of extraurethralincontinence. Though highly prevalent, UrinaryIncontinence is underdiagnosed and underreported.
EvaluationThe goals would be to identify common anduncommon forms of incontinence, impact ofincontinence on quality of life, identify other pelvicfloor conditions requiring treatment, etiologicalfactors and prognostic indicators.
History and PhysicalA thorough Urogynecological history including thepatients age, obstetric history, type of incontinence,frequency of episodes and Lower Urinary TractSymptoms is elicited. History of previous surgeries,pharmacological agents, micturition history andmodifiable risk factors like smoking are asked for.
Physical exam should be done with a comfortablyfull baldder and should include physical, pelvic andneurological examination. The bulbo cavernous / analwink reflex and anal sphincter tone should beassessed. Vaginal exam should look for SUI, Prolapse,Urethral Hypermobility and presence of diverticulum. The tone, symmetry and strength of contraction ofpelvic floor muscles should be checked. A coughstress test to check for the presence of SUI ismandatory and is done with the bladder filled to at
least 300ml. In women with prolapse, the prolapseshould be reduced and checked for occultincontinence.
Voiding Diary
Voiding Diary is a useful tool for measuring theseverity of incontinence. A 3day diary will reveal typeof incontinence, drinking habits and help identifycauses of nocturia. It also helps in evaluating responseto treatment.
Post Void Residual
Valuable screening test for bladder function,especially when combined with Uroflowmetry.Abnormal values may warrant repetition of test.
Other tests.
Urine Analysis, Blood Urea nitrogen , SerumCreatinine should be done as routine. Urine cytologyand Cystoscopy should be done in patients withmicrohaematuria. Urodynamics is reserved for MixedIncontinence, Neurogenic problems and wheneversurgery is contemplated.
ConclusionA great no of women suffering from UrinaryIncontinence remain undiagnosed. These womensuffer in silence. It is imperative that primary carephysicians understand the impact incontinence hason a woman’s quality of life. Basic evaluation is amust learn for every practicing Gynaecologist.
Evaluation ofTHE INCONTINENT WOMAN
Dr.Karthik Gunasekaran, Chennai

12 www.kfogkerala.com
How to start
laparoscopy practice…
Laparoscopy is the common surgical approach formany gynecological surgical procedures now a days.Non Availability of skilled gynecologists is the mainproblem in many areas. Most of the hospitals in Indiagynecological laparoscopy surgeries are done byeither general surgeons or doctors of other specialties.It is because of lack of trained gynecologist andgynecologist’s lack of interest in learning laparoscopy.
I personally don’t agree with general surgeonsdoing gynecological laparoscopic infertility surgicalprocedures.
To start a laparoscopy practice one need to dedicatelot of time for practicing safe surgical approach.Constant training, assisting cases and observation arethe main important aspects of improving skill ingynecological laparoscopy. Most of the teachinginstitutes in India don’t have proper laparoscopicinstruments. Most of the gynecologists have onlytheoretical knowledge on laparoscopy.
Before starting laparoscopic surgery practice thesurgeon should be very familiar with abdominal-pelvic anatomy and thorough knowledge of usinglaparoscopic instruments and different energy sourcesused for surgery. Most of laparoscopic accidentsoccurs due to lack of proper knowledge in basicsimple steps .
Hand to eye coordination- If surgeons don’t havegood hand to Eye coordination, while doing evenminor procedures one may land up in unimaginablecomplications. Good surgeon should always be a goodcamera man also; Proper knowledge on using 0 degree
and angulated telescope is main factor in successfulsurgery.
Instruments: surgeon should know how toassemble and dismantle the instruments and cleaningthe instruments and even sterilizing the instruments,and which cable connects to what instruments.Knowledge on Proper settings of current flow andgood quality cautery are other important factors.Never depend on your staff nurses on all these matters.Many Indian manufactured instruments are in marketnow a day, but most of them are of poor quality .itsalways better to have good set of imported instrumentswhile starting practice.
One experienced surgeons can operate with anyinstrument but a beginner needs a good set of properinstruments. Compromising on instruments may leadto spoiling your carrier and loosing your patient’slife.
Selection of cases in initial carrier is anotherfactor. Never try to operate complicated cases in thebeginning. Start always with simple straight forwardcases, non scared abdomen, average built patient,good experienced anesthetist and good operationtheater table which gives you to good trendelenburghelps you in comfortable surgery.
Steps to be followed before doing a case:
Check availability of carbon dioxide cylinderincluding spare one. Instruments are properlysterilized and your CO2 insufflators and camera unit,light sources are working properly. Be calm and quiet.Never be panic and scream at your assistants. The
DR. BIJU.PSBM Hospital, Karunagappally, Kollam

13www.kfogkerala.com
moment surgeon start shouting your assistantslooses confidence and they may not able dothe steps what they do routinely. Be prepared forconventional technique. Speed in surgery comes withexperience. You find there is no progress in a surgicalstep you doing for half an hour to one hour, its betterto convert to open technique. Never be hesitant indoing that. Never try heroic steps in the beginninglike dissecting lymph node or lateral pelvic walldissections. Seeing Surgeons doing these steps inlaparoscopic workshops one beginner may temptedto do the same, but one should know that they haveattained these skills by doing thousands of cases overyears. Never be hesitant to clarify your doubts byconsulting an experienced gynecological laparoscopicsurgeon.
Good knowledge in open surgery technique is otherfactor. If you cannot complete procedure bylaparoscopically one should know how to completethe steps by open laparotomy.
Once you had put the primary trochar visualinspection of structures at 360 degree to rule out any
injuries and all abdomino- pelvic organs arenormal. Same should be done after
completing the surgery also. Identifying and repairingthe visceral and vascular
Injuries are the important step to avoid sleeplessnights for surgeons. Complications can be avoidedby doing surgery very carefully and with experience..Laparoscopy is an instrument dependent surgicaltechnique.
Laparoscopy is a team effort. good assistant andcamera holding person and an experienced anesthetistare important team members .Make sure all areproperly set before starting a cases ,and doinghomework by seeing videos of experts in whichparticular surgery you are planning to do . Never mixobstetrics practice and laparoscopy practice together.To become a good laparoscopic surgeon one has todedicate lot of time in the beginning. One can dobasic laparoscopy by attending 15 days training. Butto do advanced laparoscopic surgeries long termtraining and attending laparoscopic workshopsconstantly are necessary.
13www.kfogkerala.com
AKCOG -201234 th
ALL KERALA CONGRESS OFOBSTETRICS & GYNAECOLOGY
10th, 11th & 12th Feb 2012Countour Convention CentreChanganacherry, Kottayam,
Workshop :
Infertility Workup Safe Obstetric Practices
E-mail : [email protected]
International Faculty :Dr. Sir Sabaratnam Arulkumaran
Dr. Peter Brinsden
www.akcog2012.com

14 www.kfogkerala.com14 www.kfogkerala.com
Rh antibodies were identified as the cause of anemiaway back in 1941 and by 1961 hemolytic anemia becamethe first treatable fetal disease after liley characterized itsnatural history and then successfully transfused ill fetus’sintraperitonealy with adult RBC’s. Mari etall in 2000demonstrated that moderate to severe anemia could beidentified non-invasively by measuring the peak systolicvelocity of the middle cerebral artery; a finding whichrevolutionized fetal surveillance in Rh isoimmunisedpregnancies.
PathophysiologyWhen RhD positive fetal cells enter the maternal
circulation as a result of pregnancy related events suchas miscarriage / delivery, anti D is formed. Theadministration of RhD immune globulin in theseinstances is effective in preventing the formation ofanti D in more than 99% of cases. However in therare case of inadvertent omission / improper dosingthe patient may become sensitized to the RhD antigen.These maternal antigens then cross the placenta insubsequent pregnancies and attach to RhD positivecells of the fetus resulting in sequestration anddestruction of these cells in the fetal spleen.
ScreeningCurrent guidelines for management of Rh -ve
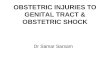
women are focused on prevention ofisoimmunization. An ICT should be done for all Rhnegative women at first contact and then repeated at28 weeks. If ICT is positive then patient is seriallyfollowed up weekly using the PSV of the MCA. TheMCA can be imaged by color / pulse Doppler in thetransverse plane of the fetal head obtained at the baseof the skull. In this plane the proximal and distalmiddle cerebral arteries are seen in their long axis,with their course almost parallel to the ultrasoundbeam. As a result of which the insonating angle is 0and the measured velocity accurately depicts the truevelocity of blood in the vessel. The MCA is assessedjust as it exits from the circle of Willis. Once the
Intrauterine Transfusion –the procedure simplified
PSV of MCA is greater than 1.5mMOM fetaltransfusion is done. As a rule of thumb if the PSV ofMCA is greater than 2 times the GA in weeks it canbe taken as greater than 1.5 MOMs.
Picture of MCA PS
Steps for transfusionMaterials and Equipment-A good 2D USG machine with Doppler facility.-20 G spinal needle.-3way cannula.-20cc syringe.-O negative CMV negative, irradiated packed
cells with a haematocrit of 80.-Pancuronium-Insulin SyringeProcedure- Under USG guidance on IM injection of
Pancuronium is given to the fetus ( 0.5mg/kg offetal weight).
- Again under USG guidance a 20G needle isinserted in the umbilical vein at the most accessibleportion. The sites that are preferred are.
Dr. Bijoy BalakrishnanCIMAR, Cochin & Edappal

15www.kfogkerala.com
a) Placental insertion siteb) Intrahepatic portion of the
umbilical veinc) Free loop of the umbilical cordAt CIMAR we prefer the intrahepatic portion of
the umbilical vein as it is immobile and easilyaccessible.
- On entering the umbilical vein fetal blood isdrawn and the following tests are done.
a) Blood group and Rh typingb) Haematocritc) Direct combs testd) Liver Function Teste) Karyotyping- Once the fetal hct is known the volume of blood
to be transfused is calculated and transfused at therate of 5-10ml/min till the hct is around 45.
- Volume of blood can be calculated from the graphbelow. Firstly the total blood volume is calculatedfrom the Graph I (A). For example at 28 weeks theblood volume would be about 100ml. This volumeis then multiplied by the transfusion coefficient. Thisfactor is obtained once the donor haematocrit andfetal haematocrit are known and plotted on Graph I(B). For instance if the donor haematocrit is 90 andthe fetal haematocrit is 10 the factor would be 0.8.
- Volume of transfusion – fetal blood volume xtrans coefficient- 100 x 0.8= 80ml.
of monitoring also depends on which zonethe MCA PSV value falls.
Graph I (A)Graph I (B)
- For the net savvy another option would be to goto the web site perinatology.com where on enteringthe Donor HCT, Fetal HCT and fetal weight theamount of blood to be transfused will be known.
- Post transfusion fetal haematocrit is re-estimated- MCA is then evaluated again and plotted on
Graph II. If the value of MCA PSV comes to zone Athen Repeat transfusion is indicated. The frequency
Graph IIDelivery:· Transfusion can be continued up to 34 weeks· Patient should be induced at 37-38 weeks
gestation· Caesarian Section is done only for obstetric
indications.· Maternal Phenobarbital should be given for 7
days before induction (30mg tid x 7 days) to inducefetal liver enzymes in order to cope up with stress ofhaemolysis.
Prognosis:· Serial IUT’s would invariably result in fetal bone
marrow suppression. As a result of which a “top up“transfusion would be required at 4-6 weeks of age.Therefore these infants should be followed up weeklywith haematocrit and reticulocyte counts. Mostimportantly the neurological outcome is the same inhydropic and non-hydropic fetuses which indirectlytells us that even severely hydropic fetuses can besalvaged. Sensory neural hearing loss is acomplication that frequently develops due to exposureto elevated bilirubin levels.
Conclusion:Kerala is miles ahead when it comes to preventing
Rh isoimmunication mainly because almost all ourdeliveries are hospitalized. However Rhisoimmunication does occur and before you decideto terminate these pregnancies do remember that theycan be SAVED!!