Embed Size (px)
Citation preview
Compliance with this Guideline is recommended Page 1 of 19
Guideline
Women and Babies: Neonatal Early Assessment Program (NEAP)
Document No: RPAH_GL2013_019 Functional Sub-Group: Clinical Governance
Corporate Governance Summary: The Neonatal Early Assessment Program (NEAP) on delivery
ward consists of risk factor assessment and four sets of measurements within the first 6 hours after birth: 1. The first physical examination. 2. The first lower limb oxygen saturation. 3. Anthropometry (accurate weight, length and head
circumference with percentiles) 4. Body fat (percentage) by air displacement plethysmography
National Standard: Standard 1 Governance for Safety and Quality in Health Care Policy Author: Clinical Academic Neonatologist and Professor International Maternal and Child Health Approved by: RPA Women and Babies Service Improvement Committee General Manager Publication (Issue) Date: January 2013 Next Review Date: January 2016 Replaces Existing Policy: N/A Previous Review Dates: N/A Note: Sydney Local Health District (LHD) and South Western Sydney LHD were established on 1 July 2011, with the dissolution of the former Sydney South West Area Health Service (SSWAHS) in January 2011. The former SSWAHS was established on 1 January 2005 with the amalgamation of the former Central Sydney Area Health Service (CSAHS) and the former South Western Sydney Area Health Service (SWSAHS). In the interim period between 1 January 2011 and the release of specific LHN policies (dated after 1 January 2011) and SLHD (dated after July 2011), the former SSWAHS, CSAHS and SWSAHS policies are applicable to the LHDs as follows: Where there is a relevant SSWAHS policy, that policy will apply Where there is no relevant SSWAHS policy, relevant CSAHS policies will apply to Sydney LHD; and relevant SWSAHS policies will apply to South Western Sydney LHD.
Compliance with this Guideline is recommended Page 2 of 19
Neonatal Early Assessment Program (NEAP)
Contents 1 Introduction ......................................................................................................................... 3
2 Policy Statement ................................................................................................................. 3
3 Principles / Guidelines ......................................................................................................... 3
3.1 Introduction ................................................................................................................... 4
3.2 Background .................................................................................................................. 4
3.3 Method of education and training .................................................................................. 6
3.4 Who performs the NEAP?............................................................................................. 7
3.5 When to perform the NEAP? ........................................................................................ 7
3.6 How to perform the NEAP?........................................................................................... 8
4 Performance Measures ..................................................................................................... 15
5 Definitions ......................................................................................................................... 15
6 References and Links ........................................................................................................ 15
Appendix 1: Rationale for early physical examination ........................................................... 19
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 3 of 19
Neonatal Early Assessment Program (NEAP) 1 Introduction
The risks addressed by this policy: Clinical risk of pathological, or neurological damage or death of babies as a result of physical abnormalities, cardiac defects, or neonatal hypoglycaemia going undetected and untreated.
The aims / expected outcome of this policy
Babies with physical abnormalities, cardiac defects, or increased risk of hypoglycaemia will be identified and appropriately managed.
2 Policy Statement
The goal of this policy is to appropriately identify infants:
(i) With physical abnormalities that have significant morbidity and/or mortality if not
detected early, soon after birth.
(ii) With cardiac, respiratory, infective or metabolic defects that require immediate or
planned intervention for optimal survival
(iii) With increased and/or high risk for neonatal hypoglycaemia. In these infants blood
glucose levels (BGLs) will be measured and early feeding will be supported when
possible. The therapeutic goal should be to not tolerate BGLs between
intervention and pathological thresholds for longer than the effect of one feed, and
to increase BGLs below pathological levels as a matter of urgency with
intravenous glucose.
3 Principles / Guidelines The overarching principles are to ensure optimal care of the baby by:
incorporating Baby Friendly Hospital Initiative (BFHI) guidelines to the mother pair ensuring safe, immediate post birth, skin-to-skin contact with early breast feeding within the first hour; competently examining the newborn for risk assessment; by streamlining care with least intervention.
Background to the Neonatal Early Assessment Program (NEAP))
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 4 of 19
3.1 Introduction Infants born at RPA Hospital undergo screening for early identification of abnormalities with potentially serious consequences or risk factors that indicate need for closer postnatal observation. These include
1) Neonatal Early Assessment Program (NEAP) in the Neonatal Assessment Room in delivery ward to establish baseline anthropometry and to identify risk factors and abnormalities that may have an immediate impact on the care or well-being of the baby.
2) Neonatal Later Assessment Program (NLAP), on the postnatal ward or at home, includes a more complete examination to detect abnormalities that are not apparent in the early period or require further testing at a later time period.
The Neonatal Early Assessment Program (NEAP) on delivery ward consists of risk factor assessment and four sets of measurements within the first 6 hours after birth:
1. Risk factor assessment and the first physical examination. 2. The first lower limb oxygen saturation. 3. Anthropometry (accurate weight, length and head circumference) 4. Body fat (percentage) by air displacement plethysmography
Neonatal Later Assessment Program (NLAP) on the postnatal ward or at home consists of four sets of measurements:
1. The late more comprehensive physical examination 2. The second lower limb oxygen saturation 3. The newborn screening blood test. 4. The hearing test (State-Wide Infant Screening_ Hearing (SWISH))
A Systems Approach to Early Neonatal Assessment Combining these assessments into a systematic program before leaving the birthing environment enables a safer, faster, more accurate and timely assessment. The one assessment, rather than multiple interruptions, is least invasive for baby and mother Risk factors or abnormalities are identified and appropriate early action implemented. Parents are encouraged to come to the assessment and understand and assist in measurement of their baby. In this way efficiency and communication are maintained and mother, baby and partner have an easy, uninterrupted entry to the postnatal ward. Furthermore optimising immediate maternal skin-to-skin contact and early breast feeding (in accordance with the safe skin to skin guideline (insert HTML link)) within the first hour is prioritised for babies born by vaginal delivery and operative delivery. Secondary to this priority, the assessment of newborns following operative delivery will occur opportunistically on a case-by-case basis. Opportunities for assessment may include after the mother and baby are admitted to the postnatal ward, between discharge from recovery and admission to the postnatal ward, or between when the baby leaves theatre and when the baby is able to join the mother in recovery, if this time is longer than usual. The timing of NEAP assessment following operative delivery is subject to change after the policy is adopted.
3.2 Background Early Risk Factor Assessment and Physical Examination The overall goal of the early assessment is to identify risk factors for early neonatal problems that will require regular postnatal observations, as well as identifying congenital and acquired abnormalities which may have an immediate impact on the baby’s care and/or wellbeing.
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 5 of 19
Early Risk Factor Assessment All babies should be reviewed for risk factors for the four main problem areas as identified on the ‘Women and Babies Newborn Care Plan and Observations Chart MR504 (NCPOC)’. These include
• Risk of hypoglycaemia • Respiratory distress • Trauma from instrumental delivery and • Risk of infection
Assessment of risk of hypoglycaemia will include the anthropometric measurements and percentage body fat as outlined below. Babies identified with risk factors will need observations as outlined in the relevant RPAH guideline and on the NCPOC. Early physical examination: The goal of this examination is to identify obvious external anomalies, as well as other congenital and acquired problems that may have an immediate impact on the baby’s care or well-being. This would include (but not be confined to) problems such as respiratory distress, consequences of birth trauma (e.g bruising, sub-galeal haemorrhage, nerve palsy), cleft palate, imperforate anus, abnormal genitalia and other dysmorphology. The examination should include a complete ‘head to toe to back’ inspection of the baby as detailed below. The findings should be documented in the relevant section of the NCPOC. Oxygen saturation screening: Routine oxygenation saturation screening of well newborns has been shown to improve early diagnosis of congenital heart disease (CHD)1 with a low false positive rate and minimal impact on resources. About half of the babies with a low saturation screen (<95%) will have either congenital heart disease (~1/3rd) or another important pathology including respiratory, infectious and metabolic problems (~2/3rd)2. Thus this is an important test of the well-being of a newborn. Saturation measurement within the first 4 to 6 hours of birth (early screen) has a lower accuracy for detection of CHD but greater sensitivity for non-cardiac pathology while screening after 24 hours (late screen) has greater sensitivity for detection of CHD, particularly left heart ductal dependent lesions. At RPAH, both early and late oxygen saturation screening will be performed in accordance with the existing protocol (HTML link to clinical guideline). Anthropometry Newborn measurement of weight, length, and head circumference reflects fetal nutrition and forms the basis on which future growth measurements are compared and important treatment decisions are made when measurements are plotted on growth curves. Several small studies have examined the accuracy of length measurements in newborns and neonates3-5. The largest study (Wood et al6) demonstrated inaccuracies in length measurements in a population-based, cross-sectional study of 602 term babies, assessed in this Department in 2010. Neonatal length was measured by standard clinical practice and by correct use of a length-board (gold standard) and measurements compared. Growth curve percentiles were used to plot length measurements. The difference from the ‘gold standard’ extended from -3.06 cm below to +2.67 cm above the gold standard. Neonates whose standard-practice length fell within 0.5 cm of the gold standard totalled 41% (241 neonates), while 59% (342) were > 0.5 cm. The change in length resulted in a change in the percentile range for 309 (53%) neonates on a standard growth curve percentile with implications for potentially erroneous clinical care. Lipmanet al. argues that primary health-care providers are often cavalier about the need for precision of length measurements7. Educating health-care workers on the importance of length measurements could increase their motivation to obtain measurements using correct techniques3. The importance of length and thus the need for accuracy in measurement are two messages that should be translated into clinical practice.
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 6 of 19
Body composition - Fat measurement (fat mass, fat free mass and body fat %) Accurately determining the nutritional status of newborns is a major public health problem8,
9.Furthermore undernourished neonates that survive are at risk of long term health outcomes, including hypertension, stroke, type 2 diabetes, obesity and cardiovascular disease10-13. Neonatal undernutrition or ‘wasting’ is a clinical diagnosis often characterised by diminished subcutaneous tissues and underlying muscles with loose wrinkled skin of the arms, thighs, elbows and knees8, 13. However this clinical sign is, in our experience at RPAH, not well recognised by a range of health providers. Thus defining who is undernourished is problematic. Conventional approaches include the use of population based percentiles (< 10th 5th or 3rd percentiles) or customised growth charts. Population based charts rely on a large cross section of neonates and use weight for gestational age by sex. Customised charts account for more maternal variables, however there is not strong evidence to support their use at present14, 15. An alternative to birth weight is the use of body composition or body fat % (BF%). The wasted, undernourished newborn is characterised by loss of the normal fat accretion in the last 4-6 weeks of pregnancy. As fat is used by the newborn as an alternative substrate to glucose for brain metabolism, BF% is a potentially very useful measure indicating degree of undernutrition and directly related to neonatal metabolic outcomes. The additional advantage is that it can distinguish the normal fat SGA from the low fat, undernourished SGA newborn and define the low fat AGA newborn at high risk of hypoglycaemia, currently not possible with any other methods. Recently a new technology using air displacement plethysmography (ADP) has become available to non-invasively, accurately and quickly measure BF% in infants from birth to 6 months of age. ADP has been validated against the four-compartment model and biological and physical phantoms16, 17and is considered the criterion method for determining BF% in neonates18-22. Several studies have investigated the BF% as an indicator of neonatal nutritional status using ADP16, 23-25(also journal article18-20, 22, 26, review27, comparative study17). We have shown that body fat is a better measure than customised charts for assessing neonatal morbidity and as good as population based charts28. The advantage of this method is it is accurate, easy, reliable, non-invasive and acceptable to parents. The cut offs for low and high fat are shown in the flow chart. These were determined by significantly better Receiver Operator Curves (ROCs) for combined morbidity assessed by 3 pre-specified outcomes (temp <36.5C, prolonged hospital stay, poor feeding (2 of 3 objective criteria). The cut off was determined by the highest sensitivity balanced by the best specificity16,28.
3.3 Method of education and training Recent evidence from an RCT of Australian medical students who received a standard neonatology training program in newborn examination versus blended learning (additional online access to a baby check learning module PENSKE) demonstrated significantly higher scores for the blended learning group on standardised blinded assessment of newborn examination29. Other studies support blended learning as a means of teaching and learning physical examination skills30-32. Formalising training in the examination of the newborn may explain the improved quality of the newborn examination undertaken by video assessment of midwives compared with senior house officers (SHOs) in a randomised control trial in the UK33. The educational value of a teaching method that is structured, skills-based, student-centred, small group and interactive (SCORPIO) was rated high or very high (100%) compared with problem-based learning and clerkship, each rated as 65%. The program was
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 7 of 19
enthusiastically received by the students and resulted in mastery of a range of core competencies necessary for care of the newborn34. We use the SCORPIO method of teaching35 which incorporates, firstly, ‘tell and show’ on how to perform each skill and then ‘do and feedback’ on correct and incorrect technique. This method has been shown to be effective in changing the behaviour of perinatal health providers and can be readily introduced with few resources36, 37.
3.4 Who performs the NEAP? A randomised controlled trial in the UK demonstrated that there was no statistical difference between resident medical officers (RMO) and community midwife examinations in appropriate referral rates to hospital or community or in inappropriate referral rates to hospital 38. However mothers were more likely to be satisfied with the newborn examination by a midwife than an RMO39 and discuss health-care issues more often than RMO33. Midwives identified many benefits to themselves, to their profession and to the mothers as a result of developing their role in the examination of the newborn baby. The major benefit cited was improved job satisfaction, which was directly related to their ability to give continuity of care to mothers and babies33.
• The goal therefore would be to expand our current mixed model of care. • The NEAP assessment will be undertaken by trained midwives and other trained
health providers and a second person who can be another health provider or the parent. The second person is required in order to measure the length accurately. This is then also used for entry into the algorithms for estimation of body fat % and lean mass.The later, more complete, ‘babycheck’ physical examination will be performed prior to discharge by RMOs, NNPs (neonatal nurse practitioners), or at home by midwives in the maternity discharge support program (MDSP).
3.5 When to perform the NEAP? The NEAP assessment will be performed after adequate skin-to-skin and early breast feeding but within the first 6 hours of birth so that risk is assessed as early and efficiently as possible. The NLAP assessment will be performed prior to discharge or at early follow up with the home MDSP midwife visit (see discharge policy).
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 8 of 19
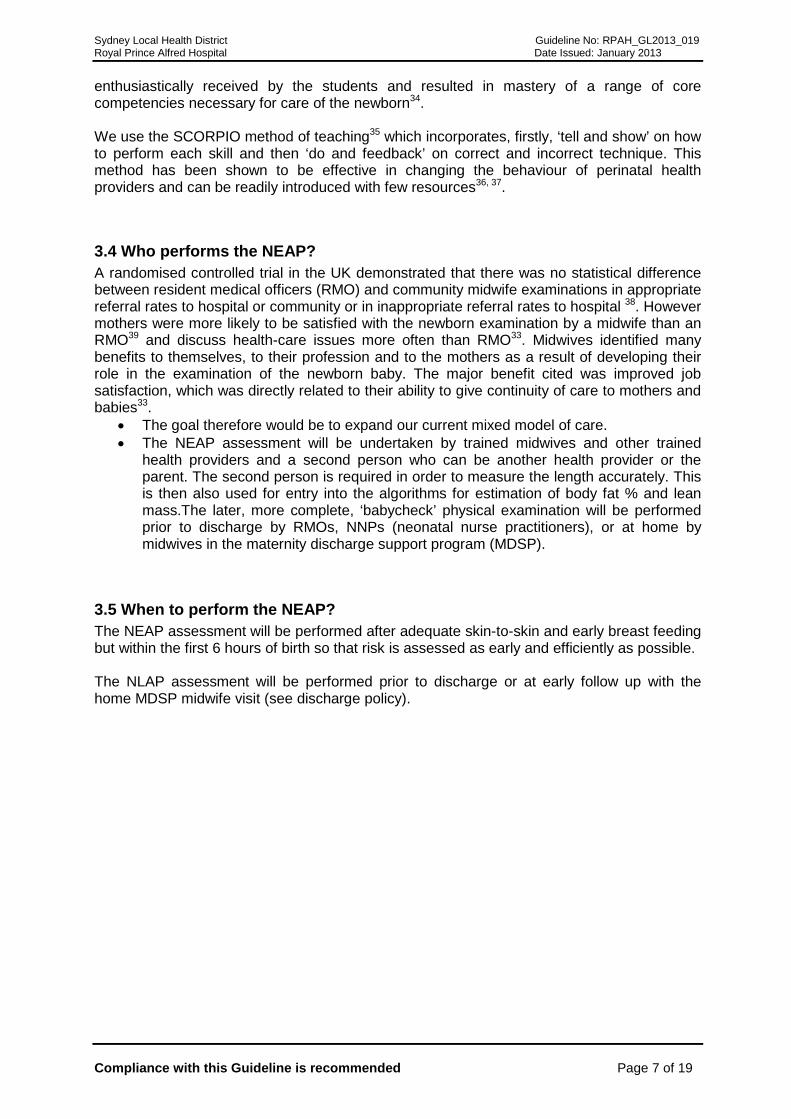
3.6 How to perform the NEAP? Figure 1: Overview
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 9 of 19
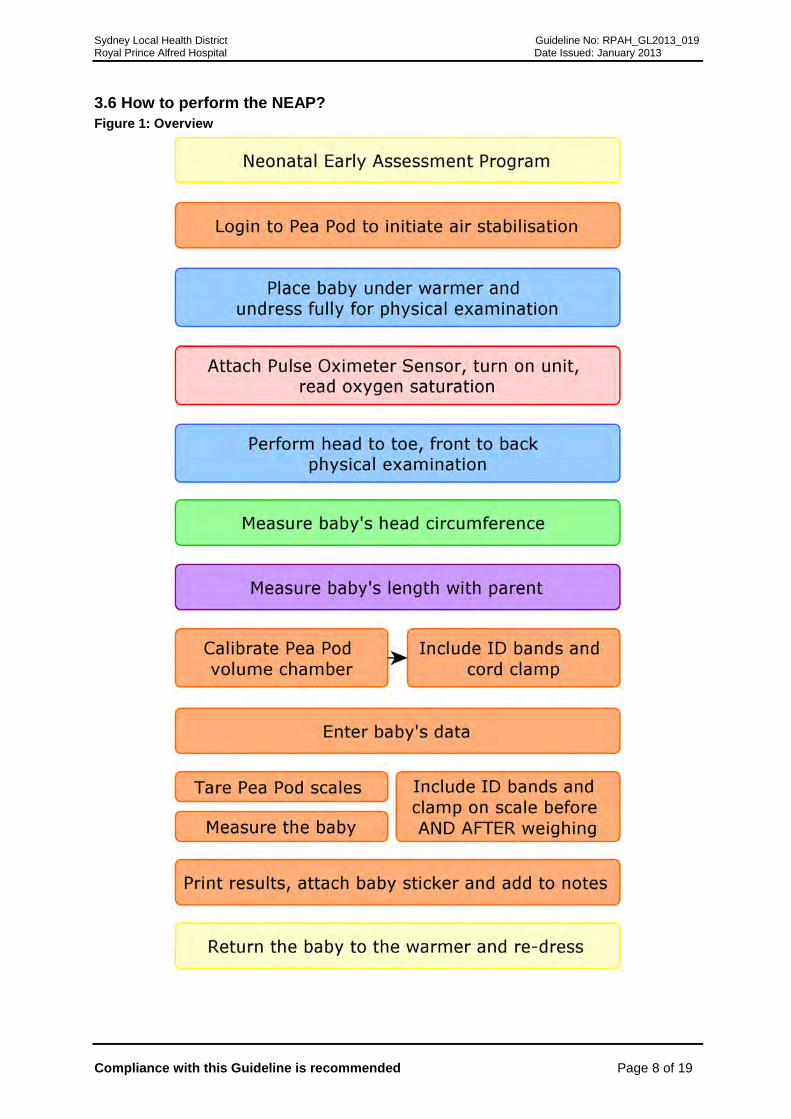
How to perform the first physical examination: The routine newborn assessment should include all aspects of the checklist on page 1 of the NCPOC. The schema below moves from head to toe, front to back (adapted from Queensland Maternity and Newborn Clinical Guidelines Program 61)40. Remind parent/s that their baby will need a second examination that will include assessment of their eyes (red reflex test), heart, and hips. Figure 2: Early Physical Examination of the Newborn Baby41
Head Palpate: • Sutures • Fontanelle • Trauma (check sub-galeal
haemorrhage)
Face Inspect: • Morphology • Eyes, Ears • Nose, Jaw
Mouth Visualise and feel palate (hard and soft)
Chest Check: • Respiratory rate • No recession • Palpate neck
Abdomen Check: • No distension • Palpate for masses • Umbilicus • Umbilical vessels (x3)
Anogenital
Check normal: • External genitalia • Anus patency, appearance
and position
Limbs Check normal: • Hands and Feet • Digits • Movements
Back
Check in ventral suspension: • Straight spine • No skin markings over
i
General Check: • Skin & Colour • Symmetrical • Proportioned
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 10 of 19
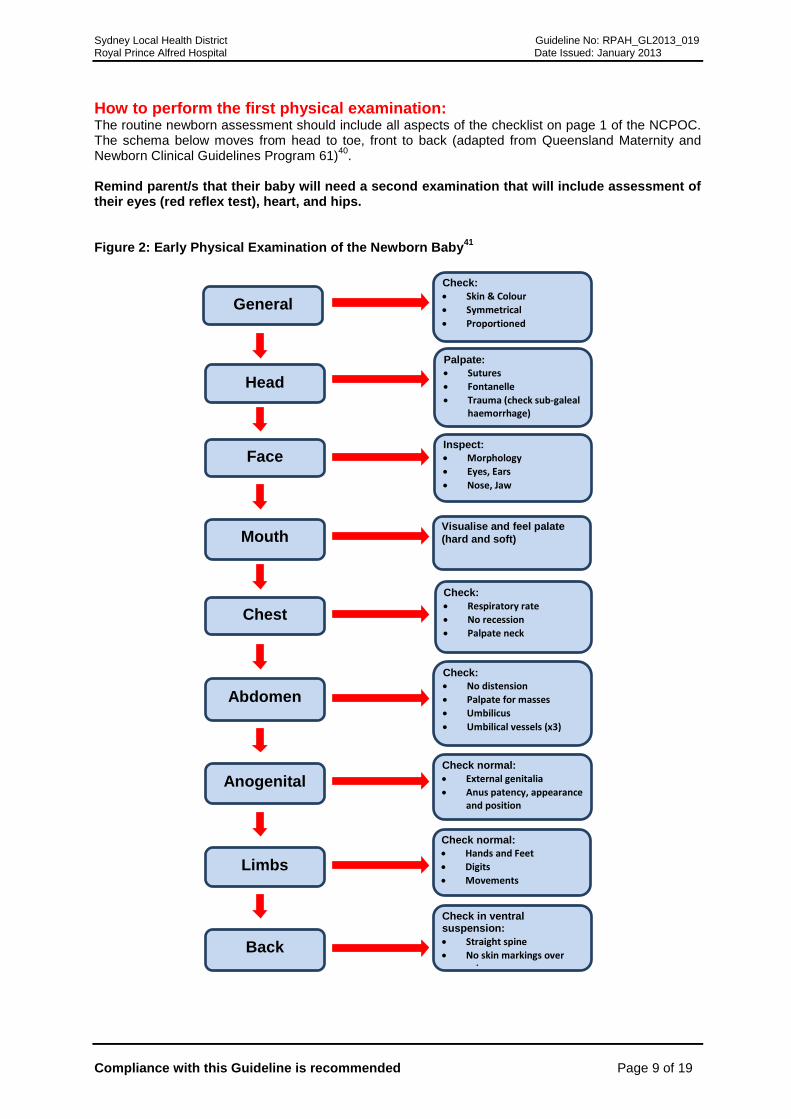
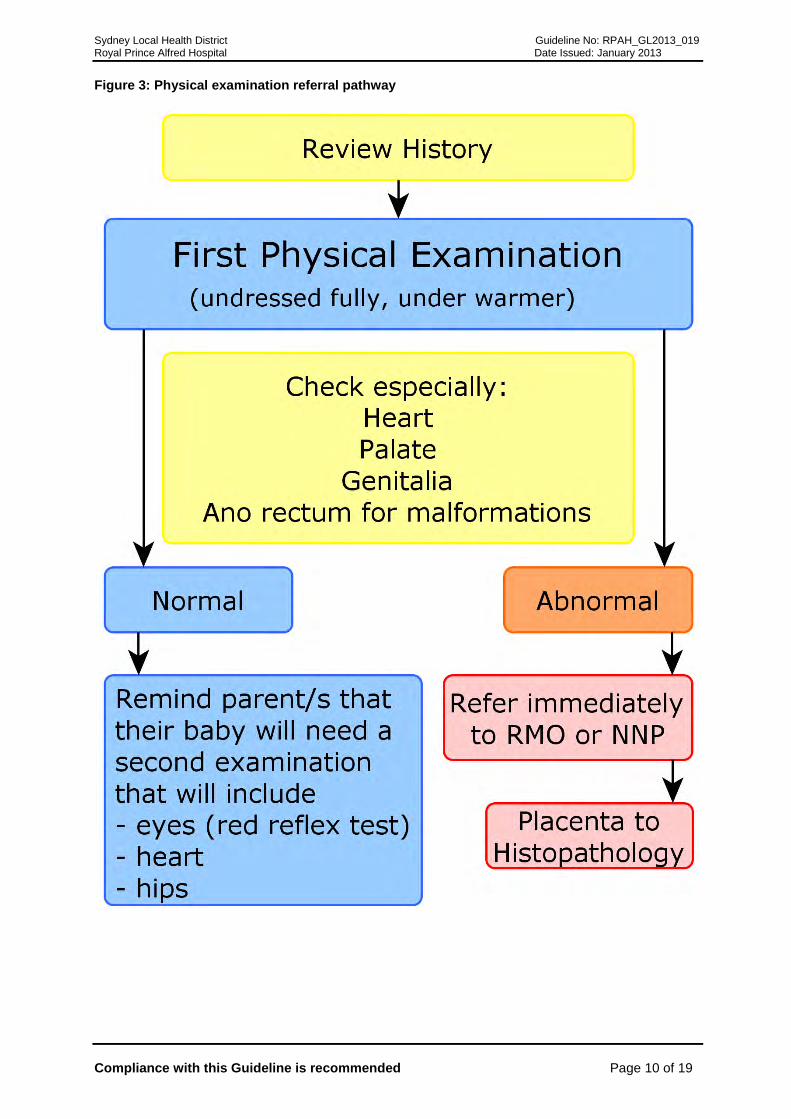
Figure 3: Physical examination referral pathway
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 11 of 19
How to measure weight: • The scales on the Pea Pod are used for accurate measurement of weight to the
nearest gram. • The newborn is bare weighed. • The weight percentile is calculated using the Beeby electronic calculator on the
computer in the NEAP room, or if unavailable the weight is plotted on New South Wales population-based birthweight percentile charts (less accurate)41.
How to measure length:
• The length-board measurement, infantometer, has been shown to be the most reliable and accurate measurement of neonatal length5, 42, 43 and more recent designs have improved ease of use such as the Easy-Glide Bearing Infantometer (Perspective Enterprises, Portage, MI, USA).
• The neonate is placed supine and unclothed on the board and held gently with his or her body aligned and head in a neutral position. One person stands at the top of the length board and holds the baby’s head in contact with the headboard while another extends the left leg by placing the hand over the left knee, depressing the knee, straightening the leg and moving the footboard to touch the plantar surface of the foot at a right angle to the leg. Recheck that the head has not moved from the headboard before taking the measurement. The actual reading is marked by an arrow as there is an offset for greater ease of reading and accuracy.
• The length percentile is calculated using the Beeby electronic calculator on the computer in the NEAP room or plotted on New South Wales population-based birth length percentile charts41 (less accurate) .
• The need for correct technique was confirmed by Lipmanet al.3, who showed significant improvement in length accuracy after an intervention involving intensive training.
How to measure head circumference:
• Head circumference is measured using disposable paper circumference tapes at the maximum fronto-occipital circumference.
• Two reproducible measurements are required. • The head circumference percentile is calculated using the Beeby electronic calculator
on the computer in the NEAP room or plotted on New South Wales population-based birth head circumference percentile charts41(less accurate).
How to perform oxygen saturation screening:
• Early oxygen saturation screening will be performed in accordance with the existing protocol (HTML link to clinical guideline)
• Perform early in assessment when infant is quiet. • Place probe around one foot with light source and receiver on each side of foot.
Secure with Coban tape. To ensure good blood flow to the foot, do not secure too tightly and do not hold the probe around the foot.
• Switch on oximeter and allow signal to stabilise. Read when stabilised and there is a good plethysmographic light pulse.
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 12 of 19
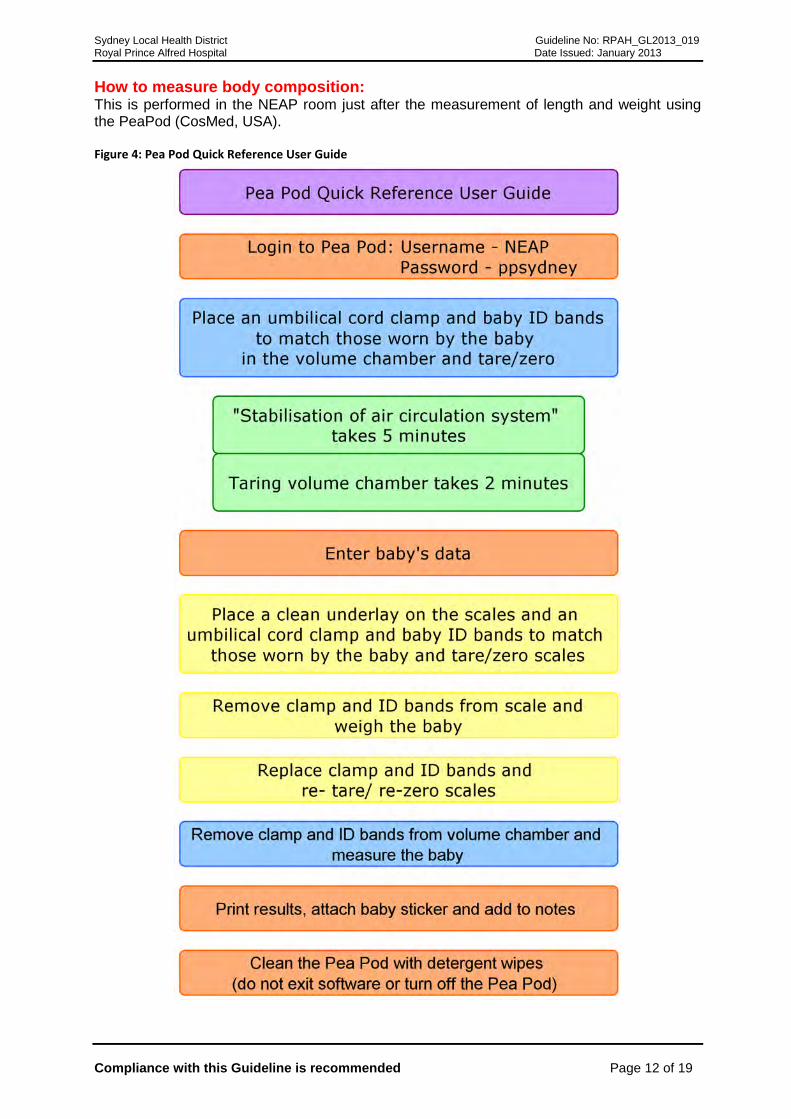
How to measure body composition: This is performed in the NEAP room just after the measurement of length and weight using the PeaPod (CosMed, USA). Figure 4: Pea Pod Quick Reference User Guide
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 13 of 19
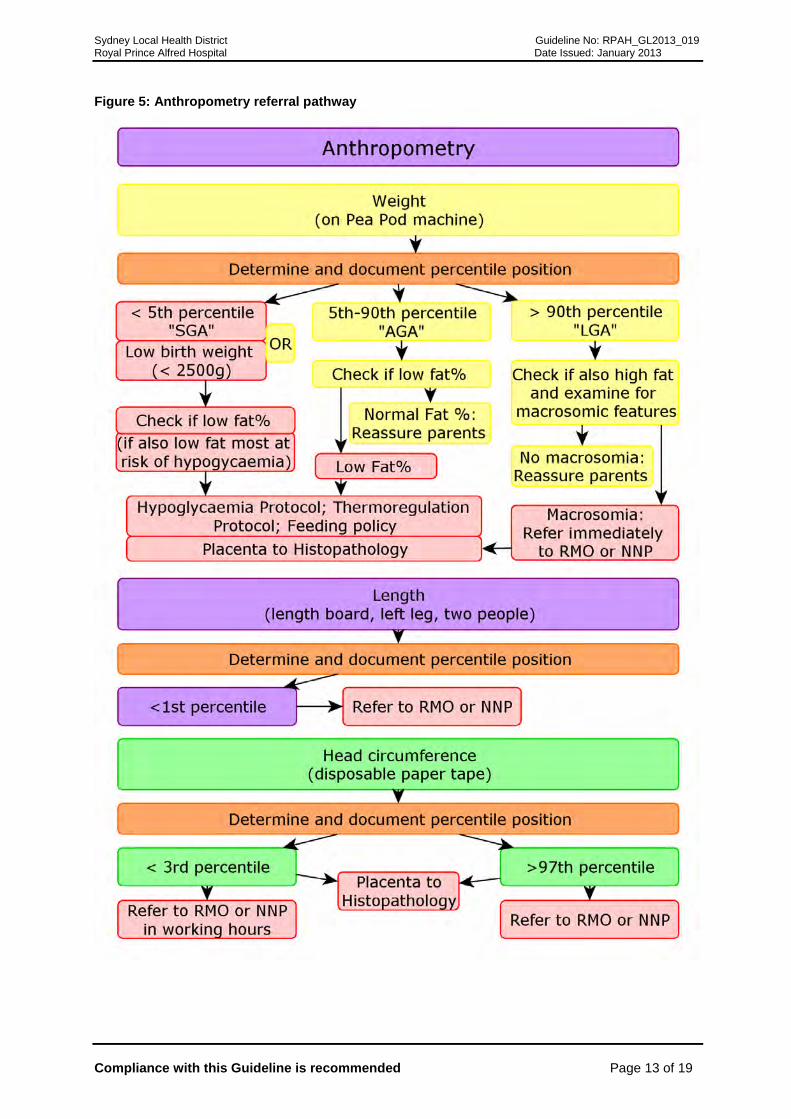
Figure 5: Anthropometry referral pathway
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 14 of 19
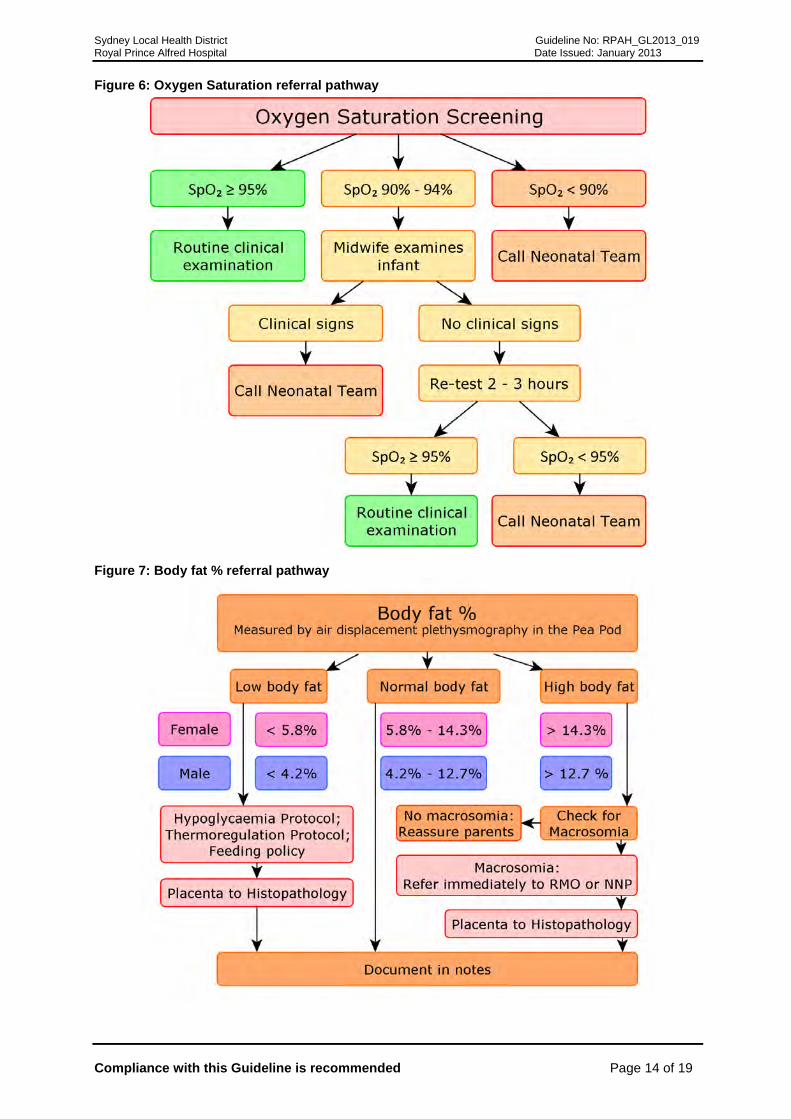
Figure 6: Oxygen Saturation referral pathway
Figure 7: Body fat % referral pathway
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 15 of 19
4 Performance Measures
Incident Information Management System 5 Definitions
Nil 6 References and Links 1 A. Meberg, A. Andreassen, L. Brunvand, T. Markestad, D. Moster, L. Nietsch, I. E. Silberg, and J.
E. Skålevik, 'Pulse Oximetry Screening as a Complementary Strategy to Detect Critical Congenital Heart Defects', Acta Pædiatrica, 98 (2009), 682-86.
2 A. Meberg, S. Brugmann-Pieper, R. Due, Jr., L. Eskedal, I. Fagerli, T. Farstad, D. H. Froisland, C. H. Sannes, O. J. Johansen, J. Keljalic, T. Markestad, E. A. Nygaard, A. Rosvik, and I. E. Silberg, 'First Day of Life Pulse Oximetry Screening to Detect Congenital Heart Defects', J Pediatr, 152 (2008), 761-5.
3 T. H. Lipman, K. D. Hench, T. Benyi, J. Delaune, K. A. Gilluly, L. Johnson, M. G. Johnson, H. McKnight-Menci, D. Shorkey, J. Shults, F. L. Waite, and C. Weber, 'A Multicentre Randomised Controlled Trial of an Intervention to Improve the Accuracy of Linear Growth Measurement', Arch Dis Child, 89 (2004), 342-6.
4 T. S. Johnson, J. L. Engstrom, and D. K. Gelhar, 'Intra- and Interexaminer Reliability of Anthropometric Measurements of Term Infants', J Pediatr Gastroenterol Nutr, 24 (1997), 497-505.
5 T. S. Johnson, J. L. Engstrom, J. A. Warda, M. Kabat, and B. Peters, 'Reliability of Length Measurements in Full-Term Neonates', J Obstet Gynecol Neonatal Nurs, 27 (1998), 270-6.
6 A. J. Wood, C. H. Raynes-Greenow, A. E. Carberry, and H. E. Jeffery, 'Neonatal Length Inaccuracies in Clinical Practice and Related Percentile Discrepancies Detected by a Simple Length-Board', J Paediatr Child Health, 49 (2013), 199-203.
7 T. H. Lipman, K. D. Hench, J. D. Logan, D. A. DiFazio, P. M. Hale, and C. Singer-Granick, 'Assessment of Growth by Primary Health Care Providers', Journal of Pediatric Health Care, 14 (2000), 166-71.
8 O. J. Adebami, and J. A. Owa, 'Comparison between Canscore and Other Anthropometric Indicators in Fetal Malnutrition', Indian J Pediatr, 75 (2008), 439-42.
9 J. E. Lawn, S. Cousens, and J. Zupan, '4 Million Neonatal Deaths: When? Where? Why?', Lancet, 365 (2005), 891-900.
10 D. J. Barker, J. G. Eriksson, T. Forsen, and C. Osmond, 'Fetal Origins of Adult Disease: Strength of Effects and Biological Basis', Int J Epidemiol, 31 (2002), 1235-9.
11 J. C. Wells, S. Chomtho, and M. S. Fewtrell, 'Programming of Body Composition by Early Growth and Nutrition', Proc Nutr Soc, 66 (2007), 423-34.
12 O. Salihoglu, G. Karatekin, R. Ilhan, and A. Nuhoglu, 'Placental Findings in Malnourished Term Neonates', Pediatr Int, 51 (2009), 494-7.
13 N. Sankhyan, V. K. Sharma, and S. Singh, 'Detection of Fetal Malnutrition Using "Can Score"', Indian J Pediatr, 76 (2009), 903-6.
14 A. E. Carberry, A. Gordon, D. M. Bond, J. Hyett, C. H. Raynes-Greenow, and H. E. Jeffery, 'Customised Versus Population-Based Growth Charts as a Screening Tool for Detecting Small for Gestational Age Infants in Low-Risk Pregnant Women', in Cochrane Database of Systematic Reviews John Wiley & Sons, Ltd 2011 ).
15 A. E. Carberry, C. H. Raynes-Greenow, R. M. Turner, and H. E. Jeffery, 'Customized Versus Population-Based Birth Weight Charts for the Detection of Neonatal Growth and Perinatal Morbidity in a Cross-Sectional Study of Term Neonates', American Journal of Epidemiology, August 21 (2013).
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 16 of 19
16 A. E. Carberry, P. B. Colditz, and B. E. Lingwood, 'Body Composition from Birth to 4.5 Months in Infants Born to Non-Obese Women', Pediatr Res, 68 (2010), 84-8.
17 A. Frondas-Chauty, I. Louveau, I. Le Huerou-Luron, J. C. Roze, and D. Darmaun, 'Air-Displacement Plethysmography for Determining Body Composition in Neonates: Validation Using Live Piglets', Pediatric research, 72 (2012), 26-31.
18 K. J. Ellis, M. Yao, R. J. Shypailo, A. Urlando, W. W. Wong, and W. C. Heird, 'Body-Composition Assessment in Infancy: Air-Displacement Plethysmography Compared with a Reference 4-Compartment Model', Am J Clin Nutr, 85 (2007), 90-5.
19 G. Ma, M. Yao, Y. Liu, A. Lin, H. Zou, A. Urlando, W. W. Wong, L. Nommsen-Rivers, and K. G. Dewey, 'Validation of a New Pediatric Air-Displacement Plethysmograph for Assessing Body Composition in Infants', Am J Clin Nutr, 79 (2004), 653-60.
20 R. D. Sainz, and A. Urlando, 'Evaluation of a New Pediatric Air-Displacement Plethysmograph for Body-Composition Assessment by Means of Chemical Analysis of Bovine Tissue Phantoms', Am J Clin Nutr, 77 (2003), 364-70.
21 A. Urlando, P. Dempster, and S. Aitkens, 'A New Air Displacement Plethysmograph for the Measurement of Body Composition in Infants', Pediatr Res, 53 (2003), 486-92.
22 M. Yao, L. Nommsen-Rivers, K. Dewey, and A. Urlando, 'Preliminary Evaluation of a New Pediatric Air Displacement Plethysmograph for Body Composition Assessment in Infants', Acta Diabetol, 40 Suppl 1 (2003), S55-8.
23 G.S. Andersen, T. Girma, J.C.K. Wells, P. Kæstel, K.F. Michaelsen, and H. Friis, 'Fat and Fat-Free Mass at Birth: Air Displacement Plethysmography Measurements on 350 Ethiopian Newborns', Pediatr Res, 70 (2011), 501-06.
24 D.A. Fields, J.M. Gilchrist, P.M. Catalano, M.L. Giannì, P.M. Roggero, and F. Mosca, 'Longitudinal Body Composition Data in Exclusively Breast-Fed Infants: A Multicenter Study', Obesity, 19 (2011), 1887-91.
25 B. E. Lingwood, A. M. Storm van Leeuwen, A. E. Carberry, E. C. Fitzgerald, L. K. Callaway, P. B. Colditz, and L. C. Ward, 'Prediction of Fat-Free Mass and Percentage of Body Fat in Neonates Using Bioelectrical Impedance Analysis and Anthropometric Measures: Validation against the Pea Pod', Br J Nutr, 107 (2012), 1545-52.
26 P. Roggero, M. L. Gianni, O. Amato, P. Piemontese, D. Morniroli, W. W. Wong, and F. Mosca, 'Evaluation of Air-Displacement Plethysmography for Body Composition Assessment in Preterm Infants', Pediatric research, 72 (2012), 316-20.
27 D. A. Fields, P. B. Higgins, and D. Radley, 'Air-Displacement Plethysmography: Here to Stay', Curr Opin Clin Nutr Metab Care, 8 (2005), 624-9.
28 A. E. Carberry, C. H. Raynes-Greenow, R. M. Turner, L. M. Askie, and H. E. Jeffery, 'Is Body Fat Percentage a Better Measure of Undernutrition in Newborns Than Birth Weight Percentiles', Pediatric Research, Advance online publication 02 October (2013).
29 A. Stewart, G. Inglis, L. Jardine, P. Koorts, and M. W. Davies, 'A Randomised Controlled Trial of Blended Learning to Improve the Newborn Examination Skills of Medical Students', Archives of Disease in Childhood Fetal & Neonatal Edition, 98 (2013).
30 H. S. Chumley-Jones, A. Dobbie, and C. L. Alford, 'Web-Based Learning: Sound Educational Method or Hype? A Review of the Evaluation Literature', Acad Med, 77 (2002), S86-93.
31 M. A Hall, M. Cuttini, A. W Flemmer, G. Greisen, N. Marlow, A. Schulze, S. Smith, A. Valls-i-Soler, P. Truffert, G. Conole, and M. Laat, 'European Online Postgraduate Educational Programme in Neonatology—the Way Forward?', European Journal of Pediatrics, 168 (2009), 449-56.
32 Anthony J. Frisby, J. Lindsey Lane, Anna Marie Carr, Ellen Ross, and Ruth P. Gottlieb, 'Development and Evaluation of an Interactive Multimedia Clinical Skills Teaching Program Designed for the Pediatric Clerkship', Teaching and Learning in Medicine, 18 (2006), 18-21.
33 C. Rogers, L. Bloomfield, and J. Townsend, 'A Qualitative Study Exploring Midwives' Perceptions and Views of Extending Their Role to the Examination of the Newborn Baby', Midwifery, 19 (2003), 55-62.
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 17 of 19
34 H. E. Jeffery, D. J. Henderson-Smart, and D. A. Hill, 'Competency-Based Learning in Neonatology', Medical Education, 30 (1996), 440-4.
35 D. A. Hill, 'Scorpio: A System of Medical Teaching', Med Teach, 14 (1992), 37-41.
36 H. E. Jeffery, M. Kocova, F. Tozija, D. Gjorgiev, M. Pop-Lazarova, K. Foster, J. Polverino, and D. A. Hill, 'The Impact of Evidence-Based Education on a Perinatal Capacity-Building Initiative in Macedonia', Med Educ, 38 (2004), 435-47.
37 J. E. Hirst, H. E. Jeffery, J. Morris, K. Foster, and E. J. Elliott, 'Application of Evidence-Based Teaching in Maternal and Child Health in Remote Vietnam', Int J Gynaecol Obstet, 104 (2009), 152-5.
38 J. Townsend, D. Wolke, J. Hayes, S. Dave, C. Rogers, L. Bloomfield, E. Quist-Therson, M. Tomlin, and D. Messer, 'Routine Examination of the Newborn: The Emren Study. Evaluation of an Extension of the Midwife Role Including a Randomised Controlled Trial of Appropriately Trained Midwives and Paediatric Senior House Officers. [Review] [74 Refs]', Health technology assessment (Winchester, England). 8(14) (2004), iii-iv.
39 Dave S. Hayes J. Townsend J. Tomlin M. Wolke D, 'Routine Examination of the Newborn and Maternal Satisfaction: A Randomised Controlled Trial', Archives of disease in childhood. Fetal and neonatal edition, 86 (2002).
40 Queensland Maternity and Neonatal Clinical Guidelines Program, 'Examination of the Newborn Baby', ed. by Queensland Health (Queensland Queensland Health, 2009).
41 P. J. Beeby, T. Bhutap, and L. K. Taylor, 'New South Wales Population-Based Birthweight Percentile Charts', J Paediatr Child Health, 32 (1996), 512-8.
42 D. P. Davies, and R. E. Holding, 'Neonatometer: A New Infant Length Measurer', Arch Dis Child, 47 (1972), 938-40.
43 A. F. Roche T. G. Lohman, & R. Martorell (eds.), Anthropometric Standardization Reference Manual (Champaign, IL: Human Kinetics Books, 1988).
44 M. Fuloria, and S. Kreiter, 'The Newborn Examination: Part I. Emergencies and Common Abnormalities Involving the Skin, Head, Neck, Chest, and Respiratory and Cardiovascular Systems', American Family Physician, 65 (2002), 61-8.
45 M.; Kreiter Fuloria, S., 'The Newborn Examination: Part Ii. Emergencies and Common Abnormalities Involving the Abdomen, Pelvis, Extremities, Genitalia, and Spine.', American Family Physician, 65 (2002), 265-70.
46 J. S. Rahi, and C. Dezateux, 'National Cross Sectional Study of Detection of Congenital and Infantile Cataract in the United Kingdom: Role of Childhood Screening and Surveillance. The British Congenital Cataract Interest Group', Bmj, 318 (7180), 362-5.
47 AAO-HNS, 'The American Academy of Otolaryngology - Head and Neck Surgery : Fact Sheet: Cleft Lip and Cleft Palate'2011) <http://www.entnet.org/HealthInformation/cleftLipPalate.cfm>.
48 A. Habel, N. Elhadi, B. Sommerlad, and J. Powell, 'Delayed Detection of Cleft Palate: An Audit of Newborn Examination', Archives of Disease in Childhood, 91 (2006), 238-40.
49 T. Sharp, N. Fraser, M. U. Shenoy, T. Randell, L. Denvir, and A. R. Williams, '46xy Girls: The Importance of Careful Newborn Examination', Journal of Pediatric & Adolescent Gynecology, 25 (2012), 103-4.
50 C. Turowski, J. Dingemann, and J. Gillick, 'Delayed Diagnosis of Imperforate Anus: An Unacceptable Morbidity', Pediatric Surgery International, 26 (1083), 1083-6.
51 Brooke E. Wilson, Claire E. Etheridge, Soundappan V. S. Soundappan, and Andrew J. A. Holland, 'Delayed Diagnosis of Anorectal Malformations: Are Current Guidelines Sufficient?', Journal of Paediatrics and Child Health, 46 (2010), 268-72.
• Legislative Compliance: Organisation, Management and Staff Obligations – Governing Body and Management manual, Policy Number 2.7.1
• Code of Conduct – Governing Body and Management Manual, Policy Number 1.1

Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 18 of 19
• Governing Body and Management Manual Section 4: Human Resources Management – http://intranet.cs.nsw.gov.au/SSWPolicies/default.htm
• Carr N and Foster P, 'Examination of the Newborn: The Key Skills; Part 1 the Eye', The Practising Midwife, 17 (2014), 26-29.
Sydney Local Health District Guideline No: RPAH_GL2013_019 Royal Prince Alfred Hospital Date Issued: January 2013
Compliance with this Guideline is recommended Page 19 of 19
Appendix 1: Rationale for early physical examination If any part of the examination is incomplete this requires documentation. Important components of screening examination
• A newborn with one anatomic malformation should be evaluated for associated anomalies44, 45.
Congenital cataract: Incidence 3/10 000 live births. In the UK, in a National survey of infantile cataracts, a substantial proportion of children with congenital and infantile cataract were not diagnosed by 3 months of age, although routine ocular examination of all newborn and young infants is recommended46. Delayed diagnosis is associated with blindness. The authors found that: 39% the child’s carers suspected an eye defect before cataract was diagnosed; 33% of the 235 identified with infantile cataract were not examined until after one year of age. Correction of cataract in infancy is an important preventable cause of visual impairment and blindness in childhood. Research suggests surgical treatment of dense cataracts is needed within the first 3 months of life.
• Examination for cataract should occur in the newborn period and at 6-8 weeks with immediate referral to an opthalmologist if positive findings.
Cleft palate: Incidence is 1 in 1000 live births in white people, 3.6 in 1000 in Native American people, 2.1 in 1000 in Japanese people, and only 0.3 in 1000 in black people. Of clefting anomalies, cleft lip and palate (50%) is the most common cranio facial anomaly; isolated cleft palate (30%); isolated cleft lip (20%)47. A UK audit found delayed detection of cleft palate was not uncommon (28% after the first day), and the features of those more likely to be missed suggested digital examination only.
• Trainee doctors and midwives should be instructed to inspect visually using a light and tongue depressor, then digitally if sub mucous cleft palate is suspected48. Referral to a multidisciplinary cleft lip/palate team is indicated.
Disorders of sexual differentiation (DSD): Incidence of genital malformations, excluding undescended testes, 4-5 per 1000 live births and ambiguous genitalia (assignment of sex impossible at birth) estimated at 1 per 4000 live births. The most common DSD is Congenital Adrenal Hyperplasia (CAH); Androgen Insensitivity Syndrome (AIS) is also common. However, not all children with these conditions are identified early 49 despite evident abnormality at birth. A recent audit of 46 XY girls found that in the 11 children only 3 were suspected DSD at birth although 10 of 11 had at least 1 significant abnormality of their external genitalia (palpable gonads in the labio-scrotal folds or in the inguinal region, single urogenital opening, enlarged phallus). Median age presentation was 18 months (range 0 d-15y)49. The impact of delay is not only psychological (late diagnosis has been shown in Turner’s syndrome, 45 XO karyotype, to have a significant impact on psychological adjustment) but also some are autosomal recessive conditions with potential consequences for future pregnancies if the diagnosis is not made. Further, risk of malignancy increases as undescended testicular tissue remains undetected; often bilateral gonadectomy and vaginoplasty are required.
• Careful neonatal genital examination can identify children with disorders of sexual differentiation.
• The impact of delay in diagnosis may have psychological impact and may also have potential consequences for future pregnancies (if autosomal recessive).
• The presence of ambiguous genitalia is a medical emergency and pituitary and adrenal integrity must be established.
• Early specialist endocrine involvement is necessary and needed and to monitor growth and development.
Ano-rectal malformations: Despite routine physical examination postpartum in the UK, one in five neonates born with imperforate anus had a delayed diagnosis50 leading to a 10% incidence of perforation. In Sydney, Australia an audit of referrals found 32 % of ano-rectal malformations were missed in the first 24 hours post birth51.
• Thorough perineal examination with separation of the buttocks during the initial newborn examination is necessary to identify the presence of ano-rectal malformations 50.