Embed Size (px)
Citation preview
9/20
Workforce-Funded Training Program Application Cover Sheet
Applicant: Move through the fields by pressing Tab or clicking the mouse. Check boxes by mouse click or pressing Enter or spacebar. Name County of residence
(First, middle initial, last)
Cell phone (______) Home or alternate phone (______)
Are you between the ages of 18 and 24? Yes No Are you 25 and older? Yes No
Do you currently live in subsidized housing (Section 8 or Stark Metropolitan)? Yes No
Is anyone in your household receiving: SNAP (food assistance) OWF (cash assistance)?
Are you currently receiving unemployment compensation? Yes No
School
Name of school you plan to attend
Major or type of training
Are you currently attending? Yes No If No, when do you plan to start? Date
When do you expect to complete/graduate? Date
Office Use Only
Staff comments
Case manager initials
C1—Eligibility 4/20
Print on white
Please PRINT clearly
Workforce Innovation and Opportunity Act Adult/DLW Profile & Eligibility Application Do NOT fill in shaded areas
Move through the fields by pressing Tab or clicking the mouse. Intake date Seeker ID WIA staff initials
Check boxes by mouse click or pressing Enter or spacebar.
Name
Full name at birth and other names used
Social Security No. Date of birth Age
Street address
Mailing address, if other than above
City State Postal County
Email Do you have computer access? Yes No
Cell phone ( ) Home or alternate phone ( )
Emergency contact ( ) Name
Gender Female Male Prefer not to disclose Hispanic or Latino? Yes No
U.S. citizen? Yes No Registered alien Refugee Other legal alien Other
Race Check all that apply.
American Indian/Alaska Native Asian
Black/ African American
Native Hawaiian/Other Pacific Islander White Other
Prefer not to disclose
Have you ever participated in any programs through this agency? Yes No
If yes, provide dates of service and what the service was.
Start Date End Date Type of Service
Are you related to or closely acquainted with any Workforce Initiative Association staff person, board member, or anyone else with a connection to OhioMeansJobs? Yes No
If Yes, provide that person’s name and their connection to you.
Name Connection
Education History—Highest Level of Schooling Completed
High School Dropout Post High School Attended College College Degree Diploma Equivalent (GED) Certificate of attendance/ completion (disabled individual)
Highest grade completed
Vocational or technical certificate Other post-secondary degree or certification
Yes No Months (if less than 1 year) Years
Professional degree Doctoral degree Master’s degree Bachelor’s degree Associate’s degree
Education Status
Are you currently enrolled in Aspire? Yes No
Are you currently attending a school or training program? Yes No
School Name Area of Training Start Date Planned End Date
List all training institutions you have attended, including vocational or career tech programs or college:
Name of School Major Dates Attended Graduated Degree
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Military Status C1—Page 2
Males only: Are you registered for Selective Service: Yes No Exempt
Yes No WIA use only
Have you served in U.S. military? If applicant answered YES to any of the questions to the left, complete and attach C1A – WIOA Addendum – Revised 7/15
Are you a spouse of a veteran?
Are you a homeless veteran?
Career Readiness
Do you have? Yes No Explain
A valid driver’s license? State A B C D (noncommercial)
If no valid license, explain.
Reliable transportation
Reliable childcare
Stable housing
Is English your native or primary language? Yes No If not, what language?
Do you feel you have a cultural barrier? Yes No
List any medical or physical restrictions you may have (e.g., hearing, lifting, etc.):
Have you been diagnosed with a disability? Yes No. If Yes, check all that apply:
Physical Mental Learning Behavioral
Please explain.
Are you enrolled in vocational rehabilitation through OOD? Yes No
Yes No Year Have you ever received services for:
Drug or alcohol treatment? Explain.
Have you ever failed a drug screen?
Mental health issues? Explain.
Misdemeanor or felony convictions? List conviction(s), arrest(s), and date(s) of same.
Are you currently on probation or parole? Explain.
Work Readiness
Yes No
1. Do you have an up-to-date resume?
2. Have you ever been fired? Please explain.
3. Is there anything preventing you from getting a job? Please explain.
Work History C1—Page 3
Employer—Current or Most Recent Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Employer Name Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Employer Name Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Employer Name Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Employer Name Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Employer Name Job Title Reason for Leaving
Hourly Wage Hours Per Week Start Date End Date Length of Employment
$ Years Months
Duties; equipment and skills you used.
Please describe any significant employment or skills not listed above.
Do you have work experience in agriculture in the last 12 months? Yes No
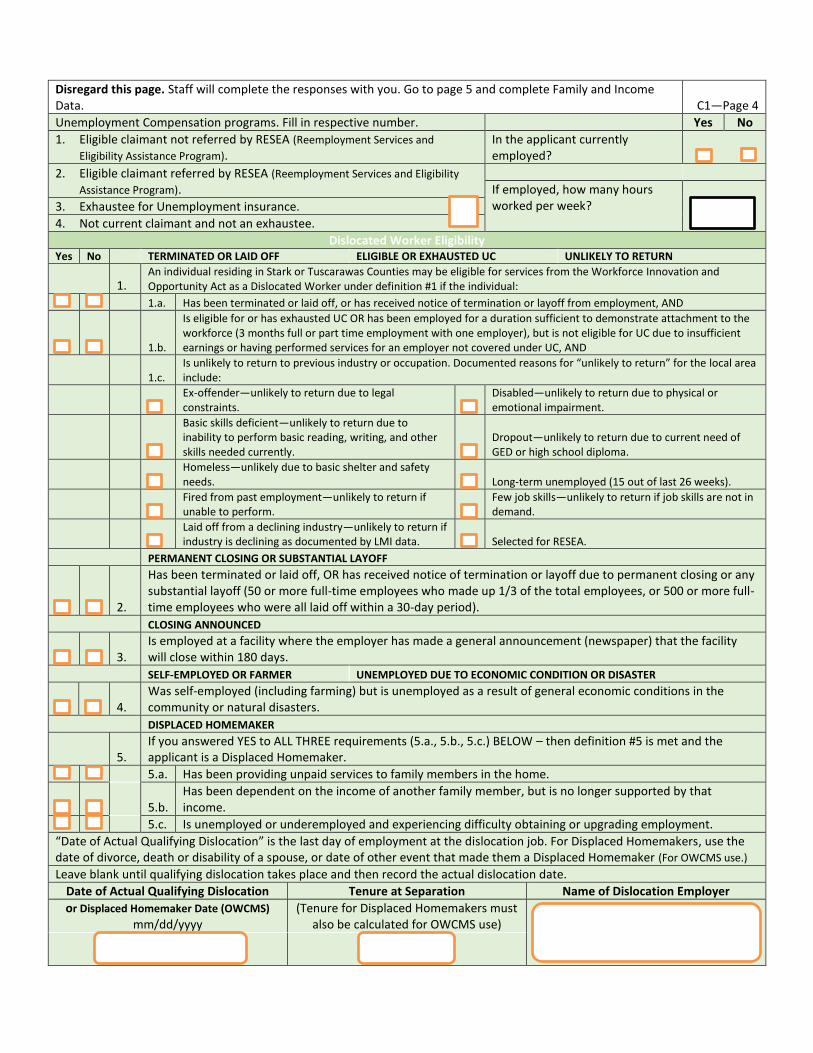
Disregard this page. Staff will complete the responses with you. Go to page 5 and complete Family and Income Data. C1—Page 4
Unemployment Compensation programs. Fill in respective number. Yes No
1. Eligible claimant not referred by RESEA (Reemployment Services and
Eligibility Assistance Program). In the applicant currently employed?
2. Eligible claimant referred by RESEA (Reemployment Services and Eligibility
Assistance Program).
If employed, how many hours worked per week?
3. Exhaustee for Unemployment insurance.
4. Not current claimant and not an exhaustee.
Dislocated Worker Eligibility Yes No TERMINATED OR LAID OFF ELIGIBLE OR EXHAUSTED UC UNLIKELY TO RETURN
1. An individual residing in Stark or Tuscarawas Counties may be eligible for services from the Workforce Innovation and Opportunity Act as a Dislocated Worker under definition #1 if the individual:
1.a. Has been terminated or laid off, or has received notice of termination or layoff from employment, AND
1.b.
Is eligible for or has exhausted UC OR has been employed for a duration sufficient to demonstrate attachment to the workforce (3 months full or part time employment with one employer), but is not eligible for UC due to insufficient earnings or having performed services for an employer not covered under UC, AND
1.c. Is unlikely to return to previous industry or occupation. Documented reasons for “unlikely to return” for the local area include:
Ex-offender—unlikely to return due to legal
constraints. Disabled—unlikely to return due to physical or
emotional impairment.
Basic skills deficient—unlikely to return due to inability to perform basic reading, writing, and other skills needed currently.
Dropout—unlikely to return due to current need of GED or high school diploma.
Homeless—unlikely due to basic shelter and safety
needs.
Long-term unemployed (15 out of last 26 weeks).
Fired from past employment—unlikely to return if
unable to perform. Few job skills—unlikely to return if job skills are not in
demand.
Laid off from a declining industry—unlikely to return if
industry is declining as documented by LMI data.
Selected for RESEA.
PERMANENT CLOSING OR SUBSTANTIAL LAYOFF
2.
Has been terminated or laid off, OR has received notice of termination or layoff due to permanent closing or any substantial layoff (50 or more full-time employees who made up 1/3 of the total employees, or 500 or more full-time employees who were all laid off within a 30-day period).
CLOSING ANNOUNCED
3.
Is employed at a facility where the employer has made a general announcement (newspaper) that the facility will close within 180 days.
SELF-EMPLOYED OR FARMER UNEMPLOYED DUE TO ECONOMIC CONDITION OR DISASTER
4.
Was self-employed (including farming) but is unemployed as a result of general economic conditions in the community or natural disasters.
DISPLACED HOMEMAKER
5. If you answered YES to ALL THREE requirements (5.a., 5.b., 5.c.) BELOW – then definition #5 is met and the applicant is a Displaced Homemaker.
5.a. Has been providing unpaid services to family members in the home.
5.b.
Has been dependent on the income of another family member, but is no longer supported by that income.
5.c. Is unemployed or underemployed and experiencing difficulty obtaining or upgrading employment.
“Date of Actual Qualifying Dislocation” is the last day of employment at the dislocation job. For Displaced Homemakers, use the date of divorce, death or disability of a spouse, or date of other event that made them a Displaced Homemaker (For OWCMS use.)
Leave blank until qualifying dislocation takes place and then record the actual dislocation date.
Date of Actual Qualifying Dislocation Tenure at Separation Name of Dislocation Employer
or Displaced Homemaker Date (OWCMS)
mm/dd/yyyy (Tenure for Displaced Homemakers must
also be calculated for OWCMS use)

Do not fill in shaded areas. Family and Income Data C1—Page 5
Married, but separated Divorced Widowed Marital status: Single Married Date Date Date
Number of children in the home Children’s ages
Complete the chart below for the members of your family. Begin by listing yourself on line 1. Complete the information in all of the columns for each family member and be as accurate as possible. If a household member has two or more sources of income, please take several lines and list each source of income and the amount of income received or earned from each source on a separate line.
Sources of Income Total Gross Income and Earnings for the Past 6 Months
Staff Only
Name of Family Member Relation to You Age
Earnings from Work, Social Security, SSI, Child Support,
OWF, Pension, Etc. Excluded Income
Included Income
Self $ $ $
$ $ $
$ $ $
$ $ $
$ $ $
$ $ $
$ $ $
$ $ $
$ $ $
$ $ $
TOTAL family six-month includable income $
TOTAL individual six-month includable income $
Please answer YES or NO to all of the questions below. YES NO
Are you currently a Pell Grant recipient?
Are you currently in default of student loan(s)?
Has your family assistance group received any of the following at any time during the past 6 months for numbers 1-7?
1. OWF (Ohio Works First)
2. Exhausting OWF within 2 years
3. DA (Disability Assistance)
4. RCA (Refugee Cash Assistance)
5. SSI (Supplemental Security Income) SSA Title XVI
6. SNAP (Supplemental Nutrition Assistance Program) food stamps
7. SNAP Employment and Training
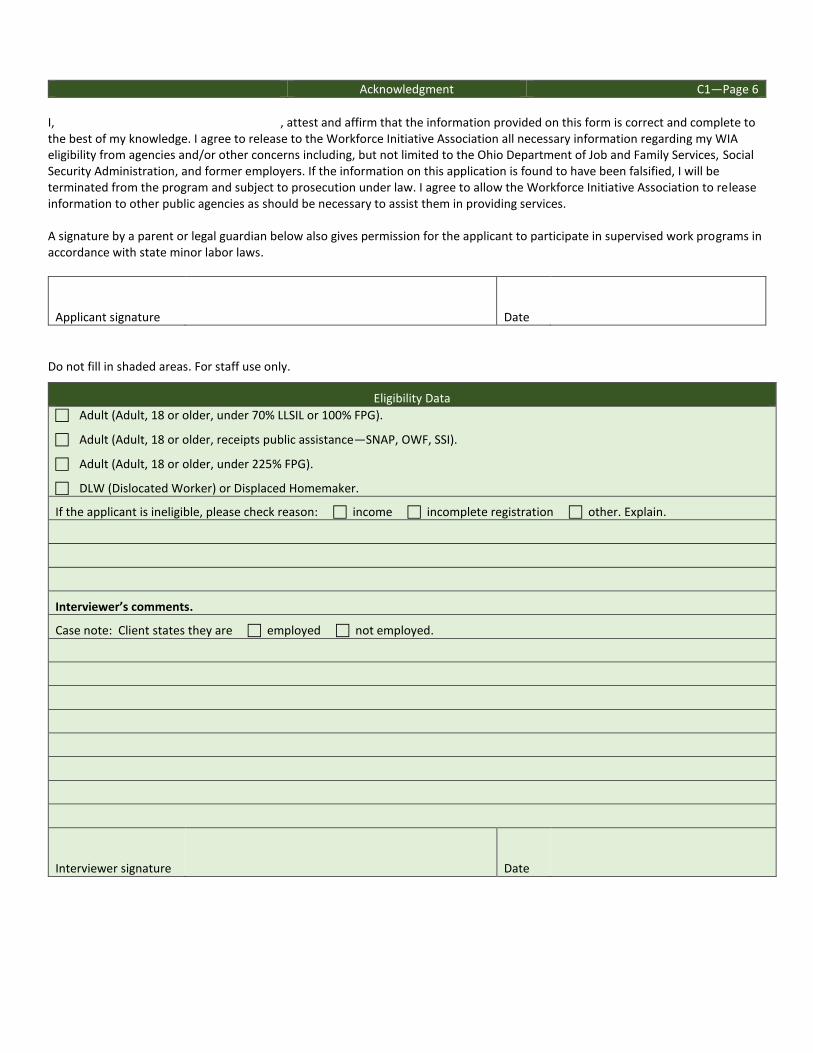
Acknowledgment C1—Page 6
I, , attest and affirm that the information provided on this form is correct and complete to the best of my knowledge. I agree to release to the Workforce Initiative Association all necessary information regarding my WIA eligibility from agencies and/or other concerns including, but not limited to the Ohio Department of Job and Family Services, Social Security Administration, and former employers. If the information on this application is found to have been falsified, I will be terminated from the program and subject to prosecution under law. I agree to allow the Workforce Initiative Association to release information to other public agencies as should be necessary to assist them in providing services. A signature by a parent or legal guardian below also gives permission for the applicant to participate in supervised work programs in accordance with state minor labor laws.
Applicant signature Date
Do not fill in shaded areas. For staff use only.
Eligibility Data
Adult (Adult, 18 or older, under 70% LLSIL or 100% FPG).
Adult (Adult, 18 or older, receipts public assistance—SNAP, OWF, SSI).
Adult (Adult, 18 or older, under 225% FPG).
DLW (Dislocated Worker) or Displaced Homemaker.
If the applicant is ineligible, please check reason: income incomplete registration other. Explain.
Interviewer’s comments.
Case note: Client states they are employed not employed.
Interviewer signature Date





























