Embed Size (px)
Citation preview

3/05/2016
1
The Research behind
Cogmed
2
Working memory:
The ability to simultaneously hold and manipulate information in the mind
Cogmed Coach Conference 05/09/14 Dr Izabela Walters
58724
3
Short term memory & working memory
Short term memory – the ability to hold information over a period of secondse.g.: repeat a sequence of digits or blocks
Working memory – the ability to hold and manipulate information
Short term memory capacity limits working memory performance: you need to be able to hold information before you can manipulate it
Cogmed Coach Conference 05/09/14 4
Executive function and working memory
Executive functionThe ability to:• start and stop behaviour
• Inhibit inappropriate behaviour• Change behaviour
• Plan and organise behaviour• Adjust behaviour in response to the environment
• Use feedback• Control attention (direct, ignore, shift)• Behave in a socially appropriate manner
Working memory is needed for some executive functions, e.g. planning, controlling attention
Cogmed Coach Conference 05/09/14

3/05/2016
2
5
Impulsivity and working memory
ImpulsivityReacting to stimuli without forethought.
Can be the result of executive dysfunction (inability to control attention), and be present without working memory dysfunction
Can co-exist with working memory impairment• controlled/top-down attention and working memory areas
overlap in the brain• Impulsive behaviour can result from the
inability/unwillingness to exert cognitive effort (working memory tasks are effortful)
Cogmed Coach Conference 05/09/14
Fluid intelligence and working memory
Fluid intelligence:Capacity to reason and solve problems in novel situations
Intelligence:• ‘What the intelligence tests measure’• it is correlated with academic capacity and the ability to solve
problems.
Consists of fluid intelligence, crystallised intelligence (fund of acquired knowledge), working memory, and speed of information processing.
• Working memory is related to intelligence – it is a part of it• Working memory can help with fluid intelligence tasks (bigger
space for reasoning), but it is not the same thing
6
7
What it is not:
”..working memory capacity is the same as central executivecapability, controlled attentionand general fluid intelligence”
(Engle, Kane, Tuholski, 1999)
If you define working memory as all of the above, you lose the ability to clearly describe it, to assess it and to selectively treat it. Working memory is related to all these functions, but it is NOT these functions.
Cogmed Coach Conference 05/09/14 Dr Izabela Walters
Newer Views of WM• Modality specific views of WM are beginning to change - There may
not be different WM functions for visual or verbal stimuli
• Capacity size and time dependent views of WM are changing…It is not about “size of WM space”, nor “decay of memory traces”
• Cognitive control mechanisms are the new keys to WM – ability to overcome interference from distracting stimuli and successfully complete the steps of the reasoning process, monitor their own performance, backtrack from wrong paths, etc. • This suggests that individuals with low WM may be able to
compensate through sustained effort • Must refresh and retrace their steps in the reasoning process
more frequently)• Requires “drive to task mastery”, and persistence or “grit”.
8

3/05/2016
3
Working memory is limited
Working memory can be improved with focused, specific and intensive training
9
Not all computerised wmtraining programs are the sameMany programsCogmed (Klingberg et al 2005)Jungle Memory (Alloway 2012)CogniFit (2008)N‐back training (Jaeggi et al 2008)Complex span training (Chein & Morrison 2010)
12 September 2014
Not all computerised wmtraining programs are the same
Many reviews:
A working memory training program can improve performance on non‐trained working memory tasksSystematic reviews: Chacko et al 2013, Melby‐Lervåg & Hulme 2013Narrative reviews: Morrison & Chein 2011, von Bastian & Oberauer 2013Meta‐analysis on Cogmed and inattention, Spencer‐Smith et al 2015Review in Science Diamond & Lee 2011, Interventions shown to aid executive function development in children 4 to 12
Understanding the ResearchCogmed (vs. everything else)
What sets Cogmed apart?• Solely simple and complex WM span tasks
o vs. mixed bag, unfocused training• Defined, sustained, and intense training protocol
o vs. train as you like• Coach driven methodology/professional support
o vs. poor or undocumented compliance and motivation
Melby-Lervåg & Hulme (2012) conducted a meta-analysis about WM training –just 8 out of 30 group comparisons were from Cogmed studies.
Measure Effect Size (d)
Mean VS WM 0.52
Cogmed VS WM 0.86
Mean Verbal WM 0.79
Cogmed Verbal WM 1.18
3/05/2016
4
13
Bacon Causes Cancer? Sort of. Not Really. Ish.
http://www.wired.com/author/sarahzhang/
Key questions1. What does it mean to be “evidence-based”?
2. Does training improve working memory?
3. Does the training generalise beyond trained tasks to non-trained tasks?
4. Are the gains sustained?
5. Can working memory training improve literacy and numeracy outcomes?
• Based on a scientific discovery
• Validated by independent researchers
• Data presented worldwide at conferences
• Studies published in peer-reviewed journals
• Validated by use in clinical (real world) setting
Embracing the term: What do we mean by evidence-based cognitive training?
Cogmed and the world of academic research: An important relationship
Original idea, prototype and funding from Karolinska Institute• Company founded by research team: Klingberg, Westerberg and developers
Company was funded by Karolinska Development AB (2001- 6/28/2010)• A fund investing only in products stemming from academic research
Klingberg independent of Pearson• Professor of Cognitive Neuroscience at Karolinska
The research published to date generates much interest• Cogmed gets research proposals from around the world
Research collaborations are a key part of strategy• Simple relationship: no payments from Cogmed, publishing freely
3/05/2016
5
How Cogmed is different to other “brain training” programs that claim to be evidence-based
• Cogmed is very careful about aligning claims with evidence
• The cognitive effects associated with Cogmed training have been demonstrated in 80+ peer reviewed published studies by many independent research groups from around the world
• Those studies all involve testing the efficacy of Cogmed – the same program used by clinicians and schools
• NOT: quote from a single scientist, “developed by neuroscientists”, based in findings from a single study, based on proprietary in-house studies
17
General quality of research
For a study to be considered to be of sufficient quality to contribute to a claim, the criteria listed below must be met
• Reliable and valid outcome measures• Design that supports the hypothesis• Statistical methods that support the question being investigated• Study on recommended population according to Cogmed training
manual - exclusions• Implementation with high fidelity to Cogmed recommendations
regarding coaching method, study population, and high quality of training
What does Cogmed Claim?1) CWMT leads to sustained improvements in working memory, from childhood to
adulthood
2) CWMT leads to sustained improvements in attention seen in both subjective and
objective measures of attention
3) Improvements in working memory following CWMT are associated with changes in
functional brain activity related to working memory and functional connectivity at rest
4) Learning outcomes in reading and math improves for many students following CWMT
5) In clinical trials, CWMT has been shown to improve attentional problems in many with
ADHD
6) Research studies of CWMT report improved cognitive functioning in daily life 7) Adults
with acquired brain injury report reductions of symptoms after CWMT in clinical trials
8) Improvements on measures of cognitive control have been demonstrated in studies
after CWMT
How do you measure the efficacy of an evidence-based program?
Performance on the training tasks
Performance on tasks similar to the training tasks
Performance on tasks that rely on skills trained
Performance in daily life

3/05/2016
6
Key questions1. What does it mean to be “evidence-based”?
2. Does training improve working memory?
3. Does the training generalise beyond trained tasks to non-trained tasks?
4. Are the gains sustained?
5. Can working memory training improve literacy and numeracy outcomes?
Research discovers working memory can be improved
Led by neuroscientist T.Klingberg, MD, PhD
The findings challenged for the first time the long-held assumption that working memory is a fixed characteristic, unable to be changed.
ReplicationKlingberg replicates first study in placebo controlled,
multicenter trial - drawing attention to WM training(Klingberg et al., 2005)

3/05/2016
7
Population: N = 53 children with ADHD (combined & inattentive), ages 7 -12 years,
no stimulant medication
n = 24 in adaptive Cogmed training group n = 26 in non-adaptive (placebo) Cogmed training groupn = 3 withdrew
Design: Multi-site, randomized, placebo controlled, double-blinded, test-retest
T1= Baseline, T2 = Post-test, T3 = 3 month follow up
Results:
Treatment group improved significantly over active control on outcomes measures:1) Non practiced visuo-spatial WM task (Span Board; WAIS-RNI)2) Non practiced verbal WM task (Digit Span; WISC-III)
Computerized training of working memory in children with ADHD: a randomized, controlled trial
Klingberg et al., 2005
Computerized training of working memory in children with ADHD: a randomized, controlled trial
Klingberg et al., 2005
“…This study shows that WM can be improved by training. In addition, we saw effects on reasoning, response inhibition, and a
decrease in parent-rated symptoms of ADHD.…”
1. Expands on Klingberg et al.,2002 – replication
2. Placebo condition (low dose training)
3. Multi-site, Randomized, Double -blinded, Placebo controlled
4. Published in leading peer-reviewed journal (JAACAP)
5. Shows results remain after 3 months
6. Shows effects on parent ratings (blinded)
7. Shows effects on neuropsychological tests (attention and impulse control)
8. Shows improvement on complex problem solving
9. Does not show significant effects on teacher ratings or head movement
SummaryKlingberg et al., 2005
Other Studies showing generalised effects of CWMT

3/05/2016
8
Does training improve working memory?
• ’’ . . . results of individual studies encourage optimism regarding the value of WM training as a tool for general cognitive enhancement’’ (Morrison & Chein, 2011, p. 46).
• Diamond and Lee (2011) specifically described Cogmed as both the most researched approach of computerized training and ‘‘one repeatedly found to be successful’’ and concluded that Cogmed improves WM and executive functions.
• ‘‘WM training programs produced reliable short-term improvements in both verbal and visuospatial WM skills’’ (Melby-Lervag & Hulme, 2013, p. 270).
Key questions1. What does it mean to be “evidence-based”?
2. Does training improve working memory?
3. Does the training generalise beyond trained tasks to non-trained tasks?
4. Are the gains sustained?
5. Can working memory training improve literacy and numeracy outcomes?
How do we monitor progress? Questionnaire
Sources:- 4-17yo: DSM-IV ADHD (attention) scale- Intrinsic Motivation Inventory (IMI)
Pre: Prior to Day 1 CPI and Training, during Start-Up Session with CoachPost: Available to complete after 80% of training has been completed
Captures users perspective of their Attention in everyday life
Expectations for CWMT, Areas they would like to improve
Training Details
3/05/2016
9
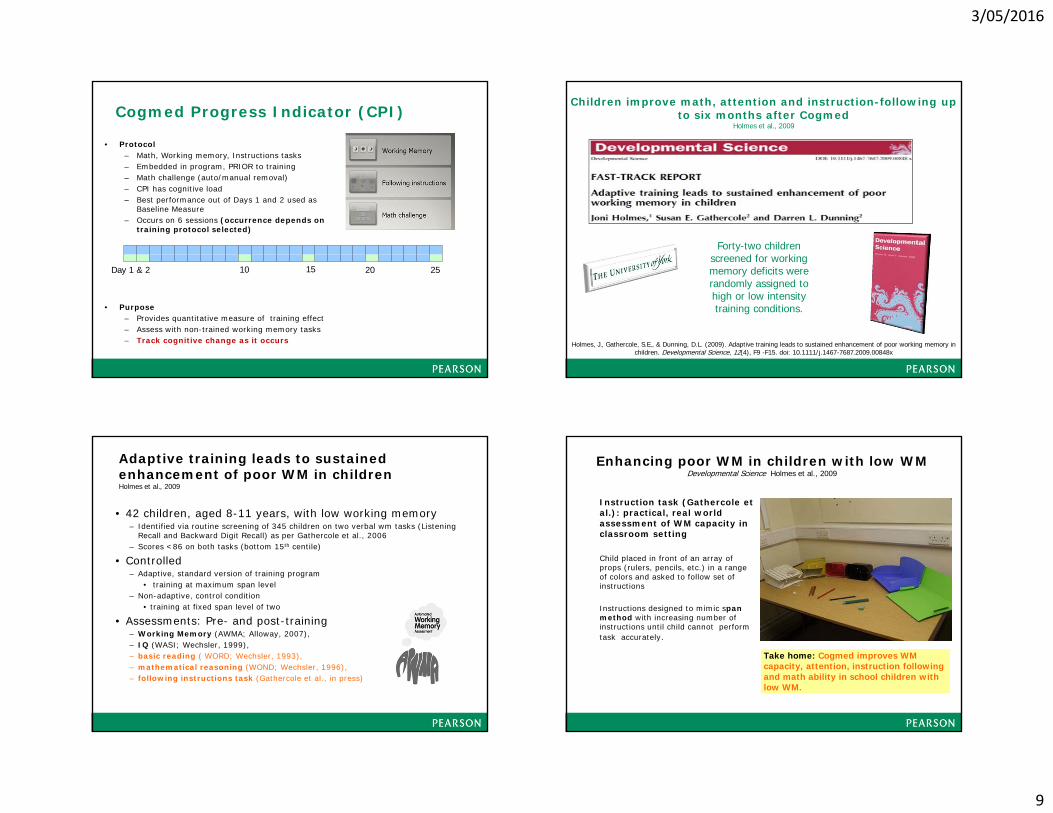
Cogmed Progress Indicator (CPI)
• Protocol– Math, Working memory, Instructions tasks– Embedded in program, PRIOR to training– Math challenge (auto/manual removal)– CPI has cognitive load– Best performance out of Days 1 and 2 used as
Baseline Measure – Occurs on 6 sessions (occurrence depends on
training protocol selected)
• Purpose– Provides quantitative measure of training effect– Assess with non-trained working memory tasks– Track cognitive change as it occurs
Day 1 & 2 10 15 2520
Children improve math, attention and instruction-following up to six months after Cogmed
Holmes et al., 2009
Forty-two children screened for working memory deficits were randomly assigned to high or low intensity training conditions.
Holmes, J., Gathercole, S.E., & Dunning, D.L. (2009). Adaptive training leads to sustained enhancement of poor working memory inchildren. Developmental Science, 12(4), F9 -F15. doi: 10.1111/j.1467-7687.2009.00848x
• 42 children, aged 8-11 years, with low working memory – Identified via routine screening of 345 children on two verbal wm tasks (Listening
Recall and Backward Digit Recall) as per Gathercole et al., 2006– Scores <86 on both tasks (bottom 15th centile)
• Controlled– Adaptive, standard version of training program
• training at maximum span level– Non-adaptive, control condition
• training at fixed span level of two
• Assessments: Pre- and post-training– Working Memory (AWMA; Alloway, 2007), – IQ (WASI; Wechsler, 1999), – basic reading ( WORD; Wechsler, 1993), – mathematical reasoning (WOND; Wechsler, 1996), – following instructions task (Gathercole et al., in press)
Adaptive training leads to sustained enhancement of poor WM in childrenHolmes et al., 2009
Enhancing poor WM in children with low WM Developmental Science Holmes et al., 2009
Instruction task (Gathercole et al.): practical, real world assessment of WM capacity in classroom setting
Child placed in front of an array of props (rulers, pencils, etc.) in a range of colors and asked to follow set of instructions
Instructions designed to mimic span method with increasing number of instructions until child cannot perform task accurately.
Take home: Cogmed improves WM capacity, attention, instruction following and math ability in school children with low WM.

3/05/2016
10
Restricted Academic Situations Task (RAST)
• 5 categories of behavior associated with ADHD scored at 30 sec intervals
• Given toys to play with for 5 minutes; examiner puts toys to the side , participants asked to complete easy math packet for 15 minutes while videotaped
• Good indicator of behavioral responses to ADHD stimulant medication
• Consistent with externalizing teacher ratings and actometer measures of ADHD
• Objective measure and sensitive to moment-to-moment changes in “off-task” behavior
Will working memory training generalize to improve off-task behavior in children with Attention-Deficit/
Hyperactivity Disorder?Green et al. 2012
Green et al 2012Publication: Neurotherapeutics Institution: University of California, Davis Investigator(s): Chloe T. Green, Debra L. Long, David Green, Ana-Maria Iosif, J. Faye Dixon, Meghan R. Miller, Catherine Fassbender, Julie B. Schweitzer
• Randomized, placebo controlled, double-blinded study of 26 children with ADHD first known research to demonstrate the impact of WM training on an ecologically valid measure of observable ADHD-associated behaviours - RAST
• Children who trained with the standard Cogmed program (adaptive WM training) improved significantly over children in the placebo group (non-adaptive WM training) on non-trained, widely used, standardized measures of WM (Digit Span and Letter-Number Sequencing; WISC) and on measures of the Restricted Academic Setting Task (RAST) that related to attention.
Reciprocal Relationship between WM, Anxiety and Learning
• 5% of children and young people experience clinical levels of anxiety
• Negative emotional states are associated with lowered performance
• Strong association between anxiety and executive functions (i.e. inhibition, set-shifting and updating information in working memory)
• Negative affect and academic performance in school is mediated or moderated by WM functioning or attentionalprocessing
>> Increasing academic performance via improvements in WM may reduce feelings of negative affect
The impact of working memory training in young people with social, emotional and behavioural difficulties L. Roughan, J.A. Hadwin / Learning and Individual Differences 21 (2011)
This study examined the impact of working memory training in 65 typically developing 4-5 year-old children.
3/05/2016
11
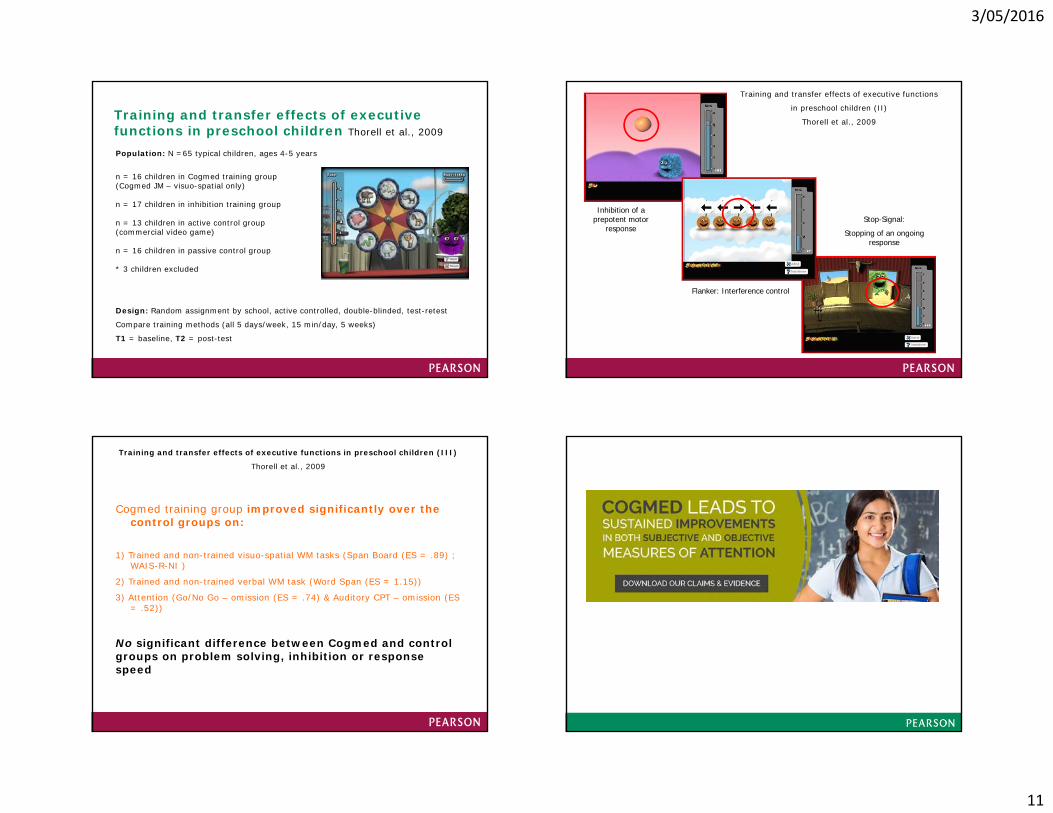
Training and transfer effects of executive functions in preschool children Thorell et al., 2009
Population: N =65 typical children, ages 4-5 years
n = 16 children in Cogmed training group(Cogmed JM – visuo-spatial only)
n = 17 children in inhibition training group
n = 13 children in active control group(commercial video game)
n = 16 children in passive control group
* 3 children excluded
Design: Random assignment by school, active controlled, double-blinded, test-retest
Compare training methods (all 5 days/week, 15 min/day, 5 weeks)
T1 = baseline, T2 = post-test
Go/No-Go:
Inhibition of a prepotent motor
responseStop-Signal:
Stopping of an ongoing response
Flanker: Interference control
Training and transfer effects of executive functions
in preschool children (II)
Thorell et al., 2009
Cogmed training group improved significantly over the control groups on:
1) Trained and non-trained visuo-spatial WM tasks (Span Board (ES = .89) ; WAIS-R-NI )
2) Trained and non-trained verbal WM task (Word Span (ES = 1.15))
3) Attention (Go/No Go – omission (ES = .74) & Auditory CPT – omission (ES = .52))
No significant difference between Cogmed and control groups on problem solving, inhibition or response speed
Training and transfer effects of executive functions in preschool children (III)
Thorell et al., 2009

3/05/2016
12
12 September 2014
A systematic review and meta-analysis of the benefits of Cogmed for inattention in daily life
Megan Spencer-Smith & Torkel Klingberg
Identified studies
12 September 2014
Study Participants Risk of bias Control group
Training site
Time of testing post‐training
Outcome measures
Age in years
Status Recruitment source Design Blindinga) Rater b) Tester
Immediate
Delayed Inattention in daily life (rater)
Visuospatial WM Verbal WM
Bjorkdahl2013+*
22‐63 Brain Injury + impaired WM
Outpatient rehabilitation clinic
RCT a) NRb) NR
Passive NR 1 week 3 months Working memory questionnaire (self)
none WAIS‐III Digit span backward
Beck 2010* 7‐17 ADHDb Private school for students with ADHD and/or LD
RCT a) pre trainingb) NR
Wait‐list Home 1 month 4 months DSM‐IV Inattention (parent)
none none
Brehmer2012
a) 20‐30b) 60‐70
Healthy Newspaper advertisement RCT a) yes b) yes
Active and non‐adaptive
Home NR 3 months CFQ (self) WAIS‐R Span board backward
WAIS‐R Digit span backward
Chacko 2013a 7‐11 ADHD Newspaper advertisements
RCT a) yesb) yes
Active and non‐adaptive
Home 3 weeks none DBD Inattention (parent)
AWMA Spatial recall AWMA Listening recall
Egeland 2013 10‐12 ADHDb Outpatient clinics at two hospitals
RCT a) NRb) Yes
Wait‐list School NR 8 months DuPaul Inattention (parent)
none none
Green 2012 7‐14 ADHDb, c Advertising, psychologists, psychiatrists, institute tracking
RCT a) yesb) Yes
Active and non‐adaptive
Home NR none Connors ADHD (parent)
none none
Gropper 2013 19‐52 LD/ADHDb Student Disability services at 3 post‐secondary institutions
RCT a) NRb) NR
Wait‐list Home 3 weeks 2 months CFQ (self) CANTAB Spatial WM (errors)
WISC‐IV Digit span
Grunewaldt 2013
5‐6 VLBW Admission records of a hospital NICU
RCT a) NRb) Yes
Wait‐list Home 1 month none DuPaul Inattention (parent)
Spatial span backwarda
Digit span backwarda
Hardy 2013 8‐16 Cancer Patients of the hospital Division of Pediatric Hematology‐Oncology
RCT a) yesd
b) YesActive and non‐adaptive
Home NR 3 months Connors Inattention (parent)
WRAML Symbolic WM
WRAML Verbal WM
Klingberg 2005
7‐12 ADHD Referrals from pediatricians, psychiatrists, special school teachers
RCT a) yesb) yes
Active and non‐adaptive
Home or school
NR 3 months DSM‐IV Inattention (parent)
WAIS‐R Span board WAIS‐R Digit span
Roughen 2011
15‐17 SEB Schools RCT a) nob) NR
Passive School 3 weeks 3 months DuPaul AttentionalControl (teacher)
none none
Westerberg 2007
34‐65 Stroke Stroke Rehabilitation Unit RCT a) pre training b) pre training
Passive Home NR none CFQ (self) WAIS‐R Span board WAIS‐R Digit span
Benefits of a Working Memory TrainingProgram for Inattention in Daily Life: ASystematic Review and Meta-Analysis
"Benefits of a WM training program generalise to improvements in everyday functioning. Initial evidence shows that the Cogmed method has significant benefits for inattention in daily life with a clinically relevant effect size"
Megan Spencer-Smith, Torkel Klingberg. PLoS ONE 10(3): e0119522
• Efficacious method with meaningful results: not all WMT approaches/programs are the same.
• The Gold Standard of Research: clear information about the inclusion criteria for the study. Analyses summarizing the effects from 12 randomized controlled trials, studying the effects related to Cogmed working memory training.
• Relevant size: Cogmed WMT has a significant (i.e. moderate) effect on inattention in daily life, an important piece of far transfer. Effects were in the moderate range (0.40-0.66), considered relevant in the education domain .
• Sustained effects: Effects on everyday attention are shown to be largely sustained.
• Cogmed is good for all: (not just ADHD)

3/05/2016
13
Key questions1. What does it mean to be “evidence-based”?
2. Does training improve working memory?
3. Does the training generalise beyond trained tasks to non-trained tasks?
4. Are the gains sustained?
5. Can working memory training improve literacy and numeracy outcomes?
Children improve math, attention and instruction-following up to six months after CogmedHolmes et al., 2009
Forty-two children screened for working memory deficits were randomly assigned to high or low intensity training conditions.
Holmes, J., Gathercole, S.E., & Dunning, D.L. (2009). Adaptive training leads to sustained enhancement of poor working memory inchildren. Developmental Science, 12(4), F9 -F15. doi: 10.1111/j.1467-7687.2009.00848x
Pre- training WM scores for non-adaptive (placebo) group
Holmes et al., 2009
60.00
70.00
80.00
90.00
100.00
110.00
120.00
Verbal STM Visuo-spatial STM Verbal WM Visuo-spatial WM
Pre- Post-
Slide courtesy of Dr. Joni Holmes
60.00
70.00
80.00
90.00
100.00
110.00
120.00
Verbal STM Visuo-spatialSTM
Verbal WM Visuo-spatialWM
Pre- Post-
**
Slide courtesy of Dr. Joni Holmes
Pre- training to post-training WM scores for non-adaptive (placebo) group
Holmes et al., 2009
3/05/2016
14
60.00
70.00
80.00
90.00
100.00
110.00
120.00
Verbal STM Visuo-spatial STM Verbal WM Visuo-spatial WM
Pre-Post-
Slide courtesy of Dr. Joni Holmes
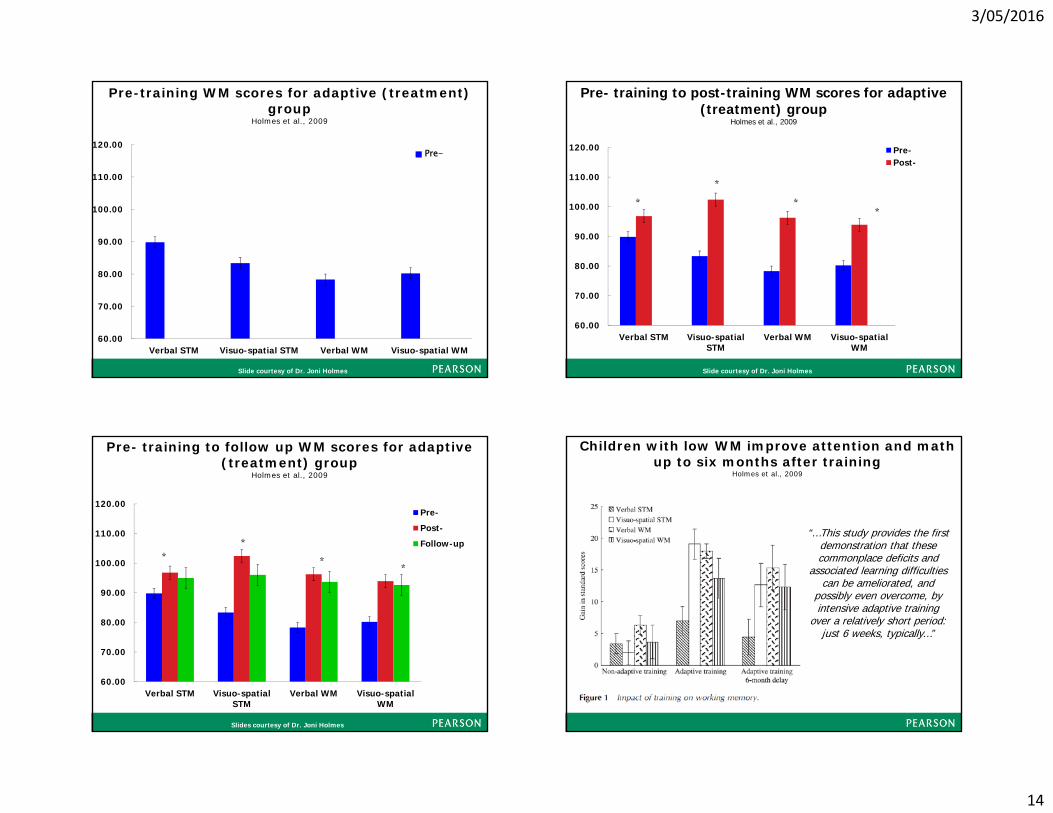
Pre-training WM scores for adaptive (treatment) group
Holmes et al., 2009
60.00
70.00
80.00
90.00
100.00
110.00
120.00
Verbal STM Visuo-spatialSTM
Verbal WM Visuo-spatialWM
Pre-Post-Follow-up
**
**
Slide courtesy of Dr. Joni Holmes
Pre- training to post-training WM scores for adaptive (treatment) group
Holmes et al., 2009
60.00
70.00
80.00
90.00
100.00
110.00
120.00
Verbal STM Visuo-spatialSTM
Verbal WM Visuo-spatialWM
Pre-
Post-
Follow-up*
** *
Slides courtesy of Dr. Joni Holmes
Pre- training to follow up WM scores for adaptive (treatment) group
Holmes et al., 2009
Children with low WM improve attention and math up to six months after training
Holmes et al., 2009
“…This study provides the first demonstration that these commonplace deficits and
associated learning difficulties can be ameliorated, and
possibly even overcome, by intensive adaptive training
over a relatively short period: just 6 weeks, typically…”
3/05/2016
15
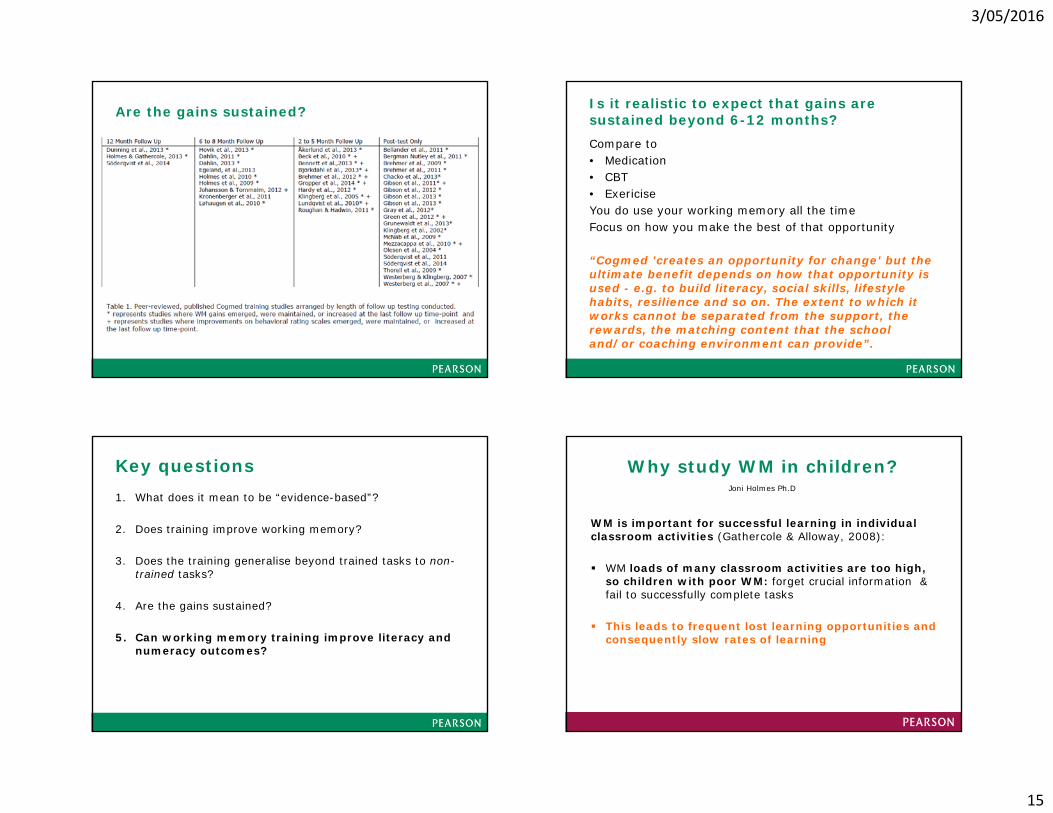
Are the gains sustained? Is it realistic to expect that gains are sustained beyond 6-12 months?Compare to • Medication• CBT• ExericiseYou do use your working memory all the timeFocus on how you make the best of that opportunity
“Cogmed 'creates an opportunity for change' but the ultimate benefit depends on how that opportunity is used - e.g. to build literacy, social skills, lifestyle habits, resilience and so on. The extent to which it works cannot be separated from the support, the rewards, the matching content that the school and/or coaching environment can provide”.
Key questions1. What does it mean to be “evidence-based”?
2. Does training improve working memory?
3. Does the training generalise beyond trained tasks to non-trained tasks?
4. Are the gains sustained?
5. Can working memory training improve literacy and numeracy outcomes?
WM is important for successful learning in individual classroom activities (Gathercole & Alloway, 2008):
WM loads of many classroom activities are too high, so children with poor WM: forget crucial information & fail to successfully complete tasks
This leads to frequent lost learning opportunities and consequently slow rates of learning
Why study WM in children? Joni Holmes Ph.D

3/05/2016
16
Improving Working Memory – Supporting Student learning – Tracy Packiam Alloway 2011
Interconnected Systems Supporting Learning
Knowledge base (LTM)
*largely mediated by language
Performance‐based factors
*working memory
Immediate and delayed effects
In recent years, academic performance has been measured in an increasing number of studies following CWMT. • Some studies have shown significant academic improvements
directly following CWMT (13, 35, 43)
• while others have not seen any effects (7) or not shown statistical significance of the effects (32, 33), compared to a non-adaptive WM training group.
However, for those studies including follow up measures, there seems to be a pattern emerging showing delayed effects on learning outcomes following CWMT• RCT by Dunning et al (33), the effect size on reading rate went
from non-existent (d= 0.04) directly following training, to medium (d = 0.66) at the follow up one year later, compared to controls.
[Far transfer] Skill/behaviour
[Near transfer]Affects
Executive functions
Rate of learning Remembering directions
Attention/Concentration
Working memory Planning
Reading comprehension Maths skills On-task
behaviour
Initiate
Manipulating information
Task monitoring Organise
Language development
Working memory training acts on underlying levels
3/05/2016
17
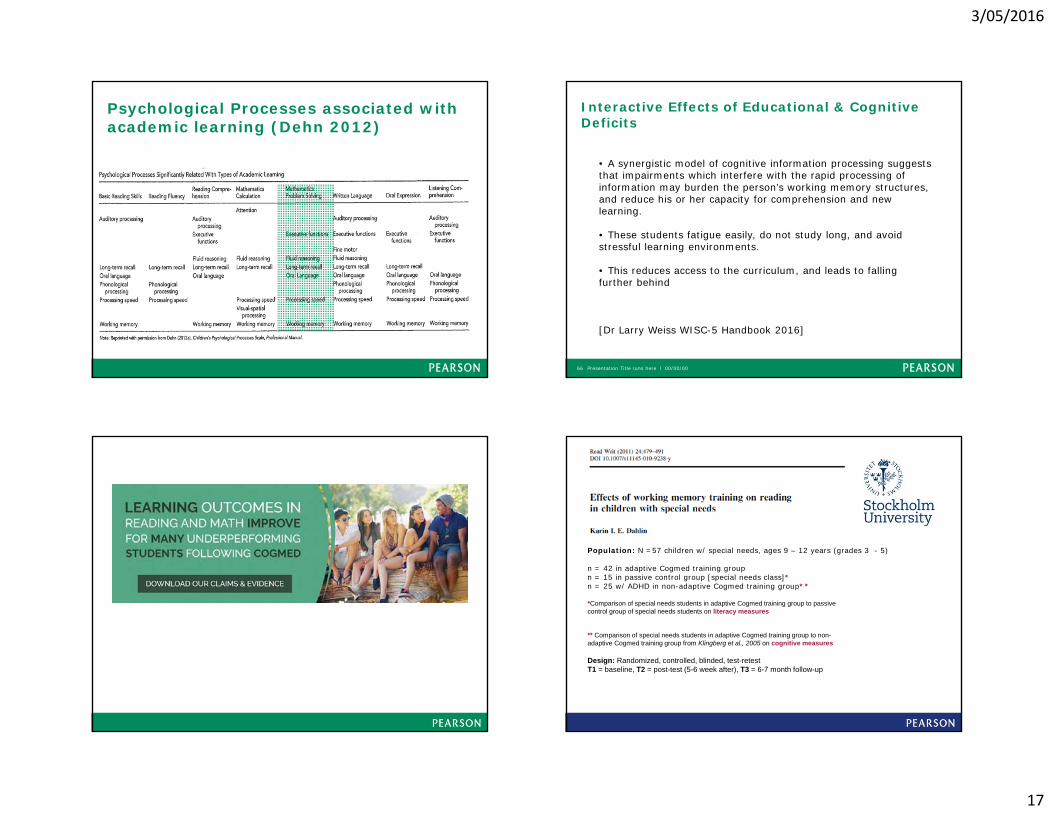
Psychological Processes associated with academic learning (Dehn 2012)
Interactive Effects of Educational & Cognitive Deficits
Presentation Title runs here l 00/00/0066
• A synergistic model of cognitive information processing suggests that impairments which interfere with the rapid processing of information may burden the person’s working memory structures, and reduce his or her capacity for comprehension and new learning.
• These students fatigue easily, do not study long, and avoid stressful learning environments.
• This reduces access to the curriculum, and leads to falling further behind
[Dr Larry Weiss WISC-5 Handbook 2016]
Population: N =57 children w/ special needs, ages 9 – 12 years (grades 3 - 5)
n = 42 in adaptive Cogmed training groupn = 15 in passive control group [special needs class]*n = 25 w/ ADHD in non-adaptive Cogmed training group**
*Comparison of special needs students in adaptive Cogmed training group to passive control group of special needs students on literacy measures
** Comparison of special needs students in adaptive Cogmed training group to non-adaptive Cogmed training group from Klingberg et al., 2005 on cognitive measures
Design: Randomized, controlled, blinded, test-retestT1 = baseline, T2 = post-test (5-6 week after), T3 = 6-7 month follow-up
3/05/2016
18
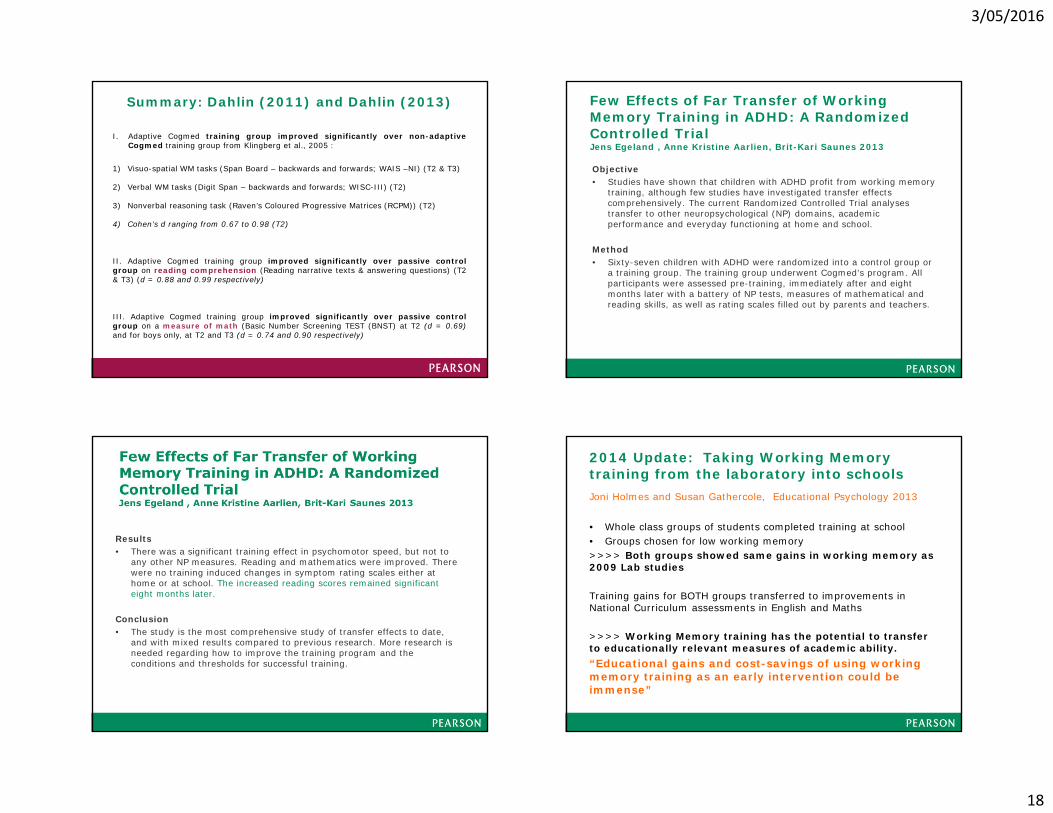
I. Adaptive Cogmed training group improved significantly over non-adaptiveCogmed training group from Klingberg et al., 2005 :
1) Visuo-spatial WM tasks (Span Board – backwards and forwards; WAIS –NI) (T2 & T3)
2) Verbal WM tasks (Digit Span – backwards and forwards; WISC-III) (T2)
3) Nonverbal reasoning task (Raven’s Coloured Progressive Matrices (RCPM)) (T2)
4) Cohen’s d ranging from 0.67 to 0.98 (T2)
II. Adaptive Cogmed training group improved significantly over passive controlgroup on reading comprehension (Reading narrative texts & answering questions) (T2& T3) (d = 0.88 and 0.99 respectively)
III. Adaptive Cogmed training group improved significantly over passive controlgroup on a measure of math (Basic Number Screening TEST (BNST) at T2 (d = 0.69)and for boys only, at T2 and T3 (d = 0.74 and 0.90 respectively)
Summary: Dahlin (2011) and Dahlin (2013) Few Effects of Far Transfer of Working Memory Training in ADHD: A Randomized Controlled Trial Jens Egeland , Anne Kristine Aarlien, Brit-Kari Saunes 2013
Objective• Studies have shown that children with ADHD profit from working memory
training, although few studies have investigated transfer effects comprehensively. The current Randomized Controlled Trial analyses transfer to other neuropsychological (NP) domains, academic performance and everyday functioning at home and school.
Method• Sixty-seven children with ADHD were randomized into a control group or
a training group. The training group underwent Cogmed’s program. All participants were assessed pre-training, immediately after and eight months later with a battery of NP tests, measures of mathematical and reading skills, as well as rating scales filled out by parents and teachers.
Results• There was a significant training effect in psychomotor speed, but not to
any other NP measures. Reading and mathematics were improved. There were no training induced changes in symptom rating scales either at home or at school. The increased reading scores remained significant eight months later.
Conclusion• The study is the most comprehensive study of transfer effects to date,
and with mixed results compared to previous research. More research is needed regarding how to improve the training program and the conditions and thresholds for successful training.
2014 Update: Taking Working Memory training from the laboratory into schoolsJoni Holmes and Susan Gathercole, Educational Psychology 2013
• Whole class groups of students completed training at school• Groups chosen for low working memory>>>> Both groups showed same gains in working memory as 2009 Lab studies
Training gains for BOTH groups transferred to improvements in National Curriculum assessments in English and Maths
>>>> Working Memory training has the potential to transfer to educationally relevant measures of academic ability. “Educational gains and cost-savings of using working memory training as an early intervention could be immense”
3/05/2016
19
Working Memory Training is Associated with Long Term Attainments in Math and ReadingStina Söderqvist* and Sissela Bergman Nutley
Followed the academic performance of two age-matched groups during 2 years. As part of the curriculum in grade 4 (age 9–10), all students in one classroom (n = 20) completed Cogmed Working Memory Training (CWMT) whereas children in the other classroom (n = 22) received education as usual. Performance on nationally standardized tests in math and reading was used as outcome measures at baseline and two years later.
At baseline both classes were normal/high performing according to national standards.
At grade 6, reading had improved to a significantly greater extent for the training group compared to the control group (medium effect size, Cohen’s d = 0.66, p = 0.045).
For math performance the same pattern was observed with a medium effect size (Cohen’s d = 0.58) reaching statistical trend levels (p = 0.091).
Moreover, the academic attainments were found to correlate with the degree of improvements during training (p < 0.053).
>> Results suggest improved working memory boosts student’s capacity to learn
Roberts study 2016
Roberts, G., Quach, J., Spencer Smith, M., Anderson, P., Gathercole, S., Gold, L., Sia, KL., Mensah, F., Rickards, F., Ainley, J. & Wake, M. (2016). Working memory intervention does not improve long-term academic outcomes: A school-based population randomised controlled trial. JAMA Pediatrics
Objective: to investigate whether 6 year-old children at risk for academic underachievement, for whom approximately 20-25 hours of formal teaching was substituted with Cogmed working memory training (CWMT), would outperform children receiving formal teaching as usual on measures of academic performance two years later.
Important highlights
• Method – good numbers and controls – we need more studies like this• Feasibility – population based assessment and training can be administered• Sustained effects on memory – yes to 12 months, not significant at 2 years• Academic outcomes – training group did not outperform control group on academic measure (WRAT4)• Importance of age – Is 6-7 a good age for training?
Limits to consider
• How school outcomes measured – strong conclusions? Based on one academic measure, variability of baseline at age 6 not measured but very important
• Intent is not to replace classroom learning• Screening - Academic performance was in the normal range, Was WM perhaps not the only bottleneck for
academic growth in a large portion of the sample?• Reported on completion of training vs quality and intensity of training – coaching and effort matters• Choice of product and protocol
Q1. Did students in this study, who trained with Cogmed at school, improve their working memory?Yes. Students that trained with Cogmed RM had significantly higher verbal WM visuo-spatial short term memory compared to the passive control at 6 months following training. Gains in visuospatial short term memory were also maintained at 12 months post-training but these improvements were no longer statistically significant 24 months post training.
Q2. If the students in this research did not experience improvements in maths or reading, does this mean Cogmed does not lead to gains in academic performance in general? This study does not answer that question. Neither does any single study. Results need to be replicated in order to be generalisable.
Further research will be done by this group to explore who training was successful for. 6 year olds may differ more in their early learning of reading and maths for other reasons (e.g. phonological awareness, vocabulary, number and letter knowledge etc.) than their different WM capacities.
Cogmed and academic change?
Factors that determine improvements on academic performance after training with Cogmed are yet not entirely understood • age at which the training is implemented • instruments used to assess the academic change
(school tests or ability tests) • the comparison condition (in this case the control group
received >20 hours more of formal education) • the degree to which working memory is taxed in those
particular tests • the maintenance of the improved working memory and
how it is utilized in learning post training

3/05/2016
20
Clinical and real world data counts too72% of schools who used Cogmed in ANZ in 2014 renewed in 2015
5/3/201678 Cogmed Coach Conference 19/07/13CogCon AUNZ 201378
Time Taken (Initial Review to Completion 8.2, 8.5)
Dr Jason McGowan, Child Development Centre
5/3/201679 Cogmed Coach Conference 19/07/13CogCon AUNZ 201379
Gain in Reading Age (20, 25 months)
Dr Jason McGowan, Child Development Centre 5/3/201680 Cogmed Coach Conference 19/07/13CogCon AUNZ 201380
Change in Reading Rate (2.6, 3.2 months / month)
80 Dr Jason McGowan, Child Development Centre

3/05/2016
21
+
Design: Randomized, Controlled, Test-Retest, 6 Month Follow Up
Sample: N = 245, 7th graders, at least 1 year behind in reading
Additional Data: SAT 10 (Reading), STAAR (Texas State Assessment), Demographics
T1April 2014
Intervention Phase I
T2 May 2014
T3 August 2014
InterventionPhase II
T4December 2014
CPI/CQBASC-2ParentBASC-2 TeacherBASC-2 StudentGRADE (Reading)
Cogmed CPI/CQBASC-2Student
CPI/CQBASC-2 ParentBASC-2TeacherBASC-2 StudentGRADE (Reading)
iLit CPI/CQBASC-2 ParentBASC-2TeacherBASC-2 StudentGRADE (Reading)
Passive iLit
Passive Passive
Cogmed Slide Library 2014
https://www.youtube.com/watch?v=8UXLSvXF8vQ
Future research – questions Do benefits persist?
Can the benefits be enhanced?e.g. Cogmed Plus
Can a reduced training schedule produce benefits?
What individual characteristics are important for benefits? Motivation (Martinussen et al 2005, Nymberg et al under review) ADHD comorbidity such as ODD (Chacko et al 2013) Age (Brehmer et al 2012)
12 September 2014
Implementing a Working Memory Program At Your School
Next webinar: Tuesday 21 June @ 12.30-1.30 (AEST)
See a recording of webinar at:www.pearsonclinical.com.au/archive

3/05/2016
22
Presentation Title runs here l 00/00/0085
Perth – Pan Pacific HotelFriday 19th August
Brisbane – Pullman HotelWednesday 17th August
Register by 24th June to receive the early bird price of $379 (Incl. GST)
Go to pearsonacademy.com.au





























