Embed Size (px)
Citation preview

Worksite Wellness in the 21st Century: The Baptist Health South Florida Experience
Theodore Feldman MD FACC FACPMedical Director, Center for Prevention and
Wellness, Baptist Health South FloridaClinical Associate Professor of Medicine
FIU Wertheim College of Medicine

Background• 130 million Americans are employed across the United
States• A huge proportion of health care cost is covered by the
employer.• Health care costs in the United States doubled from 2001-
2012• 60 percent of employers’ after-tax profits are spent on
corporate health benefits – 3 decades ago, 7 percent of corporate profits paid for health
costs• Significant attention is being paid in health maintenance

• 27 studies• 6 RCT• Small sample sizes• Outcomes: Changes in risk factors and behaviors• Follow-up: Limited in majority of studies
Evidence of Employee Health Related Issues is Limited.

Return on Investment: Projected risk modeling between changes in risk factors and the subsequent impact on ROI.

Challenges in Implementing Best Practices/Program within Employee Population
• Lack of concrete comparative effectiveness research – Temporal trends patterns of burden of disease– Impact of interventions – Concrete outcomes for prevention strategies
• Intermediate (surrogate) outcomes• Health care costs• Hard outcomes
• Effective and rigorously tested evidence is needed

Employee Health Outcomes

Where Do We Stand with CVD Employee Prevention Programs at Baptist Health South Florida?


The Baptist Health South Florida Employee Study
Design and Setting Cross sectional study conducted among employees
of BHSF, a large not-for-profit Health care organization
Incentive driven Health Risk Assessment (HRA) is offered annually to employees
Employee participation is voluntary Total employee population is approximately 15,000 9364 employees participated in 2014 HRA

The Baptist Health South Florida Employee Study
Data Collection Self-administered online questionnaire Age, gender, diet, smoking status, physical
activity levels etc Biometric measures taken by trained health
care professionals Height, weight, BMI, blood pressure, blood
glucose and total cholesterol etc

The Baptist Health South Florida Employee Study
Definition of Cardiovascular Health Metrics Ideal cardiovascular health defined by the AHA as
the absence of disease and presence of 7 health factors and behaviors
Blood pressure, cholesterol & fasting plasma glucose
Smoking, physical activity, diet & body mass index To measure and assess progress towards AHA 2020
goal the CV health metrics are categorized as Ideal, Intermediate and Poor

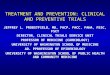
Baptist Health Employees Vs National Estimates
Total Cholesterol
Blood Pressure
Plasma Glucose
Physical Activity
Health Diet Score
Smoking BMI0%
10%20%30%40%50%60%70%80%90%
100%
8 5 4 5
51
2
3326
58
5
20
46
1
36
66 37 91 78 3 97 31
Poor Intermediate Ideal
Total Cholesterol
Blood Pressure
Plasma Glucose
Physical Activity
Health Diet Score
Smoking BMI0%
10%20%30%40%50%60%70%80%90%
100%
13 148
48
79
20
35
40 42
34
11
20
3
33
47 44 57 41 1 77 31
Poor Intermediate IdealNHANES
BHSF

Trends of the prevalence of ideal status for each cardiovascular health metric from 2011
to 2013


Metabolic Syndrome: The Impact on CVD Risk Is Real & Growing

Impact of Metabolic Syndrome: Three Year Projection for 10,000 Employees

Incremental Cost Due to Metabolic Syndrome
people with metabolic syndrome cost $259 PMPM more than people with thesame age-sex mix but without metabolic syndrome
$46 PMPM of the excess is due to events.
A larger portion of the excess—about $213 PMPM—is due to the non-event costs.


Distribution and Potential Impact of Obesity in BHSF Employees
Normal weight Overweight Grade i Obesity Grade II Obesity Grade III Obesity0
5
10
15
20
25
30
35
40
45
50
36
32
17
86
18
46
24
8
4
Females Males
• 7% (n=748) individuals met criteria for bariatric surgery • Total annual estimated cost attributable to high BMI (>25) were $8.05 million
• 74% medical and 26% work lost• 41% were contributed by 14% employees with BMI>35. • The average attributable cost per high BMI employee ranged from $598 among those
with BMI 25-29.9 to $2695 with BMI>=40.

My Unlimited PotentialWorkplace Cardio-Metabolic Risk Reduction Program
among High-Risk Employees Lifestyle intervention that combines nutritional counseling with fitness training and
close clinical observation over a duration of 12 months
Inclusion Criteria
Current BHSF Employees
High Cardio-Metabolic Risk defined as 2 or more of the following
Interventions
Three Major components – Diet/Nutrition, Physical Fitness, Wellness Check-up
Multidisciplinary team consisting of Registered Nurses, Registered Dietitians, Fitness
trainer/Exercise Physiologist
10 weeks of Supervision, 2 weeks (5 and 10) unsupervised.
Follow-up
12 weeks, 6 months, 12 months

Poorly Controlled BP
BMI >35 Total Cholesterol > 200
Triglycerides >150 LDL > 130 HDL < 40 (men) or < 50 (women)
HsCRP > 3mg/dl HbA1c >6.5 (among DM)
20
30
40
50
60
70
80
51
43
39
27
33
50
59
73
37
34
40
25
29
45
54 55
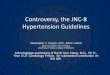
MyUP: Baseline and 12 month compar-isons of Select Outcomes
Baseline 1 year
Prev
alen
ce (i
n %
)

Impact of MyUP on Weight Loss: 12 Months FU
BMI
Category at
Baselin
e
BMI Category Change at 12-Months Follow-up
BMI Category at 12- Months
Normal Weight Over Weight Class I Obesity Class II Obesity Class III Obesity Total
Over-Weight 7 (24%) 18 (62%) 4 (14%) - - 29
Class I 2 (4%) 9 (19%) 33 (70%) 3 (6%) - 47
Class II - 1 (3%) 14 (45%) 13 (42%) 3 (10%) 31
Class III - - 1 (3%) 9 (26%) 24 (71%) 34
Total 9 28 52 25 27 141

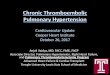
Cost Saving of MyUP on Employees Considered for Bariatric Surgery
1 year6 months
3 months
Baseline
Qualify: n=46
Qualify: n=22
Qualify=21Qualify=19
Do Not Qualify=2
Do Not Qualify=1
Do Not Qualify=1
Do Not Qualify=24
Qualify=5Qualify=4
Do Not Qualify=1
Do Not Qualify=19
Qualify=3
Do Not Qualify=16
20/46 (43%) no longer considered for Bariatric Surgery after 1 year.
Average Cost of 46 Bar. Sx= $1.4 M
Conservative Cost Saving= $0.7 M
Average Cost of 748 Bar. Sx= $18.7 M
Conservative Cost Saving= $8.3 M
Average Cost of 100 Bar. Sx= $4.1 M
Conservative Cost Saving= $1 M

BMI25.0 - 29.9
BMI30.0 - 34.9
BMI35.0 - 39.9
BMI40.0 +
Total
Number of employees with overweight and obesity3,565(52%)
1,851(27%)
831(12%)
581(9%)
6,828
Medical and work loss costs attributable to overweight and obesity
Annual medical costs $1,434,700 $1,658,000 $1,239,500 $1,033,400 $5,365,600
Annual work loss costs $518,100 $687,800 $397,200 $401,500 $2,004,700
Total annual cost$1,952,800
(26%)$2,345,800
(32%)$1,636,700
(22%)$1,434,900
(19%)$7,370,300
(100%)
Average attributable cost per high BMI employee
Medical Cost $402 $896 $1,492 $1,779 $786
Work loss Cost $145 $372 $478 $691 $294
Total average cost $548 $1,267 $1,970 $2,470 $1,079
Annual work days lost 2,015 days 2,598 days 1,550 days 1,581 days 7,744 days
Estimated medical and work loss costs attributable to overweight and obesity


MethodsInclusion Criteria
Current BHSF Employees
High Cardio-Metabolic Risk defined as 2 or more of the following
• Total cholesterol ≥ 200 mg/dl
• Systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg,
• Hemoglobin A1C ≥ 6.5%
• Body mass index (BMI) ≥ 30
Clearance from their physician
Interventions (weeks 0 – 12)
Three Major components – Diet/Nutrition, Physical Fitness, Wellness Check-up
Multidisciplinary team consisting of Registered Nurses, Registered Dietitians,
Fitness trainer/Exercise Physiologist
Had exercise stress testing at baseline and 12 weeks
10 weeks of Supervision, 2 weeks (5 and 10) unsupervised.

Screening
Baseline
12 Weeks
6 Months
12 Months
205 presented for follow-up; 205 completed blood work
230 persons in 7 groups
185 present for follow-up; 156 completed blood work
152 present for follow-up; 149 completed blood work
25 were withdrawn / dropped out from study
15 participants did not come for 6 month follow-up
27 participants did not come for 6 month follow-up
Yearly Screening Health Fair; > 15,000 participants
Exclusion Criteria (any of below) < 2 metabolic risk factors
Unwilling to commit to intervention
not interested unable to obtain clearance from
healthcare provider not willing to sign consent

Table 1: Baseline frequency of demographic and medical history characteristicsVariable Total Frequency (%) or Mean ± SD
Mean age in years ± SD 230 48.4 ± 9.6
Male (%) 230 50 (21.8)
Race 230
Hispanic (%) 110 (47.8)
Non-Hispanic White (%) 48 (20.9)
Black/African American (%) 54 (23.5)
Asian (%) 12 (5.2)
Other (%) 6 (2.6)
Marital Status frequency 230
Married (%) 130 (57.3)
Single (%) 49 (21.6)
Divorced /Separated/Widowed (%) 48 (21.1)
Missing (%) 3 (0.01)
Existing diagnosis of Diabetes (%) 230 81 (35.2)
Existing diagnosis of Hypertension (%) 230 149 (64.8)

Table 2: Baseline and 12-week follow-up comparison of metabolic variablesN at 12 weeks Mean baseline (SD) Mean
12 weeks (SD)p value
BMI 204 35.3 ± 6.5 33.7 ± 6.3 <0.001Weight (kg) 204 96.3 ± 20.3 92.3 ± 19.6 <0.001
Body Fat percentage 198 39.8 ± 7.5 38.6 ± 7.6 <0.001Systolic BP (mmHg) 204 127 ± 13 113 ± 11 <0.001Diastolic BP (mmHg) 204 81 ± 7 71 ± 6 <0.001Hemoglobin A1C (%) 205 6.4 ± 1.5 6.0 ± 1.0 <0.001
Hemoglobin A1C (%) among persons with diabetes
75 7.6 ± 1.8 6.7 ± 1.2 <0.001
Total Cholesterol (mg/dL) 205 186.3 ± 39.9 175.4 ± 35.4 <0.001Triglycerides (mg/dL) 205 133.5 ± 83.8 117.9 ± 63.4 <0.001
LDL-c (mg/dL) 205 111.4± 35.0 104.9 ± 34.0 <0.001HDL-c (mg/dL) 205 48.3 ± 12.3 47.1 ± 11.7 0.008
Median HSCRP (IQR, mg/dL)
205 4.4 (1.8 – 8.4) 3.6 (1.6 – 8.6) 0.143
METS at Max Exercise (kcal·kg−1·h−1)
175 8.8 ± 2.7 11.1 ± 2.8 <0.001
Energy level 204 5.5 ± 2.3 8.0 ± 1.9 <0.001Stress level 204 5.0 ± 2.7 4.2 ± 2.6 <0.001
A p value for paired sample t-test, Abbreviations: BMI: body mass index, BP: blood pressure, Hemoglobin A1C: glycosylated hemoglobin, LDL-c: low density lipoprotein cholesterol, HDL-c: high density lipoprotein cholesterol, HSCRP: high-sensitivity C-reactive protein, METS: metabolic equivalent of task, HQ score: health quotient score by WebMD, PHQ-9: patient health questionnaire for screening of depression.

Change from baseline at 3, 6 and 12 months among persons available at 12 months follow-up
N Mean baseline (SD)
Mean change at 3 months (95% CI)
Mean change at 6 months (95% CI)
Mean change at 1 year (95%CI)
Body Mass Index 151 35.0 ± 6.6 -1.6 ( -1.4, -1.8) -1.9 (-1.6, -2.1) -1.2 (-0.9, -1.5)
Weight (kg) 151 95.8 ± 20.5 -4.4 (-3.9,-4.8) -5.1 (-4.4, -5.8) -3.3 (-2.5, -4.2)Body Fat percentage 131 39.3 ± 7.0 -1.2 (-1.0, -1.5) -1.5 (-1.1, -1.8) -0.7 (-0.4, -1.0)
Systolic BP (mmHg) 150 127 ± 13 -14 (-12, -16) -8 (-6, -10) -4 (-2, -6)
Diastolic BP (mmHg) 150 81 ± 7.0 -11 (-9, - 12) -6 (-4, -7) -3 ( -1, - 4)
Hemoglobin A1C (%) 150 6.3 ± 1.4 -0.4 (-0.3, – 0.5) -0.4 (-0.2, -0.5) -0.3 (-0.1, – 0.4)
Hemoglobin A1C (%)
among persons with Diabetes
51 7.5 ± 1.7 -0.9 (-0.6, – 1.2) -0.9 (-0.5, -1.3) -0.6 (-0.3, – 1.0)
Total Cholesterol (mg/dL) 150 188.8 ± 40.6 -13.3 (-8.8, – 17.7)
-1.3 (3.8, – 6.3) -0.3 (- 4.9, 4.3)
Triglycerides (mg/dL) 150 136.8 ± 93.1 -21.8 (-11.1, -32.4) -13.8 (-1.7, -25.8) -10.6 (-21.6, 0.4)
LDL-c (mg/dL) 150 113.4 ± 34.5 -8.1 (-4.0, - 12.1) -0.4 (- 5.0, 4.2) 0.0 (-4.4, 4.5)
HDL-c (mg/dL) 150 48.2 ± 12.5 -0.9 (-1.9, 0.1) 2.1 (0.8,3.5) 2.8 (1.5, 4.0)HSCRP (mg/dL) 148 5.8 ± 5.6 -0.6 (- 1.2, 0.0) -1.2 (-0.7, -1.8) -1.0 (-0.3, -1.7)
Energy level 139 5.7 ± 2.2 2.5 (2.2, 2.8) 1.8 (1.4, 2.2) 1.7 (1.3, 2.1)
Stress level 140 4.8 ± 2.7 -0.9 (-0.4, -1.3) 0.0 (- 0.6, 0.5) -0.2 (-0.7, 0.4 )

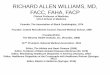
3 months 6 months 12 months0
10
20
30
40
50
60
43
51
31
1
15
9
5% weight reduction 10% weight reduction
Fre
qu
ency
(%
)
• At the end of 12 weeks, 43% had lost 5% of their weight; only 1% lost10%.
•Weight loss continued to improve with 51% and 15% losing 5 and 10% weight at 6 months
•There was sustained weight loss at 1 year though not as large as 6 months.

Poorly Controlled BP
BMI >35 Total Cholesterol > 200
Triglycerides >150
LDL > 130 HDL < 40 (men) or < 50 (women)
HsCRP > 3mg/dl HbA1c >6.5 (among DM)
20
30
40
50
60
70
80
51
43
39
27
33
50
59
73
3734
40
25
29
45
54 55
Baseline 1 year
Pre
vale
nce
(in
%)
•Most notable improvements were seen with BP control, reduction in BMI >35
and improvement in HbA1c.
•Little or no improvement was seen with the lipids and hsCRP.

Impact of MyUP on Weight Loss: 12 Months FU
BMI
Category at
Baselin
e
BMI Category Change at 12-Months Follow-up
BMI Category at 12- Months
Normal Weight Over Weight Class I Obesity Class II Obesity Class III Obesity Total
Over-Weight 7 (24%) 18 (62%) 4 (14%) - - 29
Class I 2 (4%) 9 (19%) 33 (70%) 3 (6%) - 47
Class II - 1 (3%) 14 (45%) 13 (42%) 3 (10%) 31
Class III - - 1 (3%) 9 (26%) 24 (71%) 34
Total 9 28 52 25 27 141

Impact of MyUp on Employees Considered for Bariatric Surgery
1 year6 months
3 months
Baseline
Qualify: n=46
Qualify: n=22
Qualify=21Qualify=19
Do Not Qualify=2
Do Not Qualify=1
Do Not Qualify=1
Do Not Qualify=24
Qualify=5Qualify=4
Do Not Qualify=1
Do Not Qualify=19
Qualify=3
Do Not Qualify=16
20/46 (43%) no longer considered for Bariatric Surgery after 1 year.
Average Cost of 46 Bar. Sx= $1.2 M
Conservative Cost Saving= $0.5 M
Average Cost of 748 Bar. Sx= $18.7 M
Conservative Cost Saving= $8 M

Targeting a larger segment of population: Need for Innovation!
• Newer Approaches
– Flexible/Accessible
– Repeated/Consistent Feedback
– Cost Effective
• Successful programs need to focus on offering “something for
everyone” through multichannel engagement strategies.
• Goal: optimizes personal action and, ultimately, commitment to
change.

Mobile Health: Future of Employee CVD Prevention Program

Websites, Social Media, Internet Applications, electronic mail,
PDA
BP & Glucose Control
4.7/2.4mmHg
BP reducti
on
0.66% HbA1c
net reductio
n
Lipid Markers
23/ 34 studies –
improvement in ≥ 1
Lipid Paramete
r
Physical Activity &
Nutrition
• Net Increase in Physical Activity
• 0.2 more fruit servings
• 1.5g more fiber• 1.4% less energy
from total fat
Smoking
& Weight Loss
• 30% increase in prolonged Smoking Cessation
• Net Weight Loss of 0.7kg compared to control

Baptist Hospital Employee Heart Health Project
• Purpose: A) Identification of employees at high coronary heart disease (CHD)
risk associated with the metabolic syndrome and B) reduction of risk through a
web based lifestyle modification program.
• Program Design
– 180 employees with metabolic syndrome
– Assessment of risk via standard & advanced lipid testing.
– Assessment of baseline AHA indicators for health and specifically metabolic
syndrome
– Randomization: Modification of risk through lifestyle modification directed
through the 4MyHeart onsite educator vs. standard care
• Outcome: ∆ Metabolic risk factors, weight, exercise, diet, biomarker profle
subclinical CVD measures

CVD Low Risk43%
CVD High Risk57% P value
LDL Phenotype B 53% 68% 0.04
High Lp(a) 31% 36% 0.67
Insulin Resistance 63% 69% 0.37
Elevated Apolipoprotein B 37% 44% 0.43
Elevated C-Reactive Protein 67% 60% 0.34
Endothelial Dysfunction 25% 23% 0.81
Coronary Calcium Score
CAC Zero=70%CAC 1-100=21%
CAC>100=9%
CAC Zero=35%CAC 1-100=37%CAC>100=28% <0.0001
Weight Loss Programs Can Further Benefit With Advanced Screening
Baptist Employee Healthy Heart Study: Randomized Trial on the Efficacy of an Interactive Web-Based Lifestyle Intervention
Versus Usual Care in a High Risk Employee Population

Summary
• Worksite becomes critical place to educate, encourage, and monitor personal health activities
• Self insured employers now able to offer financial based incentives to encourage heart healthy and successful preventive strategies
• Aggressive on site and internet/smartphone based programs that focus on weight loss and nutritional guidance, increased physical activity (AHA 10K steps goal), BP and glucose monitoring will be necessary to improve intermediate metrics and long term health care outcomes