Embed Size (px)
Citation preview
Document of
The World Bank
F(R OFFI(IAL l SE (ONI
Report No. 9157-TUN
STAFF APPRAISAL REPORT
REPUBLIC OF TUNISIA
HOSPITAL RESTRUCTURING Sl'PPORT PROJECT
FEBRUARY 26, 1991
Population and Human Resources DivisionCountrv Department IlEurope, Middle East and North Africa Region
This document has a restricted distribution and ma% be used by recipients onlv in the performance oftheir officiai duties. Its contents ma! not othereise be disclosed Aithout World Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
REPUBLIC OF TUNISIA
HOSPITAL RESTRUCTURING SUPPORT PROJECT
CURRENCY(October 1990)
Currency Unit Tunisian Dinar (DT)US$ 1.00 TD 0.85DT 1,00 US$1.18
FISCAL YEAR
January 1 to December 31
ABBREVIATIONS
CGRH Hospital Restructuring Management Board(Comité de Gestion de la Réforme Hospitalière)
CNI National Computer Center(Centre National d'Informatique)
GIS Center for Health Information(Centre d'Informatique Sanitaire)
CRFP Center for Educational Research and Training)(Centre de Recherche et de Formation Pédagogique)
DBE Directorate of Buildings and Equipment(Direction de Batiments et Equipements
DEP Directorate of Planning and Studies(Direction des Etudes et de la Planification)
DTH Directorate of Hospitals(Direction de la Tutelle des Hôpitaux)
EPA Public Establishment with Administrative Purpose(Etablissement Public à caractère Administratif)
EPIC Public Establishment with Industrial and Commercial Pur-posv(Etablissement Public à caractère Industriel et Commercial)
EPS Public Health Establishment(Etablissement Public de Santé)
ESC Tunis Business School(Ecole Supérieure de Commerce de Tunis)
FP Family PlanningIMR Infant Morta'itv RateINNTA National Institute of Nutrition and Food Technology
(Institut National de Nutrition et Technologie Alimentaire)MAS Ministry of Social Affairs
(Ministère des Affaires Sociales)MCH Mother and Child HealthMIS Management Information SystemsMOH Ministry of Public HealthPCU Project Coordination UnitPHN Populationi, Health and NutritionUSAID United States Agency for International Developmeint
FOR OFFICIAL USE ONLY
REPUBLIC OF TUNISIA
HOSPITAL RESTRUCTURINO SUPPORT PROJECT
STAFF APPRAISAL REPORT
TABLE OF CONTENTS
Page
HOEALTH AND POPULATION DATA & DEFINITIONS .
1OAN AND PROGRAM SUMMARY ... . . . . . . . . . . . . . . . . . . . . . . iv
I. OVERVIEW OF THE HEALT8 SECTOR. . . . . . . . . . . . . . . . . . . . 1
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1HEALTH AND DEMOGRAPHIC STATUS ... . . . . . . . . . . . . . . . . 2HEALTH SECTOR RESOURCES ... . . . . . . . . . . . . . . . . . . . 3
HEALTH SERVICES DELIVERY SYSTEM ... . . . . . . . . . . . . . . . 4
II. SECTOR ISSUES AND GOVERNNENT STRATEGY . . . . . . . . . . . . . . . 4
HEALTH FINANCING ... . . . . . . . . . . . . . . . . . . . . . . . 4Public Sector Underfunding ... . . . . . . . . . . . . . . . . . SP-ublic Sector Financia] Burden-sharing Arrangements .. . . . . . 5
INTERNAL EFFICIENCY IN HOSPITALS ... . . . . . . . . . . . . . . . 8General Inefficiencies .8.. . . . . . . . . . . . . . . . . . . . eTechnical inefficiencies . . . . . . . . . . . . . . . . . . . . . 9
GOVERNMENT STRATEGY .... . . . . . . . . . . . . . . . . . . . . 10
BA.,K EXPERIENCE WITH LENDING IN THE SECTOR ... . . . . . . . . . . 12RATIONALE FOR BANK INVOLVEMENT ... . . . . . . . . . . . . . . . 13
III. THE PROJECT . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
THE INSTITUTIONAL FRAMEWORK .......... ... .... .. . 14PROJECT OBJECTIVES ....... ... ... .. ... ... .. . . 14PROJECT DESCRIPTION ................ ..... . 15
A. Development uf Management Capabilities and Policy Adjustments. 15(a) Financial Management & Performance Evaluation Procedures. 15(b) Computerized Management Information Systeme Development 16
(c) Reorganisation of Administration & Patient Registration 17(d) Sectoral Strategy Development and Project Management. . . 18
B. Improvement of Service Quality ... . . . . .. . 19
(a) Replacement of Priority Medical Equipment . . . . . . . . 19
(b) Strengthening of Hospitals Maintenance Units . . . . . . . 19
<c) Improvement of Patients Accomodations & HcopLtal Hygiene . 19
This report is based on the findings of an appraisat mission that visited Tinisia in October, 1990. Missionmembers were Guy Eltena (Mission Leader and Heatth Economist); Salim Habk,bo (Sr. Pubtic Meetth Specialist);Claire Voltaire (Operations Anatyst); Gustaff Brest Van Kafipen (Consultant Architect); Michet Lavattee (MISSpecialist Consuttant); and Janine Battani (Hospitat Management and MIS Specialist Consuttant). GaitRichardson (SuJTeer Intern) contributed to the report.Trsk Manager: Guy Ellena (EMTPH); Divi:ion Chief: Andrew Rogerson (EM2PH); Director: Kemat Dervis (EM2);Peer Reviewers: willy de Geyndt (ASTP'> and Howard Barnun (PHRMN).
This document ha% a restricted distrihution and may be used by recipienis only in tht performance^h ter *tb t di dîe, 1tS rnt< n ma o nu! other4ise he Jmsi osed a thout World Bank authorîzation.
TABLE OF CONTENTS (continued)
IV. PROJECT COSTS AND FINANCINO . ................. . 20
PROJECT COSTS . . . . . . . . . . . . . . . . . . . . . . . . . . 20
PROJECT FINANCING ....................... . 23PROCUREMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
STATUS OF PREPARATION AND DISBURSEMENTS . . . . . . . . . . . . . 25
V. IMPLENENTATION, KANAGEMENT. SUPERVISION AND IVALUATION. . . . . . . 27
IMPLEMENTATION AND MANAGEMENT .... . . . . . . . . . . . .. . 27
SUPERVISION, MONITCRING AND EVALUATION . . . . . . . . . . . . . 28
VI. HENEFITS AND RISKS ....................... . 30
BENEFITS ........................... . 30RISKS ............................. . 32
VII. AGREEMENTS AND RECOMOENDATIONS . . . .33
ANNEXES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
1. Sector Statistical Annex2. Outline of Government Financial Strategy and Action Plan
3. Hospital Statistical Annex4. The Future Legal and Organizational Structure
of Tunisian Public Hospitals5. MIS component
STAFF APRISAL T
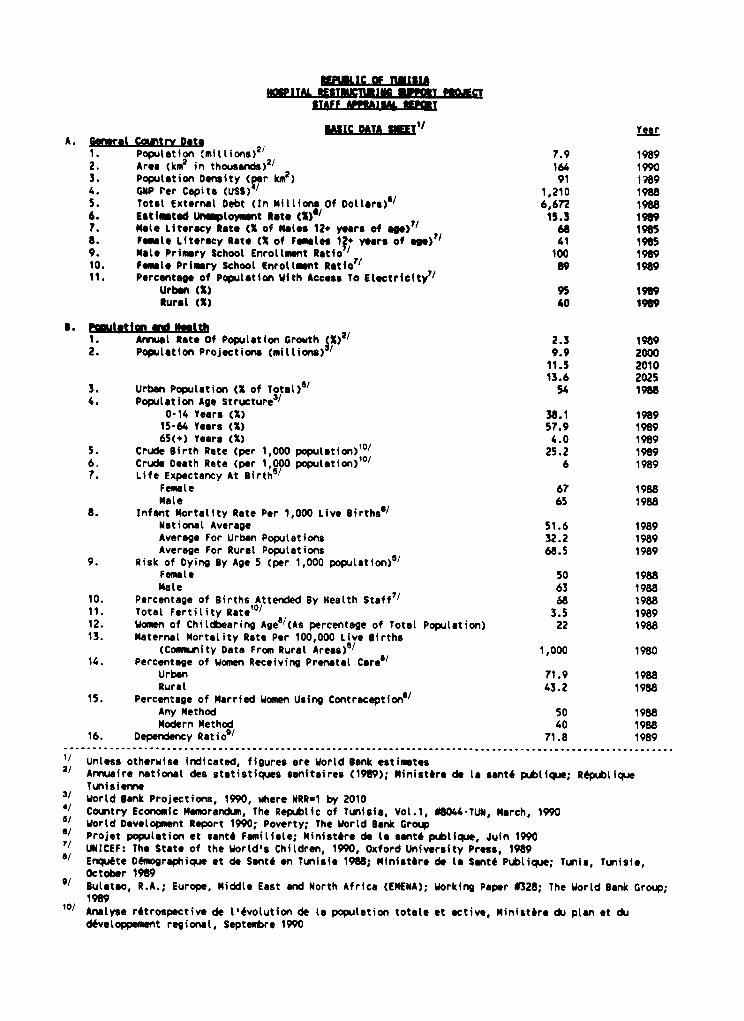
uASIC DATA SUIT' 1 Year
A. Gnrl Country Dite1 Population <millions)2' 7.9 1989
2. Aree (km in thousands)2/ 164 19903. Population Density (rr km2 ) 91 :R89
4. ONP Per Capita (US$) / 1.210 1988
5. Total External Debt (In Millions Of Dolttara'/ 6,672 19886. Estiutad Munaloymant Rate (C) 15.3 19097. Mlte Literacy Rate (X of Mates 12- ycsar of age)7' 68 1985
8. Fenal Literacy Rate (X of Fametes 12. years of ags>'M 41 19859. Mlte Primary Schooi Enroltmant Rétio'/ 100 1989
10. FamIle Primery School Enrotlmnt Ratio'/ 89 1989
11. Percentage of Population With Access To Etsctricity7/Urban (X) 95 1989
Ruret (X) 40 1909
S. Poutat1on and N ath1. Anual Rate Of Population Growth pe 2.3 19892. Population Projections (miltions) 9.9 2000
11.5 201013.6 2025
3. Urban Population (X of Totalt)3 54 1988
4. Population Age Structure3/0-14 Yeers (X) 38.1 198915-64 Years (X) 57.9 1989
65<+) Years (X) 4.0 1989
5. Crude Birth Rate (per 1,000 populition)1 °/ 25.2 1989
6. Crude Death Rate (per 1 000 population)10 / 6 1989
7. Life Expectency At airth5 /
Female 67 1988
Male 65 1988
8. Infant Mortallty Rate Per 1,000 Live Sirths/National Average 51.6 1989
Average For Urban Populations 32.2 1989
Average For Rural Poputations 68.5 1989
9. Risk of Dying *y Age 5 (per 1,000 population)5/Fem le 50 1988
Mate 63 1988
10. Percentage of Births Attended By Health Staff"/ 68 198811. Total Fertility Ratet°/ 3.5 1989
12. Women of Childbearing Ageo/<As percentage of Total Population) 22 1988
13. Materna( Mortality Rate Per 100,000 Live Slrths(Comm.u,ity Data From Rural Areas)>
5 / 1000 198014. Percentage of Women Receiving Prenatal Care0
Urban 71.9 1988
Rural 43.2 1988
15. Percentage of Married Women Using Contraception'/Any Method 50 1988Modern Method 40 1988
16. Dependency Ratio9/ 71.8 1989. . ..................................................................................................................................... ........................
2/ Unless otherwise indicated, figures are World Bank esti_tes2/ Armuaire national des statistiques sanitaires (1989>; Ministère de le santé publique; République
Tunisieme3/ Wortd Sank Projections, 1990, where MRRU1 by 20104' Country Economic Memorandum, The Republic of Tunisia, Vol .1, 0844-TUN, March, 19905/ Wortd Development Report 1990; Poverty; The Wortd Sank Groupa/ Projet population et santé Familise; Ministère de la santé publique, Juin 1990
" UNICEF: The Stète of the World's Children, 1990, Oxford University Press, 1989"' Enquéte Démographique et de Santé en Tunisie 1988; Ministère de la Santé Publique; Tunis, Tunisie,
October 19899ulatao, R.A.; Europe, Middle East and North Africa (EMENA); Working Paper 0328; The World Bank Group;
1989Io/ Analyse rétrospective de l'évolution de le population totale et active, Ministère du plan et du
développement regional, Septembre 1990
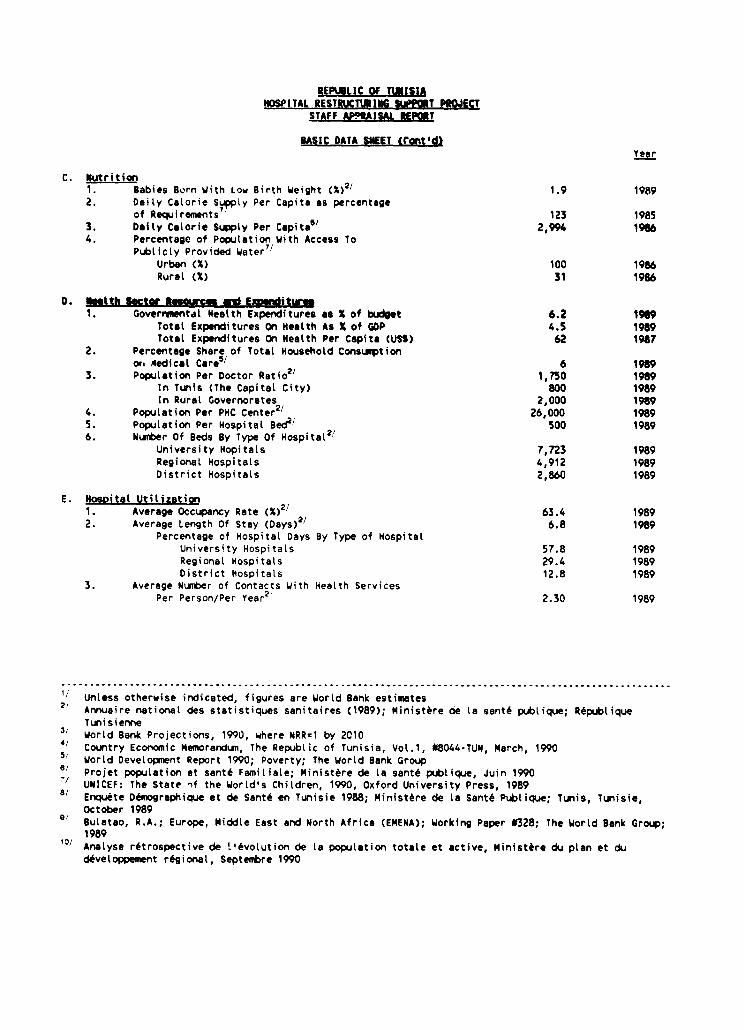
REPUBLIC Of TUWISIOSPITAL RESTRUCTURING %MPPoT P*CJECT
STAFF AP9tAISAL tEPORT
BASIC DATA S4EET tront'di_ear
C. utrition1. Babies Born With Low Birth Weight (X)2/ 1.9 19892. Daily Calorie Supply Per Capita as percentage
of Requirements 123 19853. Daily Calorie Supply Per Capitat 2,994 19864. Percentage of Population with Access To
Publicly Provided Water7 IUrban (X) 100 1986Rural (X) 31 1986
D b 1tth Sector 94m4crs and Exnditurw1. Governmental Health Expenditures as X of budget 6.2 19t9
Total Expenditures On Health As X of GOP 4.5 1989Total Expenditures On Health Per Capita (US>) 62 1987
2. Percentage Share of Total Nousehold Consumptionor Aedical Care5/ 6 1989
3. Population Per Doctor Ratio21 1,750 1989In Tunis (The Capital City) 800 1989ln Rural Governorates 2,000 1989
4. Population Per PHC Center21 26,000 19895. Population Per Hospital Bed2' 500 19896. Number Of Beds By Type Of Hospital2t
University Hopitals 7,723 1989Regional Hospitals 4,912 1989District Hospitals 2,860 1989
E. Nosoital Utilization1. Average Occupancy Rate (X)2/ 63.4 19892. Average Length Of Stay (Days)>/ 6.8 1989
Percentage of Hospital Days By Type of HospitalUniversity Hospitals 57.8 1989Regional Hospitals 29.4 1989District Hospitals 12.8 1989
3. Average Number of Contacts With Health ServicesPer Person/Per Year2 , 2.30 1989
,...........................................................................................................
'/ Unless otherwise indicated, figures are World Bank estimates2/ Annuaire national des statistiques sanitaires (1989); Ministère de la santé publique; République
Tunisienne3i World Bank Projections, 1990, where NRR:1 by 20104/ Country Economic Memorandum, The Republic of Tunisia, Vol.1, #8044-TUN, March, 19905/ World Development Report 1990; Poverty; The World Bank Groupe/ Projet population et santé Familiale; Ministère de la santé publique, Juin 1990
UNICEF: The State if the World's Children, 1990, Oxford University Press, 1989/ Enquète Démographique et de Santé en Tunisie 1988; Ministère de la Santé Publique; Tunis, Tunisie,
October 19895/ Bulatao, R.A.; Europe, Middle East and North Africa (EMENA); Working Paper #328; The World Bank Grou;
198910/ Analyse rétrospective de !'évolution de la population totale et active, Ministère du plan et du
développement régional, Septembre 1990
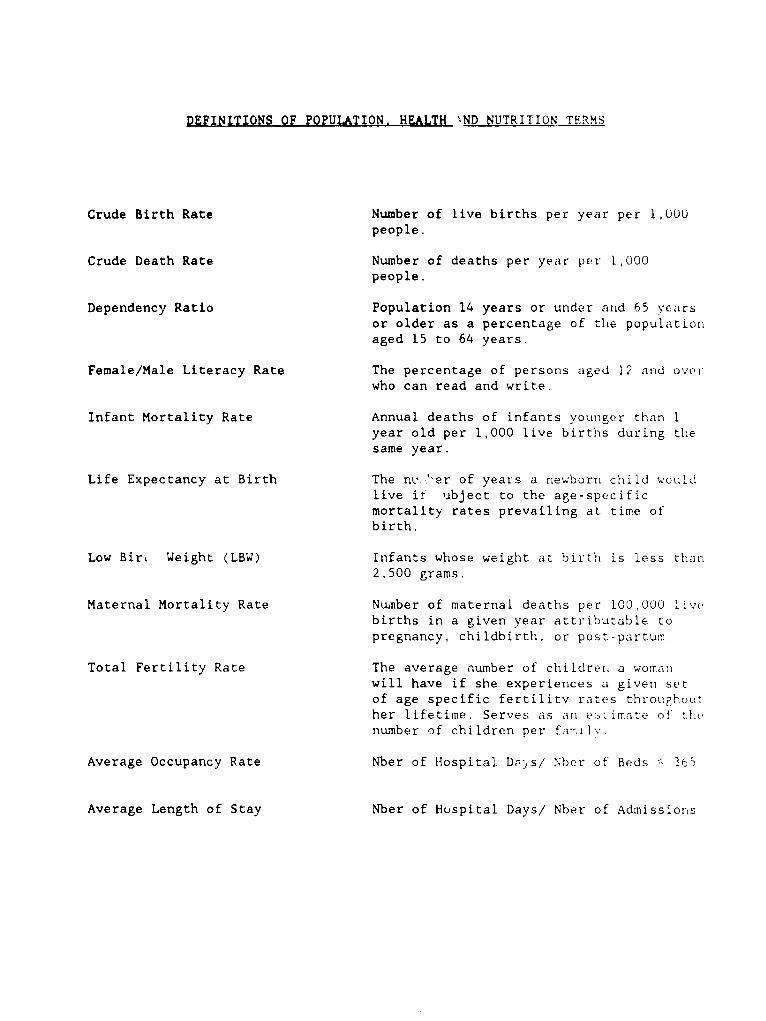
DEFINITIONS OF POPULATION. HEALTH `ND NUTRITION TERMS
Crude Birth Rate Number of live births per year per 1,000people.
Crude Death Rate Number of deaths per year per 1,000people.
Dependency Ratio Population 14 years or under and 65 yearsor older as a percentage of the populationaged 15 to 64 years.
Female/Male Literacy Rate The percentage of persoras aged 12 and ovwerwho can read and write.
Infant Mortality Rate Annual deaths of infants younlger than 1year old per 1,000 live births during tlhe
same year.
Life Expectancy at Birth The n .'-er of years a newborn child woulc!live i2 ubject to the age-specificmortality rates prevailing at time ofbirth.
Low Bir. Weight (LBW) Infants whose weight at birth is less than2,500 grams.
Maternal Mortality Rate Nunber of maternal deaths per 100,000 livebirths in a given year attributable topregnancy, childbirth, or post-partumn.
Total Fertility Rate The average number of children a womanwill have if she experiences a given setof age specific fertilitv rates throuFho)uther lifetime. Serves as an estimate of rlenumber of children per farily.
Average Occupancy Rate Nber of Hospital D-z,s/ Nher of Beds A3S5
Average Length of Stay Nber of Huspital Days/ Nber of Admissionls
i
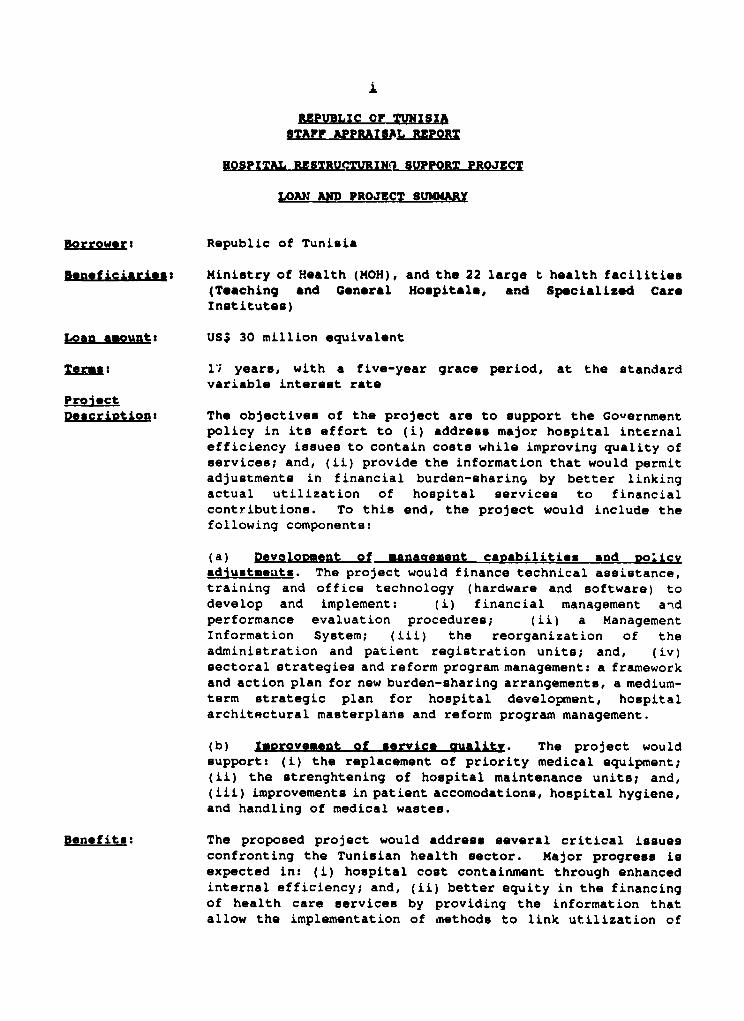
REPUBLIC cr TUNISIASTAFF APPRAtSAL RCPOR
HOSPITAL RESTRUPTURIN1 SUPPORT PROJECT
LOAN AN" PROJECT SUENARY
Borrowers Republic of Tunisia
B.npficiarieui Ministry of Health (MOH), and the 22 large t health facilities<T.aching and Genoral Noupitale, and Sp.cializ-d CaroInstitutes)
LoJan mouats US$ 30 million equivalent
Termes il years, with a five-year grace period, at the standardvariable intereut rate
ProiectDescription: The objectives of the project are to support the Government
policy in its effort to (i) address major hospital internalefficiency issues to contain costs while improving quality ofservices; and, <ii) provide the information that would permitadjustments in financial burden-sharingi by better linkingactual utilization of hospital services to financialcontributions. To this end, the project would include thefollowing components:
(a) Devolooment o: management canabilities and oglicvadiustmeutu. The project would finance technical assistance,training and office technology (hardware and software) to
develop and implement: (i) financial management and
performance evaluation procedures; (ii) a ManagementInformation System; (iii) the reorganization of theadministration and patient registration units; and, (iv)sectoral strategies and reform program management: a frameworkand action plan for new burden-sharing arrangements, a medium-term strategic plan for hospital development, hospitalarchitectural masterplans and reform program management.
(b) Improvement of service aualitv. The project wouldsupport: (i) the replacement of priority medical equipment;(ii) the strenghtening of hospital maintenance units; and,(iii) improvements in patient accomodations, hospital hygiene,and handling of medical wastes.
Denefits The proposed project would address several critical issuesconfronting the Tunisian health sector. Major progres. i.expected in: (i) hospital cost containxnent through enhancedinternal efficiency; and, (ii) better equity in the financingof health care service. by providing the information thatallow the implementation of nethode to link utilization of

ii
services with burden-sharing responsibilities. Under favorableconditions, while remaining stable in nominal terme, theGovernment budget share in MOH resources could drop from 83%to 56% by the end of the project, the social insurance programnsshare increasing from 10% to 36%. Les. favorable conditionswould limit or delay this progreas. This would periritaustained improvementu in quality of servicea in the entirepublic health sector that would benefit directly the vastmajo-ity of the population needing hospital and non-hospitalcare. In addition, the project involve maternity hospitalsand maternity departments that provide for 43% of all attendeddeliveries nationally. Hence, the qualitative improvementsfor safe deliveries, obstetrical interventions and post-partumcare would be significant.
Riaka: The main riuk relates to the technical ability of managers tonuccessfully introduce and implement the hospital reforms andovercome the system's rigiditiee and natural resistance tochange. To lower the risk due to limited experience and skillsof local managers in exercising authority, training andtechnical assistance are included in the project. Anotherpossible risk is related to the lack of incentives among civilservice phyqicians to be cost-conscious in utilizing existingresources. This risk, however, wil. be mitigated by thedeveloç -rt of a financial management model that would provideco5t ana performance indicators and, in the new hospital legalcontext would allow hospital managers to establish performance-based incentives. Finally, the benefits expected in terme ofadjustments in burden sharing arrangements will depend on thedegree of euccess that the Government will achieve innegiotiating with its social partners. For that purpose, theproject aime at generating the cost and utilization informationthat would help the Government conduct these rnagotiations inthe most favorable conditions.
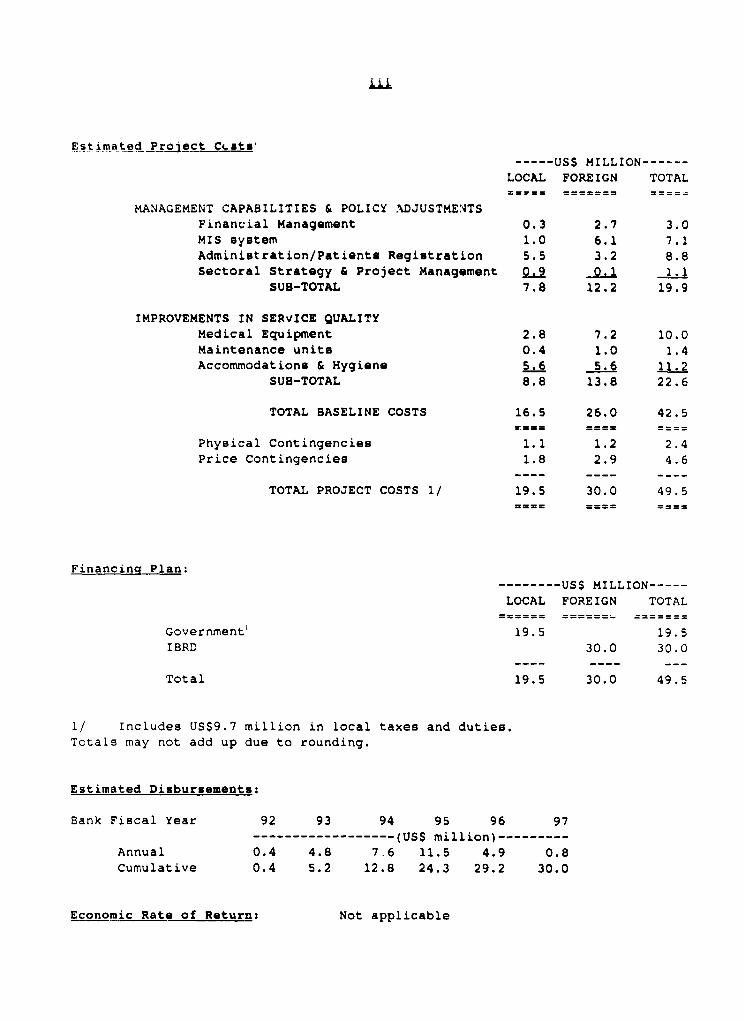
Estimated Pr_gjct C.ats'----- US$ MILLION------
LOCAL FOREIGN TOTAL
MANAGEMENT CAPABILITIES & POLICY ADJUSTMEATSFinancial Management 0.3 2.7 3.0MIS system 1.0 6.1 7.1Administration/Patients Registration 5.5 3.2 8.8Sectoral Strategy & Project Management 0.9 0.1
SUB-TOTAL 7.8 12.2 19.9
IMPROVEMENTS IN SERVICE QUALITYMedical Equipment 2.8 7.2 10.0Maintenance units 0.4 1.0 1.4Accommodations & Hygiene 5.6 5.6 11.2
SUB-TOTAL 8.8 13.8 22.6
TOTAL BASELINE COSTS 16.5 26.0 42.5
Physical Contingencies 1.1 1.2 2.4Price Contingencies 1.8 2.9 4.6
TOTAL PROJECT COSTS l/ 19.5 30.0 49.5
Financinq Plan:
-------- USS MILLION-----
LOCAL FOREIGN TOTAL= s== =w= === = == _ == == = =
Government' 19.5 19.5
IBRD 30.0 30.0
Total 19.5 30.0 49.5
l/ Includes US$9.7 million in local taxes and duties.Totals may not add up due to rounding.
Estimated Disbursements:
Bank Fiscal Year 92 93 94 95 96 97------------------ (USS million)---------
Annual 0.4 4.8 7.6 11.5 4.9 0.8Cumulative 0.4 5.2 12.8 24.3 29.2 30.0
Economic Rate of Return: Not applicable
RZPUEL!C or TUNISIA
HOSPITAL RESTRUC.,URINO SUPPORT PROJECTSTAFF APPRAISAL RZPORT
I. OVERVZEW OF Tac HEALTE SCTOR
INTRODUCTION
1.01 After a decade of *conomic growth, the Tunisian *conomy began tefalter in the early 1980'. Oil expcrt *arnings *tarted declining as a resuitof the depletion Df the Tunisian reserves and a fall in world oil prices. In1985, to thwart a balance of payment crlais, the governmnt instituted policiesthat encouraged exporte, cut back on inv*itmenta, limited wage increases, anddevalued the Tunisian Dinar. Deopite theoe m-asure-, the *conomy neared acritical state in 1986 because of a drought and the *till-declining world oilprices. More drastic measures wore implemented, including the curbing ofimports, further jeduction of Government Lnvestmente and expenditures, and thedevaluation of the Tunisian Dinar again, to a leval 17.5% below the realeffective exch,ange rate of 1984.
1.02 Since 1987, the balance of paymento han recovered, ard the budgetdeficit has been reduced. The Government of Tunisia ha. initiated the processof shifting from a state-controlled to a market-driven, export-oriented economymore capable of providing jobs and competing effectively abroad. These efforts,combined with support from the Bank in the form of five adjustment operations -two Agricultural Adjustment Loans (ASAL) in FY87 and FY89 (Lns no.2754 and3078), the FY87 Industry and Trade Policy Adjustment Loan (ITPAL, Ln no. 2781),the FY88 Structural Adjustment Lcan (SAL, Ln no. 2962) and the FY90 PublicEnterprise Restructuring Loan (PERL, Ln no. 3109)- are targeted in part to reducethe current 15% rate rf unemployment among the working population.
1.u3 The pressures on the omployment market are compounded by a 2.3%average annual population growth rate (although steadily declining, and lowerthan all other Arab countries and at a level comparable to other middle-incomeeconomies), stagnant net emigration, and rising female participation in the workforce. The Government has initiated programs, supported by Bank lending, toenhance family planning services thereby reducing population growth. However,evidence of the positive impact of population policieo on the labor market willnot be seen immediately.
1.04 The growing population will continue to otrain the Tunisian economy,as the financial needs of social sectors, namely education and health, grow.This will ha' a two-fold effect on the health sector. Firot, the demand forhealth serv .es will continue to increase both quantitatively and qualitatively,as the morbidity patterns are slowlv moving from communicable diseases to chronicand degenerative diseases more costly to address (para 1.07). Second, theresources of the sector will be constrained by a number of factors. Ifunemp]oynent remains at relatively high levels, the growth of employment-relatedinsurance contributions will be limited and priority efforts to increase theenrollment rate of segments of the population currently employed will be
- 2 -
necessary. It iE likely that Government policiez to control or reduce publicspendiLg will cotitinue to prevail and that, as a -eault, the cur:ent highGcvernment share in financing health services will have to decrease (the sharcof the Government's budget allocated to MOH has decreased trom 7.9% in 1980 to6.2% in 1989). Finally, the population's capacity to pay for health oerviceswill be constrained by the slowly growing or even stagnant purchasing power ofa large portion of the population (real wages decreased by 2.8% irn he firat halfof the 801s,, rec...itating better targeting of existing assistance programsfor the neeuy. These constraintu have reaulted in a decreabe of the percentageof GDP allocated to the public health sector over the last five years, from 2.5%in 1984 to 2.3% in 19E9.
1.05 The Tunisian health uoctor, and in particular the public sector,which provides an eetimated 50% of ambulatory car- and 90% of hospital services,faces a eerious challenges to provide more health care services and ones ofbetter quality, with limited increase in the renourcee available. As in theother sectors of the nation's economy, this translates into attempting to improvethe efficiency of the health sector operations,. while reexamining the currentfinancial burden-sharin7 arrangements to alleviate Governments alreadyoverstretched responbibi:-ities.
HEALTH AND DEMOGRAPHIC STATUS
1.06 Ir. the last three decades, the health statue of the Tunisianpopulation has improved significantly as a result of better living conditions,greater accesa to education, improved nutrition, the development of bothpreventive and curative health care services, and lower birth rates. Lifeexpectancy has increased from 41 to 67 yeare (females), and the crude death ratehas decreased from 16 per 1000 population in 1965 to 7 in 1988, as a result ofdetermined Government acticn and a GNP average annual growth rate per capita of3.4% in real terme (1965-88). The infant mortality rate (IMR), which decreasedfrom 175 deaths per 1,000 live births in 1956 to '2 per 1,000 in 1989, iscurrently the lowest in the Maghreb, while it remains on the high aide of upper-middle income countries. However, this progreas has not occurred uniformallyover the countzy, and disparities between urban and rural areas are stilisignificant. IMR remains twice as high in rural areas, where the per'-entage ofwomnen receiving prenatal care is still 35% lower than chat in urban areas.
1.07 The population of Tunisia, waich was 7.9 million in 1989, continuesto grow at a rate of 2.3% per vear, desDite a declire ia the total fertility ratefrom an average 7 children per woman in 1956 to 3.5 children per woman in 1989.Factors contributing to these improvements include an increased ma,riage age andfamily planning efforts. The morbidity patterns in Tunisia parallel theevolution of its population structure. The patterns reflect a mixture ofcommunicable diseases usually found in developing countries and a rapid increasein the prevalence of degenerative diseases and chronic conditions, such as cancerand cardio-vascular diseaaes. The latter are more common in industrializedcountries which experience longer life expectancies and older populations.
.3-
HEALTH SECTOR RESOURCES
1.08 H1uman and Physical Resources. In the post-colonial era, emphasishas been placed on increasing access to health care services. The ratio ofpopulation per physician has decreased from one physician per 8,000 population
in 1965 to one physician per 1,750 population in 1989, with urban areas havingbenefited most from this expansion of services (Annex 1, table 1). Attentionhas also been focussed on the training of specialiets. Almost 50% of physicians,of whom 72% have teaching responsibilities are *pecialized. This specializationreinforces the urban hospital-based orientation of the Tunisian health caresystem since specialist services are primarily available in the Universityhospitals or specialized institutes.
1.09 In 1989, Tunisia had nome 17,400 hoepital beda, of which 94% werepart of the public sector (Annex 1, table 2). The ratio of 2.2 hospital bedsper 1000 population compares well to other middle-income economies. However,this figure may be misleading, as a number of beds may not qualify as hospitalbeds considering the low level of associated medical equipment and etaffing.This cautionary remark applies to a large portion of private sector hospitalbeds, as well as to those in public district hospitals.
1.10 Financial resources. In 1989, total health expenditures in Tunisiaequalled approximately 4.5% of GDP, or US$62 per capita. This level ofexpenditures situates Tunisia between its Maghreb neighbors, Algeria and Morocco,which allot 5.4% of GDP (US$ 125 per capita) and 3.2% of GDP (US$ 30 per capita)hrespectively. However, it remains low compared to most OECD countries, whichallocate between 5.3% and 11.2% of their GDP (excluding Turkey at 3.5%), and temost other middle-income nations. For example, Jordan, Chile and Columbia devoterespectively 8%, 5.3% and 7.8% of their GDP to health expenditures.
1.11 In 1987, :he Government budget contributed 48% of the total sectorresources while social injurance programs and aouseholds contributed 19% and 33%,respectively. Figures for 1989, which are partly estimated, indicate that th.Government contribution has decreased to 44%, the insurance contribution and thehousehold share have grown to 20% and 36%, respectively (table 2.1). Bycomparison, in 1987 their respective distribution was 20%, 60% and 20% inAlgeria, and 23%, 21% and 56% in Morocco. Public spending, which is defined asincluding expenditures from Governments and social insurance programs, coversbetween 41% and 97% in OECD countries, compared to 67% in Tunisia (table 1.1).
TabLe 1.1: Heatth Expenditures in Maghreb and OECD countries in 1987
Heatth Expend. Heatth Public Social Householdsper capita Expend as. share SecuritysUS X ofGDP X X
.... ............. .... ...... ........ ......... ...... .....
Maghreb: Tunisia 52 4.5 48.0 18.9 33.1Algeria 92 5.3 20.0 60.0 20.0Morocco 29 3.1 23.0 21.0 56.0
. .. ..... ...... ....
OECD: Turkey 147 3.5Low 337 5.3 41.3 58.7High 2,051 11.2 97.6 2.4
Source: US DHHS 1990 and OECD Heatth Data FiLe 1989.
- 4-
HEALTH SERVICES DELIVERY SYSTEN
1.12 The Tunisian health care eystem has alom improved significantly interms of physical infrastructures. Designed as a coherent network, Public HealthFacilities are etrategically located and classified according to the level ofcare provided. At the firet level, the 1505 basic health centers, 95 districthospitals and 6 free-standing maternities (maternites autonomes) are intendedto provide basic ambulatory health care and tiret level hospital services. Atthe second level, there are 22 regional hospitalo, located primarily in ruralareas and designed to provide the population with mome *pecialized :are andhospital services. Finally, the third level of care, encompassing teaching andgeneral hospitale, as well as specialized carQ institutes, in localed in the fourlargest urban poleos (Tunis, Monastir, Sousoe and Sfax), and offers high-levelservices. The national role of these third-tier facilities should be emphasized.In 1989 they accounted, nationwide, for 43% of assioted deliveries, 45% ofhospital admissione, 60% of hospital days and 70% of surgical interventions.Au a result of this three-level system, 90% of the population is within one-hour walking distance from a public health care facility.
1.13 The ParaDublic Health Network belonge to the CNSS <Caisse Nationalede sécurité Sociale) and consiste in 6 polyclinios located in the major cities.The clinics provide ambulatory general practice, specialized care andinvestigation services to private sector workers (and their dependents)affiliated with the CNSS. The parapublic network was developed in the mid-80'sas a response to the perceived low quality of public health services and a stillinsufficient provision of services from the private sector.
1.14 Finally, the Private Health Sector is concentrated in urban centersand consists of 1567 medical offices, 602 dental offices, 968 pharmacies, 338nursing health centers and 101 laboratories. There are 35 private hospitalswhich offer 1062 beds. However, more than 60% of these beds (mainly maternities)do not qualify as hospital beds, considering the low level of medical technologyavailable.
II. SECTOR ISSUES AND GOVERNKZNT STRATEOY
2.01 In 1988, the MOH initiated a broad review of the health sector andin particular of the public sector, which highlighted two critical sets ofissues: the inadequate financing of health services, and the low internalefficiency of public sector health facilities, particularly hospitals.
HEALTH FINANCING
2.02 The financing of the health sector in Tunisia faces two majorconstraints. First, overall sector financial resources are low as a result ofthe marked underfunding of the public eector as compared to the scope of eervicesit is providing; second, financial burden-oharing arrangements enforced in thepublic sector are inadequate to mobilize the needed resources.
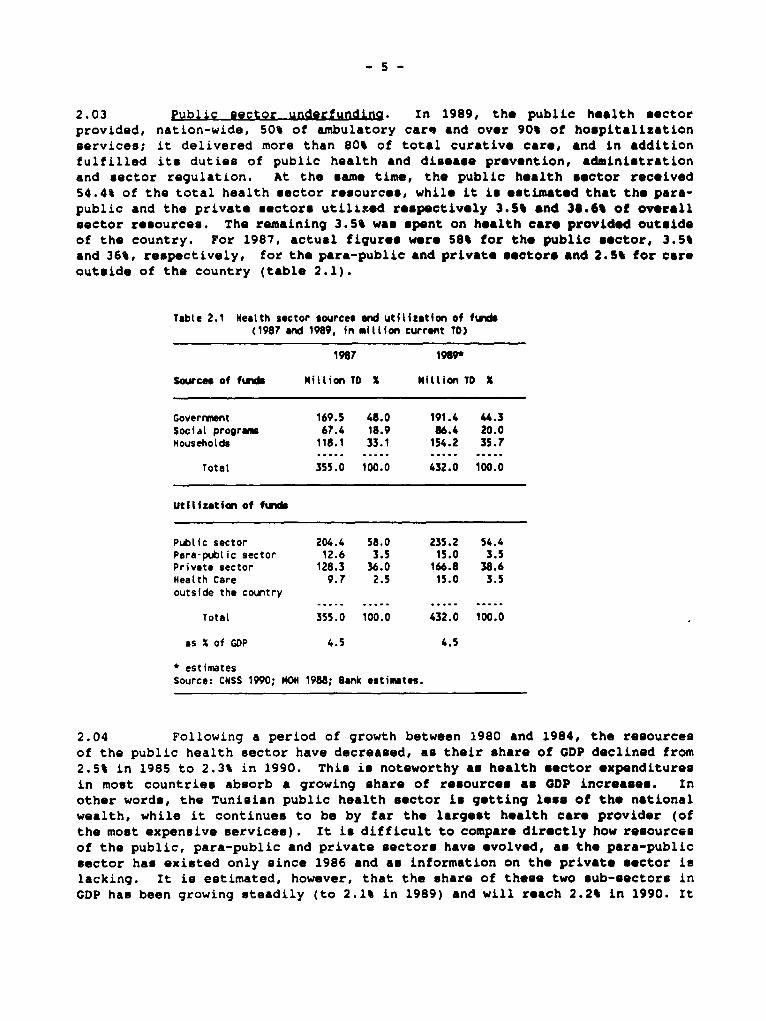
2.03 Public sector underfundina. In 1989, the public h-alth *ectorprovided, nation-wide, 50% of ambulatory car* and over 90% of hospitalizationservices; it delivered more than 80% of total curative care, and in additionfulfilled its duties of public health and diease prevention, administrationand sector regulation. At the *ame time, the public hoalth sector recoived54.4% of the total health sector resources, while it in e*timated that the para-public and the private *ectors utilited respectively 3.5% and 38.6% of overallsector reaources. The remaining 3.5% was apent on health care provided outcideof the country. For 1987, actual figures were 58% for the public sector, 3.5%and 36%, respectively, for the para-public and private seotore and 2.5% for carsoutcide of the country <table 2.1).
Table 2.1 Nealth sector sources ad utiliation of fundi(1987 and 1989, in miltion current TO>
1987 1989*
Sources of fun Mitlion TO X Mitlion TD X
Goverrnent 169.5 48.0 191.4 ".3Social progras 67.4 18.9 86.4 20.0mouseholds 118.1 33.1 154.2 35.7
....... ...... ..... . ...... .....
Total 355.0 100.0 432.0 100.0
Utitization of fund
PubLic sector 204.4 58.0 235.2 54.4Para-public sector 12.6 3.5 15.0 3.5Private sector 128.3 36.0 166.8 38.6Health Care 9.7 2.5 15.0 3.5outside the country
..... ..... . ...... ...... ..........
Total 355.0 100.0 432.0 100.0
as X of GDP 4.5 4.5
* estimatesSource: CNSS 1990; MON 1988; Bank estimates.
2.04 Following a period of growth between 1980 and 1984, the rebourcesof the public health sector have decreased, au their share of GDP declined from2.5% in 1985 to 2.3% in 1990. This in noteworthy as health sector expendituresin most countries absorb a growing share of resources as GDP incroases. Inother words, the Tunisian public health sector in getting leas of the nationalwealth, while it continues to be by far the largest health care provider (ofthe mont expensive services). It is difficult to compare directly how resourceeof the public, para-public and private sectors have *volved, as the para-publicsector han existed only mince 1986 and as information on the private sector inlacking. It is ectimated, however, that the share of theu- two sub-sectors inGDP has been growing nteadily (to 2.1% in 1989) and will reach 2.2% in 1990. It
- 6 -
appears that, while total health expenditures have remained quite stable ijrterms of GDP ehare, resources have shifted from the public to the growing para-public and private sectors. This transfer of resourcee, however, was notaccompanied by a comnmensurable transfer of responsibility in terme of activitiesperformed, and this imbalance is a major cause of the growing difficulties facingthe public health sector.
2.05 The relative decline in public health sector resources can beattributed to several factors. First, the Government contribution, in regardto the share of its budget (operating and investment) allocated to the MOH, hasdeclined between 1985 and 1989 from 7.9% to 6.2%. Nevertholess, the Governmentbudget'a contribution accounts for a growing share in MOH rec.urrent budget, from82.6% in 1985 to 83.7% in 1989 and an estimated 84.8% in 1990. Second, thesocial insurance prograrne" contribu.Wion han actually d-creased in roel terme andaccounts in 1990 for 9.1% of the public health sector remources against 12.7%in 1985. Finally, the households' contribution through direct payments and co-payments has increased significantly, but has remained stable in terms of itsshare, around 6% of MOH resources.
2.06 When associated with a low level of management capabilities, thissevere underfunding of the public health eector translates into chronic shortagesin equipment and supplies, insufficient maintenance, low staff morale and,ultimately, poor and decreasing quality of services in the entire public sectornetwork (paras 2.19-2.20). The first and second levels of care are the mostaffected by this underfunding, leading the population to seek care in the high-level hospitals where, despite the large share of allocated resources, conditionsare also uncertain and quickly deteriorating.
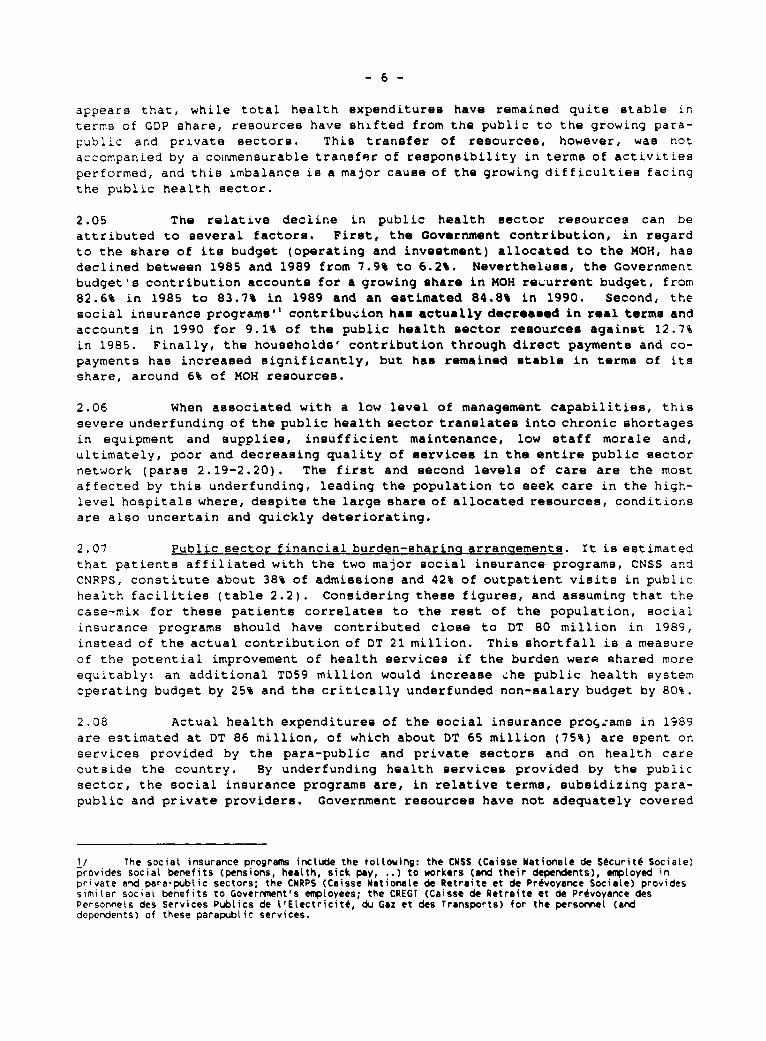
2.07 Public sector financial burden-sharino arrangements. It is estimatedthat patients affiliated with the two major social insurance programs, CNSS andCNRPS, constitute about 38% of admissions and 42% of outpatient visits in publichealth facilities (table 2.2). Considering these figures, and assuming that thecase-mix for these patients correlates to the rest of the population, socialinsurance programs should have contributed close te DT 80 million in 1989,instead of the actual contribution of DT 21 million. This shortfall is a measureof the potential improvement of health services if the burden werp shared moreequitably: an additional TD59 million would increase .he public health systemoperating budget by 25% and the critically underfunded non-salary budget by 80%.
2.08 Actual health expenditures of the social insurance proc,:ams in 1989are estimated at DT 86 million, of which about DT 65 million (75%) are spent onservices provided by the para-public and private sectors and on health careoutside the country. By underfunding health services provided by the publicsector, the social insurance programs are, in relative terme, subsidizing para-public and private providers. Government resources have not adequately covered
1/ The social insurance programs include the vottowing: the CNSS (Caisse Nationale de Sécurité Sociale)provides social benefits (pensions, health, sick pay, ..) to workers (and their dependents), eaployed inprivate and para-public sectors; the CNRPS (Caisse Nationate de Retraite et de Prévoyance Sociale) providessimilar social benefits to Goverrwent's epçtoyees; the CREGT (Caisse de Retraite et de Prévoyance desPersonnels des Services PubLics de L'Electricité, du Gaz et des Transports) for the personneL (anddependents) of these parapublic services.
th;5 def:cit, as sericus shortages have appeared, and it is unlikely that, the
Goerr~::er.t despite its commitment to improve health services, can assume this
ULz:îs ibJlity, in light of growing needs and budgetary constraints.
Table 2.2: MOH activities and social progrms coverage(1987)
Admiissions X Visits X
Indigent (Gvt) 203,507 38.4 3,266,538 41.1
CNSS 245,002 27.5 2,913,504 36.7
CNRPS 50,611 9.5 377,654 4.8
Payers 32,089 6.1 252,626 3.2
Other 96,811 18.4 ',132.402 14.3
Source: MOH 1988.
2.09 It .s not easy to determine the capacity of the social inourance
programs to bear a larger share of the MOH budget. Information on the level of
resources generated by the Social Insurance programs through employers' and
employees' contributions to health service coverage ie difficult to estimate,
since the contributions to health insurance and retirement plans are not formally
dissociated. However, it is estimated that in 1987, CNSS and CNRPS -- the two
major insurance programe -- collected TD63 million through their health
insurance scheme, while their expenditures for health services totalled TD48.8
million. This situation was not specific to 1987. Social insurance programs
have repeatedly used extra resources generated through their health insurance
schemes to compensate for deficits incurred through other benefit schemes
(pensions) or to invest in activities outside the health sector. Increasing
their contribution to the budget should therefore be possible as long as some
conditions are met (para 2.22), although a reduction in other forms of member
benefits, or improvementa in social security collection rates may be necessary.
in addition, because until now Governrment resources were matching the most
visible MOH financial gap, social insurance programe never developed pro-active
policies to expand their coverage of the employed population. Only 50.5% of the
active population is affiliated to the social insurance programs, ranging from
22.4% in the agricultural sector to 65.3% in the non-agricultural sector.
2.10 Better rates of enrollment in the social insurance programs can be
achLeved if attractive schemes are developed, and if the Government policy of
delivering free or highly subsidized vouchers for care in the public facilities
is drastically reexamined. According to prevailing Government guidelines
defining the poverty threshold (which need to be reviewed to cover recent losses
in purchasing power), the Government should provide free or highly subsidized
care to only 8% of the population. Currently about 40% of admissions and
outpatient visits in the public health sector are attributed to patients
registered as indigent (table 2.3).
- 8 -
2.11 The unwillingnese of the social insurance programs to contribute
more to the public health sector resources ie based on (i) the inability of thepublic health sector to provide adequate information on the utilization of
services and more importantly, on the actual costs of services; and, (ii) the
low quality of services provided by public facilities. The lack of provenmanaging and accounting systeme to monitor the utilization of resources and the
cost of services, the lack of critical equipment and the deteriorating physical
conditions of hospitals are major instrumental factors contributing to this
situation. The Government's strategy for the sector and the proposed project
address these specific issues.
INTERNAL EFFICIENCY 1N HOSPITALS
2.12 In general, efficiency in the whole sector is low. Although the
health care network was conceived and developed as a coherent system with a
pyramidal referral flow, it does not function efficiently. The different levels
of care do not adequately complement each other, and their potential is not
maximized. In parCicular, the district and, above all, the regional hospital
networks are underused. Distortions in service utilization are illustrated in
Annex 1, Fig. 1-4.
2.13 Low internal efficiency characterizes the Tunisian public hospital
network and results from a myriad of interrelated issues. Inefficiencies can
be identified under two main clusters, general and technical inef.iciencies.
2.14 General inefficiencies. Administrative and budgetary policies are
rigid and hamper substitution of input factors. This inflexibility obstructs
the search for cheaper combinations of inputs for service provision. Personnel
and civil service regulations impede the efficient management of staff and the
provision of incentives. Information failure is a major management handicap.
Managerial diagnosis and sensible choices of options cannot be made because
related information is not available and skilled managerial staff is lacking.
Operationally, two dimensions of these issues should be addressed:
(i) these constraints are beyond the control of the few, generally
untrained hospital administrators, hence adjustments in the
organizational and policy environmenta are necessary;
(ii) a cadre of high and mid-level hospital managers should be recruited
and managerial skills developed over a broad base so as to includethe key mid-level administrators. selective functional training of
a few top administrators would not be sufficient to significantlyimprove the system.
2.15 The lack of clear definition of responsibility among the different
levels of management, the lack of trained managers and the absence of management
systems typify the current inefficiency in the operation of the public health
sector. Hospital personnel lack management skills and standardized methods and
procedures to follow in monitoring performance in the provision of services,
patient flow, therapeutic procedures, as well as inputs such as inventory and
utilization of resources. True coste of care are unknown.
-9
2. 16 The registraticn of patients for inpatient services or outpatientvisits is strictly an administrative task, providing MOH with only very generalactivity information. Geographic origin of the patients in generally notrecorded. Deficiencies in the recording of admission diagnosis and treatmenthinder any analysis of the justification for the visit or admission at that levelof care. Social statue is usually recorded in order to collect payment forservices rendered to patients entitled to foe-for services, or co-payment in thecase of indigent and insured patients. However, the hompital management doesnot systematically compile that information which would support its budgetrequest to MOH and to the central authorities to negotiate financing levels andhospital resources with the various financiers.
2.17 In some cases, a patient can walk into a facility from one of severalentrances, receive care, and leave the facility without ever having beenregistered as a patient, thereby avoiding paying for services. Reinforcingregistration capabilities, through the improvement of patient registration andinformation areas and the provision of adequate technology, will in turnfacilitate the monitoring of patients and of care rendered. Adequate patientinformation is fundamental to effective management of health care systemsmanagement. Also, the availability of infcrmation minimizes serviceduplications, reduces coste, and contributes to patients' comfort, welfare andquality of care by checking a whole apectruà of diagnostic tests and exploratoryand invasive procedures.
2.18 Obvious flow activities, such as arrivals and releases in varioushospital departments, are generally recorded, so that aggregate indicators suchas occupancyrates and average length of stay are available (Annex 3, table 2).However, managers lack information to monitor the utilization of resources, andthere is no analysis of whether the treatment rendered is consistent with theprimary diagnosis. Occupancy rates and average length of stay vary greatlywithin and among facilitieu. The high range of variation in the average lengthof stay in some similar departments within facilities of identical level of care(Annex 3, table 3) suggeste that the variation is not due to case-mixdifferences. Rather, the level of utilization and the combination of differentinputs are almost unregulated, following no procedural standards, or are£ndirectly determined by variations in beds, equipment, materiale and personnelsupply.
2.19 Technical inefficiencies. The sources of inefficiency involvingtecnnical waste of resources are numerous. A pervasive problem negativelyaffecting hospital performance is the mediocre level of maintenance at threelevels: buildings and electro-mechanical equipment, medical equipment and supportservices. In addition to bio-medical equipment, significant probleme areencountered in the maintenance of heating systeme, ventilation, electric supply,sterilization, kitchen and laundry facilities. In general, maintenance ispostponed because capabilities are scarce or resources are limited. About 30percent of the medical equipment in hospitals is obsolete and about 60 percentof the physical amenities require refurbishing. To address these issues, MOH'sstrategy through the reform program is to allow and encourage hospital managersto buy curative maintenance services directly from the private market rather thanto build up such capabi.ities within an already inefficient system. This
- 10 -
strategy is justified by the large variety of items, apecifications and spareparts available due to the diverse sources of supply. However, development ofinstitutional capabilities would be actively promoted for diagnostic andpreventive maintenance as well as for enmergency needs.
2.eO IInefficient use of resources or the lack of such resources exacerbatethe vicious cycle of general inefficiency. The lack of simple diagnosticequipment or its poor quality leads to more expensive procedures beingundertaken. Examples abound in ultrasound, obstetrics and radiology. The lackof specific drugs may lead to unnecessary surgical treatment instead, for examplein the treatment of peptic ulcers. The lack of standards monitorinq exacerbatesover-prescribing, incorrect prescribing, or paradoxically, under-prescribing ofmedication. Patients are kept on the wards unnecessarily, waiting their turnfor diagnostic or therapeutic procedures. Continuing training on uniquely adhoc basis reduces staff quality and efficiency. Inventory and supplies managementare rudimentary resulting in mismanagement and losses. Blood banks are shortof refrigeration and processing equipment frequently leading to wastes andshortages when needs are moet acute.
OOVERNMENT STRATEOY
2.21 For decades, the Government health policy has put emphasis onimproving access to health services by investing heavily at all levels of care.As a result, and despite some regional imbalances which are being addressed,access to health care is now satisfactory. The Government's main concern hastherefore shifted towards consolidating these achievements by improving theeffectiveness, quality and efficiency of services rendered and, more generally,the economic sustdinability of health services.
2.22 The Government has outlined a comprehensive reform plan for itspublic health sector. Major reforms have been undertaken regarding:
(i) the institutional framework: the largest health facilities are beinggranted financial and administrative autonomy and efforts areunderway to progressively decentralize the management of healthactivities and resource allocation at the regional level.
(ii) the health orofession, by promoting deconcentration of personneltowards primary and secondary facilities by selective incentives;improving equipment in the peripheral units; promoting exchanges ofhealth professionals among the different levels; assessingperformance and adjusting training curricula; and,
<iii) the financial burden-sharing arrancements by updating existing fee-sch.dules for medical and non-medical services on the basis of unitcosts provided by the generalization of cost-accounting systems;reassessing the benefits criteria for free and reduced-cost vouchers,known as "indigence programs"; consolidating and harmonizingbenefits under current insurance schemes, with extension to non-insured segments of the population; and, generalizing cost-sharingmechanisms (Annex 2).
- il -
2.23 Major concrete actions have already been taken. First, regardingthe health profession, the heade of clinical departments in teaching hospitalshave been limited to five-year appointments and the extension of their terms
subject to performance aseeBsment. Also, newly recruited physicians are now
required to serve a minimum of two yeare in rural areas. Second, regarding thefinancial burden-sharing arrangements, the following meaBures have been taken(Annex 2): (i) the fees applicable to non-insured and non-indigent patiente arebeing doubled in a two-step process (November 1, 1950 and November 1, 1991); (ii)the co-payments applicable to insured and some category of indigent patients willincrease by 50% by January 1991; (iii) MOH, CNSS and CNRPS reached an agreementon a program to enhance medical technology in public hospitals. CNSS and CNRPSwould finance up to TD 50 million (US$59 million) over the next five years. Afiret TD20 millLon two-year tranche (90-91), which includes the provision ofequipment as well as of finances to cover incremental operating expendituresassociated with these investments, has been agreed.
2.24 The objective pursued by the n.^vernrment is clear: develop moreequitable burden arrangements among the health sector institutional financiers,and consequently, among the different segments of the population. To reach thisobjective, the Government strategy is to rationalize and update existingmechanisms, rather than to develop and experiment a new approach. Specifically,these mechanisme include public mandatory health insurance as the main mechanism,co-payments to control unjustified demand (both quantitatively amd qualitatively)and, finally the Government intervention to regulate the implementation of thesemechanisme and financial equilibrium. This regulatory role is critical, since,as mentionned earlier, the inadequate operation of the social ineurance programeand the populatior. professional and economic patterns combined, call for amassive financial contribution from the Government.
2.25 Therefore, achieving the stated objectives in terms of burden sharingarrangements, depende not only of the Government will and commitment, but alsoof his capacity to successfully negotiate the needed changes, with his socialpartners. These negotiated changes would take place when the information on thehospital cost and utilization patterns is available, and the magnitude of thetransfer of financial responsibility from the Government to other sectorfinanciers will largely depend on the economic situation at that time.
2.26 Large hospitals are likely to remain key actors in the overallperformance of the health sector. The Government has therefore identified theorpanization, manaaement and financino of public hosoitals as a priority areaof action. As a major step, the 22 largest facilities (teachinr hospitals andspecialized institutions) have been selected as the sites for the proposedreforms (Annex 3, table 1). Subsequent phases which are -.ot covered under theproposed project would include generalizing these rr.orms to reach regionalhospitals and, further, the whole health care netw,rk.
2.27 Two main factors justify the reform's focus on third-levelfacilities. Firet, the 22 third-tier hospitals and institutes concerned absorban estimated 50% of the public health sector's resources. Attempting to controlescalation of costs is a priority at a time when epiderniological changes mayinflate them, and efforts directed at strengthening lower levels of care requireadditional operating resources. Second, because the social insurance programs
- 12 -
either operate their own ambulatory health care network (CNSS) or rely on theprivate sector for ambulatory care, moat of the services provided to theirbeneficiaries in the public health sector occur in urban hospitals andspecialized institutes. The reform of burden-sharing arrangements, whose aimis to charge actual coste to usera through their social insurance programe andwhich would permit reallocation of resources within the sector, conetitutes amajor objective of the Government. To that end, efforts to improve efficiencyand quality of services and to gain knowledge of utilization and coat patternsare to be directed in priority towarde the third-tier facilities.
2.28 The emphasis on the reform of high-level facilities couldlegitimately raise the concern that by improving the efficiency and quality ofservices, the demand for high-level hospital services may increase. This would,in turn, further reinforce the relative over-utilization of thea- facilitiescompared to lower-level care (para 2.12) and require additional resources tomatch the increased demand. In fact, this possibility ehould not be of concernfor the following reasons: (i) the current utilization of hospital services canbe considered as "maximal", since it is constrained neither by purchasing powernor by limited bed capacity. Acceou to high-level public hospitale ie currentlysubject to minimal or no charge, for most of the population. Expected futuredemand increases due to epidemiological changes would be matched by Governmentefforts to strengthen lower-level care, thereby reducing unjustified utilizationof higher level facilities. The adjuetments considered by the Government interms of fee-for-services and co-paymente ehould ease that prospect; and, (ii)as already mentioned, the public sector provides over 90% of hospital services.The potential increase would therefore be marginal and due mainly to patientseither insured or entitled to pay for services (those who may currently accessthe private sector). This increase would be easily matched by additionalresources, as the Government is reconeidering the burden-sharing arrangements,namely the social insurance programe contribution, co-payments and fee-for-service schedules (para 2.22, 2.23 and Annex 2).
BANK EXPERIENCE WITH LENDIN0 IN THE SECTOR
2.29 In 1971, the Tunisian Government received a US$4.8 million IDA creditto address population sector issues, including improving accese to familyplanning (FP) and maternal and child health services (MCH). The credit providedfor the construction and equipment of four maternity hospitale, 29 MCH centers,and an extension of the Avicenne Paramedical Training School in Tunis. Inaddition, management consultante and technical assistance for paramedicaltraining and evaluation of the MCH/FP program were provided. The project wascompleted in 1981 at a cost of US$35 million, a figure well above the initialappraisal estimate of US$7 million. The additional cout, attributed to delaysin implementation and price eecalation, was met by additional financing providedby the Norwegian aid (NORAD) and the Government of Tunisia. The main impact ofthe project was an expansion of services.
2.30 A US$12.5 million Bank loan for a second health and populationproject became effective in 1982. The overall project objective was to integrateFP services with preventative and curative services, nutrition, health educationand sanitation in 8 governorates. Similarly to the firet project, emphasis in
- 13 -
the second one was on the expansion of services. The project was completed in1989 and involved the construction and/or remodelling of 140 health poste, 325dispensaries, 90 staff houses, 2 regional health education centers, 6 paramedicalachools, and 8 maintenance workshops. In addition, the project supported theinitial introduction of a Management Information System to enhance managementcapabilities of the MOH, the inaugu-ation of a national health education programand the implementation of a training system for health personnel.
2.31 A third health and population project was ider.tified in 1984 toextend the basic health center concept, yet it was not pursued due to concernaabout the recurrent coste and the overall relevance of such a project, if takenin isolation from systemic reforme.
2.32 Important lessons can be drawn from past Baak group involvement inTunisia's health sector. Firat, Government action has zonstantly been orientedtowards fostering growth of the sector to ensure better access to services.However, operating resources (recurrent expenditures) have never adequatelymatched needs, resulting in low quality and underutilization of services,especially at the first and second levels of care. Second, efforts to improvethis situation have been plagued by the chronic inefficiency of the publichospital sub-sector, which puts a major atrain on eector resources. Third,significant improvemento can only be achieved through a major development ofmanagement capabilities, the enhancement of managerial reaponsibilities througha higher degree of autonomy, the renewal of equipment and priority renovationto restore the quality of care to an acceptable level, while simultaneouslyaddressing the current imbalances in burden-aharing arrangements between theGovernment budget and the social insurance programe, principally the CNSS andCNRP5.
RATIONALE FOR BANK INVOLVEMENT
2.33 The comprehensive restructuring of the tertiary hospital sub-sectoris prerequisite to a review of the financial burden-sharing arrangements thatwould help contain public expenditure on higher-level curative services andrelease resources for primary health care. This restructuring encompasses majorenhancements of management capabilities and autonomy of decisions, coupled withimprovements in medical technology and priority facility renovation. The Bank'sexperience with public enterprise restructuring in most sectors of the Tunisianeconomy, and its sustained advisory role in the design of health finance reformsin particular, put it in a privileged position to assist MOH in this criticaiphase.
2.34 The proposed project would build on the overall framework of publicfinance discipline and enterprise reform pursued under the Structural AdjustmentLoan (SAL, Ln.2962-TUN) and the Public Enterprises Rationalization Loan (PERL,Ln. 3109-TUN). Parallel efforts are being undertaken in the entire humanresources sector with on-going operations and new ones under preparation in theeducation sector.
2.35 The project constitutes one aide of a two-fold comprehensive approachto the health sector that the Government has developed with the Bank support.It also includes the proposed FY91 Population and Family Health Project, whose
- 14 -
main thrust is to reatore credibility to primary and first-leve. refria'services, thereby alleviating pressure on the hospital system. The tW . i I,t t9
are closely linked, as their respective objectives and proposed dCt t arecomplementary and support each other. Their different scOpS' a;id I *M ALntervention, as well as their own set of comple., i'suee, require, *-iiev, '.kat
their implementation remain independently undertaken.
II. THE PROJECT
THE INSTITUTIONAL FRAMEWORK
3.01 The proposed project would act as a major vehicle in theimplementation of the policy orientations of the Government reform prcograur. asdescribed in paras 2.21 and 2.22. These policies emphasize the neel f:r:(i) adjusting the Ieaal and orcanizational framework in order to increaseadministrative and financial autonomy and the accountability of the Iargesthealth facilities; and (ii) reconsidering the financial burden-sharino mec amsqsto ensure regular, efficient and equitable mobilization of resources t. trehealth sector.
3.02 The project's successful implementation is contingent up^n theGovernment's commitment to introduce and pursue the adjustments outlinedpolicy framework. The hospitals considered under the project would Le,s!'e
"Etablissements Publics de Santé" (EPS). EPS's legl statutes would enabie tiedevelopment of the proposed organizational structure, institute a Board ofDirectors, concentrate the executive authority at the hospital level (GeneralManager and Directors), and allow for financial and administrative ancr'(Annex 4). Therefore, the enactment by the parliament of the law creating theEPS, whose approval by the Government has been confirmed during negotiations,and the formal conversion into EPS of the four hospitals listed under part A ofAnnex 3, Table 1, and nomination of their General Managers, are conditiorns ofeffectiveness (para 7.02 (b). The remaining eighteen hospitals w-ll betransformed into EPS as follows: eight hospitals by December 31, 1992 (part B,Annex 3, table 1), five hospitals by December 31, 1993 (part C, Annex 3,table 1), and the remaining five hospitr'a by December 31, 1994 (part D, Annex 3,table 1) (para.7.01 (a) and (b). For these hospitals, the disbursement of loanproceeds for equipment (excluding computer equipment) will be conditioned tothe prior transformation into EPS of hospitals referred to in Part B and C, and,for civil works to the prior transformation of hospitals in Part B (para. 7.03)
PROJECT OBJECTIVES
3.03 The overall objective of the proposed project is to improve the sub-sector's efficiency and quality of service, and to help alleviate the heavyburden imposed on Government resources by the largest hospitals. Specificaily,the project would support the Tunisian Government's reform program designed toattain two main objectives:
- 15 -
to Lmprove the internai efficiency of major general, specialized andmaternity hospitals, while simultaneouely containing costu andLmproving the quality of services; and,
t,) to allow future adjustmentB in financial burden-sharing through theformulation of data to better link actual utilization of hospitalservices with financial contributions by insured and non-pooruninsured patiente
3.0a The institutions targeted by the project include 10 generalaos, tals, 3 free-standing maternity hospitals and 9 specialized hospitals andinstitutes including the National Inatitute of Nutrition.
PROJECT DESCRIPTION
3.05 Within the inBtitutional framework described above (para 3.02), theproject would be implemented over a six-year period and consist of the followingcomponents:
A. Develoament of Management Capabilities and Policy Adiustments
- Financial Management and Performance Evaluation Proceduree;- Computerized Management Information Systeme Development;- Reorganiza.tion of Admi-nistrative and Patient Registration Sections;- Sectoral Strategy Development and Project Management.
B. Service-Ouality Improvements:
- Replacement of Priority Medical Equipment;- Strengthening of Hospital Maintenance Units;- Improvement of Patient Accommodations and Hospital Hygiene.
A. Development of Management Capabilities and Policy Adiustmonts(US519.9 million)
a) The Financial Management and Performance Evalvation Procedures(US$3.0 million)
3.06 Financial Management model. The project would provide 8 man-monthsof technical assistance (6 nationals and 2 foreign) to the Project CoordinationUnit (PCU), for the development of a financial management model which includesthree integrated components: (i) the financial management manual; (ii) an annualfinancial report to serve as an the evaluation tool; and (iii) a Collection ofDirectives and/or Memorandums issued by MOH as guidelines for effective financialmanagement. The manual would be prepar-d by September 30, 1991 for joint reviewby MOH and the Bank, to thoreafter be used au part of the tra-niag of managerialstaff and distributed to senior and mid-level administrators within the hospitalstransformed into EPS starting January 1, 1992 (para 7.01 (f)).
i 07 Human Resources Develodment. To implement the new hospitalorganizational structure (Annex 4), the Government is planning to progressivelycre te about 250 positions in administration, finance, hospital operations,
- 16 -
maintenance and security, and hygiere in the 22 hospitals involved. An analysisof the existing personnel resources revealo that, in view of the staff profile
required to fill the new positions, most of the staff (at least 50%) will have
to be recruited or seconded to the MOH. Placing qualified managers in their
respective positions, with clearly defined responsibilities, will be instrumental
to improving both resource and personnel management. The proposed organizational
plan would be applied in the Specialized Instituteo and Teaching Hospitalo with
enough flexibility to take into account the cpecific needs of each facility.
3.08 The project would support the following training programe which wouldinvolve more than 1000 staff in the concerned hospitals:
Trginina for General Managers. Directors and Division Chiefs inHogsital Oroanizatilon and Managements local training would be
undertaken in Tunis by MOH'o "Centre de Recherche et de Formation
Pédagogique" <CFRP), jointly with the Tunis "Ecole Supérieure deCommerce" (LSC) (140 man/months); overseas training would be
organized by CRFP in collaboration with foreign hospitals (400
man/monthe excluding meintenance staff);
Trainina for Staff in charae of developina the Manaaement Information
Syste:m overneas training for 35 people in charge of technicalsupport, systemi development and program management, would be
coordinated by the CFRP and the "Centre d'Informatique Sanitaire"
(CIS) (para 3.12), and would amount to 60 man/months. In additionto proper techniquee and practices for developing and operating the
system, staff would be trained to analyze the data generated ae a
tool for management purposes and policy development;
Trainina in Hospital Maintenance for Division and Section Chiefs:
Division chiefo would be trained overseas (220 man-montha); Section
Chiefs (electro-mechanic maintenance and biomedical maintenance)
would be trained locally (28 man-montho) with external TA for
preventive maintenance achedule development (6 man-months) and
training of trainers overseas (30 man-montho);
Support to the Hoapitai Manacement MA Dearee proaram: this program
is launched by the Tunis ESC; the prLoject would provide 6 man-months
TA (visiting foreign lecturers);
Trainina Fellowshios: 3 one-year fellowzlips in health economice,hospital planning and hospital management.
Information and orientation seminars: CRFP would organize seminars
in the 22 hospitalu to facilitate the integration of the proposed
reforme into the existing structure. Within the Medical Departmento,the heade of department, intendants and nurse supervisors would be
informed of their duties and reeponsibilities within the proposednew organizational structure. A total of about 1000 persons wouldbe involved.
- 1 7 -
b) Compgterized. Ma,nagement Information Sytemu Develooment(US $7. 1 Mi l l lon)
3.09 In order to generate and treat the information needed to provideeffective managemrent tools, a Management Information System would be developedand introdu-ed as detailed in Annex 5. It would include the provision of hardwareand software for equipping 500 work stations in the 22 hospitals, 5 of MOH'sregionai directorates and the central MOH as well as maintenance services. '0man monthe technical assistance would be provided to support, set-up and testthe systems. Staff training would be provided to 35 persons over a 5-year period(para 3.09).
3.10 Computerization of hospital data would *ignificantly er.nance thehospitals' ability to coordinate and monitor the system's inputs, outputs,consumption and utilization. Specifically, management information systems wouldimprove: (i) personnel management, (ii) management of supplies and equipment,(iii) management of patient files, (iv) monitoring of treatments rendered, (v)generation of bills for the services delivered and the resourcea used, and (vi)general accounting and financial control of the hospitall. activities.
3.11 It is essential that management policies, norms and procedures beapplied homogeneously by all hospitals in the implementation of theircomputerized systeme, and that MOH be in a position to closely monitor,coordinate and apply corrective measures when necessary. To that end, a Centerfor Health Information (CIS) would be created as an 'Etablissement Public àcaractère Industriel et Commercial" (EPIC), a legal statua identical to theexisting "Centre National d'Informatiaue" (CNI) or the "Centrei Informatique duMinistère des Finances". The draft law creating the CIS es an EPIC has beenapproved by the Government and the CIS shall have been eltablished and itsdirector appointed by Feptember 30, 1991 (para 7.01(d)>. This financiallyautonomous body would have responqibility for the managemenI'Lt standardizationand coordination of the hospital computer network developmen--. and would offerthe services of its staff to hospitals for the developrent, distribution,installation, and maintenance of comput.er systems. Contracral arrangementsbetween MOH, the EPS and the CIS will be formalized and commun, :ated to the Bankprior to the implementation ci the MIS in the first hospital.
3.12 In addition, a commission would be appointed with;i three monthsafter the creation of CIS to ensure that the needs of the userc '; the MIS arebeing met by the services provided by (CS. The commissiot wiuld includerepresentatives from the CNIS and the PCU au well as from the ins9i-utions thatuse the service (hospitale, regional directorates of health, MOI!)
c) Reoroantzation of Administrative and Patient Registration Sections(US$8.8 million)
3.13 This component involves the administration and patient registrationunits and would provide the facilities -- space, furniture, equipment, andsupplies -- necessary to carry out the new administrative services which arevital to the implementation of the reform. As the administrative and managementfunctions are currently very limited, existing facilities have not been developedand are inadequate to permit autonomous management bv the facility, according
- 18 -
ta the generic organizational chart developed (Annex 4). The implications ofthLs new operational model have been reflected in preliminary architecturalre4u reCents for the 22 hospitals, based on several parameters including the sizecf each, hospital, the condition of existing facilities, and the projection offuture needs. About 14,500 m of space would be redeeigned according to theproposed specifications, which were found to be eatisfactLcy at appraisal, andabout 8,600 m of opace would be added to the existing sites.
d) Sectoral Strateav Develooment and Proiect Management (US$1. 1 million)
3.14 Medium-term Plan for Hoseital Network Develoiment. A strategic planfor the restructuring and development of the hospital sector over the next 10years would be formulated. The project would support technical assistance (9man/months) and logistice for a multidisciplinary team constituted of membersfrom PCU and MOH's Directorate of Planning and Studies (DEP). Therecommendations of the plan would be discussed in a national seminar involvingsenior representatives from MOH, the Ministries of Planning and RegionalDevelopment, Finance, and the Interior, social insurance programs, and theprivate sector.
3.15 The plan would build upon the Government's national healthobjectives; estimates of future hospital needs of the population; financialprojections at the macro-economic and sectoral levels; and the rules andregulations shaping the institutional structure of the sub-sector. The planwould include monitoring indicators. A draft plan would be circulated forcomments to all institutions involved in its implementation. Review of the planand its implementation would be conducted on a yearly basis. The medium-termplan for hospital notwork development will be formulated and submitted to theBank for review by September 30, 1992 (para 7.01(o)).
3.16 Development of Hospital Architectural Masterplans. The developmentof architectural masterplans is critical for 9 hospitals among the largest andoldest (Annex 3, table 1). It constitutes a prerequisite for the implementationof several project components in those facilities (reorganization ofadministrative sections, introduction of the MIS). For that purpose, the projectwould finance USSS20,000 for contracting consulting firme. These masterplanswould be formulated and reviewed with the Bank by December 31, 1992. No activityrelated to the rehabilitation of administrative and patient rogistration areas(para.3.13) will be implemented in the hospitala concornod before the approvalof these masterplana by the Bank (para 7.01(g)).
3.17 Framework for Financial Burden-Sharing Arrangements. To assist theGovernment in developing new burden-aharing arrangements in line with the mainobjectives and orientation which have been defined previously (para 2.22 andAnnex 2), the project would include the following three studies to be realizedby the PCU with an external support estimated at 9 man/monthe (6 nationale and3 foreign):
the evaluation of existing free or reduced cost voucher programsknown as "Assistance Médicale Gratuite" systems, and specificationof options and time frame for reforms;
- 19 -
- the evaluation of the Health Insurance components of existing SocialInsurance programa, with special emphasis on complementary systems('assurances-groupe", "mutuelles,), and specification of optionsand tim- frame for reforme;
- the formulation of a methodology to charge actual hospitalexpenditures to the different in-titutional financiers and of atimeframe for its implementation.
3.18 During negotiations, the Government reaffirmed itc intention topursue its financial etrategy for the health sector, as outlined in paragraph2.22 and Annex 2 (letter from the Minister of Public Health provided at thebeginning of negotiations). The above-mentioned studios will be compl-ted bydecember 31, 1993 and their recommendations present.d to the Governu-nt byDecember 31, 1994 (para 7.01(c).
3.19 Reform Proaram Imiolementation and Manaaement. To support thecreation and operations of the Hospital Restructuring Management Board (CGRH)(para 5.01), in charge of coordinating and superviuing the implementation of thereform program, the project would finance technical assistance, office technologyand logistics for the PCU (para 5.03).
B. ImDrovements in Ouality of Service (USS22.6 million)
a) Replacement of Priority Medical Eauipment. (USS10.0 million)
3.20 The project would provide medical equipment to improve diagnosticand therapeutic capabilities as well as the quality of medical services wheredeficiencies have been highlighted (para 2.19). The technical specificationsand quantities of equipment have been assessed during the project preparationand appraisal based on visita conducted in the field. Equipment to be providedis exclusively replacement medical equipment whose current shortage is severelydetrimental to adequate hospital operations.
b) Strenqthenino of Hospital Maintenance Units. (USS1.4 million)
3.21 A lack of maintenance of physical facilities and medical equipmentwas identified as a major drawback of Tunisian hospitals (para 2.18) The neworganizational structure would address this problem through the creation of amaintenance section whose managerial staff would be trained (para 3.09) andprovided with required management software (para 3.10). In addition, the projectwould provide equipment and tools for the maintenance units. To ensure itsproper allocation and use, this equipment would be made available to themaintenance units only after their managerial staff have been trained.
c) Improvement of Patient Accommodations, Hospital Hvaiene, EnvironmentProtection and Hazard Prevention. (USS11.2 million)
3 .22 Unsuitable physical conditions in a number of hospital wards aredetrimental to patients and staff morale and to the medical care rendered. Inorder to improve mediocre accommodations and hygiene, the project would providefor (i) the replacement of 2/3 of existing beds and bed sets, mobile partitions
- 20 -
for patient wards, improvementa in meal distribution, and priority replacementof kktchen and laundry equipment; and, (ii) priority renovation of electric,sanitation, heating and air-conditioning networks.
3.23 Environment Protection. As part of the project, the needs andoptions of the concerned hospitals for the handling of medical wastes and hazardprotection would be assessed (2 man-mon.hs)by December 31, 1993, and specificrecommendations proposed for implementation. Pending the conclusion of thisstudy, installation costs for each of the 17 hospitals not equipped withincinerators or fire protection systems have been estimated at US$60,000 perfacility.
IV. PROJECT COSTS AND FINANCINO
PROJECT COSTS
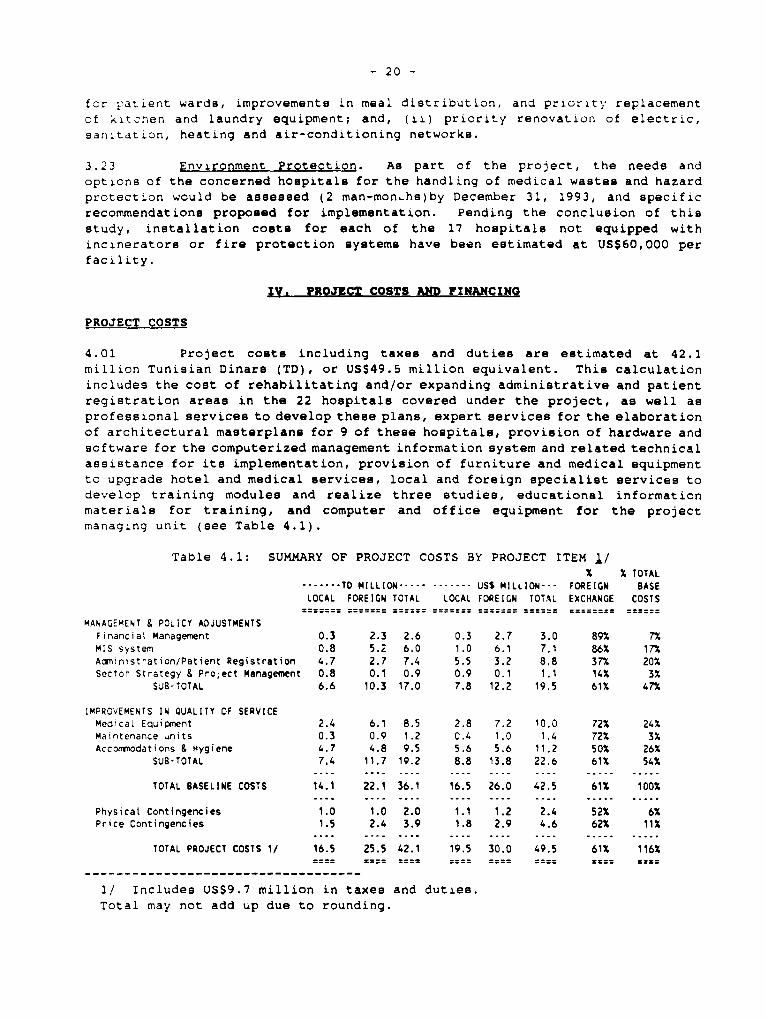
4.01 Project coste including taxes and duties are estimated at 42.1
million Tunisian Dinars (TD), or USS49.5 million equivalent. This calculationincludes the cost of rehabilitating and/or expanding administrative and patientregistration areas in the 22 hospitals covered under the project, as well asprofessional services to develop these plans, expert services for the elaborationof architectural masterplans for 9 of these hospitals, provision of hardware andsoftware for the computerized management information system and related technicalassistance for ita implementation, provision of furniture and medical equipmentto upgrade hotel and medical services, local and foreign specialist services todevelop training modules and realize three studies, educational informationmaterials for training, and computer and office equipment for the projectmanaginq unit (see Table 4.1).
Table 4.1: SUMMARY OF PROJECT COSTS BY PROJECT ITEM 1/X % TOTAL
T-OD MILLION ---- ------ US$ MILLION--- FOREIGN BASELOCAL FOREIGN TOTAL LOCAL FOREIGN TOTAL EXCHANGE COSTS
MANAGEMENT & POLICY ADJUSTMENTSFinanciat Management 0.3 2.3 2.6 0.3 2.7 3.0 89% 7%MIS system 0.8 5.2 6.0 1.0 6.1 7.1 86% 17%Administration/Patient Registration 4.7 2.7 7.4 5.5 3.2 8.8 37% 20%Sector Strategy & Project Management 0.8 0.1 0.9 0.9 0.1 1.1 14% 3%
SUB-TOTAL 6.6 10.3 17.0 7.8 12.2 19.5 61% 47%
IMPROVEMENTS IN QUALITY OF SERVICEMedicaL Equipment 2.4 6.1 8.5 2.8 7.2 10.0 72% 24%Maintenance units 0.3 0.9 1.2 0.4 1.0 1,4 72% 3%Accommodations & Hygiene 4.7 4.8 9.5 5.6 5.6 11.2 50% 26%
SUB-TOTAL 7.4 11.7 19.2 8.8 13.8 22.6 61% 54%.... .... . .... .... . .... .... . ...... ... .... .... .......... ..
TOTAL BASELINE COSTS 14.1 22.1 36.1 16.5 26.0 42.5 61% 100%.. ...................... .... ..... ---- ----. . .... . ...... .....
Physicat Contingencies 1.0 1.0 2.0 1.1 1.2 2.4 52% 6%Price Contingencies 1.5 2.4 3.9 1.8 2.9 4.6 62% 11%
TOTAL PROJECT COSTS 1/ 16.5 25.5 42.1 19.5 30.0 49.5 61% 116%==== -== == == == == === ====
l/ Includes US$9.7 million in taxes and duties.
Total may not add up due to rounding.
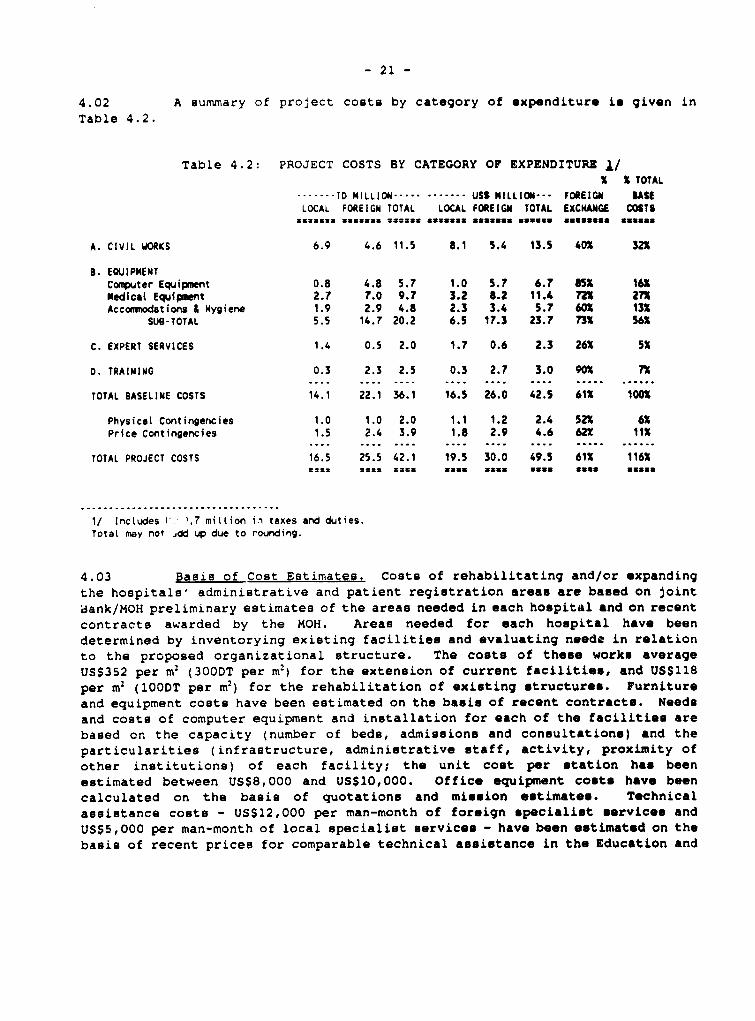
- 21 -
4.02 A summary of project conts by category of expenditure is given inTable 4.2.
Table 4.2: PROJECT COSTS BY CATEGORY OF EXPENDITURE ./X X TOTAL
-------TD MILLION .- ....... USt MILLION--- FOREIGGN USELOCAL FOREIGN TOTAL LOCAL FOREIGN TOTAL EXCNANGE COSTS
…u=--.. 33UE33 cans33 .---3 assuma* assuma eunuques mamans
A. CIVIL WORKS 6.9 4.6 11.5 8.1 5.4 13.5 40* 32K
B. EOUIPNENTCoeçuter Equipment 0.8 4.8 5.7 1.0 5.7 6.7 85K 16KM4edicat Equipmnt 2.7 7.0 9.7 3.2 t.2 11.4 72K 271Accomrodations I mygiene 1.9 2.9 4.8 2.3 3.4 5.7 60X 13X
SUS-TOTAL 5.5 14.7 20.2 6.5 17.3 23.7 73n 56X
C. EXPERT SERVICES 1.4 0.5 2.0 1.7 0.6 2.3 26X 5S
D. TRAINIMG 0.3 2.3 2.5 0.3 2.7 3.0 90K 72D. TRAINI"G 0 3~~. .. .. ...3 . .... .. .. .... ..... ......
TOTAL BASELINE COSTS 14.1 22.1 36.1 16.5 26.0 42.5 61X 100t
Physical Contingencies 1.0 1.0 2.0 1.1 1.2 2.4 52K 6KPrice Contingencies 1.5 2.4 3.9 1.8 2.9 4.6 62X 11l
TOTAL PROJECT COSTS 16.5 25.5 42.1 19.5 30.0 49.5 61X 116X
~~~~~~~~~~~~-=.. =.. ......=. a*-......*--........ .... ......
1/ Includes l' ,.7 miLLion i.i taxes and duties.TotaL may not ,dd up due to rounding.
4.03 Basis of Cost Estimates. Costs of rehabilitating and/or expandingthe hospitals' administrative and patient registration areas are based on jointaank/MOH preliminary estimates of the areas needed in each hospital and on recentcontracta awarded by the MOH. Areas needed for each hospital have beendetermined by inventorying existing facilities and evaluating neede in relationto the proposed organizational structure. The costs of these works averageUS$352 per m2 (300DT per m2) for the extension of current facilities, and US$118per m2 10ODT per m2) for the rehabilitation of existing structures. Furnitureand equipment costs have been estimated on the basis of recent contracte. Needsand costs of computer equipment and installation for each of the facilities arebased on the capacity (number of beds, admissions and consultations) and theparticularities (infrastructure, administrative staff, activity, proximity ofother institutions) of each facility; the unit cost per station has beenestimated between US$8,000 and US$10,000. Office equipment coste have beencalculated on the basis of quotations and mission estimates. T-chnicalassistance costs - US$12,OO0 per man-month of foreign specialiat *ervices andUS55,000 per man-month of local specialist services - have been estimat.d on thebasis of recent prices for comparable technical assistance in the Education and
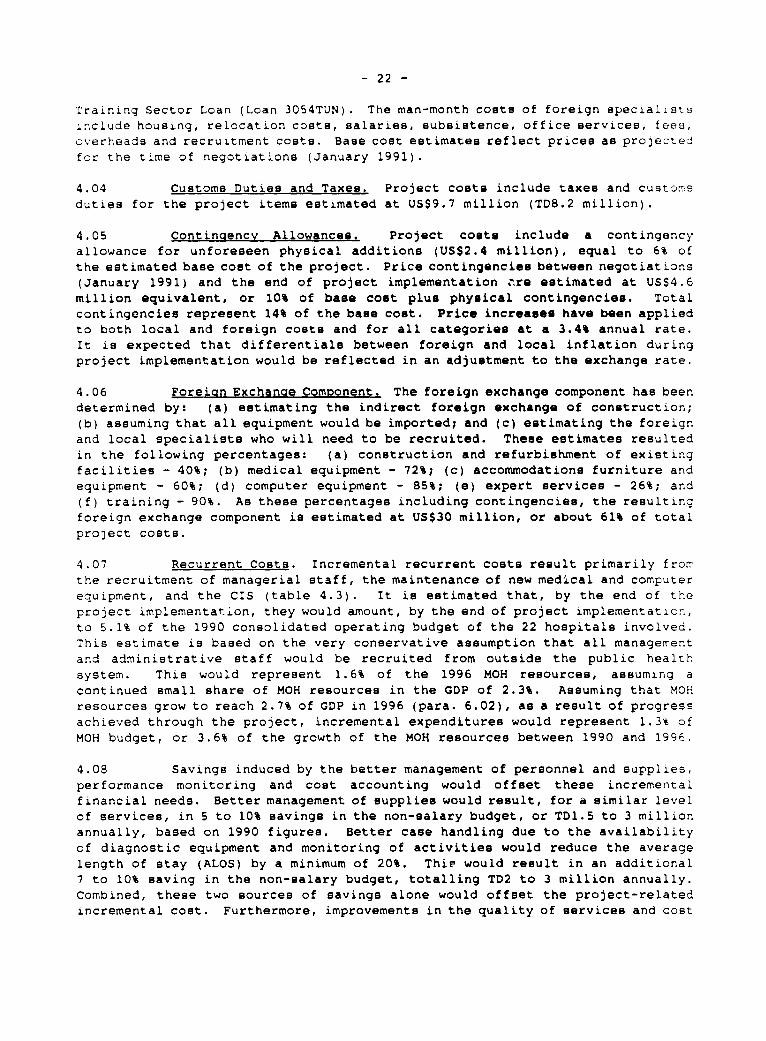
- 22 -
TraLning Sector Loan (Loan 3054TUN). The man-month coste of foreign speciallstsinclude housing, relocation coste, salaries, subsistence, office services, fees,overheads and recruitment costs. Baee cost estimates reflect prices as projeztedfor the time of negotiations (January 1991).
4.04 Custome Duties and Taxes. Project costa include taxes and customsduties for the project items estimated at USS9.7 million (TD8.2 million).
4.05 Continaencv Allowances. Project colts include a contingencyallowance for unforeseen physical additions (US$2.4 million), equal to 6% ofthe estimated base coat of the project. Price contingencies between negotiations(January 1991) and the end of project implementation are estimated at US$4.6million equivalent, or 10% of base cost plus physical contingencies. Totalcontingencies represent 14% of the base cost. Price increases have been appliedto both local and foreign coete and for all categories at a 3.4% annual rate.It is expected that differentialB between foreign and local inflation duringproject implementation would be reflected in an adjustment to the exchange rate.
4.06 Foreign Exchanae ComDonent. The foreign exchange component has beendetermined by: (a) estimating the indirect foreign exchange of construction;(b) assuming that all equipment would be imported; and (c) estimating the foreignand local specialists who will need to be recruited. These estimates resultedin the following percentages: (a) construction and refurbishment of existingfacilities - 40%; (b) medical equipment - 72%; (c) accommodations furniture andequipment - 60%; (d) computer equipment - 85%; (e) expert services - 26%; and(f) training - 90%. As these percentages including contingencies, the resultingforeign exchange component is estimated at US$30 million, or about 61% of totalproject costs.
4.07 Recurrent Costa. Incremental recurrent costs result primarily frorrthe recruitment of managerial staff, the maintenance of new medical and computerequipment, and the CIS (table 4.3). It is estimated that, by the end of theproject implementation, they would amount, by the end of project implementation,to 5.1% of the 1990 consolidated operating budget of the 22 hospitals involved.This estimate is based on the very conservative assumption that all managementand administrative staff would be recruited from outside the public healthsystem. This would represent 1.6% of the 1996 MOH resources, assuming acontinued small share of MOH resources in the GDP of 2.3%. Assuming that MOHresources grow to reach 2.7% of GDP in 1996 (para. 6.02), as a result of progressachieved through the project, incremental expenditures would represent 1.3% ofMOH budget, or 3.6% of the growth of the MOH resources between 1990 and 1996.
4.08 SavingB induced by the better management of personnel and supplies,performance monitoring and cost accounting would offset these incrementalfinancial needs. Better management of supplies would result, for a similar levelof services, in 5 to 10% savings in the non-salary budget, or TD1.5 to 3 millionannually, based on 1990 figures. Better case handling due to the availabilityof diagnostic equipment and monitoring of activities would reduce the averagelength of stay (ALOS) by a minimum of 20%. Thie would result in an additional7 to 10% saving in the non-salary budget, totalling TD2 to 3 million annually.Combined, these two sources of savinge alone would offset the project-relatedincremental cost. Furthermore, improvements in the quality of services and cost
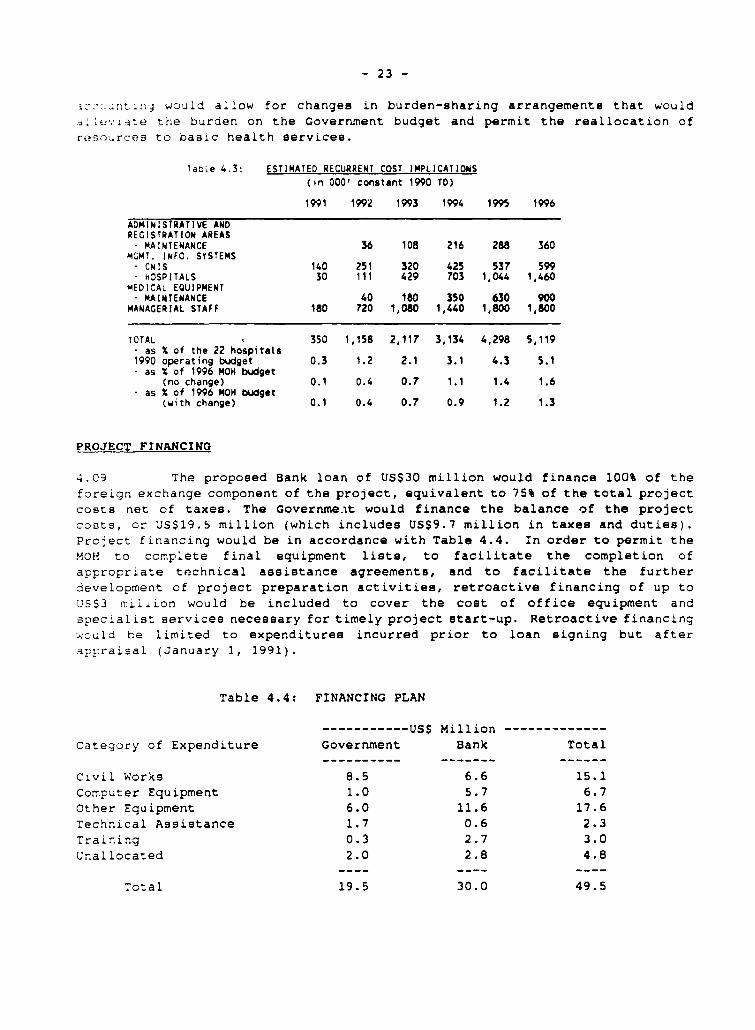
- 23 -
3c,nt:n-j would allow for changes in burden-sharing arrangements that wouldA W.': te the burden on the Government budget and permit the reallocation ofres;urces to basic health services.
table 4.3: ESTIMATED RECURRENT COST IMPLICATIONS
(in 000' constant 1990 TD)
1991 1992 1993 1994 1995 1996
ADMINISTRATIVE ANDREGISTRATION AREAS- MAINTENANCE 36 108 216 288 360
MGMT. INFO. SYSTENSCNIS 140 251 320 425 537 599
- hOSPITALS 30 111 429 703 1,044 1,460MEDICAL EQUIPMENT- MAINTENANCE 40 180 350 630 900
MANAGERIAL STAFF 180 720 1,080 1,440 1,800 1,800
TOTAL 350 1,158 2,117 3,134 4,298 5,119- as X of the 22 hospitals1990 operating budget 0.3 1.2 2.1 3.1 4.3 5.1- as X of 1996 MOH budget
(no change) 0.1 0.4 0.7 1.1 1.4 1.6- as X of 1996 NOM budget
(with change) 0.1 0.4 0.7 0.9 1.2 1.3
PROJECT FINANCING
4.09 The proposed Bank loan of US$30 million would finance 100% of theforeign exchange component of the project, equivalent to 75% of the total projectcosts net of taxes. The Goverrine.it would finance the balance of the projectcosts, cr US$19.S million (which includes US$9.7 million in taxes and duties).Project financing would be in accordance with Table 4.4. ifn order to permit theMOH to complete final equipment lists, to facilitate the completion ofappropriate technical assistance agreements, and to facilitate the furtherdevelopment of project preparation activities, retroactive financing of up toUS$3 milion would be included to cover the cost of office equipment andspecialist services necessary for timely project start-up. Retroactive financingwould be limited to expenditures incurred prior to loan signing but afterappraisal (January 1, 1991).
Table 4.4: FINANCING PLAN
-----------US$ Million -------------category of Expenditure Goverrnment Bank Total
cLvil Works 8.5 6.6 15.1Computer Equipment 1.0 5.7 6.7Other Equipment 6.0 11.6 17.6Technical Assistance 1.7 0.6 2.3Training 0.3 2.7 3.0
Unallocated 2.0 2.8 4.8
Total 19.5 30.0 49.5
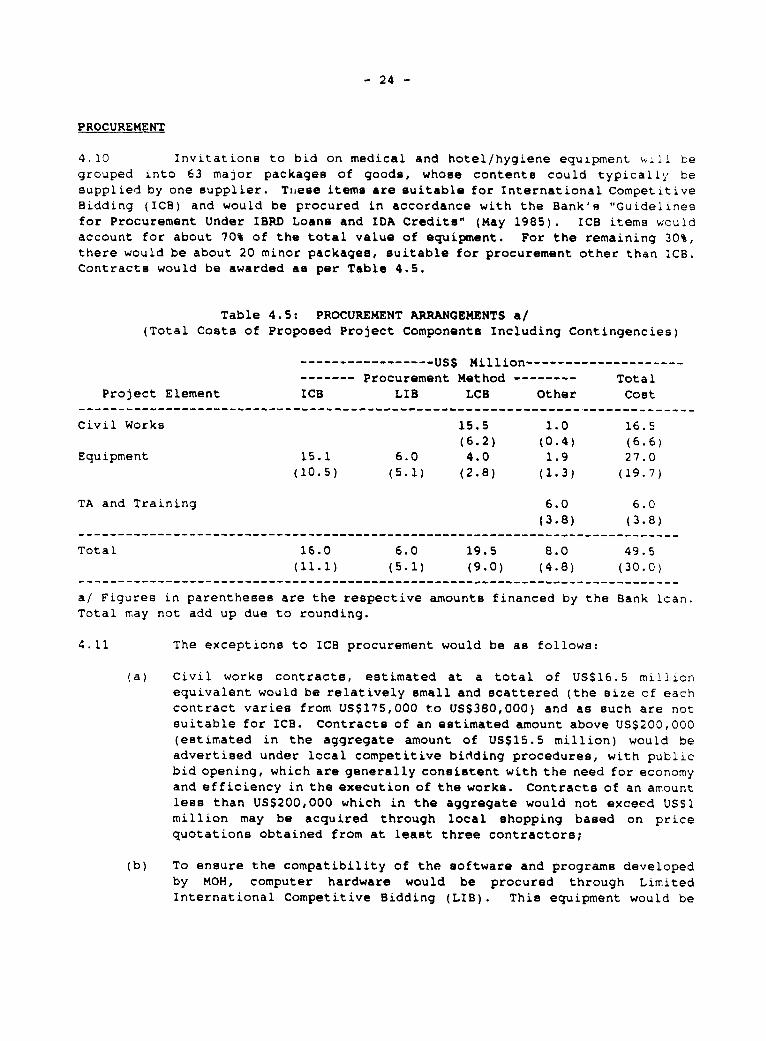
- 24 -
PROCUREMENT
4.10 Invitations to bid on medical and hotel/hygiene equipment will begrouped into 63 major packages of goode, whose contente could typically besupplied by one supplier. Tinese items are suitable for International CompetitiveBidding (ICB) and would be procured in accordance with the Bank'e "Guidelinesfor Procurement Under IBRD Loanc and IDA Credits" (May 1985). ICB items wouldaccount for about 70% of the total value of equipment. For the remaining 30%,there would be about 20 minor packages, suitable for procurement other than ICB.Contracte would be awarded as per Table 4.5.
Table 4.5: PROCUREMENT ARRANGEMENTS 8/
(Total Coste of Proposed Project Components Including Contingencies)
…-----US$ Million--------------------------- Procurement Method -------- Total
Project Element ICB LIS LCB Other Cost
Civil Works 15.5 1.0 16.5(6.2) (0.4) (6.6)
Equipment 15.1 6.0 4.0 1.9 27.0(10.5) (5.1) (2.8) (1.3) (19.7)
TA and Training 6.0 6.0(3.8) (3.8)
----------------------------------------------------------------- __---------
Total 16.0 6.0 19.5 8.0 49.5(11.1) (5.1) (9.0) (4.8) (30.0)
---------------------------------------------------------------- __----------
a/ Figures in parentheses are the respective amounts financed by the Bank loan.Total may not add up due to rounding.
4.11 The exceptions to ICB procurement would be as follows:
(a) Civil works contracte, estimated at a total of US$16.5 millionequivalent would be relatively emall and scattered (the size of eachcontract varies from US$175,000 to US$380,000) and as cuch are notsuitable for ICB. Contracte of an estimated amount above US$200,000(estimated in the aggregate amount of US$15.5 million) would beadvertised under local competitive bidding procedures, with publicbid opening, which are generally consistent with the need for economyand efficiency in the execution of the works. Contracte of an amountles6 than US$200,000 which in the aggregate would not excecd US$1million may be acquired through local shopping based on pricequotations obtained from at least three contractors;
(b) To ensure the compatibility of the software and programe developedby MOH, computer hardware would be procured through LimitedInternational Competitive Bidding (LIB). This equipment would be
- 25 -
grouped in about 10 packages averaging US$600,000 each for anaggregate amount equivalent to US$6 million.
(c) Contracts for furniture and equipment estimated to cost less thanUSS300,000 equivalent each, which in the aggregate would not exceedUS$4.0 million and which would not be expected to interest foreignsuppliers because of the variety of each contract, would beadvertised under local competitive bidding procedures (LCB);
(d) Sundry items not exceeding US550,000 in each contract and aggregatinga maximum of USS1.0 million equivalent could be purchased throughlocal shopping on the basis of a minimum of three quotations;
(e) Computer software and *pecialized programn developed as part of thesetting-up of the hospitals' MIS estimated at USS 0.9 million wouldbe procured thrcugh direct contracting in accordance with proceduresacceptable to the Bank, to ensure time - and cost -efficiency (byadapting existing programs) and continuity in the development ofthese programe in line with the overall objectives of the reforms;
(f) Fellowships, stipends, transportation costs and preparation ofeducational materials (estimated to cost about US$3.6 million) forthe training programs would be procured trough direct contractingin accordance with procedures acceptable to the Bank.
4.12 In comparison to bids for equipment to be procured through ICB,domestic manufacturera would be allowed a preferential margin of 15%, or theexisting customs duty, whichever is lower over the c.i.f. prices of competingimports. Under ICB, LIB and LCB procedures, invitations to bid and the proposedcontract awards would be reviewed by the Bank prior to final award decisionsfor all contracts over US$350,000. It is estimated that this review would coverabout 80% of the total value of equipment contracte of US$25.1 millionequivalent. The remaining 20% would be subject to selective post-award reviews.
4.13 Technical Assistance. To simplify management of technicalassistance, the MOH would obtain specialist services as comprehensive TA packagesin accordance with principles and procedures acceptable to the Bank on the basisof the "Guidelines for the Use of Consultante by World Bank Borrowers and by theWorld Bank as Executing Agency" (March 1981).
4.14 ResDonsibilitv for Procurement. To maximize efficiency and ensurelowest prices, and to take advantage of MOH experience in procurement, the PCUwould be responsible for the preparation of equipment liste and specifications,in collaboration with the MOH's Buildings and Equipment Department (DBE) andCentral Maintenance Unit (Centre National de Maintenance). The PCU would alsocoordinate the preparation of the architectural masterplans and constructionplans (para 3.14 & 3.17) and would monitor progresa in implementation.
STATUS OF PREPARATION AND DISBURSEMENTS
4.15 The funds for the proposed project would be disbursed over a periodof six and a half years, which is shorter than the average disbureement profile
- 26 -
for all sectors in Tun.sia (8 yeare). This is realistic in view of the highsoftware/ecquipment content of the project and of the fact that: (a) civil worketo be realized do not require site acquisition and are relatively minor for eachsite; (b) timely implementation of the training and medical equipment componentsiS not linlkcd to the implementation of civil works; (c; equipment liste havealready been prepared and the elaboration of technical specifications will befacilitated by the MOH computerized Bystem; (d) implementation of the projectwould be decentralized at the hospital level, thus providing greater flexibilityto each of the components. Project completion in net for March 31, 1997 andthe Closing Date would be September 30, 1997. Diebursemente would be madeagainst:
(a) 40% of the total expenditures on civil works;
(b) 100% of the foreign expenditures for directly imported computerequipment materials and of the ex-factory expendituree for locallymanufactured computer equipment; and 85% of local expenditures forother computer-related items procured locally;
(c) 100% of the foreign expenditures for directly imported hospitalequipment, furniture and educational materials and of the ex-factoryexpenditures for locally manufactured equiptment and furniture; and70% of local expenditures for other items procured locally;
(d) 100% of the total expenditures for foreign consultant services ardfellowships.
4.16 Disbursemente against contracte for goods and services exceedingUS$200,000 equivalent would be made againet normal documentation. Disbursementsagainst contracts equal or below that level as well as all items related totraining, including contracts for training services, liste of recipients in thecase of stipends, allowances and fellowships with the amounts provided andinvoices for materials and consumables would be made on the basis of Statementsof Expenditures (SOEs), available for examination by Bank missions.
4.17 Soecial Account. To facilitate timely project implementation, theGovernment would establish, maintain and operate, under terms and conditionssatisfactory to the Bank, a Special Acccunt in US dollars at the Central Bankof Tunisia to which the World Bank would make an initial deposit, equivalent toabout US$2.0 million and representing about four months of projected Bankexpenditures. The Special Account would be replenished at least every threemonths or whenever one-third of the amount of the initial deposit has beenwithdrawn, whichever comes first. Documentation for replenishment of the SpecialAccount would follow the same procedure as in paragraph 4.14. In addition,monthly bank statements would accompany replenishment requeste. Tne minimum-size withdrawal applications acceptable by the Bank will be US$200,000equivalent. Modalities concerning the use of SOEs and the Special Account wereagreed upon at negotiations.
4.18 Accounts and Audits. Separate accounts for the project would bemaintained. Each semester a detailed etatement reflecting project expendituresduring that period and proje ted expenditures for the forthcoming semester wouldbe prepared. Within 45 days after the end of each semester, copies of these

- 27 -
statements would be submitted to the Bank to tacilitate superviBion. Projectaccounts includLng the Special Account (para.4. 17) would be audited in accordancew.th the March 1982 Bank "GuidelineB for Financial Reporting and Auditing ofProjects Financed by the World Bank". Within nine months of the end of eachfiscal year, the Bank would be provided with an audit report of such scope anddetail as it may reasonably request, including a separate opinion by the auditorcf disbursements against a certified statement of expenditures. The Governmentprov.ded assurances to this effect during negotiations (para 7.02 (9g>
V. IMPLEMENTATION, MANAGEMENT, SUPERVISION AND EVALUATION
5.01 Implementation of the Government reform program would be coordinatedand supervised by a Hostoital Restructurina Manacement Board (CGRH) which wouldbe instituted to coincide with the start of the project. It would be composedof:
- the Minister of Public Health (or hie representative), Chairman;- the General Managers of the hospitals transformed into EPS;- the MOH directors involved in the reform and the Director of CNIS;
and,- the Project Coordination Unit (PCU) (para 5.03).
5.02 The CGRH would meet at least twice a year at the initiative of theMinister of Public Health or upon request from one of its members as needed toensure the coherence of all reforms and project activities and in particular (i)te discuss the proposed annual implementation program; (ii) to proposeadjustments and rescheduling as needed; and (iii) to monitor and analyze progressachieved.
IMPLEMENTATION AND MANAGEMENT
5.03 Through its management and implementation structure, the projectwould contribute to a greater capacity to plan, monitor and formulate policy atthe central level (MOH), while at the same time increasing the hospitals'responsibilities, as they progressively reinforce their management capacitythrough the project activities (new organizational structure, training, MIS..).To this end, a Project Coordination Unit (PCU) would be created and maintainedfor the duration of the project. It would be headed by a full time Coordinator,staffed with 4 technical staff, i architect, 3 administrativo staff and anaccountant, and complemented by staff from the relevant MOH rlirectorates. Itsmain responsibilities would be:
<a) to act on behalf of CGRH as the man;ging entity of all projectactivities and to propose (to its approval) annual implementationprograms. The PCU would be responsible for preparing the CGRH meetingagendas and related documentation;
(b) on behalf of the MOH, to ensure the formulation of the sectoralstrategies (meaium-term strategic hospital plan, studies on burden-
- 28 -
sharing arrangements.. )(paras 3. 15-20), to inform CGRH of theconclusione of these atudies and to monitor their implementation;
(c) to coordinate the implementation of the project components, tomonitor and evaluate progrees in performance indicators and identifyand design corrective measures when needed, to carry out ccntralizedactivities, such as procurement and diabursements (para 4.13), andto keep project accounte. In particular, PCU will provide supportand advice to hospital.' General Managers responsible for theimplementation of the project items in their establishment (para5.04); and,
(d) to liaise with the Bank (para 5.06).
5.04 As part of the efforts to decentralize responsibilities supportedby the project, the PCU would delegate responsibility for implementation at thehospitals' General Manager level. The project, as described in Chapter III, hasbeen broken down hospital by hospital, so that hospital-apecific activities areidentified and programmed over the implementation period. When nominated (para3.02 and 7.03 (b)), the General Manager would receive, from the PCU, a hospital-specific "project file" describing the scope and objectives of the project, theactivities to take place, their proposed implementation schedule and their cost.Each hospital's General Manager would be responsible for implementing theincremental project-related activities:
(a) identify and select managerial staff in accordance with job profiles,and propose their nomination to MOH;
(b) program managerial staff training in accordance with component'implementation schedule;
(c) introduce financial management and evaluation procedures as definedin the new financial management manual and directives from MOH (para3.06);
(d) ccordinate with CNIS, the development and introduction of theManagement Information Systems;
<e) coordinate and supervise all activities related to improvements ofservice quality, civil work and architectural masterplanning, andin particular assist the PCU in the elaboration of equipment listeto be procured; and,
(f) provide the PCU with quarterly progres. reports.
5.05 The establishment of CORN and PCU constitute conditions of loaneffectiveness (para. 7.02 (a). Both CGRE and PCU will be maintained, withstaffing and terus of roference acceptable to the Bank, for the duration of tueproject (para 7.01 (h).
- 29 -
SUPERVISION, MONITORINO AND EVALUATION
CD , (Fr. SUD_evision. The project would be supervised and monitored by the
23a&lk *tÀrh the normal supervision mechanism. However, as the project concept
L. t,.*th cs)îplex and innovative, and there is no prior experience in lendzng for
such naraement operations in social sectors, this would require about 25 staff-
weeks over the first two yearB of implementation and 50 staff-weeks over the
fcllowinq five years. Financial management/MIS skills are likely to be essential
for Bank staff missions. Supervision would rely on a bi-annual progress report
prepared by the PCU and on Bank miesions to elaborate remedial measures, when
needed, together with the PCU; finally, an annual progreus report would be
prepared to review achievements towards tho project i-ple-entation targets, and
towards project objectives based on the agreed monitoring indicators (para 5.07)
and implementation review meetings h-ld at least anually with the Bank. A
project completion report would be *ubaitted to the Bank within six months ofthe loan closing date (para.7.02 (i>).
5.07 Monitorina and Evaluation. The monitoring and evaluation of the
project would include two eets of indicators: (i) project implementation
indicators that would help monitor the smooth and timely implementation of the
project activities, and (ii) performance indicators related to the projectobjectives. These two sets of indicators would be specified by the PCU in
collaboration with the hoBpital managers and agreed upon with the Bank within
six months of project effectivenese. The definition of monitoring indicators
would include the specification of reference bench-mark data for each of them.
5.08 Implementation indicators would be specific for each component of
the project and related to a specified period of time (e.g.six monthe), and
would consist of ratios between the actual achievements and the targets (e.g.
number of people trained versus number of people programmed to be trained; number
of equipment procured ver3us plans for procurement; progrese in civil works..).
For non-measurable activities (like the studies), the indicator would be whether
the deadlines have been met and the reports finalized, presented and discussed
as agreed in the implementation programe.
5.09 Performance indicators related to the proiect obiectives would be
developed to monitor progress towards the project objectives as stated in para
3.04. Specifically, indicators should be developed in the following areas,
Improvemrents in Internal Efficiencv.
Managerial efficiency:- Staffing: evolution of staffing according to plans (oraanizational
chart) and availability of progrees reports;- Implementation of project activities according to plan3 and
schedules;- Availability of financial information according to Financial
Management Model;- Availability of utilization indicators: admissions, visits, Average
Length Of Stay (ALOS); Occupancy Rate (OR), and reporting on theirevolution;Availability of patients' administrative information, and analysis
of ita linkage with utilization of service;Adherence to hospital maintenance standards; etc..
- 30 -
Technical efficiency:- Changes in utilization patterns; reduction of ALOS; reduction in A',OS
differences among hospitais;Increase in equipment utilization; e.g: number of examina.lnus/
day/equipment; number of surgical intervent.ons/day/operatinr.
thsLter; etc..- Reduction in waiting time for appointments and prccedures: electivp
surgery, X-ray examinations, laboratory tests, etc..
Cost Containment
- Availability of cost information by hospital, hospital department,
group of diseases, and by unit of measurement (hospital day, visit,
treatment..) and catagory of colt (personnel, druge, etc..)
- Availability of annual financial reports and documentation for the
hospitals corncerned;- Reduction in cost differences among the different hospitals for
Bimilar clinical departments and groupa of diseases;
- Identif.cation of factors contributing to cost increases and cost
control: reports analyzing coet evolution and measures being taken;
Imorovement of Oualitv of Services.
- Quality assurance procedures; peer review;
- Monitoring and control of hospital related infection rates;
- Adherence to professionally defined standards by specialty wards;
- Pharmaceutical prescription reviews;- Patient satisfaction and social acceptability: waiting time for
appointments and procedures, surveys of client satisfaction, etc..
Definition of Adiustments in Burden-Sharina Arrangements.
- Adherence to the Government strategy and orientations (para 2.22 ani
Annex 2);- Updating of fee schedules;
- Updating of co-payments;
- Reorganization of indigence programs;
- Contribution of the social insurance programs to MOH resources, in
line with cost and utilization patterns of services provided to their
beneficiaries.
VI. BENEFITS AND RISKS
BENEFITS
6.01 The proposed project would address several of the critical issues
confronting the Tunisian health sector. Major progress is expected in: (i)
hospital cost containment and quality of services through enhanced internal
efficiency; and, (ii) better equity in the financing of health care services
through the definition of methods to link utilization of services with burden-
sharing responsibilities.
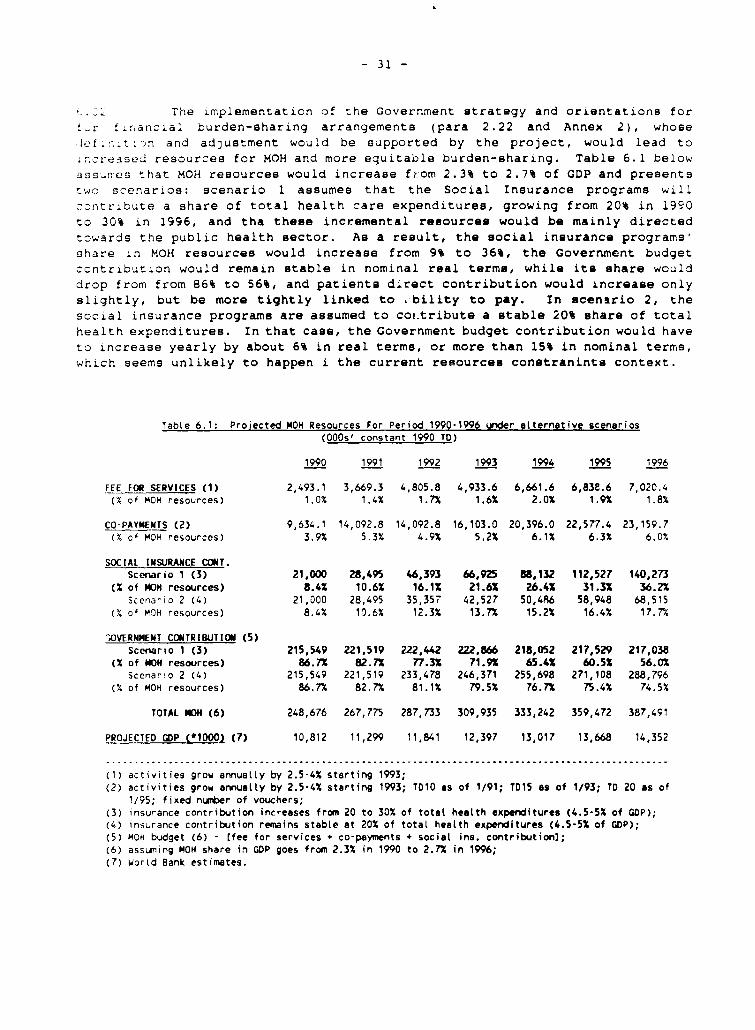
- 31 -
The implementation of the Government strategy and orientations for!*r hlr;ancLal burden-sharing arrangements (para 2.22 and Annex 2), whosehŽhr . t -n and adjustment would be supported by the project, would lead toin_reasei? resources for MOH and more equitable burden-sharing. Table 6.1 belowassurres that MOH resources would increase from 2.3% to 2.7% of GDP and presentsts2o scenarios: scenario 1 assumes that the Social Insurance programe willzDntrzbute a share of total health care expenditures, growing from 20% in 1990to 30% in 1996, and tha these incremental resources would be mainly directedtowards the public health sector. As a result, the social insurance programs'share in MOH resources would increase from 9% to 36%, the Governmcnt budgetcontribution would remain stable in nominal real terme, while its share woulddrop fromn from 86% to 56%, and patients direct contribution would increase onlyslightly, but be more tightly linked to .'bility to pay. In acensrio 2, thesocial insurance programs are assumed to cor.tribute a stable 20% share of totalhealth expenditures. In that case, the Government budget contribution would haveto increase yearly by about 6% in real terms, or more than 15% in nominal terms,which seems unlikely to happen i the current resources constranints context.
Table 6.1: Proiected MOH Resources For Period 1990-1996 under alternative scenarios(0OOs' constant 1990 Tr)
1990 1991 1992 1993 1994 1995 1996
FEE FOR SERVICES <1) 2,493.1 3,669.3 4,805.8 4,933.6 6,661.6 6,838.6 7,020.4(Y of MOH resources) 1.0% 1.4% 1.7% 1.6% 2.0% 1.9% 1.8%
CO-PAYMENTS (2) 9,634.1 14,092.8 14,092.8 16,103.0 20,396.0 22,577.4 23,159.71% of MOH resources) 3.9% 5.3% 4.9% 5.2% 6.1% 6.3% 6.0%
SOCIAL INSURANCE CONT.Scenario 1 (3) 21,000 28,495 46,393 66,925 88,132 112,527 140,273
(% of MON resources) 8.4% 10.6X 16.1% 21.6% 26.4X 31.32 36.2%Scenario 2 (4) 21,000 28,495 35,357 42,527 50,486 58,948 68,515oX of MO)H resources) 8.4% 10.6% 12.3% 13.7X 15.2% 16.4% 17.7%
,OVERNMENT CONTRIBUTION (5)Scenario 1 (3) 215,549 221,519 222,442 222,866 218,052 217,529 217,038
<X of i40H resources) 86.7% 82.7% 77.3% 71.9X 65.4X 60.5X 56.0%Scenario 2 <4) 215,549 221,519 233,478 246,371 255,698 271,108 288,796
(o of MOH resources) 86.7% 82.7% 81.1% 79.5% 76.7% 75.4% 74.5%
TOTAL MON (6) 248,676 267,775 287,733 309,935 333,242 359,472 387,491
PROJECTED GDP <*1000> (7) 10,812 11,299 11,841 12,397 13,017 13,668 14,352
(1) activities grou annualty by 2.5-4% starting 1993;(2) activities grow annually by 2.5-4% starting 1993; TD10 as of 1/91; TD15 as of 1/93; TG 20 as of
1/95; fixed numb>er of vouchers;(3) insurance contribution increases from 20 to 30X of total heatth expenditures (4.5-5 of GDP);(4) insurance contribution remains stable at 20% of total health expenditures (4.5-52 of GDP);(5) MOH budget (6) - Ifee for services + co-payments + social ins. contribution];(6) assuming MOH share in GOP goes from 2.3% in 1990 to 2.7% in 1996;(7) Wortd Bank estimates.
- 32 -
6.03 These projections are based on assumptions that include additionaliricreases in the fee-for-services after 1994 (25% on average), increases in thecost of vouchers for the indigence programa (TD15) following the completion ofthe related study, and increases in co-payments (25% on average). Theseadjustments would permit to maintain the contribution of fee-for- eervices and<o-payments stable at around 8% of MOH resources.
6.(v4 To match their incremental role in financing health services, thesocial insurance programe would have to: (i) increase their enrollment rates;and, (ii) reconsider the level of contribution of both employers and employeesin regard with the benefits provided. Increasing the currently low enrollmentrate should constitute a major objective of the social insurance programs andefforts chould focus on groupe of the population who are currently under-covered, mainly îndependent workers (non salaried) from both the agriculturaland non-agricultural sectors.
6.05 The adjustments in burden-sharing arrangements described above wouldpermit to reallocate resources towards basic health care and to improve thequality of services in the entire public health sector which would benefitdirectly the vast majority of the population needing hospital and non-hospitalcare.
6.06 In addition, the project inputs involve three maternity hospitalsin Sfax, Sousse and Tunis, and the maternity departmenta of all other generalhospitals included in the project. These facilities provide for 43% of ailattended deliveries nationally. Hence, the qualitative improvementa for safedeliveries, obstetrical interventions and post-partum care would be significant.Greater effectivenesa and efficiency in the provision of services will have apositive impact on the health statue of the Tunisian population.
6.07 Finally, the project would contribute to the protection of theenvironment through improving the handling of medical wastes and supportingactivities that would improve hospital hygiene and maintenance. Trainingfellowships for managerial hospital staff in charge of environmental hazardswould also be financed.
RISKS
6.08 The main rick of the project relates to the ability of new hoepitalmanagers to successfully introduce and implement the hospital reforma andovercome the system's rigidities and natural resistance to change. To compensatefor the limited experience and skille of local managers, an extensive trainingprogram and technical aseistance are included in the project and therestructuring program hae been phaned to allow evaluation and adjustment basedon experience with the first institutions.
6.09 Another possible risk is the lack of incentivec among civil serviceto be cost-conscious in utilizing existing resources. This zisk, however, willbe mitigated by the introduction of new budgeting procedures that would allowhospital departmente to retain most of the savinga generated through their
- 33 -
efforts, and the development of financial management standards that would allow
senior hospital managers to monitor performance.
6.10 Finally, sustained benefits in terme of a permanently reduced burden
on Gcvernment resourceB (para 6.02), ultimately depend on the outcome of the
negotiations with its social partners (the medical profession, unions andemployerb for health insurance and local communities for indigent coverage) that
will be contingent upon the broader economic developments. The project aims at
reestablishing the image of public houpitals as quality care providers and
supplying the Government with evidence on truo health sector cost and utilization
patterns that would underpin these negotiatione.
VI!. AGREEMNTS REACHED AND RECOKENUDATIONS
7.01 During negotiations, it waa confirmed that the Government had
approved the draft laws creating the "Etablissements Publics de Santé" (EPS)
(para 3.02) and the "Centre d'Informatique Sanitaire" (CIS) (para. 3.11). The
Government also provided assurances that:
(a) the draft law creating EPSB ehall be preaented to Parliament for
approval (para. 3.02);
(b) it will transform into EPS: the eight hospitals referred to in Part
B, Annex 3, table 1 by December 31, 1992; the five hospitals referred
to in Part B, Annex 3, table 1 by December 31, 1993 , and the
remaining five hospitals (part D, Annex 3, table 1) by December 31,
1994; and ensure that the new legal statutes of these hospitals is
maintained for the duration of the project (para. 3.02);
(c) The studies mentioned at paragraph 3. 17 and Annex 2 will be completed
by december 31, 1993 and their recommendations presented to the
Government by December 31, 1994 (para 3.18);
(d) The CIS shall have been established and its director appointed by
September 30, 1991 (para. 3.11);
(e) A medium-term plan for hospital network development will be
formulated and submitted for joint review with the Bank by September
30, 1992 (para 3.15), and thereafter carried out;
(f) A financial management manual acceptable to the Bank will be prepared
by September 30, 1991 to be thereafter used as part of the trainingof managerial staff and distributed to senior and mid-level
administrators within the hospitals transformed into EPS starting
January 1, 1992 (para. 3.06);
(g) Architectural masterplans would be formulated for 9 pre-selectedhospitals and reviewed with the Bank by December 31, 1992, and
thereafter carried out. No activity related to the rehabilitation
- 34 -
of administrative and patient registration areas (paj.a.3. 13) w.11be implemented in the hospitals concerned before the dpprJval of
these masterplans by the Bank (para 3.16);
(h) Both CGRH and PCU will be maintained, with staffLng and terms cf
reference acceptable to the Bank, for tte duration cf the prciezt
(para. 5.05);
(i) Joint implementation review meetings would be held at least annually,
to discues progresu and review and agree on the following scx-rncth
program (para. 5.03 (d)); and, within six months of the Loar; ClDsi..g
date, a completion report would be prepared by the PCU and submittei
to the Bank (para. 5.06); and,
(j) Project accounts, including Special Accounts, would be audited by
auditors acceptable to the Bank and in accordance with appropriate
auditing principles; and that the Bank will be provided within nine
monthe of the end of the Government's fiscal year with (i) certified
copies of the project accounts; and (ii) an audit report of such
scope and detail as the Bank may reasonably request, including a
separate opinion by the auditor on disbursements against certified
statement of expenses (para 4.17).
7.02 The Government has agreed that the following shall constitute
conditions of effectiveness:
<a) the Government will establish the Hospital Restructuring Management
Board (CGRH) and the Project Coordination Unit (PCU) (para 5.05);
and
(b) the law creating the EPS will be enacted by the Parliament; and the
four hospitals listed under part A of Annex 3, Table l will be
transformed into EPS, and their General Managers appointed (para.
3.02).
7.03 The Government also agreed that for the last 18 hospitals, the
disbursement of loan proceeds for equipment (excluding computer equipmert) >W11l
be conditioned to the prior transformation into EPS of hospitals referred to in
Part B and C of Annex 3, and, for civil works to the prior transformation of
hospitals in Part B of Annex 3 (para 3.02).
7.04 Subject to the above conditions, the project constitutes a suitale
basis for a Bank loan of USS30 million to the Republic of Tunisia.

35
ANNEXES
Table of ContentsPaoe
ANNEX 1. Sector Statistical Annex
Table 1. Personnel Resources (1989) ....................................... 36Table 2. The Health Infrastructure (1989) .37Figure 1. Division of Beds By Specialty (1989) Public Sector .38Figure 2. Division of Beds By Type of Hospital (1989) .38Figure 3. Admissions By Type of Hospital (1989) Public Sector .39Figure 4. Division of Hospital Days (1989) By Type of Hospital .39
ANNEX 2. Outline of Governe-nt Financial Strat-gy and Orientations
Appendix l.Government's letter .............................................. 40Appendix 2.Terms of reference ans Szhedule for Project supported studies ... 45
ANNEX 3. Hospital Statirtical Annex
Table 1. List of Establishments Concerned ................................. 48Figure 1. Budget Allocations 1990; 22 Teaching Hosp/Spec Institutes ........ 49Table 2. Activity Indicators of the 22 establishments ..................... 53Table 3. Comparison of Indicators of Activity in Various Univ Hosp Depts ..56
ANNEX 4. The Future Legal and Organizational Structure of TunisianPublic Hospitals
A. Objectives. 58B. Factors Considered in the selection of a legal statute .................. 59C. The Future Legal Structure .............................................. 60D. The Future Organizational Structure .................................... 61Table. organizational Chart for General Hospitals Or Spec Insts .. 65
ANNEX 5. MIS Component
A. Institutional Context ................................................... 66
B. National Deployment of the Information Technology Function .............. 67C. Application Architecture ................................................ 68D. Technical Architecture .................................................. 69E. Activities Required Prior to the Introduction of the System ............. 70F. Timetable ............................................................... 72
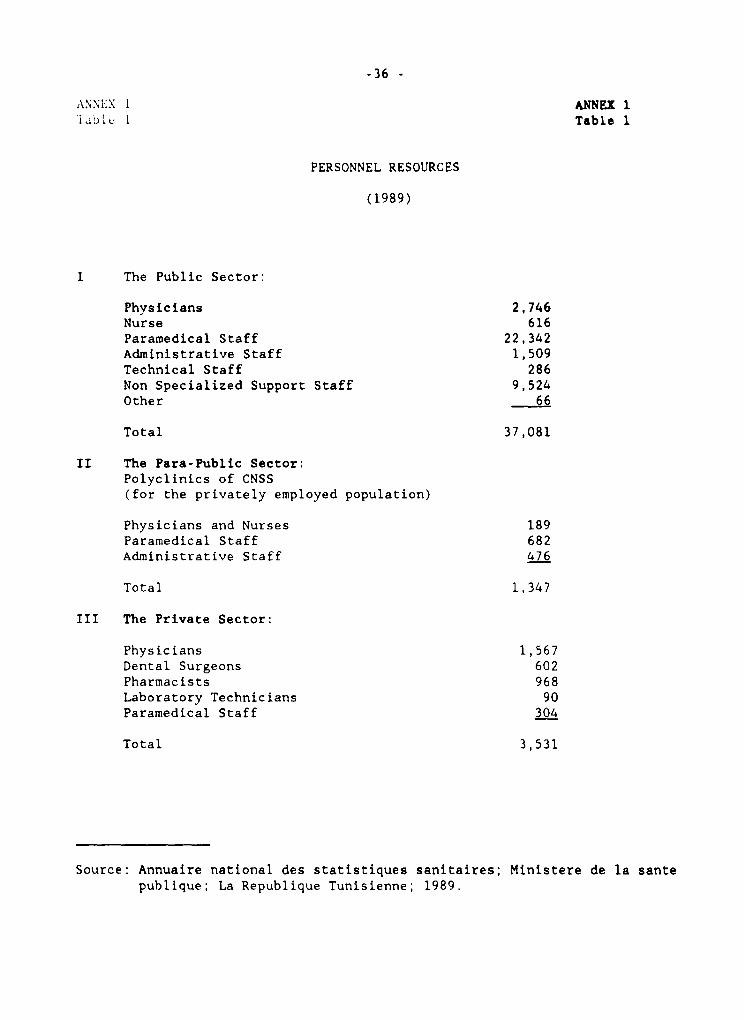
-36 -
A.NNI.X 1 ANNEX 1labl. l Table 1
PERSONNEL RESOURCES
(1989)
I The Public Sector:
Physicians 2,746Nurse 616Paramedical Staff 22,342Administrative Staff 1,509Technical Staff 286Non Specialized Support Staff 9,524Other 66
Total 37,081
II The Para-Public Sector:Polyclinics of CNSS(for the privately employed population)
Physicians and Nurses 189Paramedical Staff 682Administrative Staff 476
Total 1,347
III The Private Sector:
Physicians 1,567Dental Surgeons 602Pharmacists 968Laboratory Technicians 90Paramedical Staff 304
Total 3,531
Source: Annuaire national des statistiques sanitaires; Ministere de la santepublique; La Republique Tunisienne; 1989.
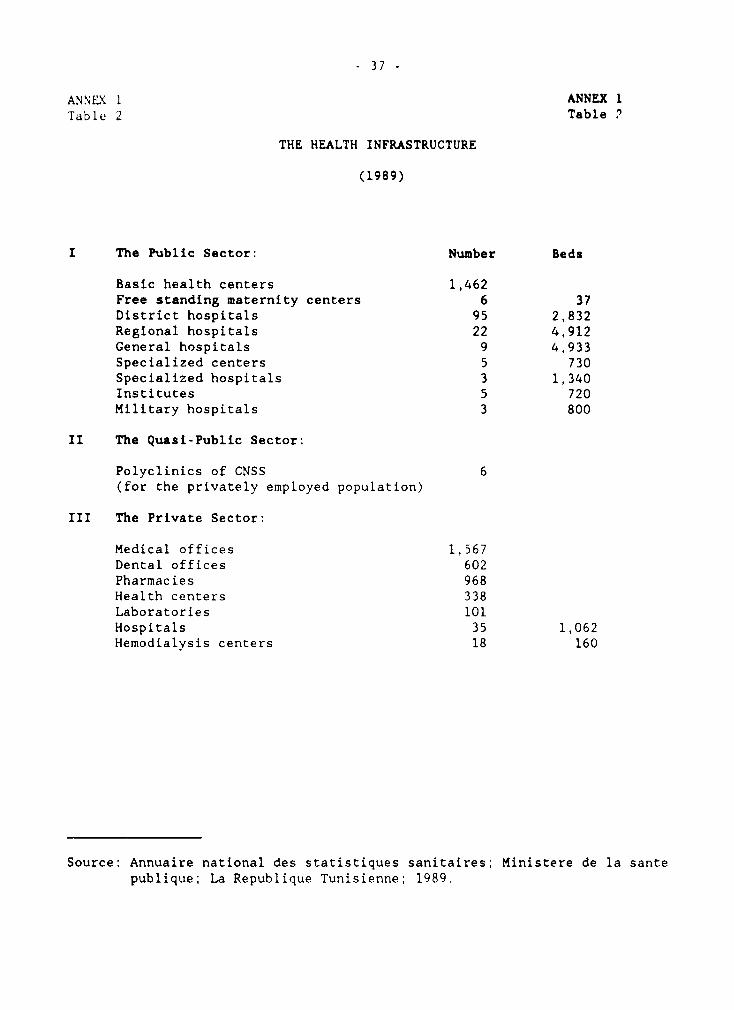
37 -
ANNIE\ 1 ANNEX 1Table 2 Table 2
THE HEALTH INFRASTRUCTURE
(1989)
I The Public Sector: Number Beds
Basic health centers 1,462Free standing maternity centers 6 37District hospitals 95 2,832Regional hospitals 22 4,912General hospitals 9 4,933Specialized centers 5 730Specialized hospitals 3 1,340Institutes 5 720Military hospitals 3 800
II The Quasi-Public Sector:
Polyclinics of CNSS 6(for the privately employed population)
III The Private Sector:
Medical offices 1,567Dental offices 602Pharmacies 968Health centers 338Laboratories 101Hospitals 35 1,062Hemodialysis centers 18 160
Source: Annuaire national des statistiques sanitaires; Ministere de la santepublique; La Republique Tunisienne; 1989.
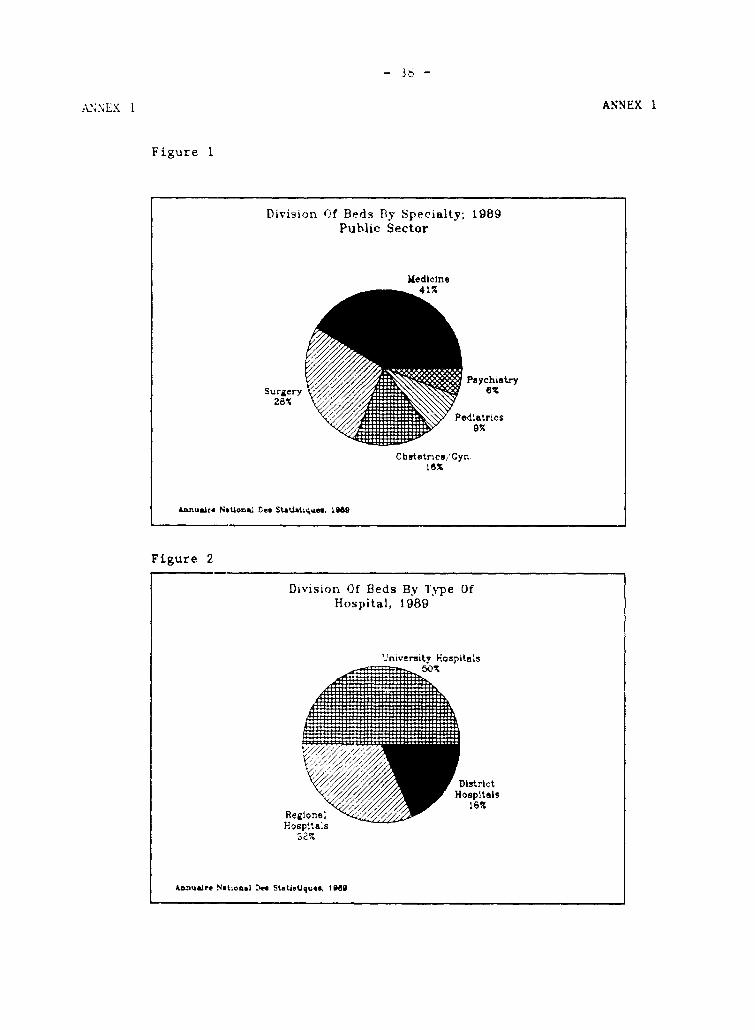
- Th -
ANNEX 1
Figure 1
DLivision Of Beds Bly Specialty; 1989Public Sector
Medicine
Paychiatry
28%
Pelatries%A ~~~~~9%
Cbutetrice/'Gyn.8%
Annuaire N§Uom&l Des StaUiatLc.e. lu9
Figure 2
Divisioin Of Beds By Type OfHospital, 1989
Univemity Hospitfls
Hospitêls
50S~~~~~6
Reglone 18
Annu.aire National Des Statistiques. tuBai
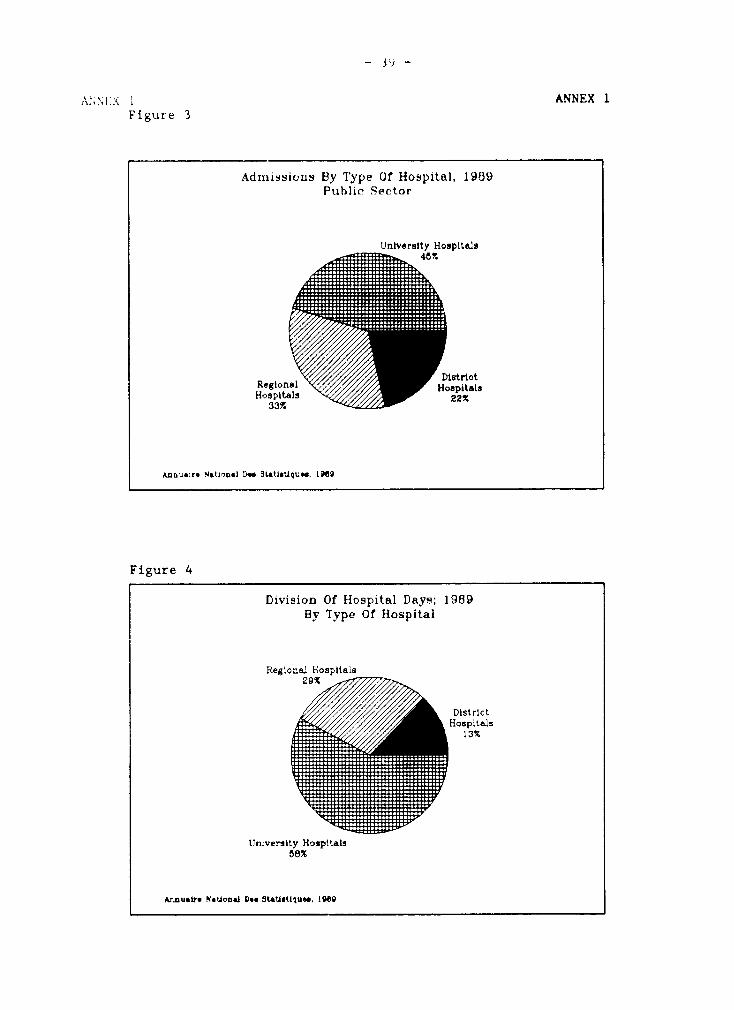
ANNEX 1Figure 3
Admnissioils By lype 0f Hospital. 1989Public Sector
Universlty Hospîtêls
Hospitel Hospitai :408p als ~~~~22%
ese SLaUatAqu«.u I .
Figure 4
Division Of Hospital Days; 1989By Type of Hospital
Regtonali Hospitais
DistrIctHospLteL1s
University Hospitais58%
Arnuao .stue I98.D
- 40 -ANNEX 2 ANNEX 2Page 1 of 8 Page 1 of 8
GOVERNMENT HEALTH FINANCING ORIENTATIONS AND STRATEGY
Avoendix 1: Letter from Minister of Public Health
Translation of FrenchOroinal
Mr. Kemal Dervis Tunis, February 1, 1991Director - North Africa Regional OfficeWorld BankWashington, D.C.
Dear Sir:
Followinq the aide-mémoiru from the Bank and the exchanges ofcorrespondence between the Ministry of Public Health (MOH) and the Bank, I writeto inform you of the principal orientations of the Tunisian Government for futurehealth financing arrangements.
1. The strategy adopted by the Government in implementing its healthpolicy has long been based on the overriding need to expand health services toensure adequate health coverage for the whole country. This has involved theconstruction and equipping of a number of different facilities, training andrecruitment of personnel with qualifications in different areas and at differentlevels, and the allocation, mainly from the Government budget, of operatingfunds.
2. With shifting morbidity trende, changes in socioeconomic and culturalpatterns, and the availability of health professionals qualified in differentareas and at different levels, it became necessary to develop that strategy insuch a way as to ensure greater effectiveness, increased efficiency, andimprovements in terms of impact and quality of the present health system.
3. To achieve those objectives, the public sector had to be assured ofadequate operating resources to enable it to respond to the increasingly pressingneeds of a more and more demanding population and of a growing number ofqualified professionals. The problem of health financing, the subject of severaldifferent studies over recent years, should therefore be addressed in thiscontext.
4. The different sources of financing were identified and theirproportions evaluated and analyzed with a view to possible re-examination ofburden-sharing arrangements and resource allocation.
- 41 -
ANNEX 2 ANNEX 2
Page 2 of 8 Page 2 of 8
4.1 The Government budget remains the principal source of funding tomeet the etrategic needu of the health sector, as well as diseaseprevention, and total or partial financing of curative care.
4.2 The social insurance programu contribute to financing the publichealth sector through contractual lump-sum payments to the NationalTreasury and to certain hospitals, against which their membersreceive free care in the public health facilities.
4.3 Household contributions to public h.alth financing come from twosources: patients who pay their own fees or have them paid by athird party, and co-payments (tickets modérateurs) from personsentitled to partially free health care (indigents and members ofsocial insurance programe).
5. Any health financing reform first requires a re-examination of thedifferent sources' contributions as well as resource management along morerational and more rigorous lines. Accordingly, it was necessary to review:
- the nomenclature of medical acta and the respective fee echedules,applicable in the public, parapublic and private sectors;
- fee schedules for consultations and hospitalization in public healthfacilities, applicable to paying patients;
- the Assistance Médicale Gratuite (AMG) system, with a view tarationalizing its administration in such areas as beneficiaryidentification, allocation procedures, membership fees;
- the percentage of co-payment required for each consultation and eachhospitalization from persons entitled to highly subsidized healthcare;
- operation of the public health facilities, providing them with themeans of assessing their production costs and leading to possibleoperating-cost sharing arrangements among the different sources offinancing.
6. The Government adopted the hospital restructuring support projectthat is to be jointly financed with the World Bank.
This reform essentially targets improvements in service qualitywhile containing costs: evaluation of quality of care, health facilitymanagement audits, and consensus committees. It will also help establish thegeneral crientations for public health financing.
This reform is one of the prerequisites for a sector financingreview, and especially for any new burden-sharing arrangements, since it willprovide a basis for calculating the cost of the health services provided in thepublic facilities and identifying the different categories of beneficiaries.
ANNEX 2 ANNEX 2
Page 3 of 8 Page 3 of 8
Based on the results obtained n the Etablissements Publics de Santé(EPS), the Government will review the various financial burden-sharingalternatives for the public health sector.
7. Without waiting for thoas remultu, the Government has adopted anumber of statutory and regulatory measures designed to increase householdcontributions to public health financing.
7.1 The nomenclature of medical acte was reviced and publi.hed by jointorder of the Minister of Economy and Finance and the Minister ofPublic Health on September 25, 1990.
An interdepartmental commission, based at MOH, is currentlyestablishing the values of the key letters used in the nomenclature to identifymedical acte for purposes of the fee achedule.
This fee schedule will be reviewed periodically to adapt it to thechanging production costs of health care by comparison with those recorded inthe hospital facilities covered by the reform.
7.2 Revised fee schedules for consultations and hospitalization in MOHhospitals and health facilities were issued by joint order of theMinister of Economy and Finance and the Minister of Public Healthon December 13, 1990.
Under the revised fee schedules, the 1990 rates are to be doubledas of November 1, 1991 in a two-step process, the firet step startingJanuary 1, 1991, and the second November 1, 1991. Beyond thosefees, the costs of supplementary examinations auch as X-rays, labtests, and functional and endoscopic explorations, as well as thecosts of surgery, represent additional charges, the rates for whichare set in the nomenclature and current fee schedulei.
7.3 Under the finance law for fiscal 1991, the annual AMG membershipfee has gone up by 66% from TD 6 to TD 10. This annual fee ispayable by holders of AMG Type II carde, preeently numbering 663,000.
7.4 Under the same law, contributions to health care and hospitalizationcos-s in the form of co-payments from beneficiaries of highlysubsidized care who are required to make co-payments were increasedby 33-50% over 1990 rates.
Persons entitled to highly subsidized care and required to makeco-payments are holders of the AMG Type II card and members of thesocial insurance programs.
7.5 Thanks to the revised fee schedules for paying patients and theincrease in co-payments and annua] AMG membership fees, the 1991
ANNEX 2 ANNEX 2
Pa-e 4 of 8 Page 4 of 8
operating budget shows an increase of TD 6 million in self-generatedhospital revenues.
Moreover, thoae measures will help reduce health care consumptionin the univeruity hospitals and eneure better distribution of demandthroughout the entire health and hospital network.
8. With a view to reforming the AMG system, the Government has alreadyasked the National AMG Commission to conduct an analytical and critical studyof the present *yst.m, in place mince 1987. The commission will provide apreliminary appraisal, which will serve as a baais for the indigence programsstudy included in the hospital restructuring project.
In addition, as part of the draft law submittad to the Governmenton organization of the health sector, MOH includes free medical assistance forevery indigent Tunisian citizen, hie spouse, and hie legally dependent children.The list of beneficiaries will be drawn up periodically by mutual agreementbetween MOH and the Ministry of Social Affaira.
The same draft law provides for reduced fee echedules for healthcare and hospitalization for certain categorias of Tunisians, which will beestablished, as will the financing arrangements, by decree. The reduced feeschedules will subsequently be established in the same decree by reference tocosts calculated in accordance with the new management methods.
The establishment of eligibility criteria and procedures for issuingAMG cards will allow for more rational management of the health assistanceprograms for low-income families.
The Government will base the reform of the AMG system on the findingsof the study included in the hospital restructuring project. Measures torationalize this system will subsequently be implemented, in such areas aseligibility criteria, membership procedures and services provided.
9. The social insurance systeme are going to have to play anincreasingly important role in public health financing for various reasons, ofwhich the main ones are their expanding memberships and the riaing coste ofcare.
Thus the contributions from the social inp-.rance systems and theway these are paid to the hospitals will be revi½ed by reference to costcalculations based on the methode introduced in the hospitals through thehospitals management reform.
To that end, the draft law on health organization provides thatcontracts defining modalities for health coverage of social insurance programsbeneficiairies, will link those programs to MOH, acting on behalf of the EPS.
- 44 -
ANNEX 2 ANNEX 2Page S utf 8 Page 5 of 8
A commisoion based at the Ministry of Social Affaire is etudying thedifferent social insurance systema currently in effect, with a view to surveyinqbernefits and member contributions.
This study will serve as a preliminary appraisal for a possibleoverhaul of the social security systeme, particularly with respect to theirhealth insurance component, as set out in the hospital restructuring supportproject.
Laetly, the social insurance programe, besides the annual lump-sumcontribution to the MOH op.rating budget, are linksd to certain hospitale underopecial contracte allowing for reimbursement for epecific procodures on a f.e-for-service basie: cardiovaecular interventions and kidney transplante mince1987 (cost increase in 1991), and CAT scans aince 1990.
Other pathologies or therapeutic or diagnostic techniques may becovered by similar contracte in the near future. Negotiationa to this end arealready in progresa oetween the Minietry of Social Affaire and MOH.
In addition, the social insurance programe will finance the purchaseof hospital equipment as defined by MOH. This program to strengthen publichealth facilities will apan over a 5-year period etarting in 1990, for a minimumannual outlay of TD 10 million. The subprogram for the years 1990-1991 is inexecution, while that for the two-year period 1992-1993 will be prepared duringthe third quarter of 1991.
The above demonstrates the significance of the efforts already made.
Very truly yours,
The hinister of Public Health/a/ Dali Jazi

- 45 -
ANNEX 2 ANNEX 2
Page 6 cf 8 Page 6 cf 8
GOVERNMENT HEALTH FINANCING ORIENTATIONS AND STRATEGY
Aoopendix 2Terms of Reference and Scheduleof Proiect Supoorted Studies
A. Reassessaent of the benefits criteria for fr-- and r-duced-costvouchers, ("indigence program-s).
1. The project would support the Government's effort to review thecurrent programs to better target the benefits provided to the real needy,through the realization of a study that would:
review the current ayateme, "AMG Type I and Type II", givingspecific attention to analyzing the population concerned,their economic conditions and geographical locations;
specify options for reforms of the system to (i) bettertarget free care to the needy; the study would review theselection criteria to be applied and estimate the cost ofmaintaining this category of benefits; and (ii) reduce thenumber of subsidized vouchers (AMG Type II) to the minimumlevel by exploring two main options: a marked increase inthe cost of the annual voucher and improvements incollection of co-payment; or the compulsory integration ofthe largest segment of this population into the Socialinsurance schemes through a lump sum contribution based onestimated revenue (minimal salary for example).
2. This study would be carried out by December 1993, its conclusionsreviewed with the Bank, and its final recommendations included into theproposal for a framework for new financial burden-arrangements to be presentedto the Government by December 31, 1994.
B. Role and contribution of social insurance progra-s.
3. Most of the services provided by the public sector to the socialinsurance programs' beneficiaries are hoepital-based, since out-patient careis provided both by the CNSS own facilities and by the private sector. One ofthe options currently under consideration to move away from the lump sumapproach, would be to projressively shift towards a contribution directlylinked to actual cost incurred. Once a given hospital gains knowledge of itscost and utilization patterns, ite proportional share in the lump sum would be
ANNEX 2 ANNEX 2
Page 7 of 8 Page 7 of 8
cost and utilization patterns, its proportional share in the lump sum would te
deducted and replaced in the following year's allocation, with the actual ccs'
amount. Since the knowledge of actual costs is linked to the actual
implementation of the MIS in hospitals, the social programs' expected increabe
in financial commitment would be progressive.
4. On the basis of the preliminary results provided through theproject, the MOH would develop by December 1993, a methodology to serve as a
basis for new contractual arrangements with the social insurance programs.
This methodology would be integrated to the proposal for a framework for newfinancial burden-arrangements to be presented to the Government by December
31, 1994.
5. It is difficult to assess the level of contribution from employers
and employees to the social insurance programs for health benefits as long as:
(i) the contributions for the various benefit programs (health, pensions) are
not formally separated; and, (ii) in addition to contributing to the main
social programs (CNSS and CNRPS), households as well as employers contribute
on a voluntary basis to a myriad of complementary inhurance systems(assurances-groupe, mutuelles). Initially conceived to provide additional
benefits to ensures, these schemes have developed greatly, resulting in
duplicated benefits and waste of resources.
6. The project would help reconsider the current provision of health
benefits under the different compulsory and voluntary schemes, by supporting a
study that would:
evaluate health benefits under existing social insuranceprograms, namely reviewing, the CNSS and CNRPS as well asother schemes providi job related health care and coverage
of professional risks. The study would assess the current
enrollment rates, and amount and utilization of resourcescollected;
collect information and evaluate the various complementaryschemes, "assurances-groupe, mutuelles"; assess the sources
and amount of financing, and the utilization of resources;
specify options for reforme to (i) increase the enrollmentrates in the social insurance schemes; and, (ii) limitduplication of coverage. Special consideration would begiven to the conditions of enforcement of the law 86-86 of
09/01/1986 organizing the provision of social benefits forthe public and private sec..ors, and to the role that thecomplementary schemes would play.

- 47 -
ANNEX 2 ANNEX 2Page 8 of 8 Page 8 of 8
7. This study would be carried out by December 31, 1993, itsconclusions reviewed with the Bank, and its final recommendations includedinto the proposal for a framework for new financial burden-arrangementu to be
presented to the Government by December 31, 1994.
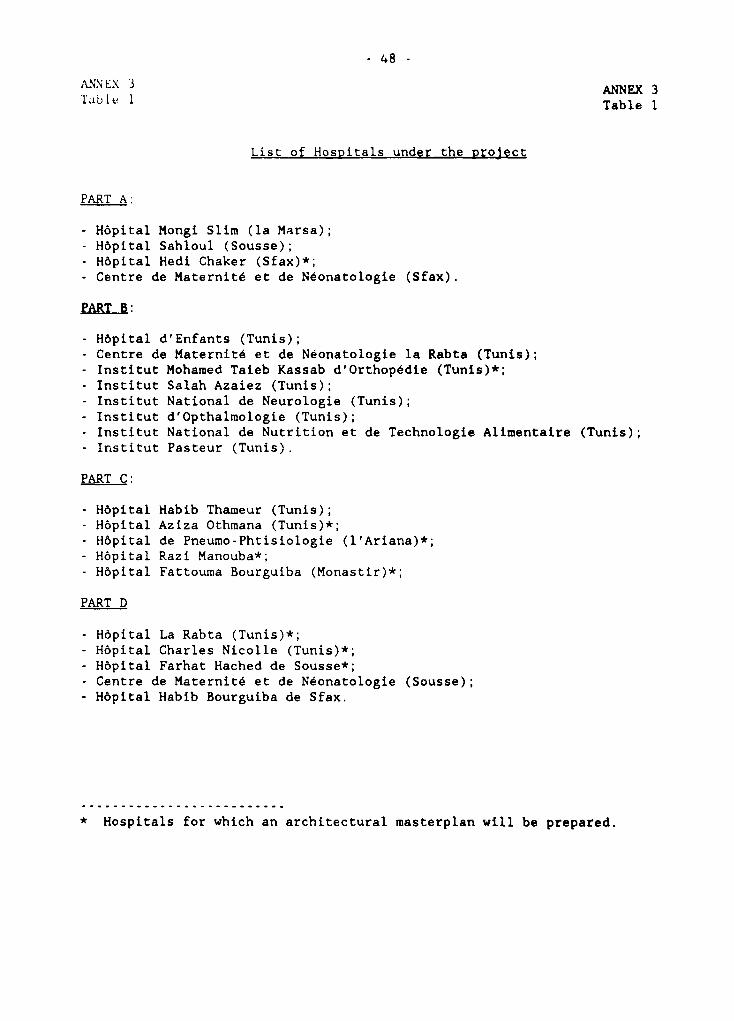
48 -
ANNEX 3 ANNEX 3Table 1 Table 1
List of Hospitals under the project
PART A:
- Hôpital Mongi Slim (la Marsa);- Hôpital Sahloul (Sousse);- Hôpital Hedi Chaker (Sfax)*;- Centre de Maternité et de Néonatologie (Sfax).
PART B:
- Hôpital d'Enfants (Tunis);- Centre de Maternité et de Néonatologie la Rabta (Tunis);- Institut Mohamed Taieb Kassab d'Orthopédie (Tunis)*;- Institut Salah Azaiez (Tunis);- Institut National de Neurologie (Tunis);- Institut d'Opthalmologie (Tunis);- Institut National de Nutrition et de Technologie Alimentaire (Tunis);- Institut Pasteur (Tunis).
PART C:
- Hôpital Habib Thameur (Tunis);- Hôpital Aziza Othmana (Tunis)*;- Hôpital de Pneumo-Phtisiologie (l'Ariana)*;- Hôpital Razi Manouba*;- Hôpital Fattouma Bourguiba (Monastir)*;
PART D
- Hôpital La Rabta (Tunis)*;- Hôpital Charles Nicolle (Tunis)*;- Hôpital Farhat Hached de Sousse*;- Centre de Maternité et de Néonatologie (Sousse);- Hôpital Habib Bourguiba de Sfax.
* Hospitals for which an architectural masterplan will be prepared.
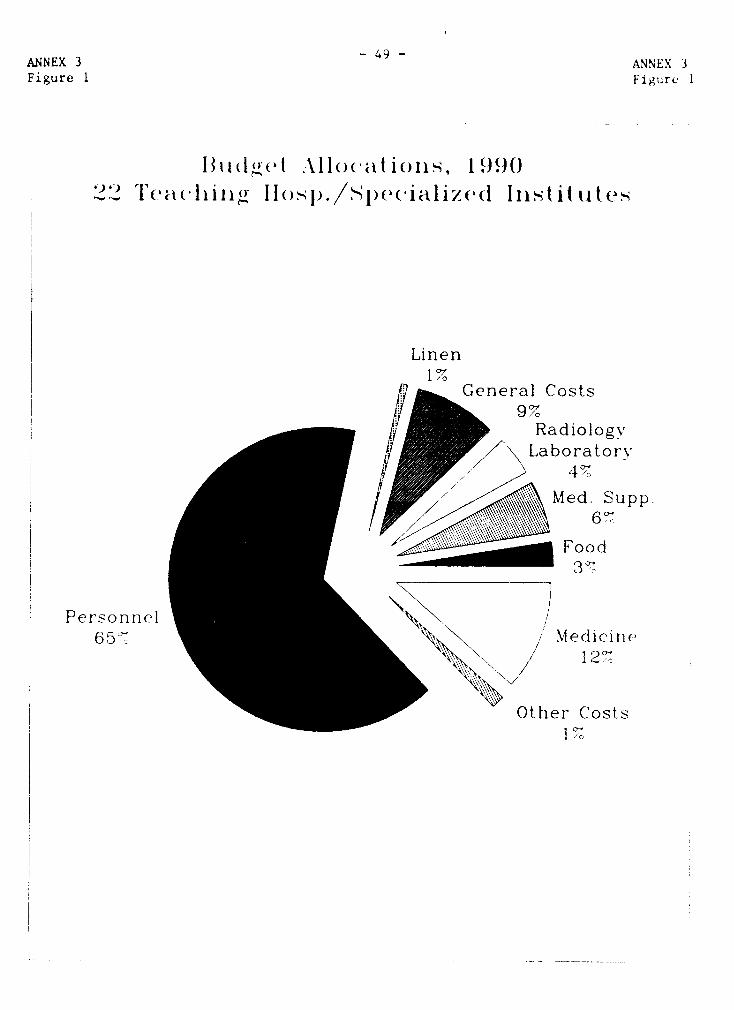
ANNEX 3 - 4 ANNEX 3Figure 1 Figure I
iU(igel .\ 11O(w t ioIls, I 99()l'e<'I (.11il i Io ). 1)e a c e (l g I j. t Aitt
Linen1 ~~~~~~~~~~1%
General Costs9%
RadiologyvLaboratorv
/pMed. Supp.
Foo d
Personnel65`7 Medicine
12'7
Other Costs
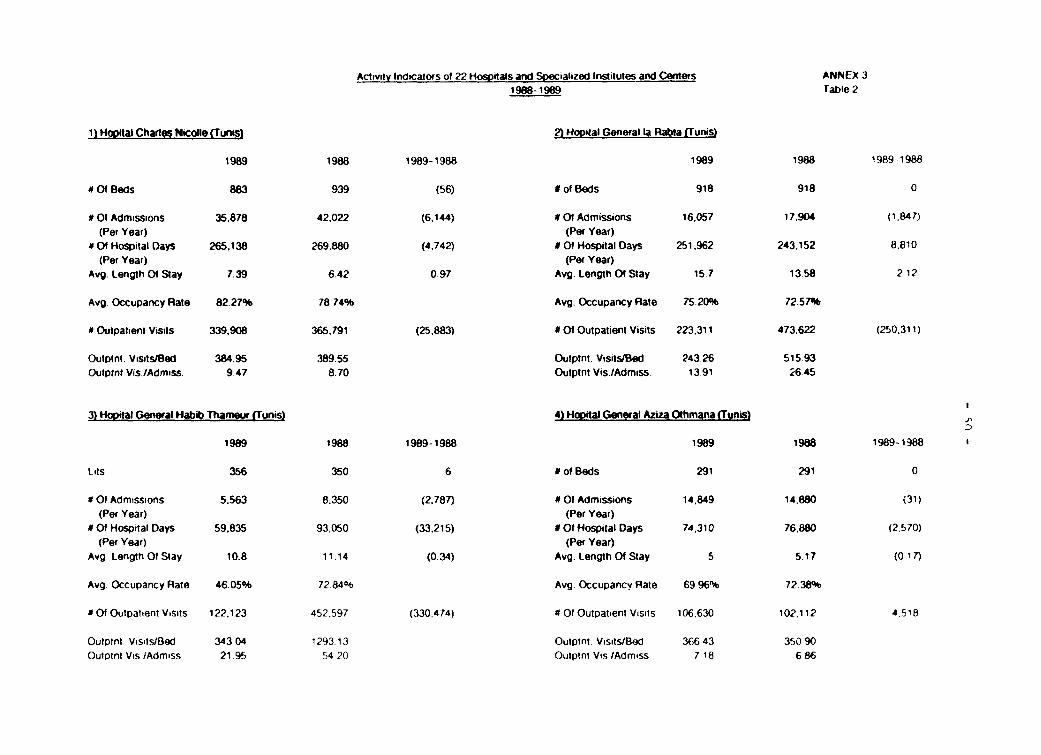
Act,vîty Indicators of 22 Hospitals and Specialized Institutes and Centers ANNEX 319s8-1989 Table 2
1) Hopdtal Charles Nicolle (Tunis) 2) Hopital General la Rabta (Tunis)
1989 1988 1989-1988 1989 1988 1989-1988
# Of Beds 883 939 (56) # of Beds 918 918 0
# Ot Admissions 35.878 42,022 (6,144) # O1 Admissions 16.057 17.904 (1.847)(Per Year) (Per Year)
# Of Hospital Days 265,138 269.880 (4.742) # Of Hospital Days 251.962 243.152 8,810(Per Year) (Per Year)
Avg. LengthOfStay 7.39 642 097 Avg. LengthOfStay 157 1358 212
Avg. Occupancy Rate 82-27% 7 74% Avg. Occupancy Rate 75.20% 72 57%
# Outpalienl Visils 339.908 365,791 (25.883) # Of Outpatient Visits 223.311 473.622 (250.311)
Oulptnt. VisitstBed 384.95 389.55 Outptnt. VisitstBed 243.26 515.93Outptnt Vis /Admiss. 9 47 8.70 Outptnt Vis./Admiss. 13.91 26.45
3) Hopital General Habib Thameur (Tunis) 4) Hopital General Aziza Othmana (Tmmis)
1989 1988 1989-1988 1989 1988 1989-1988
Lnis 356 350 6 # of Beds 291 291 0
#OI Admissions 5.563 8.350 (2.787) MOt Admissions 14,849 14.880 (31)(Per Year) (Per Year)
M O Hospital Days 59.835 93,050 (33,215) MOt Hospital Days 74.310 76880 (2,570)(Per Year) (Per Year)
Avg. Length Of Stay 10.8 11.14 (0.34) Avg. Length Of Stay 5 5.17 (0 17)
Avg Occupancy Rate 46.05% 72.84% Avg. Occupancv Rate 69 96% 72.38%
# Of Oulpatient Vîsits 122.123 452.597 (330.474) M Of Oulpatient Visils 106.630 102.112 4.518
Oulptnt VisilslBed 343 04 1293.13 Oulptnt Visits/Bed 366 43 350 90Outptnt Vis iAdmiss 21 95 54 20 Oulptnt Vos /Admiss 7 18 6 86
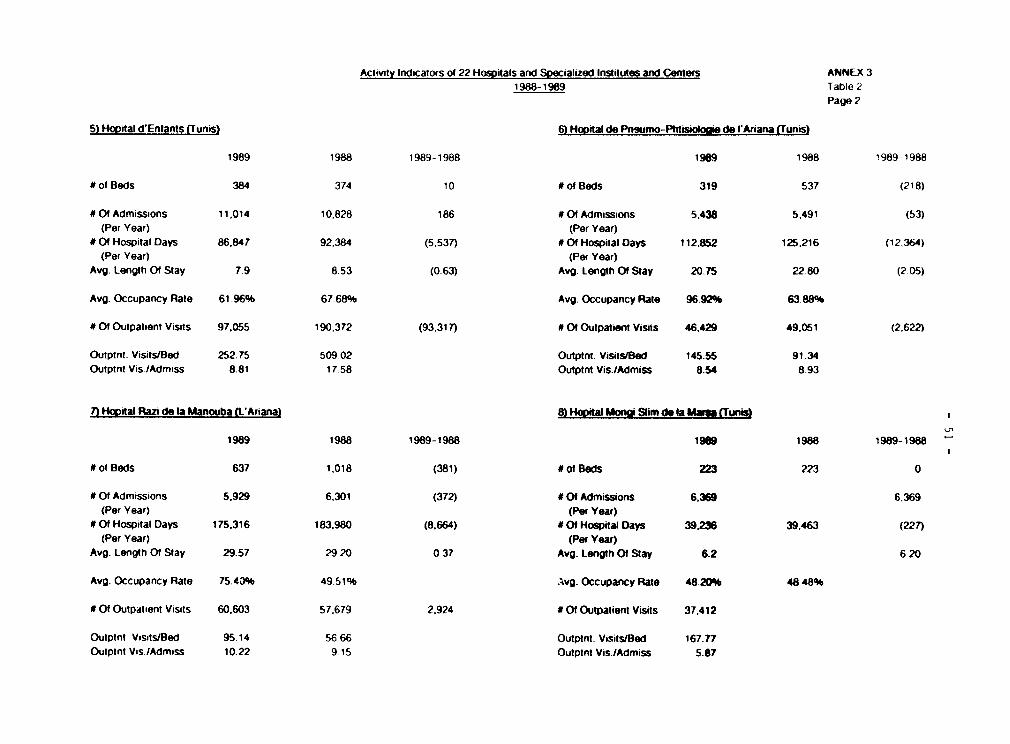
Activity Ind.cators ot 22 Hosvitals and Soecialized Institutes and Centers ANNEX 31988-1989 Table 2
Page 2
5) Hopital d-Enlants (Tunis) 6) Hopital de Pngumo-Phtisioloaie de l'Ariana (Tunis)
1989 1988 1989-1988 1989 1988 1989-1988
NofBeds 384 374 10 0of Beds 319 537 (218)
01 Admissions 11.014 10.828 186 Of Admissions 5.438 5.491 (53)(Per Year) (Per Year)
# Of Hospital Days 86,847 92.384 (5,537) # Of Hospital Days 112.852 125.216 (12.364)(Per Year) (Per Year)
Avg. Length Of Stay 7.9 8.53 (0.63) Avg. Length Of Stay 20.75 22 80 (2 05)
Avg. Occupancy Rate 61.96% 67.68% Avg. Occupancy Rate 96.92% 63 88%
# 0t Outpatient Visits 97.055 190,372 (93.317) # Of Outpatient Visits 46.429 49.051 (2.622)
Outptnt. VisitstBed 252.75 509.02 Outptnt. Visits/Bed 145.55 91.34Outptnt Vis.lAdmiss 8.81 17.58 Outptnt Vis./Admiss 8.54 8.93
7) Hopîtal Razi de la Manouba (L-Ariana) 8) HoDital Nnai Slim de la Maau (Tunis
1989 1988 1989-1988 1909 1988 1989-1988 -
o0f Beds 637 1,018 (381) #ot Beds 223 223 û
# Of Admissions 5.929 6.301 (372) # Of Admissions 6.369 6.369(Pet Year) (Per Year)
#Of Hospital Days 175.316 183.980 (8.664) 40f Hospital Days 39.236 39.463 (227)(Per Year) (Per Year)
Avg. Length Of Stay 29.57 29 20 0.37 Avg. Length Of Stay 6.2 6 20
Avg. Occupancy Rate 75.43% 49 51% .vg. Occupancy Rate 48.20% 48.48%
# Of Outpaîient Vîsîts 60.603 57.679 2.924 # 01 Outpatient Visits 37.412
Outptnt Visits/Bed 95.14 5666 Outpint. VisitsfBed 167.77Outptnt Vis./Admiss 10.22 9.15 Outptnt Vis./Admiss 5.87
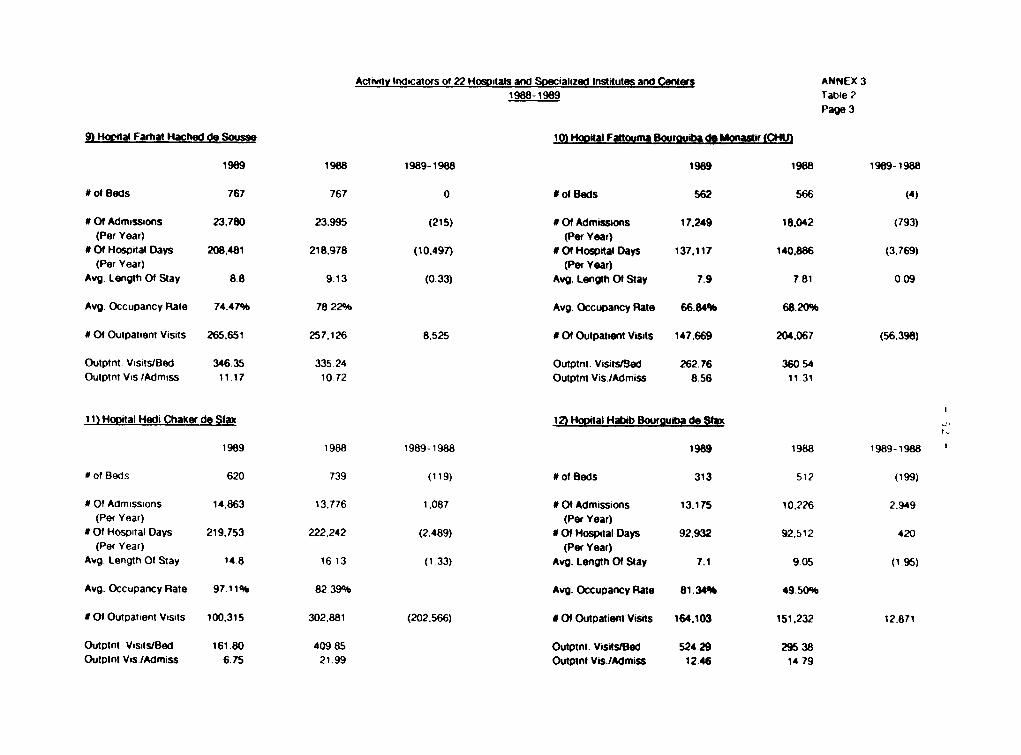
Actuvity Indicators of 22 Hospitals and Soefcialized Institutes and Cent.q ANNEX 3
1988-1989 Table 2Page 3
9) Hocital Farhat Hached de Sousse 10) HoDital Fattouma Bouaruiba de Monalir (CHU)
1989 1988 1989-1988 1989 1988 1989-1988
# of Beds 767 767 0 # of Beds 562 566 (4)
# OQ Admissions 23.780 23.995 (215) # Of Admissions 17.249 18.042 (793)
(Per Year) (Per Year)
# Of Hospital Days 208.481 218.978 (10,497) # 0f Hospital Days 137,117 140.886 (3.769)
(Per Year) (Per Year)
Avg. Length Of Stay 8.8 9.13 (0-33) Avg. Length Of Stay 7.9 7.81 0 09
Avg. Occupancy Rate 74.47% 78 22% Avg. Occupancy Rate 66.84% 68.20%
# Of Ouipatient Visits 265,651 257,126 8,525 # Of Outpationt Visits 147.669 204.067 (56.398)
Outptnt. Visits/Bed 346.35 335 24 Outptnt. Visits/8ed 262.76 360 54
Oulptnt Vis./Admiss 11.17 10 72 Outptnt Vis./Admiss 8.56 11.31
t 1) HoDiital Hedi Chaker de Stax 12) Hopital Habib Bourguiba de Stax
1989 1988 1989-1988 1989 1988 1989-1988
#of Beds 620 739 (119) #of Beds 313 512 (199)
0 f Admissions 14.863 13.776 1.087 #Of Admissions 13.175 10,226 2.949
(Per Year) (Per Year)
SOI Hospital Days 219.753 222,242 (2,489) #S 0 Hospital Days 92,932 92,512 420
(Per Year) (Per Year)
Avg. LengtnOftStay 14.8 1613 (1.33) Avg. LengthOfStay 7.1 9.05 (195)
Avg. Occupancy Rate 97.11% 8239% Avg. Occupancy Rate 81.34% 49.50%
# Of Outpatient Visits 100,315 302,881 (202.566) # Of Outpatient Vîsits 164.103 151,232 12.871
Outptnt VisitslBed 161.80 409.85 Outptnt. Visits/Bed 524.29 295 38
Outpint Vis./Admiss 6.75 21.99 Outpint Vis.JAdmiss 12.46 14,79
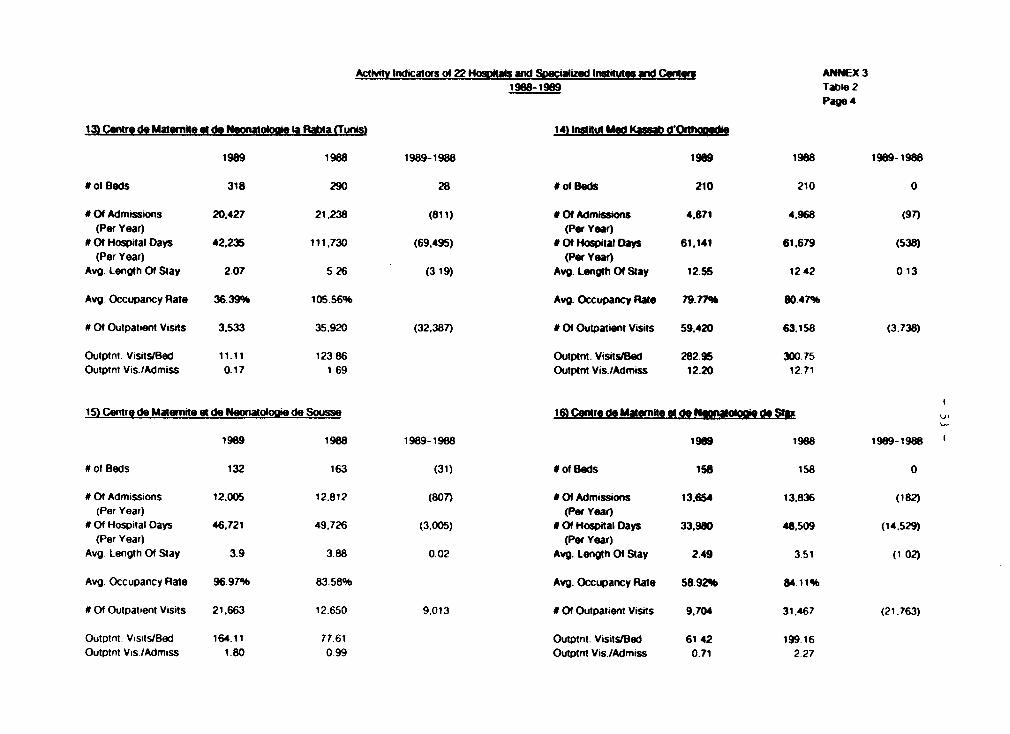
Activitv Indicators of 22 HosDas and Soecialized Insututos and Conl«s ANNEX 31988-1989 Table 2
Page 4
13) Centre de Matrnite et do Nunatolooie la Rat*a (Tunis 14) Instkut Md KasM (I' _
1989 1988 1989-1988 1989 1988 1989- 1988
# ot Beds 318 290 28 # of Beds 210 210 0
* Of Admissions 20,427 21,238 (811) # 0f Admissons 4,871 4.968 (97)(Per Year) (Per Year)Of Hospital Days 42,235 111.730 (69.495) #0f Hospital Days 61.141 61.679 (538)(Per Year) (Per Year)
Avg. Length Of Stay 2.07 5.26 (3-19) Avg. Length Of Stay 1255 12.42 0 13
Avg. Occupancy Rate 36.39% 105.56% Avg- Occupancy Rate 79.77% 80.47%
# 0< Outpatient Visits 3.533 35,920 (32.387) # Of Outpatient Visits 59.420 63.158 (3.738)
Outptnt. Visits/Bed 11.11 12386 Outptnt. Visits/Bed 28295 300.75Oulptnt Vis./Admiss 0.17 1 69 Oulptni Vis.,Admiss 12.20 12.71
15) Centre de Matemite et de Neonatologie de Sousse 16) Centre de Matemite et de NonatokNi» de S11a
1989 1988 1989-1988 1989 1988 1989-1988
#ot Beds 132 163 (31) #do Beds 158 158 0
# Of Admissions 12.005 12.812 (807) # 0 Admissions 13.654 13,836 (182(Per Year) (Per Year)
# Of Hospital Days 46,721 49,726 (3.005) # Of Hospital Days 33.980 48.509 (14.529)(Per Year) (Per Year)
Avg. Length Of Stay 3.9 3.88 0.02 Avg. Length Of Stay 2.49 3.51 (1 02)
Avg. Occupancy Rate 96.97% 83.58% Avg. Occupancy Rate 58.92% 84.11%
# Of Oulpatient Visits 21.663 12.650 9.013 # 0f Outpatient Visits 9.704 31,467 (21.763)
Outpint. Vismts/Bed 164.11 77.61 Outptnt. Visisl8ed 6142 199 16Outpint Vis./Admiss 1.80 0 99 Outptnt Vis./Admiss 0.71 2 27
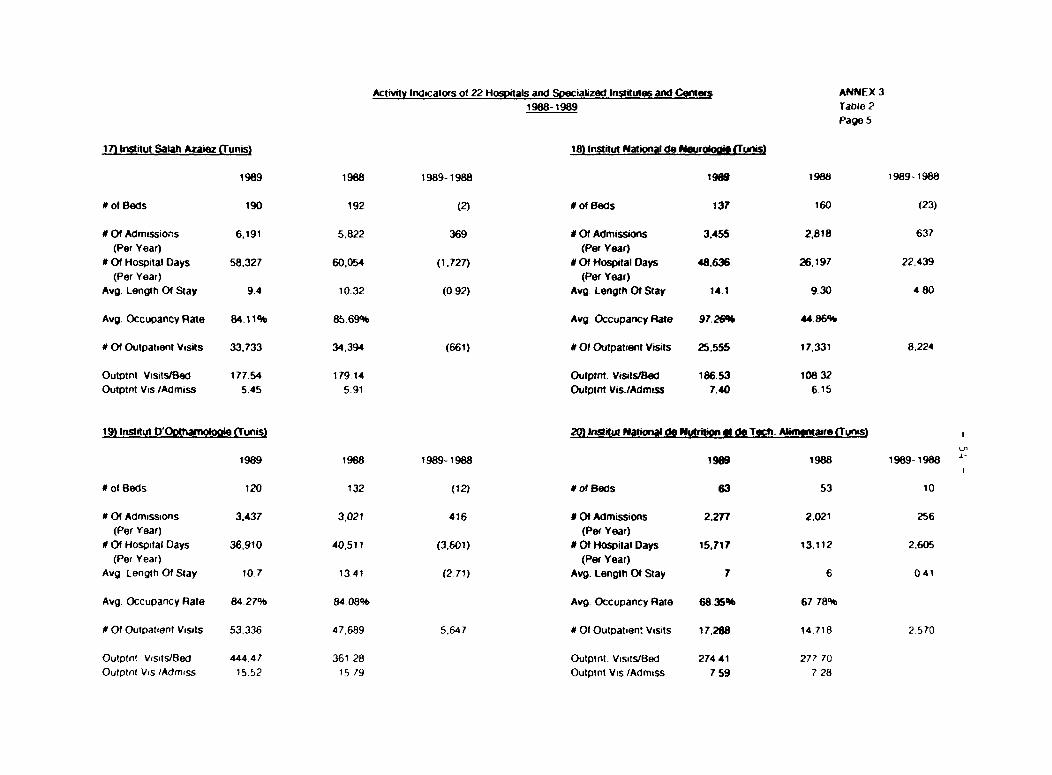
Activity Indicators of 22 Hospitals and SPecialized Institutes and Center ANNEX 31988-1989 Table 2
Page 5
17* Instnut Salah Azaiez QTunis) 18) Institut National de NIuriobd (Tunis)
1989 1988 1989-1988 1989 1988 1989- 1988
4ofBeds 190 192 (2) DofBeds 137 160 (23)
# Of Admissions 6.191 5.822 369 # Of Admissions 3.455 2.818 637(Per Year) (Per Year)* 0f Hospital Days 58.327 60,054 (1.727) 4Of Hospital Days 48636 26,197 22.439(Per Year) (Per Year)Avg. Length 0f Stay 9.4 10.32 (0,92) Avg. Length Of Stay 14.1 9.30 4 80
Avg. Occupancy Rate 84.11% 85.69% Avg- Occupancy Rate 97.26% 44.86%
# 0f Outpatient Visits 33.733 34,394 (661) # Of Outpatient Visits 25.555 17z331 8.224
Outptnt Visits/Bed 177.54 179 14 Outptnt. VisiuIBed 186-53 108 32Outpint Vis./Admiss 5.45 5.91 Outptnt Vis./Admiss 7.40 6.15
19) Institut D'Oothamoloaie «unis) 20) Institut Ntional de Nutrition g dle Toch Amxntaire (Tunis)
1989 1988 1989-1988 1989 1988 1989-1988
of Beds 120 132 (12) DofBeds 63 53 10
#Of Admissions 3.437 3,021 416 # Of Admissions 2.277 2.021 256(Per Year) (Per Year)0 Of Hospital Days 36,910 40,511 (3.601) # Ot Hospital Days 15.717 13.112 2.605(Per Year) (Per Year)
Avg Lengli Of Stay 10.7 13.41 (2.71) Avg. Length Of Stay 7 6 0 41
Avg. Occupancy Rate 84.27% 84 08% Avg. Occupancy Rate 68 35% 67 78%
0 f Oulpattent Vîsîts 53.336 47.689 5.647 #OfOutpatien Vîsils 17.288 14.718 2.570
Outptnt V'sîsà'Bed 444.47 361 28 Outptnt. Vîsits/led 274.41 277 70Outptnt Vis /Admiss 15.52 15 79 Outptnt V,s./AdmiSS 7.59 7 28
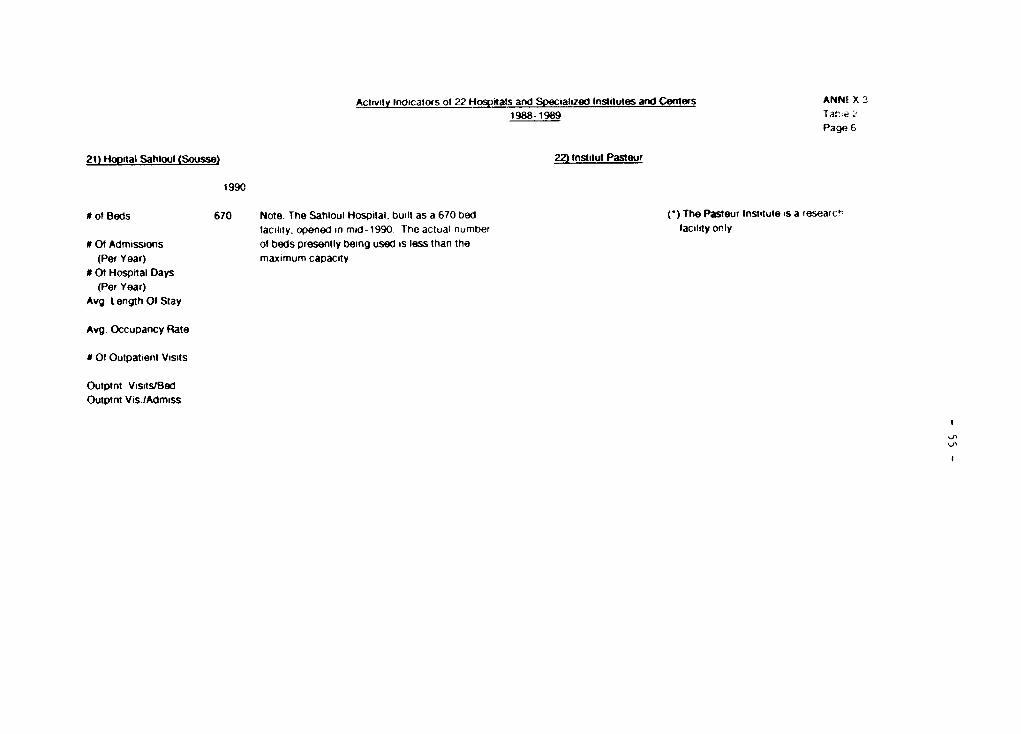
Activty Ind.catoxs of 22 Hospitals and Specialized Institutes and Centers ANNE X 31988-1989 Tab-e 6
Page 6
21) Hopital Sahloul (Sousse) 22) Institut Pasteur
1990
# of Beds 670 Note: The Sahioul Hospital, built as a 670 bed ()The Pasteur Institute ,s a researct'laclty. op,ened in md-1990 Theactual number lacility only
M Of Admissions of beds presently being used is less than the(Per Year) maximum capacity.
# O Hospital Days(Per Year)
Avg. Length 0f Stay
Avg. Occupancy Rate
# Of Outpatient Visits
Outptnt Vîsits/BedOulptnt Vis.IAdmiss
'p
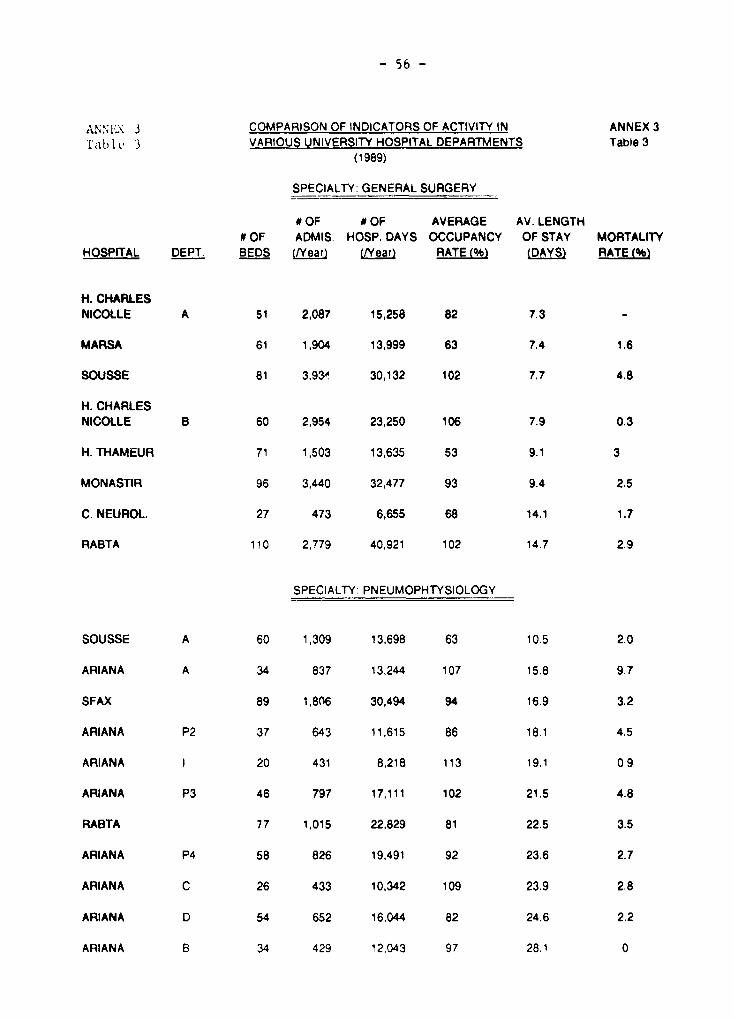
- 56 -
AxN.X : COMPARISON OF INDICATORS OF ACTIVITY IN ANNEX 3lable' 3 VARIOUS UNIVERSITY HOSPITAL DEPARTMENTS Table 3
(1989)
SPECIALTY: GENERAL SURGERY
# OF 0 OF AVERAGE AV. LENGTH# OF ADMIS. HOSP. DAYS OCCUPANCY OF STAY MORTALITY
HOSPITAL DEPT. BEDS (NYear) (Near) RATE (%b (DAYS) RATE (%)
H. CHARLESNICOLLE A 51 2,087 15,258 82 7.3 -
MARSA 61 1,904 13,999 63 7.4 1.6
SOUSSE 81 3,93ô. 30,132 102 7.7 4.8
H. CHARLESNICOLLE B 60 2,954 23,250 106 7.9 0.3
H. THAMEUR 71 1,503 13,635 53 9.1 3
MONASTIR 96 3,440 32,477 93 9.4 2.5
C. NEUROL. 27 473 6,655 68 14.1 1.7
RABTA 110 2,779 40,921 102 14.7 2.9
SPECIALTY: PNEUMOPHTYSIOLOGY
SOUSSE A 60 1,309 13,698 63 10.5 2.0
ARIANA A 34 837 13,244 107 15.8 9.7
SFAX 89 1,806 30,494 94 16.9 3.2
ARIANA P2 37 643 11,615 86 18.1 4.5
ARIANA I 20 431 8,218 113 19.1 0.9
ARIANA P3 46 797 17,111 102 21.5 4.8
RABTA 77 1,015 22,829 81 22.5 3.5
ARIANA P4 58 826 19,491 92 23.6 2.7
ARIANA C 26 433 10,342 109 23.9 2.8
ARIANA D 54 652 16,044 82 24.6 2.2
ARIANA B 34 429 12,043 97 28.1 0
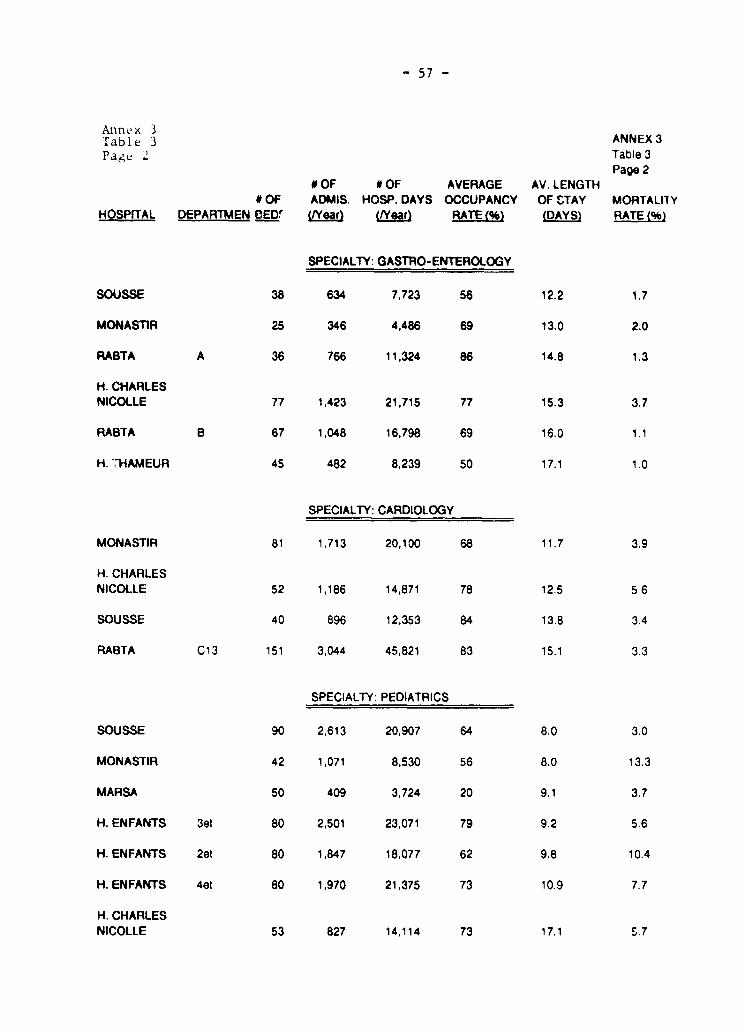
- 57 -
Annex 3Table 3 ANNEX 3
Pag Table 3AV.g ENGTH Page 2
0 OF OF AVERAGE AV. LENGTHO OF ADMIS. HOSP. DAYS OCCUPANCY OF STAY MORTALIlY
HOSPITAL DEPARTMEN EEDr (/Year) (Year) RATE(e% (DAYS RATE(%
SPECIALTY: GASTRO-ENTEROLOGY
SOUSSE 38 634 7,723 56 12.2 1.7
MONASTiR 25 346 4,486 69 13.0 2.0
RABTA A 36 766 11,324 86 14.8 1.3
H. CHARLESNICOLLE 77 1,423 21,715 77 15.3 3.7
RABTA B 67 1,048 16,798 69 16.0 1.1
H. rHAMEUR 45 482 8,239 50 17.1 1.0
SPECIALTY: CARDIOLOGY
MONASTIR 81 1,713 20,100 68 11.7 3.9
H. CHARLESNICOLLE 52 1,186 14,871 78 12.5 5.6
SOUSSE 40 896 12,353 84 13.8 3.4
RABTA C13 151 3,044 45,821 83 15.1 3.3
SPECIALTY: PEDIATRICS
SOUSSE 90 2,613 20,907 64 8.0 3.0
MONASTIR 42 1,071 8,530 56 8.0 13.3
MARSA 50 409 3,724 20 9.1 3.7
H. ENFANTS 3et 80 2,501 23,071 79 9.2 5.6
H. ENFANTS 2et 80 1,847 18,077 62 9.8 10.4
H. ENFANTS 4et 80 1,970 21,375 73 10.9 7.7
H. CHARLESNICOLLE 53 827 14,114 73 17.1 5.7
ANNEX 4 ANNEX 4Page 1 of 7 Page 1 of 7
THE FUTURE LEGAL AND ORGANIZATIONAL STRtUCTUREoF TUNISIAN PUBLIC HOSPITALS
A. OBJECTIVES
1. The objectives sought by the envisagei change in the hoapitals' legal
statue muet form the basis for any decision. There are five essential aime:
(i) Firet, the hospitals need to know their conte by act or by any other
reference unit, and be able to control thes coste. The structuremuet therefore include all the neceusary management tools, especiallyas regards personnel. These elementa muet not be scattered overseveral levels (ministry, region, local). The hoaspital muet be self-managing in order that its managers may have available to them allthe data they need and be able to control th-m.
(ii) It is accordingly essential that the hospital have a strong
management that is assigned precise powers and ie capable offormulating a etrategy for the establishment, obtaining the supportof the medical staff for this strategy, then putting it into effect.It must be able to dialogue with the doctors on an equal footing andto obtain from the different hospital departmente all the data
required for monitoring costa. In the present state of hospitalorganization, it is vital that their management be etrengthened.In practice, this etrengthening will have to be followed byappointment of appropriate individuale to the positions defined.
(iii) Greater flexibility in personnel management, essentially as regardsnon-medical personnel, in order to give hospital management more
freedom of action and to motivate the personnel and increase theirinvolvement in the efficient operation of the hospitals.
(iv) The fourth objective relates to procurement procedures. Thepurchasing of minor items is a long-drawn-out process because ofthe centralization of this purchasing through the ministry. It is
apparent that the real needs of the end users are not wellunderstood; while maintenance, which is in part handled on a
centralized basis, suffers from a lack of efficiency. Increasedflexibility in procurement procedures and decentralization of
equipment management therefore form the fourth objective, to bepursued with a view to heightened efficiency.
(v) Finally, the "situation" of the hospital accountant must beconsidered. Hie position is neither fully "in" the hospital norfully "outeide" it. He is not therefore sufficiently motivated toensure efficient collection of receipte. This situation definitelyneeds to be changed Bo that a more active role can be assigned tothis officer whose function is crucial for the prompt payment ofsuppliers, collection of claims and a balanced cash position for thehospital.
At41NEX 4 ANNEX 4Page .! f 7 Page 2 of 7
2. The profile of the structure to be establiehed should have thefoilowing shape: an autonomous establishment, with a strong management and moreflexible and attractive terme o' employment, acting on the basis of simplifiedadministrative procedurea designed to promote sound, efficient and responsiblemanagement.
B. FACTORS CONSIDERED IN TUE SELECTION OF A LEGAL STATUTE
3. The legal and organizational structure adopted muet be consideredwith the management objectives enumerated above. Existing structure .nodels wereexamined and a comparison made focusing on the functions or organe essential forhospital activity, viz.:
- a deliberative decision-making organ as chief authority;- the director or director general;- supervisory authority;- the consultative bodies;
- the personnel;- procurement and contracte;- accounting;
- control of expenditures.
4. No form of existing organization that has been considered iB entirelyin alignment wi-,! the above objectives. Thus:
5. The present status (EPA = Public Establishment with AdministrativePurpose) of the hospitals is the least appropriate in light of the aima pursued:insufficient management authority assigned to the manager, administrativecommittee with all its members drawn exclusively from the hospital concerned,division of powers among different levels as regards personnel management andprocurement procedures, centralized ministerial management of certain functions,and very wide-ranging supervision over the establishment.
6. The Regional Agricultural Development Commissariats (with adaptedEPA status) are in a better position in that the regional commissioners areassigned full powers in personnel matters (Article 2 of the Decree of June 29,1989) and with regard to conclusion of contracte (Article 14`. Similarly,Articles 12 and 13 of the decree dispense with the requirement if prior approvalby the controller for commitments of less than TD 20,000. However, it muet benoted that the committee assisting the regional cc,.nmissioner han only aconsultative role, which could result in intensifi'.. supervision or inadequatemanagement audit.
7. The experience of Habib Thameur (Etablissement Public à CaractèreIndustriel et Commercial -- EPIC), considered in light of the decree establishingthe hospital, presents some most interesting innovations regarding administrativeorganization, the first of which is unauestionably the fact that this is thefirst time EPIC status has been accorded to a hospital. Tne President and CEOhas authority over all staff (Article 10 zf the Decree of November 17, 1986).By reason of its being classed as an EPIC dccounting is not performed by
- 60 -
ANNEX 4 ANNEX 4Page 3 of 7 Page 3 of 7
an authorizing officer and then by an accountant, theae two functions beingcombined in one individual.
8. On the other hand, Lt ha. to be admitted that this status is notfully in line with what in currently *ought. Apart from the President, theBoard cf Directors is made up exclusively of representatives of the ministries,who are external to the hospital (Article 3 of the same decree). This Board candelegate its powers to the head of the establishment (Article 8). The rulea onfinancial and technical controle are not developed in detail and are veryflexible (Articles 5, 7, 14, 15 and 16), and appear inadequate in the contextof an organization operating very largely with public funda.
9. The general legislation on EPICs would not be fully appropriateeither, since it is insufficiently adapted to hospital activity and theobjectives pursued. For instance, the Director is appointed by the Board(Commercial Code); the accounts are governed by private law while there is aState controller whose powers (Articles 'I5 and 16 of the Law of February 1,1989) remain vague.
C. THE FUTURE LEGAL STRUCTURE
10. Since none of the existing forma of organization is entirelycompatible with hospital activity, the solution in therefore to create a newpublic establishment which, because of its purposes and special features, wouldbe specifically designated a Public Health Establishment ("Etablissement Publicde Santé" - EPS)1/. The essential legal characteristic of public establishmentsis the fact that they can be modeled, by means of the legialation institutingthem, according to the activities pursued.
11. The essential difference between EPA statua, even in the adaptedform, and that of an EPIC, lies in the accounting rules. he personnelregulations can be adjusted, even if the choice is a delicate one. The powersof the head of the establishment are balanced by a decision-making Board andministerial supervision that is lighe but covers the main pointa. When it comesto accounting, however, the traditional rule in public accounting requiringseparation of the roles of authorizing officer and accountant in ignored in anEPIC. The accounts are governed by private law, and are kept and managed in theorganization concerned by employeea *ubject to the authority of the head of theestablishment.
12. In view of the objectives pursued, the EPS structure nhould bedeveloped from the existing legal structures (adapted EPA or EPIC), taking thefollowing points into consideration:
1/ A draft law creating the EPS has been presented to the Goverrnent andits final version will be *ubmitted to Parliament for approval, as acondition of loan effectiveness.

- 61 -
ANNEX 4 ANNEX 4
Page 4 of 7 Page 4 of 7
(i) An EPIC can handle a public health service function withoutdifficulty. The care activity, which is the establishment's purpose,is not contrary to the industrial and commercial capacity, especiallymince in actual tact it is primarily a question of promotingknowledge of coste and equilibrium between receipto and expenditures.
(ii) Tunisian law includes legiolation on EPICo. The personnelregulations, institutions and method of operation of EPICs, and therelevant procurement rules are laid down in broad outline. Tunisiaalso has experience with a hospital establishment set up as an EPIC(Habib Thameur).
(iii) However, the principle of separation as applied in the "adaptedEPAs" represents an additional guarantee for public funds thatgenerally takes the form of a three-phaoe set-up: the authorizingofficer, the head of the establishment, who makes the decisions;the controller, who approves expenditures in advance; the accountant,who is answerable to the Ministry of Finance and personallyresponsible for hie actions, who ef fects the paymento. The principleof separation is also a source of complications, because it dilutesresponsibilities and can slow procedures. Moreover, it presumes,to enable the authorizing officer to have full control of matters,that expenditures are committed at the right moment, that the cashposition is known and that there is a good information systemfunctioning between the office of the accountant and that of theauthorizing officer.
13. Taking all the above objectives and constraints into account, thepublic establishment would be based on the following:
- a Board of Directors and a General Manager that are strong and whoserespective powers dre balanced;
- supervisory authority that is light but covers the essentials;- management support organe that permit both efficiency and control.
D. THE FUTURE ORGANIZATIONAL STRUCTURE
14. The organizational structure is *ummarized in the attached chart(figure 1). The adaptation effort has been focuoing essentially on:
- the Board of Directors;
- the General Manager;
- the supervisory authority;- the health council;- the control organs;- the personnel regulations.
- h 2 -
ANNEX 4 ANNEX 4
Page 5 of 7 Page 5 of 7
(a) The Board of Directors
15. It ie firet of all necessary to institute a mechanism through which
the establishment can be provided with a tronq Board of Directors that ie
capable of enhuring a aood balance between the Director General's oowers and its
own. To this end the Board has to be made up partly of membere f rom outside the
establishment and partly of memberu from within it. The Board musc also be the
place where the financing sources for the hospital (State and Social Security
Fund) are informed about the running of the hospital, are associated with this
management and verify what is done.
16. This Board can be composed pursuant to the legislation creating the
Public Health Establishment as follows: the Director General; one representative
of the Ministry of Planning and Finance; two representatives of the Ministry of
Health with the possibility that one of them can be the Regional Director of
Health; one representative of the Ministry of Education, Higher Education and
Scientific research; one representative of the Ministry of Social Affaire; one
representative of the local authority concerned; the chairman of the Health
Council; one representative of the clinical staff; one representative of the
nonclinical personnel (laborers, administrative personnel, etc.); one
representative of the staff union; and the State Controller.
17. The responsibility of the Board of Directors must be enumerated on
a limitative basis, without possibilitv of deleoation to the General Manager.
The Board muBt deliberate on the hospital's five-year plan, its annual program,
the operating and capital budgets for the year, the apecial regulations governing
the establishment's personnel, if such regulations exist, the hospital's bylaws,
procurement, sale and exchange of real estate, the .eases of more than 18 yaers,
borrowing, and acceptance or rejection of donations and legacies entailing
charges.
18. The Board appoints the members of the control bodies: bid opening
and evaluation committee, internal contract committee (this area is not part of
the General Manager's role). It muet mandatorily draw up inventories, balance
sheets, and the administrative and profit and lose accounts within a short period
to be specified. It is required to approve the largest contracte, within the
framework of a detailed liet. It is to meet at frequent and regular intervals.
(b) The General Manager
19. Aioointed by decree (and not designated by the Board of Directors
from among its members), the General Manager muet be assigned strong power,
balanced by the powers held by the Board of Directors. He muet primarily have
all powers and exercise all authority over the personnel (recruitment,
assignment, promotions, careers, discipline, reassignment within the hospital,
pay, etc.) and allocate funding among the departments with the agreement of the
Board of Directors.
20. It muet be possible for him to be supported by directorB and
administrative services that will enable him to handla, in addition to the day-
to-day management of the establishment, the preparation of the five-year plan
- 63 -
A>;:E< 4 ANNEX 4
Pa-je 6 of 7 Page 6 of 7
of action, the hospital'e annual program and the budget. Depending on the sizeof the establishment, there may also be a Deputy General Manager.
21. He will execute the Board's resolutions, award contracte andrepresent the establishment at law. He will be charged with supervision ofaccounting and will be responsible for the accounte being properly kept. Hemay not combine his position with any other. Ti facilitate the hospital'soperation, he muet be empowered to handle all mattere not *pecifically reservedfor the Board of Directors. Finally, the General Manager be dismissed at anytime by the Government.
(c) Suvervisorv authoritv
22. The role of the oupervisory authorities, i.e., the Ministry ofFinance and the Ministry of Health, will be limited to certain specific matters.They will be required to approve the five-year plan, the annual budget based onan annual program, and staffing levels.
23. The supervisory authorities muet authorize heavy equipment purchases,including major data-processing systems, and also the creation or closing ofbeds. The latter two functions are designed to permit observance of the NationalHospital Plan (that would result from the hospital medium-term ntrategic plan)which is an integral part of the National Health Plan.
(d) The Bealth Council
24. This council will be made up of all the establishment's departmentheads and will elect its chairman from among ite members. It muet also includerepresentatives of other professional categories, medical and clinical, in thehuspital. Ite consultative responsibilities will relate to the five-year plan,the annual program and the budget. It will express its opinion on theorganization of the services and the medical choices connected with executionof the budget. It is desirable that it should also be made responsible forevaluation of the hospital'e structures and medical activities. The DirectorGeneral will be a member of the council.
(e) Control Organe
25. These will comprise the State controller, the technical controller,the bid opening and evaluation committee, and the internal contracta committee.TO these must be added the outside audits prescribed by the Basic Law on EPIC.(Article 13). The composition of the bodies involved muet be precieelyspecified. The Board of Directors will name the members of these essentialbodies. The roles of the different organs are already well defined by therelevant legislation. It will probably be advisable to carefully *pell out therole of the State Controller, which is as yet unclear in the absence ofimplementing decrees.
- 6. -
ANNEX 4 ANNEX 4
Paye 7 of 7 Page 7 of 7
(f) Personnel Regulations
New personnel could be hired on the basie of regulations *pecific
j t PrE'S, comprising general rules laid down in the pertinent legielation,
while the specific rules can be spelled out either by means of regulations for
the purpose or else by specific decisions of *ach establishment, in order to
ensure that the Regulations are compatible with the ipecial feature. of hospital
activity and to avoid rigid rules through the practice of variable working houre,
part-time work, different wage and salary matrixes, adapted advancement or
promotion schemes, and special overtime arrangements. Recruitment of staff for
highly specialized functions, who will definitely b. neded to raie the qualityand efficiency of management of the establishments, will then be possible without
difficulty: financial experts, computer specialiete, biomedical engineere,
communications specialist, etc.
27. Introduction of even greater flexibility would make it possible for
detached public service personnel to opt for integration into the EPS and to
benefit from its special status. This would provide motivation for staff most
interested in finding work of a different sort.
28. A choice has to be made among these different options, while bearing
in mind that if the form of organization remains unchanged it will be difficult
if not impossible to change working methods. On this basis, a form allowing the
most adaptations should be adopted. Specific rules for today's hospital
functions are needed. The second solution proposed, i.e., the possibility for
the EPS to recruit its new personnel directly in accordance with ite neede, would
be the most appropriate. In particular, special emphasis muet be placed on the
special requirements to be met by the management teamn. The high level of
expertise that its members muet possess means that specialties moat certainly
located outside the sphere of the Ministry of Health and possibly the entire
public service will have to be recruited.
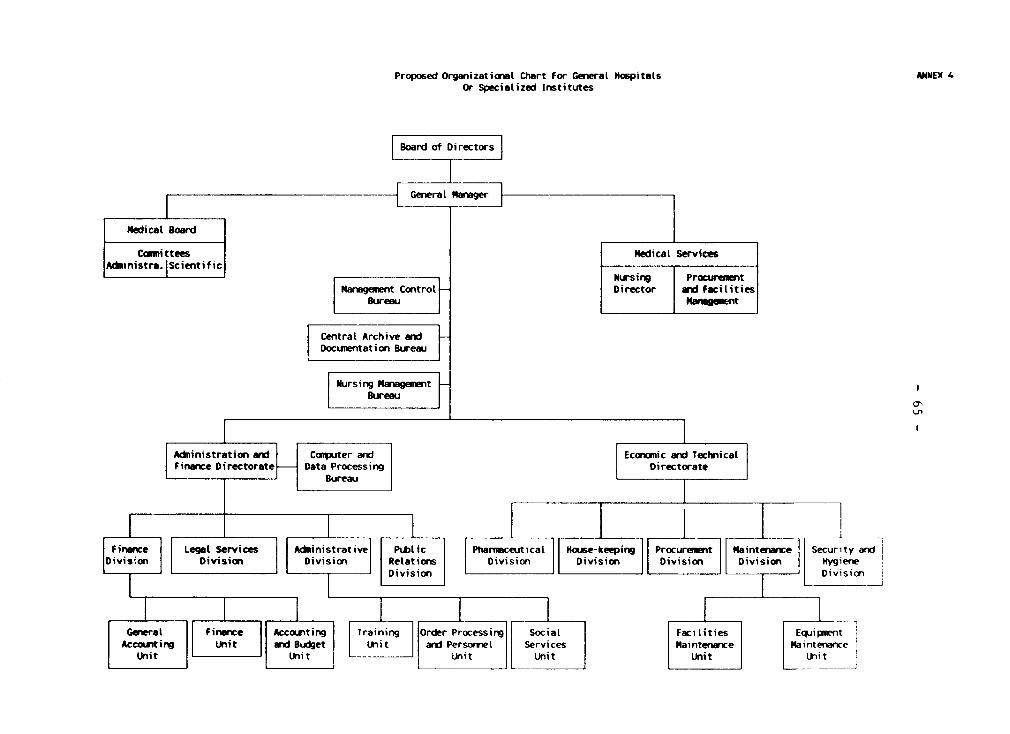
Proposed Organizational Chart For Generat Hospitats ANiEX 4Or Specialized Institutes
|Board of Directors
|Generat Mlarager|
itedicat Board
Comlittees medicat ServicesAdbmnistra. [Scientific Nrig Pouem
NEursin n9 Prac'NtentManagemnent Controt _ Director and facilities
Bureau M nt
|Central Archive end !Docunentation Bureau
| ursing Management Bureau 0 o
Adninistration and Coerputer ard | Econrxnic and TechnicalFinance Directorate Data Processing Di rectorate
Bureau l
| Finance | | Legat Services Atinistrative PtDt ic Ptarimceuticat House-keeping Proureunent Maintenance Security andi|Division | | Division Division Retations Division Division ivision Division Lgene
Genera F Training Order Processing Socia- Fa es EquipoentAccountiru U n Buet Unit and Personmt Services Mainte nnce Maintenance
Unit Unitt ULni t
- 66 -
ANNEX 5 ANNEX 5Page 1 of 8 Page 1 of 8
HOSPITAL RESTRUCTURINO SUPPORT PROJECT
MIS COMPONENT
1. "Information technology i. a management tool that can be usedoperationally, tactically and strategically." Computerization therefore assumesthe prior existence of management procedures, rules and practices that arerecognized and implemented consistently throughout the entity.
A. INSTITUTioNAL CONSEST
2. Two basic approaches, one centralized and the other decentralized,were considered in the selection of the computer 3ystem. The scope of thechanges envisaged under Tunisia's overall hospital reform project is such thatoversight mechanisms muet be established at a very high decisionmaking level --ministerial -- in order to ensure uniformity in the application of computerprocedures, as well as rigor in compliance with the rules governing theimplementation of information technology in the hospital network.
3. Moreover, the historical lack of recognized management practicesand experience in management information techniques, the need to formulate andimplement sound policies, rules, standards and consistent procedures, and theneed to select/develop customized systems to contain the upward spiral of costshave led to a decision to establish a strong computerized information structureat the ministerial level.
4. The National Center for Computers and Health (Centre Nationald'Informatique Sanitaire -- CNIS) is therefore to be established. Its role andmain activities would be (i) standardization of the information technologyfunction" in the health network and (ii) the provision of computer services tohospitals. The main activities carried out by the CNIS would include but notbe limited to:
(a) Administrative orcanization of the health computer svstem:
- policies
- rules- standards- communication and
(b) Technical orcanization of the health computer sostem:
- selection of technology- selection of equipment
- preparation and management of invitations to bid- selection and introduction of development methodologies- structure of information systema and other types of system
engineering- high-level technical support
- 67 -
ANNEX 5 ANNEX 5
Page 2 of 8 Page 2 of 8
formulation of computerization prioritieB (hospitals, regionalcenters and health ministry)formulation of system criteria
techniques (hardware and telecommunications>application (information system)
(c) User traininQ:
- in the use of equipment- in the une of computer procedures and systeme.
B. NATIONAL DEPLOYKENT oF THE IXFORMATION TECENOLOGY FUNCTION
5. The CNIS would provide uniformity in the computerization of the
hospitale and would foster *tructured and planned deployment adapted both to
the capacity for absorption and assimilation of the new function by the
hospitale, as well as to the Center's support capacity.
6. The CNIS' role. An objective, clear and permanent linkage muet be
established between the CNIS and usera at all levels, who are its beneficiaries.An information technology commission consisting of representatives from the
Center and the user sectors involved in the computerization projecte would
therefore be established to ensure the best possible fit between user needs andthe services offered by the CNIS. It should also improve coordination of the
implementation and development of information systeme and contribute to the
development of medium- and long-term planning of the information technologyfunction in the health sector.
7. Oraanization of the CNIS. The Center's legal statua would be thatof an EPIC, which is the optimal way to give it the financial and management
autonomy needed to carry out its reform objectives and to offer the hospitalsthe services best adapted to their needs.
8. In order to respond to the needs of the hospitals, CNIS personnelwould consist of 5 bac+6, 24 bac+4 and 40 bac+2. To the extent that the
employment market permits, recruitment will seek a good balance between academictraining and pertinent professional experience.
9. Rate of return and the information technoloav comDonent. In orderfor the information technology tool to fully meet the needs and objectives of
the hospital reforme, a series of appropriate indicators for the various phases
and levels of computerization will be developed by the CNIS to show the impact
of the information technology component, in particular:
- study of coste, benefits and rate of return of the applicationsdeveloped;
- analysis of the development of information technology and its impact
on the management of health establishments.
- 68 -
ANNEX 5 ANNEX 5Page 3 of 8 Page 3 of 8
C. APPLICATION ARCHITECTURE
10. SuoDort for computer avctemo in aimed *orentially at alladministrative aspects, with the exception of the medical record. In point offact, a management information system for patient clinical records in now uuedby the medical community and *hould be extended to all hospitalo. This *ystemcould be used au a basis for the establishment of clinical data filea that couldbe compiled electronically when computerized management of the clinical recordsis further developed.
11. The systems now available for personnel management and payroll, aswell as supplies and management of pharmacy inventories, will continue to beused initially. The data that they contain in fact have a definite value thatcould be capitalized on and which muat not be underestimated when a newadministrative management model is introduced.
12. Needs. The information technology function will be geared towardsupport for the basic administrative functions. The application archltecturecorresponding to those needs will involve:
(a) Personnel manacement
(b) Management of supplies and inventories(replacement of the CNI's SAMAH system)
(c) Management of the oatient'u adminiotrative recordSelection of an information system with the fo!lowingcharacteristics:- single administrative identification number for each patient- admission functions such as:
sociological data on the patienthospitalization; pre-admission; admissionbed managementcollection of chargesdischarges and tranefers.
(d) Inouttino of data on treatment received by the patient:- medication provided- laboratory and radiological tests for diagnostic purposes- medical and surgical records- diagnoses
(e) Billino for services receivedLink between the administrative data on the patient and data on thetreatment received
(f) General accounting and financial control(i) selection of a computer system meeting the needs of the
financial management model selected for the reforms
- h9 -
ANNEX 5 ANNEX 5Page 4 of 8 Page 4 of 8
(ii) establishment and development of pertinent interfaces betweenthe eystem and other management information systems.
13. Acquisition versus development. Given the magnitude of theinvestments required and the planned timetable, it was decided to adapt existingsystems with a minimum of adjustments to Tunisia's needs.
14. Teot and simulation environment. An information technologylaboratory, to be used for tests and simulations on the possible solutionsoffered by the market, *hould be opened as soon as possible at the ministrylevel, even before the CNIS is established. In addition to tests and simulationsof eysteme, the laboratory could acquire an initial base of expertise on thetechnical environment recommended in the section on "technical architecture."The selection of a physical site that could accommodate the equipment packageselected for a specialized institute, as well as its acquisition andinstallation, should be taken care of in the very short run. Ministry systemspersonnel would then be able to become familiar with the technical componentscf the system (hardware and software) and be exposed to the various problems andtechnological obstacles that they will have to overcome when doing tests toselect the appropriate software. The devalopment of technical expertise is inour view key to the success of the computerization project.
D. TECHNICAL ARCHITECTURE
15. Selection of a comouter manufacturer. The Ministry should ensurethat a single technological environment is selected for all of the hospitals,and used as well at the regional level and for the CNIS. The manufacturer shouldbe an internationally recognized company.
16. Choice of eauioment. Several equipment options for the hospitals,regional centers and CNIS have been considered: central processing unit withterminals; central processing unit with microcomputers linked to terminals; andmicrocomputer network with a server.
17. The option selected was that of a state-of-the-art microcomputernetwork that can grow with neede. The financial investment is directlyproportional to the level of computerization to be reached. The network permitsreal-time interaction with the databases located in the server, which alsomanages communications. Processing is done at work stations that have theapplication and other programe such as spreadsheets and word processors,additional computerization benefits of the various departments of the hospital.
18. Choice of software. This involves:
(a) Svstem software: In view of the architecture of the network system,each workstation will need to have its own operating system. So asto contain costs and minimize training needs, a standard operatingsoftware system already known by the system specialists and usershas been selected.
- 70 -
ANNEX 5 ANNEX 5Page 5 of 8 Page 5 of 8
(b) Network management software: Software with a very good reputationin industry that has become the leader in this type of product ehouldbe selected.
(c) Database manaaement software: There are several pou.ibilities.The evaluation of Ministry system *p.cialists on this matter shouldcertainly be taken into consideration. Selection will reflect inparticular the applications that will be used in the establihments,costa associated with utilization and the large volume of informationto be processed.
(d) Selection of development lanouace:s This will be dictated by theselection of the database which ie generally ausociated with afourth-generation languacr. Another language, language "C," willhave to be learned by ' NIS system upecialist., mince it is neededfor the development of more complex functions. This training willessentially involve the system specialistu.
(e) Aiplication software: CNIS officials will evaluate on a prioritybasis the use of software already developed abroad.
E. ACTIVITIES REQUIRED PRIOR TO TES INTRODUCTION OF TEE SYSTEM
19. The objective for hospital information technology is the developmentover the next five years of a system that can meet the basic needs of the 22hospitals affected by the reforme. Initially, the system to be implemented inthe hospitals will manage patient administrative records, which will over thelonger run permit computerization of patient medical records. The system willenable the hospitals to pursue the following objectives.
20. Meraing of the vatient administrative and medical records: adoptionof a sinale medical record number for each patient. This single identificationnumber will be assigned for both out-patient consultations and hospitalizations.The merging of the records does not exclude remote registration for hospitalswith a decentralized structure. The record will still be treated as a singleentity in the data bank.
This approach allows for a smoother transition and is more likelyto succeed since it does not throw established procedures into question. Itwould also be very difficult to devise a centralized registration system forhospitals that treat more than 900 patients a day (difficulty of having onewaiting room and still protecting the well-being of patients and their families).The patient's physical record (paper record) will have to bear the singleidentification number. A centralized record would make it easier for managersto identify their clientele and facilitate more rigorous follow-up for thepatients. This system could reduce costs by eliminating duplicate testingbecause the contents of the medical record are unknown (i.e. radiology,exploratory procedures).
A'.';r`X C> ANNEX S
J' f Pa?e 6 Cf 8
* . ()eu al, data to streaimline the orerations of the hospitals and
! 2'.' i r:'e.r ed . The admnLnistrators would have an accurate profile of tKh:
; jentele Ln termiis of both numbers and diagnoses so that the operat Lo8u
:; t': various hospitals can be compared and any necessary corrective measures
ti,.n;. Moreover, the entering of medical procedures billable when the patient
is dLscharged would allow for better tracking of accounts payable. In order tc>
re ai,Ie to respond to this need for streamlining, each hospital must:
(a) Centralize the inputting of hospitalisation data:
-pecify information needed when a oatient is hospitalized;- specify standard input terminology, e.o. medical specialties,
names of physicians, diagnosi9;- establish a single identification number for beds at the
hospital center and information that needs to be recorded tofacilitate bed management, e.g. ward, apecialty, type of room,etc.;
- determine procedures for inter-departmental communicationsregarding changes occurringduring hospitalization, e.g. changein bed, specialty, ph-sician, acute case to chronic case,departure or death, etc.;determine what medical procedures are billable when the patient
is di-charged and have to be checked on a routing slip while
the patient is being treated;
- information control. This involves verification that all in-
patients and their locations are correctly recorded. Each
department must therefore on a daily basis at a given time
during the day verify that its patient list is up to date and
notify the hospital admission office of any corrections to be
made immediately.
(b) Determine the data needed by managers regarding clinical or emergencyconsultations.
A system responding to these needs will be introduced in the 22
hospitals over the next five years.

F . * IMITA81 F
PERIOD S 5 T A G E S IA C T IO 1 S AU D C ONU E MT S
_ I __ __ __ ______ ____________ _ ____ __ _ __
STAGE lo. 1
Mtnth 1 Estatlishment of CNIS I - 11 employees: 2 methods and procedures analystsof the reform and recruitment 7 developers
of information technology 2 software specialistsstaff
Months l to 3 Identification of a syste. - Market scudy and selection of appropriate softwareof the reform responding to the needs - Acquisition of know-how required for its use: prograamming, network software
of tunisian hospitats j - Determination of specific needs of hospitals with regard to the sofrware selected- Invitation to bid and technicat tests on different systees and equipnent to ensure system pe-'cn.ince and
comptability wth software and apptications used and to establish standards for tunisia.et établir des standards pour la Tunisie.
Mcnth 4 to 7 Adaptation of the syste i - Alternative 1: Engage a foreign software speciatist to make the necessary changes and train CNIS staffof the reform to Tunisian hospital needs ! (Contract duration: 2 onths)
- Alternative 2: Send 2 CNIS staff abroad to make the necessary modifications under the supervision cf asottware specialist (diration of intership broad: 4 enths)
(urlation of sciatist support 2 oenths)
4 Minor changes will be made to the software to adapt it to the specific needs of the hospitals (inc.uding(the printîng of forms, labels for patient records, identification cards, routiing sltips, receîpts,
I control slips, special Lists, etc, and inputing of discharge data for bilLing.
STACE Mo. 2 The Ophthatlology Institute is b cin coidered to be the pitot hospital ouing toits preoi-ity to the CUIs _d its ti-ited mdr of services ad activities.
Mois 1 Prerequisite for the New administration in placede la reforme pilot hospital
Mois 3 Appointment of a project chief for the hospital wfho is tikely to be a hospital ackn,instra:o,de la réforme extremely familiar with existing procedures and human resources. Ne will be assiste0 by two Cb:S staff
specialists in organization and methods and a support technician.Il devra egalement contrôler la réalisation des objectifs.
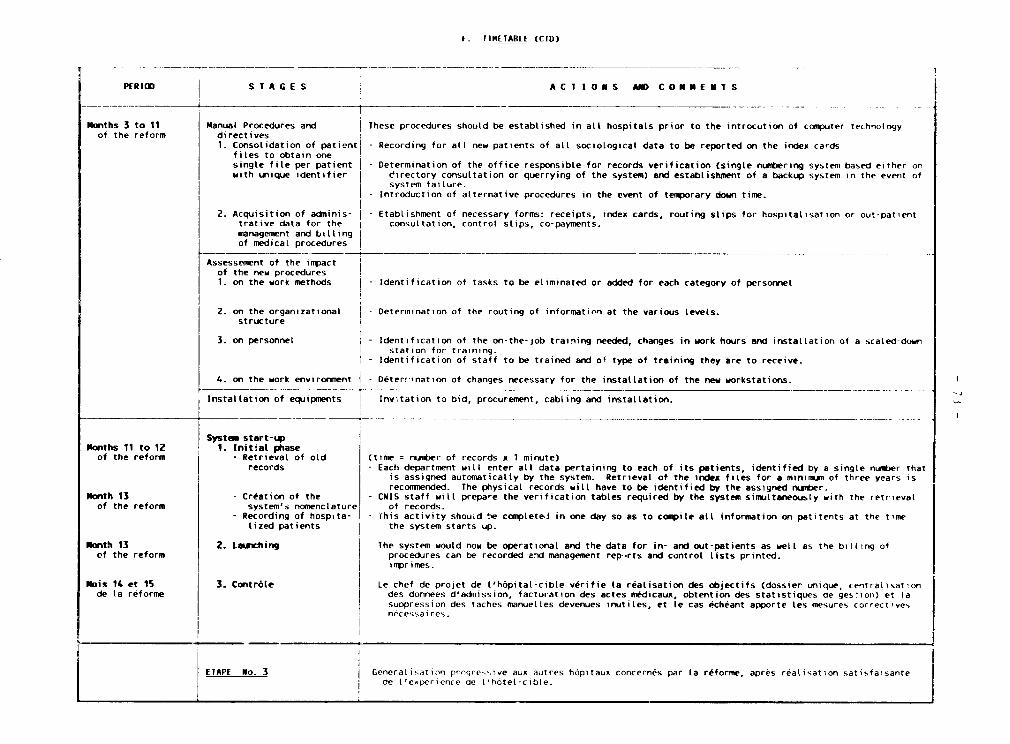
f1 IMlETARlE (CTD)
PERIOD S T A G E S A C T1 IO M S AM CO NUE MT S
Months 3 to 11 Manuat Procedures and These procedures shoutd be established in all hospitals prior to the introcution of computer technologyof the reform directives
1. Consolidation of patienti - Recording for a(l new patients of all sociological data to be reported on the index cardsfiles to obtain onesingle file per patient - Determination of the office responsible for records verification (single numbering system based either onwith unique identifier rirectory consultation or querrying of the system) and establishment of a backup system in the event of
systefi failure.- Introduction of alternative procedures in the event of temporary down time.
2. Acquisition of adminis- - Etablishment of necessary forms: receipts, index cards, routing stips for hospitalisation or out-patienttrative data for the consultation, controI stlips, co-payments.management and billingof medical procedures !__ __
Assessement of the impact
of the new procedures1. on the work methods - Identification of tasks to be eliminated or added for each category of personnel
2. on the organizational - Determination of the routing of informatio'n at the various levels.structure 1
3. on personnel I - Identification of the on-the-job training needed, changes in work hours and installation of a scaled-down- station for training.Identification of staff to be trained and of type of training they are to receive.
4. on the work environnent | - Déterrination of changes necessary for the installation of the new workstations.
Installation of equipments Inv,tation to bid, procurement. cabling and installation.
_~~~ ____-~----_____ ,____- - - - ______ _ ____ __-_-
Systea start-uP iMnths 11 to 12 1. Initial phaseof the reform - Retrieval of old (time = number of records x 1 minute)
records - Each department will enter all data pertaining to each of its patients, identified by a single njumber thatis assigned automatically by the system. Retrieval of the index fites for a minimum of three years isrecommended. The physical records wiilI have to be identified by the assigned numaber.
Ponth 13 - Création of the - CNIS staff will prepa,e the verification tables required by the system simultaneously w.ith the retrievalof the reform system's nomenclature of records.
- Recording of hospita- I - fhis activity shou-d be completeJ in one day so as to compile atl information on patitents at the timelized patients the system starts up.
Month 13 2. Launching l lhe system would now be operational and the data for in- and out-patients as weLl as the biltlng ofcf the reform procedures can be recorded a-id management rep.rts and controI lists printed.
imprimes.
Mois 14 et 15 3. Contrôle | Le chef de projet de l'hôpital-cible vérifie la réalisation des objectifs (dossier unique, centratisationde la réforme des donnees d'admission, facturation des actes medicaux, obtention des statistiques ce gesilori) et ta
suopression des tâches manuelles devenues inutiles, et le cas échéant apporte les mesures correct,vesnecessaires.
ETAPE No. 3 Géneraltiation prqre-..ive aux autres hôpitaux concernés par la reforme, apres réalisation satisfaisantede l'e,Iperience de ['hotel-cible.





























