Embed Size (px)
Citation preview
World Vision Relief amp Development Inc
FINAL EVALUATION BUNDIBUGYO CHILD SURVIVAL PROJECT
BUNDIBUGYO DISTRICT UGANDA
Beginning Date October 1 1989 Ending Date September 30 1992
Submitted to
PVO Child Survival Grants Program Office of Private and Voluntary Cooperation
Bureau for Food for Peace and Voluntary Assistance Room 103-C SA-2
Agency for International Development 515 23rd Avenue NW Washington DC 20523
PVO Headquarters Contact
Milton Amayun MD MPH World Vision Relief amp Development Inc
919 W Huntington Drive Monrovia CA 91016
December 21 1992
TABLE OF CONTENTS
I ExEcmwE SUM ARY A Child Survival Project Final Evaluation 1
II INTRODUCTION AND PURPOSE OF EVALUATION 3 A Project Objectives 3 B Midterm Evaluation Objectives 3 C Final Evaluation Objectives 4
III EVALUATION METHODOLOGY 4 A General Methodology 4 B Interviews and Survey 3 C Survey Data Analysis 5 D Fiscal Analysis 6 E Sustainability 6
IV BAcKGROUND 6 A Project Background 6 B Project Location 7 C Population Characteristics 7 D Target Groups 8
V FNDINGS 8 A NMidtermAc hieveInents8 B Project Design-Implementation Plan and Funding 9 C Project Funding 11
VI IN ERVENION ACHIEVEMENTS 13 A Immunization 13 B Oral Rehydration Therapy 14 C Nutrition 14 D Birth Spacing-High-Risk Births 15 E Maternal Death 15
VII SURVEY AND INTERVIEW RESULTS 17 A Results of Interviews with Income-generation Groups 18 B Interviews with 90 Mothers of Children Less Than Three Years of Age 19 C Interviews with Community Health Workers 22 D Interviews with Village Health Committees 23 E Interviews with Traditional Birth Attendants 25 F Interviews with World Vision Core Staff 26 G Interviews with MOLGMOH 28 H Interviews with NGOs 29
VIII SusTAINABiLrr 29 A General 29 B Sustainability Status 29 C Local Political Leaders-Local Capacity 30 D Estimated Recurrent Costs and Projected Revenues-CostBenefit 31 E Current Year Costs 32 F Unsustainable Costs 33 G Sustainability Plan-Community Participation and Cost Recovery 34
i
IX NEw INInVEtIONS 39 A Acute Respiratory Infection as a HealthProblem 39 B Intervention Strategies for ARI 40
X RECONM A71ONS 40 A Short-Term Recommendations 40 B Intermediate-Term Recommendations 41C Long-Term Recommendations 42
AFFENDICES
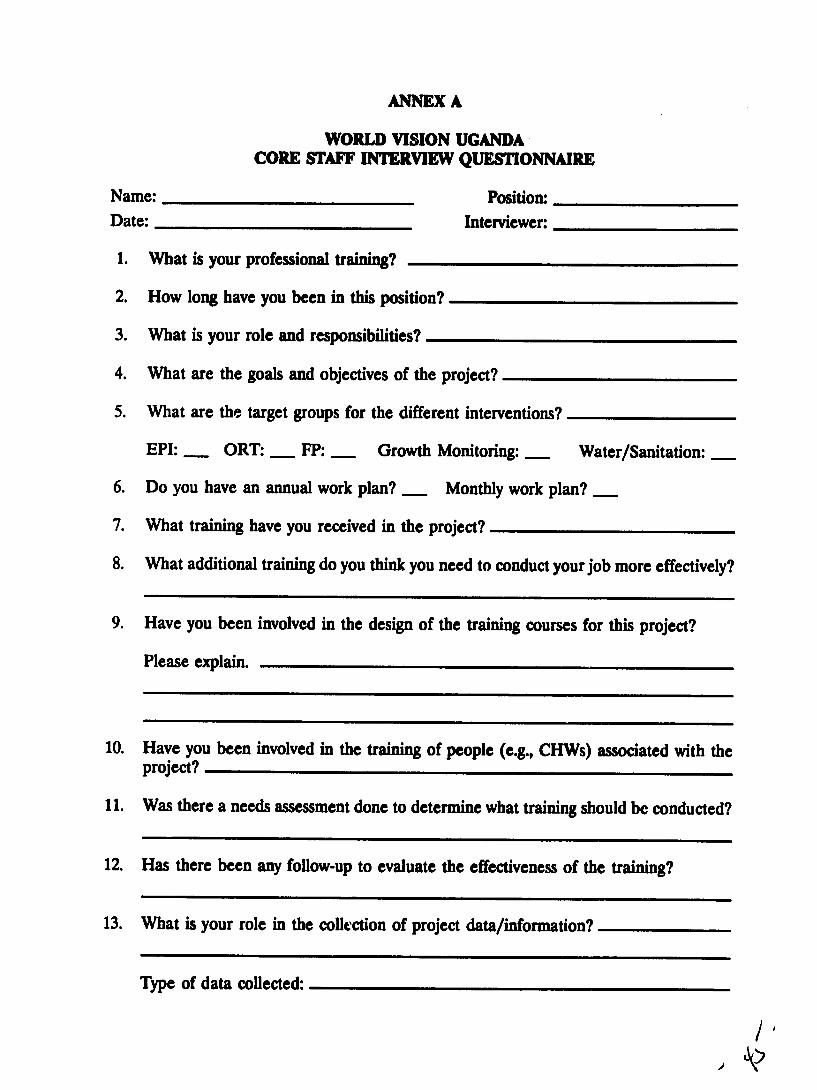
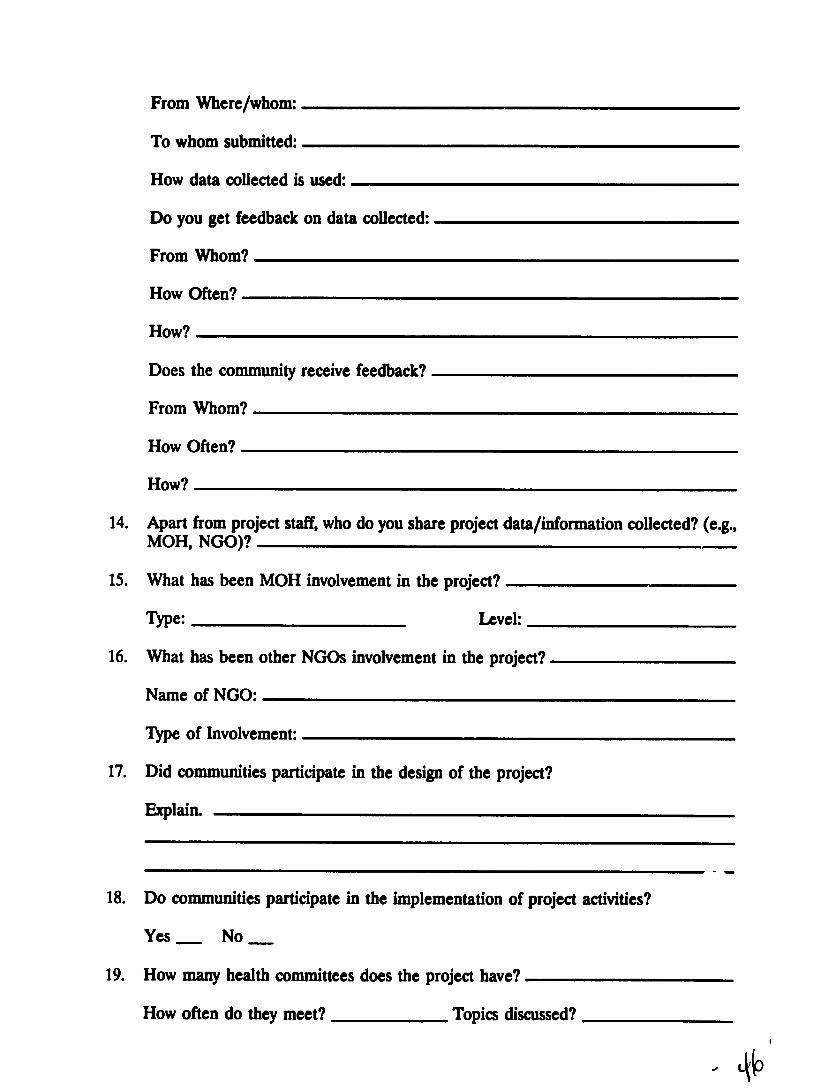
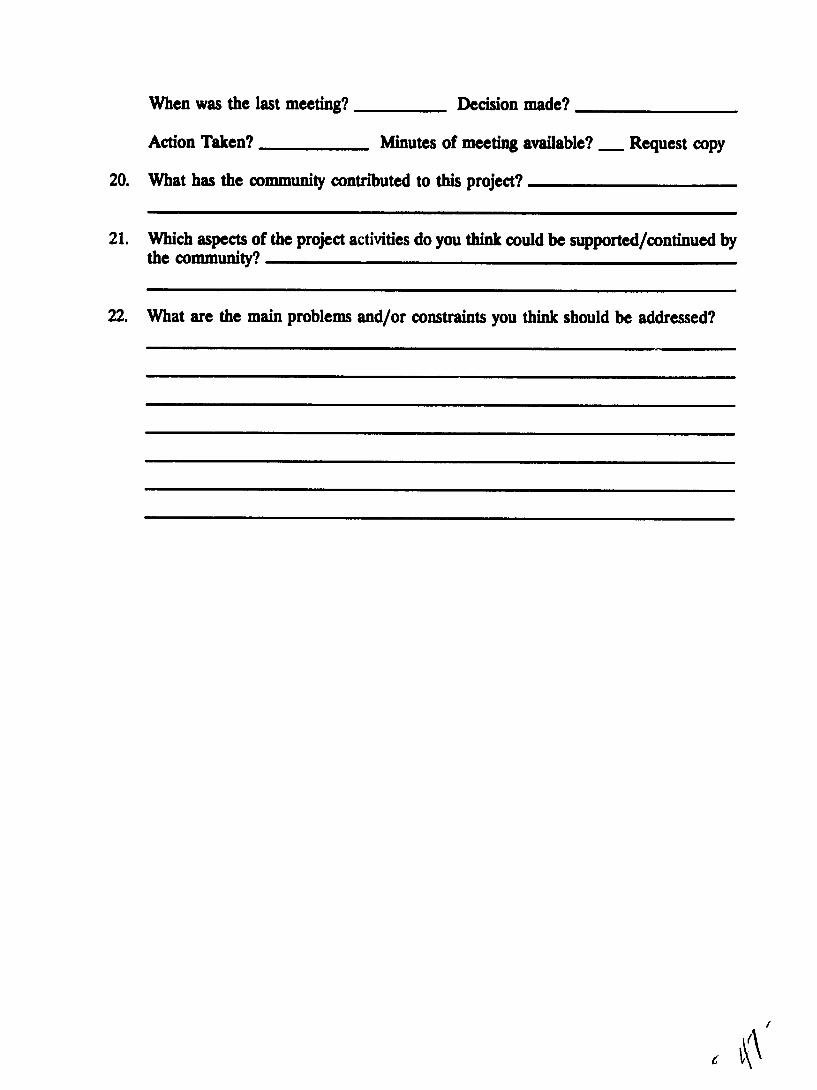
A Questionnaire for Core Staff B Questionnaire for Mothers C Questionnaire for CHWsTBAsD Questionnaire for Community Health Committee E Questionnaire for Ministry of Health F Questionnaire for NGOs G List of Documents Reviewed H Fiscal Expenditures by Category and Intervention
ii
AC AMREF ANC ARI BCG BCSP CBHCA CDD CHW CS CSP DIP DMO DPT EPI FP FY GOU GTZ HIS HIV HPN IGA MCH MMR MOH MOLG MTE NGO OPV ORTORS PHC PVO RC SSS TBA TOT Tr UCBHCA UNEPI UNICEF USAID VHC VHW WCBA WVWVI WRD WVU
AnBREVIAITM
Area Coordinator African Medical Research Foundation Antenatal Care Acute Respiratory Infection Bacilli Calmette-Guerin (tuberculosis vaccine) Bundibugyo Child Survival Project Community-based Health Care Association Control of Diarrheal Disease Community Health Worker Child Survival Child Survival ProjectDetailed Implementation Plan District Medical OfficerDistrict Medical Office DiphtheriaPertussisTetanus vaccine Expanded Program on Immunization Family PlanningFiscal Year Government of Uganda German NGO Health Information SystemHuman Immunodeficiency Virus Health Population and Nutrition Income-Generating Acdvity Maternal and Child Health Maternal Mortality Rate Ministry of Health Ministry of Local Government Midterm Evaluation Nongovernmental Organization Oral Polio Vaccine Oral Rehydration TherapyOral Rehydration Solution Primary Health Care Private Voluntary Organization Resistance Council SugarSalt Solution Traditional Birth Attendant Training of Trainers Tetanus Toxoid Uganda Community-Based Health Care Association Uganda National Expanded Program on Immunization United Nations Childrens Fund US Agency for International Development Village Health Committee Village Health Worker Women of Childbearing Age World VisionWorld Vision International World Vision Relief amp Development World Vision Uganda
iim
ExEc vE SuMMiav
A Child Survival Project Final Evaluation
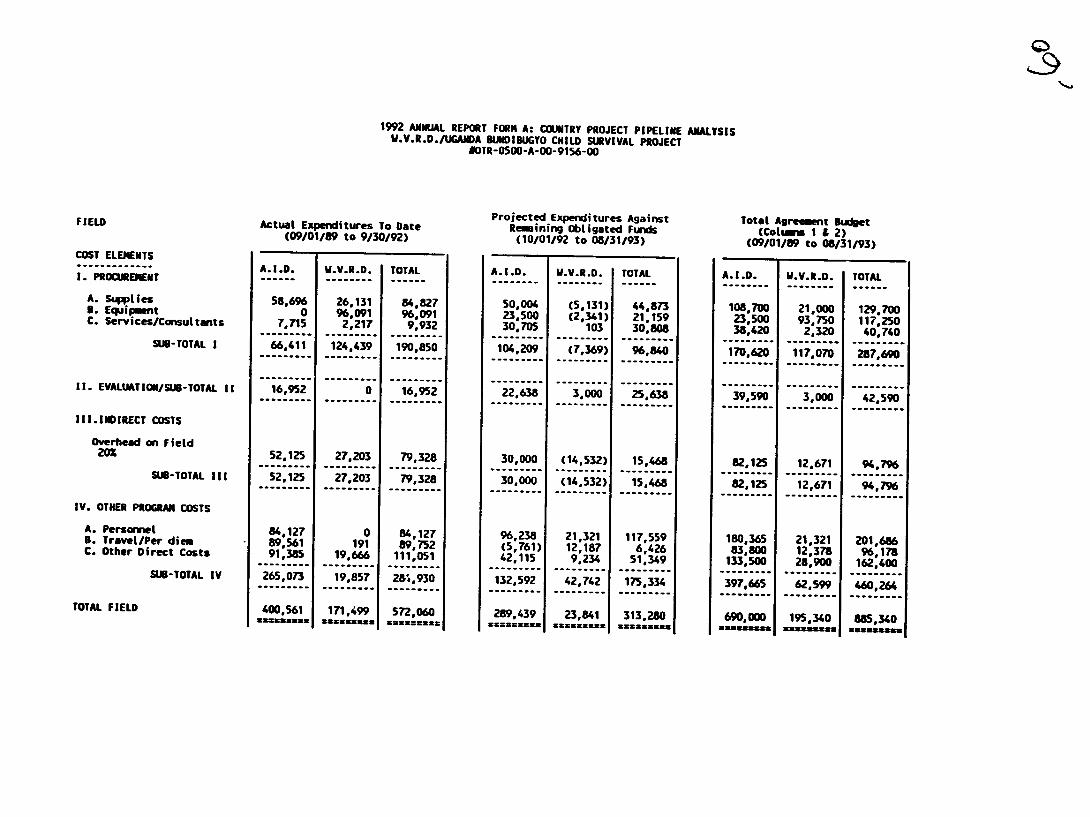
World Vision Relief amp Development received a $600000 matching grant from the FVAPVA Office of Private Voluntary Cooperation of USAID to implement a Child Survival project (CSP) in western Uganda for three years from October 1989 through Septembe 1992 The projects full implementation was delayed one year due to civil disturbances in portions of the impact area Unexpended funds are available and have been approved by USAID for a one-year no-cost project extension through September 1993
The goal of the project is to reduce the morbidity and mortality of children under five years through education and strategic support of the Ministry of Healths Maternal and Child HealthFamily Planning (MCHFP) activities over the life of the project The project impact location was negotiated with the MOH and the District Medical Officer (DMO) Ntoroko County Bundibugyo district was selected The implementation strategy is to establish train and empower Village Health Committees (VHC) Community Health Workers (CHW) Traditional Birth Attendants (TBA) and local regional and district-level political and other community leaders
A midterm evaluation was conducted September 13-23 1991 in order to provide midshycourse assessment and to propose recommendations for improvements and increased efficiency WV initiated a Plan of Action in response to the midterm evaluation findings The final evaluation took place September 19-30 1992 The evaluation team was composed of representatives from WVRD headquarters the Ministry of Health the African Medical Research Foundation (AMREF) the Uganda Community-based Health Care Association (UCBHCA) and an independent consultant Subsequent to the departure of the final evaluation team the final KAP survey using the WHOEPI method was completed (The full survey report accompanies this evaluation report)
The final evaluation process included interviews a 90-household survey study focus group discussions with key community participants and a review of pertinent documents Major findings were presented and thoroughly discussed at field and national levels with World Vision Uganda (WVU) core staff A briefing was given to the USAID Health Population and Nutrition (HPN) officer at Kampala The briefing included the information that a total of 30812 Expanded Program on Immunization (EPI) service contacts were made and 60r5 TI contact services were provided The following accomplishments related to the major objectives were recorded
Tau t Achieved
1 Fully immunized at lt 12 months 70 50
2 Immunize women of childbearing age(WCBA) with Tr2 50 48
1
3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
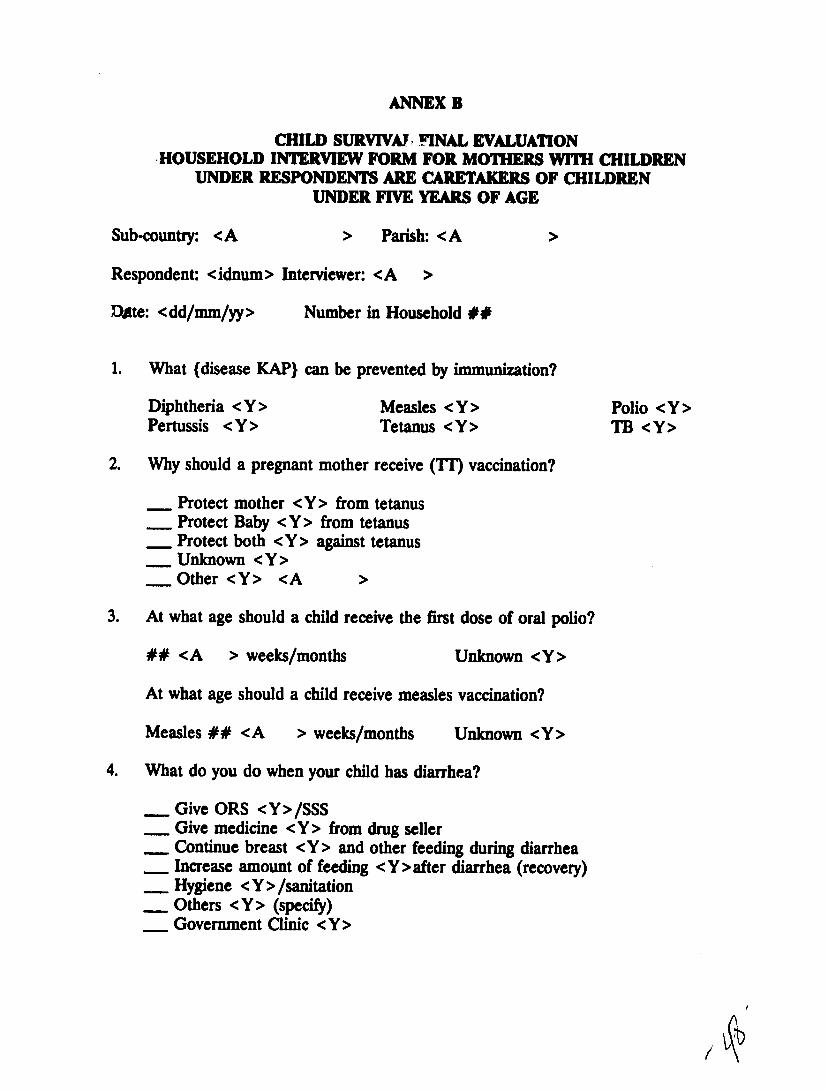
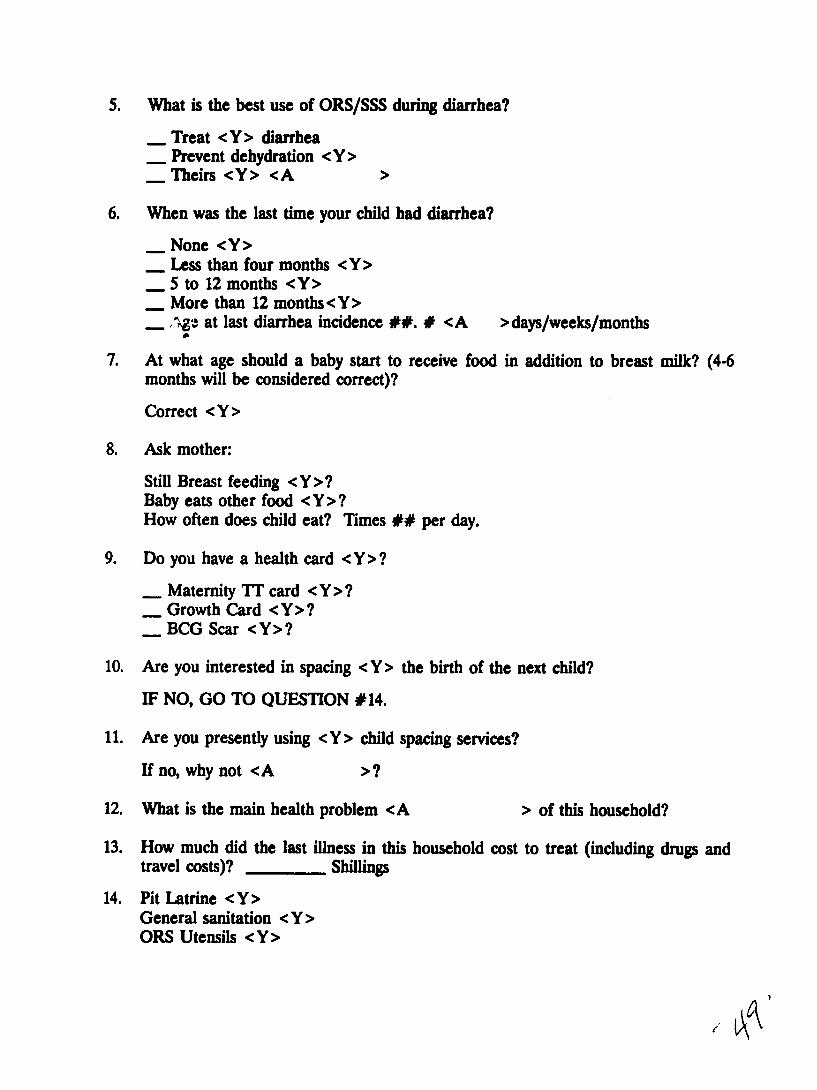
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
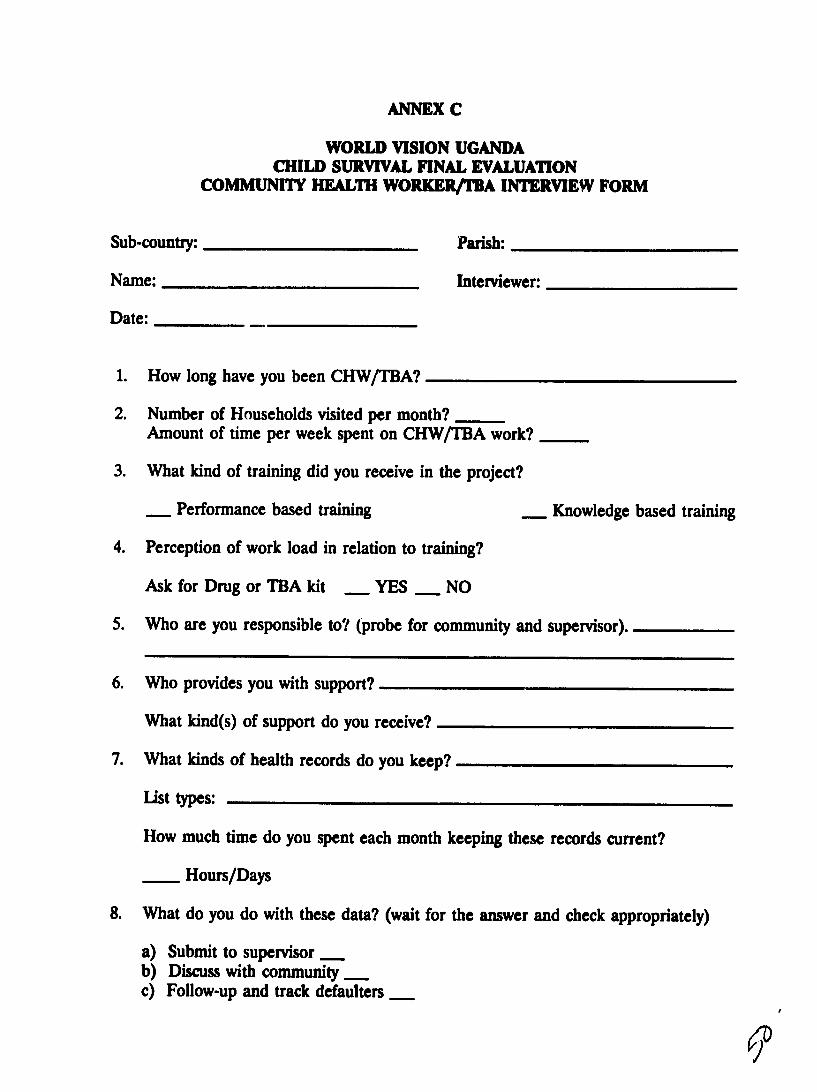
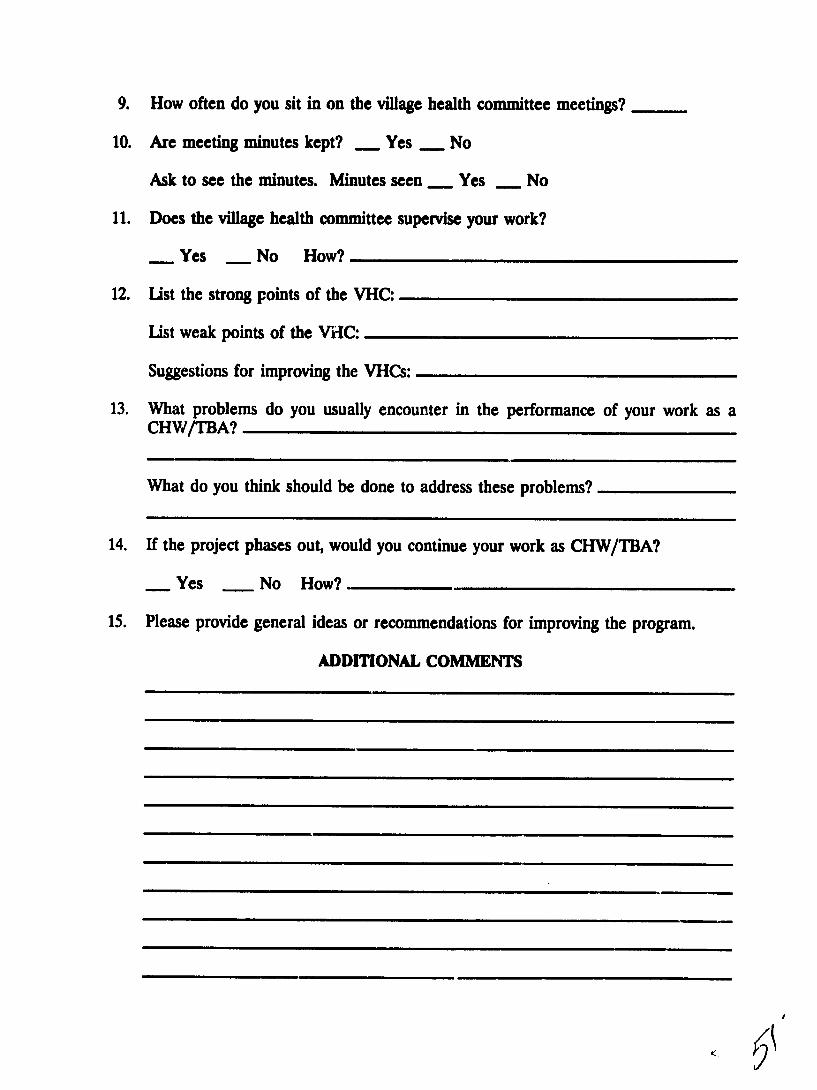
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
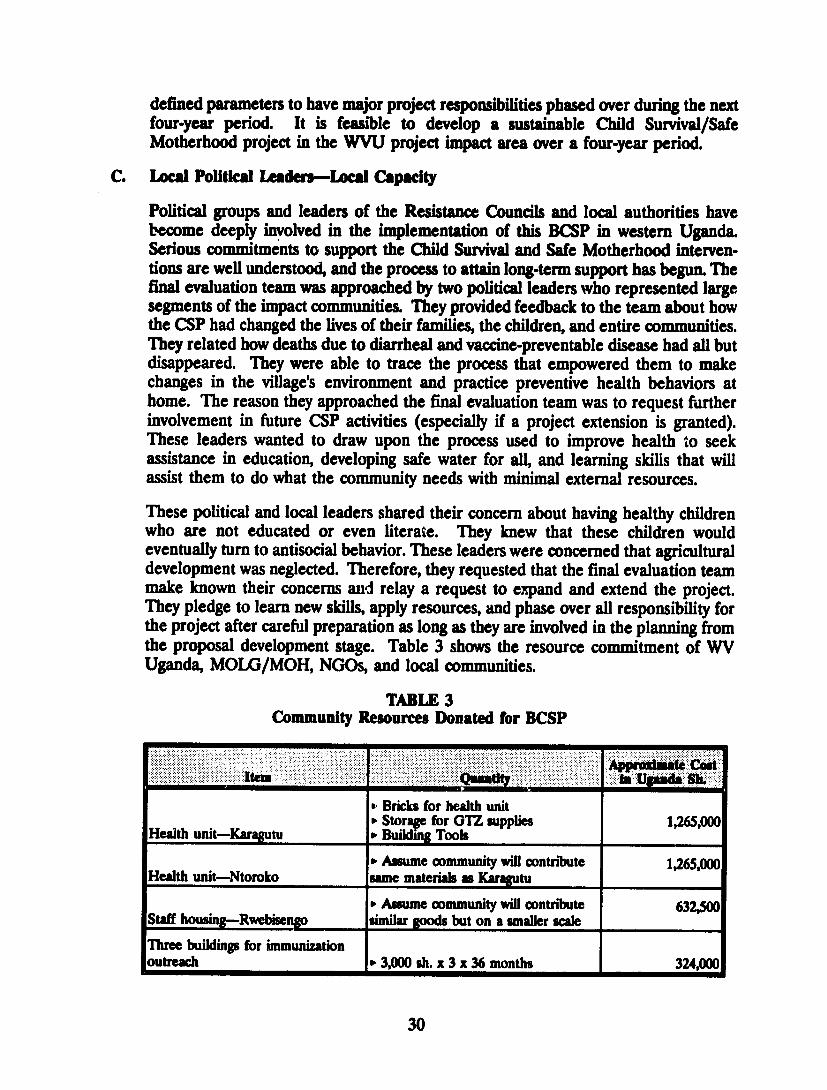
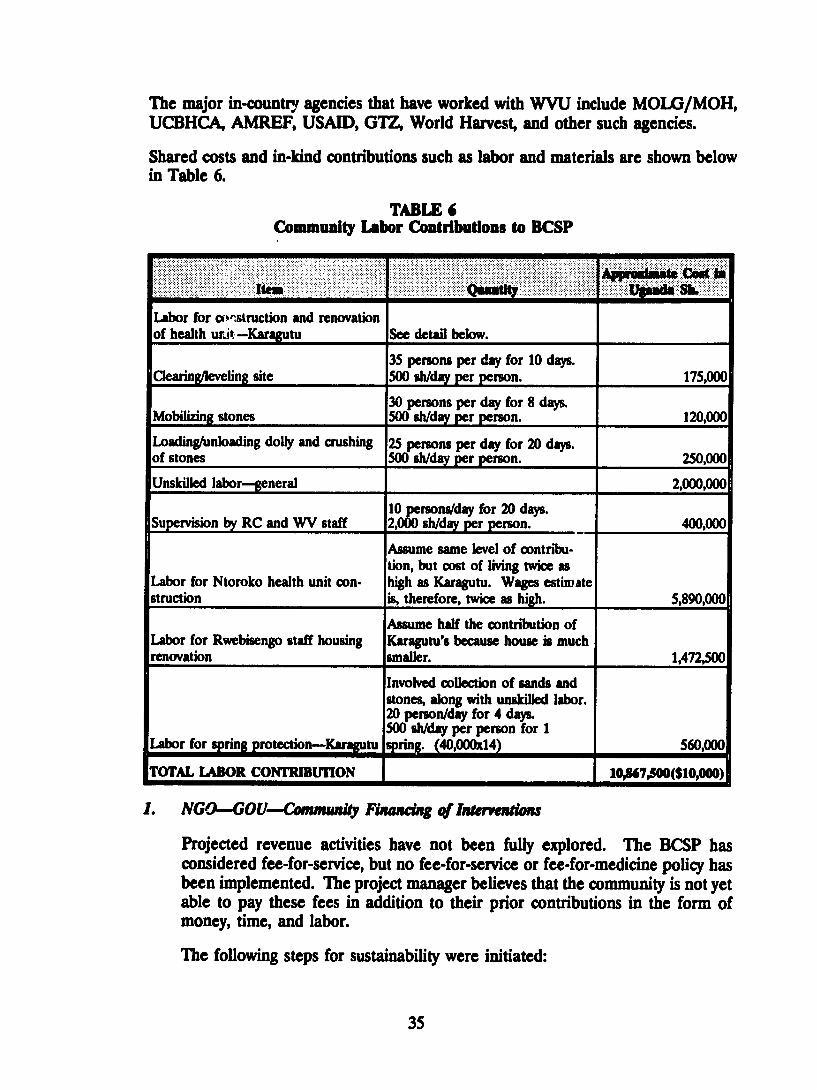
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
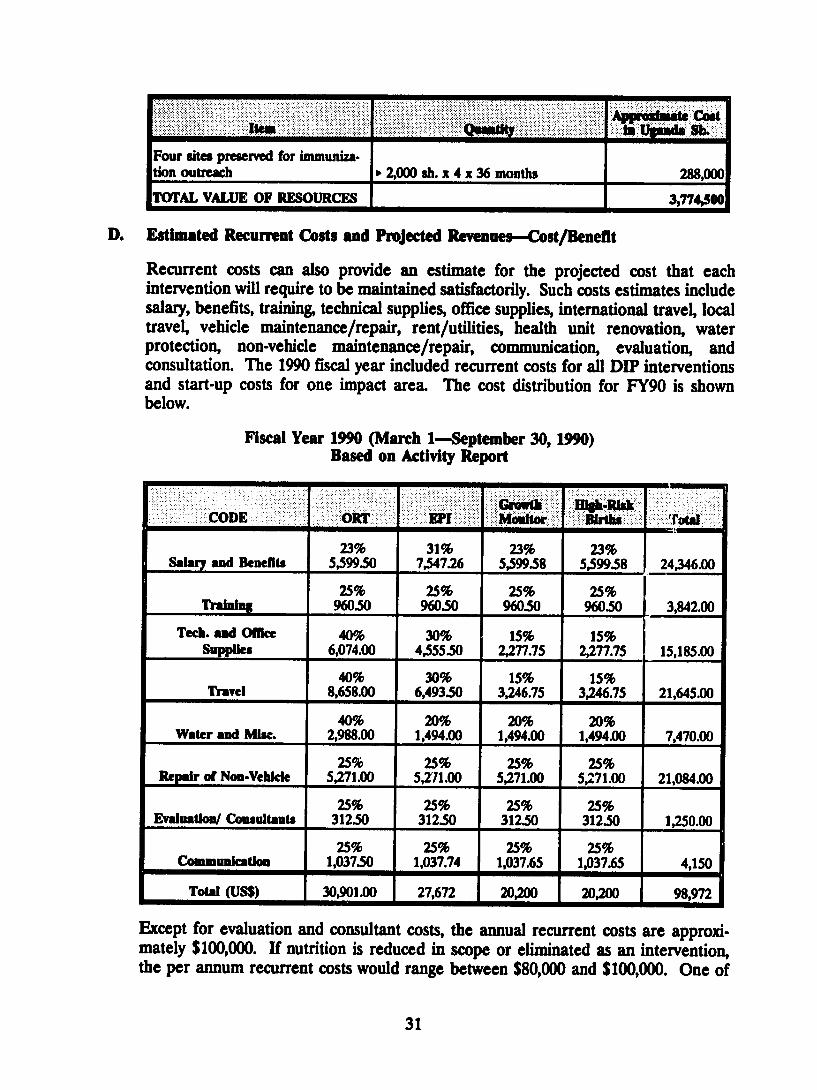
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
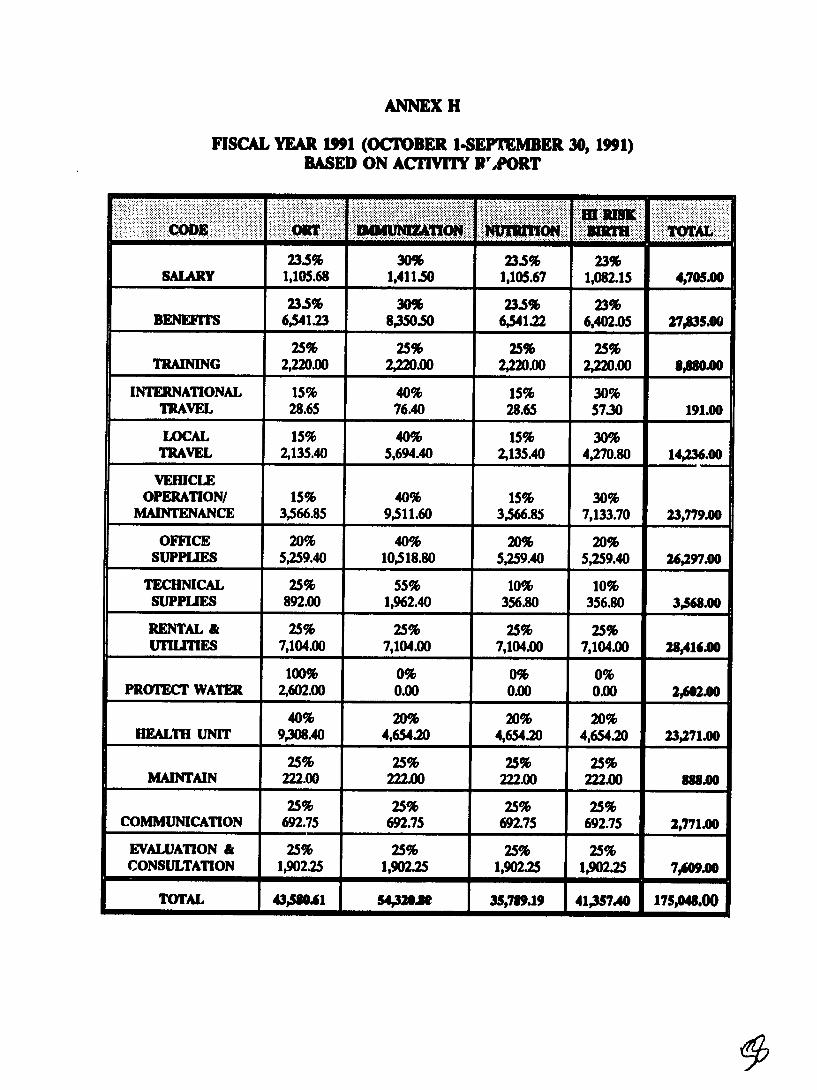
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
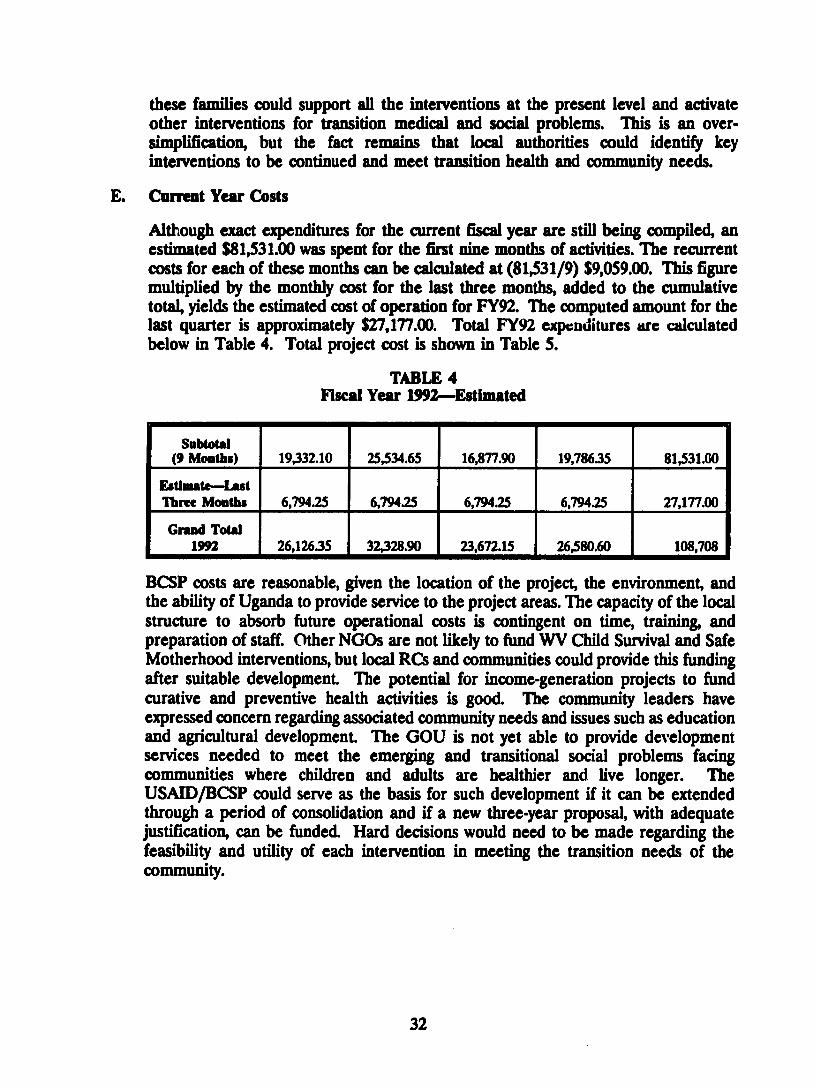
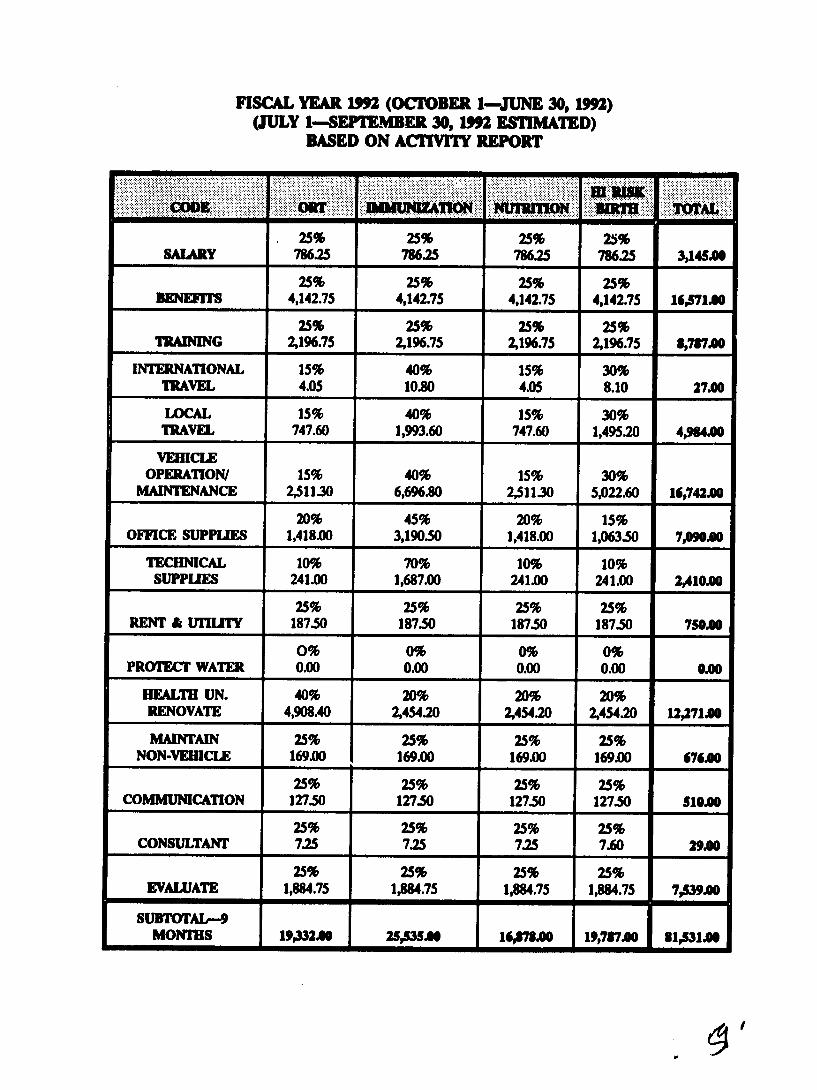
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
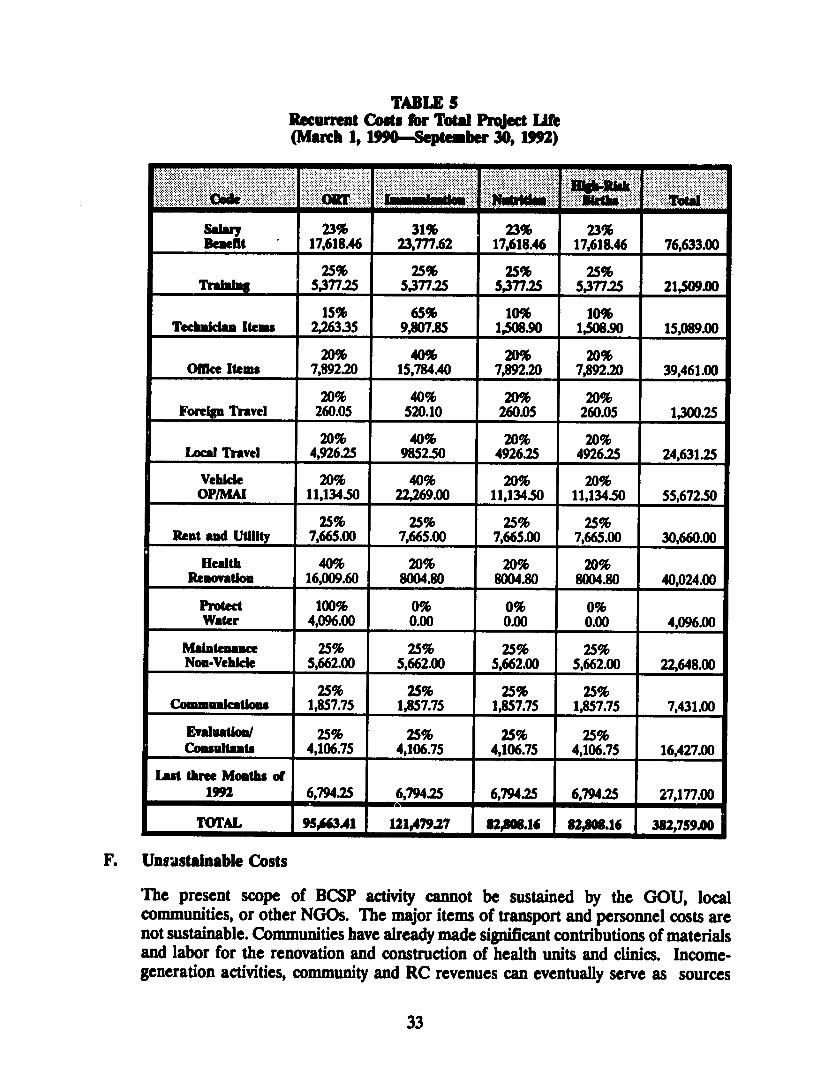
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
TABLE OF CONTENTS
I ExEcmwE SUM ARY A Child Survival Project Final Evaluation 1
II INTRODUCTION AND PURPOSE OF EVALUATION 3 A Project Objectives 3 B Midterm Evaluation Objectives 3 C Final Evaluation Objectives 4
III EVALUATION METHODOLOGY 4 A General Methodology 4 B Interviews and Survey 3 C Survey Data Analysis 5 D Fiscal Analysis 6 E Sustainability 6
IV BAcKGROUND 6 A Project Background 6 B Project Location 7 C Population Characteristics 7 D Target Groups 8
V FNDINGS 8 A NMidtermAc hieveInents8 B Project Design-Implementation Plan and Funding 9 C Project Funding 11
VI IN ERVENION ACHIEVEMENTS 13 A Immunization 13 B Oral Rehydration Therapy 14 C Nutrition 14 D Birth Spacing-High-Risk Births 15 E Maternal Death 15
VII SURVEY AND INTERVIEW RESULTS 17 A Results of Interviews with Income-generation Groups 18 B Interviews with 90 Mothers of Children Less Than Three Years of Age 19 C Interviews with Community Health Workers 22 D Interviews with Village Health Committees 23 E Interviews with Traditional Birth Attendants 25 F Interviews with World Vision Core Staff 26 G Interviews with MOLGMOH 28 H Interviews with NGOs 29
VIII SusTAINABiLrr 29 A General 29 B Sustainability Status 29 C Local Political Leaders-Local Capacity 30 D Estimated Recurrent Costs and Projected Revenues-CostBenefit 31 E Current Year Costs 32 F Unsustainable Costs 33 G Sustainability Plan-Community Participation and Cost Recovery 34
i
IX NEw INInVEtIONS 39 A Acute Respiratory Infection as a HealthProblem 39 B Intervention Strategies for ARI 40
X RECONM A71ONS 40 A Short-Term Recommendations 40 B Intermediate-Term Recommendations 41C Long-Term Recommendations 42
AFFENDICES
A Questionnaire for Core Staff B Questionnaire for Mothers C Questionnaire for CHWsTBAsD Questionnaire for Community Health Committee E Questionnaire for Ministry of Health F Questionnaire for NGOs G List of Documents Reviewed H Fiscal Expenditures by Category and Intervention
ii
AC AMREF ANC ARI BCG BCSP CBHCA CDD CHW CS CSP DIP DMO DPT EPI FP FY GOU GTZ HIS HIV HPN IGA MCH MMR MOH MOLG MTE NGO OPV ORTORS PHC PVO RC SSS TBA TOT Tr UCBHCA UNEPI UNICEF USAID VHC VHW WCBA WVWVI WRD WVU
AnBREVIAITM
Area Coordinator African Medical Research Foundation Antenatal Care Acute Respiratory Infection Bacilli Calmette-Guerin (tuberculosis vaccine) Bundibugyo Child Survival Project Community-based Health Care Association Control of Diarrheal Disease Community Health Worker Child Survival Child Survival ProjectDetailed Implementation Plan District Medical OfficerDistrict Medical Office DiphtheriaPertussisTetanus vaccine Expanded Program on Immunization Family PlanningFiscal Year Government of Uganda German NGO Health Information SystemHuman Immunodeficiency Virus Health Population and Nutrition Income-Generating Acdvity Maternal and Child Health Maternal Mortality Rate Ministry of Health Ministry of Local Government Midterm Evaluation Nongovernmental Organization Oral Polio Vaccine Oral Rehydration TherapyOral Rehydration Solution Primary Health Care Private Voluntary Organization Resistance Council SugarSalt Solution Traditional Birth Attendant Training of Trainers Tetanus Toxoid Uganda Community-Based Health Care Association Uganda National Expanded Program on Immunization United Nations Childrens Fund US Agency for International Development Village Health Committee Village Health Worker Women of Childbearing Age World VisionWorld Vision International World Vision Relief amp Development World Vision Uganda
iim
ExEc vE SuMMiav
A Child Survival Project Final Evaluation
World Vision Relief amp Development received a $600000 matching grant from the FVAPVA Office of Private Voluntary Cooperation of USAID to implement a Child Survival project (CSP) in western Uganda for three years from October 1989 through Septembe 1992 The projects full implementation was delayed one year due to civil disturbances in portions of the impact area Unexpended funds are available and have been approved by USAID for a one-year no-cost project extension through September 1993
The goal of the project is to reduce the morbidity and mortality of children under five years through education and strategic support of the Ministry of Healths Maternal and Child HealthFamily Planning (MCHFP) activities over the life of the project The project impact location was negotiated with the MOH and the District Medical Officer (DMO) Ntoroko County Bundibugyo district was selected The implementation strategy is to establish train and empower Village Health Committees (VHC) Community Health Workers (CHW) Traditional Birth Attendants (TBA) and local regional and district-level political and other community leaders
A midterm evaluation was conducted September 13-23 1991 in order to provide midshycourse assessment and to propose recommendations for improvements and increased efficiency WV initiated a Plan of Action in response to the midterm evaluation findings The final evaluation took place September 19-30 1992 The evaluation team was composed of representatives from WVRD headquarters the Ministry of Health the African Medical Research Foundation (AMREF) the Uganda Community-based Health Care Association (UCBHCA) and an independent consultant Subsequent to the departure of the final evaluation team the final KAP survey using the WHOEPI method was completed (The full survey report accompanies this evaluation report)
The final evaluation process included interviews a 90-household survey study focus group discussions with key community participants and a review of pertinent documents Major findings were presented and thoroughly discussed at field and national levels with World Vision Uganda (WVU) core staff A briefing was given to the USAID Health Population and Nutrition (HPN) officer at Kampala The briefing included the information that a total of 30812 Expanded Program on Immunization (EPI) service contacts were made and 60r5 TI contact services were provided The following accomplishments related to the major objectives were recorded
Tau t Achieved
1 Fully immunized at lt 12 months 70 50
2 Immunize women of childbearing age(WCBA) with Tr2 50 48
1
3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
IX NEw INInVEtIONS 39 A Acute Respiratory Infection as a HealthProblem 39 B Intervention Strategies for ARI 40
X RECONM A71ONS 40 A Short-Term Recommendations 40 B Intermediate-Term Recommendations 41C Long-Term Recommendations 42
AFFENDICES
A Questionnaire for Core Staff B Questionnaire for Mothers C Questionnaire for CHWsTBAsD Questionnaire for Community Health Committee E Questionnaire for Ministry of Health F Questionnaire for NGOs G List of Documents Reviewed H Fiscal Expenditures by Category and Intervention
ii
AC AMREF ANC ARI BCG BCSP CBHCA CDD CHW CS CSP DIP DMO DPT EPI FP FY GOU GTZ HIS HIV HPN IGA MCH MMR MOH MOLG MTE NGO OPV ORTORS PHC PVO RC SSS TBA TOT Tr UCBHCA UNEPI UNICEF USAID VHC VHW WCBA WVWVI WRD WVU
AnBREVIAITM
Area Coordinator African Medical Research Foundation Antenatal Care Acute Respiratory Infection Bacilli Calmette-Guerin (tuberculosis vaccine) Bundibugyo Child Survival Project Community-based Health Care Association Control of Diarrheal Disease Community Health Worker Child Survival Child Survival ProjectDetailed Implementation Plan District Medical OfficerDistrict Medical Office DiphtheriaPertussisTetanus vaccine Expanded Program on Immunization Family PlanningFiscal Year Government of Uganda German NGO Health Information SystemHuman Immunodeficiency Virus Health Population and Nutrition Income-Generating Acdvity Maternal and Child Health Maternal Mortality Rate Ministry of Health Ministry of Local Government Midterm Evaluation Nongovernmental Organization Oral Polio Vaccine Oral Rehydration TherapyOral Rehydration Solution Primary Health Care Private Voluntary Organization Resistance Council SugarSalt Solution Traditional Birth Attendant Training of Trainers Tetanus Toxoid Uganda Community-Based Health Care Association Uganda National Expanded Program on Immunization United Nations Childrens Fund US Agency for International Development Village Health Committee Village Health Worker Women of Childbearing Age World VisionWorld Vision International World Vision Relief amp Development World Vision Uganda
iim
ExEc vE SuMMiav
A Child Survival Project Final Evaluation
World Vision Relief amp Development received a $600000 matching grant from the FVAPVA Office of Private Voluntary Cooperation of USAID to implement a Child Survival project (CSP) in western Uganda for three years from October 1989 through Septembe 1992 The projects full implementation was delayed one year due to civil disturbances in portions of the impact area Unexpended funds are available and have been approved by USAID for a one-year no-cost project extension through September 1993
The goal of the project is to reduce the morbidity and mortality of children under five years through education and strategic support of the Ministry of Healths Maternal and Child HealthFamily Planning (MCHFP) activities over the life of the project The project impact location was negotiated with the MOH and the District Medical Officer (DMO) Ntoroko County Bundibugyo district was selected The implementation strategy is to establish train and empower Village Health Committees (VHC) Community Health Workers (CHW) Traditional Birth Attendants (TBA) and local regional and district-level political and other community leaders
A midterm evaluation was conducted September 13-23 1991 in order to provide midshycourse assessment and to propose recommendations for improvements and increased efficiency WV initiated a Plan of Action in response to the midterm evaluation findings The final evaluation took place September 19-30 1992 The evaluation team was composed of representatives from WVRD headquarters the Ministry of Health the African Medical Research Foundation (AMREF) the Uganda Community-based Health Care Association (UCBHCA) and an independent consultant Subsequent to the departure of the final evaluation team the final KAP survey using the WHOEPI method was completed (The full survey report accompanies this evaluation report)
The final evaluation process included interviews a 90-household survey study focus group discussions with key community participants and a review of pertinent documents Major findings were presented and thoroughly discussed at field and national levels with World Vision Uganda (WVU) core staff A briefing was given to the USAID Health Population and Nutrition (HPN) officer at Kampala The briefing included the information that a total of 30812 Expanded Program on Immunization (EPI) service contacts were made and 60r5 TI contact services were provided The following accomplishments related to the major objectives were recorded
Tau t Achieved
1 Fully immunized at lt 12 months 70 50
2 Immunize women of childbearing age(WCBA) with Tr2 50 48
1
3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
AC AMREF ANC ARI BCG BCSP CBHCA CDD CHW CS CSP DIP DMO DPT EPI FP FY GOU GTZ HIS HIV HPN IGA MCH MMR MOH MOLG MTE NGO OPV ORTORS PHC PVO RC SSS TBA TOT Tr UCBHCA UNEPI UNICEF USAID VHC VHW WCBA WVWVI WRD WVU
AnBREVIAITM
Area Coordinator African Medical Research Foundation Antenatal Care Acute Respiratory Infection Bacilli Calmette-Guerin (tuberculosis vaccine) Bundibugyo Child Survival Project Community-based Health Care Association Control of Diarrheal Disease Community Health Worker Child Survival Child Survival ProjectDetailed Implementation Plan District Medical OfficerDistrict Medical Office DiphtheriaPertussisTetanus vaccine Expanded Program on Immunization Family PlanningFiscal Year Government of Uganda German NGO Health Information SystemHuman Immunodeficiency Virus Health Population and Nutrition Income-Generating Acdvity Maternal and Child Health Maternal Mortality Rate Ministry of Health Ministry of Local Government Midterm Evaluation Nongovernmental Organization Oral Polio Vaccine Oral Rehydration TherapyOral Rehydration Solution Primary Health Care Private Voluntary Organization Resistance Council SugarSalt Solution Traditional Birth Attendant Training of Trainers Tetanus Toxoid Uganda Community-Based Health Care Association Uganda National Expanded Program on Immunization United Nations Childrens Fund US Agency for International Development Village Health Committee Village Health Worker Women of Childbearing Age World VisionWorld Vision International World Vision Relief amp Development World Vision Uganda
iim
ExEc vE SuMMiav
A Child Survival Project Final Evaluation
World Vision Relief amp Development received a $600000 matching grant from the FVAPVA Office of Private Voluntary Cooperation of USAID to implement a Child Survival project (CSP) in western Uganda for three years from October 1989 through Septembe 1992 The projects full implementation was delayed one year due to civil disturbances in portions of the impact area Unexpended funds are available and have been approved by USAID for a one-year no-cost project extension through September 1993
The goal of the project is to reduce the morbidity and mortality of children under five years through education and strategic support of the Ministry of Healths Maternal and Child HealthFamily Planning (MCHFP) activities over the life of the project The project impact location was negotiated with the MOH and the District Medical Officer (DMO) Ntoroko County Bundibugyo district was selected The implementation strategy is to establish train and empower Village Health Committees (VHC) Community Health Workers (CHW) Traditional Birth Attendants (TBA) and local regional and district-level political and other community leaders
A midterm evaluation was conducted September 13-23 1991 in order to provide midshycourse assessment and to propose recommendations for improvements and increased efficiency WV initiated a Plan of Action in response to the midterm evaluation findings The final evaluation took place September 19-30 1992 The evaluation team was composed of representatives from WVRD headquarters the Ministry of Health the African Medical Research Foundation (AMREF) the Uganda Community-based Health Care Association (UCBHCA) and an independent consultant Subsequent to the departure of the final evaluation team the final KAP survey using the WHOEPI method was completed (The full survey report accompanies this evaluation report)
The final evaluation process included interviews a 90-household survey study focus group discussions with key community participants and a review of pertinent documents Major findings were presented and thoroughly discussed at field and national levels with World Vision Uganda (WVU) core staff A briefing was given to the USAID Health Population and Nutrition (HPN) officer at Kampala The briefing included the information that a total of 30812 Expanded Program on Immunization (EPI) service contacts were made and 60r5 TI contact services were provided The following accomplishments related to the major objectives were recorded
Tau t Achieved
1 Fully immunized at lt 12 months 70 50
2 Immunize women of childbearing age(WCBA) with Tr2 50 48
1
3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
ExEc vE SuMMiav
A Child Survival Project Final Evaluation
World Vision Relief amp Development received a $600000 matching grant from the FVAPVA Office of Private Voluntary Cooperation of USAID to implement a Child Survival project (CSP) in western Uganda for three years from October 1989 through Septembe 1992 The projects full implementation was delayed one year due to civil disturbances in portions of the impact area Unexpended funds are available and have been approved by USAID for a one-year no-cost project extension through September 1993
The goal of the project is to reduce the morbidity and mortality of children under five years through education and strategic support of the Ministry of Healths Maternal and Child HealthFamily Planning (MCHFP) activities over the life of the project The project impact location was negotiated with the MOH and the District Medical Officer (DMO) Ntoroko County Bundibugyo district was selected The implementation strategy is to establish train and empower Village Health Committees (VHC) Community Health Workers (CHW) Traditional Birth Attendants (TBA) and local regional and district-level political and other community leaders
A midterm evaluation was conducted September 13-23 1991 in order to provide midshycourse assessment and to propose recommendations for improvements and increased efficiency WV initiated a Plan of Action in response to the midterm evaluation findings The final evaluation took place September 19-30 1992 The evaluation team was composed of representatives from WVRD headquarters the Ministry of Health the African Medical Research Foundation (AMREF) the Uganda Community-based Health Care Association (UCBHCA) and an independent consultant Subsequent to the departure of the final evaluation team the final KAP survey using the WHOEPI method was completed (The full survey report accompanies this evaluation report)
The final evaluation process included interviews a 90-household survey study focus group discussions with key community participants and a review of pertinent documents Major findings were presented and thoroughly discussed at field and national levels with World Vision Uganda (WVU) core staff A briefing was given to the USAID Health Population and Nutrition (HPN) officer at Kampala The briefing included the information that a total of 30812 Expanded Program on Immunization (EPI) service contacts were made and 60r5 TI contact services were provided The following accomplishments related to the major objectives were recorded
Tau t Achieved
1 Fully immunized at lt 12 months 70 50
2 Immunize women of childbearing age(WCBA) with Tr2 50 48
1
3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333

3 Reduce malnutrition rate among 509b 1613 children 0-35 months Service contacts
4 Reduce the number of deaths due to diarrheal dehydration reported 60 8 deaths
5 Mothers of children lt5 years know how to correctly prepare and use ORT 50 91 and 85
6 Increase the number of couples using a modern method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 74 trained
Establish and train VHCs 61 trained
8 Increase the number of homes with latrines 30 89 achieved
9 Health education messages or contacts 46730
Most objectives were well realized The exceptions were reduced achievements on the family planning and malnutrition objectives
A total of 6549 family planning education contacts were made during the three-year project period The greatest constraint was a lack of FP commodities and Government of Uganda (GOU) requirements for staff and physical examination requirements
By consensus the final evaluation team endorses the no-cost one-year extension through September 1993 The major recommendation is for WVRD to provide a matching grant proposal to USAID FVAPVC Office for a new three-year CSP The proposal should contain a sustainability phase-over plan involving the MOH the present project community-based structure and other levels of political and local authorities The proposal to USAID should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP and careful consideration of expansion and a demonstration of the projects replication capacity
The final evaluation findings showed tremendous community-level impact with documented gains in the reduction of deaths from diarrhea and vaccine-preventabledisease The evaluation further demonstrated that villagers were aware of their behavior and its impact on death and morbidity The potential for highly sustainable child survival and safe motherhood interventions through a second project is promising based on the findings of the achievements of the first three years
2
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
II IMTDUC N AND PUROE OF EVAWATWN
A Project Objectives
The goal of this project is in collaboration with the Ministry of Health o reduce morbidity and mortality in childien under five years old in Bundibugyo district of Uganda from vaccine-preventable diseases dehydration due to diarrhea aid malnutrition The CSP set the following end-of-project objectives
1 Provide full immunization coverage to 70 cf the children before their first birthday
2 Immunize 50 of women of childbearing age with T2
3 Reduce by 60 the existing malnutrition rate among children 0-35 months
4 Reduce by 60 the number of deaths due to diarrheal dehydration
5 Ensure that 50 of mothers with children under five know how to properly prepare and use ORT for diarrhea in their children
6 Increase to 30 the number of couples using a modem method of contracepshytion
7 Train one CHW and one TBA for each Resistance Council (RC) zone 8 Increase to 30 the number of houses wth latrines through health education
campaigns
9 Protect 50 of springs and pipe water into Karugtu
B Midterm Evaluation Objectives
The purpose of the Midterm Evaluation (MTE) was to assess the progress achieved during the first two years of project life and to recommend necessary strategies to fully achieve project objectives The MTE results would provide a basis for the endshyof-project evaluation The following specific objectives were established for the MTE
1 To assess project achievements against revised objectives 2 To provide suggestions to improve the health information system (HIS)
currently in place 3 To suggest ways of improving existing strategies and to identify new strategies
for sustainability 4 To provide recommendations on future directives to improve the quality of
services for the third year of the project
3
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
C Final Evaluation Objectives
The WVRD Final Evaluation of the Bundibugyo Child Survival Project (BCSP) in Uganda intends to comply with all USAID requirements specifically those related to project sustainability assessment according to guidelines
The following specific objectives were established
1 Conduct a project Sustainability Assessment using the USAID guidelines developed for Final Evaluation
2 Review strategies implemented and progress made towards sustaining project benefits
3 Identify other strategies to further enhance the sustainability of CS intervenshytions
4 Conduct an assessment of costbenofit ratios by intervention
5 Provide suggestions for inclusion of new interventions eg pneumonia control safe motherhood activities in the extensionexpansion phase to be proposed for FY94-FY96
Ill EvALUATON MEmoDoWGy
A General Methodology
The BCSP was initiated on October 1 1989 It did not begin full implementation until 1991 A midterm evaluation was conducted in September 1991 Various reports and assessments were used to monitor the progress of intervention activities The midterm evaluation process identified program areas that could be adjusted to enhance their potential for success During the final evaluation the team analyzed reports conducted a household survey and reviewed previous evaluation documents yielding both quantitative and qualitative sources of information
WVRD assigned an advance staff (intern) to initiate the final evaluation process involving a thorough collection of data and conduct of important interviews This procedure greatly assisted the evaluation exercise and considerably expanded the range of information available to the final evaluation team The BCSP has in place a complex HIS Recently the reporting forms were simplified and the field staff are reconciling records with the new format Several interview survey instruments were developed that could be used to compare findings with those from the midterm interviews New questionnaires were designed to evaluate progress made toward the DIP objectives (see Annex A) The final evaluation team was divided into three subgroups with specific assignments given to each group Interviews were conducted at headquarters and in the impact areas with various levels of project beneficiaries MOLGMOH Officials NGOs and WVU core staff
4
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
B Intervim and Survey
Interviews were conducted in 90 randomly selected households in the impact area villages Using the survey sampling formula of Kish and Leslie based on a population of 24200 and an expected frequency (EPI coverage level reported at midterm) of 27 a random sample of 26 would yield a confidence level of 95 while 45 randomly sampled households would provide up to a 99 confidence level It was not possible to use a total random selection process but the confidence level attained through the 90 household interviews should be adequate for valid observations and findings
During the random selection of villages the World Health Organization software COS t3 (Costat option) was used to select communities from all three impact areas k random computer-generated sample of 30 households was selected for interviews in each of the three impact areas (90 total) Throughout the evaluation projectrecords and documents were reviewed WVU headquarters and field staff were interviewed and meetings were held with key NGO personnel (See Annex B for a list of documents reviewed) After the field survey results were tabulated and analyzed an open meeting and briefing regarding the main evaluation findings was held with the WVU field implementation staff at the central headquarters in Karagutu A similar briefing was conducted for the USAID HPN officer in Kampala
Interviews were conducted with core WVU BCSP staff MOH NGOs village health workers (VHW) TBAs VHCs and MOLGRC officials Income-generation associations and other village focus groups were also interviewed In some instances CHWs and community health committees were observed and interviewed to determine their competence and viability The views of VHCs on sustainability and cost benefitrecovery mechanisms were solicited All WVU local project-area site facilities were visited and village water sources such as covered springs and water protection activities were observed Mothers and other community recipients were interviewed in groups and as individuals Observations were recorded during the 90 households interviews regarding EPI and child health cards for children and Tetanus toxoid (TI) cards for women Household utensils for ORSSSS preparation pitlatrines drying racks and cleanliness around each compound visited were also assessed
C Survey Data Analysis
Survey results were analyzed manually and also with Epi Info Analysis software Interviews were summarized and analyzed within the subgroups Daily team meetings were conducted A compilation of findings was shared among the team members on the last day of formal final evaluation effort (September 30 1992) From the considerable data collected recommendations were generated at three levels
0 Present and immediate future ie one-year consolidation Future CS proposal and Long-term applications for expansion and replicability
5
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
D Flscal Analysis
The entire fiscal structure was carefully examined to assess start-up and recurrent costs and other direct support expenditures The midterm evaluation report assessed cost per intervention which included general costs and the recommendation that the BCSP try to develop more intervention-specific cost indicators The final evaluation fiscal analysis tried to further assess cost per intervention Household expenditures for the most recent illness were researched through the survey process
E Sustainablity
Sustainability issues were addressed through interviews documents and observations Various aspeci that are clearly sustainable have been identified Other related aspects were examined and researched with various groups and organizations These were further analyzed in terms of revenue generation and community financing of various health care components Lessons learned showed that child survival activities depend largely on the involvement of the community and its leadership in conjunction with effective transfer of technical skills
EVALUATION TEAM
TaIm Mm atl Affliation
Florence AO Ebanyat MD DPH MPH Assistant Director of Medical Services (MCHFP) MOH GOU Entebbe Uganda
Ben 0 Osuga AMR DCH Technical Advisor UCBHCA OXFAM - Uganda Program Entebbe Uganda
Pamela Kerr RN MPH (Candidate) Program Development Officer WVRD Monrovia California
Lisa Rendon MSPH Intern WVRD Monrovia California
Juma Nabembezi MD DPH DTCH Project Coordinator AMREF Entebbe Uganda
David Newberry Consultant - Team Leader Global Consultants Atlanta GeorgiaIV BACKGROUND
A Project Background
Early in 1989 World Vision Uganda completed a needs assessment survey in Bundibugyo district The main assessment objective was to identify the health problems of women and children living in under-served rural communities of western
6
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
Uganda A matching grant USAID-WVRD CSP proposal was developed in conjunction with the longer-term objectives of the GOU Ministry of Health The project was approved and the Detailed Implementation Plan (DIP) was developed jointly with various officials including the District Health Officer of Bundibugyo district World Vision agreed to implement the CSP in the northern half of the district known as Ntoroko County The German NGO GTZ was assigned to cover the remainder of Bundibugyo district The CSP was approved for matching grant support by USAID through its Bureau for Food for Peace and Voluntary Assistance Office of Private and Voluntary Assistance (FVAPVA) Actual start-up activities began in 1989 implementation in all three impact communities serving about 24000 beneficiaries commenced in 1990 A midterm evaluation was conducted in September 1991 A pla of action was drawn up for review and implementation of the recommendations of the midterm evaluation report to consolidate achievements and to improve CSP efficiency
B Project Location
The CSP serves a population of 24250 as estimated from the 1991 Population and Housing Census of Uganda The CSP is located in Ntoroko County and operates in the northern part of Bundibugyo district Ntoroko County is divided into three subshycounties Rwebisengo Karugutu and Ntoroko A project-based operational headquarters was established at a central point location in Karugutu An acting project manager and 18 implementation and support staff provided basic project implementation services to all communities Each of the three project locations has an area coordinator (AC) and a core WV team Each of the impact sub-counties has different geographical characteristics Karagutu lies in a mountainous terrain Ntoroko is located beside Lake Albert and Rwebisengo is situated on a low-lying grassland plain All the impact areas have potable water needs that must be addressed through three different approaches
C Population Characteristics
The most recent census data show a total of 24250 persons in the three sub-counties served by the BCSP Each of the three communities has distinct physical cultural and social features The people living in the Rwebisengo area are nomadic by nature and widely dispersed Tribes include Batuku Bamba and Batoro These tribes are mostly traditionally dependent on cattle a few fishermen live in one village The Rwebisengo population is 13592 of whom 525 are children under one year of age and 76 are between 12 and 23 months
Karugutu has a more stable but mixed population of Bamba Bakonjo and Batoro tribes These are mostly small-scale farmers who live in widely separated compounds in the mountains They are quite comfortable living on and farming small nearly vertical plots The census population is reported as 7792 of whom 66 are children under 12 months
Ntoroko is basically a fishing community located on the shore of Lake Albert A fair segment of the male population resides on several large islands during the major
7
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
fishing season There many ethnic groups among these nomadic people The total population is nearly 3000 persons subject to temporary migration Ntoroko is often isolated due to poor roads and heavy rains during the wet season
D Tarpet Groups
The DIP stipulated emphasis on children under five years of age and women of childbearing age (WCBA) 15-49 years World Vision has primarily implementedstrategies through health education training and direct support of government activities The midterm evaluation reported substantial progress on EPI nutrition ORT and water and sanitation activities It further identified the progress achieved in creating awareness through active involvement of political units such as the RCs It also cited the BCSP for its work the communities the MOH and other NGOs in the area The final evaluation team confirmed these findings and found even geater achievements particularly in the degree of community and individual household involvement in the interventions
V FINDINGS
A Midterm Achievements
The overall goal of the BCSP is to reduce mortality and morbidity among children 0-59 months due to vaccine-preventable diseases dehydration from diarrhea and malnutrition The MOH has the lead role in providing services and assigningprofessional staff to the impact areas The midterm evaluation report documented considerable achievements and progress on EPI nutrition ORT and water and sanitation activities It found a well-trained infrastructure to support and implementCS interventions In particular the active involvement and support of the local political unit-the RCs-and the grass-roots level of household participation were found to be effective means of modifying human behavior Although the project was delayed in getting started in all three impact areas the momentum in communityparticipation was seen as a superb achievement The objectives and achievements reviewed during the midterm evaluation include
Objeclves
ruk Afllnm 1 Fully immunized at lt 12 months 70 27
2 Immunize WCBA with T2 50 29
3 Reduce malnutrition rate among children 0- 35 months 50 Not Measured
4 Reduce the number of deaths due to diarrheal dehydration 60 8 deaths reported
8
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
Task Objectiv
5 Mothers of children lt5 years know how to correctly prepare and use ORT for diarrheal dehydration 50 91 and 85
6 Increase the number of couples using a modem method of family planning 30 4
7 Train TBAs and CHWs 66 CHWs 66 trained 56 TBAs 28 trained
8 Increase the number of homes with latrines 30 80 mean for2 project areas
B Project Design-Implementation Plan and Funding
1 PhWi High-Risk Groups
RC leaders and other community members participated in enrolling families with high-risk individuals The definition for high risk was any segment of the population with a greater than average danger of developing one or more of the targeted diseases WVU considered the following groups high risk
a Babies born lt2500 grams weight or grossly small for gestation age
Children of weaning age identified as malnourished or who fail to gain weight Children with recurrent diarrhea
Children with one or both parents who have died because of war or AIDS
aMothers below 16 and above 45 years of age Pregnant mothers with anemia malaria or history of spontaneous abortion
2 Sbu for Immuniations
The BCSP will assist the Uganda National EPI through training of staff furnishing cold chain equipment establishing static and outreach centers and providing transport for immunization scouts Each infant born in the impact communities will be enrolled in a vaccination register and followed until fully immunized Appropriate intervals between doses and correct age for immunizashytion will be monitored monthly Review of cards from a few children by spot check will determine status by age and interval A baseline survey was scheduled to determine present knowledge and attitudes as well as current practices on immunizations and tetanus toxoid
Additionally major presentations regarding CS activities will be made during market days during which vaccination teams will address the people and offer
9
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
immunizations to children and mothers Passive and sentinel surveillance
mechanisms will be established to monitor trends of morbidity and mortality
3 Sftlcg for Dliffeal DLiwNsa
Bundibugyo district has not been targeted for ORT promotion by governmental organizations or NGOs The baseline survey determined that 25 of the mothers in Karagutu village had heard of ORT (Dolozi) and its use rate was about five per 100 diarrhea episodes Combined ORS sachets and home-based sugarsalt solution (SSS) were established as the basic remedial approach to treat dehydration In addition home-based fluids such as tea and porridge were encouraged The use of fruit juices and sugar cane juice was also encouragedThe rate of diarrheal diseases was found to be Io r at the midterm evaluation than the baseline prevalence rate Behaviors targeted for health education include
Early replacement of fluids bull Referral of complicated diarrhea
Continued breastfeeding and catch-up feedingLinkage between diarrhea and fecal contamination
Prevention of diarrhea by hygienic means and safe water
4 Strategy for Ntriional improwmntU
Three percent of the children were estimated to suffer from malnutrition according to UNICEF data The BCSP baseline survey showed a 44 rate of malnutrition based on 80 of children below standard weight for age During the final evaluation a team member suggested that height for age might be a better indicator as severe stunting has been reported in parts of UgandaRegular and routine weighing of infants and children will be the main activity for growth monitoring The project would especially target malnutrition associated with childhood illnesses infection and diarrhea Major efforts targeted to improve nutrition include
Growth monitoring especially for children lt3 years malnourished and high-risk groups
Education of mothers on nutrition improvements in children with emphasis on breastfeeding and weaning practices
Motivation of household members to plant gardens to provide improved
basic food supply
5 Sftgy for BhO Spacing
The project includes a birth-spacing component with particular focus on modern contraceptives The baseline survey showed 1out 60 households reported using the pill Natural methods such as breastfeeding withdrawal and abstinence are traditionally accepted means of birth spacing The BCSP will train 50
10
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
CHWs and 50 TBAs in birth-spacing promotion One constraint noted during the midterm evaluation was that family planning commodities and supplies from the MOH are limited The child spacing component also targeted mothers through health education and training sessions associated with other intervenshytions
6 0wer Ilae uiosw
Prevention of disease through cleaner environment and safe disposal of human waste was established as a basic community need These interventions were developed from baseline survey findings The project elected to include a strategy for promotion of latrines and to provide potable water without the use of USAID funding That part of the project would be accorplshed by compleshymenting local and community efforts and those of political authorities Other NGOs including WHO and UNICEF collaborated with World Vision in developing activities that complemented the ORT intervention by establishing basic prevention measures Extensive training and close supervision of community-based workers and volunteers was the main focus for construction of latrines and the provision of potable water Treating diarrheal diseases with properly mixed ORT continued breastfeeding use of home fluids and supplemental feedings were also encouraged Mothers were instructed to watch for signs of dehydration associated with serious consequences from diarrhea
C Project Funding
The midterm evaluation reported that funding for the BCSP was 53 spent ($354885) as of August 31 1991 These amounts included recurrent and indirect costs and were based on the total planned budget at the country level of $667940 USAID provided $510000 with a matching fund of $157940 from World Vision While actuai bookkeeping and accounting mechanisms for deliberate calculations of cost per intervention have not been established by USAID most Child Survival projects attempt to provide an estimate of categorical expenditures Recurrent costs can provide an estimate for the projected costs that will be required for each intervention to be maintained satisfactorily The final evaluation team attempted to assess the costs of various components Although a recommendation that emerged from the midterm evaluation was to begin to track costs by intervention it was still not possible to trace actual recurrent costs by intervention at the time of the final evaluation However computed cost estimates included the following categories salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentalutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation
Table 1 displays estimated intervention cost per beneficiary
11
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
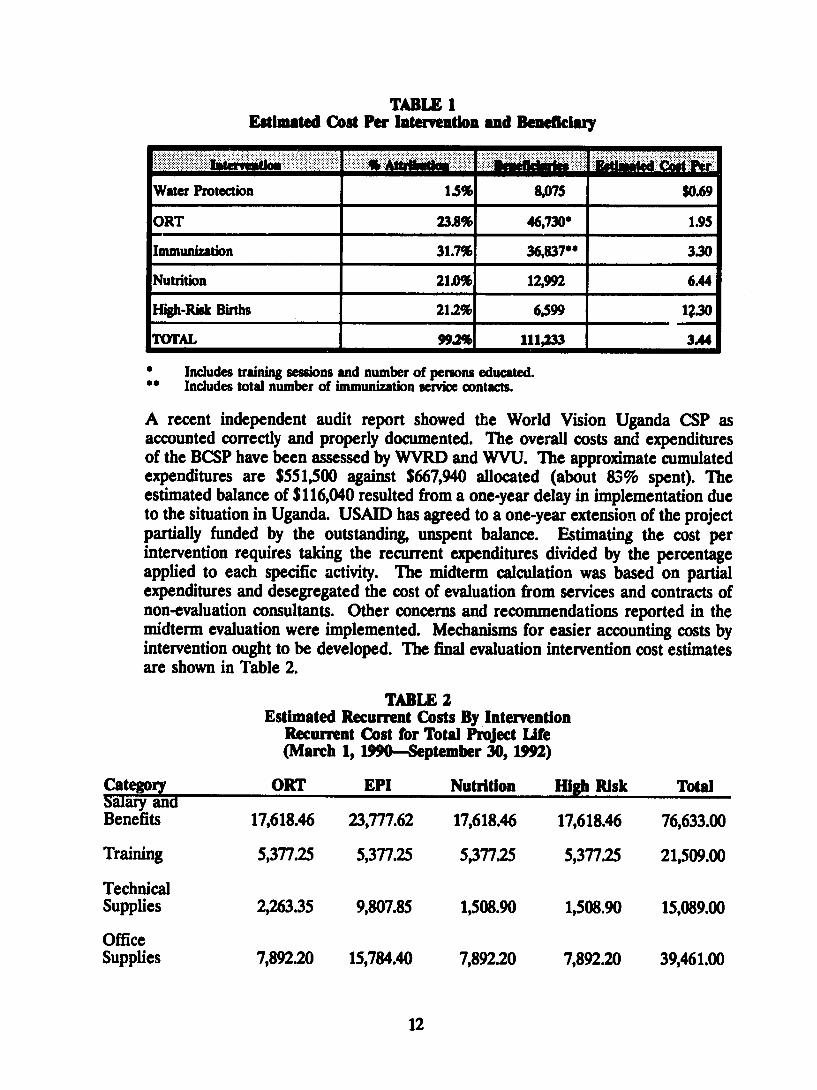
TABLE I Estimated Cost Per Intervention and Beneficary
Water Protection 15 8075 $069
ORT 238 467300 195
Immunization 317 3683700 330
Nutrition 2101 12992 644
High-Riok Births 2121 6599 130
TOTAL 992 111233 344
Includes training sessions and number of persons educated Includes total number of immunization service contacts
A recent independent audit report showed the World Vision Uganda CSP as accounted correctly and properly documented The overall costs and expenditures of the BCSP have been assessed by WVRD and WVU The approximate cumulated expenditures are $551500 against $667940 allocated (about 83 spent) The estimated balance of $116040 resulted from a one-year delay in implementation due to the situation in Uganda USAID has agreed to a one-year extension of the project partially funded by the outstanding unspent balance Estimating the cost per intervention requires taking the recurrent expenditures divided by the percentage applied to each specific activity The midterm calculation was based on partial expenditures and desegregated the cost of evaluation from services and contracts of non-evaluation consultants Other concerns and recommendations reported in the midterm evaluation were implemented Mechanisms for easier accounting costs by intervention ought to be developed The final evaluation intervention cost estimates are shown in Table 2
TABLE 2 Estimated Recurrent Costs By Intervention
Recurrent Cost for Total Project Life (March 1 1990-September 30 1992)
Category Salary and
ORT EPI Nutrition High Risk Total
Benefits 1761846 2377762 1761846 1761846 7663300
Training 537725 537725 537725 537725 2150900
Technical Supplies 226335 980785 150890 150890 1508900
Office Supplies 789220 1578440 789220 789220 3946100
12
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
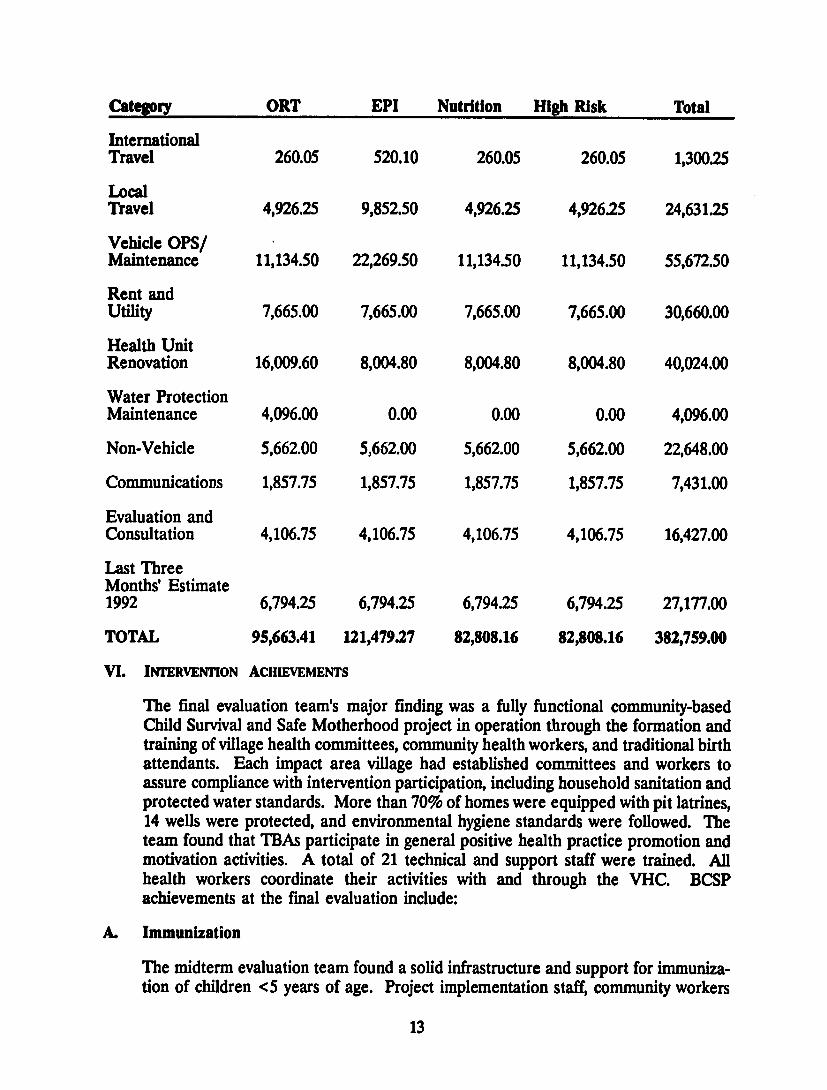
Categmoy ORT EPI Nutrition High Risk Total
International Travel 26005 52010 26005 26005 130025
Local Travel 492625 985250 492625 492625 2463125
Vehicle OPS Maintenance 1113450 2226950 1113450 1113450 5567250
Rent and Utility 766500 766500 766500 766500 3066000
Health Unit Renovation 1600960 800480 800480 800480 4002400
Water Protection Maintenance 409600 000 000 000 409600
Non-Vehicle 566200 566200 566200 566200 2264800
Communications 185775 185775 185775 185775 743100
Evaluation and Consultation 410675 410675 410675 410675 1642700
Last Three Months Estimate 1992 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 8280816 8280816 38275900
VI INTERVENTION ACHIEVEMENTS
The final evaluation teams major finding was a fully functional community-based Child Survival and Safe Motherhood project in operation through the formation and training of village health committees community health workers and traditional birth attendants Each impact area village had established committees and workers to assure compliance with intervention participation including household sanitation and protected water standards More than 70 of homes were equipped with pit latrines 14 wells were protected and environmental hygiene standards were followed The team found that TBAs participate in general positive health practice promotion and motivation activities A total of 21 technical and support staff were trained All health workers coordinate their activities with and through the VHC BCSP achievements at the final evaluation include
A Immunization
The midterm evaluation team found a solid infrastructure and support for immunizashytion of children lt5 years of age Project implementation staff community workers
13
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
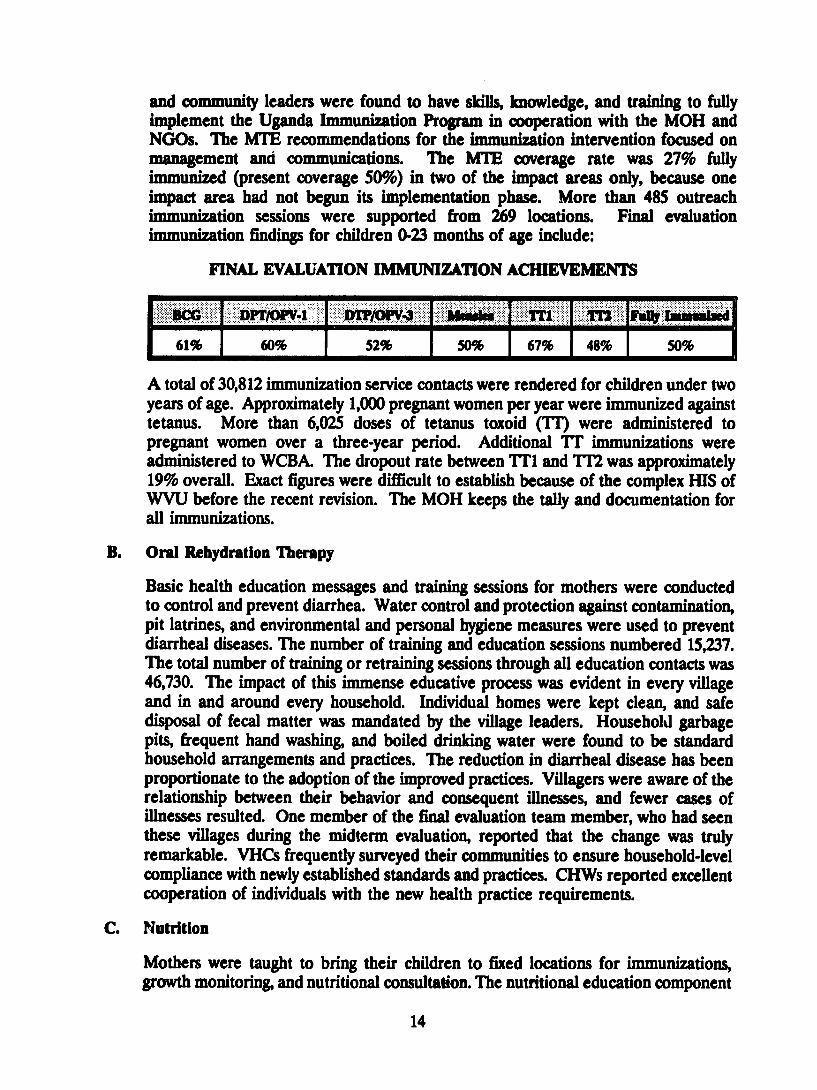
and community leaders were found to have skills knowledge and training to fully implement the Uganda Immunization Program in cooperation with the MOH and NOOs The MTE recommendations for the immunization intervention focused on management and communications The MTE coverage rate was 27 fully immunized (present coverage 509) in two of the impact areas only because one impact area had not begun its implementation phase More than 485 outreach immunization sessions were supported from 269 locations Final evaluation immunization findings for children 0-23 months of age include
FINAL EVALUATION IMMUNIZATION ACHIEVEMENTS
RC DTII1 DTP~4 Msl ~ Tfl FmiwImaulu
6H 60 52 50 67 48 50l
A total of 30812 immunization service contacts were rendered for children under two years of age Approximately 1000 pregnant women per year were immunized against tetanus More than 6025 doses of tetanus toxoid (TI) were administered to pregnant women over a three-year period Additional TT immunizations were administered to WCBA The dropout rate between T1 and T172 was approximately 19 overall Exact figures were difficult to establish because of the complex HIS of WVU before the recent revision The MOH keeps the tally and documentation for all immunizations
B Oral Rehydration Therapy
Basic health education messages and training sessions for mothers were conducted to control and prevent diarrhea Water control and protection against contamination pit latrines and environmental and personal hygiene measures were used to prevent diarrheal diseases The number of training and education sessions numbered 15237 The total number of training or retraining sessions through all education contacts was 46730 The impact of this immense educative process was evident in every village and in and around every household Individual homes were kept clean and safe disposal of fecal matter was mandated by the village leaders Household garbage pits frequent hand washing and boiled drinking water were found to be standard household arrangements and practices The reduction in diarrheal disease has been proportionate to the adoption of the improved practices Villagers were aware of the relationship between their behavior and consequent illnesses and fewer cases of illnesses resulted One member of the final evaluation team member who had seen these villages during the midterm evaluation reported that the change was truly remarkable VHCs frequently surveyed their communities to ensure household-level compliance with newly established standards and practices CHWs reported excellent cooperation of individuals with the new health practice requirements
C Nutrition
Mothers were taught to bring their children to fixed locations for immunizations growth monitoring and nutritional consultation The nutritional education component
14
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333
was used in motivating households to grow home gardens and to encourage better food consumption by pregnant women and children Training in the correct interpretation of the growth curve for infants and eating for two concepts were highlighted TBAs play a key role in the growth-monitoring intervention Newborns are registered by the CHWs for immunization while both TBAs and CHWs cooperate with parents to encourage supplementary feedings at four months continued breastfeeding and growth monitoring The MTE recommended reassessment of the nutrition objective and a better data collection system for monitoring growth
WVU initiated a plan of action in response to the MTE Both the nutrition and child spacing components should be clearly defined during the extension phaseFollowing the MTE efforts to improve the nutrition intervention were begun There was no accurate baseline for malnutrition incidence Food supply is seasonal in most of the impact areas while traditional beliefs discourage any crop experimentation Food supply is sporadic and even more costly because of expenditures for transportashytion The BCSP documented 1613 nutrition service contacts by the end of the threeshyyear project
D Birth Spacing-High-Risk Births
The DIP objective was to increase the number of couples using modern methods of family planning to 30 The strategy for achievement involved training CHWs and TBAs and educating and motivating couples to adopt modern FP methods The midterm findings showed positive training achievements and high interest generated through focus discussion groups The government of Uganda has established FP criteria that make full implementation of village-level child spacing intervention difficult to implement A physical examination is required for some modern birth control devices The MOH has responsibility for the supply and distribution of FP commodities and services The BCSP conducted 6549 child spacing sessions duringthe three-year phase The rate of FP receptors is estimated to be 4 Familyplanning awareness greatly increased but service delivery is erratic Karagutu now has a dispensary that offers these services but it depends on delivery by the DMO Other areas must still rely on going to Fort Portal or natural methods
Mens attitudes towards family planning have improved greatly The majority of men in the community support family planning methods and are willing to use at least natural child spacing measures A few men still do not agree with the goal of familyplanning and some women continue to have large families to compete with their husbands other wives
E Maternal Death
The general purpose of this intervention objective was to reduce mortality amongWCBA More specifically it was to reduce mortality related to births that could have been identified previously as high risk or completely prevented through familyplanning measures and immunization The quantitative objectives are as follows
15
1 Immunize 50 of pregnant mothers with TI 2 Increase to 30 the number of couples using a modem FP method
Several input mechanisms contributed toward achievement of these objectivesDistribution of contraceptives and training of TBAs were undertaken by the Ministry of Health-Uganda Training sessions for CHWs included facets that promotedmodem family planning as well as breastfeeding and other natural methods The final evaluation team identified the following achievements
Sixty-one CHWs and 74 TBAs were trained in promotion of family planning The TBAs have had more extensive training in the identification of high-riskmothers However they lack TBA kits and referral facilities are located 45 minutes away by car
World Vision has provided its vehicles to serve as ambulances for obstetric emergencies which has been very effective in reducing the maternal mortality rate A review committee should be established to review each emergency evacuation to determine better solutions Communities need to conduct a caseshyby-case review of the referral and emergency transport system and to developlong-term solutions
While there is a tremendous amount of knowledge regarding the importance of child spacing implementation of this knowledge through the use of familyplanning has been minimal (See household interview survey for percentage of women practicing) This minimal implementation level seems to be largely attributed to the erratic availability of contraceptives This service is the basic responsibility of the MOLGMOHDMO in Bundibugyo
The immunization of WCBA with a second dose of tetanus toxoid has reached a 484 (25185207) coverage rate
Africa - Maternal Mortality
The annual number of maternal deaths in Africa during 1985-1990 was 150000 This figure accounted for 30 of the worlds 500000 deaths that occurred annually in this time period For African women the lifetime risk of dying from pregnancy-related causes is I in 24
Uganda - National Level
Because the registration of births and deaths is grossly deficient it is extremelydifficult to estimate the maternal mortality rate (MMR) for the country Based on Kampala hospital statistics the MMR is 265 per 100000 live births2 Further
World Health Ornization MATERNAL MORTALIY FACT SHEET 1987
Kampikaho A MATERNAL MORTALITY IN FIVE KAMPALA HOSPITALS 1980-1986
Master of Public Health Thesis Universty of Sydney Australia Februaiy 1988
16
2
complicating the estimate for the country is the fact that most deliveries take place outside a health facility within the home of the mother or the TBA UNICEF (1989) estimates that only 26 of women deliver in health facilities a statistic that varies across regions In a report published by the Ministry of Health 3 14 districts (not including Bundibugyo) submitted a figure of 91 deaths per 23655 live births for the year 1990
Regional Level
Two hospitals Virika and Buhinga were contacted for data regarding maternal death in Fort Portal While Fort Portal is not in Bundibugyo district it is more accessible than the hospital in the city of Bundibugyo At Virika between June 1991 and September 1992 24 maternal deaths were recorded Unfortunately there were no cumulative totals for births and staff was unavailable for an estimate At Buhinga records were analyzed from January 1992 to September 1992 Of 542 live births 13 ended in maternal death Causes of death included hemorrhage anemia sepsis cervical cancer induced abortion obstructed labor placenta previa ruptured uterus eclampsia and AIDS-related complications
Project Impact Area
A total of 68 maternal deaths was estimated for the year before the project started Since the project began there have been no maternal deaths recalled Data were based on informal interviews with 17 CHWs and 5 TBAs Before BCSP women were usually carried to the roadside by homemade stretcher and the family waited for transport
VII SURVEY AND INExViEW RESULTS
One surprising outcome of the WVU CSP implementation was the spontaneous formation of income-generation groups These evolved from focus groups formed for health education and information-enhancement purposes These are mostly groups comprised of women Representatives from VHCs expressed great interest in starting additional groups for fund-raising and income generation to raise money for health promotion and to provide treatment services Income-generation group interviews are summarized below Most women do some type of agricultural work Their produce is usually sold at the market This money is then spent by the women for the families needs A small percentage of women have no access to money and rely completely upon their husbands
Health Planning Unit Ministry of Health-Uganda HEALTH INFORMATION QUARTERLY Vol 8 No 3 Sept 1991 Health Education Printing Unit Entebbe 1991
17
A Results of Interviews with Income-generation Groups
b Number of groups interviewed - 7 Period of operation - Between 5 months and 3 yearsAverage membership - 30 (range 6 to 70 members)Group initiators Mainly key persons from VHCs or CHWs
2 Group Objetie
bull Improved socioeconomic and health status of families Union for common purpose Forum for exchange of ideas on health and developmentImplementation of other interventions as may be determined
3 Saegies to Achive Objecties
Cattle raisin and sale of milk Poultry farmingFund-raising borrowing and lending money among group membership (revolving loan scheme)
Brick production and sales Bee-keeping and sale of honey products
bull House construction and rental Buying and selling treatment drugs Buying and selling hides and animal skins Handicraft production and sales
4 Achewments
The groups interviewed were at different levels of achievzment of their various objectives Achievements attained include
40 acres of land purchased bull 240000 shillings raised by individuals in the groups
Funds established for purchasing cattle and sewing machines bull Reserve funds established for loans to members bull 20000 bricks produced and ready for use by two groups
50-plus chicken flock with egg production and sales 10 or more cows purchased for meat and dairy products
Groups used as forums for idea exchange and community development
Health education sessions were also conducted
S Conhthas
Some of the major constraints cited by members of income-generation groups interviewed include
18
10 Need for technical support and advice in establishing market outlets for products and use of acquired resources Lack of credit facilities and capital for projectsLack of equipment
bull Need for structures to house members for meetings and productionfacilities
6 Fuarw C
Groups will continue to raise funds among themselves and interested investors to purchase scheduled equipment items such as sewing machines and ox ploughs Other plans include
Construction of shops and rental units Purchase of grinding mill Request for technical assistance on IGA farming methods and marketing of local productsAcquisition of loans from World Vision and other PVOs to finance planned projects Tanning hides production of leather and other tannery products
B Interviews with 90 Mothers of Children Less Than Three Years of Age
1 General Findings The interview form used with mothers of children less than three years of age can be found in Annex B
The average household size was comprised of six persons Parents reported an obvious decline in morbidity and mortality associated with diarrhea and the usual childhood vaccine-preventable diseases during the project Mothers showed a noticeable improvement in their household sanitation and in basic knowledge about health Mothers reported that the project should consolidate the present activities and interventions and would also like to see additional assistance in the provision of maternity services and ambulance or emergency transport services to meet transition community needs Other ideas expressed include
bull Train more CHWs and TBAs Provide pediatric curative services Provide primary school education Include income generation activities
Mothers reported that immunization activities health education and protected water supply are all sustainable functions of the CHWs TBAs and VHCs
2 Knowledge about ImmwAiaon Of the six childhood immunizable diseases identified by UNEPI 956 of mothers mentioned measles 778 mentioned polio 744 mentioned whooping cough 856 mentioned tetanus 53 mentioned tuberculosis and
19
233 mentioned diphtheria The majority of mothers knew that Tr protects either mother child or both from the disease Ten percent knew that TI protects the mother from tetanus 156 knew that TT protects the baby from tetanus and 578 knew that IT protects both mother and baby Only 166 of mothers did not know its use A total of 876 of children had a BCG scar Sixty-six percent of mothers knew that measles vaccine is given at nine months a smaller percentage of mothers 378 knew that the first dose of polio vaccine is given at birth or within the first week of life
3 Knowledge of Ceuutiu of Dkanhml Divuse (CDD) Mothers were questioned about the last episode of diarrhea in the household 71o occurrence of diarrhea as recalled by the mother was 588 These episodes included bull 623 that occurred within the last four months
283 occurred within 5 to 12 months 94 that occurred more than one year ago
The rate and number of diarrhea episodes have been dramatically reduced especially when analyzed by age of children Only half of these diarrheas occurred in children less than 18 months in age while nearly 87 occurred in the cohort under 5 years of age Local families thought that bilharzia dysentery was responsible for some of the diarrhea in Ntoroko Pit latrines were actually observed in 90 of homes
The majority of mothers 944 gave ORT (ORSSSS) when their child had diarrhea and 878 knew that ORT was for prevention of dehydrationHowever fewer mothers (323 1561 and 67 respectively) mentioned continuing with breastfeeding increasing feedings in the recovery stage and ensuring proper hygiene when a child has diarrhea Few mothers took their children to a clinic (44) or gave drugs (10) during episodes of diarrhea Such findings show great gains in behavior at the household level regarding CDD and diarrhea treatment
Although the majority of mothers 944 gave ORT to a child with diarrhea some mothers did not know how to correctly mix SSS While tumpeco mugs were found in most households teaspoons for measurements and treatment were scarce Only a few mothers used other home-based ORT such as pineapple juice or porridge All mothers practiced breastfeeding and 911 started weaning at 3-6 months A total of 90 of mothers fed the weaned babies 3-4 times a day
4 NuampWxon Knowledg and Grewtamp Meding
Eighty-six percent of mothers had growth-monitoring cards The survey found that growth monitoring and charting was irregular and was done only during the first year of life while the child was still being immunized Few mothers could
20
correctly interpret the growth chart However most of the children seen appeared well nourished Most mothers monitored the growth of their children by
Physical appearance-fat or healthy lookingbull Good appetite--eats well
Desire to play-activitybull Use of bracelets around ankles wrists and waist that show tightness when
weight gains occur
5 Kxowledge ofAnuiatal Care (ANC) aud PP Services
The majorit- of mothers had a maternal tetanus toxoid card (744) and the majority of expectant mothers had received ITcoverage Tetanus toxoid coverage of WCBA was not assessed
Although 972 of mothers expressed interest in using child spacing services only 22 were using a modern method the pill Reasons for not using services include
bull Side effects Services not available (661)Using natural method abstinence or rhythm (306)
bull Not aware (1811) Currently pregnant (83)Spouse refusal (56)
6 Thansion Disease Problems
During the interview the following diseases were identified (in the order of magnitude) as the most serious health problem in that household
a Malariafeverb CoughASIC Diarrhea d Backache e Worms f Scabies g Iyphoid
hilharzia Whooping Cough
j Tuberculosis
7 Health Evendtww for the Most Racen Household lness
The average expenditure on curative services during the most recent illness was 8622 Uganda shillings per household Three households experienced extreme illness that required long-term and expensive care When the data were adjusted for these illnesses the average health care expenditure was 5500
21
shillings The money was spent for treatment of cough malaria TB typhoid
and bilharzia
8~Gwnrl Obserathm
Diarrhea episodes in children have declined due to increased awareness among mothers about diarrhea through health education In addition the majority of homes have good sanitation coupled with the high immunization coverage that prevents diseases such as measles that cause diarrhea Mothers management of a child with diarrhea is up-to-date with ORT but mothers should be encouraged to continue breastfeeding giving more foods and ensuring proper personal and food hygiene and good sanitation
There is a need to make teaspoons available to mothers if they have to correctly mix SSS In addition mothers should be encouraged to use other home-based ORT where available such as porridge rice water banana and pineapple juice and sugarcane juice
While the prevalence of malnutrition appears low growth monitoring should be extended into the community by giving CHWs weighing scales instead of keeping weighing scales only at health units and immunization outreach stations Mothers will easily take their child to CHWs for growth monitoring even after the child has completed the course of immunization
Emphasis should be placed on prevention of the common diseases since they are generally preventable Drugs for the treatment of common diseases could be made available at a village pharmacy Drugs could also be provided to CHWs as an IGA for treating patients who are far away from a health unit either in the mountains in Karugutu or the ranches in Rwebisengo
C Interviews with Community Health Workers
A total of 19 CHWs were interviewed (See Annex C for interview form) These workers had served from 15 to 3 years Their weekly workload ranged from 94 households visited to as few as 18 (average was 52 per week) CHWs ranked their workload from 70 to 100 homes The amount of time spent in each household varied from one to two full hours Training was provided by the WVU CSP staff and in conjunction with the MOH Training was given in categories as follows
Educating on health Immunization Family Planning bull Growth Monitoring ORS Breastfeeding Nutrition Hygiene and Sanitation
bull Safe Water Mobilization and Promotion
Workers listed the chain of responsibility as beginning with the Village Health Committee or Resistance Council to the World Vision project staff and then to the community Support was provided by the VHC and RCs with assistance from WVU The VHCs were particularly effective in providing assistance in difficult homes
22
World Vision was perceived as strong in providing education training knowledge and resources such as bicycles boats and lunch Pliowance Workers reportedspending one to three hours per week keeping reccitds Records were maintained by18 of the 19 interviewed CHWs kept the follawing rosters
Household Rosters 18 Vital Events Roster 18
bull Child Health 3 P Immunization Defaulters 3
The CHWs attended VHC meetings about two times per month Disposition of records
Eighteen submit to supervisorMonthly meetings are arranged to discuss results
bull Seven discuss records with VHC (community)bull Three reported using information for follow-up and baby tracking
A total of 19 CHWs reported that the VHC supervised their work in one form or another by home visits by endorsing reports by assisting in follow-up household visits and by asking the community about CHW performance Constraints identified during the CHW interviews included bull Poor road network to houses-in some the travel distance is long and difficult
even on a bicycle
bull Communities expect too much (food money drugsetc)
bull Resistance to behavioral change is occurring-harmful cultural practices continue
Too many households to monitor
Lack of supplies-medicine family planning etc CHWs sometimes use their money to buy items
Lack of pay for considerable activity and effort
Eighteen CHWs said they would continue to work after the project phased out One said he would not continue but felt the community would spread the knowledge
D Interviews with Village Health Committees
General
1 In Karagutu subcounty 61 VHCs have been trained Eight of the 61 were interviewed (131) The interview form used is in Annex D
Membership on the VHC was by direct open vote of the community Most members have served about one year Major VHC duties include
23
Pbull Planning implementation and evaluation of project activities Participating in meetings and home visits Traininp and health education activities Reviewing reports submitted by CHWs and TBAs Providing feedback to the community-at-largeAssisting in ensuring individual compliance with health standards and practices
2 Meetings are conducted monthly or as needed to identify and resolve health probleirs establish priorities and assist intervention implementation The major role of the VHC is to motivate the community to participate in health care practice preventive health behaviors ensure health care and serve as the focal group for completing projects The ViCs assure materials labor and organization for community construction projects VHCs provide maintenance of water sources supervise CHWs and TBAs and assist in the health education process
3 The VHC has had a dramatic impact on village health practices and environshymental hygiene standards Immunization compliance has greatly benefited from VHC assistance in tracking defaulters Other interventions related to child and maternal health have profited from VHC input
4 The VHC has exercised a lead role in safe water development and assisted in nutrition activities ORT and CDD control are areas in which the VHCs have functioned very well to achieve better community understanding for the conditions contributing to these problems and their control
5 The VHCs expressed the need to continue after the project closes but felt that limitations would naturally result if the CSP were terminated too early They requested additional training assistance in income-generation activities and health education before taking over full responsibility for community health activities
Strengths of VHC
1 Good in support of health education and income-generation activities- also conduct educational activities
2 Helpful in communicating mobilization and cooperation3 Support work of CHWs
Weaknesses of VHC
1 Irregular attendance and failure to call meetings2 Need more training3 Not endorsing monthly reports4 Expect payment from WV such as CHW compensation boots lunch allowance
and bicycles5 Low motivation
24
Observations
1 There is a gap between the CHWs and the VHCs because the CHWs are provided with both material and financial support The VHCs feel entitled to such support and resources
2 The VHCs interviewed expressed concern about not having adequate office supplies including stationery for keeping notes and minutes of meetings They are also interested in adult literacy training as part of the VHC training options
3 The VHCs used information received from the CHWs TBAs and communities overall to establish health needs They prioritized projects but due to limited resources they felt constrained in responding to mnlor problems identified
4 CHWs reported that the VHCs supervised their work in one form or another by home visits endorsing reports follow-up visits and asking the communityabout CHW performance
E Interviews with Traditional Birth Attendants
1 Of 74 TBAs trained 12 were interviewed (162) (See Annex C) The age range was from 24 to 60 years and their length of service was from 10 to 33 years These TBAs attended from five to ten deliveries per month Most spent one or two days a week visiting five to ten homes The main TBA activities include antenatal care nutritional counseling and advising childbearing women regarding MCHFP They kept records of deliveries referrals and cases seen
2 Those interviewed had received adequate training and were well prepared for their tasks All were committed to continuing to practice after the WV project was completed Many felt their workload was increasing due to referrals from untrained TBAs in the community TBAs rtported they were responsible to the community and supervised by their VHC but reported though the CHW Most attended VHC meetings at least once a month Many reported that VHC members participated in the house-to-house visits The TBAs participated in health education and training activities
3 The training of 74 TBAs is greater than the set target of 50 It was noted that the age range of those trained included a fairly high percentage of elderly women
4 The TBAs are devoted to their work but once they are trained by WV they are no longer paid the TBA fee-for-service because the villagers believe they are paid by the project Untrained TBAs on the other hand continue to be paid service fees
5 None of the TBAs interviewed had kits Many did not have gloves or any other protective garments They identified a need for some suitable lying-in shelter for conducting deliveries All the CSP communities are isolated from any type of maternity facility
25
6 While many of the TBAs are not literate they are assisted by family members in recording their activities Those interviewed complained that they had no means for storing these records and loss or damage by insects and rodents was a common problem
7 While training has improved their skills most TBAs reported concern regarding the lack of adequate referral service in face of increasing workloads All were aware that there has been a dramatic reduction in maternal mortality
8 The degree of cooperation between the TBAs and VHCs was impressive They received and provided mutual support in health education motivation and mobilization for health care TBAs CHWs VHCs and community leaders specified that emergency obstetric transport and clinic faciliti - Were urgently needed
9 Generally the TBAs provided education messages on child spacing They were not directly involved in provision of family planning services or commodities The GOU restrictions regarding the need for physical examinations and other training requirements may have some bearing on this finding
F Interviews with World Vision Core Staff
1 General Findins
a Twelve of 19 core staff were interviewed in the field and three others were interviewed at WVU headquarters in Kampala (See Annex A for interview form used) Professional training totaled 345 years with a pershyperson average of three years All WV staff could correctly state the goals and objectives of the CSP More importantly all could specify their role in the process of reaching objective targets
b All staff had either annual or monthly work plans One support staff works without a plan due to the support nature of her activity
c More than 83 of the staff had been trained under the project Themajor training focus has been Training of Trainers (TOT) All 12 core staff reported a perceived need to have additional training in subjects such as computer skills statistics social mobilization training of trainers and MCHPH
d All collected data Most were involved in the analysis and presentation of feedback to the various levels of jurisdiction
e Clear perception of MOH and NGO involvement were reported Community leaders were described as actively involved in all phases of implementation Core staff felt that CSP activity should continue until a phased plan of action for consolidation and sustainability is completed
26
2 01wvatIon
a Additional training is needed for core staff for all levels of villageworkers and for community committee members No computer is assigned to the Karagutu facility No core staff person there has been trained in computer use
b Income-generation groups lacked credit access technical supportequipment appropriate skills for managing their own affairs and marketing know-how The WV core staff believed they lacked technical skills necessary to adequately support full-scale IGAs
c Most field staff are posted to hardship areas where their families Annot join them In at least two of these impact areas even basic food supplies are erratic and what is available is limited Product selection is based on profit (after transport costs have been added on)
d There is no formal process for training backup VHC members or trainingVHC replacements Concern was expressed regarding incentives given to CHWs but not to VHC members Incentives should be given to all or none
3 Constraints
a Several problem areas were identified by the WVU core staff
P Bad roads are often impassable
0 Travel is often difficult because few private transport vehicles pass between project areas and the field headquarters office at Karagutu
The DMO has not been able to provide full support to all intervenshytions especially family planning
There is still resistance to positive behavior change at the household level
Computerization of the field headquarters location is badly needed
bull AIDS ARI and other transition health needs are rapidly overtakingthe impact communities that have been most successful in controlshyling vaccine-preventable diseases
The most successful projects need greater flexibility to assist in the development of emerging community needs such as primary education safe water sanitation and maternity clinic facilities
b As communities mature in securing better health and improved environshyments their needs are more clearly focused on improvements in quality
27
of life which the project is not empowered to implement Food scarcity is a continual problem in some of the impact areas but agricultural assistance is technically not available
c World Vision is the only source of transport for emergency medical evacuation for obstetric trauma or other life-threatening illnesses
d Frustration was expressed with the growth-monitoring intervention as a means of eliminating severe malnutrition Staff felt that severe malnutrishytion due to poverty was particularly difficult to overcome Nutritional rehabilitationdemonstration centers have mixed success as treatment facilities Clients are often rehabilitated and require repeated treatment due to the basic problem of poverty
e Impact areas suffer from a lack of essential drugs and curative treatment options MOH facilities are under-served
f Children now thrive and survive as healthy youngsters They urgently need education (primary schooling) or run the danger of developing antisocial behaviors
G Interviews with MOLGMOH
Three MOLGMOH staff interviews were conducted Two interviewees were service providers and the other was general manager for all health services and activities within the Bundibugyo district (See Annex E for interview format) All were knowledgeable about the BCSP goals and objectives Each had participated in training in conjunction with the project They had significant roles in planning supervision and other support activities related to the project Post-training evaluation was used to determine performance and to assess impact activities The MOH perceived the WV BCSP activities as consistent and an important means of strengthening preventive health measures at the household level WV was givencredit for sharing information and monthly reports Sharing of resources between BCSP and MOLGMOH has been an important factor in this project World Vision was classified as excellent for immunization ANC maternity needs family planning and personal and environmental hygiene The MOH was less appreciative of the family planning services This was a reverse charge based on a lack of supplies The MOLGMOH stated that they would be able to sustain immunization FP nutrition maternity services training supervision and some supplies and essential drug needs
Officials recommended that WV BCSP continue for three to five years to further consolidate gains made during the first three years Officials would like to see the project expand IGAs and water projects and begin to develop agriculture and educational services The MOLGMOH would relax FP requirements and establish a regular supply of child-spacing commodities
28
H Interviews with NGOs
Two NGOs with linkages to the BCSP were interviewed (Anex F) Both were quite familiar with the goals and objectives of the project and provided extensive support and coordination The German NGO GTZ has linked directly with WV Uganda and communities to renovate repair and construct health facilities and clinics Collaborative efforts for water protection and health services were cited Both reported the obvious success of the BCSP based on positive feedback from the communities One NGO felt they could support immunization water and sanitation and some training once WVU phased over The NGOs were unanimous in recommending a five- to seven-year extension because this type of community developmental project requires time to consolidate and develop sustainable selfshysupporting activities
VIII SUSTAm ABrrv
A General
From observations made and interviews with various community-level resource persons it is likely that limited services and components will be sustained Training by staff members of the project and MOLGMOH will continue There is a need to augment the level of training to improve appropriate communication skills and community-based development approaches Training of trainers and facilitators will continue with input from outside sources to pay for the training while local communities and MOLGs could provide facilities Courses conducted under the auspices of the UCBHCA could be used to focus on improvement of communication and training skills and promotion of community development through self-reliance funding and determination
In the case of the BCSP all key staff had not completed the four-phase TOT series by the end of the initial project lifetime (time of final evaluation) The Project Manager could be given additional training through the UCBHCA and USAID Several appropriate training courses and BCSP-related topics were identified during the final evaluation exercise Core staff would benefit from the TOT course which would provide the opportunity to perfect program planning management monitoring and evaluation apart from communication skills Qualitative data from interviews reports surveys and evaluations clearly indicate a fairly high sustainability potentialof Child Survival benefits
B Sustainability Status
The USAID funding for the WVU CSP was scheduled to end on September 30 1992 Delayed initiation has resulted in unspent funds sufficient for a one-year no-cost extension (USAID has agreed to the extension) The project is presently viable to the extent that several key components would likely continue on a scaled-down basis The ultimate decision to phase out the BCSP lies with WVRD headquarters and USAID A new three-year extension proposal could be developed that includes wellshy
29
defined parameters to have major project responsibilities phased over during the next four-year period It is feasible to develop a sustainable Child SurvivalSafe Motherhood project in the WVU project impact area over a four-year period
C Loca PoliticalLeaders-Lo Capacity
Political groups and leaders of the Resistance Councils and local authorities have become deeply involved in the implementation of this BCSP in western Uganda Serious commitments to support the Child Survival and Safe Motherhood intervenshytions are well understood and the process to attain long-term support has begun The final evaluation team was approached by two political leaders who represented large segments of the impact communities They provided feedback to the team about how the CSP had changed the lives of their families the children and entire communities They related how deaths due to diarrheal and vaccine-preventable disease had all but disappeared They were able to trace the process that empowered them to make changes in the villages environment and practice preventive health behaviors at home The reason they approached the final evaluation team was to request further involvement in future CSP activities (especially if a project extension is granted)These leaders wanted to draw upon the process used to improve health to seek assistance in education developing safe water for all and learning skills that will assist them to do what the community needs with minimal external resources
These political and local leaders shared their concern about having healthy children who are not educated or even literate They knew that these children would eventually turn to antisocial behavior These leaders were concerned that agricultural development was neglected Therefore they requested that the final evaluation team make known their concerns and relay a request to expand and extend the projectThey pledge to learn new skills apply resources and phase over all responsibility for the project after careful preparation as long as they are involved in the planning from the proposal development stage Table 3 shows the resource commitment of WV Uganda MOLGMOH NGOs and local communities
TABLE 3 Community Resources Donated for BCSP
Appmsisaat CostteiM ft Upda SI
Bricks for health unit Storage for GTZ supplies 1265000
Health unit-Karagutu Building Tools
SAssume community will contribute 1265000 Health unit-Ntoroko same materials as Karagutu
PAssume community will contnbute 632500 Staff housin-Rwebseno similar goods but on a smaller scale
Three buildings for immunization outreach 3000 h x 3 x 36 months 324000
30
Appnauatacost
Four sites preserved for immunizashytion outreach 2000 sh x 4 x 36 months 288000
TOTAL VALUE OF RESOURCES _ 3774S00
D Estimated Recurrent Costs and Projected Revenues-CostBenefit
Recurrent costs can also provide an estimate for the projected cost that each intervention will require to be maintained satisfactorily Such costs estimates include salary benefits training technical supplies office supplies international travel local travel vehicle maintenancerepair rentutilities health unit renovation water protection non-vehicle maintenancerepair communication evaluation and consultation The 1990 fiscal year included recurrent costs for all DIP interventions and start-up costs for one impact area The cost distribution for FY90 is shown below
Fiscal Year 1990 (March 1--September 30 1990) Based on Activity Report
Gm 100hWI CODE OKF EPI Monit Ie
23 31 23 23 Salary and Benefits 559950 754726 559958 559958 2434600
25 25 25 25 Train[ 96050 96050 96050 96050 384200
Tecb and Office 40 30 15 15 Supplies 607400 455550 227775 227775 1518500
40 30 15 15 Travel 865800 649350 324675 324675 2164500
40 20 20 20 Water and Mic 298800 149400 149400 149400 747000
25 25 25 25 Repair of Non-Vehikle 527100 527100 527100 527100 2108400
25 25 25 25 Evalhatkl Consultants 31250 31250 31250 31250 125000
25 25 25 25Communkation 103750 103774 103765 103765 4150
Total (US$) 3090100 27672 20200 20200 98972
Except for evaluation and consultant costs the annual recurrent costs are approxishymately $100000 If nutrition is reduced in scope or eliminated as an intervention the per annum recurrent costs would range between $80000 and $100000 One of
31
these families could support all the interventions at the present level and activate other interventions for transition medical and social problems This is an overshysimplification but the fact remains that local authorities could identify key interventions to be continued and meet transition health and community needs
E Current Year Costs
Although exact expenditures for the current fiscal year are still being compiled an estimated $8153100 was spent for the first nine months of activities The recurrent costs for each of these months can be calculated at (815319) $905900 This figure multiplied by the monthly cost for the last three months added to the cumulative total yields the estimated cost of operation for FY92 The computed amount for the last quarter is approximately $2717700 Total FY92 expcnditures are calculated below in Table 4 Total project cost is shown in Table 5
TABLE 4 Fiscal Year 1992-Estimated
Subtotal (9 Months) 1933210 2553465 1687790 1978635 8153160
Estimate-Last Three Mouths 679425 679425 679425 67945 2717700
Grand Total 1992 2612635 3232890 2367215 2658060 108708
BCSP costs are reasonable given the location of the project the environment and the ability of Uganda to provide service to the project areas The capacity of the local structure to absorb future operational costs is contingent on time training and preparation of staff Other NGOs are not likely to fund WV Child Survival and Safe Motherhood interventions but local RCs and communities could provide this funding after suitable development The potential for income-generation projects to fund curative and preventive health activities is good The community leaders have expressed concern regarding associated community needs and issues such as education and agricultural development The GOU is not yet able to provide development services needed to meet the emerging and transitional social problems facing communities where children and adults are healthier and live longer The USAIDBCSP could serve as the basis for such development if it can be extended through a period of consolidation and if a new three-year proposal with adequate justification can be funded Hard decisions would need to be made regarding the feasibility and utility of each intervention in meeting the transition needs of the community
32
TABLE 5 Recunet Cots fbr Total Project Life (March 1 19O-Sepember 30 1992)
i~i~iii~iil~iiiiii iiiiiii
i i
Salr 23 31 23 23Beelt 1761846 2377762 1761846 1761846 7663300
25 25 25 25 Traal 537725 537725 537725 537725 2150oo
15 65 10 10 Teclula Item 22635 98075 150890 150890 1508900
20 40 20 20 Office Items 789220 1578440 789220 789220 3946100
20 40 20 20 Foreign Travel 26005 52010 26005 26005 130025
20 40 20 20Local Travel 492625 985250 492625 492625 2463125
Vehicle 20 40 20 20 OPMAi 1113450 2226900 1113450 1113450 5567250
25 25 25 25 Rea and Utility 766500 766500 766500 766500 3066000
Health 40 20 20 20 Removation 1600960 800480 800480 800480 4002400
Protect 100 0 0 0 Water 409600 000 000 000 409600
Malntenance 25 25 25 25 No-Vehle 566200 566200 566200 566200 2264800
25 25 25 25Communlcatoms 185775 185775 185775 185775 743100
Evalato 25 25 25 25 Csultants 410675 410675 410675 410675 1642700
Last three Mouths of im 679425 679425 679425 679425 2717700
TOTAL 9566341 12147927 820616 828016 38275900
F Unsustainable Costs
The present scope of BCSP activity cannot be sustained by the GOU local communities or other NGOs The major items of transport and personnel costs are not sustainable Communities have already made significant contributions of materials and labor for the renovation and construction of health units and clinics Incomeshygeneration activities community and RC revenues can eventually serve as sources
33
of money to support a large share of operational activity Innovative approachesinvolving shared transport staff and local resources could be developed Political leaders have already given their commitment to the activities conducted under the WVU project Their future involvement in planning managing and supporting Child Survival and Safe Motherhood project activities would ensure eventual transition with full community maintenance
Other capital expenditures could be defined as unsustainable costs The majorproject-specific costs that are not sustainable include
Refresher courses for TBAs (The MOHDMO has admitted that he cannot finance these) Vehicle maintenance and repair costs have also been cited as not sustainable at this time
Bicycle parts and maintenance for the CHWs cannot be sustained
The project headquarters and its office space requires rent and utility costs that cannot be maintained at this time
G Sustalnabllity Plan-Community Participation and Cost Recovery
The DIP did not include a comprehensive plan for transferring the CSP over to any jurisdiction The DMO and the GOU requested WVU to assist them in providing services to the impact areas where the need was greatest and underserved The DMO and MOLGMOH have provided support in training transport staff vaccines and other items in support of this project Most of these will be extended over time but the major problem is that the development of a functioning and sustainable health project takes longer than three years The other NGOs operate on the assumption that such gains will require seven to ten years The DMO thought that project development would take about five years A more realistic time frame would be from five to ten years
The MOLGMOH will continue to support EPI and basic health clinic services where renovated or newly constructed clinics are operational The DMO made a commitment to provide FP commodities provide continued assistance in training and generally collaborate with WVU A proposal to furnish staff to the project has been delayed due to financial problems and policy changes at the federal level in UgandaThe major sustainability strategies listed in the DIP include
Encourage community leadership Create MOH ownership
bull Enhance collaboration with other NGOs Build local capabilitiesDevelop cost sharing Initiate cost-recovery schemes Establish income-generation activities
34
The major in-country agencies that have worked with WVU include MOLGMOH UCBHCA AMREF USAID GTZ World Harvest and other such agencies
Shared costs and in-kind contributions such as labor and materials are shown below in Table 6
TABLE 6 Community Labor Contributions to BCSP
Apudwste COAt 10
Labor for ostruction and renovation of health un - Karagutu See detail below ________
Clearingleveling site 35 persons per day for 10 days 500 shday per person 175000
Mobilizing stones 30 persons per day for 8 days500 shday per person 120000
Loadingnloading dolly and crushing of stones
25 persons per day for 20 days 500 shday per person 250000
Unskilled labor-general 2000000
10 personsday for 20 days Supervision by RC and WV staff 2000 shday per person 400000
Assume same level of contribushytion but cost of living twice as
Labor for Ntoroko health unit con- high as Karagutu Wages estimate struction is therefore twice as high 5890000
Assume half the contribution of Labor for Rwebisengo staff housing Karagutus because house is much renovation smaller 1472500
Involved collection of sands and stones along with unskilled labor 20 personday for 4 days500 sbday per person for 1
Labor for spring protection-Karagutu spring (40000x14) 560000
tOTAL LABOR CONTRIBUnON 1U7500($1ooo)
1 NGO-GOU-Commmu4y Mmxciag 4f Inlereution
Projected revenue activities have not been fully explored The BCSP has considered fee-for-service but no fee-for-service or fee-for-medicine policy has been implemented The project manager believes that the community is not yet able to pay these fees in addition to their prior contributions in the form of money time and labor
The following steps for sustainability were initiated
35
Total support for personnel and supplies for immunization control of diarrheal disease watersanitation and child spacing was tentatively promised from MOHDMO This promise was confirmed by the new DMO during the final evaluation teams interview with him
Training of CHWs and TBAs may also be taken over by MOHDMO
The MOHDMO has promised continued supplies of contraceptives
The MOHDMO and community have expressed the desire to maintain fixed immunization sites and construct new outreach sites The comshymunity is currently gathering funds to purchase resources for construction materials -uch as bricks WVRD has a tentative plan to contribute partially with remaining funds to new outreach centers as well
Taxation at a local level is occurring and a set amount is allocated for the district for health expenditures However the District Development Committee has the power to authorize how much money shall be allocated to the different areas The BCSP is not guaranteed anything more than what they currently receive
CHWs and TBAs have expressed the commitment to serve voluntarily free-of-charge well rafter World Vision and USAID leave Their knowledge will continue to promote child spacing family planning and some information or education regarding nutrition and breastfeeding
CHWs and TBAs also promote and teach ORS home method Their training has required them to request repeat demonstrations from mothers in order to ensure their knowledge of ORS preparation
The community has established a spring maintenance crew for each of the 14 protected springs in the Karagutu area
The communities VHCs are very supportive However further financial commitment is questionable VHCs have just begun discussing methods for sustainability in the future
Midterm evaluation recommendations were followed up with a plan of action for implementing all appropriate recommendations
Record keeping and the HIS were simplified
HIS recommendations were implemented by a field visit from WVRD staff The system has been streamlined and is now functioning While some questionable information is collected the entire system is operating well
36
The midterm Training of Trainers recommendation has been implemented The TOT training was conducted by UCBHCA in three phases
Income Generation
Currently only a few income-generating groups have been formed Four of the groups use chickens and eggs handcrafts cattle-raising and sewing as means of generating revenue The fifth group has created an acting ambulance fund for transport in case of an emergency The project manager and area coordinators have no dollar estimate for these groups as they are very few and not totally operational
During CHWTBA training participants are encouraged to discuss sustainability of which income generation is one aspect However the project manager believes it has been difficult to motivate groups when there is no funding for start-up costs Lack of this kind of assistance has posed a barrier for some groups
Further suggestions and ideas discussed with the community have been farming sewingtailoring fishing and other handicraft activities that might prove profitable
Cost Recovery and Cost Reduction Attempts
Community participation in the form of labor construction materials buildings and monies has increased substantially since the projects beginning
The project has used the established RC system as means of communicashytion and information dissemination
Reduction of in-country consultation has been stressed There has been only one in-country consultation The other consultations have been funded through NGO donation or have been budgeted for evaluation by World Vision
An intern was recruited to assist in the determination of various costs and revenues This too alleviated the cost of an external consultant
A consolidation of unnecessary record-keeping instruments was performed Three forms were created to facilitate information flow from the community health worker to the area coordinator to the project managerThere were seven forms death register TBA form WCBA form immunization default form woman information register child information register and household register
A strict management system of financial resources was implemented
37
The project manager was made master signatory for all purchases A second signature was also required
The accountant was instructed to collaborate with the storekeeper to verify items and quantities purchased
Advances of cash for salary and benefits were to be authorized by the project manager
The project manager accepted no expenditure amounting to more than 50 of the staff members salary
Staff problems were addvessed
The project manager redefined the expectations and job duties of key manageliat staff resulting in higher output
Support staff was educated on project objectives the operational means necessary to achieve these objectives and their role in achieving them Their increased awareness of the project facilitated a higher output
Technical staff was encouraged to ensure field operation success
All staff was educated further in the different roles each staff member plays This heightened awareness greatly reduced confusion about job duties and expectations
Bicycles for CHWs were selected as means of transport They do not require fuel
Use of Ugandan staffing has been stressed throughout the project
2 Community Pwa tion
Members of the Village Health Committees were interviewed as were political leaders at the local and RC levels In two cases these leaders came to the final evaluation team because of their involvement and commitment in the BCSP These leaders wanted to share their good experiences with the WVU staff and use their training and knowledge gained through implementation They wanted the team to know that they strongly support the project and want it to continue until a full transition can be achieved These leaders saw the remarkable impact of Child Survival interventions on reducing deaths from communicable diseases They expressed concern that transition health problems and disease conditions would not be solved through government health service programs More importantly they saw the value of the WVU process for achievement in solving health problems and want to use that same process for other social problems as well
38
The BCSP project empowered communities to meet their basic health needs and sustain effective child survival by training CHWs TBAs and VHCs Theyconducted focus group sessions and made numerous village and community contacts The communities were found to be actively involved in the designimplementation and monitoring of the CS project in their village They reported going house-to-house for health and hygiene inspections These health committees shared their concern over AIDS and how it is transmitted One VHC member related how many of the villagers have died from the disease this year Each of the 74 villages has a VHC that meets on a regular basis These committees are elected by a democratic process whereby the villagers stand behind the candidate of their choice All committees meet on a regular basis keep meeting minutes and function as supervisors for CHWs The VHCs were actively involved in assessing village health needs and problems using disease information to make decisions conducting health education sessions and enforcing health standards Pit latrines preventive health practices and local disease problems are issues reportedly addressed by VHCs The major barrier to total assumption of the BCSP by local communities is poverty
IX NEw INTERVENTIONS
A Acute Respiratory Infection as a Health Problem
Mothers were asked during the household survey which was the most serious health problem in their home The most frequent illness identified was Acute RespiratoryInfection (ARI) It would be prudent for the BCSP to consider adding an ARI intervention component for several very good reasons First the similarity in approach between diarrheal disease and ARI is striking Both illnesses occur repeatedly and are caused by different and multiple organisms Other considerations that support adding an ARI intervention include
ARI was among the most common diseases identified by mothers in the project area In Uganda 11 of all hospital deaths are due to ARI (ARI-Implemenshytation Plan 1992-95 MOH) ARI and diarrhea have many similarities and the GOU sees fit to include ARI in PHC programs
Worldwide children under five years of age have one to three episodes annually and ARI causes four million deaths annually in this age group Fifty percent of ARI illnesses are viral in which antibiotics are not effective In the project area the associated factors appear to be
Weather In the mountains in Karugutu most mothers cook in their houses Smoke irritates the respiratory tract and increases susceptibility to ARI
Phawdk In the dry and dusty areas of Rwebisengo and Ntoroko indiscriminate spitting of sputum occurs increasing the droplet transmisshysion of ARI
39
Nubdim According to UNICEF about 23 of children under five years are malnourished Although most children seen in the project area appeared well nourished if growth monitoring is constantly used mild to moderate forms of malnutrition can be detected Malnutrition weakens immunity In the presence of malnutrition ARI is most likely to occur
B Intervention Strategies for ARI
New intervention strategies for ARI should include
A survey to determine the magnitude and causal factors of AR bull Health education for mothers ahers on causes preventive measures and home
therapyGrowth monitoring-Vitamin A therapy if warranted Teaching health workers about case findings and effective case managementEquipping village pharmacies with drugs to treat AR Operational research
X RECOMMENDATIONS
A Short-Term Recommendations
1 The BCSP should be extended and expanded Now that the approved one-year no-cost extension through USAID has been formalized a second CSP proposal should be developed and submitted to USAID Terms of the new CSP should include a consolidation phase a developed plan for achieving sustainability through the proven implementation process achieved during the present CSP careful consideration of expansion and a demonstration of the projects replication capacity
2 Target new diseases such as ARI and AIDS for interventions AIDS education in relation to basic health education and MCHFP services should be developed and strengthened
3 Core staff should be computer-trained and a computer and printer should be installed at the Karagutu facility Patrick could ensure technical backup from Kampala via the radio link
4 Training provided to VHC members should be consistent with that presentlygiven to CHWs and TBAs (as appropriate) This would provide backup service for CHWs and reduce the population covered per worker while providing a cost-reduction mechanism in operational expenditures
5 Provide BCSP core staff with additional training related to project goals and objectives and to meet the emerging needs of participating communities Each core staff member should have at least one training seminar or workshop experience each year
40
6 Provide additional training in leadership management monitoring and evaluation to all appropriate levels of community and project staff
7 All village-based individuals need to be provided training to ensure that emerging community problems are solved and expanded community services are provided CHWs could be trained as vaccinators to expand immunization outreach efforts in remote areas
8 Several types of technical expertise will be required during the next project phase Some of these can be acquired through hiring additional staff supported through USAID funds Other technical experts could be acquired through some contract mechanism between WV and individuals or through a larger contract with an agency that has the needed technical expertise Either ampi pan-time or full-time medical person should be added to the staff or such expertise should be purchased on a contract basis As the project becomes more sophisticated the greater is the need for a medical expert WVU should recruit a person with skills in developing and writing grant proposals and requests for assistance Such a person could train individuals from selected communities on how to write and submit development or assistance proposals
9 Clear personnel performance pay and discipline guidelines need to be written and circulated to all core project staff Documented feedback to employees should be provided within five working days of a personnel appraisal
B Intermediate-Term Recommendations
1 Any extension or expansion of WVU CSP activity should include additional training of staff in simple IGA technical and management skills Suitable technical expertise for the entire range of IGAs should be either hired directly as a full-time position or through a contractual arrangement with some suitable expert organization
2 Adult literacy should be linked to all community-based activities including focus groups VHCs TBAs CHWs and IGAs
3 Training of some staff members should be conducted in specialized skills such as simple computer operations management of IGAS elementary statistics demography participatory rural appraisals rapid appraisal procedures bookkeeping and simple accounting techniques
4 A stronger child spacing component should be developed consistent with the GOUs Maternal and Child Health and Family Planning Five-Year Plan (1993shy1998) (See Annex Z)
5 Additional TBAs should be trained to provide better maternity service and to overcome the problem of having just a few facilities in distant locations Refresher courses should be provided to TBAs to increase skills and broaden
41
the scope of ANC activities The selection process for new TBAs should also target younger women
6 It is recommended that IGAs be incorporated as part of the longer-termfeatures for achieving sustainability by providing a source of funds for selected community-based projects
7 Communities and VHCs should be encouraged to provide TBAs with suitable delivery shelters equipped with materials for their operation Support could be provided through small IGAs or perhaps one-time fund-raising projects
8 Income-generation groups require full WVU technical support through either hired experienced staff with intricate skills needed to guide such groups or a fund established for contracting for such services
9 Increase the involvement of contact activity and cooperation between the project and the district CBHCA Develop linkages during the next project grantproposal development stage Exchange formal agreements between the BCSP district authorities RCs and communities regarding the Detailed Implementashytion Plan (DIP) written for future project grants
C Long-Term Recommendations
1 Develop a new CSP proposal that includes formal agreements between agencieslocal authorities political leaders and communities Such agreements should be written and roles clearly defined resources identified and phaseover time frames established
2 The project will need to assist in the renovation and upgrading of various health units in the three impact areas Possibilities should be increased for static MCHFP services laboratory and maternity facilities and small pediatric wards This activity should be in collaboration with the MOH MOLG other NGOs and the RC system along with local populations
3 TBAs should be trained and authorized to promote community-based distribution of contraceptives This recommendation is contingent uponestablishing a regular supply of FP commodities from the MOH
4 Further education is needed about the role of the TBA Payment of traditional delivery fees to TBAs should be resumed to enhance sustainability All TBAs should be trained to eliminate the fee differential based on training The main mechanism for restructuring the allocation and use of trained TBAs rests with the VHCs
5 TBAs should be used in growth-monitoring activities They should be providedwith weighing scales that could be taken to each home This would involve additional training in nutrition interpretation of weight and height curves and use of equipment
42
6 Adult literacy should be included as part of the TBA training option Report forms should be revised so that simple pictorial HIS reports can be preparedby illiterate TBAs TBAs should be provided with kits and suitable storagecontainers
7 Establish a task force for emergency obstetric evacuation The entire spectrum of referral for obstetric cases ambulance service and medical emergencies needs to be developed in conjunction with the MOH MOLG communityleaders RCs and VHCs Trained personnel should be available for obstetric emergencies
8 Due to hardship conditions involved in serving in isolated areas a process of rotation of core staff should be ionsidered Hardship allowances and salaries should be reviewed at least twice annually to adjust for inflation
9 VHCs should be trained in all aspects of health and related activities to ensure continuity of services and to support TBAs and CHWs Individual effort should be recognized
Incentives should be equalized or abandoned All incentives should be generated and paid at the community level eg repairs to bicycles used for health activities
10 New CSP interventions for ARI AIDS and malaria should be considered for inclusion in future project designproposals
12 Establish linkages with appropriate groups for greater community responsibility in primary health care and revolving drug schemes that require commercial purchase of medicines and cost-recovery means to ensure a complete cycle Simple bookkeeping and inventory skills should be taught to selected individuals while the treatment component could be handled through the CHW TBA or VHC CHWs TBAs and VHCs could be paired with other successful individuals or groups to learn while on the job for periods ranging from a few days to a week The present ratio between community workers and households covered is 1150 it should be approximately 120-30 More CHWs should be trained for a better ratio
13 Future project proposals should contain tighter sustainability indicators targeted phaseover and specific designation of roles and resources
14 Social services need special review to determine how they fit into the emerging community needs and contribute to improvements in the quality of life Appropriate linkages with involved sectors and departments should be stipulated Establish a specific resource center in the project impact area that could meet multiple needs arising from implementation activities The resource center could serve as the adult literacy center support agriculture study and provide training enhancements
43
15 Staff secondment needs to be reviewed as soon as it is feasible Additional project staff will need to be hired if the project consolidates and extends
16 Initial efforts to establish an at ris register failed to produce the desired effect The entire concept including criteria definition should be revised so that efforts to reduce morbidity and mortality are directed to the individuals at greatest risk
17 Existing income generation groups should be used as change agents for child survival and safe motherhood practices Each income generation group could be provided with training similar to that provided to CHWs Adult literacyagriculture basic food production and storage child education and other development projects could be initiated and supported through such groups
18 Train more CHWs Help develop road repair and building and provideagriculture development and assistance
44
ANNEX A
WORLD VISION UGANDA CORE STAFF INTERVIEW QUESTIONNAIRE
Name Position Date Interviewer
1 What is your professional training
2 How long have you been in this position
3 What is your role and responsibilities
4 What are the goals and objectives of the project
5 What are the target groups for the different interventions
EPI __ ORT - FP - Growth Monitoring - WaterSanitation
6 Do you have an annual work plan - Monthly work plan
7 What training have you received in the project
8 What additional training do you think you need to conduct your job more effectively
9 Have you been involved in the design of the training courses for this project
Please explain
10 Have you been involved in the training of people (eg CHWs) associated with the project
11 Was there a needs assessment done to determine what training should be conducted
12 Has there been any follow-up to evaluate the effectiveness of the training
13 What is your role in the collection of project datainformation
Type of data collected
i
From Wherewhom
To whom submitted
How data collected is used
Do you get feedback on data collected
From Whom
How Often
How
Does the community receive feedback
From Whom
How Often
How
14 Apart from project staff who do you share project datainformation collected (eg MOH NGO)
15 What has been MOH involvement in the project
Type Level
16 What has been other NGOs involvement in the project
Name of NGO
Type of Involvement
17 Did communities participate in the design of the project
Explain
18 Do communities participate in the implementation of project activities
Yes __ No
19 How many health committees does the project have
How often do they meet Topics discussed
When was the last meeting Decision made
Action Taken Minutes of meeting available - Request copy
20 What has the community contributed to this project
21 Which aspects of the project activities do you think could be supportedcontinued by the community
22 What are the main problems andor constraints you think should be addressed
A
ANNEX B
CHILD SURVIVAY FINAL EVALUATION -HOUSEHOLD INTERVIEW FORM FOR MOTHERS WITH CHILDREN
UNDER RESPONDENTS ARE CARETAKERS OF CHILDREN UNDER FIVE YEARS OF AGE
Sub-country ltA gt Parish ltA gt
Respondent ltidnumgt Interviewer ltA gt
Dote ltddmmyygt Number in Household
1 What (disease KAP) can be prevented by immunization
Diphtheria lt Y gt Measles lt Y gt Polio ltYgt Pertussis ltYgt Tetanus ltYgt TB ltYgt
2 Why should a pregnant mother receive (IT) vaccination
_ Protect mother ltYgt from tetanus Protect Baby ltYgt from tetanus Protect both ltYgt against tetanus Unknown lt Y gt Other ltYgt ltA gt
3 At what age should a child receive the first dose of oral polio
ltA gt weeksmonths Unknown ltYgt
At what age should a child receive measles vaccination
Measles ltA gt weeksmonths Unknown ltYgt
4 What do you do when your child has diarrhea
- Give ORS lt Y gtSSS Give medicine ltYgt from drug seller Continue breast ltYgt and other feeding during diarrhea Increase amount of feeding ltY gt after diarrhea (recovery)
- Hygiene ltYgtsanitation _ Others ltYgt (specify)
Government Clinic ltYgt
5 What is the best use of ORSSSS during diarrhea
Treat lt Y gt diarrhea Prevent dehydration ltYgt Theirs ltYgt ltA gt
6 When was the last time your child had diarrhea
None ltYgt Less than four months ltYgt 5 to 12 months ltY gt More than 12 monthslt Ygt ItAgat last diarrhea incidence ltA gtdaysweeksmonths
7 At what age should a baby start to receive food in addition to breast milk (4-6
months will be considered correct)
Correct lt Y gt
8 Ask mother
Still Breast feeding ltYgt Baby eats other food ltYgt How often does child eat Times per day
9 Do you have a health card ltYgt
-Maternity TT card lt Y gt Growth Card ltY gt BCG Scar ltYgt
10 Are you interested in spacing ltYgt the birth of the next child
IF NO GO TO QUESTION 14
11 Are you presently using ltYgt child spacing services
If no why not ltA gt
12 What is the main health problem ltA gt of this household
13 How much did the last illness in this household cost to treat (including drugs and travel costs) Shillings
14 Pit Latrine ltYgt General sanitation ltYgt ORS Utensils ltYgt
ANNEX C
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
COMMUNITY HEALTH WORKERTBA INTERVIEW FORM
Sub-country Parish Name Interviewer
Date
1 How long have you been CHWTBA
2 Number of Households visited per month Amount of time per week spent on CHWTBA work
3 What kind of training did you receive in the project
- Performance based training Knowledge based training
4 Perception of work load in relation to training
Ask for Drug or TBA kit - YES - NO
5 Who are you responsible to (probe for community and supervisor)
6 Who provides you with support
What kind(s) of support do you receive
7 What kinds of health records do you keep
List types
How much time do you spent each month keeping these records current
HoursDays
8 What do you do with these data (wait for the answer and check appropriately)
a) Submit to supervisor b) Discuss with community c) Follow-up and track defaulters
9 How often do you sit in on the village health committee meetings
10 Are meeting minutes kept - Yes _ No
Ask to see the minutes Minutes seen - Yes __ No
11 Does the village health committee supervise your work
-Yes - No How
12 List the strong points of the VHC
List weak points of the VHC
Suggestions for improving the VHCs
13 What problems do you usually encounter in the performance of your work as a CHWTBA
What do you think should be done to address these problems
14 If the project phases out would you continue your work as CHWTBA
Yes -No How
15 Please provide general ideas or recommendations for improving the program
ADDITIONAL COMMENTS
ANNEX D
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR VILLAGE HEALTH COMMITTEE
SUB-COUNTY
Name Position
Committee Name Parish
1 How long have you been a member of the project
2 How were you selected as a member of the committee
3 How would you see this project continuing once the donors pull-out
How much time would you need to take over
4 How often does your committee meet with
Community _ CSP staff
5 Do you participate in the planning and evaluation of health activities in your village
Yes __ No
If yes how If no why not
6 How does the committee determine what are the health needs of the community
How does the committee select services
7 Are the services provided in your community effective in meeting communities health needs Explain
8 Has the health of children in your community improved Yes __ No __
If yes why If no why not
9 What resources (human financial material) has your community contributed to the project
10 How much time do you spend per week for health activities
11 Is the committee involved in obtaining health information in this community
Yes - No
If yes how
How is the information used
12 How does the community communicate with the committee
13 What aspects of the project can your community continue to support to ensure sustainability of project activities once project funds phase out
Who will manage it
14 Before the project phases out what other support (training supplies etc) does your communityhealth committee see as needed to provide them the toolsskills to continue to manage activities
ANNEX E
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR MOH
Name Position
Date Interviewer
1 How long have you been in this position
2 What is your role and responsibilities
3 What are the goals and objectives of this project
4 Are the goals and objectives of this project in conformity with MOH policies and
strategies Yes - No shy
5 Have you been involved in the training of people associated with this project
Yes __ No -
If yes please describe the type of people trained and task duration
eoh Tsk Draion DAt
a
b
C
6 Has there been any follow-up to evaluate the effectiveness of the training
Yes __ No
If yes please describe
How often
How is this data used
Do the data conform to MOH needs Explain
7 What support do you receive from the project
8 Does the project provideshare reports on their activities
Yes _ No
If yes please describe
How often
How is this data used
Do the data conform to MOH data needs Explain
9 What has been MOH involvement in the project
Type of involvement
At what level
10 Do you perceive project activities as being effective
Yes - No
If yes why
If no why not
11 Which aspects of the project will the MOHMOLG be able to sustain once the project ends (training supervision supplies)
12 CommentsRecommendations for the project
ANNEX F
WORLD VISION UGANDA CHILD SURVIVAL FINAL EVALUATION
INTERVIEW GUIDELINES FOR NGOs
Name Position
Date Interviewer
1 What role has your organization played and is playing in this project Explain (type of involvement etc)
2 Are staff of your organization involved and interact with the CSP staff If yes please describe
3 Have you participated in meetings with CSP staff (DCBHCA)
Yes __ No
4 Do you perceive project activities as being effective Yes __ No _
If yes why
If no why not
5 Which aspects of the project can your organization continue once project funding phases out
6 CommentsRecommendations
ANNEX G DOCUMENTS REVIEWED
1 Midterm Evaluation Report Bundibugyo Child Survival Project November 5 1991
2 Bundibugyo Child Survival First Year Report First Annual Report Bundibugyo Child Survival Project
3 Bundibugyo Uganda Child Survival Project Setailed Implementation Plan October 1 1989-September 30 1992
4 UNICEF Expanded Program of Immunization fc Control of AIDS in Uganda Stand-Alone-Noting Document October 1991
5 District Mobilization for Prevention of AIDS in Uganda Trainers Guide for Health Workers MOH Republic of Uganda
6 Acute Respiratory Infection (ARI) Implementation Plan 1992-1995 Ministry of Health Government of Uganda
7 Training Guidelines for Trainers of Community Counselling Aides Published by AIDS Control Program MOH PO Box 6 Entebbe Uganda
8 WVRD Final Evaluation Report Kamalapur Child Survival Project Dacca Bangladesh
9 Training in the Collection and Use of Information for Community Health Workers Ben Osuga African Medical and Research Foundation
ANNEX H
FISCAL YEAR 1991 (OCTOBER 1-SEPTEMBER 30 1991) BASED ON ACTIVITY R7 PORT
110 UIIZamp0~ m TMAL
235 30 235 23 SALARY 110568 141150 110567 108215 47050
235 30 235 23 BENEFITS 654123 835050 654122 640205 2783500
25 25 25 25 TiNING 222000 222000 222000 222000 s8o00
INTERNATIONAL 15 40 15 30 TRAVEL 2865 7640 2865 5730 19100
LOCAL 15 40 15 30 TRAVEL 213540 569440 213540 427080 1423600
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 356685 951160 356685 713370 2377900
OFFICE 20 40 20 20 SUPPLIES 525940 1051880 525940 525940 2629700
TECHNICAL 25 55 10 10 SUPPLIES 89200 196240 35680 35680 356800
RENTAL amp 25 25 25 25 UTIUTIES 710400 710400 710400 710400 2841600
100 0 0 0 PROTECT WATER 260200 000 000 000 260200
40 20 20 20 HEALTH UNIT 930840 465420 465420 465420 2327100
25 25 25 25 MAINTAIN 22200 22200 22200 22200 8800
25 25 25 25 COMMUNICATION 69275 69275 69275 69275 277100
EVALUATION amp 25 25 25 25 CONSULTATION 190225 190225 190225 190225 760900
TOTAL 435M61 s432e 3571919 4135740 17504800
FISCAL YEAR 1992 (oCTOBER 1-JUNE 30 1992)(JULY I-SEPrMBER 301992 ESTIMATED)
BASED ON ACTIVITY REPORT
m
25 25 25 25 SALARY 78625 78625 78625 78625 314500
25 25 25 25 BENEFITS 414275 414275 414275 414275 1657100
25 25 25 25 TRAINING 219675 219675 219675 219675 373700
INTERNATIONAL 15 40 15 30 TRAVEL 405 1080 405 810 2700
LOCAL 15 40 15 30 TRAVEL 74760 199360 74760 149520 498400
VEHICLE OPERATION 15 40 15 30
MAINTENANCE 251130 669680 251130 502260 167420
20 45 20 15 OFFICE SUPPLIES 141800 319050 141800 106350 70900
TECHNICAL 10 70 10 10 SUPPLIES 24100 168700 24100 24100 241000
25 25- 25 25 RENT amp UiLITY 18750 18750 18750 18750 75000
0 0 0 0 PROTECT WATER 000 000 000 000 000
HEALTH UN 40 20 20 20 RENOVATE 490840 245420 245420 245420 1227100
MAINTAIN 25 25 25 25 NON-VEiICLE 169)0 16900 169)0 16900 6760
25 25 25 25 COMMUNICATION 12750 12750 12750 12750 $10
25 25 25 25 CONSULTANT 725 725 725 760 290
25 25 25 25 EVALUATE 188475 18475 188475 188475 753900
SUBTOTAL-9 MONTHS 19332A0 25pM3 16780 19787M0 153110
--------- --------- --------- --------------------------- -------------------------------- -------------------------------- ---------
--------- --------- ---------
--------------------------- ------------------- --------- --------- --------- ---------
---------- ------------------ ---------------------------- ----------------------------
----------------- ------------------------------------------ ---------------------- -------------------
---------------------- --------- -- -------------------
Q
1992 ANNUAL REPORT FORM A COUNTRY PROJECT PIPELINE ANALYSIS WVRDUGANDA BUNDIBUGYO CHILD SURVIVAL PROJECT
NOTR-O500-A-O0-9156-00
Projected Expenditures Against Total Agreement BudgetFIELD Actual Expenditures To Date Remaining Obligated Funds (Colum I amp 2) (090189 to 93092) (100192 to 083193) (090189 to 083193)
COST ELEMENTS -------------TAID WVRD TOTAL AID WVRD TOTAL AID WVRD TOTAL 1 PROCUREMENT ------ - - - - -- -- -- ------
A Supies 58696 26131 84827 50004 (5131) 44873 108700 21000 129700 B Equipment 0 96091 96091 23500 (2341) 21159 23500 93750 117250C ServicesConsultants 7715 2217 9932 30705 103 30808 38420 2320 40740
U---- -- - -- ------------------------------------- ---------- -------------------SW-TOTAL I 66411 124439 190850 104209 (7369) 96840 170620 117070 287690
--------- ------------------ -------------------
ii EVALUATIONSU-TOTAL ii 16952 0 16952 22638 3000 25638 39590 3000 42590 -- -- ------------------ --------- ---------
IIIINDIRECT COSTS
Overhead on Field 202 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
SUB-TOTAL I1 52125 27203 79328 30000 (14532) 15468 82125 12671 94796
IV OTHER PROGRAMI COSTS
A Personnel 84127 0 84127 96238 21321 117559 180365 21321 201686 B TravelPer diem 89561 191 89752 (5761) 12187 6426 83800 12378 96178C Other Direct Costs 91385 19666 111051 42115 9234 51349 133500 28900 162400
SW-TOTAL IV 265073 19857 28930 132592 42742 175334 397665 62599 460264 ---------- ---------
TOTAL FIELD 400561 171499 572060 289439 23841 313280 690000 195340 885340 333323333 333333333 33zzrz z3838xzzzzxzzm 323333 33333333333Z 333333333 333333333