Embed Size (px)
Citation preview

Wound Healingand Skin IntegrityPRINCIPLES AND PRACTICE
Edited by Madeleine Flanagan


Wound Healing and Skin Integrity


Wound Healing and Skin IntegrityPrinciples and Practice
Edited by
Madeleine FlanaganMSc (Dist), BSc (Hons), Cert Ed (FE), RN
Principal LecturerSchool of Life and Medical SciencesPostgraduate MedicineUniversity of Hertfordshire, UK
A John Wiley & Sons, Ltd., Publication

This edition first published 2013C© 2013 by John Wiley & Sons, Ltd
Registered office: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to apply forpermission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwell.
The right of the author to be identified as the author of this work has been asserted in accordance with the UKCopyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted,in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except aspermitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. All brandnames and product names used in this book are trade names, service marks, trademarks or registeredtrademarks of their respective owners. The publisher is not associated with any product or vendor mentionedin this book. It is sold on the understanding that the publisher is not engaged in rendering professionalservices. If professional advice or other expert assistance is required, the services of a competent professionalshould be sought.
The contents of this work are intended to further general scientific research, understanding, and discussiononly and are not intended and should not be relied upon as recommending or promoting a specific method,diagnosis, or treatment by health science practitioners for any particular patient. The publisher and the authormake no representations or warranties with respect to the accuracy or completeness of the contents of thiswork and specifically disclaim all warranties, including without limitation any implied warranties of fitnessfor a particular purpose. In view of ongoing research, equipment modifications, changes in governmentalregulations, and the constant flow of information relating to the use of medicines, equipment, and devices, thereader is urged to review and evaluate the information provided in the package insert or instructions for eachmedicine, equipment, or device for, among other things, any changes in the instructions or indication of usageand for added warnings and precautions. Readers should consult with a specialist where appropriate. The factthat an organization or Website is referred to in this work as a citation and/or a potential source of furtherinformation does not mean that the author or the publisher endorses the information the organization orWebsite may provide or recommendations it may make. Further, readers should be aware that InternetWebsites listed in this work may have changed or disappeared between when this work was written and whenit is read. No warranty may be created or extended by any promotional statements for this work. Neither thepublisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication Data
Wound healing and skin integrity : principles and practice / edited by Madeleine Flanagan, MSc (Dist), BSc(Hons), Cert Ed (FE), RN, principal lecturer, School of Life and Medical Sciences, Postgraduate Medicine,University of Hertfordshire, UK.
pages cmIncludes bibliographical references and index.ISBN 978-0-470-65977-9 (pbk. : alk. paper) – ISBN 978-1-118-44181-7 (mobi) – ISBN 978-1-118-44202-9
(ebook/epdf) – ISBN 978-1-118-44206-7 (epub) 1. Wounds and injuries–Treatment. 2. Skin–Wounds andinjuries–Treatment. I. Flanagan, Madeleine.
RD95.W68 2013617.4′77044–dc23
2012039436
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not beavailable in electronic books.
Cover images courtesy of Julia Schofield (main image of varicose eczema), Ann Marie Brown (skin tear),Shiu-Ling Briggs (infected leg ulcer) and Madeleine Flanagan (pressure ulcer)Cover design by Andy Meaden
Set in 9.5/11.5 pt Palatino by Aptara R© Inc., New Delhi, India
1 2013

Contents
List of Contributors xPreface xiiAcknowledgements xiv
Section 1 Principles of Best Practice 1
1 Evidence and Clinical Decision-making 3Carolina WellerIntroduction: what is effective clinical
decision-making? 3What is evidence-based health care? 4Common misperceptions about
evidence-based practice 5Challenges to changing practice 7Factors influencing clinical judgement 8Evidence-based practice: hierarchy
of evidence 9Evidence-informed decisions 11Critical appraisal frameworks 11Clinical guidelines 13Summary 13Useful resources 14Useful critical appraisal frameworks 14Further reading 15References 15
2 Maintaining Skin Integrity 18Arne Langøen and Janice BianchiIntroduction 18Impaired skin barrier function in the
clinical setting 23
Management of vulnerable skin 27Summary 30Useful resources 30References 30
3 Physiology of Wound Healing 33Mary MartinIntroduction 33Types of wound healing 35Wound chronicity 35Normal wound healing 36Optimising healing: general factors 38Optimising healing: local factors 39Delayed wound healing 40Tissue repair in chronic wounds 40The inflammatory response 41Proliferation of new tissue 43Wound closure 45Summary 48Useful resources 48References 48
4 Assessing Skin Integrity 52Annemarie Brown and Madeleine FlanaganIntroduction 52Assessing skin integrity 53Listening: problem orientation
and knowledge 53Looking: problem clarification and
knowledge construction 55Touch: hands on fact finding 56

vi Contents
Smell: subconscious information gathering 57Assessing wounds 58Wound bed preparation 58Data collection 60Effective documentation 63When to seek specialist help? 63Summary 63Useful resources 64References 64
5 Principles of Wound Management 66Madeleine FlanaganIntroduction 66Principles of wound management 67Effective wound management 67Controlling bacterial burden: wound
cleansing 68Controlling bacterial burden: wound
debridement 69Autolytic debridement 69Enzymatic debridement 69Biosurgical debridement 70Mechanical debridement 70Sharp debridement 70Hydrosurgical debridement 71Ultrasound (acoustic pressure wound
therapy) 71Regulating moisture balance 71Wound dressings 72Passive inert dressings 74Interactive dressings 75Antibacterial dressings 79Summary 83Useful resources 83References 83
6 Wound Infection 87Valerie Edwards-Jones andMadeleine FlanaganIntroduction 87Bacterial invasion of the skin 88Wound pathogens 88Factors increasing the risk of
wound infection 90The significance of bacteria
within wounds 90Significance of biofilms 92Identifying wound infection 92Microbiological assessment of wounds 93Principles of managing infected wounds 95Summary 99Useful resources 99References 99
7 Psychological Impact of SkinBreakdown 102Patricia PriceIntroduction 102Psychological impact on the individual and
society 103Adaptation to chronic illness 103Stress and skin disease 103Depression 104Adjustment to physical
change/disfigurement 105Coping strategies 105Social support 106Body image 106Living with skin breakdown and chronic
wounds: symptom management 107Measuring impact of skin breakdown 108Factors affecting treatment 109Interventions 111Clinical reflection 112Summary 113Useful resources 113References 113
Section 2 Challenging Wounds 117
8 Pressure, Shear and Friction 119Keryln CarvilleIntroduction 119Prevalence and incidence 120Pathophysiology 120Risk factors 122Psychological impact 122Current best practice 123Prevention strategies 123Pressure ulceration: assessment
considerations 123Treatment strategies: pressure ulcers 128Education and support 132Criteria for specialist referral 133Summary 133Useful resources 133Clinical guidelines 133Organisations 133Further reading 133References 133
9 Diabetic Foot Disease 136Jan ApelqvistIntroduction 136Aetiology 137Psychological impact 139

Contents vii
Principles of diabetic foot ulcer management 140Diabetic foot ulceration: assessment
considerations 140Assessment of vascular status 143Assessment of wound infection 143Management of diabetic foot ulcers 145Vascular intervention 145Foot surgery and amputation 146Debridement 147Infection in diabetic foot wounds 147Osteomyelitis 148Offloading – non-weight-bearing 148Wound dressings: special considerations 149Foot care 149Education and support 150Provision of specialist diabetic
foot services 151Criteria for specialist referral 151Summary 151Useful resources 151References 152
10 Chronic Ulcers of the Lower Limb 155Jeanette MuldoonIntroduction 155Epidemiology 155Comorbidities and underlying pathologies 156Rheumatoid arthritis and vasculitis 156Venous leg ulceration 156Factors that affect venous return 158Rarer leg ulcer aetiologies 160Psychological impact 161Principles of managing leg ulcers 161Leg ulceration: assessment considerations 161Vascular assessment for arterial disease 164Management of chronic oedema in
leg ulcers 166Wound dressings: special considerations 168Prevention of ulcer recurrence 169Education and support 170Provision of specialist services 170Criteria for specialist referral 171Summary 171Useful resources 171Further reading 172References 172
11 Lymphoedema 175David KeastIntroduction 175Pathophysiology 176Risk factors 178Psychological impact 179
Current best practice 179Prevention strategies: risk factor
management 180Lymphoedema: assessment considerations 180Treatment strategies 184Education and support 189Provision of specialist services 190Criteria for specialist referral 190Summary 190Useful resources 190References 191
12 Malignant Wounds 193Wayne NaylorIntroduction 193Malignant wounds: aetiology 194Psychological impact 195Principles of palliative wound management 196Malignant wounds: assessment
considerations 196Management of malignant wounds 198Education and support 204Provision of specialist services 204Criteria for specialist referral 204Summary 205Useful resources 205References 205
13 Skin Integrity and Dermatology 208Julia SchofieldIntroduction 208Prevalence and incidence of skin disease 209Quality of life 209Cost of skin diseases 209Management principles 210Important common skin problems and their
management 211Provision of dermatology specialist services 220Summary 221Useful resources 222Further reading 222References 222
14 Surgical Wounds 224Alan WidgerowIntroduction 224Classification of surgical wounds 224Principles of surgical wound management 227Surgical wounds: assessment considerations 227Preoperative management 228Intraoperative management 229Postoperative management 230

viii Contents
Wound closure 231Management of surgical scars 234Common reconstructive
surgical options 236Education and support 237Criteria for specialist referral 238Summary 238Useful resources 239References 239
15 Neglected Wounds 242Kim Deroo, Lesley Robertson-Laxton,Sabina Sabo and Arlene A. SardoIntroduction 242BODY PIERCINGS 242Risk factors (post-piercing infection) 243Factors delaying healing 243Complications 243Principles of wound management 243Practical management 243Practical tips 244Healing rates 244Criteria for specialist referral 244Summary 245Further reading 245References 245BULLOUS PEMPHIGOID 245Risk factors 245Differential diagnosis 245Clinical features 245Factors delaying healing 246Complications 246Principles of wound management 246Practical management 246Criteria for specialist referral 246Summary 246Further reading 247References 247CALCIPHYLAXIS 247Risk factors 247Differential diagnosis 247Clinical features 247Factors delaying healing 248Complications 248Principles of wound management 248Practical management 248Criteria for specialist referral 248Summary 248Further reading 249References 249FISTULAS 249Risk factors 249Diagnostic procedures 249Clinical features 249Factors delaying healing 249
Complications 249Principles of wound management 250Practical management 250Criteria for specialist referral 250Summary 250Further reading 251References 251NECROTISING FASCIITIS 251Risk factors 251Differential diagnosis 251Clinical features 252Factors delaying healing 252Complications 252Principles of wound management 252Practical management 252Criteria for specialist referral 253Summary 253Further reading 253References 253PYODERMA GANGRENOSUM 253Risk factors 253Differential diagnosis 254Clinical features 254Factors delaying healing 254Complications 254Principles of wound management 254Practical management 254Criteria for specialist referral 254Summary 255Further reading 255References 255SELF-INFLICTED WOUNDS (SELF-HARM) 255Risk factors 255Differential diagnosis 255Factors delaying healing 255Clinical features 255Complications 256Principles of wound management 256Practical management 256Criteria for specialist referral 257Summary 257Further reading 257References 257SKIN TEARS 257Risk factors 257Differential diagnosis 258Factors delaying healing 258Clinical features 258Complications 258Principles of wound management 258Practical management 259Criteria for specialist referral 259Summary 259Further reading 259References 259

Contents ix
Section 3 Improving SkinIntegrity Services 261
16 Reducing Wound Care Costs andImproving Quality: A Clinician’sPerspective 263Theresa HurdIntroduction 263Health economics: a clinician’s perspective 264Barriers to best-practice wound care and
prevention 265The costs of wound care 266Best-practice wound prevention and care
programmes 267Clinical results 268The impact of best-practice wound
prevention and care on health economics 272Redesigning clinical care, business and
information processes 274Indirect economic benefits 274Summary 275
Useful resources 275References 276
17 Dressings: The Healing Revolution 278Douglas Queen and Keith HardingIntroduction 278Evolution of new wound dressing
technologies 279The healing revolution 280Dressing evolution led by technology:
an example 282Patient-centred dressing evolution: an
example 282Advanced wound technologies 283The future: wound care as a
clinical specialty 284Summary 287Useful resources 287References 287
Index 291

List of Contributors
Jan Apelqvist MD, PhD, Department of Endocrinol-ogy, University Hospital of Skane, Division forClinical Sciences, University of Lund, Malmo,Sweden
Janice Bianchi MSc, BSc, RGN, RMN, PGcert TLHE,Medical Education Specialist and Honorary Lec-turer at Glasgow University, Nursing and Health-care School, University of Glasgow, Scotland, UK
Annemarie Brown MSc, BSc (Hons), RN, Tissue Via-bility Solutions, Castle Point and Rochford Pri-mary Care Trust, Southend Primary Care Trust,Southend-on-Sea, Essex, UK
Keryln Carville RN, STN (Cred), PhD, Assoc Profes-sor Domiciliary Nursing Silver Chain NursingAssociation & Curtin University of Technology,Osborn Park, Perth, Western Australia
Kim Deroo RN, MN, NP(c), Wound and ChronicDisease Management, Nursing Practice Solu-tions, Inc, Toronto, Ontario, Canada
Valerie Edwards-Jones PhD, FIBMS, FRSM, Schoolof Research, Enterprise, and Innovation, Fac-ulty of Science and Engineering, ManchesterMetropolitan University, Manchester, UK
Madeleine Flanagan MSc (Dist), BSc Hons, Cert Ed(FE), RN, School of Life and Medical Sciences,Postgraduate Medicine, University of Hertford-shire, Hatfield, Hertfordshire, UK
Keith Harding MB, FRCGP, FRCP, FRCS, Direc-tor Wound Healing Research Unit, DirectorTIME Institute, Medical School Cardiff Univer-sity, Cardiff, Wales, UK
Theresa Hurd MSN, Med, Wound and Chronic Dis-ease Management, Nursing Practice Solutions,Inc., Toronto, Ontario, Canada
David Keast BSc, Aging Rehabilitation and GeriatricCare Research Centre, Lawson Health ResearchInstitute, St Joseph’s Parkwood Hospital, Lon-don, Ontario, Canada
Arne Langøen RN, Asc. Professor, Stord/ Hauge-sund University College, Department of Health,Klingenbergvegen, Norway
Mary Martin D4 Consultancy, Dublin, IrelandJeanette Muldoon RN, Head of Clinical Services,
Activa Healthcare, Burton-on Trent, Stafford-shire, UK
Wayne Naylor BSc (Hons), PG Cert (PalliativeCare), Nat Cert (Official Statistics), PalliativeCare Council of New Zealand, Wellington, NewZealand
Patricia Price PhD, BA (Hons), CPsychol, AFBPsS,FHEA, School of Healthcare Studies, Cardiff Uni-versity, Cardiff, Wales, UK
Douglas Queen BSc, PhD, MBA, Honorary ResearchFellow, Wound Healing Research Unit Medi-cal School, Cardiff University, Cardiff, Wales,UK
Lesley Robertson-Laxton MSN, NP, Wound andChronic Disease Management, Nursing PracticeSolutions, Inc, Toronto, Ontario, Canada
Sabina Sabo RN, MN, Wound, Skin and OstomyConsultant, Nursing Practice Solutions, Inc.,Toronto, Canada

List of Contributors xi
Arlene A. Sardo NP-Adult, MS/ACNP, ENC(C),CCN(C), Wound and Chronic Disease Manage-ment, Nursing Practice Solutions, Inc., Toronto,Ontario, Canada; Faculty of Health Sciences,School of Nursing, McMaster University, Hamil-ton, Ontario, Canada
Julia Schofield MB, Department of Dermatology,Lincoln County Hospital, United LincolnshireHospitals NHS Trust, Lincoln, Lincolnshire, UK,School of Life and Medical Sciences, Universityof Hertfordshire, Hatfield, Hertfordshire, UK
Carolina Weller PhD, MEd (Research), GCHE, BN,RM, RN, School of Public Health and Preven-tive Medicine, Monash University, Melbourne,Australia
Alan Widgerow MD, MBBCh, FCS (Plast), MMed(Wits), FACS, Laboratory for Tissue Engineer-ing & Regenerative Medicine, Aesthetic & PlasticSurgery Institute, University of California, Irvine,CA, USA

Preface
Wounds are everywhere, occurring in the youngand elderly, in hospital and at home, and affectpatients in every clinical speciality around theworld. Skin breakdown impacts on a significantproportion of the global population each year andhas a major effect on sufferers, relatives, and theircarers. Many wounds and skin integrity problemsare self managed as those affected may lack accessto specialist services and professional expertise. Asa result, clinicians who manage wounds work in adiverse range of healthcare environments and theirwork involves addressing the prevention, treat-ment, care needs, and long-term support of peoplewith skin damage. Even though skin and woundproblems are one of the commonest reasons thatpeople present to their doctors, relatively few arereferred for specialist advice.
There has always been common ground betweenwound management and other clinical specialitiesincluding dermatology and vascular medicine. Butin recent years, the overlap between clinical spe-cialities concerned with the prevention and main-tenance of skin integrity has become more appar-ent as integrated pathways of care have becomewidely accepted as a way of improving continuityand collaboration among multidisciplinary teamswhich until now has not been a feature of traditionalwound care services. In recent years, an empha-sis on service integration has brought the speciali-ties of wound mangement and dermatology much
closer, together as it makes sound economic sensefor health providers to develop services which crosstraditional boundaries, promoting integrated work-ing, development of extended role practitioners,and improvements in patient care.
This book aims to reflect these trends by cut-ting across the traditional service boundaries andis designed to be of practical help to any clini-cian responsible for managing wounds and skinintegrity problems in hospitals or community set-tings including nurses, doctors, podiatrists, phar-macists, and physiotherapists. It has been writtenwith the needs of clinicians with a special interestin the promotion and maintenance of skin integrityin mind and provides the opportunity to developwound management, skin integrity, and dermatol-ogy expertise by integrating relevant aspects ofthese related disciplines into one comprehensiveresource. Thus, the primary goal for this book isto help clinicians acquire and develop advancedknowledge and skills to effectively promote andmaintain skin integrity in patients of all ages basedon the best available evidence. This supports theglobal health agenda by building and supportinga skilled workforce with the aim of maintainingand improving health within a knowledge-based,patient-centred healthcare system.
Section 1 covers Principles of Best Practice for allwound types beginning with a review of how toeffectively make evidence-based clinical decisions

Preface xiii
to improve quality of everyday practice and con-tinues with applied physiology of skin barrierintegrity and wound healing, and chapters focusingon the generic principles of wound management,wound infection, and the psychological impact ofskin breakdown.
Section 2, Challenging Wounds, considers spe-cific types of nonhealing wounds such as pressureulcers, leg ulcers, diabetic foot wounds, surgicaland malignant wounds as well as lymphoedemaand dermatological conditions associated with skinbreakdown. Section 3, Improving Skin Integrity Ser-vices examines the importance of reducing health-care costs from a clinical perspective and the needto demonstrate the value of skin integrity serviceprovision to key stakeholders. It concludes with ananalysis of the impact that advanced wound tech-nologies have had on the healing revolution andpredicts the evolution of wound management inthe future. The expert practitioners who have con-tributed to this book have willingly drawn upontheir wealth of personal experience, knowledge,and skills to share practical tips and advice pre-viously not published in a single resource.
Each chapter begins by providing an overviewof key issues and summarises the specific prin-ciples of wound management by wound type toprovide a practical guide that is accessible to clin-icians regardless of professional background, andacknowledges that in different healthcare settings avariety of health professionals may assume the leadrole for wound management and may do so withlimited resources. The book is written from a broadinternational perspective avoiding nationally spe-cific terms and agendas and addresses the need ofclinicians to access evidence-based information fora broad range of wound types and is extensivelyreferenced throughout.
Each chapter concludes with a section on pro-vision of specialist services and “further informa-tion” which lists selected, free internet resources
that have been carefully chosen because they repre-sent best practice, are evidence based, well written,and relevant to an international audience. Wherepossible, examples of current, consensus clinicalpractice guidelines are provided to support clini-cal decision making.
Chapter 15, Neglected Wounds, provides a quick,practical guide to the types of wound sometimesmismanaged due to lack of clinical experience andis written using a concise, easy-to-read style. It pro-vides key details about those wounds that are dif-ficult to heal but less commonly encountered ineveryday practice and includes essential informa-tion about factors delaying healing, complications,tips for practical wound management, and criteriafor specialist referral, and is intended to offer prac-tical, no-nonsense help for busy clinicians.
This book will be useful for anyone with aresponsibility for teaching clinicians, students, andpatients to manage wounds and skin integrity prob-lems as well as practitioners studying wound heal-ing, skin integrity, pressure ulcer prevention, der-matology, and palliative care as part of sciencedegrees for doctors and health professionals alliedto medicine, and those with a research interest inskin integrity and wounds.
The global wound care community is a tight-knitgroup of dedicated and enthusiastic health profes-sionals who are keen to share their knowledge andexperience to improve the life of patients with com-promised skin integrity. I am pleased to observe thatthis community is growing year on year as practi-tioners researchers, and healthcare industry gainknowledge and push the boundaries about what ispossible to improve the lives of patients with non-healing wounds. If this book helps one clinician heala single patient’s wound, then the effort involvedwill have been well worth it.
Madeleine Flanagan

Acknowledgements
My thanks go to all the health professionals andpatients I have had the privilege to meet dur-ing my career who have stimulated my inter-est in chronic wounds, to my students for ask-ing difficult questions and giving me the impe-tus to capture current thinking in a book, andto my contributors who were handpicked fortheir specialist knowledge and practical exper-
tise. But most of all, special thanks goes to Edand Max who have lived through the writing,editing, and proof reading of this book – with-out whose unfailing support, I just couldn’t havedone it.
This book is dedicated to Maxwell Coupland whois a very special little boy.

Section 1Principles of Best Practice


1 Evidence and ClinicalDecision-making
Carolina WellerSchool of Public Health and Preventive Medicine, Monash University, Melbourne, Australia
Overview� Evidence-based practice integrates the best available research evidence with information about patient preferences, clini-
cian skills and available resources to make decisions about patient care.� Barriers to the use of research-based evidence can occur when time, access to the literature, search skills, critical appraisal
skills and implementation skills are lacking.� Evidence-based clinical decision-making requires comparison of all relevant sources. In the absence of randomised
controlled trials involving a direct comparison of treatments of interest, indirect treatment comparisons and systematicreviews provide useful evidence.
� Clinical guidelines appear to be one of the most effective methods of applying evidence to improve quality of care butlittle is known about the best way to implement them into everyday practice.
� Selective reading of high-quality evidence is one of the most effective strategies to improve research dissemination andchanges in practice. There are now good sources of evidence-based information available on the Internet that help identify,appraise and apply research findings to clinical practice.
Introduction: what is effective clinicaldecision-making?
Clinical decision-making is an essential part ofeffective wound management and is based onclinical judgement which consists of professionalperformance and human judgement. Health careproviders increasingly recognise the importanceof making decisions based on the best possible
evidence. Making decisions that will impact on thehealing outcome of individuals in the clinical work-place take place every day but reliability of clinicaljudgement is often variable as many different fac-tors will influence decisions; these include the typeof clinical setting, interpersonal relationships, avail-able diagnostic data, scope of practice and individ-ual skill (DiCenso et al., 2010). The process of clin-ical decision-making should ideally include use of
Wound Healing and Skin Integrity: Principles and Practice, First Edition. Edited by Madeleine Flanagan.C© 2013 John Wiley & Sons, Ltd. Published 2013 by John Wiley & Sons, Ltd.

4 Wound Healing and Skin Integrity
research findings, clinical guidelines, and evidence-based treatment algorithms (Rose, 2011). Improvingthe implementation of evidence-based practice(EBP) and public health depends on behaviourchange. Health care outcomes such as choice of typeof compression to encourage patient adherence tocompression therapy are often based on decisionsmade within an organisation, which adds anotherlayer of complexity to clinical decision-making.Clinical decisions that impact directly on patientsafety and quality of care are made by healthprofessionals based on previous knowledge andexperience. The care received by patients in relationto wound care is often dependent on factors that arerelated to characteristics of individual health pro-fessionals, such as education and training in woundcare as well as behaviour of people in the workplace(Grol, 2002). For patients to benefit from treatment,clinicians must have a mastery of skills, includinghistory-taking and physical examination, althougheffective clinical decision-making does not begin orend there, continuous, self-directed lifelong learn-ing is paramount to advance wound managementand improve quality of care.
What is evidence-based health care?
Best practice research evidence refers to method-ologically sound, clinically relevant research aboutthe effectiveness and safety of interventions, theaccuracy and precision of assessment measures,the power of prognostic indicators, the strength ofcausal relationships, the cost-effectiveness of inter-ventions and the meaning of illness or patient expe-riences (Sackett et al., 1996).
Over 10 years ago, the Cochrane systematicreviews (Cullum et al., 2000; O’Meara et al., 2009)reported the importance of multi-component com-pression bandages to heal people with venous legulcers (VLUs) and the importance of Ankle BrachialPressure Index (ABPI) assessment to exclude arte-rial disease prior to compression application. Thistype of evidence should guide clinical practice, butwhat if the clinician does not have access to a hand-held Doppler and is unable to refer to a vascularlaboratory or specialist wound clinic due to geo-graphical or cost factors? Even if a Doppler is avail-able the clinician may not have the confidence toassess the patients and measure the ABPI as found
in a recent cross-sectional survey of practice nurses(PNs) working in Australian general practice clin-ics. This study identified that knowledge of VLUmanagement was sub-optimal and current practicedid not comply with evidence-based VLU manage-ment guidelines (Weller and Evans, 2012). Despiterecognition by PNs that specialist wound clinicsprovide a valuable resource, more than 40% didnot refer patients for treatment and a third retainedpatients for over 3 months before referring them forspecialist assessment. In the United Kingdom, PNstypically have sole responsibility for determiningthe patient’s treatment plan (Ertl, 1992; McGuckinand Kerstein, 1998). Despite 70% of PNs havingsome responsibility for determining VLU manage-ment, less than 20% stated that they used bestpractice guidelines to direct treatment (Weller andEvans, 2012).
Despite availability of evidence to support legulcer management, studies have identified deficien-cies in general practice management of leg ulcer-ation, specifically the under-use of ABPI measure-ments, over-reliance on dressings and lack of under-standing of compression therapy (McGuckin andKerstein, 1998; Graham et al., 2003; Sadler et al.,2006).
Research evidence alone is never sufficient tomake a clinical decision. Clinicians often weighup the benefits and risks, inconvenience and costsassociated with alternative management strategies,and in doing so consider the patient’s values.Patient values and preferences refer to the under-lying assumptions and beliefs that are involvedwhen clinicians, together with patients, weigh whatthey will gain making a clinical management deci-sion such as choosing a compression system thatis easy for the nurse to apply, is less expensiveand is more comfortable for the patient. Heal-ing time can be improved simply by addressingthe issue of nurse application, patient adherenceand cost-effectiveness (Weller et al., 2010b, 2010c).EBP involves the incorporation of research evi-dence, clinical expertise and client values in clinicaldecision-making (Sackett et al., 1996). Applicationof high-quality evidence to clinical decision-makingrequires knowledge of how to access evidence in thefirst place; includes an understanding of literaturesearching and application of critical appraisal skillsto differentiate lower- from higher-quality clinicalstudies (Weller, 2009).

Evidence and Clinical Decision-making 5
Common misperceptions aboutevidence-based practice
� Clinicians believe they already ‘do’ EBP;� EBP is a passing trend;� EBP leads to ‘cook book’ medicine;� EBP is expensive and time-consuming;� EBP is a restriction of clinical freedom;� ‘I have always done it this way, so I know it
works’.
How does evidence fit into clinicaldecision-making in clinical practice?
The skills necessary to provide an evidence-basedsolution to a clinical problem includes severalaspects such as defining the problem, conducting anefficient search to locate the best evidence, criticallyappraising the evidence and considering that evi-dence and its implications in the context of patients’circumstances and values (Box 1.1).
Clinicians report that the major barrier to usingcurrent research evidence is time, effort and skillsneeded to access the right information (Cabanaet al., 1999). A high proportion of new researcharticles are peer reviewed and published, althoughthe addition of systematically combining resultsin context of other similar studies is still lack-ing. Ideally, clinicians could access updated well-conducted systematic reviews for all clinical ques-tions, however only about 10% of randomised con-trolled trials (RCTs) are incorporated in Cochranereviews (Mallett and Clarke, 2003) and at least 90%of reviews recommended further research (El Dibet al., 2007). Despite these limitations, systematicreviews can improve decision-making (Box 1.2).
EBP integrates the best available research evi-dence with information about patient preferences,clinician skill level and available resources to makedecisions about patient care (Sackett et al., 1996).Attaining these skills requires knowledge, motiva-tion and application (Guyatt et al., 2000). Clini-cians often have questions about the care of theirpatients, but many go unanswered (Dawes andSampson, 2003). Barriers to the use of research-based evidence can occur when time, access to jour-nal articles, search skills, critical appraisal skills andunderstanding of the language used in research arelacking.
The aim of evidence-based health care is toprovide the appropriate means for making effec-tive clinical decisions, not only for avoiding habit-ual practice but also for enhancing clinical per-formance. An EBP culture connects research evi-dence, patient preferences, the available resourcesand clinical expertise, to include these factors inthe decision-making process. Clinical judgementprovides health professionals with a methodologyfor comparing decisions between practitioners withdifferent training and experience, and improvingdecision-making. Keeping up to date with woundcare research is a mammoth task and is a chal-lenge for busy clinicians. Evidence-based healthcare requires clinicians to engage with research evi-dence in decision-making at the workplace. But isit unrealistic to assume that research results willbe implemented in clinical practice as translationalresearch can be hindered by two main aspects: howthe evidence is generated, and how the evidenceis implemented? When generating evidence, onemajor barrier to uptake of research into clinicalpractice is that the ‘practice’ described in clinicaltrials or research environments may not be gen-eralisable from the setting (hospital community),circumstances (number of clinicians with woundmanagement knowledge), patient groups (chronic,acute wounds) and resources (Doppler ultrasound,wound dressings, compression bandages) availablein daily practice of many clinicians.
For evidence to be translated to clinical practicethe clinician needs to be aware of the evidence,and accept and adhere to findings. Although it isbroadly accepted that effective health care deci-sions require the integration of research evidenceand individual preferences, it is not unusual to findthat evidence generated by researchers does notalways get implemented in a timely and depend-able way and may not take into account patientinput (Cabana et al., 1999). One could questionwhether practitioners and patients benefit from cur-rent best practice and whether EBP affects treat-ment outcomes in a positive way when research thatshould change practice is often ignored for years,for example pressure ulcer risk assessment and pre-vention, moist wound healing principles (Winter,1995, 1962, 2006; Cullum et al., 2000) and com-pression for treatment of venous ulcers (Fletcheret al., 1997; Cullum et al., 2001; O’Meara et al.,2009).

6 Wound Healing and Skin Integrity
Box 1.1 Steps for appraising the literature
1. Ask an answerable question from a clinical issue
PICOT is one technique that can used to develop clinical research questions. PICOT is an acronym for the five different areasthe technique considers: patient/population, intervention or issue, comparison with another intervention or issue, outcomeand timeframe; e.g. Which interventions help people adhere to compression therapies for venous leg ulceration?
2. Search for valid external evidence
Quick access to pre-appraised information is available at
� The Cochrane Library� PubMed Clinical Queries� ACP Journal Club� Evidence-based Medicine
3. Critically appraise the evidence for relevance and validity
Methods
Consider
� Study design, e.g. randomised controlled trial, cohort study, survey;� Clinical setting, e.g. hospital, community;� Patient population, e.g. sample size, inclusion/exclusion criteria;� Describe intervention group and control group;� Blinding (if applicable), e.g. double blind, single blind;� Statistical analysis, e.g. suitability of tests;� Relevance of outcome measures, e.g. time to complete healing;� Follow-up, e.g. duration, all patients accounted for.
Results
Consider
� Relevance of outcomes, e.g. number needed to treat, sensitivity, specificity;� Time points of reporting;� Compliance with intervention/therapy/medications;� Adverse effects.
4. Apply the results back to the patient
There is low-quality evidence that leg ulcer clinical care may not improve adherence to compression therapy or healing ratesor prevent recurrence when compared to home care. Because of the lack of reliable evidence, it is not possible to recommendnurse clinical care interventions. There is a need to improve and increase interaction with patients emphasising the adherencein future compression trials (Field, 1994).
5. Record the information for the future
Audit your clinical practice by checking your everyday practice against published EBP on a regular basis.
Although EBP has an increasingly broad-basedsupport in health care, it remains difficult to gethealth care professionals to engage and practice it(Thompson et al., 2005). Across most domains in
wound care, practice has lagged behind researchand knowledge by at least several years andoften longer (Bates et al., 2003). There are manyimpediments to introducing evidence and clinical

Evidence and Clinical Decision-making 7
Box 1.2 Summary of systematic review: compression for venous leg ulcers (O’Meara et al., 2009)
Objectives: To undertake a systematic review of all RCTs of the clinical effectiveness of compression bandage or stockingsystems in the treatment of venous leg ulceration.
Specific questions addressed by the review are
� Does the application of compression bandages or stockings aid venous ulcer healing?� Which compression bandage or stocking system is the most effective?
Search strategy: For this update the Cochrane Wounds Group Specialised Register (14/10/08) was searched; the CochraneCentral Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 4 2008); Ovid MEDLINE (1950 to October Week1 2008); Ovid EMBASE (1980 to 2008 Week 41); and Ovid CINAHL (1982 to October Week 1 2008). No date or languagerestrictions were applied.
Selection criteria: RCTs recruiting people with venous leg ulceration that evaluated any type of compression bandage systemor compression hosiery were eligible for inclusion. Comparators included no compression (e.g. primary dressing alone, non-compressive bandage) or an alternative type of compression. Trials had to report an objective measure of ulcer healing inorder to be included (primary outcome for the review). Secondary outcomes of the review included ulcer recurrence, costs,quality of life, pain, adverse events and withdrawals. There was no restriction on date, language or publication status of trials.
Data collection and analysis: Details of eligible studies were extracted and summarised using a data extraction table. Dataextraction was performed by one review author and verified independently by a second review author.
Main results: Overall, 39 RCTs reporting 47 comparisons were included. Review question 1: there was reasonable evidencefrom seven RCTs that venous ulcers heal more rapidly with compression than without. Review question 2: findings from sixtrials of single-component compression suggested that this strategy was less effective than multi-component compression.
Authors’ conclusions: Compression increases ulcer healing rates compared with no compression. Multi-component systemsare more effective than single-component systems. Multi-component systems containing an elastic bandage appear moreeffective than those composed mainly of inelastic constituents.
guidelines into routine daily practice (Grol andGrimshaw, 2003).
One aspect that researchers need to considerwhen designing a clinical trial is that the popula-tion, measurement tools and interventions will berelevant to the clinical patient group. Some haveargued that RCTs are too limited (Gottrup, 2010;Gottrup and Apelqvist, 2010) but others disagreeand argue that wound care research needs high-level evidence reported in a transparent way so clin-icians and health policymakers can improve woundcare with the best available evidence to guide prac-tice (Barton, 2000; Weller et al., 2010d; Weller andMcNeil, 2010). For implementing evidence, clinicalguidelines appear to be one of the most promisingand effective tool for improving the quality of carebut little is known about the optimal implemen-tation strategy. There are many good examples ofinternationally agreed clinical guidelines in woundmanagement that define best practice and are easyto implement to guide local practice (SIGN, 2010;Australian Wound Management Association Inc.and New Zealand Wound Care Society Inc., 2011).
Challenges to changing practice
Even when most clinicians are aware of evidence,there may be little impact on quality of care due tothe many complexities involved in changing prac-tice. Change within organisation structures may behindered by many factors, and barriers to trans-forming clinical competence into clinical perfor-mance can arise due to varied reasons (Thomp-son et al., 2005). For example, the patient or healthcare system may not be able to afford effective bestpractice treatments. Practitioners may experienceexcessive workloads, inadequate practice organisa-tion, financial pressures and lack of time they areable to spend with each patient which may resultin less than optimal care. To introduce evidenceinto clinical practice it is appropriate to identifythe groups affected by the proposed change/s inpractice. It is paramount to assess the preparednessof the group to change and identify likely enablingfactors, including resources, skills and knowledge.
In addition, the practice of ‘traditional habits’,e.g. failing to apply compression bandage routinely

8 Wound Healing and Skin Integrity
in people with venous ulcers (omission) or inap-propriate use of ‘new’ dressing (commission) canimpact negatively on healing outcomes and qualityof life for people with chronic wounds. Althoughindividual clinical practice environments will varyfor each health professional, aspects such as pro-fessional discipline, availability of information andcurrent resources in the workplace need to be con-sidered when considering change to health ser-vice environment. The amount, structure and typeof clinical information available are often out ofdate, not evidence based, variable across clinicaldomains and not centrally organised on informa-tion which leads to uncertainty associated with clin-ical decision-making. However, the first hurdle toovercome is the awareness and ability to identifyhigh-quality evidence.
Health professionals work in different set-tings/institutions with differing levels of expertiseand may handle similar decisions very differently.Clinical organisations limit or shape choices associ-ated with clinical decisions. Some solutions devel-oped in one place may not be directly transferableor applicable to another health care environment orpatient group. Although there are many RCTs andpublished systematic reviews in wound care pro-viding information on decisions about compressiontherapy as the best practice treatment for peoplewith VLUs, there are still examples of lack of com-pression application by some communities and PNs(Annells et al., 2008; Newall et al., 2009). Evidence-based health care decision-making requires com-parison of all relevant competing interventions. Inthe absence of RCTs involving a direct compari-son of all treatments of interest, indirect treatmentcomparisons and network meta-analysis provideuseful evidence for judiciously selecting the besttreatment(s) (Hoaglin et al., 2011). To implementan intervention requires both access and knowl-edge. For compression, this is challenging enough;becoming familiar with the many different types ofbandages, contraindications of application, adverseeffects and monitoring require improved educationand better specific training in wound care to lead tobetter wound care outcomes for patients (Gottrup,2004). Patients must also contend with competingclaims and advice from clinicians, adverse effects;or the fear of, and sometimes the lack of funding topay for compression treatments.
EBP implementation remains limited in clinicalpractice. There are practical problems of implemen-
tation, which include training, access to research,and development of and access to tools to dis-play evidence and support for decision-making.There may also be practical difficulties of imple-mentation due to the disease burden of the patientgroup, funding models and workforce shortageswhich have been reported to have hindered suc-cessful adoption of evidence-based strategy thatwas known to improve health outcomes in a woundcare group. A supportive professional environmentcan greatly influence the use of research-based evi-dence to inform clinical decisions of an individual(Spring, 2008).
Factors influencing clinical judgement
Clinical decision-making is the ability to sift andsynthesise information, make decisions and appro-priately implement them. Clinical decision-makingis a complex process whereby practitioners deter-mine the type of information they collect, recog-nise problems according to the cues identified dur-ing information collection, e.g. wound assessment,and then decide upon appropriate interventions toaddress those problems (Sox et al., 2010).
Although many factors influence the decision-making process, there are a myriad of other factorsthat serve as barriers to this process. Even whenclinicians know and accept what to do, it is possiblethat with workloads they forget or neglect to do it(Glasziou and Haynes, 2005). To achieve effectiveclinical decision-making, health professionals needto be encouraged to make decisions and assumeresponsibility for their decisions. Evidence fromsuccessful health service change projects suggeststhat an environment that is genuinely collabora-tive, cooperative, democratic and involves all stake-holder groups including the patient is imperativefor success (Atallah, 1999; Adderley and Thomp-son, 2007; Grol et al., 2007; Avorn and Fischer, 2010).Factors affecting decision-making must be iden-tified and aspects such as adequate time, techni-cal support and sufficient resources to implementthe proposed change must be evaluated to encour-age shared decision-making. These factors must beunderstood, the barriers be identified and strate-gies to minimise these barriers be developed andimplemented (Griffin et al., 2011). Habits do notchange easily, despite best intentions. Omissions areparticularly easy for preventive measures such as
Evidence and Clinical Decision-making 9
compression hosiery when the venous ulcer hashealed, as these aspects are not the pressing focusof the management visit.
Patient safety and quality of care will bene-fit from clarification of decision-making strategies,in the development of guidelines and care path-ways. Clinical decision support may include a vari-ety of tools (printed and electronic) that makeknowledge and information available to the clin-ician to access important information (Kawamotoet al., 2005). Much has been written about effectingorganisational change within health care (Oxmanet al., 1995; Walter et al., 2003; Davies et al.,2008; Wilkinson et al., 2011) and more recently inwound health care (Gottrup et al., 2010), thoughthe need to further promote knowledge and evi-dence to already busy health professionals canbe improved. Groups such as the Cochrane Col-laboration, national health and research organisa-tions such as the National Health Scheme, NationalHealth and Medical Research Council, NationalInstitute of Clinical Studies Joanna Briggs Cen-tre and high-quality wound journals that providehigh-quality appraisal of research findings andexisting evidence can help the clinician to takeup the information offered. Some resources avail-able include, but are not limited to, the NHS Evi-dence Base, American College of Physicians (ACP)database/journal updates journal clubs, onlineservices, BMJ clinical, EBM/Practice Databases,EBM clinical decision support, DYNAMED clini-cal, Database of Abstracts of Reviews of Effective-ness Centre, Centre for Evidence-Based Medicine,McMaster University Evidence Based Medicine.
Even when high-quality syntheses of evidence ispresented to clinicians, the information presentedwill be shaped by the clinician’s previous knowl-edge (Davies et al., 2008). Clinician’s experience isthen connected to the context and culture whereindividuals work, as well as to their role and posi-tion in the organisation to shape effective use andimplementation of evidence in practice. One aspectthat has been successful in part is the initiationof wound care champions (McNees and Kueven,2011) who take on the responsibility of promotingeffective change using research evidence to improvequality of care for people with compromised skinintegrity.
Personal contact with respected wound care anddermatology colleagues can bring about change,although it is imperative that these key leaders are
competent in identifying and critically appraisingthe best available evidence and take responsibil-ity for designing and implementing research that isrobust. This mechanism may not work if the profes-sional practice of these distinguished and respectedwound care experts includes traditional unprovenways of doing things and may in turn be highlyresistant to effective implementation of evidence-based care. To achieve EBP in wound care, clini-cal decision-making should be scientifically based.Future research should focus on which interven-tions are most effective in optimising wound heal-ing, as well as investigating cost-effectiveness oftreatment (Cowan and Stechmiller, 2009).
Evidence-based practice: hierarchyof evidence
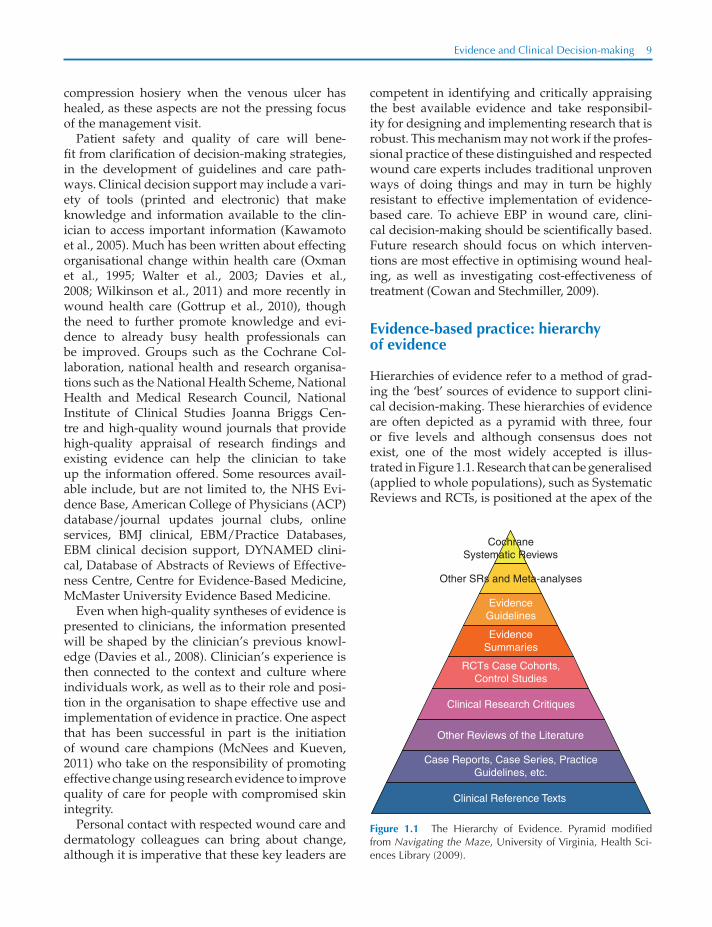
Hierarchies of evidence refer to a method of grad-ing the ‘best’ sources of evidence to support clini-cal decision-making. These hierarchies of evidenceare often depicted as a pyramid with three, fouror five levels and although consensus does notexist, one of the most widely accepted is illus-trated in Figure 1.1. Research that can be generalised(applied to whole populations), such as SystematicReviews and RCTs, is positioned at the apex of the
EvidenceSummaries
RCTs Case Cohorts,Control Studies
Clinical Research Critiques
Other Reviews of the Literature
Case Reports, Case Series, PracticeGuidelines, etc.
Clinical Reference Texts
EvidenceGuidelines
CochraneSystematic Reviews
Other SRs and Meta-analyses
Figure 1.1 The Hierarchy of Evidence. Pyramid modifiedfrom Navigating the Maze, University of Virginia, Health Sci-ences Library (2009).

10 Wound Healing and Skin Integrity
pyramid and evidence where it is not appropriateto generalise, such as data obtained from qualita-tive research and expert opinion, is usually foundat the bottom of these hierarchies. The hierarchyindicates the relative importance that can be givento a particular study design. The higher a method-ology is ranked, the stronger it is assumed to be.At the top is the systematic review/meta-analysiswhich integrates results of a number of similar tri-als to produce findings of higher statistical power.At the bottom is the opinions of respected author-ities, e.g. consensus clinical guidelines thought toprovide the weakest level of evidence.
Systematic reviews
A systematic review is a way of summarising theresults of multiple research studies in a format thatgives a critical assessment of the efficacy and safetyof the specific intervention under review. The mainobjective of a systematic review is to provide sum-mary information to help clinicians make decisionsabout health care interventions based on best evi-dence available (Box 1.2).
Systematic reviews are a very efficient way toaccess the body of research as they save timefor busy clinicians who can read a critical syn-opsis of current research evidence in one docu-ment. Searches are undertaken on multiple elec-tronic databases such as CENTRAL and includeMEDLINE, EMBASE and other specialist databases(e.g. TRoPHI, CINAHL, LILACS), which ensure acomprehensive search. The search strategy oftenincludes grey literature, trials registers citations, ref-erences and may include contacting experts in thefield and are not limited by language, year, loca-tion and publication status. A systematic reviewof the literature differs from a literature review,being based on a scientific design, which aims toreduce bias and increase reliability and provide acomprehensive picture of all of the available evi-dence. The information available in a systematicreview includes critical appraisal, interpretation ofresults and reliable basis for decision-making forhealth care, policy and future research.
Cochrane systematic reviews (Cochrane WoundGroup) aim to bring together the body of evidenceto inform decision-making. Cochrane reviews arepeer reviewed, updated regularly and are free ofconflicted funding. Protocols are published prior toreview and outline the question definition, eligibil-
ity criteria and outcome measures to reduce impactof bias and are published in The Cochrane Library.Cochrane reviews can be accessed via the CochraneLibrary: www.thecochranelibrary.com
A systematic review is comprised of� clearly stated objectives;� pre-defined eligibility criteria;� explicit, reproducible methodology;� a systematic search;� assessment of validity of included studies;� systematic synthesis and presentation of find-
ings.
Other sources of systematic reviews include� Agency for Healthcare Research and Quality:
www.ahrq.gov;� Joanna Briggs Institute: www.joannabriggs.edu
.au;� BMJ Clinical Evidence: www.clinicalevidence
.com;� Bandolier: www.medicine.ox.ac.uk/bandolier.
Randomised controlled trials
The RCT is considered the best research design todetermine the effectiveness of health care interven-tions. Study participants are randomly assigned toreceive a new intervention (experimental group) orstandard intervention or no intervention (controlgroup). Randomisation should ensure that chancedetermines the allocation of participants to onegroup or other so that the only difference betweenthe two groups should be the intervention. Partic-ipants progress is monitored over a specified timeperiod (follow up) and then specific outcomes areevaluated. The random allocation of participantsis used to ensure that the intervention and controlgroups are similar in all respects (which is diffi-cult in chronic conditions) with the exception of thetherapeutic or preventative measure being tested(Weller et al., 2010a, 2010c).
Practice point
Is the RCT the best way to provide the evidence baseto support wound management decisions?
Originally in medicine RCTs were perceived as the ’goldstandard’ in terms of levels of evidence and research.In contrast, social science approaches used to explore

Evidence and Clinical Decision-making 11
aspects of patient experience have traditionally beenundervalued and seen as unscientific. However, in 1995,Gyatt et al. recognised the greater value of systematicreviews and meta-analyses as they form a comparativeanalysis of research. Since then, concerns have beenraised about the ranking of evidence in relation to whichis the most relevant to clinical practice.
The hierarchy is not fixed and there is debate aboutthe relative positions of different research methodologies.Although the RCT is traditionally considered as being anobjective method of removing bias, its design is expen-sive, slow and produces results that may not reflect every-day practice. Methodologies that are lower in ranking arenot always inferior, for example a well-conducted obser-vational study may provide more convincing evidenceabout a treatment than a poorly conducted RCT. Althoughrandomised studies are considered more robust, it wouldbe unethical to perform an RCT which exposed patientsto a risk of skin integrity breakdown, for example a studyevaluating the effect of no intervention in patients at highrisk of pressure ulceration.
Finally, the evidence hierarchy focuses on quantita-tive research methodologies; however, it is important tochoose the most appropriate study design to answer theresearch question. For example, it is usually not possibleto identify individual’s feelings and personal experienceof living with a chronic wound such as a leg ulcer withoutusing qualitative techniques.
It is therefore important for health care professionalsto develop skills to critically evaluate a range of sourcesof evidence and to raise awareness of the value of eval-uating a balanced portfolio of credible evidence whensuggesting changes to practice.
Evidence-informed decisions
As stated by Sackett, almost 15 years ago, exter-nal clinical evidence can inform, but can neverreplace, individual clinical expertise, and it is thisexpertise that decides whether the external evi-dence applies to the individual patient at all and,if so, how it should be integrated into a clinicaldecision. Similarly, any external guideline mustbe integrated with individual clinical expertise indeciding whether and how it matches the patient’sclinical state, predicament and preferences, andthus whether it should be applied (Sackett et al.,1996).
A busy clinician will look for the result overview.Aspects such as the type of study, the type of par-ticipants and the outcome measures are importantas these should be evaluated in their own context
of clinical practice. Some questions that will helpwhen weighing up the relevance of evidence are
(1) Are the participants described similar to mypatient group?
(2) Is the intervention something that is used inmy practice?
(3) Is the setting similar to my clinical practiceenvironment?
(4) Are the resources used in the study availablein my clinical practice for my patient group?
If the answers to these questions are yes, clini-cians can make a judgement about the overall qual-ity of evidence based on the criteria as follows:
� risk of bias;� heterogeneity;� precision;� reporting bias;� generalisability;� quality (level) of evidence.
The Grading of Recommendations Assessment,Development and Evaluation (GRADE) WorkingGroup has developed a commonsense and trans-parent approach to grading quality of evidence andstrength of recommendations. Many internationalorganizations endorse this approach includingthe World Health Organisation and the CochraneCollaboration.
Critical appraisal frameworks
Critical appraisal of research includes both qualita-tive and quantitative methods, though concentrateson the analysis of the approaches taken to dataanalysis. Applying a framework of questions to cri-tique a paper allows the reader to critically appraisepublished work, identify its strengths and limi-tations and give opportunities to make informedjudgements about the study (Box 1.3). The criti-cal appraisal of published research can inform thedevelopment of research questions, hypothesis andmethodological approaches, or confirm that thebody of knowledge that exists is sufficiently robust.Appraising any publication requires three mainelements:
(1) What are the results?(2) Are the results of the study valid?(3) Are the results applicable to my patients?

12 Wound Healing and Skin Integrity
Box 1.3 Assessing validity: checklist for various study designs
RCT
� Was the randomisation method outlined adequately?� Was the randomisation method concealed?� Were treatment and control groups similar in characteristics (age, gender, etc.) at baseline?� Were patients and clinicians blinded to treatment?� Were outcomes assessed objectively?� Were all patients starting trial accounted for at conclusion?� Were patients analysed in the groups to which they were randomised, e.g. analysed by intention to treat?
Cohort
� Is the study prospective or retrospective?� Were the control and study group similar in characteristics at baseline (except for exposure)?� Were all patients starting the trial accounted for at conclusion?� Were researchers conducting assessment of outcome blind to exposure status?� Were the main potential confounders identified and taken into account in the analysis?
Case–control
� Were the cases clearly defined?� Were cases and controls taken from comparable populations?� What percentage of cases and controls participated in the study?� Were study measures identical for cases and controls?� Were study measures objective or subjective and is recall bias likely if they were subjective?� Were the main potential confounders identified and taken into account in the analysis?
Cross-sectional study
� Was the study sample clearly defined?� Was a representative sample achieved?� Were all relevant exposures, potential confounding factors and outcomes measured accurately?� Were patients with a wide range of severity of disease assessed?
Case study
� Were cases identified prospectively or retrospectively?� Are the cases a representative sample?� Were all relevant exposures, potential confounding factors and outcomes measured accurately?
Other considerations
� Discuss strengths and weaknesses of study (internal and external validity, see above).� Discuss the study in context of other available literature and/or current standard of care.� What is the best study design for investigating the research question?� Can the study outcomes be generalised to your patients?� What are the clinical implications of this study?

Evidence and Clinical Decision-making 13
Specific frameworks such as the ConsolidatedStandards of Reporting Trials (CONSORT) state-ment (Moher et al., 2010) provides guidance onhow to conduct a rigorous RCT for researchersbut it can also be used by clinicians as a frame-work when appraising the results. The CONSORTstatement has the potential to play a crucial rolein influencing the quality of research and clinicalpractice and to improve wound care. Implemen-tation of the CONSORT statement can clarify tothe reader what exactly was done in the RCT, towhom and when, so that practitioners and healthcare providers can determine study validity and rel-evance to their patient group. RCTs are one method-ological approach to add to the body of evidencewhich can inform clinical practice. There are manyother quantitative and qualitative approaches thatcan also inform clinical practice.
Clinical guidelines
Clinical guidelines are ‘systematically developedstatements to assist clinician and patient decisionsabout appropriate healthcare for specific circum-stances’ (Field, 1994). The main purpose of clinicalguidelines is to help clinicians provide quality careand to aid in the evaluation of that care with bestpractice. The development and implementation of(evidence-based) clinical practice guidelines is oneof the promising and effective tools for improvingthe quality of care (Barker and Weller, 2010). How-ever, many guidelines are not used after dissemina-tion. Implementation activities frequently produceonly moderate improvement in patient manage-ment (Grol and Buchan, 2006; Grol, 2010). Clinicalwound care practice guidelines, including specificguidelines for VLUs, skin tears, diabetic foot, pres-sure ulcers, are now available in many countries(SIGN, 2010) and most take time and resources tocollate and distribute.
Practice point
There are many clinical guidelines available for woundand skin care; almost every country has its own version ofclinical practice guidelines. Clinicians are faced with thedilemma of choosing from an abundance of guidelinesof variable quality or developing new guidelines of theirown.
Clinical guidelines should be critically evaluated toensure that they
� focus on aspects of care delivery that are concernedwith difficult decisions or choices to make clinicalmanagement easier;
� are based on current scientific evidence drawn fromwell-designed clinical trials or meta-analyses and cleararguments based on clinical skills and experience;
� contain clear practice recommendations that provide aclear description of desired performance and specificadvice about what to do in which situation and whichfactors should be taken into account;
� are compatible with existing norms and values of clin-icians and are not too controversial.
(Burgers et al., 2003)
As users of clinical practice guidelines, healthcare professionals need to know how much con-fidence they can place in the practice recommenda-tions made. Systematic methods of making judge-ments can reduce errors and improve communi-cation, although some guidelines contradict otherpublications. A system for grading the quality ofevidence and the strength of recommendations thatcan be applied across a wide range of interventionsand contexts has been developed (Brouwers et al.,2010). Clinical judgements about the strength of arecommendation require consideration of the bal-ance between benefits and harms, the quality ofthe evidence and translation of the evidence intospecific circumstances. Understanding of EBP isa useful resource when making such judgements.Resource utilisation or how cost-effective the inter-vention is often lacking in published study results.Good evidence for the cost-effectiveness of manytreatments aimed at improving skin integrity arelacking (Grimshaw et al., 2004).
Summary
There is an international effort to improve evidence-based, cost-effective and accountable clinical prac-tice. In Australia, the National Health and HospitalsReform Commission has a strong focus on continu-ous learning and evidence-based improvements tohealth care delivery (Bennett, 2009). In the UnitedStates, the Institute of Medicine is building the con-cept of a value and science-driven learning healthcare system that is effective and efficient; and in the

14 Wound Healing and Skin Integrity
United Kingdom, guidance from the National Insti-tute for Health and Clinical Excellence, combinedwith quality and outcome frameworks that includefinancial incentives, seeks to align clinical practicewith best available evidence (Scott, 2009; Scott andGlasziou, 2012).
Evidence-based guideline development reflectsone approach to improving patient care: it assumeshealth professionals are rational decision-makerswho will act on convincing information. A beliefthat developing and disseminating systematicreviews and guidelines will improve patient out-comes ignores the complexity of change in healthcare. Guidelines do not implement themselves, theyneed to be developed, well executed and sustainedin implementation programs and even then suchprogrammes usually have only a moderate effect onperformance in terms of improvements in patientcare (Solberg et al., 2000). Many factors play crucialroles in hindering changes in health care. These fac-tors are related not only to professional decision-making but also to patient behaviour, interactionwith colleagues, team functioning and organisa-tional conditions for change, resources and eco-nomic or legal conditions (Grol and Buchan, 2006).Challenges can arise when clinical guidelines areintroduced into routine daily practice as cliniciansfind it difficult to be aware of all the relevant validevidence due to the volume of published research.Plans for change in practice should be based oncharacteristics of the evidence or guideline itselfand barriers and facilitators to change (Grol andGrimshaw, 2003). Some barriers to adoption of evi-dence may be information overload as it is notuncommon that clinicians find it difficult to beaware of all published evidence as there are so manyjournals to consider. Even if evidence is accepted,clinicians and guidelines may not target correctgroups. To carry out a clinical intervention requiresboth access and knowledge.
Evidence-based research provides informationon which to base clinical decisions and a supportfor decision-making by providing best outcomedata. Comparative effectiveness research using sys-tematic review analysis to compare similar treat-ments or procedures in maximising the choice ofthe most effective cost/benefit option within thecontext of best evidence is a valuable adjunct to pro-tect patients from ineffective or harmful treatments(Lean et al., 2008).
Translational research is the process evolvingfrom EBP that translates the results of clinicaltrials into sustainable changes in practice (Leanet al., 2008). It has become a useful tool inimproving decision-making in the clinical settingand was developed to be a foundation betweenresearchers, clinicians and patients. Translationalresearch using evidence-based and comparativeeffectiveness research will continue to evolve, andmay prove to be a useful tool to improve decision-making in the clinical setting (Bauer and Chiappelli,2010). EBP that integrates best available researchevidence with information about patient prefer-ences, clinician skills and available resources canimprove clinical decisions in wound care.
Useful resources
Canadian resources
http://ktclearinghouse.ca – The KT Clearinghouse web-site is funded by the Canadian Institute of HealthResearch (CIHR) and is a comprehensive resourceincorporating the Centre for Evidence Based Medicinein Toronto.
McMaster University.
European resources
www.thecochranelibrary.com – Cochrane SystematicReviews covers all areas of clinical practice includingthe Cochrane Skin Group and the Cochrane WoundGroup.
www.cks.nhs.uk – It provides summary of evidence-based clinical guidelines (UK).
www.evidence.nhs.uk – National Health Service (UK)approved evidence website.
International resource
The GRADE system to evaluate the quality (level) of evi-dence and strength of recommendations. Available at:www.gradeworkinggroup.org.
Useful critical appraisal frameworks
CONSORT (Consolidated Standards of Reporting Tri-als) Transparent Reporting of Trails. Available at:http://www.consort-statement.org/home/

Evidence and Clinical Decision-making 15
Registered Nurses Association of Ontario. Available at:www.rnao.org/bestpractices
NHS National Institute for Health and Clinical Studies.Available at: www.guidance.nice.org.au
Critical Appraisal Skill Program (CASP). Available at:www.phru.nhs.uk/casp/critical_appraisal_tools.htm
Further reading
Gottrup, F., Apelquvist, J., Price, P. (2010) Outcomesin controlled and comparative studies on nonhealingwounds. Journal of Wound Care, 19(6), 237–268.
Greenhalgh, T. (2001) How to Read a Paper: The Basics ofEvidence Based Medicine. London: BMJ.
Guyatt, G., Rennie, D., Meade, M., Cook, D. (2008) Users’Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice. 2nd ed. Chicago, IL: McGraw-Hill Medical.
References
Adderley, U., Thompson, C. (2007) A study of thefactors influencing how frequently district nurses re-apply compression bandaging. Journal of Wound Care,16, 217–221.
Annells, M., O’neill, J., Flowers, C. (2008) Compres-sion bandaging for venous leg ulcers: the essential-ness of a willing patient. Journal of Clinical Nursing, 17,350–359.
Atallah, A.N. (1999) The Cochrane Collaboration: sharedevidence for improving decision-making in humanhealth. Sao Paulo Medical Journal, 117, 183–184.
Australian Wound Management Association Inc., NewZealand Wound Care Society Inc. (2011) Australia andNew Zealand Clinical Practice Guideline for Prevention andManagement of Venous Leg Ulcers. Canberra: CambridgePublishing.
Avorn, J., Fischer, M. (2010) ‘Bench to behavior’: translat-ing comparative effectiveness research into improvedclinical practice. Health Affairs, 29, 1891–900.
Barker, J., Weller, C. (2010) Developing clinical prac-tice guidelines for the prevention and management ofvenous leg ulcers. Wound Practice and Research, 18, 10.
Barton, S. (2000) Which clinical studies provide the bestevidence? The best RCT still trumps the best observa-tional study. British Medical Journal, 321, 255–256.
Bates, D.W., Kuperman, G.J., Wang, S., et al. (2003) Tencommandments for effective clinical decision support:making the practice of evidence-based medicine a real-ity. Journal of the American Medical Informatics Associa-tion, 10, 523–530.
Bauer, J.G., Chiappelli, F. (2010) Transforming scientificevidence into better consumer choices. Bioinformation,5, 297–9.
Bennett, C.C. (2009) A healthier future for all Australians:an overview of the final report of the National Healthand Hospitals Reform Commission. Medical Journal ofAustralia, 191, 383–7.
Brouwers, M.C., Kho, M.E., Browman, G.P., et al. (2010)AGREE II: advancing guideline development, report-ing and evaluation in health care. Canadian MedicalAssociation Journal, 182, E839–E842.
Burgers, J.S., Grol, R.P., Zaat, J.O., et al. (2003) Char-acteristics of effective clinical guidelines for generalpractice. British Journal of General Practice, 53, 15–19.
Cabana, M.D., Rand, C.S., Powe, N.R., et al. (1999) Whydon’t physicians follow clinical practice guidelines? Aframework for improvement. The Journal of the Ameri-can Medical Association, 282, 1458–1465.
Cowan, L.J., Stechmiller, J. (2009) Prevalence of wet-to-dry dressings in wound care. Advanced Skin WoundCare, 22, 567–573.
Cullum, N., Nelson, E.A., Fletcher, A.W., Sheldon, T.A.(2000) Compression for venous leg ulcers. CochraneDatabase of Systematic Reviews, CD000265.
Cullum, N., Nelson, E.A., Fletcher, A.W., Sheldon, T.A.(2001) Compression for venous leg ulcers. CochraneDatabase of Systematic Reviews, CD000265.
Davies, H., Nutley, S., Walter, I. (2008) Why ‘knowledgetransfer’ is misconceived for applied social research.Journal of Health Services Research and Policy, 13, 188–190.
Dawes, M., Sampson, U. (2003) Knowledge managementin clinical practice: a systematic review of informationseeking behavior in physicians. International Journal ofMedical Informatics, 71, 9–15.
Dicenso, A., Bryant-Lukosius, D., Martin-Misener, R.,et al. (2010) Factors enabling advanced practice nursingrole integration in Canada. Nursing Leadership (TorontoOntario), 23(2010), 211–238.
El Dib, R.P., Atallah, A.N., Andriolo, R.B. (2007) Mappingthe Cochrane evidence for decision making in healthcare. Journal of Evaluation in Clinical Practice, 13, 689–692.
Ertl, P. (1992) How do you make your treatment decision?Professional Nurse, 7, 543–552.
Field, M.J. (1994) Practice guidelines and quality ofcare. Journal of the National Medical Association, 86, 255–256.
Fletcher, A.A., Cullum, N.N., Sheldon, T.T. A. (1997)A systematic review of compression treatment forvenous leg ulcers. British Medical Journal, 315, 576–580.
Glasziou, P., Haynes, B. (2005) The paths from researchto improved health outcomes. ACP Journal Club, 142,A8–A10.

16 Wound Healing and Skin Integrity
Gottrup, F. (2004) Optimizing wound treatment throughhealth care structuring and professional education.Wound Repair and Regeneration, 12, 129–133.
Gottrup, F. (2010) Controversies in wound healing. Inter-national Journal of Lower Extremity Wounds, 9, 9.
Gottrup, F., Apelqvist, J. (2010) The challenge of usingrandomized trials in wound healing. British Journal ofSurgery, 97, 303–304.
Gottrup, F., Apelqvist, J., Price, P. (2010) Outcomesin controlled and comparative studies on non-healingwounds: recommendations to improve the quality ofevidence in wound management. Journal of Wound Care,19, 237–268.
Graham, I.D., Harrison, M.B., Shafey, M., Keast, D.(2003) Knowledge and attitudes regarding care of legulcers. Survey of family physicians. Canadian FamilyPhysician, 49, 896–902.
Griffin, S.C., Claxton, K.P., Palmer, S.J., Sculpher,M.J. (2011) Dangerous omissions: the consequencesof ignoring decision uncertainty. Health Economics, 20,212–224.
Grimshaw, J.M., Thomas, R.E., Maclennan, G., et al.(2004) Effectiveness and efficiency of guideline dissem-ination and implementation strategies. Health Technol-ogy Assessment, 8(iii–iv), 1–72.
Grol, R. (2002) Changing physicians’ competence andperformance: finding the balance between the individ-ual and the organization. Journal of Continuing Educa-tion in the Health Professions, 22, 244–251.
Grol, R. (2010) Has guideline development gone astray?Yes. British Medical Journal, 340, c306.
Grol, R., Buchan, H. (2006) Clinical guidelines: what canwe do to increase their use? Medical Journal of Australia,185, 301–302.
Grol, R., Grimshaw, J. (2003) From best evidence tobest practice: effective implementation of change inpatients’ care. Lancet, 362, 1225–1230.
Grol, R.P., Bosch, M.C., Hulscher, M.E., Eccles, M.P.,Wensing, M. (2007) Planning and studying improve-ment in patient care: the use of theoretical perspectives.Milbank Quarterly, 85, 93–138.
Guyatt, G.H., Meade, M.O., Jaeschke, R.Z., Cook, D.J.,Haynes, R.B. (2000) Practitioners of evidence basedcare. Not all clinicians need to appraise evidence fromscratch but all need some skills. British Medical Journal,320, 954–955.
Hoaglin, D.C., Hawkins, N., Jansen, J.P., et al. (2011) Con-ducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Forceon Indirect Treatment Comparisons Good ResearchPractices: part 2. Value in Health, 14, 429–437.
Kawamoto, K., Houlihan, C.A., Balas, E.A., Lobach,D.F. (2005) Improving clinical practice using clinicaldecision support systems: a systematic review of trialsto identify features critical to success. British MedicalJournal, 330, 765.
Lean, M.E., Mann, J.I., Hoek, J.A., Elliot, R.M., Schofield,G. (2008) Translational research. British Medical Journal,337, a863.
Mallett, S., Clarke, M. (2003) How many Cochranereviews are needed to cover existing evidence on theeffects of health care interventions? ACP Journal Club,139, A11.
Mcguckin, M., Kerstein, M.D. (1998) Venous leg ulcersand the family physician. Advances in Wound Care, 11,344–346.
Mcnees, P., Kueven, J.A. (2011) The bottom line on woundcare standardization. Healthcare Financial Management,65, 70–74, 76.
Moher, D., Hopewell, S., Schulz, K.F., et al. (2010)CONSORT 2010 explanation and elaboration: updatedguidelines for reporting parallel group randomised tri-als. Journal of Clinical Epidemiology, 63, e1–e37.
Newall, N., Miller, C., Lewin, G., et al. (2009) Nurses’experiences of participating in a randomised con-trolled trial (RCT) in the community. Wound Practiceand Research, 17, 24–34.
O’meara, S., Cullum, N.A., Nelson, E.A. (2009) Compres-sion for venous leg ulcers. Cochrane Database of System-atic Reviews, CD000265.
Oxman, A.D., Thomson, M.A., Davis, D.A., Haynes, R.B.(1995) No magic bullets: a systematic review of 102trials of interventions to improve professional prac-tice. Canadian Medical Association Journal, 153, 1423–1431.
Rose, L. (2011) Interprofessional collaboration in the ICU:how to define? Nursing in Critical Care, 16, 5–10.
Sackett, D.L., Rosenberg, W.M., Gray, J.A., Haynes, R.B.,Richardson, W.S. (1996) Evidence based medicine:what it is and what it isn’t. British Medical Journal, 312,71–72.
Sadler, G.M., Russell, G.M., Boldy, D.P., Stacey, M.C.(2006) General practitioners’ experiences of managingpatients with chronic leg ulceration. Medical Journal ofAustralia, 185, 78–81.
Scott, I.A. (2009) The NHHRC final report: view from thehospital sector. Medical Journal of Australia, 191, 450–453.
Scott, I.A., Glasziou, P.P. (2012) Improving the effective-ness of clinical medicine: the need for better science.Medical Journal of Australia, 196, 304–308.
SIGN (2010) Scottish Intercollegiate Guidelines Network(SIGN) 120 – National Clinical Guidelines for Manage-ment of Chronic Venous Leg Ulcers. Edinburgh, Scotland:NHS Quality Improvement Scotland.
Solberg, L.I., Brekke, M.L., Fazio, C.J., et al. (2000)Lessons from experienced guideline implementers:attend to many factors and use multiple strategies. JointCommission Journal on Quality Improvement, 26, 171–188.
Sox, H.C., Helfand, M., Grimshaw, J., et al. (2010) Com-parative effectiveness research: Challenges for medical