Embed Size (px)
Citation preview

www.diabetesclinic.ca 1
INTENSIVE INSULIN THERAPY
J. Robin Conway M.D.
Diabetes Clinic, Smiths Falls, ON
1-800-717-0145

www.diabetesclinic.ca 2
Objectives
• Optimize diabetes management
• Assist you in initiating insulin in your office– When to start insulin therapy?– Insulins, doses, delivery options– Patient training

www.diabetesclinic.ca 3
Challenges in Initiating Insulin?
1. Patient attitudesPatient attitudes– Fear of needles– Insulin viewed as a threat by patient & physician– Hypoglycemia
2. Physician AttitudesPhysician Attitudes– Discomfort with insulin
• Lack of knowledge and experience
– Fear of needles

www.diabetesclinic.ca 4
Type 1 Diabetes:
• Impaired or absent ß cell function: insulin secretion
• Normal insulin action: insulin sensitivity
• The insulin deficiency results in unacceptable blood glucose control

www.diabetesclinic.ca 5
Type 2 Diabetes: Double Impairment
• Impaired ß cell function: insulin secretion
• Impaired insulin action: insulin resistance
• Results in unacceptable blood glucose control

www.diabetesclinic.ca 6
Type 1 & 2 Diabetes: Key Concepts
• Minimizing the complications of diabetes requires:– Early diagnosis and treatment of diabetes
– Maintaining HbA1C level < 7%
• Achieving HbA1C < 7% requires control of post-prandial and fasting hyperglycemia

www.diabetesclinic.ca 7
CDA Guidelines (for glycemic control)
Normal Optimal
A1C level (0.04-0.06)
(< 0.07)
Preprandialglycemia(mmol/L)
3.5-6.1 4-7
Postprandialglycemia(mmol/L)
4.4-7.8 7-11
Haars s et al., CMAJ 2003; 159 (Suppl.): S1-29. Gerstein, H.C. et al. CDA views on the UKPDS and revision of the guidelines affected by the results of this study.

www.diabetesclinic.ca 8
Steps to Glycemic Control
• Establish glycemic objectives– Target fasting and post-prandial glycemia
• Diet counseling with exercise component
• Diabetes education for every patient
• Pharmacological treatment; oral and insulin

www.diabetesclinic.ca 9
Patient Counselling Topics
A.Review symptoms and treatment of hypoglycemia
B.Proper training and correct use of glucose monitor
C.Target desired glycemic levels for each patient

www.diabetesclinic.ca 10
A. Hypoglycemia
• Definition: Glycemia < 3.8 mmol
• Patients may experience hypoglycemia at different glycemic levels

www.diabetesclinic.ca 11
Symptoms of HypoglycemiaMild• < 3.3 mmol/L• Neurovegetative
symptoms– Sweating– Trembling– Palpitations– Anxiety– Tingling– Pallor – Hunger
Moderate to Severe• < 2.8 mmol/L• Symptoms of glucopenia
– Confusion – Visual disturbances– Weakness– Speech disorder– Behavioural disorder– Drowsiness– Coma– Convulsions

www.diabetesclinic.ca 12
Preventing Hypoglycemia
• Check BG 4-6 times per day
• Carry glucose tablets
• Have Glucagon Kit available

www.diabetesclinic.ca 13
Preventing Hypoglycemia• Test before driving and ideally 1 hour later
(target: over 5.5 mmol/L)
• Perform two SMBG 30 minutes apart prior to bedtime (confirming rising or falling BG)
• When drinking alcohol, perform SMBG hourly
• With exercise, perform SMBG pre- and post-exercise
• If hypoglycemia episodes persist, raise target glucose levels

www.diabetesclinic.ca 14
Hypoglycemia Treatment Guidelines
The Rule of 15The Rule of 15• If BG is 4 mmol/L or below
– Treat with 15 grams of carbohydrates (glucose tabs)
– Check BG in 15 minutes, and if not above 4 mmol/L, repeat treatment
Glucagon• Current emergency kit readily available and
knowledgeable person trained to administer

www.diabetesclinic.ca 15
PreventingHyperglycemia and DKA
• Monitor BG 4-6 times per day
• Use Correction Boluses when appropriate

www.diabetesclinic.ca 16
Hyperglycemia Treatment GuidelinesThe Key to Preventing DKA
1st BG over 14 mmol/L:1st BG over 14 mmol/L:• Take a correction bolus, check again
in 1 hour
• Call physician immediately or go to ER if nausea and vomiting are present

www.diabetesclinic.ca 17
B. Patient Training
• Training by a multidisciplinary team at DEC is IDEAL for:– Diet counseling – Education on the injection sites – Education on the various injection devices– Evaluation of the patient’s support network
• Other resources may exist for training, i.e. retail pharmacy

www.diabetesclinic.ca 18
C. Blood Glucose Monitoring
• To adjust the insulin treatment
• To detect or confirm hypoglycemia or severe hyperglycemia
• To adjust treatment to the circumstances of daily life using an insulin scale prescribed by the attending physician
• To improve patient safety and increase motivation to comply with treatment

www.diabetesclinic.ca 19
Ideal Testing Frequency
• Stable type 2 – 1-2 readings/day
• Type 1 or Unstable type 2– 3-8 readings/day
• Important to stress the need to vary testing times– AC, PC, h.s. and prn during the night

www.diabetesclinic.ca 20
Injection Tools and Options
• Durable delivery devices– Novolin-Pen® 3 – Novolin-Pen® Junior– InDuo®
– Innovo®
– HumaPen®
• Insulin pumps• Syringes
• Disposable: multidose, prefilled (3.0 mL)– NovolinSet® (NPH,
Toronto, 30/70 )– Humulin® N

www.diabetesclinic.ca 21
Advancing Insulin Therapy Through Device Innovation

www.diabetesclinic.ca 22
We are trying to duplicate how the pancreas works in
releasing insulin for someone who doesn’t
have diabetes
Goal of Insulin Therapy

www.diabetesclinic.ca 23
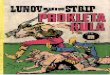
Non-diabetic Insulin and Glucose Profiles
9.0
6.0
3.0
07 8 9 101112 1 2 3 4 5 6 7 8 9
Insulin
Glucose
a.m. p.m.
Breakfast Lunch Supper75
50
25
0 Basal insulin
Basal glucose
Insulin(µU/mL)
Glucose(mmo/L)
Time of Day

www.diabetesclinic.ca 24
Insulin Preparations
Start 3-4 hrs. Peakless
Humulin® U vial only
Lantus (Glargine) vial only
Levemir (Detemir) cartridge
Prolonged action
Start 1.5 hrs
Peak 7 hr
Novolin®ge NPH
Humulin® N
IntermediateVial and cartridge
Start 30-60 min.
Peak 4 hr
Novolin®ge Toronto Humulin® R
Short-acting (regular) Vial and cartridge
Start < 15 min.
Aspart (NovoRapid®) Lispro (Humalog®)
Rapid-actingVial and cartridge

www.diabetesclinic.ca 25
Insulin PreMixes
• Regular + intermediate– Novolin® 10/90, 20/80, 30/70, 40/60, 50/50– Humulin® 30/70, 20/80
• Analogue Pre-Mix– Humalog® 25/75 (insulin lispro protamine
suspension)– NovoMix 30* (protaminated insulin aspart)
* Not available

www.diabetesclinic.ca 26
Normal Blood Glucose Levels
Blood Glucose (mmols)
10-
8-
6-
4-
2-
0
8am noon 6pm 2am 4am 8am
Time

www.diabetesclinic.ca 27
Normal Blood Glucose Levels
Blood Glucose (mmols)
10-
8-
6-
4-
2-
0
8am noon 6pm 2am 4am 8am
Time

www.diabetesclinic.ca 28
Two injections/day
Blood Glucose (mmols)
8am noon 6pm 2am 4am 8am
Time
R or H + N in AM R or H + N at Supper
10-
8-
6-
4-
2-
0

www.diabetesclinic.ca 29
Three injections/day
Blood Glucose (mmols)
8am noon 6pm 2am 4am 8am
Time
R or H + N in AM
R or H at Supper
N before bed
10-
8-
6-
4-
2-
0

www.diabetesclinic.ca 30
Four injections/day
Blood Glucose (mmols)
8am noon 6pm 2am 4am 8am
Time
R or H at every meal N or U once or twice/day
10-
8-
6-
4-
2-
0

www.diabetesclinic.ca 31
Continuous Infusion
Blood Glucose (mmols)
8am noon 6pm 2am 4am 8am
Time
10-
8-
6-
4-
2-
0

www.diabetesclinic.ca 32
Limitations of Regular Human Insulin
• Slow onset of activity– Should be given 30 to 45 minutes before meal
• Inconvenient for patients• Long duration of activity
– Lasts up to 12 hours
• Potential for late postprandial hypoglycaemia (4-6 hours)– Need for additional snack

www.diabetesclinic.ca 33
Adherence to Injection Recommendation Adherence to Injection Recommendation (Canada)(Canada)
4%
42%32%
22%
0
100
30–45 min 15–30 min 0–15 min 0–15 min
% o
f R
es
po
nd
ents
B e f o r e Meal After
"When do you inject your insulin?"
1998 Roper Starch Canada, Premix Insulin Using Respondents.

www.diabetesclinic.ca 34
Dissociation of Regular Human Insulin
Regular Human Insulin
10-3 M 10-3 M 10-5 M 10-8 M peak time2-4 hr
formulation
capillary membrane
hexamers dimers monomers

www.diabetesclinic.ca 35
Objectives for the Development of Short-Acting Insulin Analogues
• Modify time action to address
– Postprandial hyperglycemia
– Hypoglycemia
• Improve safety and convenience

www.diabetesclinic.ca 36
Whats’ new in type 1 diabetes treatment?
• Insulin analogues.
• Physiological insulin replacement
• Aggressive “intensive” management– 4 injections per day– Insulin infusion pumps– Continuous glucose monitoring systems– Integrated technologies for monitoring control

www.diabetesclinic.ca 37
Non-diabetic Insulin and Glucose Profiles
9.0
6.0
3.0
07 8 9 101112 1 2 3 4 5 6 7 8 9
Insulin
Glucose
a.m. p.m.
Breakfast Lunch Supper75
50
25
0 Basal insulin
Basal glucose
Insulin(µU/mL)
Glucose(mmo/L)
Time of Day

www.diabetesclinic.ca 38
NovoRapid® (insulin aspart)
Time-Action Profile0 2 4 6 8 10 12 14 16 18 20 22 24
Onset: 10-20 minutesMaximum effect: 1-3 hoursDuration: 3-5 hours
NovoRapid®
Rapid-acting insulin analogue

www.diabetesclinic.ca 39
We are trying to duplicate how the pancreas works in
releasing insulin for someone who doesn’t
have diabetes
Goal of Insulin Therapy

www.diabetesclinic.ca 40
Insulin Therapy Options
• MDI therapyMDI therapy– 0.5 units/kg = total daily dose– 4x/day 40% NPH @ hs and 60% rapid acting
analogue ac meals– For patients with significant complications (i.e.
renal failure, foot infections, CVD, etc…)

www.diabetesclinic.ca 41
In someone without diabetes, the pancreas delivers a small amount of
insulin continuously to cover the body’s
non-food related insulin needs.
Basal Insulin

www.diabetesclinic.ca 42
The amount of insulin required to cover the food you eat.
Fast-acting or Short-acting (clear) insulin works as a
Bolus Insulin
Bolus Insulin

www.diabetesclinic.ca 43
Why count carbs?
• More precise way of measuring the impact of a meal on blood sugar
• Lets you decide how much insulin is needed to “cover” the meal
• Greater flexibility -eat what you want, when you want to eat it

www.diabetesclinic.ca 44
Fine Tuning: Bolus Doses
• Carbohydrate counting or pre-determined meal portion
• Individualized insulin to carbohydrate dose or insulin to meal dose
• Adjust bolus based on post-meal BGs or next pre-meal BG

www.diabetesclinic.ca 45
Fine Tuning: Basal Rate
• Monitor BG pre-meal, post-meal, bedtime, 12am, and 2-4am
• Test fasting BG with skipped meals
• Adjust nighttime basal based on 2-4am and pre-breakfast BG
• Adjust basal by 0.1 u/hr to avoid over-correction

www.diabetesclinic.ca 46
Novolin®ge 30/70
Time-Action Profile
Premixed insulin
Onset: 0.5 hourMaximum effect: 2-12 hoursDuration: 24 hours

www.diabetesclinic.ca 47
30/70 - Twice/day

www.diabetesclinic.ca 48
30/70 Dose Calculation
• Weight = 80 kg• 80 kg x 0.3 U/kg = 24 U• 2/3 in the AM = 16 Units• 1/3 at supper = 8 Units

www.diabetesclinic.ca 49
Dosage Changes
• Change insulin dose so that peak of action corresponds to most abnormal value (pre-meal)
• If all values are abnormal - start with fasting glycemia followed by lunch, supper and bedtime
• Change the dose by increments of 1-4 U• Not more than twice/week• Monitor for PATTERNS in hypoglycemia

www.diabetesclinic.ca 50
NovoRapid® Penfill®
Rapid-acting human insulin analogue(insulin aspart)
Novolin®ge Toronto Penfill®
Short-acting insulin(insulin injection, human biosynthetic)
Novolin®ge NPH Penfill®
Intermediate-acting Insulin (insulin injection, human biosynthetic)
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424
Onset: 10-20 minutesMaximum effect: 1-3 hoursDuration: 3-5 hours
Onset: 0.5 hourMaximum effect: 1-3 hoursDuration: 8 hours
Onset: 1.5 hoursMaximum effect: 4-12 hoursDuration: 24 hours
Full Range of Novo Nordisk Insulins

www.diabetesclinic.ca 51
Somogyi Effect
• Hyperglycemia secondary to asymptomatic hypoglycemia (especially at night)
• If the insulin is increased in evening, the problem worsens
• Check capillary glycemia around 3 a.m. to eliminate hypoglycemia
• In this case, reduce the h.s. NPH

www.diabetesclinic.ca 52
Follow-Up: The Patient’s Role
Every DayEvery Day• Check BG 4-6 times a day,
and always before bed• Follow hypoglycemia
guidelines• Follow hyperglycemia
guidelines
Every 3 monthsEvery 3 months• Visit healthcare provider -
even if feeling well
• Review log book and pump settings with physician
• Get an A1c test
Every monthEvery month Review DKA prevention Check BG
- 3am (overnight)- 1 and/or 2-hour post-meal BG for all meals on a given
day

www.diabetesclinic.ca 53
Case Study #1
• Patient R.M., DM for 9 years• BMI = 34, • Meds: metformin 1000 mg BID and
glyburide 10 mg BID, Avandia 8 mg OD• HbA1C is 9.5 %, FBS 11.8
What is the next step?

www.diabetesclinic.ca 54
Case Study #2• Patient K.G., DM for 15 years• BMI = 23• Meds: Metformin 1000 mg BID and Gluconorm 2
mg TID• HbA1C = 8.5%, FBS 7.4• Post MI
What is the next step?