Embed Size (px)
Citation preview

www.RomeCriteria.orgwww.RomeCriteria.org
17291729

Rome III
17801780

1743
N Sartorius, N Sartorius, WHO ICD-10, 1994WHO ICD-10, 1994N Sartorius, N Sartorius, WHO ICD-10, 1994WHO ICD-10, 1994
classification is a way of seeing the
world at a point in time. There is no doubt
that scientific progress and experience
classification is a way of seeing the
world at a point in time. There is no doubt
that scientific progress and experience
with the use of these guidelines
will ultimately require their
revision and update.
with the use of these guidelines
will ultimately require their
revision and update.
AA

Vision of Rome Foundation
Promote clinical recognition and legitimization of FGIDs
Develop a scientific understanding of the pathophysiological mechanisms to achieve optimum treatment
Promote clinical recognition and legitimization of FGIDs
Develop a scientific understanding of the pathophysiological mechanisms to achieve optimum treatment
17031703
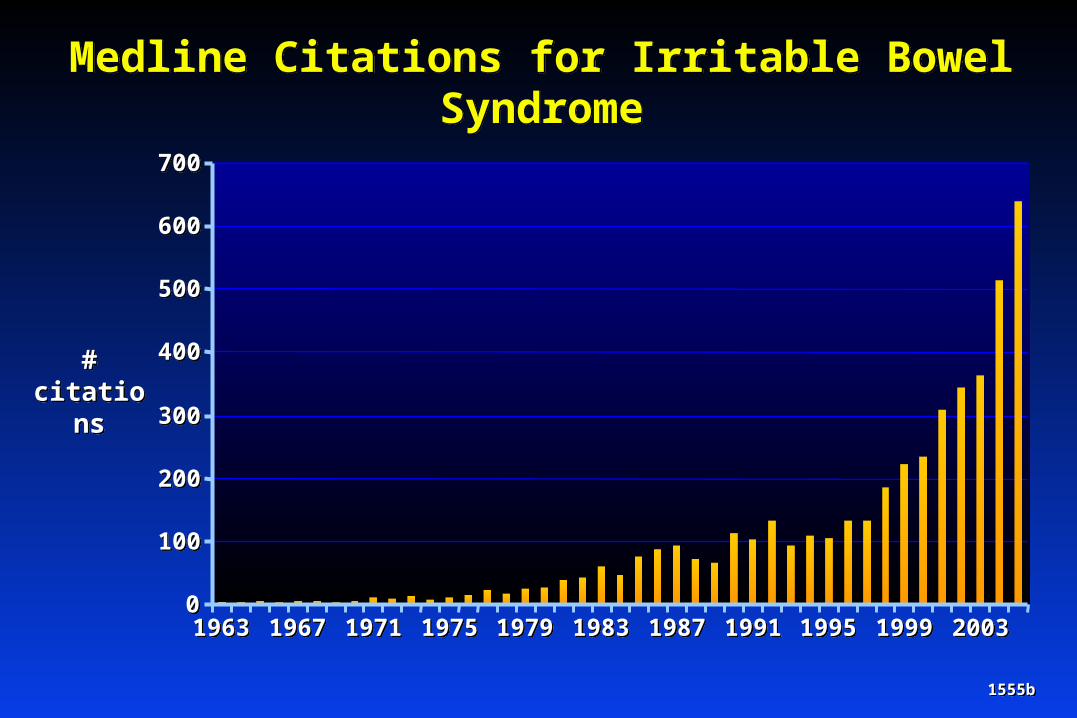
Medline Citations for Irritable Bowel SyndromeMedline Citations for Irritable Bowel Syndrome
1555b1555b
00
100100
200200
300300
400400
500500
600600
700700
19631963 19671967 19711971 19751975 19791979 19831983 19871987 19911991 19951995 19991999 20032003
# citations
# citations

Rome PublicationsRome Publications
Gastroenterology International
Journal
Gastroenterology International
Journal
19891989 19901990 1994199419991999 20002000
20062006
1st IBS criteria1st IBS criteria
1992-19955 Rome I
publications
1992-19955 Rome I
publications
2003Rome
Foundation
2003Rome
Foundation
Gastroenterology Supplement
+Rome III BookDegnon Assoc.
Gastroenterology Supplement
+Rome III BookDegnon Assoc.
16831683
1st FGID classification
1st FGID classification
Rome I BookLittle Brown
Rome I BookLittle Brown
Rome IIGut
Supplement
Rome IIGut
Supplement
Rome II BookDegnon Assoc.

IBS Rome Criteria Medline CitationsRome Criteria Medline Citations
1555a1555aYearYear
# citations
# citations
00
1010
2020
3030
4040
5050
6060
7070
8080
19921992 19931993 19941994 19951995 19961996 19971997 19981998 19991999 20002000 20012001 20022002 20032003 20042004
9090
100100
105105
20052005
Rome III
Rationale for Diagnostic Criteria Rationale for Diagnostic Criteria
16861686
Rome III - Rationale for Symptom Criteria
1203
Symptoms not explained by abnormal motility Symptoms defined by multiple factors
MotilityVisceral hypersensitivityInflammation and mucosal immune dysfunctionBrain-gut dysfunction
Epidemiological supportFactor analysis defines symptom-based subgroupsFrequencies similar across populations
Treatment implications Provides diagnostic standards
For clinical trials and clinical careModeled after DSM system in psychiatry
Symptoms not explained by abnormal motility Symptoms defined by multiple factors
MotilityVisceral hypersensitivityInflammation and mucosal immune dysfunctionBrain-gut dysfunction
Epidemiological supportFactor analysis defines symptom-based subgroupsFrequencies similar across populations
Treatment implications Provides diagnostic standards
For clinical trials and clinical careModeled after DSM system in psychiatry

FGID - Conceptual Model
PhysiologyPhysiology• Motility• Sensation• Inflammation• Altered bacterial
flora
• Motility• Sensation• Inflammation• Altered bacterial
flora
FGID• Symptoms
• Behavior
BrainCNS
GutENS
PsychosocialFactors
PsychosocialFactors
• LIfe stress• Psychologic state• Coping• Social support
• LIfe stress• Psychologic state• Coping• Social support
Early LifeEarly Life• Genetics• Environment• Genetics• Environment
OutcomeOutcome• Medications• MD visits• Daily function• Quality of life
• Medications• MD visits• Daily function• Quality of life
1035

Rome III
Rationale for Diagnostic Criteria Administrative Structure
Rationale for Diagnostic Criteria Administrative Structure
16871687

16821682
Rome Foundation, Inc. 1996Rome Foundation, Inc. 1996
Rome CommitteesRome Committees
14 Committees87 Members18 Countries
14 Committees87 Members18 Countries
Intnl. Resource Committee
Intnl. Resource Committee
12 PharmaceuticalsFDA, IFFGD, NIH
12 PharmaceuticalsFDA, IFFGD, NIH
AdministrationAdministration
2 Committees16 Members4 Countries
2 Committees16 Members4 Countries
George DegnonCarlar Blackman
Kathy Haynes
George DegnonCarlar Blackman
Kathy Haynes
Working TeamsWorking Teams
6 Committees28 Members7 Countries
6 Committees28 Members7 Countries
CD CommitteeCD Committee
Board of DirectorsBoard of DirectorsD. Drossman (President) USAD. Drossman (President) USA
E. Corazziari Italy N. Talley USAM. Delvaux France W.G. Thompson CanadaR. Spiller UK W. Whitehead USAJ. Kellow Australia L. Chang USA
E. Corazziari Italy N. Talley USAM. Delvaux France W.G. Thompson CanadaR. Spiller UK W. Whitehead USAJ. Kellow Australia L. Chang USA

Rome III
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects
16891689

Rome III Book – August, 2006
Gastroenterology 13th Issue – April, 2006Reduced Versions of Chapters
New Working Teams Severity,
Brain Imaging,
Role of Physiology in FGID’s
Sponsored Research (Epidemiology, Validation, Spanish Translation of Rome III)
Validated Questionnaire with “Red Flags”
Translations in numerous languages Web site: www.romecriteria.org CD Slide Set (6 Committees) - 2008
Rome III Book – August, 2006
Gastroenterology 13th Issue – April, 2006Reduced Versions of Chapters
New Working Teams Severity,
Brain Imaging,
Role of Physiology in FGID’s
Sponsored Research (Epidemiology, Validation, Spanish Translation of Rome III)
Validated Questionnaire with “Red Flags”
Translations in numerous languages Web site: www.romecriteria.org CD Slide Set (6 Committees) - 2008 1690a1690a
Rome III – Activities/Projects

• UPDATE SLIDE
• Outcomes
• physiology

Rome III Working Teams
Guidelines for Brain Imaging in the FGIDsEmeran Mayer, USA, Chair Qasim Aziz, UK, Co-Chair Douglas Bremner, USA Mark Kern, USA Brad Kuo, USA Richard Lane, USA Bruce Naliboff, USA Irene Tracey, UK
Guidelines for Severity in the FGIDsDouglas A. Drossman, USA, ChairLin Chang, USA, Co-Chair Nicholas Bellamy, Australia Hugo Gallo Torres, FDA, USA Tony Lembo, USA Fermin Mearin, Spain Nancy Norton, IFFGD, USA Peter Whorwell, UK
Guidelines for Brain Imaging in the FGIDsEmeran Mayer, USA, Chair Qasim Aziz, UK, Co-Chair Douglas Bremner, USA Mark Kern, USA Brad Kuo, USA Richard Lane, USA Bruce Naliboff, USA Irene Tracey, UK
Guidelines for Severity in the FGIDsDouglas A. Drossman, USA, ChairLin Chang, USA, Co-Chair Nicholas Bellamy, Australia Hugo Gallo Torres, FDA, USA Tony Lembo, USA Fermin Mearin, Spain Nancy Norton, IFFGD, USA Peter Whorwell, UK
17961796

Basic Science – Jack Wood, USA, ChairLionel Bueno, France John Kellow, Australia
Epidemiology – Fermin Mearin, Spain, ChairGeorge Longstreth, USAPaul Moayyedi, CanadaNick Talley, USA
Diagnosis and Criteria – Arnold Wald, USA, ChairBrooks Cash, USAEnrico Corazziari, ItalyTony Lembo, USAStu Spechler, USAJan Tack, Belgium
Basic Science – Jack Wood, USA, ChairLionel Bueno, France John Kellow, Australia
Epidemiology – Fermin Mearin, Spain, ChairGeorge Longstreth, USAPaul Moayyedi, CanadaNick Talley, USA
Diagnosis and Criteria – Arnold Wald, USA, ChairBrooks Cash, USAEnrico Corazziari, ItalyTony Lembo, USAStu Spechler, USAJan Tack, Belgium
Rome III CD Committees
17971797

Psychosocial, HRQOL, Brain Imaging – Ami Sperber, Israel, ChairElspeth Guthrie, UKRona Levy, USABruce Naliboff, USAKevin Olden, USA
Management, Treatment Trial Design - William Chey, USA, ChairLin Chang, USAMichel Delvaux, FranceE. Jan Irvine, CanadaW. Grant Thompson, Canada
Pediatric – Carlo Di Lorenzo, USA, ChairMarc Benninga, NetherlandsErnesto Guiraldes, ChileJeffrey Hyams, USAPaul Hyman, USA
Psychosocial, HRQOL, Brain Imaging – Ami Sperber, Israel, ChairElspeth Guthrie, UKRona Levy, USABruce Naliboff, USAKevin Olden, USA
Management, Treatment Trial Design - William Chey, USA, ChairLin Chang, USAMichel Delvaux, FranceE. Jan Irvine, CanadaW. Grant Thompson, Canada
Pediatric – Carlo Di Lorenzo, USA, ChairMarc Benninga, NetherlandsErnesto Guiraldes, ChileJeffrey Hyams, USAPaul Hyman, USA
Rome III CD Committees
17981798

Rome III
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees
16911691

Rome III – Timeline for CD Committees
Board selects Chair/Co-Chairs* – October 2005 Chairs/Co-Chairs select committees* – December 2005 Chairs/Co-Chairs conference call – December 2005 Content Development – February–May 2006 Orientation/Process Learning at DDW – May 2006 Graphic Development I – May–December 2006 CD Committee Meeting I – January 2007 Graphic Development II – January-April 2007 CD Committee Meeting II – May 2007 Graphic Development III – May-October 2007 Submission to Board and Release – January 2008
Board selects Chair/Co-Chairs* – October 2005 Chairs/Co-Chairs select committees* – December 2005 Chairs/Co-Chairs conference call – December 2005 Content Development – February–May 2006 Orientation/Process Learning at DDW – May 2006 Graphic Development I – May–December 2006 CD Committee Meeting I – January 2007 Graphic Development II – January-April 2007 CD Committee Meeting II – May 2007 Graphic Development III – May-October 2007 Submission to Board and Release – January 2008
* Criteria: 1) Research record, 2) Intl. recognition, 3) Ability to work in group4) Geographical diversity
* Criteria: 1) Research record, 2) Intl. recognition, 3) Ability to work in group4) Geographical diversity 17811781

Rome III Committees
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees Chapter Structure
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees Chapter Structure
16931693

Rome III Committees – Chapter Structure
Criteria Related ChaptersIntroductionDiagnostic Entities
Definition Epidemiology Diagnostic Criteria Justification for Change in Criteria Clinical Evaluation Physiological Features Psychological Features Treatment Recommendations for Future Research
Content Area ChaptersRevised chapters maintain same structureNew chapter formats created by chair/co-chair
Criteria Related ChaptersIntroductionDiagnostic Entities
Definition Epidemiology Diagnostic Criteria Justification for Change in Criteria Clinical Evaluation Physiological Features Psychological Features Treatment Recommendations for Future Research
Content Area ChaptersRevised chapters maintain same structureNew chapter formats created by chair/co-chair
16941694

Rome III Committees
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees Chapter Structure Changes for Rome III
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Slide Set Committees Chapter Structure Changes for Rome III
16951695

Time Frame: “Criteria fulfilled in last 3 months with symptom onset at least 6 months prior to diagnosis”
Classification Changes: Rumination now a Functional Gastroduodenal Disorder FAPS is a separate Category (not Functional Bowel)
Two Pediatric Categories: Neonate/Toddler Child/Adolescent
Functional Dyspepsia De-emphasized for Research Postprandial Distress Syndrome Epigastric Pain Syndrome
More Restrictive Criteria for GB and SO Dysfunction Stool Consistency to Identify IBS Subtypes
Time Frame: “Criteria fulfilled in last 3 months with symptom onset at least 6 months prior to diagnosis”
Classification Changes: Rumination now a Functional Gastroduodenal Disorder FAPS is a separate Category (not Functional Bowel)
Two Pediatric Categories: Neonate/Toddler Child/Adolescent
Functional Dyspepsia De-emphasized for Research Postprandial Distress Syndrome Epigastric Pain Syndrome
More Restrictive Criteria for GB and SO Dysfunction Stool Consistency to Identify IBS Subtypes
17771777
Changes for Rome III – Classification and Criteria

Rome III Criteria* – Irritable Bowel Syndrome
Rome III Criteria* – Irritable Bowel Syndrome
Improvement with
defecation
Improvement with
defecation
Recurrent abdominal pain or discomfort at least 3 days/monthIn the last 3 months associated with 2 or more :
Recurrent abdominal pain or discomfort at least 3 days/monthIn the last 3 months associated with 2 or more :
Onset associated with
a change in frequency of
stool
Onset associated with
a change in frequency of
stool
Onset associated with
a change in form
(appearance) of stool
Onset associated with
a change in form
(appearance) of stool
andand andand
Longstreth GF, Gastroenterology 2006Longstreth GF, Gastroenterology 2006 17821782
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.

00
2525
5050
7575
100100
%Hard or lumpy
stools
%Hard or lumpy
stools
00 2525 5050 7575 100100
% Loose or watery stools% Loose or watery stools
IBS-UIBS-U
IBS-CIBS-C IBS-MIBS-M
IBS-DIBS-D
Rome III – Subtypes of IBSRome III – Subtypes of IBS
17091709

Functional Dyspepsia (B1a)Rome IIIRome III
Postprandial Distress
Syndrome(B1a)
Postprandial Distress
Syndrome(B1a)
EpigastricPain
Syndrome(B1b)
EpigastricPain
Syndrome(B1b)
17921792
EPSPDS
FD

Diagnostic Criteria* for Functional Dyspepsia
Rome IIIRome III
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
17931793
Must include one or more of the following:Must include one or more of the following:
And No evidence of structural disease (including
at upper endoscopy) that is likely to explain the symptoms
And No evidence of structural disease (including
at upper endoscopy) that is likely to explain the symptoms
Bothersome postprandial
fullness
Bothersome postprandial
fullness
Earlysatiation
Earlysatiation
Epigastricpain
Epigastricpain
Epigastricburning
Epigastricburningoror orororor

Diagnostic Criteria* forPostprandial Distress Syndrome
Rome IIIRome III
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
17941794
Must include one or both of the following:Must include one or both of the following:
Bothersome postprandial fullness
occurring after ordinary-sized meals
at least several times a week
Bothersome postprandial fullness
occurring after ordinary-sized meals
at least several times a week
Early satiation
that prevents finishing a regular meal
and occurs at least several times a week
Early satiation
that prevents finishing a regular meal
and occurs at least several times a week
oror

Diagnostic Criteria* forEpigastric Pain Syndrome
Must include all of the following:Must include all of the following:
Rome IIIRome III
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
17951795
generalized or localized to other abdominal or chest regions
generalized or localized to other abdominal or chest regions
relieved by defecation or flatulence
relieved by defecation or flatulence
fulfilling criteria for gallbladder or sphincter of Oddi disorders
fulfilling criteria for gallbladder or sphincter of Oddi disorders
Pain or burning which is: intermittent, localized to the epigastrium of at least moderate severity,
at least once per week, and NOT:
Pain or burning which is: intermittent, localized to the epigastrium of at least moderate severity,
at least once per week, and NOT:

Rome III
Diagnostic Criteria: Must include episodes of pain located in the epigastrium and/or right upper quadrant and ALL of the following:
Episodes lasting 30 minutes or longer Recurrent symptoms occurring at different intervals (not daily) Pain:
Builds up to a steady level Is moderate to severe enough to interrupt daily activities Is not relieved by:
Bowel movements Postural change Antacids
Other structural symptoms that could explain symptoms are excluded
Supportive Criteria: The pain may present with one or more of: Association with nausea or vomiting Radiates to the back and/or right infra subscapular region Awakens from sleep in the middle of the night
Diagnostic Criteria: Must include episodes of pain located in the epigastrium and/or right upper quadrant and ALL of the following:
Episodes lasting 30 minutes or longer Recurrent symptoms occurring at different intervals (not daily) Pain:
Builds up to a steady level Is moderate to severe enough to interrupt daily activities Is not relieved by:
Bowel movements Postural change Antacids
Other structural symptoms that could explain symptoms are excluded
Supportive Criteria: The pain may present with one or more of: Association with nausea or vomiting Radiates to the back and/or right infra subscapular region Awakens from sleep in the middle of the night 18001800
Functional Gall Bladder and Sphincter of Oddi DisordersFunctional Gall Bladder and Sphincter of Oddi Disorders

Rome III
Diagnostic Criteria: Must include ALL of the following:Diagnostic Criteria: Must include ALL of the following:
Functional Gall Bladder DisorderFunctional Gall Bladder Disorder
Criteria for functional gallbladder and sphincter of Oddi disorder
Criteria for functional gallbladder and sphincter of Oddi disorder
Gallbladder is presentGallbladder is present
Normal liver enzymes, conjugated bilirubin, and amylase/lipase
Normal liver enzymes, conjugated bilirubin, and amylase/lipase
18011801

Diagnostic Criteria: Must include BOTH of the following:Diagnostic Criteria: Must include BOTH of the following:
Criteria for functional gallbladder and sphincter of Oddi disorder
Criteria for functional gallbladder and sphincter of Oddi disorder
Normal amylase/lipaseNormal amylase/lipase
Functional Biliary Sphincter of Oddi DisorderFunctional Biliary Sphincter of Oddi Disorder
Rome III
18021802
Supportive Criterion:Elevated serum transaminases, alkaline phosphatase, or conjugated bilirubin temporarily related to at least two pain episodes
Supportive Criterion:Elevated serum transaminases, alkaline phosphatase, or conjugated bilirubin temporarily related to at least two pain episodes
Diagnostic Criteria: Must include BOTH of the following:Diagnostic Criteria: Must include BOTH of the following:Functional Pancreatic Sphincter of Oddi DisorderFunctional Pancreatic Sphincter of Oddi Disorder
Criteria for functional gallbladder and sphincter of Oddi disorder
Criteria for functional gallbladder and sphincter of Oddi disorder
Abnormal amylase/lipaseAbnormal amylase/lipase

Rome III Committees
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Committees Chapter Structure Changes for Rome III Issues and Limitations
Rationale for Diagnostic Criteria Administrative Structure Activities/Projects Timeline for Committees Chapter Structure Changes for Rome III Issues and Limitations
16981698

Rome III Committees – Issues and Limitations
Criteria Not Fully Evidence BasedLimited data for most functional GI disorders Original criteria by consensusChanges based on new evidenceNew changes need validation
The Field is Expanding and GrowingInformation not “set in stone”Knowledge can quickly become outdated Classifications will change – e.g., “Organification”
Need for Quality ControlDisclosure of relationships with PharmaceuticalsConfidentiality statementsInternational Resource CommitteeEmbargo on information until final editing stages
Criteria Not Fully Evidence BasedLimited data for most functional GI disorders Original criteria by consensusChanges based on new evidenceNew changes need validation
The Field is Expanding and GrowingInformation not “set in stone”Knowledge can quickly become outdated Classifications will change – e.g., “Organification”
Need for Quality ControlDisclosure of relationships with PharmaceuticalsConfidentiality statementsInternational Resource CommitteeEmbargo on information until final editing stages
17781778

Future Issues for Rome Foundation
Global educational programs
Support for validation studies
Partner with regulatory agencies
Working team initiatives
Mechanism for research support
Diversification in structure
Global educational programs
Support for validation studies
Partner with regulatory agencies
Working team initiatives
Mechanism for research support
Diversification in structure17031703

What’s new?Functional dyspepsia• Dyspepsia as previously defined unhelpful• De-emphasize functional dyspepsia• New syndromes suggested for research: PDS and EPS
Nausea and vomiting• Two new syndromes (CIN and CVS)

“Pain or discomfort centered in the upper abdomen”
Rome Working Teams I and IIRome Working Teams I and II
“Pain or discomfort centered in the upper abdomen”
Rome Working Teams I and IIRome Working Teams I and II
Definition of Dyspepsia Definition of Dyspepsia
Talley et al. Gut 1999;45:II37-42 Talley et al. Gut 1999;45:II37-42
Rome III discards this definitionRome III discards this definition

Functional Dyspepsia: Rationale for Changes from Rome II
No single symptom present in all patients with functional dyspepsia
Considerable variation in symptom pattern between patients
Despite Rome II recommendations, studies still include heartburn and acid regurgitation as “dyspepsia”1
1Armstrong et al. Can J Gastroenterol 2002; 16; 439-50 Peura et al. Am J Med 2004; 116: 740-8 Moayyedi et al. Gastroenterology 2004; 127: 1329-37
1Armstrong et al. Can J Gastroenterol 2002; 16; 439-50 Peura et al. Am J Med 2004; 116: 740-8 Moayyedi et al. Gastroenterology 2004; 127: 1329-37

Dyspepsia Usually PolysymptomaticDyspepsia Usually Polysymptomatic
99% >2; > 80% >5; < 0.1% 1 symptom99% >2; > 80% >5; < 0.1% 1 symptom
Aliment Pharmacol Ther. 2003;17:1481-91

Functional Dyspepsia (FD): Rome II
12 weeks (within 12 months) of persistent or recurrent dyspepsia 12 weeks (within 12 months) of persistent or recurrent dyspepsia (pain or discomfort centered in upper abdomen)(pain or discomfort centered in upper abdomen)
No evidence of organic disease likely No evidence of organic disease likely to explain symptoms (including EGD)to explain symptoms (including EGD)
Not irritable bowel syndrome (IBS)Not irritable bowel syndrome (IBS)
Subgroups (ulcer-like, dysmotility-like) based on predominant Subgroups (ulcer-like, dysmotility-like) based on predominant symptomsymptom
Talley et al. Gut 1999;45(Suppl. 1):I28–31Talley et al. Gut 1999;45(Suppl. 1):I28–31
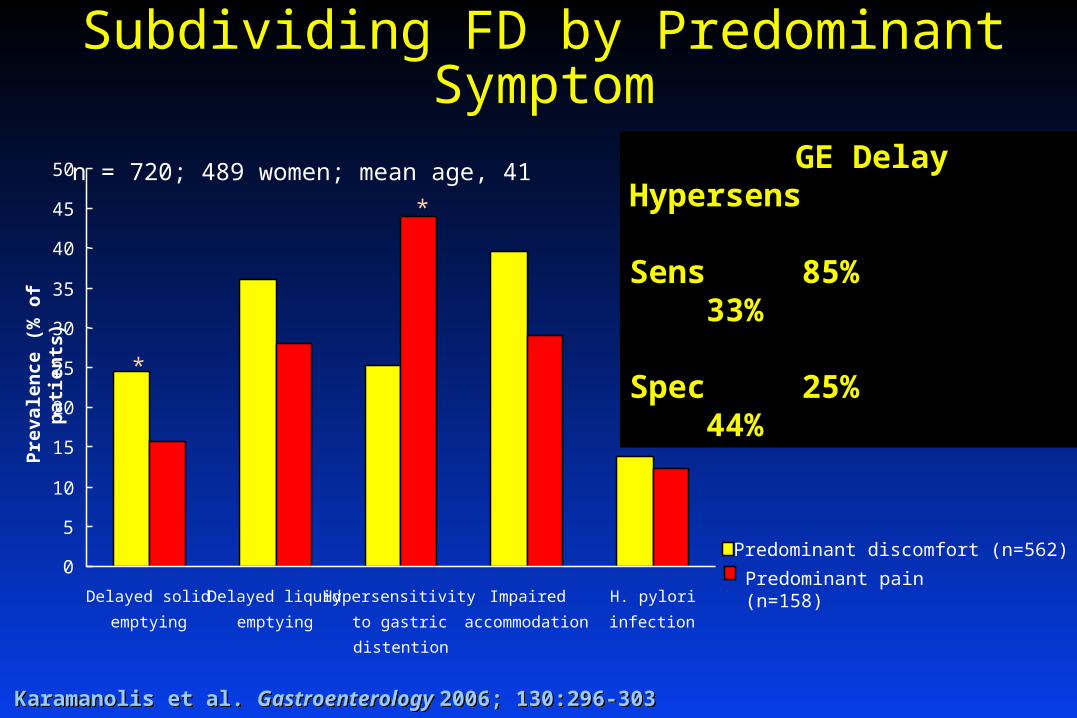
Subdividing FD by Predominant Symptom
Karamanolis et al. Gastroenterology 2006; 130:296-303 Karamanolis et al. Gastroenterology 2006; 130:296-303
Pre
vale
nce
(%
of
pat
ien
ts)
n = 720; 489 women; mean age, 41
0
5
10
15
20
25
30
35
40
45
50
Delayed solid
emptying
Delayed liquid
emptying
Hypersensitivity
to gastric
distention
Impaired
accommodation
H. pylori
infection
Predominant discomfort (n=562)
Predominant pain (n=158)
*
*
GE Delay Hypersens
Sens 85% 33%
Spec 25% 44%

Unexplained pain or discomfort centered in upper abdomen (Rome II FD)
De-emphasize FDDe-emphasize FD
Not one disorder
Lack of evidence for the predominant symptom as criterion
Support from factor analysis in tertiary care and in general population
Expert opinion
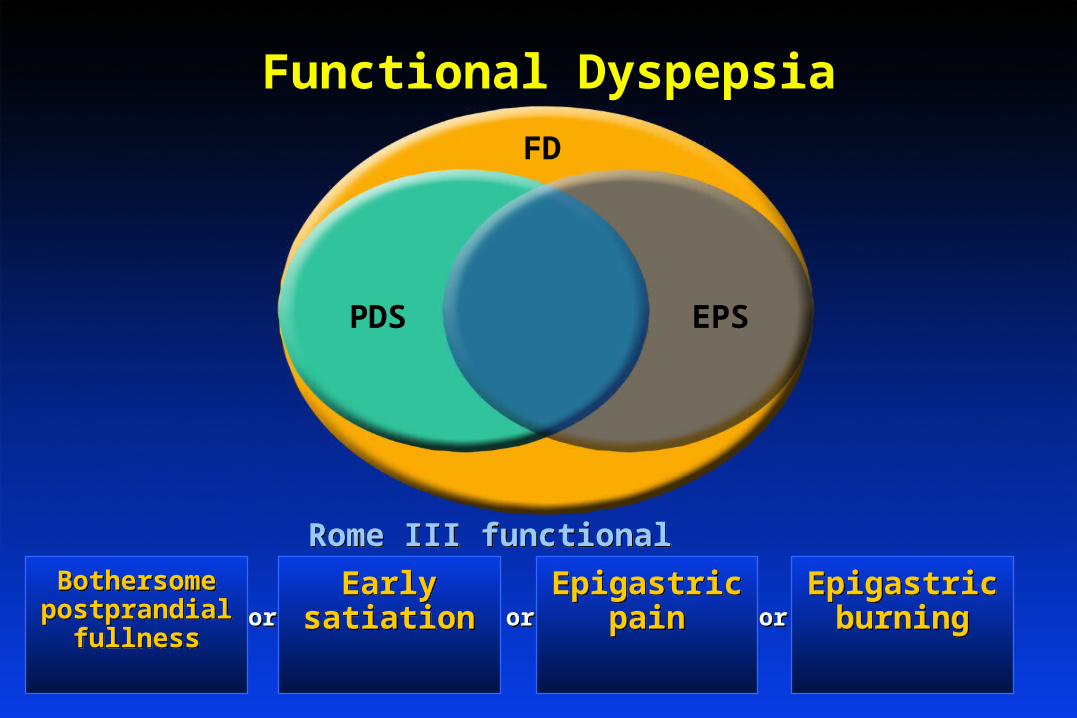
Functional Dyspepsia
Rome III functional dyspepsiaRome III functional dyspepsia
EPSPDS
FD
Bothersome postprandial
fullness
Bothersome postprandial
fullness
Earlysatiation
Earlysatiation
Epigastricpain
Epigastricpain
Epigastricburning
Epigastricburningoror orororor

Functional Dyspepsia
Rome IIIRome III
Postprandial Distress
Syndrome
Postprandial Distress
Syndrome
EpigastricPain
Syndrome
EpigastricPain
SyndromeEPSPDS
FD
FD retained for clinical practice PDS and EPS proposed for research based on factor analysis and expert opinion
FD retained for clinical practice PDS and EPS proposed for research based on factor analysis and expert opinion

Diagnostic Criteria* forPostprandial Distress Syndrome (PDS)
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
Must include one or both of the following:Must include one or both of the following:
Bothersome postprandial fullness occurring after ordinary-sized meals
at least several times a week
Bothersome postprandial fullness occurring after ordinary-sized meals
at least several times a week
Early satiation
that prevents finishing a regular meal
and occurs at least several times a week
Early satiation
that prevents finishing a regular meal
and occurs at least several times a week
oror
Rome IIIRome III

Factor Analysis Supports EPS and PDS45% of the U.S. population report upper
GI symptoms
Telephone survey of 21,128 adults
Camilleri et al. Clin Gastroenterol Hepatol. 2005;3:543-52 Camilleri et al. Clin Gastroenterol Hepatol. 2005;3:543-52

Study Population n Result Westbrook 2002 Population sample 2300 3 dyspeptic symptom factors
Fischler 2003 Tertiary care 438 4 dyspeptic symptom factors
Jones 2003 Population sample 888 3 dyspeptic symptom factors
Kwan 2003 Tertiary care 1012 3 dyspeptic symptom factors
Whitehead 2003 Tertiary care 1041 4 dyspeptic symptom factors
Camilleri 2005 Population sample 21128 3 dyspeptic symptom factors
Piessevaux submitted Population sample 2025 3 or 4 dyspeptic symptom factors
Tack in preparation Tertiary care 638 3 dyspeptic symptom factors
Factor analyses in populations and referral practice
All found a meal related factorAll found a meal related factor

Diagnostic Criteria* forEpigastric Pain Syndrome (EPS)
Must include all of the following:Must include all of the following:
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
* Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
Pain or burning which is: Intermittent, Localized to the epigastrium of at least moderate severity,
at least once per week, and NOT:
Pain or burning which is: Intermittent, Localized to the epigastrium of at least moderate severity,
at least once per week, and NOT:
Rome IIIRome III
generalized or localized to other abdominal or chest regions
generalized or localized to other abdominal or chest regions
relieved by defecation or flatulence
relieved by defecation or flatulence
fulfilling criteria for gallbladder or sphincter of Oddi disorders
fulfilling criteria for gallbladder or sphincter of Oddi disorders

Distinct Dyspepsia Subgroups: New Data
EPS 135 (39%)
CIN n=37 (11%)
PDS (early satiety)
114 (32%)
25 (7%)
16 (5%)
9 (3%)
7 (2%)
Observed (n) Expected (n)
p-value
EPS vs. CIN
16 35 0.006
EPS vs. PDS
32 83 <0.001
PDS vs. CIN
23 33 0.078
Comparison of overlap of subgroups between observed and expected
* Assuming the subgroups were independent* Assuming the subgroups were independent Choung et al. DDW 2006 Choung et al. DDW 2006
Olmsted County population dataOlmsted County population data

Rome III
Overlap with GERD
Heartburn does not exclude a diagnosis of FD (PDS or EPS)if dyspepsia persists despite a trial of adequate acid suppression
Evidence: expert opinion
Overlap with GERD
Heartburn does not exclude a diagnosis of FD (PDS or EPS)if dyspepsia persists despite a trial of adequate acid suppression
Evidence: expert opinion

Overlap with IBS
Coexisting IBS no major impact on symptom pattern or putative pathophysiological mechanisms
Corsetti et al. Am J Gastroenterol. 2004;99:1152-9 Corsetti et al. Am J Gastroenterol. 2004;99:1152-9
0
5
10
15
20
25
30
35
40
45
50
Delayed emptying H. pylori positive Hypersensitivity Impairedaccommodation
Prev
alen
ce (%
of p
atie
nts)
Dyspepsia
Dyspepsia + IBS*
* P<0.05
Rome IIIRome III

Nausea and Vomiting
Cyclic vomiting syndrome (CVS) now a recognized syndrome in adults
AJG 2001; 96: 684-8

Cyclic vomiting syndrome (CVS)At least 3 months, with onset at least 6 month previously, of:
Stereotypical episodes of vomiting regarding onset (acute) and duration (less than one week)
3 or more discrete episodes in the prior year Absence of nausea and vomiting between episodes
Supportive criteria: History of migraine headaches or a family history of migraine headaches
Rome IIIRome III

Chronic idiopathic nausea (CIN)
Separate from FD (factor analyses)
Bothersome nausea, occurring at least several times per week in the last 3 months
Not usually associated with vomiting
Absence of abnormalities at upper endoscopy or metabolic disease that explains the nausea
Rome IIIRome III

Rome III: What’s new?Functional dyspepsia• Dyspepsia as previously defined unhelpful: focus on early
satiation and/or postprandial fullness and/or epigastric pain• De-emphasize functional dyspepsia• New syndromes suggested for research: PDS and EPS
Nausea and vomiting• Two new syndromes (CIN and CVS)
Irritable Bowel Syndrome
Functional Bloating
Functional Constipation
Functional Diarrhea
Unspecified Functional Bowel Disease
Functional Bowel DisordersFunctional Bowel Disorders

• Introduction of a frequency threshold of 3 days/ month over 3 months for symptoms
• Reduction of the duration of symptoms before one can make firm diagnosis from 12 to 6 months
• Refining of subtypes
• Introduction of a frequency threshold of 3 days/ month over 3 months for symptoms
• Reduction of the duration of symptoms before one can make firm diagnosis from 12 to 6 months
• Refining of subtypes
Main Changes in IBS CriteriaMain Changes in IBS Criteria

Rome II Diagnostic criteria for IBS
Rome II Diagnostic criteria for IBS
At least 12 weeks, which need not be consecutive, in the preceding 12 months of abdominal discomfort or pain that has two of three features:
Relieved with defecation; and/or
Onset associated with a change in frequency of stool; and/or
Onset associated with a change in form (appearance) of stool.
Thompson et al Gut 1999;45 Suppl 2:II43-II47 Thompson et al Gut 1999;45 Suppl 2:II43-II47

Rome III Diagnostic Criteria for IBS*
Rome III Diagnostic Criteria for IBS*
Recurrent abdominal pain or discomfort
3 days per month in the last three months
associated with two or more of the following Improvement with defecation; and/or Onset associated with a change in frequency of stool; and/or Onset associated with a change in form (appearance) of stool
* Criteria fulfilled for the last 3 months with symptom onset 6 months prior to diagnosis

Subclassifying IBSWhy bother?
Important for choosing therapies which alter bowel habit Subtypes likely to have different pathophysiology
Transit Stool consistency Rectal sensitivity?

Diarrhea-predominant 1 or more of 2, 4, or 6 and none of 1, 3, or 5 (or 2 of 2, 4 or 6 and 1 of 1 or 5 but not 3)
Diarrhea-predominant 1 or more of 2, 4, or 6 and none of 1, 3, or 5 (or 2 of 2, 4 or 6 and 1 of 1 or 5 but not 3)
Previous Features Used to Subclassify IBS Patients
Constipation-predominant 1 or more of 1, 3, or 5 and none of 2, 4, or 6 (or 2 of 1, 3 or 5 and 1 of 2, 4 or 6)
Constipation-predominant 1 or more of 1, 3, or 5 and none of 2, 4, or 6 (or 2 of 1, 3 or 5 and 1 of 2, 4 or 6)
1. Fewer than three bowel movements a week
2. More than three bowel movements a day
3. Hard or lumpy stools
4. Loose (mushy) or watery stools
5. Straining during a bowel movement
6. Urgency (having to rush to have a bowel movement)
1. Fewer than three bowel movements a week
2. More than three bowel movements a day
3. Hard or lumpy stools
4. Loose (mushy) or watery stools
5. Straining during a bowel movement
6. Urgency (having to rush to have a bowel movement)
Problems With Old SystemProblems With Old System
Complex to apply and caused confusion in both patients and clinicians!
Multidimensional but different dimensions don’t correlate well
Failed to deal adequately with patients with both hard and loose stools
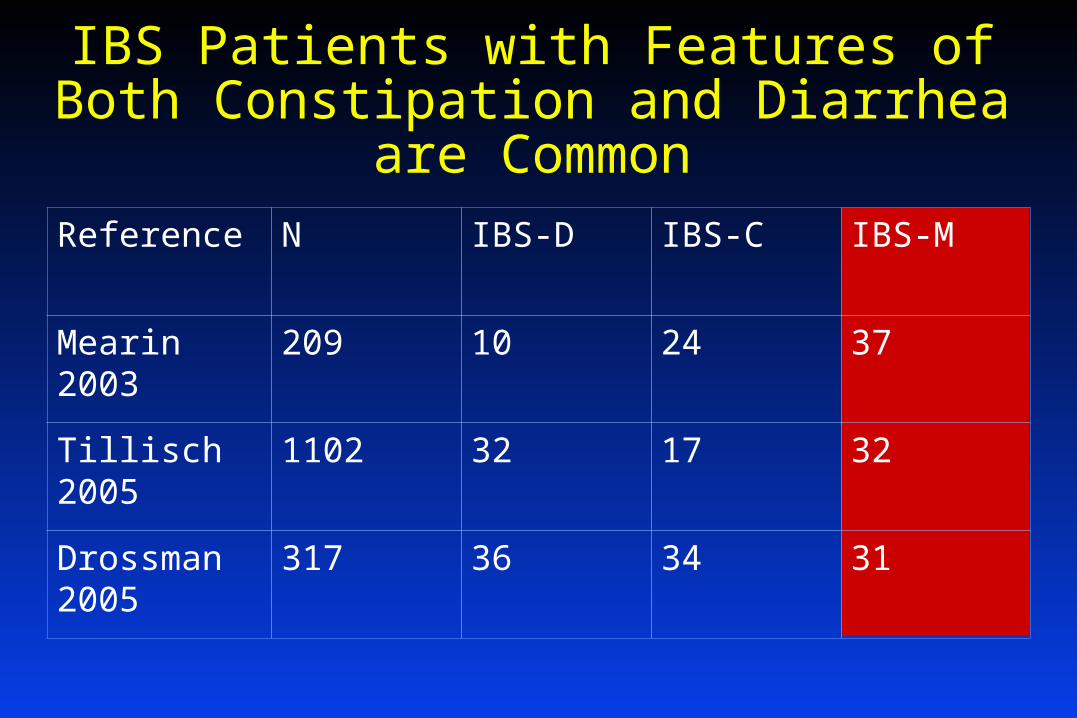
IBS Patients with Features of Both Constipation and Diarrhea are Common
Reference N IBS-D IBS-C IBS-M
Mearin 2003 209 10 24 37
Tillisch 2005 1102 32 17 32
Drossman 2005
317 36 34 31

• Assessed from stool form
Rome III subtyping is based on Stool Consistency alone
Rome III subtyping is based on Stool Consistency alone

Defining Stool ConsistencyBristol Stool Form Scale
Hard Hard
NormalNormal
LooseLoose

Why Stool Consistency as Main Determinant of Subtype?
Correlates best with colonic transit

Colonic Transit & Stool FormColonic Transit & Stool Form
Colonic transittime (hours)
Colonic transittime (hours)
Bristol stool form scoreBristol stool form score
1 2 3 4 5 6 7
80
40
0
O'Donnell et al Br Med J 1990;300:439-40 O'Donnell et al Br Med J 1990;300:439-40

Why Stool Consistency as Main Determinant of Subtype?
Correlates best with colonic transit
Correlates best with what patients and community samples think of as “diarrhoea”
Principle determinant of incontinence
Other features occur in IBS with both loose & hard stools Stool frequency <3/weeks or >3/day
Urgency, Sense of incomplete evacuation
Principle determinant of incontinence
Other features occur in IBS with both loose & hard stools Stool frequency <3/weeks or >3/day
Urgency, Sense of incomplete evacuation

Association of bowel symptoms with stool consistency
Tillisch et al Am J Gastroenterol. 2005; 100:896-904Tillisch et al Am J Gastroenterol. 2005; 100:896-904

Proposed New Subtyping Based on Stool Consistency Alone
IBS with constipation - IBS-C IBS with diarrhoea - IBS-D IBS mixed type - IBS-M (IBS unsubtyped - IBS-U)
IBS-mixed : patients with both hard & loose stools over periods of hours or days
IBS-mixed : patients with both hard & loose stools over periods of hours or days
Alternating IBS
Patients who change subtype over periods of weeks and months

00 2525 5050 7575 10010000
2525
5050
7575
100100
IBS-MIBS-M
IBS-DIBS-D
IBS-CIBS-C
IBS-UIBS-U
%Loose or Watery Stools%Loose or Watery Stools
% Hard or Lumpy Stools
% Hard or Lumpy Stools
Rome III Subtypes of IBS
46%46%
3.9%3.9% 32%32%
17%17%
Tillisch et al Am J Gastroenterol. 2005;100:896-904 Tillisch et al Am J Gastroenterol. 2005;100:896-904

Quantifying Stool FormDate Pain Pain
Severity
Urgency
Y/N
Bloating
Y/N
1 2 3 4 5 6 7 8
Pain: grade 0-10 0= absent 5=moderate 10 very severeStool form1= separate hard lumps, like nuts 6 = fluffy pieces with ragged edges2= sausage shaped but lumpy 7 = watery, no solid pieces 3= like a sausage or snake, but with cracks
on its surface4= like a sausage or snake, smooth and soft5= soft blobs with clear cut edges
Pain: grade 0-10 0= absent 5=moderate 10 very severeStool form1= separate hard lumps, like nuts 6 = fluffy pieces with ragged edges2= sausage shaped but lumpy 7 = watery, no solid pieces 3= like a sausage or snake, but with cracks
on its surface4= like a sausage or snake, smooth and soft5= soft blobs with clear cut edges

Changes to IBS classificationRome III Summary
No change to basic criteria
Length of time needed to define chronicity reduced to 6 months
Threshold 3 days / month introduced for frequency of pain / discomfort
Subtyping simplified (stool consistency)
Stability of subtypes and link to other features like visceral sensitivity and response to treatment remain to be determined
Stability of subtypes and link to other features like visceral sensitivity and response to treatment remain to be determined

FUNCTIONAL GALLBLADDER AND
SPHINCTER OF ODDI DISORDERS
NOT EXPLAINED BY STRUCTURAL ABNORMALITIES
Epigastric or right upper quadrant
pain
Motility abnormalities of the Gallbladder, the Biliary, and Pancreatic Sphincter of
Oddi

DIAGNOSTIC CRITERIA FOR FUNCTIONAL GALLBLADDER AND SPHINCTER OF ODDI DISORDERS
time
PAINSteady
30 min
severe
moderate
mild
Pain located in the epigastrium
and/or right upper quadrant
Epigastric or right upper quadtrant pain
Recurrent symptoms occurring
at different intervals (not daily)
Episodes lasting 30 minutes or longer The pain builds up to a steady level
The pain is moderate to severe enough to interrupt the patient’s daily activities or lead to an emergency department visit
Not Relieved by 1. Bowel Movements 2. Postural Change 3. Antacids
Supportive Criteria The pain may present with one or
more of the following:
a. Associated with nausea and vomiting
b. Radiates to the back and/or right infra subscapular region
c. Awakens from sleep in the middle of the night
EVIDENCE : C
ONSENSUS

Structural
alterations
ROME III ALGORITHM FOR FUNCTIONAL GB DISORDERS
Diagnostic criteria for functional GB and SO disorders LFTs/pancreatic, enzyme, US
Esophagogastroduodenoscopy
Normal findingsAppropriate
investigation andtreatment
GB CCK cholescintigraphy
GBEF < 40% GBEF > 40%
Cholecystectomy Reassess
EVIDENCE C

Structural alterations explaining
the symptoms
ROME III ALGORITHM FOR FUNCTIONAL BILIARY SO DISORDERS
CholecystectomizedDiagnostic criteria for functional GB and SO disorders
LFTs/pancreatic enzymes, USEsophagogastroduodenoscopy
EUS, MRCP
Appropriate Investigation
and treatment
BiliaryType I
BiliaryType II
BiliaryType III
Pain andOne or two of type
I criteria
Pain andNone of the type
I criteria Milwaukee Classification
Pain and LFTs in 2 occasions andAt ERCP Dilated CBD >12mm and Delayed contrast
drainage
Milwaukee Classification Revised Pain and LFTs in 2 occasions andAT US Dilated CBD >8mm
EVIDENCE :
CONSENSUS
Structural alterations explaining
the symptoms
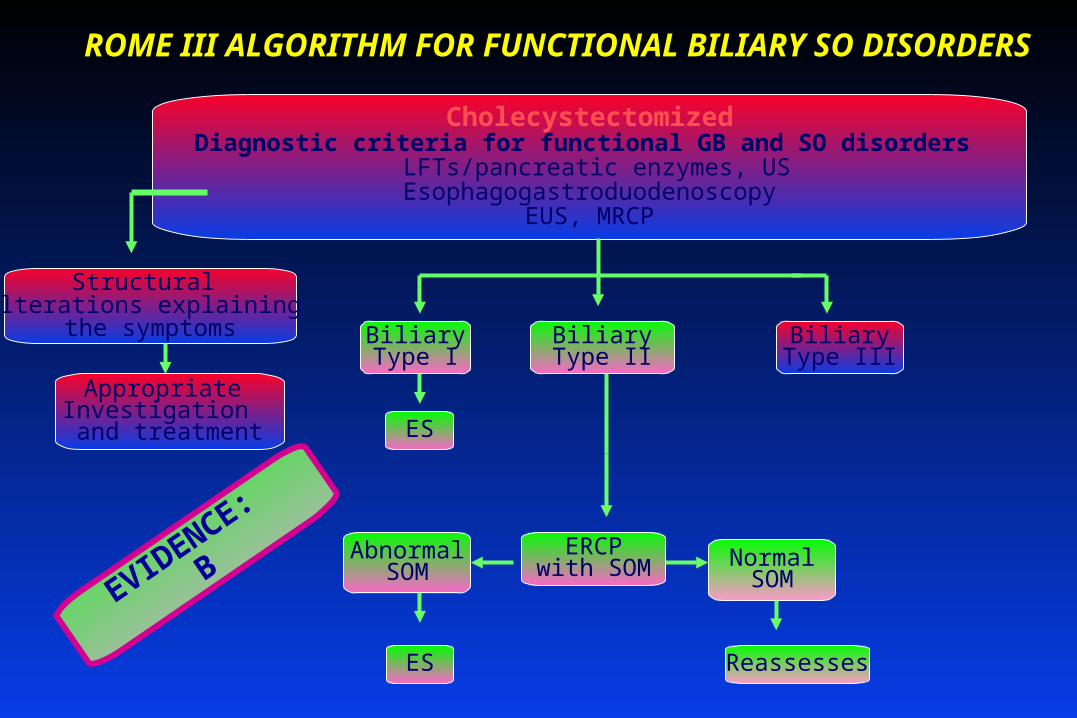
ROME III ALGORITHM FOR FUNCTIONAL BILIARY SO DISORDERS
CholecystectomizedDiagnostic criteria for functional GB and SO disorders
LFTs/pancreatic enzymes, USEsophagogastroduodenoscopy
EUS, MRCP
Appropriate Investigation
and treatment
BiliaryType II
BiliaryType I
ES
BiliaryType III
ERCPwith SOM Normal
SOMAbnormal
SOM
ES Reassesses
EVIDENCE:
B
Structural alterations explaining
the symptoms
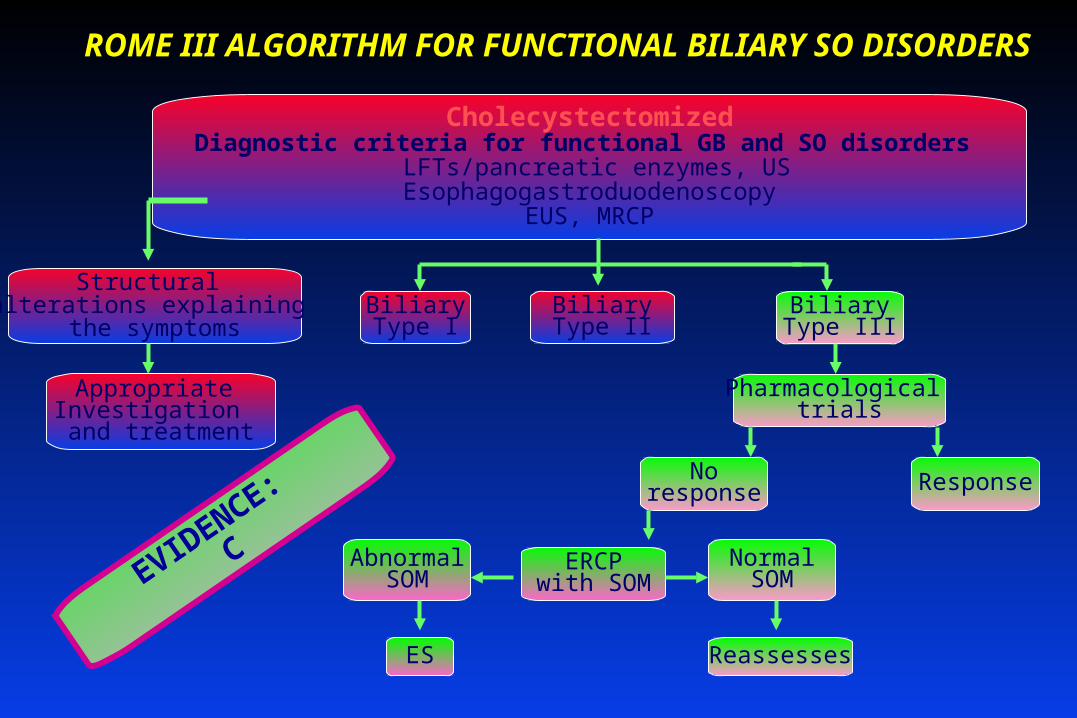
ROME III ALGORITHM FOR FUNCTIONAL BILIARY SO DISORDERS
CholecystectomizedDiagnostic criteria for functional GB and SO disorders
LFTs/pancreatic enzymes, USEsophagogastroduodenoscopy
EUS, MRCP
Appropriate Investigation
and treatment
BiliaryType II
BiliaryType I
BiliaryType III
Pharmacological trials
ResponseNoresponse
ERCPwith SOM
NormalSOM
AbnormalSOM
ES Reassesses
EVIDENCE:
C

ROME III ALGORITHM FOR FUNCTIONAL BILIARY SO DISORDERS
Appropriate Investigation
and treatment
Structural alterations explaining
the symptoms
Cholecystectomized ,Criteria for functional GB and SO Disorders
Clinical history, LFTs/pancreatic enzymes, USEsophagogastroduodenoscopy
EUS, MRCP
BiliaryType I
ES
AbnormalSOM
BILI[CHOLEDOCHO]SCINTIGRAPHY
Response
Pharmacological trials
BiliaryType III
BiliaryType II
Reassesses
NormalSOM
ES
ERCPwith SOM
Noresponse
EVIDENCE B

ROME III ALGORITHM FOR FUNCTIONAL PANCREATIC SO DISORDERS
Criteria for functional GB and SO disorders, Elevated amylase and lipase
No obvious association with alchool, gallstones, drugs, Ca2+ US, Esophagogastroduodenoscopy, CT, EUS,MRCP
Diagnostic ERCP
EVIDENCE B
No Structural
abnormalities
Abnormal
Structural
abnormalities
Sphincterotomy
Reassess
SO manometry
Normal

Functional Esophageal
FunctionalAbdominal Pain
FunctionalBilliary
FunctionalAnorectal
FunctionalGastroduodenal
IBS & Functional Bowel
Rome IIIDiagnostic
Questionnaire
Rome IIIDiagnostic
Questionnaire

Rationale for Changing to Ordinal Scales to Measure Symptom Frequency
• Rome II questionnaire applied the same frequency threshold to all symptoms
• Some symptoms are not clinically meaningful unless they occur daily while others are significant if they occur at all
• Rome II questions were difficult to understand because they incorporated multiple frequency thresholds
• Scales for judging relative severity would be useful

Goals of the Questionnaire Development and Validation Process
• Develop a questionnaire that incorporates the Rome III criteria as an aid to diagnosis
• Insure that questions are understandable
• Validate the questionnaire & the criteria by comparing to diagnoses made by clinicians

Study ICompare 4 Alternative Response Scales
• Subjects 120 healthy controls & 84 FGID
• Design: 4 versions of the questionnaire were completed in counterbalanced order
– Binary: No or rarely vs. often
– Specific Frequency: Monthly, weekly, daily
– Relative Frequency: Occasionally, often, always
– Bothersome: A little bit, moderately, quite a bit

Subjects are Inconsistent in How They Use the Binary Response Scale
0%
20%
40%
60%
80%
100%
never monthly >weekly
"never or rarely" "often"
Frequency of Abdominal Pain or Discomfort

Principal Findings of Study I • For intermediate symptom frequencies, ordinal scales are
more reliable
• Specific Frequency Scales give the best balance between sensitivity & specificity but Relative Frequency Scales perform almost as well
• Bothersome Scale performs similar to Relative Frequency Scale but is not appropriate to some symptoms

Two Scales Selected for Rome III
Specific Frequency Scale
Never
Less than 1 day a month
One day a month
One day a week
More than 1 day a week
Every day
Relative Frequency Scale
Never or rarely
Sometimes
Often
Most of the time
Always

Questionnaire Development
• Rome board suggested initial questions
• Working teams provided additional items
• Questionnaire Committee met for 2 days to insure that the questions matched the diagnostic criteria
• Data from the validation study were referred back to the Rome board & working teams for revisions to criteria & thresholds

Sample QuestionSample QuestionIn the last 3 months, how
often did you have discomfort or pain anywhere in your abdomen?
Never
Less than 1 day a month
One day a month
Two to three days a month
One day a week
More than one day a week
Every day

Study II: Validation Study• Subjects
– 554 healthy controls (75% participation)
– 399 FGIDs (66% participation)
• 328 IBS, 27 constipation, 10 FD, 32 miscellaneous
• There were 4 study sites: UNC, Mayo Clinic, University of Michigan, & University of Toronto
• Test – retest agreement on diagnosis assessed in 53 controls & 51 patients over 2 weeks

Understandability• 18 of 77 questions were rated difficult to understand by
1% or more of subjects
• 4 questions were rated difficult by 2%
• All but one of these 18 questions were revised
• No revision for, “In the last 3 months, how often did you feel uncomfortably full after a regular sized meal.” (Rated difficult by 1.2%)

Selecting Frequency Thresholds so ThatLess Than 10% of Controls are “Abnormal”
0%
5%
10%
15%
20%
25%
30%
35%
40%
Healthy
Frequency of Abdominal Pain or Discomfort

0%
5%
10%
15%
20%
25%
30%
35%
40%Healthy
IBS
0%
5%
10%
15%
20%
25%
30%
35%
40%Healthy
IBS
Frequency of Abdominal Pain or Discomfort
Selecting Frequency Thresholds so ThatLess Than 10% of Controls are “Abnormal”
Selecting Frequency Thresholds so ThatLess Than 10% of Controls are “Abnormal”
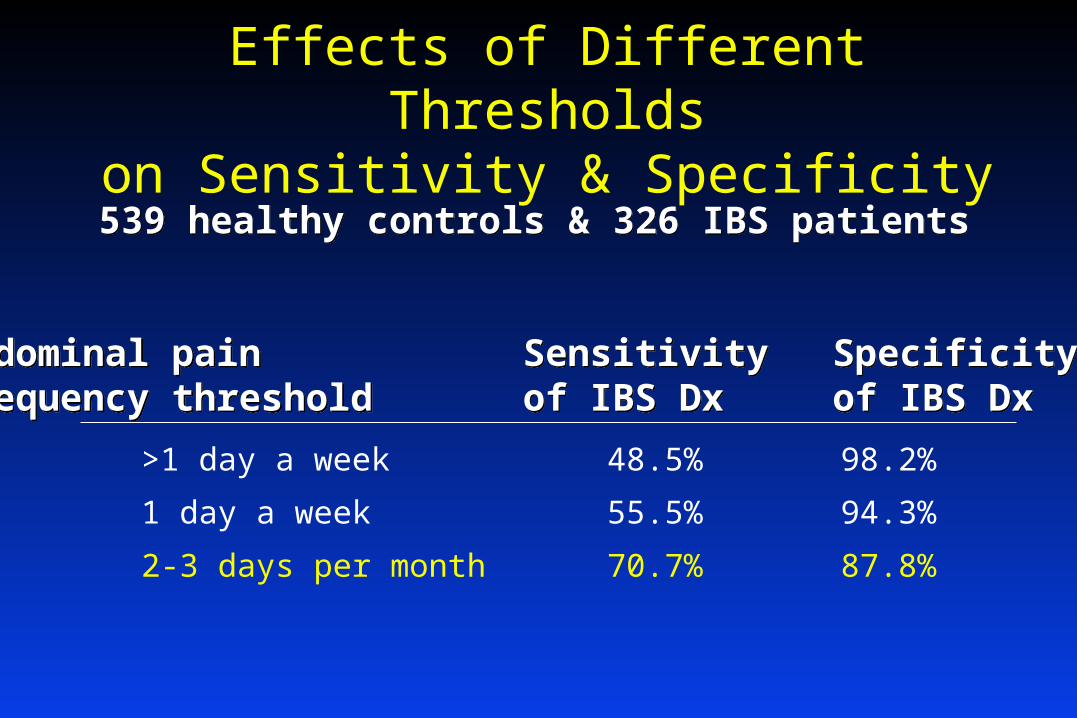
Effects of Different Thresholdson Sensitivity & Specificity
>1 day a week 48.5% 98.2%
1 day a week 55.5% 94.3%
2-3 days per month 70.7% 87.8%
539 healthy controls & 326 IBS patients 539 healthy controls & 326 IBS patients
Abdominal pain Sensitivity SpecificityFrequency threshold of IBS Dx of IBS DxAbdominal pain Sensitivity SpecificityFrequency threshold of IBS Dx of IBS Dx

Specificity: Percent of Healthy Controls Who Would be
MisclassifiedMisdiagnosed Controls
Estimated
Specificity
IBS 12.2% 87.8%
Constipation 3.5% 96.5%
Diarrhea 0.1% 99.1%
Functional dyspepsia 5.9% 94.1%
Postprandial distress 0.7% 99.3%
Epigastric pain 0 100%
Chronic idiopathic nausea 0.9% 99.1%

Reliability: Test-Retest Agreement Over a 2-Week Interval
Specificity Test-Retest Agreement
IBS 87.8% 81.7%
Constipation 96.5% 93.3%
Diarrhea 99.1% 96.2%
Functional dyspepsia 94.1% 84.6%
Postprandial distress 99.3% 85.6%
Epigastric pain 100% 98.1%
Chronic idiopathic nausea 99.1% 96.2%

Conclusions• A major innovation of Rome III is ordinal scale with
individual frequency thresholds
• Rome III diagnostic questionnaire is reliable:– Questions reflect the criteria & are understandable– Test-retest reliability is excellent– Specificity of diagnostic criteria is excellent

Application of Diagnostic CriteriaApplication of Diagnostic Criteria
Consensus derived criteriaConsensus derived criteria
QuestionnaireQuestionnaire
ValidationValidation
Published trial and survey dataPublished trial and survey data
Can it be applied to my patient?Can it be applied to my patient?
Consensus derived criteriaConsensus derived criteria
QuestionnaireQuestionnaire
ValidationValidation
Published trial and survey dataPublished trial and survey data
Can it be applied to my patient?Can it be applied to my patient?

To Interpret Data Obtained UsingTo Interpret Data Obtained UsingRome III Questionnaire, I Must Consider:Rome III Questionnaire, I Must Consider:
1.1. Was the questionnaire altered?Was the questionnaire altered?
2.2. What was the purpose of the study?What was the purpose of the study?
3.3. How was the study population selected?How was the study population selected?
4.4. Can the data (evidence) from Can the data (evidence) from thatthat trial or trial or survey be survey be applied to my patient?applied to my patient?
1.1. Was the questionnaire altered?Was the questionnaire altered?
2.2. What was the purpose of the study?What was the purpose of the study?
3.3. How was the study population selected?How was the study population selected?
4.4. Can the data (evidence) from Can the data (evidence) from thatthat trial or trial or survey be survey be applied to my patient?applied to my patient?

1. 1. Was the Questionnaire Altered?Was the Questionnaire Altered?
Questions – how were they asked? Questions – how were they asked?
Also, algorithms, inclusions and exclusionsAlso, algorithms, inclusions and exclusions
Determined by consensus, existing dataDetermined by consensus, existing data To suit their study, investigators may adjust:To suit their study, investigators may adjust:
Time requisite (acute vs. chronic)Time requisite (acute vs. chronic) Cut-off levels for inclusionCut-off levels for inclusion ExclusionsExclusions

Frequency Scale “Cut-offs”Frequency Scale “Cut-offs”
How often in last 3 months did you have pain?How often in last 3 months did you have pain?
a. Nevera. Neverb. Once a month or lessb. Once a month or lessc. Two to three times/monthc. Two to three times/month
d. Once a weekd. Once a weeke. Several times a weeke. Several times a weekf. Every dayf. Every day
Cut-offs determine who is included!Cut-offs determine who is included!
1. (cont) Was the questionnaire altered?1. (cont) Was the questionnaire altered?
Rome IIIRome III

Frequency Scale “Cut-offs”Frequency Scale “Cut-offs”
How often in last 3 months did you have pain?How often in last 3 months did you have pain?
a. Nevera. Neverb. Once a month or lessb. Once a month or less
c. Two to three times/monthc. Two to three times/monthd. Once a weekd. Once a weeke. Several times a weeke. Several times a weekf. Every dayf. Every day
Cut-offs determine who is included!Cut-offs determine who is included!
1. (cont) Was the questionnaire altered?1. (cont) Was the questionnaire altered?
SurveySurvey

Frequency Scale “Cut-offs”Frequency Scale “Cut-offs”
How often in last 3 months did you have pain?How often in last 3 months did you have pain?
a. Nevera. Neverb. Once a month or lessb. Once a month or lessc. Two to three times/monthc. Two to three times/monthd. Once a weekd. Once a week
e. Several times a weeke. Several times a weekf. Every dayf. Every day
Cut-offs determine who is included!Cut-offs determine who is included!
1. (cont) Was the questionnaire altered?1. (cont) Was the questionnaire altered?
Clinical trialClinical trial

ExclusionsExclusionsQ8. ..did you often have heartburn..?Q8. ..did you often have heartburn..?Q9. ..did you .. have difficulty swallowing..?Q9. ..did you .. have difficulty swallowing..?
Rome II coding:Rome II coding:Functional heartburnFunctional heartburn; ; Q8=yes, and no to dysphagiaQ8=yes, and no to dysphagiaFunctional dysphagiaFunctional dysphagia; ; Q9=yes, and no to heartburnQ9=yes, and no to heartburn
1.1. If “yes” to both, If “yes” to both, neitherneither disorder exists because, disorder exists because, according to the coding, one excludes the other.according to the coding, one excludes the other.
2.2. Data not applicable to excluded patients.Data not applicable to excluded patients.
1. (cont) Was the questionnaire altered?1. (cont) Was the questionnaire altered?

1.1. To aid diagnosisTo aid diagnosis
2.2. To select subjects for clinical researchTo select subjects for clinical research
3.3. To survey populationsTo survey populations
2. 2. What was the Purpose of the Study?What was the Purpose of the Study?

2. 2. What was the Purpose of the Study?What was the Purpose of the Study?
1.1. To aid diagnosisTo aid diagnosis Severity/frequency relevantSeverity/frequency relevant InclusiveInclusive Symptoms nowSymptoms now
2.2. To select subjects for clinical researchTo select subjects for clinical research Severity/frequency more relevantSeverity/frequency more relevant ExclusiveExclusive Symptoms nowSymptoms now
3.3. To survey populationsTo survey populations Severity/frequency less importantSeverity/frequency less important InclusiveInclusive Symptoms ever, or during defined periodSymptoms ever, or during defined period

3. 3. How was the Study Population Selected?How was the Study Population Selected?
Were Rome III criteria used?Were Rome III criteria used?
How were subjects recruited (adverts, How were subjects recruited (adverts, tertiary care, CROs)? tertiary care, CROs)?
Were there investigator adjustments (e.g. Were there investigator adjustments (e.g. time requirement, cut-offs, exclusions)?time requirement, cut-offs, exclusions)?

4. 4. Can Data from a Trial or Survey be Applied to Can Data from a Trial or Survey be Applied to my Patient?my Patient?
Does my patient fulfill the same criteria?Does my patient fulfill the same criteria?
Is he or she similar to the study population?Is he or she similar to the study population?
Do the time requisites, scales, and exclusions used in Do the time requisites, scales, and exclusions used in the study exclude my patient?the study exclude my patient?
In a trial where placebo effect>therapeutic gain, will my In a trial where placebo effect>therapeutic gain, will my patient realize a similar placebo effect?patient realize a similar placebo effect?

Summary: When Applying Results of a Study where Summary: When Applying Results of a Study where the Rome Criteria were Used, Ask:the Rome Criteria were Used, Ask:
1.1. How were criteria translated into questions: How were criteria translated into questions: – Time requirement, cut-offs, and exclusions?Time requirement, cut-offs, and exclusions?
2.2. Were there unique adjustments for:Were there unique adjustments for:– Clinical Trial?Clinical Trial? - - severe cases nowsevere cases now
– Epidemiological survey?Epidemiological survey? - - include all casesinclude all cases
– Clinical Practice?Clinical Practice? -- precision precision
3.3. Does my local population or my patient resemble the Does my local population or my patient resemble the study’s population?study’s population?
4.4. Will my management help my patient achieve as great a Will my management help my patient achieve as great a placebo effect as those in the study?placebo effect as those in the study?

Use of the Rome CriteriaUse of the Rome Criteria
ClinicalTrials
ClinicalResearch
ClinicalPractice

Existing Trials
Expert Panels
Regulatory Authorities
Existing TrialsImproved methodology
Meta-analysesNegative trials?
Regulatory AuthoritiesEMEA PTC 2003
FDA Advices
Expert PanelsDefinition of a Responder, Vienna 1998
European Panel, APT 2003Rome I, Rome II

Challenges for FGIDs clinical trials Natural course of the condition
–Unstable symptom pattern–Fluctuating intensity
Multicomponent pathophysiology–Multiple therapeutic targets–Multiple endpoints
Bias of outcome measures–High placebo response–Difficulty to maintain double masking–Contamination by parallel interventions–Lack of placebo control for some interventions
• Psychotherapy, hypnotherapy, sphincterotomy
Avoiding harm–FGID non-life-threatening
Natural course of the condition–Unstable symptom pattern–Fluctuating intensity
Multicomponent pathophysiology–Multiple therapeutic targets–Multiple endpoints
Bias of outcome measures–High placebo response–Difficulty to maintain double masking–Contamination by parallel interventions–Lack of placebo control for some interventions
• Psychotherapy, hypnotherapy, sphincterotomy
Avoiding harm–FGID non-life-threatening

Definition of the Studied PopulationDefinition of the Studied Population
Compromise between the largest target in the population and a strictly homogenous group Compromise between the largest target in the population and a strictly homogenous group
Clearly define the FGID to be treated Define subgroups
Transit abnormalities Explicit inclusion/exclusion criteria
Gender Symptoms intensity Comorbidities Treatment exclusions
Clearly define the FGID to be treated Define subgroups
Transit abnormalities Explicit inclusion/exclusion criteria
Gender Symptoms intensity Comorbidities Treatment exclusions

The Standard Trial Design
• Superiority trial– The most robust design:
• parallel groups, randomized allocation, double blind
– Single intervention– Placebo-controlled
• Superiority trial– The most robust design:
• parallel groups, randomized allocation, double blind
– Single intervention– Placebo-controlled
Run-in Treatment Phase Run-out
Placebo
Intervention

Per
cen
tag
e o
f re
spo
nd
ers
Weeks
0
20
40
60
0 2 4 6 8 10 12 14 16
* * * **
****
*
Treatment Follow-up
**
**
*
**p < 0.001*p < 0.05
Alosetron (n = 237) Placebo (n = 221)
80
70
50
30
10
Camilleri et al. Lancet 2000; 355: 1035-1040.
0
10
20
30
40
50
60
70
-2 1 3 5 7 9 11 13 15
TegaserodPlacebo
Follow-upRun-in
Novick et al. APT 2002; 16:1877-1888.

From Rome II to Rome IIIFrom Rome II to Rome III
• Unsolved issues with standard design Duration of the treatment intervention
4 weeks versus 12 weeks Longer treatments: 6 months
Outcome measures
Alternative trial designs On-demand or « Pro Re Nata (PRN) » treatments Treatment – Re-treatment design
• Unsolved issues with standard design Duration of the treatment intervention
4 weeks versus 12 weeks Longer treatments: 6 months
Outcome measures
Alternative trial designs On-demand or « Pro Re Nata (PRN) » treatments Treatment – Re-treatment design

PlaceboPlacebo
Active DrugActive Drug
Treatment – Re-treatment
RR
NRNR
Active DrugActive Drug
EMEA PTC 2003
PlaceboPlacebo NRNR
RR
No symptomNo symptom
Symptoms +Active DrugActive Drug
PlaceboPlacebo
Active DrugActive Drug
NRNR
Carry-overUnblinding of the intervention
Enrichment in respondersNatural cycle of symptoms
Ethical considerations

Tack et al. Gut 2005; 54: 1707-1713
IBS-C symptoms
Abdominal discomfort/pain
=9.3% =16.6% =9.1% =15.91%
Re
sp
on
de
rs (
%)
Tegaserod
Placebo
1stT
RT
1stT
RT
0
10
20
30
40
50
RR
NRNR No sympNo symp
symp(37% R)symp(37% R)Active drugActive drug
Active drugActive drug
PlaceboPlacebo
PlaceboPlaceboNRNR
RR4 weeks4 weeks
1
4 weeks4 weeks

Definition of Outcome Measures
Primary outcome Global assessment Adequate relief Definition of a responder
Symptom questionnaire
Pain assessment
Primary outcome Global assessment Adequate relief Definition of a responder
Symptom questionnaire
Pain assessment
Secondary outcomes Mechanism of intervention Symptoms influenced by a
specific pharmacodynamic effect
Quality of life Health economics
Tolerance and safety
Secondary outcomes Mechanism of intervention Symptoms influenced by a
specific pharmacodynamic effect
Quality of life Health economics
Tolerance and safety

Definition of a Responder
SomewhatSomewhat
CompletelyCompletely
MarkedlyMarkedly
Symptom ReliefSymptom Relief
25 %25 % 75 %75 %50 %50 % 100 %100 % TimeTime

Conclusion
Rome criteria have driven significant methodological advances over the last two decades for the design of FGIDs clinical trials.
Alternative designs need to be further explored but should not replace standard comparative trials.
Outcome measures and definition of a responder are critical issues influencing the clinical relevance of the results.
Rome criteria have driven significant methodological advances over the last two decades for the design of FGIDs clinical trials.
Alternative designs need to be further explored but should not replace standard comparative trials.
Outcome measures and definition of a responder are critical issues influencing the clinical relevance of the results.





























