Embed Size (px)
Citation preview
Department of Health Services
Hospice Agency
Uniform Account Report
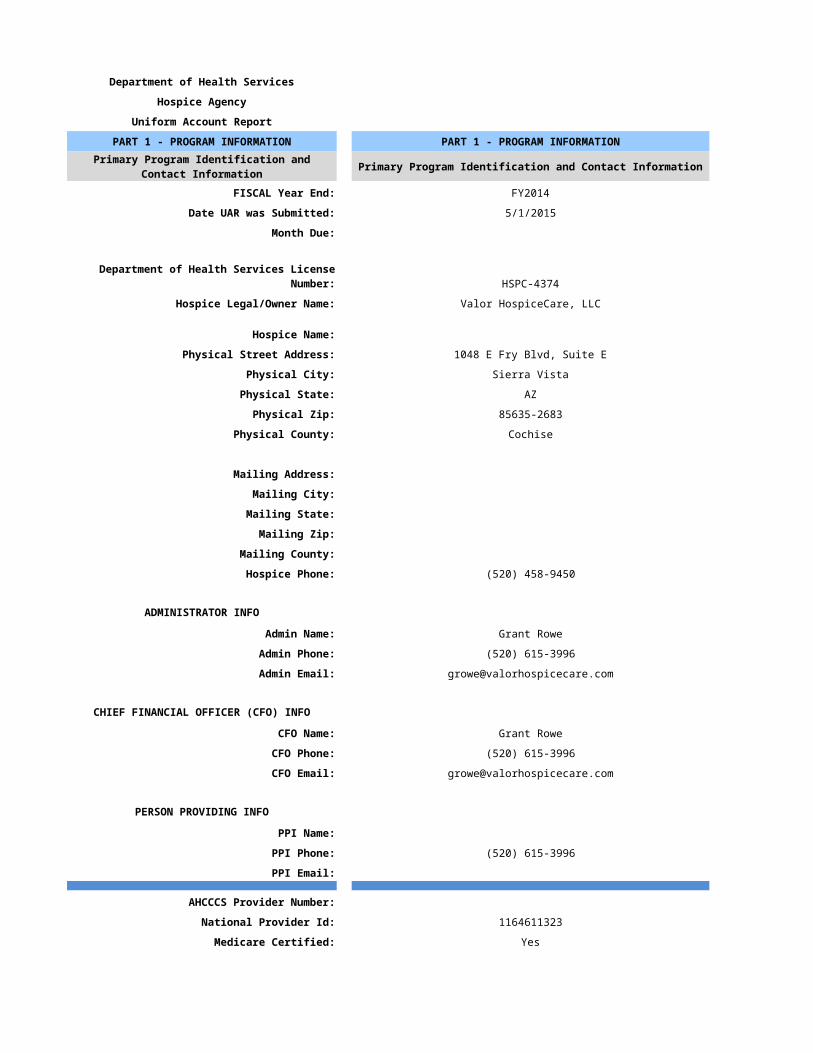
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information
FISCAL Year End: FY2014
Date UAR was Submitted: 5/1/2015
Month Due:
Department of Health Services License Number: HSPC-4374
Hospice Legal/Owner Name: Valor HospiceCare, LLC
Hospice Name:
Physical Street Address: 1048 E Fry Blvd, Suite E
Physical City: Sierra Vista
Physical State: AZ
Physical Zip: 85635-2683
Physical County: Cochise
Mailing Address:
Mailing City:
Mailing State:
Mailing Zip:
Mailing County:
Hospice Phone: (520) 458-9450
ADMINISTRATOR INFO
Admin Name: Grant Rowe
Admin Phone: (520) 615-3996
Admin Email: [email protected]
CHIEF FINANCIAL OFFICER (CFO) INFO
CFO Name: Grant Rowe
CFO Phone: (520) 615-3996
CFO Email: [email protected]
PERSON PROVIDING INFO
PPI Name:
PPI Phone: (520) 615-3996
PPI Email:
AHCCCS Provider Number:
National Provider Id: 1164611323
Medicare Certified: Yes
CCN (Medicare/Medicaid Certification Number): 31586
Primary Program Identification and Contact Information
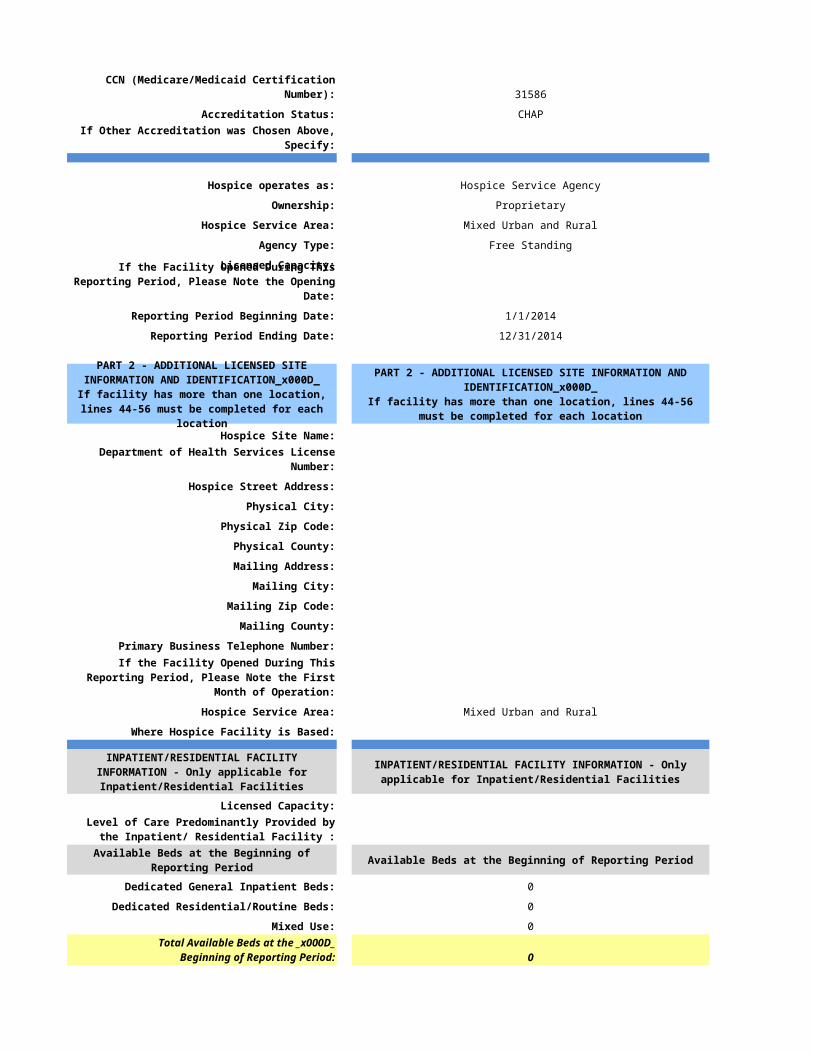
Accreditation Status: CHAP
If Other Accreditation was Chosen Above, Specify:
Hospice operates as: Hospice Service Agency
Ownership: Proprietary
Hospice Service Area: Mixed Urban and Rural
Agency Type: Free Standing
Licensed Capacity:
Reporting Period Beginning Date: 1/1/2014
Reporting Period Ending Date: 12/31/2014
Hospice Site Name:
Department of Health Services License Number:
Hospice Street Address:
Physical City:
Physical Zip Code:
Physical County:
Mailing Address:
Mailing City:
Mailing Zip Code:
Mailing County:
Primary Business Telephone Number:
Hospice Service Area: Mixed Urban and Rural
Where Hospice Facility is Based:
Licensed Capacity:
Available Beds at the Beginning of Reporting Period
Dedicated General Inpatient Beds: 0
Dedicated Residential/Routine Beds: 0
Mixed Use: 0
0
If the Facility Opened During This Reporting Period, Please Note the Opening Date:
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
If the Facility Opened During This Reporting Period, Please Note the First Month of Operation:
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Level of Care Predominantly Provided by the Inpatient/ Residential Facility :
Available Beds at the Beginning of Reporting Period
Total Available Beds at the Beginning of Reporting Period:
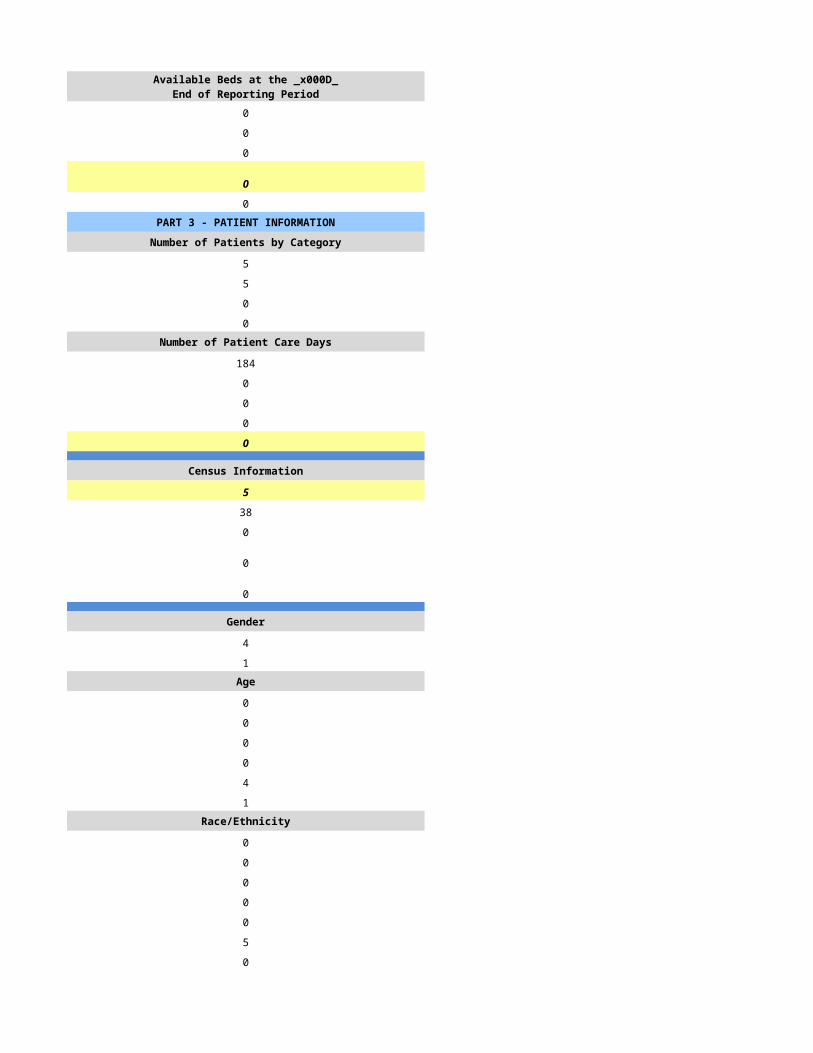
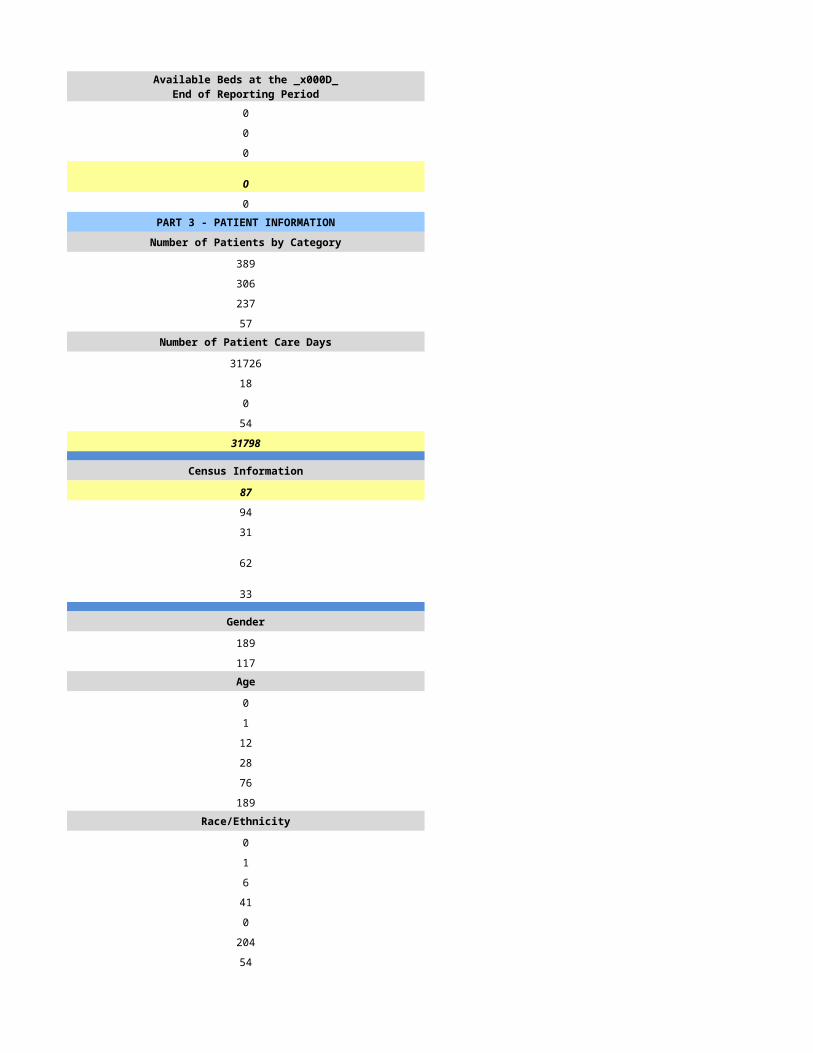
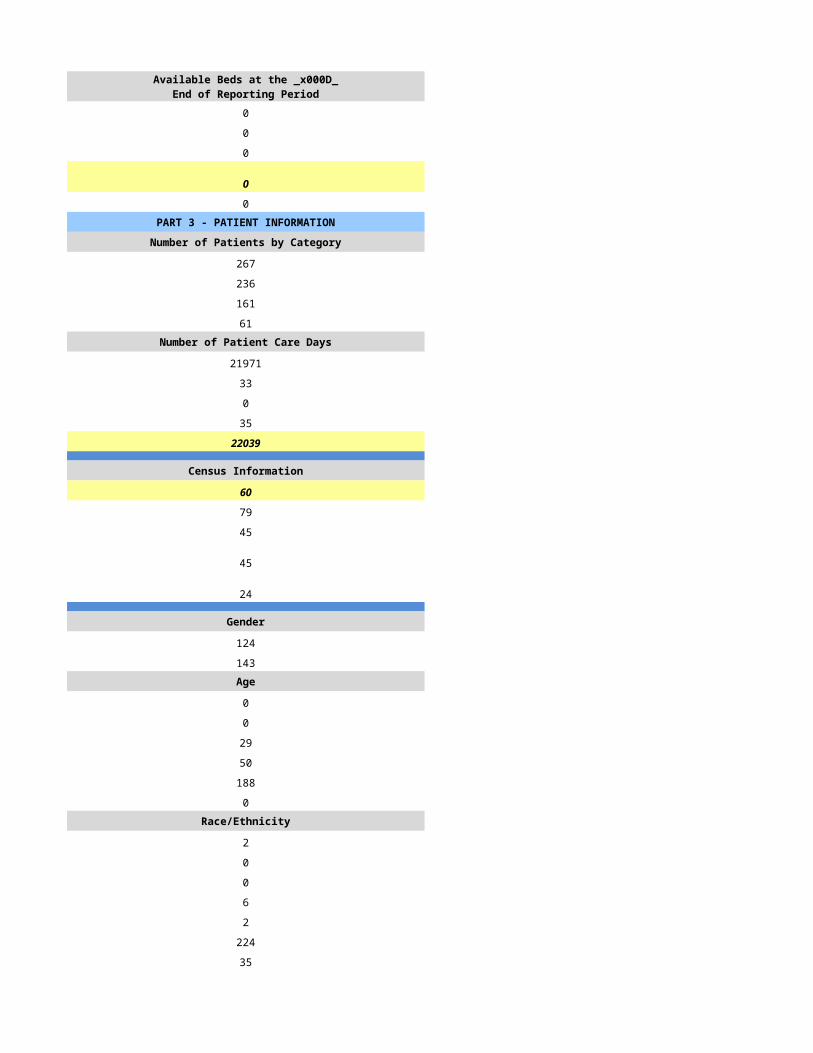
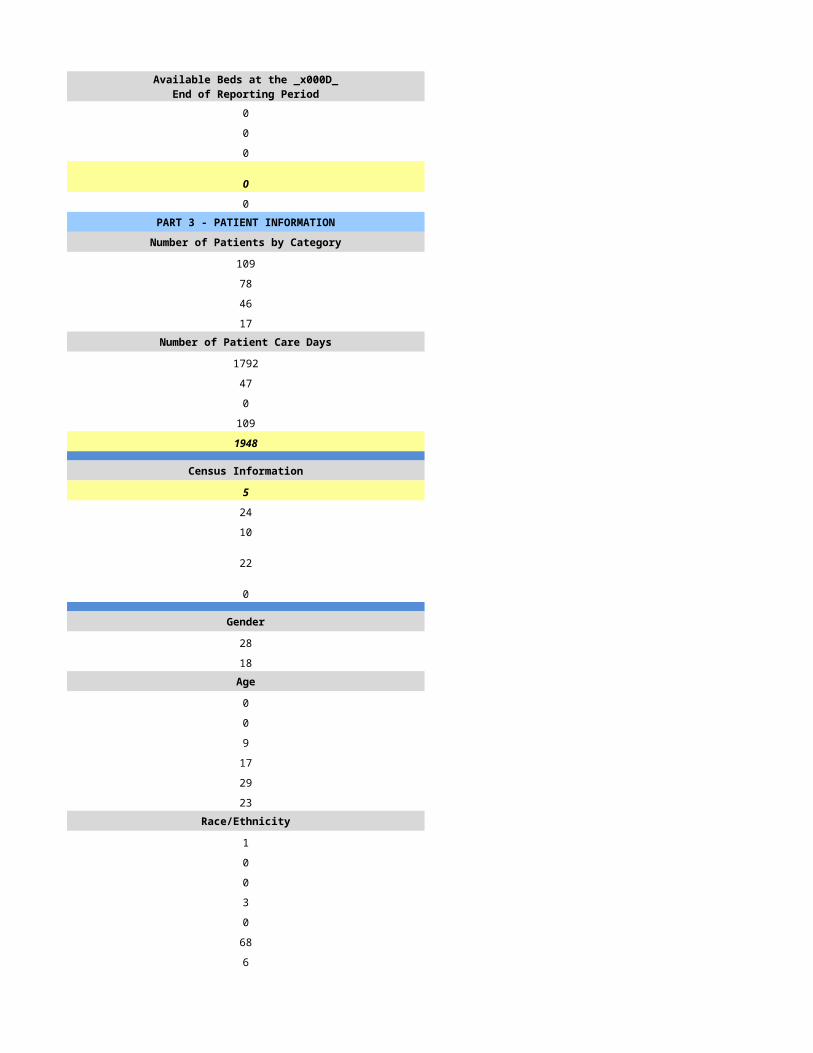
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
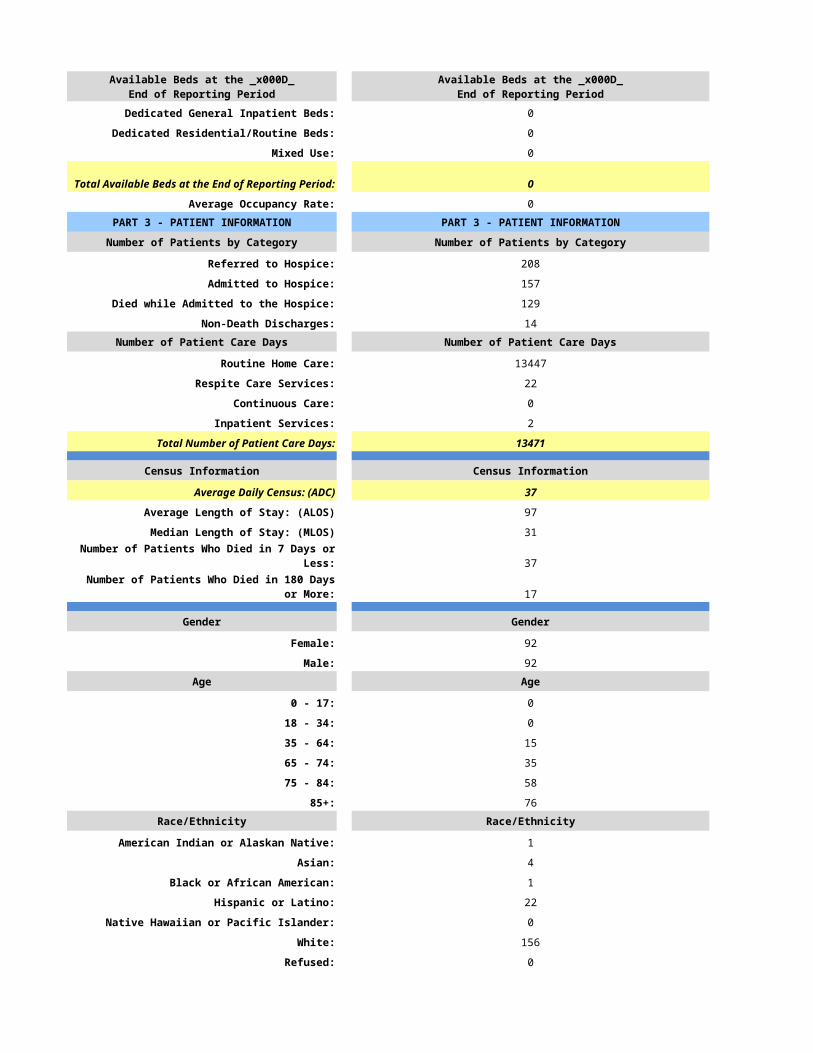
Dedicated General Inpatient Beds: 0
Dedicated Residential/Routine Beds: 0
Mixed Use: 0
0
Average Occupancy Rate: 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
Referred to Hospice: 208
Admitted to Hospice: 157
Died while Admitted to the Hospice: 129
Non-Death Discharges: 14Number of Patient Care Days Number of Patient Care Days
Routine Home Care: 13447
Respite Care Services: 22
Continuous Care: 0
Inpatient Services: 2
Total Number of Patient Care Days: 13471
Census Information Census Information
Average Daily Census: (ADC) 37
Average Length of Stay: (ALOS) 97
Median Length of Stay: (MLOS) 31
Number of Patients Who Died in 7 Days or Less: 37
17
Gender Gender
Female: 92
Male: 92Age Age
0 - 17: 0
18 - 34: 0
35 - 64: 15
65 - 74: 35
75 - 84: 58
85+: 76Race/Ethnicity Race/Ethnicity
American Indian or Alaskan Native: 1
Asian: 4
Black or African American: 1
Hispanic or Latino: 22
Native Hawaiian or Pacific Islander: 0
White: 156
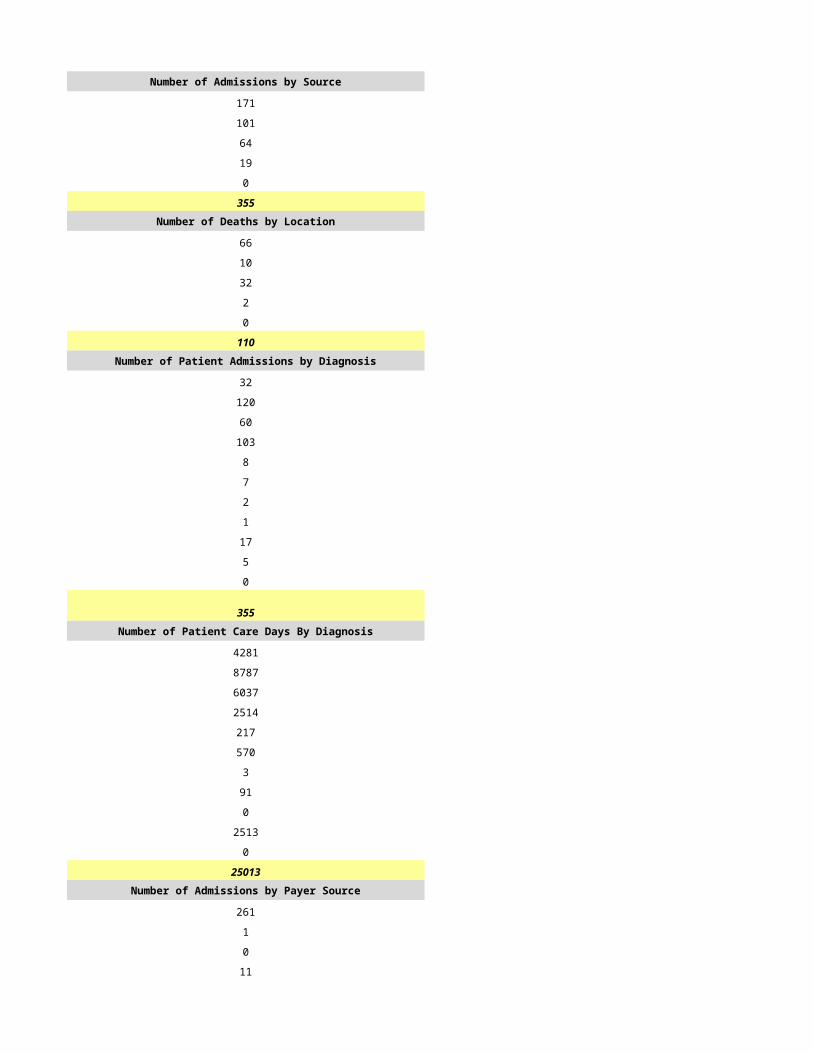
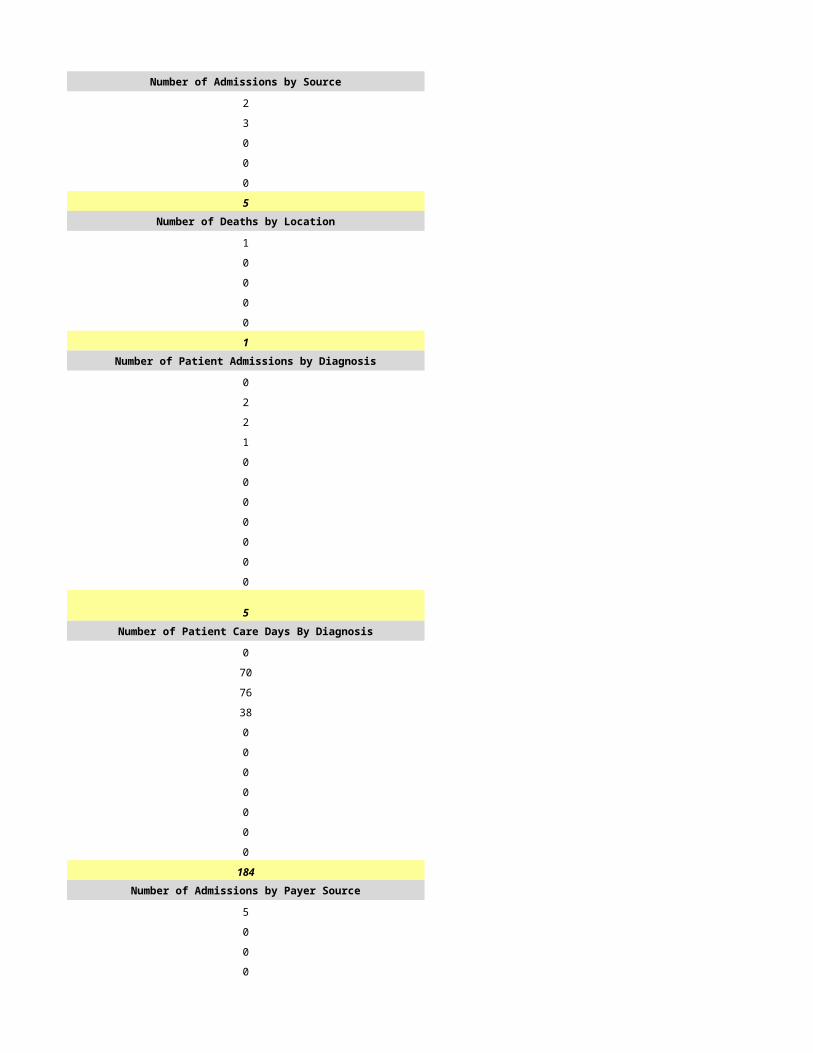
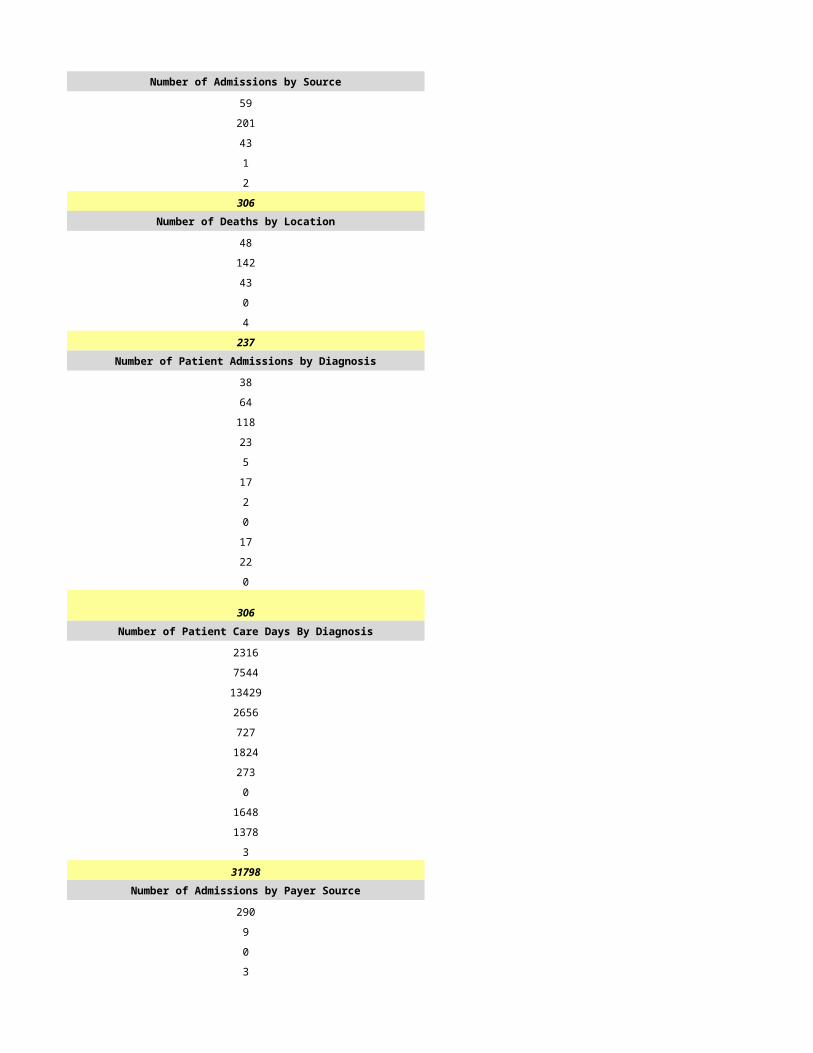
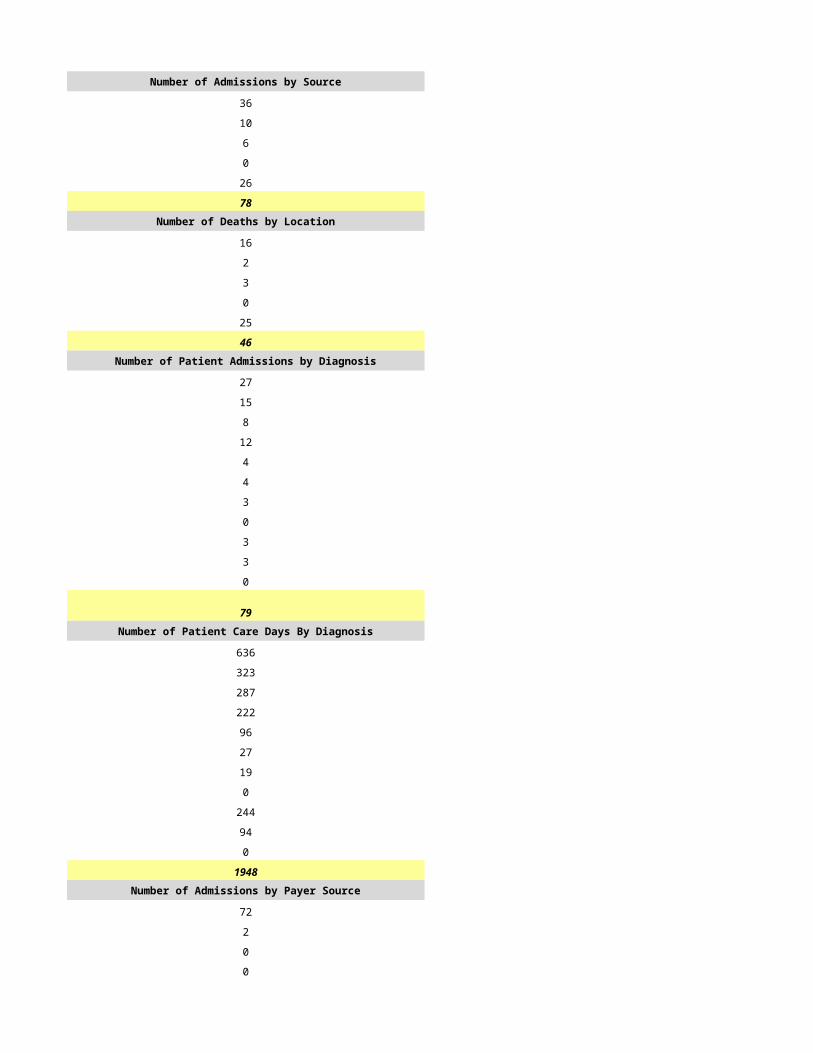
Refused: 0Number of Admissions by Source Number of Admissions by Source
Patient's Home: 127
Total Available Beds at the End of Reporting Period:
Number of Patients Who Died in 180 Days or More:
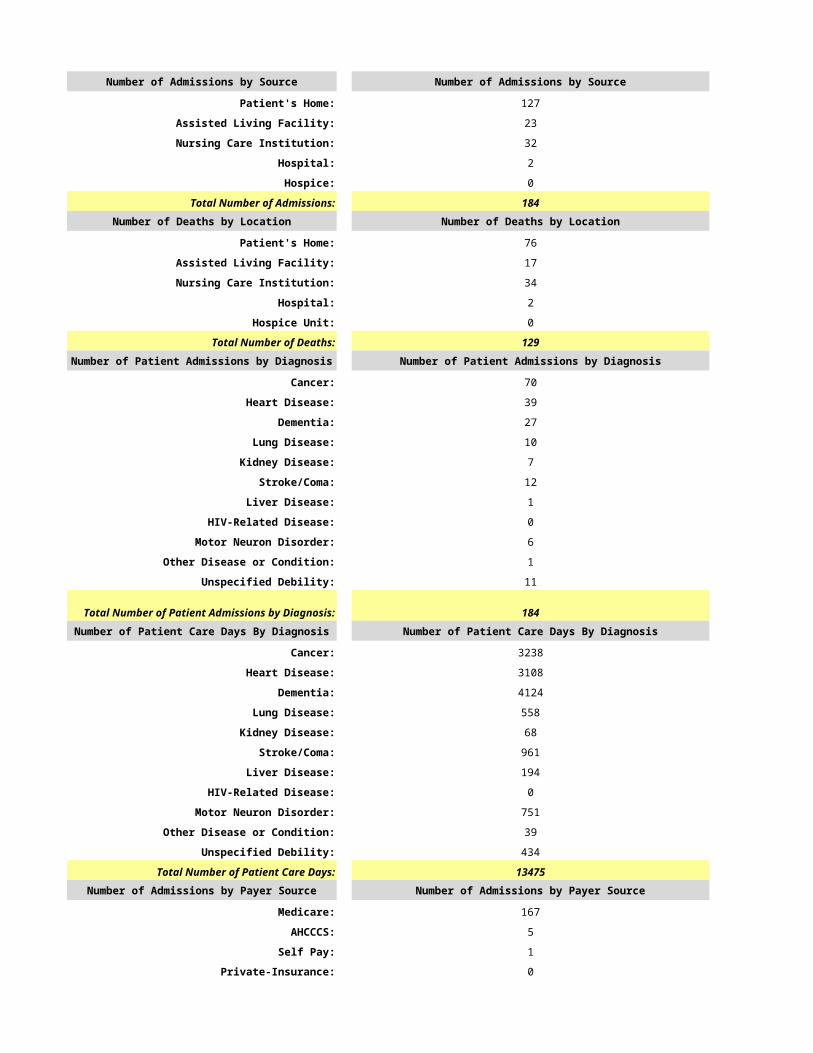
Assisted Living Facility: 23
Nursing Care Institution: 32
Hospital: 2
Hospice: 0
Total Number of Admissions: 184Number of Deaths by Location Number of Deaths by Location
Patient's Home: 76
Assisted Living Facility: 17
Nursing Care Institution: 34
Hospital: 2
Hospice Unit: 0
Total Number of Deaths: 129Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
Cancer: 70
Heart Disease: 39
Dementia: 27
Lung Disease: 10
Kidney Disease: 7
Stroke/Coma: 12
Liver Disease: 1
HIV-Related Disease: 0
Motor Neuron Disorder: 6
Other Disease or Condition: 1
Unspecified Debility: 11
Total Number of Patient Admissions by Diagnosis: 184Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
Cancer: 3238
Heart Disease: 3108
Dementia: 4124
Lung Disease: 558
Kidney Disease: 68
Stroke/Coma: 961
Liver Disease: 194
HIV-Related Disease: 0
Motor Neuron Disorder: 751
Other Disease or Condition: 39
Unspecified Debility: 434
Total Number of Patient Care Days: 13475Number of Admissions by Payer Source Number of Admissions by Payer Source
Medicare: 167
AHCCCS: 5
Self Pay: 1
Private-Insurance: 0
Other: 11
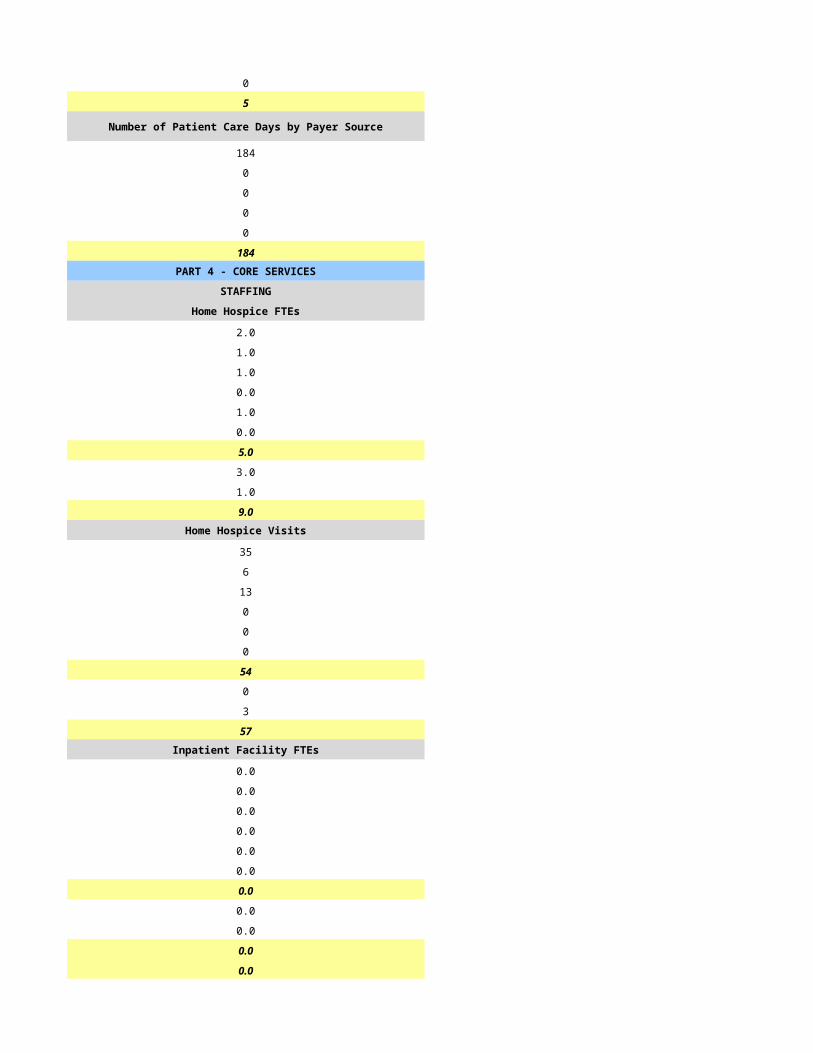
Total Number of Patient Admissions: 184
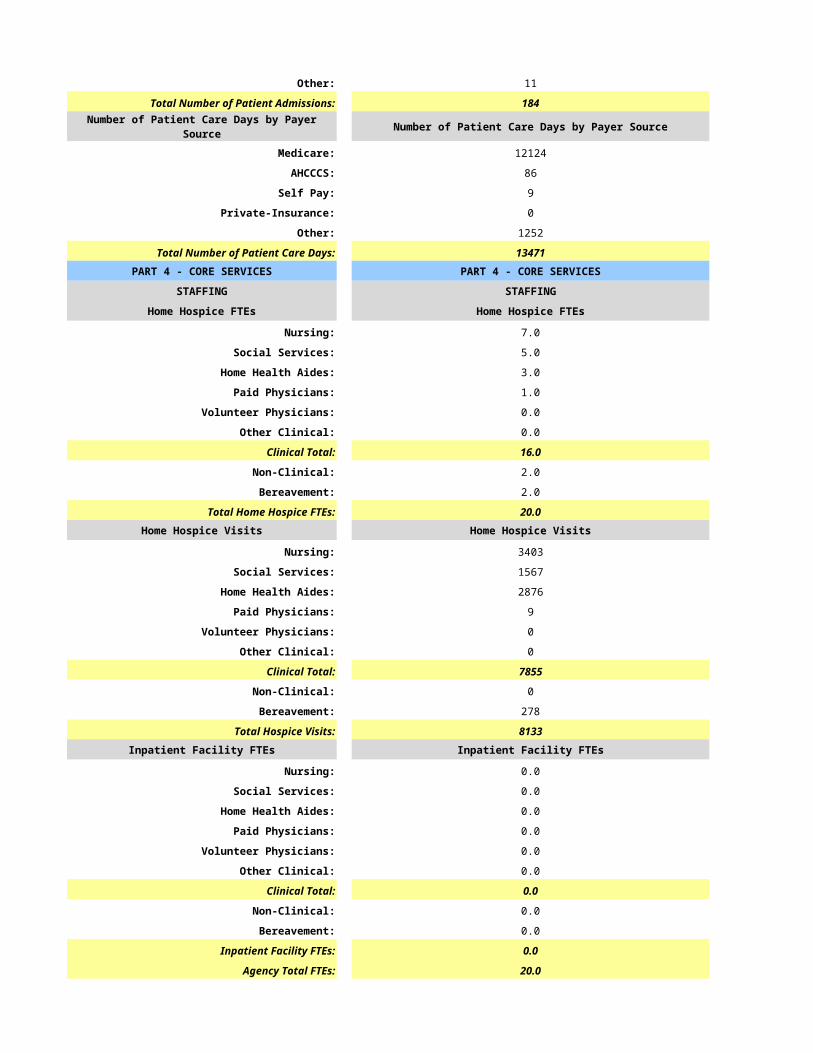
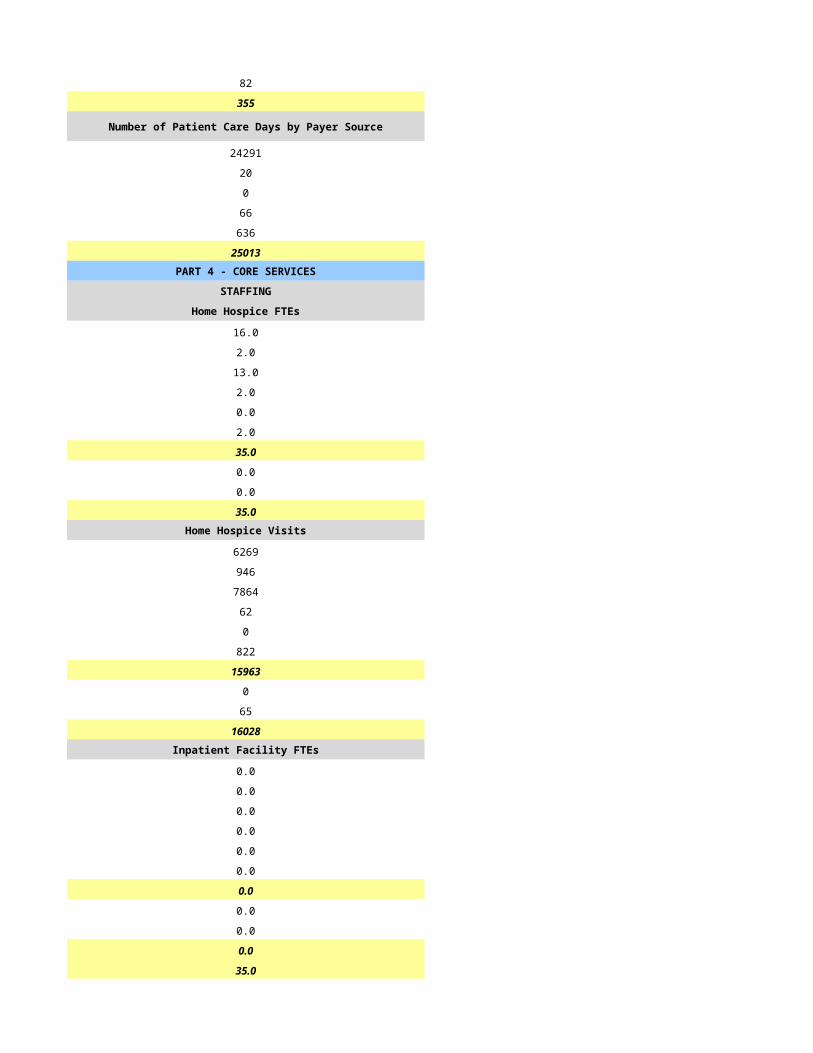
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
Medicare: 12124
AHCCCS: 86
Self Pay: 9
Private-Insurance: 0
Other: 1252
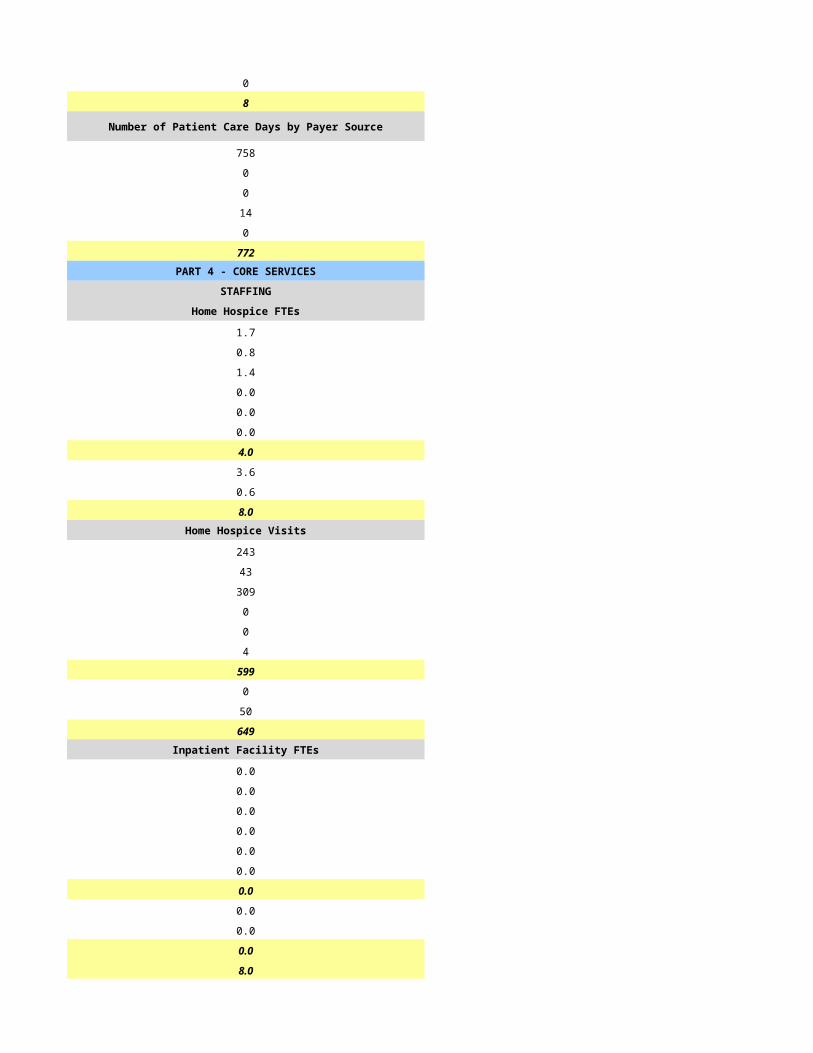
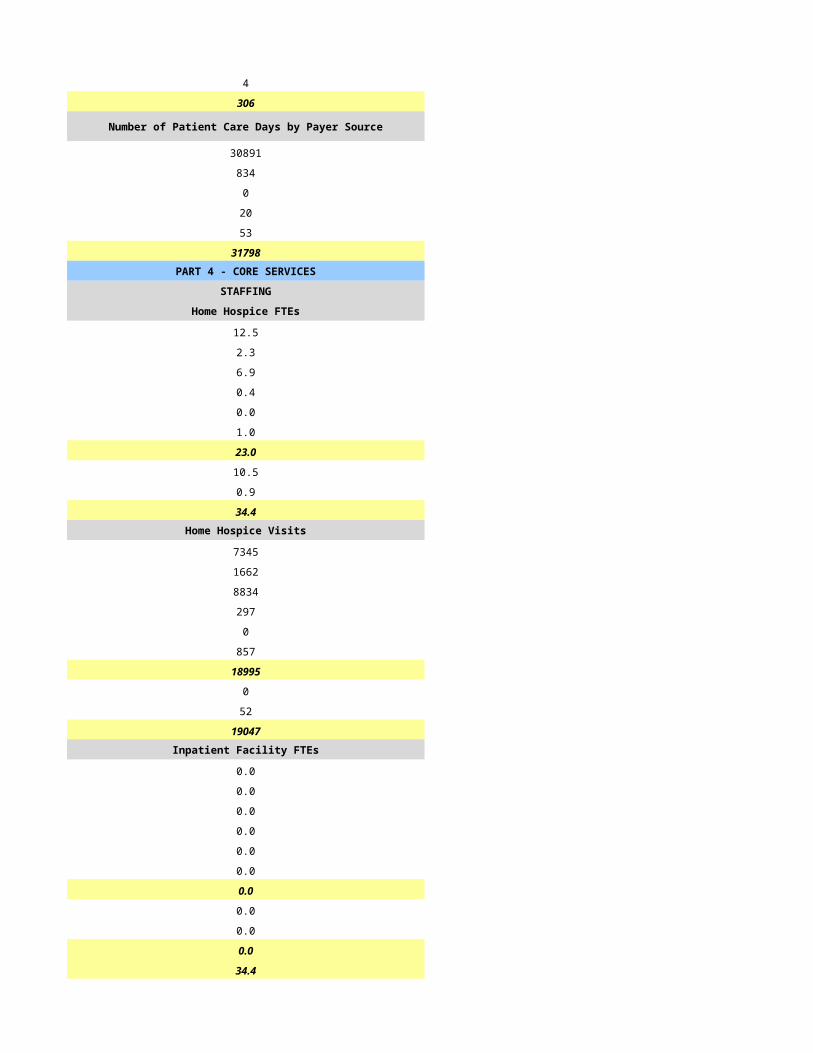
Total Number of Patient Care Days: 13471PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
Nursing: 7.0
Social Services: 5.0
Home Health Aides: 3.0
Paid Physicians: 1.0
Volunteer Physicians: 0.0
Other Clinical: 0.0
Clinical Total: 16.0
Non-Clinical: 2.0
Bereavement: 2.0
Total Home Hospice FTEs: 20.0Home Hospice Visits Home Hospice Visits
Nursing: 3403
Social Services: 1567
Home Health Aides: 2876
Paid Physicians: 9
Volunteer Physicians: 0
Other Clinical: 0
Clinical Total: 7855
Non-Clinical: 0
Bereavement: 278
Total Hospice Visits: 8133Inpatient Facility FTEs Inpatient Facility FTEs
Nursing: 0.0
Social Services: 0.0
Home Health Aides: 0.0
Paid Physicians: 0.0
Volunteer Physicians: 0.0
Other Clinical: 0.0
Clinical Total: 0.0
Non-Clinical: 0.0
Bereavement: 0.0
Inpatient Facility FTEs: 0.0
Agency Total FTEs: 20.0
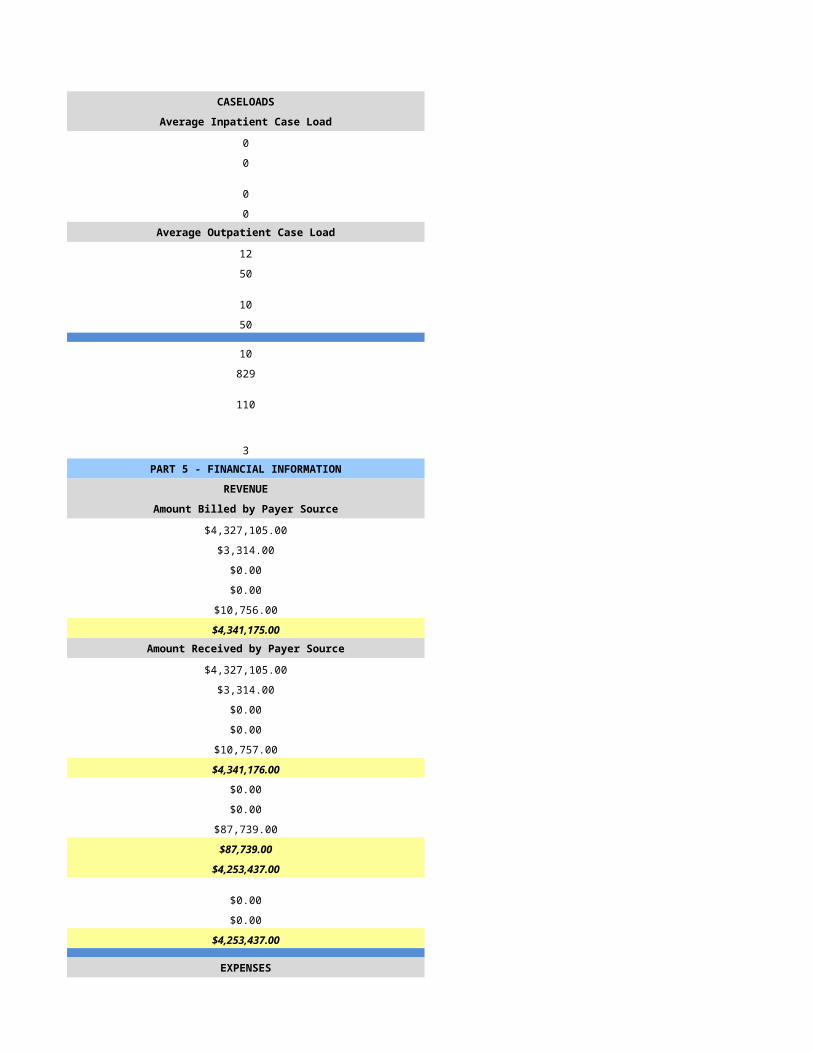
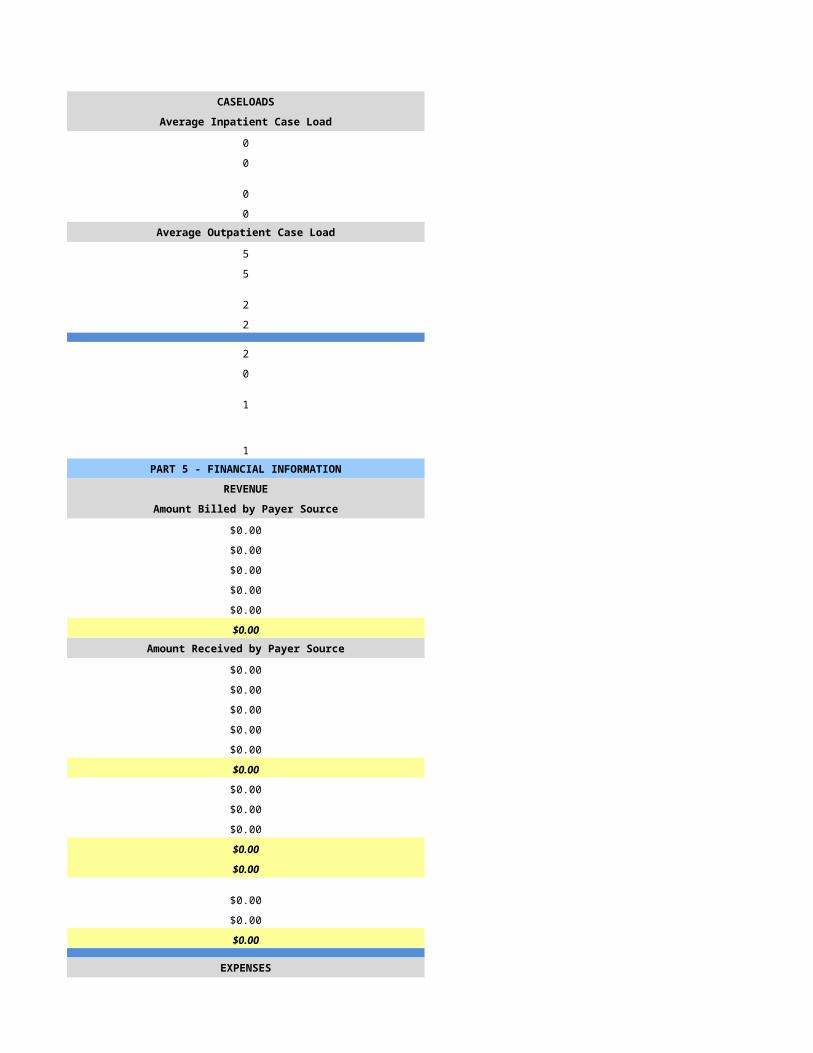
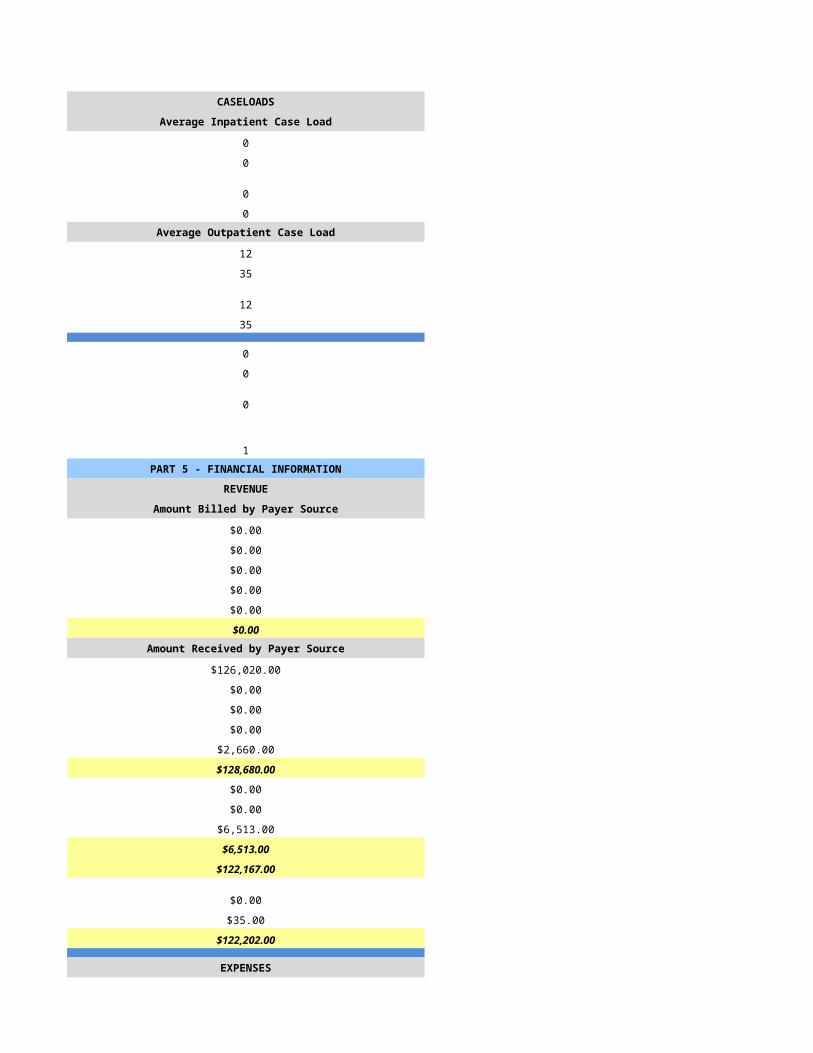
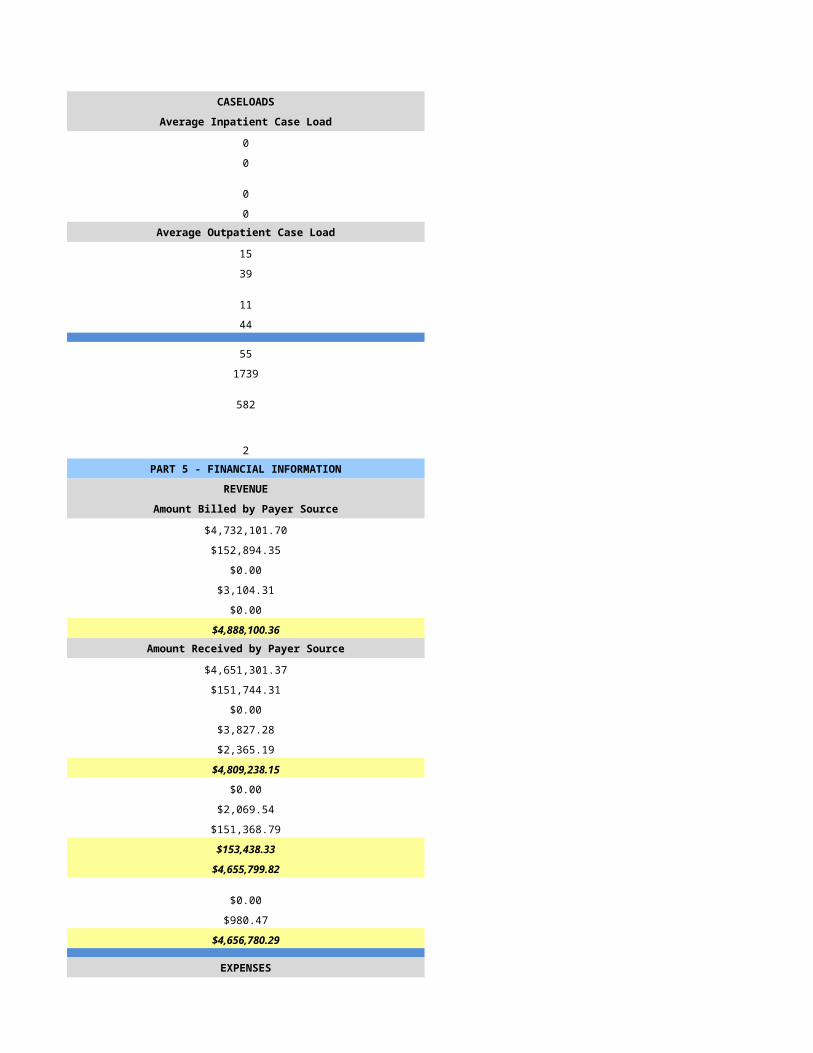
CASELOADS CASELOADS
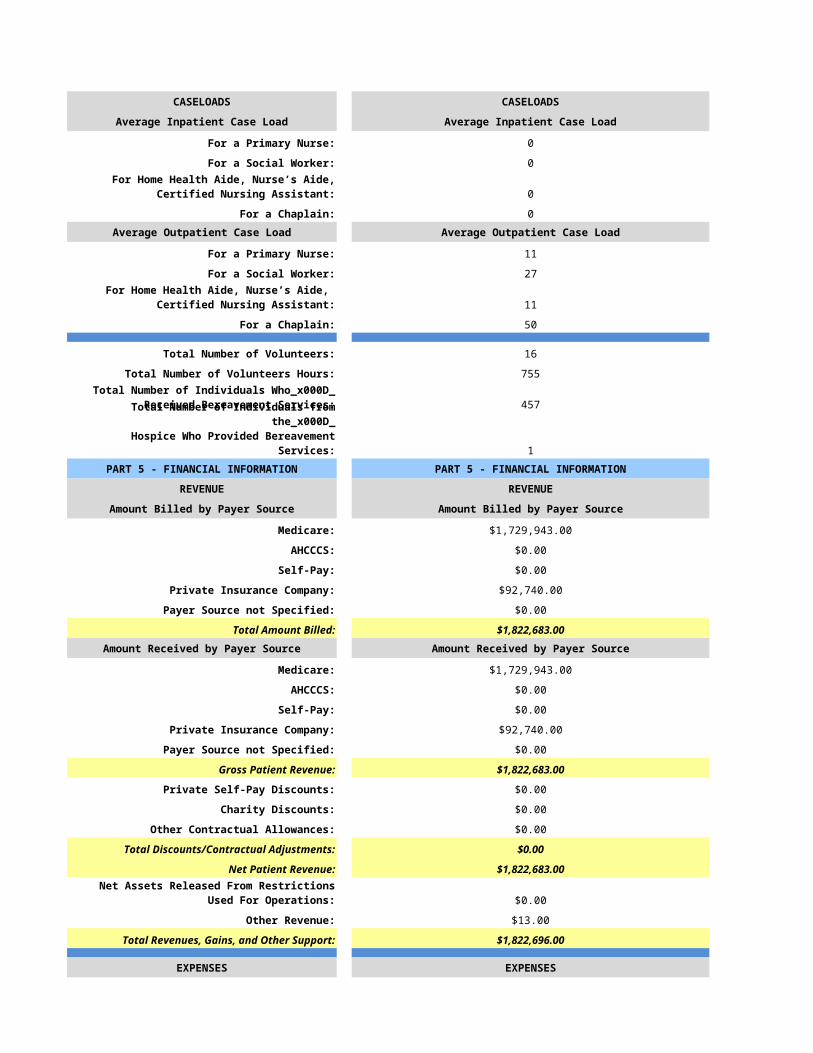
Average Inpatient Case Load Average Inpatient Case Load
For a Primary Nurse: 0
For a Social Worker: 0
0
For a Chaplain: 0Average Outpatient Case Load Average Outpatient Case Load
For a Primary Nurse: 11
For a Social Worker: 27
11
For a Chaplain: 50
Total Number of Volunteers: 16
Total Number of Volunteers Hours: 755
457
1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
Medicare: $1,729,943.00
AHCCCS: $0.00
Self-Pay: $0.00
Private Insurance Company: $92,740.00
Payer Source not Specified: $0.00
Total Amount Billed: $1,822,683.00Amount Received by Payer Source Amount Received by Payer Source
Medicare: $1,729,943.00
AHCCCS: $0.00
Self-Pay: $0.00
Private Insurance Company: $92,740.00
Payer Source not Specified: $0.00
Gross Patient Revenue: $1,822,683.00
Private Self-Pay Discounts: $0.00
Charity Discounts: $0.00
Other Contractual Allowances: $0.00
Total Discounts/Contractual Adjustments: $0.00
Net Patient Revenue: $1,822,683.00
$0.00
Other Revenue: $13.00
Total Revenues, Gains, and Other Support: $1,822,696.00
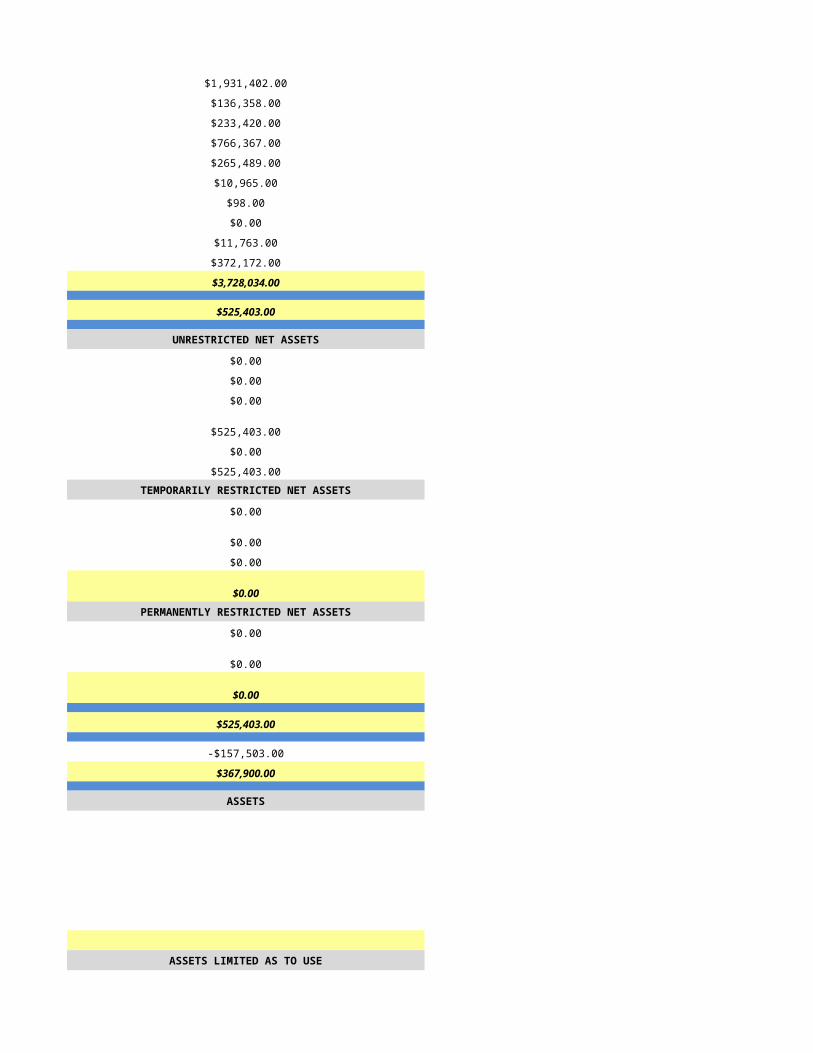
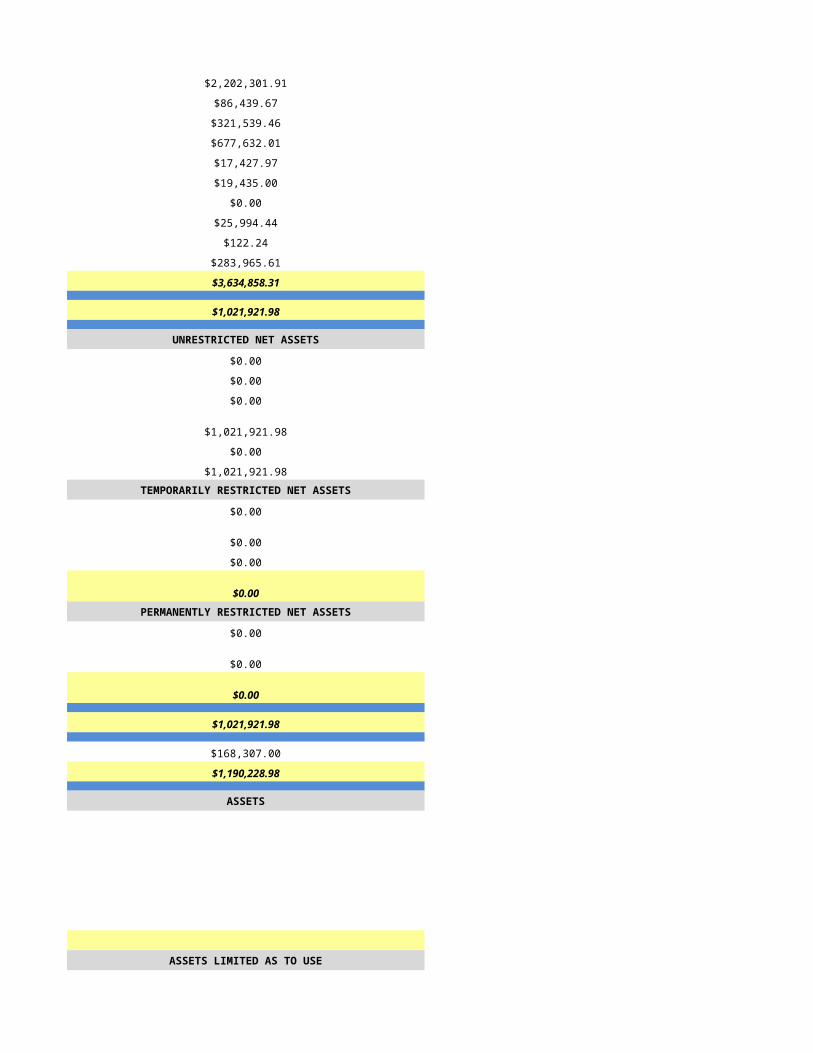
EXPENSES EXPENSES
FTE Salaries and Wages: $700,427.00
Contract or Registry Staff: $0.00
For Home Health Aide, Nurse’s Aide, Certified Nursing Assistant:
For Home Health Aide, Nurse’s Aide, Certified Nursing Assistant:
Total Number of Individuals Who Received Bereavement Services:
Total Number of Individuals from the Hospice Who Provided Bereavement Services:
Net Assets Released From Restrictions Used For Operations:
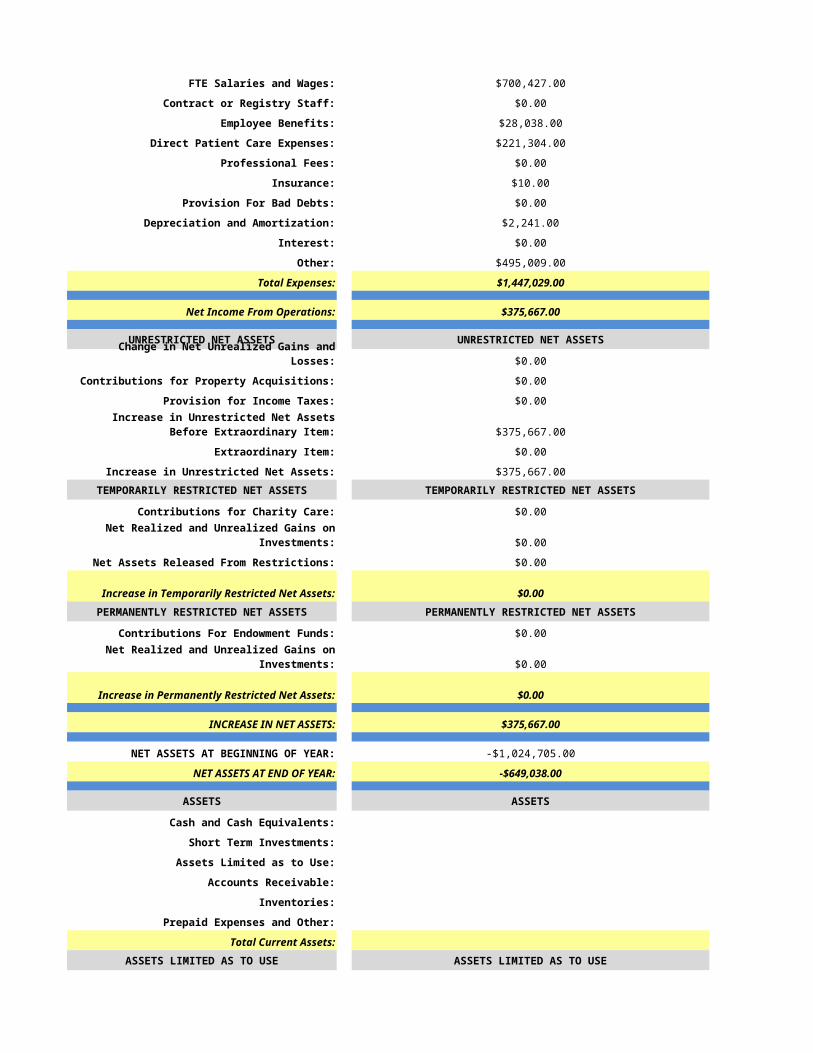
Employee Benefits: $28,038.00
Direct Patient Care Expenses: $221,304.00
Professional Fees: $0.00
Insurance: $10.00
Provision For Bad Debts: $0.00
Depreciation and Amortization: $2,241.00
Interest: $0.00
Other: $495,009.00
Total Expenses: $1,447,029.00
Net Income From Operations: $375,667.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
Change in Net Unrealized Gains and Losses: $0.00
Contributions for Property Acquisitions: $0.00
Provision for Income Taxes: $0.00
$375,667.00
Extraordinary Item: $0.00
Increase in Unrestricted Net Assets: $375,667.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
Contributions for Charity Care: $0.00
$0.00
Net Assets Released From Restrictions: $0.00
Increase in Temporarily Restricted Net Assets: $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
Contributions For Endowment Funds: $0.00
$0.00
Increase in Permanently Restricted Net Assets: $0.00
INCREASE IN NET ASSETS: $375,667.00
NET ASSETS AT BEGINNING OF YEAR: -$1,024,705.00
NET ASSETS AT END OF YEAR: -$649,038.00
ASSETS ASSETS
Cash and Cash Equivalents:
Short Term Investments:
Assets Limited as to Use:
Accounts Receivable:
Inventories:
Prepaid Expenses and Other:
Total Current Assets:ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
Internally Designated For Capital Acquisition:
Other Board Designated Funds:
Increase in Unrestricted Net Assets Before Extraordinary Item:
Net Realized and Unrealized Gains on Investments:
Net Realized and Unrealized Gains on Investments:
Held by Trustee:
Total Assets Limited As To Use:
Long Term Investments:
Property and Equipment, Net:
Other Assets:
TOTAL ASSETS:
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
Current Portion of Long Term Debt:
Accounts Payable and Accrued Expense:
Other:
Total Current Liabilities:
Long Term Debt Less Current Portion:
Other Liabilities:
Total Liabilities:
NET ASSETS NET ASSETS
Unrestricted:
Temporarily Restricted:
Permanently Restricted:
Total Net Assets:
TOTAL LIABILITIES AND NET ASSETS:
Comments:
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/2/2015 5/3/2015
HSPC-5697 HSPC-6340
Companion Hospice and Palliative Care of Mariposa Wings of Hope Hospice & Palliative Care
1930 South Alma Road, Suite D105 11811 N. Tatum Blvd
Mesa Phoenix
AZ AZ
85210 85028
Maricopa Maricopa
480-459-5552 602-971-0304
Susan Tschudy Angela Katz
480-459-5552 602-971-0304
[email protected] [email protected]
Chuck McCann Angela Katz
714-557-0883 602-971-0304
Cathy Storr, Axiom Healthcare Group
310-707-1945 Angela Katz
[email protected] [email protected]
814044
1851688253 1710312897
Yes YES
03-1608 31631
JCAHO CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Assisted Living - Based Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Primarily Urban Primarily Urban
Home Health-Based
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
307 5
267 5
110 0
85 0Number of Patient Care Days Number of Patient Care Days
24270 184
175 0
225 0
343 0
25013 0
Census Information Census Information
69 5
72 38
40 0
38 0
22 0
Gender Gender
181 4
121 1Age Age
0 0
0 0
18 0
35 0
72 4
177 1Race/Ethnicity Race/Ethnicity
2 0
1 0
5 0
21 0
0 0
273 5
0 0Number of Admissions by Source Number of Admissions by Source
171 2
101 3
64 0
19 0
0 0
355 5Number of Deaths by Location Number of Deaths by Location
66 1
10 0
32 0
2 0
0 0
110 1Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
32 0
120 2
60 2
103 1
8 0
7 0
2 0
1 0
17 0
5 0
0 0
355 5Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
4281 0
8787 70
6037 76
2514 38
217 0
570 0
3 0
91 0
0 0
2513 0
0 0
25013 184Number of Admissions by Payer Source Number of Admissions by Payer Source
261 5
1 0
0 0
11 0
82 0
355 5
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
24291 184
20 0
0 0
66 0
636 0
25013 184PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
16.0 2.0
2.0 1.0
13.0 1.0
2.0 0.0
0.0 1.0
2.0 0.0
35.0 5.0
0.0 3.0
0.0 1.0
35.0 9.0Home Hospice Visits Home Hospice Visits
6269 35
946 6
7864 13
62 0
0 0
822 0
15963 54
0 0
65 3
16028 57Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
35.0 0.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
12 5
50 5
10 2
50 2
10 2
829 0
110 1
3 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$4,327,105.00 $0.00
$3,314.00 $0.00
$0.00 $0.00
$0.00 $0.00
$10,756.00 $0.00
$4,341,175.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$4,327,105.00 $0.00
$3,314.00 $0.00
$0.00 $0.00
$0.00 $0.00
$10,757.00 $0.00
$4,341,176.00 $0.00
$0.00 $0.00
$0.00 $0.00
$87,739.00 $0.00
$87,739.00 $0.00
$4,253,437.00 $0.00
$0.00 $0.00
$0.00 $0.00
$4,253,437.00 $0.00
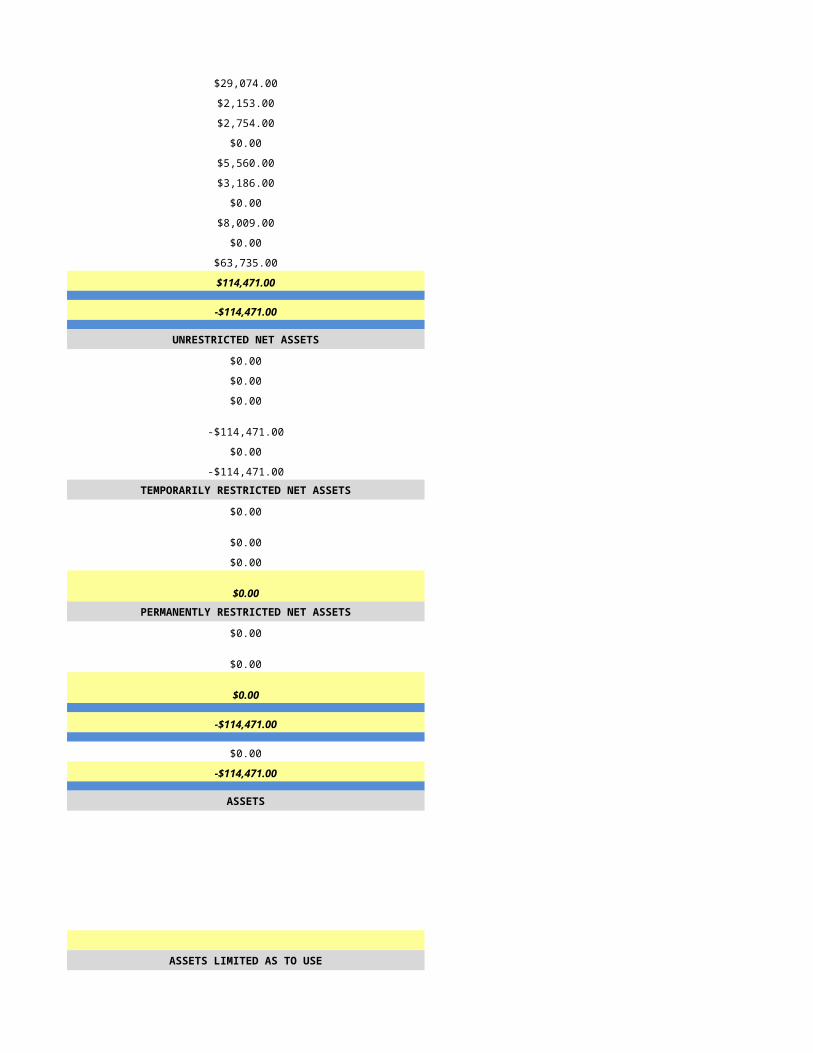
EXPENSES EXPENSES
$1,931,402.00 $29,074.00
$136,358.00 $2,153.00
$233,420.00 $2,754.00
$766,367.00 $0.00
$265,489.00 $5,560.00
$10,965.00 $3,186.00
$98.00 $0.00
$0.00 $8,009.00
$11,763.00 $0.00
$372,172.00 $63,735.00
$3,728,034.00 $114,471.00
$525,403.00 -$114,471.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$525,403.00 -$114,471.00
$0.00 $0.00
$525,403.00 -$114,471.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$525,403.00 -$114,471.00
-$157,503.00 $0.00
$367,900.00 -$114,471.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/4/2015 5/5/2015
HSPC-3739 HSPC-3847
Valor HospiceCare, LLC
Affinity Hospice of Life
1860 E. River Road, Suite 200 1661 E Camelback Road, Ste 350
tucson Phoenix
AZ AZ
85718-5836 85016
Pima Maricopa
3001 Keith St NW
Cleveland
TN
37312
Bradley
(520) 615-3996 423-473-5264
Grant Rowe
(520) 615-3996
Grant Rowe
(520) 615-3996
Courtney Carlton
(520) 615-3996 423-473-5264
965022 138621
1578569430 1538124938
Yes Yes
31562 03-1566
Not Accredited ADHC
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Primarily Urban
Free Standing Free Standing
NA
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Valor HospiceCare, LLC
HSPC-3739
1131 S. La Canada Dr, Suite 103
Green Valley
85614-1944
Pima
(520) 339-0200
Mixed Urban and Rural Primarily Urban
Free Standing
NA
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
172 18
104 8
78 6
29 16Number of Patient Care Days Number of Patient Care Days
8832 758
24 10
0 0
6 4
8862 772
Census Information Census Information
24 9
93 98
35 52
19 1
2 0
Gender Gender
62 3
66 5Age Age
0 0
0 0
4 1
16 1
33 4
75 2Race/Ethnicity Race/Ethnicity
0 0
0 0
3 0
18 0
1 0
106 7
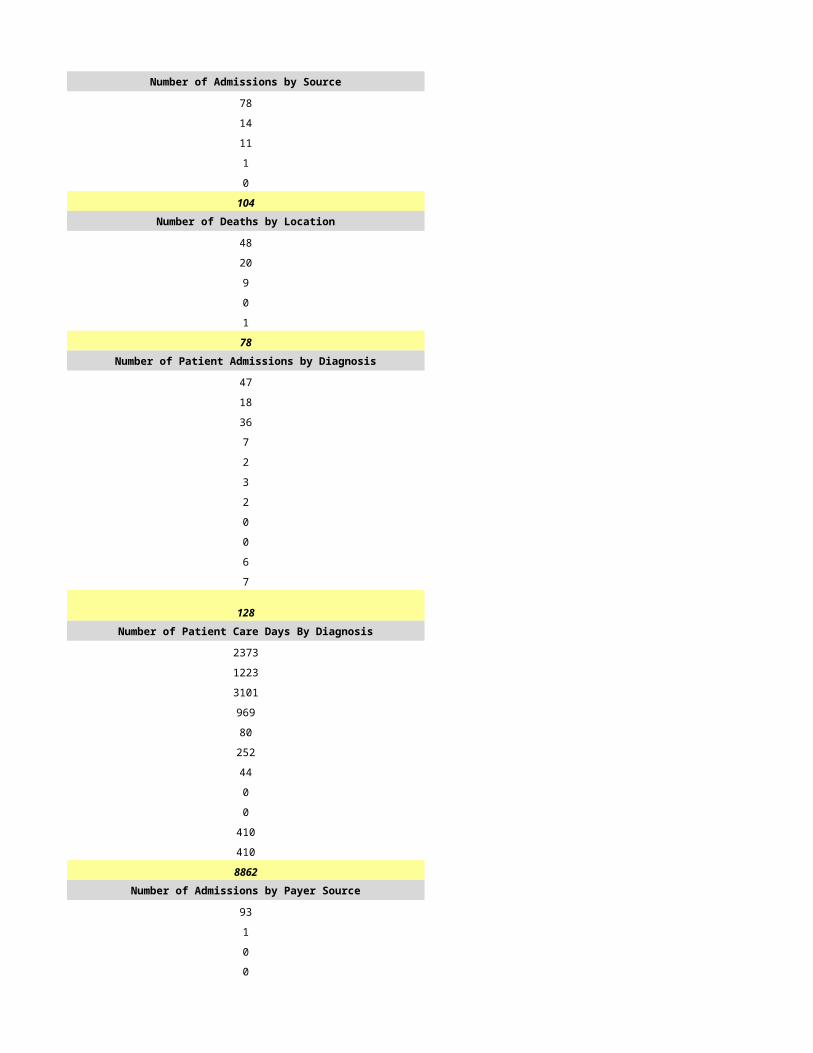
0 1Number of Admissions by Source Number of Admissions by Source
78 6
14 1
11 1
1 0
0 0
104 8Number of Deaths by Location Number of Deaths by Location
48 4
20 1
9 1
0 0
1 0
78 6Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
47 0
18 4
36 3
7 0
2 0
3 0
2 0
0 0
0 1
6 0
7 0
128 8Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2373 118
1223 314
3101 226
969 90
80 0
252 0
44 0
0 0
0 24
410 0
410 0
8862 772Number of Admissions by Payer Source Number of Admissions by Payer Source
93 8
1 0
0 0
0 0
10 0
104 8
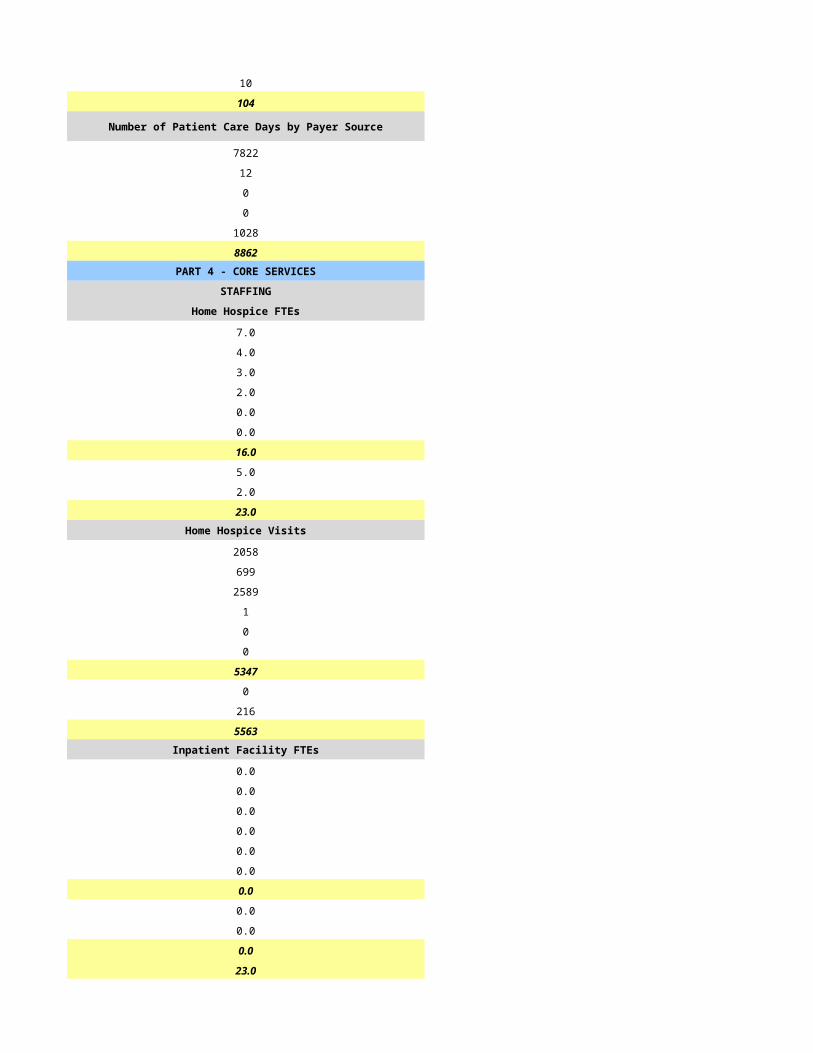
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
7822 758
12 0
0 0
0 14
1028 0
8862 772PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
7.0 1.7
4.0 0.8
3.0 1.4
2.0 0.0
0.0 0.0
0.0 0.0
16.0 4.0
5.0 3.6
2.0 0.6
23.0 8.0Home Hospice Visits Home Hospice Visits
2058 243
699 43
2589 309
1 0
0 0
0 4
5347 599
0 0
216 50
5563 649Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
23.0 8.0
CASELOADS CASELOADS
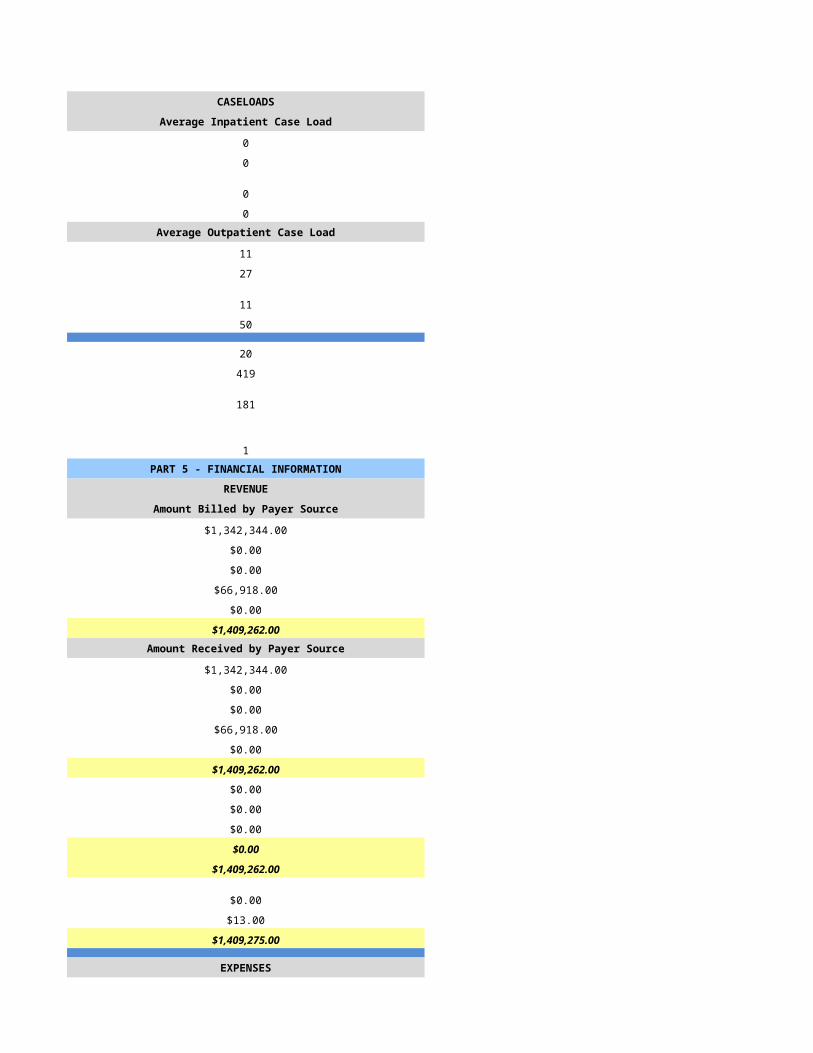
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
11 12
27 35
11 12
50 35
20 0
419 0
181 0
1 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,342,344.00 $0.00
$0.00 $0.00
$0.00 $0.00
$66,918.00 $0.00
$0.00 $0.00
$1,409,262.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$1,342,344.00 $126,020.00
$0.00 $0.00
$0.00 $0.00
$66,918.00 $0.00
$0.00 $2,660.00
$1,409,262.00 $128,680.00
$0.00 $0.00
$0.00 $0.00
$0.00 $6,513.00
$0.00 $6,513.00
$1,409,262.00 $122,167.00
$0.00 $0.00
$13.00 $35.00
$1,409,275.00 $122,202.00
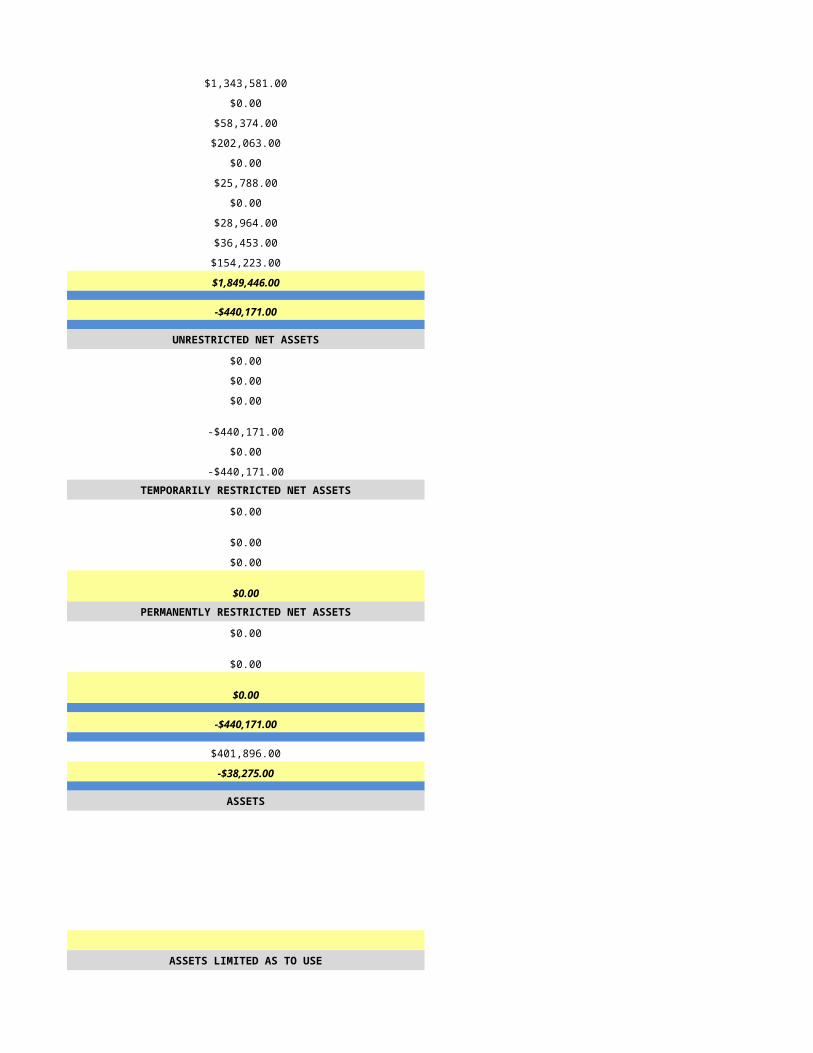
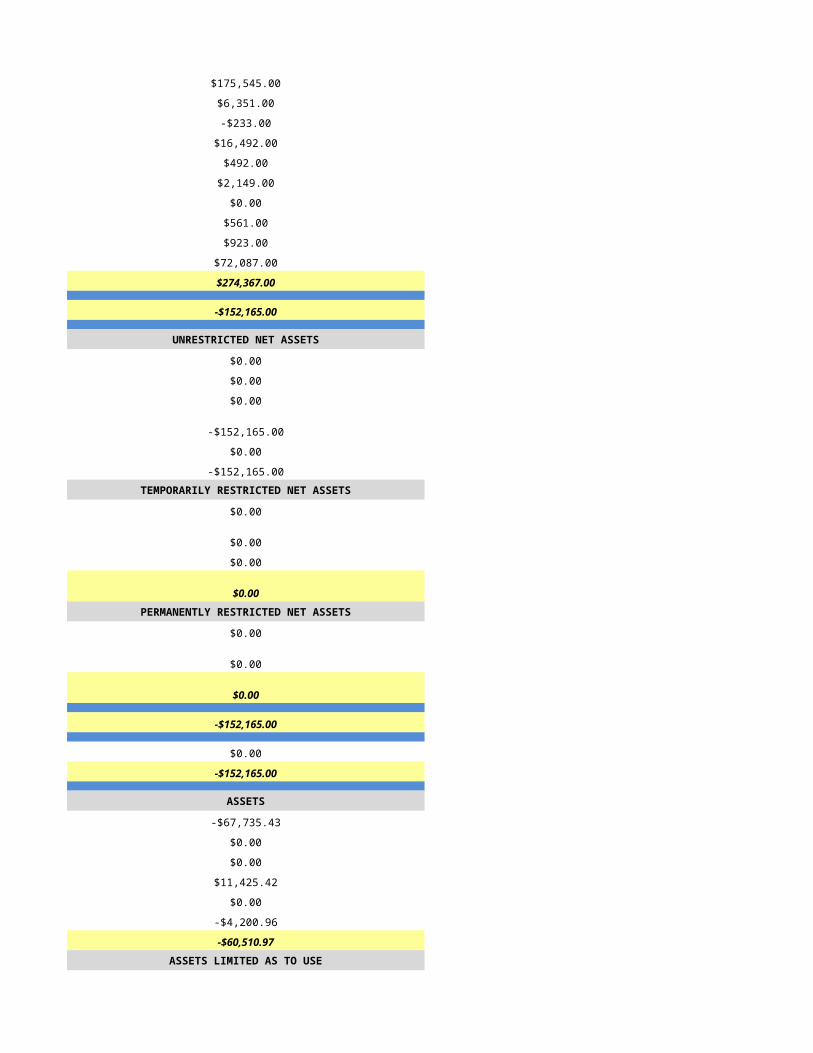
EXPENSES EXPENSES
$1,343,581.00 $175,545.00
$0.00 $6,351.00
$58,374.00 -$233.00
$202,063.00 $16,492.00
$0.00 $492.00
$25,788.00 $2,149.00
$0.00 $0.00
$28,964.00 $561.00
$36,453.00 $923.00
$154,223.00 $72,087.00
$1,849,446.00 $274,367.00
-$440,171.00 -$152,165.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$440,171.00 -$152,165.00
$0.00 $0.00
-$440,171.00 -$152,165.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$440,171.00 -$152,165.00
$401,896.00 $0.00
-$38,275.00 -$152,165.00
ASSETS ASSETS
-$67,735.43
$0.00
$0.00
$11,425.42
$0.00
-$4,200.96
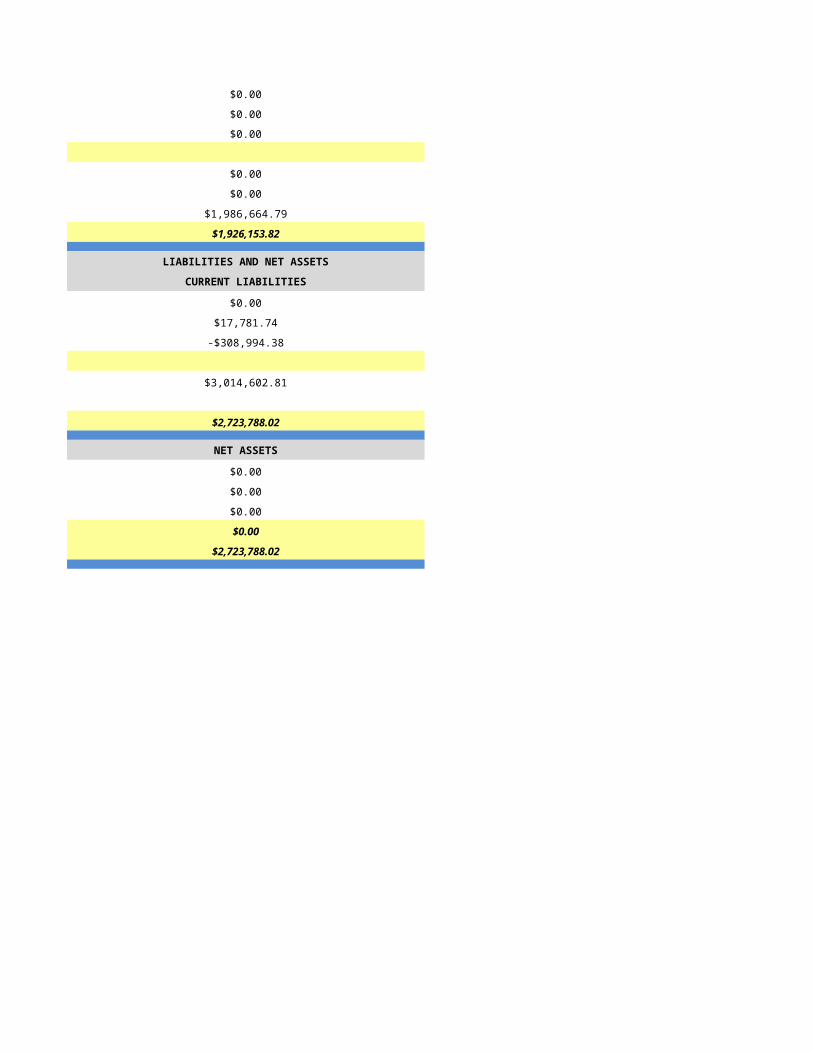
-$60,510.97ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$1,986,664.79
$1,926,153.82
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$17,781.74
-$308,994.38
$3,014,602.81
$2,723,788.02
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$2,723,788.02
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/7/2015 5/9/2015
HSPC-7131 HSPC-3710
Agape Hospice and Palliative Care LLC Villa Alba Corporation
Agape Hospice & Palliative Care Americare Hospice and Palliative Care
2980 N. Swan Rd. Ste. 222 1212 N. Spencer Street, Ste 2
Tucson Mesa
AZ AZ
85712 85203
Pima Maricopa
(520) 207-5817 (480) 726-7773
April Rosa Christine Minch
520-207-5817 (480) 726-7773
[email protected] [email protected]
Samuel Burns Angelina Saguid
520-207-5817 (480) 726-7773
[email protected] [email protected]
Samuel Burns Christine Minch
520-207-5817 (480) 726-7773
[email protected] [email protected]
853014 none
1679826549 1679558050
Yes Yes
03-1614 03-1563
JCAHO Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
0 n/a
1/1/2014 1/1/2014
12/31/2014 12/31/2014
The Villa
HSPC 5156
1103 S Mesa Drive
Mesa
85210
Maricopa
PO Box 0790
Mesa
85203
Maricopa
(480) 292-7205
mm/dd/yyyy
Primarily Urban Primarily Urban
Free Standing
0 n/a
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 6
0 0
0 0
0 6
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 6
0 0
0 0
0 6
0 4PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
389 425
306 377
237 216
57 108Number of Patient Care Days Number of Patient Care Days
31726 34010
18 388
0 0
54 295
31798 34693
Census Information Census Information
87 95
94 78
31 32
62 59
33 34693
Gender Gender
189 219
117 158Age Age
0 0
1 0
12 27
28 70
76 124
189 156Race/Ethnicity Race/Ethnicity
0 2
1 7
6 7
41 20
0 1
204 212
54 128Number of Admissions by Source Number of Admissions by Source
59 237
201 50
43 30
1 0
2 60
306 377Number of Deaths by Location Number of Deaths by Location
48 80
142 66
43 22
0 0
4 48
237 216Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
38 79
64 56
118 92
23 38
5 7
17 11
2 14
0 0
17 21
22 26
0 33
306 377Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2316 5147
7544 7046
13429 10589
2656 3540
727 494
1824 930
273 604
0 0
1648 1593
1378 379
3 4371
31798 34693Number of Admissions by Payer Source Number of Admissions by Payer Source
290 355
9 0
0 0
3 8
4 14
306 377
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
30891 33728
834 0
0 0
20 400
53 565
31798 34693PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
12.5 8.0
2.3 3.0
6.9 8.0
0.4 1.0
0.0 0.0
1.0 2.0
23.0 22.0
10.5 10.0
0.9 1.0
34.4 33.0Home Hospice Visits Home Hospice Visits
7345 6790
1662 1640
8834 11912
297 430
0 0
857 870
18995 21642
0 558
52 274
19047 22474Inpatient Facility FTEs Inpatient Facility FTEs
0.0 6.0
0.0 0.5
0.0 6.0
0.0 0.5
0.0 0.0
0.0 0.5
0.0 13.5
0.0 1.0
0.0 0.5
0.0 15.0
34.4 48.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 4
0 1
0 4
0 1Average Outpatient Case Load Average Outpatient Case Load
15 16
39 40
11 16
44 40
55 67
1739 1630
582 240
2 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$4,732,101.70 $5,590,366.66
$152,894.35 $0.00
$0.00 $0.00
$3,104.31 $0.00
$0.00 $336,465.00
$4,888,100.36 $5,926,831.66Amount Received by Payer Source Amount Received by Payer Source
$4,651,301.37 $5,704,303.72
$151,744.31 $0.00
$0.00 $0.00
$3,827.28 $0.00
$2,365.19 $336,465.00
$4,809,238.15 $6,040,768.72
$0.00 $0.00
$2,069.54 $0.00
$151,368.79 $113,937.06
$153,438.33 $113,937.06
$4,655,799.82 $5,926,831.66
$0.00 $0.00
$980.47 $0.00
$4,656,780.29 $5,926,831.66
EXPENSES EXPENSES
$2,202,301.91 $1,643,681.95
$86,439.67 $0.00
$321,539.46 $131,708.31
$677,632.01 $2,701,608.28
$17,427.97 $210,900.49
$19,435.00 $49,861.16
$0.00 $0.00
$25,994.44 $26,793.88
$122.24 $56,353.67
$283,965.61 $1,049,622.52
$3,634,858.31 $5,870,530.26
$1,021,921.98 $56,301.40
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,021,921.98 $56,301.40
$0.00 $0.00
$1,021,921.98 $56,301.40TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,021,921.98 $56,301.40
$168,307.00 $0.00
$1,190,228.98 $56,301.40
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
Had low Workers Comp. Ins. rate quoted for 2014; paid large adjustment in 2015.
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/10/2015 5/11/2015
HSPC-4800 HSPC-5120
New Hope Hospice of Arizona, Inc New Hope Hospice of Bullhead City
Beacon of Hope Hospice Beacon of Hope Hospice
500 N. Lake Havasu Ave, Ste B106 3550 North Lane, Suite 102
Lake Havasu City Bullhead City
AZ AZ
86403 86422
Mohave Mohave
2191 Lemay Ferry Road, Ste 300 2191 Lemay Ferry Road, Suite 300
St. Louis St. Louis
MO MO
63125 63125
St. Louis St. Louis
(314) 815-3500 (314) 815-3500
Devin Bell Julie Horton
(928) 854-4200 (928) 444-8122
[email protected] [email protected]
Tim Mohan Tim Mohan
(314) 815-3418 (314) 815-3418
[email protected] [email protected]
Tim Mohan Tim Mohan
(314) 815-3418 (314) 815-3418
[email protected] [email protected]
801275 801366
1699709857 1437435708
Yes Yes
03-1607 03-1610
Other Other
ACHC ACHC
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Primarily Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Primarily Rural Primarily Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
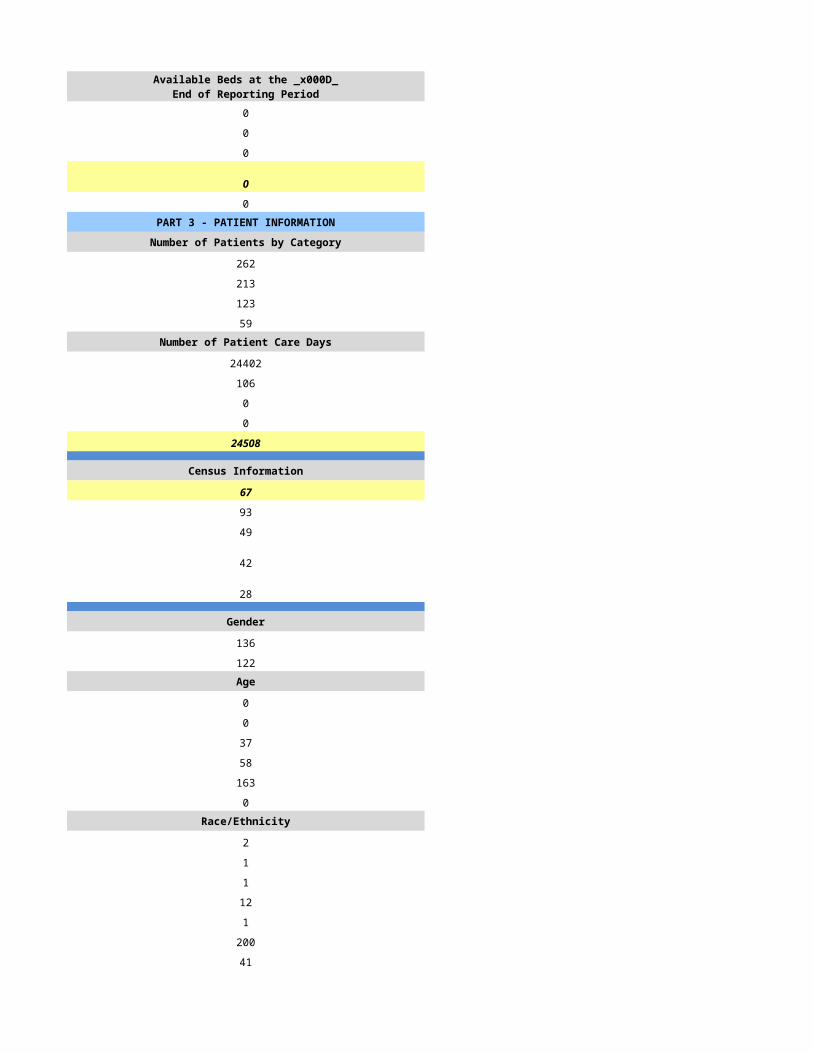
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
267 262
236 213
161 123
61 59Number of Patient Care Days Number of Patient Care Days
21971 24402
33 106
0 0
35 0
22039 24508
Census Information Census Information
60 67
79 93
45 49
45 42
24 28
Gender Gender
124 136
143 122Age Age
0 0
0 0
29 37
50 58
188 163
0 0Race/Ethnicity Race/Ethnicity
2 2
0 1
0 1
6 12
2 1
224 200
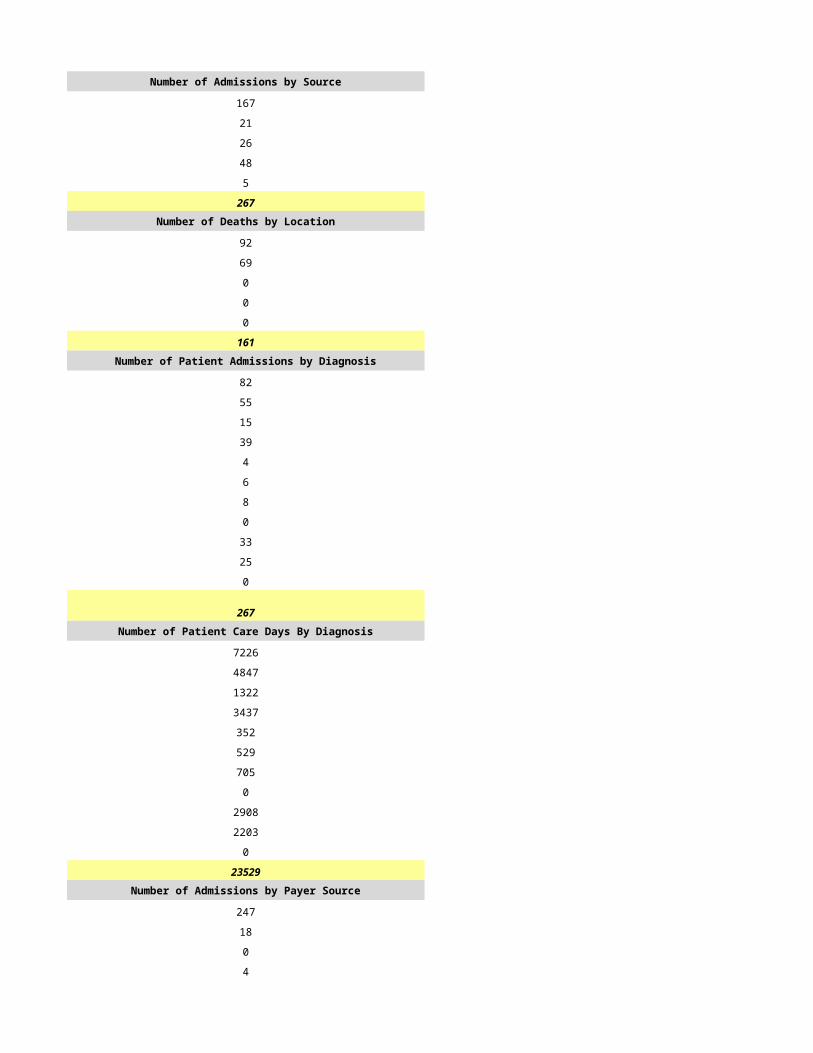
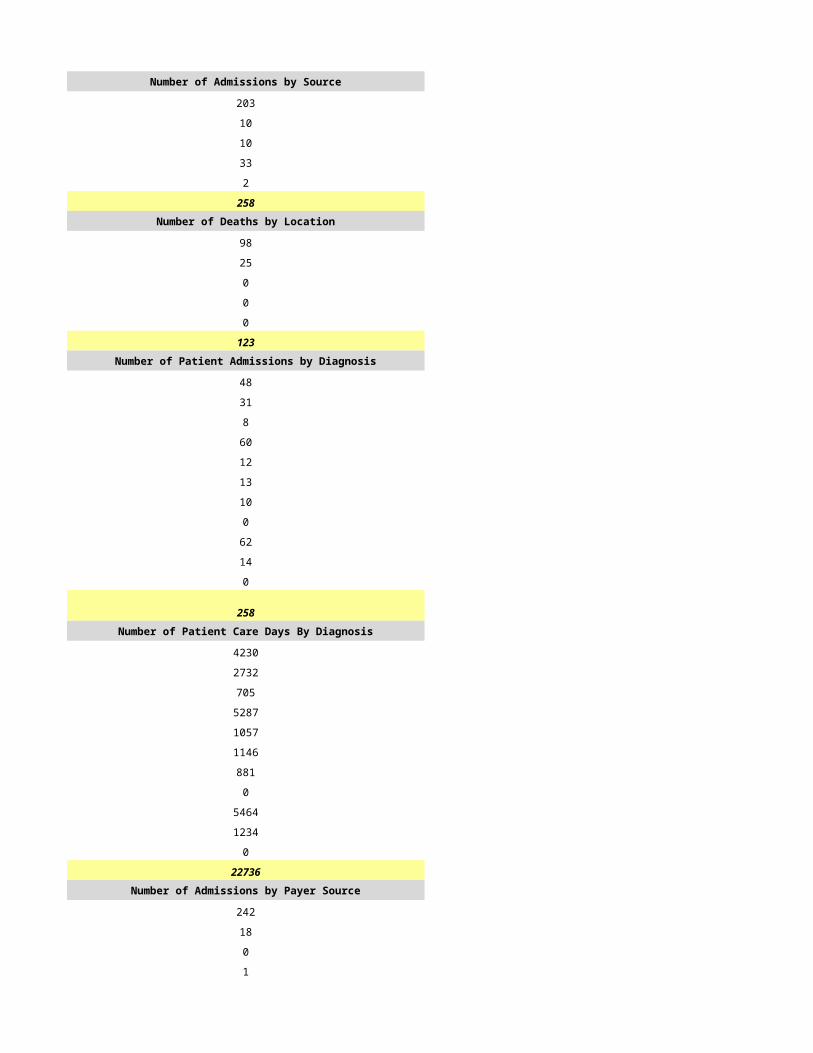
35 41Number of Admissions by Source Number of Admissions by Source
167 203

21 10
26 10
48 33
5 2
267 258Number of Deaths by Location Number of Deaths by Location
92 98
69 25
0 0
0 0
0 0
161 123Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
82 48
55 31
15 8
39 60
4 12
6 13
8 10
0 0
33 62
25 14
0 0
267 258Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
7226 4230
4847 2732
1322 705
3437 5287
352 1057
529 1146
705 881
0 0
2908 5464
2203 1234
0 0
23529 22736Number of Admissions by Payer Source Number of Admissions by Payer Source
247 242
18 18
0 0
4 1
0 0
269 261
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
21587 21150
1573 1573
0 0
350 87
0 0
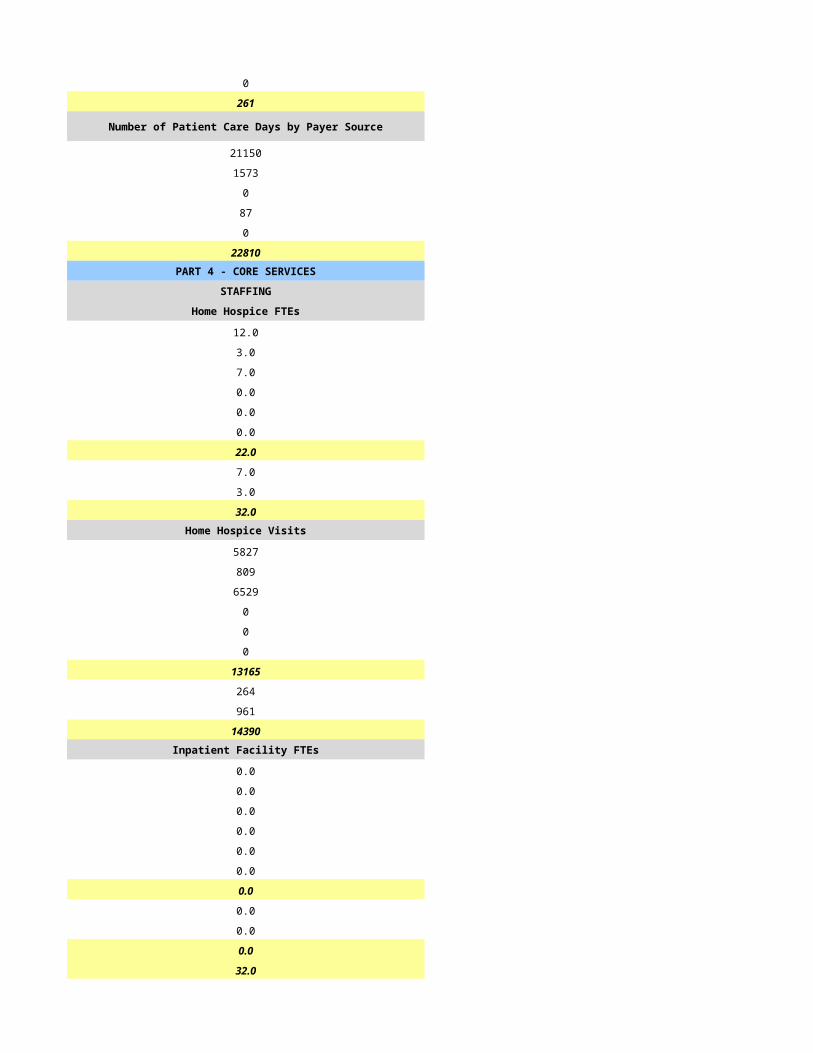
23510 22810PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
14.0 12.0
3.0 3.0
5.0 7.0
0.0 0.0
0.0 0.0
0.0 0.0
22.0 22.0
6.0 7.0
2.0 3.0
30.0 32.0Home Hospice Visits Home Hospice Visits
7328 5827
870 809
5476 6529
0 0
0 0
0 0
13674 13165
432 264
1440 961
15546 14390Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
30.0 32.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 0
0 0
0 0
0 0
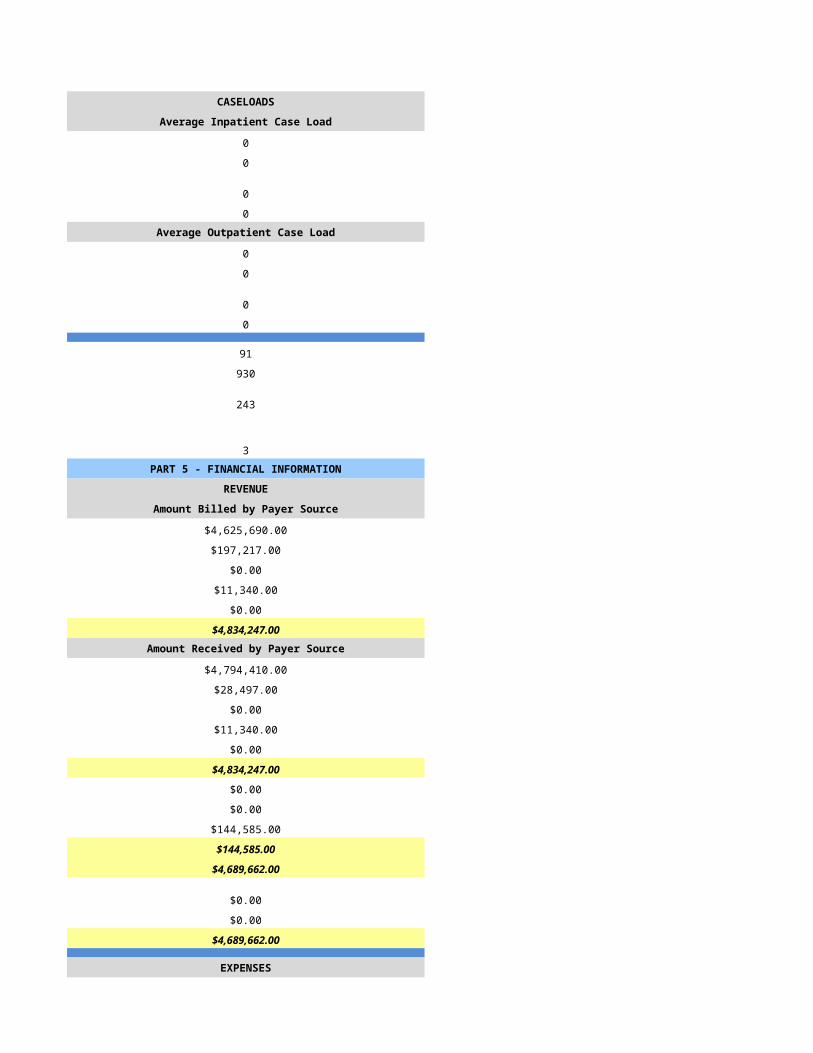
84 91
669 930
304 243
2 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,304,631.00 $4,625,690.00
$124,796.00 $197,217.00
$0.00 $0.00
$0.00 $11,340.00
$0.00 $0.00
$3,429,427.00 $4,834,247.00Amount Received by Payer Source Amount Received by Payer Source
$3,168,926.00 $4,794,410.00
$260,501.00 $28,497.00
$0.00 $0.00
$0.00 $11,340.00
$0.00 $0.00
$3,429,427.00 $4,834,247.00
$0.00 $0.00
$0.00 $0.00
$66,831.00 $144,585.00
$66,831.00 $144,585.00
$3,362,596.00 $4,689,662.00
$0.00 $0.00
$0.00 $0.00
$3,362,596.00 $4,689,662.00
EXPENSES EXPENSES
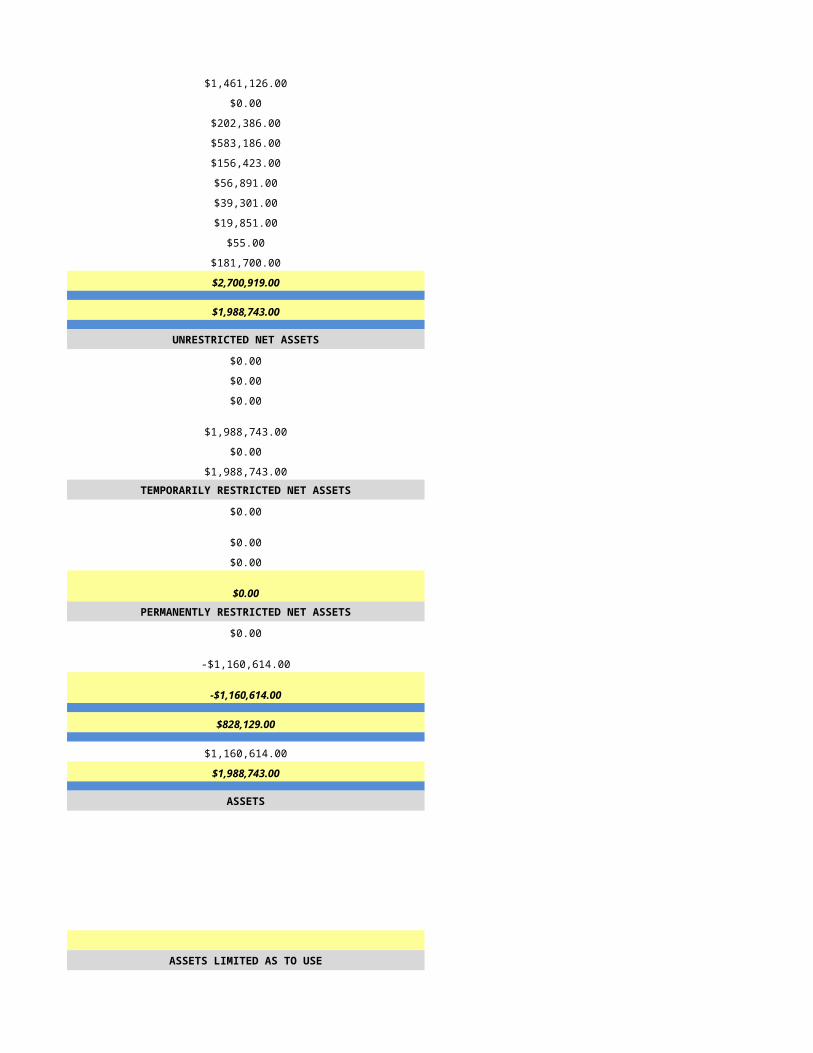
$1,201,548.00 $1,461,126.00
$0.00 $0.00
$166,062.00 $202,386.00
$366,361.00 $583,186.00
$171,855.00 $156,423.00
$34,529.00 $56,891.00
$65,492.00 $39,301.00
$18,088.00 $19,851.00
$0.00 $55.00
$124,126.00 $181,700.00
$2,148,061.00 $2,700,919.00
$1,214,535.00 $1,988,743.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,214,535.00 $1,988,743.00
$0.00 $0.00
$1,214,535.00 $1,988,743.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
-$911,353.00 $0.00
-$911,353.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 -$1,160,614.00
$0.00 -$1,160,614.00
$303,182.00 $828,129.00
$911,353.00 $1,160,614.00
$1,214,535.00 $1,988,743.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/12/2015 5/13/2015
HSPC-4987 HSPC-6544
ARC Therapy Services, LLC Community Hospice Group, LLC
Brookdale Hospice Chandler Canyon River Community Hospice
2545 W. Frye Rd, Ste 10B 2050Willow Creek Road
Chandler Prescott
AZ AZ
85224 86301
Maricopa Yavapai
111 Westwood Place, Ste 400 450 North Dobson, Suite 108
Brentwood Mesa
TN AZ
37027 85201
Williamson Maricopa
480-361-5645 480-456-9300
Lisa Morrison Richard Bass
480-361-5645 480-456-9300
[email protected] [email protected]
Mark Ohlendorf Karen Monville
414-918-5000 480-456-9300
[email protected] [email protected]
Julie A. McGlasson Ramsey David Badre
615-564-8034 912-634-9197
[email protected] [email protected]
429014
1922317742 1952578957
Yes Yes
03-1618 03-1582
CHAP Not Accredited
None
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Primarily Urban Primarily Urban
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
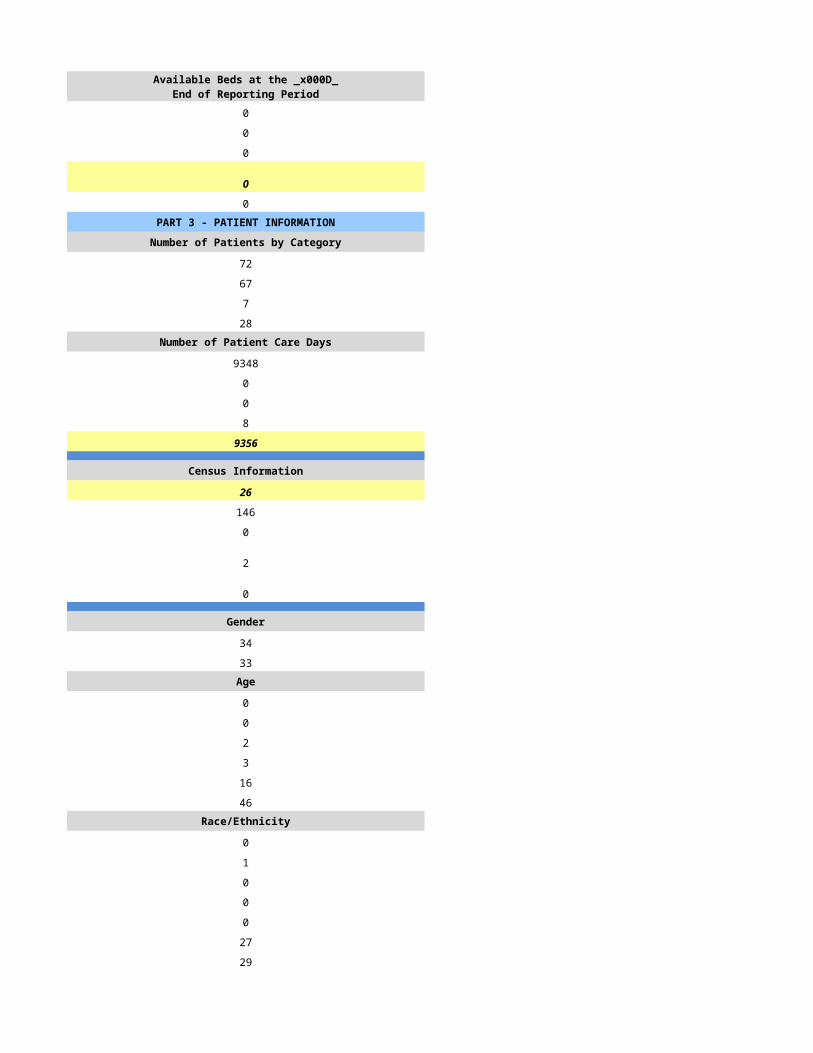
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
72 109
67 78
7 46
28 17Number of Patient Care Days Number of Patient Care Days
9348 1792
0 47
0 0
8 109
9356 1948
Census Information Census Information
26 5
146 24
0 10
2 22
0 0
Gender Gender
34 28
33 18Age Age
0 0
0 0
2 9
3 17
16 29
46 23Race/Ethnicity Race/Ethnicity
0 1
1 0
0 0
0 3
0 0
27 68
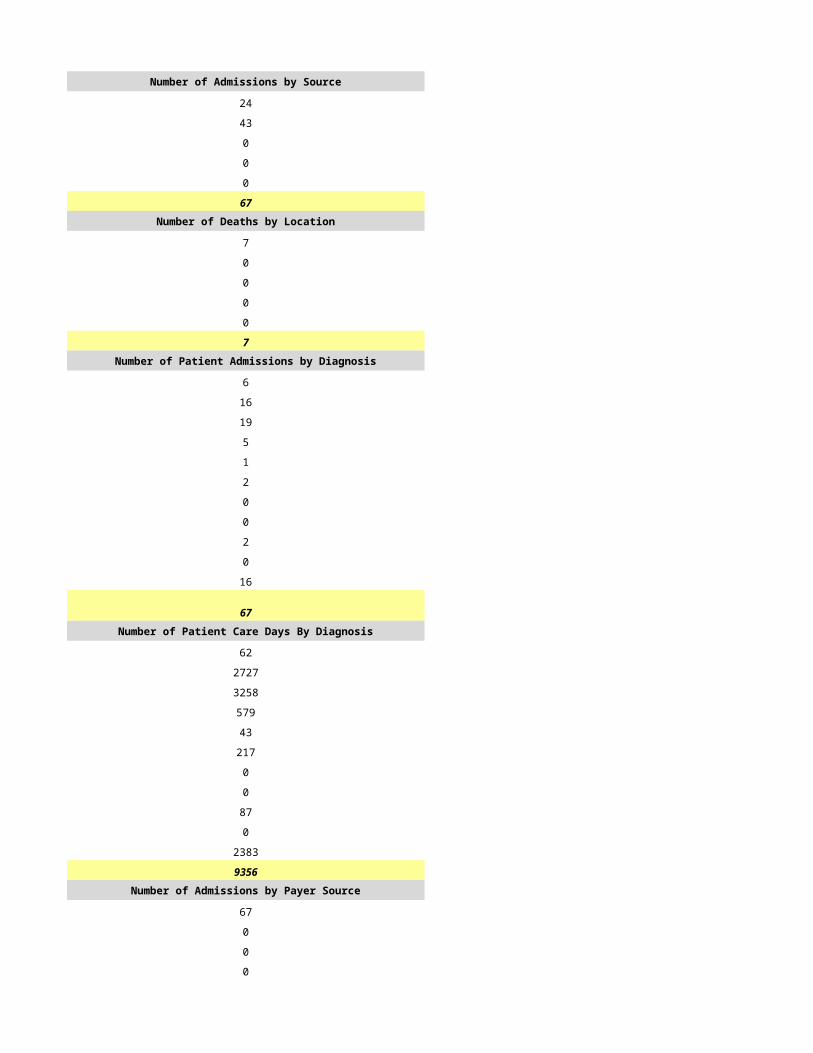
29 6Number of Admissions by Source Number of Admissions by Source
24 36
43 10
0 6
0 0
0 26
67 78Number of Deaths by Location Number of Deaths by Location
7 16
0 2
0 3
0 0
0 25
7 46Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
6 27
16 15
19 8
5 12
1 4
2 4
0 3
0 0
2 3
0 3
16 0
67 79Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
62 636
2727 323
3258 287
579 222
43 96
217 27
0 19
0 0
87 244
0 94
2383 0
9356 1948Number of Admissions by Payer Source Number of Admissions by Payer Source
67 72
0 2
0 0
0 0
0 5
67 79
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
9356 1887
0 12
0 0
0 0
0 49
9356 1948PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
4.5 2.0
1.5 1.0
1.1 2.0
0.0 0.0
0.0 0.0
0.0 0.0
7.1 5.0
2.0 1.0
0.0 0.3
9.1 6.3Home Hospice Visits Home Hospice Visits
2479 281
396 210
2432 389
0 0
0 0
86 0
5393 880
562 0
0 360
5955 1240Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
9.1 6.3
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
12 5
36 5
12 5
36 3
3 3
250 75
16 29
0 4PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,618,600.00 $600,270.00
$0.00 $5,543.00
$0.00 $0.00
$0.00 $0.00
$0.00 $15,489.00
$1,618,600.00 $621,302.00Amount Received by Payer Source Amount Received by Payer Source
$1,618,600.00 $367,860.00
$0.00 $5,543.00
$0.00 $0.00
$0.00 $0.00
$0.00 $15,489.00
$1,618,600.00 $388,892.00
$0.00 $0.00
$0.00 $0.00
$129,009.00 $0.00
$129,009.00 $0.00
$1,489,591.00 $388,892.00
$0.00 $0.00
$0.00 $0.00
$1,489,591.00 $388,892.00
EXPENSES EXPENSES
$815,627.00 $189,062.00
$0.00 $6,258.00
$42,583.00 $25,811.00
$218,085.00 $127,759.00
$45,950.00 $28,673.00
$0.00 $2,524.00
$29,792.00 $0.00
$0.00 $1,606.00
$0.00 $0.00
$175,918.00 $214,087.00
$1,327,955.00 $595,780.00
$161,636.00 -$206,888.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$161,636.00 -$206,888.00
$0.00 $0.00
$161,636.00 -$206,888.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$161,636.00 -$206,888.00
$0.00 $0.00
$161,636.00 -$206,888.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/14/2015 5/15/2015
HSPC-4766 HSPC-2206
Casa de la Luz LLC
CARONDELET HOSPICE AND PALLIATIVE CARE Casa de la Luz Hospice
1802 WEST ST MARYS STREET 7740 N. Oracle Road
TUCSON Tucson
AZ AZ
85745 85704
PIMA Pima
(520) 205-7700 520-544-9890
Nancy Epperson Callene Bentoncoury
(520) 205-7562 520-544-9890
[email protected] [email protected]
Joel Bojorquez Ken M. Winchester
520-872-7308 520-544.9890
[email protected] [email protected]
Joel Bojorquez Ken M. Winchester
520-872-7308 520-544-9890
[email protected] [email protected]
652306 483149
1063597169 1386619799
Yes Yes
03-1501 31547
JCAHO Not Accredited
Hospice Service Agency Hospice Service Agency with one or more Inpatient Facilities
Voluntary (Not For Profit) Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Hospital - Based Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
In Patient Unit
HSCP-3560
5830 N. Fountains Ave., Bldg 2
Tucson
85704
Pima
7740 N. Oracle Road
Tucson
85704
Pima
520-575-6425
Mixed Urban and Rural Mixed Urban and Rural
Free Standing
Mixed Use General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 9
0 9
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 9
0 9
0 8PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
1206 2248
780 1692
682 1491
130 247Number of Patient Care Days Number of Patient Care Days
38972 110850
63 250
0 0
658 2630
39693 113730
Census Information Census Information
107 312
51 63
15 16
263 553
36 110
Gender Gender
410 926
370 766Age Age
0 0
4 7
136 183
155 268
230 474
255 760Race/Ethnicity Race/Ethnicity
0 8
8 12
19 28
227 167
13 1
479 1348
34 128Number of Admissions by Source Number of Admissions by Source
495 849
89 121
54 59
15 663
127 0
780 1692Number of Deaths by Location Number of Deaths by Location
483 581
18 394
39 96
7 1
135 419
682 1491Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
326 537
108 216
60 330
102 170
24 47
31 57
39 35
1 1
2 84
87 128
0 87
780 1692Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
14435 24758
8362 20546
3522 35876
5343 11673
429 2012
611 1630
1407 782
293 278
419 6523
4449 5033
423 4619
39693 113730Number of Admissions by Payer Source Number of Admissions by Payer Source
634 1477
48 20
2 1
63 128
33 66
780 1692
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
33096 106219
1446 1288
769 2
2183 5367
2199 854
39693 113730PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
21.6 47.8
6.0 7.2
7.6 17.4
0.5 4.7
0.0 0.0
2.6 4.3
38.0 81.4
20.0 52.1
3.0 1.4
61.0 134.9Home Hospice Visits Home Hospice Visits
10192 58405
3111 7263
6703 24640
425 3279
0 0
0 6757
20431 100344
0 0
2419 4172
22850 104516Inpatient Facility FTEs Inpatient Facility FTEs
0.0 11.0
0.0 1.8
0.0 15.9
0.0 0.2
0.0 0.0
0.0 2.5
0.0 31.3
0.0 5.9
0.0 0.0
0.0 37.2
61.0 172.1
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 4
0 8
0 8
0 8Average Outpatient Case Load Average Outpatient Case Load
0 14
17 47
9 15
30 41
95 137
4058 7459
1202 1489
3 51PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$9,440,673.12 $16,618,136.34
$712,183.00 $178,981.81
$336,023.25 $16,898.86
$292,651.25 $747,703.31
$0.00 $359,975.22
$10,781,530.62 $17,921,695.54Amount Received by Payer Source Amount Received by Payer Source
$4,521,794.48 $16,627,592.82
$420,256.19 $191,314.66
$7,119.81 $19,645.88
$192,448.72 $731,846.43
$0.00 $547,369.14
$5,141,619.20 $18,117,768.93
$168,486.90 $0.00
$252,340.57 $157,146.00
$0.00 $21,327.62
$420,827.47 $178,473.62
$4,720,791.73 $17,939,295.31
$0.00 $0.00
$3,401,977.00 $216.17
$8,122,768.70 $17,939,511.48
EXPENSES EXPENSES
$3,473,015.49 $9,605,182.74
$91,169.89 $88,354.65
$767,297.86 $1,829,385.65
$473,225.08 $3,642,595.80
$355,232.96 $34,947.43
$0.00 $122,499.98
$0.00 $0.00
$1,903.16 $240,268.17
$0.00 $81,362.12
$3,122,357.16 $2,376,501.84
$8,284,201.60 $18,021,098.38
-$161,432.90 -$81,586.90
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$161,432.90 -$81,586.90
$0.00 $0.00
-$161,432.90 -$81,586.90TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$161,432.90 -$81,586.90
$0.00 $1,482,794.47
-$161,432.90 $1,401,207.57
ASSETS ASSETS
$2,950.00
$0.00
$82,893.30
$25,936,567.10
$4,334,518.25
$13,039,077.10
$43,396,005.75ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$85,029,737.04
$677,085.81
$129,102,828.60
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$510,036.35
$5,923,020.66
$4,756,168.68
$44,632.34
$32,078,492.62
NET ASSETS NET ASSETS
$96,941,442.65
$82,893.33
$0.00
$97,024,335.98
$129,102,828.60
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/17/2015 5/18/2015
HSPC-0023 HSPC-2902
RCHP-Sierra Vista, Inc.
Casa de la Paz Hospice CHARLES WM.LEIGHTON JR HOSPICE
185 S. Moorman Avenue 524 W MALEY PLACE
Sierra Vista WILLCOX
AZ AZ
85635 85643
Cochise COCHISE
151 B Colonia de Salud P.O. BOX 115
Sierra Vista WILLCOX
AZ AZ
85635 85644
Cochise COCHISE
520-417-3080 (520) 384-5878
Dr Dean French MARJORY SCOTT
520-263-3001 (520) 384-5878
[email protected] [email protected]
Steve Calabrese WARREN KNOWLES
520-263-3002 (520) 384-5878
[email protected] [email protected]
Sharon Reynolds SHAYNA DEBUSK
520-263-3912 (520) 384-5878
[email protected] [email protected]
866419 N/A
1437186269 1366440083
Yes YES
031529 03-1551
JCAHO NOT ACCREDITED
N/A
Hospice Service Agency HOSPICE SERVICE AGENCY
Proprietary Voluntary (Not For Profit)
Primarily Rural Primarily Rural
Hospital-Based Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
(999) 999-9999
mm/dd/yyyy
Primarily Rural Primarily Rural
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
370 79
232 71
184 53
47 22Number of Patient Care Days Number of Patient Care Days
12160 6775
67 7
0 0
0 161
12227 6943
Census Information Census Information
33 19
53 44
22 22
78 25
16 11
Gender Gender
121 34
111 37Age Age
4 0
3 0
22 6
34 7
71 19
98 39Race/Ethnicity Race/Ethnicity
0 0
3 0
4 1
47 6
0 0
164 64
14 0Number of Admissions by Source Number of Admissions by Source
208 41
13 1
11 8
0 21
0 0
232 71Number of Deaths by Location Number of Deaths by Location
160 21
18 2
6 9
0 21
0 0
184 53Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
82 21
49 9
25 8
16 10
16 4
6 5
3 4
0 0
5 1
5 9
25 0
232 71Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
3289 870
2456 1726
2161 999
1785 911
554 328
80 52
56 206
0 0
42 337
115 1514
1689 0
12227 6943Number of Admissions by Payer Source Number of Admissions by Payer Source
194 63
17 0
7 5
14 3
0 0
232 71
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
10179 6426
1016 0
222 180
810 337
0 0
12227 6943PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
4.2 3.0
1.6 1.0
2.4 2.0
0.0 0.5
0.5 0.0
1.0 0.3
9.7 6.8
1.6 1.0
0.6 0.5
11.9 8.3Home Hospice Visits Home Hospice Visits
7008 1398
628 322
3463 881
0 0
35 0
399 0
11533 2601
1647 428
239 52
13419 3081Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
11.9 8.3
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
11 13
33 26
9 13
33 5
280 16
1617 1359
1257 53
3 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$4,241,697.00 $717,837.16
$438,427.00 $0.00
$82,332.00 $0.00
$335,110.00 $59,624.20
$0.00 $17,696.32
$5,097,566.00 $795,157.68Amount Received by Payer Source Amount Received by Payer Source
$1,458,243.00 $717,837.16
$78,917.00 $0.00
$0.00 $0.00
$126,959.73 $59,624.20
$0.00 $17,696.32
$1,664,119.73 $795,157.68
$0.00 $0.00
$82,332.00 $0.00
$0.00 $0.00
$82,332.00 $0.00
$1,581,787.73 $795,157.68
$0.00 $0.00
$0.00 $341.92
$1,581,787.73 $795,499.60
EXPENSES EXPENSES
$840,104.56 $505,092.53
$0.00 $25,480.06
$178,078.27 $45,160.23
$236,648.86 $219,783.69
$30,700.00 $0.00
$5,207.55 $25,964.04
$0.00 $0.00
$53,801.48 $0.00
$0.00 $0.00
$101,231.06 $91,298.54
$1,445,771.78 $912,779.09
$136,015.95 -$117,279.49
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$136,015.95 -$117,279.49
$0.00 $0.00
$136,015.95 -$117,279.49TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$136,015.95 -$117,279.49
$0.00 $315,947.00
$136,015.95 $198,667.51
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/19/2015 5/20/2015
HSPC-4796 HSPC-3553
Community Hospice Group, LLC Sun Valley Hospice LLC
Copper Communities Hospice Cornerstone Hospice of Arizon
136 South Broad Street 7310 N 16 St. Suite 230
Globe Phoenix
AZ AZ
85506 85020
Gila Maricopa
450 North Sobson, Suite 108
Mesa
AZ
85201
Maricopa
480-456-9300 (602) 263-0925
Richard Bass Diane Kazala
480-435-9300 (602) 263-0925
[email protected] [email protected]
Karen Monville Ryan Jessup
480-435-9300 (949) 288-5884
[email protected] [email protected]
Ramsey David Badre Diane Kazala
912-634-9197 (602) 263-0925
[email protected] [email protected]
583314 908288
19992030779 1538443569
Yes Yes
03-1591 03-1554
JCAHO JCAHO
None
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Mixed Urban and Rural
Free Standing Free Standing
N/A NA
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A NA
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Primarily Urban Mixed Urban and Rural
N/A NA
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
111 121
78 110
63 77
30 82Number of Patient Care Days Number of Patient Care Days
11465 20980
156 157
0 1
22 159
11643 21297
Census Information Census Information
32 58
97 209
32 117
16 19
12 18
Gender Gender
30 58
33 37Age Age
0 0
1 0
19 6
15 17
15 31
28 44Race/Ethnicity Race/Ethnicity
6 0
0 1
0 6
12 14
0 1
55 73
5 0Number of Admissions by Source Number of Admissions by Source
74 79
1 9
3 4
0 14
0 4
78 110Number of Deaths by Location Number of Deaths by Location
60 63
0 7
3 5
0 1
0 2
63 78Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
28 9
25 27
10 26
6 24
3 3
0 2
8 2
0 0
0 10
3 7
0 0
83 110Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2427 1091
3400 6589
2776 5180
2244 3761
66 1279
0 763
672 878
0 0
0 1756
58 0
0 0
11643 21297Number of Admissions by Payer Source Number of Admissions by Payer Source
65 106
11 0
0 3
4 1
3 0
83 110
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
10755 19873
329 0
0 0
67 1417
492 7
11643 21297PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.0 11.0
1.0 1.0
3.0 7.0
0.0 1.0
0.0 0.0
0.0 1.5
7.0 21.5
0.5 8.0
0.5 0.5
8.0 30.0Home Hospice Visits Home Hospice Visits
2245 5735
439 542
1909 5887
0 144
0 0
0 359
4593 12667
0 0
1609 0
6202 12667Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
8.0 30.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
11 15
32 35
11 20
16 40
6 29
355 563
54 107
2 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$2,551,492.00 $3,648,868.00
$0.00 $0.00
$0.00 $0.00
$35,559.00 -$1,775.00
$2,425.00 $1.00
$2,589,476.00 $3,647,094.00Amount Received by Payer Source Amount Received by Payer Source
$1,620,582.00 $3,957,377.00
$0.00 $8,452.00
$0.00 $0.00
$35,559.00 $30,523.00
$2,425.00 $0.00
$1,658,566.00 $3,996,352.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,658,566.00 $3,996,352.00
$0.00 $0.00
$0.00 $0.00
$1,658,566.00 $3,996,352.00
EXPENSES EXPENSES
$555,544.00 $1,746,295.00
$8,068.00 $1,970.00
$96,681.00 $335,226.00
$346,512.00 $637,859.00
$40,981.00 $167,090.00
$14,280.00 $746.00
$0.00 -$18,209.00
$2,173.00 $11,196.00
$0.00 $0.00
$384,671.00 $543,822.00
$1,448,910.00 $3,425,995.00
$209,656.00 $570,357.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$209,656.00 $570,357.00
$0.00 -$909,091.00
$209,656.00 -$338,734.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$209,656.00 -$338,734.00
$0.00 $6,341,893.00
$209,656.00 $6,003,159.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/21/2015 5/22/2015
HSPC-3868 HSPC-4245
B.Jackson & K Gilbreth Kent Allen
Desert Oasis Hospice East Valley Hospice
20815 North 25th Place A-106 1311 W. Chandler Blvd., Ste. 200
Phoenix Chandler
AZ AZ
85050 85224
Maricopa Maricopa
602-424-4204 480-895-5434
Katherine Gilbreth Kent Allen
602-424-4204 480-895-5434
[email protected] [email protected]
None Kim Allen
N/A 480-895-5434
Richard K. Dixon Gwen Tvedt
321-473-8561 480-895-5434
[email protected] [email protected]
108714
1033165352 1114123387
Yes
03-1568 31578
Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Mixed Urban and Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
N/A HSCP-9999
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A (999) 999-9999
mm/dd/yyyy
Primarily Urban Mixed Urban and Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
239 264
194 141
149 77
57 46Number of Patient Care Days Number of Patient Care Days
23084 12348
60 13
0 0
26 24
0 12385
Census Information Census Information
63 34
87 80
87 85
36 25
27 5
Gender Gender
104 161
42 115Age Age
0 0
0 0
8 12
23 26
44 87
119 108Race/Ethnicity Race/Ethnicity
2 1
0 0
7 9
6 7
0 0
167 208
12 12Number of Admissions by Source Number of Admissions by Source
36 85
152 52
4 4
0 0
1 0
0 141Number of Deaths by Location Number of Deaths by Location
27 61
116 50
4 9
0 0
1 0
0 120Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
15 37
53 26
56 33
18 12
6 1
10 4
5 2
0 0
10 4
21 21
0 1
0 141Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
1098 3385
5814 2852
11167 3007
1496 840
319 1
638 771
131 43
0 0
617 1285
1890 131
0 70
0 12385Number of Admissions by Payer Source Number of Admissions by Payer Source
184 137
6 0
0 0
0 1
4 3
0 141
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
21951 12176
751 0
0 0
0 13
468 196
0 12385PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
6.0 5.0
1.0 2.0
4.0 3.0
4.0 1.0
1.0 0.0
0.0 0.0
0.0 11.0
0.0 4.0
1.0 38.0
0.0 53.0Home Hospice Visits Home Hospice Visits
6919 2193
1066 633
6096 3996
0 126
0 0
671 573
0 7521
21 0
30 0
14803 7521Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
17.0 53.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
21 0
63 0
13 0
63 0
10 16
109 7547
392 314
2 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,154,217.00 $1,979,382.00
$107,914.00 $0.00
$0.00 $0.00
$0.00 $0.00
$67,249.00 $0.00
$0.00 $1,979,382.00Amount Received by Payer Source Amount Received by Payer Source
$3,174,785.00 $1,904,358.00
$108,618.00 $0.00
$0.00 $0.00
$0.00 $0.00
$67,687.00 $0.00
$3,351,090.00 $1,904,358.00
$0.00 $0.00
$0.00 $25,597.00
$21,711.00 $0.00
$21,711.00 $25,597.00
$3,329,379.00 $1,878,761.00
$0.00 $0.00
$5,524.00 $3,888.00
$3,334,903.00 $1,882,649.00
EXPENSES EXPENSES
$1,231,766.00 $990,848.00
$117,378.00 $6,600.00
$317,153.00 $110,253.00
$597,980.00 $203,999.00
$72,500.00 $22,642.00
$0.00 $46,149.00
$0.00 $0.00
$5,915.00 $0.00
$0.00 $260.00
$433,935.00 $227,284.00
$2,776,627.00 $1,608,035.00
$558,277.00 $274,614.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$558,277.00 $274,614.00
$0.00 $0.00
$558,277.00 $274,614.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$558,277.00 $274,614.00
$103,872.00 $1,270,582.00
$77,988.00 $1,545,196.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/23/2015 5/24/2015
HSPC-5656 HSPC-5605
Emblem Healthcare, Inc.
Emblem Hospice Gemini Hospice
88 South San Marcos Place 3690 E Riggs Rd Ste 4
Chandler Chandler
AZ AZ
85225 85249
Maricopa Maricopa
(480) 821-8338 480-883-1353
Reginald Simmons Casey Carter
480-888-5609 480-883-1353
[email protected] [email protected]
NA Mary Marshall
NA 480-883-1353
Sandra Whitley Casey Carter
949-540-1926 480-883-1353
[email protected] [email protected]
861964 843349
1487999405 1194060806
Yes Yes
03-1595 31615
CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
Mixed Urban and Rural Mixed Urban and Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
241 247
204 164
127 66
37 113Number of Patient Care Days Number of Patient Care Days
25417 23890
56 64
0 1
70 66
25543 24021
Census Information Census Information
70 66
132 116
0 50
36 9
15 14
Gender Gender
306 91
211 73Age Age
0 0
0 0
11 14
48 38
50 51
408 61Race/Ethnicity Race/Ethnicity
2 2
4 0
9 5
10 14
0 0
150 143
342 0Number of Admissions by Source Number of Admissions by Source
0 110
0 47
0 5
0 0
0 2
0 164Number of Deaths by Location Number of Deaths by Location
62 41
0 19
66 5
0 0
0 1
128 66Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
19 23
45 71
67 16
27 30
5 5
12 6
5 4
1 0
7 9
13 0
3 0
204 164Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
1380 1877
3722 10994
10938 4584
3657 3465
49 437
430 1100
161 320
34 0
1577 813
3181 0
414 431
25543 24021Number of Admissions by Payer Source Number of Admissions by Payer Source
196 158
7 0
0 0
1 1
0 5
204 164
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
25334 23705
139 0
0 0
70 7
0 309
25543 24021PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.0 0.0
4.7 0.0
7.1 0.0
0.0 0.0
0.0 0.0
0.0 0.0
14.8 0.0
0.0 0.0
0.0 0.0
14.8 0.0Home Hospice Visits Home Hospice Visits
404 4343
246 971
9258 5264
1 236
0 0
15815 1003
25724 11817
0 0
66 25
25790 11842Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
4.0 0.0
0.0 0.0
4.0 0.0
18.8 0.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 10
0 30
0 13
0 22
0 19
0 533
0 86
0 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$4,096,634.40 $4,123,923.57
$979.44 $0.00
$0.00 $0.00
$5,826.80 $3,697.25
-$28,614.80 $64,199.52
$4,074,825.84 $4,191,820.34Amount Received by Payer Source Amount Received by Payer Source
$4,096,634.40 $4,030,119.22
$979.40 $0.00
$0.00 $0.00
$5,826.80 $1,887.52
-$28,614.80 $0.00
$4,074,825.80 $4,032,006.74
$0.00 $0.00
$0.00 $64,199.52
$0.00 $95,614.08
$0.00 $159,813.60
$4,074,825.80 $4,032,006.74
$0.00 $0.00
$0.00 $0.00
$4,074,825.80 $0.00
EXPENSES EXPENSES
$1,489,886.54 $1,369,018.46
$120,514.79 $0.00
$266,011.41 $8,552.36
$731,773.92 $368,831.80
$205,901.19 $10,209.28
$27,580.42 $17,437.05
$65,254.27 $0.00
$21,075.10 $12,136.85
$0.00 $1,314.24
$52,637.11 $1,021,855.60
$2,980,634.75 $2,809,355.64
$1,094,191.05 $3,682,151.32
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,094,191.05 $0.00
$0.00 $0.00
$1,094,191.05 $0.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,094,191.05 $0.00
$0.00 $73,456.90
$1,094,191.05 $536,098.98
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/25/2015 5/26/2015
HSPC-1059 HSPC-5172
Odyssey HealthCare Operating A, LP
Gentiva Hospice Gerinet Palliative Care, LLC
5210 E Williams Circle, Ste 100 2100 N. Wilmot Road 208
Tucson Tucson
AZ AZ
85711 85172
Pima Pima
12900 Foster St, Ste 400
Overland Park
KS
66213
Johnson
(520) 577-0270 (520) 300-9337
Michael J. Johnson Karen Brannon
(520) 577-0270 (520) 300-9337
[email protected] [email protected]
Eric Slusser Richard Carpe, Interim CFO
(770) 951-6101 (714) 640-7319
[email protected] [email protected]
Kalpita Pathak Rosa Guaderrama
(913) 814-2075 (714) 640-5040
[email protected] [email protected]
03-1538 756115
1-295736270 1053625848
Yes Yes
03-1538/648404 03-1605
Not Accredited CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Primarily Urban
Free Standing Home Health-Based
n/a
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Gerinet Service Agency
HSCP-9999 HSCP-5172
2100 N. Wilmot Road 208
Tucson
85172
Pima
(999) 999-9999 (520) 300-9337
mm/dd/yyyy
Mixed Urban and Rural Primarily Urban
Home Health-Based
n/a
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
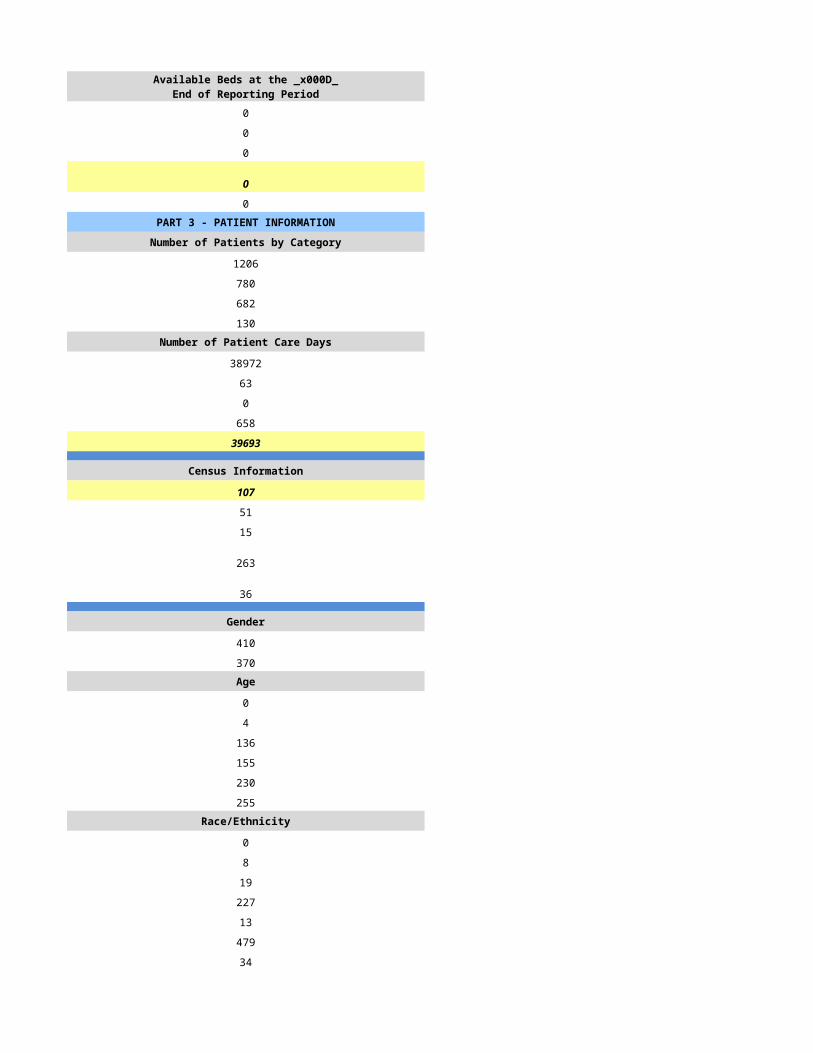
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
346 215
346 197
298 133
98 62Number of Patient Care Days Number of Patient Care Days
23800 17950
99 111
0 0
154 174
24053 18235
Census Information Census Information
66 50
137 93
31 48
79 34
38 33
Gender Gender
206 163
140 112Age Age
0 0
1 0
36 14
58 42
93 65
158 154Race/Ethnicity Race/Ethnicity
4 0
1 0
4 0
55 9
0 0
280 266
2 0Number of Admissions by Source Number of Admissions by Source
177 81
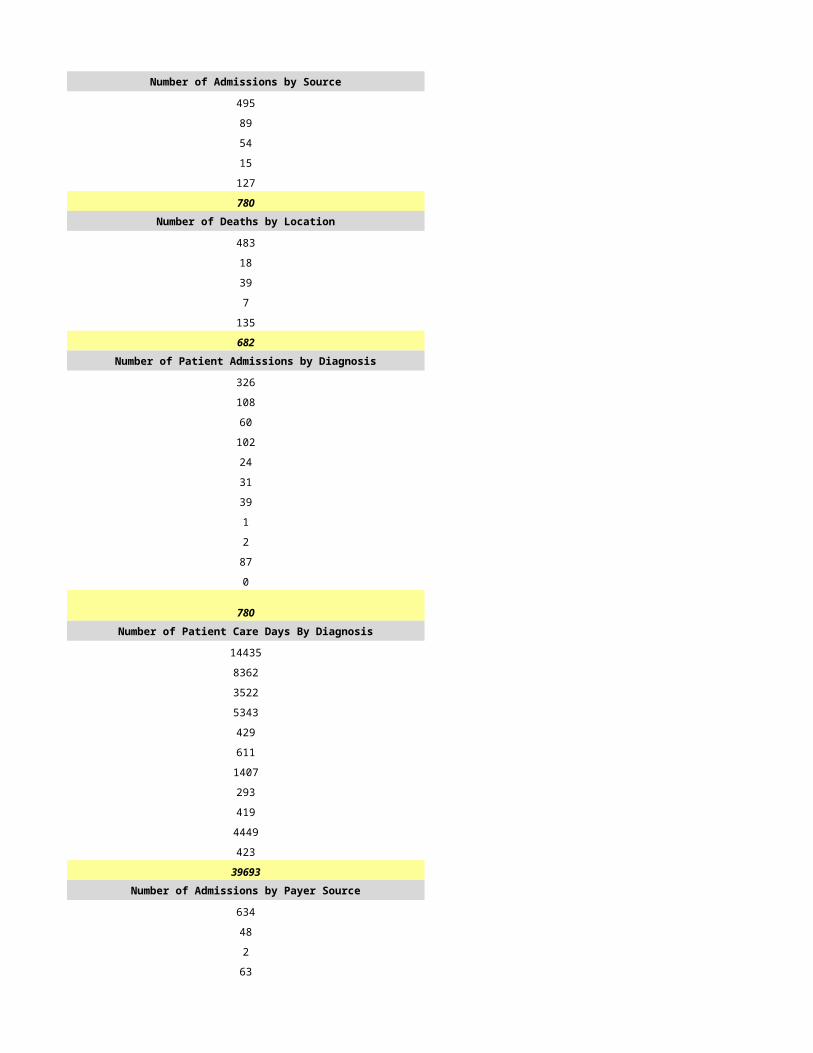
105 80
63 31
1 0
0 6
346 198Number of Deaths by Location Number of Deaths by Location
177 40
105 62
63 28
1 0
0 3
346 133Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
94 42
40 27
51 22
44 0
11 14
30 0
16 16
0 0
0 19
52 58
8 0
346 198Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
5334 2460
2757 3132
5717 7110
2913 360
490 99
2084 0
502 1360
0 0
0 629
3793 3046
463 39
24053 18235Number of Admissions by Payer Source Number of Admissions by Payer Source
309 198
10 0
0 0
24 0
3 0
346 198
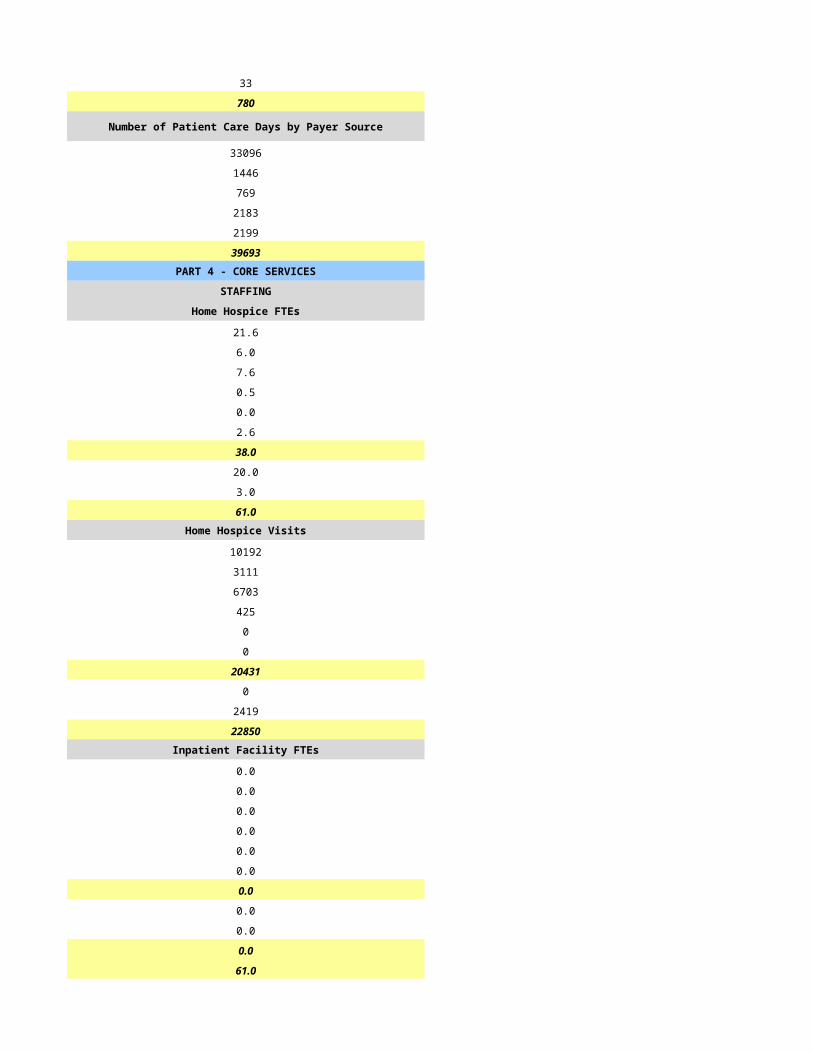
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
22139 18196
540 0
40 0
1317 0
17 39
24053 18235PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
11.0 6.0
2.0 2.0
11.0 1.0
3.0 0.0
0.0 0.0
0.1 5.0
27.1 14.0
13.0 5.0
3.0 1.0
43.1 20.0Home Hospice Visits Home Hospice Visits
7497 4194
1511 469
10421 3669
422 3
0 0
1346 648
21197 8983
0 0
239 51
21436 9034Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
43.1 20.0
CASELOADS CASELOADS
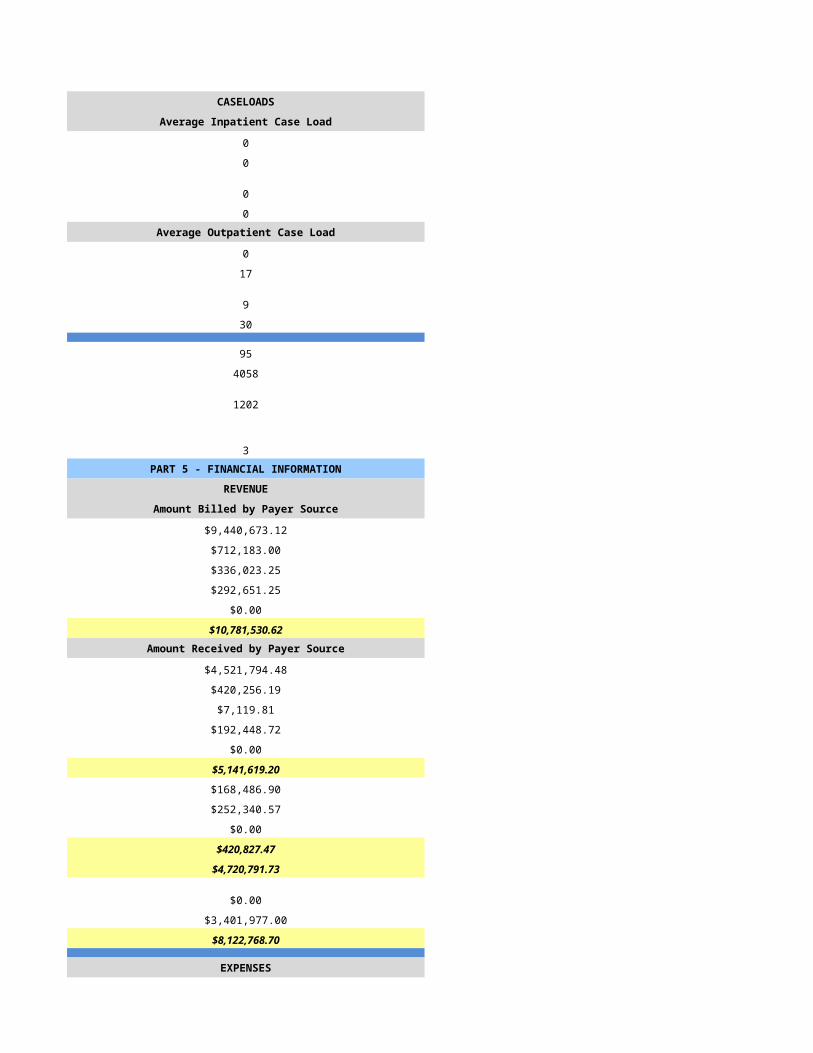
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
13 11
40 33
9 11
30 0
20 8
923 90
957 62
3 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$4,841,077.50 $2,942,846.00
$56,532.55 $0.00
-$53.00 $0.00
$411,367.96 $0.00
$2,074.33 $0.00
$5,310,999.34 $2,942,846.00Amount Received by Payer Source Amount Received by Payer Source
$4,841,099.19 $2,723,737.00
$62,223.34 $0.00
-$53.00 $0.00
$410,877.00 $0.00
$2,074.33 $0.00
$5,316,220.86 $2,723,737.00
$0.00 $0.00
$2,074.33 $0.00
$175,467.25 $0.00
$177,541.58 $0.00
$5,138,679.28 $2,723,737.00
$0.00 $0.00
$0.00 $0.00
$5,138,679.28 $2,723,737.00
EXPENSES EXPENSES
$1,977,515.79 $1,536,869.00
$281,402.72 $0.00
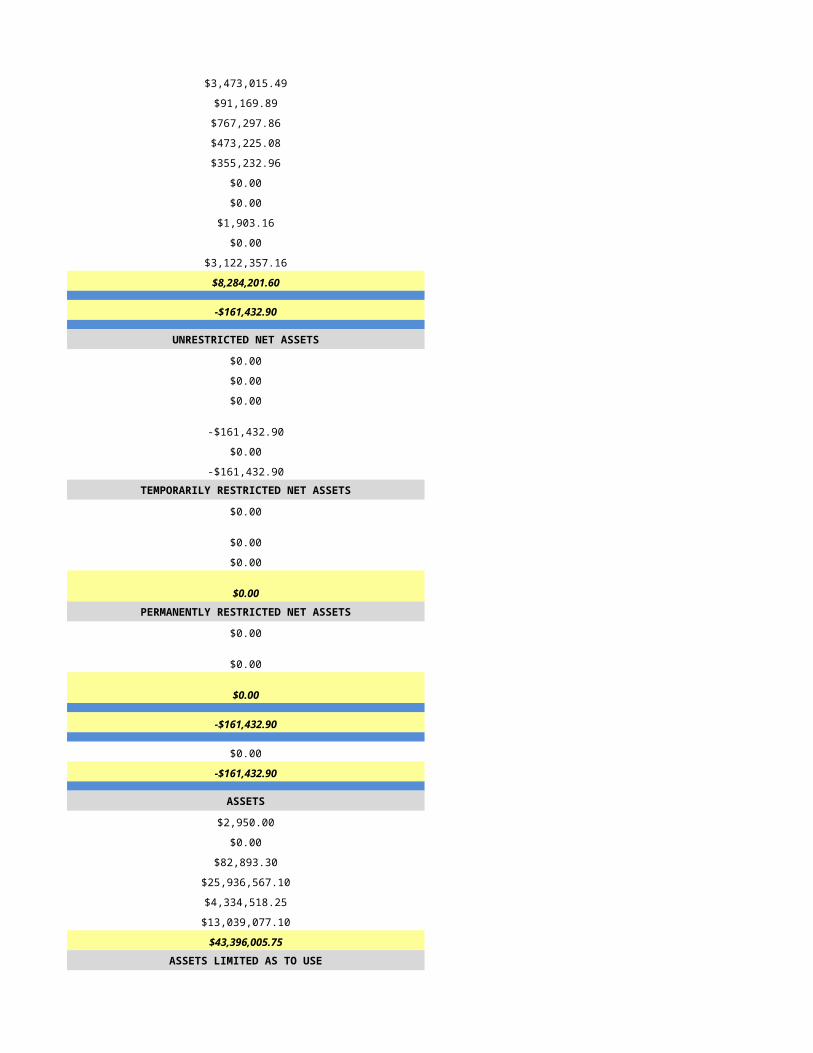
$483,386.30 $0.00
$1,416,238.92 $630,491.00
$238,555.76 $0.00
$0.00 $0.00
$0.00 $0.00
$30,418.32 $17,450.00
$0.00 $81,248.00
$579,585.36 $850,899.00
$5,007,103.17 $3,116,957.00
$131,576.11 -$393,220.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 -$800.00
$131,576.11 -$394,020.00
$0.00 $0.00
$131,576.11 -$394,020.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
-$58,079.00 $0.00
-$58,079.00 $0.00
$73,497.11 -$394,020.00
$0.00 $0.00
$73,497.11 -$394,020.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
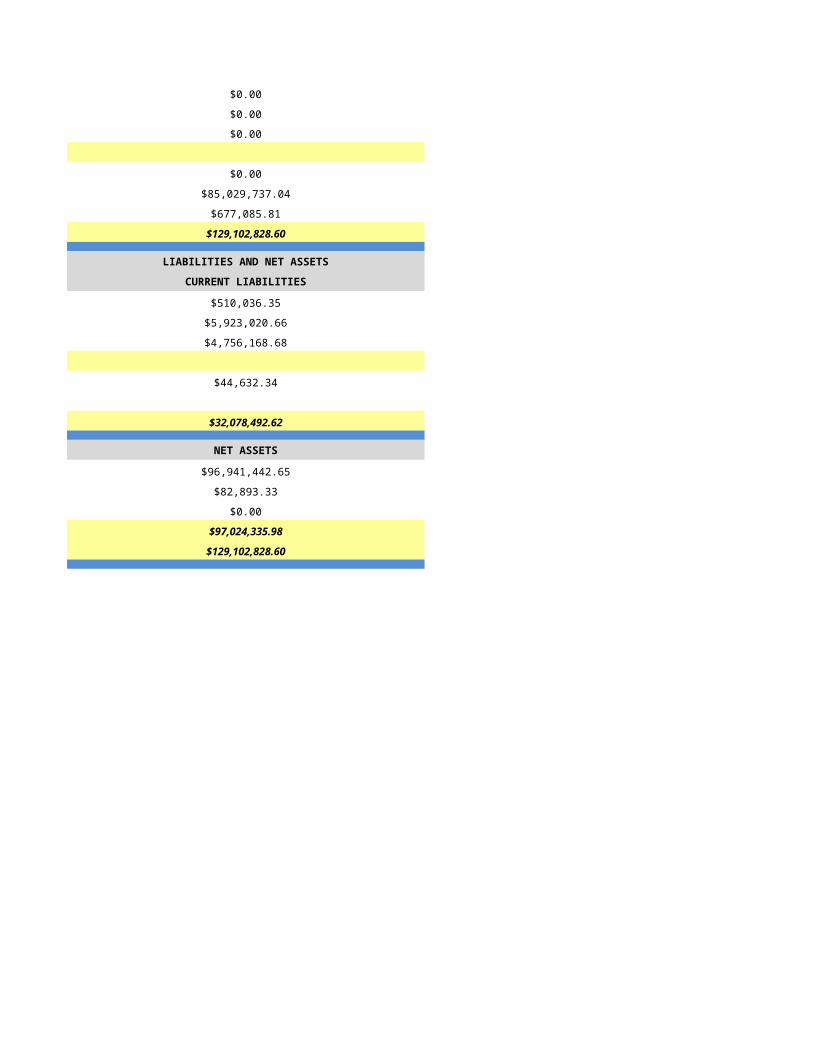
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/27/2015 5/28/2015
HSPC-4260 HSPC-4514
Good Samaritan Society - Prescott Hospice Grace Hospice of Arizona, Inc.
Good Samaritan Society - Prescott Hospice Grace Hospice of Arizona, Inc.
1065 Ruth Street 108 2141 East Broadway Road, Suite 110
Prescott Tempe
AZ AZ
86301 85252
Yavapai Maricopa
5314 South Yale Avenue, Suite 420
Tulsa
OK
74135
Tulsa
928-778-5655 480-775-2599
Deborah Burton Alicia Coterillo Ferguson
928-778-5655 480-775-2599
[email protected] [email protected]
Grant Tribble Roger Bruhn
605-362-3327 918-894-3487
Paula Sedillo Greg Houpe
928-778-5655 918-770-4441
[email protected] [email protected]
N/A 527048
1851381578 1306152152
Yes Yes
03-1584 03-1587
CHAP CHAP
Hospice Service Agency Hospice Service Agency
Voluntary (Not For Profit) Voluntary (Not For Profit)
Primarily Rural Primarily Urban
Nursing Care Institution - Based Free Standing
N/A N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Marley House
HSPC 4260
1063 Ruth St
Prescott
86301
Yavapai
928-443-5400
Primarily Rural Primarily Urban
Nursing Care Institution - Based
N/A N/A
Mixed Use
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
10 0
0 0
10 0
9 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
10 0
0 0
9 0
9 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
421 464
308 291
270 253
113 159Number of Patient Care Days Number of Patient Care Days
12162 39868
8208 488
0 1
1186 288
21556 40645
Census Information Census Information
59 111
68 149
8 70
110 136
26 5
Gender Gender
224 163
174 130Age Age
1 0
0 0
29 32
56 48
104 100
208 113Race/Ethnicity Race/Ethnicity
0 0
1 3
0 11
11 24
3 0
349 243
30 12Number of Admissions by Source Number of Admissions by Source
69 207
44 86
35 0
119 0
41 0
308 293Number of Deaths by Location Number of Deaths by Location
80 124
63 45
63 57
0 0
64 27
270 253Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
88 77
46 95
44 31
43 40
12 6
19 10
5 7
0 0
27 14
35 3
10 10
346 293Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
3595 7758
4769 15307
4824 5395
4604 7111
124 342
780 1000
86 834
18 0
412 0
2297 2896
47 2
21556 40645Number of Admissions by Payer Source Number of Admissions by Payer Source
328 262
5 0
1 0
12 16
0 15
346 293
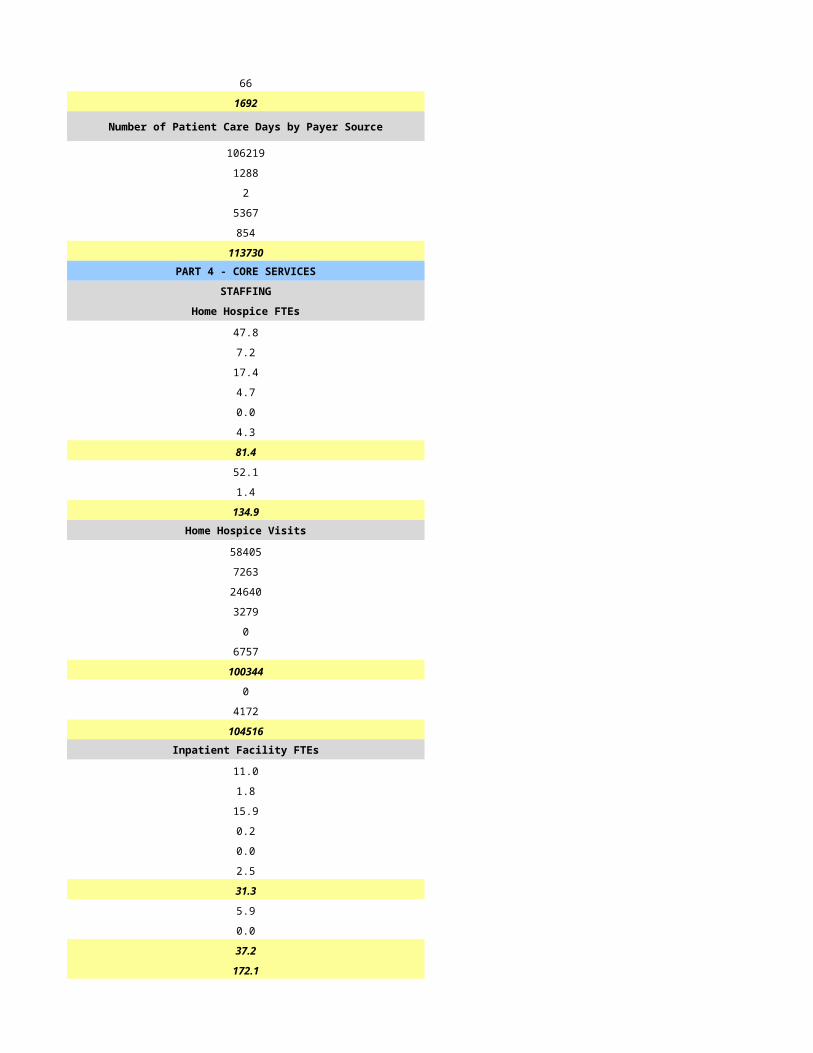
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
20859 37995
146 0
5 0
138 1135
408 1515
21556 40645PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
6.0 15.9
1.0 9.8
3.0 8.2
1.0 0.0
0.0 0.0
2.0 3.5
13.0 37.4
9.0 9.1
0.0 0.3
22.0 46.8Home Hospice Visits Home Hospice Visits
5774 10616
909 2668
5749 10549
362 387
0 0
43 3603
12837 27823
0 0
489 0
13326 27823Inpatient Facility FTEs Inpatient Facility FTEs
7.0 0.0
1.0 0.0
4.0 0.0
1.0 0.0
0.0 0.0
0.0 0.0
13.0 0.0
0.0 0.0
2.0 0.0
15.0 0.0
37.0 46.8
CASELOADS CASELOADS
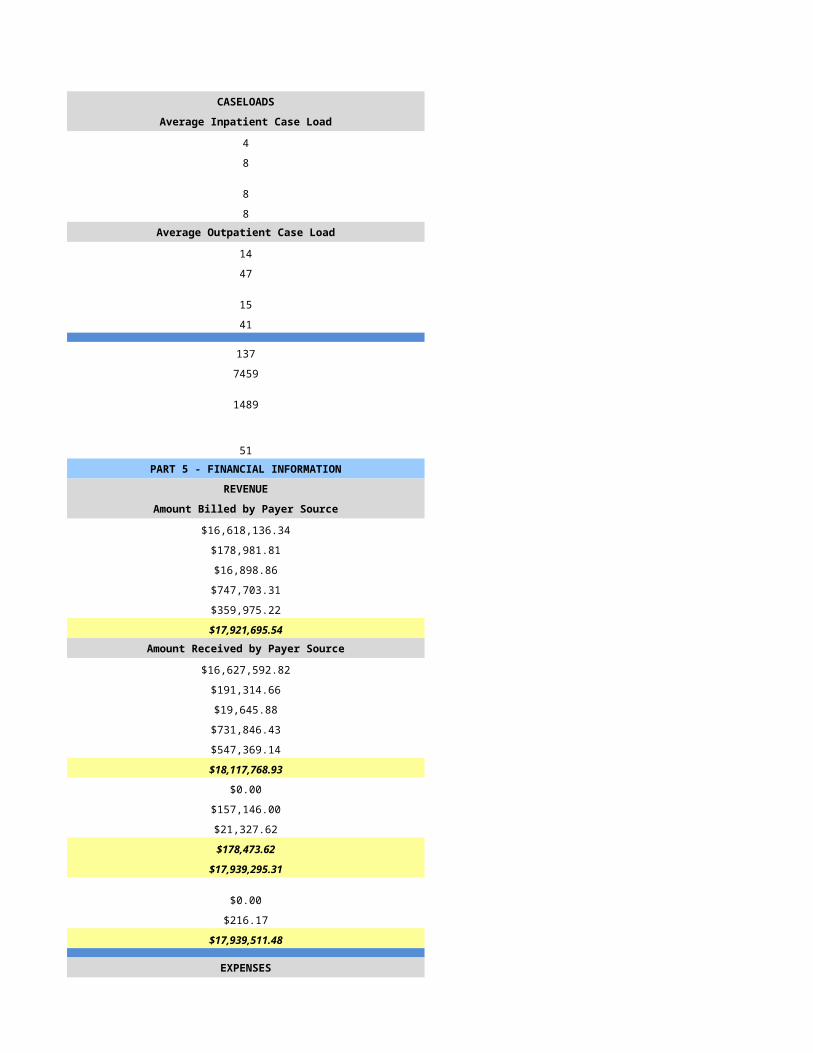
Average Inpatient Case Load Average Inpatient Case Load
5 0
5 0
5 0
4 0Average Outpatient Case Load Average Outpatient Case Load
0 99
0 49
0 291
0 37
50 31
2938 1405
339 509
3 6PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $6,274,519.00
$0.00 $0.00
$0.00 $0.00
$0.00 $163,901.00
$0.00 $481.00
$0.00 $6,438,901.00Amount Received by Payer Source Amount Received by Payer Source
$4,604,900.00 $6,274,519.00
$0.00 $0.00
$191,853.00 $0.00
$6,300.00 $163,901.00
$971,340.00 $481.00
$5,774,393.00 $6,438,901.00
$0.00 $0.00
$0.00 $0.00
-$2,891,859.00 $0.00
-$2,891,859.00 $0.00
$2,882,534.00 $6,438,901.00
$0.00 $0.00
$176,924.00 $0.00
$3,059,458.00 $6,438,901.00
EXPENSES EXPENSES
$2,478,753.00 $2,975,186.00
$131,986.00 $169,307.00
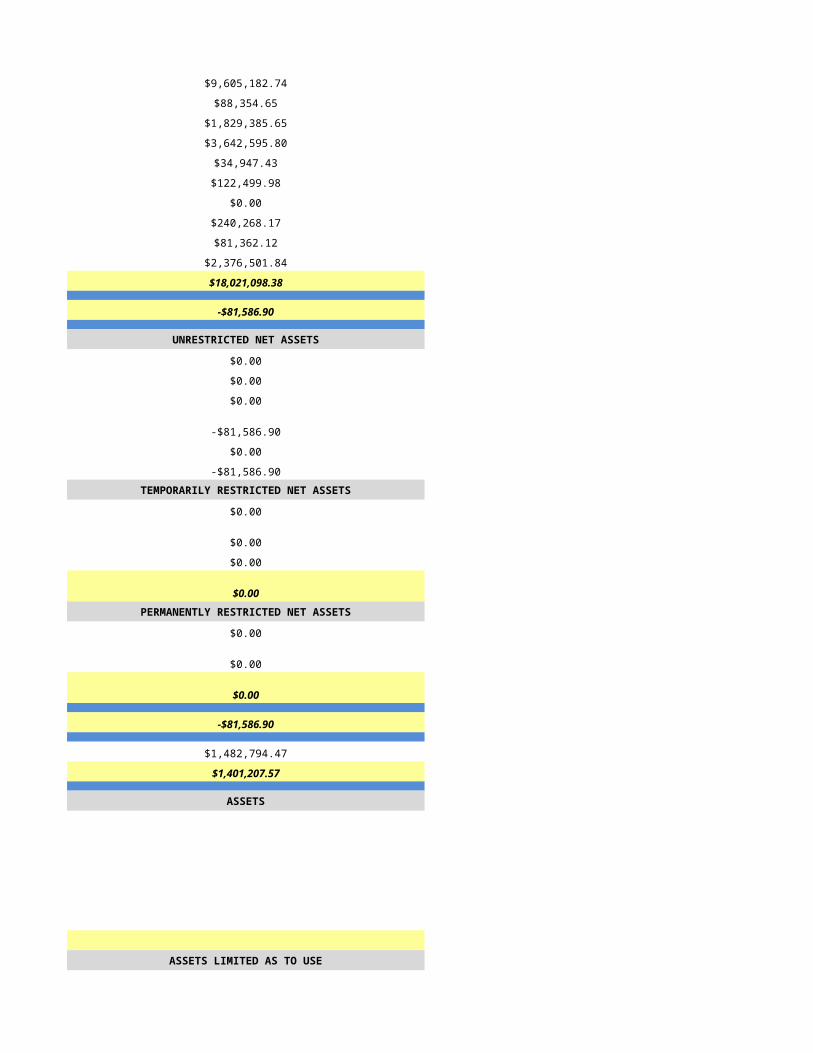
$433,575.00 $376,935.00
$62,649.00 $943,000.00
$102,240.00 $201,012.00
$11,234.14 $46,118.00
$0.00 $0.00
$79,847.00 $29,251.00
$0.00 $0.00
$1,045,318.86 $892,573.00
$4,345,603.00 $5,633,382.00
-$1,286,145.00 $805,519.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $805,519.00
$0.00 $0.00
$0.00 $805,519.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $805,519.00
$217,995.93 $4,911,529.00
-$1,273,466.92 $5,717,048.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/29/2015 5/30/2015
HSPC-3752 HSPC-1987
Central Arizona Home Health Care, Inc.
Granite Mountain Hospice Heartland Hospice
3107 Clearwater Drive, Suite B 3112 N. Swan Rd.
Prescott Tucson
AZ AZ
86305 85712
Yavapai Pima
Same
(928)-445-2522 520-325-2790
Amy Pollman, RN Theresa Linnane
(928)-445-2522 520-325-2790
[email protected] [email protected]
Todd Higgins Matt Kang
(502)-596-7953 419-252-5500
[email protected] [email protected]
Patrick Franks Theresa Linnane
(435)-652-7255 520-325-2790
[email protected] [email protected]
040063 6233736
1174575781 1457302267
Yes yes
03-1564 35148
Not Accredited CHAP
N?A
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Primarily Urban
Home Health-Based Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A Heartland Hospice
N/A HSPC 5681
N/A 75 W. Calle de las Tiendas
N/A Green Valley
N/A 85614
N/A Pima
N/A
N/A
N/A
N/A
N/A 520-625-4368
N/A
Primarily Rural Primarily Urban
N/A Free Standing
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
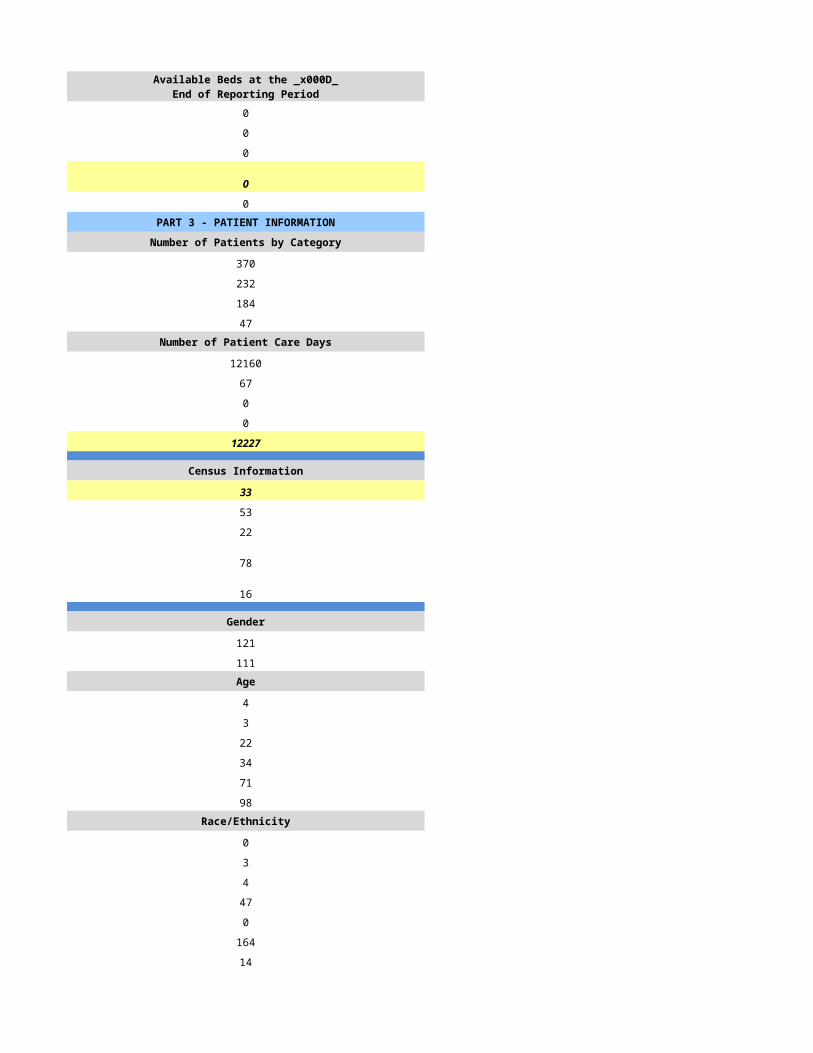
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
262 455
204 256
146 204
52 60Number of Patient Care Days Number of Patient Care Days
15896 29812
206 76
0 1
165 11
16267 29900
Census Information Census Information
45 82
91 100
28 53
49 48
7 229
Gender Gender
94 175
110 143Age Age
0 0
1 0
25 20
47 55
52 100
79 143Race/Ethnicity Race/Ethnicity
0 0
0 2
0 8
1 24
0 0
9 208
194 76Number of Admissions by Source Number of Admissions by Source
139 175
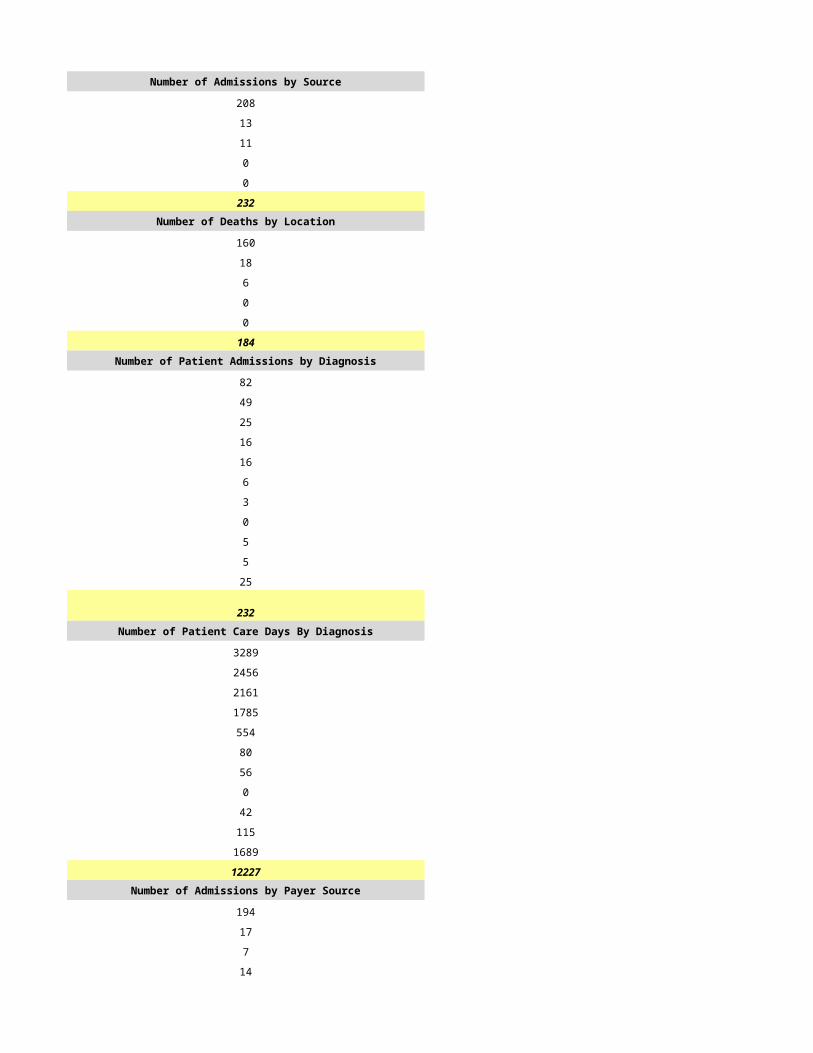
40 101
5 42
0 0
20 0
204 318Number of Deaths by Location Number of Deaths by Location
114 120
32 62
0 22
0 0
0 0
146 204Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
94 83
47 52
0 61
23 24
0 6
0 9
1 4
0 0
39 13
0 66
0 0
204 318Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
4849 4729
4251 8053
0 8866
1851 2903
100 1066
0 896
0 194
0 0
3579 3151
1637 42
0 0
16267 29900Number of Admissions by Payer Source Number of Admissions by Payer Source
184 206
1 0
0 0
15 7
4 34
204 247
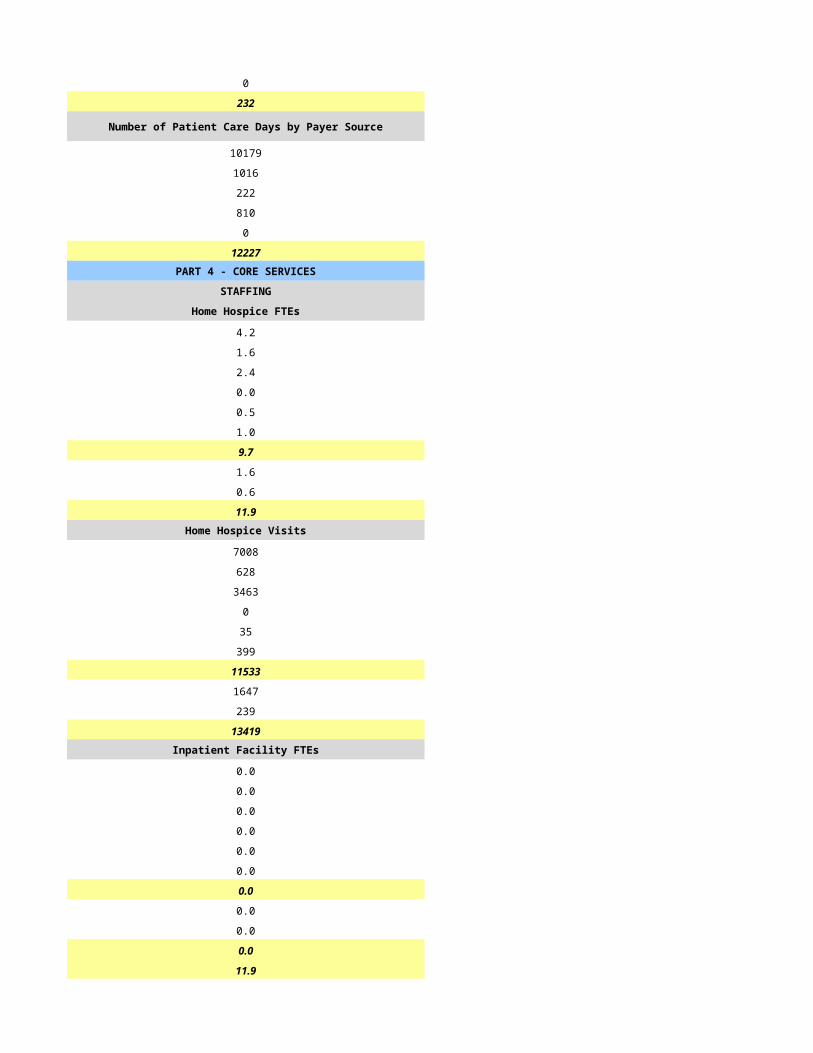
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
15193 23273
25 0
0 0
715 3643
334 2984
16267 29900PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
4.3 9.8
1.3 3.2
2.3 8.3
1.0 0.4
0.0 0.0
1.0 2.0
9.7 24.0
3.5 8.0
1.0 1.0
14.2 33.0Home Hospice Visits Home Hospice Visits
3482 7695
931 1169
3221 9198
108 323
0 0
9 1467
7751 19852
0 679
123 389
7874 20920Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
14.2 32.0
CASELOADS CASELOADS
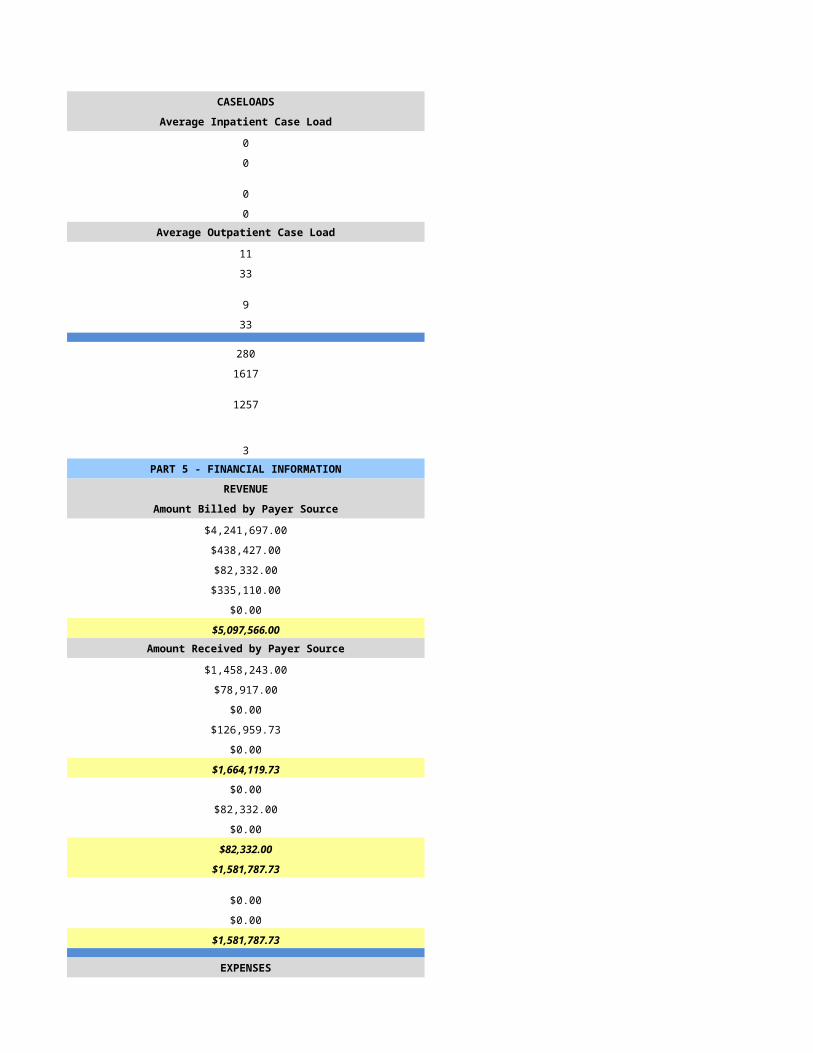
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
13 9
28 30
10 11
22 50
18 36
944 1151
251 377
5 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$2,696,691.00 $3,931,618.00
$4,500.00 $0.00
$0.00 $0.00
$97,070.00 $860,790.00
$0.00 $0.00
$2,798,261.00 $4,792,408.00Amount Received by Payer Source Amount Received by Payer Source
$2,698,493.00 $3,931,618.00
$0.00 $0.00
$0.00 $0.00
$72,544.00 $860,790.00
$31,919.00 $0.00
$2,802,956.00 $4,792,408.00
$0.00 $0.00
$0.00 $470,613.00
$0.00 $459,862.00
$0.00 $3,861,933.00
$2,802,956.00 $0.00
$0.00 $0.00
$0.00 $0.00
$2,802,956.00 $3,861,933.00
EXPENSES EXPENSES
$891,527.00 $1,797,646.00
$220,400.00 $0.00
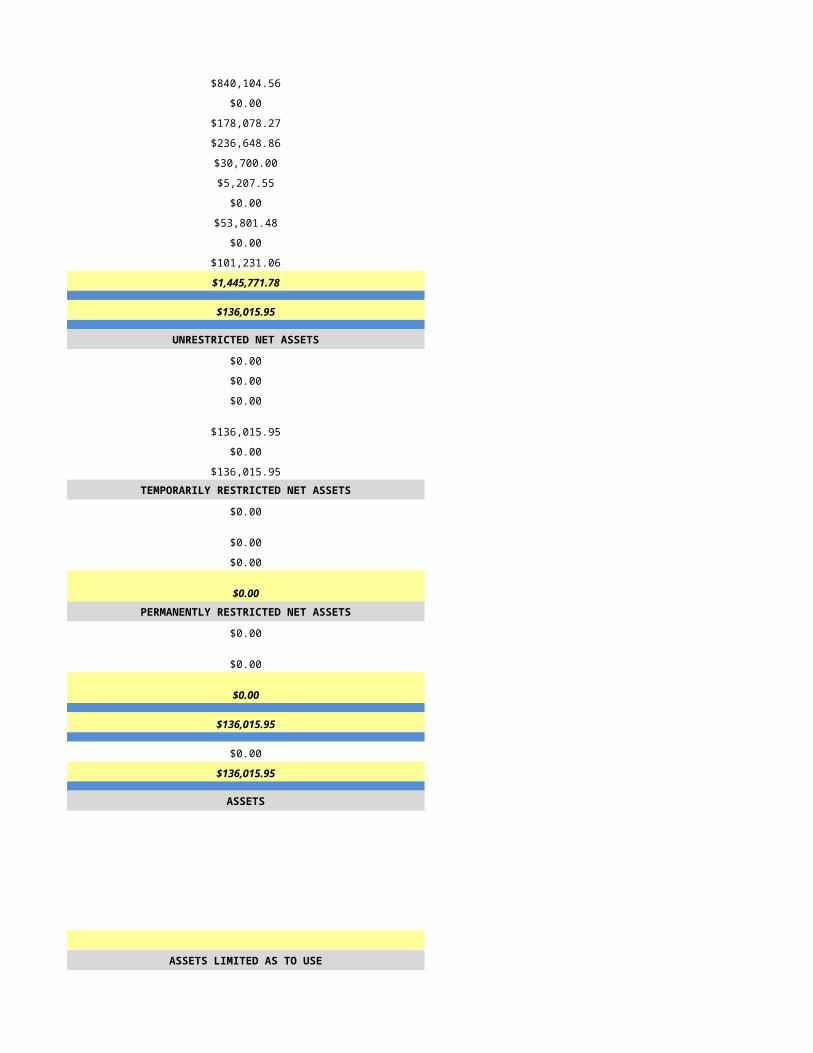
$119,699.00 $439,688.00
$287,168.00 $1,278,461.00
$0.00 $0.00
$0.00 $5,866.00
$0.00 $37,239.00
$0.00 $0.00
$0.00 $0.00
$762,564.00 $109,936.00
$2,281,358.00 $3,668,836.00
$521,598.00 $193,097.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$521,598.00 $193,097.00
$0.00 $0.00
$521,598.00 $193,097.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$521,598.00 $193,097.00
$598,704.16 $863,193.00
$1,120,302.16 $1,056,290.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
5/31/2015 6/1/2015
HSPC-1110 HSPC-4786
Eugene Stevens, M.D. Mahlega Abdsharafat & Kianoush Rahbar
Highway Christian Hospice, Inc. Homestead Hospice & Palliative Care of Arizona
67 E Weldon Ave Ste 317 312 N Alma School Rd Ste 11
Phoenix Chandler
AZ AZ
85012 85224
Maricopa Maricopa
same
n/a
n/a
n/a
602-274-1952 (480)584-3734
Eugene Stevens, M.D. Theresa Salerno
602-274-1952 (480)584-3734
[email protected] [email protected]
Eugene Stevens, M.D. Ali Dehdashti
602-274-1952 (678)966-0077
[email protected] [email protected]
Eugene Stevens, M.D. Kristina Petry
602-274-1952 (480)584-3734
[email protected] [email protected]
377730 640250
1225092760 1831428747
Yes Yes
31540
Not Accredited JCAHO
n/a
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Mixed Urban and Rural
Free Standing Free Standing
n/a N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
n/a N/A
Primarily Urban Mixed Urban and Rural
n/a N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
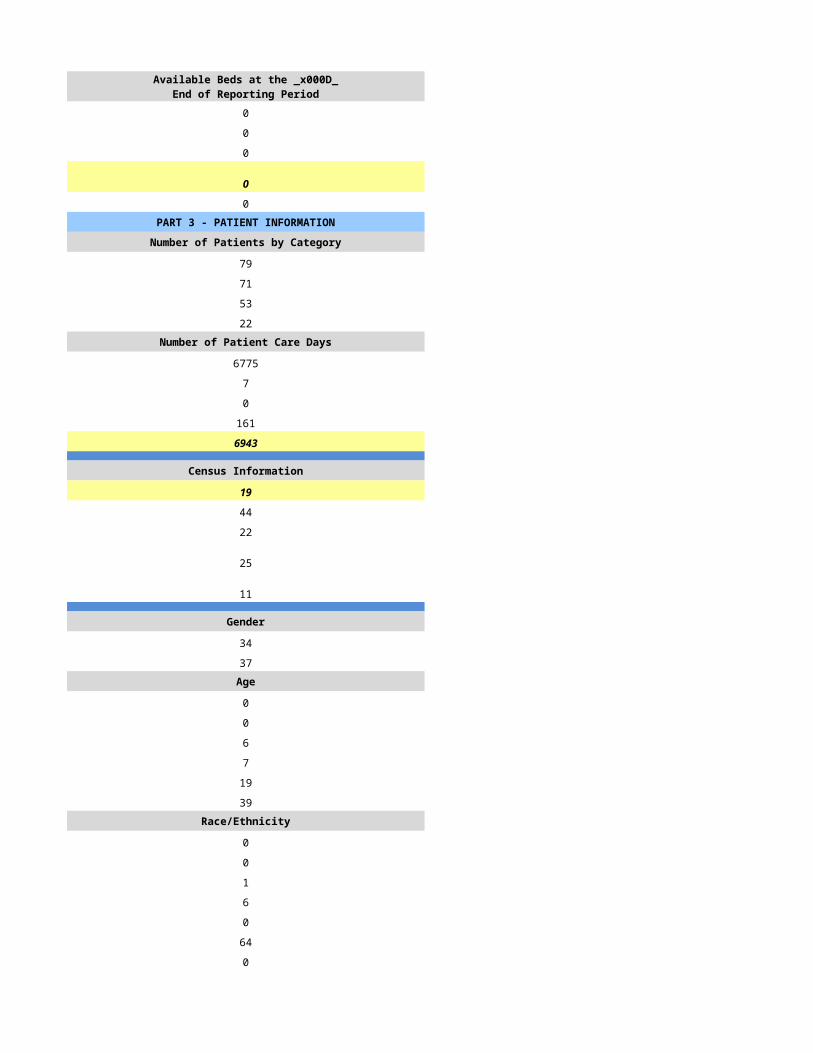
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
40 273
28 163
32 91
0 55Number of Patient Care Days Number of Patient Care Days
2186 29231
0 190
0 0
0 174
2186 29595
Census Information Census Information
6 81
84 135
21 107
7 12
5 21
Gender Gender
24 142
11 80Age Age
0 0
0 0
1 10
0 31
1 62
33 119Race/Ethnicity Race/Ethnicity
0 0
1 1
0 3
0 16
0 0
34 129
0 81Number of Admissions by Source Number of Admissions by Source
5 33
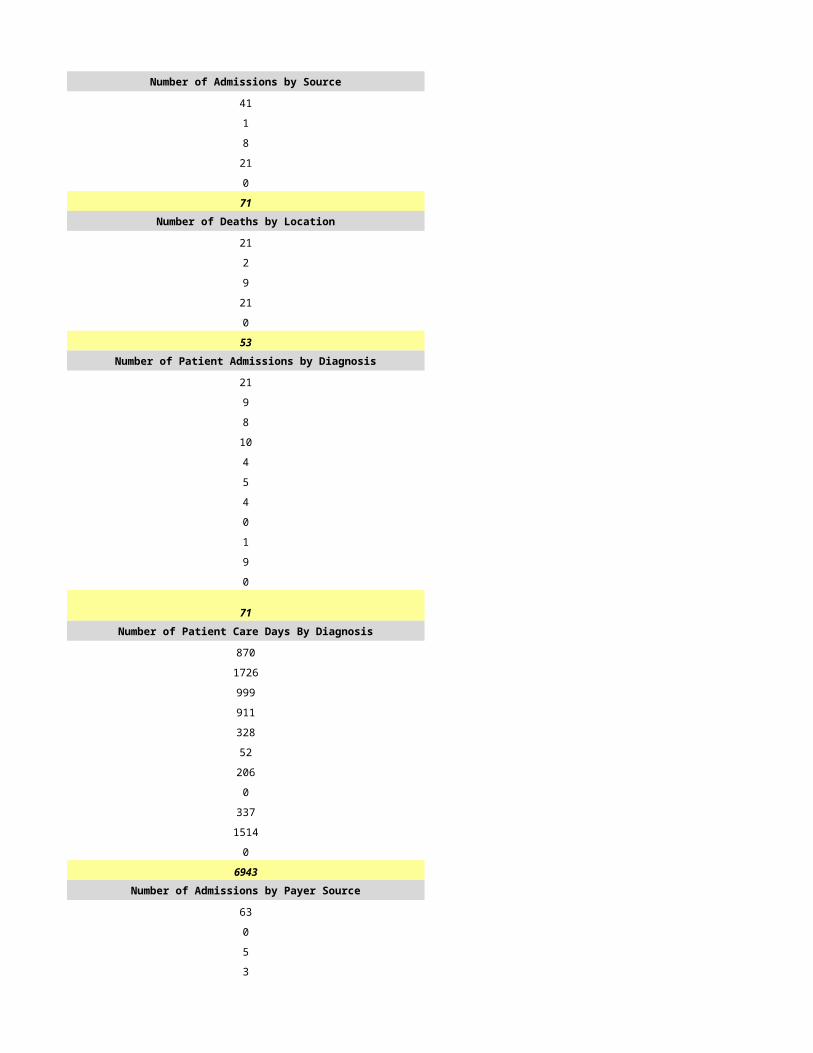
2 55
21 12
0 0
0 2
28 102Number of Deaths by Location Number of Deaths by Location
7 31
2 50
23 5
0 0
0 5
32 91Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
6 25
7 58
5 45
4 10
0 2
2 6
0 3
0 0
0 14
4 0
0 0
28 163Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
179 3610
825 9103
279 10163
341 2241
0 31
2 1180
0 138
0 0
263 3129
297 0
0 0
2186 29595Number of Admissions by Payer Source Number of Admissions by Payer Source
28 159
0 1
0 0
0 3
0 0
28 163
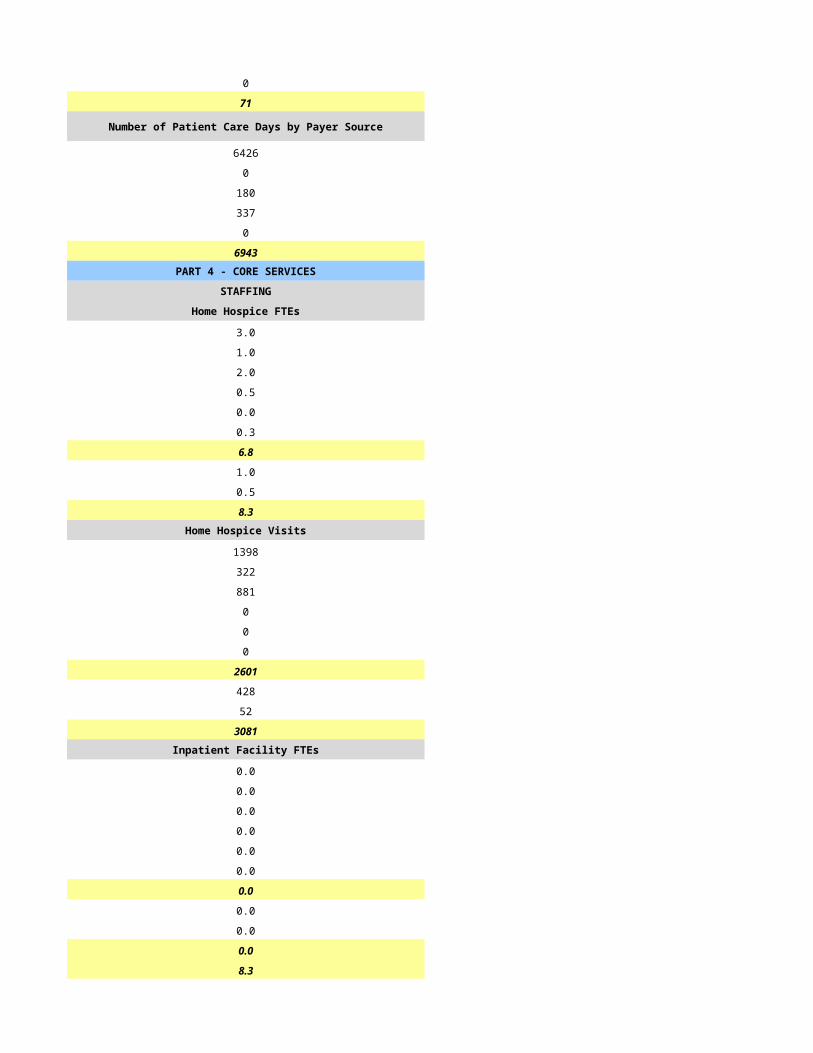
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
2186 29030
0 252
0 0
0 313
0 0
2186 29595PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
0.7 20.0
0.5 2.0
0.6 29.0
1.0 0.0
0.0 0.0
0.2 2.0
3.0 53.0
1.0 21.0
0.2 0.0
4.0 74.0Home Hospice Visits Home Hospice Visits
808 5335
308 1121
593 12530
0 0
0 0
268 1269
1977 20255
98 0
196 0
2271 20255Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 74.0
CASELOADS CASELOADS
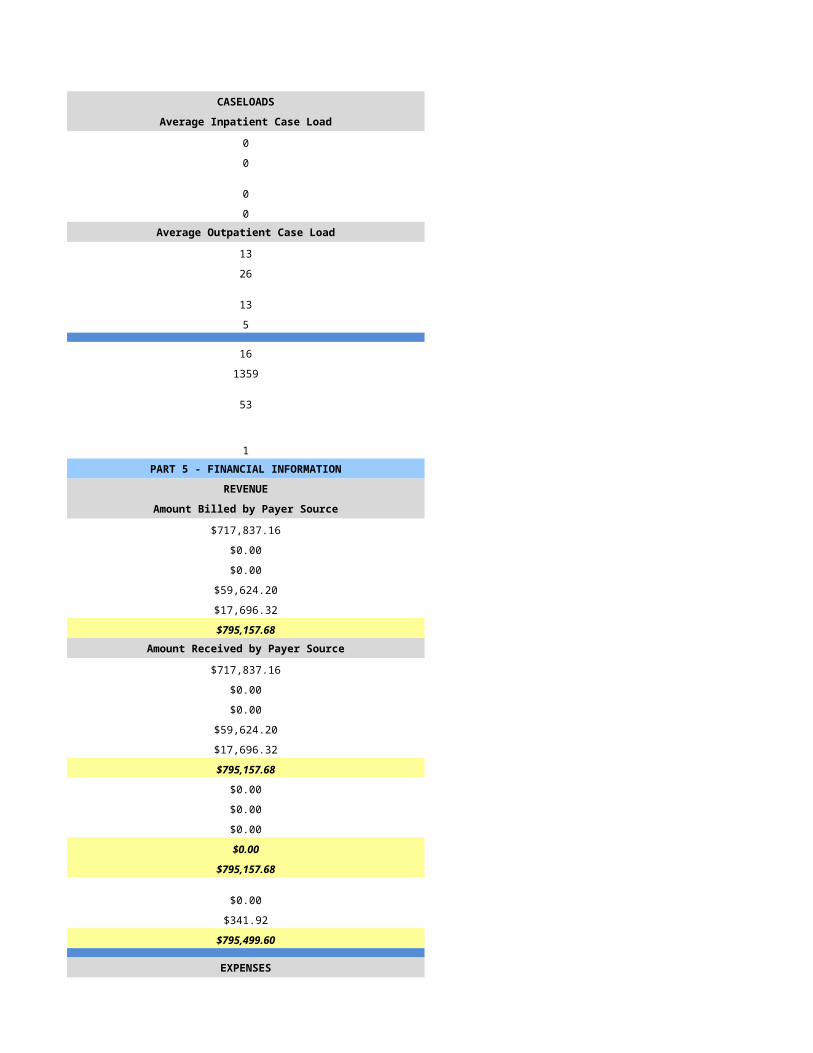
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
8 15
10 40
9 10
10 40
17 45
588 1102
93 308
13 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $4,834,057.40
$0.00 $49,659.36
$0.00 $0.00
$0.00 $27,639.30
$0.00 $0.00
$672,430.03 $4,911,356.06Amount Received by Payer Source Amount Received by Payer Source
$346,624.00 $4,834,057.40
$0.00 $49,659.36
$0.00 $0.00
$0.00 $27,639.30
$0.00 $0.00
$346,624.00 $4,911,356.06
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$346,624.00 $4,911,356.06
$0.00 $0.00
$4,201.00 $0.00
$350,825.00 $4,911,356.06
EXPENSES EXPENSES
$248,581.00 $2,028,697.83
$0.00 $0.00
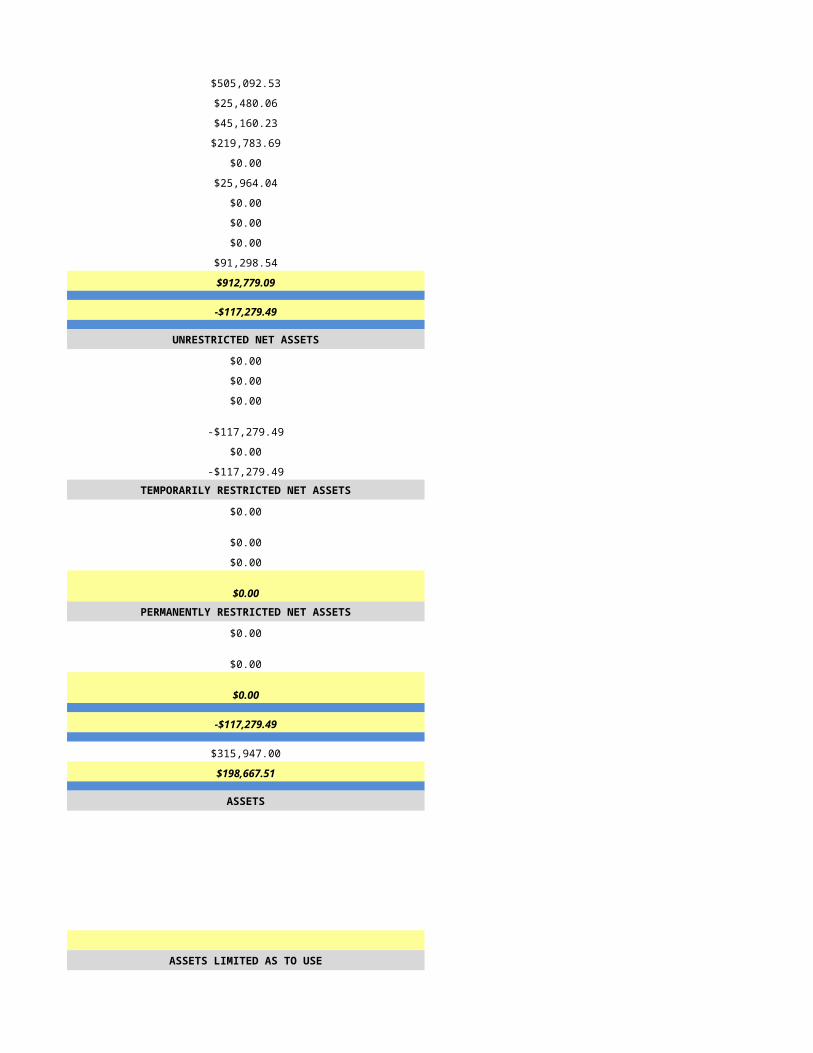
$34,484.00 $84,943.38
$58,224.00 $1,118,727.11
$3,762.00 $5,274.11
$34,624.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$39,146.00 $736,432.30
$418,821.00 $3,974,074.73
$0.00 $937,281.33
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$67,996.00 $937,281.33
$0.00 $0.00
-$67,996.00 $937,281.33TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $937,281.33
$0.00 $0.00
$0.00 $937,281.33
ASSETS ASSETS
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$0.00
$0.00
$0.00
$0.00
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$0.00
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/2/2015 6/3/2015
HSPC-7132 HSPC-4397
Hospice at Home of Arizona, LLC RTA Hospice, Inc.
Hospice at Home of Arizona Hospice Compassus - Bullhead City
7254 E. Southern Ave. Suite 111 1225 Hancock Road, Suite 200
Mesa Bullhead City
AZ AZ
85209 86442
Maricopa Mohave
480-478-0643 (928) 763-6433
Bonna Longo Cynthia Head
480-478-0643 (928) 763-6433
[email protected] [email protected]
Jon Longo Anthony James
480-478-0643 (615) 425-5418
[email protected] [email protected]
Jon Longo Emmy Nteziryayo
480-478-0643 (615) 425 5438
[email protected] [email protected]
03-1623 433947
1376986463 1063653236
Yes Yes
03-1623 03-1581
CHAP JCAHO
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Mixed Urban and Rural Mixed Urban and Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
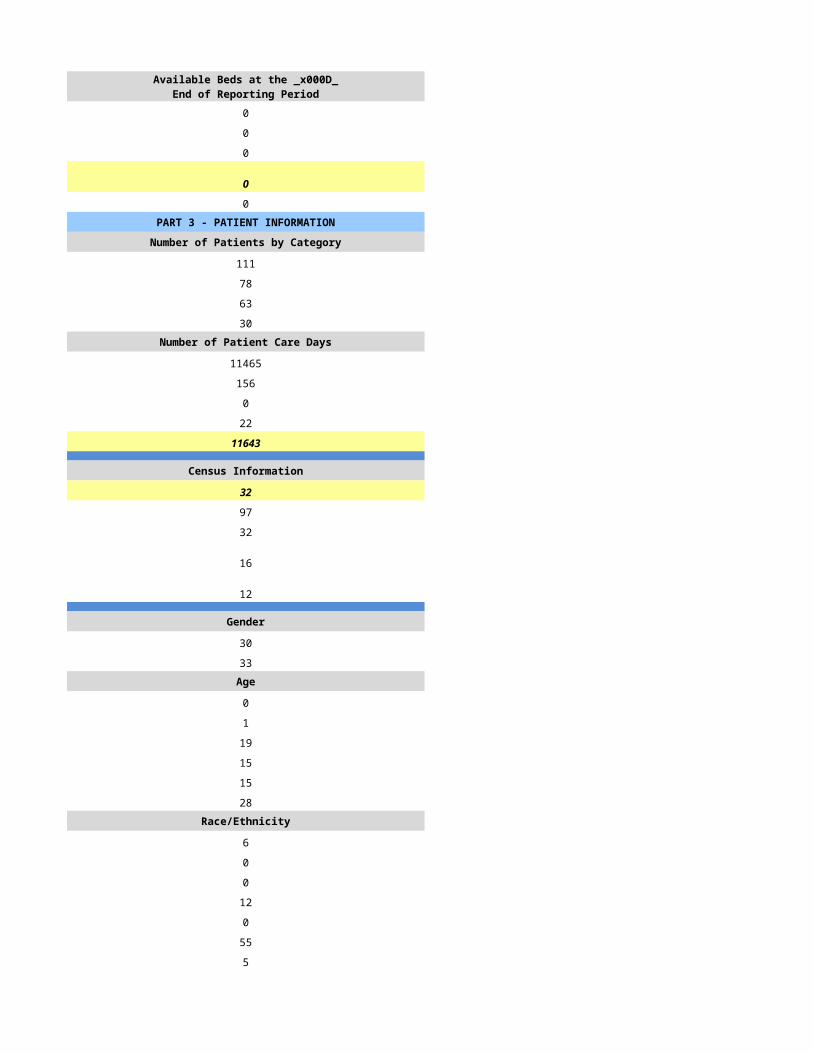
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
60 214
42 157
21 123
9 29Number of Patient Care Days Number of Patient Care Days
2766 10396
29 11
0 0
6 0
2801 10407
Census Information Census Information
8 29
70 68
6 21
10 42
1 12
Gender Gender
25 94
17 63Age Age
0 3
0 1
0 35
6 43
10 44
26 31Race/Ethnicity Race/Ethnicity
0 1
0 0
0 1
0 6
0 0
42 149
0 0Number of Admissions by Source Number of Admissions by Source
40 75
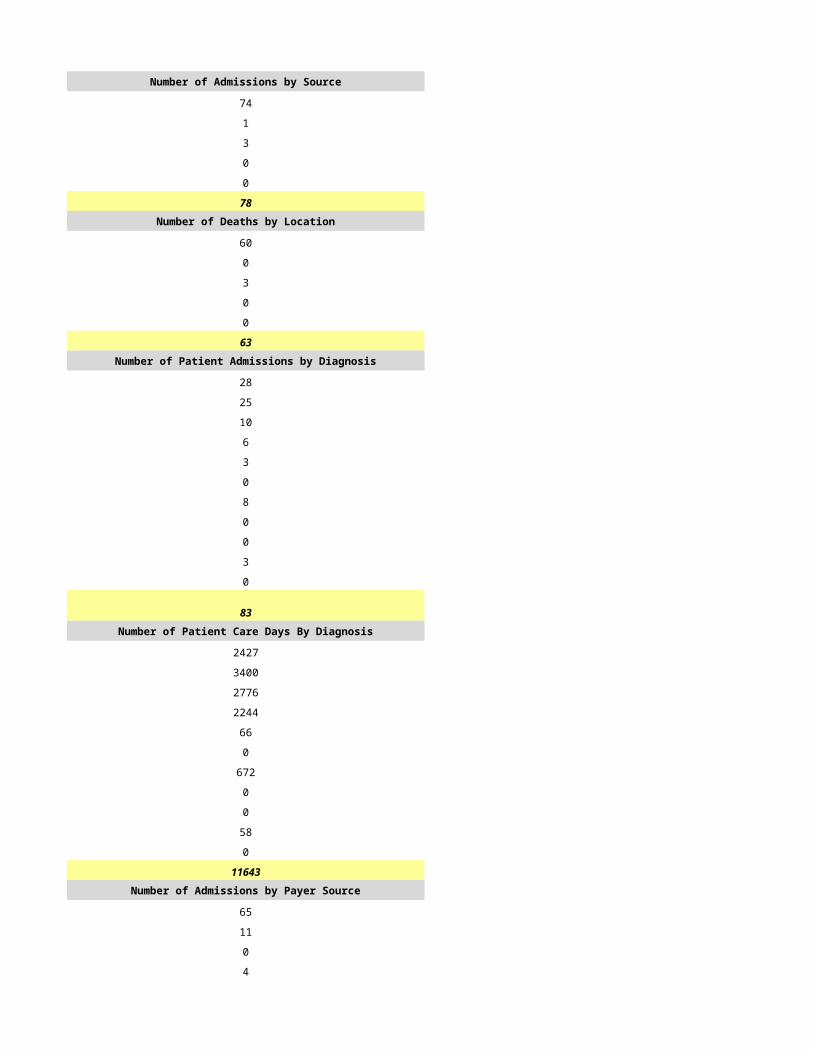
2 3
0 6
0 72
0 1
42 157Number of Deaths by Location Number of Deaths by Location
18 115
2 8
0 0
0 0
1 0
21 123Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
9 66
14 23
10 9
4 26
2 8
3 0
0 0
0 0
0 0
0 25
0 0
42 157Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
397 2365
1308 2365
707 473
182 1419
17 473
190 0
0 0
0 0
0 0
0 946
0 2366
2801 10407Number of Admissions by Payer Source Number of Admissions by Payer Source
42 135
0 15
0 0
0 7
0 0
42 157
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
2801 8945
0 981
0 0
0 481
0 0
2801 10407PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
4.5 5.1
1.3 1.4
1.3 3.1
1.2 0.0
0.0 0.0
0.5 1.8
8.7 11.4
2.5 4.2
0.0 1.1
11.2 16.7Home Hospice Visits Home Hospice Visits
1053 2644
108 873
615 2279
14 0
0 0
0 661
1790 6457
0 0
3 0
1793 6457Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
11.2 16.7
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
12 6
25 21
12 9
30 26
6 13
171 1173
77 0
2 0PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$429,428.86 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$429,428.86 $0.00Amount Received by Payer Source Amount Received by Payer Source
$385,624.50 $1,394,773.00
$0.00 $109,435.00
$0.00 $56,084.00
$0.00 $34,900.00
$0.00 $0.00
$385,624.50 $1,595,192.00
$0.00 $1,243.00
$0.00 $56,084.00
$0.00 $31,284.00
$0.00 $88,611.00
$385,624.50 $1,506,581.00
$50.00 $0.00
$2.29 $0.00
$385,676.79 $1,506,581.00
EXPENSES EXPENSES
$178,969.85 $702,913.00
$2,374.15 $30,000.00
$20,940.29 $128,928.00
$24,291.84 $152,500.00
$54,020.28 $2,080.00
$3,959.98 $2,002.00
$0.00 $466.00
$0.00 $5,839.00
$0.00 $45.00
$44,707.73 $217,193.00
$329,264.12 $1,241,966.00
$56,412.67 $264,615.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$56,412.67 $264,615.00
$12,499.98 $0.00
$68,912.65 $264,615.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$68,912.65 $264,615.00
$12,439.46 $0.00
$81,352.11 $264,615.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/4/2015 6/5/2015
HSPC-0038 HSPC-0017
RTA Hospice, Inc. RTA Hospice, Inc.
Hospice Compassus - Casa Grande Hospice Compassus - Payson
1675 E. Monument Plaza Drive 511 South Mudspring Road, Suite 1
Casa Grande Payson
AZ AZ
85222 85541
Pinal Gila
(520) 421-7143 (928) 472-6340
Cheryse Austin Mary Rogers
(520) 423-4345 (480) 251-0061
[email protected] [email protected]
Anthony James Anthony James
(615) 425-5418 (615) 425-5418
[email protected] [email protected]
Emmy Nteziryayo Emmy Nteziryayo
(615) 425 5438 (615) 425 5438
[email protected] [email protected]
164096 190992
1023048857 1568492395
Yes Yes
03-1521 03-1523
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency with one or more Inpatient Facilities
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Hospice Compassus - Payson
HSCP-3613
Payson
85541
Gila
(928) 472-6340
Mixed Urban and Rural Mixed Urban and Rural
Free Standing
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 7
0 0
0 0
0 7
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
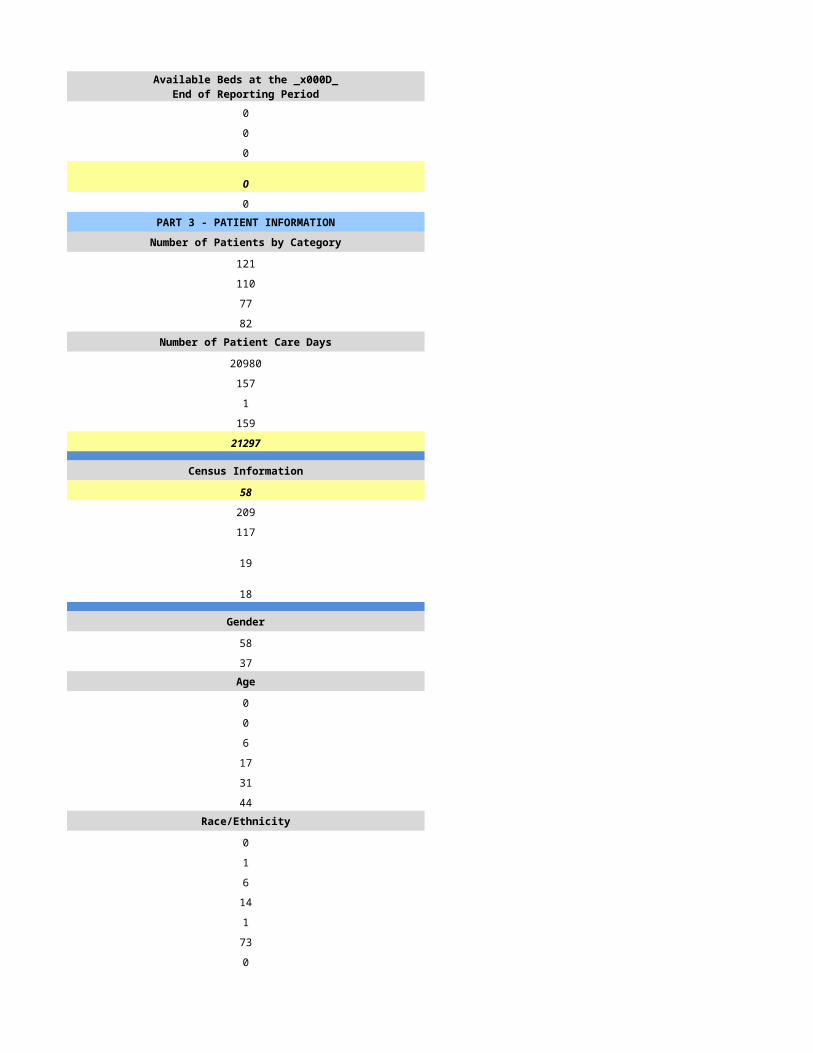
0 7
0 0
0 0
0 7
0 2PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
345 297
259 246
191 214
56 55Number of Patient Care Days Number of Patient Care Days
16901 29020
121 526
0 0
3 383
17025 29929
Census Information Census Information
47 82
78 115
22 29
68 83
18 27
Gender Gender
127 142
132 104Age Age
0 0
0 0
44 34
53 50
79 75
83 87Race/Ethnicity Race/Ethnicity
12 8
0 1
8 0
39 0
0 0
191 183
9 54Number of Admissions by Source Number of Admissions by Source
128 122
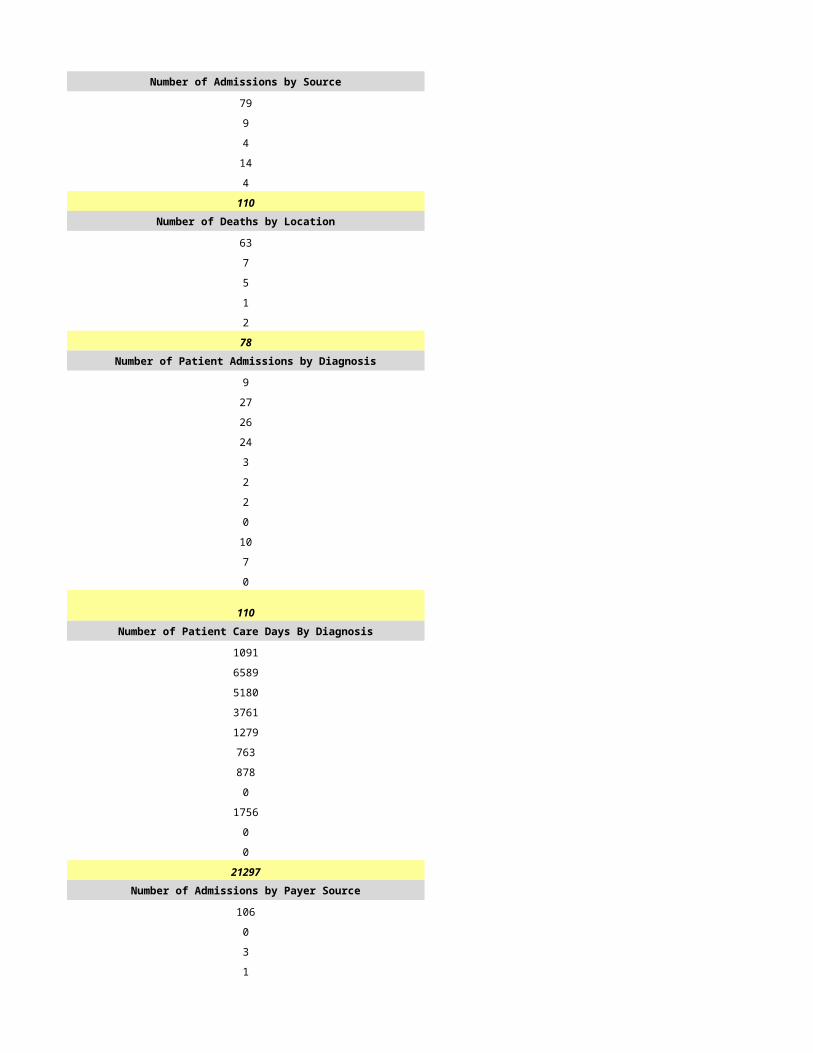
12 7
15 32
103 80
1 5
259 246Number of Deaths by Location Number of Deaths by Location
143 92
16 12
30 47
2 0
0 63
191 214Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
93 76
23 52
41 27
33 44
14 4
0 0
0 0
0 0
0 0
55 43
0 0
259 246Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
1980 2363
3564 7876
4752 3938
1188 5119
396 394
0 0
0 0
0 0
0 0
2373 2363
2772 7876
17025 29929Number of Admissions by Payer Source Number of Admissions by Payer Source
246 228
5 8
0 0
8 10
0 0
259 246
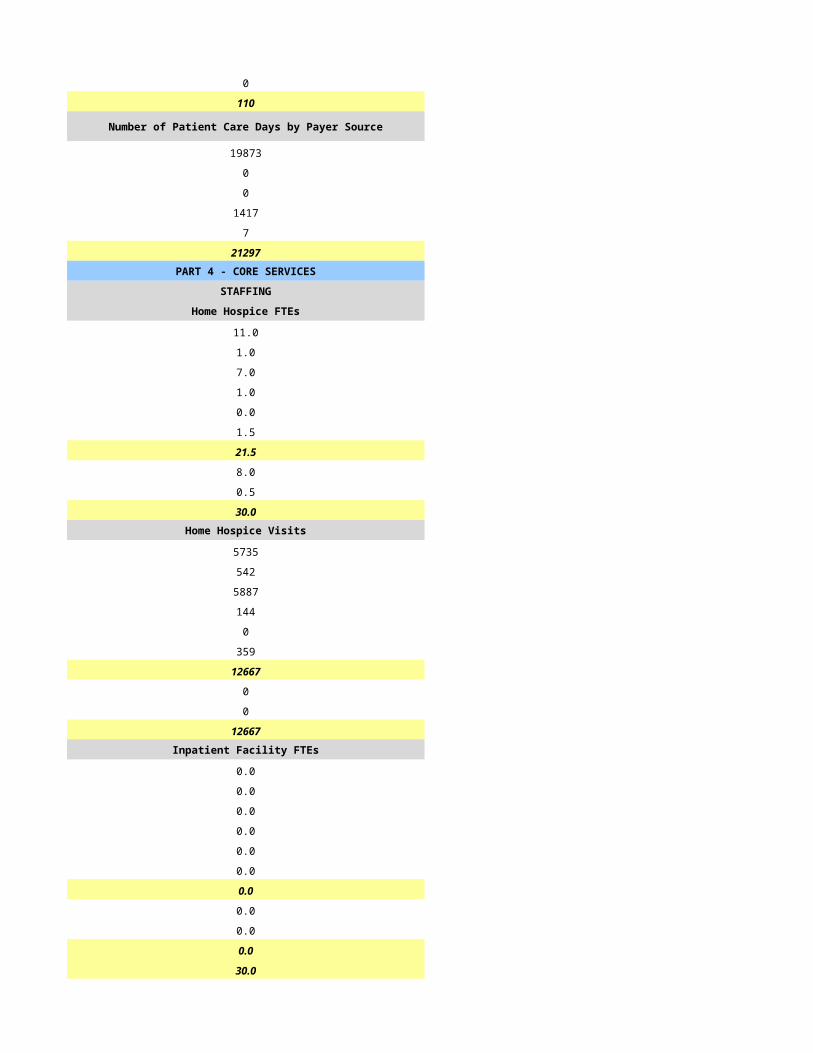
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
16215 27718
305 971
0 0
505 1240
0 0
17025 29929PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
7.2 9.0
1.1 2.3
4.0 6.4
0.0 0.0
0.0 0.0
5.0 12.2
17.3 29.9
5.4 5.2
0.1 1.1
22.8 36.2Home Hospice Visits Home Hospice Visits
6771 2644
1041 873
4681 2279
0 0
0 0
1200 661
13693 6457
0 0
0 0
13693 6457Inpatient Facility FTEs Inpatient Facility FTEs
0.0 4.4
0.0 0.0
0.0 3.8
0.0 0.0
0.0 0.0
0.0 0.0
0.0 8.2
0.0 0.0
0.0 0.0
0.0 8.2
22.8 44.4
CASELOADS CASELOADS
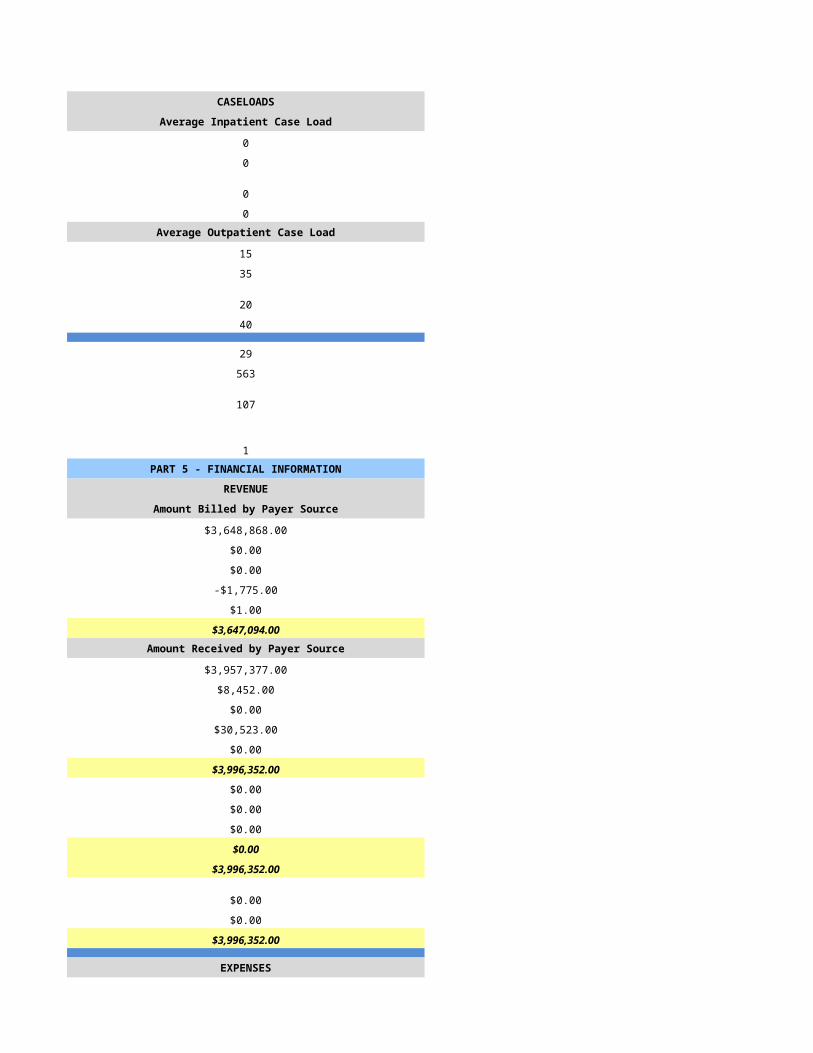
Average Inpatient Case Load Average Inpatient Case Load
0 1
0 0
0 1
0 0Average Outpatient Case Load Average Outpatient Case Load
7 9
42 34
12 12
32 45
17 23
883 866
0 0
0 0PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$2,660,590.00 $4,364,077.00
$41,238.00 $190,554.00
$48,683.00 $81,689.00
$27,937.00 $90,975.00
$50.00 $0.00
$2,778,498.00 $4,727,295.00
$2,943.00 $2,421.00
$48,683.00 $81,689.00
$57,349.00 $89,461.00
$108,975.00 $173,571.00
$2,669,523.00 $4,553,724.00
$0.00 $0.00
$0.00 $0.00
$2,669,523.00 $4,553,724.00
EXPENSES EXPENSES
$1,082,625.00 $2,064,319.00
$51,540.00 $87,240.00
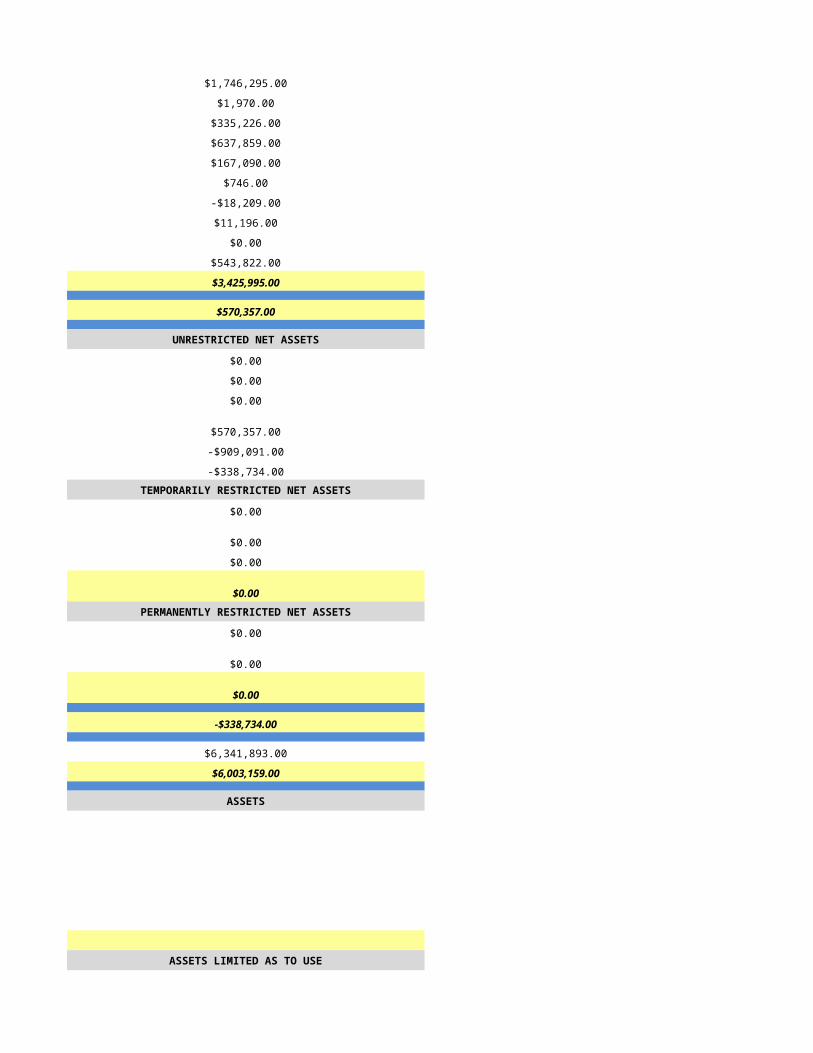
$201,388.00 $407,743.00
$379,815.00 $511,057.00
$7,907.00 $5,644.00
$3,159.00 $5,660.00
$2,950.00 $0.00
$52,018.00 $8,293.00
$67.00 $43.00
$310,993.00 $422,679.00
$2,092,462.00 $3,512,678.00
$577,061.00 $1,041,046.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$577,061.00 $1,041,046.00
$0.00 $0.00
$577,061.00 $1,041,046.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$577,061.00 $1,041,046.00
$0.00 $0.00
$577,061.00 $1,041,046.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
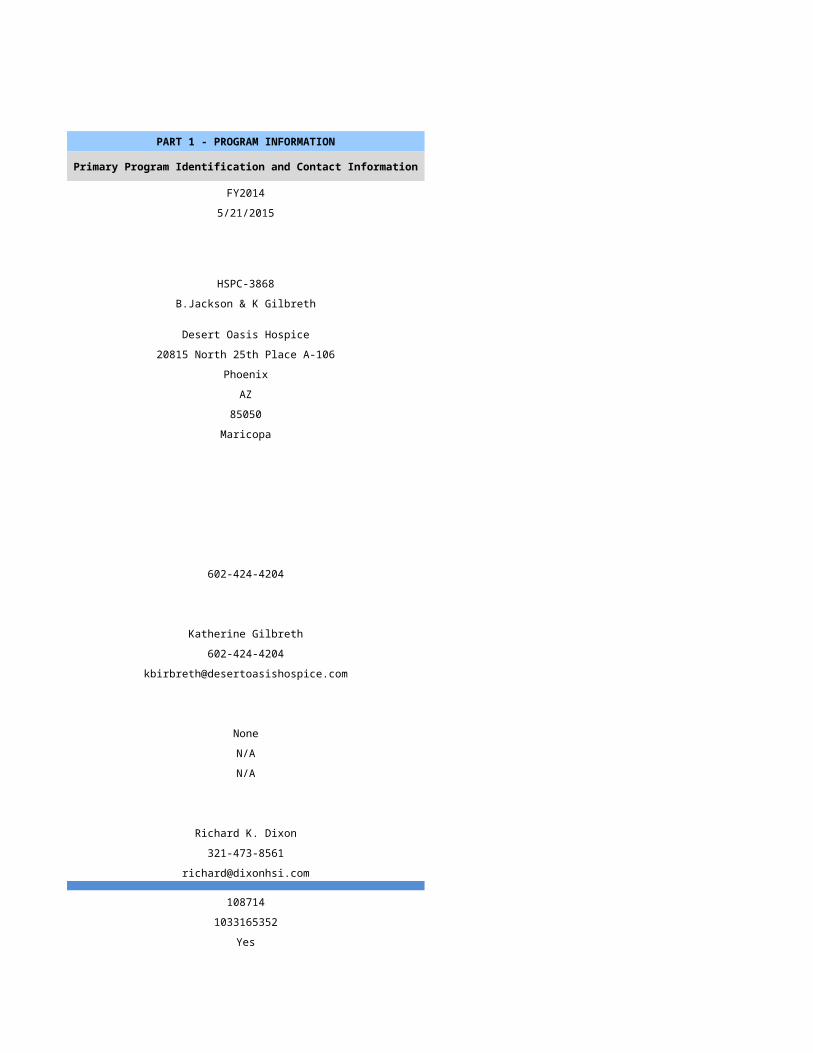
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/6/2015 6/7/2015
HSPC-3729 HSPC-2047
RTA Hospice, Inc. RTA Hospice, Inc.
Hospice Compassus - Sedona Flagstaff Hospice Compassus - White Mountain
70 Bell Rock Plaza, Suite A 1789 West Commerce Drive, Suite A
Sedona Lakeside
AZ AZ
86351 85929
Coconino Navajo
(928) 284-0180 (928) 368-4400
Susan Blanchard Debra Brackey
(928) 202-7307 (928) 368-7140
[email protected] [email protected]
Anthony James Anthony James
(615) 425-5418 (615) 425-5418
[email protected] [email protected]
Emmy Nteziryayo Emmy Nteziryayo
(615) 425 5438 (615) 425 5438
[email protected] [email protected]
954918 579906
1457381295 1568492304
Yes Yes
03-1560 03-1550
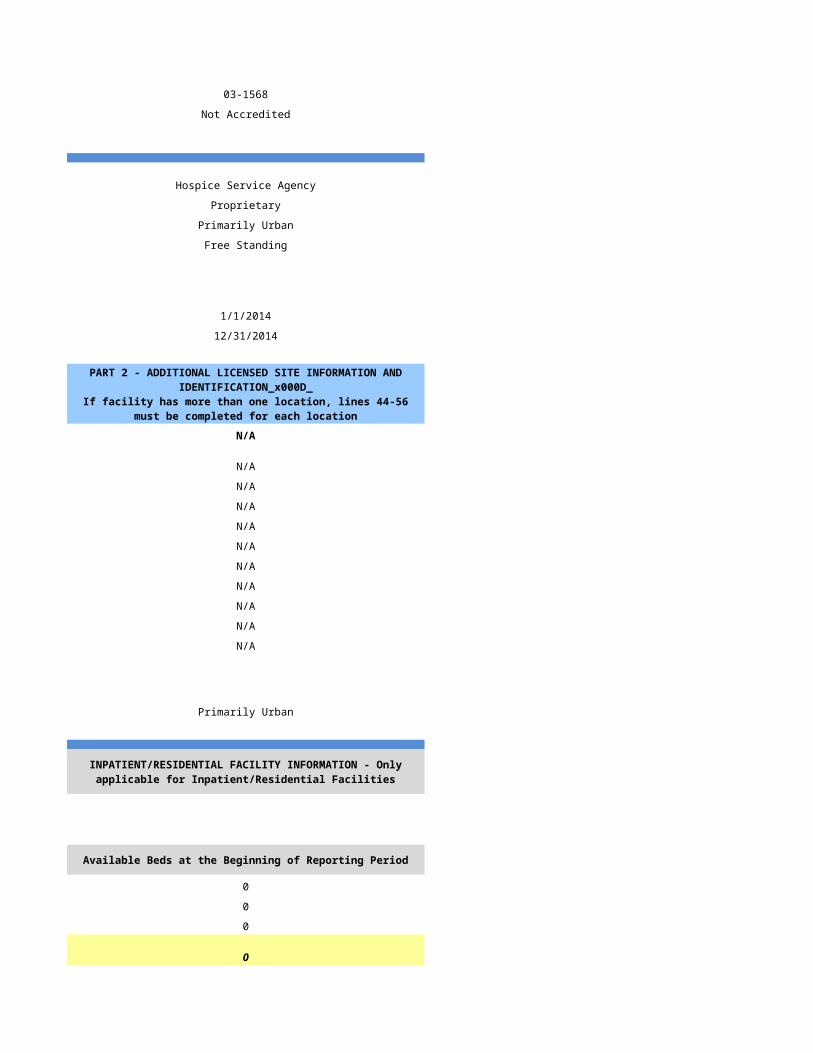
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Mixed Urban and Rural Mixed Urban and Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
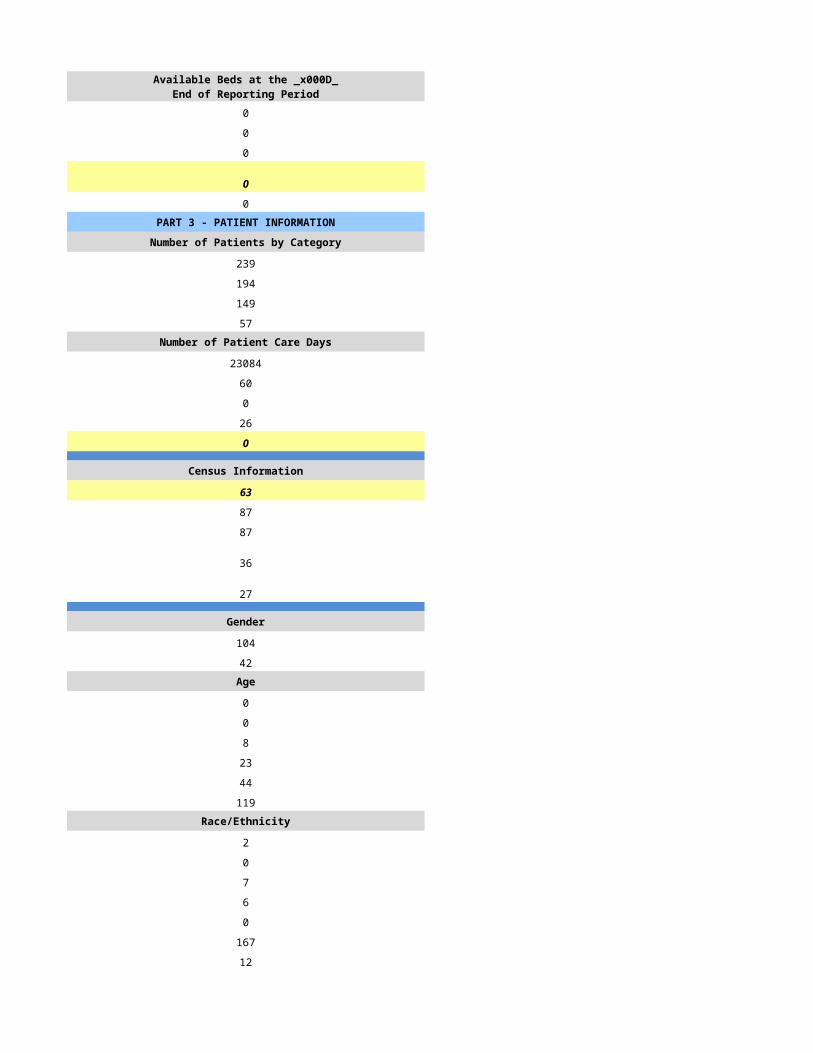
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
964 460
721 353
518 279
262 66Number of Patient Care Days Number of Patient Care Days
90079 30193
669 168
0 0
213 146
90961 30507
Census Information Census Information
249 84
129 81
54 30
127 79
77 25
Gender Gender
403 180
318 173Age Age
0 0
1 1
93 46
114 77
197 106
316 123Race/Ethnicity Race/Ethnicity
74 25
1 0
11 1
33 17
2 0
580 300
20 10Number of Admissions by Source Number of Admissions by Source
472 166
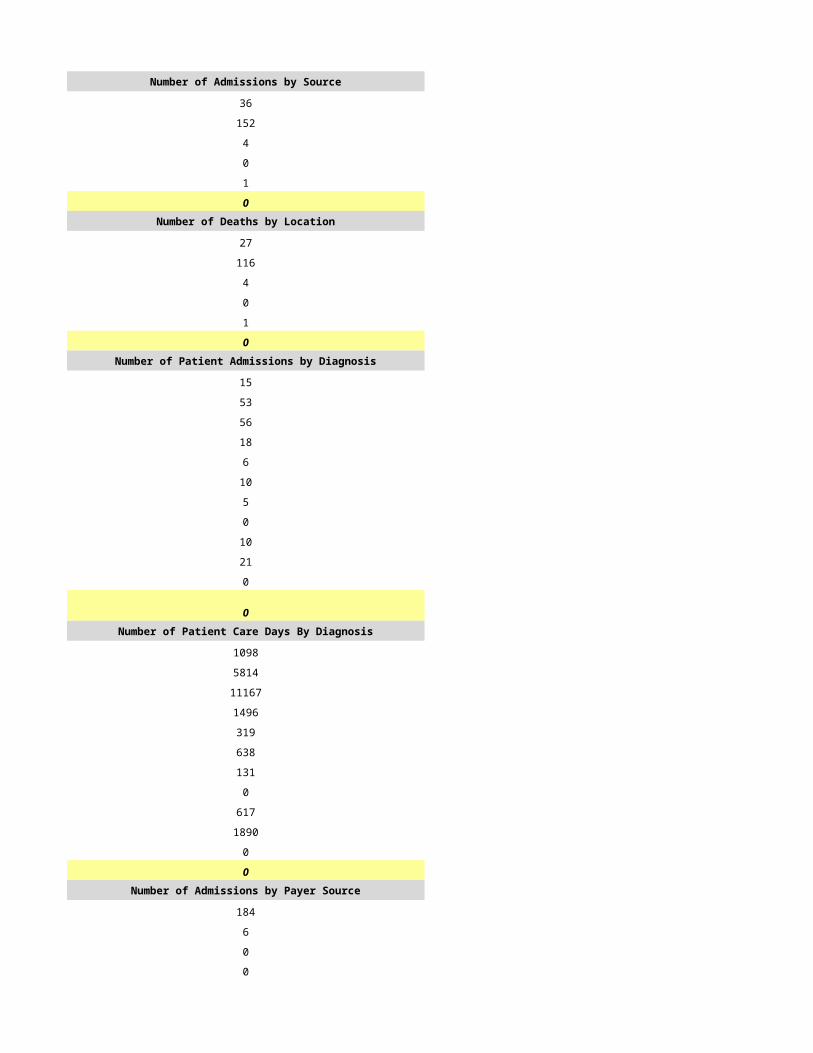
68 35
7 5
166 144
8 3
721 353Number of Deaths by Location Number of Deaths by Location
327 208
88 37
99 16
3 18
1 0
518 279Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
194 100
180 94
70 58
94 54
6 7
0 0
0 0
0 0
0 0
175 40
2 0
721 353Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
14851 5649
18563 2260
14851 3955
11138 5085
619 0
0 0
0 0
0 0
0 0
4950 0
25989 13558
90961 30507Number of Admissions by Payer Source Number of Admissions by Payer Source
668 339
23 3
0 0
30 11
0 0
721 353
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
84320 29277
2885 263
0 0
3756 967
0 0
90961 30507PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
17.9 9.2
5.2 2.1
16.2 5.9
0.0 0.0
0.0 0.0
25.3 10.1
64.6 27.3
11.9 5.1
2.1 0.1
78.6 32.5Home Hospice Visits Home Hospice Visits
21686 9040
5647 1522
22272 6293
0 0
0 0
6462 3531
56067 20386
0 0
20 0
56087 20386Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
78.6 32.5
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
14 9
48 40
15 14
59 56
39 29
1945 1599
0 0
0 0PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$15,034,511.00 $4,482,980.00
$465,260.00 $30,906.00
$191,697.00 $74,483.00
$283,228.00 $31,637.00
$13.00 $0.00
$15,974,709.00 $4,620,006.00
$5,841.00 $746.00
$191,697.00 $74,483.00
$1,179,154.00 $93,010.00
$1,376,692.00 $168,239.00
$14,598,017.00 $4,451,767.00
$0.00 $0.00
$0.00 $0.00
$14,598,017.00 $4,451,767.00
EXPENSES EXPENSES
$4,276,555.00 $1,530,629.00
$302,521.00 $115,511.00
$698,023.00 $291,196.00
$1,811,455.00 $692,321.00
$11,884.00 $4,387.00
$14,527.00 $5,280.00
$38,966.00 $3,615.00
$26,706.00 $72,008.00
$103.00 $25.00
$771,437.00 $364,476.00
$7,952,177.00 $3,079,448.00
$6,645,840.00 $1,372,319.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$6,645,840.00 $1,372,319.00
$0.00 $0.00
$6,645,840.00 $1,372,319.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$6,645,840.00 $1,372,319.00
$0.00 $0.00
$6,645,840.00 $1,372,319.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/8/2015 6/9/2015
HSPC-4172 HSPC-0044
RTA Hospice, Inc. Hospice Family Care, Inc.
Hospice Compassus - Yuma Hospice Family Care, Inc.
1025 West 24th Street, Suite 15 1550 S. Alma School Road
Yuma Mesa
AZ AZ
85364 85210-2109
Yuma Maricopa
Same as Above
(928) 344-6100 (480) 461-3144
Amberly Davis-Owens Jody Phister
(928) 446-9375 (480) 461-3144
[email protected] [email protected]
Anthony James Ron Marino
(615) 425-5418 (704) 662-1764
[email protected] [email protected]
Emmy Nteziryayo Dale Martin
(615) 425 5438 (704) 662-1770
[email protected] [email protected]
325400 408650
1659432243 1518943919
Yes Yes
03-1573 03-1537
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency with no Inpatient Facilities
Proprietary Proprietary
Mixed Urban and Rural Primarily Urban
Free Standing Free Standing
0
1/1/2014 1/1/2014
12/31/2014 12/31/2014
(999) 999-9999
mm/dd/yyyy
Mixed Urban and Rural Primarily Urban
0
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
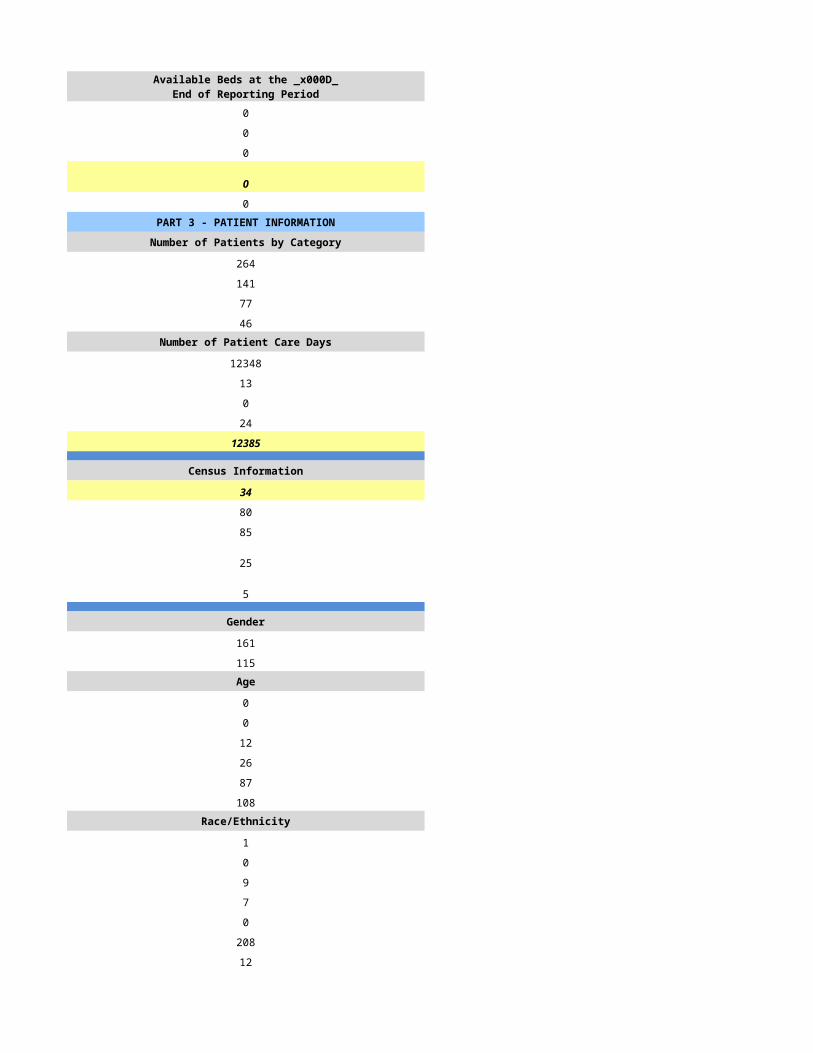
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
537 451
410 379
270 212
181 121Number of Patient Care Days Number of Patient Care Days
59626 47649
489 347
0 343
71 800
60186 49139
Census Information Census Information
165 135
143 56
62 123
68 36
47 49
Gender Gender
198 194
212 176Age Age
0 0
2 1
55 37
70 70
147 109
136 162Race/Ethnicity Race/Ethnicity
1 4
0 1
2 10
138 18
1 1
242 324
26 21Number of Admissions by Source Number of Admissions by Source
197 249
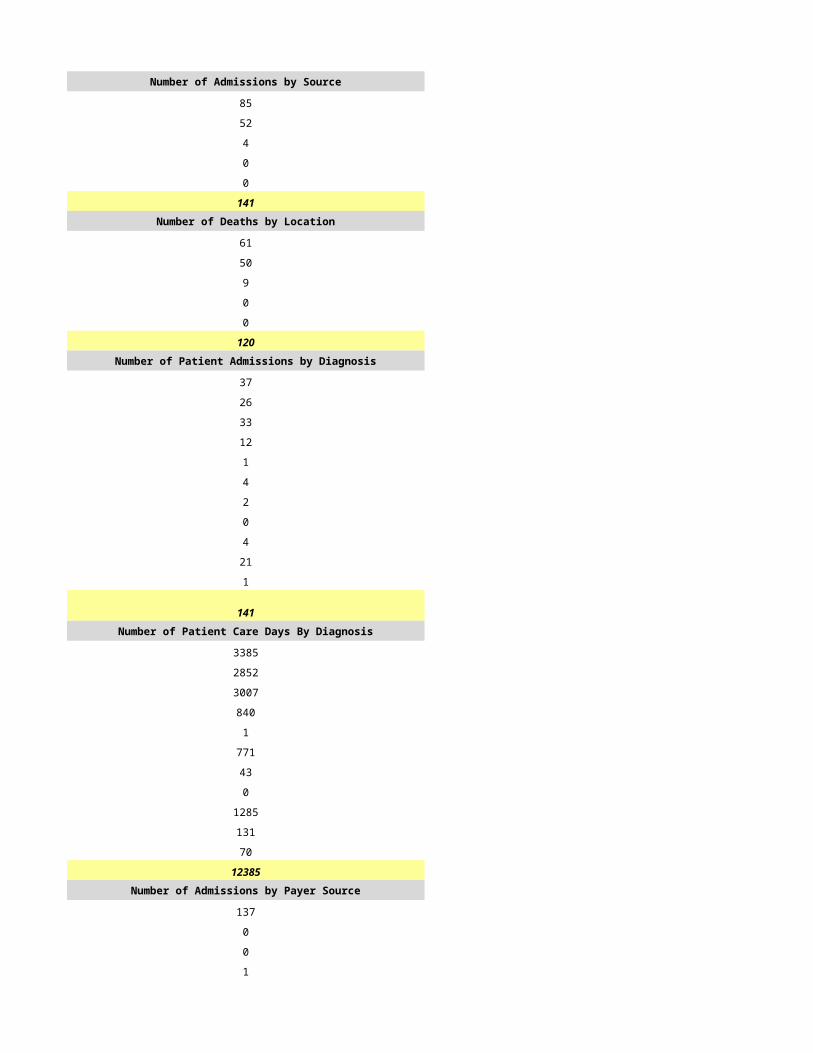
35 96
91 11
83 23
4 0
410 379Number of Deaths by Location Number of Deaths by Location
175 123
39 68
56 7
0 14
0 0
270 212Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
75 86
166 114
43 68
33 54
8 11
0 1
0 6
0 0
0 14
85 25
0 0
410 379Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
8897 6431
16224 14729
6280 13567
5234 6967
0 611
0 6
0 403
0 0
0 2254
4187 3371
19364 0
60186 48339Number of Admissions by Payer Source Number of Admissions by Payer Source
374 336
16 0
0 0
20 20
0 23
410 379
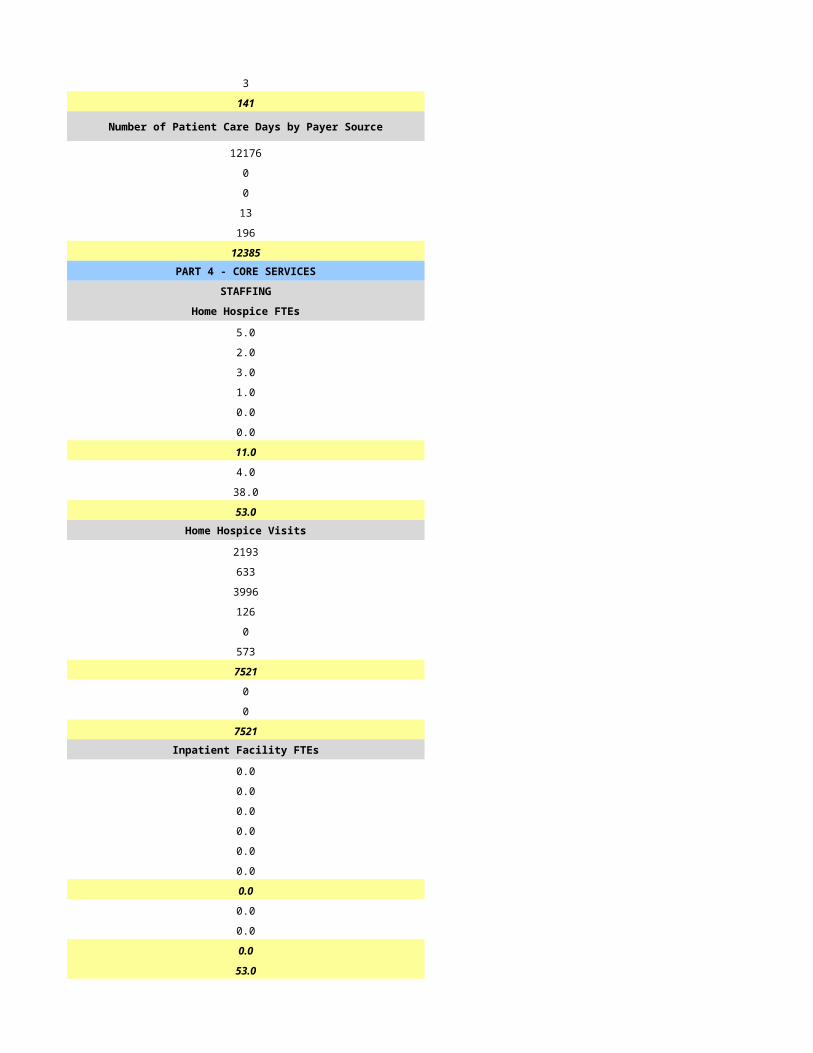
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
54963 46032
2326 0
0 0
2897 1456
0 851
60186 48339PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
15.8 12.4
3.1 3.5
14.4 10.2
0.0 0.0
0.0 0.0
14.0 2.0
47.3 28.1
7.1 0.0
1.1 1.3
55.5 29.4Home Hospice Visits Home Hospice Visits
20841 12627
4055 3238
18250 12598
0 0
0 0
4320 0
47466 28463
0 0
0 296
47466 28759Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
55.5 29.4
CASELOADS CASELOADS
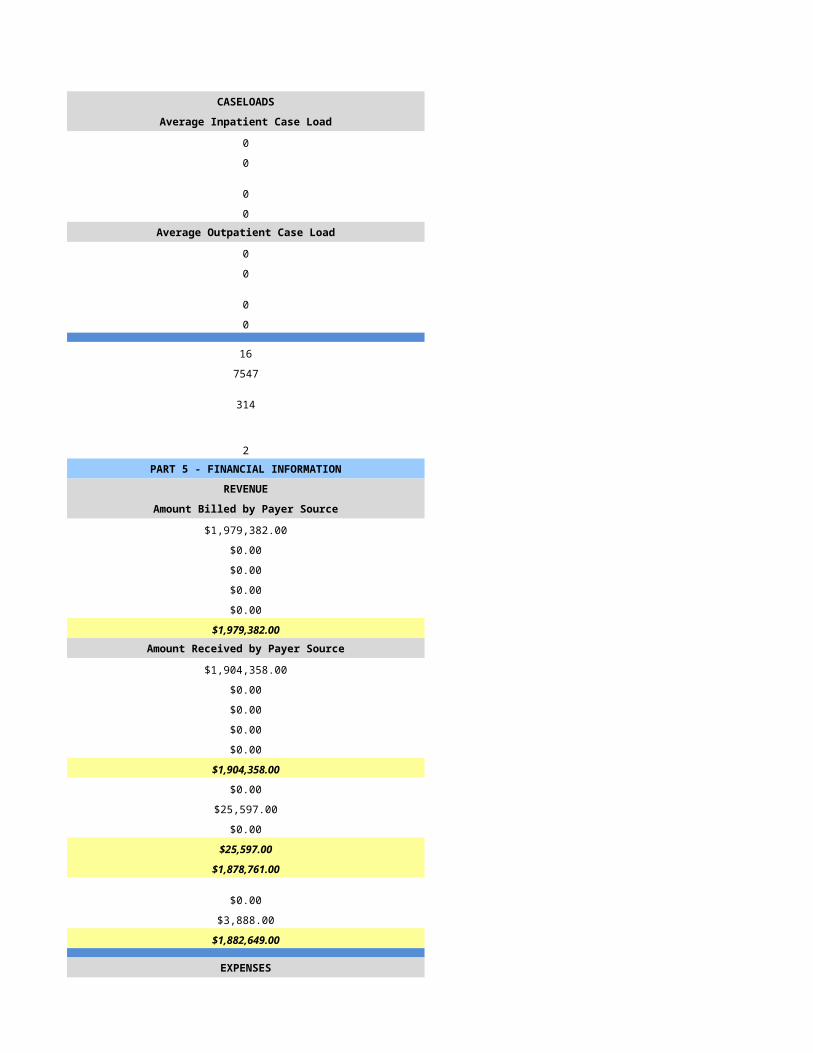
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
10 12
54 35
11 12
60 60
53 17
1634 2078
0 400
0 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $7,931,671.00
$0.00 $0.00
$0.00 $0.00
$0.00 $218,924.00
$0.00 $0.00
$0.00 $8,150,595.00Amount Received by Payer Source Amount Received by Payer Source
$8,514,307.00 $7,931,671.00
$266,433.00 $0.00
$320,437.00 $0.00
$108,617.00 $218,924.00
$39.00 $0.00
$9,209,833.00 $8,150,595.00
$25,142.00 $0.00
$320,437.00 $0.00
$252,871.00 $39,132.00
$598,450.00 $39,132.00
$8,611,383.00 $8,111,463.00
$0.00 $0.00
$0.00 $55,210.00
$8,611,383.00 $8,166,673.00
EXPENSES EXPENSES
$2,742,511.00 $3,416,751.00
$196,238.00 $332,206.00
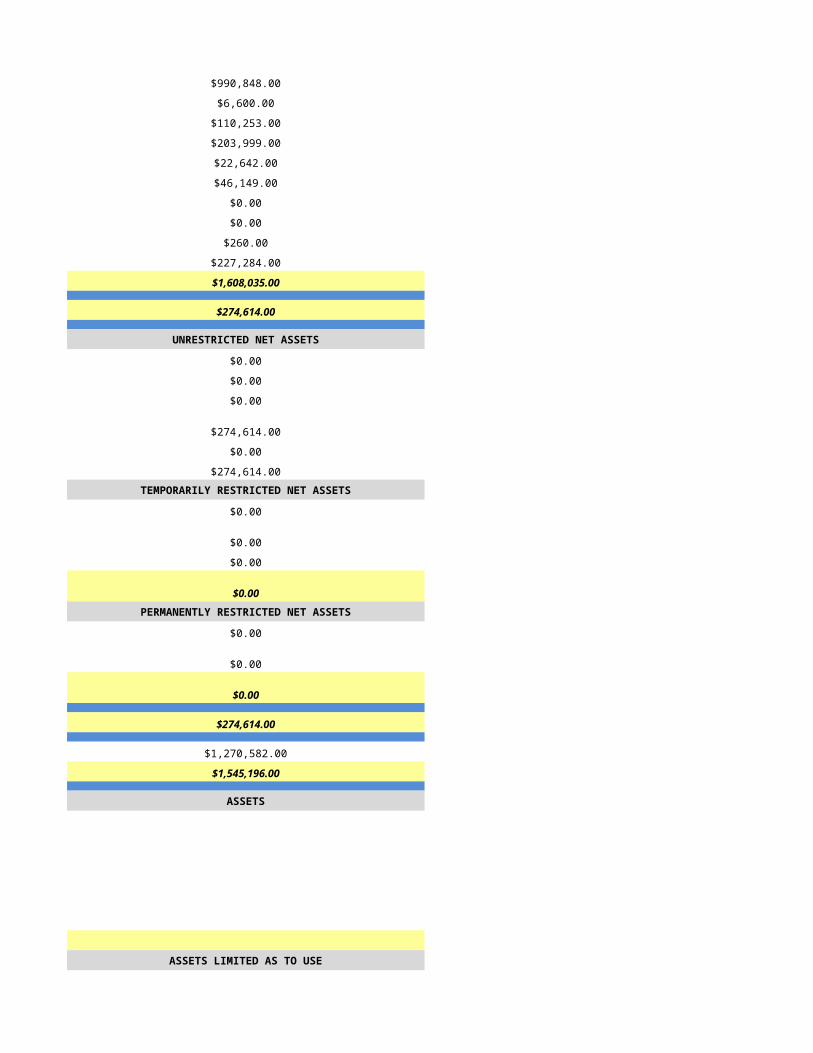
$439,528.00 $549,932.00
$1,060,457.00 $910,440.00
$8,399.00 $0.00
$10,691.00 $0.00
$4,427.00 $193,553.00
$20,910.00 $63,753.00
$64.00 $0.00
$387,756.00 $832,177.00
$4,870,981.00 $6,298,812.00
$3,740,402.00 $1,867,861.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$3,740,402.00 $1,867,861.00
$0.00 $0.00
$3,740,402.00 $1,867,861.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$3,740,402.00 $1,867,861.00
$0.00 $0.00
$3,740,402.00 $1,867,861.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/10/2015 6/11/2015
HSPC-0050 HSPC-0011
Hospice of Arizona, LLC HOSPICE OF HAVASU, INC.
Hospice of Arizona HOSPICE OF HAVASU, INC.
19820 N 7th Ave S, Suite 130 365 S. LAKE HAVASU AVENUE
Phoenix LAKE HAVASU CITY
AZ AZ
85027 86403-9368
Maricopa MOHAVE
same as above PO BOX 597
LAKE HAVASU CITY
AZ
86405-0597
MOHAVE
602-678-1313 (928) 453-2111
Carol Maclean DANIEL MATHEWS
602-678-1313 (928) 453-2111
[email protected] [email protected]
Don Borchert RUTHANNE DEWITT
469-363-3422 (928) 453-2111
[email protected] [email protected]
Don Borchert WILLIAM J. BEHRENS, CPA, MPA
469-363-3422 (304) 624-5471
[email protected] [email protected]
193475 421412
1992714778 1649254517
Yes Yes
31525 03-1543
CHAP Not Accredited
Hospice Service Agency with one or more Inpatient Facilities Hospice Service Agency with one or more Inpatient Facilities
Proprietary Voluntary (Not For Profit)
Mixed Urban and Rural Primarily Rural
Free Standing Free Standing
38
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Hospice of Arizona POLIDORI HOUSE
HSCP-0050 HSCP-4682
19820 N 7th Ave, Suite 130 1970 BAHAMA AVENUE
Phoenix LAKE HAVASU CITY
85027 86403-3607
Maricopa MOHAVE
same as above PO BOX 597
LAKE HAVASU CITY
86405-0597
MOHAVE
602-678-1313 (928) 453-2111
n/a
Mixed Urban and Rural Primarily Rural
Free Standing Free Standing
38
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 6
0 6
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
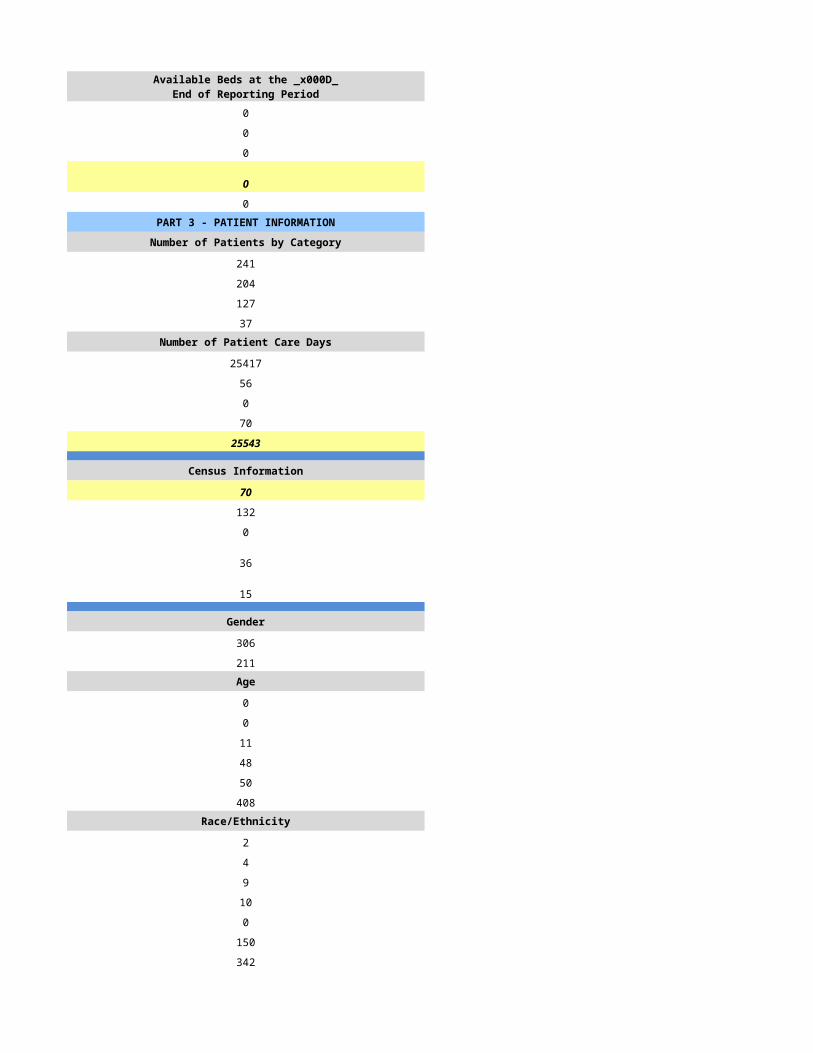
0 0
0 0
0 6
0 6
0 3PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
1790 725
1101 482
883 424
324 50Number of Patient Care Days Number of Patient Care Days
96517 41683
698 260
1 0
6236 767
103452 42710
Census Information Census Information
283 117
109 76
20 14
351 160
109 49
Gender Gender
753 334
583 271Age Age
0 0
5 0
133 52
176 116
302 189
720 248Race/Ethnicity Race/Ethnicity
1 6
24 2
41 1
74 7
0 5
961 584
0 0Number of Admissions by Source Number of Admissions by Source
278 279
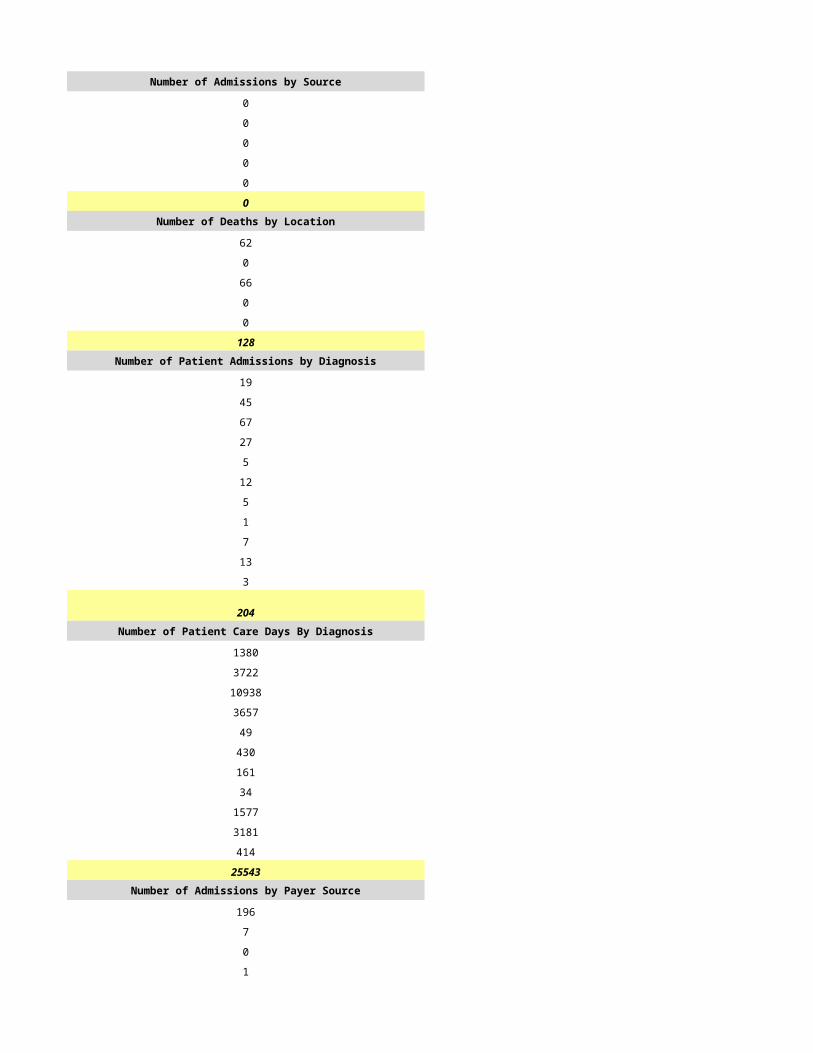
337 91
480 11
6 22
0 79
1101 482Number of Deaths by Location Number of Deaths by Location
132 204
199 91
78 19
5 20
469 90
883 424Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
259 169
280 112
125 50
0 55
35 17
91 14
23 11
0 0
9 13
1 41
278 0
1101 482Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
14232 6058
24742 13800
26071 7487
0 6026
656 1114
6085 3031
929 512
0 0
1307 3468
151 1214
29279 0
103452 42710Number of Admissions by Payer Source Number of Admissions by Payer Source
968 441
0 15
1 0
109 21
23 5
1101 482
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
96611 40370
0 497
138 0
5951 1379
752 464
103452 42710PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
48.9 19.7
6.9 11.2
30.2 13.5
0.0 0.2
0.0 0.0
0.0 5.6
86.0 50.2
33.5 23.2
2.0 5.0
121.5 78.4Home Hospice Visits Home Hospice Visits
76579 13584
5734 3997
69453 15725
1348 473
0 0
0 0
153114 33779
0 0
0 628
153114 34407Inpatient Facility FTEs Inpatient Facility FTEs
13.1 4.2
1.7 1.0
4.1 4.0
0.0 0.0
0.0 0.0
0.0 0.0
18.9 9.2
1.0 0.0
0.0 0.0
19.9 9.2
141.4 87.6
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
14 1
38 3
11 1
102 0Average Outpatient Case Load Average Outpatient Case Load
14 10
38 10
11 9
102 36
120 216
9536 17631
0 1466
0 5PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $6,679,737.04
$0.00 $198,619.08
$0.00 $637.54
$0.00 $144,172.54
$0.00 $72,955.10
$0.00 $7,096,121.30Amount Received by Payer Source Amount Received by Payer Source
$17,565,162.00 $6,679,737.04
$0.00 $198,619.08
$0.00 $637.54
$615,405.00 $144,172.54
$0.00 $72,955.10
$18,180,567.00 $7,096,121.30
$0.00 $0.00
$0.00 $72,640.30
$0.00 $283,964.80
$0.00 $356,605.10
$18,180,567.00 $6,739,516.20
$0.00 $0.00
$0.00 $1,115,972.35
$18,180,567.00 $7,855,488.55
EXPENSES EXPENSES
$7,879,488.00 $4,593,069.38
$939,387.00 $1,524.00
$1,634,411.00 $983,851.90
$2,780,770.00 $906,102.90
$92,755.00 $20,868.00
$48,089.00 $58,591.00
$0.00 $0.00
$1,714,406.00 $176,376.88
$54,370.00 $39,816.36
$6,582,047.00 $638,771.76
$21,725,723.00 $7,418,972.18
-$3,545,156.00 $436,516.37
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 -$41,094.96
$0.00 $0.00
$0.00 $0.00
-$3,545,156.00 $395,421.41
$0.00 $0.00
-$3,545,156.00 $395,421.41TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 -$3,515.46
$0.00 -$12,647.56
$0.00 -$16,163.02PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$3,545,156.00 $379,258.39
-$1,638,499.00 $8,549,223.16
-$5,183,655.00 $8,928,481.55
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/12/2015 6/13/2015
HSPC-4682 HSPC-3721
HOSPICE OF HAVASU, INC. (HSPC-0011) Hospice of Phoenix
HOSPICE OF HAVASU, INC. (HSPC-0011) Hospice of the Pines
13175 East Highway 169
Dewey
AZ AZ
86327
Mohave Yavapai
P O Box 47090
Phoenix
AZ
86327
Maricopa
928-632-0111
Beth Funk
928-632-0111
Satty Bhowra
602-550-4065
Satty Bhowra
602-550-4065
950437
11342443157
Yes
03-1559
Not Accredited
Hospice Service Agency
Proprietary
Primarily Rural
Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
POLIDORI HOUSE
HSPC-4682 HSCP-9999
1970 BAHAMA AVENUE
LAKE HAVASU CITY
86403-3607
MOHAVE
PO BOX 597
LAKE HAVASU CITY
86405-0597
MOHAVE
(928) 453-2111 (999) 999-9999
mm/dd/yyyy
Primarily Rural
Free Standing
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
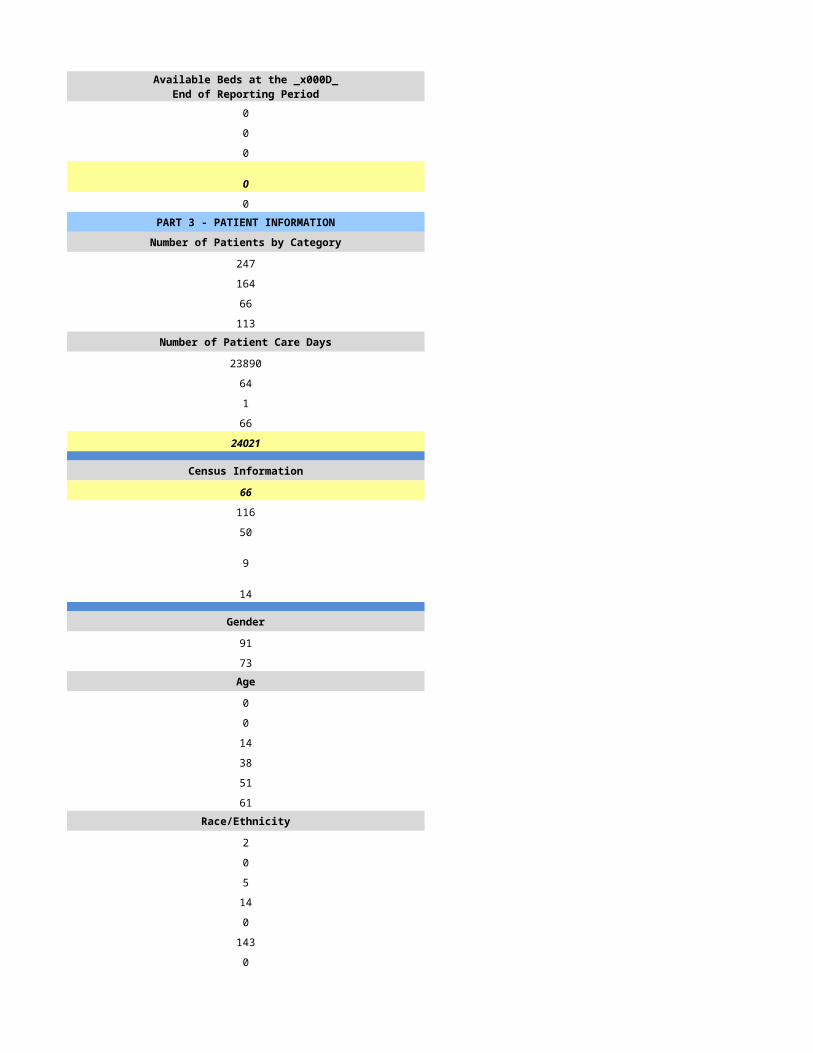
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
0 220
0 190
0 163
0 39Number of Patient Care Days Number of Patient Care Days
0 19111
0 202
0 0
0 39
0 19352
Census Information Census Information
0 53
0 101
0 50
0 35
0 36
Gender Gender
0 132
0 108Age Age
0 1
0 1
0 23
0 44
0 56
0 115Race/Ethnicity Race/Ethnicity
0 5
0 0
0 0
0 9
0 0
0 226
0 0Number of Admissions by Source Number of Admissions by Source
0 153
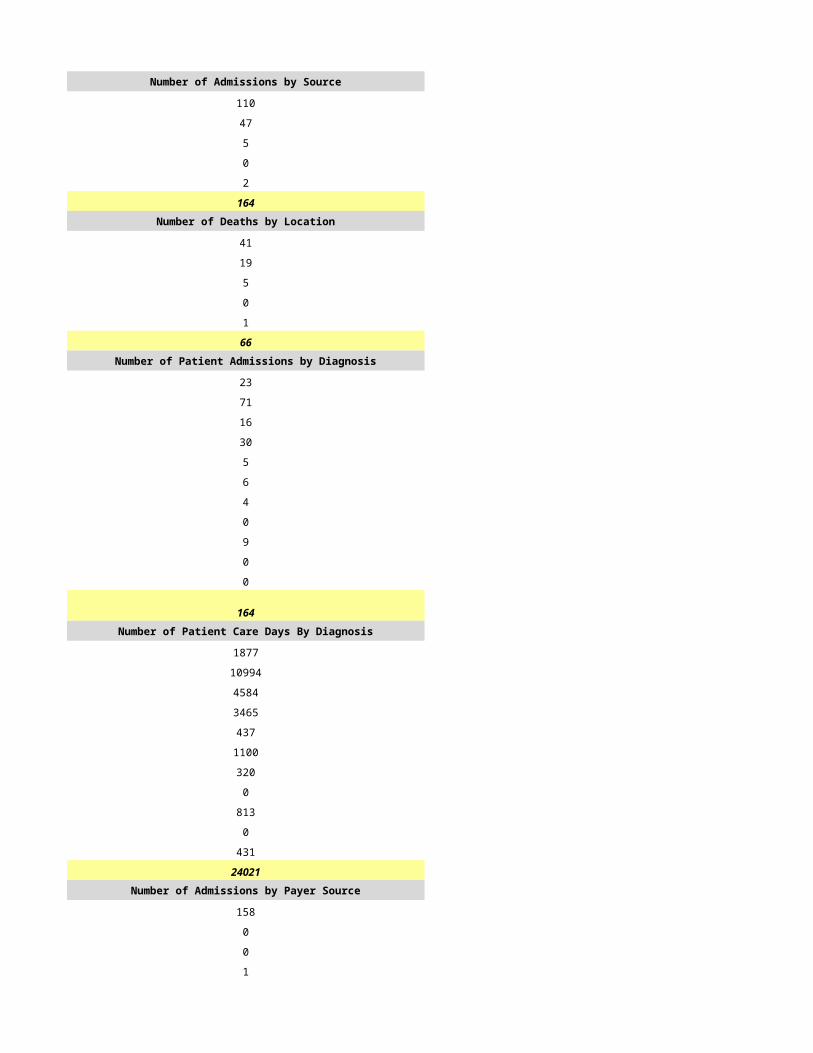
0 26
0 11
0 0
0 0
0 190Number of Deaths by Location Number of Deaths by Location
0 99
0 50
0 14
0 0
0 0
0 163Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
0 76
0 37
0 25
0 21
0 2
0 9
0 2
0 0
0 10
0 6
0 2
0 190Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
0 4924
0 4533
0 3762
0 3520
0 19
0 479
0 345
0 0
0 892
0 466
0 412
0 19352Number of Admissions by Payer Source Number of Admissions by Payer Source
0 170
0 10
0 0
0 9
0 1
0 190
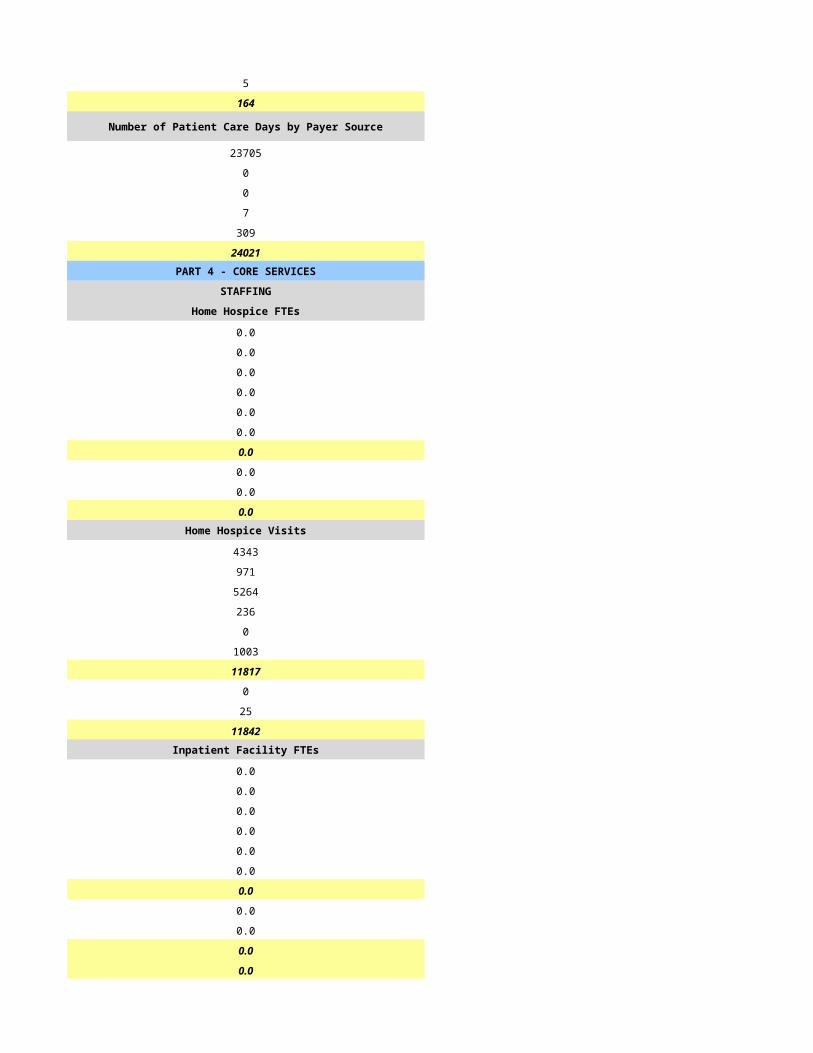
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
0 17559
0 949
0 0
0 652
0 192
0 19352PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
0.0 9.0
0.0 2.0
0.0 6.0
0.0 2.0
0.0 0.0
0.0 1.0
0.0 20.0
0.0 2.0
0.0 1.0
0.0 23.0Home Hospice Visits Home Hospice Visits
0 8706
0 1017
0 5371
0 10
0 0
0 142
0 15246
0 898
0 213
0 16357Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 23.0
CASELOADS CASELOADS
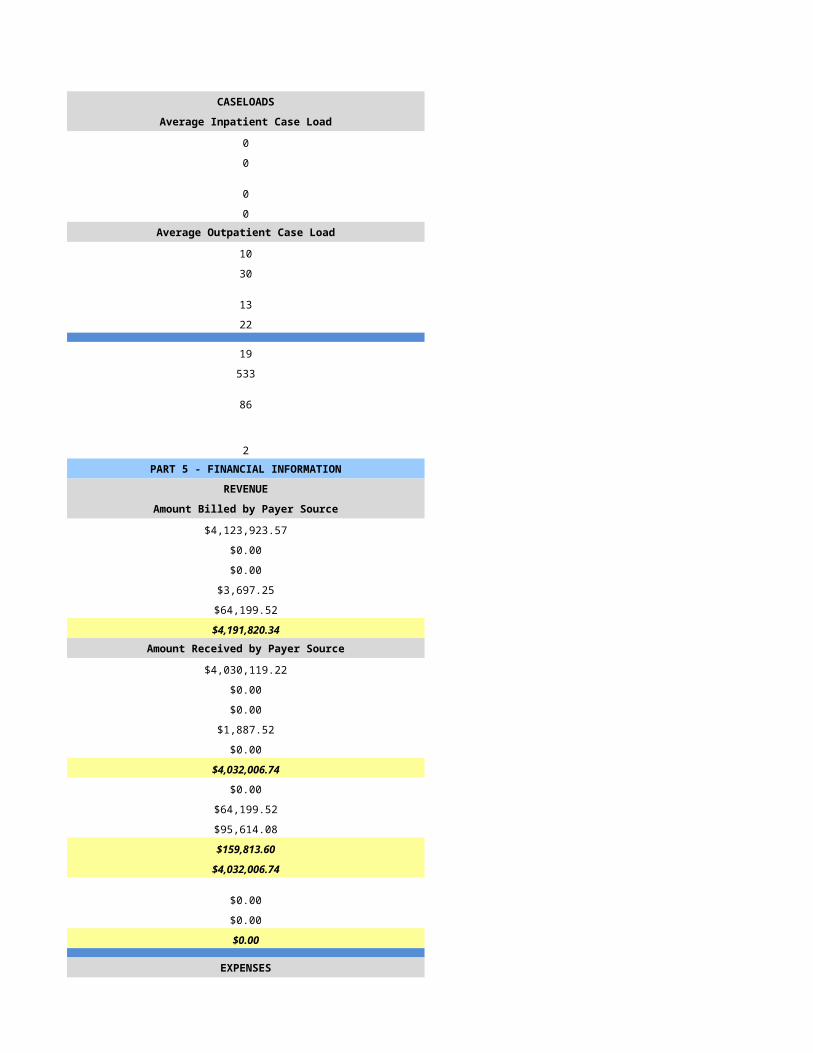
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 6
0 26
0 8
0 26
0 44
0 2446
0 174
0 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $3,108,309.95
$0.00 $155,061.53
$0.00 $0.00
$0.00 $111,241.25
$0.00 $33,879.58
$0.00 $3,408,492.31Amount Received by Payer Source Amount Received by Payer Source
$0.00 $2,948,758.41
$0.00 $20,746.16
$0.00 $0.00
$0.00 $31,920.10
$0.00 $0.00
$0.00 $3,001,424.67
$0.00 $19,104.04
$0.00 $33,879.58
$0.00 $82,642.36
$0.00 $135,625.98
$0.00 $2,865,798.69
$0.00 $0.00
$0.00 $0.00
$0.00 $2,865,798.69
EXPENSES EXPENSES
$0.00 $1,719,850.42
$0.00 $222,738.15
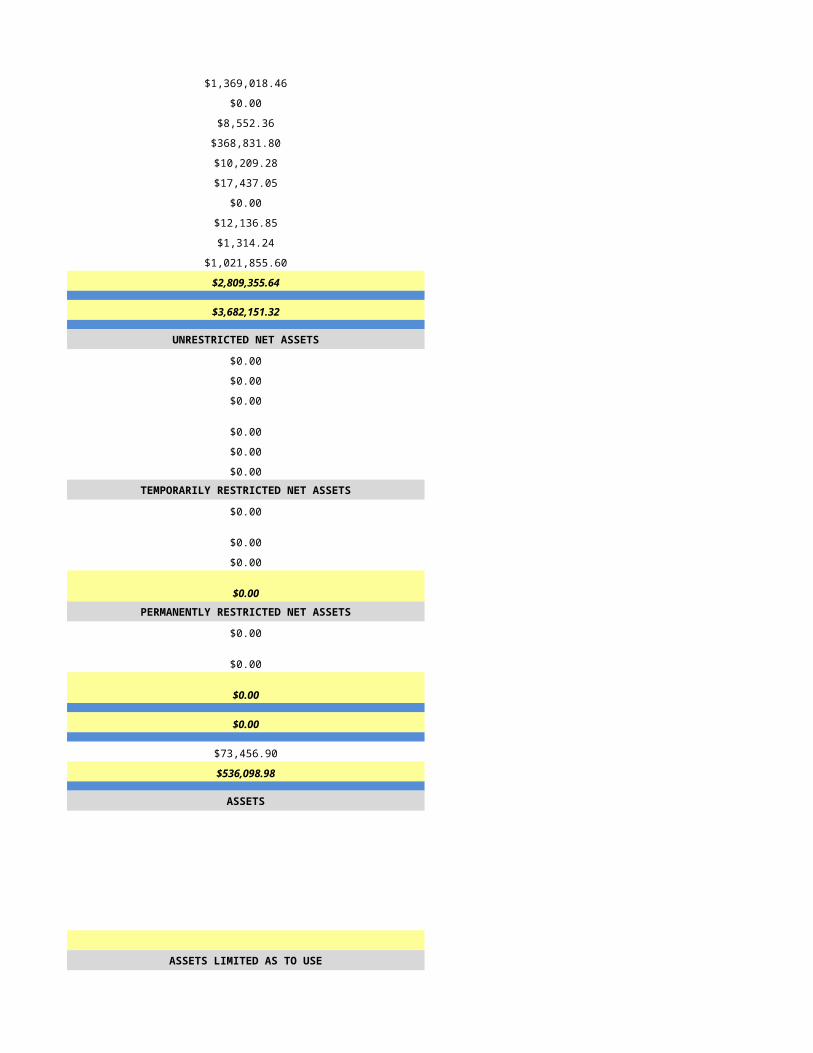
$0.00 $34,351.73
$0.00 $515,934.66
$0.00 $4,324.11
$0.00 $15,471.00
$0.00 $101,106.05
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $2,613,776.12
$0.00 $252,022.57
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $252,022.57
$0.00 $0.00
$0.00 $252,022.57TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $252,022.57
$0.00 $0.00
$0.00 $252,022.57
ASSETS ASSETS
$457,308.41
$0.00
$0.00
$711,291.73
$0.00
$0.00
$1,168,600.14ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$1,168,600.14
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$84,205.98
$0.00
$0.00
$84,205.98
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$84,205.98
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/14/2015 6/15/2015
HSPC-3721 HSPC-3648
Hospice of Phoenix Community Hospice Group, LLC
Hospice of the Pines Hospice of the South West, LLC
13175 East Highway 169 450 North Dobson, Suite 108
Dewey Mesa
AZ AZ
86327 85201
Yavapai Maricopa
P O Box 47090
Phoenix 450 North Dobson, Suite 108
AZ AZ
86327
Maricopa 85201
928-632-0111 480-456-9300
Beth Funk Richard Bass
928-632-0111 480-456-9300
[email protected] rbass@avianthea;thcare.com
Satty Bhowra Karen Monville
602-550-4065 480-456-9300
[email protected] [email protected]
Satty Bhowra Ramsey David Badre
602-550-4065 912-634-9197
[email protected] [email protected]
950437 9411551
11342443157 1568569846
Yes Yes
03-1559 03-1557
Not Accredited Not Accredited
None
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Primarily Urban
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Primarily Rural Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
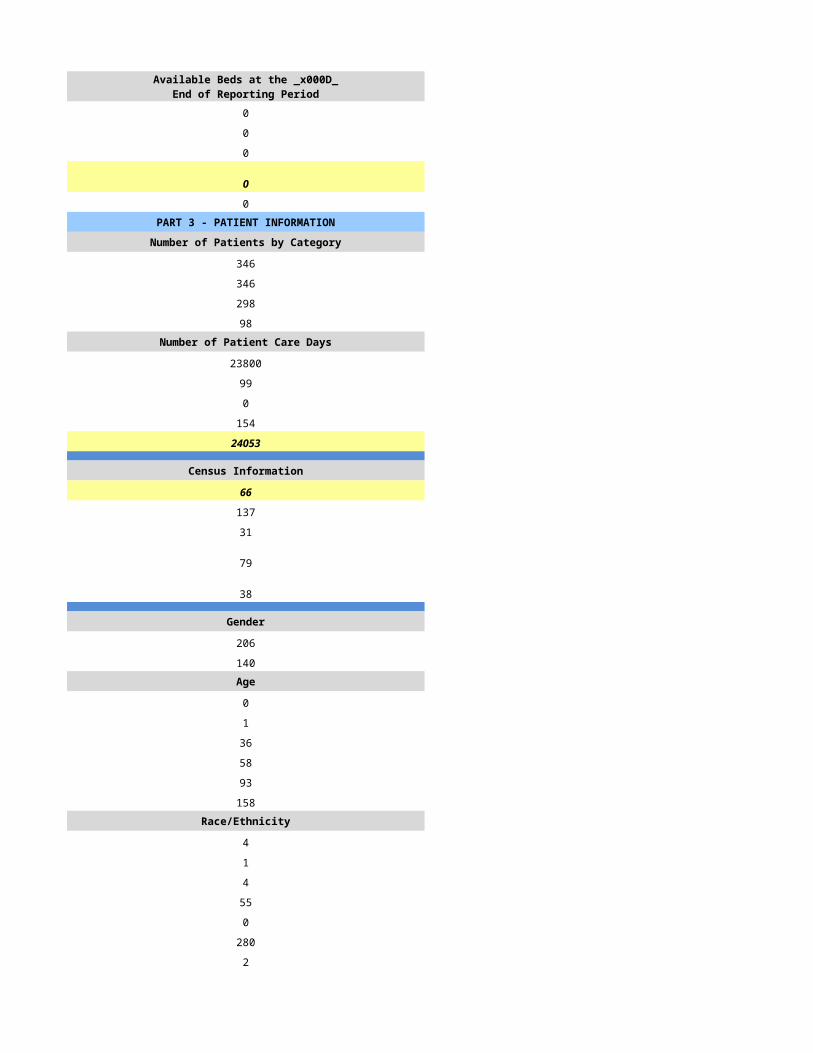
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
220 334
190 180
163 146
39 96Number of Patient Care Days Number of Patient Care Days
19111 27538
202 161
0 3
39 188
19352 27890
Census Information Census Information
53 76
101 83
50 30
35 45
36 28
Gender Gender
132 70
108 76Age Age
1 0
1 0
23 14
44 25
56 64
115 77Race/Ethnicity Race/Ethnicity
5 3
0 0
0 4
9 3
0 1
226 158
0 11Number of Admissions by Source Number of Admissions by Source
153 70
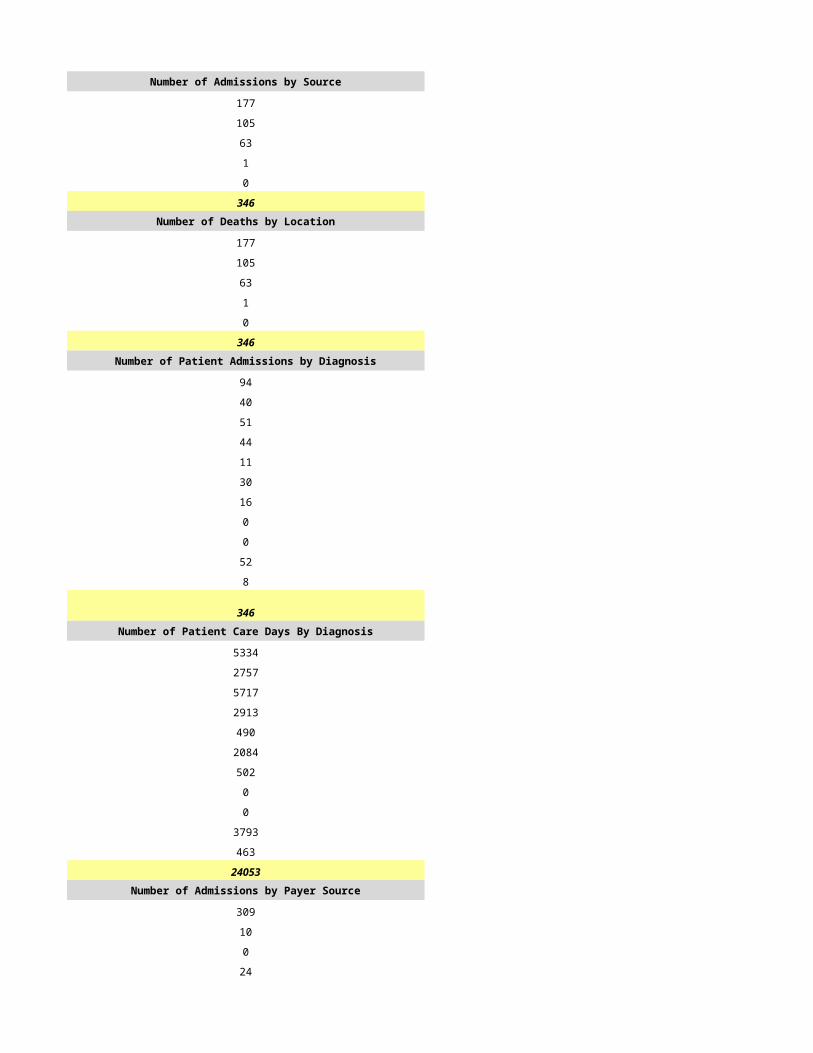
26 63
11 40
0 0
0 11
190 184Number of Deaths by Location Number of Deaths by Location
99 47
50 53
14 35
0 0
0 11
163 146Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
76 38
37 25
25 40
21 41
2 4
9 13
2 4
0 0
10 5
6 12
2 2
190 184Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
4924 2324
4533 5798
3762 8222
3520 6256
19 67
479 1135
345 485
0 0
892 1622
466 1642
412 339
19352 27890Number of Admissions by Payer Source Number of Admissions by Payer Source
170 164
10 4
0 0
9 6
1 10
190 184
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
17559 24108
949 297
0 0
652 758
192 2727
19352 27890PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
9.0 5.0
2.0 2.0
6.0 8.0
2.0 0.0
0.0 0.0
1.0 0.0
20.0 15.0
2.0 2.5
1.0 0.5
23.0 18.0Home Hospice Visits Home Hospice Visits
8706 5476
1017 1190
5371 8223
10 0
0 0
142 0
15246 14889
898 0
213 1894
16357 16783Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
23.0 18.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
6 15
26 38
8 9
26 50
44 22
2446 1491
174 157
1 6PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,108,309.95 $6,594,576.00
$155,061.53 $108,642.00
$0.00 $0.00
$111,241.25 $127,792.00
$33,879.58 $9,418.00
$3,408,492.31 $6,840,428.00Amount Received by Payer Source Amount Received by Payer Source
$2,948,758.41 $3,937,920.00
$20,746.16 $108,643.00
$0.00 $0.00
$31,920.10 $127,792.00
$0.00 $9,418.00
$3,001,424.67 $4,183,773.00
$19,104.04 $0.00
$33,879.58 $0.00
$82,642.36 $0.00
$135,625.98 $0.00
$2,865,798.69 $4,183,773.00
$0.00 $0.00
$0.00 $0.00
$2,865,798.69 $4,183,773.00
EXPENSES EXPENSES
$1,719,850.42 $1,550,887.00
$222,738.15 $38,254.00
$34,351.73 $327,337.00
$515,934.66 $768,875.00
$4,324.11 $103,215.00
$15,471.00 $49,785.00
$101,106.05 $0.00
$0.00 $119,698.00
$0.00 $17,886.00
$0.00 $1,030,363.00
$2,613,776.12 $4,006,300.00
$252,022.57 $177,473.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$252,022.57 $177,473.00
$0.00 $0.00
$252,022.57 $177,473.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$252,022.57 $177,473.00
$0.00 $0.00
$252,022.57 $177,473.00
ASSETS ASSETS
$457,308.41
$0.00
$0.00
$711,291.73
$0.00
$0.00
$1,168,600.14ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$1,168,600.14
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$84,205.98
$0.00
$0.00
$84,205.98
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$84,205.98
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/16/2015 6/17/2015
HSPC-4886 HSPC-6197
Hospice of the West, LLC Hospice Promise, LLC
Hospice of the West, LLC Hospice Promise, LLC
21410 N 19th Ave, Suite 100 1211 W Bell Road, Suite 101
Phoenix Surprise
AZ AZ
85027 85378
Maricopa Maricopa
(602) 343-6422 (623) 209-7003
Rhea Go-Coloma Deborah Horning
(602) 343-6422 (623) 792-0070
[email protected] [email protected]
None
(999) 999-9999 NA
NA
Stacie Davis Deborah Horning
(970) 613-0022 (623) 792-0070
[email protected] [email protected]
616111 000029
1578874053 1770917692
Yes Yes
03-1592 03-1630
CHAP CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
N/A
41911
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
N/A
Mixed Urban and Rural Mixed Urban and Rural
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
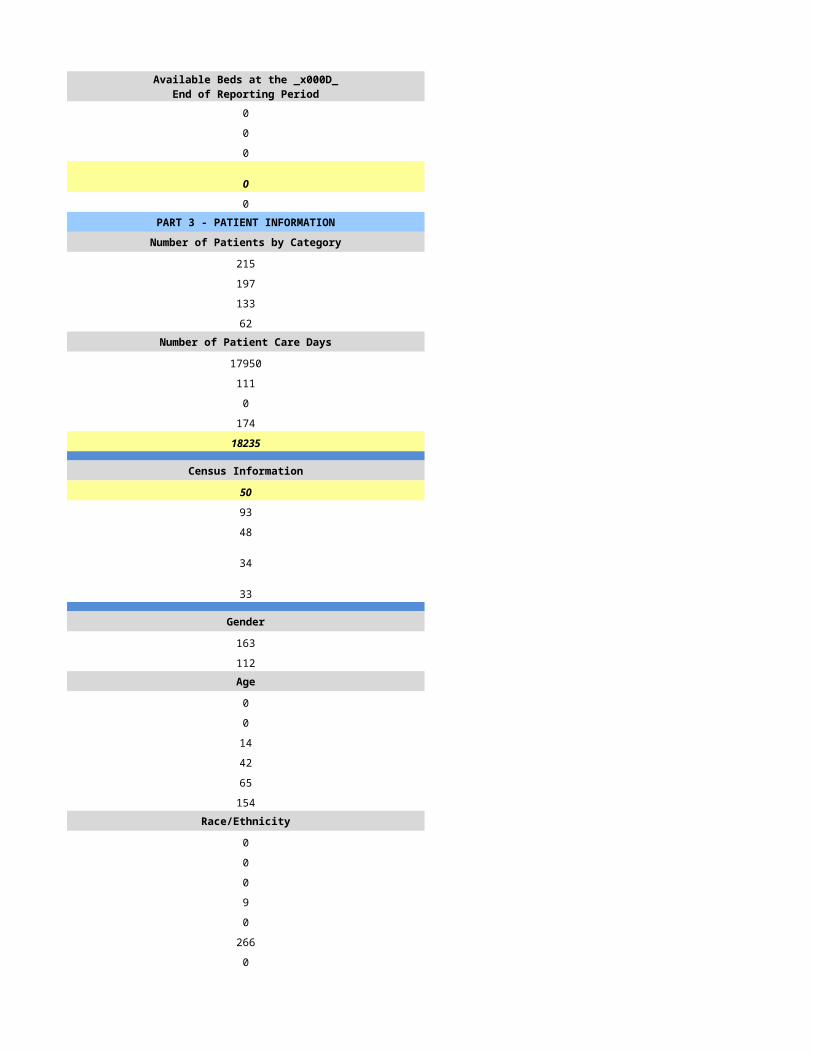
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
574 25
390 20
283 3
102 2Number of Patient Care Days Number of Patient Care Days
43695 1131
175 0
1 0
177 0
44048 1131
Census Information Census Information
121 3
119 51
38 26
77 0
82 0
Gender Gender
308 11
178 9Age Age
0 0
0 0
14 0
38 2
80 10
354 8Race/Ethnicity Race/Ethnicity
2 1
5 0
20 0
61 2
2 0
378 16
9 1Number of Admissions by Source Number of Admissions by Source
132 8
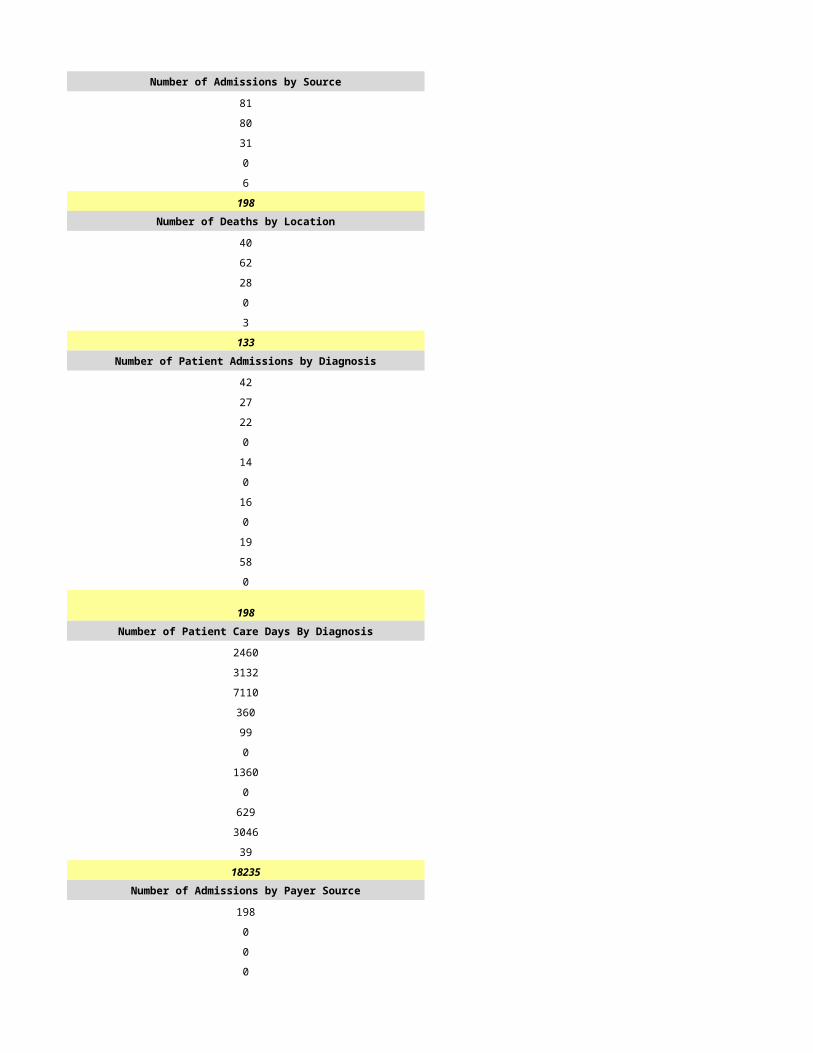
197 12
55 0
0 0
6 0
390 20Number of Deaths by Location Number of Deaths by Location
81 1
143 2
47 0
0 0
12 0
283 3Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
50 5
65 3
144 7
35 1
11 1
15 1
7 1
0 0
28 1
18 0
17 0
390 20Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
0 332
0 117
0 434
0 12
0 89
0 12
0 94
0 0
0 41
0 0
0 0
0 1131Number of Admissions by Payer Source Number of Admissions by Payer Source
353 18
0 0
0 0
9 0
28 2
390 20
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
42704 943
0 0
0 0
320 0
1024 188
44048 1131PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
17.0 1.0
6.0 0.5
11.0 0.5
0.0 1.0
3.0 0.0
0.0 0.5
37.0 3.5
21.0 2.0
1.5 0.5
59.5 6.0Home Hospice Visits Home Hospice Visits
12865 381
4824 111
16700 352
0 0
0 0
76 0
34465 844
3594 0
56 1
38115 845Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
59.5 6.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
11 12
30 40
11 10
35 60
26 1
2622 16
534 1
8 4PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$7,109,806.43 $24,978.00
$0.00 $0.00
$0.00 $0.00
$53,156.35 $0.00
$155,856.97 $0.00
$7,318,819.75 $24,978.00Amount Received by Payer Source Amount Received by Payer Source
$7,109,806.43 $24,978.00
$0.00 $0.00
$0.00 $0.00
$209,013.32 $0.00
$0.00 $0.00
$7,318,819.75 $24,978.00
$0.00 $0.00
$157,435.40 $0.00
$191,540.35 $0.00
$348,975.75 $0.00
$6,969,844.00 $24,978.00
$0.00 $0.00
$0.00 $0.00
$6,969,844.00 $24,978.00
EXPENSES EXPENSES
$3,802,180.53 $314,314.00
$522,567.19 $387.00
$452,329.04 $59,835.00
$1,234,142.40 $16,580.00
$170,329.67 $39,157.00
$47,943.31 $3,075.00
$0.00 $0.00
$1,716.00 $202.00
$13,027.20 $0.00
$761,484.55 $96,433.00
$7,005,719.89 $529,983.00
-$35,875.89 -$505,005.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$35,875.89 -$505,005.00
$0.00 -$81,661.00
-$35,875.89 -$586,666.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$35,875.89 -$586,666.00
$0.00 $95,403.00
-$35,875.89 -$491,263.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/18/2015 6/19/2015
HSPC-5232 HSPC-3842
D.A. Home Health Management LLC Infinity Hospice Care, LLC
Hospice Sanctuary LLC Infinity Hospice Care, LLC
14201 N 87th Street, D145A 5110 N. 40th St., 107
Scottsdale Phoenix
AZ AZ
85260 85018
Maricopa Maricopa
(602) 633-6100 (602) 381-0375
Valerie Nelson, RN, BSN Darren Bertram
(602) 633-6100 602-381-0375
[email protected] [email protected]
Daniel Ardelean Darren Bertram
(602) 633-6100 602-381-0375
[email protected] [email protected]
Tara DeMarco Darren Bertram
(602) 633-6100 602-381-0375
[email protected] [email protected]
Not Accredited 74045
1255616082 1467414664
Yes Yes
03-1604 31565
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Mixed Urban and Rural
Home Health-Based Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Primarily Urban Mixed Urban and Rural
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
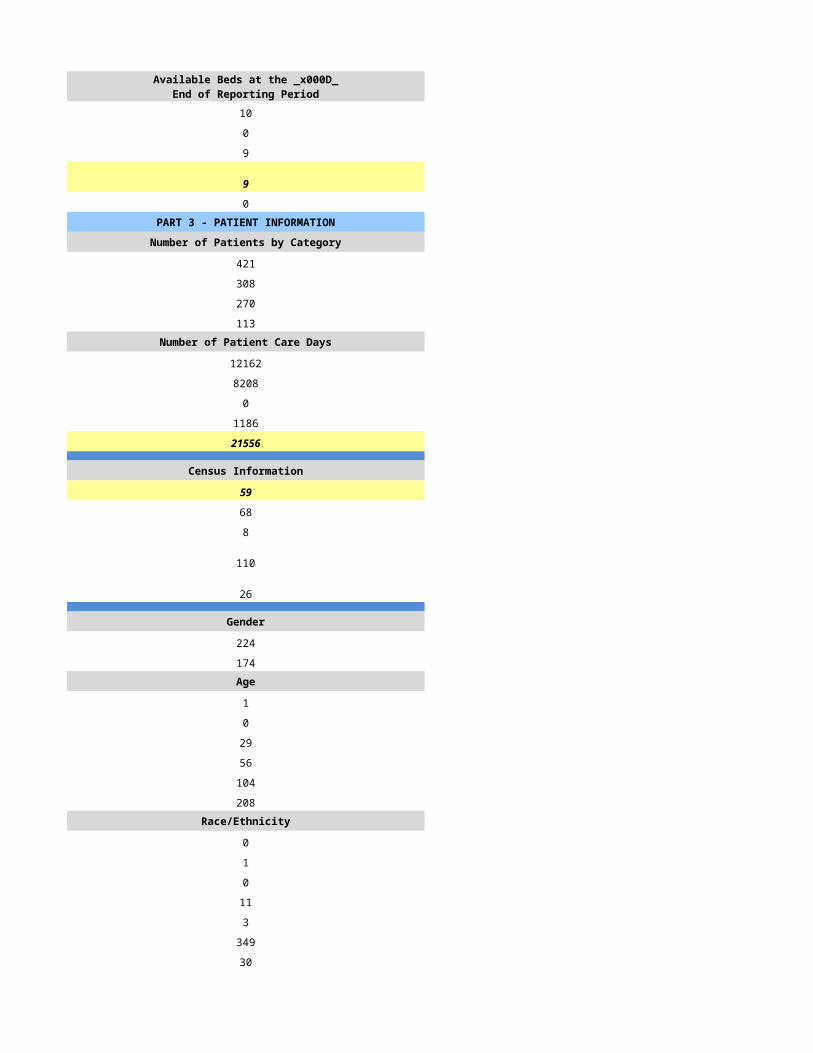
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
193 272
135 237
69 126
50 56Number of Patient Care Days Number of Patient Care Days
7384 18288
5 273
0 0
7 81
7396 18642
Census Information Census Information
20 51
132 121
55 51
21 23
35 25
Gender Gender
107 119
58 103Age Age
0 0
1 0
7 26
21 35
46 56
90 105Race/Ethnicity Race/Ethnicity
1 0
0 3
1 7
8 0
0 1
131 131
24 80Number of Admissions by Source Number of Admissions by Source
41 159
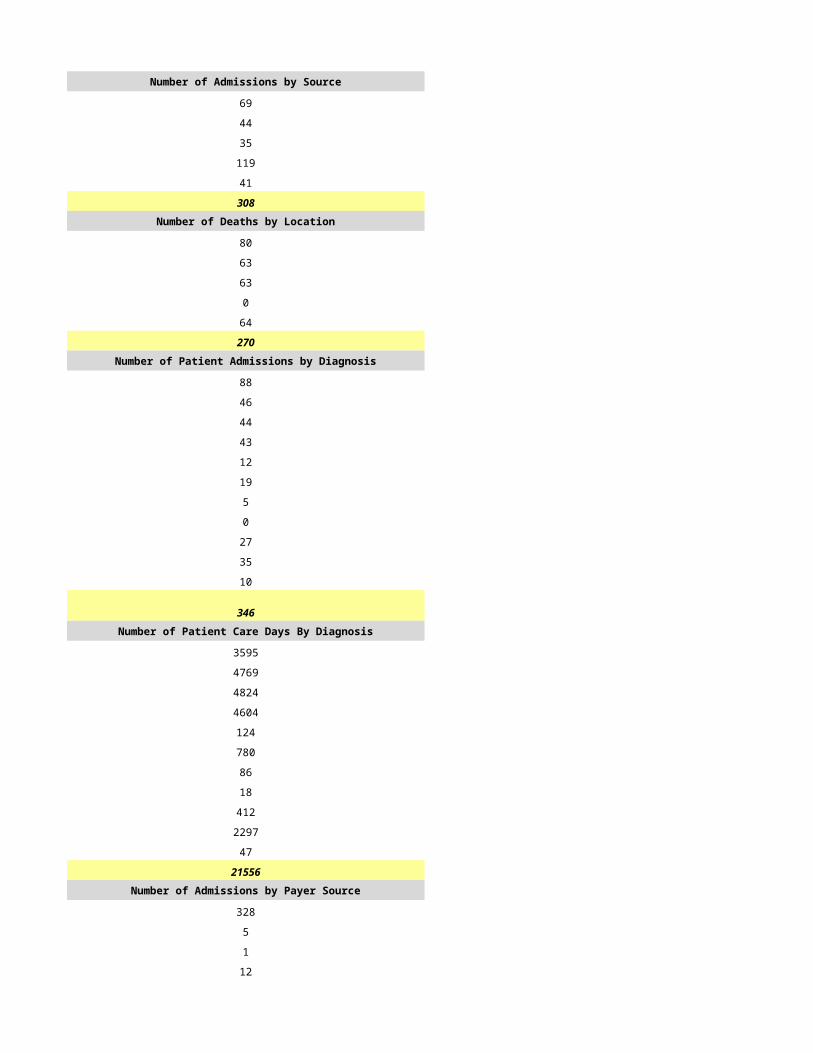
94 1
0 10
0 0
0 0
135 170Number of Deaths by Location Number of Deaths by Location
35 104
84 0
0 21
0 0
0 1
119 126Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
25 52
39 41
19 22
13 23
2 11
10 8
1 7
0 1
10 2
16 3
0 0
135 170Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
743 3998
1769 6014
1911 3340
444 2337
426 1034
483 607
326 555
0 12
358 359
34 386
902 0
7396 18642Number of Admissions by Payer Source Number of Admissions by Payer Source
125 159
0 0
0 1
3 10
7 0
135 170
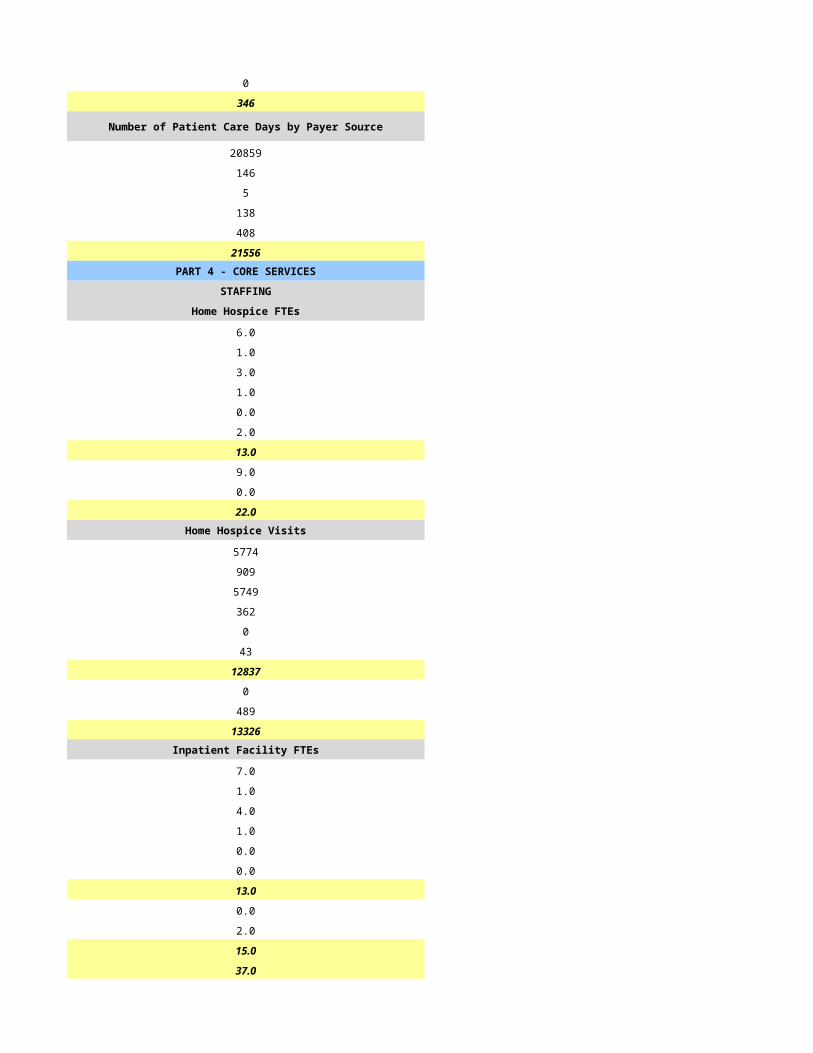
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
7359 17930
0 95
0 372
0 245
37 0
7396 18642PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
16.0 5.0
2.0 2.0
4.0 5.0
2.0 1.0
0.0 0.0
1.0 2.0
25.0 15.0
17.0 4.0
2.0 1.0
44.0 20.0Home Hospice Visits Home Hospice Visits
3844 3832
1489 512
4119 5967
172 301
0 0
416 0
10040 10612
0 498
5 120
10045 11230Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
44.0 20.0
CASELOADS CASELOADS
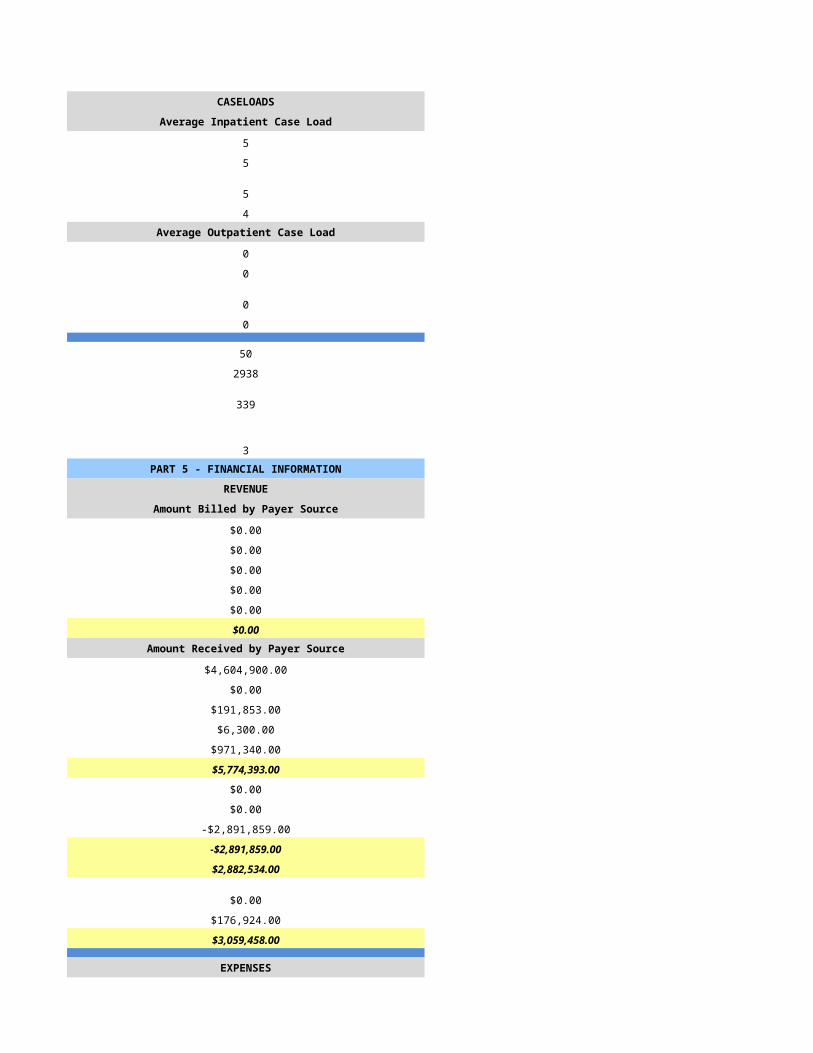
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
13 15
45 50
10 10
60 60
0 48
0 1671
100 147
2 5PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$2,408,910.00 $3,141,183.58
$0.00 $6,051.50
$0.00 $0.00
$0.00 $38,525.15
$0.00 $0.00
$2,408,910.00 $3,185,760.23Amount Received by Payer Source Amount Received by Payer Source
$2,408,910.00 $3,029,602.97
$0.00 $0.00
$0.00 $0.00
$0.00 $30,533.73
$0.00 $356.66
$2,408,910.00 $3,060,493.36
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$2,408,910.00 $3,060,493.36
$0.00 $0.00
$0.00 $900.00
$2,408,910.00 $3,061,393.36
EXPENSES EXPENSES
$1,356,537.00 $1,394,561.44
$189,342.00 $0.00
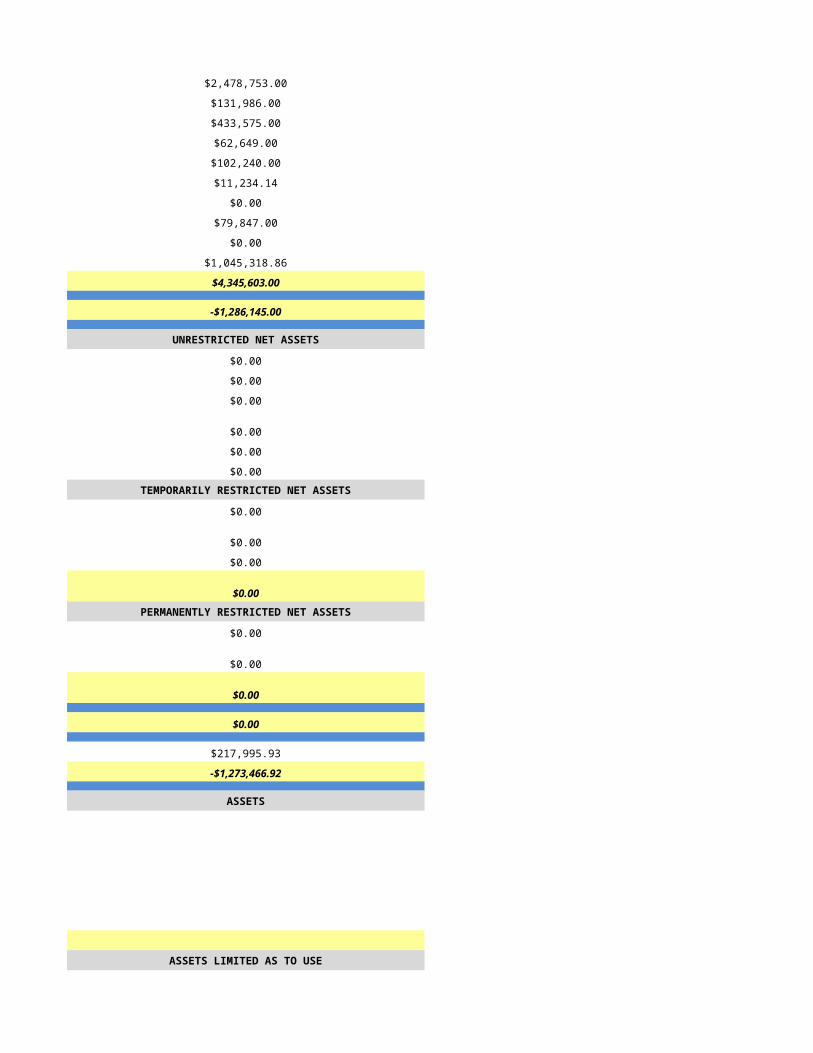
$130,039.00 $244,662.29
$246,922.00 $552,851.73
$47,290.00 $26,583.46
$24,233.00 $20,437.62
$0.00 $79,675.02
$0.00 $48,161.20
$106,544.00 $261,222.11
$206,431.00 $1,118,579.20
$2,307,338.00 $3,746,734.07
$101,572.00 -$685,340.71
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$101,572.00 -$685,340.71
$999.00 $0.00
$102,571.00 -$685,340.71TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$102,571.00 -$685,340.71
-$175,195.00 -$475,645.60
-$72,624.00 -$1,160,986.31
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
The extraordinary item represents a prior period adjustment.
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/20/2015 6/21/2015
HSPC-5951 HSPC-3040
PF Development 20, LLC Kingman Hospital, Inc.
Kindred at Home - Hospice - Glendale Kingman Regional Medical Center Hospice
17035 North 67th Avenue, Ste 8 2202 Stockton Hill Rd. Ste 200
Glendale Kingman
AZ AZ
85308 86409
Maricopa Mohave
Same as above
(623)-236-3949 928-692-4680
Laura William, RN Brian Turney
(623)-236-3949 928-757-2101
[email protected] [email protected]
Todd Higgins Timothy Blanchard
(502)-596-7953 928-757-2101
[email protected] [email protected]
Patrick Frank Nancy Pfaff
(435)-652-7255 928-692-4680
[email protected] [email protected]
Pending 722878
1134564776 1538347836
Yes Yes
03-1617 31552
JCAHO Other
DNV
Hospice Service Agency Hospice service Agency
Proprietary Voluntary (Not For Profit)
Primarily Rural Primarily Rural
Home Health-Based Hospital - Based
N/A 12
41091
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A Joan & Diana Hospice Home
N/A HSPC4872
N/A 812 Airway
N/A Kingman
N/A 86409
N/A Mohave
N/A
N/A
N/A
N/A
N/A 928-681-8710
N/A
Primarily Rural Primarily Rural
N/A Hospital - Based
N/A 12
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
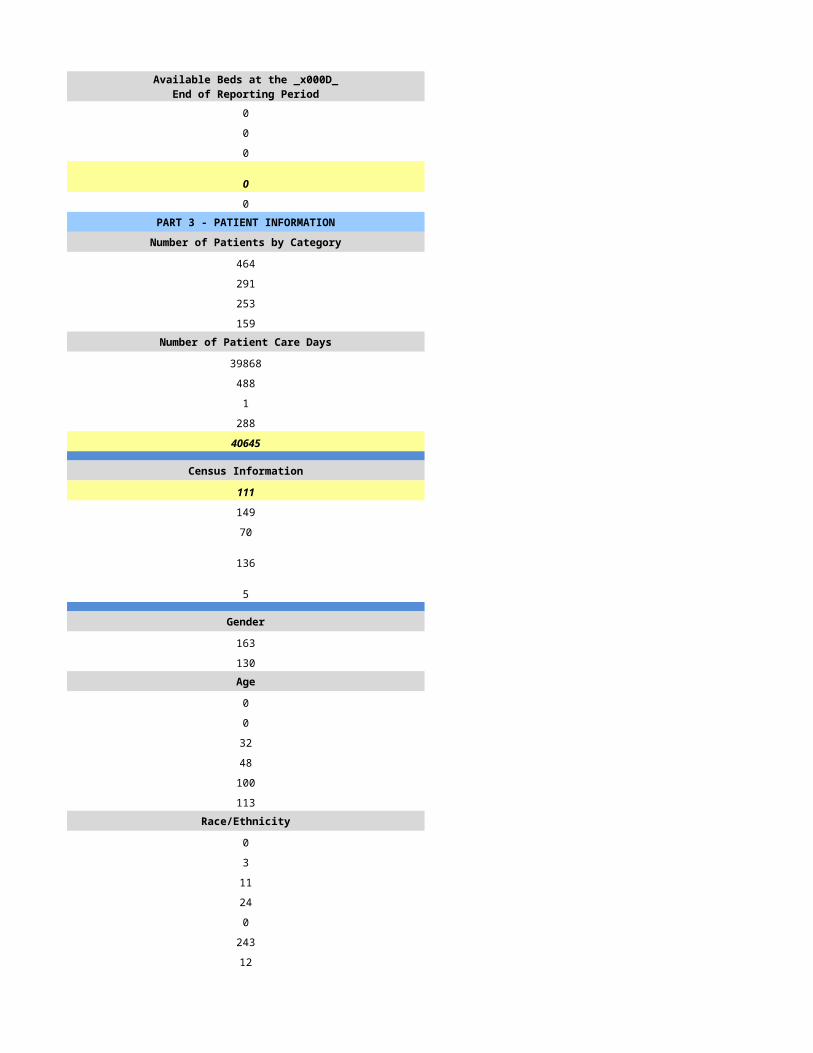
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
26 407
15 315
6 278
13 32Number of Patient Care Days Number of Patient Care Days
1222 17429
2 607
0 0
0 431
1224 18467
Census Information Census Information
3 67
64 71
50 72
3 94
0 26
Gender Gender
8 164
7 151Age Age
0 0
0 0
3 12
3 101
6 110
3 92Race/Ethnicity Race/Ethnicity
0 4
0 3
0 0
0 10
0 1
5 297
10 0Number of Admissions by Source Number of Admissions by Source
15 89
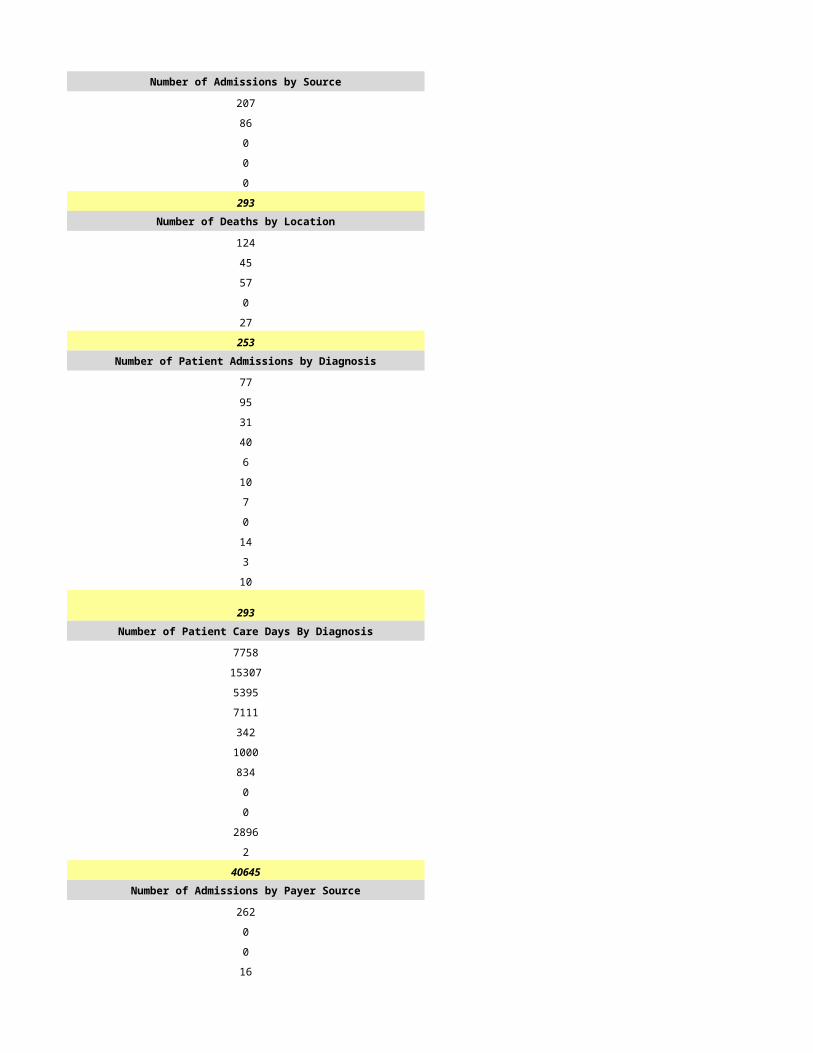
0 0
0 0
0 201
0 25
15 315Number of Deaths by Location Number of Deaths by Location
4 163
0 0
2 0
0 0
0 115
6 278Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
5 150
3 38
0 51
2 32
0 11
0 8
0 10
0 0
1 10
4 5
0 0
15 315Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
324 8864
205 2216
0 2956
311 1846
0 502
0 467
0 554
0 0
141 693
243 369
0 0
1224 18467Number of Admissions by Payer Source Number of Admissions by Payer Source
15 274
0 8
0 9
0 24
0 0
15 315
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
1196 17168
0 387
0 206
24 706
4 0
1224 18467PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
1.0 11.0
1.0 2.5
1.0 7.5
0.0 0.5
0.0 0.0
0.0 1.0
3.0 23.0
0.0 3.0
1.0 1.0
4.0 27.0Home Hospice Visits Home Hospice Visits
246 4087
61 1647
134 3159
0 178
0 0
0 260
441 9331
0 968
0 520
441 10819Inpatient Facility FTEs Inpatient Facility FTEs
0.0 6.0
0.0 0.5
0.0 5.5
0.0 0.3
0.0 0.0
0.0 0.0
0.0 12.0
0.0 0.5
0.0 0.5
0.0 13.0
4.0 40.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 3
0 3
0 3
0 3Average Outpatient Case Load Average Outpatient Case Load
1 12
1 24
1 15
1 30
0 51
0 4618
0 260
0 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$191,414.00 $8,479,675.00
$0.00 $215,040.00
$506.00 $106,090.00
$10,113.00 $403,421.00
$0.00 $0.00
$202,033.00 $9,204,226.00Amount Received by Payer Source Amount Received by Payer Source
$202,012.84 $2,819,218.00
$0.00 $9,252.00
$505.92 $3,591.00
$10,131.16 $117,345.00
$0.00 $0.00
$212,649.92 $2,949,406.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $6,254,820.00
$212,649.92 $2,949,406.00
$0.00 $0.00
$0.00 $0.00
$212,649.92 $2,949,406.00
EXPENSES EXPENSES
$200,203.00 $1,743,125.00
$245.00 $12,041.00
$21,578.00 $528,917.00
$234,610.00 $283,218.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $222,205.00
$0.00 $0.00
$0.00 $412,453.00
$456,636.00 $3,201,959.00
-$243,986.08 -$252,553.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$243,986.08 $0.00
$0.00 $0.00
-$243,986.08 $0.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$243,986.08 $0.00
$45,906.00 $0.00
-$198,080.08 $0.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/22/2015 6/23/2015
HSPC-3040 HSPC-4872
Kingman Hospital, Inc. Kingman Hospital, Inc.
Kingman Regional Medical Center Hospice Kingman Regional Medical Center Hospice
2202 Stockton Hill Rd. Ste 200 812 Airway Ave.
Kingman Kingman
AZ AZ
86409 86409
Mohave Mohave
928-692-4680 928-692-4680
Brian Turney Brian Turney
928-757-2101 928-757-2101
[email protected] [email protected]
Timothy Blanchard Timothy Blanchard
928-757-2101 928-757-2101
[email protected] [email protected]
Nancy Pfaff Nancy Pfaff
928-692-4680 928-692-4680
[email protected] [email protected]
722878 722878
1538347836 1538347836
Yes Yes
31552 31552
Other Other
DNV DNV
Hospice service Agency Hospice service Agency
Voluntary (Not For Profit) Voluntary (Not For Profit)
Primarily Rural Primarily Rural
Hospital - Based Hospital - Based
12 12
41091 41091
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Kingman Regional Medical Center Hospice Joan & Diana Hospice Home
HSPC3040 HSPC4872
2202 Stockton Hill Rd. Ste 200 812 Airway
Kingman Kingman
86409 86409
Mohave Mohave
928-681-8710 928-681-8710
Primarily Rural Primarily Rural
Hospital - Based Hospital - Based
12 12
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
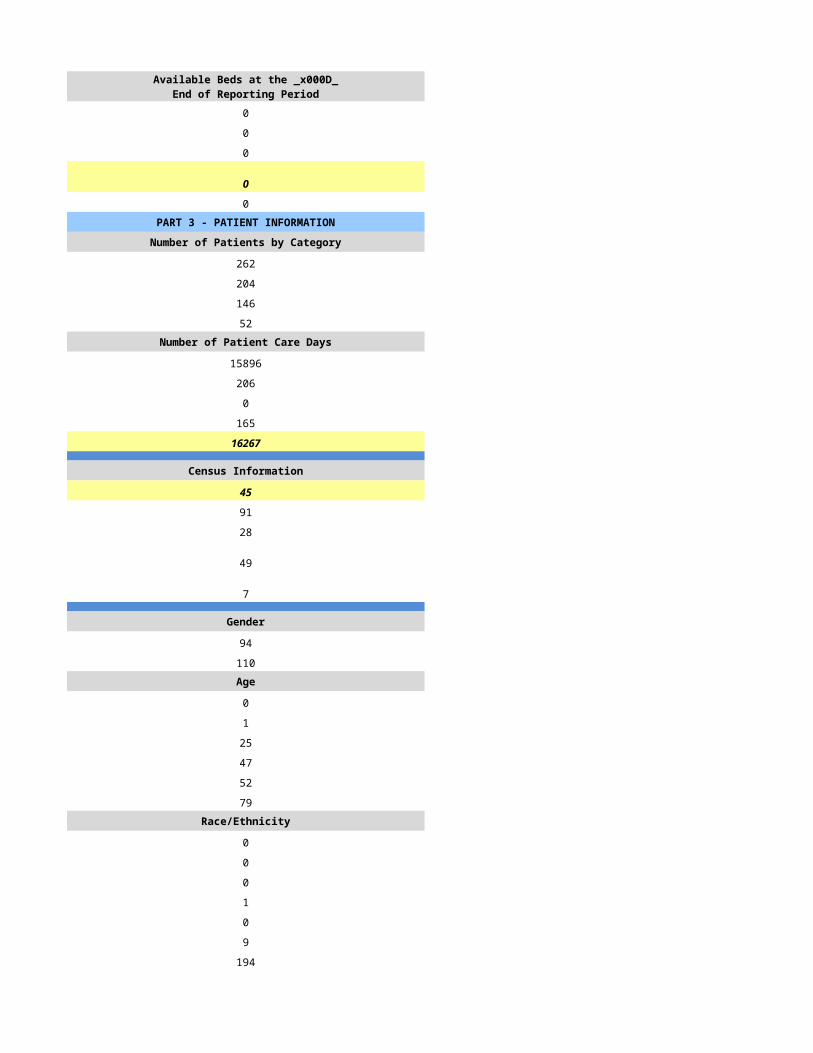
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
407 407
315 315
278 278
32 32Number of Patient Care Days Number of Patient Care Days
17429 17429
607 607
0 0
431 431
18467 18467
Census Information Census Information
67 67
71 71
72 72
94 94
26 26
Gender Gender
164 164
151 151Age Age
0 0
0 0
12 12
101 101
110 110
92 92Race/Ethnicity Race/Ethnicity
4 4
3 3
0 0
10 10
1 1
297 297
0 0Number of Admissions by Source Number of Admissions by Source
89 89
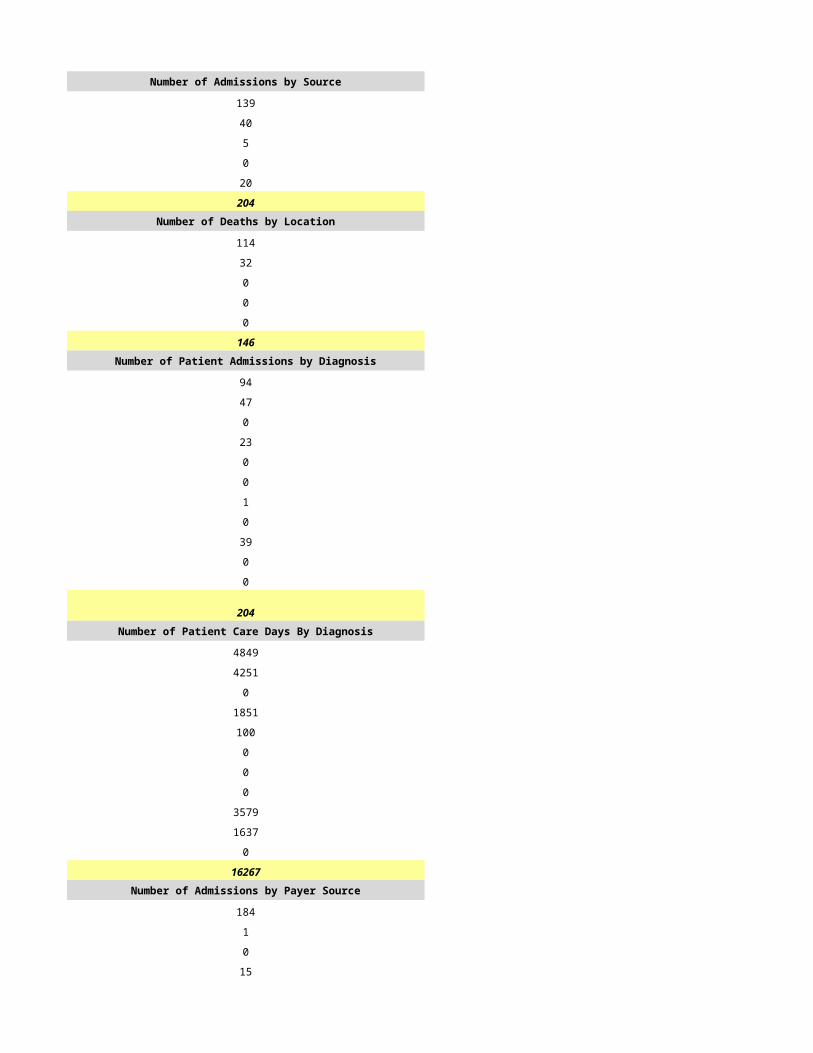
0 0
0 0
201 201
25 25
315 315Number of Deaths by Location Number of Deaths by Location
163 163
0 0
0 0
0 0
115 115
278 278Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
150 150
38 38
51 51
32 32
11 11
8 8
10 10
0 0
10 10
5 5
0 0
315 315Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
8864 8864
2216 2216
2956 2956
1846 1846
502 502
467 467
554 554
0 0
693 693
369 369
0 0
18467 18467Number of Admissions by Payer Source Number of Admissions by Payer Source
274 274
8 8
9 9
24 24
0 0
315 315
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
17168 17168
387 387
206 206
706 706
0 0
18467 18467PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
11.0 11.0
2.5 2.5
7.5 7.5
0.5 0.5
0.0 0.0
1.0 1.0
23.0 23.0
3.0 3.0
1.0 1.0
27.0 27.0Home Hospice Visits Home Hospice Visits
4087 4087
1647 1647
3159 3159
178 178
0 0
260 260
9331 9331
968 968
520 520
10819 10819Inpatient Facility FTEs Inpatient Facility FTEs
6.0 6.0
0.5 0.5
5.5 5.5
0.3 0.3
0.0 0.0
0.0 0.0
12.0 12.0
0.5 0.5
0.5 0.5
13.0 13.0
40.0 40.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
3 3
3 3
3 3
3 3Average Outpatient Case Load Average Outpatient Case Load
12 12
24 24
15 15
30 30
51 51
4618 4618
260 260
3 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$8,479,675.00 $8,479,675.00
$215,040.00 $215,040.00
$106,090.00 $106,090.00
$403,421.00 $403,421.00
$0.00 $0.00
$9,204,226.00 $9,204,226.00Amount Received by Payer Source Amount Received by Payer Source
$2,819,218.00 $2,819,218.00
$9,252.00 $9,252.00
$3,591.00 $3,591.00
$117,345.00 $117,345.00
$0.00 $0.00
$2,949,406.00 $2,949,406.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$6,254,820.00 $6,254,820.00
$2,949,406.00 $2,949,406.00
$0.00 $0.00
$0.00 $0.00
$2,949,406.00 $2,949,406.00
EXPENSES EXPENSES
$1,743,125.00 $1,743,125.00
$12,041.00 $12,041.00
$528,917.00 $528,917.00
$283,218.00 $283,218.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$222,205.00 $222,205.00
$0.00 $0.00
$412,453.00 $412,453.00
$3,201,959.00 $3,201,959.00
-$252,553.00 -$252,553.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/24/2015 6/25/2015
HSPC-5422 HSPC-5765
Blaine Whitson Maggies Hospice, Inc.
Living Waters Hospice, LLC Maggies Hospice, Inc.
3711 Highway 68 314 N. Alarcon Street
Golden Valley Prescott
AZ AZ
86413 86301
Mohave Yavapai
387 Magnolia Ave 103-135
Corona
CA
92879
Riverside
928-565-9000 928-775-2290
Suzanne Skelly Diane Tryggestad
928-565-9000 602-889-4400
[email protected] [email protected]
Randy Denham
928-565-9000 (999) 999-9999
rdenham@lwhospice/com
Suzanne Skelly Diane Tryggestad
928-565-9000 602-889-4400
[email protected] [email protected]
861934 925710
1922366947 1073854428
Yes Yes
03-1611 31625
JCAHO Other
ACHC
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Primarily Urban
Free Standing Free Standing
41709
1/1/2014 1/1/2014
12/31/2014 12/31/2014
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Mixed Urban and Rural Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
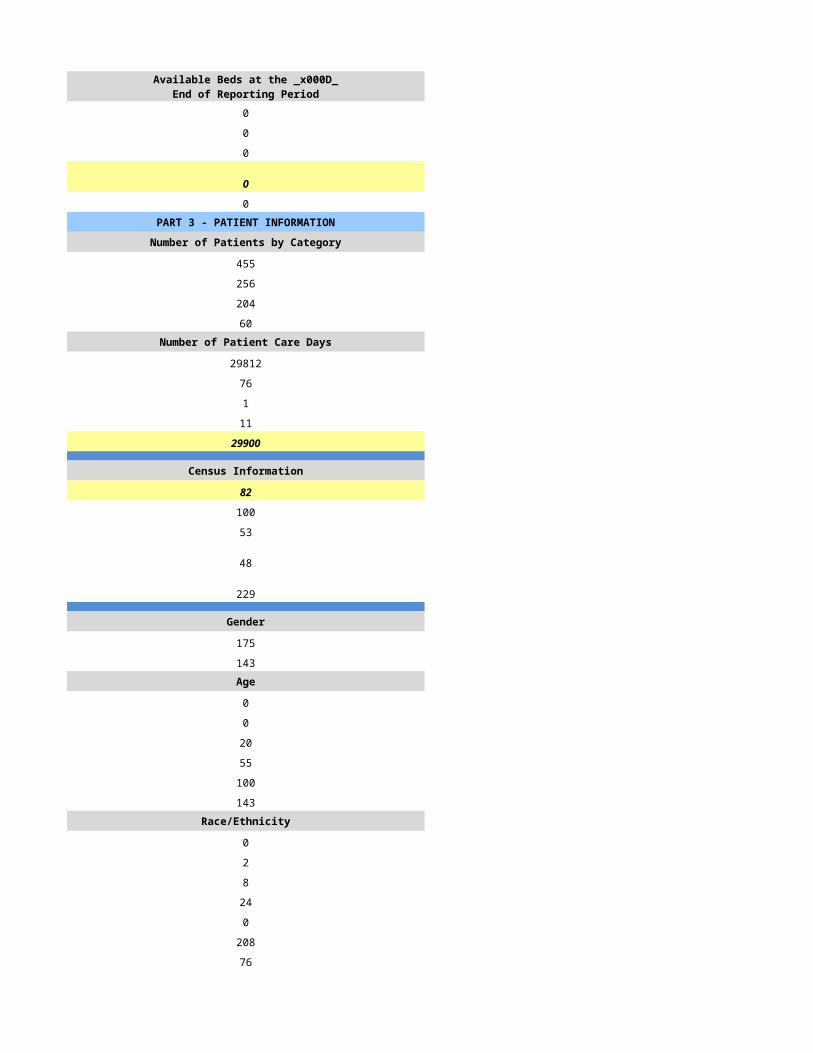
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
242 50
116 49
85 30
42 5Number of Patient Care Days Number of Patient Care Days
11944 3858
5 35
6 0
0 25
11955 3918
Census Information Census Information
33 11
94 31
24 16
20 12
6 0
Gender Gender
54 38
62 11Age Age
0 0
0 0
5 6
31 5
42 13
38 25Race/Ethnicity Race/Ethnicity
2 0
3 0
0 0
3 1
0 0
107 46
1 2Number of Admissions by Source Number of Admissions by Source
85 40
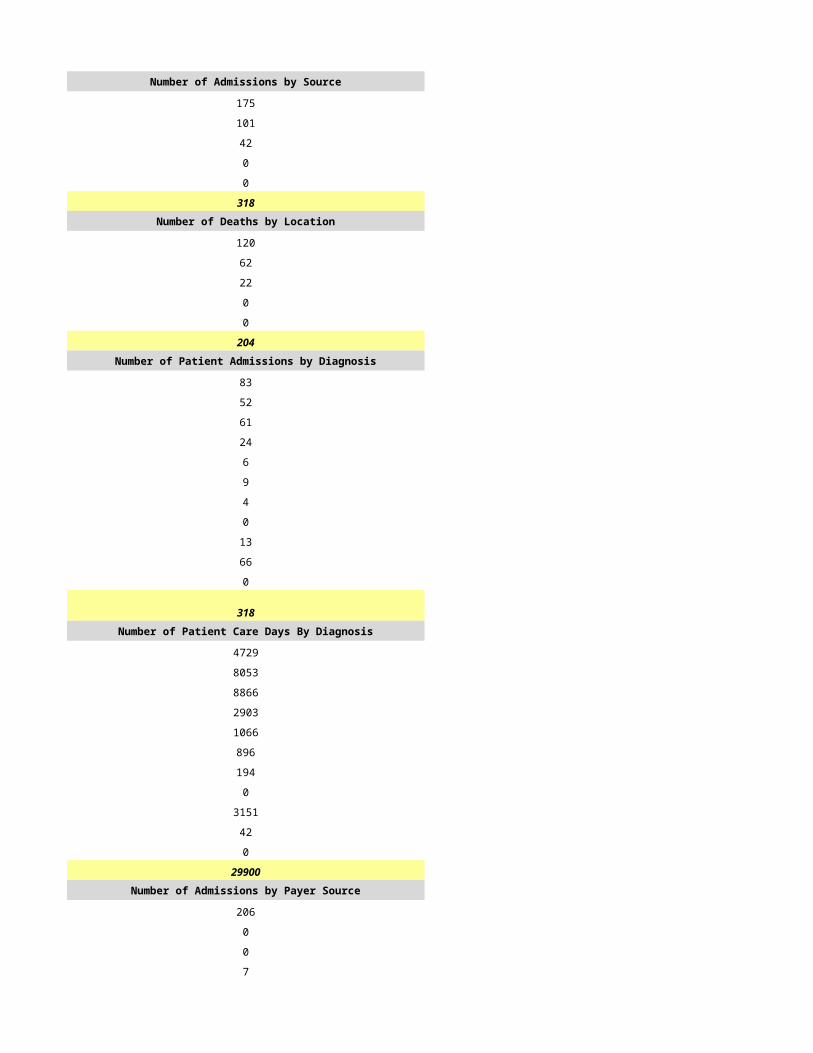
26 1
5 0
0 8
0 1
116 50Number of Deaths by Location Number of Deaths by Location
58 24
21 6
6 0
0 0
0 0
85 30Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
34 10
26 4
18 13
20 0
5 4
4 1
1 4
1 0
3 11
4 3
0 0
116 50Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2528 543
1627 74
3821 136
1665 315
565 12
782 0
326 17
35 0
278 1064
328 1716
0 41
11955 3918Number of Admissions by Payer Source Number of Admissions by Payer Source
113 42
1 0
0 0
2 2
0 6
116 50
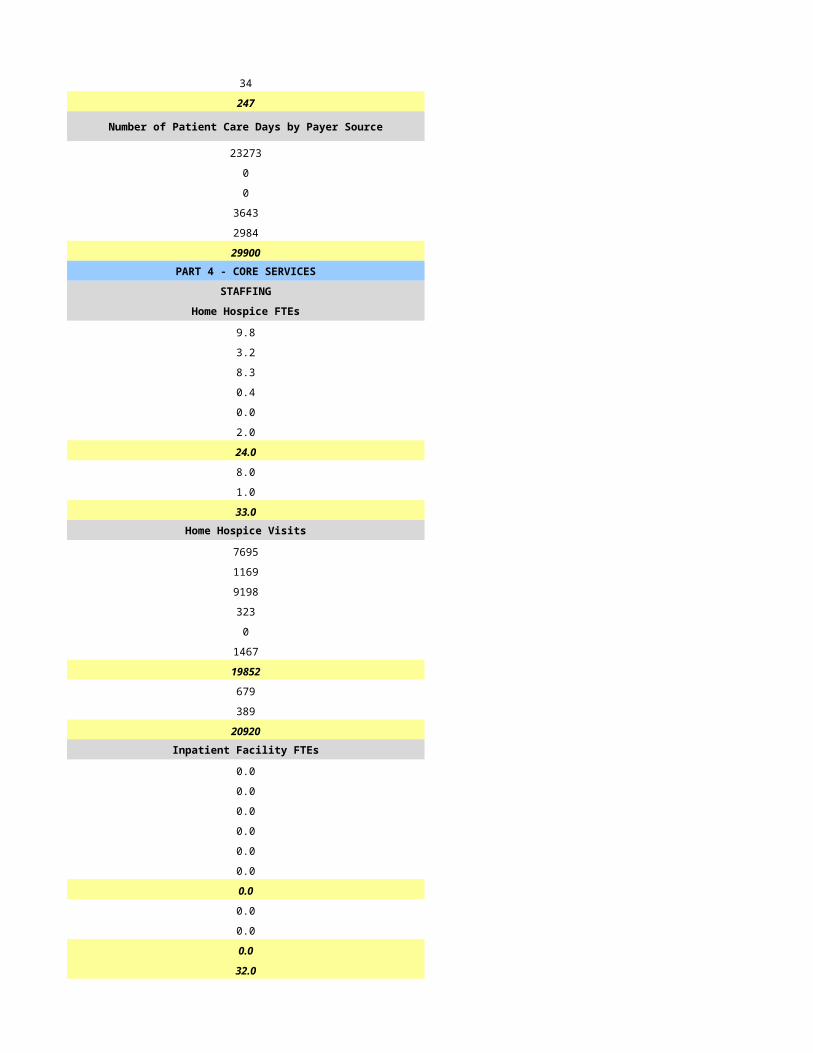
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
11692 3461
41 0
0 0
222 63
0 394
11955 3918PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
5.0 1.5
0.7 0.5
2.4 1.5
0.0 1.0
0.0 0.0
0.9 1.0
8.9 5.5
5.7 0.5
0.2 0.5
14.8 6.5Home Hospice Visits Home Hospice Visits
3748 1048
334 174
2813 921
12 1
0 0
482 0
7389 2144
0 159
54 41
7443 2344Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
14.8 6.5
CASELOADS CASELOADS
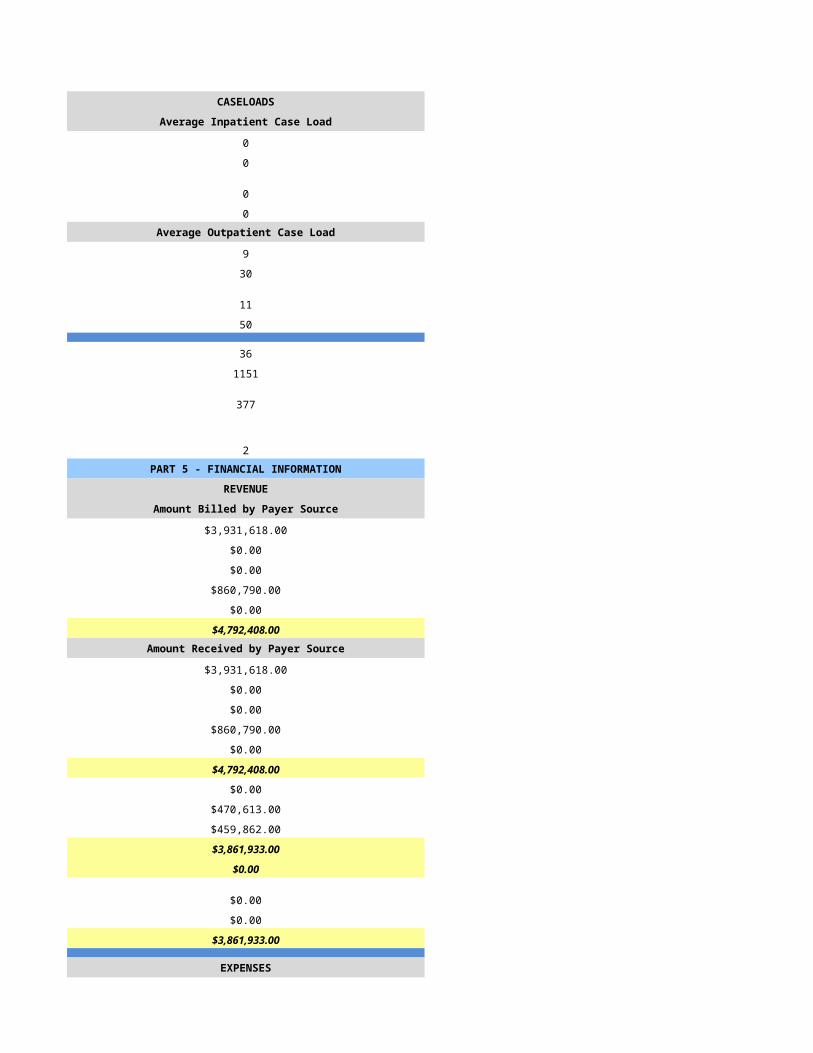
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
9 10
33 15
9 10
33 15
16 3
857 74
204 30
2 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,815,461.02 $943,519.00
$3,291.12 $0.00
$0.00 $0.00
$34,503.24 $64,955.00
$0.00 $0.00
$1,853,255.38 $1,008,474.00Amount Received by Payer Source Amount Received by Payer Source
$1,779,151.80 $529,738.00
$0.00 $0.00
$0.00 $0.00
$25,488.88 $0.00
$0.00 $23,331.00
$1,804,640.68 $553,069.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,804,640.68 $553,069.00
$1,640,332.00 $0.00
$0.00 $626.00
$3,444,972.68 $553,695.00
EXPENSES EXPENSES
$920,992.00 $303,556.00
$91,089.00 $54,613.00
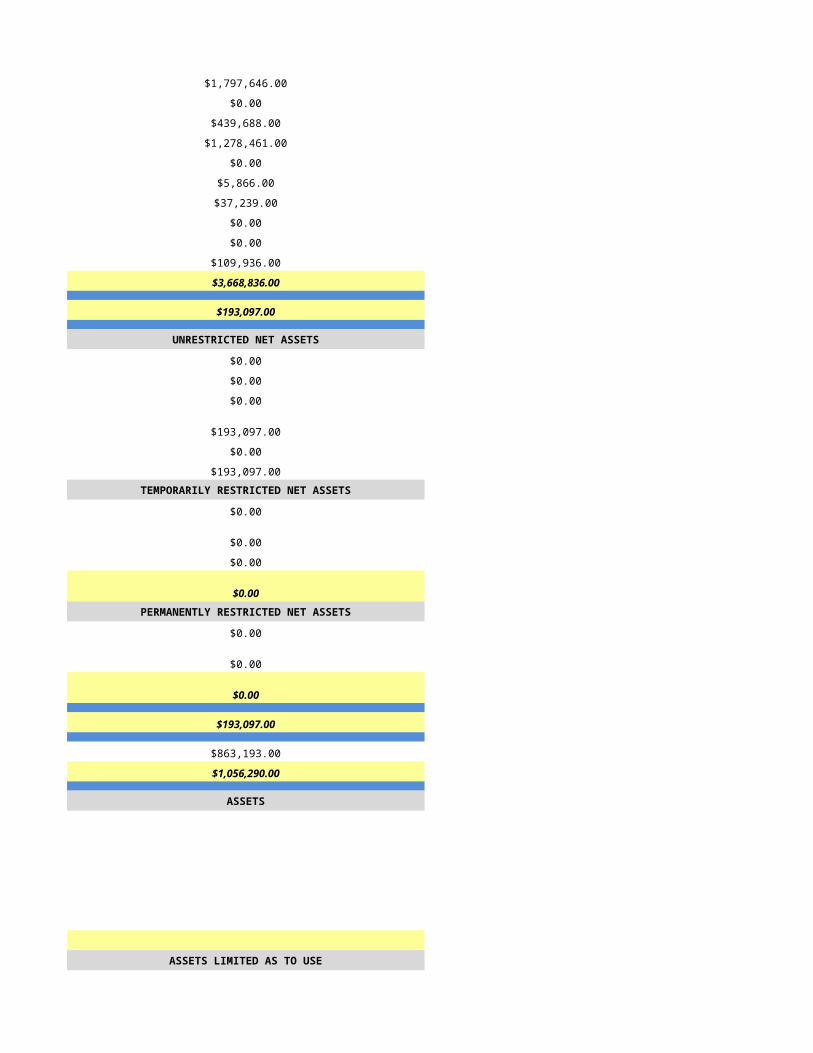
$0.00 $23,998.00
$315,925.00 $92,202.00
$45.00 $5,895.00
$47,564.00 $6,658.00
$700.00 $0.00
$46,630.00 $439.00
$0.00 $115.00
$217,387.00 $50,661.00
$1,640,332.00 $538,137.00
$1,804,640.68 $15,558.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,804,640.68 $15,558.00
$0.00 $0.00
$1,804,640.68 $15,558.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,804,640.68 $15,558.00
$0.00 -$41,097.00
$1,804,640.68 -$25,539.00
ASSETS ASSETS
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$0.00
$0.00
$0.00
$0.00
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$0.00
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/26/2015 6/27/2015
HSPC-5170 HSPC-3821
Mesa View Hospice, LLC Mohave Hospice
4072 EAST FARM ROAD 2755 Silver Creek Rd Bld D Ste125
LITTLEFIELD Bullhead City
AZ AZ
86432 86442
MOHAVE Mohave
Same As Above
702-346-3088 (928)763-3620
Shannel Rowley Jill Young
702-324-8681 (928)763-6979
[email protected] [email protected]
Travis Wakefield Jeff Aspacher
702-349-1913 (615)465-3435
[email protected] [email protected]
Ty Wakefield Jill Young & Brittany Meredith
702-785-3127 (928)763-6979
[email protected] [email protected] & [email protected]
N/a
1134448475 1720073422
Yes Yes
291529 03-1534
CHAP CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Mixed Urban and Rural
Free Standing Home Health - Based
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Mesa View Hospice, LLC N/A
HSPC5170
330 FALCON RIDGE PKWY BLDG 200 STE a
MESQUITE
89027
CLARK NV
702-346-3088
Primarily Rural Mixed Urban and Rural
Free Standing
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
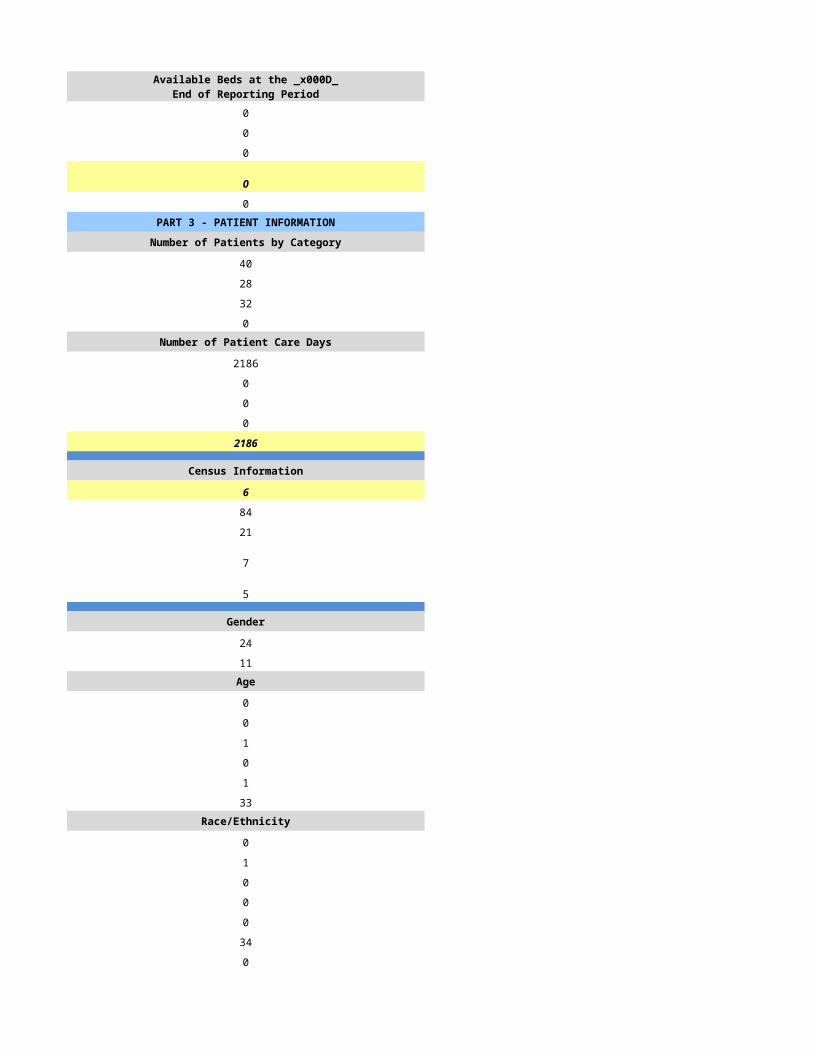
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
10 11
10 11
8 10
2 1Number of Patient Care Days Number of Patient Care Days
260 346
4 0
0 0
0 0
264 346
Census Information Census Information
0 3
0 72
0 18
4 3
0 0
Gender Gender
6 7
4 4Age Age
0 0
0 0
0 2
4 1
2 2
4 2Race/Ethnicity Race/Ethnicity
0 0
0 0
0 0
0 1
0 0
10 10
0 0Number of Admissions by Source Number of Admissions by Source
10 9
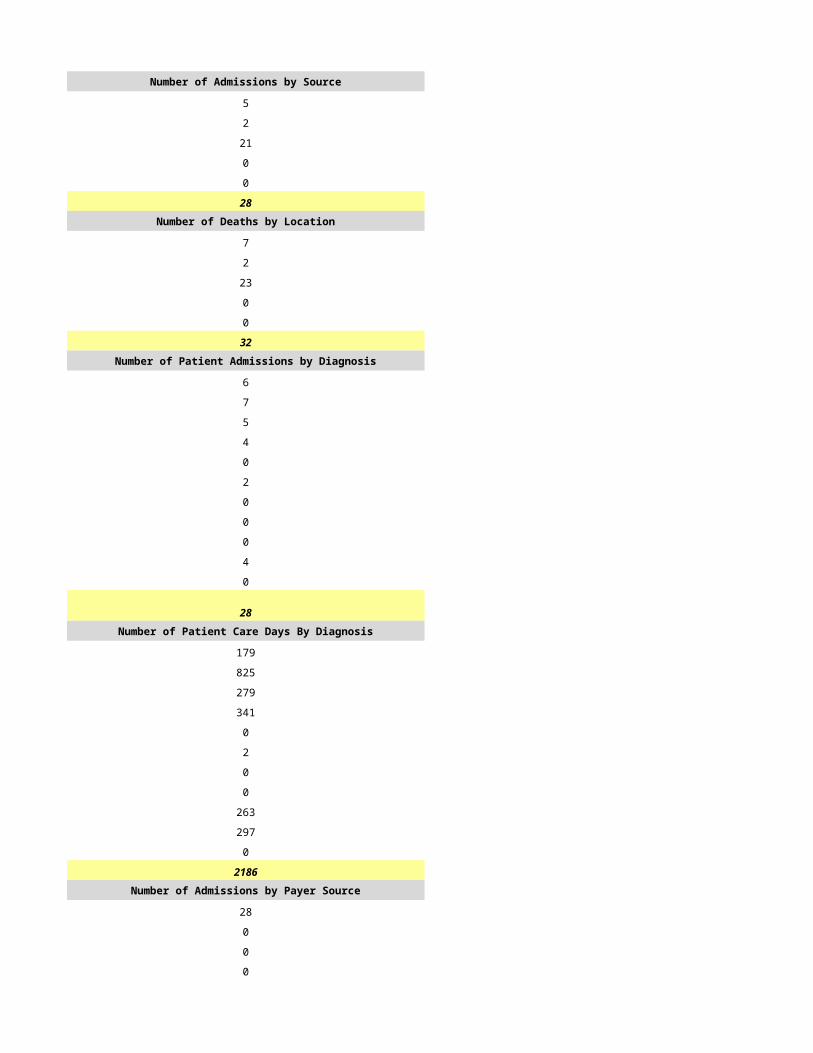
0 2
0 0
0 0
0 0
10 11Number of Deaths by Location Number of Deaths by Location
8 9
0 1
0 0
0 0
0 0
8 10Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
4 8
2 0
4 0
0 0
0 0
0 2
0 1
0 0
0 0
0 0
0 0
10 11Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
149 225
62 0
49 0
4 0
0 0
0 108
0 3
0 0
0 0
0 0
0 0
264 346Number of Admissions by Payer Source Number of Admissions by Payer Source
10 10
0 1
0 0
0 0
0 0
10 11
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
264 333
0 13
0 0
0 0
0 0
264 346PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
5.0 1.5
1.0 0.5
2.0 0.3
0.0 0.0
0.0 0.0
0.0 0.0
8.0 3.0
0.0 0.3
1.0 0.3
9.0 4.0Home Hospice Visits Home Hospice Visits
195 130
17 17
52 80
0 0
0 0
0 0
264 227
0 15
10 88
274 330Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
9.0 0.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 3
0 1
0 3
0 3
2 1
2 6
8 39
4 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$0.00 $46,701.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $2,158.00
$0.00 $48,859.00Amount Received by Payer Source Amount Received by Payer Source
$54,292.51 $46,701.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $2,158.00
$54,292.51 $48,859.00
$0.00 $0.00
$0.00 $0.00
$0.00 $83.00
$0.00 $83.00
$54,292.51 $48,776.00
$0.00 $0.00
$0.00 $0.00
$54,292.51 $48,776.00
EXPENSES EXPENSES
$0.00 $77,070.00
$0.00 $0.00
$0.00 $18,268.00
$0.00 $6,792.00
$0.00 $3,581.00
$0.00 $943.00
$0.00 -$299.00
$0.00 $0.00
$0.00 $0.00
$0.00 $9,917.00
$0.00 $116,272.00
$54,292.51 -$67,496.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$54,292.51 -$67,496.00
$0.00 $0.00
$54,292.51 -$67,496.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$54,292.51 -$67,496.00
$0.00 $0.00
$54,292.51 -$67,496.00
ASSETS ASSETS
$46,618.32
$0.00
$0.00
$0.00
$0.00
$0.00
$46,618.32ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$0.00
$0.00
$46,618.32
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$0.00
$5,873.02
$0.00
$5,873.02
NET ASSETS NET ASSETS
$46,618.32
$0.00
$0.00
$46,618.32
$52,491.34
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/28/2015 6/29/2015
HSPC-4800 HSPC-5120
New Hope Hospice of Arizona New Hope Hospice of Bullhead City
500 N. Lake Havasu Ave, Ste B106 3550 North Lane, Suite 102
Lake Havasu City Bullhead City
AZ AZ
86403 86422
Mohave Mohave
2191 Lemay Ferry Rd, Ste 300 2191 Lemay Ferry Rd, Ste 300
St. Louis St. Louis
MO MO
63125 63125
St. Louis St. Louis
314.815.3500 314.815.3500
Devin Bell Matt Robinson
928.854.4200 928.444.8122
[email protected] [email protected]
Tom Mohan Tim Mohan
314.815.3418 314.815.3418
[email protected] [email protected]
Tom Mohan Tim Mohan
314.815.3418 314.815.3418
[email protected] [email protected]
801275 801366
1699709857 1437435708
YES YES
03-1607 03-1610
Other Other
ACHC ACHC
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Primarily Rural
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Primarily Rural Primarily Rural
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
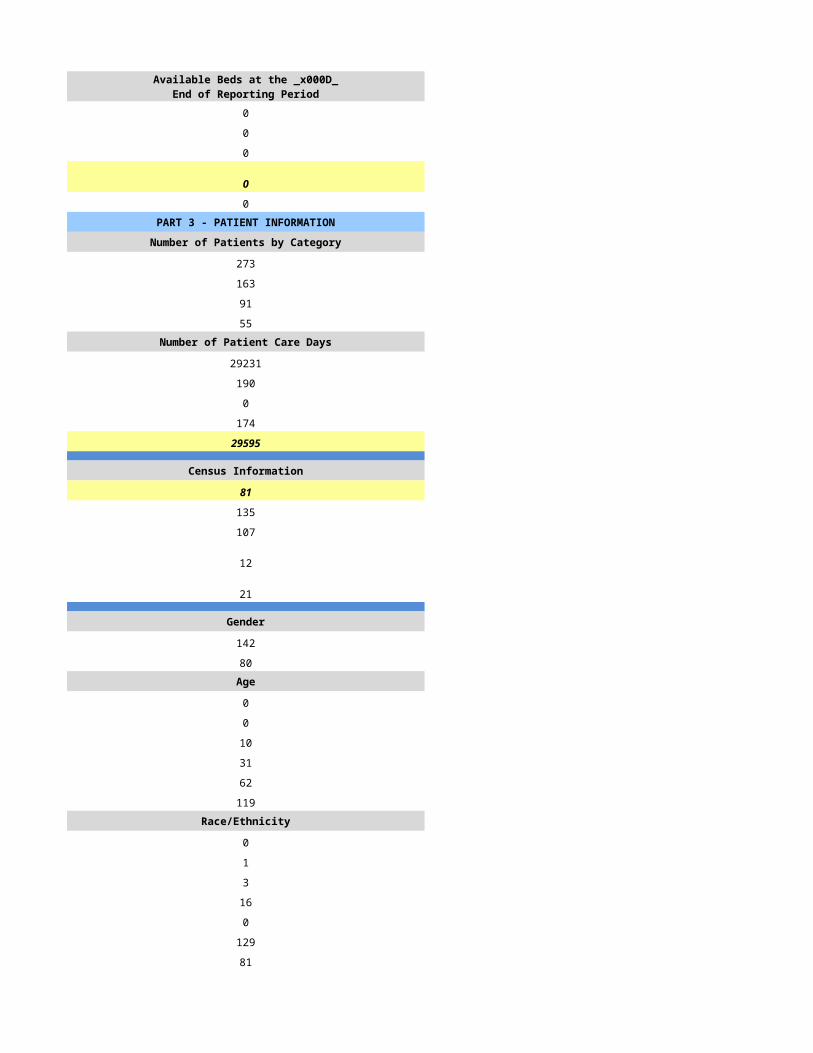
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
267 262
236 213
161 123
61 59Number of Patient Care Days Number of Patient Care Days
21971 24402
33 106
0 0
35 0
22039 24508
Census Information Census Information
62 68
79 93
44 49
45 42
24 28
Gender Gender
124 136
143 122Age Age
0 0
0 0
29 37
50 58
188 163
0 0Race/Ethnicity Race/Ethnicity
2 2
0 1
0 1
6 12
2 1
224 200
35 41Number of Admissions by Source Number of Admissions by Source
167 203
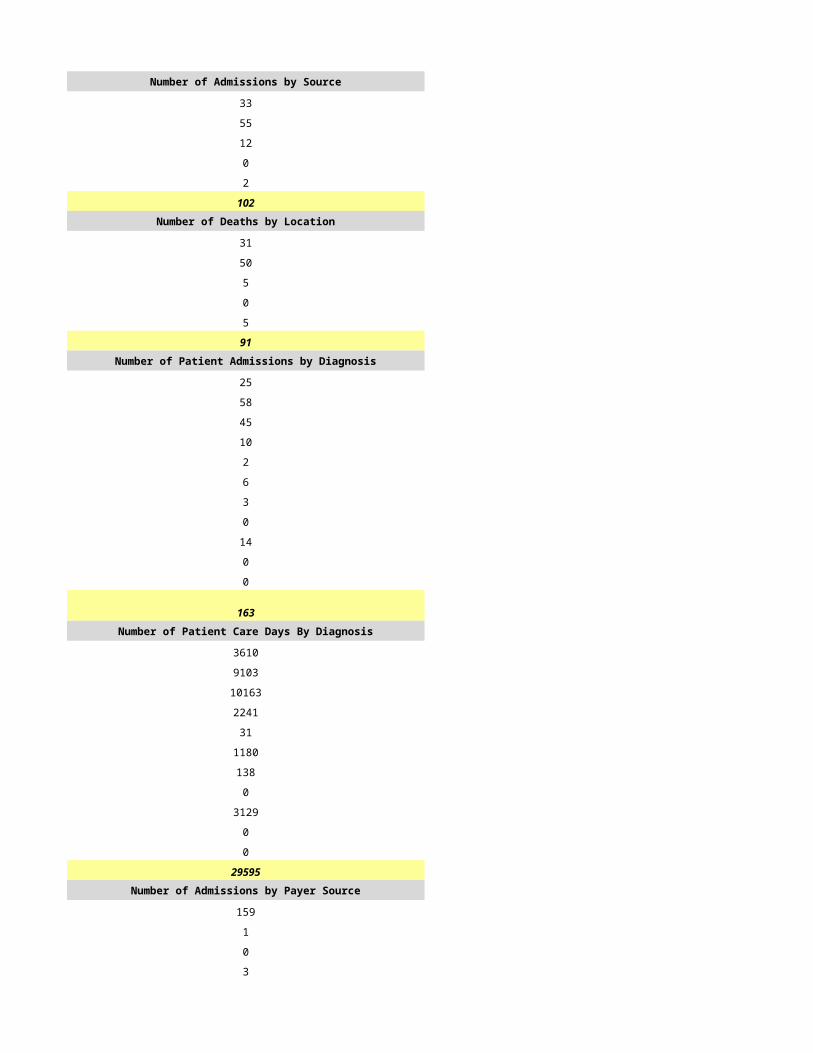
21 10
26 10
48 33
5 2
267 258Number of Deaths by Location Number of Deaths by Location
92 98
69 25
0 0
0 0
0 0
161 123Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
82 48
55 31
15 8
39 60
4 12
6 13
8 10
0 0
33 62
25 14
0 0
267 258Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
7226 4230
4847 2732
1322 705
3437 5287
352 1057
529 1146
705 881
0 0
2908 5464
2203 1234
0 0
23529 22736Number of Admissions by Payer Source Number of Admissions by Payer Source
247 242
18 18
0 0
4 1
0 0
269 261
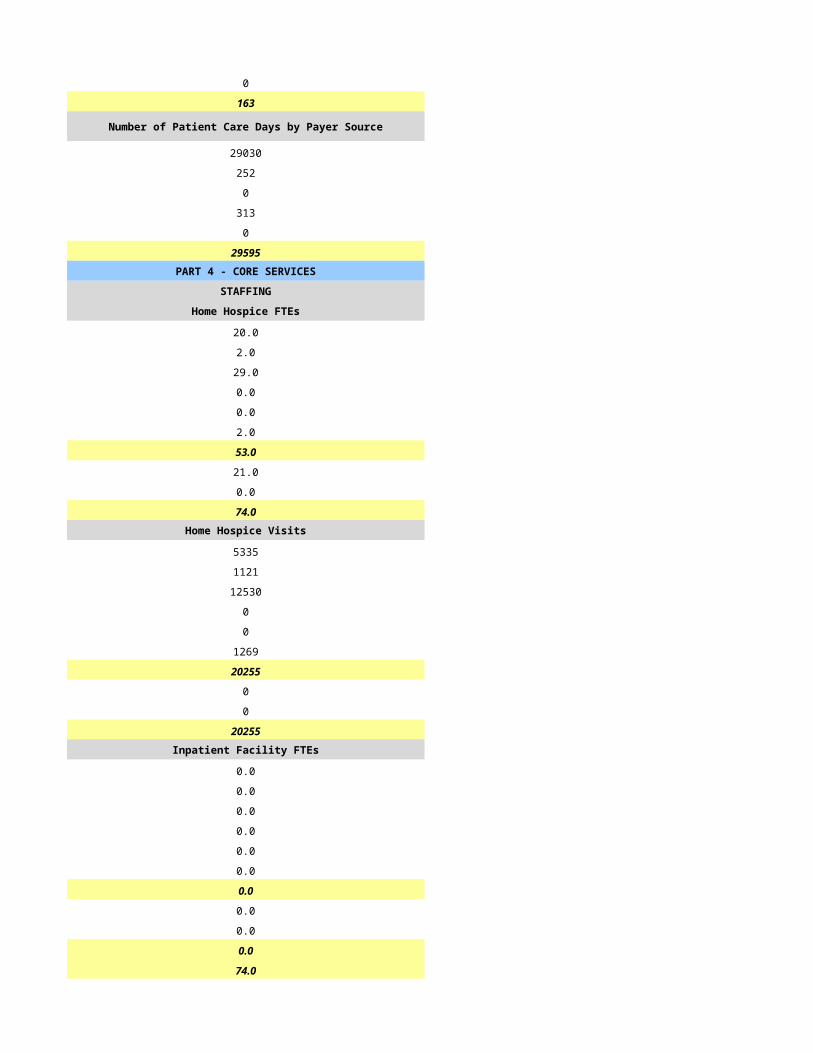
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
21587 21150
1573 1573
0 0
350 87
0 0
23510 22810PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
14.0 12.0
3.0 3.0
5.0 7.0
0.0 0.0
0.0 0.0
0.0 0.0
22.0 22.0
6.0 7.0
2.0 3.0
30.0 32.0Home Hospice Visits Home Hospice Visits
7328 5827
870 809
5476 6529
0 0
0 0
0 0
13674 13165
432 264
1440 961
15546 14390Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
30.0 32.0
CASELOADS CASELOADS
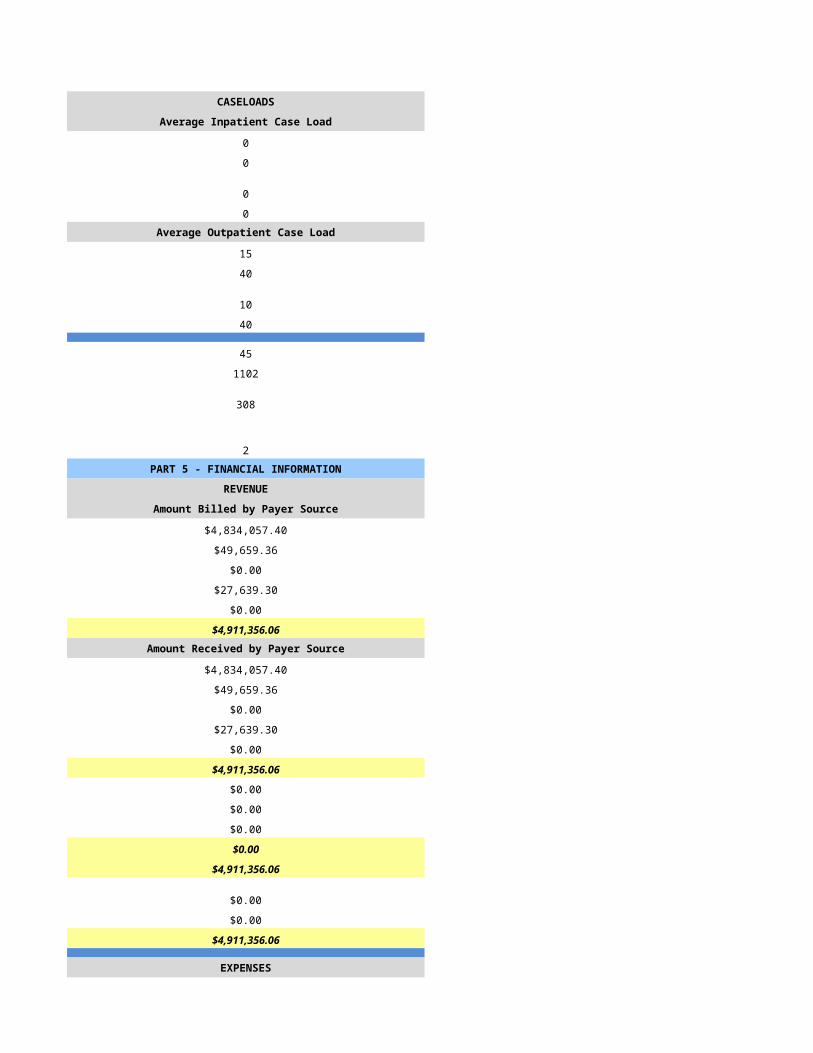
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 0
0 0
0 0
0 0
84 91
669 930
304 243
2 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,304,631.00 $4,625,690.00
$124,796.00 $197,217.00
$0.00 $0.00
$0.00 $11,340.00
$0.00 $0.00
$3,429,427.00 $4,834,247.00Amount Received by Payer Source Amount Received by Payer Source
$3,168,926.00 $4,794,410.00
$260,501.00 $28,497.00
$0.00 $0.00
$0.00 $11,340.00
$0.00 $0.00
$3,429,427.00 $4,834,247.00
$0.00 $0.00
$0.00 $0.00
$66,831.00 $144,585.00
$66,831.00 $144,585.00
$3,362,596.00 $4,689,662.00
$0.00 $0.00
$0.00 $0.00
$3,362,596.00 $4,689,662.00
EXPENSES EXPENSES
$1,201,548.00 $1,461,126.00
$0.00 $0.00
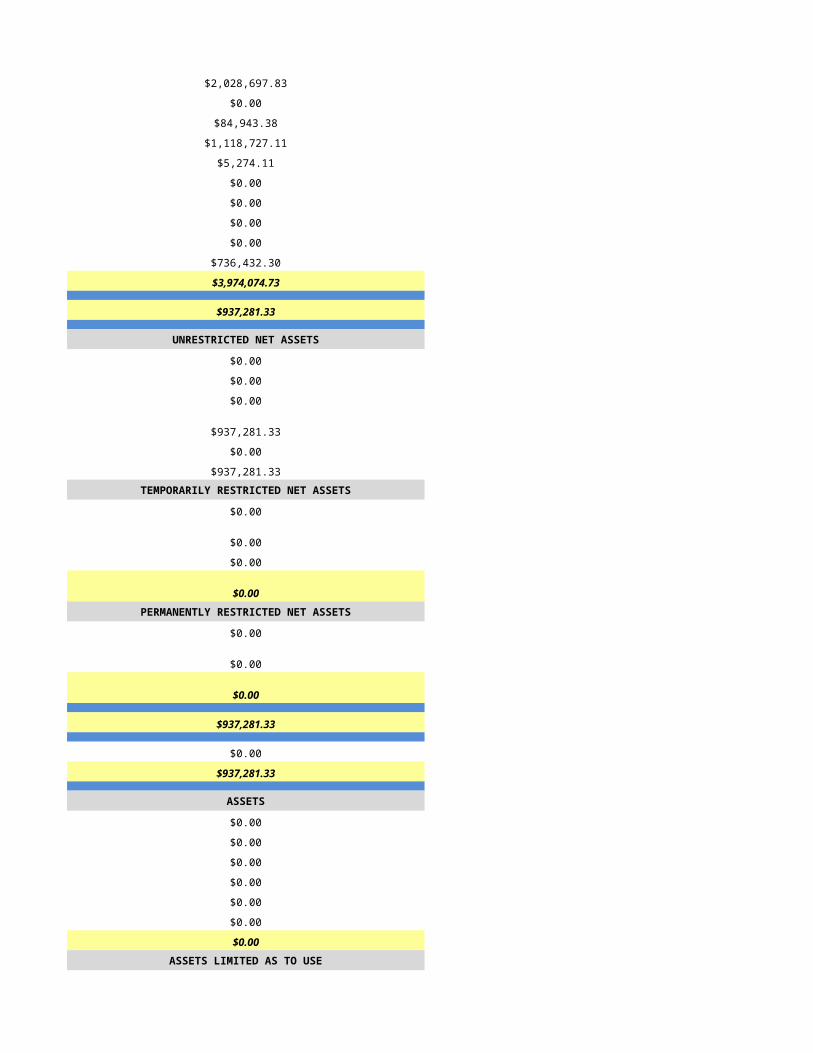
$166,062.00 $202,386.00
$366,361.00 $583,186.00
$171,855.00 $156,423.00
$34,529.00 $56,891.00
$65,492.00 $39,301.00
$18,088.00 $19,851.00
$0.00 $55.00
$124,126.00 $181,700.00
$2,148,061.00 $2,700,919.00
$1,214,535.00 $1,988,743.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,214,535.00 $1,988,743.00
$0.00 $0.00
$1,214,535.00 $1,988,743.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
-$911,353.00 -$1,160,614.00
-$911,353.00 -$1,160,614.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$303,182.00 $828,129.00
$911,353.00 $1,160,614.00
$1,214,535.00 $1,988,743.00
ASSETS ASSETS
$222,249.00 $222,249.00
$0.00 $0.00
$0.00 $0.00
$2,642,944.00 $2,642,944.00
$0.00 $0.00
$77,057.00 $77,057.00
$2,942,250.00 $2,942,250.00ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00 $0.00
$0.00 $0.00
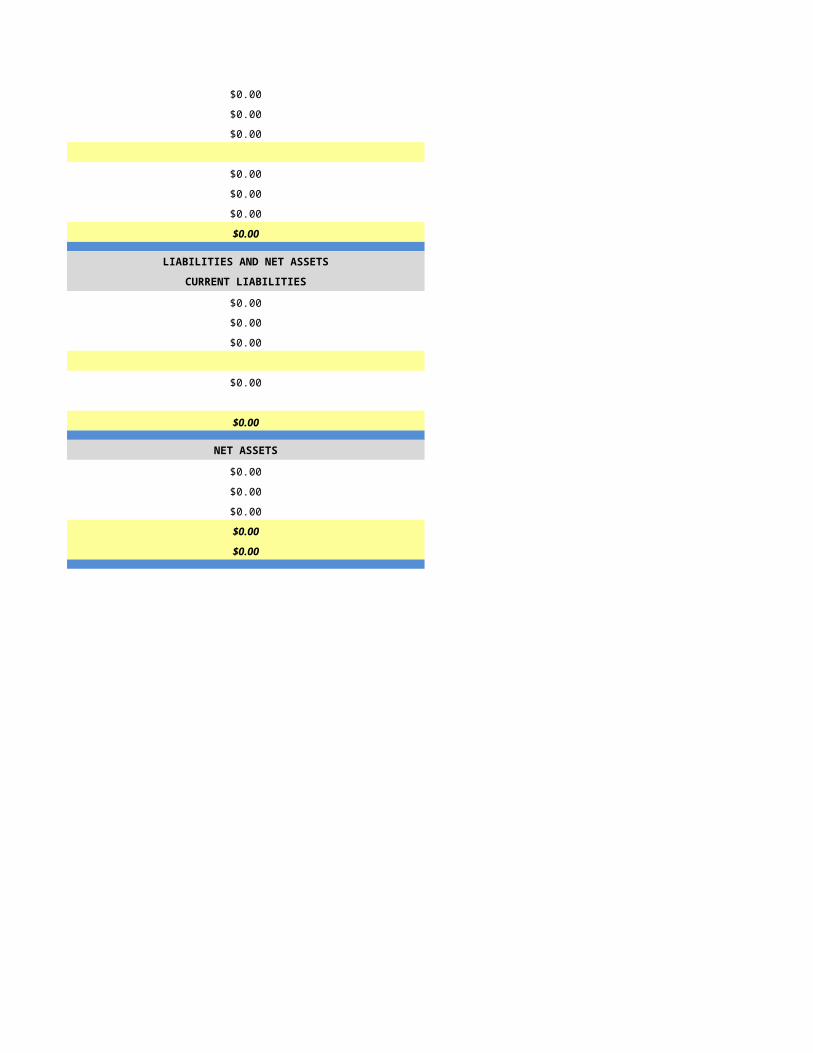
$0.00 $0.00
$0.00 $0.00
$374,727.00 $374,727.00
$8,098.00 $8,098.00
$3,325,075.00 $3,325,075.00
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$379,159.00 $379,159.00
$752,976.00 $752,976.00
$0.00 $0.00
$112,728.00 $112,728.00
$1,451,685.00 $1,451,685.00
NET ASSETS NET ASSETS
$1,873,390.00 $1,873,390.00
$0.00 $0.00
$0.00 $0.00
$1,873,390.00 $1,873,390.00
$3,325,075.00 $3,325,075.00
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
6/30/2015 7/1/2015
HSPC-3009 HSPC-0007
Northern Arizona Healthcare
Northern Arizona Hospice Northland Hospice and Palliative Care, Inc.
203 S Candy Lane 452 N Switzer Canyon Dr
Cottonwood Flaggstaff
AZ AZ
86326 86001
Yavapai Coconino
203 S Candy Lane PB Box 997
Cottonwood Flaggstaff
AZ AZ
86326 86002-0997
Yavapai Coconino
928-639-6676 928-779-1227
Loretta Wellborn Diana Watt
928-773-2492 928-779-1227
[email protected] [email protected]
Christine Pearson
928-773-2519
Dale Wong Richard K. Dixon
928-773-2429 321-473-8561
[email protected] [email protected]
34505AZ 110495
1730110925 1558323583
Yes Yes
031502AZ 31512
Not Accredited Not Accredited
NA
Hospice Service Agency Hospice Service Agency
Voluntary (Not For Profit) Voluntary (Not For Profit)
Primarily Rural Mixed Urban and Rural
Free Standing Free Standing
NA
1/1/2014 1/1/2014
12/31/2014 12/31/2014
NA Olive White Hospice Home
NA ALH4018
NA 752 N Switzer Canyon Drive
NA Flaggstaff
NA 86001
NA Coconino
NA PO Box 997
NA Flaggstaff
NA 86002-0997
NA Coconino
NA 928-779-1227
NA
Primarily Rural Mixed Urban and Rural
NA Assisted Living - Based
NA
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 10
0 0
0 10
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
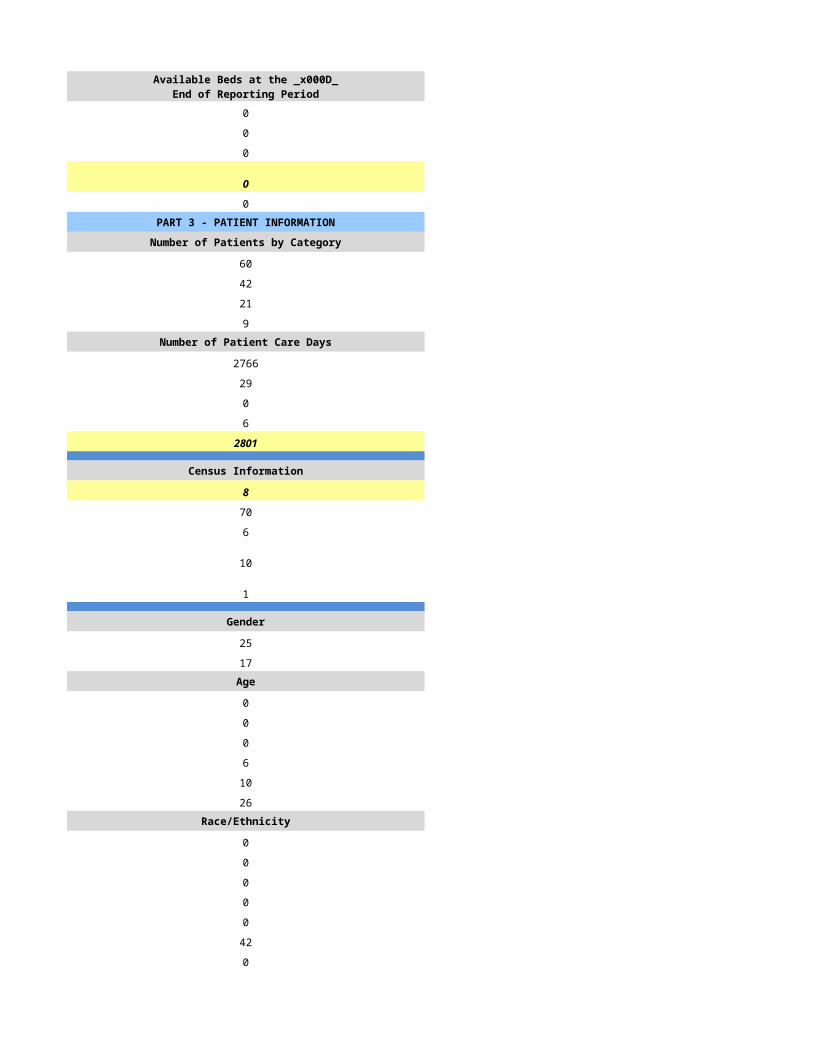
0 0
0 10
0 0
0 10
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
174 411
166 158
157 131
9 27Number of Patient Care Days Number of Patient Care Days
5420 11439
15 4
0 0
35 0
5470 11443
Census Information Census Information
11 21
33 64
7 64
88 45
7 7
Gender Gender
84 93
82 65Age Age
0 2
0 4
24 26
39 35
49 42
54 49Race/Ethnicity Race/Ethnicity
2 31
0 1
0 1
2 13
0 2
162 106
0 4Number of Admissions by Source Number of Admissions by Source
0 114
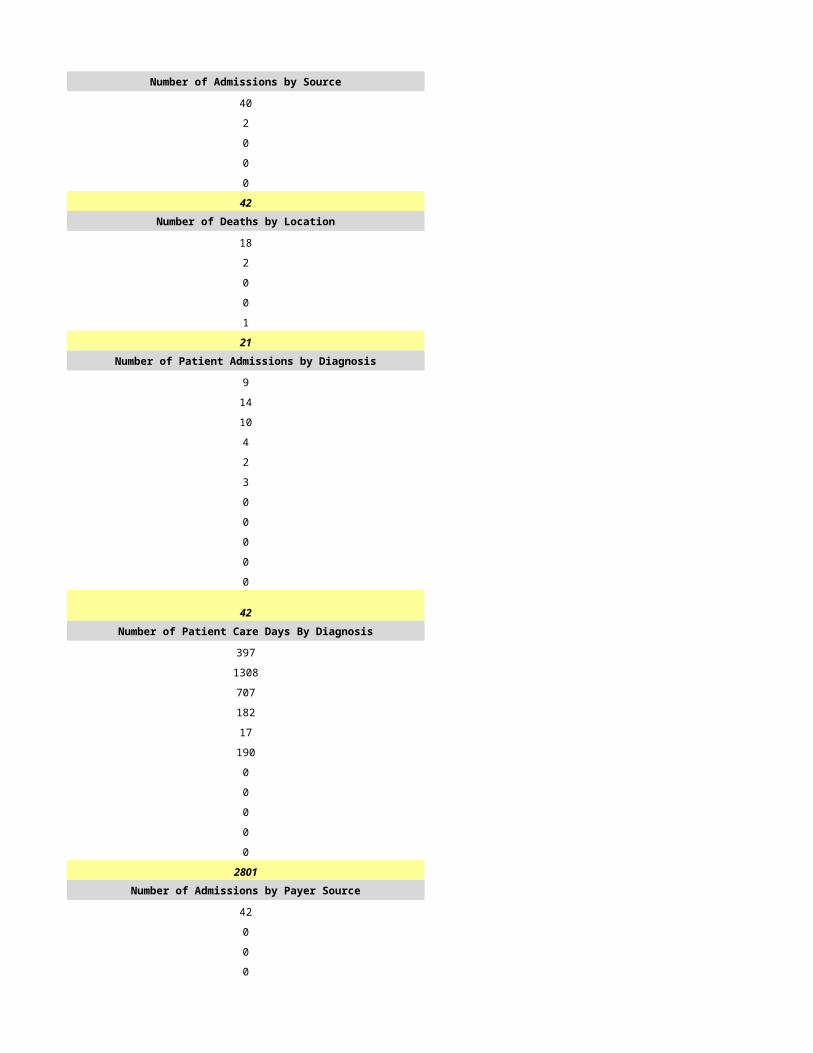
0 12
0 1
0 30
0 1
0 158Number of Deaths by Location Number of Deaths by Location
0 59
0 72
0 0
0 0
0 0
0 131Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
71 0
19 0
2 0
33 0
9 0
16 0
9 0
0 0
5 0
2 0
0 158
166 158Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2264 0
1049 0
5 0
630 0
140 0
299 0
160 0
0 0
215 0
285 0
423 11443
5470 11443Number of Admissions by Payer Source Number of Admissions by Payer Source
149 124
2 10
11 1
5 15
0 8
167 158
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
5063 5674
65 686
224 651
118 625
0 3807
5470 11443PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.0 4.0
0.9 2.0
0.0 1.0
0.0 2.0
0.0 0.0
0.4 0.0
4.0 9.0
1.8 5.0
0.0 1.0
6.0 15.0Home Hospice Visits Home Hospice Visits
0 1362
0 1228
0 586
0 0
0 0
0 3176
0 6352
0 0
0 135
0 6487Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
6.0 0.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 14
0 30
0 8
0 30
24 139
732 6442
74 1379
7 4PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,252,000.00 $1,262,702.00
$0.00 $55,767.00
$0.00 $52,514.00
$0.00 $50,191.00
$0.00 $306,258.00
$1,252,000.00 $1,727,432.00Amount Received by Payer Source Amount Received by Payer Source
$1,252,000.00 $1,011,268.00
$0.00 $55,767.00
$0.00 $52,514.00
$0.00 $50,191.00
$0.00 $306,258.00
$1,252,000.00 $1,475,998.00
$0.00 $0.00
$0.00 $0.00
$481,000.00 $42,588.00
$481,000.00 $42,588.00
$771,000.00 $1,433,410.00
$0.00 $0.00
$0.00 $514,550.00
$771,000.00 $1,947,960.00
EXPENSES EXPENSES
$521,000.00 $1,329,922.00
$0.00 $112,417.00
$0.00 $248,330.00
$41,000.00 $269,154.00
$32,000.00 $65,660.00
$0.00 $44,497.00
$0.00 $0.00
$0.00 $47,523.00
$0.00 $43,412.00
$157,000.00 $341,938.00
$751,000.00 $2,502,853.00
$20,000.00 -$554,893.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$20,000.00 -$554,893.00
$0.00 $0.00
$20,000.00 -$554,893.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$20,000.00 -$554,893.00
$25,500.00 $4,319,981.00
$45,500.00 $3,765,088.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/2/2015 7/3/2015
HSPC-3896 HSPC-3566
Optum Palliative and Hospice Care Optum Palliative and Hospice Care, Inc.
6245 East Broadway Blvd, Suite 600 3003 N. Central Avenue
Tucson Phoenix
AZ AZ
85711 85012
Pima Maricopa
(520)407-8000 602-749-5900
Jean Stewart Vern J. Wulfekuhle
(520)407-8000 602-749-5900
[email protected] [email protected]
Patrick Hanson Patrick K. Hanson
(952) 205-0447 (952)205-0447
[email protected] [email protected]
Jean Stewart Vern J. Wulfekuhle
(520)407-8000 602-749-5900
[email protected] [email protected]
233283 905747
168795409 1700815099
Yes Yes
31555
CHAP CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Mixed Urban and Rural Primarily Urban
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
HSCP-9999
(999) 999-9999
mm/dd/yyyy
Mixed Urban and Rural Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period

0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
332 333
225 345
215 237
65 177Number of Patient Care Days Number of Patient Care Days
24105 30387
84 165
0 0
103 97
24292 30649
Census Information Census Information
67 84
64 58
26 21
71 158
56 79
Gender Gender
169 258
129 175Age Age
0 0
1 4
34 51
31 69
67 112
92 197Race/Ethnicity Race/Ethnicity
3 4
0 2
3 12
32 44
1 0
167 216
19 155Number of Admissions by Source Number of Admissions by Source
109 132
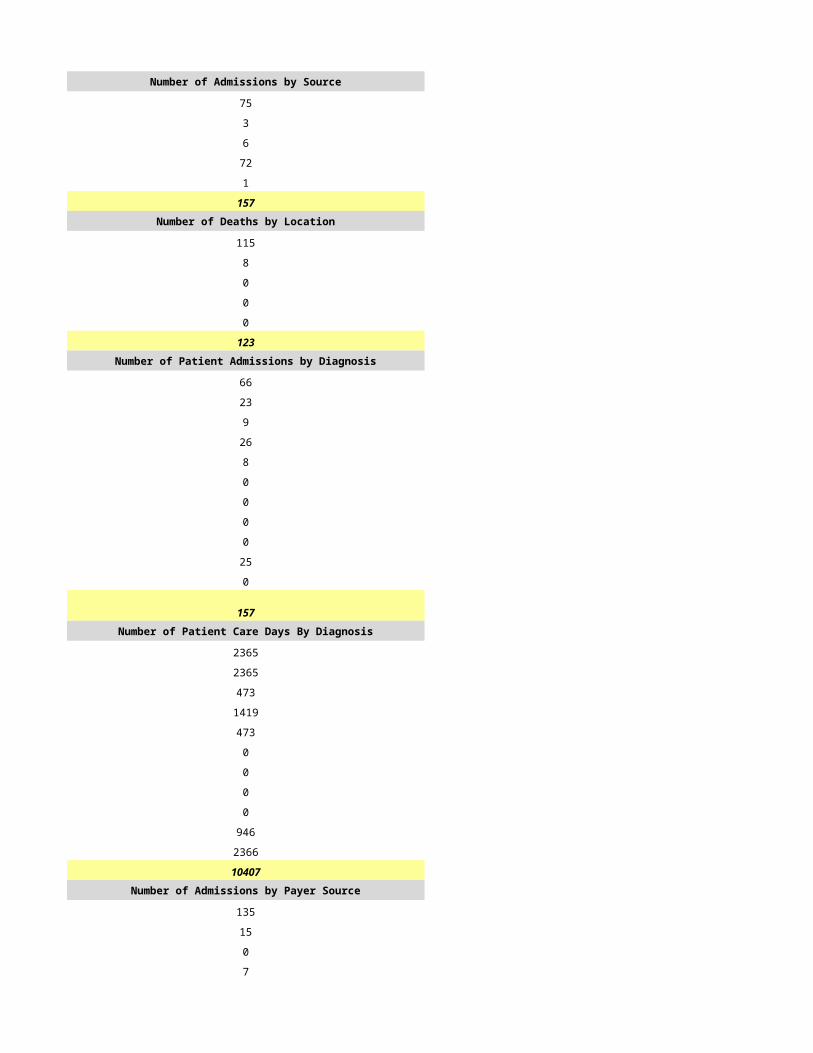
20 81
89 83
7 47
0 2
225 345Number of Deaths by Location Number of Deaths by Location
104 107
19 33
85 96
7 0
0 1
215 237Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
41 60
32 46
39 95
11 64
10 7
11 23
3 16
0 0
27 22
51 10
0 2
225 345Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2192 4397
3131 6389
5837 11451
1522 3522
270 1339
912 1927
15 639
0 0
6960 970
3453 15
0 0
24292 30649Number of Admissions by Payer Source Number of Admissions by Payer Source
188 308
0 0
0 31
0 6
37 0
225 345
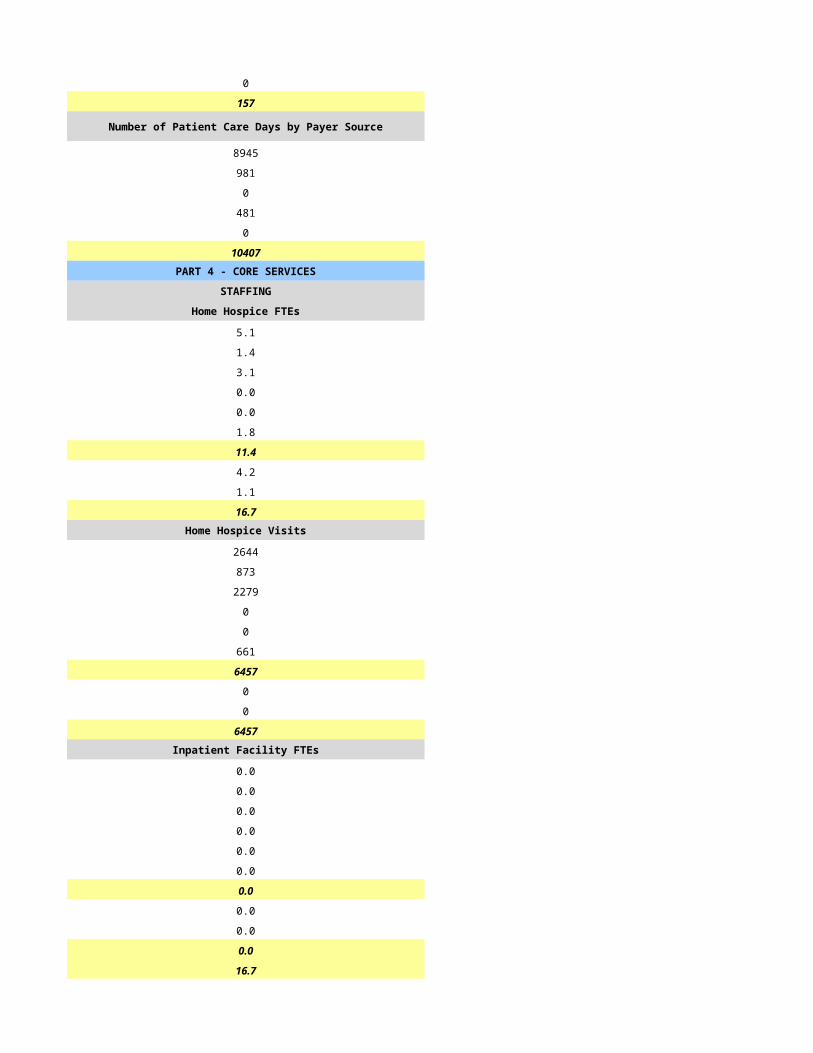
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
22286 27827
0 0
0 0
0 2569
2006 253
24292 30649PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
6.0 11.6
2.0 4.8
6.0 9.1
0.8 2.3
0.0 0.0
0.0 0.1
14.8 27.9
5.0 7.0
1.0 0.8
20.8 35.7Home Hospice Visits Home Hospice Visits
3686 5649
897 1316
3770 5267
213 439
0 0
954 0
9520 12671
13 971
134 1
9667 13643Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
20.8 35.7
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
9 12
35 40
10 10
50 50
12 45
632 2675
2850 735
8 6PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,407,691.00 $0.00
$0.00 $0.00
$0.00 $0.00
$180,756.00 $0.00
$21,643.00 $0.00
$3,610,090.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$3,407,691.00 $0.00
$0.00 $0.00
$0.00 $0.00
$180,756.00 $0.00
$21,643.00 $0.00
$3,610,090.00 $0.00
$0.00 $0.00
$21,643.00 $0.00
$0.00 $0.00
$21,643.00 $0.00
$3,588,447.00 $0.00
$0.00 $0.00
$0.00 $0.00
$3,588,447.00 $0.00
EXPENSES EXPENSES
$2,212,949.00 $0.00
$1,015.00 $0.00
$342,005.00 $0.00
$593,002.00 $0.00
$0.00 $0.00
$0.00 $0.00
$59,819.00 $0.00
$0.00 $0.00
$0.00 $0.00
$336,101.00 $0.00
$3,544,891.00 $0.00
$43,556.00 $0.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$43,556.00 $0.00
$0.00 $0.00
$43,556.00 $0.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$43,556.00 $0.00
$0.00 $0.00
$43,556.00 $0.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/4/2015 7/5/2015
HSPC-0020 HSPC-5648
Pillars Hospice Care, LLC
Peppis House Pillars Hospice Care, LLC
2715 N Wyatt Dr 3038 E Cactus Road 3
Tucson Phoenix
AZ AZ
85712 85032-7150
Pima Maricopa
5301 E Grant Rd
Tucson
AZ
85712
Pima
520-324-2438 602-788-1138
Mary Steele Margaret Napientek
520-324-2438 602-788-1138
[email protected] [email protected]
Steve Bush Marilyn Berglund
520-324-1160 602-788-1138
[email protected] [email protected]
Bret Hicks Margaret Napientek
520-324-1614 602-788-1138
[email protected] [email protected]
407222 841341
1477542892 1588917264
Yes Yes
031514 03-1616
Other CHAP
CMS
Hospice Service Agency Hospice Service Agency
Voluntary (Not For Profit) Proprietary
Primarily Urban Primarily Urban
Hospital - Based Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Primarily Urban Primarily Urban
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
16 0
16 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
16 0
16 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
1565 72
983 47
881 24
111 18Number of Patient Care Days Number of Patient Care Days
38678 6647
277 0
0 0
2429 12
41384 6659
Census Information Census Information
113 18
46 101
9 82
446 7
39 1
Gender Gender
535 30
448 29Age Age
15 0
7 0
146 1
155 7
273 21
387 30Race/Ethnicity Race/Ethnicity
2 0
9 1
10 2
122 2
0 0
828 48
12 6Number of Admissions by Source Number of Admissions by Source
382 12
103 47
21 0
19 0
458 0
983 59Number of Deaths by Location Number of Deaths by Location
301 4
105 19
11 0
19 0
445 1
881 24Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
291 6
59 30
22 7
92 7
56 2
43 2
30 1
1 0
8 1
379 3
2 0
983 59Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
14113 743
6218 3815
3849 759
3323 949
920 10
1312 268
595 9
4 0
1854 99
9162 7
34 0
41384 6659Number of Admissions by Payer Source Number of Admissions by Payer Source
836 59
43 0
3 0
91 0
10 0
983 59
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
35807 6659
1824 0
32 0
3680 0
41 0
41384 6659PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
17.0 2.0
7.0 1.0
7.0 1.5
1.0 1.0
0.0 0.0
0.0 0.0
32.0 6.0
6.0 2.5
1.0 0.3
39.0 3.0Home Hospice Visits Home Hospice Visits
16257 1226
4145 441
10270 2071
1367 103
0 0
304 0
32343 3841
784 0
260 0
33387 3841Inpatient Facility FTEs Inpatient Facility FTEs
7.0 0.0
1.0 0.0
6.0 0.0
1.0 0.0
0.0 0.0
0.0 0.0
15.0 0.0
1.0 0.0
1.0 0.0
17.0 0.0
56.0 0.0
CASELOADS CASELOADS
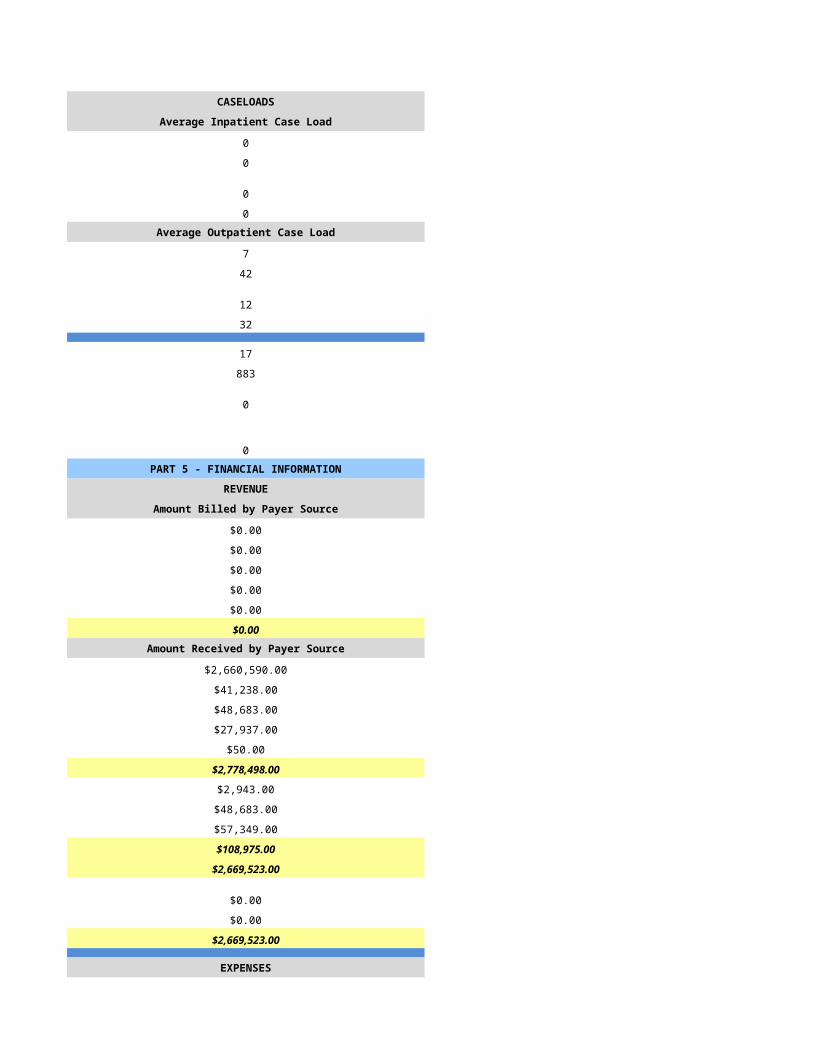
Average Inpatient Case Load Average Inpatient Case Load
6 0
8 0
8 0
8 0Average Outpatient Case Load Average Outpatient Case Load
12 18
20 18
13 10
30 18
100 7
8500 261
1534 24
4 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$9,004,170.00 $1,187,516.00
$472,286.00 $0.00
$48,137.00 $0.00
$1,482,932.00 $0.00
$0.00 $0.00
$11,007,525.00 $1,187,516.00Amount Received by Payer Source Amount Received by Payer Source
$9,004,170.00 $1,108,232.00
$472,286.00 $0.00
$48,137.00 $0.00
$1,482,932.00 $0.00
$0.00 $0.00
$11,007,525.00 $1,187,516.00
$0.00 $0.00
$0.00 $0.00
$3,390,232.00 $53,788.00
$3,390,232.00 $0.00
$7,617,293.00 $1,133,728.00
$0.00 $0.00
$0.00 $148.00
$7,617,293.00 $1,133,876.00
EXPENSES EXPENSES
$3,973,455.00 $453,753.00
$32,770.00 $200.00
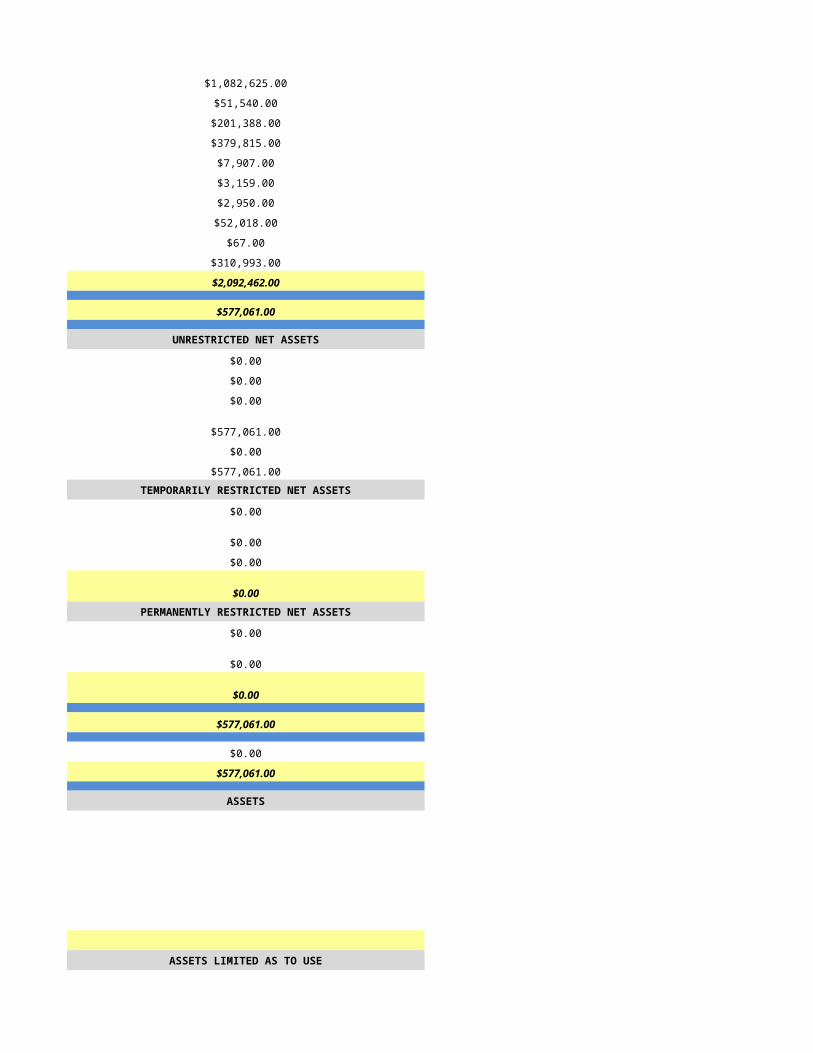
$794,691.00 $68,577.00
$1,099,291.00 $146,947.00
$0.00 $82,898.00
$0.00 $4,483.00
$0.00 $0.00
$204,408.00 $842.00
$0.00 $2,574.00
$0.00 $116,456.00
$6,104,615.00 $876,730.00
$1,512,678.00 $257,146.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,512,678.00 $0.00
$0.00 $0.00
$1,512,978.00 $0.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,512,978.00 $0.00
$0.00 $44,028.00
$1,512,978.00 $271,174.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/6/2015 7/7/2015
HSPC-4076 HSPC-4331
Abode Healthcare, Inc. Prime Care Hospice, LLC
Premier Hospice & Palliative Car Prime Care Hospice, LLC
4530 E Sea Blvd, Suite 165 4225 West Glendale Ave. Suite A 100
Phoenix Phoenix
AZ AZ
85028 85051
Maricopa Maricopa
P O Box 47090
AZ
85068
Maricopa
602-274-7572 623-847-2323
Michael McMaude Jerene Maierle
(970) 828-2212 623-847-2323
[email protected] [email protected]
David Kosloff Satty Bhowra
(206) 576-0087 602-550-4065
[email protected] [email protected]
Elissa Lieberg Satty Bhowra
(206) 576-0086 (602) 550-4065
[email protected] [email protected]
957714 433523
1609944669 1770769978
Yes yes
03-1553 31579
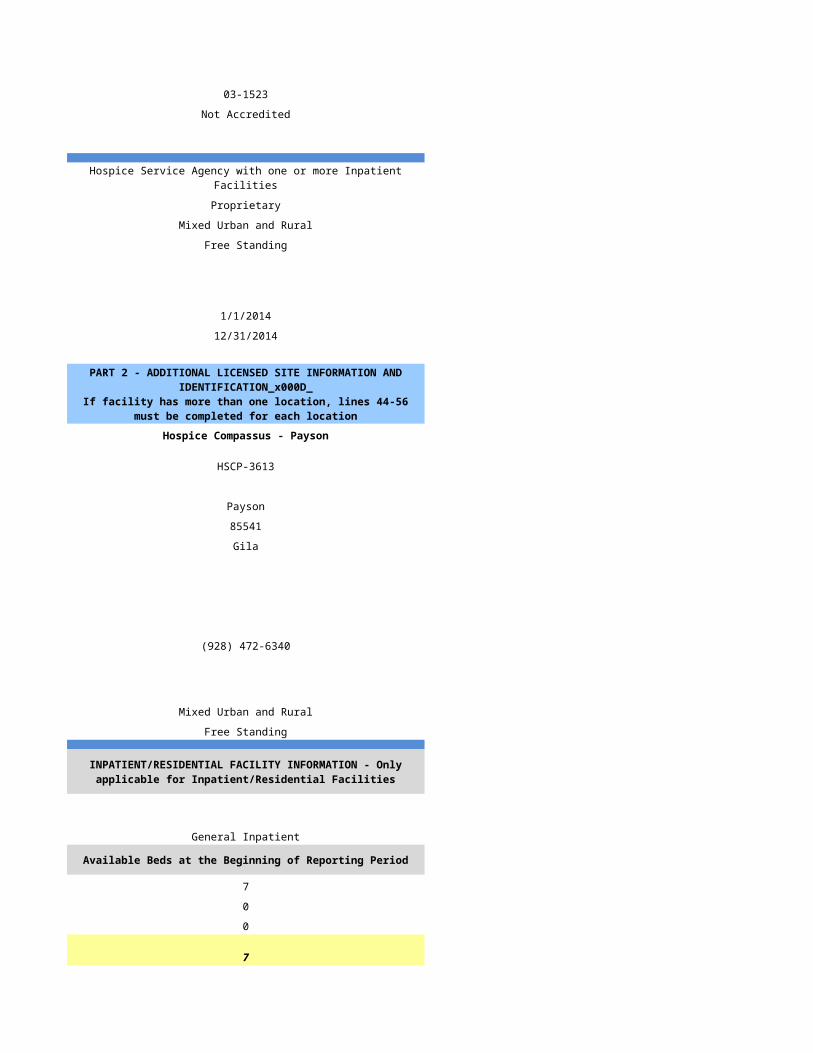
ADHC CHAP
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
HSCP-9999
(999) 999-9999 (999) 999-9999
mm/dd/yyyy mm/dd/yyyy
Primarily Urban Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
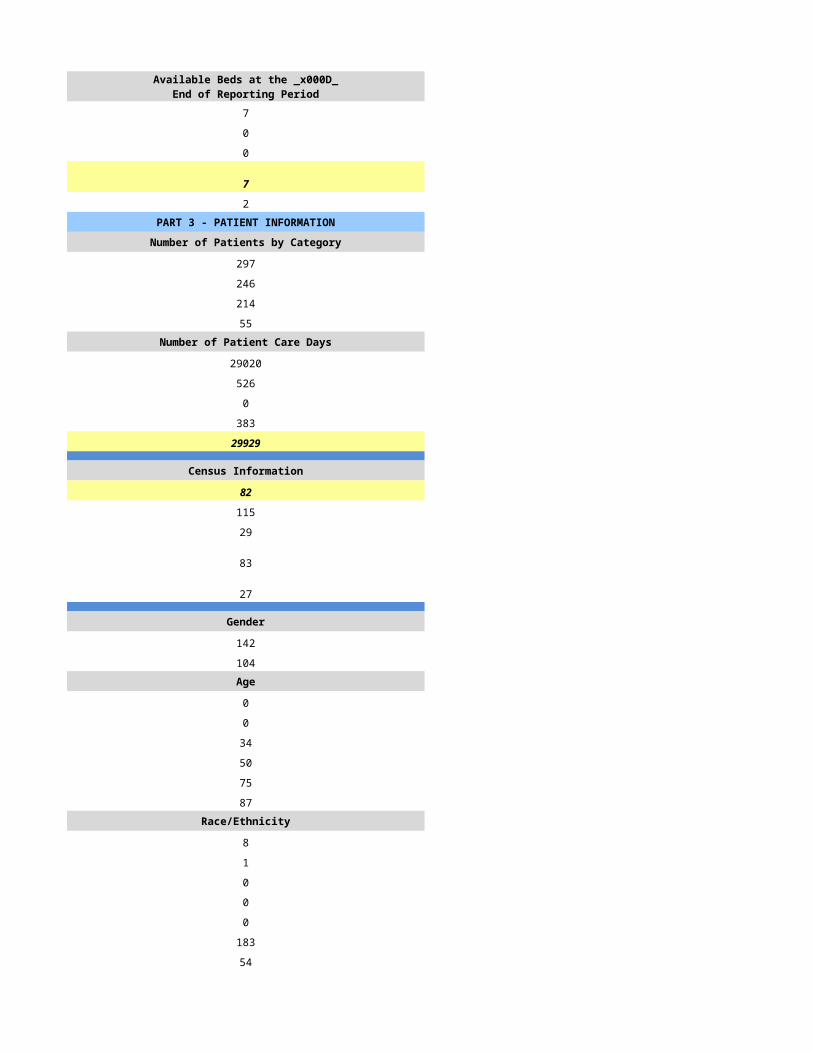
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
0 305
407 157
0 132
123 49Number of Patient Care Days Number of Patient Care Days
36997 22471
70 134
49 0
381 188
37497 22793
Census Information Census Information
103 62
81 126
35 49
104 28
84 20
Gender Gender
0 100
0 57Age Age
0 0
0 1
0 10
0 16
0 44
0 86Race/Ethnicity Race/Ethnicity
0 0
0 1
0 1
0 15
0 0
0 140
0 0Number of Admissions by Source Number of Admissions by Source
15 60
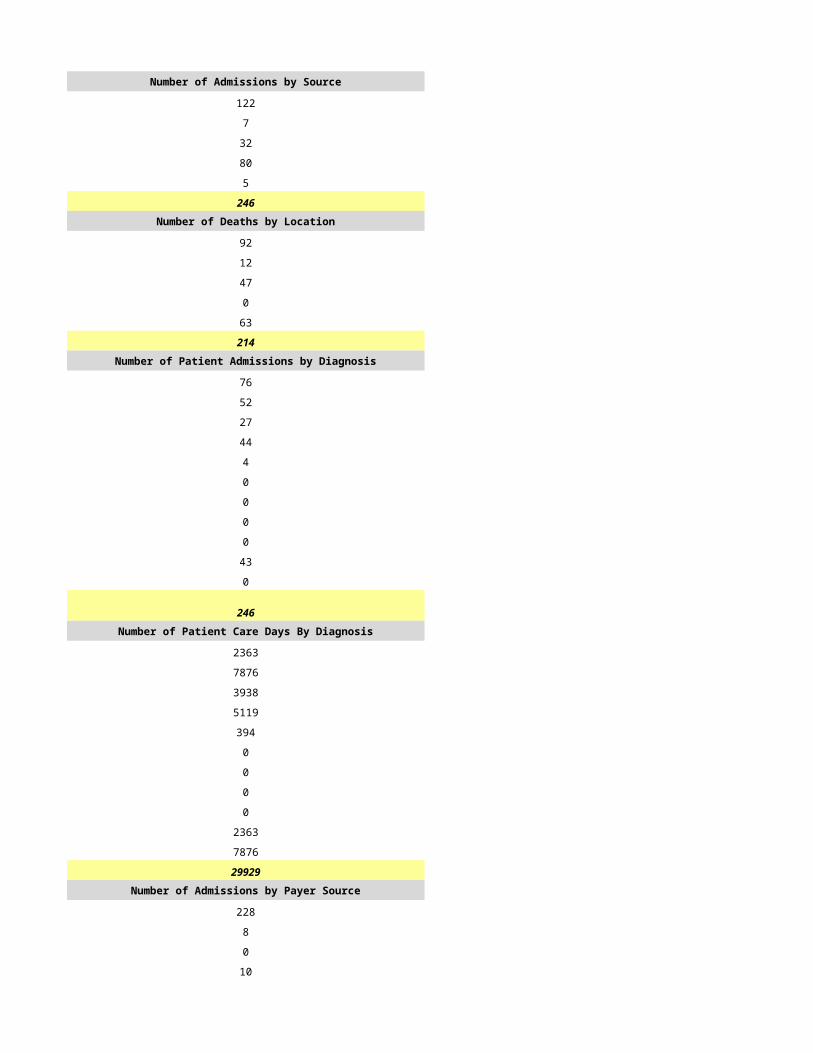
288 69
0 23
104 0
0 5
407 157Number of Deaths by Location Number of Deaths by Location
107 46
258 58
16 19
26 2
6 7
413 132Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
58 28
78 31
143 36
64 22
42 1
4 6
14 4
0 0
4 0
0 28
0 0
407 156Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
55 4406
85 3350
72 8135
57 2878
24 63
28 585
0 257
0 0
0 222
55 2897
0 0
376 22793Number of Admissions by Payer Source Number of Admissions by Payer Source
375 147
0 0
11 3
22 7
0 0
407 157
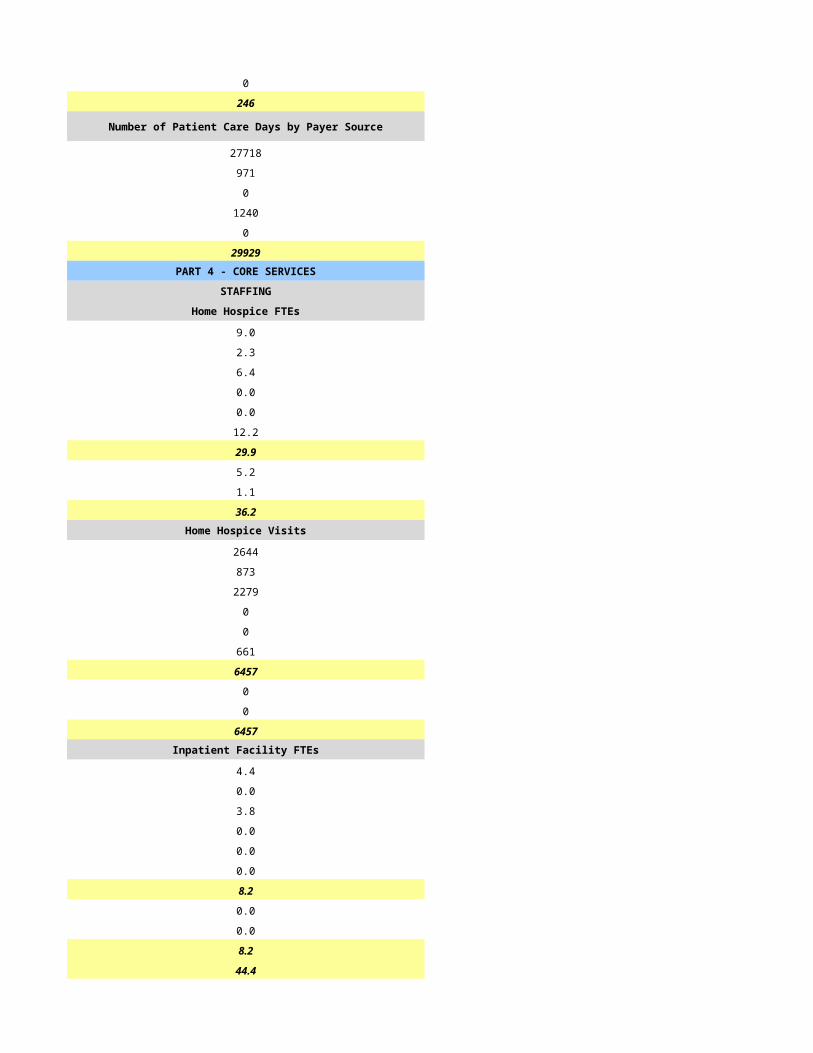
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
346 21684
0 186
10 71
20 852
0 0
376 22793PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
6.5 8.0
1.0 2.0
11.4 5.5
0.0 3.0
0.0 0.0
9.3 2.0
28.2 20.5
6.4 13.0
3.0 0.5
37.6 34.0Home Hospice Visits Home Hospice Visits
0 22926
0 3316
0 21685
0 196
0 0
0 829
0 48952
0 0
0 60
0 49012Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
37.6 34.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
0 12
0 30
0 12
0 60
0 13
0 979
0 132
0 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$6,832,749.00 $3,678,757.60
$0.00 $30,677.28
$0.00 $11,639.54
$30,174.00 $158,013.43
$0.00 $0.00
$6,862,923.00 $3,879,087.85Amount Received by Payer Source Amount Received by Payer Source
$6,063,547.00 $3,678,477.93
$0.00 $41,186.20
$0.00 $11,639.54
$71,359.00 $98,355.06
$0.00 $0.00
$6,134,906.00 $3,829,658.73
$0.00 $50,621.21
$0.00 $11,639.54
$17,537.00 $75,537.39
$17,537.00 $137,798.14
$6,117,369.00 $3,691,860.59
$0.00 $0.00
$2,544.00 $0.00
$6,119,913.00 $3,691,860.59
EXPENSES EXPENSES
$2,896,607.00 $2,105,125.96
$338,214.00 $112,900.00
$407,848.00 $15,362.56
$1,092,159.00 $659,825.58
$38,099.00 $10,959.70
$19,297.00 $18,723.00
$43,722.00 $337,531.81
$13,657.00 $1,977.00
$37,473.00 $245.49
$716,305.00 $199,861.20
$5,603,381.00 $3,462,512.30
$516,532.00 $229,348.29
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$516,532.00 $229,348.29
$0.00 $0.00
$516,532.00 $229,348.29TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$516,532.00 $229,348.29
$30,093,818.00 $0.00
$30,610,350.00 $229,348.29
ASSETS ASSETS
$310,133.31
$0.00
$0.00
$610,439.60
$0.00
$0.00
$920,572.91ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
$0.00
$0.00
$0.00
$0.00
$3,521.46
$0.00
$924,094.37
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
$0.00
$82,553.83
$0.00
$0.00
$82,553.83
NET ASSETS NET ASSETS
$0.00
$0.00
$0.00
$0.00
$82,553.83
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/8/2015 7/9/2015
HSPC-4985 HSPC-5715
Dr. Khalid Shirif Khalid Shirif
Reflections Hopsice Renaissance Hospice
1840 E University Dr. 1840 E University Dr Ste 3
Mesa Mesa
AZ AZ
85203 85203
Maricopa Maricopa
(480) 246-3560 480-268-2660
Robert Lafler Robert Lafler
(480) 246-3560 480-268-2660
[email protected] [email protected]
Babara Mackerman Barbara Mackerman
(480) 246-3560 480-268-2660
[email protected] [email protected]
Amy Craig Amy Craig
(480) 246-3560 480-268-2660
[email protected] [email protected]
829168
1295038297 1295074904
Yes Yes
31601 31619
JCAHO JCAHO
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
HSCP-9999
Primarily Urban Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
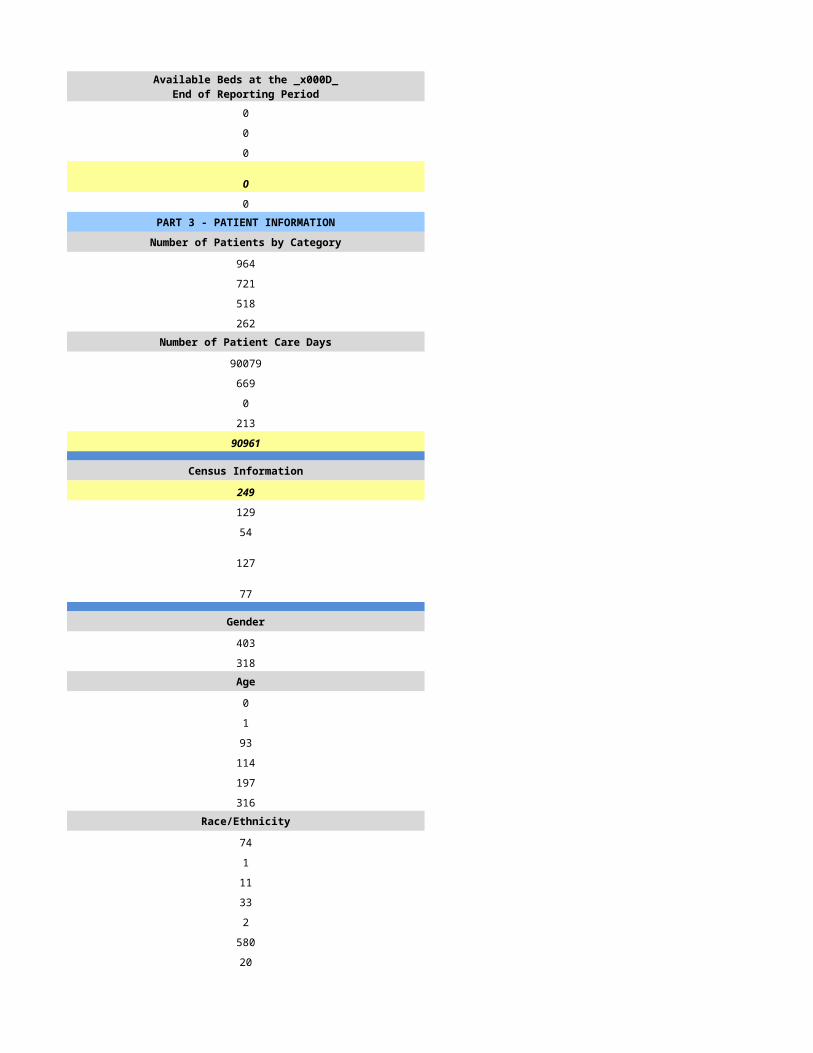
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
505 3
337 3
208 1
163 6Number of Patient Care Days Number of Patient Care Days
39252 418
258 4
2 0
140 0
39652 422
Census Information Census Information
109 1
140 85
59 90
58 0
35 0
Gender Gender
205 5
132 2Age Age
0 0
0 0
24 0
54 2
103 1
156 4Race/Ethnicity Race/Ethnicity
3 0
2 0
12 1
30 0
3 0
278 6
0 0Number of Admissions by Source Number of Admissions by Source
109 3
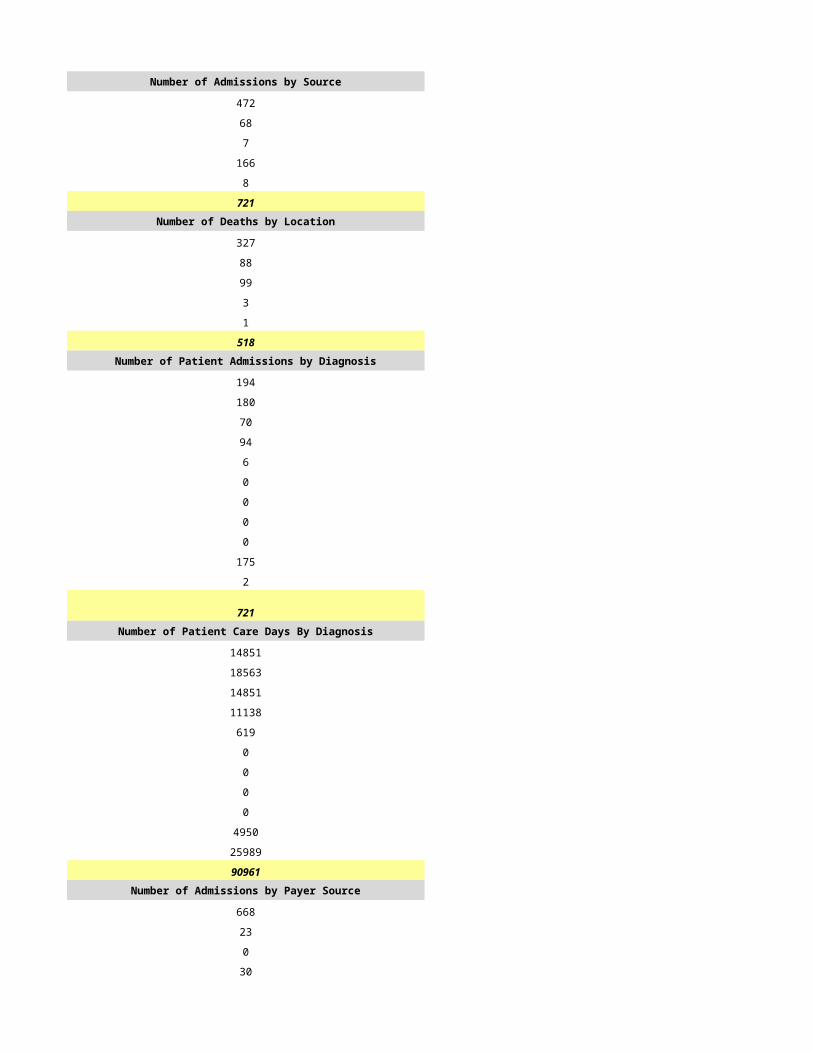
187 0
33 0
2 0
6 0
337 3Number of Deaths by Location Number of Deaths by Location
55 1
116 0
26 0
2 0
9 0
208 1Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
55 1
55 1
133 1
19 0
4 0
15 0
6 0
0 0
19 0
10 0
21 0
Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
5234 9
6891 26
17114 173
2442 90
523 0
730 0
349 0
0 0
1745 0
698 0
3926 0
39652 298Number of Admissions by Payer Source Number of Admissions by Payer Source
322 3
0 0
4 0
11 0
0 0
337 3
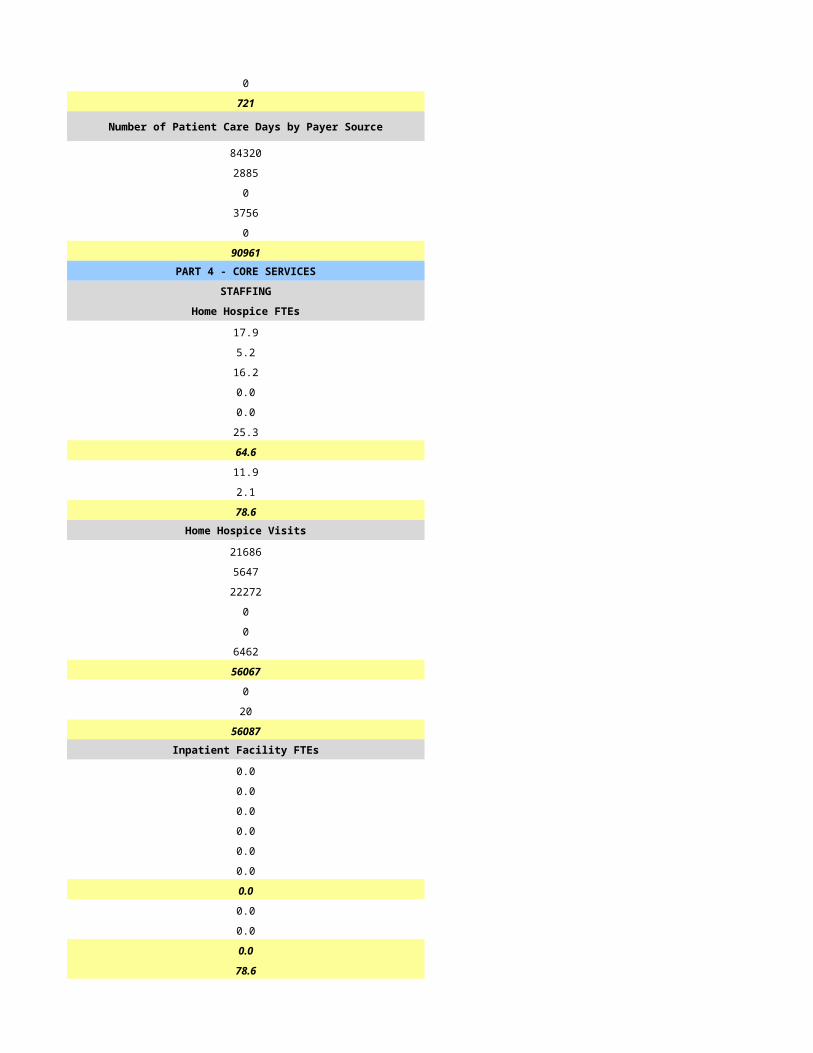
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
39055 422
0 0
387 0
210 0
0 0
39652 422PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
14.0 14.0
3.0 3.0
14.0 14.0
2.0 2.0
0.0 0.0
3.0 9.0
36.0 42.0
11.0 10.0
1.0 2.0
48.0 54.0Home Hospice Visits Home Hospice Visits
10811 187
2620 34
22748 310
40 0
0 0
2917 24
39136 555
1071 0
845 4
41052 559Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
48.0 54.0
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
13 7
35 7
11 7
52 7
25 5
1098 17
517 3
8 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$6,630,168.75 $96,593.64
$329.62 $0.00
$0.00 $0.00
$38,325.29 $0.00
$0.00 $0.00
$6,668,823.66 $96,593.64Amount Received by Payer Source Amount Received by Payer Source
$6,497,564.88 $94,661.78
$0.00 $0.00
$0.00 $0.00
$12,003.12 $0.00
$0.00 $0.00
$6,509,568.00 $94,661.78
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$6,509,568.00 $94,661.78
$0.00 $0.00
$0.00 $0.00
$6,509,568.00 $94,661.78
EXPENSES EXPENSES
$2,680,125.63 $0.00
$931,530.30 $12,427.00
$292,819.51 $0.00
$1,430,992.00 $19,693.00
$6,650.00 $2,024.00
$72,573.00 $0.00
$0.00 $0.00
$0.00 $0.00
$358.00 $0.00
$322,514.00 $9,741.00
$5,737,562.44 $43,885.00
$772,005.56 $50,776.78
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$772,005.56 $50,776.78
$0.00 $0.00
$772,005.56 $50,776.78TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$772,005.56 $50,776.78
$157,407.00 $0.00
$929,412.56 $50,776.78
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/10/2015 7/11/2015
HSPC-4126 HSPC-5345
Sacred Heart Hospice, Inc Martin Hanson
Sacred Heart Hospice Sante Hospice
15255 N 40th Street, Ste 125 8502 Princes Road, Suite 200
Phoenix Scottsdale
AZ AZ
85032 85255
Maricopa Maricopa
7141 N 51st Ave, Suite C 8502 Princes Road, Suite 200
Glendale Scottsdale
AZ AZ
85302 85255
Maricopa Maricopaa
(602)476-2047 480-745-3015
Irma G Ruiz Cody Houglum
(602) 476-2047 480-745-3015
[email protected] [email protected]
Eric L Hayes Greg Ficek
623-939-7584 971-599-5017
[email protected] [email protected]
Susan Tunks Ramsey D Badre
(602) 476-2047 912-634-9197
[email protected] [email protected]
564561 N/A
1437277100 1700154531
Yes Yes
31588 03-1606
JCAHO CHAP
No
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
0 N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
Primarily Urban Primarily Urban
0 N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
238 341
95 203
43 128
67 61Number of Patient Care Days Number of Patient Care Days
11004 19255
28 41
0 0
3 72
11035 19368
Census Information Census Information
30 53
84 81
42 51
0 38
0 11
Gender Gender
63 69
48 59Age Age
0 0
0 0
11 4
20 25
32 62
48 112Race/Ethnicity Race/Ethnicity
0 0
3 1
5 0
33 1
0 0
63 27
7 174Number of Admissions by Source Number of Admissions by Source
76 60
17 120
2 23
0 0
0 0
95 203Number of Deaths by Location Number of Deaths by Location
12 21
29 69
2 21
0 0
0 0
43 111Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
17 32
43 45
10 49
14 34
5 6
0 7
2 3
0 0
1 13
3 10
0 4
95 203Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
834 1270
6279 3996
1627 9145
1343 1325
498 568
0 170
177 100
0 0
76 1588
201 1023
0 173
11035 19358Number of Admissions by Payer Source Number of Admissions by Payer Source
92 201
2 0
0 0
1 2
0 0
95 203
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
10321 19348
108 0
0 0
606 10
0 0
11035 19358PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.5 6.5
1.0 1.0
2.5 6.0
2.0 1.0
0.3 0.0
1.0 0.0
10.3 14.5
6.0 3.0
2.0 0.0
18.3 17.5Home Hospice Visits Home Hospice Visits
2141 4337
963 1380
2219 5002
90 173
0 35
966 7
6379 10934
0 97
173 229
6552 11260Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
18.3 17.5
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
9 12
30 65
12 10
30 85
9 10
537 1032
74 120
14 4PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,703,597.00 $3,375,268.00
$18,265.51 $0.00
$0.00 $0.00
$95,516.76 $1,352.00
$0.00 $0.00
$1,817,379.27 $3,376,620.00Amount Received by Payer Source Amount Received by Payer Source
$1,257,599.81 $3,084,629.00
$22,532.00 $0.00
$0.00 $0.00
$7,763.85 $1,352.00
$0.00 $0.00
$1,287,895.66 $3,085,981.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,287,895.66 $3,085,981.00
$0.00 $0.00
$0.00 $0.00
$1,287,895.66 $3,085,981.00
EXPENSES EXPENSES
$815,493.02 $1,269,247.00
$0.00 $162,628.00
$28,101.99 $380,266.00
$143,826.03 $439,135.00
$1,750.00 $29,894.00
$23,646.07 $6,256.00
$0.00 $0.00
$2,463.00 $2,035.00
$8,122.86 $2,838.00
$55,753.59 $416,102.00
$1,079,156.56 $2,708,401.00
$208,739.10 $377,580.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$208,739.10 $377,580.00
$0.00 $0.00
$208,739.10 $377,580.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$208,739.10 $377,580.00
-$24,657.00 $0.00
$184,082.10 $377,580.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/12/2015 7/13/2015
HSPC-5171 HSPC-3731
Holden Enterprises, Inc. / Ruth Siegel
Seasons Hospice of Arizona LLC SHAPC, LLC dba Serenity Hospice & Palliative Care
2020 N Central Ave Suite 170 2999 North 44tth Street, 225
Phoenix Phoenix
AZ AZ
85004-4424 85018
Maricopa Maricopa
Same
480.606.1011 602.216.2273
Chrissy Beardsley Shawn McAffee, CEO
480.606.1013 602.216.2273
[email protected] [email protected]
David Donenberg see CEO
847.692.1092
Jermaine Lynch Larry Litman / Kelli Casady
847-692-1083 602-789-8104
[email protected] [email protected]
689505
1053609727 1912969387
Yes Yes
03-1603 31561
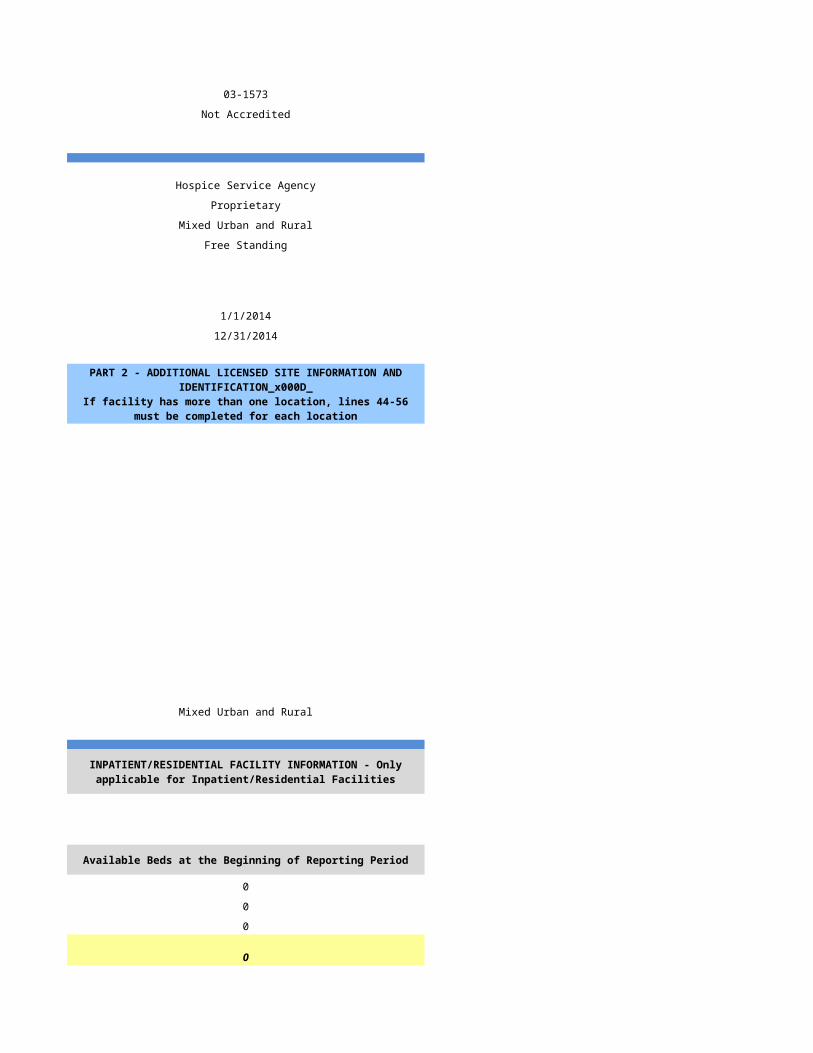
JCAHO Not Accredited
Hospice Service Agency Hospice Service Agency with one or more hospice inpatient facilities
Proprietary Proprietary
Mixed Urban and Rural Mixed Urban and Rural
Free Standing Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A SHAPC, LLC dba Serenity House
HSPC-4736
4122 North 17th Street
Phoenix
85016
Maricopa
Same
602-216-2273
Mixed Urban and Rural Mixed Urban and Rural
Free Standing
N/A
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 20
0 0
0 0
0 20
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
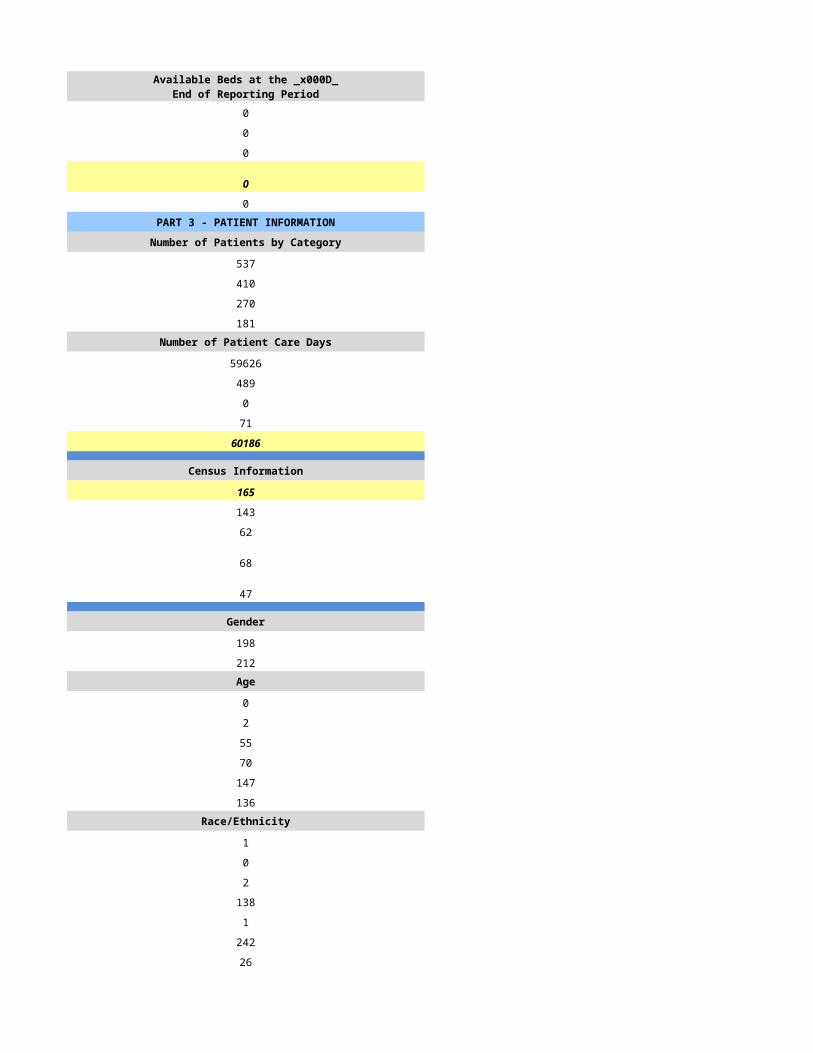
0 20
0 0
0 0
0 20
0 4PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
309 707
309 541
234 412
96 118Number of Patient Care Days Number of Patient Care Days
32433 52538
145 425
0 0
517 1061
33095 54024
Census Information Census Information
91 148
95 138
30 22
85 169
82 64
Gender Gender
233 271
177 270Age Age
0 0
0 5
33 85
67 114
94 141
115 196Race/Ethnicity Race/Ethnicity
4 5
0 4
11 19
29 64
0 3
329 354
37 92Number of Admissions by Source Number of Admissions by Source
11 194
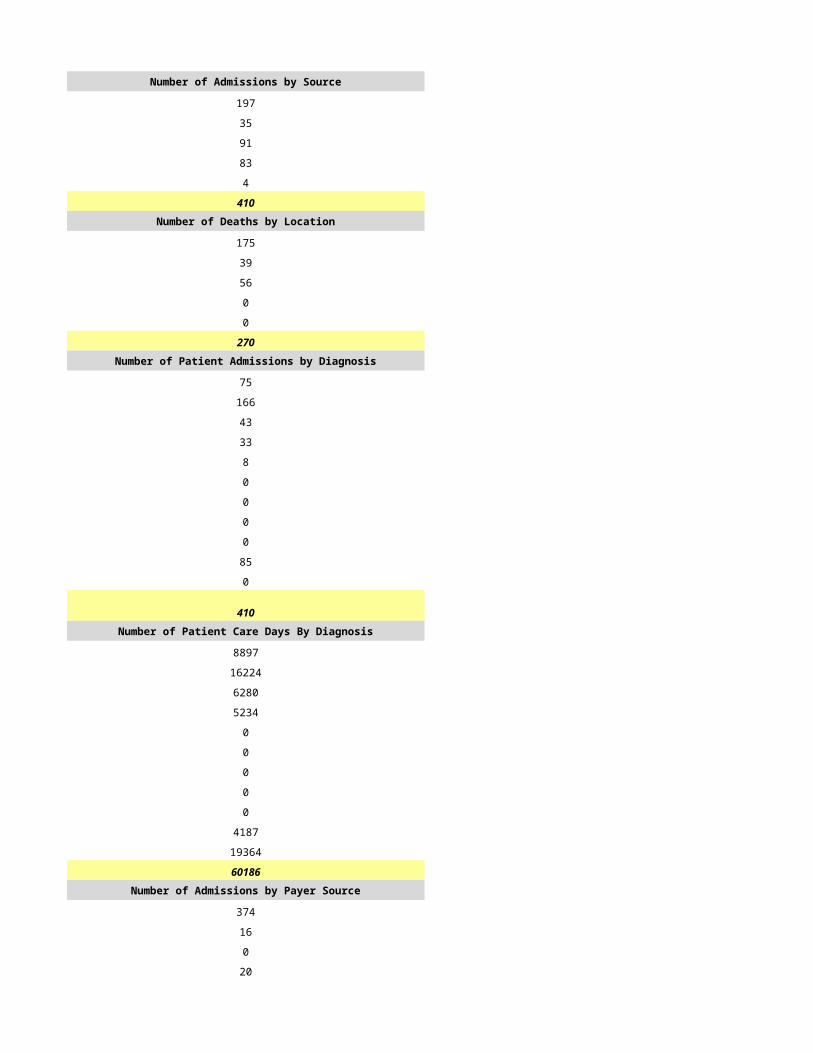
81 99
110 29
95 0
0 219
309 541Number of Deaths by Location Number of Deaths by Location
90 100
0 66
85 28
59 1
0 217
234 412Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
33 132
50 123
38 112
27 71
5 23
0 34
3 20
4 1
25 13
124 12
0 0
309 541Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
3491 4824
5506 13162
8434 20129
2531 9310
88 646
0 2439
20 768
399 24
3511 2028
7496 245
1619 449
33095 54024Number of Admissions by Payer Source Number of Admissions by Payer Source
280 470
2 27
0 0
25 11
2 33
309 541
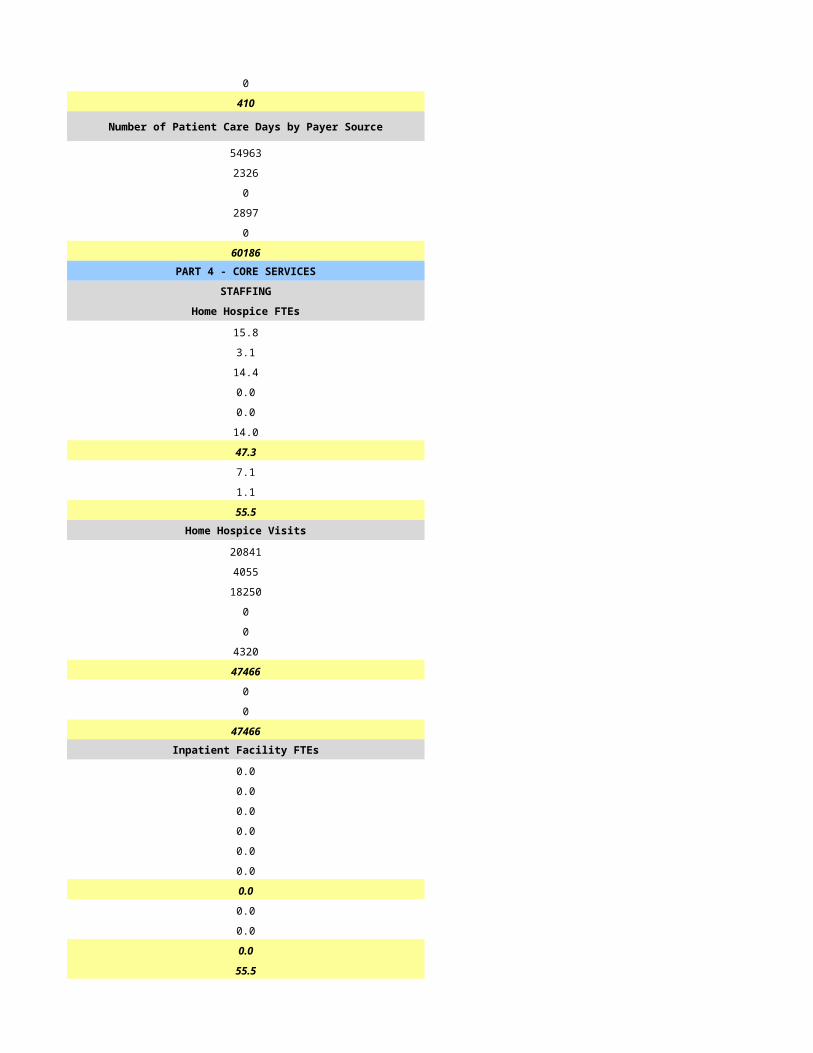
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
31651 52401
16 298
37 0
1163 919
228 406
33095 54024PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
7.0 18.6
7.0 4.3
9.0 12.3
3.0 1.3
0.0 0.0
2.0 3.4
28.0 40.0
12.0 17.9
0.0 1.0
40.0 59.0Home Hospice Visits Home Hospice Visits
9196 13315
2277 3102
8322 16746
224 317
0 0
2198 163
22217 33643
960 0
11 201
23188 33844Inpatient Facility FTEs Inpatient Facility FTEs
0.0 8.0
0.0 0.4
0.0 9.0
0.0 0.7
0.0 0.0
0.0 0.4
0.0 18.0
0.0 4.8
0.0 0.0
0.0 23.0
0.0 82.0
CASELOADS CASELOADS
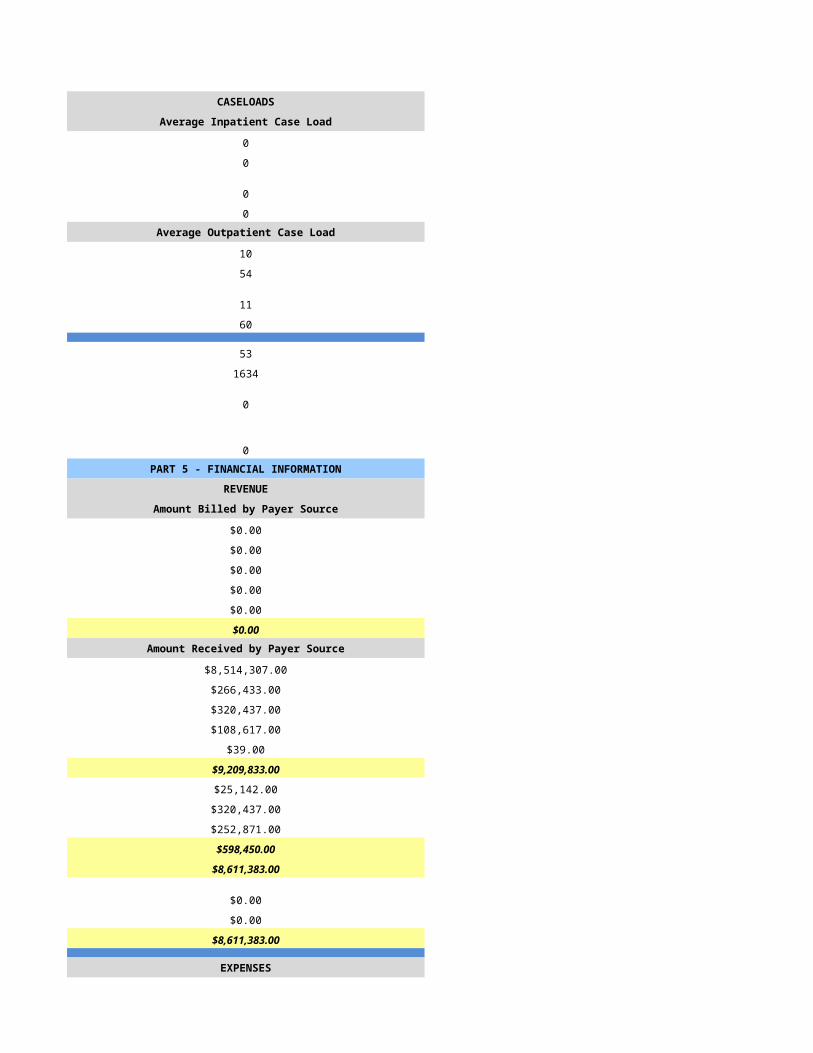
Average Inpatient Case Load Average Inpatient Case Load
0 6
0 6
0 6
0 6Average Outpatient Case Load Average Outpatient Case Load
42 21
84 35
38 17
129 46
42 34
334 898
847 746
0 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$5,327,450.00 $10,020,872.00
$21,294.00 $0.00
$59,052.00 $0.00
$199,416.00 $0.00
-$150.00 $0.00
$5,607,062.00 $10,020,872.00Amount Received by Payer Source Amount Received by Payer Source
$5,052,391.00 $9,172,358.00
$21,294.00 $143,127.00
$59,052.00 $0.00
$159,589.00 $83,540.00
-$2,570.00 $621,847.00
$5,607,062.00 $10,020,872.00
$0.00 $0.00
-$25,896.00 $0.00
-$2,283.00 $19,759.00
-$28,179.00 $19,759.00
$5,578,883.00 $10,040,631.00
$0.00 $0.00
$0.00 $0.00
$5,578,883.00 $10,040,631.00
EXPENSES EXPENSES
$2,675,395.00 $4,405,942.00
$6,570.00 $165,162.00
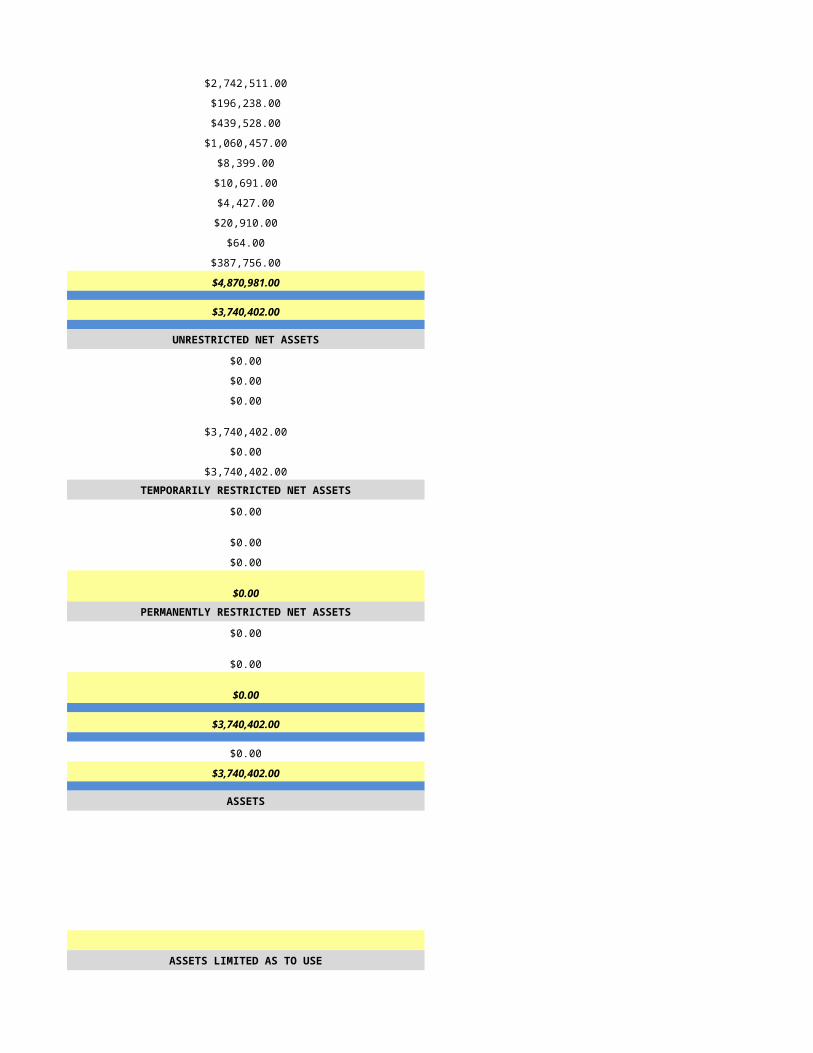
$514,655.00 $935,280.00
$817,944.00 $1,229,647.00
$0.00 $377,659.00
$0.00 $66,173.00
$57,759.00 $0.00
$94,712.00 $0.00
$33,782.00 $339,524.00
$1,002,221.00 $1,839,972.00
$5,203,038.00 $9,359,359.00
$0.00 $681,272.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $681,272.00
$0.00 $0.00
$0.00 $681,272.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$335,307.00 $681,272.00
$894,008.00 $0.00
$1,229,315.00 $681,272.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
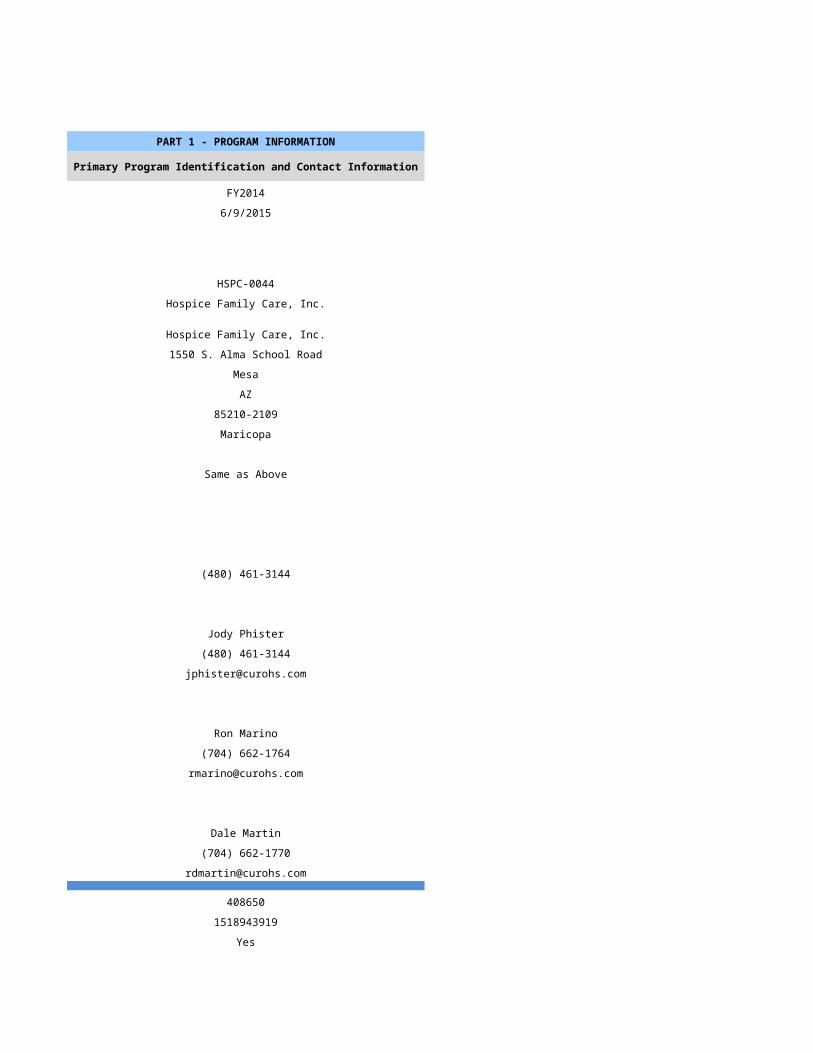
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/14/2015 7/15/2015
HSPC-5033 HSPC-4398
Soreo Pathways LLC Soulistic Medical Institute dba Soulistic Hospice
Soreo Pathways LLC Soulistic Hospice
2475 E Water St 26 Tubac Rd., Ste C1 & C2
Tucson Tubac
AZ AZ
85719 85646-1990
Pima Santa Cruz
P.O. Box 1990
Tubac
AZ
85646-1990
Santa Cruz
520-547-7000 (520) 398-2333
Wendy Sokol Swager Marayeh Cunningham, Ph.D.
520-547-7000 (520) 398-2333
[email protected] [email protected]
Raymond Wallace Catherine J. Lilly
520-547-7000 (520) 398-3970
[email protected] [email protected]
Raymond Wallace Marayeh Cunningham, Ph.D.
520-547-7000 (520) 398-2333
[email protected] [email protected]
688732 397148
1235449182 1386833473
Yes Yes
03-1599 31577
CHAP Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Voluntary (Not For Profit)
Primarily Urban Mixed Urban and Rural
Home Health-Based Free Standing
0
1/1/2014 1/1/2014
12/31/2014 12/31/2014
Soulistic Hospice
HSCP-4398
131 E. Speedway Bouldevard
Tucson
85705
Pima
P.O. Box 1990
Tubac
85646-1990
Santa Cruz
(520) 398-2333
mm/dd/yyyy
Primarily Urban Mixed Urban and Rural
Free Standing
0
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
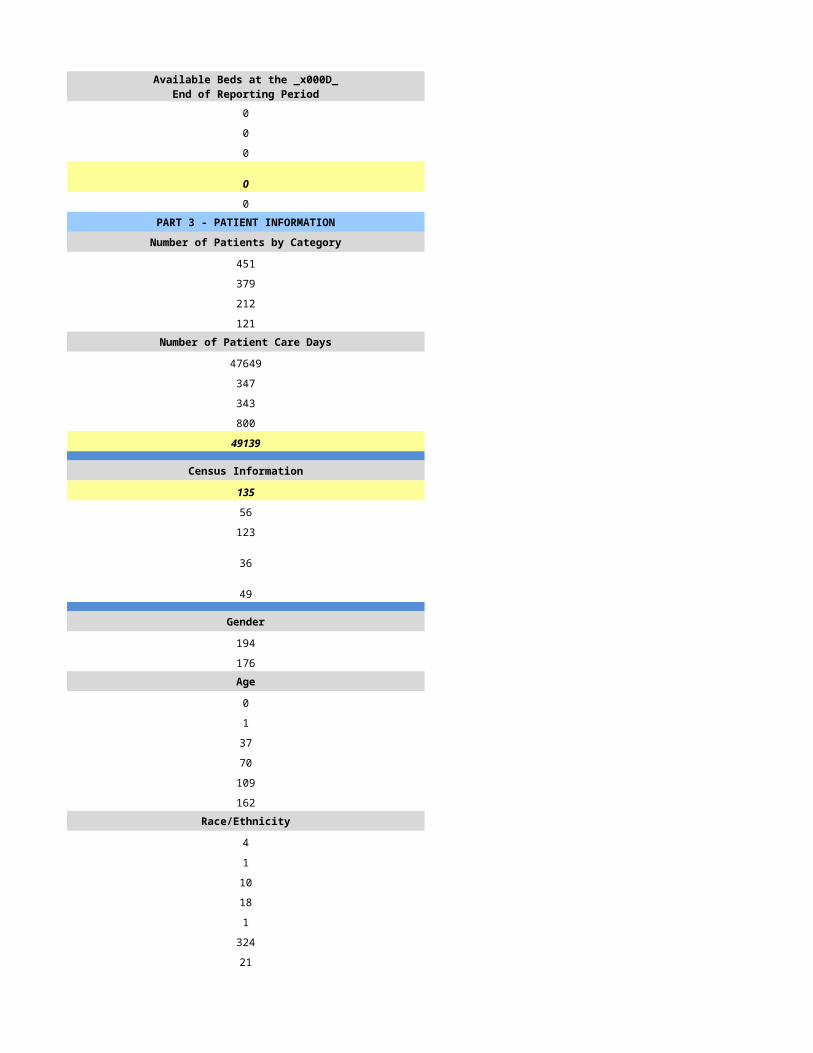
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
281 351
218 227
164 136
45 70Number of Patient Care Days Number of Patient Care Days
20082 33170
102 0
1 0
65 6
20250 33176
Census Information Census Information
55 91
82 141
14 79
62 21
14 20
Gender Gender
117 141
101 86Age Age
0 0
2 1
11 5
40 19
63 38
102 164Race/Ethnicity Race/Ethnicity
2 3
3 1
7 2
32 50
0 0
178 152
51 19Number of Admissions by Source Number of Admissions by Source
118 137
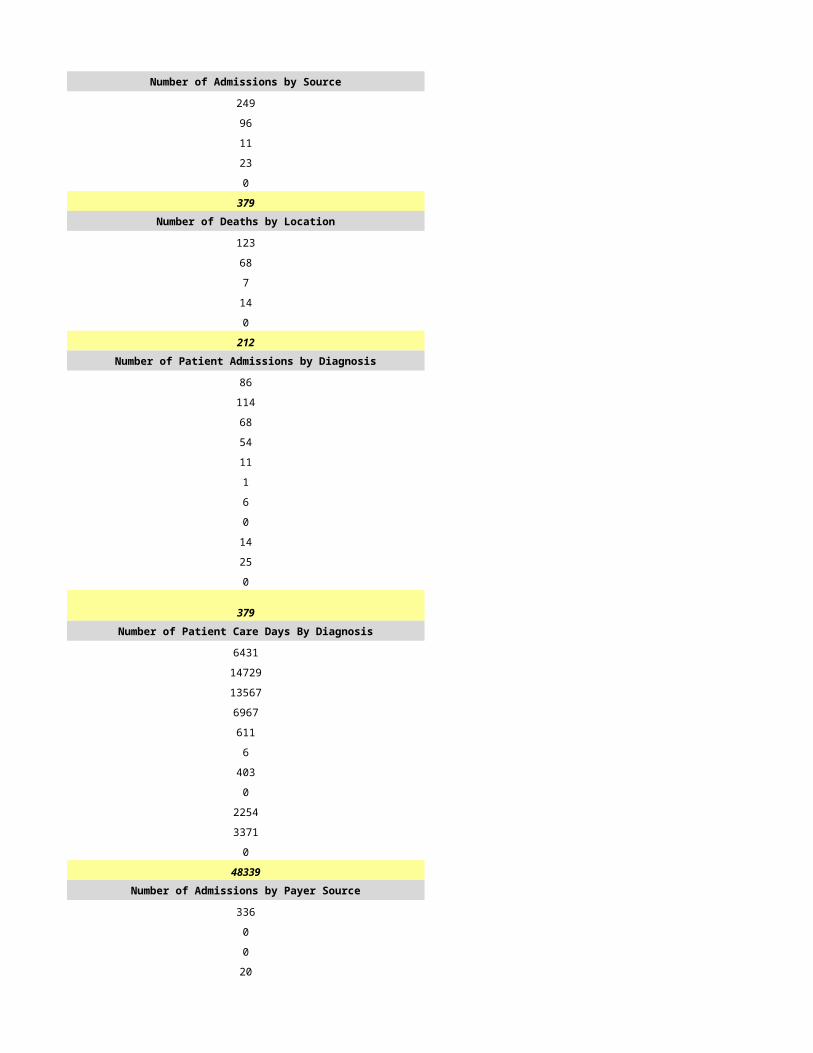
53 83
53 7
0 0
0 0
224 227Number of Deaths by Location Number of Deaths by Location
60 69
48 60
55 7
0 0
1 0
164 136Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
36 36
65 81
57 40
23 9
8 0
7 46
7 1
1 0
7 2
7 12
0 0
218 227Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2424 1248
6478 1766
7695 500
1586 580
123 0
287 1426
412 9
3 0
967 46
275 27601
0 0
20250 33176Number of Admissions by Payer Source Number of Admissions by Payer Source
209 214
0 10
0 0
0 1
9 2
218 227
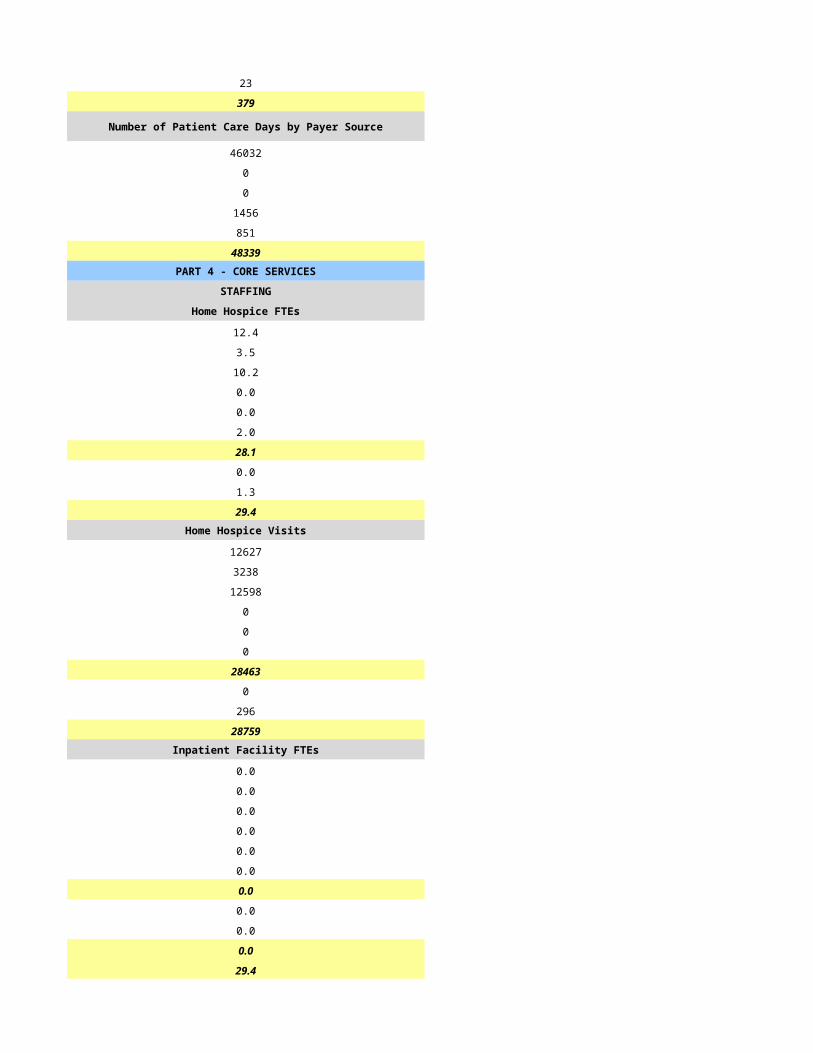
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
19965 32398
0 484
0 0
0 115
285 179
20250 33176PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
8.0 16.4
2.5 1.5
6.0 7.6
1.0 0.0
0.0 0.0
1.5 1.5
19.0 27.0
5.0 0.1
0.5 0.1
24.5 27.2Home Hospice Visits Home Hospice Visits
4612 5783
1121 669
6363 7857
12 0
0 702
0 1033
12108 16044
753 207
334 1
13195 16252Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
24.5 27.2
CASELOADS CASELOADS
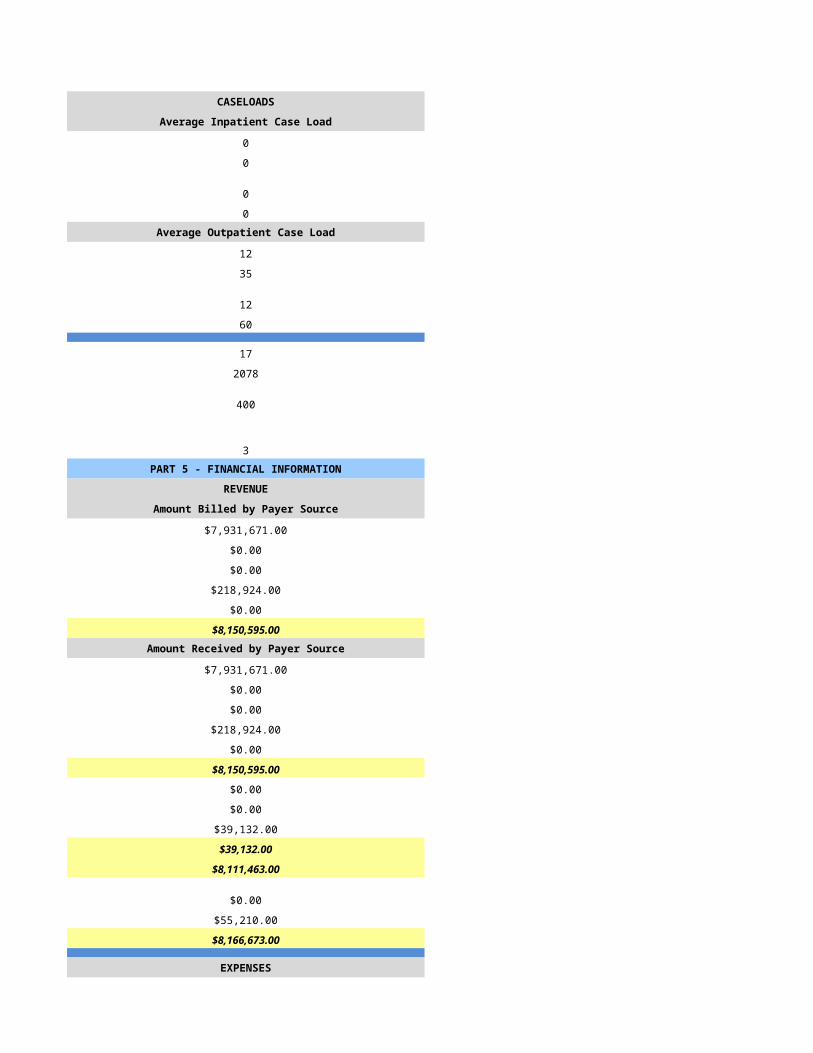
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
12 13
45 67
15 13
30 78
15 13
382 754
268 146
1 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$3,004,000.00 $4,817,258.00
$3,000.00 $54,192.00
$1,000.00 $0.00
$0.00 $46,360.00
$0.00 $16,260.00
$3,008,000.00 $4,934,070.00Amount Received by Payer Source Amount Received by Payer Source
$3,004,000.00 $4,721,641.00
$3,000.00 $52,786.00
$1,000.00 $0.00
$0.00 $26,308.00
$0.00 $0.00
$3,008,000.00 $4,800,735.00
$0.00 $0.00
$36,000.00 $22,590.00
$38,000.00 $137,263.00
$74,000.00 $159,853.00
$2,934,000.00 $4,640,882.00
$0.00 $0.00
$0.00 $8,006.00
$2,934,000.00 $4,648,888.00
EXPENSES EXPENSES
$1,394,000.00 $1,435,584.00
$103,000.00 $0.00
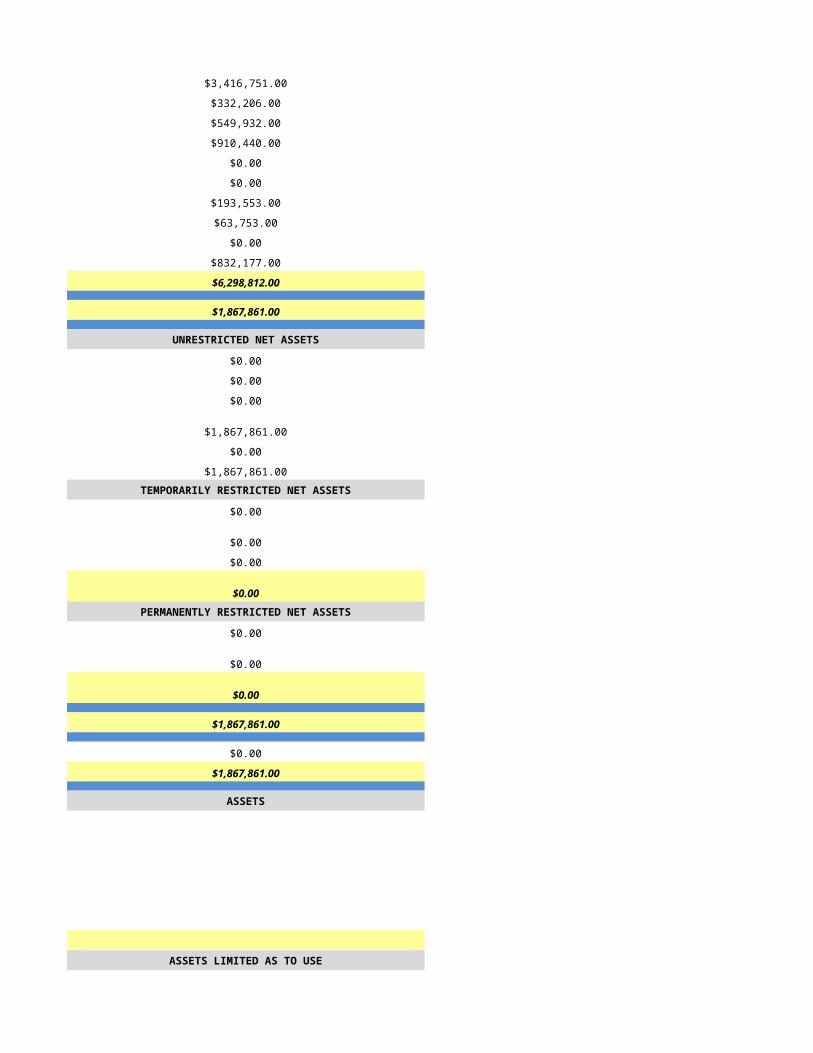
$202,000.00 $96,781.00
$677,000.00 $555,301.00
$16,000.00 $560.00
$45,000.00 $7,359.00
$0.00 $0.00
$0.00 $41,589.00
$0.00 $2,864.00
$277,000.00 $2,256,977.00
$2,714,000.00 $4,397,015.00
$220,000.00 $251,873.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$220,000.00 $251,873.00
$0.00 $0.00
$220,000.00 $251,873.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$220,000.00 $251,873.00
$424,000.00 $1,916,133.00
$644,000.00 $2,168,006.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
Financials are presented on an accrual basis.
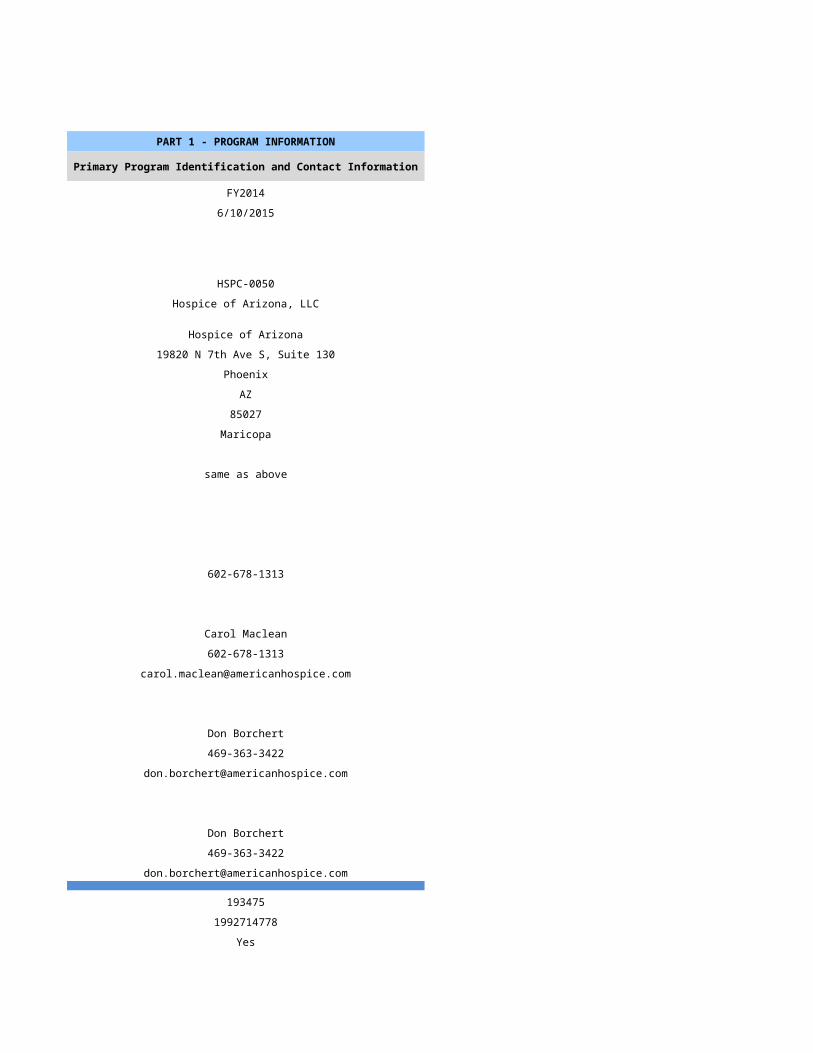
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/16/2015 7/17/2015
HSPC-2833 HSPC-4899
Southern Utah Home Health, Inc. Sun Valley LLC
Southern Utah Hospice Sun Valley LLC
640 E 700 S, Ste 101 7227 E Baseline Rd. Ste. 129
St. George Mesa
UT AZ
84770 85209
Washington Maricopa
Same As Above
(435)-634-9300 (480) 558-2002
Deborah Cox, RN Diane Kazala
(435)-634-9300 (480) 558-2002
dcox @homehealthwest.com [email protected]
Todd Higgins Ryan Jessop
(502)-596-7953 (949) 282-5884
[email protected] [email protected]
Patrick Franks Diane Kazala
(435)-652-7255 (480)558-2002
[email protected] [email protected]
951253 na
1194724682 1326366717
Yes Yes
46-1522 31574
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Primarily Urban
Home Health-Based Free Standing
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A na
N/A HSCP-9999
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A
N/A (999) 999-9999
N/A mm/dd/yyyy
Primarily Rural Primarily Urban
N/A
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
164 156
142 133
118 129
32 28Number of Patient Care Days Number of Patient Care Days
7509 39437
17 148
0 5
16 135
7542 39725
Census Information Census Information
21 109
62 153
28 46
48 20
1 56
Gender Gender
76 91
66 41Age Age
2 0
1 0
12 2
22 8
36 21
69 46Race/Ethnicity Race/Ethnicity
0 1
0 3
1 1
1 9
0 0
88 119
52 0Number of Admissions by Source Number of Admissions by Source
88 68
20 41
34 15
0 0
0 9
142 133Number of Deaths by Location Number of Deaths by Location
89 52
29 42
0 28
0 0
0 7
118 129Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
55 22
53 21
0 50
14 15
0 4
0 9
0 1
0 1
12 9
8 1
0 0
142 133Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
2585 6486
2810 6914
0 14058
193 4787
196 1336
0 1969
0 215
0 411
871 3548
887 1
0 0
7542 39725Number of Admissions by Payer Source Number of Admissions by Payer Source
127 126
4 0
0 2
10 2
1 3
142 133
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
7084 39546
177 0
0 11
229 133
52 35
7542 39725PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.8 8.0
1.3 1.0
3.1 6.0
0.0 1.0
0.0 0.0
0.4 1.0
8.5 17.0
0.8 5.0
1.0 0.5
10.3 22.5Home Hospice Visits Home Hospice Visits
3001 7163
752 1974
2407 7111
0 168
0 0
12 0
6172 16416
0 925
358 0
6530 17341Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
10.3 22.5
CASELOADS CASELOADS
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
9 14
18 35
10 20
18 50
25 26
720 1080
175 137
45 1PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$1,103,177.00 $3,194,972.00
$180,283.00 $0.00
$456.00 $0.00
$34,694.00 $32,505.00
$0.00 $1.00
$1,318,610.00 $3,227,478.00Amount Received by Payer Source Amount Received by Payer Source
$1,091,812.00 $3,495,749.00
$64,276.00 $0.00
$0.00 $13,260.00
$15,345.00 $16,725.00
$9,045.00 $0.00
$1,180,478.00 $3,525,734.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$1,180,478.00 $3,525,734.00
$0.00 $0.00
$0.00 $0.00
$1,180,478.00 $3,525,734.00
EXPENSES EXPENSES
$375,864.00 $1,355,928.00
$225,450.00 $116.00
$40,697.00 $288,647.00
$169,103.00 $473,554.00
$0.00 $163,384.00
$0.00 $12,224.00
$0.00 $37,203.00
$0.00 $19,390.00
$0.00 $0.00
$485,719.00 $609,650.00
$1,296,833.00 $2,960,096.00
-$116,355.00 $565,638.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$116,355.00 $565,638.00
$0.00 $3,883.00
-$116,355.00 $569,521.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$116,355.00 $569,521.00
$338,849.00 $0.00
$222,494.00 $569,521.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/18/2015 7/19/2015
HSPC-3646 HSPC-5156
The Crossing Hospice Care, Inc. Villa Alba Corporation
The Crossing Hospice Care, Inc. dba THEMA Health Services The Villa
1500 E. Bethany Home Road Suite 250 1103 S. Mesa Drive
Phoenix Mesa
AZ AZ
85014 85210
Maricopa Maricopa
602-889-4400 (480) 292-7205
Diane Tryggestad Christine Minch
602-889-4400 (480) 726-7773
[email protected] [email protected]
Angelina Saguid
(999) 999-9999 (480) 726-7773
Diane Tryggestad Christine Minch
602-889-4400 (480) 726-7773
[email protected] [email protected]
499552 none
1811981566 1679558050
Yes Yes
31556 03-1563
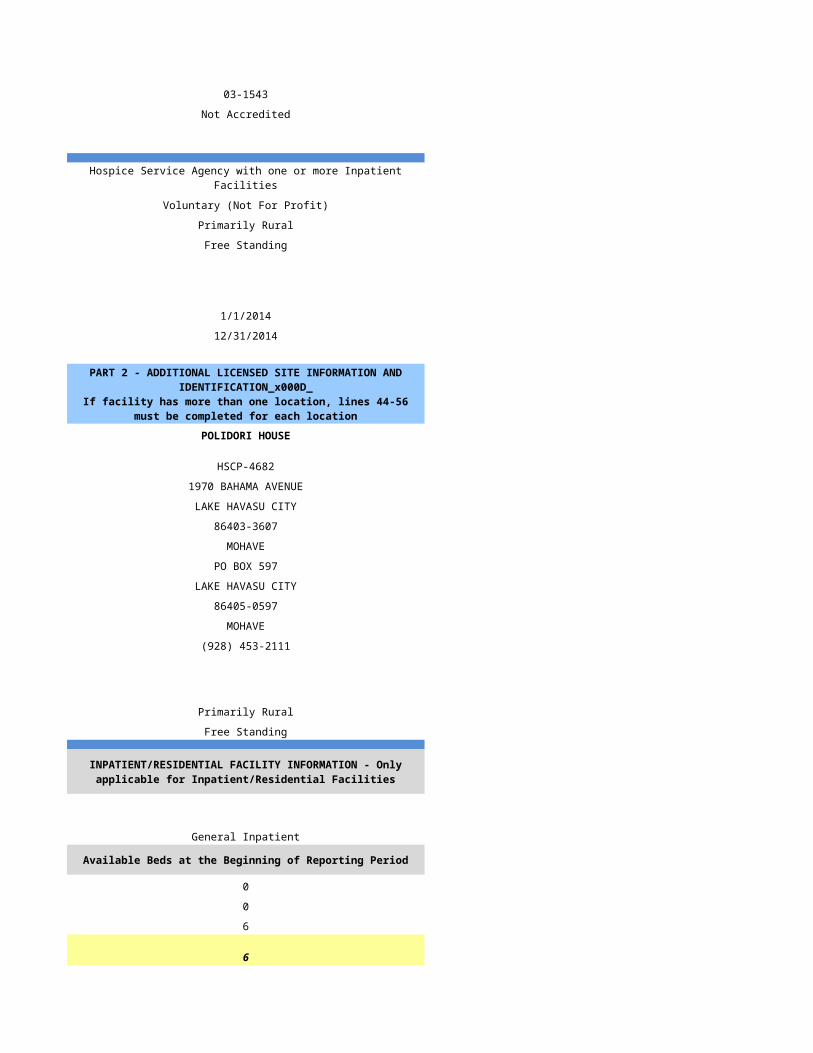
Not Accredited Not Accredited
Hospice Service Agency Hospice Service Agency with one or more Inpatient Facilities
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
n/a
1/1/2014 1/1/2014
12/31/2014 12/31/2014
The Crossing Hospice Care, Inc. dba THEMA Health Services The Villa
HSPC3646 HSPC 5156
2123 Sunset Pointe Dr., B3 1103 S Mesa Drive
Miami Mesa
85539 85210
Gila Maricopa
PO Box 0790
Mesa
85211
Maricopa
928-425-8330 (480) 292-7205
mm/dd/yyyy mm/dd/yyyy
Primarily Urban Primarily Urban
Free Standing Free Standing
n/a
General Inpatient
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 6
0 0
0 0
0 6
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
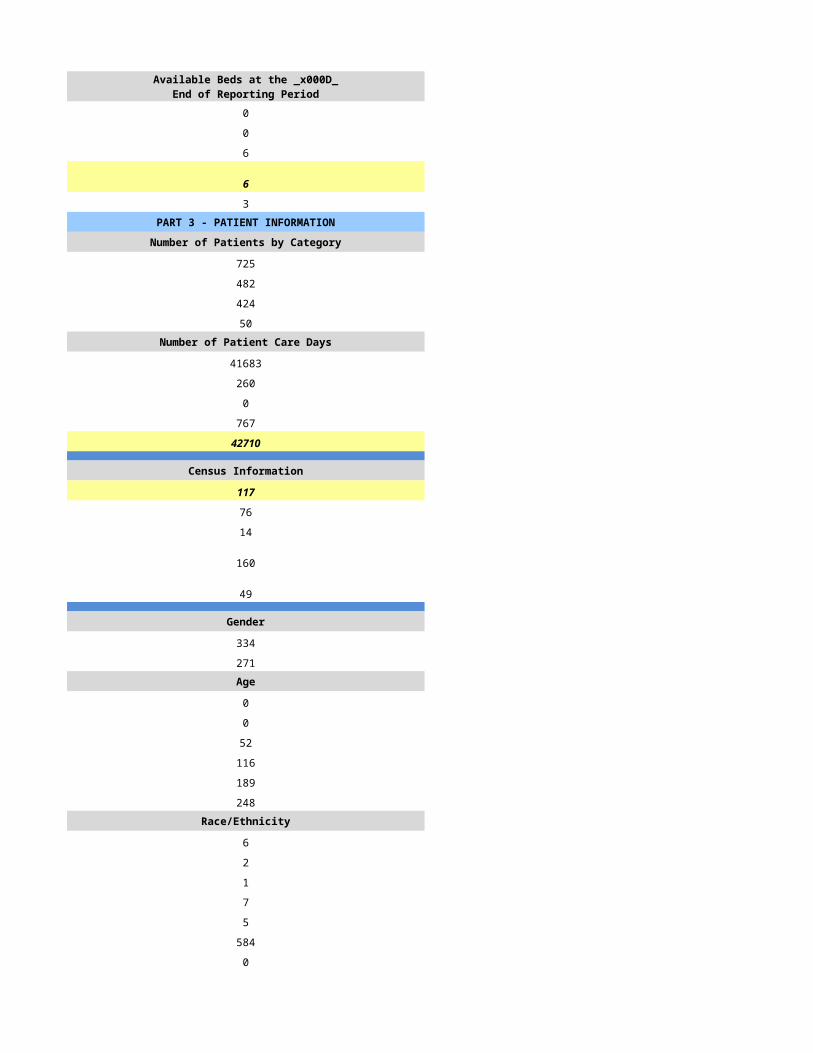
0 6
0 0
0 0
0 6
0 4PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
410 425
383 377
309 216
144 108Number of Patient Care Days Number of Patient Care Days
48522 34010
694 388
0 0
576 295
49792 34693
Census Information Census Information
136 95
82 78
25 32
84 59
23 34693
Gender Gender
212 219
169 158Age Age
0 0
1 0
36 27
54 70
103 124
189 156Race/Ethnicity Race/Ethnicity
12 2
0 7
4 7
11 20
3 1
140 212
213 128Number of Admissions by Source Number of Admissions by Source
337 237
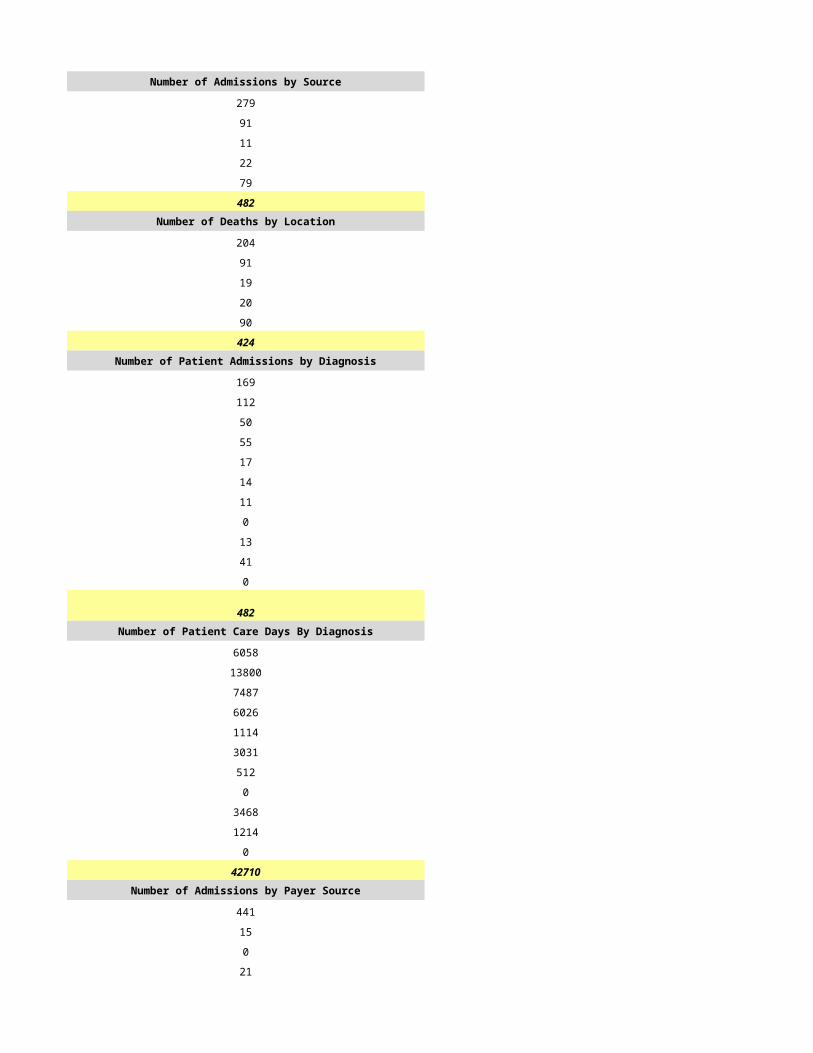
1 50
26 30
46 0
0 60
410 377Number of Deaths by Location Number of Deaths by Location
168 80
1 66
140 22
0 0
0 48
309 216Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
90 79
111 56
31 92
46 38
13 7
0 11
15 14
0 0
67 21
37 26
0 33
410 377Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
6873 5147
10603 7046
3935 10589
6095 3540
1536 494
0 930
1162 604
0 0
4801 1593
10984 379
42 4371
46031 34693Number of Admissions by Payer Source Number of Admissions by Payer Source
294 355
9 0
0 0
12 8
6 14
321 377
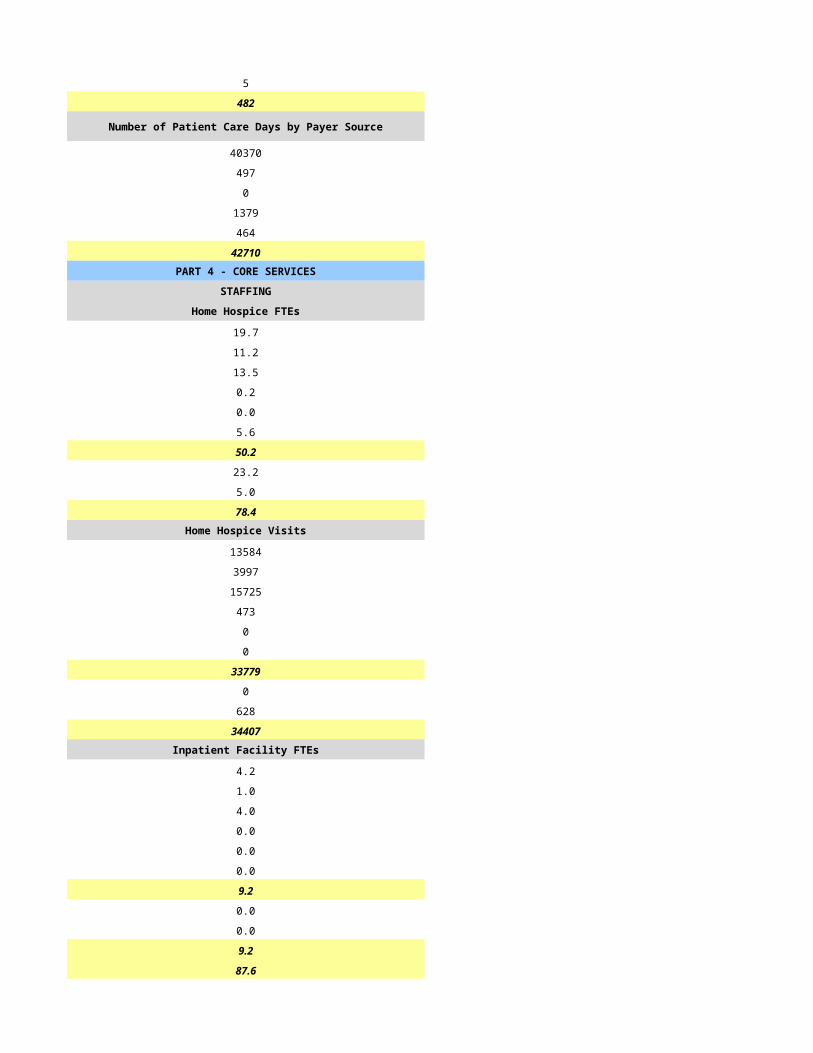
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
39899 33728
255 0
0 0
420 400
626 565
41200 34693PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
10.0 8.0
2.0 3.0
8.0 8.0
4.0 1.0
0.0 0.0
1.5 2.0
25.5 22.0
11.0 10.0
1.5 1.0
38.0 33.0Home Hospice Visits Home Hospice Visits
8608 6790
1447 1640
7858 11912
15 430
0 0
0 870
17928 21642
2284 558
22 274
20234 22474Inpatient Facility FTEs Inpatient Facility FTEs
0.0 6.0
0.0 0.5
0.0 6.0
0.0 0.5
0.0 0.0
0.0 0.5
0.0 13.5
0.0 1.0
0.0 0.5
0.0 15.0
38.0 48.0
CASELOADS CASELOADS
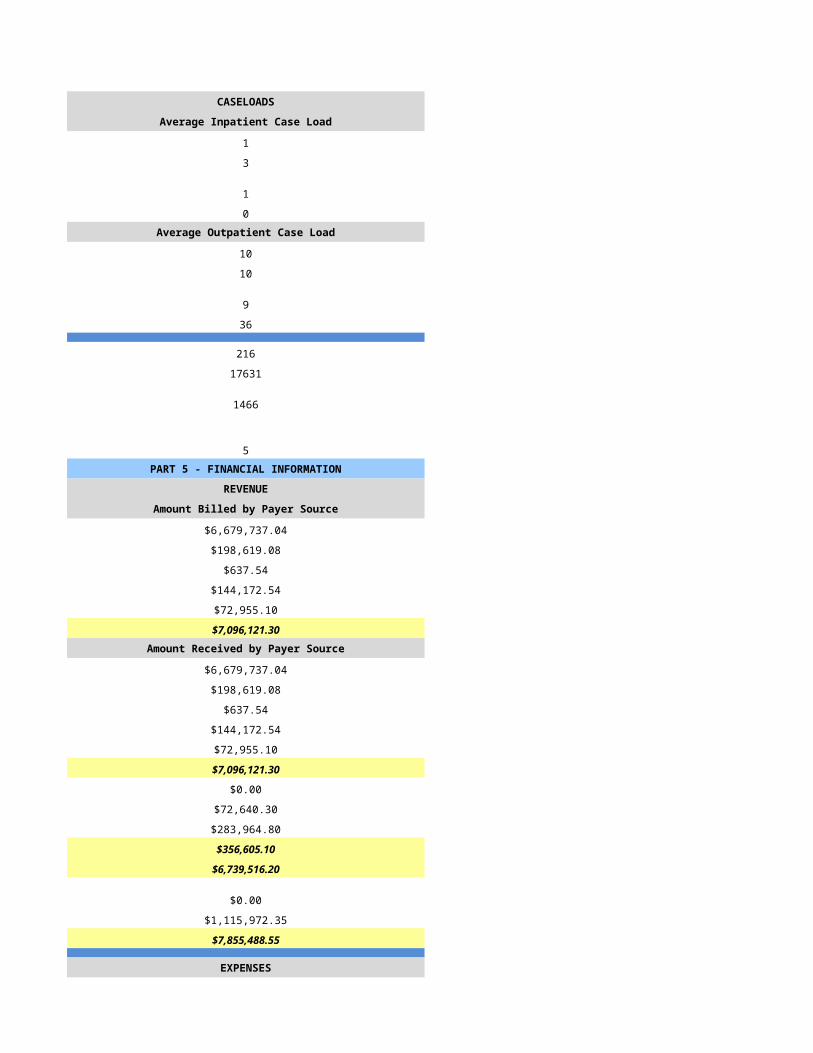
Average Inpatient Case Load Average Inpatient Case Load
15 4
25 1
17 4
35 1Average Outpatient Case Load Average Outpatient Case Load
0 16
0 40
0 16
0 40
44 67
1042 1630
298 240
8 2PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$11,382,805.00 $5,590,366.66
$26,760.00 $0.00
$0.00 $0.00
$39,149.00 $0.00
$0.00 $336,465.00
$11,448,714.00 $5,926,831.66Amount Received by Payer Source Amount Received by Payer Source
$6,359,689.00 $5,704,303.72
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$75,634.00 $336,465.00
$6,435,323.00 $6,040,768.72
$0.00 $0.00
$0.00 $0.00
$711,544.00 $113,937.06
$711,544.00 $113,937.06
$5,723,779.00 $5,926,831.66
$0.00 $0.00
$4,087.00 $0.00
$5,727,866.00 $5,926,831.66
EXPENSES EXPENSES
$3,322,043.00 $1,643,681.95
$198,753.00 $0.00
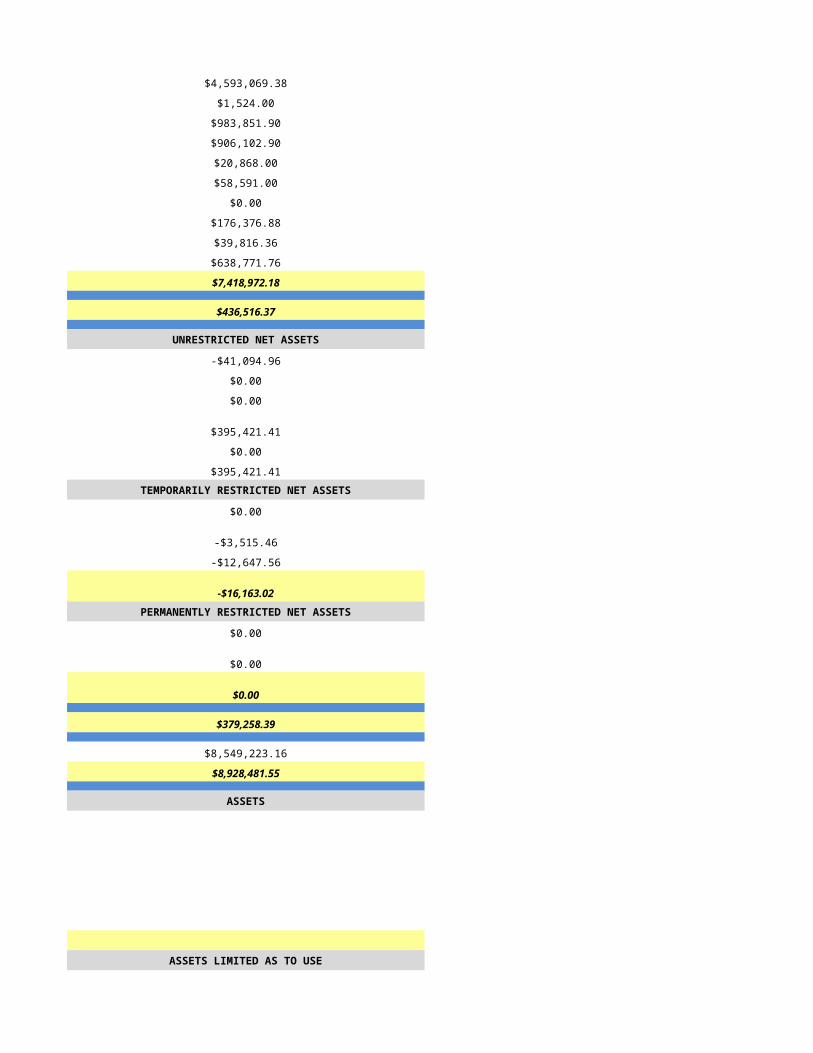
$344,113.00 $131,708.31
$1,141,138.00 $2,701,608.28
$22,080.00 $210,900.49
$53,855.00 $49,861.16
$0.00 $0.00
$27,725.00 $26,793.88
$0.00 $56,353.67
$324,601.00 $1,049,622.52
$5,434,308.00 $5,870,530.26
$293,558.00 $56,301.40
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$293,558.00 $56,301.40
$0.00 $0.00
$293,558.00 $56,301.40TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$293,558.00 $56,301.40
$470,672.00 $0.00
$764,230.00 $56,301.40
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/20/2015 7/21/2015
HSPC-4948 HSPC-4488
VALLEY OF THE SUN HOSPICE, LLC Community Hospice Group, LLC
VALLEY OF THE SUN HOSPICE, LLC Verde Valley Community Hospice
1717 W. Northern Ave., Suite 117 859 Cove Parkway, Suite 103
Phoenix Cottonwood
AZ AZ
85021 86326
MARICOPA Yavapai
450 Morth Dobson, Suite 108
Mesa
AZ
85201
Maricopa
602-535-8254 480-456-9300
GERALD TOLLIVER Richard Bass
602-535-8254 480-456-9300
[email protected] [email protected]
GREGORY ANDERSON Karen Monville
602-535-8254 480-456-9300
[email protected] [email protected]
GREGORY ANDERSON Ramsey David Badre
602-535-8254 912-634-9197
[email protected] [email protected]
471487
1316265432 1538320411
Yes Yes
31600 03-1583
CHAP Not Accredited
None
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Urban Primarily Urban
Free Standing Free Standing
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A
Primarily Urban Primarily Urban
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
40 120
40 92
14 66
16 15Number of Patient Care Days Number of Patient Care Days
4394 9260
0 9
11 1
0 3
4405 9273
Census Information Census Information
12 25
126 82
123 21
3 15
4 7
Gender Gender
29 7
7 35Age Age
0 0
0 0
1 12
4 17
7 20
25 43Race/Ethnicity Race/Ethnicity
0 0
2 0
0 0
1 3
0 0
32 68
2 21Number of Admissions by Source Number of Admissions by Source
37 48
0 39
2 6
1 0
0 0
40 93Number of Deaths by Location Number of Deaths by Location
13 34
0 26
1 6
0 0
0 0
0 66Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
0 34
0 15
20 19
0 10
3 3
0 0
0 2
0 0
0 5
15 5
2 0
40 93Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
0 1656
1983 1509
0 2355
230 2039
0 161
0 0
0 84
0 0
2028 841
164 628
0 0
4405 9273Number of Admissions by Payer Source Number of Admissions by Payer Source
40 85
0 3
0 0
0 2
0 3
40 93
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
4405 8850
0 110
0 0
0 66
0 247
4405 9273PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
3.0 3.0
1.0 1.0
1.5 3.0
1.0 0.0
0.0 0.0
2.0 0.0
9.0 7.0
3.0 2.0
1.0 0.3
13.0 9.3Home Hospice Visits Home Hospice Visits
1335 2909
231 553
1843 2145
18 0
0 0
0 0
3427 5607
160 0
76 1443
3663 7050Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
13.0 9.3
CASELOADS CASELOADS
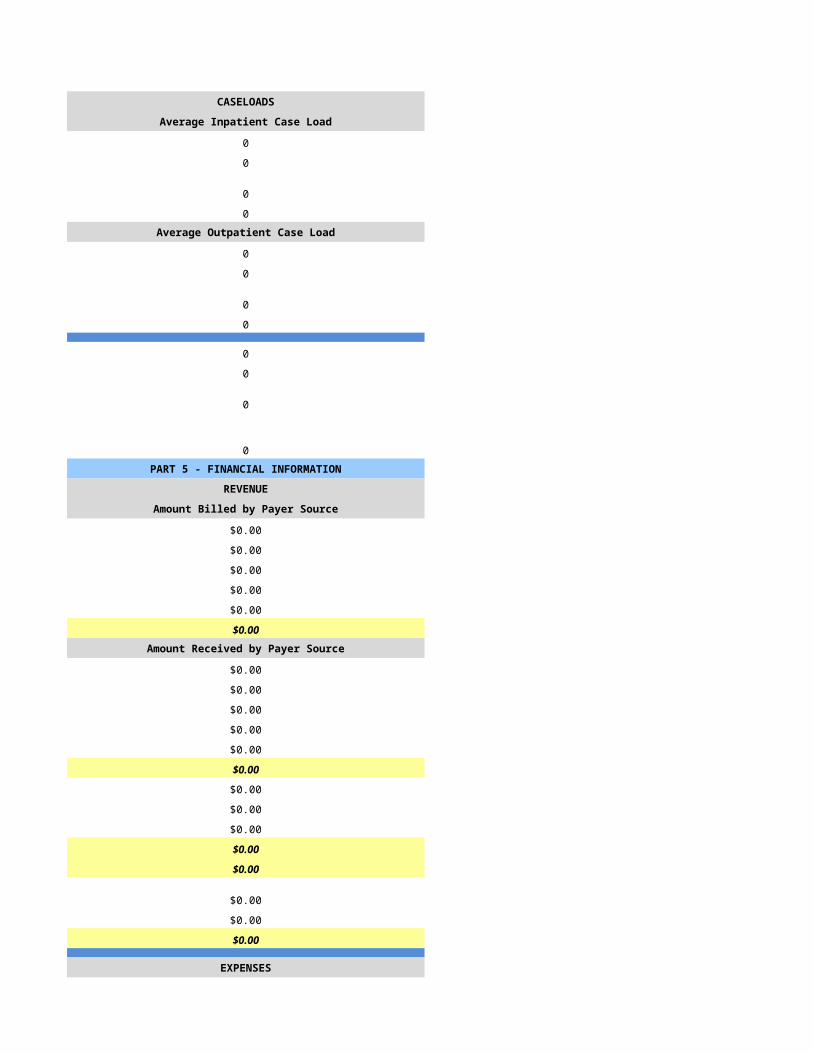
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
8 8
20 25
8 8
20 25
1 17
19 1499
18 62
3 3PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$763,546.00 $2,499,294.00
$0.00 $37,501.00
$0.00 $0.00
$0.00 $11,330.00
$1,988.00 $36,198.00
$765,534.00 $2,584,323.00Amount Received by Payer Source Amount Received by Payer Source
$691,856.82 $1,520,373.00
$0.00 $37,501.00
$0.00 $0.00
$0.00 $11,330.00
$1,987.72 $36,198.00
$693,844.54 $1,605,402.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$693,844.54 $1,605,402.00
$0.00 $0.00
$0.00 $0.00
$693,844.54 $1,605,402.00
EXPENSES EXPENSES
$323,056.00 $531,508.00
$0.00 $929.00
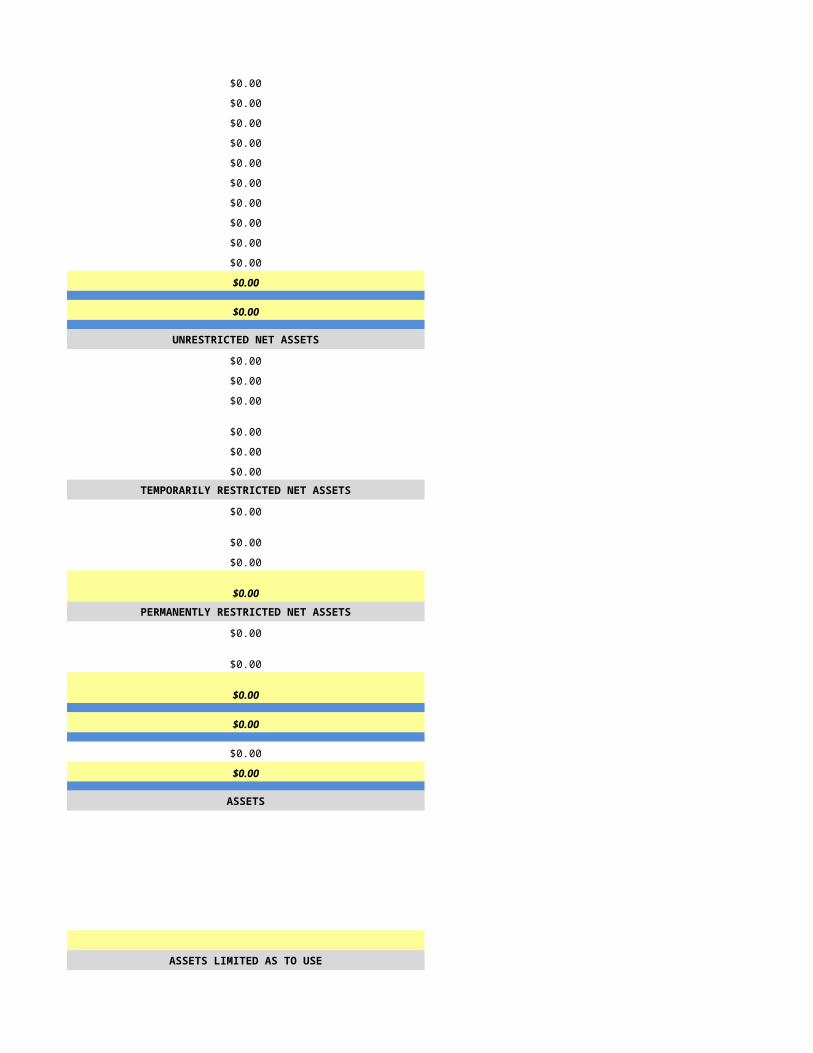
$66,635.00 $73,368.00
$125,599.00 $206,172.00
$44,045.00 $34,320.00
$0.00 $14,179.00
$0.00 $0.00
$0.00 $7,160.00
$15,000.00 $0.00
$125,349.00 $409,398.00
$699,684.00 $1,277,034.00
-$5,839.46 $328,368.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$5,839.46 $328,368.00
$0.00 $0.00
-$5,839.46 $328,368.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$5,839.46 $328,368.00
$0.00 $0.00
-$5,839.46 $328,368.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS
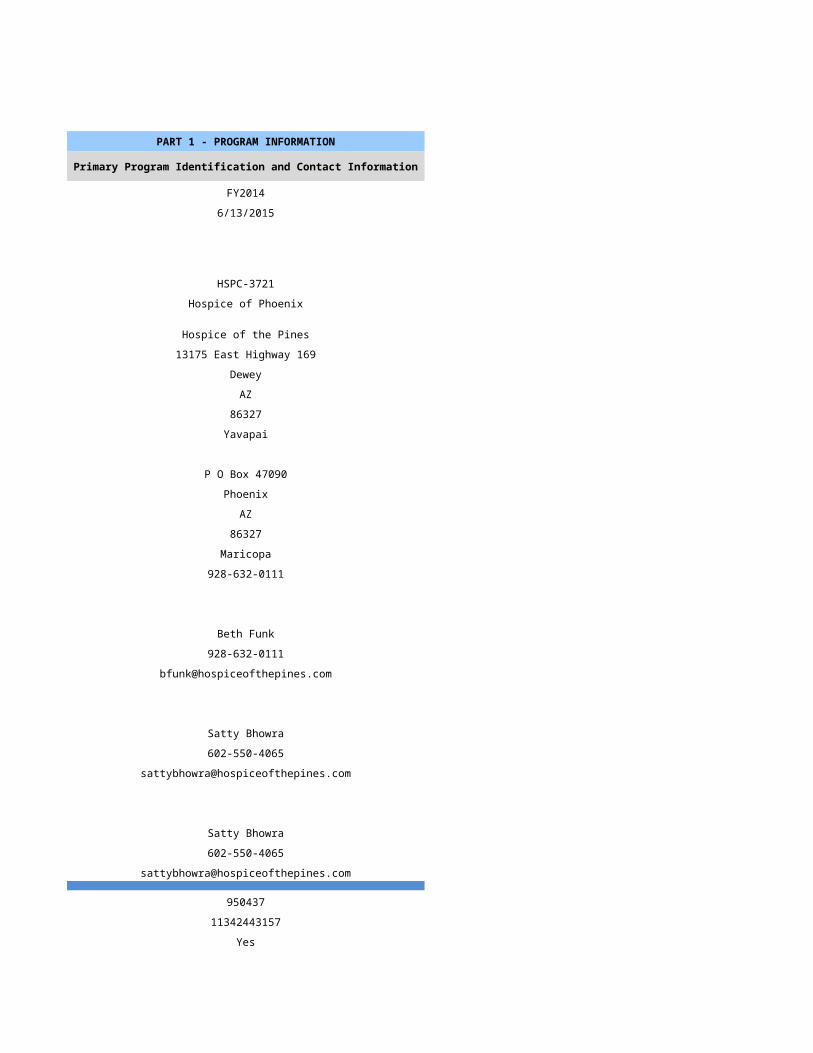
PART 1 - PROGRAM INFORMATION PART 1 - PROGRAM INFORMATION
Primary Program Identification and Contact Information Primary Program Identification and Contact Information
FY2014 FY2014
7/22/2015 7/23/2015
HSPC-4401 HSPC-5462
Southern Nevada Home Health Care, Inc. Red Rock Healthcare, Inc
Virgin Valley Hospice Zions Way Hospice
315 Calais Dr. Ste B 47 6th Ave
Mesquite Page
NV AZ
89027 86040
Clark Coconino
Same PO Box 1015
Page
AZ
86040
Coconino
(702)-346-7565 928-645-0366
Tina Hinze, RN Brent Guerisoli
(702)-228-0282 928-645-0366
[email protected] [email protected]
Todd Higgins NA
(502)-596-7953 NA
Patrick Franks Sandra Whitley
(435)-652-7255 949-540-1926
[email protected] [email protected]
N/A 436372
1194828350 1669746525
Yes Yes
29-1517 03-1594
Not Accredited JCAHO
NA
Hospice Service Agency Hospice Service Agency
Proprietary Proprietary
Primarily Rural Mixed Urban and Rural
Home Health-Based Home Health-Based
N/A
1/1/2014 1/1/2014
12/31/2014 12/31/2014
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
N/A NA
Primarily Rural Mixed Urban and Rural
N/A
N/A
N/A
Available Beds at the Beginning of Reporting Period Available Beds at the Beginning of Reporting Period
0 0
0 0
0 0
0 0
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
PART 2 - ADDITIONAL LICENSED SITE INFORMATION AND IDENTIFICATION
If facility has more than one location, lines 44-56 must be completed for each location
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
INPATIENT/RESIDENTIAL FACILITY INFORMATION - Only applicable for Inpatient/Residential Facilities
Available Beds at the End of Reporting Period
Available Beds at the End of Reporting Period
0 0
0 0
0 0
0 0
0 0PART 3 - PATIENT INFORMATION PART 3 - PATIENT INFORMATION
Number of Patients by Category Number of Patients by Category
41 102
37 98
38 44
7 26Number of Patient Care Days Number of Patient Care Days
1501 11534
5 74
0 0
0 13
1506 11621
Census Information Census Information
4 32
45 166
21 83
15 14
2 6
Gender Gender
13 186
24 129Age Age
0 0
0 0
3 64
9 59
14 53
11 139Race/Ethnicity Race/Ethnicity
0 161
0 0
0 2
0 3
0 0
37 60
0 89Number of Admissions by Source Number of Admissions by Source
33 300
0 11
4 0
0 4
0 0
37 315Number of Deaths by Location Number of Deaths by Location
33 31
0 0
5 12
0 0
0 0
38 43Number of Patient Admissions by Diagnosis Number of Patient Admissions by Diagnosis
14 7
8 8
1 17
3 10
0 3
0 4
0 5
0 0
4 10
7 13
0 19
37 96Number of Patient Care Days By Diagnosis Number of Patient Care Days By Diagnosis
700 1816
199 847
71 2058
126 1089
0 363
0 726
0 726
0 0
276 968
134 2784
0 242
1506 11621Number of Admissions by Payer Source Number of Admissions by Payer Source
34 74
0 16
0 0
3 5
0 1
37 96
Number of Patient Care Days by Payer Source Number of Patient Care Days by Payer Source
1387 8958
0 1937
0 0
119 605
0 121
1506 11621PART 4 - CORE SERVICES PART 4 - CORE SERVICES
STAFFING STAFFING
Home Hospice FTEs Home Hospice FTEs
1.5 4.0
0.8 1.0
1.0 2.0
0.0 0.0
0.0 0.0
0.0 1.0
3.3 8.0
0.3 3.0
0.3 0.0
3.8 11.0Home Hospice Visits Home Hospice Visits
677 2578
104 554
426 1337
0 0
0 0
10 55
1217 4524
0 0
204 0
1421 4524Inpatient Facility FTEs Inpatient Facility FTEs
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
0.0 0.0
3.8 11.0
CASELOADS CASELOADS
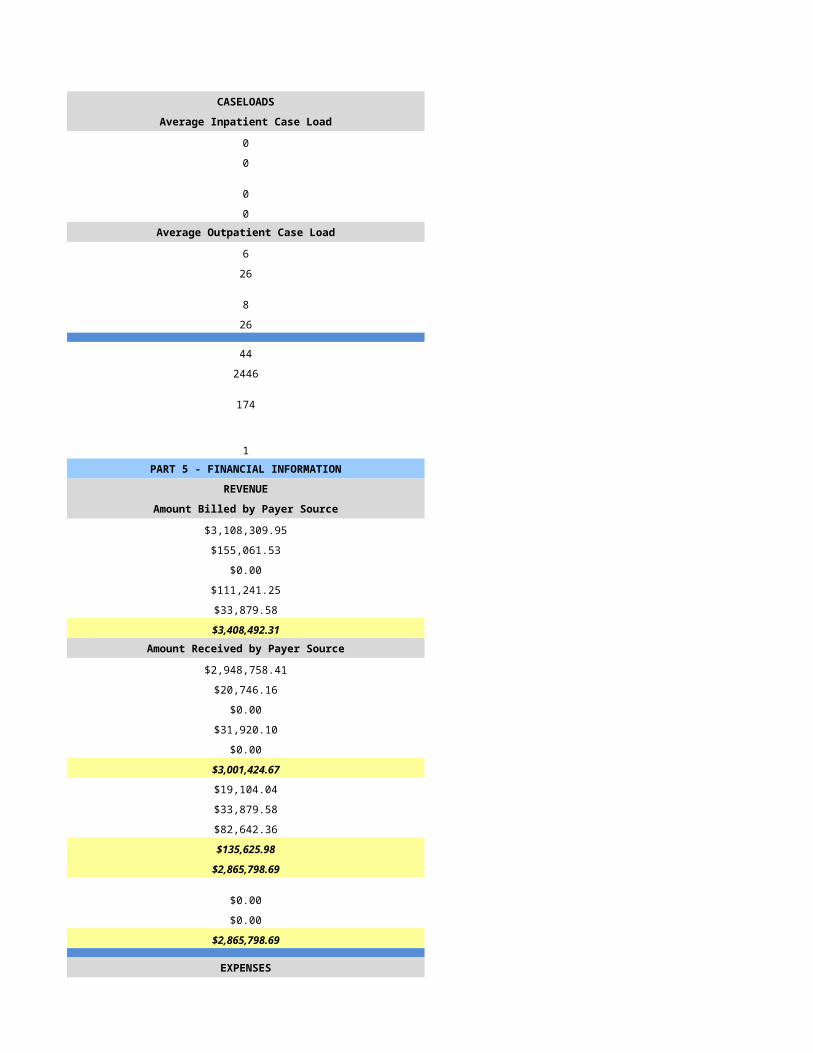
Average Inpatient Case Load Average Inpatient Case Load
0 0
0 0
0 0
0 0Average Outpatient Case Load Average Outpatient Case Load
4 0
8 0
4 0
8 0
9 0
285 0
22 0
4 0PART 5 - FINANCIAL INFORMATION PART 5 - FINANCIAL INFORMATION
REVENUE REVENUE
Amount Billed by Payer Source Amount Billed by Payer Source
$570,288.00 $0.00
$6,077.00 $0.00
$0.00 $0.00
$6,802.00 $0.00
$2,926.00 $0.00
$586,093.00 $0.00Amount Received by Payer Source Amount Received by Payer Source
$301,670.00 $1,497,602.00
$0.00 $464,365.00
$0.00 $0.00
$22,148.00 $108,043.00
$709.00 $162,968.00
$324,527.00 $2,232,978.00
$0.00 $0.00
$0.00 $0.00
$0.00 $354,498.00
$0.00 $354,498.00
$324,527.00 $1,878,480.00
$0.00 $0.00
$0.00 $0.00
$324,527.00 $1,878,480.00
EXPENSES EXPENSES
$167,080.00 $171,933.00
$23,497.00 $0.00
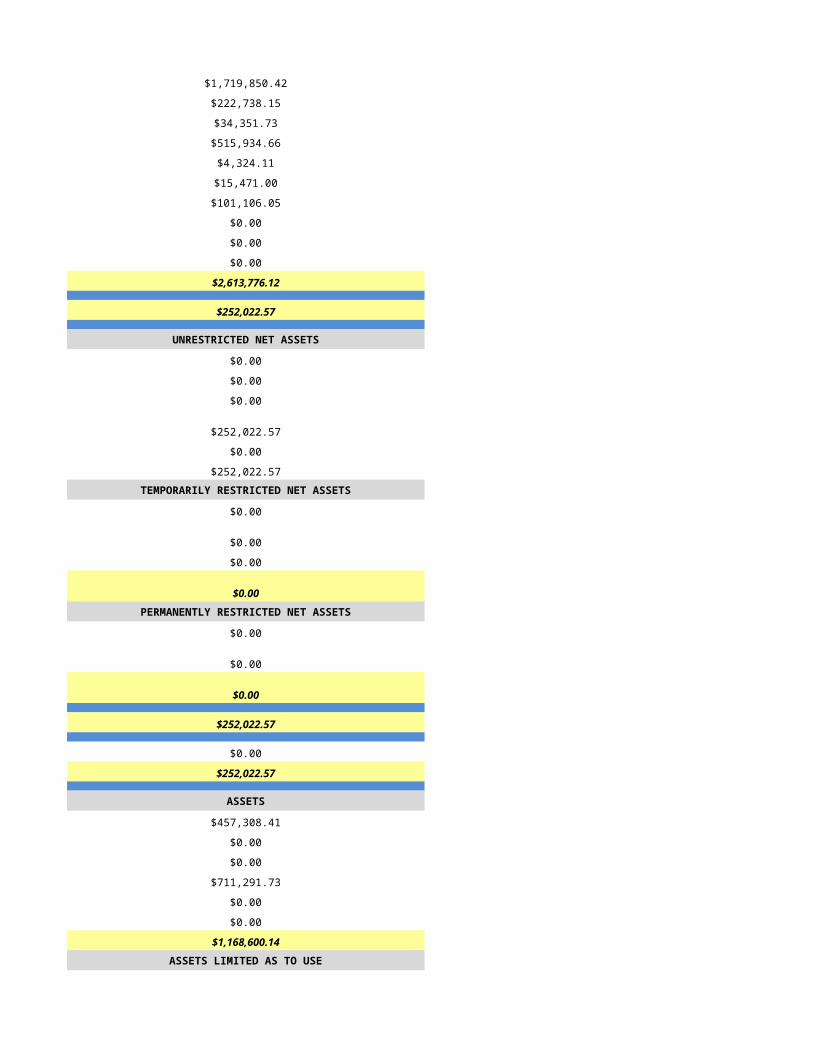
$19,715.00 $20,582.00
$95,411.00 $96,705.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$259,005.00 $391,116.00
$564,708.00 $680,336.00
-$240,181.00 $1,198,144.00
UNRESTRICTED NET ASSETS UNRESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$240,181.00 $1,198,144.00
$0.00 $0.00
-$240,181.00 $1,198,144.00TEMPORARILY RESTRICTED NET ASSETS TEMPORARILY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00PERMANENTLY RESTRICTED NET ASSETS PERMANENTLY RESTRICTED NET ASSETS
$0.00 $0.00
$0.00 $0.00
$0.00 $0.00
-$240,181.00 $1,198,144.00
$60,186.78 $0.00
-$179,994.22 $1,198,144.00
ASSETS ASSETS
ASSETS LIMITED AS TO USE ASSETS LIMITED AS TO USE
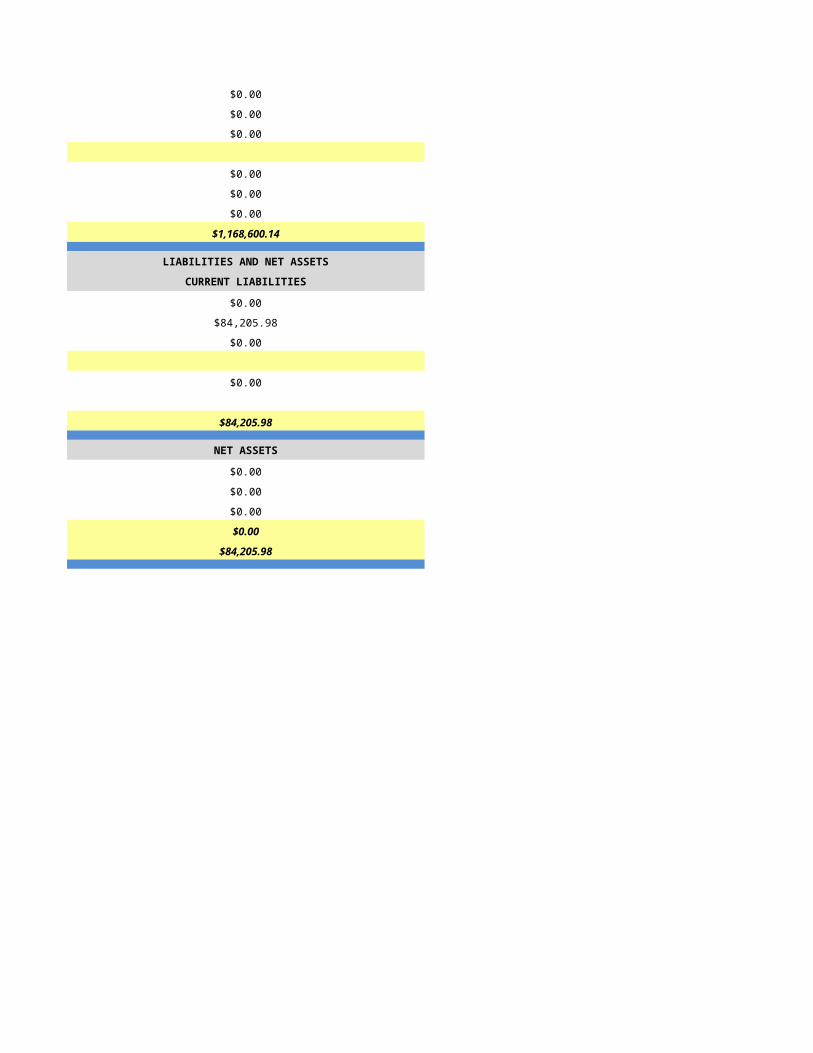
LIABILITIES AND NET ASSETS LIABILITIES AND NET ASSETS
CURRENT LIABILITIES CURRENT LIABILITIES
NET ASSETS NET ASSETS