Embed Size (px)
Citation preview

SCIENTIFIC ARTICLE
Median nerve cross-sectional area and MRI diffusioncharacteristics: normative values at the carpal tunnel
Lawrence Yao & Neville Gai
Received: 27 August 2008 /Revised: 3 November 2008 /Accepted: 7 November 2008 / Published online: 9 January 2009# ISS 2008
AbstractObjective Enlargement of the median nerve is an objectivepotential imaging sign of carpal tunnel syndrome. Diffusiontensor MRI (DTI) may provide additional structuralinformation that may prove useful in characterizing medianneuropathy. This study further examines normal values formedian nerve cross-sectional area (CSA), apparent diffu-sion coefficient (ADC), and fractional anisotropy (FA).Materials and methods Twenty-three wrists in 17 healthyvolunteers underwent MRI of the wrist at 3 T. In 13subjects, DTI was performed at a B value of 600 mm2/s.Median nerve CSA, ADC, and FA were analyzed atstandardized anatomic levels.Results Mean (SD) median nerve CSA within the proximalcarpal tunnel was 10.0 (3.4) mm2. The mean (SD) FA of themedian nerve was 0.71 (0.06) and 0.70 (0.13) proximal toand within the carpal tunnel, respectively. There was asignificant difference between nerve CSA and ADC, butnot FA, at the distal forearm and proximal carpal tunnel.Nerve CSA, ADC, and FA did not differ between men andwomen or between dominant and non-dominant wrists.Nerve CSA at the proximal carpal tunnel was positivelycorrelated with subject age and body mass index.Conclusion Our results suggest a 90% upper confidencelimit for normal median nerve CSA of 14.4 mm2 at theproximal carpal tunnel, higher than normal limits reportedby many ultrasound studies. We observed a differencebetween the CSA and ADC, but not the FA, of the mediannerve at the distal forearm and proximal carpal tunnellevels.
Keywords Magnetic resonance imaging .
Diffusion tensor imaging .Median nerve .
Carpal tunnel syndrome . Fractional anisotropy
Introduction
Carpal tunnel syndrome (CTS) is the most commonperipheral nerve entrapment syndrome and is characterizedby potentially disabling pain and paresthesia affecting thehand and forearm. Many conditions may predispose orcontribute to CTS, including occupational tasks that entailrepetitive motion at the wrist and hand. The diagnosis ofCTS is typically based on clinical signs and symptoms.Electrodiagnostic tests, particularly nerve conduction stud-ies, may help confirm CTS and gauge the severity ofmedian neuropathy. Ultrasound and magnetic resonanceimaging (MRI) may depict enlargement of the mediannerve in cases of CTS, either within or just proximal to thecarpal tunnel [1–5]. Other MRI findings of CTS includepalmar bowing of the transverse carpal ligament andhyperintensity of the median nerve on T2-weighted images[5, 6]. Diffusion-weighted MR imaging (DWI) providesphysiological information about the mobility of watermolecules and may aid tissue characterization [7]. Direc-tional anisotropy of water diffusibility characterizes struc-turally ordered tissues such as peripheral nerves and can bequantified with MRI by estimation of the diffusion tensor[8]. Diffusion tensor MR imaging (DTI) consists ofmultiple DWI acquisitions with directionally varyingdiffusion sensitization. The diffusion tensor can be summa-rized by spatially invariant scalar quantities such asfractional anisotropy (FA) [9].Recent experience with DTIsuggests that the median nerve in patients with CTSexhibits diminished FA [10]. Another recent study suggests
Skeletal Radiol (2009) 38:355–361DOI 10.1007/s00256-008-0626-1
L. Yao (*) :N. GaiClinical Center, Radiology and Imaging Sciences,10 Center Drive,Bethesda, MD 20892, USAe-mail: [email protected]

that the FA of the median nerve proximal to the carpaltunnel may differ from that within the carpal tunnel innormal subjects [11]. As MR imaging techniques improve,features of the median nerve may be visualized with greaterclarity, and quantitative parameters derived from MRI maybe estimated with higher precision. This study furtherexamines normative values for median nerve cross-sectionalarea (CSA), apparent diffusion coefficient (ADC), and FAproximal to and within the carpal tunnel as measured bycurrent MRI and DTI methods at 3 T.
Materials and methods
Subjects
Seventeen healthy volunteers underwent MRI. There wereeight men and nine women. Average subject age and bodymass index (BMI) were 37 years (range, 22–60) and24.6 kg/m2 (range, 16.8–30.7), respectively. Thirteen of17 subjects also underwent DTI. Only the dominant wristunderwent DTI in seven of 13 subjects, while both wristsunderwent DTI in six of 13 subjects to examine intra-subject differences between dominant and non-dominantwrists. Subjects were free of wrist symptoms and had nohistory of wrist surgery or fracture. Our InstitutionalReview Board approved the study protocol. Informedconsent was obtained from all volunteers after explainingthe procedure.
MRI technique
Subjects were scanned in the prone, arm overhead position.MRI was performed on a 3-T (Philips Achieva) scannerequipped with quasar dual mode gradients and using amulti-channel wrist coil (Invivo, Orlando, FL, USA). Themaximum gradient strength was 80 mT/m, and themaximum slew rate was 200 T m−1 s−1. 3D isotropic turbospin echo imaging (~0.35 mm3 voxel size) was performedon all wrists. The 3D turbo spin-echo (TSE) sequenceemployed a relaxation enhancement radiofrequency (RF)pulse, spatially non-selective, partial, refocusing RF pulses,and an excitation RF pulse optimized for minimal echospacing and improved slab profile. Other scan parametersinclude TE/TR=35/420 ms, echo train length (ETL)=15,half-Fourier phase sampling, and sensitivity encoding(SENSE) in phase and slice encoding directions, scantime=4 min 50 s. Diffusion-weighted MRI was performedusing a multi-shot, spin-echo prepared echo planar se-quence at a B value of 600 mm2/s. Diffusion-weightedimaging (DWI) was acquired in six non-collinear directionsfor calculation of the diffusion tensor. DWI was acquiredwith spectral fat saturation, sensitivity encoding (SENSE),
half-Fourier phase sampling, TR=1470 ms, TE=83 ms,shots=4, echo train length=19, signal averages=6, voxelsize=1×0.7×3 mm, slices=11, scan time=4 min 10 s. TheFA was calculated using commercially available software(Philips, v R2.53) and is defined as [9]:
FA ¼ 3=2ð Þ1=2� L1 � Lð Þ2þ L2 � Lð Þ2þ L3 � Lð Þ2h i1=2�
L21 þ L22 þ L23� �1=2
where L1, L2, and L3 are the eigenvalues of the diffusiontensor, and L is the mean of the eigenvalues. The apparentdiffusion coefficient (ADC) was calculated based on thesignal of diffusion weighted images acquired with equaldiffusion sensitization in three, orthogonal directions (Sx, Sy,Sz) and without diffusion sensitization (SB=0):
ADC ¼ �1=Bð Þ � ln Sx � Sy � Sz� �1=3.
SB¼0
h i
Image analysis
Median nerve CSA was measured on reformations of theisotropic TSE acquisition using a free-hand region-drawingtool on a diagnostic, softcopy workstation (CarestreamPACS, v 10.1). Regions were defined on a standardizedaxial plane of visualization (Fig. 1a) established usinginteractive, mutli-planar reformation supported by theworkstation. Medial and lateral bony landmarks definedthe standardized, reformatted axial plane: the proximalmargin of the hamulus of the hamate and the proximalmargin of the spine of the trapezium. The followinganatomic landmarks defined three axial levels (Figs. 1b–d)for analysis: (1) distal forearm—the mid inferior radioulnarcompartment; (2) proximal carpal tunnel—the proximalaspect of the lunato-capatate joint; and (3) distal carpaltunnel—the mid-hamulus of the hamate. The CSA of themedian nerve was measured at these three standardizedanatomic levels. The height and width of the carpal tunnelwas also measured in the standardized axial plane at thelevel of the hamulus of the hamate. Width was based on thelandmarks comprised by the hamulus of the hamate andthe spine of the trapezium, while height was based on thepalmar cortex of the capitate and the flexor retinaculum(Fig. 1a). The CSA of the carpal tunnel was estimated aspi×height×width/4. The FA and ADC were recorded forthe median nerve at the distal forearm (Fig. 2) and proximalcarpal tunnel levels. For these measurements, regions ofinterest were defined within the nerve as visualized on theB=0 and so-called isotropic B=600 mm2/s EPI images,where
SB isotropicð Þ ¼ Sx � Sy � Sz� �1=3
Regions for the median nerve on DWI were defined to fallwithin the visualized boundary of the nerve to minimize
356 Skeletal Radiol (2009) 38:355–361

volume averaging artifact. Diffusion characteristics werenot analyzed at the distal carpal tunnel level due to lessreliable visualization of the nerve at this level on DWI inthe dedicated wrist coil.
An experienced musculoskeletal radiologist performedCSA measurements and region definitions for FA and ADC
determinations. The same radiologist repeated measure-ments for the dominant wrists after a period of greater than2 months for assessment of intraobserver variance. Mea-surement error was estimated based on the difference in thetwo readings, Δ(R1, R2), for n subjects, as error=[SD(Δ(R1, R2))1−n]/2
1/2.
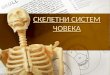
Fig. 1 Reformatted isotropicTSE imaging of the wrist illus-trating the ‘standardized’ axialimaging plane and the threestandardized levels of mediannerve analysis. a Coronal refor-matted image illustrates thelandmarks that define the axialreference plane (R), theproximal margin of the hamulusof the hamate, and the midscaphomultangular articulation.Planes 1, 2, and 3 indicate thedistal forearm, proximal carpaltunnel, and distal carpal tunnellevels as defined for this study.b–d. Reformatted axial imagesat the standardized level definedas ‘distal forearm’ (b), ‘proxi-mal carpal tunnel’ (c), and ‘dis-tal carpal tunnel’ (d). Mediannerve is indicated by the whitearrow. The width (W) and height(H) measurements for the carpaltunnel are illustrated in d, asdefined by bony landmarks andthe flexor retinaculum
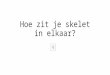
Fig. 2 Spin-echo prepared,multi-shot EPI diffusion-weighted imaging of the wrist inthe axial plane at the level ofthe proximal carpal tunnel. Themedian nerve is indicated bythe arrow. a The B=0 image.b The isotropic B=600 s/mm2
image, as described in“Materials and methods.” c Thecalculated ADC image based onimages shown in a and b. Theunits for ADC on the color scaleare ×10−3 mm2/s. d The calcu-lated FA map based on thediffusion tensor. The unitlessnumbers for FA on the colorscale are ×10−3
Skeletal Radiol (2009) 38:355–361 357

Statistics
Differences in median nerve CSA, ADC, and FA atdifferent anatomic levels were tested with a paired t test.Differences in these parameters between men and womenwere examined with a t test. Single tailed 90% upper limitsfor measurements were estimated as mean+(1.2816)×SD.Correlations between nerve CSA and diffusion character-istics and carpal tunnel width, area, subject age, and BMIwere calculated with Pearson’s r. Intraobserver variancewas quantified with an intraclass correlation coefficient(SPSS, release 11.0.1).
Results
Median nerve CSA
Mean (SD) median nerve CSA at the distal forearm,proximal, and carpal tunnel was 8.6 (2.7), 10.0 (3.4), 8.8(2.3) mm2, respectively (see Table 1). The 90% upper limitfor median nerve CSA at these three anatomic levels is12.1, 14.4, and 11.7 mm2, respectively. The differencebetween median nerve CSA at the proximal carpal tunneland distal forearm level is significant (Table 2). There wasno significant difference in median nerve CSA between thedistal forearm and distal carpal tunnel or between theproximal and distal carpal tunnel.
MR diffusion characteristics
The mean (SD) FA of the median nerve was 0.71 (0.06) and0.70 (0.13) at the distal forearm and at the proximal carpaltunnel, respectively (Table 1). The mean (SD) ADC of themedian nerve was 1.24 (0.38) and 1.46 (0.21)×10−3 mm2/sat these levels, respectively. The ADC of the median nervewas significantly greater at the proximal carpal tunnel than atthe distal forearm. The FA of the median nerve did not sig-nificantly differ between these two anatomic levels (Table 2).
MR features versus subject features
Median nerve CSA, FA, and ADC are not significantlydifferent between men and women at any anatomic level.The correlations between median nerve CSA and carpaltunnel width are shown in Table 3. Median nerve CSA atthe three anatomic levels is significantly correlated withcarpal tunnel width.
Carpal tunnel width was significantly correlated withADC at the proximal carpal tunnel level but not at the distalforearm (Table 3). Greater carpal tunnel height and carpaltunnel area were also correlated with higher median nerveADC at the carpal tunnel (r=0.63, p=0.03 and r=0.64, p=0.02, respectively). Carpal tunnel width, height, and areawere not correlated with FA of the median nerve.
Increasing age and BMI are associated with a largermedian nerve at the proximal carpal tunnel level but not at
Table 1 Mean median nerve measurements by anatomic level
Nerve level CSA (min–max) (SD)a ADC (min–max) (SD)b FA (min–max) (SD)b
Distal forearm 8.6 (4.5–12.9) (2.7) 1.24 (0.77–1.96) (0.38) 0.71 (0.60–0.80) (0.06)Proximal CT 10.0 (4.7–17.9) (3.4) 1.46 (1.01–1.73) (0.21) 0.70 (0.51–0.86) (0.13)Distal CT 8.8 (4.1–13.2) (2.3) NA NA
CSA is in mm2 , ADC is in 10−3 mm2 /s, FA is unitlessCT carpal tunnel, NA ADC and FA were not analyzed at the distal CT levela n=17b n=13
Table 2 Mean differences in median nerve measurements between anatomic levels
Nerve level CSA (SEM) (p)a ADC (SEM) (p)b FA (SEM) (p)b
Distal forearm–proximal CT −1.4 (0.7) (0.05) −0.220 (0.090) (0.04) 0.01 (0.04) (0.89)Proximal CT–distal CT 1.2 (0.7) (0.09) NA NADistal forearm–distal CT −0.2 (0.4) (0.61) NA NA
CSA is in mm2 , ADC is in 10−3 mm2 /s, FA is unitlessCT carpal tunnel, SEM standard error of the mean, NA ADC and FA were not analyzed at the distal CT levela n=17b n=13
358 Skeletal Radiol (2009) 38:355–361

the other anatomic levels (Table 3). Age and BMI are notcorrelated with median nerve ADC or FA. Age is correlatedwith BMI in our subject group (r=0.64, p<0.01). Thecorrelations of age and BMI with median nerve caliber atthe proximal carpal tunnel level are not independentlysignificant when corrected for BMI and age, respectively.
Dominant versus non-dominant wrist
There were no significant differences in median nerve CSA,FA, or ADC at any anatomic level between the dominantand non-dominant wrists in six subjects.
Intraobserver variance
Measurement error and intraclass correlation coefficient aresummarized for the various median nerve measurements inTable 4. For median nerve CSA, error is less whenmeasured at the distal forearm, as compared to within thecarpal tunnel.
Conclusion
Imaging studies have described alterations in median nerveCSA and profile in CTS. Changes in median nerve profile,as manifested by flattening ratios for the nerve, arepotentially less reliable and more difficult to apply thannerve CSA, given the frequent non-ovoid morphology ofthe nerve.
Most studies measure median nerve CSA at the proximalcarpal tunnel level, although the nerve may also be enlargedat the distal forearm and distal carpal tunnel levels in cases
of CTS [12, 13]. In CTS, enlargement of the nerve maypredominate at the proximal carpal tunnel level. Hence, theratio of median nerve area at the proximal carpal tunnel tothe area at the distal forearm has been proposed as a morerobust diagnostic marker of CTS [14].
Our results suggest 90% (single tail) upper confidencelimits for normal median nerve CSA of 12.0 and 14.4 mm2,at the distal forearm and within the proximal carpal tunnel,respectively. These values are similar to those reported in aprior 3-T MRI study by Monagle et al. [15]. Averagemedian nerve CSA in normal subjects, as measured byultrasound, varied from 6.1 to 10.4 mm2 [16]. Our findingsfor normal median nerve CSA are similar to those reportedin ultrasound studies by Nakamichi and Tachibana [1] andCartwright et al [2]. Based on receiver operating character-istic analysis, an ultrasound study by Yesildag et al. [3]defined an upper limit of 10.5 mm2 for normal mediannerve CSA at the proximal carpal tunnel level, while anultrasound study by Wong et al. [4] proposed an upper limitof 9.8 mm2.A potential reason for smaller average, mediannerve CSAs observed on ultrasound as compared to MRImight relate to anatomic differences in the perceivedboundary of the nerve. On MRI, the nerve is defined inpart by fat surrounding the epineurium, and areal measure-ments of the nerve likely encompass the epineurium. Theecho interface defining the hypoechoic nerve on ultrasoundlikely occurs at the internal boundary of the epineurium,and areal measures made on ultrasound based on thehypoechoic portion of the nerve may exclude theepineurium [4].
Our study suggests that the median nerve CSA may begreater at the proximal carpal tunnel level than at the distal
Table 3 Correlations between median nerve measurements andsubject characteristics
Age (p) BMI (p) Carpal tunnelwidth (p)
CSAa
Distal forearm 0.01 (0.97) 0.21 (0.45) 0.62 (0.01)Proximal CT 0.50 (0.04) 0.65 (0.01) 0.50 (0.04)Distal CT 0.06 (0.83) 0.30 (0.28) 0.54 (0.03)ADCb
Distal forearm −0.13 (0.68) −0.11 (0.75) 0.37 (0.22)Proximal CT 0.08 (0.81) 0.25 (0.46) 0.56 (0.05)FAb
Distal forearm −0.16 (0.61) −0.14 (0.69) −0.08 (0.80)Proximal CT 0.11 (0.72) 0.31 (0.35) 0.16 (0.60)
Correlations represent Pearson’s r. p values <0.05 are shown in boldCT carpal tunnela n=17b n=13
Table 4 Intraobserver variance for two serial median nervemeasurements
Errorc ICC
CSAa
Distal forearm 0.9 0.88Proximal CT 1.6 0.72Distal CT 1.7 0.60ADCb
Distal forearm 0.190 0.71Proximal CT 0.136 0.57FAb
Distal forearm 0.054 0.53Proximal CT 0.064 0.70
Error estimates are based on two readings by the same radiologist, asdescribed in “Materials and methods”ICC intraclass correlation coefficienta n=17b n=13c For error, CSA is in mm2 , ADC is in 10-3 mm2 /sec, FA is unitless
Skeletal Radiol (2009) 38:355–361 359

forearm level in normal subjects. In their MR study,Monagle et al. [15] did not observe a significant differencein nerve areas between the distal forearm and proximalcarpal tunnel in asymptomatic subjects or in subjects withCTS. The MR study by Allmann et al. [17] reported similarmean median nerve areas at the distal forearm and proximalcarpal tunnel in asymptomatic subjects but did notspecifically test for intrasubject differences. Ultrasoundstudies have not clearly demonstrated different normalthresholds in median nerve CSA at the distal forearm ascompared to the carpal tunnel level [4, 12].
Our results also suggest a trend toward larger mediannerve CSA at the proximal carpal tunnel level in oldersubjects. Cartwright et al. [2] made a similar observationusing ultrasound. In our study group, however, greater agewas also associated with higher BMI, and BMI wassimilarly associated with larger median nerve CSA at theproximal carpal tunnel. The implication of this observationis unclear. Both obesity and age have been established asrisk factors for CTS [18]. Conceivably, subclinical nervecompression may contribute to nerve enlargement over timein asymptomatic subjects. We also observed an associationbetween larger median nerves at the distal forearm andcarpal tunnel and wider carpal tunnels. Larger wrists mayconceivably exhibit larger median nerves. These relation-ships suggest that a single threshold for ‘normal’ nerveCSA is inherently limited, by ignoring potential sources ofnormal variation in median nerve CSA.
Compressive neuropathy and resultant nerve swellingmay conceivably exhibit an increase in mobile water andaltered water compartmentalization within the nerve. Anexperimental model of sciatic nerve injury in rats hasshown a decrease in diffusion anisotropy [19] within theinjured nerve; another similar study in frogs has showndiminished diffusion anisotropy but no increase in ADCwithin injured nerves [20]. Edema could potentiallyincrease free water within the endoneural space aroundaxons, or in the extracellular space between nerve fascicles,outside the perineurium.
We did not observe a difference in the FA of the mediannerve between anatomic levels proximal to and within thecarpal tunnel, as reported by Kabakci et al. [11]. We alsodid not observe an association between FA and ADC of themedian nerve and subject age as reported in that study [11].The intersubject variances we observed in FA and ADC ofthe median nerve were considerable (coefficient of varianceup to 16% and 31%, respectively), even with an optimizedtechnique at 3 Tesla. Measurement error might partiallyexplain the considerable overlap between the FA values ofthe median nerve between normal volunteers and patientswith CTS reported by Khalil et al [10].
We did not anticipate the observed correlation of carpaltunnel width, height, and area with ADC of the median
nerve in the proximal carpal tunnel, and the implication isunclear. This could be related to the observed relationshipbetween carpal tunnel width and nerve CSA. Analysis of alarger nerve or a larger carpal tunnel may be subject to lessvolume averaging of the nerve with surrounding tissuecharacterized by lower ADC (fat, tendon, retinaculum)yielding corresponding higher observed ADC values forthe nerve.
Our study is limited by small subject numbers and theuse of one observer. This limits our power to detectdifferences in nerve features such as CSA, FA and ADC,between anatomic levels and between dominant and non-dominant wrists, if they should exist. Our analysis ofintraobserver error shows that ROI determination for asmall structure such as the median nerve is also a source ofconsiderable measurement variance, even for CSA deter-minations on fairly high resolution, isotropic MR images.This has implications for the application of strict mediannerve CSA thresholds to clinical cases, especially whereimage resolution may be lower than in our study.
Further research will determine whether the FA ordiffusivity of the median nerve can be determined withsufficient reliability to make these parameters clinically usefulin the evaluation of suspected CTS. The precision andpotential utility of DTI of the median nerve should improvein conjunction with continuous advances in MRI hardwareperformance. The upper normal limit for median nerve size asmeasured on high resolution MRI may differ from thatreported by ultrasound studies, may differ between the distalforearm and proximal carpal tunnel levels, and appears to varywith both patient age, BMI, and carpal tunnel width.
References
1. Nakamichi K, Tachibana S. Ultrasonographic measurement ofmedian nerve cross-sectional area in idiopathic carpal tunnelsyndrome: diagnostic accuracy. Muscle Nerve 2002;26(6): 798–803.
2. Cartwright MS, Shin HW, Passmore LV, Walker FO. Ultrasono-graphic reference values for assessing the normal median nerve inadults. J Neuroimaging 2008, May 8.
3. Yesildag A, Kutluhan S, Sengul N, Koyuncuoglu HR, Oyar O,Guler K, Gulsoy UK. The role of ultrasonographic measurementsof the median nerve in the diagnosis of carpal tunnel syndrome.Clin Radiol 2004;59(10): 910–915.
4. Wong SM, Griffith JF, Hui AC, Lo SK, Fu M, Wong KS. Carpaltunnel syndrome: diagnostic usefulness of sonography. Radiology2004;232(1): 93–99.
5. Pasternack II, Malmivaara A, Tervahartiala P, Forsberg H, VehmasT. Magnetic resonance imaging findings in respect to carpal tunnelsyndrome. Scand J Work Environ Health 2003;29(3): 189–196.
6. Jarvik JG, Yuen E, Kliot M. Diagnosis of carpal tunnel syndrome:electrodiagnostic and MR imaging evaluation. Neuroimaging ClinN Am 2004;14(1): 93–102.
7. Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E, Laval-Jeantet M. MR imaging of intravoxel incoherent motions:
360 Skeletal Radiol (2009) 38:355–361

application to diffusion and perfusion in neurologic disorders.Radiology 1986;161(2): 401–407.
8. Basser PJ, Pierpaoli C. Microstructural and physiological featuresof tissues elucidated by quantitative-diffusion-tensor MRI. J MagnReson B 1996;111(3): 209–219.
9. Le Bihan D, Mangin JF, Poupon C, Clark CA, Pappata S, MolkoN, Chabriat H. Diffusion tensor imaging: concepts and applica-tions. J Magn Reson Imaging 2001;13(4): 534–546.
10. Khalil C, Hancart C, Le Thuc V, Chantelot C, Chechin D, CottenA. Diffusion tensor imaging and tractography of the median nervein carpal tunnel syndrome: preliminary results. Eur Radiol 18:2283–2291.
11. Kabakci N, Gürses B, Firat Z, Bayram A, Uluğ AM, KovanlikayaA, Kovanlikaya I. Diffusion tensor imaging and tractography ofmedian nerve: normative diffusion values. Am J Roentgenol2007;189(4): 923–927.
12. Sarría L, Cabada T, Cozcolluela R, Martínez-Berganza T, GarcíaS. Carpal tunnel syndrome: usefulness of sonography. Eur Radiol2000;10(12): 1920–1925.
13. Wong SM, Griffith JF, Hui AC, Tang A, Wong KS. Discrimina-tory sonographic criteria for the diagnosis of carpal tunnelsyndrome. Arthritis Rheum 2002;46(7): 1914–1921.
14. Mesgarzadeh M, Schneck CD, Bonakdarpour A, Mitra A, ConawayD. Carpal tunnel: MR imaging. Part II. Carpal tunnel syndrome.Radiology 1989;171(3): 749–754.
15. Monagle K, Dai G, Chu A, Burnham RS, Snyder RE. QuantitativeMR imaging of carpal tunnel syndrome. AJR Am J Roentgenol1999;172(6): 1581–1586.
16. Seror P. Sonography and electrodiagnosis in carpal tunnelsyndrome diagnosis, an analysis of the literature. Eur J Radiol2008;67(1): 146–152.
17. Allmann KH, Horch R, Uhl M, Gufler H, Altehoefer C, Stark GB,Langer M. MR imaging of the carpal tunnel. Eur J Radiol 1997;25(2): 141–145.
18. Becker J, Nora DB, Gomes I, Stringari FF, Seitensus R, PanossoJS, Ehlers JC. An evaluation of gender, obesity, age and diabetesmellitus as risk factors for carpal tunnel syndrome. Clin Neuro-physiol 2002;113(9): 1429–1434.
19. Stanisz GJ, Midha R, Munro CA, Henkelman RM. MR propertiesof rat sciatic nerve following trauma. Magn Reson Med 2001;45(3): 415–420.
20. Beaulieu C, Does MD, Snyder RE, Allen PS. Changes in waterdiffusion due to Wallerian degeneration in peripheral nerve. MagnReson Med 1996;36(4): 627–631.
Skeletal Radiol (2009) 38:355–361 361