Embed Size (px)
Citation preview

Yue Yan, Daniel Saenz, Poonam YadavProf. Bhudatt Paliwal
� Background
� Method and materials
� Study cancer sites
• Prostate
• Head & neck
• Lung
� Discussion and summary
� Questions and answer
2
3
� Motivations for flattening filter free (FFF) beams :
� Pros:▪ Greatly increase dose rate[1-5] (600 MU/min->1400 MU/min (2400 MU/min) for
6X (10X) beam for Varian TrueBeam system) decreased treatment time. More
obvious in treatment modalities requiring large MUs (e.g. SBRT, SRS).
▪ Large decrease in external scatter from the gantry head and lower leakage
dose [5] which may benefit the dose sparing effect to OARs[6].
▪ Greatly reduced neutron contamination to patient when using high energy
beam for treatment[7].
▪ Reduced uncertainty in dose calculation caused by scatter from flattening
filter[1].
� Cons for FFF Beams:▪ Soft spectrum tends to give lower mean dose for PTV coverage[1]. It also tends
to increase internal scatter[8] which may compromise the dose sparing effect to
OARs.
▪ High dose rate delivery is more sensitive to patient’s motion[9].

� Beam commissioning of TrueBeam (Varian, CA) system is completed in Eclipse
treatment planning system(Version 10)
� Energies: 6X and 10X
� Beam modalities: both FFF and flattened (Conv.) beams
� Identical optimal objectives and parameters (e.g. field size, energy, etc.) are used to
design the plan
� VMAT and static IMRT are used to design the plan
� Data Matrix[10]:
� Conformity index:�
� Target coverage: �
� Conformity number: �
� Gradient index: �
� Be Close to unity means better dose distribution for all data matrix elements
4

� Dose description:
• ,
� Optimal objectives:
5
Optimization objectives of VMAT & Static IMRT for prostate cancer
StructureType of
constraint Volume(%) Dose(Gy) Priority
Prostate PTV lower 100 78 100
Prostate PTV upper 0 78 100
Penile bulb upper 40 50 50
Left hip upper 0 45 50
Hot upper 0 39 50
Bladder upper 30 50 50
Rectum upper 30 50 50
SV PTV-Prostate lower 100 70.2 100
SV PTV-Prostate upper 20 72 100
SV PTV-Prostate upper 0 78 100
Right hip upper 0 45 50
Rectum Avoid upper 0 78 50
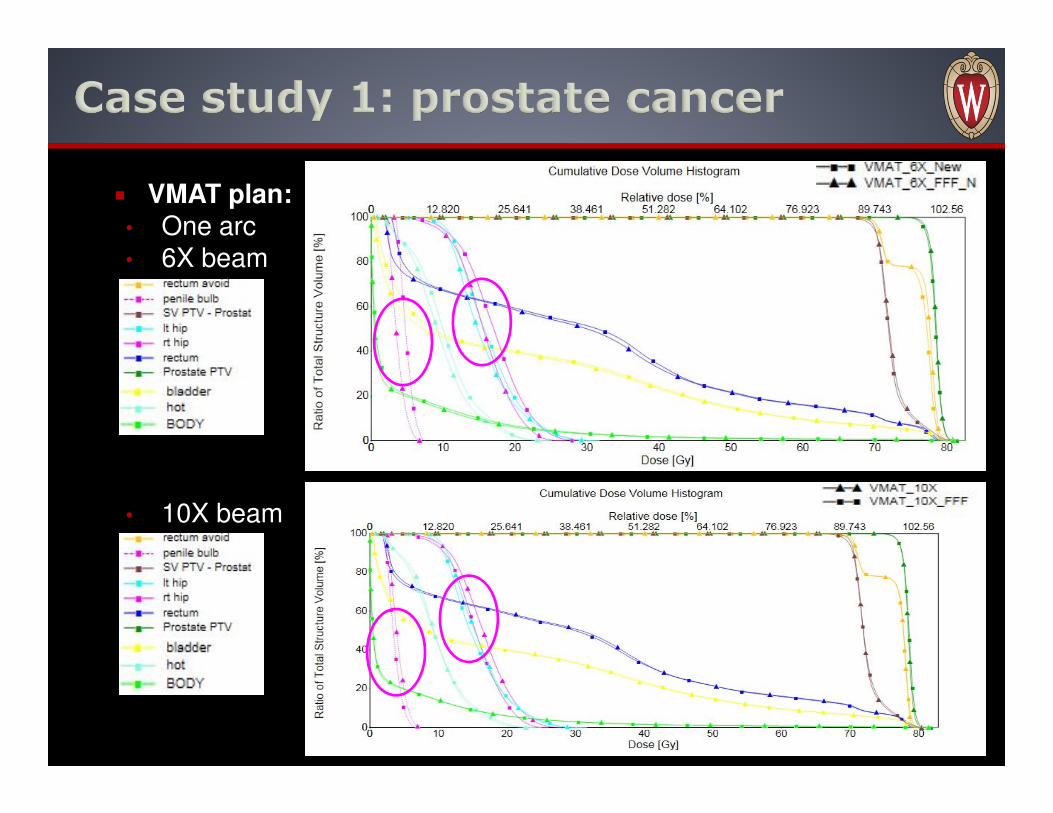
� VMAT plan:• One arc• 6X beam
• 10X beam
6
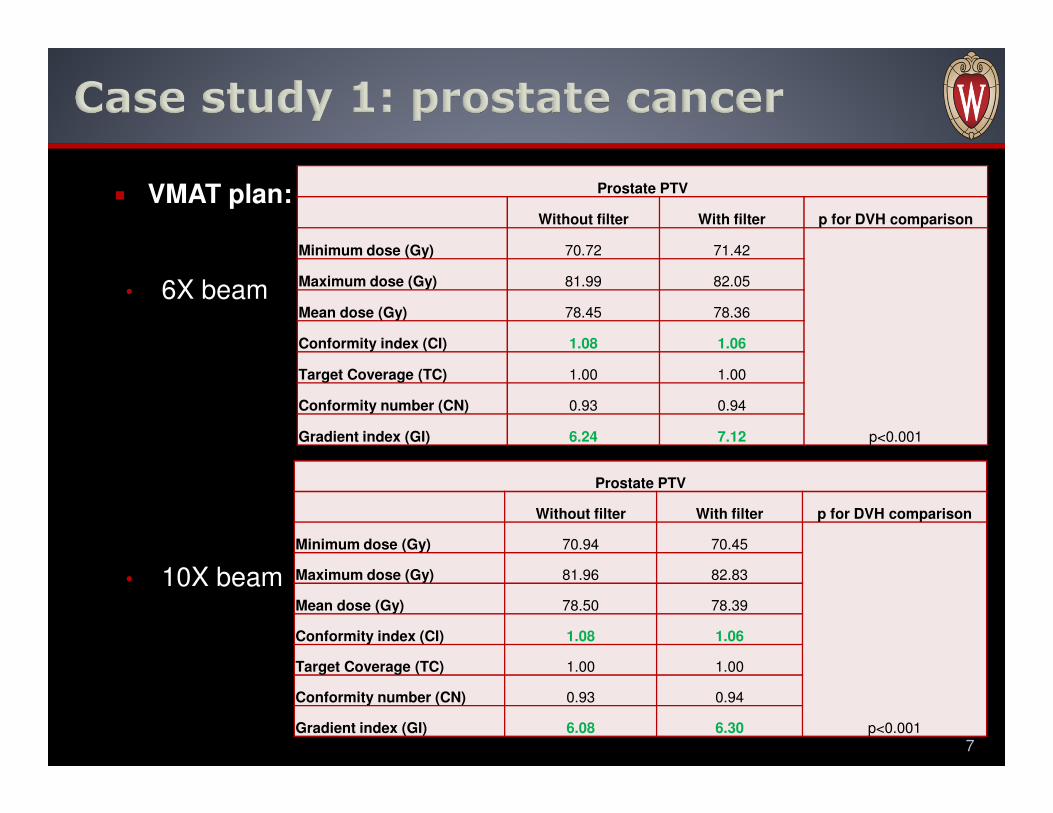
� VMAT plan:
• 6X beam
• 10X beam
7
Prostate PTV
Without filter With filter p for DVH comparison
Minimum dose (Gy) 70.72 71.42
p<0.001
Maximum dose (Gy) 81.99 82.05
Mean dose (Gy) 78.45 78.36
Conformity index (CI) 1.08 1.06
Target Coverage (TC) 1.00 1.00
Conformity number (CN) 0.93 0.94
Gradient index (GI) 6.24 7.12
Prostate PTV
Without filter With filter p for DVH comparison
Minimum dose (Gy) 70.94 70.45
p<0.001
Maximum dose (Gy) 81.96 82.83
Mean dose (Gy) 78.50 78.39
Conformity index (CI) 1.08 1.06
Target Coverage (TC) 1.00 1.00
Conformity number (CN) 0.93 0.94
Gradient index (GI) 6.08 6.30
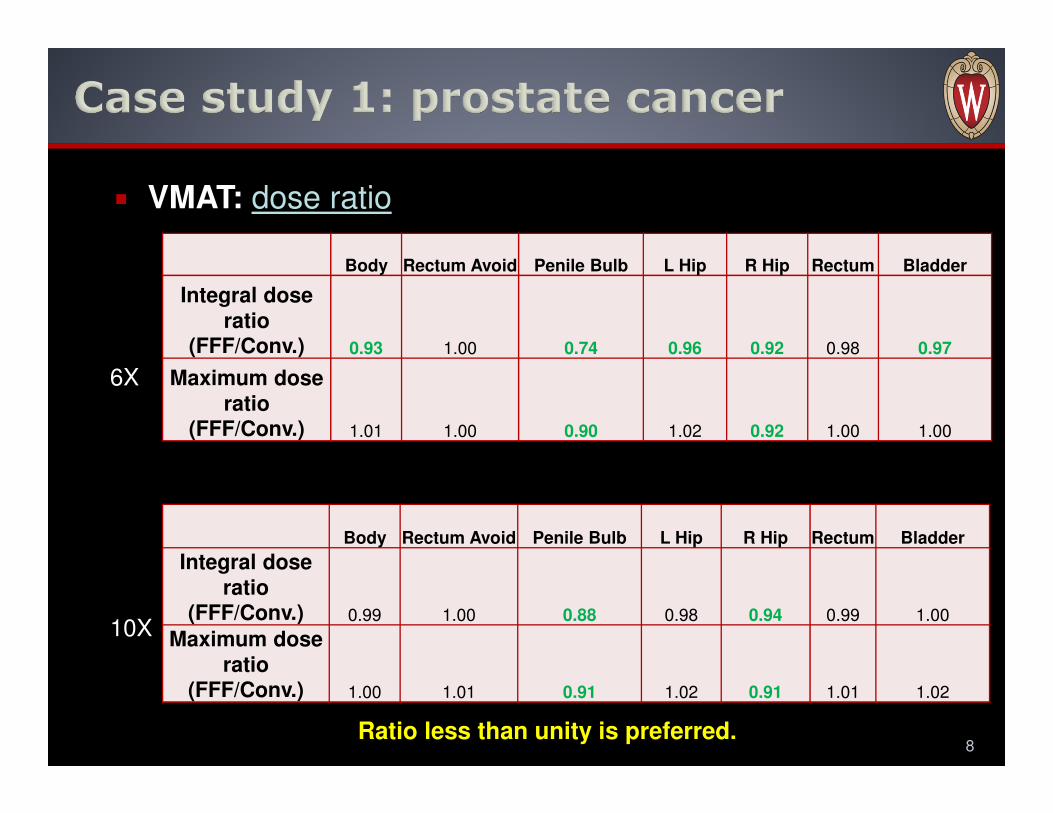
� VMAT: dose ratio
8
6X
10X
Body Rectum Avoid Penile Bulb L Hip R Hip Rectum Bladder
Integral dose
ratio (FFF/Conv.) 0.93 1.00 0.74 0.96 0.92 0.98 0.97
Maximum dose
ratio (FFF/Conv.) 1.01 1.00 0.90 1.02 0.92 1.00 1.00
Body Rectum Avoid Penile Bulb L Hip R Hip Rectum Bladder
Integral dose
ratio (FFF/Conv.) 0.99 1.00 0.88 0.98 0.94 0.99 1.00
Maximum dose
ratio (FFF/Conv.) 1.00 1.01 0.91 1.02 0.91 1.01 1.02
Ratio less than unity is preferred.
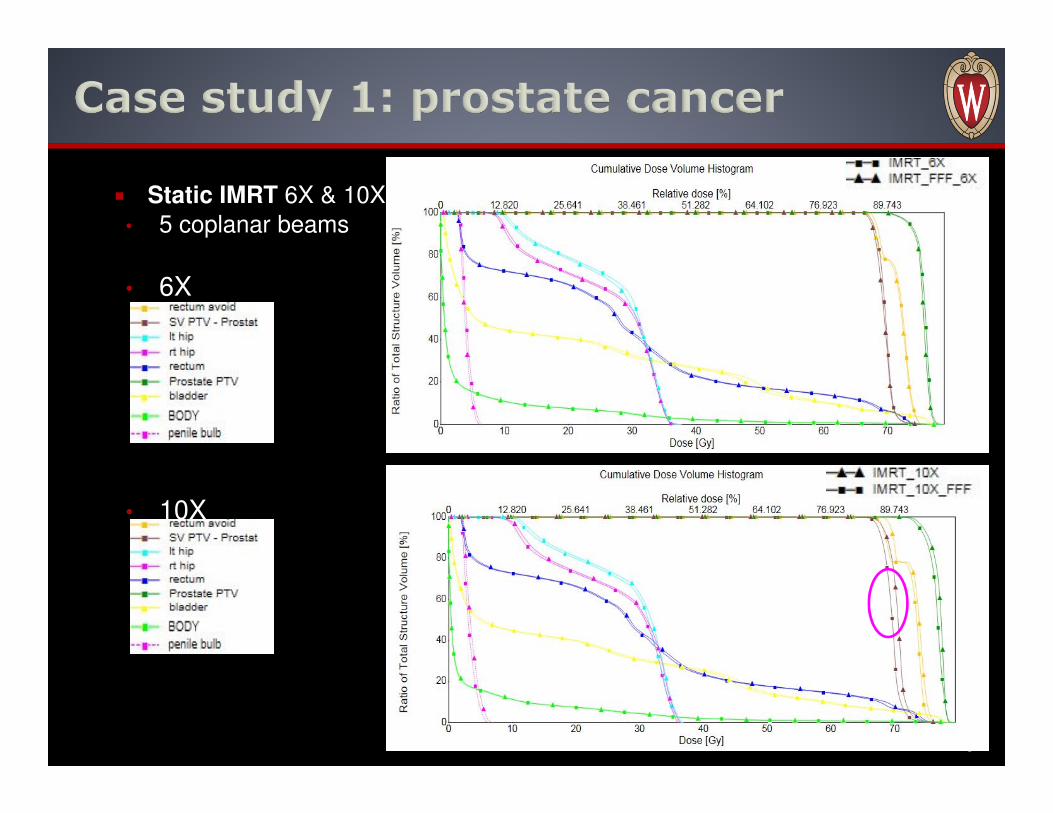
� Static IMRT 6X & 10X
• 5 coplanar beams
• 6X
• 10X
9
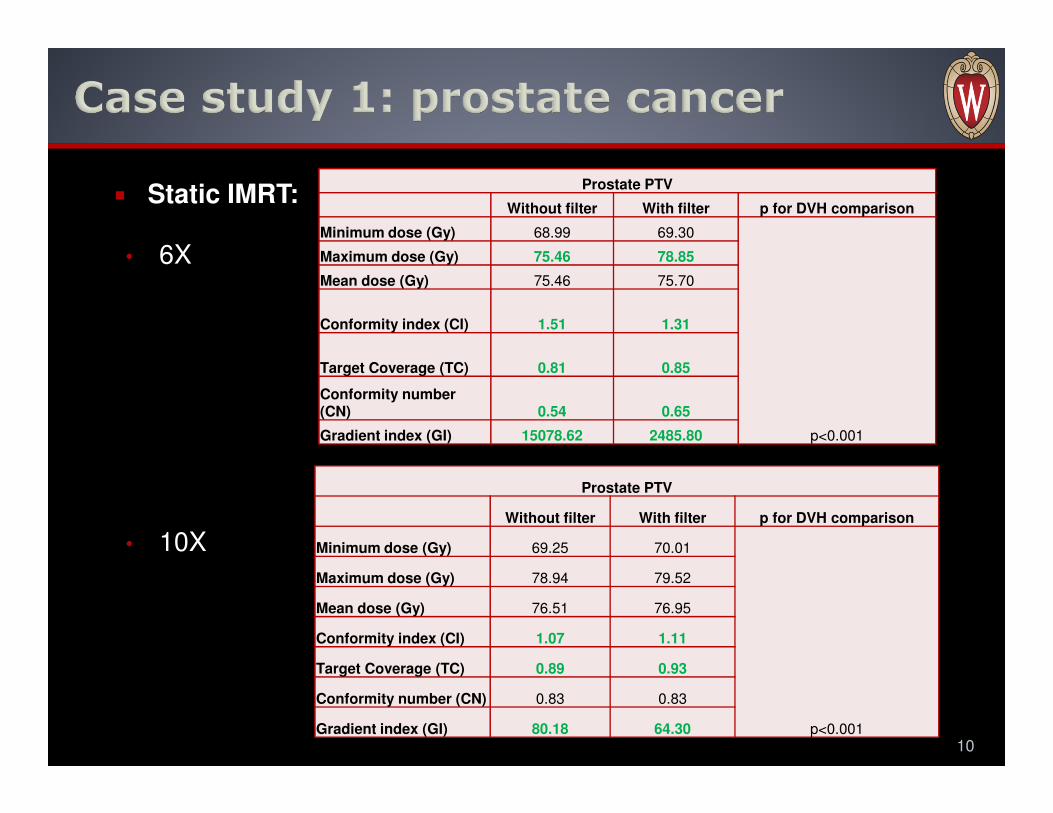
� Static IMRT:
• 6X
• 10X
10
Prostate PTV
Without filter With filter p for DVH comparison
Minimum dose (Gy) 68.99 69.30
p<0.001
Maximum dose (Gy) 75.46 78.85
Mean dose (Gy) 75.46 75.70
Conformity index (CI) 1.51 1.31
Target Coverage (TC) 0.81 0.85
Conformity number (CN) 0.54 0.65
Gradient index (GI) 15078.62 2485.80
Prostate PTV
Without filter With filter p for DVH comparison
Minimum dose (Gy) 69.25 70.01
p<0.001
Maximum dose (Gy) 78.94 79.52
Mean dose (Gy) 76.51 76.95
Conformity index (CI) 1.07 1.11
Target Coverage (TC) 0.89 0.93
Conformity number (CN) 0.83 0.83
Gradient index (GI) 80.18 64.30

� Static IMRT:
• 6X
• 10X
11
Body Rectum Avoid Penile Bulb L Hip R Hip Rectum Bladder
Integral
dose ratio (FFF/Conv.) 1.01 1.00 0.94 0.99 0.99 0.99 1.02
Maximum
dose ratio (FFF/Conv.) 1.00 1.00 0.94 1.01 1.02 1.00 1.00
Body Rectum Avoid Penile Bulb L Hip R Hip Rectum Bladder
Integral
dose ratio (FFF/Conv.) 1.00 0.99 0.90 0.98 0.98 0.99 1.01
Maximum
dose ratio (FFF/Conv.) 0.99 0.99 0.92 0.99 0.99 0.99 1.00
Ratio less than unity is preferred.
12
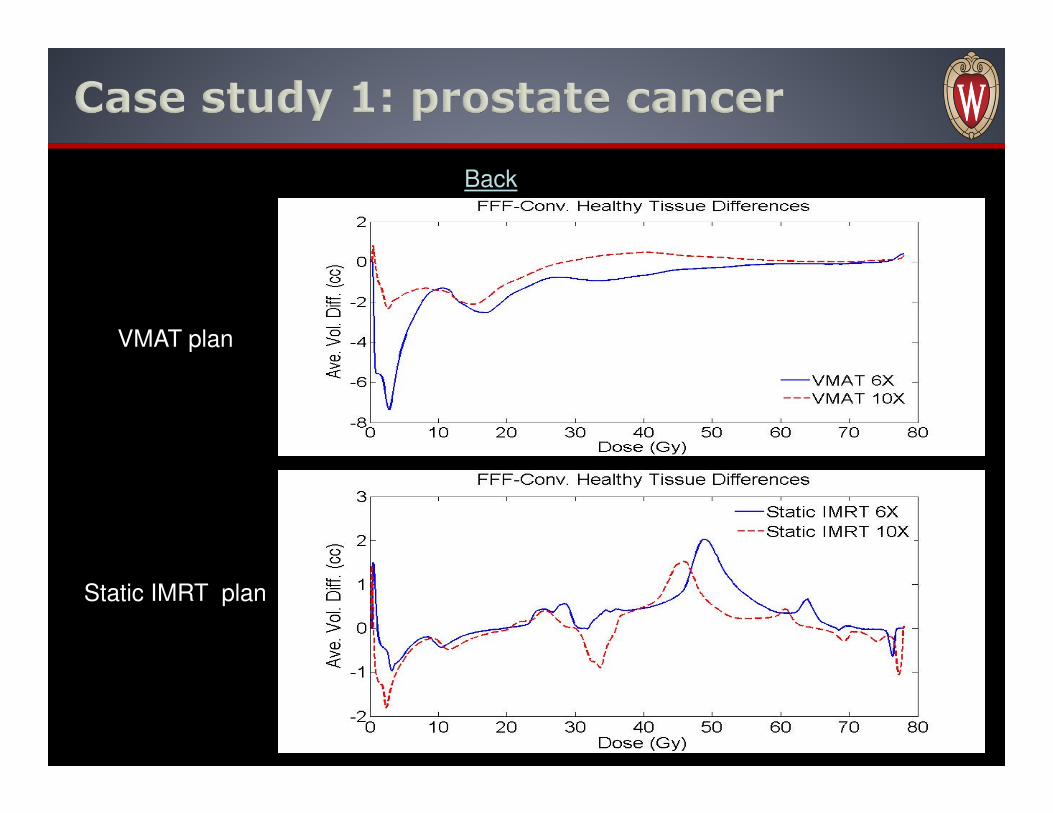
Back
VMAT plan
Static IMRT plan
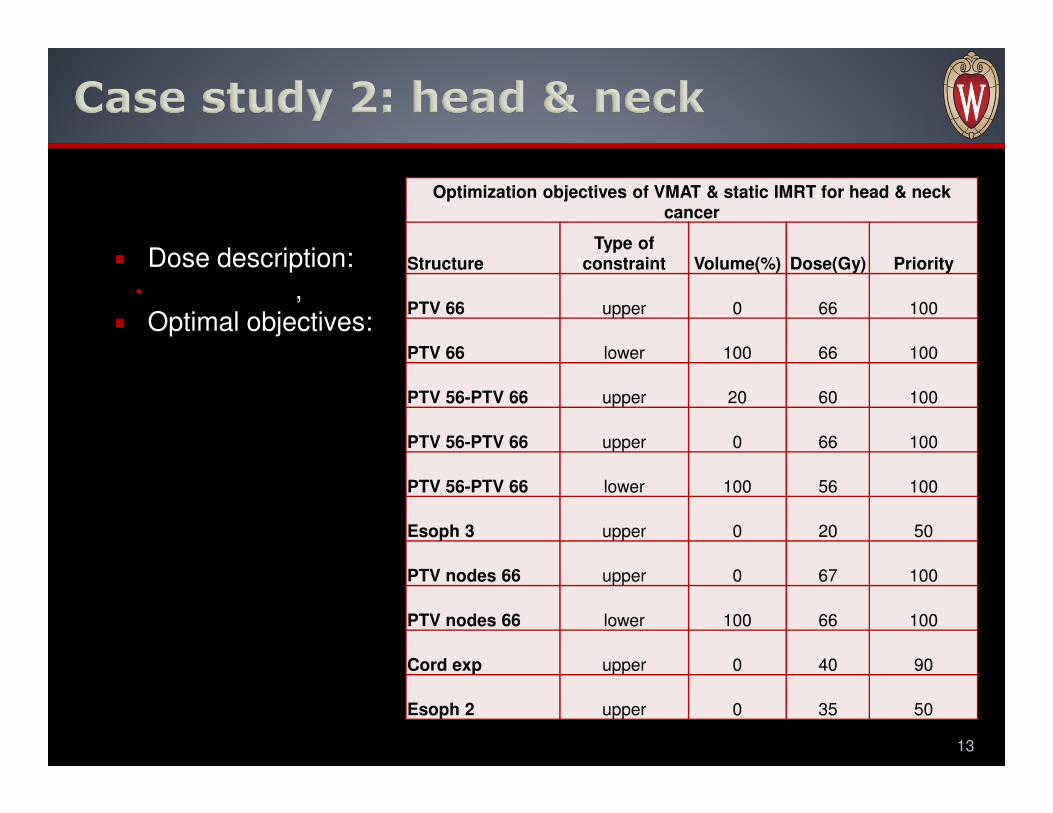
� Dose description:• ,
� Optimal objectives:
13
Optimization objectives of VMAT & static IMRT for head & neck cancer
StructureType of
constraint Volume(%) Dose(Gy) Priority
PTV 66 upper 0 66 100
PTV 66 lower 100 66 100
PTV 56-PTV 66 upper 20 60 100
PTV 56-PTV 66 upper 0 66 100
PTV 56-PTV 66 lower 100 56 100
Esoph 3 upper 0 20 50
PTV nodes 66 upper 0 67 100
PTV nodes 66 lower 100 66 100
Cord exp upper 0 40 90
Esoph 2 upper 0 35 50
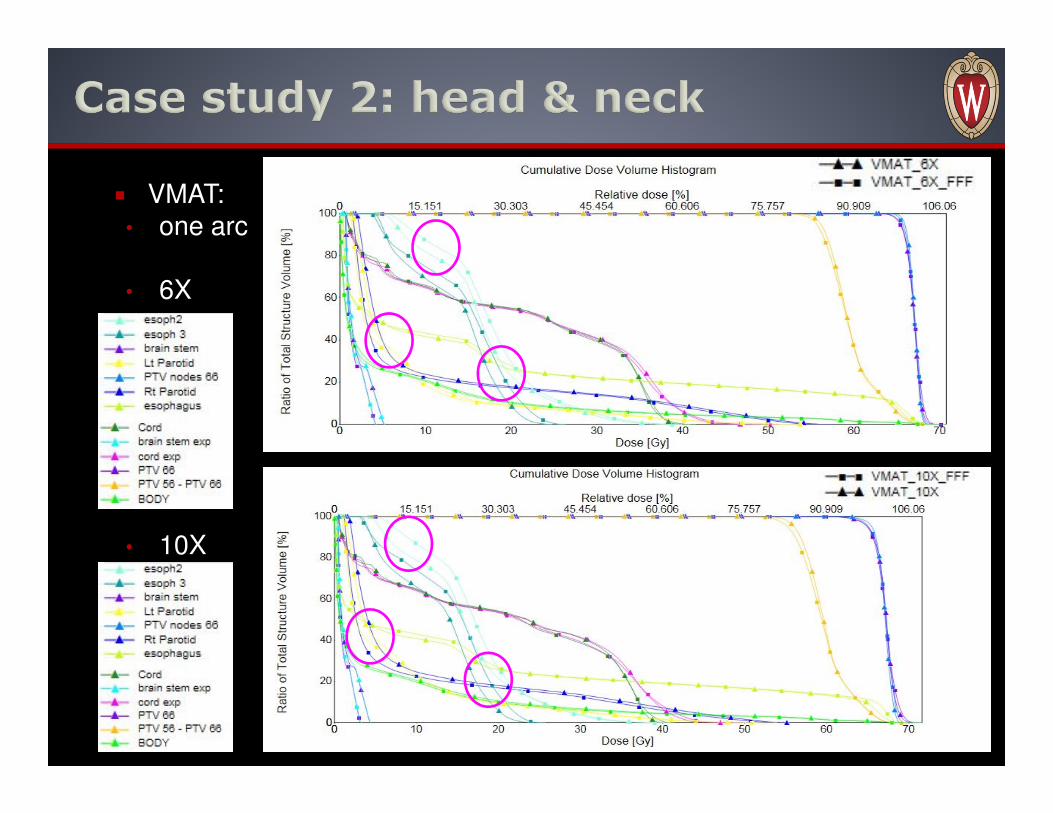
� VMAT: • one arc
• 6X
• 10X
14
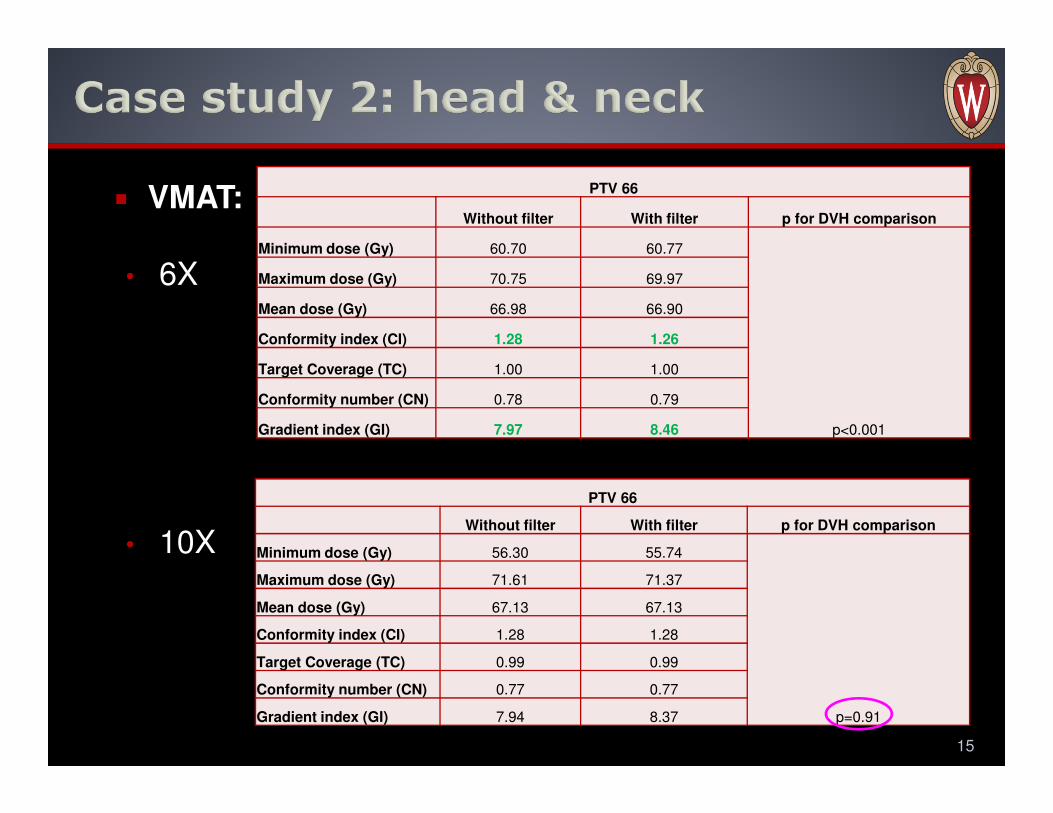
� VMAT:
• 6X
• 10X
15
PTV 66
Without filter With filter p for DVH comparison
Minimum dose (Gy) 60.70 60.77
p<0.001
Maximum dose (Gy) 70.75 69.97
Mean dose (Gy) 66.98 66.90
Conformity index (CI) 1.28 1.26
Target Coverage (TC) 1.00 1.00
Conformity number (CN) 0.78 0.79
Gradient index (GI) 7.97 8.46
PTV 66
Without filter With filter p for DVH comparison
Minimum dose (Gy) 56.30 55.74
p=0.91
Maximum dose (Gy) 71.61 71.37
Mean dose (Gy) 67.13 67.13
Conformity index (CI) 1.28 1.28
Target Coverage (TC) 0.99 0.99
Conformity number (CN) 0.77 0.77
Gradient index (GI) 7.94 8.37

� VMAT:
16
6X
10X
Body Brain StemBrain Stem
Exp L Parotid R Parotid Cord Esophagus
Integral dose
ratio (FFF/Conv.) 0.96 0.82 0.82 0.90 0.90 0.99 1.02
Maximum
dose ratio (FFF/Conv.) 1.01 0.81 0.81 1.00 0.97 1.02 1.00
Body Brain StemBrain Stem
Exp L Parotid R Parotid Cord Esophagus
Integral dose
ratio (FFF/Conv.) 0.95 0.75 0.75 0.92 0.86 0.99 1.03
Maximum
dose ratio (FFF/Conv.) 1.00 0.73 0.73 0.97 1.00 1.01 1.01
Ratio less than unity is preferred.

� Static IMRT: � 7 coplanar beams
• 6X
• 10X
17
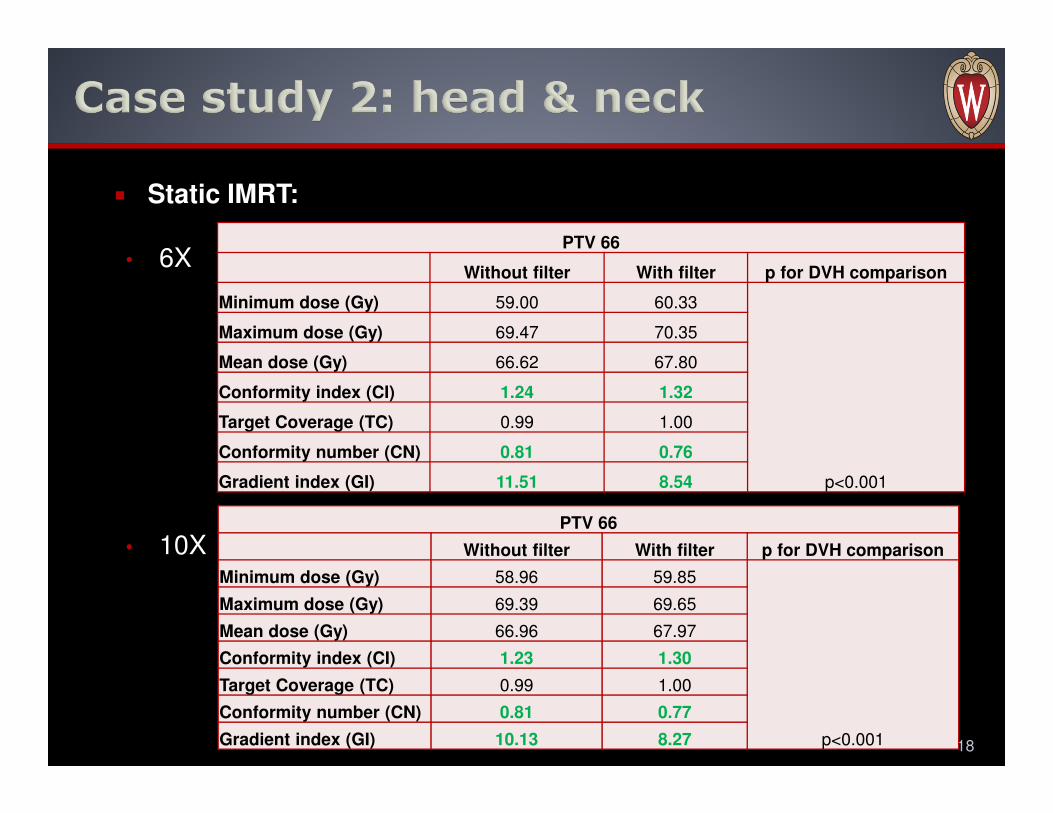
� Static IMRT:
• 6X
• 10X
18
PTV 66
Without filter With filter p for DVH comparison
Minimum dose (Gy) 59.00 60.33
p<0.001
Maximum dose (Gy) 69.47 70.35
Mean dose (Gy) 66.62 67.80
Conformity index (CI) 1.24 1.32
Target Coverage (TC) 0.99 1.00
Conformity number (CN) 0.81 0.76
Gradient index (GI) 11.51 8.54
PTV 66
Without filter With filter p for DVH comparison
Minimum dose (Gy) 58.96 59.85
p<0.001
Maximum dose (Gy) 69.39 69.65
Mean dose (Gy) 66.96 67.97
Conformity index (CI) 1.23 1.30
Target Coverage (TC) 0.99 1.00
Conformity number (CN) 0.81 0.77
Gradient index (GI) 10.13 8.27

� Static IMRT:
19
Body Brain StemBrain Stem
Exp L Parotid R Parotid Cord Esophagus
Integral dose
ratio (FFF/Conv.) 0.96 0.82 0.82 0.90 0.90 0.99 1.02
Maximum
dose ratio (FFF/Conv.) 1.01 0.81 0.81 1.00 0.97 1.02 1.00
6X
Body Brain StemBrain Stem
Exp L Parotid R Parotid Cord Esophagus
Integral dose
ratio (FFF/Conv.) 0.97 0.85 0.84 0.92 0.93 0.99 0.98
Maximum
dose ratio (FFF/Conv.) 0.99 0.79 0.79 0.98 0.98 0.97 0.97
10X
Ratio less than unity is preferred.
20
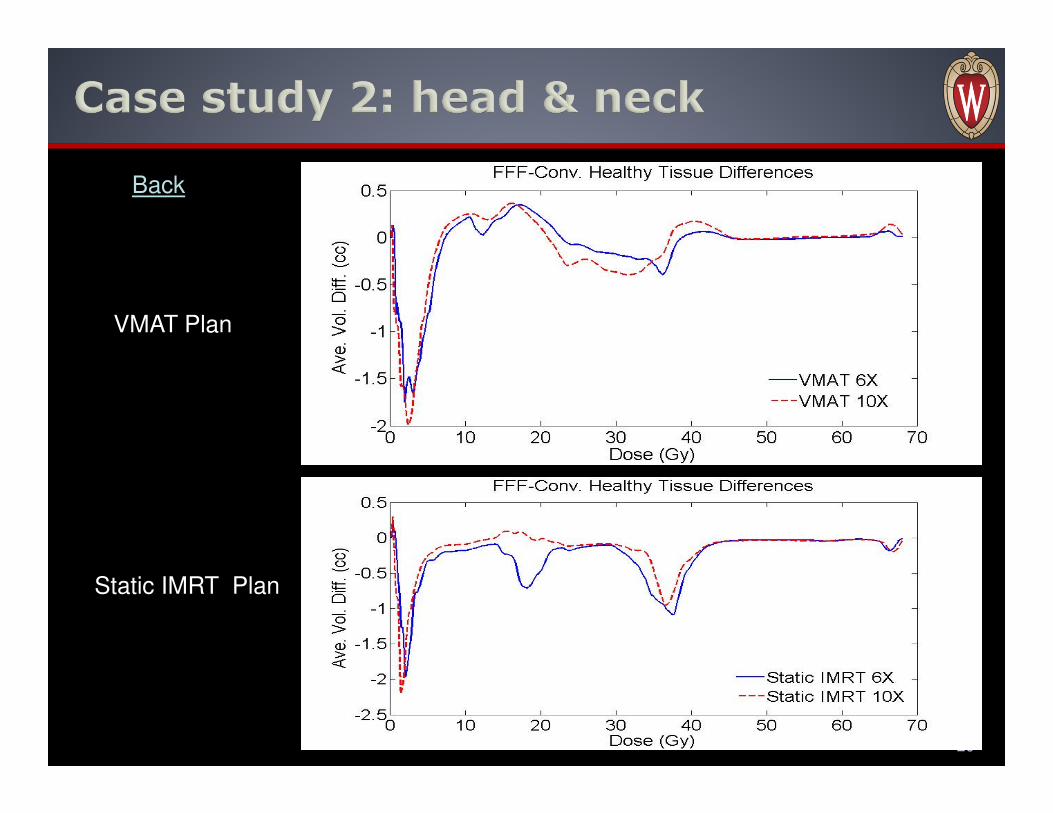
Back
VMAT Plan
Static IMRT Plan
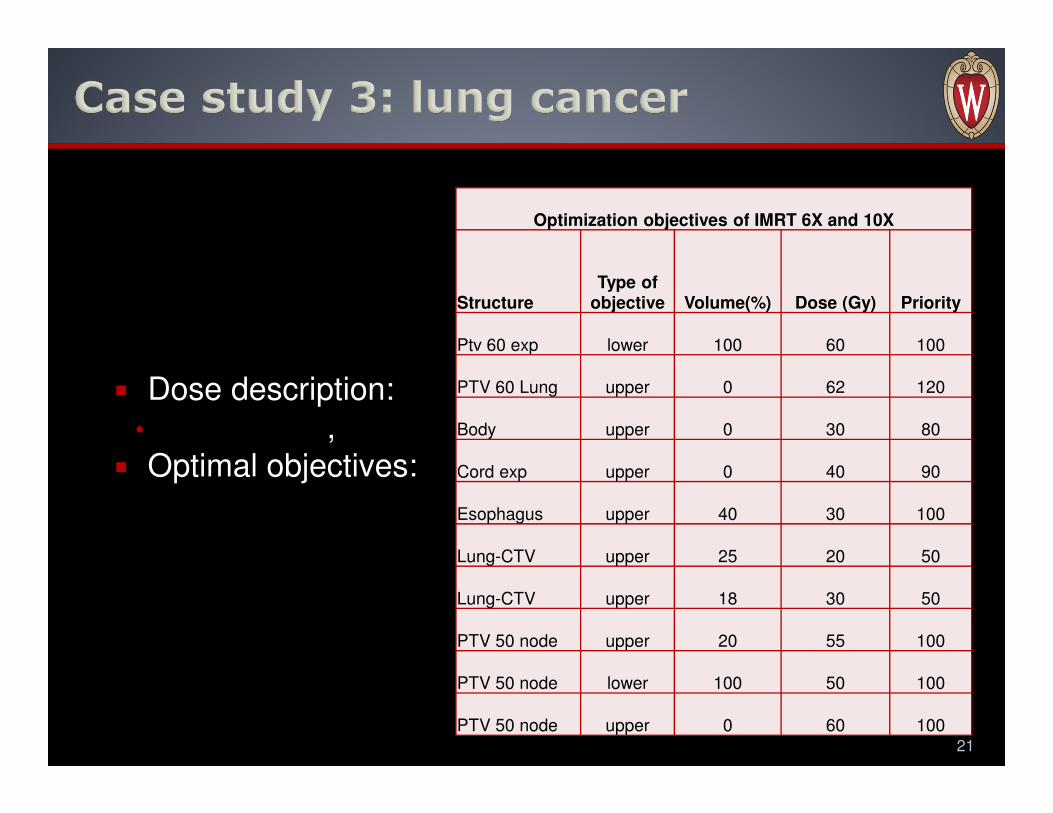
� Dose description:
• ,
� Optimal objectives:
21
Optimization objectives of IMRT 6X and 10X
StructureType of
objective Volume(%) Dose (Gy) Priority
Ptv 60 exp lower 100 60 100
PTV 60 Lung upper 0 62 120
Body upper 0 30 80
Cord exp upper 0 40 90
Esophagus upper 40 30 100
Lung-CTV upper 25 20 50
Lung-CTV upper 18 30 50
PTV 50 node upper 20 55 100
PTV 50 node lower 100 50 100
PTV 50 node upper 0 60 100

� Static IMRT:• 9 beams 6X
22
Conv. Beam
FFF. Beam

� Static IMRT:
• 6X
• 10X
23
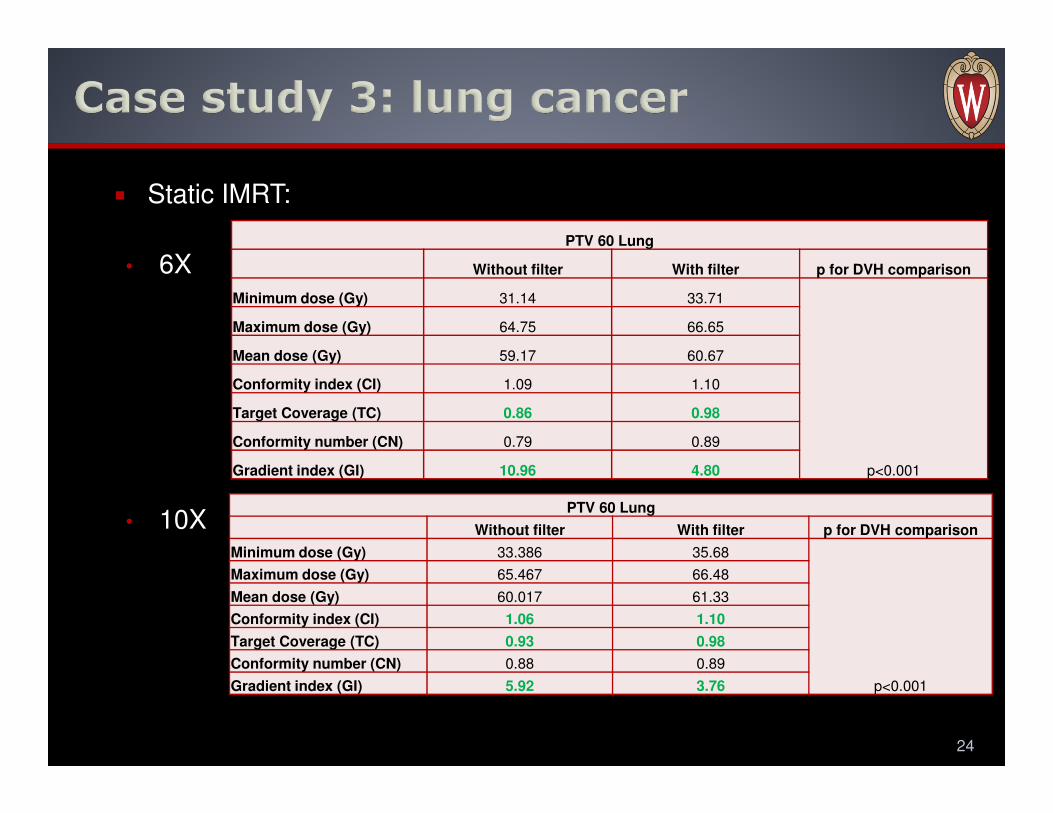
� Static IMRT:
• 6X
• 10X
24
PTV 60 Lung
Without filter With filter p for DVH comparison
Minimum dose (Gy) 31.14 33.71
p<0.001
Maximum dose (Gy) 64.75 66.65
Mean dose (Gy) 59.17 60.67
Conformity index (CI) 1.09 1.10
Target Coverage (TC) 0.86 0.98
Conformity number (CN) 0.79 0.89
Gradient index (GI) 10.96 4.80
PTV 60 Lung
Without filter With filter p for DVH comparison
Minimum dose (Gy) 33.386 35.68
p<0.001
Maximum dose (Gy) 65.467 66.48
Mean dose (Gy) 60.017 61.33
Conformity index (CI) 1.06 1.10
Target Coverage (TC) 0.93 0.98
Conformity number (CN) 0.88 0.89
Gradient index (GI) 5.92 3.76
Static IMRT:
6X
10X
25
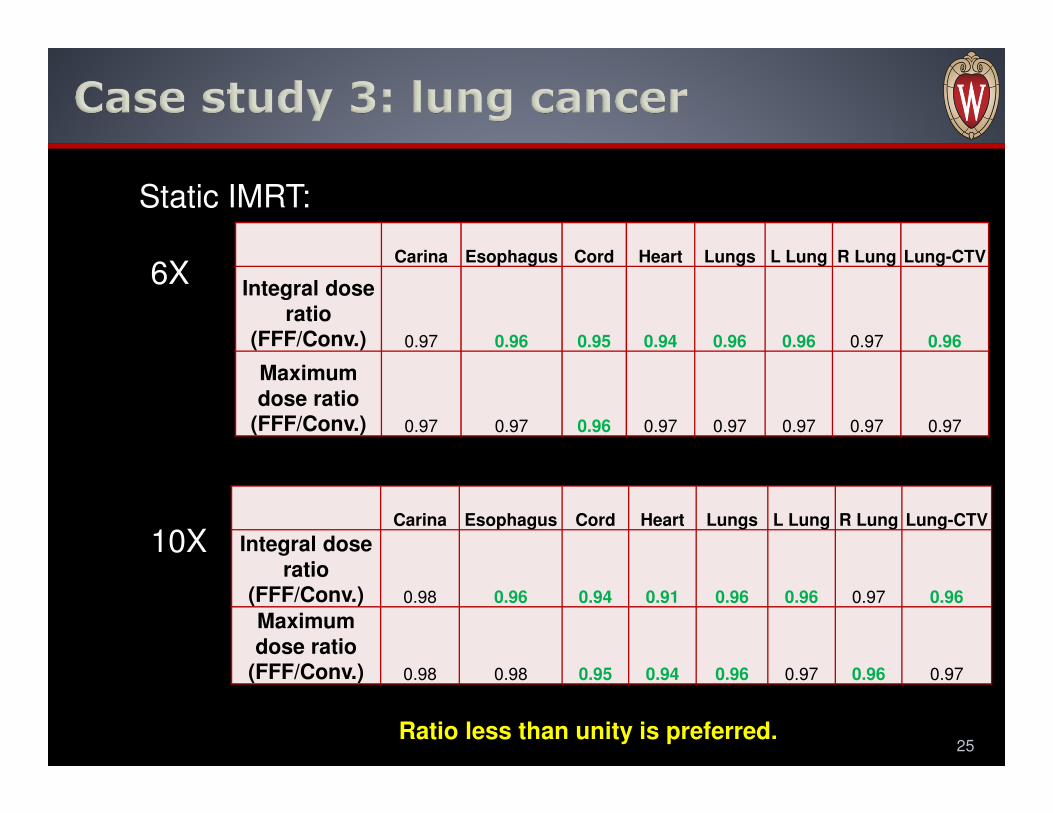
Carina Esophagus Cord Heart Lungs L Lung R Lung Lung-CTV
Integral dose
ratio (FFF/Conv.) 0.97 0.96 0.95 0.94 0.96 0.96 0.97 0.96
Maximum
dose ratio (FFF/Conv.) 0.97 0.97 0.96 0.97 0.97 0.97 0.97 0.97
Carina Esophagus Cord Heart Lungs L Lung R Lung Lung-CTV
Integral dose
ratio (FFF/Conv.) 0.98 0.96 0.94 0.91 0.96 0.96 0.97 0.96
Maximum
dose ratio (FFF/Conv.) 0.98 0.98 0.95 0.94 0.96 0.97 0.96 0.97
Ratio less than unity is preferred.
26

� FFF beam usually can provide comparative treatment
plan with improved dose sparing effect to ORAs.
� However, the soft spectrum of FFF beam lead to lower
mean dose for target coverage, which may need extra
consideration in treatment plan.
� Density inhomogeneity in PTV is an important factor to
influence both PTV coverage and sparing effect to
OARs for FFF beam and it may lead to unacceptable
PTV coverage for FFF beam.
� Completely removing flatten filter may NOT be optimal.
27

� [1] Georg D, Knöös T and McClean B.(2011) Current status and future perspective
of flattening filter free photon beams. Med Phys 38(3):1280-1293.
� [2] Huang YF, Siochi RA, Bayouth JE.(2012) Dosimetric properties of a beam
quality-matched 6 MV unflattened photon beam. J Appl Clin Med Phys 13(4):71-81.
� [3] Vassiliev ON, Titt U, Kry SF, Pönisch F, Gillin MT and Mohan R. (2006) Monte
Carlo study of photon fields from a flattening filter-free clinical accelerator. Med Phys
33(4):820-827.
� [4] Reggiori G, Mancosu P, Castiglioni S, Alongi F, Pellegrini C, Lobefalo F, Catalano
M, Fogliata A, Arcangeli S, Navarria P, Cozzi L and Scorsetti M. (2012) Can
volumetric modulated arc therapy with flattening filter free beams play a role in
stereotactic body radiotherapy for liver lesions? A volume-based analysis. Med Phys
39(2):1112-1118.
� [5] Titt U, Vassiliev ON, Pönisch F, Dong L, Liu H and Mohan R.(2006) A flattening
filter free photon treatment concept evaluation with Monte Carlo. Med Phys
33(6):1595-1602.
� [6] Kry SF, Vassiliev ON and Mohan R.(2010) Out-of-field photon dose following
removal of the flattening filter from a medical accelerator. Phys Med Biol 55 2155-
2166.
� [7] Kry SF, Howell RM, Titt U, Salehpour M, Mohan R and Vassiliev ON. (2008)
Energy spectra, sources, and shielding considerations for neutrons generated by a
flattening filter-free Clinac. Med Phys 35(5):1906-1911.
28
� [8] Chofor N, Harder D. Willborn KC and Poppe B. (2011) Internal scatter, the
unavoidable major component of the peripheral dose in photon-beam radiotherapy.
Phys. Med. Biol. 57 1733-1743.
� [9] Ong CL, Dahele M, Cuijpers JP, Senan S, Slotman BJ and Verbakel WFAR.
(2013) Dosimetric impact of intrafraction motion during RapidArc stereotactic
vertebral radiation therapy using flattened and flattening filter-free beams. Int J
Radiat Oncol Biol Phys 86(3): 420-5.
� [10] Zhang GG, Ku L, Dilling TJ, Stevens CW, Zhang RR, Li W and Feygelman V.
(2011) Volumetric modulated arc planning for lung stereotactic body radiotherapy
using conventional and unflattened photon beams: a dosimetric comparison with 3D
technique. Radiat Oncol 6:152.
29
e
http://www.medphysics.wisc.edu





![[Paliwal, Manisha] Business Ethics(BookFi.org)[1]](https://img.pdfslide.net/doc/110x75/5695d1ba1a28ab9b0297b41d/paliwal-manisha-business-ethicsbookfiorg1.jpg)