Embed Size (px)
Citation preview

Updated Public assessment report
EU worksharing project paediatric data
Zantac 150 and 300 mg tablets
Zantac syrup: 150 mg/10 ml
Zantac 50 mg/2 ml solution for injection
[ranitidine]
Marketing authorisation holder: GlaxoSmithKline
Rapporteur Medicines Evaluation Board, The
Netherlands
Co-rapporteur Instituto Nacional da Farmacia e do
Medicamento, Portugal
Start 1st round
Clock-off period
Procedure re-start date
1 February 2007
1 May 2007 – 8 November 2007
8 November 2007
Finalisation procedure 13 March 2008
Date of this updated public assessment
report
18 March 2013

2
Currently approved adult indication(s): Oral formulations:
- Duodenal ulcer and benign gastric ulcer,
including that associated with non-steroidal anti-inflammatory agents.
- Prevention of non-steroidal anti-inflammatory drug (NSAID) (including aspirin) associated duodenal ulcers, especially in patients with a history of peptic ulcer disease.
- Duodenal ulcer associated with Helicobacter pylori infection.
- Post-operative ulcer. - Reflux oesophagitis. - Symptom relief in gastro-oesophageal
reflux disease. - Zollinger-Ellison Syndrome.
- Chronic episodic dyspepsia, characterised by pain (epigastric or retrosternal) which is related to meals or disturbs sleep but not associated with the above conditions.
- Prophylaxis of stress ulceration in seriously ill patients.
- Prophylaxis of recurrent haemorrhage from peptic ulcer.
- Prophylaxis of Mendelson's syndrome.
Injection:
- Duodenal ulcer. - Benign gastric ulcer.
- Post-operative ulcer. - Reflux oesophagitis.
- Zollinger-Ellison Syndrome. - Prophylaxis of stress ulceration in
seriously ill. - Prophylaxis of recurrent haemorrhage
from peptic ulcer.
- Prophylaxis of Mendelson's syndrome.
Pharmaceutical form(s) affected by this
project:
Tablets/Syrup/Solution for injection
Strenght(s) affected by this variation:
Tablets: 150 and 300 mg
Syrup: 150 mg/10 ml
Solution for injection: 50 mg/2 ml

3
Content
I Recommendation............................................................................................ 4
I.1 Scope of the variation ................................................................................... 4
I.2 Supplementary paragraph ............................................................................. 5
I.2.1 Peptic ulcer disease ................................................................................ 5
I.2.2 Gastro-oesophageal reflux disease ........................................................... 5
I.2.3 Prophylaxis of stress ulceration ................................................................ 6
II. Scientific discussion ...................................................................................... 6
II.1 Quality aspects ......................................................................................... 6
II.2 Non-Clinical aspects .................................................................................. 6
II.3 Clinical aspects ......................................................................................... 6
II.3.1 Study RC1 998/00023/00 ........................................................................ 6
II.3.2 Pharmacokinetics ..................................................................................11
II.3.3 Pharmacodynamics and Efficacy ..............................................................13
II.3.4 Efficacy data .........................................................................................13
II.3.5 Safety .................................................................................................15
III OVERALL CONCLUSION ................................................................................22
IV. Final agreed changes in the Smpc’s ...............................................................24
Annex I: The MHRA report on Zantac tablets, Zantac effervescent tablets, 300mg,
150mg, Zantac injection 50mg/2ml, Zantac syrup 75mg/5ml .....................................28
Annex II – Safety data overview.............................................................................50
Annex III: Cited references ....................................................................................53

4
Note for the reader:
This updated public assessment report (March 2013) reflects the discussion in the EU
worksharing project paediatric data (procedure finalised on March 13th 2008) for
ranitidine in the treatment of “short term treatment of peptic ulcer and in treatment of
gastro-oesophageal reflux, including reflux oesophagitis and symptomatic relief of
gastro-oesophageal reflux disease” in paediatric populations”.
On 26 November 2009 an Article 45 of the Regulation (EC)No 1901/2006, as amended
on medicinal products for paediatric use (SE/W/0007/pdWS/001) was finalised (Date of
public assessment report February 9th 2010). The data submitted within this article 45
worksharing procedure partly overlapped the data as discussed in this public assessment
report. Based on the new available data in combination with the previous art 45
procedure it was concluded that the new data did not alter the conclusions as stated in
the previous report.
I RECOMMENDATION The Rapporteurs conclude that based on the submitted paediatric data on safety and
efficacy for ranitidine (Zantac 150 and 300 mg tablets, Zantac syrup 150 mg/10 ml and
Zantac solution for injection 50 mg/2ml) the paediatric indications (short term treatment
of peptic ulcer and in treatment of gastro-oesophageal reflux, including reflux
oesophagitis and symptomatic relief of gastro-oesophageal reflux disease) and posology
as mentioned in the SmPC’s under section 4.1 and 4.2 are acceptable. In addition
changes to SmPC sections 4.8, 5.1 (i.v. formulation only), 5.2 were agreed upon. Refer
to section III of this report for final agreed SmPC’s texts.
I.1 Scope of the variation Zantac (ranitidine hydrochloride) is a histamine H2-receptor antagonist that inhibits
gastric acid secretion. It was first approved in Italy in 1981 and is now available in over
130 countries. In 1998 paediatric information on Zantac has been submitted to the US
Food and Drugs Administration (FDA), under the paediatric exclusivity rules. Reports of
two pharmacokinetic studies and five controlled clinical studies of the use of ranitidine in
children in an oral and intravenous formulation, together with a list of published
information available at the time of submission were submitted.
The UK Medicines and Healthcare Products Regulatory Agency (MHRA) requested the
paediatric data previously submitted to the FDA in 2001. These data were submitted,
however as a result of the Article 30 procedure which was initiated, a full review of the
data was not completed. In 2004 the MHRA requested re-submission of these data. This
was done in September 2004 and was followed shortly after by a Type II variation
proposing SmPC wording and a clinical overview of the available supporting data,
including clinical studies and published literature. This resulted in additional paediatric
indications being added to the UK SmPCs.
This submission contains paediatric data previously submitted to the FDA and the MHRA
concerning the use of Zantac in paediatric patients. It also contains the information
requested as part of the worksharing assessment procedure.
The MAH proposes to broaden the present paediatric indication for the oral formulations
for the treatment of peptic ulcer (age unspecified), to include indications for the long
term management of peptic ulcer and the treatment of gastro-oesophageal reflux
(including reflux oesophagitis and gastro-oesophageal reflux disease) from 1 month of
age and above. In addition to the above for the injection formulation, the MAH has
applied for the following indications from 1 month onwards: the short term treatment of
peptic ulcer and the prevention of stress ulcers in seriously ill children.

5
I.2 Supplementary paragraph In this paragraph the submitted general literature on ranitidine is summarised. See
Annex III for a list of references.
I.2.1 Peptic ulcer disease
Primary duodenal ulcer occurs in children of all ages but is most often seen in those over
10 years of age (Gryboski, 1991). Peptic ulcers in young children are more unusual and
are typically secondary to systemic illnesses or drugs. Duodenal ulcers in older children
and adolescents have a relapsing course that is increasingly recognized as being related
to coexisting, chronic active antral gastritis and Helicobactor-pylori infection (Sherman,
1994).
Not all primary duodenal ulcers in the paediatric population are related to H. pylori and
their cause remains unknown. Treatment of these patients requires anti-ulcer treatment
and long-term maintenance therapy (Sherman, 1994).
A number of studies are available regarding the use of oral ranitidine in peptic ulcer
disease in children. A few of these are placebo- or cimetidine-controlled. Evaluative
procedures are similar to those used in adults, with therapeutic efficacy defined as
endoscopic proof of ulcer healing. Dosage regimens of up to 5 to 10 mg/kg/day have
been reported in the literature for use of Zantac in the treatment of peptic ulcer disease
(e.g. de Angelis & Banchini, 1989; Scorza et al, 1990; Oderda & Ansaldi, 1988).
The general consensus for maintenance therapy seems to be a single night time dose of
3- 5mg/kg for one month (de Angelis & Banchini, 1989; Scorza et al, 1990; Oderda
& Ansaldi, 1988).
Ranitidine has also been used as a component of multi-drug regimens to eradicate H.
pylori in children. Scherbakov et al (2001) evaluated the efficacy of triple therapy
regimens comprising amoxicillin (750 mg/day) and metronidazole (30-40mg/kg/day)
with one of proprietary omeprazole (20-40mgday), generic omeprazole (20-40mg/day)
or ranitidine (150 mg twice daily) in 106 children aged 5 to 15 years. The H. pylori
eradication rate in the ranitidine group (n=35) was 74.3%, whilst the ulcer healing rate
at 7 days was 100%. Two patients relapsed 4 weeks after the start of treatment, thus
the 6 week ulcer healing rate with ranitidine was 94.3%. The regimen containing
proprietary omeprazole was more effective than the ranitidine.
There are limited published data on the clinical use of parenteral ranitidine in children
with peptic ulcer disease. Blumer investigated the pharmacokinetics and
pharmacodynamics of intravenous and oral ranitidine in paediatric patients with duodenal
or gastric ulcer (Blumer et al, 1985). This study involved three phases, two of which
involved parenteral administration: a dose ranging phase designed to determine the dose
of ranitidine required to inhibit gastric acid secretion by ≥ 90%, and intravenous bolus
regimen in which the drug was administered every 6 hours at a dose designed to yield
the average serum concentration required to inhibit gastric acid secretion by ≥ 90%. The
patient received oral ranitidine therapy once their nasogastric tubes were removed. Bolus
doses of between 0.13 and 0.80 mg/kg were administered every 6 hours for an
unspecified therapy. All ulcers were healed on repeat endoscopy at the end of the 6 week
study period.
I.2.2 Gastro-oesophageal reflux disease
Gastro-oesophageal reflux disease (GORD) is a common motility disorder in infancy and
childhood but in the majority of neurologically normal infants symptoms resolve by age
one. Many infants are successfully managed by conservative treatment such as dietary
management and attention to posture. The rationale for medical treatment will be
influenced by signs of more serious disease such as oesophagitis, excessive irritability,
failure to thrive, apnoea, or chronic pulmonary disease (Cezard, 2004). Oral
administration of ranitidine (5-10 mg/kg/day) has been shown to produce symptomatic
and endoscopic improvement in children. Endoscopic examination reported the frequency
of erosive oesophagitis healing of 75-85% at week 8 and 100% at week 12. Patients with
refractory erosive oesophagitis have received doses up to 20 mg/kg/day.
De Angelis and Banchini (1989) reported their experience of the use of ranitidine in
the treatment and prophylaxis of gastro-intestinal disorders in 391 children aged from 72

6
hours to 16 years. The children received oral ranitidine at a dose of 6-8 mg/kg/day
initially, followed by maintenance therapy of 3-4mg/kg/day. Intravenous administration
was used in appropriate cases, such as those with upper gastrointestinal haemorrhage or
in severe oesophagitis due to the ingestion of caustic substances. Reflux oesophagitis
was treated in 185 patients; in 25 severe cases, endoscopy revealed re-epithelialisation
in all patients. In those children with less severe oesophagitis, 95% showed at endoscopy
disappearance or marked improvement of lesions, both macroscopically and
histologically.
In an open label prospective study, Karjoo and Kane (1995) found visual and/or
histologic evidence of peptic oesophagitis in 84% of 153 patients 6-18 years of age
(mean 9.9 years) with chronic abdominal pain lasting more than 3 weeks. These 129
children were initially treated with 4mg/kg ranitidine twice daily for 2 weeks, increasing
to 4mg three times daily for a further 2 weeks. If symptoms persisted patients were
switched to omeprazole. Seventy percent of patients had symptom improvement with
ranitidine.
The effect of high dose ranitidine (10mg/kg twice daily) has been compared with
omeprazole (40mg/day/1.73m2) in 25 paediatric patients (aged 6 months to 13.4 years)
who had previously not responded to 8 weeks of ranitidine at 8mg/kg/day and cisapride
(Cucchiara et al, 1993). Both drugs produced comparable oesophagitis healing and
symptom relief.
I.2.3 Prophylaxis of stress ulceration
For prophylaxis of stress ulceration in critically ill children ranitidine is administered either
as an intermittent intravenous infusion (2-6mg/kg/day in divided doses) (Harrison et al,
1998; Kuusela et al, 1997; Kuusela, 1998; Lopez-Herce et al 1988; Osteyee et al
1994; Rylance 1987; Santucci et al, 1991) or as a continuous infusion (0.1-
0.2mg/kg/hr) (Osteyee et al, 1994; Santucci et al, 1991; Dimand et al 1989;
Eddleston et al, 1989) has been successfully used to maintain gastric pH levels above
4.0. Both dosing regimens were effective in increasing and maintaining gastric pH above
4, however the pH values fluctuate more with the intermittent regimens (Osteyee et al,
1994; Santucci et al, 1991).
Oral (via naso-gastric tube) vs intravenous administration of ranitidine in prevention of
stress ulceration has been studied. (Lopez-Herce et al, 1988; Hartemann et al 1987)
The median time pH was above 4 was less in the oral group. The authors suggest that
oral ranitidine may not be as effective due to decreased oral absorption in critically ill
children (Lopez-Herce et al, 1988).
II. SCIENTIFIC DISCUSSION II.1 Quality aspects
N/A II.2 Non-Clinical aspects
See for Non-Clinical aspects section 4.2 of the SmPC for Zantac Syrup 150 mg/10 ml.
II.3 Clinical aspects Several studies have previously been submitted to the MHRA, and the rapporteur took
the liberty to copy the MHRA report as an annex to this report (see Annex I). Therefore
only Study RC1 998/00023/00, which was not included in the submission to the MHRA,
will be discussed in detail in this report, see below. Also an overview of the safety data is
summarized in this report (see Annex II).
II.3.1 Study RC1 998/00023/00
A randomized, double-blind, parallel, single-dose, placebo-controlled study design was
used to investigate the pharmacokinetics and pharmacodynamics of ranitidine 75 mg
administered as Zantac 75 tablets. Seven centers were to enroll children ages 4-11 with
suspected abnormal acid reflux. Approximately 24 evaluable subjects with a

7
randomization schedule of 2:l active to placebo were to be enrolled. All subjects were to
undergo a Screening Visit (Visit l), and those who qualified were to be scheduled to
attend a pharmacokinetic and pharmacodynamic evaluation visit (Visit 2, Treatment
Visit) within 14 days of Visit 1. At Visit 2, an intravenous catheter for blood sampling and
for potential fluid administration was to be inserted, and a gastric pH probe was to be
placed. After an approximate l-hour baseline period of gastric pH monitoring, subjects
were to receive a double-blind, randomized, single-dose administration of study drug.
Subjects were to undergo 6-hours of gastric pH sampling for pharmacodynamic
information and provide ten 2.5 mL samples of blood at scheduled intervals for
pharmacokinetic information. Safety was to be assessed by adverse event monitoring for
the duration of Visit 2.
II.3.1.1 Study objectives
Primary:
Characterize the pharmacokinetics of ranitidine 75 mg in a pediatric population
following a single-dose.
Determine the effect on intragastric pH in a pediatric population of single dose
ranitidine 75mg as compared to placebo.
Secondary:
Obtain adverse experience data in a pediatric population following single doses of
ranitidine 75mg.
II.3.1.2 Pharmacodynamic measures
At Visit 2, each subject had a gastric pH probe inserted through the nose while in the
sitting position. The probe's presence in the stomach was confirmed by the distance of
the tip from the nostril and the recording of a consistent baseline gastric pH (I 3.0) on Qe
pH monitor. For some subjects, x-ray was used to confirm positioning. Only water (not
exceeding 200 mL) was provided to the subject as an aid to swallowing the tube. pH
values were determined prior to dosing and at 4 second intervals for six hours after study
drug administration. In the event that an appropriate and consistent baseline pH could
not be obtained, the subject was to be removed from the study.
From the pH data, the following parameters were calculated for each subject for both the
last 30 minutes of the pre-treatment period and for study hours 0-6 (post-treatment):
AUC of H+ ion concentration,
median gastric pH over the total duration, and
percentage of time gastric pH 3 and gastric pH 4
II.3.1.3 Results
Seventy-one subjects were screened and not enrolled. The reasons these screened
subjects were not enrolled are presented in the following table.
Reason a Screened Subject Was Not Enrolled Number of subjects
Family or subject unwilling/unable to participate (exact reason not specified) 16
Unable to swallow pills 12
Insufficient signs or symptoms of reflux 12
Unwilling/unable to have pH probe 9
Unwilling/unable to fit study into schedule 8
Family unwilling for child to undergo study procedures 6
Prohibitive medical condition 5
Prohibited concomitant medication(s) 2
Subject responding to other medication(s) 1
Total number of subjects 17
A total of 31 subjects were enrolled from the six investigational sites. (One of the 7
investigational sites did not enrol1 any subjects.) Two enrolled subjects were intubated

8
but not randomized due to withdrawn consent. Twenty-nine subjects were randomized to
study drug.
The mean age of the randomized subjects was 8.3 years (range: 4 to 11 years).
Seventeen (59%) of the subjects were male and 12 (41%) were female. All 29 subjects
were white.
The mean height was 133.3 cm (range: 105 - 193 cm) and the mean weight was 31.97
kg (range: 14.4 - 56.2 kg).
On average, the subjects in the placebo group appeared to be slightly older (8.7 years
versus 8.2 years), taller (138.3 cm versus 130.7 cm), and heavier (33.77 kg versus
31.02 kg) than those in the Zantac 75 group.
Among the randomized subjects, the mean number of months with acid reflux symptoms
prior to screening was 35.0 (range: 2-1 12 months), however, there was a notable
difference between the treatment groups. The duration was shorter for the Zantac 75
subjects (mean 30.8, median 14.0) as compared to the placebo subjects (mean 43.0,
median 46.0).
All randomized subjects had at least two acid reflux symptoms at the screening visit, with
no particular symptom being reported more or less often than the others were.
II.3.1.4 Pharmacodynamic Response Data
All 29 randomized subjects had sufficient pH data (at least 5.5 hours) to be included in
the analysis of the pharmacodynamic parameters.
The pharmacodynamic parameters were calculated based on gastric pH values taken
every four-seconds. All pH values outside the physiological range (i.e., <0.7 or 8.5)
were excluded from all statistical analyses. These pH values are referred to as 'invalid pH
values'.
Figure 5 presents the mean gastric pH during the 6.5 hours of measurement for the
Zantac 75 and placebo groups. Gastric pH values are similar for both groups during the
pretreatment period but begin to diverge approximately one half hour after drug
administration. Values in the Zantac 75 group show the greatest rate of increase
between 0.5 to 1 hour after dosing, reaching their highest level approximately 4 hours
after dosing, then slowly decreasing but remaining higher than the placebo group
throughout the balance of the measurements. Gastric pH in the placebo group shows
little change over the period of observation.

9
The following table summarizes the mean value for the pharmacodynamic parameters by
treatment group for both the pre-treatment and post-treatment phases.
Pharmacodynamic Parameter
Phase (hours)
Zantac 75 (N=19)
Placebo (N=10)
AUC for H+ Pre (-0.5 to 0) 39.11 41.99
Post (0 to 6) 227.42 555.11
Median gastric pH Pre (-0.5 to 0) 1.27 6 1.161
Post (0 to 6) 2.861 1.247
% of time gastric pH>4 - Pre (-0.5 to 0) l.2% 1.4%
Post (0 to 6) 31.3% 4.4%
% of time gastric pH>3 - Pre (-0.5 to 0) 1.7% 2.4%
Post (0 to 6) 37.6% 5.3%
No statistically significant treatment group differences were observed for any of the
pharmacodynamic parameters during the pretreatment period. The Zantac 75 treatment
group had numerically lower values than the placebo group for the pretreatment
pharmacodynamic parameters area under the H+ time curve from -0.5 to 0 hours,
percentage of pretreatment time pH>4, and percentage of pretreatment time pH>3. The
Zantac 75 group had a numerically higher value of pretreatment median pH than the
placebo group.
Statistically significant differences between the Zantac75 and placebo treatment groups
were observed for all of the pharmacodynamic parameters from 0-6 hours. The mean
area under the curve for H+ was significantly lower for Zantac 75 subjects (227.42 vs.
555.11, p<0.001); the median pH was significantly greater for Zantac 75 subjects (2.861
vs. 1.247, p=0.014). The Zantac 75 treatment group had larger mean values for the
following post-treatment pharmacodynamic parameters: median pH, percentage of time
pH>4, and percentage of time pH>3. The p-values for the hypothesis tests of equality of
10
means with respect to each post-treatment pharmacodynamic parameter were all less
than 0.015.
In the planned analysis of the pharmacodynamic parameters, the two treatment groups
were compared using- a two-sample t-test. This methodology assumes the distribution
was normal and the variance was the same in both treatment groups. However, the
results of the planned analysis indicated that these assumptions may not have been
valid. Therefore a post-hoc analysis of each pharmacodynamic parameter using a non-
parametric test was performed. For all pharmacodynamic parameters, the analysis
results and conclusions of the planned two-sample t-test are confirmed using a non-
parametric test.
Extent of Exposure
Each subject received a single dose of either Zantac 75 (N=19) or placebo (N=10).
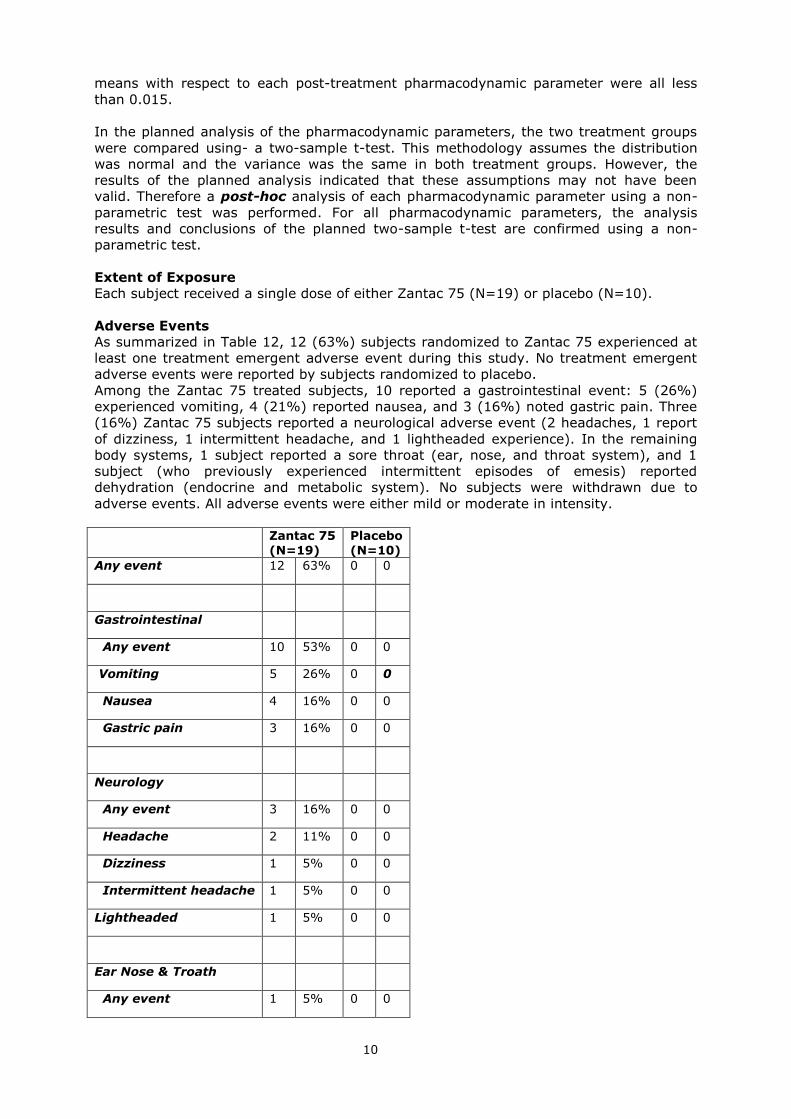
Adverse Events
As summarized in Table 12, 12 (63%) subjects randomized to Zantac 75 experienced at
least one treatment emergent adverse event during this study. No treatment emergent
adverse events were reported by subjects randomized to placebo.
Among the Zantac 75 treated subjects, 10 reported a gastrointestinal event: 5 (26%)
experienced vomiting, 4 (21%) reported nausea, and 3 (16%) noted gastric pain. Three
(16%) Zantac 75 subjects reported a neurological adverse event (2 headaches, 1 report
of dizziness, 1 intermittent headache, and 1 lightheaded experience). In the remaining
body systems, 1 subject reported a sore throat (ear, nose, and throat system), and 1
subject (who previously experienced intermittent episodes of emesis) reported
dehydration (endocrine and metabolic system). No subjects were withdrawn due to
adverse events. All adverse events were either mild or moderate in intensity.
Zantac 75
(N=19)
Placebo
(N=10)
Any event 12 63% 0 0
Gastrointestinal
Any event 10 53% 0 0
Vomiting 5 26% 0 0
Nausea 4 16% 0 0
Gastric pain 3 16% 0 0
Neurology
Any event 3 16% 0 0
Headache 2 11% 0 0
Dizziness 1 5% 0 0
Intermittent headache 1 5% 0 0
Lightheaded 1 5% 0 0
Ear Nose & Troath
Any event 1 5% 0 0

11
Nasal discomfort 1 5% 0 0
Endocrine & metabolic
Any event 1 5% 0 0
Dehydration 1 5% 0 0
Deaths, Serious Adverse Events, and Other Significant Adverse Events
There were no deaths, serious adverse events, or pregnancies reported in this study.
Rapporteur’s comments
No serious adverse events or deaths were reported during the conduct of this study.
Twelve (63%) subjects randomized to Zantac 75 experienced at least one treatment
emergent adverse event during this study. No treatment emergent adverse events were
reported by subjects randomized to placebo. The frequency of these events is
comparable to those seen in prescription ranitidine clinical trails, with the exception of
vomiting which is increased. No new adverse events were noted that were not already
high lighted the prescription and non-prescription adult clinical trails and spontaneous
reporting with ranitidine over the last 15 years. Therefore, these results do not raise any
safety concerns about the use of Zantac 75 in this population.
II.3.1 Pharmacokinetics
For pharmacokinetics of ranitidine in paediatric patients reference has been made to
published data and four studies investigating the pharmacokinetics of ranitidine in
paediatric patients were included in Module 5 of this submission:
Pharmacokinetics of ranitidine syrup in children. Report No GGL/91/005. Protocol
No 69-RAN-1149.
The pharmacokinetics and pharmacodynamics of intravenous ranitidine (1mg/kg)
in children in intensive care. Report No GGA/87/002. Protocol No. RAN-69-1149
(Rylance et al. 1987).
A pharmacokinetic and pharmacodynamic study of intravenous ranitidine in
neonates. Report No RC1998/00030/00. Published as Wells et al. Br J Clin
Pharmacol 1998; 38: 402-407.
A double-blind, placebo-controlled, pharmacokinetic, pharmacodynamic evaluation
of ranitidine 75 mg tablets in four through eleven year old subjects with suspected
abnormal acid reflux. Report No RC1998/00023/00. Protocol No RAN20006.
Published information regarding average pharmacokinetic values for ranitidine in children
with peptic ulcer disease are similar to those for adults when corrections for body weight
are made (Blumer et al, 1985; Leeder et al, 1986). Pharmacokinetic values for
ranitidine following either oral or intravenous administration are similar for an individual
child (Blumer et al, 1985). The bioavailability of ranitidine given orally averaged 48%
(Blumer et al, 1985). The pharmacokinetic parameters following intravenous and oral
administration are summarised in Table 1.
Table 1: Pharmacokinetic parameters following administration of Zantac in paediatric Patients.
Author / protocol
Population Age
N
Dose (mg/kg
body weight)
Admin (IV or O)
T1/2 (h)
Mean
±SD
Vd (L/kg) Mean
±SD
Cl /F (ml/(min*kg))
Mean ±SD
Blumer et al
3.5-16y 11 iv: 0.13-
0.80 1.8±0.3 2.3±0.9 22 ± 8#
1985 3.5-16y 12 po (tablet): dose ≥ 90%
2.0±0.5 2.5±1.0 22 ± 8#

12
inh gastric
output
Leeder et al
<6y 6 iv: 1.25 or
2.5 2.2±2.1 1.3±0.8 11 ±7
1986 6-11.9 y >12 y
11 6
iv: 1.25 or 2.5
iv: 1.25 or 2.5
2.1±1.0 1.7±0.5
1.1±0.5 1.0±0.3
9 ± 3 10 ± 3
Adults 6 iv: 2.5 1.9±0.3 1.0±0.1 8.8 ± 0.7
Fontana et al. 1993
Neonate 1d 27 iv: 2.4 3.5 1.5 ± 0.9
5.0 ± 0.5
RAN-69-1149
1 day- 1 m 1.5 m- 12 y
2 15
iv: 1
4.2 ±
0.7 2.1 ± 0.6
1.0 ±
0.1 2.4 ± 1.2
2.7 ± 0.6 13 ± 5
69-RAN-
1149 0.5-14y 10
po (syrup):
2
2.7 ±
0.5 27 ± 10
Wells et al,
Term neonates
13 iv: 2 6.6 ± 2.8
1.8 ± 0.6
4.1 ± 2.4
1998 1-29 d ECMO
RAN20006 4-11y 19 po 75 mg
(median 2.5
mg/kg)
2.1 ± 0.7
4.9 ± 3.7
25 ± 10
Key: T½ = half life, Vd=volume of distribution, CL= plasma clearance of ranitidine, ECMO= extracorporeal membrane oxygenation. # Cl in ml/min/kg were estimated by assessor from 794 and 788 ml/min/1.73m2 (Blumer et al. 1985) using the individual body weight of the children.
The pharmacokinetics of ranitidine in the four studies included in this submission are
comparable to the previous published data. Following oral administrion as syrup or
tablets only limited data (N=4) are available in children <3 years of age but
pharmacokinetics were in line with that of the older children. In comparison with infants
and children, the neonate may have substantially reduced renal and plasma clearance of
ranitidine (Fontana et al, 1993, Wells et al, 1998, Rylance et al. 1987). In neonates
undergoing ECMO, total clearance was related to estimated glomerular filtration rate (see
Figure below).
0
1
2
3
4
5
6
7
8
9
0 10 20 30 40 50 60 70
estimated GFR (ml/min/1.7m2)
Cl (m
l/(m
in*k
g))
Figure 1. Ranitidine clearance as function of glomerular filtration rate
(calculated according to Schwarz) in neonates undergoing ECMO (Wells et al,
1998).

13
In conclusion, pharmacokinetics of ranitidine following either oral or intravenous
administration are similar for an individual child and pharmacokinetics are comparable in
paediatric and adult patients when corrections for body weight are made. In neonates the
clearance is substantially lower and due to the lower GFR in neonates the dose interval
may need to be lengthened.
II.3.3 Pharmacodynamics and Efficacy
Six controlled pharmacodynamic and/or clinical studies of use of ranitidine oral and
intravenous formulation in children are included in Module 5 of this submission:
An investigation to compare the safety and efficacy of ranitidine 150mg nocte with
placebo in the prevention of symptomatic duodenal ulcer relapse in paediatric
patients. Report No GGL/95/006. Protocol No RAN M15.
Evaluation of the efficacy and pharmacokinetics of ranitidine in paediatric ulcer
disease. Protocol No RAN I-145. No study report - published as Blumer et al 1985
Evaluation of the efficacy and pharmacokinetics of ranitidine in paediatric ulcer
disease. Protocol No RAN I-145A. Study stopped prematurely.
A double-blind, randomized trial of ranitidine therapy in patients with cystic
fibrosis and pancreatic insufficiency. Report No UCD/95/013. Protocol No RAN-
147.
A comparison of continuous intravenous infusion and bolus injections of ranitidine
in critically ill paediatric patients for inhibition of gastric acid production. Report
No UCD/95/019. Protocol No RAN-7001.
A double-blind, placebo-controlled, pharmacokinetic, pharmacodynamic evaluation
of ranitidine in four through eleven year old subjects with suspected abnormal
acid reflux. Report No RC1998/00023/00. Protocol No RAN20006
In addition to the studies conducted by the MAH, published literature on therapeutic use
of ranitidine in the clinical management of paediatric patients, ranging from neonates to
adolescents is submitted. These publications are referred to in the supplementary
paragraph.
II.3.4 Efficacy data
There were no company- sponsored clinical efficacy studies for the following proposed
indications: ‘the treatment of gastro-oesophageal reflux, (including reflux oesophagitis
and the symptom relief of gastro-oesophageal reflux disease) and the prophylaxis of
stress ulceration in seriously ill patients for the injection formulation’.
For the proposed indication of short and long term treatment of peptic ulcer, the
following trials were undertaken:
II.3.4.1 Study 145 and 145A
Both of these open label trials provided supportive data for the use of ranitidine for the
short term treatment of peptic ulcer, which is already indicated for the oral formulations.
Study 145 was an open-label single centre study (conducted in the US) of 12 patients,
aged 3.5-16 years, with endoscopically diagnosed duodenal and/or gastric ulcers
associated with epigastric pain and/or vomiting and melaena. After an initial treatment
with intravenous therapy, patients received oral therapy 12 hourly for 6 weeks. Ulcers
were healed in all cases at 6 weeks. In study 145A, 3 children received oral therapy for 6
weeks with ranitidine syrup, after a similar initial phase to study 145. Ulcers healed in 2
out of 3 cases.
Studies RAN 147 and 701 were also small studies that did not provide any useful data for
the proposed indications.
II.3.4.2 Study RAN M15.
This double-blind, placebo controlled trial, undertaken in 194 children aged 8 to 16
(mean 13 years) with duodenal ulcer compared the efficacy of ranitidine 150mg at night
with placebo, in the prevention of duodenal ulcer over a 12 month treatment period. The
cumulative ulcer relapse at 12 months was only 30 % in those receiving placebo

14
compared to 9% for ranitidine (p<0.001). Relapse rates of 70 to 80% have been
reported for adult populations, suggesting that the natural history of duodenal ulcer
disease in this population differed from that in the adult population. It is also of note that
few patients suffered a symptomatic relapse – six in the placebo group and two in the
ranitidine group.
Although the risk of relapse was reduced with maintenance ranitidine therapy, the
incidence of symptomatic relapse was low in both groups. In addition, H.pylori status was
not considered; present management of peptic ulceration would include this. In
summary, these data do not provide robust evidence for the indication of ‘long term’
treatment of peptic ulceration in children aged 1 month and above.
Issue raised
With regard to the proposed therapeutic indication ‘prophylaxis of stress ulceration in
seriously ill children’, The MAH was asked to provide further information on whether or
not there is evidence that the prophylaxis of stress ulceration in seriously ill children with
ranitidine:
- is associated with a decrease in gastric bleeding,
- had a better overall outcome,
- did not result in an increase in infections/complications compared to those who did
not undergo prophylaxis with ranitidine.

15
Response of the MAH to the issue
In response the MAH stated that analysis of the literature has revealed no additional
studies conducted with ranitidine for the prophylaxis of stress ulceration further to those
submitted previously. The MHRA, in their review of the data package in consultation with
expert advice from the Commission on Human Medicines, found that the use of ranitidine
was well established in this indication (the scientific justification for this position is not
available for assessment). Additional confirmation regarding the use of ranitidine in this
indication was provided in a clinical expert statement which discusses current clinical
practice for the treatment of the prophylaxis of stress ulceration in a paediatric intensive
care unit at Addenbrooke’s hospital in the UK. GSK believe that the available studies and
literature show that ranitidine is used for the prophylaxis of stress ulceration in the
paediatric population and thus the SPC should reflect this with appropriate information
for the prescriber. As discussed the dosing recommendation proposed in the SPC are in
line with the guidance in the British National Formulary for Children (BNFc) and is
supported by the literature, where doses of up to 6 mg/kg/day have been used.
Previously the MAH submitted literature discussing the prophylaxis of stress ulceration in
critically ill children. Ranitidine administered either as an intermittent intravenous infusion
(2-6mg/kg/day in divided doses) (Harrison et al, 1998; Kuusela et al, 1997; Kuusela,
1998; Lopez-Herce et al 1988; Osteyee et al 1994; Rylance 1987; Santucci et al,
1991) or as a continuous infusion (0.1-0.2mg/kg/hr) (Osteyee et al, 1994; Santucci et
al, 1991; Dimand et al 1989; Eddleston et al, 1989) has been successfully used to
maintain gastric pH levels above 4.0. Both dosing regimens were effective in increasing
and maintaining gastric pH above 4, however the pH values fluctuate more with the
intermittent regimens (Osteyee et al, 1994; Santucci et al, 1991).
In general this surrogate endpoint (pH >4) is accepted and has shown a reasonable
relation with the clinical outcome of the prevention of gastric and duodenal ulcera. The
relation to the prevention of bleedings (and their complications) remains to be
established. Therefore, it can not be assumed that the depicted effects from literature are
clinical meaningful for the applied ‘prophylaxis of stress ulceration in seriously ill
children’. The MAH was not able to convincingly show that ranitidine is associated with a
decrease in gastric bleeding, had a better overall outcome or did not result in an increase
in infections/complications compared to those who did not undergo prophylaxis with
ranitidine.
II.3.5 Safety
A cumulative review of all serious and non-serious clinical trial and spontaneous adverse
events in children and adolescents aged less than 18 years associated with ranitidine
administration has been provided. A search of the safety database revealed a total of 971
adverse event reports associated with ranitidine administration in patients aged less than
18 years that have been received worldwide by the GSK global safety group since first
launch in 1981 up to 02 August 2004. Review of the most commonly reported events in
cases received up to 02 August 2004 did not highlight any safety issues for paediatric
patients. In addition PSURs covering the time period from June 2001 – May 2006 are also
included.
Isue raised
It was noted that it is difficult to compare severity and frequency of undesirable effects
between adults and children. The MAH was asked to provide comparative data on this
point.
Resolving the issue
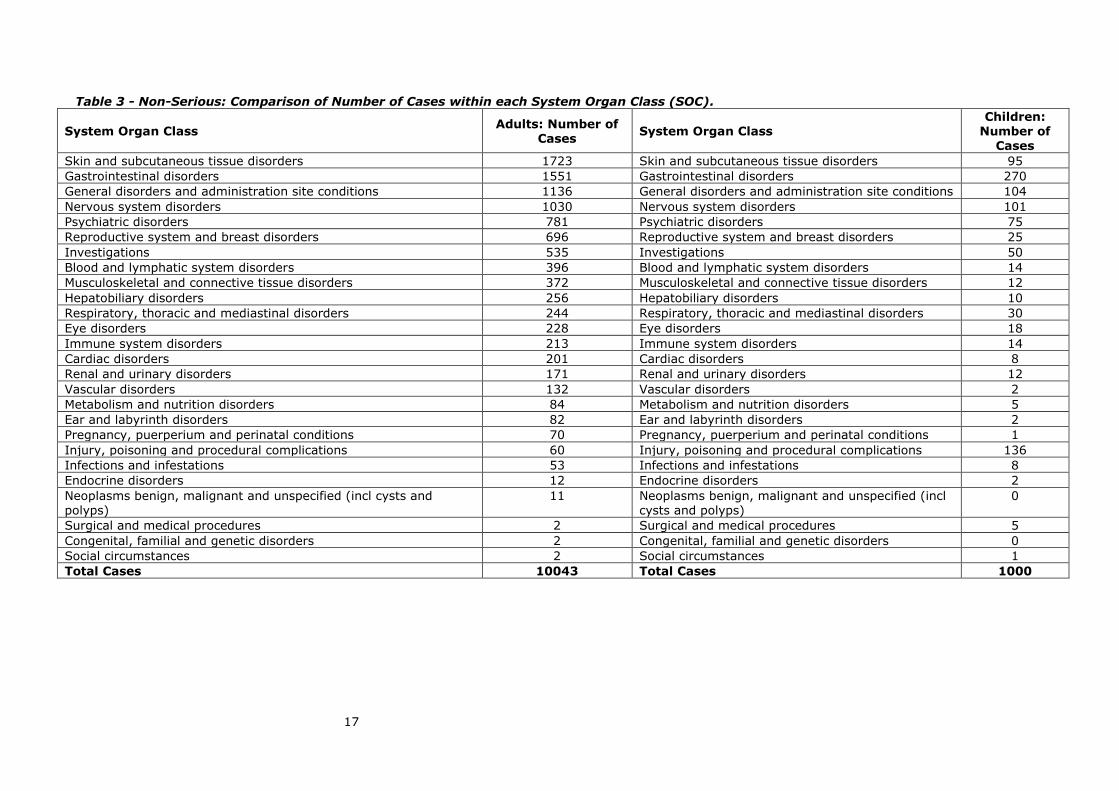
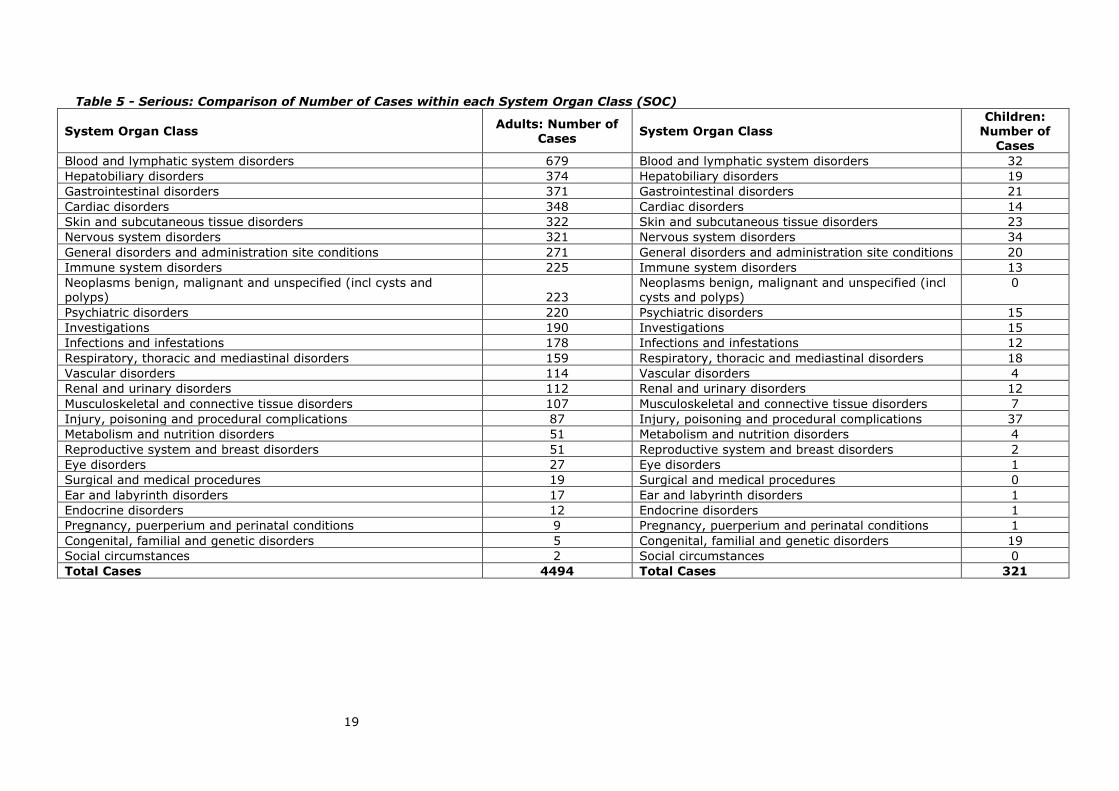
The MAH responded by providing a tabular comparison of the non-serious and serious
AEs in both the adult (greater than 18 years) and the paediatric population (less than 18
years) by system organ class, as well as a comparison of events from a cumulative
summary of events reported for ranitidine. See tables 2-5 below.

Table 2 - Body System Distribution: Comparison Between Adults (age >18 Years) and Children (< 18 Years)Non-serious Cases: System Organ Class (SOC) Comparison Based on the Primary AE.
System Organ Class Adults: Number of
Cases System Organ Class
Children: Number of
Cases
Skin and subcutaneous tissue disorders 1723 Gastrointestinal disorders 270
Gastrointestinal disorders 1551 Injury, poisoning and procedural complications 136
General disorders and administration site conditions 1136 General disorders and administration site conditions 104
Nervous system disorders 1030 Nervous system disorders 101
Psychiatric disorders 781 Skin and subcutaneous tissue disorders 95
Reproductive system and breast disorders 696 Psychiatric disorders 75
Investigations 535 Investigations 50
Blood and lymphatic system disorders 396 Respiratory, thoracic and mediastinal disorders 30
Musculoskeletal and connective tissue disorders 372 Reproductive system and breast disorders 25
Hepatobiliary disorders 256 Eye disorders 18
Respiratory, thoracic and mediastinal disorders 244 Blood and lymphatic system disorders 14
Eye disorders 228 Immune system disorders 14
Immune system disorders 213 Renal and urinary disorders 12
Cardiac disorders 201 Musculoskeletal and connective tissue disorders 12
Renal and urinary disorders 171 Hepatobiliary disorders 10
Vascular disorders 132 Cardiac disorders 8
Metabolism and nutrition disorders 84 Infections and infestations 8
Ear and labyrinth disorders 82 Surgical and medical procedures 5
Pregnancy, puerperium and perinatal conditions 70 Metabolism and nutrition disorders 5
Injury, poisoning and procedural complications 60 Endocrine disorders 2
Infections and infestations 53 Ear and labyrinth disorders 2
Endocrine disorders 12 Vascular disorders 2
Neoplasms benign, malignant and unspecified (incl cysts and polyps)
11 Social circumstances 1
Surgical and medical procedures 2 Pregnancy, puerperium and perinatal conditions 1
Congenital, familial and genetic disorders 2
Social circumstances 2
Total Cases 10043 Total Cases 1000
17
Table 3 - Non-Serious: Comparison of Number of Cases within each System Organ Class (SOC).
System Organ Class Adults: Number of
Cases System Organ Class
Children: Number of
Cases
Skin and subcutaneous tissue disorders 1723 Skin and subcutaneous tissue disorders 95
Gastrointestinal disorders 1551 Gastrointestinal disorders 270
General disorders and administration site conditions 1136 General disorders and administration site conditions 104
Nervous system disorders 1030 Nervous system disorders 101
Psychiatric disorders 781 Psychiatric disorders 75
Reproductive system and breast disorders 696 Reproductive system and breast disorders 25
Investigations 535 Investigations 50
Blood and lymphatic system disorders 396 Blood and lymphatic system disorders 14
Musculoskeletal and connective tissue disorders 372 Musculoskeletal and connective tissue disorders 12
Hepatobiliary disorders 256 Hepatobiliary disorders 10
Respiratory, thoracic and mediastinal disorders 244 Respiratory, thoracic and mediastinal disorders 30
Eye disorders 228 Eye disorders 18
Immune system disorders 213 Immune system disorders 14
Cardiac disorders 201 Cardiac disorders 8
Renal and urinary disorders 171 Renal and urinary disorders 12
Vascular disorders 132 Vascular disorders 2
Metabolism and nutrition disorders 84 Metabolism and nutrition disorders 5
Ear and labyrinth disorders 82 Ear and labyrinth disorders 2
Pregnancy, puerperium and perinatal conditions 70 Pregnancy, puerperium and perinatal conditions 1
Injury, poisoning and procedural complications 60 Injury, poisoning and procedural complications 136
Infections and infestations 53 Infections and infestations 8
Endocrine disorders 12 Endocrine disorders 2
Neoplasms benign, malignant and unspecified (incl cysts and polyps)
11 Neoplasms benign, malignant and unspecified (incl cysts and polyps)
0
Surgical and medical procedures 2 Surgical and medical procedures 5
Congenital, familial and genetic disorders 2 Congenital, familial and genetic disorders 0
Social circumstances 2 Social circumstances 1
Total Cases 10043 Total Cases 1000

18
Table 4 - Serious Cases: System Organ Class (SOC) Comparison Based on the Primary AE.
System Organ Class Adults: Number of
Cases System Organ Class
Children: Number of
Cases
Blood and lymphatic system disorders 679 Injury, poisoning and procedural complications 37
Hepatobiliary disorders 374 Nervous system disorders 34
Gastrointestinal disorders 371 Blood and lymphatic system disorders 32
Cardiac disorders 348 Skin and subcutaneous tissue disorders 23
Skin and subcutaneous tissue disorders 322 Gastrointestinal disorders 21
Nervous system disorders 321 General disorders and administration site conditions 20
General disorders and administration site conditions 271 Hepatobiliary disorders 19
Immune system disorders 225 Congenital, familial and genetic disorders 19
Neoplasms benign, malignant and unspecified (incl cysts and polyps) 223 Respiratory, thoracic and mediastinal disorders 18
Psychiatric disorders 220 Investigations 15
Investigations 190 Psychiatric disorders 15
Infections and infestations 178 Cardiac disorders 14
Respiratory, thoracic and mediastinal disorders 159 Immune system disorders 13
Vascular disorders 114 Infections and infestations 12
Renal and urinary disorders 112 Renal and urinary disorders 8
Musculoskeletal and connective tissue disorders 107 Musculoskeletal and connective tissue disorders 7
Injury, poisoning and procedural complications 87 Vascular disorders 4
Metabolism and nutrition disorders 51 Metabolism and nutrition disorders 4
Reproductive system and breast disorders 51 Reproductive system and breast disorders 2
Eye disorders 27 Eye disorders 1
Surgical and medical procedures 19 Endocrine disorders 1
Ear and labyrinth disorders 17 Pregnancy, puerperium and perinatal conditions 1
Endocrine disorders 12 Ear and labyrinth disorders 1
Pregnancy, puerperium and perinatal conditions 9
Congenital, familial and genetic disorders 5
Social circumstances 2
Total Cases 4494 Total Cases 321
19
Table 5 - Serious: Comparison of Number of Cases within each System Organ Class (SOC)
System Organ Class Adults: Number of
Cases System Organ Class
Children: Number of
Cases
Blood and lymphatic system disorders 679 Blood and lymphatic system disorders 32
Hepatobiliary disorders 374 Hepatobiliary disorders 19
Gastrointestinal disorders 371 Gastrointestinal disorders 21
Cardiac disorders 348 Cardiac disorders 14
Skin and subcutaneous tissue disorders 322 Skin and subcutaneous tissue disorders 23
Nervous system disorders 321 Nervous system disorders 34
General disorders and administration site conditions 271 General disorders and administration site conditions 20
Immune system disorders 225 Immune system disorders 13
Neoplasms benign, malignant and unspecified (incl cysts and polyps) 223
Neoplasms benign, malignant and unspecified (incl cysts and polyps)
0
Psychiatric disorders 220 Psychiatric disorders 15
Investigations 190 Investigations 15
Infections and infestations 178 Infections and infestations 12
Respiratory, thoracic and mediastinal disorders 159 Respiratory, thoracic and mediastinal disorders 18
Vascular disorders 114 Vascular disorders 4
Renal and urinary disorders 112 Renal and urinary disorders 12
Musculoskeletal and connective tissue disorders 107 Musculoskeletal and connective tissue disorders 7
Injury, poisoning and procedural complications 87 Injury, poisoning and procedural complications 37
Metabolism and nutrition disorders 51 Metabolism and nutrition disorders 4
Reproductive system and breast disorders 51 Reproductive system and breast disorders 2
Eye disorders 27 Eye disorders 1
Surgical and medical procedures 19 Surgical and medical procedures 0
Ear and labyrinth disorders 17 Ear and labyrinth disorders 1
Endocrine disorders 12 Endocrine disorders 1
Pregnancy, puerperium and perinatal conditions 9 Pregnancy, puerperium and perinatal conditions 1
Congenital, familial and genetic disorders 5 Congenital, familial and genetic disorders 19
Social circumstances 2 Social circumstances 0
Total Cases 4494 Total Cases 321

A cumulative summary of events for the serious and non-serious cases reported
for adults and children was reviewed. Overall, the events reported were similar
for adults and children.
For the serious cases, irritability was reported more frequently in children than in
adults. However, this would not be unexpected in infants and children with
gastroesophageal reflux disease. Accidental overdose was also reported more
frequently with children; about half of the reports involved an error in the amount
of ranitidine syrup.
For the non-serious cases, retching, tooth discolouration, irritability, crying,
accidental overdose/overdose, and medication errors were reported more
frequently in children compared to adults. Irritability and crying would not be
unexpected in infants and children with gastroesophageal reflux disease. Retching
was reported only with the syrup formulation and many cases reported the event
was due to the taste of the medication.
Ten cases total of tooth discolouration in children were reported to GSK. Three of
these cases involved co-suspect or multiple concurrent medications. One other
case reported the discolouration was removed with cleaning. Three cases did not
provide further details and outcome was unknown. Two other cases reported
events that occurred after a year or more of therapy; outcome was not reported.
The remaining case reported the event occurred after 4 months of therapy; no
action was taken and outcome was unresolved.
The majority of cases reporting overdose/accidental overdose involved a
dispensing error with the syrup. The majority of cases reporting medication
errors involved ranitidine syrup and either an accidental overdose or another
medication dispensed in error instead of ranitidine, mainly cetirizine (Zyrtec).
This issue is considerd resolved. The MAH however could not explain the tooth
discoloration and therefore was asked to add this adverse event to SPC section
4.8.
Patient exposure
Cumulatively, patient exposure to ranitidine tablets is estimated to be
approximately 41.6 billion treatment days.
Adverse events (post-marketing)
Period 1981 up to 02 August 2004
The MAH provided a cumulative review of all serious and non-serious clinical
adverse events in children and adolescents aged less than 18 years associated
with ranitidine administration, since first launch in 1981 up to 02 August 2004.
The cases involving paediatric patients (n=971) represent about 5% of all
ranitidine cases in the MAH’s Safety Database. The majority of the 971 cases were
non-serious spontaneous reports received from medical professionals and
described patients 2 years of age or younger. Appendix 1 shows the most
common MedDRA System Organ Class for the reported adverse events.
Most patients received ranitidine to treat a condition (e.g. gastroesophageal reflux
disease, ulcer) for which some of the reported events (e.g. vomiting, irritability,
abdominal pain, crying, insomnia) could be a symptom. Review of the most
commonly reported events in cases received up to 02 August 2004 did not
highlight any safety issues for paediatric patients.
Period 01 June 2004 to 31 May 2006
Table 6 shows an overview of the adverse reactions in paediatric patients (<18
years) by MedDRA System Organ Class reported in PSURs during period 01 June
2004 to 31 May 2006 for Zantac.

21
Table 6 - Overview of the adverse reactions in paediatric patients (<18 years)
by MedDRA System Organ Class reported in PSURs during period 01 June 2004 to 31 May 2006 for Zantac. System Organ Class Adverse reaction Total
Blood and the lymphatic system disorders
Thrombocytopenia (1) Agranulocytosis (1) Aplastic anaemia (1) Leukopenia (1)
4
Psychiatric disorders Insomnia (2) Suicide attempt (1)
3
Nervous system disorders Psychomotor hyperactivity (1) Tardive dyskinesia (1) Tremor (3) Convulsion (1) Dysgeusia (3) Hyper somnia (1) Somnolence (2)
12
Eye disorders Eye disorder (1) 1
Vascular disorders Flushing (1) 1
Respiratory, thoracic and mediastinal disorders
Choking (1) Apnoea (2)
Epistaxis (1)
4
Gastrointestinal disorders Vomiting (8) Haematochezia (1) Dysphagia (1) Consipation (1)
Abdominal pain (1) Colitis ulcerative (1) Faeces discoloured (2) Oral discomfort (1) Stomach discomfort (1)
17
Hepato-biliary disorders Hepatitis (1) 1
Skin and subcutaneous tissue disorders Rash (3) Alopecia (2) Photosensitivity reaction (1)
6
Renal and urinary disorders Urine odour abnormal (2) Tubulointerstitial nephritis (2)
4
Reproductive system and breast disorders
Hypertrophy breast (1) Gynaecomastia (1)
2
Congenital and familial/genetic disorders Epidermolysis bullosa (1) Ventricular septal defect (3) Cleft palate (1) Syndactyly (1) Talipes (1)
7
General disorders and administration site conditions
Drug ineffective (2) Feeling jittery (1) Condition aggravated (1) Chills (1) Irritability (1) Malaise (1) Pyrexia (1)
8
Investigations Increased Blood Amylase (1) 1
Injury and poisoning Overdose (18) Medication error (8) Incorrect dose (2)
26
Total: 97
Several remarks were made:
- The periods covered by the cumulative overview and the PSURs show a time
overlap of several months.
- A complete overview of the adverse reactions, subdivided in serious and
nonserious, in children and adolescents aged less than 18 years associated
with ranitidine administration, since 03 August 2004 to 31 May 2006 is lacking.
- The cases in the PSURs reporting adverse events were not restricted to
paediatric patients only
This seriously hampered assessment of the cumulative reported adverse reactions
in the paediatric population. However, neither the review of the paediatric cases in
the period from 1 June 2004 to 31 May 2006, nor the cumulative review of

22
paediatric case report up to August 2004 did highlighted any safety issues.
Therefore the above mentioned shortcommings were considered acceptable.
Pregnancy
Cumulative, a total of 280 reports (258 spontaneous, 22 clinical trial). Forty-three
of the 280 reports involved patients given ranitidine for labour or caesarean
section. Outcomes of pregnancies in the remaining 237 cases in which ranitidine
was administered during pregnancy for other indications are summarised below.
Outcome Total Number
Normal infant 76
Spontaneous abortion/miscarriage 6
Elective termination 6
Stillbirth 2
Abnormal infant 23
Pregnancy ongoing/unknown 124
Total 237
Issue raised
The MAH was requested to specify the category ‘Pregnancy ongoing/unknown’ in
‘Pregnancy ongoing’ and ‘Pregnancy unknown’. In addition, an explanation was
asked as to why no follow-up has been received for pregnancy cases in category
‘unknown’.
Resolving the issue
The MAH responded by stating that ‘Pregnancy Ongoing’ and ‘Pregnancy
Unknown’, which are coded in the safety database at the time of the initial report,
are assumed to be both unknown since GSK have not received any follow-up
information on the outcome. Therefore they are placed in the same category.
GSK is diligent in following up on all case reports of pregnancy, however, due to
the nature of spontaneous reporting receipt of follow-up information cannot be
guaranteed.
The issue is considered resolved.
Long-term safety data; effect on development (growth, motor, mentally, sexually)
and cognition
In study RAN M15 (duration of 12 months), there were minor haematological
abnormalities detected in 89% of patients treated with ranitidine. In addition,
15% of patients had minor elevations of serum alkaline phosphatase levels. No
other long-term data (in particular, longitudinal growth measurements) were
available from this study.
III OVERALL CONCLUSION There is some clinical evidence in the published literature to support the use of
Zantac in paediatric practice. Limited data exist concerning the use of ranitidine in
children for indications other than peptic ulcer. This includes studies in
gastroesophageal reflux disease and prophylaxis of stress ulceration and upper
gastrointestinal bleeding.
Literature strongly suggests that oral ranitidine therapy is effective in the
treatment of gastro-oesophageal reflux disease and peptic ulceration in children.
Submitted peadiatric data considering the intravenous ranitidine therapy showed
conflicting results in the prevention of bleeding from stress ulcers in children,
therefore no firm conclusions can be drawn. Efficacy in the prevention of bleeding
remains to be demonstrated.

23
Studies have confirmed the pharmacokinetics and pharmacodynamics of ranitidine
in both oral and intravenous regimens. Pharmacokinetics of ranitidine following
either oral or intravenous administration are similar for an individual child and
pharmacokinetics are comparable in paediatric and adult patients when
corrections for body weight are made. In neonates the clearance is substantially
lower and was related to the lower glomerular filtration rate encountered in these
patients.
From the clinical trial data and spontaneous reports, ranitidine appears to be well
tolerated in the short term treatment, with an adverse effect profile similar to that
in adults. The limited long term safety data from study RAN M15 (duration of 12
months) did not reveal unexpected safety issues.
The ethanol content of ranitidine syrup is high (7.5%). The clinical implications of
this are not known but the use of ethanol in formulations for paediatric patients is
not recommendable. Further the fixed oral dose of 150 mg limits the
administration to children above 30 kg. This is reflected in the SmPC.
The limited literature suggests some efficacy concerning the use of ranitidine in
children for indications peptic ulcer, gastroesophageal reflux disease and upper
gastrointestinal bleeding. While no unexpected safety issues were seen, the
proposed indications have been approved.
24
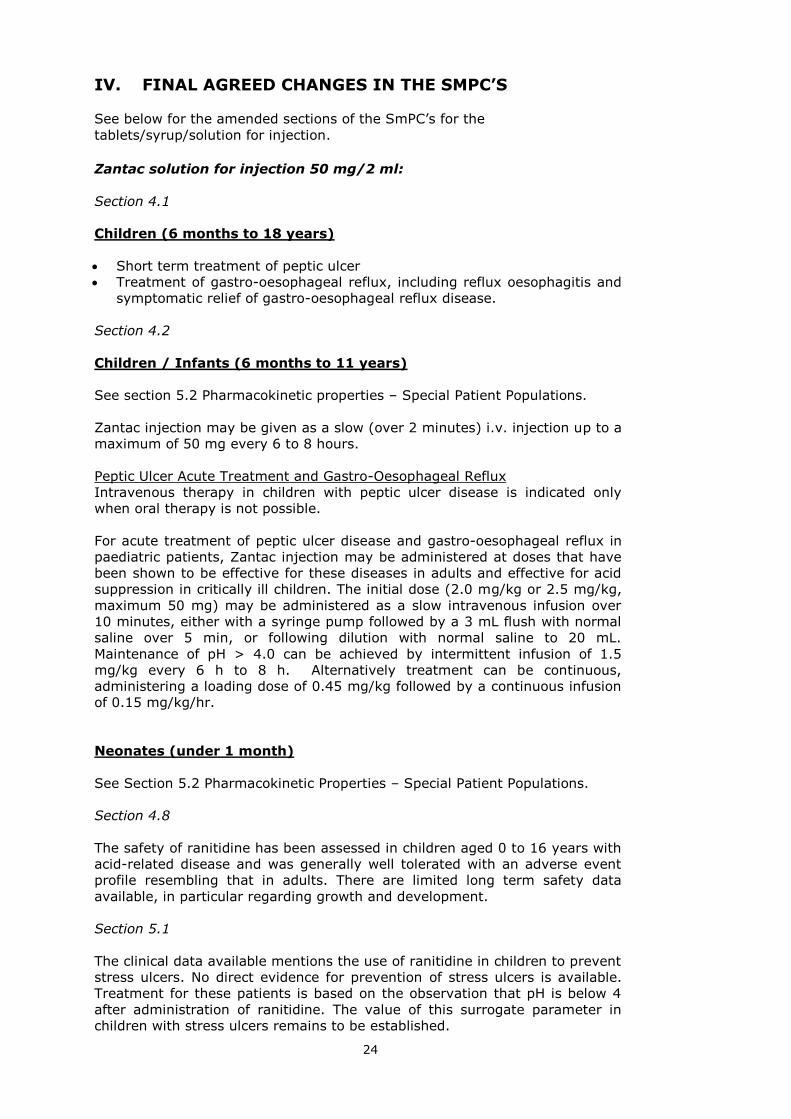
IV. FINAL AGREED CHANGES IN THE SMPC’S
See below for the amended sections of the SmPC’s for the
tablets/syrup/solution for injection.
Zantac solution for injection 50 mg/2 ml:
Section 4.1
Children (6 months to 18 years)
Short term treatment of peptic ulcer
Treatment of gastro-oesophageal reflux, including reflux oesophagitis and
symptomatic relief of gastro-oesophageal reflux disease.
Section 4.2
Children / Infants (6 months to 11 years)
See section 5.2 Pharmacokinetic properties – Special Patient Populations.
Zantac injection may be given as a slow (over 2 minutes) i.v. injection up to a
maximum of 50 mg every 6 to 8 hours.
Peptic Ulcer Acute Treatment and Gastro-Oesophageal Reflux
Intravenous therapy in children with peptic ulcer disease is indicated only
when oral therapy is not possible.
For acute treatment of peptic ulcer disease and gastro-oesophageal reflux in
paediatric patients, Zantac injection may be administered at doses that have
been shown to be effective for these diseases in adults and effective for acid
suppression in critically ill children. The initial dose (2.0 mg/kg or 2.5 mg/kg,
maximum 50 mg) may be administered as a slow intravenous infusion over
10 minutes, either with a syringe pump followed by a 3 mL flush with normal
saline over 5 min, or following dilution with normal saline to 20 mL.
Maintenance of pH > 4.0 can be achieved by intermittent infusion of 1.5
mg/kg every 6 h to 8 h. Alternatively treatment can be continuous,
administering a loading dose of 0.45 mg/kg followed by a continuous infusion
of 0.15 mg/kg/hr.
Neonates (under 1 month)
See Section 5.2 Pharmacokinetic Properties – Special Patient Populations.
Section 4.8
The safety of ranitidine has been assessed in children aged 0 to 16 years with
acid-related disease and was generally well tolerated with an adverse event
profile resembling that in adults. There are limited long term safety data
available, in particular regarding growth and development.
Section 5.1
The clinical data available mentions the use of ranitidine in children to prevent
stress ulcers. No direct evidence for prevention of stress ulcers is available.
Treatment for these patients is based on the observation that pH is below 4
after administration of ranitidine. The value of this surrogate parameter in
children with stress ulcers remains to be established.
25
Section 5.2
Special Patient Populations
Children/infants (6 months and above)
Limited pharmacokinetic data show that there were no significant differences
in half-life (range for children 3 years and above: 1.7 - 2.2 h) and plasma
clearance (range for children 3 years and above: 9 - 22 ml/min/kg) between
children and healthy adults receiving intravenous ranitidine when correction is
made for body weight. Pharmacokinetic data in infants is extremely limited
but appears to be in line with that for older children.
Neonates (under 1 month)
Limited pharmacokinetic data from term babies undergoing treatment with
Extracorporeal Membrane Oxygenation (EMCO) suggests that plasma
clearance following iv administration may be reduced (1.5-8.2 ml/min/kg) and
the half-life increased in the new-born. Clearance of ranitidine appeared to be
related to the estimated glomerular filtration rate in the neonates.
Zantac Tablets 150 & 300mg; Effervescent tablets 150 & 300mg:
Section 4.1
Children (3 to 18 years)
Short term treatment of peptic ulcer.
Treatment of gastro-oesophageal reflux, including reflux oesophagitis and
symptomatic relief of gastro-oesophageal reflux disease.
Section 4.2
Children 12 years and over For children 12 years and over the adult dosage is given.
Children from 3 to 11 years and over 30 kg of weight
See section 5.2 Pharmacokinetic properties – Special Patient Populations.
Peptic Ulcer Acute Treatment
The recommended oral dose for the treatment of peptic ulcer in children is 4
mg/kg/day to 8 mg/kg/day administered as two divided doses to a maximum
of 300mg ranitidine per day for a duration of 4 weeks. For those patients with
incomplete healing, another 4 weeks of therapy is indicated, as healing
usually occurs after eight weeks of treatment.
Gastro-Oesophageal Reflux
The recommended oral dose for the treatment of gastro-oesophageal reflux in
children is 5 mg/kg/day to 10 mg/kg/day administered as two divided doses
in a maximum dose of 600mg (the maximum dose is likely to apply to heavier
children or adolescents with severe symptoms).
Neonates
Safety and efficacy in new-born patients has not been established.
Section 4.8
The safety of ranitidine has been assessed in children aged 0 to 16 years with
acid-related disease and was generally well tolerated with an adverse event
26
profile resembling that in adults. There are limited long term safety data
available, in particular regarding growth and development.
Section 5.2
Special Patient Populations
Children (3 years and above)
Limited pharmacokinetic data have shown that there are no significant
differences in half-life (range for children 3 years and above: 1.7 - 2.2 h) and
plasma clearance (range for children 3 years and above: 9 - 22 ml/min/kg)
between children and healthy adults receiving oral ranitidine when correction
is made for body weight.
Zantac syrup:
Section 4.1
Children (3 to 18 years)
Short term treatment of peptic ulcer
Treatment of gastro-oesophageal reflux, including reflux oesophagitis and
symptomatic relief of gastro-oesophageal reflux disease.
See section 4.4 Special warnings and precautions for use.
Section 4.2
Children 12 years and over
For children 12 years and over the adult dosage is given.
Children (3 to 11 years)
See section 5.2 Pharmacokinetic properties – Special Patient Populations.
Zantac syrup contains approximately 7.5%w/v ethanol. Therefore an
alternative formulation of ranitidine may be considered necessary for at-risk
groups, including children (see section 4.4 Special warnings and precautions
for use).
Peptic Ulcer Acute Treatment
The recommended oral dose for the treatment of peptic ulcer in children is 4
mg/kg/day to 8 mg/kg/day administered as two divided doses to a maximum
of 300mg ranitidine per day for a duration of 4 weeks. For those patients with
incomplete healing, another 4 weeks of therapy is indicated, as healing
usually occurs after eight weeks of treatment.
Gastro-Oesophageal Reflux
The recommended oral dose for the treatment of gastro-oesophageal reflux in
children is 5 mg/kg/day to 10 mg/kg/day administered as two divided doses
in a maximum dose of 600mg (the maximum dose is likely to apply to heavier
children or adolescents with severe symptoms).
Neonates
Safety and efficacy in new-born patients has not been established.
Section 4.4
Zantac syrup contains approximately 7.5%w/v ethanol (alcohol), i.e. up to
405 mg per 5ml spoonful which is equivalent to about 11ml of beer or 5ml of

27
wine. It is harmful for those suffering from alcoholism. It should be taken
into account in pregnant or lactating women, high risk groups (those suffering
from alcoholism, liver disease, epilepsy, brain injury or disease) and children
(see section 4.2). It may modify or increase the effect of other medicines.
Section 4.8
The safety of ranitidine has been assessed in children aged 0 to 16 years with
acid-related disease and was generally well tolerated with an adverse event
profile resembling that in adults. There are limited long term safety data
available, in particular regarding growth and development.
Section 5.2
Special Patient Populations
Children (3 years and above)
Limited pharmacokinetic data have shown that there are no significant
differences in half-life (range for children 3 years and above: 1.7 - 2.2 h) and
plasma clearance (range for children 3 years and above: 9 - 22 ml/min/kg)
between children and healthy adults receiving oral ranitidine when correction
is made for body weight.
28
ANNEX I: THE MHRA REPORT ON ZANTAC TABLETS,
ZANTAC EFFERVESCENT TABLETS, 300MG, 150MG,
ZANTAC INJECTION 50MG/2ML, ZANTAC SYRUP 75MG/5ML
ASSESSMENT REPORT MA NUMBER: PLs 10949/0042, 10949/0137-8, 10949/0108-9
PRODUCT NAME: Zantac tablets, Zantac effervescent tablets 300mg,150mg Zantac injection 50mg/2ml Zantac syrup 75mg/5ml
LICENCE HOLDER: Glaxo SmithKline UK Ltd
THERAPEUTIC CLASSIFICATION: Histamine 2 –receptor antagonist
MEETING: COMMISSION ON HUMAN
MEDICINES- 14 December 2005
ACTIVE INGREDIENT Ranitidine
LEGAL STATUS: POM
A national variation application to include paediatric indications for the long
term management of peptic ulcer and the treatment of gastro-oesophageal
reflux (including reflux oesophagitis and gastro-oesophageal reflux disease)
from 1 month of age and above. In addition, for the injection formulation the
MAH has applied for the following indications from 1 month onwards: the
short term treatment of peptic ulcer and the prevention of stress ulcers in
seriously ill children.
EXECUTIVE SUMMARY This is a national variation application for ranitidine tablets, injection and
syrup. Discussion and CHM Advice (page 29)
The Commission considered that the use of ranitidine was well
established, particularly for the treatment of gastro-oesophageal reflux
and the prevention of stress ulcers in seriously ill children and that there
were no safety issues associated with its use in children. However, the
Commission noted that there were insufficient data regarding dosage to
warrant extrapolation from adults for prevention of stress ulcers. The
Commission considered that there were sufficient published data to grant
the indication for the treatment of gastro-oesophageal reflux.
The submitted data for the indication for the long term treatment of peptic
ulcer were considered to be poor and this condition is uncommon in
children. In addition, current practice for the treatment of peptic ulceration
does not generally include the use of H2 antagonists for long periods. The
Commission therefore advised that this indication should be refused.
The Commission advised that the MAH should be not use ethanol in
paediatric formulations unless this was necessary.
1. INTRODUCTION This is a national variation application for ranitidine (tablets, injection and
syrup) that includes several changes to the current licence with respect to its
use in children. These data were requested by the MHRA following changes to
the US licence as a result of the paediatric exclusivity provision. The MHRA
contacted companies whose products appear on the FDA Paediatric exclusivity
granted list1. This is a list of active substances (with relevant sponsors) for
which the FDA has granted data exclusivity in return for the submission of
paediatric studies carried out in compliance with an FDA written request. The

29
MAH have submitted these data to support an application for a licence
variation.
The current granted US paediatric indications for ranitidine are: the treatment
of duodenal and gastric ulcers, gastro-oesophageal reflux disease and erosive
oesophagitis, and the maintenance of healed duodenal and gastric ulcers. The
US labelling also includes details regarding the pharmacokinetic studies.
The applicant proposes to broaden the present paediatric indication of the oral
formulations for the treatment of peptic ulcer (age unspecified), to include
indications for the long term management of peptic ulcer and the treatment of
gastro-oesophageal reflux (including reflux oesophagitis and gastro-
oesophageal reflux disease) in children aged 1 month and above. In addition
to the above, there is a further indication for the injection formulation that is
not included in the US label: the prevention of stress ulcers in seriously ill
children, from 1 month of age and above.
2. LICENSING HISTORY Ranitidine, an H2 receptor antagonist, which was first authorised in 1981, is
an established drug substance in 98 markets worldwide including the USA,
Japan and all Member States (MS) of the EU. In the UK, prescription only
licences (POM) include tablets, effervescent tablets and syrup formulations. In
addition, there are Pharmacy (P) and General Sales (GSL) licences for the
75mg tablet for the short-term symptomatic relief of heartburn, dyspepsia
and hyperacidity and for the prevention of these symptoms in adults. The
current variations apply to the POM licences only.
Ranitidine is licensed in the UK for use in adults for gastro-oesophageal reflux
disease (GORD), the treatment of duodenal ulcer, gastric ulcer, NSAID
associated ulcer, post-operative ulcer, duodenal ulcer associated with
Helicobacter pylori (in combination with appropriate antibiotics), relief of
chronic-episodic dyspepsia, and the long term management of Zollinger-
Ellison syndrome. Ranitidine is also authorised in the UK in adults for the
prophylaxis of gastro-intestinal haemorrhage from stress ulcer, recurrent
haemorrhage in patients with bleeding peptic ulcer and Mendelson’s
syndrome.
In children (age limits unspecified), ranitidine oral formulations are currently
licensed for the treatment of peptic ulcer at a dose of 2mg/kg to 4 mg/kg
twice daily to a maximum of 300mg/day. The injection formulation is
currently not licensed in children for any indication.
1 http://www.fda.gov./cder/pediatric/exgrant.htm
Ranitidine underwent an Article 30 referral procedure in 2002, the purpose of
which was to harmonise the SmPC throughout Member States. However, the
referral was withdrawn in 2003, due to procedural difficulties. However, one
of the outstanding issues was the extremely high alcohol content of the syrup
formulation. At this time, GSK agreed to the proposal to add a precautionary
statement in the SmPC regarding this.
3. BACKGROUND
Gastro-oesophageal Reflux Disease Gastro-oesophageal Reflux (GOR) is an extremely common and usually self-
limiting condition, affecting 20 – 67% of infants. GOR is the passage of gastric
contents into the oesophagus. It occurs as the result of transient,
inappropriate relaxation of the lower oesophageal sphincter, permitting the
stomach contents to pass into the oesophagus. In most infants with GOR the
outcome is benign and self- limiting. The peak incidence of GOR is around 4
months and it resolves spontaneously by 1 to 2 years of age in most patients.
There may be parental anxiety or intolerance of symptoms which lead to
medical advice being sought. This form of GOR is best managed with
reassurance and on-going clinical monitoring.

30
In a minority of cases gastro-oesophageal reflux is complicated by
oesophagitis, respiratory symptoms, neuro-behavioural symptoms or failure
to thrive and is then referred to as gastro-oesophageal reflux disease
(GORD). Many of these children have underlying conditions, such as cerebral
palsy, cystic fibrosis and congenital abnormalities. Treatment is medically
indicated in such cases, which represent a small percentage of cases with
GOR.
Omeprazole is currently the only authorised treatment for GORD and is
currently restricted to the indication of severe ulcerating oesophagitis, in
children aged 1 year and above. Other drug options include the use of
domperidone and metoclopramide, which are used in less severe cases of
GORD, and ranitidine. None of these drugs are authorised for use in GOR and
GORD.
In 2004, the US data for omeprazole was assessed; the CSM advised against
an indication for ‘acid- related disorders (including non-ulcerating GORD) and
the treatment of Helicobacter pylori. (See assessment report at mhra.gov.uk.)
Peptic Ulcer Disease
The term “peptic ulcer disease” (PUD) refers to a defect in the gastrointestinal
mucosa which has been exposed to acid and pepsin. The defect penetrates
through the mucosa and muscularis mucosa into the sub-mucosa or muscular
layer. Primary peptic ulcers are usually duodenal, whereas secondary peptic
ulcers can be duodenal or gastric. In infancy, 80% of ulcers are secondary.
After the age of 6, 70% of ulcers are primary.
The pathogenesis of PUD in children, as in adults, is multifactorial with the
final common pathway being a breakdown in the normal mucosal defence
which permits acid peptic digestion of the mucosa. In their summary of
current clinical practice that was submitted in the dossier, the MAH quoted
rates of infection of H.pylori in primary PUD in children that varied between
39% and 91%, although the original articles were not referenced.
The clinical manifestations of PUD vary according to the age of the patient. In
neonates, the two major presentations are gastro-intestinal haemorrhage
and/or perforation. Most ulcers in this age group are acute and are secondary
to stress, with other medical disorders usually present. Neonates may also
present with vomiting, feeding difficulties, or failure to thrive.
Chronic peptic ulceration (primary PUD) occurs most commonly in children
over the age of 5 years. Older children and adolescents have clinical
manifestations similar to adults; i.e., epigastric pain which is relieved by food
or antacids; nocturnal pain; nausea; vomiting; anaemia; perforation; and
occult or gross bleeding. However, younger children may present with vague
symptoms such as abdominal pain, nausea and vomiting. Suspected peptic
ulcer should be diagnosed by endoscopy, by which in addition to visualisation
of the ulcer, the presence of H.pylori can be established.
The treatment of peptic ulcer disease in children has largely been
extrapolated from adult experience, due to lack of data. Treatment usually
includes agents that block acid secretion (H2 antagonists or proton pump
inhibitors (PPIs) and eradication of H.pylori, if present (with amoxicillin,
metronidazole or clarithromycin and a PPI).
Prior to the current understanding of the role H.pylori in the pathogenesis of
chronic peptic ulcer, H2-receptor antagonists were the mainstay of ulcer
therapy for adults and children. Ranitidine has a higher affinity for the H2
receptor and is considered to be 2-4 times more potent than cimetidine. It is
longer acting and has few adverse effects, mainly nausea, vomiting and
headache. It also has significantly less effect on the cytochrome P450 system
than cimetidine. The use of two other H2 receptor antagonists, famotidine and
nizatidine, is limited in children. Surgery is reserved for children with
perforation, haemorrhage, obstruction and, rarely, intractable pain.
Stress ulceration
31
Peptic ulcers may arise as a complication of physiological stress in severely ill
children. Stress is believed to compromise the gastric mucosal defence
mechanisms and allow normal amounts of gastric acid to cause ulceration,
which is frequently associated with acute haemorrhage. The therapeutic
strategy for prevention or treatment of stress ulcers or haemorrhage is to
maintain intragastric pH above 4.0 (Kelly, 1994). For the prophylaxis of stress
ulceration and subsequent gastrointestinal bleeding in critically ill children,
ranitidine administered as an intermittent infusion (2 to 6 mg/kg/day given in
divided doses), or as a continuous infusion (0.1 to 0.2mg/kg/hr), has been
used to maintain intragastric pH levels above 4.0.
4. RANITIDINE AND FDA PAEDIATRIC EXCLUSIVITY The data submitted to the FDA resulted in the labelling change as summarised
below (full details available on the FDA web-site).
In the FDA’s Medical Review, the assessor concluded that: ‘current medical
practice and response to H2 antagonists suggests that adult efficacy data with
H2 antagonists may be extrapolated to children, except for critically- ill
children where the pathophysiology seems to be different to other children’.
4.1 US label changes
These are extensive and include (in the clinical pharmacology section), the
following indications in children aged 1 month and above: the treatment of
duodenal and gastric ulcers, gastro-oesophageal reflux disease and erosive
oesophagitis, and the maintenance of healed duodenal and gastric ulcers. For
Zantac injection only there is a statement suggesting that: ‘Limited data in
neonatal patients (less than one month of age) receiving ECMO suggest that
ZANTAC may be useful and safe for increasing gastric pH for patients at risk
of gastrointestinal haemorrhage’. In addition, there are pharmacokinetic
statements added for both oral and injection formulations.
5. PROPOSED VARIATION- SPC CHANGES Proposed SPC changes for Zantac tablets, effervescent tablets and syrup
include: additional indications for the long term management of peptic ulcer
and the treatment of gastro-oesophageal reflux, including reflux oesophagitis
and the symptomatic relief of gastro-oesophageal reflux disease. A
pharmacokinetic statement is also included.
Proposed SPC changes for Zantac injection include: the ‘acute’ treatment of
peptic ulcer, gastro-oesophageal reflux, including reflux oesophagitis and the
symptomatic relief of gastro-oesophageal reflux disease. The prophylaxis of
stress ulceration in seriously ill patients is also a proposed new indication in
children.
6. SUBMITTED DOCUMENTATION The MAH submitted the following sponsored studies, in addition to published
studies: Pharmacokinetic (PK)/Pharmacodynamic(PD) Studies- Oral PK study-
Study RAN 2006
Intravenous studies -Protocol RAN-1149, Wells et al (neonates) and RAN 701
Efficacy studies-Study RAN M15 was the pivotal trial for the indication for the
long term treatment of peptic ulcers in children. Additional studies included
open label trials Study 145,145A, studies RAN 147 and 701. 6.1 Clinical expert report
The clinical expert was insufficiently critical regarding the limitations of the
data submitted for the proposed indications.
6.2 Pharmacokinetic (PK)/Pharmacodynamic(PD) Studies

32
A detailed review of the pharmacokinetic (PK) and pharmacodynamic(PD)
data submitted has been summarised in Annex 7.
6.2.1 Oral formulations
Four studies were submitted (see table 1); one company –sponsored trial and
three published studies.8
Table 1: Oral Paediatric Pharmacokinetic Studies Reviewed
Study No Source
1 Blumer J, et al. J Paediatrics,
1985;107: 301
2 Supplemental NDA for Paediatric
Labelling, NDA 18 -703 Zantac Tablets
3 Mallet E, et al. Eur J Clin Pharmac,
1989;36: 641
4 Study RAN 2006
6.2.1.1 Overall conclusions: pharmacokinetic studies of oral ranitidine
Table 2 provides a summary of the submitted oral paediatric pharmacokinetic
studies:
Table 2: Cross-study comparison of oral paediatric pharmacokinetic
data (mean values)
Study
No, age,
no
Dose
T0.5
(hr)
CL
(ml/min/m2)
Vd
(L/kg)
Tmax
(hr)
Cmax
(ng/ml)
AUC12hr
(hr*ng/ml)
1. 3-
6yrs
(12)
150 mg
(tablet)
2.0
(0.5)
455s
(192)
2.5
(1.0)
NA NA NA
2. 7m-
14yrs(8)
2 mg/kg
Single
dose
(syrup)
2.4
(0.5)
NA NA 1.61
(0.50)
244
(109)
1045
(324)
2 mg/kg
Steady
state
2.7
(0.5)
NA NA 1.66
(0.82)
320
(199)
1428
(578)
3. 6w-
6m (11)
5 mg/kg
(iv soln)
2.8
(0.8)
664
(NA)
NA 1.2
(0.4)
476
(164)
NA
4 4-11
yrs (24)
2.7mg/kg 2.1 25.5
(ml/min/kg)
4.94 2.7 476.6
(median)
The submitted data are limited, mainly due to poor methodology and due
to limited numbers, particularly in children under 3 years old. However,
from studies 1 and 4, which were the most robust in design, the
parameters in children were similar to that in adults when adjusted for
body weight.
These data support the inclusion of a statement in Section 5.2 of the Sm
PC and also the proposed dosage regimen for short term treatment of
ulcers.
6.2.2 Intravenous administration
Two company- sponsored trials were submitted, in addition to five published
studies. Study RAN 701 provided no useful information; in addition, 3 of the
publications were abstracts. The company- sponsored study by Wells et al
was undertaken in neonates receiving Extracorporeal Membrane Oxygenation
(EMCO) and is summarised below.

33
Table 3: Intravenous Paediatric Pharmacokinetic Studies Reviewed
Study No Source
1 Blumer J, et al. J Paediatrics,
1985;107: 301
5 Leeder JS, et. Acta Pharm Tox,
1986;59: 79
6 Leeder JL, et al. Clin Pharmac Ther,
1989;12: 7
7 Wiest, DB et al. Dev Pharmac Ther,
1989;12: 7
8 Rylance G. In: Perspective on
therapeutics in Northern Europe:
Hyperacidity states, London 1987;52
9 Protocol RAN-1149
10 Wells et al
RAN 701
6.2.2.1 A Pharmacokinetic and Pharmacodynamic Study of Ranitidine in
Neonates. Report No RC1998/00030/00. Published as Wells et al. Br J Clin
Pharmacol 1998; 38: 402-407 (study no 10.)
Objectives:
To characterise the pharmacokinetics of ranitidine administered as a single
intravenous dose in neonates
To characterize the pharmacokinetics of ranitidine administered as a
continuous intravenous infusion, using a dosing regimen which provides
therapeutically meaningful gastric acid suppression based on the data
from the single dose pharmacokinetic/pharmacodynamic evaluation in the
same subjects.
To collect information on the safety of single and multiple doses of
ranitidine in neonates.
Methodology
This was an open-label single intravenous dose study followed by a constant-
rate intravenous infusion of ranitidine conducted in 12 term neonates
(younger than 1 month of age) presenting to the intensive care unit with a
medically established need for H2-blocker therapy. All subjects had potentially
reversible cardiac or pulmonary failure requiring treatment with
Extracorporeal Membrane Oxygenation (EMCO). Primary diagnoses included:
meconium aspiration (N=6), sepsis (N=1), hypoplastic lungs (N=1), and
persistent pulmonary hypertension (N=1)
Ranitidine (2.0mg/kg) was administered over 10 minutes into the
postmembrane side of the ECMO circuit. Blood samples (1.5mL each) were
collected at baseline and 0.08, 0.167, 0.25, 0.5, 0.75, 1, 2, 3, 4, 6, 12, 18
and 24 hours. Twenty-four hours after the initial dose, a continuous
intravenous infusion of ranitidine (0.083mg/kg/hr) was started and continued
for 72 hours or until ECMO was discontinued. Gastric pH measurements were
conducted at specified times throughout the study. If the stomach pH fell to
<4, the rate of the infusion was increased in increments of 0.042mg/kg/hr
(1mg/kg/24hours).
Results
Pharmacokinetic parameters are provided below in table 4. As expected, in
this study ranitidine had a much longer half-life and lower clearance in
neonates than in older children and adults.
After a single 2mg/kg dose of ranitidine, mean intragastric pH increased to >5
within 90 minutes and remained >5 for 16 hours in subjects with an initial pH
of ≤ 4. The investigators therefore suggested that if intermittent intravenous

34
administration is used, a dose interval of ≥ 12 hours might be appropriate in
this population. Total clearance was related to estimated glomerular filtration
rate. Consequently, the dose interval may need to be lengthened in neonates
with severely compromised renal function.
The plasma concentration and pharmacodynamic data suggested that a
continuous infusion of 2mg/kg/24 hours is adequate to maintain intragastric
pH above 4 in greater than 90% of term neonates undergoing ECMO. Of the
13 subjects enrolled, five had an initial gastric pH of ≤ 4. In five subjects,
gastric pH increased to > 4 within 90 minutes after ranitidine was
administered and remained above 4 for a minimum of 15 hours.
Conclusions
This study provided useful data to inform dosing recommendations in
neonates. Although ECMO significantly increases the vascular volume and
may impact the pharmacokinetics of drugs with small volumes of distribution,
the impact of ECMO is minimal for drugs such as ranitidine with a large
volume of distribution. Therefore, it would be possible to extrapolate the
pharmacokinetics data from this study to neonates with normal renal function.
In addition, these data suggest that a dose of 2mg/kg should be sufficient to
increase gastric pH to >4 for at least 16 hours.
6.2.2.2 Overall conclusions: pharmacokinetic studies- intravenous ranitidine
Results are compared in Table 4:
Table 4: Pharmacokinetic parameters following administration of Zantac in
Paediatric patients
Values for half-life and clearance were consistent amongst all ages, with
the exception of the neonates, in whom ranitidine had a much longer half-
life and lower clearance. This was not surprising, in view of the
underdeveloped hepatic and renal capacities in neonates.
There was a lot of variability of kinetic parameters for all age groups (this
is also the case in adults).
The submitted data are limited, mainly due to poor methodology.
However, the parameters in children (excluding neonates) were similar to
those in adults.
These data support the inclusion of a statement in Section 5.2 of the Sm
PC and also the proposed dosage regimen for short term treatment of
ulcers.

35
6.2.3 Pharmacodynamic studies
6.2.3.1 Results of pharmaocodynamic studies are presented in Table 5.
Table 5: Pharmacodynamic data in children
Dose Result
Study 1 0.13 to 0.8 mg/kg IV C90%* to 60ng/ml
Study 3 5 mg/kg po (iv form.) <100 ng /ml results in
pH<4.0, which occurs 9
hrs after the dose
Study 4 2 mg/kg po (syrup) Gastric pH<2.5 in 33%
of patients with serum
drug levels ranging from
18-331 ng/ml. No drug
levels reported for
patients with gastric
pH>2.5
Study 8 1 mg/kg IV 2/20 subjects failed to
produce gastric ph>3.5
with ranitidine conc>60
ng/ml over 6 hr
Study 9
Study 9 1 mg/kg IV Of 10 patients with
gastric pH≤2.0 prior to
drug therapy, had no
acid suppression and the
remaining 8 had variable
response
RAN 20006 75mg oral tablet or
placebo
Rapid decrease in acidity
at 30 min (H+ ,pH
measurements).
Greatest effect (% time
at pH >3) at 1-5hrs.
Report No
RC1998/00030/00
2mg/kg/24 hrs in
neonates
In 5/12 subjects, gastric
pH increased to > 4
within 90 minutes after
ranitidine was
administered and
remained above 4 for a
minimum of 15 hours.
* Serum ranitidine concentration needed to inhibit baseline gastric acid
secretion by ≥90%
In all studies, the pharmacodynamic response was quite variable among
individuals across studies, with many subjects exhibiting complete lack of
response, even after achieving serum ranitidine concentrations shown to
suppress 90% of gastric acid secretion in subjects from Study 1 (see 6.2.1.1.
The large inter-subject variability in gastric acid suppression among the
studies is likely to be due to the different patient diagnoses and the
pharmacodynamic endpoints implemented.
Study 1, RAN 20006 and RC1998/00030/00 (which was undertaken in
neonates receiving ECMO), were the best designed of the 5 studies and
provided the most useful information, as all provided baseline data. In
addition, study 2006 was placebo controlled. In study 1, the subjects had
confirmed active PUD, which is the proposed indication for IV ranitidine.
In adult studies, the ED 50 (dose required to produce 50% of the maximum
effect) is usually measured, whereas this was not measured in the paediatric

36
studies. It is therefore difficult to compare paediatric values with those from
adult studies. However, inter-subject variability is also evident in such
studies. In addition, in one study (Wyeth, 1998), the duration with pH above
4 was similar to that in study RAN 20006.
6.3.2.2 Overall conclusions regarding pharmacodynamic studies
From the available data, the pharmacodynamic response appears to be similar
in children to that in adults. 6.3 Efficacy data
There were no company- sponsored clinical efficacy studies for the following
proposed indications: the treatment of gastro-oesophageal reflux, (including
reflux oesophagitis and the symptom relief of gastro-oesophageal reflux
disease) and, for injection formulations, the prophylaxis of stress ulceration in
seriously ill patients.
6.3.1 Study RAN M15
The objective of this single centre double-blind, placebo controlled trial that
was undertaken in Moscow in 1992-4 was to establish the safety and efficacy
of ranitidine 150mg at night compared to placebo in the prevention of
duodenal ulcer over a 12 month treatment period.
Study Design
195 children aged 8 to 16 (mean 13 yrs), with a male to female ratio of 2:1,
who had endoscopically confirmed ulcers (≥ 5mm in diameter), received open
therapy with ranitidine 150mg bd, for 4 to 8 weeks. On endoscopic
confirmation of healing, children were randomly assigned to either ranitidine
150mg at night or placebo in a double-blind, parallel group study. Symptom
assessment was repeated at 2 monthly intervals with endoscopy every 4
months for up to 12 months.
Inclusion criteria
- endoscopically confirmed duodenal ulcer ≥5mm diameter
- aged between 8 – 16 years
- requirement for an H2-receptor as part of normal clinical management
- able to start treatment within 3 days of the pre-study endoscopy
- written consent provided by child and/or legal guardian
- endoscopic confirmation of ulcer healing after 4 or 8 weeks for entry into
long-term phase
Exclusion criteria
- endoscopic confirmation of gastric ulcer or erosive oesophagitis
- concomitant use of potentially ulcerogenic drugs
- other serious condition
- previous gastric surgery
- treatment with therapeutic doses of anti-ulcer drugs immediately prior to
entry to the study
The primary efficacy analysis in the maintenance phase was based on the
number of patients who had relapsed (symptomatically and endoscopically)
on each treatment at each visit. Patients who reported moderate or severe
symptoms were regarded as symptomatically relapsed. Patients with
endoscopically proven duodenal ulcer, regardless of severity of symptoms,
were regarded as endoscopically relapsed. Patients who reported moderate or
severe symptoms and had an endscopically confirmed duodenal ulcer were
regarded as endoscopically and symptomatically relapsed. The following two
relapse rates were calculated:
Modified Crude Relapse Rate

37
Symptomatic and endoscopic relapse: patients who withdrew from the study
without a relapse before the nth month assessment (n=2, 4, 6, 8, 10, 12)
were excluded from the calculation of modified crude relapse rate from that
visit onwards. Endoscopic relapse also excluded those patients who withdrew
from the study with symptomatic relapse not proven by endoscopy.
At each visit (cumulatively including unscheduled visits), the proportion of
patients relapsed on each treatment was compared using the Mantel-Haenszel
chi-square test without continuity correction. If the sample size assumption
required for the Mantel-Haenszel test was not satisfied then Fisher’s exact
test was used.
Crude Relapse Rate
Symptomatic and endoscopic relapse: patients who withdrew from the study
without a relapse before the nth month assessment (n=2, 4, 6, 8, 10, 12)
were treated as relapsed in the calculation of crude relapse rate from that
visit onwards. Endoscopic relapse excluded those patients who withdrew from
the study with symptomatic relapse not proven by endoscopy. Treatments
were compared by means of the Mantel-Haenszel or Fisher’s exact test as
described above.
Secondary efficacy analysis
Symptomatic Relapse Confirmed by Endoscopy
At each visit (cumulatively including unscheduled visits) the proportion of
patients experiencing a symptomatic relapse, confirmed by endoscopy on
each treatment was compared using the Mantel-Haenszel chi-square test or
Fischer’s exact test.
Secondary efficacy analyses included the proportion of symptomatic relapses
and the time to relapse (symptomatic, endoscopic and symptomatic
confirmed by endoscopy).
Results
Baseline characteristics of participants
The baseline characteristics of the participants were similar in both groups.
Most of the patients were newly diagnosed (68%), whilst the median duration
of peptic ulcer disease in the others was 2 years. A positive family history of
peptic ulcer disease was reported in > 40% of the population. Whilst most
patients presented with mild or moderate epigastric pain, 32% had no pain at
the time of the initial endoscopy. Gastritis was reported at endoscopy for
nearly all patients.
Efficacy analysis
Ulcer healing was observed in 177 of 194 (91%) patients after 4 weeks of
treatment. 16 patients continued treatment to 8 weeks- all patients had
healed ulcers on repeat endoscopy.
191 children entered the long term phase; 189 were included in the Modified
Intention To Treat (MITT) efficacy analysis. Within 4 months, 17 patients
receiving placebo suffered relapse (18%), compared with 5 patients in the
ranitidine group (5%) (p=0.006). The cumulative ulcer relapse rate at 12
months was 30% for placebo and 9% for ranitidine (p<0.001).
However, it is of note that few patients suffered a symptomatic relapse – six
in the placebo group and two in the ranitidine group.
Results of repeat endoscopic examination for the long-term phase are
summarised below in table 6:
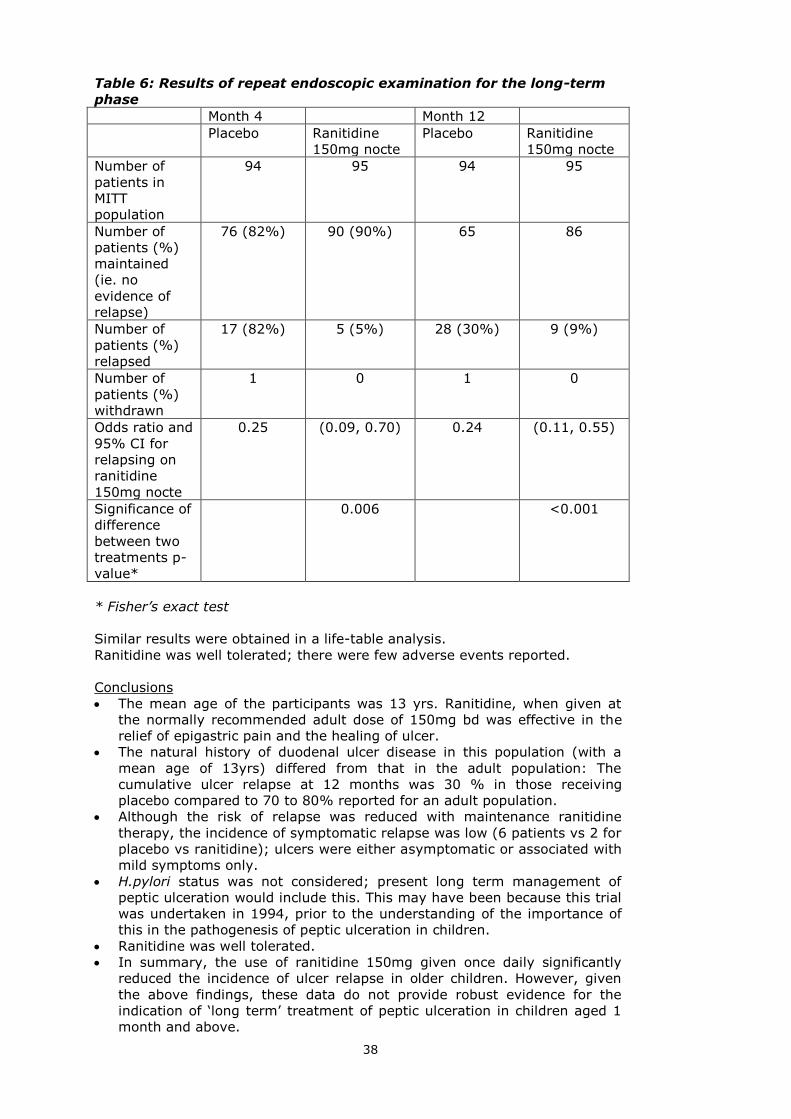
38
Table 6: Results of repeat endoscopic examination for the long-term
phase
Month 4 Month 12
Placebo Ranitidine
150mg nocte
Placebo Ranitidine
150mg nocte
Number of
patients in
MITT
population
94 95 94 95
Number of
patients (%)
maintained
(ie. no
evidence of
relapse)
76 (82%) 90 (90%) 65 86
Number of
patients (%)
relapsed
17 (82%) 5 (5%) 28 (30%) 9 (9%)
Number of
patients (%)
withdrawn
1 0 1 0
Odds ratio and
95% CI for
relapsing on
ranitidine
150mg nocte
0.25 (0.09, 0.70) 0.24 (0.11, 0.55)
Significance of
difference
between two
treatments p-
value*
0.006 <0.001
* Fisher’s exact test
Similar results were obtained in a life-table analysis.
Ranitidine was well tolerated; there were few adverse events reported.
Conclusions
The mean age of the participants was 13 yrs. Ranitidine, when given at
the normally recommended adult dose of 150mg bd was effective in the
relief of epigastric pain and the healing of ulcer.
The natural history of duodenal ulcer disease in this population (with a
mean age of 13yrs) differed from that in the adult population: The
cumulative ulcer relapse at 12 months was 30 % in those receiving
placebo compared to 70 to 80% reported for an adult population.
Although the risk of relapse was reduced with maintenance ranitidine
therapy, the incidence of symptomatic relapse was low (6 patients vs 2 for
placebo vs ranitidine); ulcers were either asymptomatic or associated with
mild symptoms only.
H.pylori status was not considered; present long term management of
peptic ulceration would include this. This may have been because this trial
was undertaken in 1994, prior to the understanding of the importance of
this in the pathogenesis of peptic ulceration in children.
Ranitidine was well tolerated.
In summary, the use of ranitidine 150mg given once daily significantly
reduced the incidence of ulcer relapse in older children. However, given
the above findings, these data do not provide robust evidence for the
indication of ‘long term’ treatment of peptic ulceration in children aged 1
month and above.

39
6.3.2 Study 145
Study 145 was an open-label single centre study (conducted in the US) of 12
patients, aged 3.5-16 years, with endoscopically diagnosed duodenal and/or
gastric ulcers. All children had a history of epigastric pain, nine had nausea
and vomiting and one child had melaena.
Phase 1 was designed to support the dosing in Phase 2. During this phase,
each child received an intravenous ranitidine loading dose of 0.6mg/kg over
15 minutes, followed by a continuous intravenous infusion of 0.2mg/kg/hr. At
the end of each hour, a bolus dose equal to 20% of the initial loading dose
was infused and the continuous infusion dose increased by 20%. Doses were
increased in stepwise fashion until gastric acid secretion was inhibited by at
least 90%. Pharmacokinetic sampling was performed both before and after
dosing. The doses administered during this phase ranged from 13.4 to
74.5mg (0.3 to 2.1mg/kg).
Phase 2 was begun on the following day. For this phase, ranitidine was
administered as an intravenous bolus every 6 hours until the patient could
resume enteral feeding. The dose administered was designed to yield the
average serum concentration required to inhibit gastric acid secretion by at
least 90%. Calculations of this dose were based on data from Phase 1. The
doses administered during this phase ranged from 0.13 to 0.80mg/kg/dose.
Phase 3 was designed for the collection of efficacy and safety data. In this
phase, ranitidine was administered orally (as tablets). The dose chosen for
each patient was based on the information obtained in Phases 1 and 2.
Ranitidine was administered every 12 hours for 6 weeks. The doses
administered during this phase were 37.5mg every 12 hours (9 patients) and
75mg every 12 hours (3 patients).
Results
A total of 12 patients, aged 3.5-16 years, with endoscopically diagnosed
duodenal and/or gastric ulcers were enrolled. At the completion of 6 weeks of
treatment, endoscopic examinations revealed that all of the ulcers were
healed. Follow-up evaluations performed at the discretion of the investigator
for up to 12 months after treatment revealed no evidence of recurrence in any
of the children.
Ranitidine was effective at the doses studied in healing duodenal and gastric
ulcers and preventing ulcer recurrence in these patients. The investigator
recommended a paediatric oral dose from 1.25 to 1 .90mg/kg every 12 hours
to treat gastric and duodenal ulcers.
6.3.3 Study 145A
This was an open-label, single centre study to evaluate the efficacy of
ranitidine in the treatment of gastric and/or duodenal ulcers in children. This
study was similar in design to Study 145, except that the patients were
administered ranitidine syrup instead of tablets. Ranitidine was to be
administered every 6 hours as a 15-minute intravenous infusion. When the
patient was able to resume enteral feeding, ranitidine was to be administered
orally (syrup formulation) for 6 weeks. Pharmacokinetic and
pharmacodynamic data were to be collected during the first 2 days of the
study.
A total of three patients aged 5-8 years were enrolled in the study. All
patients responded well to ranitidine therapy over an approximate 6-week
course of treatment. In two of the three patients, the ulcer healed.
6.3.4 Study RAN-701

40
This study compared the use of a continuous infusion with bolus injections of
ranitidine with regard to the inhibition of gastric acid production in critically ill
children. A total of 51 patients aged 4-12 years were enrolled and randomized
to either ranitidine 0.2mg/kg/hr (n=24) or a bolus infusion of ranitidine
1.6mg/kg every 8 hours (n=27).
Twenty (20) patients in the ranitidine 0.2mg/kg/hr treatment group and 19
patients in the ranitidine 1.6mg/kg every 8hr treatment group completed the
study. Efficacy measurements were dependent on intragastric pH
measurements. However, there were inconsistencies in the electronic
intragastric pH data, poor quality blood serum assay data and concern
regarding reliability of the results. Analyses of the data were therefore not
performed.
6.3.5 Study RAN-147
A double-blind, randomized trial of ranitidine therapy in patients with cystic
fibrosis and pancreatic insufficiency.
This study compared the effects of Pancrease and ranitidine 150 mg bd with
Pancrease therapy alone, on pulmonary function, fat and carbohydrate
absorption in 8 children (boys) with cystic fibrosis and pancreatic
insufficiency. The investigators reported that fat and carbohydrate absorption
was improved in 5 patients compared with placebo, but there was no
difference in pulmonary function between the groups.
6.3.6 Efficacy data- published reports
The FDA undertook a comprehensive review of the literature for the proposed
indications (excluding the use of ranitidine for the prophylaxis of stress
ulceration). For all of the proposed indications, these data only included
reviews, open label studies and case reports.
6.3.6.1 .Literature review for the prophylaxis of stress ulceration in seriously
ill children
The Clinical Expert report included a review of the published literature for the
prophylaxis of stress ulceration, which is a proposed indication for the
ranitidine injection formulation. There were no company- sponsored efficacy
trials for this indication.
In this review, there were no published randomised controlled trials with
appropriate end-points such as bleeding. Therefore, no robust evidence was
provided that use in the prophylaxis of stress ulcer provides protection
against bleeding.
In further support for this indication, in their response to a request for
supplementary information (section 7, Q2), the MAH has quoted The
American Society of Health-System Pharmacists guidelines published in 1999
on prophylaxis of stress ulceration. These guidelines specifically reviewed the
literature with regard to stress-induced bleeding associated with trauma,
surgery and acute organ failure, including published meta-analyses that
demonstrated the efficacy of H2 receptor antagonists versus placebo in
adults. They recommend the prophylaxis of stress ulceration in an ICU setting
for adults using medications including H2 receptor antagonists. For children,
although it was noted that there was a distinct lack of published randomised
controlled trials with appropriate end-points such as bleeding, some studies
have suggested that prophylaxis of stress-ulcer might be of use for children.
For example, Kuuseal et al (1997) showed a decreased risk of endoscopically
diagnosed gastric lesions in mechanically ventilated infants treated with
ranitidine. Despite the lack of controlled studies in cases of trauma and
surgery, the guidelines recommended prophylaxis of stress ulcer in the case
of thermal injuries and highlighted that “the risk of stress-induced bleeding is
greater in children with respiratory failure, coagulopathy, a Paediatric Risk of
Mortality Score of ≥ 10, and thermal injuries.”

41
Although there have been no appropriate randomised controlled trials
undertaken in children, there is a large volume of literature discussing the
prophylaxis of stress ulceration in critically ill children. Ranitidine, when
administered either as an intermittent intravenous infusion at a dose of 2-
6mg/kg/day in divided doses; (Harrison et al, 1998; Kuusela et al, 1997;
Kuusela, 1998; Lopez-Herce et al 1988; Osteyee et al 1994; Rylance
1987 and Santucci et al, 1991), or as a continuous infusion at a rate of 0.1-
0.2mg/kg/hr; (Osteyee et al, 1994; Santucci et al, 1991; Dimand et al
1989 and Eddleston et al, 1989), has been successfully used to maintain
gastric pH levels above 4.0. Both dosing regimens were effective in raising
and maintaining gastric pH above 4. However, the pH values fluctuated more
with the intermittent regimens. (Osteyee et al, 1994 and Santucci et al,
1991). Harrison et al recommended that critically ill children with normal renal
and hepatic function should be treated with a minimum of 3mg/kg/day and
the dose be titrated based on gastric pH.
Oral (via naso-gastric tube) vs intravenous administration of ranitidine for the
prevention of stress ulceration has also been studied. (Lopez-Herce et al,
1988; Hartemann et al 1987) The median time pH was above 4 was less in
the oral group. The authors therefore suggested that oral ranitidine may not
be as effective due to decreased absorption in critically ill children. (Lopez-
Herce et al, 1988).
Conclusions
In this review, there were no published randomised controlled trials with
appropriate end-points such as bleeding. Therefore, no robust evidence was
provided that the prophylaxis of stress ulcer provides protection against
bleeding.
Although the ASHP guidelines recommend prophylaxis of stress ulcer in the
case of thermal injuries, this recommendation does not appear to be evidence
based.
6.3.6.2 Literature review for gastro-oesophageal reflux disease
The Clinical Expert report included a review of the published literature for the
proposed indication of the treatment of gastro-oesophageal reflux (GOR),
including reflux oesophagitis and gastro-oesophageal reflux disease. There
were no company- sponsored efficacy trials submitted for this indication. In
the literature review there is an absence of randomised controlled trials to
support the proposed indication; a recent literature review by Cezard in 2004
also found a lack of evidence to support the use of H2 anatagonists for GOR.
In a case series De Angelis and Banchini (1989) reported their experience
of the use of ranitidine in the treatment and prophylaxis of gastro-intestinal
disorders in 391 children aged from 72 hours to 16 years. The children
received oral ranitidine at a dose of 6-8 mg/kg/day initially, followed by
maintenance therapy of 3-4mg/kg/day. Intravenous administration was used
in appropriate cases, such as those with upper gastro-intestinal haemorrhage
or in severe oesophagitis due to the ingestion of caustic substances. Reflux
oesophagitis was treated in 185 children; in 25 severe cases, endoscopy
revealed re-epithelialisation in all cases. In those children with less severe
oesophagitis, 95% had disappeared or showed marked improvement of
lesions, both macroscopically and histologically. In an open label prospective
study, Karjoo and Kane (1995) found visual and/or histological evidence of
oesophagitis in 84% of 153 children aged 6-18 years old (mean 9.9 years)
with chronic abdominal pain lasting more than 3 weeks. The children were
initially treated with 4mg/kg ranitidine twice daily for 2 weeks, increasing to
4mg three times daily for a further 2 weeks. If symptoms persisted patients
were switched to omeprazole. Seventy percent of patients had mild to
moderate symptom improvement with ranitidine. The effect of high dose
ranitidine (10mg/kg twice daily) was compared with omeprazole

42
(40mg/day/1.73m2) in 25 children (aged 6 months to 13.4 years) with
oesophagitis, who had previously not responded to 8 weeks of ranitidine at
8mg/kg/day and cisapride (Cucchiara et al, 1993). Both drugs produced
comparable healing and relief of symptoms. In further support for this
indication (RSI response, section 7, Q2), the MAH has quoted the North
American Society for Paediatric Gastroenterology and Nutrition clinical
practice guidelines (published in 2001) on the diagnosis and treatment of
gastro-oesophageal reflux (GOR). Recommendations were based on a review
of the medical literature for infants and children, (excluding neonates less
than 72 hours old), premature infants and infants and children with
neurological or anatomical impairments or disorders. Despite the lack of
robust evidence, overall recommendations supported the use of H2 receptor
antagonists for the relief of symptoms and mucosal healing in children with
GOR. Specifically, acid suppressants such as H2 receptor antagonists were
recommended for infants with recurrent vomiting, heartburn, oesophagitis
and in patients with asthma and symptoms of GOR. The recommended daily
dose of oral ranitidine in the treatment of gastro-oesophageal reflux in
children was 5-10mg/kg/day administered as two divided doses. The use of
parenteral therapy was recommended only when oral therapy is not
advisable, at a dose of 2-5mg/kg/day administered in divided doses.
Conclusions
In this review, there were no published randomised controlled trials
submitted. Therefore, no robust evidence was provided to support the
proposed indication of treatment of gastro- oesophageal reflux.
Although the North American Society for Paediatric Gastroenterology and
Nutrition clinical practice guidelines recommend the use of ranitidine for this,
this recommendation did not appear to be evidence based.
6.3.7 Overall conclusions regarding efficacy data for all proposed indications
There were no randomised controlled trials submitted for the following
proposed indications: the treatment of gastro-oesophageal reflux (including
reflux oesophagitis and the symptom relief of gastro-oesophageal reflux
disease) and the prophylaxis of stress ulceration in seriously ill patients for
injection formulations.
The only double blind randomised controlled trial that was submitted for the
prevention of duodenal ulcer was poorly designed as it did not consider the
presence of H.pylori in participants. This may have been because this trial was
undertaken in 1994, prior to the understanding of the importance of H.pylori
in the pathogenesis of peptic ulceration. Even taking this into consideration,
the results of this trial, whilst supportive, did not provide robust evidence that
ranitidine is superior to placebo for the proposed indication.
Overall, the submitted efficacy data were extremely disappointing. In
particular no randomised controlled trial was undertaken in children with
gastro-oesophageal reflux. This should not have been difficult to perform.
6.4 Safety
Adverse effects of ranitidine
Known adverse effects of ranitidine include diarrhoea and other gastro-
intestinal disturbances, altered liver function tests (rarely liver damage),
headache, dizziness, agitation, visual disturbances, rash, alopecia and
tiredness. Rare side-effects include acute pancreatitis, acute interstitial
nephritis, tachycardia, bradycardia, AV block, confusion, depression, and
hallucinations (particularly in the very ill), hypersensitivity reactions (including
fever, arthralgia, myalgia, anaphylaxis), blood disorders (including
agranulocytosis, leucopenia, pancytopenia, thrombocytopenia), and skin
reactions (including erythema multiforme and toxic epidermal necrolysis).
There have been occasional reports of gynaecomastia and impotence
associated with the use of ranitidine.

43
6.4.1 Clinical trial data
The safety data from the submitted clinical trials were detailed in the Medical
Review of the FDA assessment report. In all studies except RAN 701,
ranitidine was well tolerated. There were few reported adverse events, mostly
relating to the gastro-intestinal tract. Routine laboratory data were collected
for all studies.
Study RAN-701
This study assessed inhibition of gastric acid production in 51 critically ill
children. Five (2 1%) patients in the ranitidine 0.2mg/kg/hr group reported
five adverse events and 2 (7%) patients in the 1.6mg/kg Q8hr group reported
two adverse events. The most frequently reported adverse events were death
(3 fatalities) and hypotension. It should be noted that death was not an
unexpected event as this study was conducted in very critically ill patients.
Long term safety data
In study RAN M15 (duration of 12 months), there were minor haematological
abnormalities detected in 89% of patients treated with ranitidine. In addition,
15% of patients had minor elevations of serum alkaline phosphatase levels.
No other long term data (in particular, longitudinal growth measurements)
were available from this study.
6.4.2 Cumulative review of safety- post-marketing reports
A search of the safety database revealed a total of 971 adverse event reports
associated with ranitidine administration in children that had been received
worldwide by GSK from the first launch of Zantac in 1981 until 02 August
2004. The majority of cases were spontaneous, non-serious, and reported by
medical professionals. Twenty-nine percent of all reports were received from
consumers. Cases were received mainly from the US (59%). The majority of
cases involved children aged two years of age or younger. The majority of the
971 cases (74%) were non-serious, spontaneous reports received from
medical professionals and described patients 2 years of age or younger. Most
patients received ranitidine to treat a condition (e.g. GERD, ulcer) for which
some of the reported events (e.g. vomiting, irritability, abdominal pain,
crying, insomnia) could be a symptom. Review of these data did not highlight
any safety issues for children.
Published reports on safety
The FDA undertook a comprehensive review of the literature report. No
significant safety issues were identified in clinical studies involving over 350
and 450 children who received oral and parenteral ranitidine respectively.
7. REQUEST FOR SUPPLEMENTARY INFORMATION (RSI) Following assessment of the data, the following questions were raised by the
MHRA:
7.1. Regarding the proposed changes to section 4.2: please could the
applicant clarify the terms ‘acute’ and ‘long term’ treatment.
Response of the MAH :
‘As the available information reviewed has not been generated as a result of a
specific development programme for the use of Zantac in children, a range of
recommendations on duration of treatment were identified in the literature for
the proposed paediatric indications. Despite this, a number of publications
described treatment duration of paediatric peptic ulcers ranging from four to
eight weeks with oral formulations (Blumer et al 1985; Accadia et al 1986;
de Angelis & Banchini 1989; Scorza et al 1990). Additionally,

44
recommendations for an initial 4 weeks treatment period with an extension to
8 weeks if healing was not resolved was proposed by J Sondheimer (Current
Pediatric Diagnosis and Treatment 1992, Hathway & Hay. Chapter 19.), and
treatment in children with H2 receptor antagonists for 1 to 2 weeks to relieve
symptoms and 6 weeks of treatment required for resolution of chronic peptic
ulcer was recommended by Bisset et al (Forfar and Arneils Textbook of
Pediatrics 2004, Chapter 17.).
Long term maintenance therapy has been shown to reduce the rate of ulcer
reoccurrence in follow-up studies of six months to 1 year duration
(Deganello et al 1990; Scorza et al 1990; Sherman 1994). However,
evidence now indicates that reoccurrence of ulcer after cessation of therapy
could be due to infection with H.pylori and this should be considered in cases
of peptic ulcer with longer time to resolution. Thus GSK propose that this
should be indicated in the proposed text for long-term treatment of peptic
ulcer. Additionally, ranitidine is also used during multi component therapy
regimens of H.pylori infection, with an initial proposed therapy of 2 weeks
(University of Michigan Health System Guidelines for Clinical Care - Peptic
Ulcer, May 2005) and 94.3% healing rate observed in a trial covering 6 weeks
of triple therapy (Scherbakov et al 2001.
Data for the parenteral treatment of peptic ulcer is limited and generally
considered clinically only when oral administration is not possible. Therefore
GSK propose additional wording to indicate this treatment regimen. Taking
into consideration the data available, GlaxoSmithKline feels that dosing of
Zantac for the acute treatment of peptic ulcer in paediatric populations should
be from four weeks to eight weeks for oral administration of Zantac. Further,
the duration of long-term maintenance therapy has been proposed in line with
the literature discussed, however as recent understanding of the aetiology of
peptic ulcers has shown a strong association with infection with H.pylori. GSK
have proposed wording to alert the health care provider to this possibility.
Further GlaxoSmithKline propose that the wording for parenteral
administration should be clarified to indicate that this is not the primary
treatment option’.
7.2. Please could the ‘Clinical Expert’ provide further justification for
the proposed indications of long term management of peptic
ulcer, treatment of gastro-oesophageal reflux, including reflux
oesophagitis and the symptom relief of gastro-oesophageal reflux
disease for oral and injection formulations, and also for the
prophylaxis of stress ulceration in seriously ill patients for
injection formulations.
Response of the MAH:
‘Zantac injection is indicated for the treatment of peptic ulcer, treatment of
gastro –oesophageal reflux, including reflux oesophagitis and symptom relief
of gastro oesophageal reflux disease. It is also indicated for the prophylaxis of
stress ulceration in seriously ill patients.
The American Society of Health-System Pharmacists published guidelines in
1999 on prophylaxis of stress ulceration. These guidelines specifically
reviewed the literature pertaining to stress-induced bleeding associated with
trauma, surgery and acute organ failure, including published meta-analyses
demonstrating the efficacy of prophylaxis with H2 receptor antagonists versus
no prophylaxis in adults (Tryba et al 1991; Cook et al 1991; Cook et al
1996). The ASHP guidelines recommend the prophylaxis of stress ulceration in
an ICU setting for adults using with medications including H2 receptor
antagonists. For the paediatric population it was noted that there was a
distinct lack of published randomised controlled trials with appropriate end-
points such as bleeding and to provide conclusive evidence that prophylaxis of
stress ulcer provides protection against bleeding. However, some studies have

45
suggested that prophylaxis of stress-ulcer may be of use for paediatric
populations, for example Kuuseal et al (1997) showed a decreased risk of
endoscopically diagnosed gastric lesions in mechanically ventilated infants
treated with ranitidine. Despite this lack of controlled studies in cases of
trauma and surgery, the guidelines did recommend prophylaxis of stress ulcer
in the case of thermal injuries and highlighted that “the risk of stress-induced
bleeding is greater in pediatric patients with respiratory failure, coagulopathy,
a Paediatric Risk of Mortality Score of ≥ 10, and thermal injuries”. Taking into
account these guidelines and the most recently reviewed data as provided
(D2004-4586), GSK believes that ranitidine should be indicated for the
prophylaxis of stress ulceration in the paediatric population.
In 2001 the North American Society for Paediatric Gastroenterology and
Nutrition published clinical practise guidelines outlining the diagnosis and
treatment of Gastrooesophageal reflux (GER). Recommendations were based
on a review of the medical literature available pertaining to infants and
children, but excluding neonates less than 72 hours old, premature infants
and infants and children with neurological or anatomic impairments or
disorders. Overall recommendations supported the use of H2 receptor
antagonists for the relief of symptoms and mucosal healing in children with
GER. Specifically acid suppressants such as H2 receptor antagonists were
recommended for infants with recurrent vomiting, heartburn, oesophagitis
and in patients with asthma and symptoms of GER. Therefore, GSK feels that
the extensive body of literature surrounding the use of H2 receptor
antagonists in paediatric populations with GER taken together with these
guidelines support the use of ranitidine for paediatric GER. An extensive body
of literature, including clinical study data, published literature and guidelines
have been reviewed during this submission. A number of clinical care
guidelines were consulted during this review however, as stated in such
guidelines and acknowledged by GSK, there are few prospective randomized
studies specifically in paediatric populations for the proposed indications.
However GSK believe that the comprehensive review as submitted (D2004-
4586) further supports the use of ranitidine in the paediatric populations in
the indications proposed.’
7.3. During the Article 30 procedure, in 2003 one of the outstanding
issues was the high alcohol content of the syrup formulation. At
this time, GSK agreed to the proposal to add a precautionary
statement in the SmPC regarding this. Please could the applicant
comment on this and whether any further steps have been taken
to address this issue.
Response of the MAH:
‘The referral under Article 30 of directive 2001/83/EC to harmonize the SmPC
for Zantac/Ranitidine HCl was halted in 2003. As a consequence GSK are
currently reviewing this issue internally and propose to submit this as a type
II variation at later date’.
8. DISCUSSION
8.1 Do the data support the new indications?
8.1.1 Efficacy considerations
As discussed in the conclusions of the section on efficacy (in section
6.3.7), the submitted data for the proposed indications were
disappointing, even though several studies had been sponsored by the
applicant.

46
For the long term treatment of peptic ulcer, the results of this trial, whilst
supportive, did not provide robust evidence that ranitidine is superior to
placebo for the proposed indication.
With regard to the indications of the treatment of gastro-oesophageal
reflux (including reflux oesophagitis and the symptom relief of gastro-
oesophageal reflux disease) and the prophylaxis of stress ulceration in
seriously ill patients, no randomised controlled trials were submitted and
the published data did not provide sufficient evidence of efficacy. Although
it is recognised that it would be difficult to undertake a randomised
controlled trial in seriously ill children to provide robust evidence for the
prophylaxis of stress ulceration, the submitted studies did not provide
sufficient data regarding dosage to warrant extrapolation from efficacy in
adults.
8.1.2 Safety considerations
From the data submitted, no particular safety concerns were identified.
However, there were only limited long term safety data available from
study RAN M15 (duration of 12 months). It was disappointing that in this
study, no longitudinal growth measurements were undertaken.
The ethanol content of ranitidine syrup is high (approximately 9%). The
clinical significance of this is not known.
Overall conclusion regarding the proposed indications
The efficacy and safety data submitted do not support the proposed
indications of the long term treatment of peptic ulcer, the treatment of
gastro-oesophageal reflux (including reflux oesophagitis and the symptom
relief of gastro-oesophageal reflux disease) and the prophylaxis of stress
ulceration in seriously ill patients
However, as oral ranitidine is already licensed for the treatment of peptic
ulcers in children and given that it established practice in acute treatment
to use the intravenous route in some cases, it seems reasonable to
consider that this indication can be extrapolated to the injection
formulations (see below section 8.2 for discussion about dosage).
8.1.3 Is the proposed age of 1 month onwards supported?
8.1.3.1 For oral formulations:
At present, the oral formulations are licensed for the treatment of peptic
ulceration with no age restriction. The applicant proposes a lower age limit
of one month onwards for all indications.
The pharmacokinetic data submitted were very limited in children aged 1
month to 3 years.
In addition, there were very limited efficacy and pharmacodynamic data in
this age group.
It is therefore proposed that the lower age limit for the short term
treatment of peptic ulcers with oral ranitidine should be 3 years of age.
8.1.3.2 For the intravenous formulation
The submitted pharmacokinetic data, although limited, were consistent in
children aged 6 months and above.
There are no significant safety issues in any age group
It is therefore proposed that the lower age limit for the short term
treatment of peptic ulcers with oral ranitidine should be 6 months of age.
8.1.4 Proposed dosage and method of administration
8.1.4.1Intravenous (IV) ranitidine
The MAH proposes the following regimen for IV ranitidine for children aged 1
month to 16 years:

47
SmPc Section 4.2 Posology and Method of administration (See section 5.2
Pharmacokinetic properties- Special patient Populations)
Zantac injection may be given as slow (over 2 minutes) i.v injection up to a
maximum of 50mg every 6 to 8 hours.
Peptic ulcer-Acute treatment: the recommended dose for the treatment of
peptic ulcer in children is 2 mg/kg/day to 4 mg/kg/day administered as 3 or 4
divided doses.
In section 4.2 for adults and children over 12 years of age only, the SmPC
states the following:
Zantac injection may be given either as slow (over a period of at least 2
minutes) intravenous injection of 50mg, after a dilution to a volume of at
least 20ml per 50mg dosage, which may be repeated every 6- 8 hrs, or as an
intermittent infusion at a rate of 25mg per hour for 2 hours.
The dosage regimen suggested in the BNF for Children ( BNFC, 2005) is as
follows:
By slow intravenous injection
Neonate: 0.5–1mg/kg every 6–8 hours
Child 1 month–18 years: 1mg/kg (max. 50mg) every 6–8 hours (may be
given as an intermittent infusion at a rate of 25mg/hour)
By continuous intravenous infusion
Neonate: 30–60micrograms/kg/hour (max. 3mg/kg daily)
Child 1 month–18 years: 125–250micrograms/kg/hour
Administration
For slow intravenous injection dilute to a concentration of 2.5mg/mL with
sodium chloride 0.9%, glucose 5% or compound sodium lactate intravenous
infusion. Give over at least 3 minutes.
For continuous intravenous infusion, further dilution is required.
Comments:
In the posology for children under 12 years of age, dilution for slow
injection is not recommended;
In addition, there are no details regarding infusion (intermittent or
continuous) in this age group
The proposed dosage (2-4mg/kg for slow injection) is consistent with the
available pharmacokinetic and pharmacodynamic data. The proposed
dosage regimen is similar to that suggested in the BNFC.
The dosage regimen proposed by the MAH is reasonable. However, a
dosage regimen for infusion should be provided, in addition to details
about dilution.
27
8.1.4.2 Oral formulations
The MAH proposes the following dosing regimen for oral ranitidine for the
treatment of acute peptic ulcer:
4-8 mg/kg/day, in 2 divided doses to a maximum of 300 mg/day
The dosage regimen suggested in the BNF for Children ( BNFC, 2005) is as
follows:
By mouth
Neonate: 1–2mg/kg 3 times daily but absorption unreliable (initially 2mg/kg 3
times daily for gastro-oesophageal reflux)
Child 1–6 months: 1 mg/kg 3 times daily (max. 9mg/kg daily in divided
doses)
6 months–12 years: 2–4 mg/kg (max. 150mg) twice daily
12–18 years: 150 mg twice daily

48
Comments
The dosage proposed by the MAH (4-8mg/kg/day) is consistent with the
available pharmacokinetic and pharmacodynamic data. The proposed
dosage regimen is similar to that suggested in the BNFC.
9. OVERALL CONCLUSIONS The submitted data for the proposed indications were extremely
disappointing, even though several studies had been sponsored by the
applicant. In particular, no randomised controlled trial had been
undertaken in children with gastro-oesophageal reflux, which should not
have been difficult to perform. However, in the case of prophylaxis of
stress ulceration in seriously ill children, it is recognised that it would be
difficult to undertake randomised controlled trials.
There were no randomised controlled trials submitted for the following
proposed indications: the treatment of gastro-oesophageal reflux
(including reflux oesophagitis and the symptom relief of gastro-
oesophageal reflux disease) and the prophylaxis of stress ulceration in
seriously ill patients. For these indications, the submitted clinical
guidelines recommend the use of ranitidine. However, these
recommendations do not appear to be evidence based.
The only double blind randomised controlled trial that was submitted for
the prevention of duodenal ulcer was poorly designed, as it did not
consider the presence of H.pylori in participants. This may have been
because this trial was undertaken in 1994, prior to the understanding of
the importance of this in the pathogenesis of peptic ulceration in children.
Even taking this into consideration, robust evidence of efficacy was not
provided because of the low rate of relapse in the placebo group and the
lack of clinical symptoms in either group after treatment. 28
It is therefore considered that there is inadequate evidence of a favourable
risk/benefit profile for the following proposed indications: the long term
management of peptic ulcer and the treatment of gastro-oesophageal
reflux (including reflux oesophagitis and gastro-oesophageal reflux
disease) from 1 month of age and above and the prevention of stress
ulcers in seriously ill children.
However, the CHM may consider that as the oral formulations are already
licensed for the short term treatment of peptic ulceration in children, and
that there is no evidence of any safety concern, that the risk/ benefit
assessment is favourable for this indication for the injection formulation.
In addition, a safer alternative to the oral liquid formulation is required for
young children as it has a high alcohol content (8%). The MAH has agreed
to submit a variation to add a precautionary statement to the SmPC but
this is not considered to be adequate.
The lack robust of efficacy data for GORD has been highlighted particularly
with respect to cisapride, and more recently with domperidone and
lanzoprazole and omeprazole. The quality of submitted data for ranitidine
further emphasises the need for appropriately designed studies to be
undertaken in this common condition.
10. MINUTES OF DISCUSSION BY COMMISSION ON HUMAN
MEDICINES Expert advice was provided by a consultant paediatric gastroenterologist. The
Commission considered that the use of ranitidine was well established,
particularly for the treatment of gastro-oesophageal reflux and the prevention
of stress ulcers in seriously ill children and that there was no safety issues
associated with its use in children. It was also considered that it would be
difficult to persuade the company to undertake clinical trials for these
49
conditions in children. However, the Commission noted that there were
insufficient data regarding dosage to warrant extrapolation from adults for
prevention of stress ulcers. The Commission considered that should further
dosage data be provided, that it would be possible to consider granting this
indication. With regard to the indication for the treatment of gastro-
oesophageal reflux, the Commission considered that there were sufficient
published data of acceptable quality to grant this.
The submitted data for the indication for the long term treatment of peptic
ulcer was considered to be poor and this condition is uncommon in children.
In addition, current practice for the treatment of peptic ulceration does not
generally support the use of H2 antagonists for long periods. The Commission
therefore advised that this indication should be refused.
There was some discussion with regard to the alcohol content of ranitidine
syrup. It was considered that although this concentration should not pose any
serious risk to children, the ethanol should not be used in paediatric
formulations unless this was necessary.
11. FINAL ADVICE OF COMMISSION 1. On the evidence before them, the Commission advised that the variation
application to the Marketing Authorisation for Zantac tablets/
injection/syrup:
2. Should be refused for the indication for the long term treatment of peptic
ulcer.
3. Should be refused for the indication for the prophylaxis of stress ulceration
in seriously ill patients for the injection formulation.
4. Should be granted for the indication for the treatment of gastro-
oesophageal reflux (including reflux oesophagitis and the symptom relief
of gastro-oesophageal reflux disease).
5. Should be granted for the indication for the short term treatment of peptic
ulcers for the injection formulation for children in whom oral therapy is
unsuitable.
6. The Commission considered that:
7. There is inadequate evidence of efficacy for the indication for: the long
term treatment of peptic ulcer and that this condition is uncommon in
children.
8. There is inadequate evidence of efficacy for the indication for gastro-
oesophageal reflux (including reflux oesophagitis and the symptomatic
relief of gastro-oesophageal reflux disease) but the clinical experience of
the use of ranitidine is well established for this condition and there are no
known safety concerns.
9. Although there is inadequate evidence of efficacy for the indication for:
the prophylaxis of stress ulcers, it would be difficult to undertake a clinical
trial in this situation, which is a common and serious problem in children.
However, there are insufficient data regarding dosage to warrant
extrapolation from adult data.
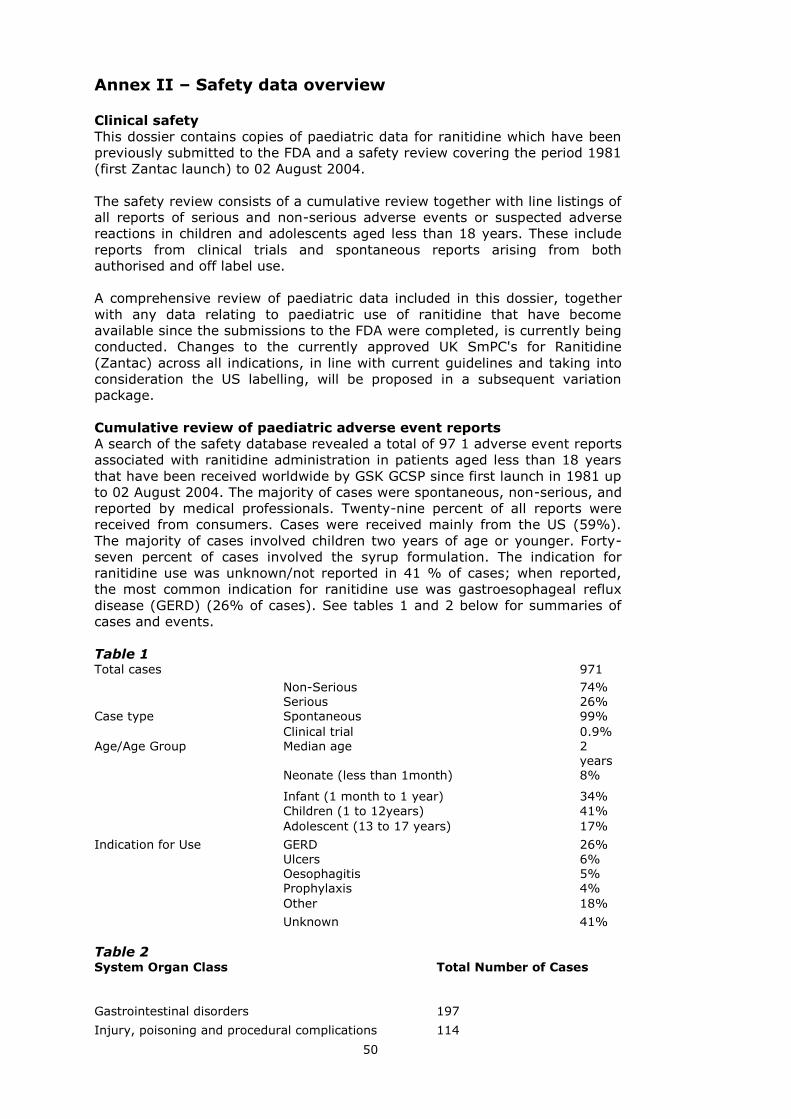
50
Annex II – Safety data overview Clinical safety
This dossier contains copies of paediatric data for ranitidine which have been
previously submitted to the FDA and a safety review covering the period 1981
(first Zantac launch) to 02 August 2004.
The safety review consists of a cumulative review together with line listings of
all reports of serious and non-serious adverse events or suspected adverse
reactions in children and adolescents aged less than 18 years. These include
reports from clinical trials and spontaneous reports arising from both
authorised and off label use.
A comprehensive review of paediatric data included in this dossier, together
with any data relating to paediatric use of ranitidine that have become
available since the submissions to the FDA were completed, is currently being
conducted. Changes to the currently approved UK SmPC's for Ranitidine
(Zantac) across all indications, in line with current guidelines and taking into
consideration the US labelling, will be proposed in a subsequent variation
package.
Cumulative review of paediatric adverse event reports
A search of the safety database revealed a total of 97 1 adverse event reports
associated with ranitidine administration in patients aged less than 18 years
that have been received worldwide by GSK GCSP since first launch in 1981 up
to 02 August 2004. The majority of cases were spontaneous, non-serious, and
reported by medical professionals. Twenty-nine percent of all reports were
received from consumers. Cases were received mainly from the US (59%).
The majority of cases involved children two years of age or younger. Forty-
seven percent of cases involved the syrup formulation. The indication for
ranitidine use was unknown/not reported in 41 % of cases; when reported,
the most common indication for ranitidine use was gastroesophageal reflux
disease (GERD) (26% of cases). See tables 1 and 2 below for summaries of
cases and events.
Table 1 Total cases 971
Non-Serious 74% Serious 26% Case type Spontaneous 99%
Clinical trial 0.9% Age/Age Group Median age 2
years Neonate (less than 1month) 8%
Infant (1 month to 1 year) 34%
Children (1 to 12years) 41%
Adolescent (13 to 17 years) 17%
Indication for Use GERD 26%
Ulcers 6% Oesophagitis 5% Prophylaxis 4%
Other 18%
Unknown 41%
Table 2 System Organ Class Total Number of Cases
Gastrointestinal disorders 197
Injury, poisoning and procedural complications 114

51
Nervous system disorders 104
Skin and subcutaneous tissue disorders 87
Psychiatric disorders 81
General disorders and administration site conditions 77 Investigations 50 Blood and lymphatic system disorders 39
Respiratory, thoracic and mediastinal disorders 35 Hepatobiliary disorders 27 Reproductive system and breast disorders 24
Immune system disorders 23 Cardiac disorders 18 Infections and infestations 17 Renal and urinary disorders 17 Musculoskeletal and connective tissue disorders 16
Eye disorders 15
Metabolism and nutrition disorders 9 Vascular disorders 7
Endocrine disorders 4 Congenital, familial and genetic disorders 4
Surgical and medical procedures 3
Ear and labyrinth disorders 3 Total Number of Cases 971
As shown in Table 2, the most common MedDRA System Organ Classes
(SOCs) for the reported adverse events include Gastrointestinal disorders
(20%), Injury, poisoning and procedural complications (12%), and Nervous
system disorders (1 1%).
Gastrointestinal Disorders
The most commonly reported gastrointestinal events were vomiting (116
reports), diarrhoea (a listed event, 41 reports), and abdominal pain (37
reports). Overall, the majority of such reports were non-serious and resolved
or improved at the time of reporting. A number of cases of vomiting and
abdominal pain were reported in association with an overdose of ranitidine or
confounded by co-suspect medications or underlying medical conditions. In
addition, many cases of vomiting we e reported as associated with the taste
of the medication (mainly the syrup). These cases also may be related to the
disease state being treated.
Injury, Poisoning, and Procedural Complications
The majority of cases in the Injury, poisoning, and procedural complications
SOC described overdose of ranitidine. Most of these cases were non-serious
and involved a medication error. Thirty-three percent of overdose cases did
not report adverse events. Of the cases reporting medication error, 16%
reported that the syrup was administered intravenously. Only two of these
cases reported adverse events (all nonserious); one case reported
hypertension in a patient with a history of blood pressure fluctuations just
prior to ranitidine administration and the other case reported injection site
erythema. Ten cases of medication error reported that cetirizine (Zyrtec) was
given instead of ranitidine and in four cases the patient received ranitidine
instead of cetirizine; all cases were non-serious and the most common events
that occurred were vomiting and somnolence.
Nervous System Disorders
The most commonly reported events in the nervous system disorders SOC
included tremor (21 reports), headache (a listed event, 26 reports), seizure
(25 reports) and somnolence (38 reports). Cases of seizure were either
confounded by CO-suspect or concurrent medications andlor underlying
medical problems (e.g. epilepsy, vomiting, prematurity). Most cases of
somnolence were non-serious and were confounded by either a dispensing

52
error, concurrent medications (e.g. clonazeparn, phenobarbitone), underlying
medical conditions (e.g. apnoea), or symptom of another event (e.g.
anaphylaxis, a cold). Several cases of somnolence were reported in
association with an overdose of ranitidine. The majority of cases of headache
and tremor were nonserious and resolved or improved at the time of
reporting. Most cases of tremor were confounded by CO-suspect or concurrent
medications (e.g. cisapride, metocloprarnide) or significant medical history
(e.g. seizures) or were reported in association with overdose or convulsion.
Reversible involuntary movement disorders is a listed event in the ranitidine
Global Datasheet.
Other events
Forty-five reports of rash were received. The majority of cases were non-
serious and resolved or improved at the time of reporting. Rash is a listed
event in the ranitidine Global Datasheet. Twenty-two cases of pyrexia were
received with 18 cases reported as serious. The majority of cases described
pyrexia as a symptom of another event (e.g. infection, hypersensitivity
reaction) or were confounded by significant medical history (e.g. liver
transplant, leukaemia). Almost half of the cases were reported as resolved or
improved.
Reports of crying (25 reports), irritability (37 reports), and insomnia (26
reports) were also received. The majority of these cases were non-serious and
involved patients less than 2 years in age with gastroesophageal reflux. In
addition, most cases were confounded by CO-suspect or concurrent
medications (e.g. cisapride, hyoscyarnine, steroids, vaccines) or underlying
medical conditions (e.g. nervousness, global developmental delay) and were
resolved or improved at the time of reporting. These events are also
symptoms of infants with GERD and may be related to their underlying
disease.
Conclusion
Cases involving paediatric patients (n=971) represent about 5% of all
ranitidine cases in the GCSP safety database. The majority of the 971 cases
were non-serious, spontaneous reports received from medical professionals
and described patients 2 years of age or younger. Most patients received
ranitidine to treat a condition (e.g. GERD, ulcer) for which some of the
reported events (e.g. vomiting, irritability, abdominal pain, crying, insomnia)
could be a symptom. Review of the most commonly reported events in cases
received up to 02 August 2004 did not highlight any safety issues for
paediatric patients.
53
Annex III: Cited references
Oral Ranitidine Oderda G, Altare F, Dell’Olio D et al. Prognostic value of serum pepsinogen I in children with peptic ulcer. Pediatr Gastroenterol Nutr 1988; 7: 645-650. Socha J, Rondio H, Chaba-Celinksa D et al. Ranitidine treatment of peptic and related diseases in children. In: Misiewicz JJ, Wormsley KG, eds. The Clinical Use of Ranitidine: Medicine Publications Foundation 1982; 305=309.
Angelis de GL, Banchini G. Ranitidine in paediatric patients – personal experience. Clin Trials J 1989; 26: 370-375. Scorza A, Conti-Nibali S, Sferlazzas C, et al. Ranitidine in children with peptic ulcer and patients with pancreatic cystic fibrosis. Int J Clin Pharmacol Res 1990; 10: 179-
182. Minella R, Basile P, Stalano A et al. Ranitidine treatment in podiatry. Medicina
Universalis 1989; 2: 1-5. Accadia L, Federici T, Gabrielle L. Primary duodenal ulcer in children. Follow-up and long term therapy of 12 cases [in Italian]. Minerva Pediatrica 1986; 38: 413-415.
Deganello A, Tamassia G, Gaburro D. Peptic disease in paediatric patients: a diagnostic and therapeutic contribution. Drugs Experiment Clin Res 1990; 16: 75-83. Tadi M et al. Clinical efficacy of ranitidine in the treatment of paediatric duodenal ulcer [in Japanese]. Jap J Pediatr 1984; 37: 405-408.
Murphy MS, Eastham EJ, Jimenez M, et l. Duodenal ulceration: review of 110 cases. Arch Dis Childhood 1987; 62: 554-558. Tam PKH, Saing H. The use of H2-receptor antagonist in the treatment of peptic ulcer disease in children. J Pediatr Gastroenterol Nutr 1989; 8: 41-46.
Cordone G, Venzano V, Ricci F, et al. Ranitidine in primary peptic ulcer in childhood complicated by acute hemorrhage [in Italian]. Pediatr Med Chir 1986; 8: 85-88. Oderda G, Ansaldi N. Peptic ulcers in childhood. Lancet 1988; 1(8580): 302-303. Oderda G, Farina L, Ansalid N. Peptic ulcer in children: 5 years follow-up after ranitidine therapy. Pediatr Res 1988; 24: 417.
Karjoo M, Kane R. Omeprazole treatment of children with peptic esophagitis refractory to ranitidine therapy. Arch Pediatr Adolesc Med 1995; 149: 267-271. Rosioru C, Glassman MS, Halata MS et al. Esophagitis and Helicobacter pylori in children: incidence and therapeutic implications. Am J Gastroenterol 1993; 88: 510-513.
Berezin S, Medow MS, Glassman MS, et al. Chest pain of gastroenterological origin.
Arch Dis Child 1988; 63: 1457-1460. Berezin S, Medow MS, Glassman M, et al. Use of the intra-esophageal acid perfusion test in provoking non-specific chest pain in children. J Pediatr 1989: 115: 709-712.
Berezin S, Medow MS, Glassman MS, et al. Esophageal chest pain in children with asthma. J Pediatr Gastroenterol Nutr 1991; 12: 52-55. Mallet E, Mouterde O, Dubois F, et al. Use of ranitidine in young infants with gastro-oesophageal reflux. Eur J Clin Pharmacol 1989; 36: 641-642.
Caffarena PE, Bisio G, Cappuccio G, et al. The use of ranitidine syrup in paediatric surgery [in Italian]. Rass Ital Chir Pediatr 1990; 32 (2): 81-9.

54
Rylance G. The use of ranitidine in paediatric gastroenterology. In: Perspective on
Therapeutics in Northern Europe: Hyperaciditiy States, London 1987; No 52: 4-5.
Cucchiara S, Minella R, Iervolino, et al. Omeprazole and high dose ranitidine in the treatment of refractory reflux oesophagitis. Arch Dis Child 1993; 69: 655-659. Treem WR, Davis PM, Hyams JS. Gastroesophageal reflux in the older child:
presentation, response to treatment and longterm follow-up. Clin Pediatr 1991; 30: 435-550. Taylor G, Taylor S, Abrams R et al. Dental erosion associated with asymptomatic gastroesophageal reflux. ASDC J Dent Child 1992; 59: 182-185. Baron TH, Richter JE, Singh S, et al. Unusual presentation of mucosal hypersensitivity
secondary to gastroesophageal reflux disease. Am J Gastroenterol 1993; 88 (2): 289-292. Sarda H, Allisy C, Le Loc’h H, et al. Effectiveness of omeprazole in treatment of refractory ulcerative oesophagitis (Letter) [in French]. Arch Fr Pediatr 1993; 50: 83.
Zaatar R, Younoszai MK, Mitros F. Pseudo Zollinger-Ellison syndrome in a child
presenting with anaemia. Gastroenterology 1987; 92: 508-512. De Giacomo C, Fiocca R, Villani L, et al. Omeprazole treatment of severe peptic disease associated with antral G cell hyperfunction and hyperpepsinogenemia I in an infant. J Pediatr 1990; 117: 989-993.
Hyman PE, Hassall E. Marked basal gastric acid hypersecreation and peptic ulcer disease medical management with a combination of H2-histamine receptor antagonist and anticholinergic. J Pediatr Gastroenterol Nutr 1988; 7: 57-63. Sutphen JL, Dillard VL. Effect of ranitidine on twenty-four hour gastric acidity in infants.
J Pediatr 1989; 114: 472-474.
Balestrazzi P, Gregori G, Bernasconi S, et al. Bradycardia and neurological disorders associated with ranitidine in a child. Am J Dis Child 1985; 139: 442. Gustafsson PM, Kjellman N-IM, Tibbling L. A trial of ranitidine in asthmatic children and adolescents with or without pathological gaster—oesophageal reflux. Eur Respir J
1992; 5: 201-206. Goresky GV, Finley GA, Bissonnete B, et al. Efficacy, duration, and absorption of a paediatric oral liquid preparation of ranitidine hydrochloride. Can J Anaesth 1992; 39: 791-798.
Hermaszewski R, Hayllar J, Woo P. Gastro-duodenal damage due to non-steroidal anti-inflammatory drugs in children. Br J Rheumatol 1993; 32: 69-72. De Giacomo C, Maggiore G, Scotta MS. Ranitidine and loss of colour vision in a child.
Lancet 1984; 2 (8393): 47. Maak DK, Spiller HA. Rare dystonic reaction from accidental overdose of ranitidine in
a 3 month old. Vet Hum Toxicol 1993; 35: 343. Dubois A, Bruossine L, Blayo M, et al. Lethargy in a neonate treated with ranitidine [in French]. Pédiatrie 1993; 48: 335-336. Parenteral Ranitidine Leeder JS, Brill-Edwards M, Chin T, et al. Pharmacokinetics of ranitidine in paediatric
patients. Acta Pharmacol Toxicol 1986; 59: 79 (abstract). Blumer JL, Rothstein FC, Kaplan BS, et al. Pharmacokinetic determination of ranitidine pharmacodynamics in paediatric ulcer disease. J Pediatr 1985; 107: 301-306.

55
Leeder JS, Harding L, MacLeod SM. Ranitidine pharmacokinetics in children. Clin Pharmacol Therap 1985; 37: 201 (abstract A23).
Hyman PE, Abrams C, Garvey TQ. Ranitidine tachyphylaxis. Gastroenterol 1985; 88: 1426 (abstract).
Hyman PE, Garvey TQ, Harada T. Effect of ranitidine on gastric acid hypersecretion in an infant with short bowel syndrome. J Pediatr Gastroenterol Nutr 1985; 4: 316-319. Fontana M, Tornaghi R, Petrillo M, et al. Ranitidine treatment in newborn infants: effects on gastric acidity and serum prolactin levels. J Ped Gastroenterol Nutr 1993; 16: 406-11.
Lopez-Herce J, Dorao P, Elola P, et al. Frequency and prophylaxis of upper gastrointestinal hemorrhage in critically ill children: a prospective study comparing the efficacy of almagate, ranitidine and sucralfate. Crit Care Med 1992; 20: 1082-1089. Agura ED, Vila E, Petersen FB, et al. The use of ranitidine in bone marrow
transplantation. Transplantation 1988; 46: 53-6.
Nahum E, Reish, Naor N, et al. Ranitidine-induced bradycardia in a neonate – a first report. Eur J Pediatr 1993; 152: 933 – 34. Bush A, Busst CM, Knight WB, et al. Cardiovascular effects of tolazoline and ranitidine. Arch Dis Child 1987; 62: 241-46.
Rylance G. The use of ranitidine in paediatric gastroenterology. In: Perspectives on therapeutics in Northern Europe: hyperacidity states, London 1987; 52: 4-5. Skinner MH, Lenert L, Blaschke TF. Theophylline toxicity subsequent to ranitidine: a possible drug-drug interaction. Am J Med 1989; 86: 129-32.
Behrman RE, Kliegman RM. Nelson Essentials of Pediatrics, Fourth Edition. Saunders
Company, 2002, pp 469-513. Cezard JP. Managing gastro-oesophageal reflux disease in children. Digestion 2004; 69 (suppl 1): 3-8. Dimand RJ, Burckart G, Concepcion W et al Pharmacokinetics of Continuous Infusion
Ranitidine in Postoperative Paediatric Liver Transplant Patients: Intragastric pH, Bleeding and Metabolic Alkalosis. Gastroenterology 1989; 5(2): A125 Eddleston JM, Booker PD, Green JR Use of Ranitidine in Children Undergoing Cardiopulmonary Bypass. Critical Care Medicine 1989; 17(1): 26-9
Goyal A, Treem WR, Hyams JS. Severe upper gastrointestinal bleeding in healthy full-term neonates. Am J Gastroenterol 1994;89:613-616. Gryboski D. Peptic ulcer disease in children. Medical Clinics of North America 1991;
75(4): 889-902 Harrison AM et al Gastric pH control in critically ill children receiving intravenous
ranitidine. Crit. Care Med 1998;26(8):1433-1436 Hartemann E, Berthier JC, Gerbier F Assessment of Intragastric pH in Critically Ill Children. Effects of Ranitidine. Intensive Care Med. 1987; 13(6): 448 Hathway WE and Hay WW. Current Pediatric Diagnosis and Treatment, Eleventh Edition.
Appleton and Lange, 1992, pp 528 – 558. Kelly DA. Do H2 receptor antagonists have a therapeutic role in childhood? J Pediatr Gastroenterol Nutr 1994; 19: 270-276.
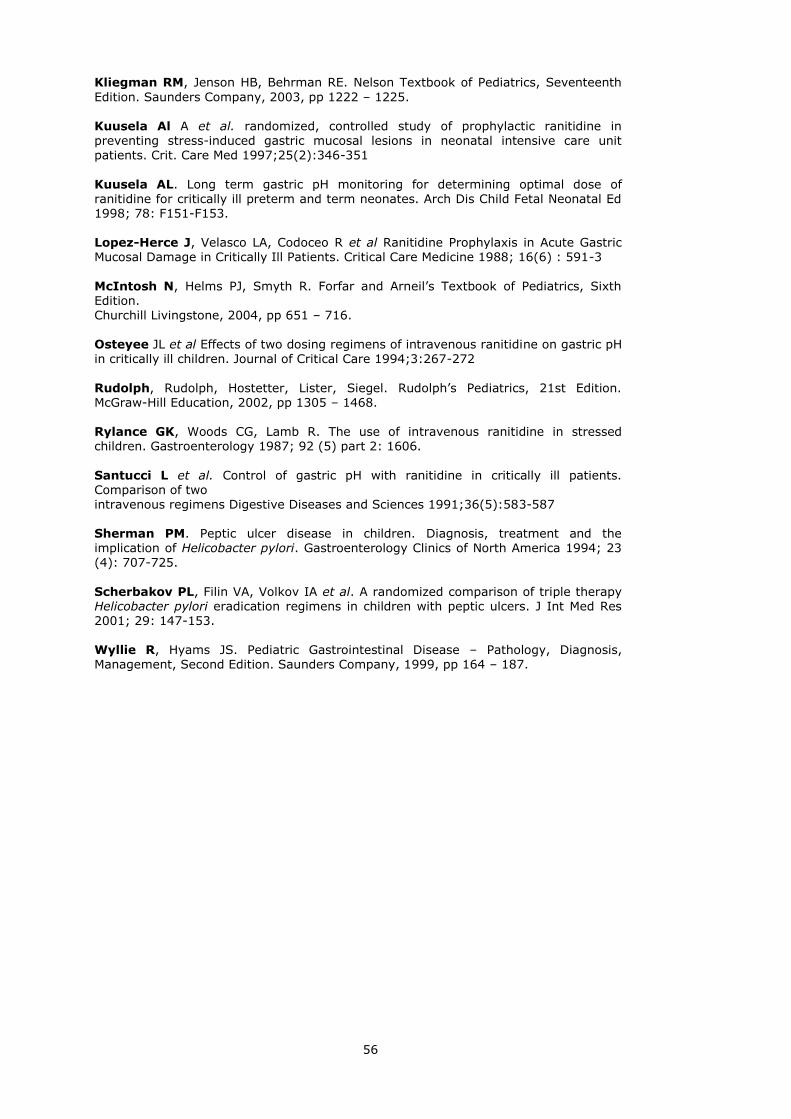
56
Kliegman RM, Jenson HB, Behrman RE. Nelson Textbook of Pediatrics, Seventeenth
Edition. Saunders Company, 2003, pp 1222 – 1225.
Kuusela Al A et al. randomized, controlled study of prophylactic ranitidine in preventing stress-induced gastric mucosal lesions in neonatal intensive care unit patients. Crit. Care Med 1997;25(2):346-351
Kuusela AL. Long term gastric pH monitoring for determining optimal dose of ranitidine for critically ill preterm and term neonates. Arch Dis Child Fetal Neonatal Ed 1998; 78: F151-F153. Lopez-Herce J, Velasco LA, Codoceo R et al Ranitidine Prophylaxis in Acute Gastric Mucosal Damage in Critically Ill Patients. Critical Care Medicine 1988; 16(6) : 591-3
McIntosh N, Helms PJ, Smyth R. Forfar and Arneil’s Textbook of Pediatrics, Sixth Edition. Churchill Livingstone, 2004, pp 651 – 716. Osteyee JL et al Effects of two dosing regimens of intravenous ranitidine on gastric pH
in critically ill children. Journal of Critical Care 1994;3:267-272
Rudolph, Rudolph, Hostetter, Lister, Siegel. Rudolph’s Pediatrics, 21st Edition. McGraw-Hill Education, 2002, pp 1305 – 1468. Rylance GK, Woods CG, Lamb R. The use of intravenous ranitidine in stressed children. Gastroenterology 1987; 92 (5) part 2: 1606.
Santucci L et al. Control of gastric pH with ranitidine in critically ill patients. Comparison of two intravenous regimens Digestive Diseases and Sciences 1991;36(5):583-587 Sherman PM. Peptic ulcer disease in children. Diagnosis, treatment and the implication of Helicobacter pylori. Gastroenterology Clinics of North America 1994; 23 (4): 707-725.
Scherbakov PL, Filin VA, Volkov IA et al. A randomized comparison of triple therapy Helicobacter pylori eradication regimens in children with peptic ulcers. J Int Med Res 2001; 29: 147-153. Wyllie R, Hyams JS. Pediatric Gastrointestinal Disease – Pathology, Diagnosis, Management, Second Edition. Saunders Company, 1999, pp 164 – 187.





























