Embed Size (px)
Citation preview
Zeljko Dujic, MD, PhD
Department of Integrative Physiology, University of Split School of Medicine, Croatia
Presentation outline
Breath hold diving
a) Historical overviewb) Challenging the traditional
conceptsc) Physiological diving responsed) Hemodynamic impactse) Similarities to OSA

Historical overview of breath-hold diving
Reaches long ago in the past (fishing, collection of sponges and pearls)
Ama divers – 2 000 years ago
After World War II became an international sport
Apnea disciplines and current records
Static apneaWorld record: 11 min 35 sec
Dynamic apneaWorld record: 265 m
Constant weightWorld record: 123 m
No limitWorld record: 214 m

Diving depth:Diving depth:
Boyle’s law (the volume Boyle’s law (the volume toto which compressed which compressed gas gas is reduced due to increase in surrounding is reduced due to increase in surrounding pressurepressure))
TThe influence of the hydrostatic pressure on the he influence of the hydrostatic pressure on the chest wall, heart and arterieschest wall, heart and arteries
PProfessional breath hold diver, rofessional breath hold diver, - TLC on the surface 9.6 l, RV 2.2 l- TLC on the surface 9.6 l, RV 2.2 l- on the depth of 133 msw - on the depth of 133 msw accordingaccording Boyle’s law Boyle’s law TLC TLC should be reduced to should be reduced to 0.67 l?0.67 l?- collapse of the lungs?- collapse of the lungs?
RRedistribution of the blood from the periphery edistribution of the blood from the periphery toto the intrathoracic vascular pool and heart the intrathoracic vascular pool and heart (more than 1 liter) under the influence of the (more than 1 liter) under the influence of the increasedincreased hydrostatic pressure hydrostatic pressure
FFor the enlargement of maximal diving depth, or the enlargement of maximal diving depth, diver begins with the largest volume of the air in diver begins with the largest volume of the air in the lungs (squeezing out the blood from intrathe lungs (squeezing out the blood from intra--thoracic vascular pool before dive)thoracic vascular pool before dive)
AAma exhalation through the whistlema exhalation through the whistle
AAir packaging in lungs (squeezes out the blood ir packaging in lungs (squeezes out the blood and increases VC from 22-39 %)and increases VC from 22-39 %) Danger: rupture Danger: rupture of the alveolof the alveolii and loss of the consci and loss of the consciousnessousness
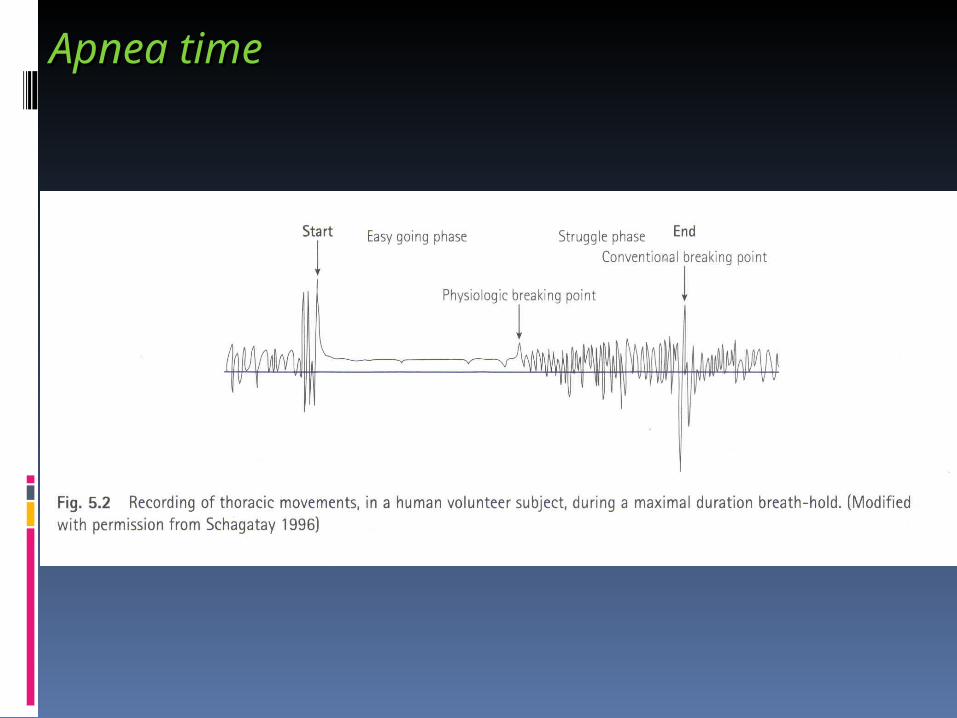
Apnea timeApnea time
Apnea time depends Apnea time depends on following on following parametersparameters::
1.1. PPhysiologic hysiologic response to response to hypercapnia and hypercapnia and hypoxiahypoxia
2. I2. Intensity of metabolism (assisted dives-ntensity of metabolism (assisted dives-pendulums, cold water pendulums, cold water increases 3 fold O2 increases 3 fold O2 consumptionconsumption))
3. C3. Capacities apacities for for O2 and CO2 (TLC, training - O2 and CO2 (TLC, training - larger activity of the anaerobic and larger activity of the anaerobic and reduced aerobic metabolism,reduced aerobic metabolism, hyperventilation) hyperventilation)
4. P4. Psychological tolerability sychological tolerability to hypercapnia to hypercapnia and and hypoxia hypoxia
Physiological challenges during apnea diving
Physiological/psychological response to hypoxia and hypercapnia
PaO2 – 30 mmHg, SaO2 – 50%, PaCO2 – 55 mmHg
Extreme ambient hydrostatic pressure Barotrauma at descent and ascent Pulmonary edema and alveolar hemorrhage
Increased gas uptake and nitrogen supersaturation N2 narcosis Decompression sickness (Deco stops)
From Lindholm & Lundgren, J Appl Physiol. 2009 Jan;106(1):284-92.
Diving responseDiving response
Paul Bert (1870) Paul Bert (1870) reported reduced heart reported reduced heart rate (rate (bradycardiabradycardia)) inin forcefullyforcefully div divinging ducksducks
NNumerous animal (birds and mammals) umerous animal (birds and mammals) and and human researchhuman research
Human Diving response
1.1. Changes of cardiac rhythm (bradycardia)Changes of cardiac rhythm (bradycardia)
2.2. Peripheral vasoconstriction and Peripheral vasoconstriction and redistribution of blood to the central blood redistribution of blood to the central blood reservoirreservoir
3.3. Arterial pressure increaseArterial pressure increase
4.4. Reduction of cardiac outputReduction of cardiac output
5.5. Contraction of the spleen? (observation from Contraction of the spleen? (observation from our laboratory)our laboratory)
1. Changes in cardiac rhythm
Initial anticipatory tachycardia (stimulation Initial anticipatory tachycardia (stimulation of the lungof the lung mechanoreceptors; mechanoreceptors; hyperventilation; excitement?)hyperventilation; excitement?)
Increased parasympathetic inputIncreased parasympathetic input t to SA node o SA node (Irving 1963.)(Irving 1963.)
immersion of the face in the cold waterimmersion of the face in the cold water
enlargement of venous inflow and enlargement of venous inflow and distention of heart cavitiesdistention of heart cavities
Arrhythmias (bradyarrhythmia and extraArrhythmias (bradyarrhythmia and extra beats)beats)
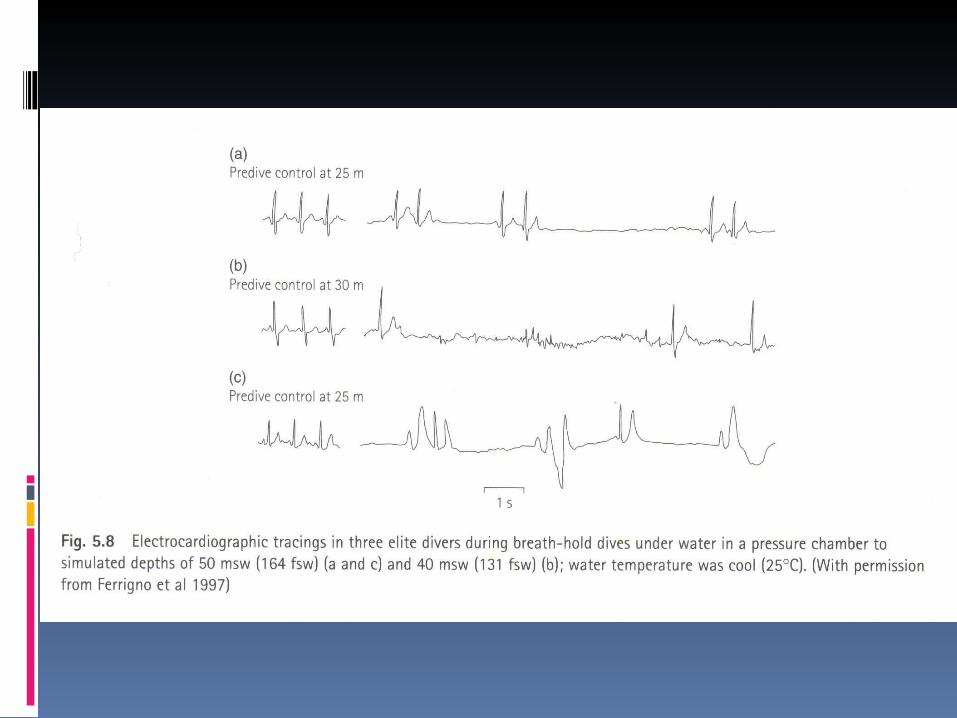
Slika 5.8
2. Peripheral vasoconstriction and blood redistribution
Increased sympathetic outflow to the Increased sympathetic outflow to the periphery – reduced blood flow to the periphery – reduced blood flow to the peripheral tissues and skinperipheral tissues and skin
AAnaerobic metabolism on the peripherynaerobic metabolism on the periphery (lactate increase)(lactate increase)
Blood centralization to the brain and heartBlood centralization to the brain and heart
100 % increase of cerebral flow through 100 % increase of cerebral flow through middle cerebral artery (MCA)middle cerebral artery (MCA)
significant increase of significant increase of blood blood flow through the carotid arteryflow through the carotid artery
100 % ↑ of the cerebral flow 100 % ↑ of the cerebral flow throthrough middle cerebral artery ugh middle cerebral artery (M(MCACA)) with ultrasound (TCD) with ultrasound (TCD)
COCO22 retention - cerebral retention - cerebral vasodilatation - prevention of vasodilatation - prevention of hypoxic damageshypoxic damages
cerebral desaturationcerebral desaturation

OSA
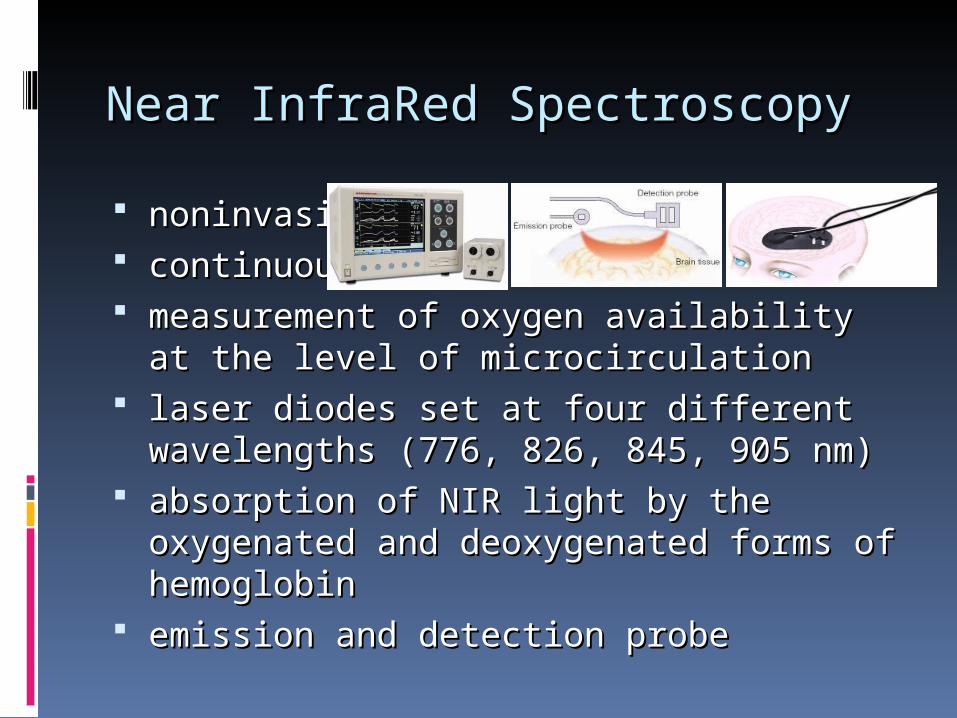
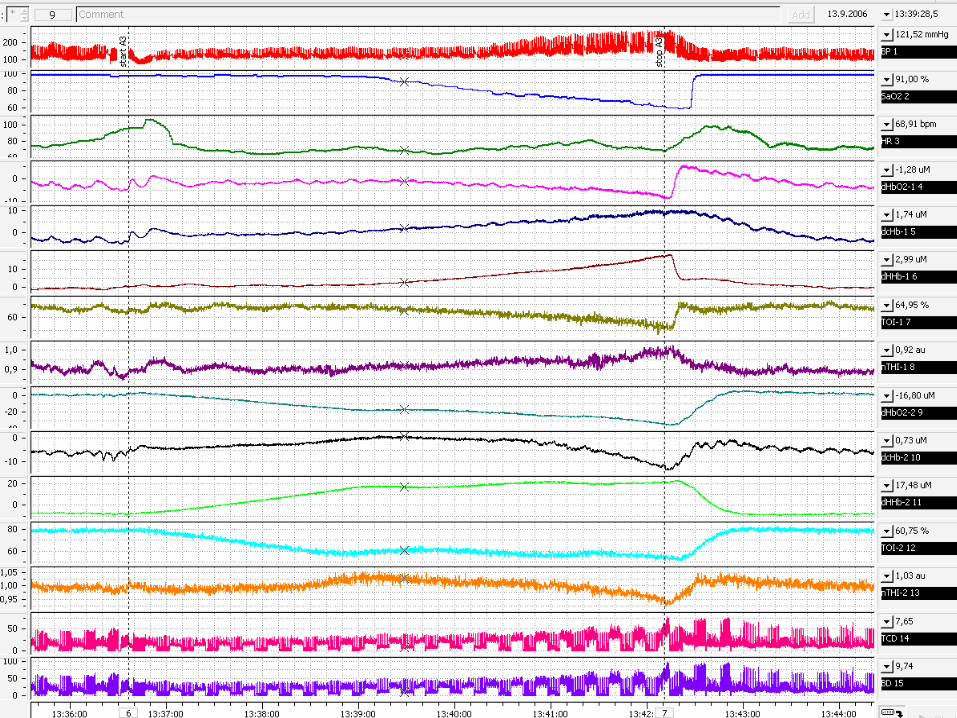
Near InfraRed SpectroscopyNear InfraRed Spectroscopy
noninvasivenoninvasive continuous continuous measurement of measurement of oxygen availability at the oxygen availability at the
level of microcirculation level of microcirculation laser diodes set at four different laser diodes set at four different
wavelengths (776, 826, 845, 905 nm)wavelengths (776, 826, 845, 905 nm) absorption of NIR light by the oxygenated absorption of NIR light by the oxygenated
and deoxygenated forms of hemoglobin and deoxygenated forms of hemoglobin emiemission and detection probession and detection probe

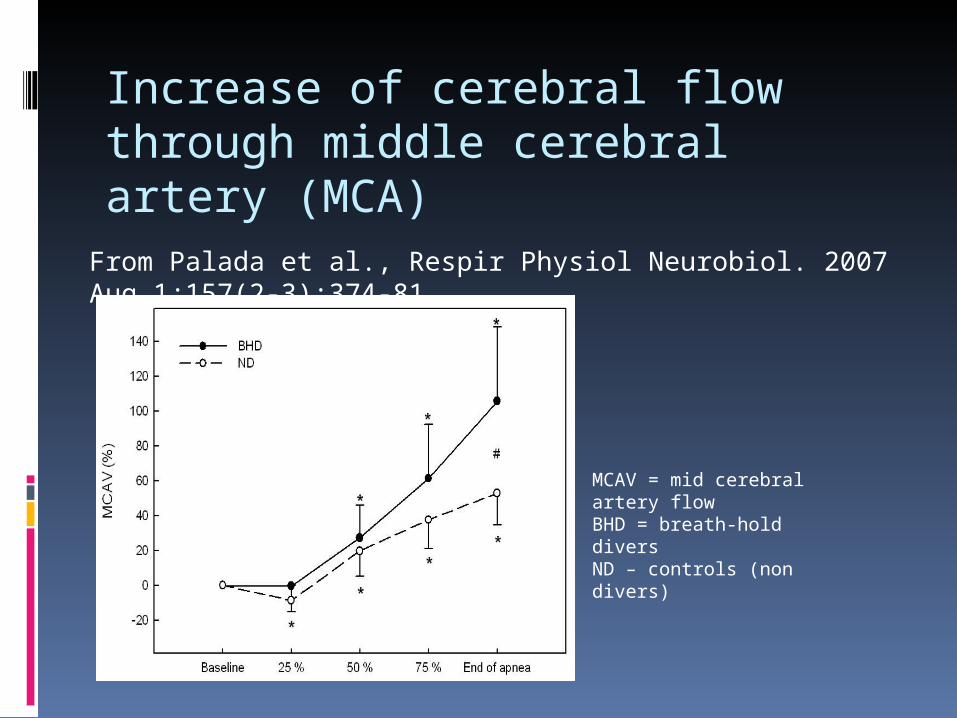
From Palada et al., Respir Physiol Neurobiol. 2007 Aug 1;157(2-3):374-81
MCAV = mid cerebral artery flowBHD = breath-hold diversND – controls (non divers)
Increase of cerebral flow through middle cerebral artery (MCA)
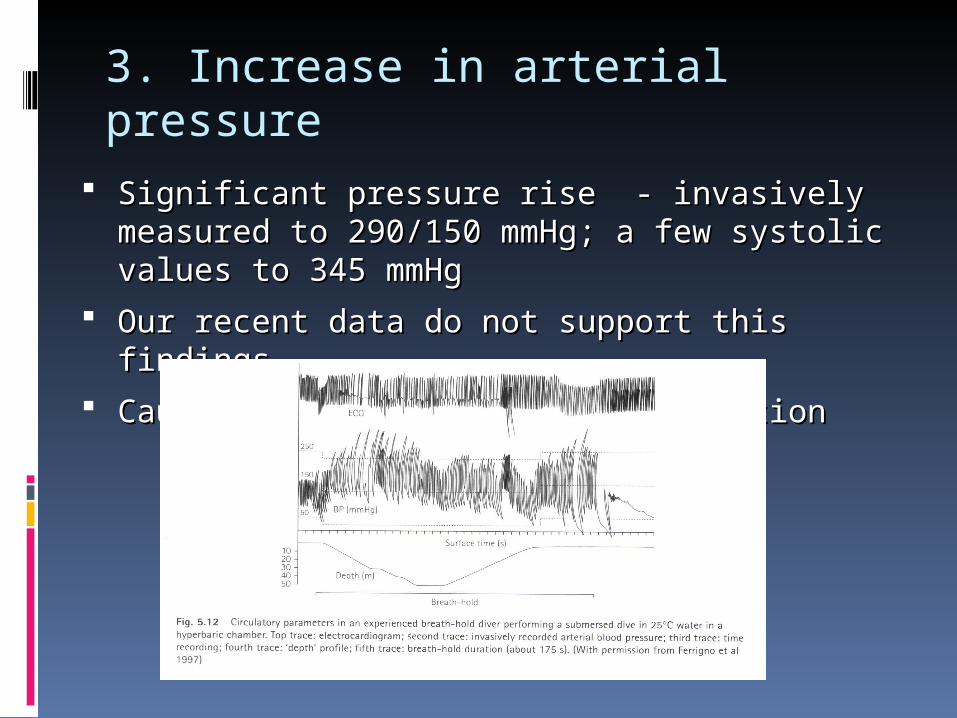
3. Increase in arterial pressure
SignificantSignificant pressurepressure rise - invasively measured rise - invasively measured to 290/150to 290/150 mmHg; a fewmmHg; a few systolic values to 345 systolic values to 345 mmHgmmHg
Our recent data do not support this findingsOur recent data do not support this findings Caused by peripheral vasoconstrictionCaused by peripheral vasoconstriction
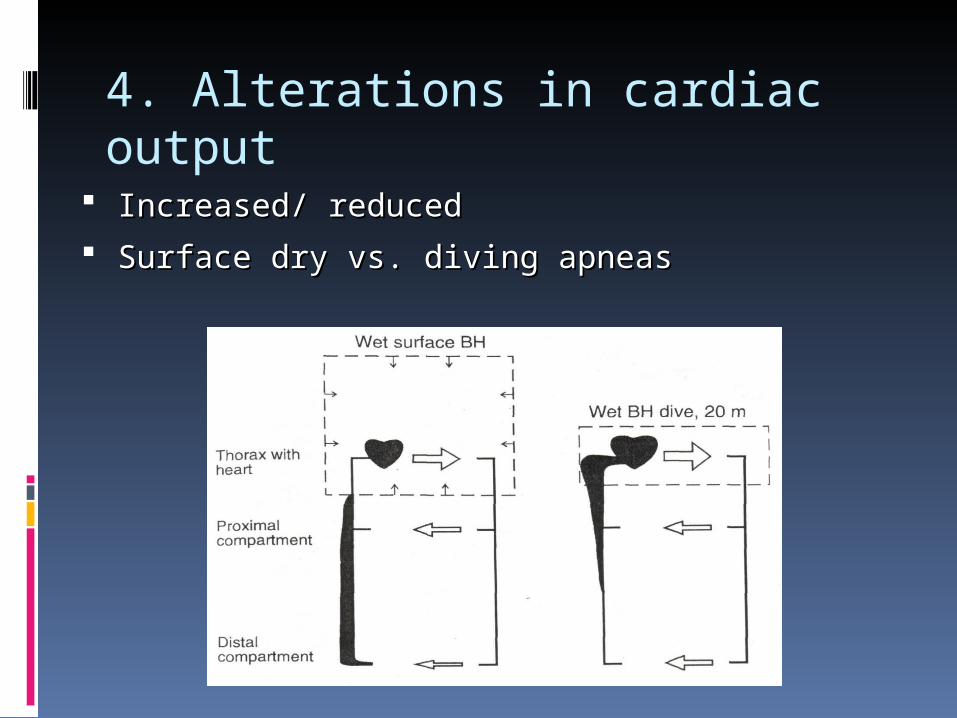
4. Alterations in cardiac output
Increased/ reducedIncreased/ reduced Surface Surface dry dry vs. diving apneasvs. diving apneas
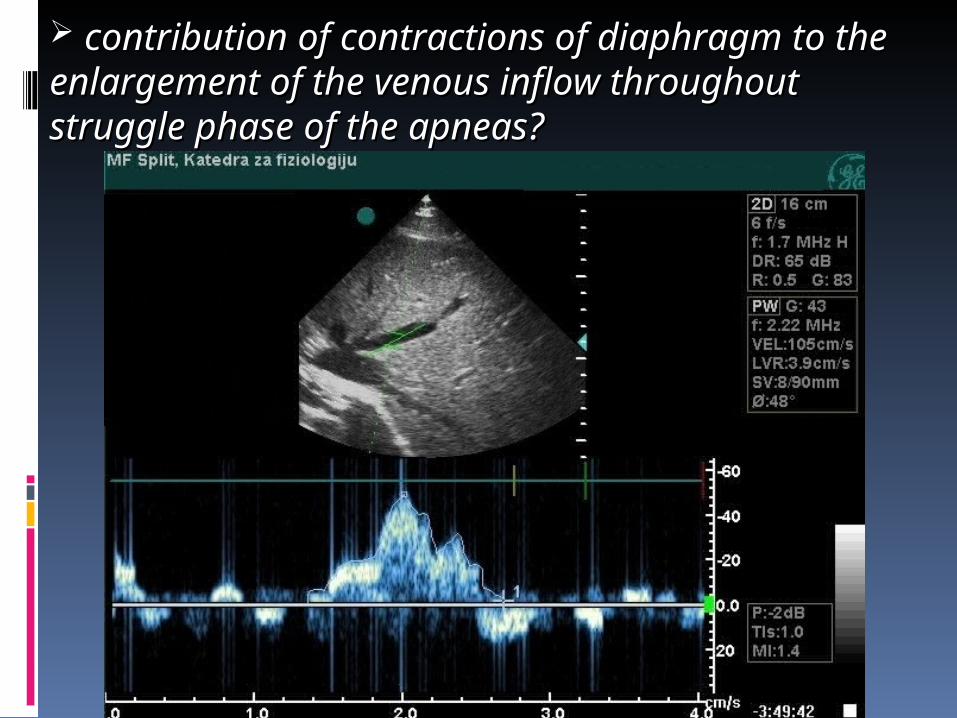
contribution of contractions of diaphragm to contribution of contractions of diaphragm to the enlargement of the venous inflowthe enlargement of the venous inflow throughout struggle phase of the apneas?throughout struggle phase of the apneas?
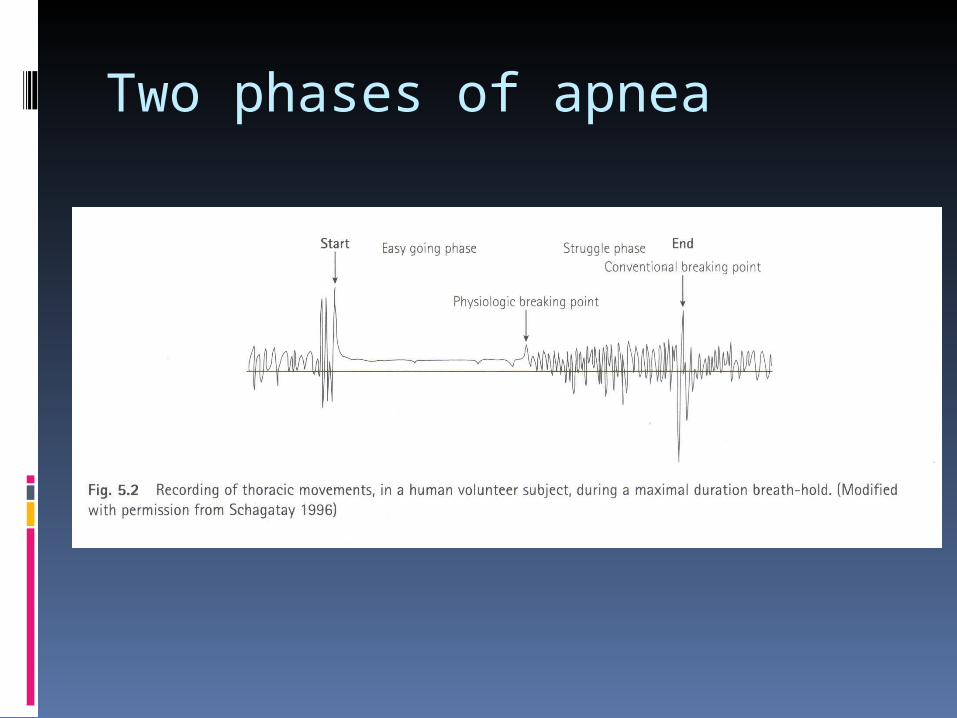
Two phases of apnea
Points of interest
Cardiovascular effects of breath-hold diving
Cerebrovascular impacts of apnea
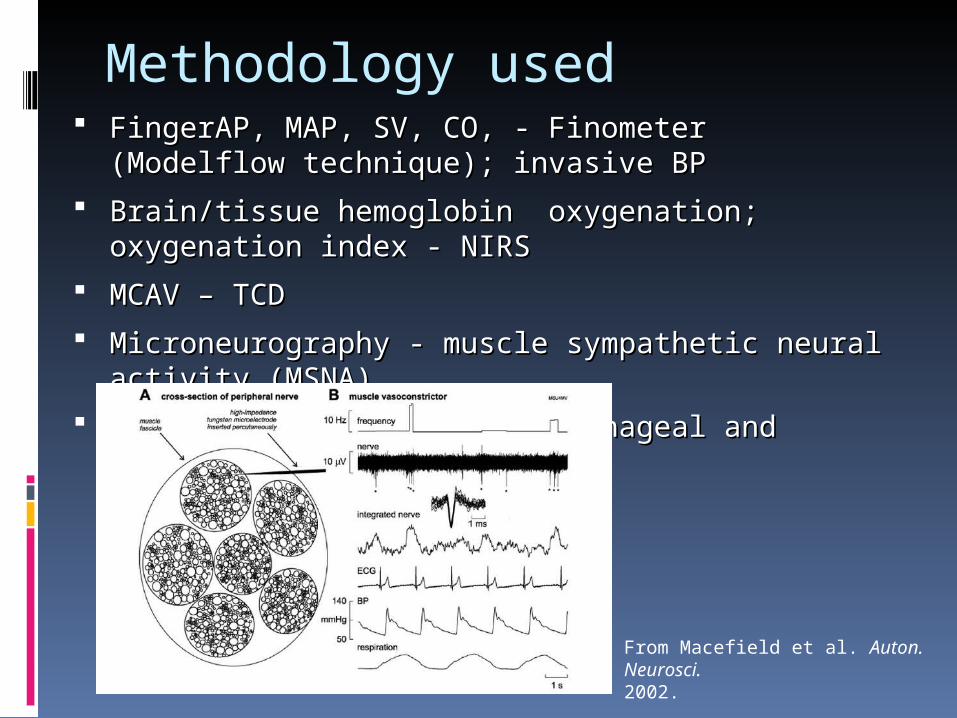
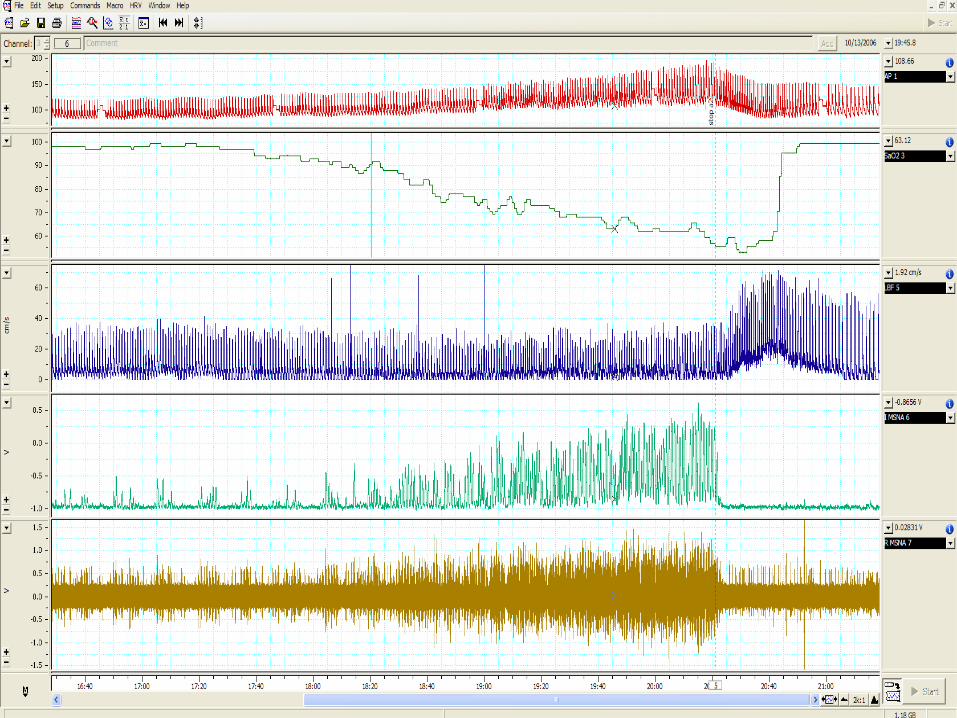
Methodology used FinFingergerAP, MAP, SV, CO, - Finometer (Modelflow AP, MAP, SV, CO, - Finometer (Modelflow
technique); invasive BPtechnique); invasive BP
Brain/tissue hemoglobin oxygenation; oxygenation Brain/tissue hemoglobin oxygenation; oxygenation index - NIRSindex - NIRS
MCAV – TCDMCAV – TCD
Microneurography - mMicroneurography - muscle sympathetic neural uscle sympathetic neural activity (MSNA)activity (MSNA)
Respiratory mechanics – esophageal and gastric Respiratory mechanics – esophageal and gastric balloonsballoons
From Macefield et al. Auton. Neurosci.2002.
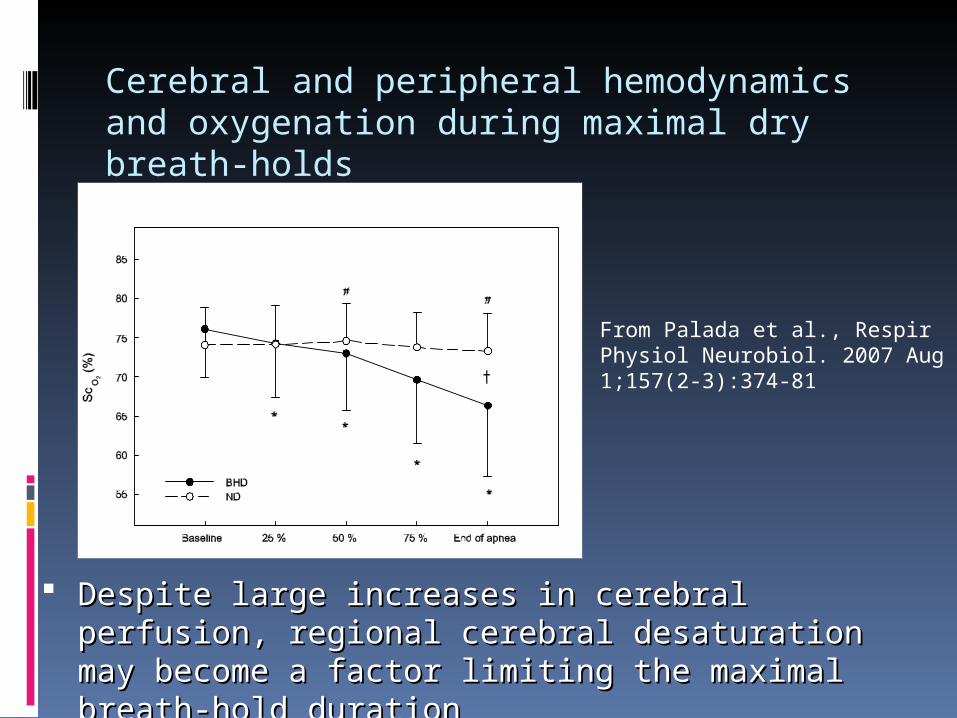
Cerebral and peripheral hemodynamics and oxygenation during maximal dry breath-holds
Despite large increases in cerebral perfusion, Despite large increases in cerebral perfusion, regional cerebral desaturation may become a factor regional cerebral desaturation may become a factor limiting the maximal breath-hold durationlimiting the maximal breath-hold duration
From Palada et al., Respir Physiol Neurobiol. 2007 Aug 1;157(2-3):374-81
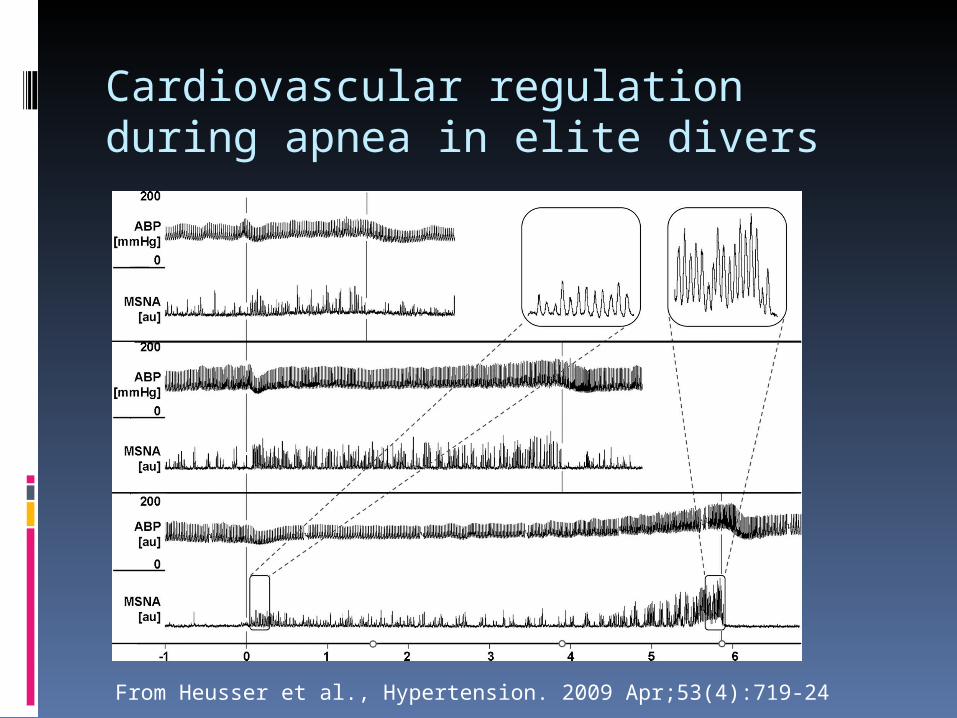
Cardiovascular regulation during apnea in elite divers
From Heusser et al., Hypertension. 2009 Apr;53(4):719-24

Restoration of hemodynamics in apnea struggle phase in association with involuntary breathing movements
Contribution of diaphragm Contribution of diaphragm contractions to the contractions to the enlargement of the venous enlargement of the venous inflow throughout struggle inflow throughout struggle phase of the apneaphase of the apnea
From Palada et al., Respir Physiol Neurobiol. 2008 Apr 30;161(2):174-81.
IImportance of “diving response”mportance of “diving response”
in the saving and redistribution of in the saving and redistribution of oxygen reserve throughout apneas oxygen reserve throughout apneas
iincrease in blood flow through vital ncrease in blood flow through vital organs (brain and heart) organs (brain and heart)
decrease of blood flow trough the decrease of blood flow trough the periphery (splanperiphery (splancchhnnic, muscular and ic, muscular and skinskin vascular vascular pool)pool)
DDiving response will appear in:iving response will appear in:
breath hold diving breath hold diving inin the depth the depth
the surface apnea with facethe surface apnea with face iimmersion inmmersion in the cold waterthe cold water
the surface apnea without face the surface apnea without face immersion (with or without cold immersion (with or without cold stimulus stimulus tto the face)o the face)
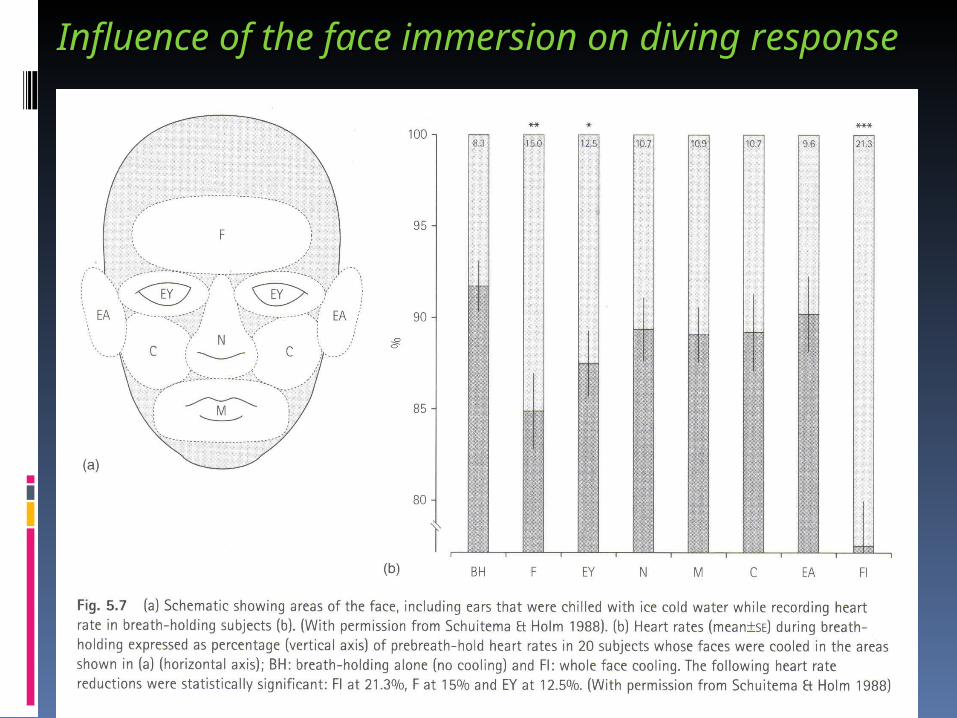
Influence of the face immersion on divingInfluence of the face immersion on diving rresponseesponse
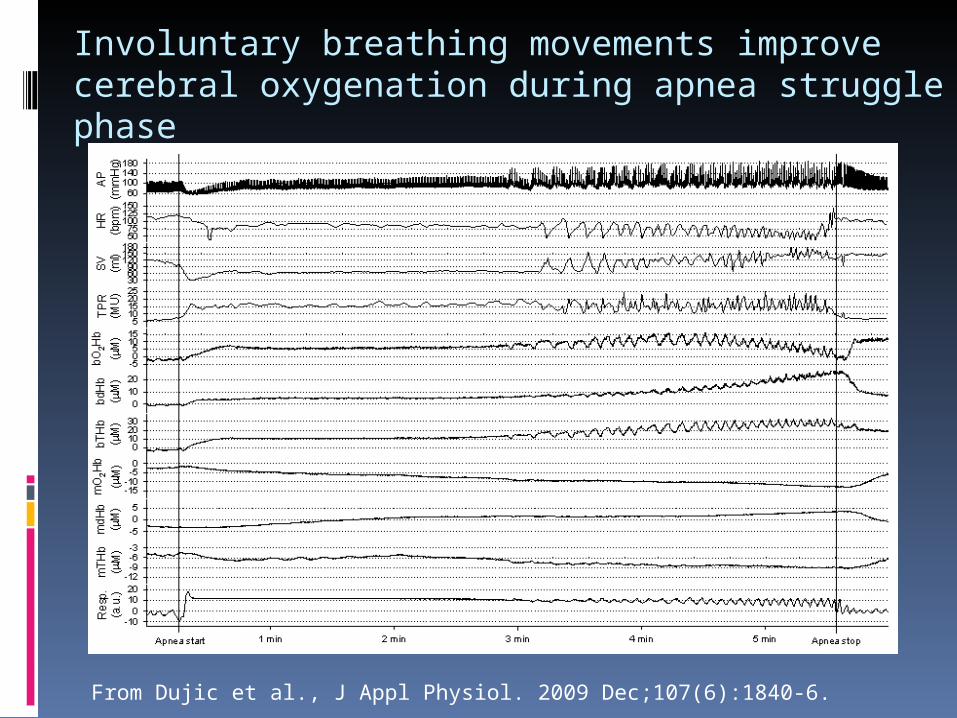
Involuntary breathing movements improve cerebral oxygenation during apnea struggle phase
From Dujic et al., J Appl Physiol. 2009 Dec;107(6):1840-6.
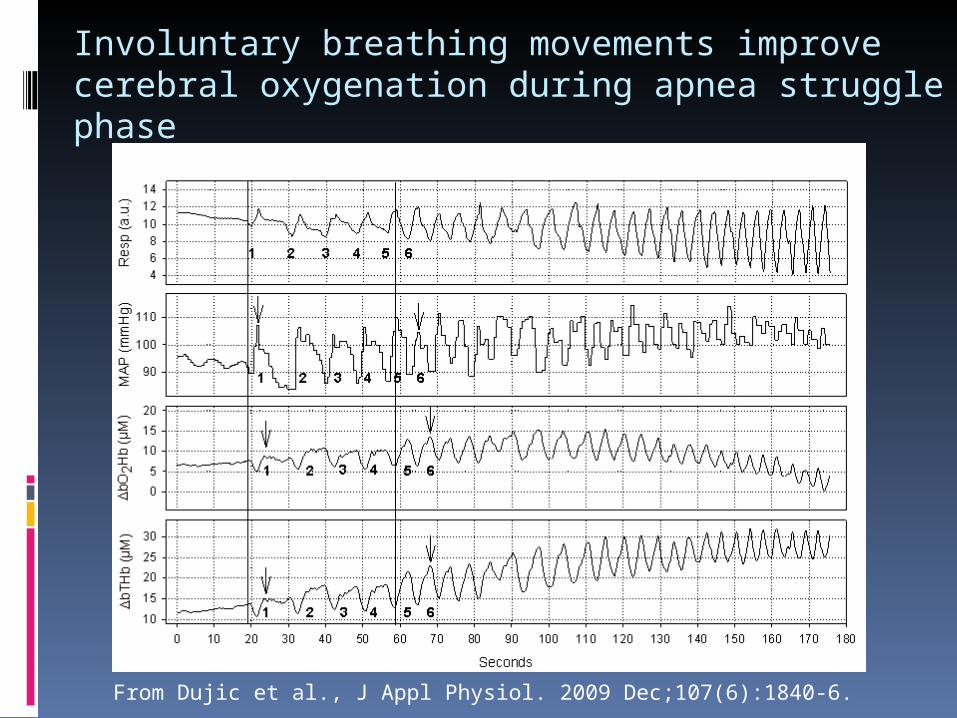
Involuntary breathing movements improve cerebral oxygenation during apnea struggle phase
From Dujic et al., J Appl Physiol. 2009 Dec;107(6):1840-6.
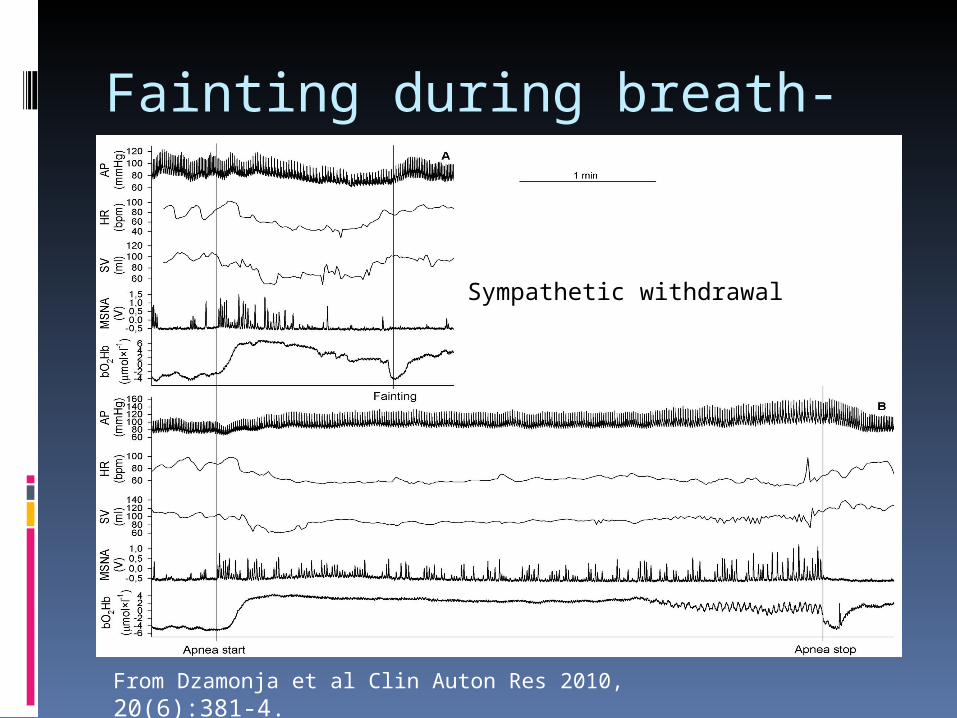
Fainting during breath-hold
From Dzamonja et al Clin Auton Res 2010, 20(6):381-4.
Sympathetic withdrawal
Conclusion
Increased sympathetic activity, restoration Increased sympathetic activity, restoration of hemodynamic parameters through the of hemodynamic parameters through the IBM and CO2-mediated central IBM and CO2-mediated central vasodilatation act vasodilatation act synergistically to synergistically to improve cerebral oxygenation and enable improve cerebral oxygenation and enable prolongation of maximal apnea time.prolongation of maximal apnea time.
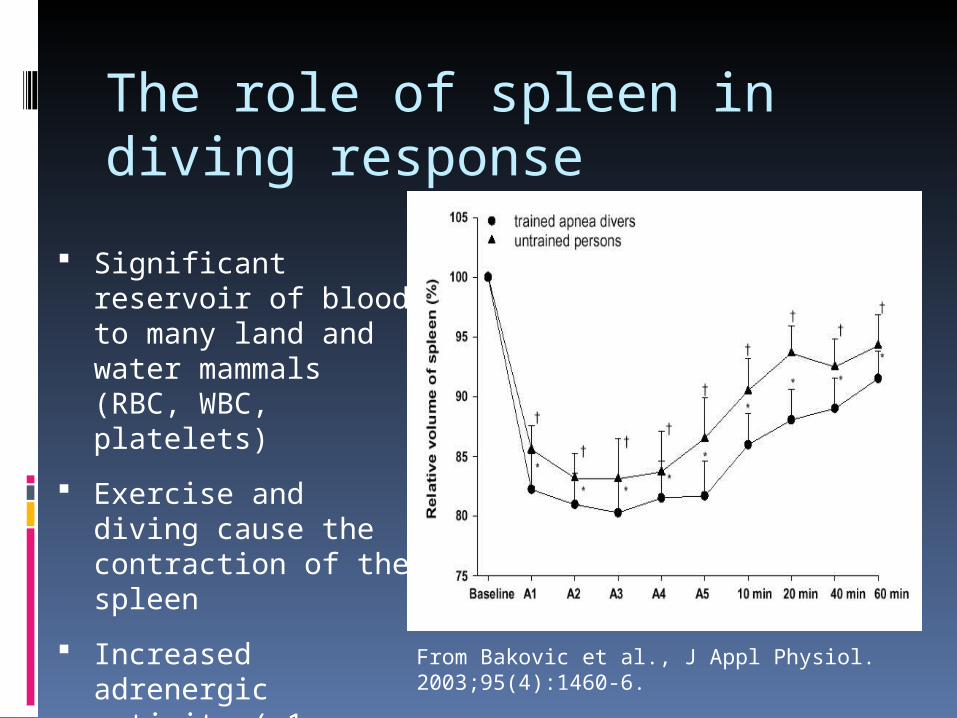
The role of spleen in diving response
Significant reservoir of blood to many land and water mammals (RBC, WBC, platelets)
Exercise and diving cause the contraction of the spleen
Increased adrenergic activity (α1-stimulation)
Constitutive part of SNS?
From Bakovic et al., J Appl Physiol. 2003;95(4):1460-6.
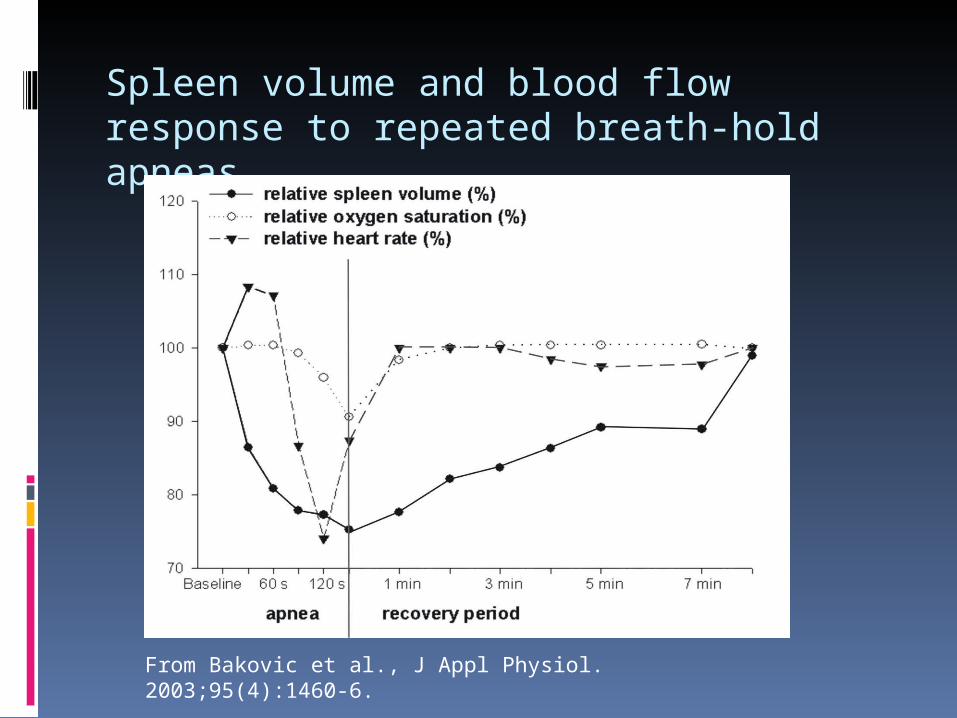
Spleen volume and blood flow response to repeated breath-hold apneas
From Bakovic et al., J Appl Physiol. 2003;95(4):1460-6.
Breath-hold diving and Obstructive sleep apnea
Includes three most important symptoms of Includes three most important symptoms of sleep apnea syndrome: cyclic hypoxemia, sleep apnea syndrome: cyclic hypoxemia, hypercapnia and absence of ventilationhypercapnia and absence of ventilation
Extrapolation of the results to the OSA and Extrapolation of the results to the OSA and connection between OSA and hypertensionconnection between OSA and hypertension
Unique human model of OSA?Unique human model of OSA?
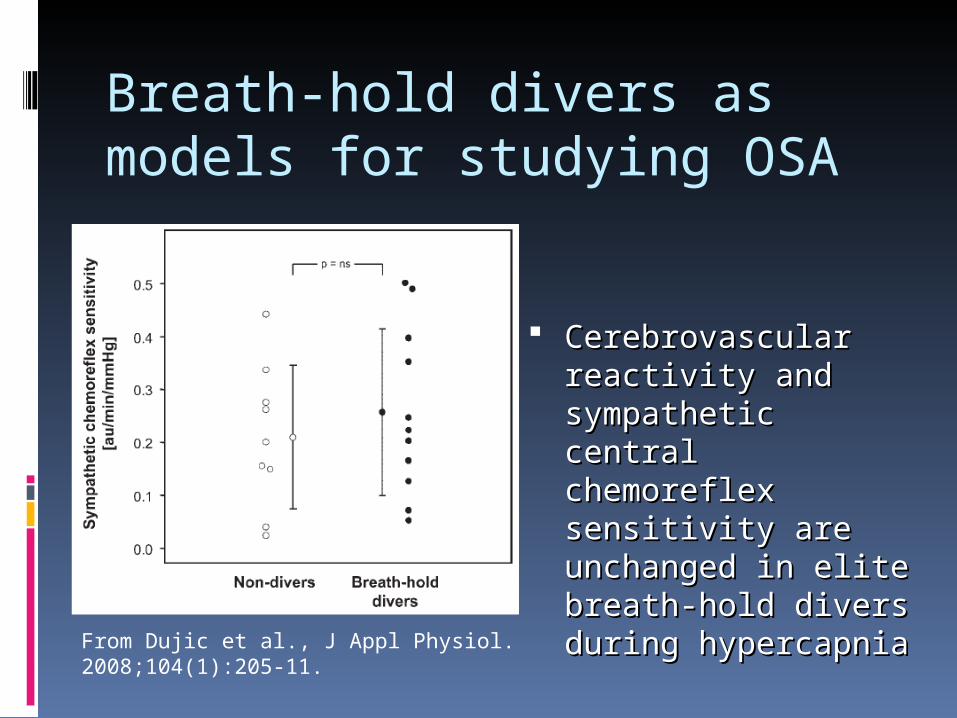
Breath-hold divers as models for studying OSA
Cerebrovascular Cerebrovascular reactivity and reactivity and sympathetic central sympathetic central chemoreflex chemoreflex sensitivity are sensitivity are unchanged in elite unchanged in elite breath-hold diversbreath-hold divers during hypercapniaduring hypercapnia
From Dujic et al., J Appl Physiol. 2008;104(1):205-11.
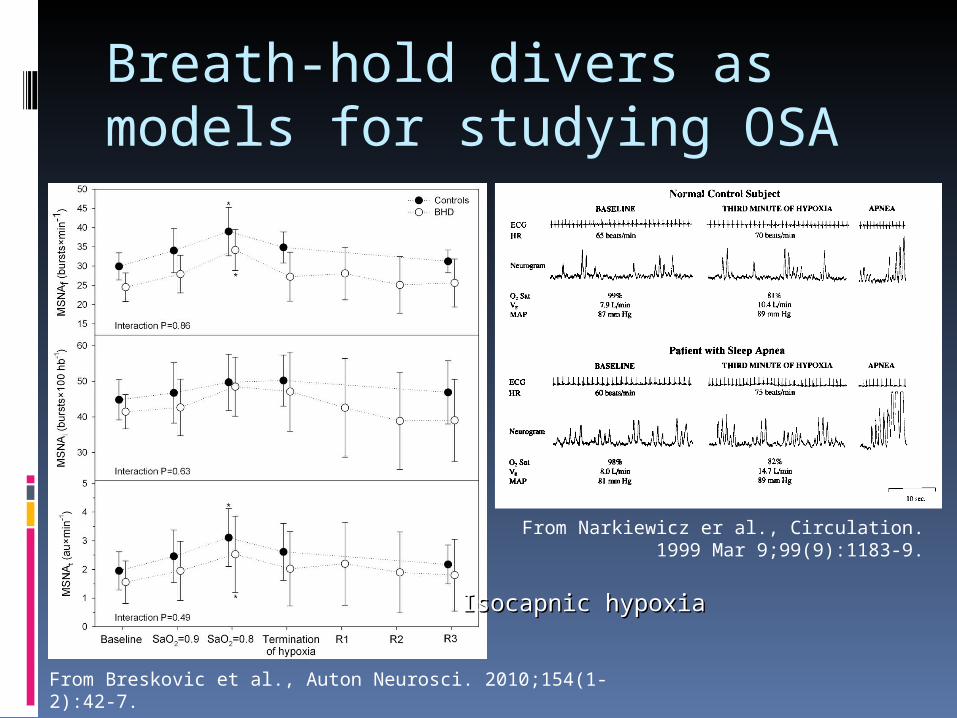
Breath-hold divers as models for studying OSA
From Narkiewicz er al., Circulation. 1999 Mar 9;99(9):1183-9.
From Breskovic et al., Auton Neurosci. 2010;154(1-2):42-7.
Isocapnic hypoxiaIsocapnic hypoxia
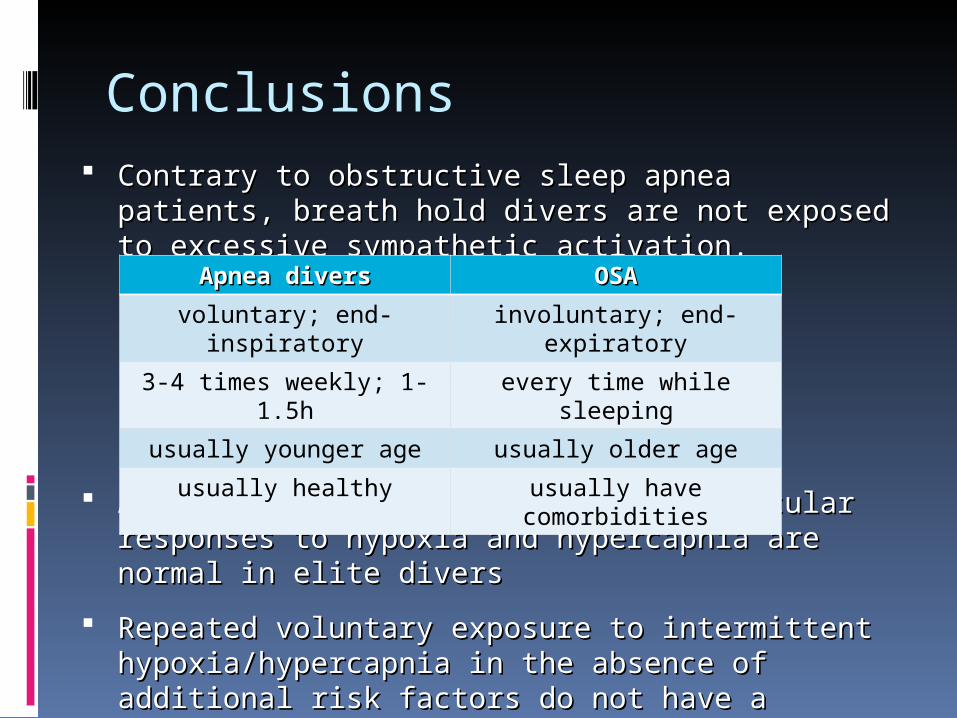
Conclusions Contrary to obstructive sleep apnea patients, breath Contrary to obstructive sleep apnea patients, breath
hold divers are not exposed to excessive hold divers are not exposed to excessive sympathetic activation.sympathetic activation.
Autonomic, ventilatory, and cardiovascular responses Autonomic, ventilatory, and cardiovascular responses to hypoxia and hypercapto hypoxia and hypercapniania are normal in elite divers are normal in elite divers
RRepeated voluntary exposure to intermittent epeated voluntary exposure to intermittent hypoxia/hypercapnia in the absence of additional risk hypoxia/hypercapnia in the absence of additional risk factors do not have a negative chronic impact on factors do not have a negative chronic impact on central and peripheral chemosensitivitycentral and peripheral chemosensitivity
Apnea diversApnea divers OSAOSA
voluntary; end-inspiratory
involuntary; end-expiratory
3-4 times weekly; 1-1.5h every time while sleeping
usually younger age usually older age
usually healthy usually have comorbidities
Ongoing studies Further characterization of IBMs –
respiratory mechanics – transdiaphragmatic pressure
IBMs – brain survival response/reflex
Analyses of discharge properties of sympathetic neural system
Unique coactivation of SNS and PNS
Spleen – the importance of large platelets recruitment in acute coronary incidents
Heart failure – autonomic adaptations, mitochondrial function, intervention

Thank you
www.mefst.hr/physiology





























