1© ECRI Institute 2011
Wake up! This is alarming!ALARM FATIGUE
Kara Polichetti
2© ECRI Institute 2011
Alarm fatigue occurs when clinical personnel fail to respond appropriately to alarms due to excessive or inability to understand the priority or critical nature of alarms. As a result, clinical personnel will be desensitized to alarms, and will ignore them and even turning them off.
What is Alarm Fatigue?
http://www.youtube.com/watch?v=9rdcso5cpN8
3
4
An Alarming ChallengeMore and more devices with alarmsMore and more patients are connected to one – or
many alarm-based devices150-400 alarms per patient per day can be typical in a
critical care unitAlarm-based devices are not standardized in many
institutionsFlexible alarm setting features allow for inconsistent
use of alarms
5
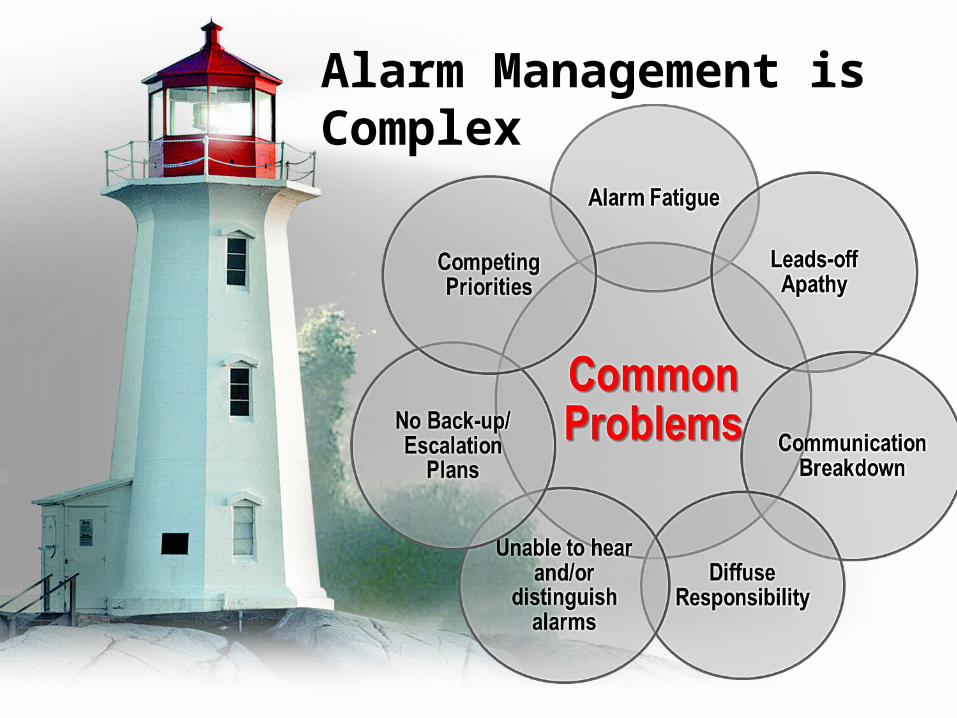
Alarm Management is Complex
6
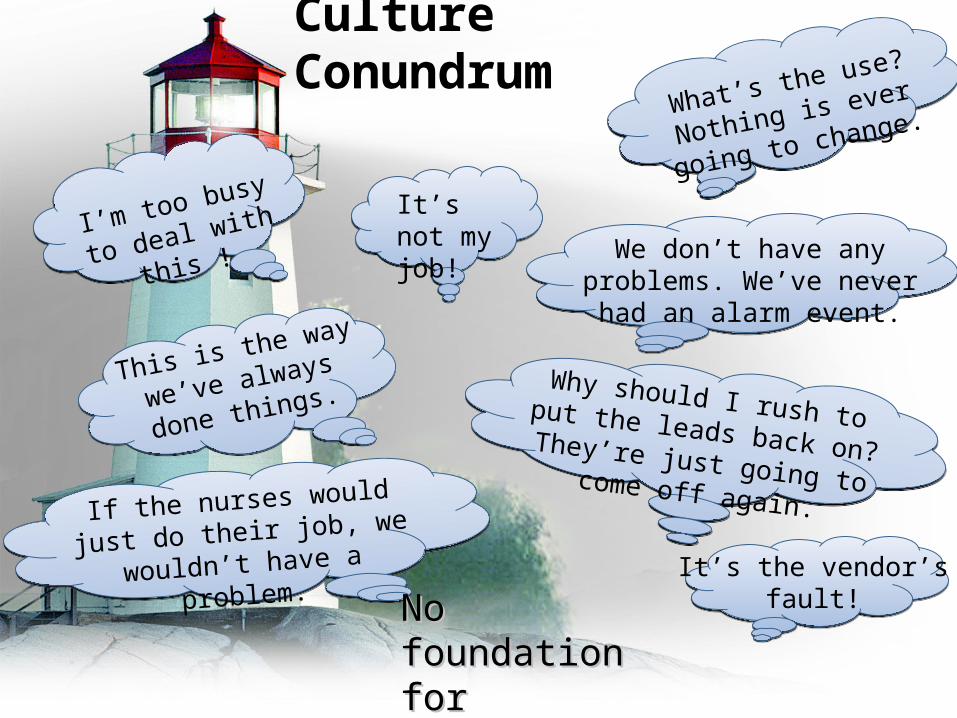
Culture Conundrum
If the nurses would just do
their job, we wouldn’t have
a problem.
We don’t have any problems. We’ve never
had an alarm event.
Why should I rush to put the leads back on? They’re just going to come off again.
It’s not my job!I’m too busy
to deal with
this !
What’s the use? Nothing
is ever going to change.
It’s the vendor’sfault!
This is the way
we’ve always
done things.
No foundationNo foundationfor improvementfor improvement
7
ALARM FATIGUEWhy is it important?
The Food and Drug Administration (FDA) received 566 reports of patient deaths related to alarms on monitoring devices from 2005 through 2008
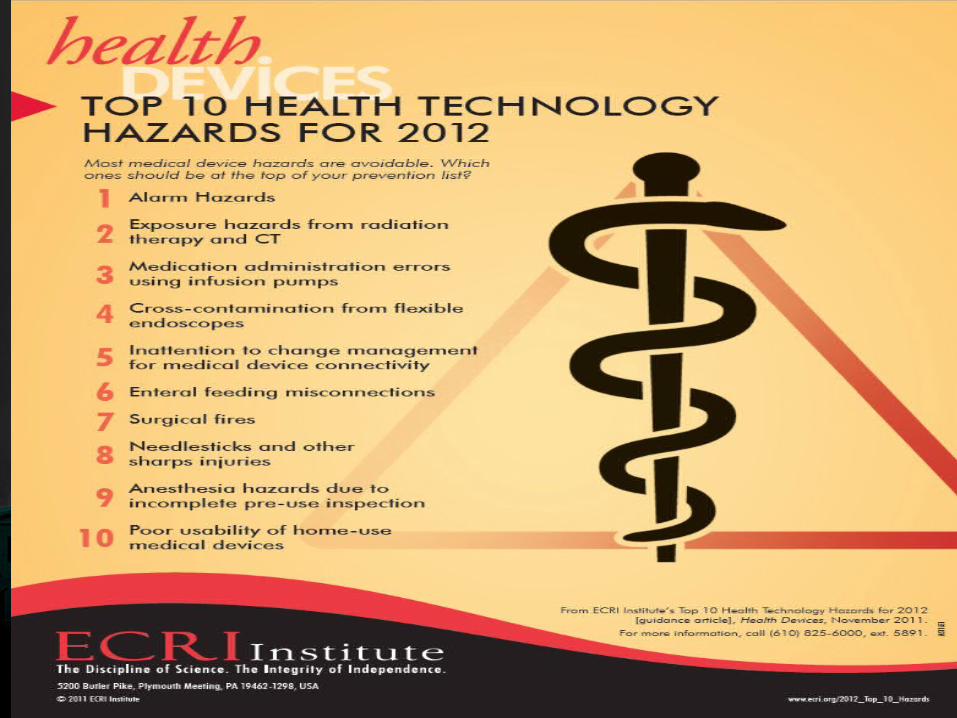
The ECRI Institute has identified alarm hazards as their number 1 top hazard for 2012
JCAHO recognized Alarm Fatigue as critical and integrated this into their accreditation standards

8
The Consequences are Alarming
“Alarm Fatigue” a Concern for New Haven Hospitals. New Haven Register, June 11, 2011
And Still in the News
9
A Typical Event
“Patient admitted with chest pain and shortness of breath---Was on a monitored unit. At 3:25 am, patient’s nurse noticed the leads were off and on checking on the patient found him in the bathroom unresponsive. Resuscitation efforts were unsuccessful. Monitor showed the leads had come off at 2:32 am …”
Alarm Interventions During Medical Telemetry Monitoring: A Failure Mode & Effects Analysis, A Pennsylvania Patient Safety Advisory Supplemental Review, March 2008
10
Example of Alarm Fatigue
Ventilator-dependent patient – frequent coughing
Coughing triggers high-pressure alarmFrequent response to alarm by nurse with
no real problemPressure alarm limit increased to minimize
the number of false-positive alarmsAn accident waiting to happen
Patient movement crimps breathing circuit Secretions clog the endotracheal tube Inadequate ventilation (inhalation or expiration)
11
Some Questions to AskDoes the nurse understand the purpose of the
high-pressure alarm?Was the nurse’s competence in ventilator use
validated? Does the hospital have a policy for who can and
cannot set ventilator alarms? Is there a policy on how ventilator alarms should
be set? If so, is it generic or does it consider specific
circumstances? Does the hospital have ventilator responsive-valve
features, which can reduce nuisance high-pressure alarms?
12
CausesStudies have shown as many as 99%
of ICU alarms are false or non-critical alarms.
These are called nuisance alarms and are the leading contributor to alarm fatigue
Alarms fail to function as expectedIt is difficult to distinguish which
machine's alarm is going offNurses may block out noise in order to
concentrate on current task.
13
Nurses have an overabundance of notifying devices (nurse calls, pagers, phones, overhead pagers, and monitor alarms)
Lower patient to nurse ratios increase the number of relevant alarms per nurse
Monitors with undirected alarms alert all nurses instead of specific nurses
NURSES PROBLEMS?
14
Underreporting Some estimates suggest that the actual number
of alarm-related deaths is ten-fold higher or more than what problem data shows
Ability to do analytics on data is very limited I literally had to read every report (around 20) in
a recent problem reporting analysisActual reports often don’t have much
information Typical language (paraphrased) - During use of
device alarm did not sound and patient died
Problem Reporting Data
15 16
16
Assess if sufficiently staffed with enough nurses
How many nuisance/false-positive alarms are there in the unit per day
Tiered response system would allow for quicker response time and delegation
Set individual parameters Actionable/tailored alarms would
create less nuisance alarms The combination of all alerts to one
device, "Smart alarms" to monitor multiple device in relation to each other
Centralized monitoring with allocated staff member to alarm personnel
Pop up screens EDUCATION & TRAINING!!!
How can we improve?
17
References
Borowski, M., Gorges, M. & Fried, R. (2011). Medical device alarms: biomed tech. 56(2): 73-83
ECRI Institute. Alarm related terms. Paper presented at the advancing safety in medical science clinical alarms 2011 summit. Herndon, October 4-5, 2011.
FDA: US Food and Drug Administration. (2011). FDA patient safety news: alarm monitoring problems. Available at: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/psn/transcript-rss.cfm?show=106. Accessed July 10, 1012.
Graham K., & Cvach, M. (2010). Monitor alarm fatigue: standardizing use of physiological monitors and decreasing nuisance alarms. American journal of critical care. 19(1): 28-34
Korniewicz, D & Kenney, B. (2012). Precenting ventilator alarm fatigue: before you silence that next nuisance alarm, be sure to read this article. Advance for nurses. 5(1): 15-18.
Lynn L. & Curry, J. (2011). Patterns of unexpected in-hospital deaths: a root cause analysis. Patient safety in surgery. 5(1):3
Taenzer A., Pyke J. & McGrath, S. (2011). A review of current and emerging approaches to address failure-to-rescue. Anesthesiology 115:421–31

18
THANK YOU!!!
Recommended