ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspondfax: +1416 978
E-mail addr
(L. McGillis H
Social Science & Medicine 61 (2005) 2482–2491
www.elsevier.com/locate/socscimed
A narrative approach to understanding the nursing workenvironment in Canada
Linda McGillis Hall�, Diana Kiesners
CIHR New Investigator, University of Toronto, Faculty of Nursing, 50 St. George Street, Toronto, Ont., Canada M5S 3H4
Available online 20 June 2005
Abstract
Narrative interviews were conducted with hospital nurses participating in a research study designed to provide
support and assistance to hospitals as they addressed work life issues for nurses in an attempt to create quality work
environments. The eight interviews were conducted in a sample of Canadian hospitals and generated themes relating to
an imbalance between the effort that nurses put into their work and rewards attained from it. Seigrist’s ((1996) Journal
of Occupational Health Psychology, 1, 27–41, (2002) In: P.L. Perrewe & D.G. Ganster (Eds.), Historical perspectives on
stress and health. Research in Occupational Stress and Well Being (vol. 2). Boston, MA: Jai Press) effort–reward
imbalance model was used to frame this study. The nurses’ narratives suggest that multiple factors constitute the nurses’
work environment and their experiences and perceptions of it. Issues which surfaced repeatedly in the interviews related
to changing needs of hospitalized patients in today’s health care system and the associated workload, the widespread
shortage of nurses, and the imbalance this creates for nursing work. A crucial finding is the extent to which the nurse is
impacted by the adequacy of care they are able to provide. These narratives outline the tremendous burden of guilt and
the overcommitment that nurses bear when factors in the work environment prevent them from providing complete,
quality care. Nurses are experiencing frustration and stress that is impacting their worklife, family and home life,
personal health, and possibly patient outcomes.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Nurses work environment; Effort–reward imbalance; Canada
Introduction
A number of recent reports and research studies have
identified an urgent need to improve the working
conditions of nurses (Advisory Committee on Healthy
Human Resources (ACHHR), 2002; Aiken et al., 2001;
Baumann et al., 2001; Health Canada, 2001; Nursing
Task Force, 1999; Page, 2003; Wunderlich, Sloan, &
e front matter r 2005 Elsevier Ltd. All rights reserve
cscimed.2005.05.002
ing author. Tel.: +1416 978 2869;
8222.
ess: [email protected]
all).
Davis, 1996). Warnings that an ageing population of
nurses combined with a lack of new graduates signifies a
major nursing shortage is of serious concern for a health
care system in which nurses constitute a substantial
proportion of the workforce. The quality of nursing
work life affects not only the recruitment and retention
of nurses but also outcomes for patients, the system and
families.
The burnout of experienced nurses and the difficulty
of recruiting new ones are at least partially due to a
stressful and undesirable work environment. Many
factors combine to create stressful work conditions for
nurses, among them: ‘‘heavy workloads, long hours, low
d.

ARTICLE IN PRESS
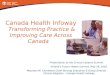
Intrinsic(person)
Extrinsic(situation)
Imbalance(Overcommitment)
High effortLow reward
DemandsObligations
MoneyEsteemSecurity
Career opportunities
Fig. 1. Effort–reward imbalance model (Seigrist, 1996).
L. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–2491 2483
professional status, difficult relations in the workplace,
difficulty in carrying out professional roles, and a variety
of workplace hazards’’ (Baumann et al., 2001, p. 1).
Work life factors are interrelated in complex and
intricate ways. In a recent study of 720 Canadian nurses
the likelihood of emotional exhaustion was found to
increase when nurses were at risk of an effort and reward
imbalance (O’Brien-Pallas et al., 2004). Increased acuity,
complexity and intensity of patient care combined with
downsized nursing leadership have led to increased
workload, while this in turn has resulted in decreased
satisfaction and nursing morale, increased absenteeism
and reduced quality of patient care (ACHHR, 2002).
Greenglass and Burke (2001) investigated the effects
of hospital restructuring on nurses and found that the
most significant and consistent predictor of stress among
nurses in hospitals being downsized was workload. ‘‘The
greater the nurse’s workload as a result of changes in the
hospital,’’ the authors found, ‘‘the greater the impact of
restructuring and the greater the nurse’s emotional
exhaustion, cynicism, depression, and anxiety’’ (p.
104). Decreased job satisfaction, professional efficacy,
and job security were also related to increased workload.
Restructuring has also been found to have a greater,
more negative effect on younger nurses, a finding with
severe potential implications for both retention and
recruitment (Burke & Greenglass, 2000).
Nurses believe that patients’ well-being and safety are
increasingly jeopardized by deterioration of nurses’
working conditions (Aiken et al., 2001; Keddy, Gregor,
Foster, & Denney, 1998; Nicklin & McVeety, 2002).
When patient care must be compromised because nurses
do not have enough time to achieve quality outcomes,
job satisfaction and morale also suffer. These may be
connected with high levels of absenteeism (Zboril-
Benson, 2002).
Restructuring and increased workload are also related
to high levels of absenteeism among nurses. In one
study, nearly 25% of 2000 respondents reported that
they had seriously considered leaving nursing; of these,
half cited overwork and stress as their main reasons
(Zboril-Benson, 2002). Another 15.6% cited disillusion
with nursing, while high job dissatisfaction, full-time
work, 12-h shifts and working in an acute care setting
were also predictors of absence. This suggests that 12-h
shifts may not be practicable in the present health care
work environment, particularly for older nurses. When
nurses were asked for a solution to the problem of
absenteeism, provision of adequate staffing levels was
the most common response (Zboril-Benson, 2002).
While a nursing shortage may result in short-term
bargaining opportunities for nurses, this is highly
market dependent and likely to fluctuate. Some nurses
have tended to advocate for themselves by leaving an
undesirable work environment. Nurses often migrate to
other countries where signing bonuses, educational
support and full-time work are all incentives that can
create a drain of nurses going abroad (Heitlinger, 2003).
Publications to date have directed limited attention to
the work environment in which nurses work and its
impact on the nurse and subsequently the patient. This
study is based on the nurses’ experience in the work
environment using a qualitative approach involving
interviews. The interviews highlighted areas identified as
major nursing workplace issues such as patient acuity
and the staffing levels available to meet patient work-
load needs.
Theoretical framework
The nursing work environment includes a number of
dimensions (e.g., physical and psycho-social) that can be
influenced by organizational management practices
(Koehoorn, Lowe, Rondeau, Schellenberg, & Wagar,
2002). Many of the issues that were identified in the
nursing work in this study include areas related to the
field of psychosocial work environments. Thus, the
theoretical model for effort–reward imbalance at work
(ERI) (Seigrist, 1996, 2002) as outlined in Fig. 1 was
used to frame this research. Emerging from social
reciprocity theory, ERI asserts that ongoing high effort
at work in combination with low reward leads to distress
reactions that result in adverse long-term effects on the
physical and mental health of employees (Seigrist, 2002,
2004). Effort refers to the demands of work. Rewards
are transmitted to employees as scarce resources
including money, esteem, and career opportunities.
There are two dimensions to the model: an extrinsic
situational dimension of work-related demands and
rewards, and an intrinsic personal dimension of ways
of coping with demanding situations and of eliciting
extrinsic rewards, as measured by the construct of
overcommitment (Seigrist, 2002).

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–24912484
Method
A narrative inquiry approach was employed in this
study as it allows individuals to tell stories about
experiences from their daily lives (Sandelowski, 1991).
Interviews were conducted with eight hospital nurses,
one from each of the eight hospital settings participating
in the research. The study was developed out of concern
for the effects of the reorganization of health care on the
nursing work environment. The nurses were asked to
describe in their own words issues of importance to them
in their working lives—‘‘what it’s like to be a nurse in
today’s work environment.’’ The intent was to provide
an opportunity for nurses to speak out about work life
issues; to obtain their understanding of designated
working life issues; to discover other areas of developing
concern; and to listen to their recommendations for
needed change—to acquire, in effect, a snapshot of a
health care system in transformation from the perspec-
tive of the nurse.
Sample and data collection process
The study received approval from the university ethics
review board as well as the ethics boards of all eight of
the hospitals involved in the study. Interviews were
conducted with a sample of eight nurses from the study
hospitals who had indicated willingness to discuss the
work environment of nurses with an interviewer. The
hospitals involved were acute care, publicly funded
hospitals that were randomly selected from across the
province of Ontario, Canada. The eight hospitals
represent teaching, community, and small rural organi-
zations located in different geographical regions of
Ontario, which enhances the representativeness of the
sample.
Names of possible interviewees were provided to the
principal investigator of the study by on-site contact
persons for each institution. These potential interviewees
were nurses who identified an interest in participating in
the study. Purposive sampling was used to select
individuals from each site who were contacted by
telephone, informed of the purpose of the interviews
and asked if they were still willing to be interviewed. All
of the nurses who expressed willingness to participate in
these interviews were female. The subjects were em-
ployed in either Medical or Surgical units in their
respective institutions and presented a wide range of
nursing experience from 9 months to 40 years. Seven of
the nurses interviewed were employed full-time,
although most had worked part-time at one point or
another in their careers. One currently worked part-
time, a situation that suited her lifestyle. Six were
Registered Nurses while one subject was a Registered
Practical Nurse.
The interviews were approximately 1 h long. Marrow
(1996) suggested that research findings can take on an
unreal character when that research is conducted away
from the clinical setting, thus, it was felt that proximity
to the work environment might make it easier for
subjects to connect with and discuss work life issues even
when they were not on duty. Whenever possible,
interviews were conducted at the health care institution
where the subject worked, both for the convenience of
the nurses and to put them at ease by being interviewed
in a familiar setting. Interview rooms were booked at
their institutions so that the interviews would take place
in privacy and the nurses would not be interrupted by
work matters.
Structure of interviews
Interviews were such that the interviewer to some
extent guided the interview by asking open-ended
questions related to the topics of interest (Bowling,
1997). Nurses were asked to talk about any issues related
to their work lives that were important to them and that
would help to illuminate ‘‘what it’s like to be a nurse in
today’s work environment.’’ Specific areas of interest
were derived from a substantive review of the literature.
Some of the concepts and categories were therefore pre-
established, while others emerged from the interviews.
Various techniques have been recommended for
conducting qualitative research interviews. According
to Britten (2000), the interviewer should begin with
questions that are easy for the interviewee to answer and
move towards difficult or sensitive issues in the course of
the interview. Cohen and Manion (1994) found a
‘‘funnel’’ approach to be useful, in which the interview
begins with a wide focus and gradually becomes more
specific. Price (2002) stated that, although it is important
not to force data or shape it according to research or
other paradigms, entirely undirected interviews often
produced results that were relatively superficial. He
suggested that probes be structured at three levels of
inquiry: action, knowledge and philosophy. Questions
should be formed according to their level of anticipated
intrusion, descriptions of action being assumed within
this framework to be the least invasive and philosophical
questions—those concerned with beliefs, values and
feelings—the most invasive. Knowledge-based questions
are best asked in the middle of the interview. This
‘‘laddered’’ technique was used when possible and when
probes appeared necessary.
Following the interview, subjects were asked whether
they wished any details or portions of the interview
deleted. Every attempt was made to ensure that the
subjects were satisfied with the outcome and course of
the interviews, and to ascertain that they had no
reservations about what had been discussed. They were
told that if any such reservations arose at any time

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–2491 2485
following the interviews they should not hesitate to call
the interviewer to discuss them, and that if there was any
part of the discussion they wanted excluded from the
study their wishes would be honoured.
Analysis
All of the interviews were transcribed verbatim, and
the transcriptions checked to ensure accuracy. The data
analysis was guided by a methodology for identifying
and interpreting narratives (Lieblich, Tuval-Mashiach,
& Zilber, 1998). Each of the transcribed interviews was
read closely to identify a particular participant’s story,
the narrative theme underlying it. Portions of these
narrative themes were highlighted and these segments of
the transcripts were reread to capture the essence of the
individual story, and summaries created. These were
then analysed with reference to the topic areas
established before the interviews and new categories
that arose in the course of interviewing. Care was taken
to maintain the nurses’ viewpoints and the balance of
their narratives to maintain their emphasis, and their
words.
Results
Description of the sample
The eight participants were employed in either
Medical or Surgical units in their respective institutions
and presented a wide range of nursing experience, from
9 months to 40 years. The range of experience was a
fortuitous artefact that helped demonstrate how the
concerns of nurses might develop throughout their
careers. The majority of the nurses interviewed were
registered nurses who were employed full-time, although
most had worked part-time at one point or another in
their careers. One currently worked part-time, a situa-
tion that suited her lifestyle, and one participant was a
licensed practical nurse.
Themes
Detailed analysis of the transcripts revealed three key
themes communicated by the nurses: patient acuity,
workload and understaffing; and adequacy of patient
care. Workload and understaffing dominated the
narratives, although this was strongly linked to patient
acuity and the adequacy of patient care provided. These
key nursing work environment issues are now described
and discussed in the context of the ERI model, as they
were revealed in the nurses’ narratives, and implications
for health policy and management decisions are
presented.
Extrinsic dimension: The situation
Effort
Extrinsic factors in the work situation of nurses lead
to the efforts they put forth in their work. These can
include time pressures, interruptions, responsibility, the
pressure to work overtime, physical demands, and
increasing demands from work overall (Seigrist, 1996,
2002).
Patient acuity. The primary area reported by all of the
nurse participants as a major cause of stress in their
working lives was patient acuity, which is consistent
with the ‘‘effort’’ dimension of the theoretical model.
The effort dimension explores whether a job has become
more and more demanding (Seigrist, 1996, 2002; Seigrist
et al., 2004). In this study, nurses identified that patients
were sicker; often presenting with multiple conditions
rather than just one:
I think the major source of stress for nurses is that
patients are sicker nowadays. Patients are not coming
in with just Chronic Obstructive Pulmonary Disease
(COPD), for example. They’re coming in with COPD
and congestive heart failure and kidney failure—you
know, every body system is going. So that’s a lot for
a nurse because you’re not just focussing on one area.
You’re focussing on every area and acuity has gone
way up. And there are that many more procedures
and paperwork involved with them. (Nurse 2).
Another aspect of ‘‘effort’’ relates to employees
having a lot of responsibility in their work. Nurses in
this study described escalating work responsibility in
their everyday work. Whereas a nurse might once have
been required to care for three very sick patients out of
six in a shift, now all six could be critically ill or fresh
post-operative patients. Less critically ill patients who
would once have been hospitalized are often dealt with
on an out-patient basis, raising the average acuity of
those patients remaining in hospital. In addition, the
patient population is ageing as patients are getting older.
As well as their medical problems, now they are
recovering from surgery so their other problems are
compounded. Issues of acuity are connected with
workload, which is itself influenced by the nurse–patient
ratio and staff mix. However, it is striking that of all the
factors considered in the interviews, increased patient
acuity was the one agreed upon as major by all
respondents. In general, the patients are sicker, the
nurses are fewer, and the result is increased stress for the
nurse. Although acuity is agreed to have been on the rise
for some time, nurse–patient ratios often have not
reflected this increase:
The acuity is high, very high. You have very ill
patients. We are the only active Medical floor in the

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–24912486
hospital. It’s a sort of almost step-down from ICU or
a step-up to ICU. So you do have very ill patients.
The acuity has been increasing over the years with no
additional staff provided to the unit. (Nurse 8).
We have a lot of really sick patients right now but our
nurse–patient ratio doesn’t change. If you have four
patients, you might have two that are really sick and
two that are less sick. They’re all sick, but their acuity
levels will be different. A four-patient workload with
varied levels might not be as difficult as a four-patient
workload where the acuity for all four is at the highest
level. In general, the acuity is increasing. (Nurse 1).
They come in and they’re really, really sick. It’s hard
because if you’ve got four patients and they’re all
really acute then you’re running around trying to
make sure everything is done whereas if you’ve got at
least one patient who can manage a little bit on their
own or do something for themselves, then it’s not so
bad. (Nurse 4).
Workload and understaffing. The constant time pres-
sures associated with a heavy workload are part of the
demands and obligations included in the ‘‘effort’’
dimension of the EFI model (Seigrist, 1996). Workload
was reported to be extremely high and appeared, even to
the minimally experienced, to be increasing:
I haven’t been a nurse for that long, but a lot of
people seem to be saying the same things—that it’s
too hard or that people are staying later at work
because they didn’t have time to finish everything
during the day. (Nurse 1).
A nurse with 21 years of work experience felt that the
increase in workload was accelerating:
It’s amazing but I just don’t think anything has been
as bad as it has been in the last five years. I’m trying
to think of why that is and all I can think of is just
that people are getting older; they need more help
with activities of daily living, like just washing,
dressing and walking because of physical infirmities.
We have so many more machines attached to people
nowadays. I really do think that we had better
staffing in the past. (Nurse 5).
Nurses were frustrated at being denied a sense of
completion with regard to patient care or, indeed, to any
given task. For some it was simply a question of feeling
they had done a good job, had completed their care
according to their own standards. A nurse who came to
hospital nursing after working in Community Health
compared the care:
In the community you’re one on one and in the
hospital it’s like 50 to one. You can never finish a
task. In the community you went in and you did what
you had to do and you really didn’t leave until it was
completed or the patients were set for that moment.
You did everything you needed to do. Here at the
hospital, you never feel like you ever finish a task.
You just prioritize and finish what you have to at
that moment. Actually sometimes I’m embarrassed
that hospital patients are not getting the care they
should. My workload is so extreme that after a shift I
kind of pray that I’ve done everything, because I’m
flying constantly all day long. (Nurse 7).
Sometimes patients felt apologetic about asking for
help from nurses they know are already overburdened.
At other times they appeared to see first hand how
overwhelmed their nurses were:
They read the papers, they know what’s going on.
The first thing they’ll say, a lot of them, is, ‘‘I’m so
sorry for bothering you. I know you’re busy.’’ So
then you have to say, ‘‘No, I’m here for you. I’m your
nurse. So what can I do for you?’’ (Nurse 2).
They feel really badly because their nurse is running
around like a chicken with her head cut off. ‘‘Oh,
poor so and so. She was really running yesterday.’’
They don’t want to ring the buzzer and that’s not
what it’s all about. ‘‘You know, if you need help,’’ I
tell them, ‘‘push the buzzer, because it’s the squeaky
wheel that gets the grease here. If you don’t buzz for
me, I won’t know.’’ (Nurse 5).
Reward
Extrinsic factors in the work situation of nurses
include the rewards received for work. These can include
salary, respect, adequate support and treatment, esteem,
recognition, job security, promotion prospects, undesir-
able change, and career opportunities (Seigrist, 1996,
2002).
Esteem and recognition: Adequacy of patient care. One
of the components of ‘‘reward’’ relates to the adequacy
of the recognition and esteem that the employee receives
from their superiors and colleagues (Seigrist, 1996,
2002). This is considered an important dimension of
worklife balance. Individuals who are perceived to be
overcommitted to their work have a strong desire for
esteem (Tsutsumi et al., 2002). Nurses in this study
clearly demonstrate overcommitment to their work, yet
recognition of their work is not described. Rather,
nurses articulate how the level of patient care they
were able to provide was a significant work life issue for
many of them. Nurses were unhappy about being unable
to provide the level of care that they considered
adequate, which in turn impacts on their perception of

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–2491 2487
esteem. There was little time to communicate with
patients:
You know, what’s rewarding about nursing is talking
to people and helping them. That’s how you find out
things that maybe you weren’t aware of, that will
help with the care you’re giving them. I think that’s a
big part of it. But it’s so busy now you can’t
always give all the care that you would want to give.
(Nurse 1).
I wish I were allowed to work at a more relaxed pace,
that I had more time to go in and chat with my
patients rather than being so task-oriented all the
time. Because I really do think that emotional bond is
important with patients. I would just like to have
more time to do teaching and to be able to have that
chat with them. (Nurse 5).
Nurses traditionally gain recognition and esteem from
patients through their experiences involving teaching.
Patient education was regarded by nurses in this study as
a crucial aspect of patient care and one nearly
impossible to find time for.
Let’s say the patient is a new diabetic. You have to
make sure that you get the doctor’s order to the
Diabetic Educator and that the patient knows what
the supplies are and that they practice giving
themselves the injection. You have to make sure that
they’re able to do it at home on their own, when
you’re not doing it anymore and that they’re ready to
function independently outside of the hospital,
that they’re not leaving the hospital unprepared.
(Nurse 6).
The pressures of time and workload meant that nurses
were constantly multitasking, doubling and tripling up
on activities, performing diagnostic functions while
carrying out routine tasks:
You have to start asking questions right off the bat.
While you’re bathing them you’re asking them who
they live with, where they live, how they are getting
home. You have to. You don’t have time to say,
‘‘Okay, now we’ll discuss your ileostomy.’’ While
you’re making the bed you’re saying ‘‘Oh, the ostomy
nurse—do you know if she’s booked to come in on
Tuesday to discuss the types of prosthetics that
you’re going to need and give you the forms for the
doctor to sign to have it paid for?’’ (Nurse 6).
Some nurses reported that basic hygiene and house-
keeping—‘‘beds and baths’’, were becoming compro-
mised because of lack of time and overwhelming nursing
workload. The nurses’ time was completely taken up
with more critical issues. Making patients comfortable
and relaxed by cleaning them up is considered by nurses’
to be an important precondition to their successful
therapy and healing that nurses were not able to carry
out in this work climate:
One man was very sick and, even though he’d had a
post-operative wash, he had a bit of blood here and
there, and a little bit of urine here and there. I
couldn’t not wash him and then ask him to get up for
a walk and do the deep breathing, the coughing
and all the exercises that I wanted him to do in order
to get better. I had to make him feel good first.
(Nurse 5).
Intrinsic dimension: The person
Intrinsic factors in the work situation of nurses lead to
the coping mechanisms used to deal with work,
primarily in the form of overcommitment. This can
include a need for approval, disproportionate irration-
ality and the inability to withdraw from work (Seigrist,
1996, 2002).
Overcommitment
Seigrist (2002) suggests that employee response to
demands is an excessive work-related overcommitment,
which may be characterized through the inability to
withdraw from work obligations. This was evident with
the nurses in this study. No matter how hard or how
long nurses worked, there did not seem to be enough
hours in the day to handle the workload. Some nurses
reported missing breaks and meals on a frequent basis.
The lack of respite could be extreme:
Lots of times we don’t take an afternoon break—
that’s almost non-existent—and a supper break. We
don’t take care of ourselves break-wise because we
want to get out on time. Quite often I work shifts
with very little break. I have even worked twelve-
hour shifts with no break, especially on the night
shift. You could not leave the floor. I sit there and eat
my sandwich while I’m charting and hardly have time
to go to the washroom. (Nurse 5).
Nurses said they knew that if they took breaks they
would have to work overtime in order to get their work
done. This is consistent with the EFI model, where the
demands or obligations of the job can pressure employ-
ees to work overtime (Seigrist et al., 2004). Nurses felt,
however, that it was better to work the overtime, as they
would feel better if they went and took 20min to sit
down. Some thought their health was being affected by
this workload.
I think that nursing is affecting everybody’s health
with the length of the shifts, the stress, and the
physical demand of night shifts. It has to take a toll
on someone’s life. I have a nurse’s back and am

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–24912488
emotionally exhausted every day. I come home and I
think, ‘‘Now tomorrow when I go back I will be
positive,’’ but it takes me five minutes on the floor
and I’m back in the same boat I was before because
situations do not change. (Nurse 8).
Depending on the nurse and the institution, workload
might be rated from somewhat stressful to so crushingly
high that interviewees were considering leaving their
institutions or jobs because of it. This represents the
excessive work-related commitment, or overcommit-
ment experienced by employees who cannot let go of
work, and it stays with them after they have left work
(Seigrist, 2002). One nurse repeatedly used the word
‘‘frantic’’ to describe her work situation. To an
interviewee who had been a nurse for 40 years, the
effects of current nursing workload on the profession
were overwhelming:
You go home every day knowing you haven’t
completed your job. There is no way that you can
finish your workload. You have to decide on what is
most important and hopefully what is left isn’t and
wasn’t that important because there is just too much
for the workload, for the amount of nurses. The
hospitals have cut and cut. You are portering and
you are lifting, you are taking on the job of the
orderly. You are everything. (Nurse 8).
The majority of nurses reported extreme physical
exhaustion at the end of shift and the sense of having
been on the run throughout. This behaviour is
characteristic of the imbalance that is created when
employees are overcommitted to their work (Seigrist,
1996). Because of increases in patient acuity, nurse–pa-
tient ratio was not necessarily an accurate predictor of
workload. As one nurse explained,
I used to be able to handle four or five patients, even
six, quite nicely because usually several of them were
going home or they weren’t that sick, but now you
have six that are sick! (Nurse 3).
The imbalance between effort and reward in nursing work
The model of ERI suggests that when there is a lack of
reciprocity between the work expended and the reward
or gains to the employee, a negative outcome results
(Seigrist, 1996, 2002). In this study, the stress and
burnout of excessive workload was accompanied by
high levels of absenteeism. Because it was often difficult
to replace staff on short notice and because some
institutions had the practice of replacing the second sick
call on a shift but not the first, absenteeism further
increased the workload for the remaining nurses and, in
a circular manner, contributed to their stress and
potential absenteeism. When acuity was high and
workload was at a critical level, the practice of not
replacing the first sick call placed a burden on the nurses
who were present. If there was a second sick call, if two
nurses were absent, the unit would begin calling around
to try to find a replacement nurse. However, this was not
always possible; casual and part-time pools might be
already over-used and replacement staff simply not
available. Even if a replacement could be found, there
was sometimes a lengthy period of time during which
nurses had to deal with an inadequate nurse–patient
ratio. Nurses might end up staying at work for extra
hours, even though they had already worked a full 12-h
shift. For one nurse, a contentious issue was trying to
balance her duties as Charge Nurse with her patient
load, a balance that was easier to achieve on some days
than on others:
On some days it doesn’t work at all, because I still
have a patient assignment even though I’m the
Charge Nurse. I have three patients. Sometimes
that’s hard if there’s stuff going on because you’re
striving to look after your patients and there’s other
stuff going on and you feel like you’re being torn
between everything that needs doing. (Nurse 2).
High workload and the resultant stress were also
linked in some nurses’ minds with both nurse and
patient safety. When nurses were rushing around,
accidents were more likely to occur and nurses were
more likely to injure themselves. The ongoing disparity
of effort and rewards is prevalent in nurse’s work.
Seigrist (2002) suggests that an imbalance is main-
tained when an alternative choice is unavailable, when
the condition is accepted for strategic reasons, or as a
personal coping style of the individual. It is evident that
workload has fostered the level of imbalance reported by
nurses in this study. Workload as an issue is affected by
acuity, absenteeism and understaffing. It in turn affects
stress levels, perceived quality of patient care, absentee-
ism and possible risk of injury to nurses. Often under-
staffing is a budgetary issue, but some institutions are
finding it difficult to recruit nurses even when they
actively seek them. It is impossible to overestimate the
importance of workload as a factor causing an
imbalance in the working lives of nurses. Some felt that
even talking about other worklife concerns served to
obscure the importance of this central issue:
The workload is getting to everybody these days. It’s
the sheer mental stress that is involved. You come
home and you bring it home with you and you’re just
exhausted because of the workload. You bring the
tiredness home, the stress levels home. (Nurse 8).
I think workload is everything. Work environment is
everything. I’ve stuck with it as long as I have
because of the people and the work environment I

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–2491 2489
used to have. This is very stressful, the way things are
here now. You’d always have a day where you had a
stressful day, that’s part of nursing, but you
shouldn’t have to work 150% every day. It gets to
the point where you can’t even say hello to a patient.
You should be able to breathe. You should be able to
work at a natural pace instead of always being
pressured and pushed. That’s what’s happening here
now. (Nurse 3).
The absence or insufficiency of non-nursing staff such
as porters interacted with and created other problems
for nursing staff. With porters in short supply, in some
institutions volunteers are helping with transport.
However, their participation is limited as the nurse still
has to get the patient onto the stretcher as volunteers are
not allowed to provide direct patient care. It is obvious
that the patient care requirements of the unit were not
necessarily reflected in the staff mix:
On weekends we’re still doing X-rays, we’re still
sending patients up to the OR, just like fromMonday
to Friday, but we’re down one nurse and we don’t
have a desk clerk after 3:00 pm. So when a new
patient comes in, the nurse is putting the chart
together, which has got a lot of documentation,
completing the requisitions, phoning for the electro-
cardiogram (ECG) because the patient is going to the
OR. Then you’ve got to phone the respiratory
technologist (RT) to do the ECG because there’s
no ECG technician on during the weekend. The
nurse is now answering the phone to the relatives,
putting the charts together, making all of these
arrangements while trying to look after her own set
of patients. Weekends are not fun! (Nurse 6).
It was often reported that technology had actually
increased nurses’ workload. Nurses’ suspected that most
technologies presented to them as labour-saving devices
actually increased workload and were used as an excuse
to reduce staffing or to introduce other organizational
economies. These perceptions highlight the dualism that
seems to occur between management and staff, each
with competing priorities and values (Traynor, 1999):
We have morphine pumps, epidural lines, femoral
lines, so you’re doing vital signs frequently. For post-
operative patients on a patient controlled-anesthesia
(PCA) pump, you have to do vitals every hour for
twelve hours. For five years we’ve had PCA pumps.
To change the rate of the cartridge now takes two
nurses. There are so many problems with the pumps
that for accountability—holy smokes! They haven’t
saved us any time. (Nurse 6).
Now we have very expensive monitors because you
have to be doing vital signs every 15min for a couple
of hours. So you’re in there all the time, it’s almost
one-on-one nursing care. But you don’t have one-on-
one staffing to support this. (Nurse 6).
One nurse said that she knew extra staffing was the
solution but also knew that funds did not exist to
implement it, causing her to feel hopeless about the
whole situation. This tendency for nurses to discuss the
financial state of their workplace demonstrates how the
language of fiscal rationing has permeated the nursing
workplace (Traynor, 1999). Another nurse who logged
24 patient care hours in a single shift wondered if anyone
noticed, again underscoring the dualism between man-
agement and the nursing staff (Traynor, 1999):
But if I were to say what the solution is, once again it
comes down to more staffing. And I know that’s not
going to happen because, the way it is now, we don’t
even have the funding for current staffing needs.
(Nurse 8).
I often wonder why we’re doing these things. Does
anyone ever look at that and say, ‘Wow, better not
let that happen again!’ (Nurse 3).
Discussion
The nurses who participated in this study varied in age
and years of experience in nursing, yet all had a similar
story to tell about their work environment. The findings
from this study illustrate the degree to which factors
such as patient acuity, workload and understaffing
shape the work environment for nurses and create
imbalance. The nurses’ narratives explored here suggest
that multiple factors constitute the nurses’ work
environment and their experiences and perceptions of
the work environment.
Nursing work environments: High effort and low reward
These work environment factors demonstrate a high-
effort workplace with little or no evidence of reward
conditions in place for nurses. Seigrist (2002) suggests
that the lack of balance between high effort and low
reward in work situations affects health. Preliminary
evidence of this is apparent in these narratives from
nurses with descriptions of absenteeism, taking home
feelings of guilt and excessive stress. The EFI model is
based on the notion of reciprocity, whereby the efforts
of the employee at work are reinforced through rewards
that are socially defined (Seigrist, 2004). A failure to
achieve reciprocity results in an imbalance with high
effort and low rewards. This results in decreased self
esteem and long-term stress for employees (Seigrist,
1996, 2004). Several studies have identified these

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–24912490
concerns in nursing work environments (Aiken et al.,
2001; Baumann et al., 2001; Kluska, Spence Laschinger,
& Kerr, 2004; McGillis Hall, 2003; O’Brien-Pallas et al.,
2004; Page, 2003).
Implications for policy makers and administrators
Several predictable issues surfaced repeatedly in the
interviews related to the changing needs of hospitalized
patients in today’s health care system, and the wide-
spread shortage of nurses. A crucial finding in this study
is the extent to which the nurse is impacted by the
adequacy of care they are able to provide. Nursing
practice is a profession, and nurses have an inherent
sense of caring in their work and a sensitivity to the
needs of their patients. These narratives outline the
tremendous burden of guilt that nurses bear when
factors in the work environment prevent them from
providing complete, quality care. As well, nurses
identified the key role they play in health care teaching
and preparing patients for their discharge back into their
homes and the community.
From the nurses’ perspective, the care they are
providing in today’s hospital health care environment
is inadequate. The perceptions that nurses have of access
to resources has been found to impact the amount of
ERI they experience (Kluska et al., 2004). Nurses are
experiencing frustration and stress that is impacting
their worklife, family and home life, as well as their
personal health. In telling their stories, these nurses have
provided an opportunity from which health care policy
makers and administrators can develop an understand-
ing of these experiences, and how these experiences are
shaping the practice of hospital nursing today. These
narratives about the nursing work environment will
inform interventions that can be tailored to improve the
quality of patient care that nurses are able to provide.
Nurses’ awareness of the impact of their own personal
behaviours on patients was evident. These narratives
may also serve to provide a mechanism by which nurses
can reflect on their practice in the work environment,
and how it impacts patient outcomes. This in turn could
have long-term implications on patient and system
outcomes.
The ERI model provides a useful tool for studying the
worklife of nurses. Government funding cutbacks in the
past decade have forced health care settings to
restructure and downsize nursing positions (McGillis
Hall, 2005). The result is a work environment that lacks
balance and is contributing to adverse outcomes for the
system (e.g., absenteeism) and the nurse (e.g., stress).
Using the information from these narratives, health care
administrators can re-examine the nursing work envir-
onment and the work of nurses within it. Tangible
efforts to redesign nursing work that involve nurses in
the process should lead to a better understanding of the
staffing required to maintain a safe and healthy patient
care work environment.
The importance of placing an emphasis on workplace
health is underscored in this study. Nurses are a
fundamental component of patient care delivery sys-
tems. Their work may not always be quantifiable in
strict fiscal terms. Nurses in this study demonstrated
patterns of coping with job demands that reflect
overcommitment to their work. It is apparent from this
study that stress-reduction approaches should be im-
plemented in nursing workplaces. These provide a
tremendous potential for intervention approaches that
can promote the esteem and recognition rewards that
nurses need to achieve balance in their work. Interven-
tions can be designed to provide direct support for
nurses dealing with real-life issues in the workplace. The
importance of listening to nurses’ stories about the
challenges they undergo in their workplaces can only
help to inform us of the key issues in the workplace that
need to be addressed for the successful retention of
nurses in the profession.
Acknowledgements
Funded by the Ministry of Health and Long Term
Care, Ontario, Canada.
References
Advisory Committee on Health Human Resources, (2002). Our
health, our future: Creating quality workplaces for Cana-
dian nurses. Final Report of the Canadian Nursing Advisory
Committee. Available from http://www.hc-sc.gc.ca.
Aiken, L. H., Clarke, S. P., Sloane, D. M., Sochalski, J. A.,
Busse, R., Clarke, H., et al. (2001). Nurses’ reports on
hospital care in five countries. Health Affairs, 20(3), 43–53.
Baumann, A., O’Brien-Pallas, L.O., Armstrong-Stassen, M.,
Blythe, J., Bourbonnais, R., Cameron, S., Irvine Doran,
D.I., Kerr, M., McGillis Hall, L., Vezina, M., Butt, M., &
Ryan, L. (2001). Commitment and care: the benefits of a
healthy workplace for nurses, their patients and the system—
A policy synthesis. Canadian Health Services Foundation &
The Change Foundation. Available from www.chsrf.ca and
www.changefoundation.ca.
Bowling, A. (1997). Unstructured interviewing and focus
groups. In . Research methods in health: Investigating health
and health services (pp. 336–351). Philadelphia: Open
University Press.
Britten, N. (2000). Qualitative interviews in health care
research. In C. Pope, & N. Mays (Eds.). Qualitative research
in health care (2nd ed., pp. 11–19). London: BMJ Books.
Burke, R. J., & Greenglass, E. R. (2000). Hospital restructuring
and downsizing in Canada: Are less experienced nurses at
risk? Psychological Reports, 87(3 Pt. 1), 1013–1021.

ARTICLE IN PRESSL. McGillis Hall, D. Kiesners / Social Science & Medicine 61 (2005) 2482–2491 2491
Cohen, L., & Manion, L. (1994). Research methods in education
(3rd ed.). New York, London: Routledge.
Greenglass, E. R., & Burke, R. J. (2001). Stress and the effects
of hospital restructuring on nurses. Canadian Journal of
Nursing Research, 33(2), 93–108.
Health Canada. (2001). Healthy nurses, healthy workplaces.
Ottawa, Canada: The Office of Nursing Policy: Health
Policy & Communications Branch, Health Canada.
Heitlinger, A. (2003). The paradoxical impact of health care
restructuring in Canada on nursing as a profession.
International Journal of Health Services, 33(1), 37–54.
Keddy, B., Gregor, F., Foster, S., & Denney, D. (1998).
Theorizing about nurses’ work lives: The personal and
professional aftermath of living with healthcare ‘reform’.
Nursing Inquiry, 6, 58–64.
Kluska, K. M., Spence Laschinger, H. K., & Kerr, M. S. (2004).
Staff nurse empowerment and effort–reward imbalance.
Canadian Journal of Nursing Leadership, 17(1), 112–127.
Koehoorn, M., Lowe, G.S., Rondeau, K.V., Schellenberg, G.,
& Wagar, T.H., (2002). Creating high-quality health care
workplaces. (CPRN Discussion Paper No. W|14). Retrieved
January 24, 2005, from the Canadian Health Services
Research Foundation Web site: http://www.chsrf.ca/final_
research/commissioned_research/programs/pdf/cr-cprn_e.pdf.
Lieblich, A., Tuval-Mashiach, R., & Zilber, T. (1998).Narrative
research: Reading, analysis and interpretation. Thousand
Oaks, CA: Sage.
Marrow, C. (1996). Using qualitative research methods in
nursing. Nursing Standard, 11(7), 43–45.
McGillis Hall, L. (2003). Nursing staff mix models and
outcomes. Journal of Advanced Nursing, 44(2), 217–226.
McGillis Hall, L. (2005). Strategies used to rebuild nursing
following restructuring. Canadian perspectives. Journal of
Research in Nursing, 10(1).
Nicklin, W., & McVeety, J. E. (2002). Canadian nurses’
perceptions of patient safety in hospitals. Canadian Journal
of Nursing Leadership, 15(3), 11–21.
Nursing Task Force. (1999). Good nursing, good health: An
investment for the 21st century. Ontario Ministry of Health.
O’Brien-Pallas, L., Thomson, D., McGillis Hall, L., Pink, G.,
Kerr, M., Wang, S., Li, X., et al. (2004). Evidence-based
standards for measuring nurse staffing and performance. Final
report. Toronto, ON: Canadian Health Services Research
Foundation.
Page, A. (2003). Keeping patients safe: Transforming the work
environment of nurses. Washington, DC: National Academy
Press.
Price, B. (2002). Laddered questions and qualitative data
research interviews. Journal of Advanced Nursing, 37(3),
273–281.
Sandelowski, M. (1991). Telling stories: Narrative approaches
in qualitative research. Image: Journal of Nursing Scholar-
ship, 23, 161–166.
Seigrist, J. (1996). Adverse health effects of high effort-low
reward conditions. Journal of Occupational Health Psychol-
ogy, 1, 27–41.
Seigrist, J. (2002). Effort–reward imbalance at work and health.
In P. L. Perrewe, & D. G. Ganster (Eds.), Historical and
current perspectives on stress and health. Research in
occupational stress and well being, vol. 2. Boston, MA: Jai
Press.
Seigrist, J. (2004). Adverse health effects of effort-reward
imbalance—applying the model to Eastern Europe. Re-
trieved January 27, 2005, from http://www.magtud.sote.hu/
siegrist.htm.
Seigrist, J., Starke, D., Chandola, T., Godin, I., Marmot, M.,
Niedhammer, I., & Peter, R. (2004). The measurement of
effort–reward imbalance at work: European comparisons.
Social Science & Medicine, 58, 1483–1499.
Traynor, M. (1999). Managerialism and nursing: Beyond
oppression and profession. London: Routledge.
Tsutsumi, A., Kayaba, K., Nagami, M., Miki, A., Kawano, Y.,
Ohya, Y., Odagiri, Y., & Shimomitsu, T. (2002). The
effort-reward imbalance model: experience in Japanese
working population. Journal of Occupational Health, 44,
398–407.
Wunderlich, G. S., Sloan, F. S., & Davis, C. K. (1996). Nursing
staff in hospitals and nursing homes: Is it adequate?.
Washington, DC: National Academy Press.
Zboril-Benson, L. R. (2002). Why nurses are calling in sick: The
impact of health-care restructuring. Canadian Journal of
Nursing Research, 33(4), 89–107.
Recommended