KEY FACTS AND FIGURES ON CARE FOR FRAIL OLDER PEOPLE
© 2014 Deloitte LLP. All rights reserved. www.deloitte.co.uk/centreforhealthsolutions
Health and social care spend on people aged65 and over, with at leastone long term conditionis increasing and iscurrently around
(£15 billion for those over 75)£30 billion
people aged 65 and over live incare homes, where average age is 85 and prevalence of dementiaover 70%
960,000 people aged 65 or over act as unpaid carers and
only 93,000receive support services
The number of carersworking more than
a week has doubled 50 hours
Over
414,000 people
In Scotlandimplementing telehealthand telecare cost around
providing grossbenefits valued at
80,000sheltered housing spaces and
67,000will be needed in London by 2041
care home places
£10 million
£48 million
The NHS funding gapis predicted to grow to
by 2021£30 billion
do not have a relevant qualification
Of the 1.56 million adult social care workers
almost 40%
In the next 20 years numberof UK over 65s are projectedto rise nearly
50%
1% in 1985,2% in 2010, 5% in 2035
Populationover 85
Over 65s accountfor
unplanned A&E admissions
2 millionOver the past 5 years A&E attendances for over 80s have
and those conveyed by ambulance by
increased 65%
75%
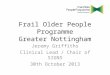
AN INTEGRATED MODEL OF CARE FOR FRAIL OLDER PEOPLE
AVOIDING ESCALATIONOF CARE
multidisciplinary teams of primary, community and social care staffworking together across the traditional boundaries
INTERMEDIATE CARE
PROMOTING RETURNTO HOME CARE POST ESCALATION
HOSPITAL CARE
HOME CARE
manage risk
plan for dischargeon admission• Trigger frailty patient alert on admission including alerting MDT discharge team
• Engage social care and adopt co-ordinated discharge plan on admission
promote selfmanagement• Support patients and carers to self-manage by providing guidance, education materials and advice service
• Use technology assisted support where indicated
early intervention• Commission prevention and early intervention strategies targeted at those with greatest need
• Provide all over 75s with annual health check
• Joint GP and consultant led service including consultant led community clinics and enhanced support to care homes
admit only when needed• Implement a referral gateway to control referrals and appropriate hospital use
• Priority access to diagnostic tests for patients at risk
better enablepatients to return home• Develop frailty pathway protocols to support efficient transition from hospital into home/intermediate care
• Multi-disciplinary team (MDT) agree on medical needs, post discharge
• Agree discharge plan with patient and carer
• Assign dedicated social worker to each patient on risk register to advise on eligibility and provide social care packages
enhance efficiencyof acute treatment• Provide access to patient records from multiple settings via IT solutions
• Implement a hospital frailty pathway including geriatric assessment and medication review
• Identify and register all patients over 75 and stratify according to risk of hospitalisation
• Develop electronic alert system to flag risks with all local providers ideally via shared electronic patient records
Provide hospital service via intermediate & primary care• Provide hospital input to primary care and care homes via technology e.g. telehealth
• Deliver hospital at home or other re-ablement service
• Upskill community and primary care workers
Recommended