ARTICLE IN PRESS
Sleep Medicine Reviews (2007) 11, 209–230
1087-0792/$ - sdoi:10.1016/j.s
�Correspondifax: +1 206 543
E-mail addr
www.elsevier.com/locate/smrv
CLINICAL REVIEW
A systematic review of valerian as a sleep aid:Safe but not effective
Diana M. Taibia,�, Carol A. Landisb, Heidi Petryc, Michael V. Vitiellod
aWomen’s Health Nursing Research Training Grant, Department of Family and Child Nursing, University ofWashington, Box 357262, Seattle, WA 98195-7262, USAbBiobehavioral Nursing and Health Systems, University of Washington, Box 357266, Seattle,WA 98195-7266, USAcUniversity of Washington Bothell, 18115 Campus Way NE, Box 358532, Bothell, WA 98011, USAdPsychiatry and Behavioral Sciences, Psychology and Biobehavioral Nursing and Health Systems, Universityof Washington, Box 356560, Seattle, WA 98195-6560, USA
KEYWORDSValerian;Sleep;Complementarytherapies;Herbal therapies;Insomnia
ee front matter & 2007mrv.2007.03.002
ng author. Tel.: +1 2066656.ess: [email protected]
Summary Valerian is an herb that is widely available in a variety of commercialpreparations and is commonly used as a sleep aid. A recent systematic review andmeta-analysis of valerian concluded that evidence in support of the effectiveness ofthe herb was inconclusive. Therefore, in an effort to more closely examine this issue,a systematic review was conducted to examine the evidence on the efficacy ofvalerian as a sleep aid with specific attention to the type of preparations tested andthe characteristics of the subjects studied. A comprehensive search of studiesinvestigating valerian was conducted through computerized databases and handsearches of reference lists. Standardized forms were used to summarize findings andstandardized criteria were used to assess study quality. Out of 592 articles initiallyidentified, a total of 36 articles describing 37 separate studies met criteria forreview: 29 controlled trials evaluated for both efficacy and safety, and eight open-label trials evaluated for safety only. Most studies found no significant differencesbetween valerian and placebo either in healthy individuals or in persons with generalsleep disturbance or insomnia. None of the most recent studies, which were also themost methodologically rigorous, found significant effects of valerian on sleep.Overall, the evidence, while supporting that valerian is a safe herb associated withonly rare adverse events, does not support the clinical efficacy of valerian as a sleepaid for insomnia.& 2007 Published by Elsevier Ltd.
Published by Elsevier Ltd.
543 3906;
ton.edu (D.M. Taibi).
Introduction
Approximately one-third of the adults in the UnitedStates report symptoms of insomnia; including

ARTICLE IN PRESS
D.M. Taibi et al.210
difficulty falling and/or remaining asleep at night.1
Herbal therapies are commonly used for chronicsymptoms of disturbed sleep. According to a recentsurvey, approximately 1.6 million Americans usecomplementary and alternative medical (CAM)therapies to treat their sleep disturbance.2 Valerianis among the top-selling herbals in the US and ismarketed as a promoter of restful sleep. In 2005,valerian was the 13th top-selling herb in US withestimated sales totaling $3.4 million.3
A previous systematic review4 and a recent meta-analysis5 both concluded that effects of valerian onsleep were promising, but inconclusive. Previousreviews have discussed various types of valerianproducts without specific attention to importantdifferences in source species and in preparationtechniques used (e.g., ethanol and water versusextractions with water alone). Because the chemi-cal constituents in valerian products vary depend-ing on species and extraction methods,6,7 failureto evaluate the evidence based on the type ofproduct used may have obscured an accurateassessment of valerian effects on sleep. The speciesused most commonly is Valeriana officinalis,although V. edulis (Mexican valerian) and V. wall-ichii (Indian valerian) are also used therapeutically.In general, extractions are prepared by soaking thedried root and rhizome (the underground portion ofthe stem) of valerian in a solution (called amenstruum), then centrifuging or drying the mix-ture to extract and concentrate plant constituents.The solutions used are typically: water alone,ethanol and water, or methanol and water. Theratio of alcohol to water affects the proportion ofconstituents obtained. According to the AmericanHerbal Pharmacopeia, extraction of valerenic acidsrequires at least 30% alcohol, whereas extraction ofvalepotriates requires 70% alcohol.7 The influenceof extraction on the physiological effects ofvalerian remains unknown because the relativecontributions of constituents responsible for to theplant’s sedative effects have not been determined,and effects may depend on synergy of variouscompounds (e.g., valerenic acids, amino acids,valepotriates).8
In this review, we evaluate the research evidenceon valerian as a sleep aid taking into account thetypes of products used. In addition, we consideredwhether the subjects in these studies were healthy,complained of general sleep disturbance, or metdiagnostic criteria for insomnia: Diagnostic andStatistical Manual of Mental Disorders (DSM-III/IV);International Classification of Diseases (ICD-9/10);or International Classification of Sleep Disorders(ICSD). Finally, we make a recommendation aboutits usefulness as a sleep aid and clarify areas in
which further research on valerian effects on sleepmight be useful.
Materials and methods
The search strategy sought to obtain all relevantpublished data-based articles based on the follow-ing general criteria: (1) valerian root was adminis-tered orally, either alone or in combination withhops, lemon balm, or passion flower (herbs com-monly combined with valerian in commercialpreparations); and (2) a subjective or objectivesleep measure (e.g., polysomnography or actigra-phy) was at least one of the study’s primaryoutcomes. A systematic computerized searchof research databases was performed usingthe following keywords (where * is a wildcard):valerian*, valerenic, valepotriate*, and baldrian(‘‘valerian’’ in German). Databases included in thesearch were Pubmed, the Cochrane Central Regis-ter of Controlled Trials, EMBASE, PsychINFO,CINAHL, International Pharmaceutical Abstracts,and Dissertation Abstracts. The search was limitedto human clinical trials in the databases thatallowed this specification (Pubmed, Cochrane,and EMBASE). Reference lists from relevant arti-cles, reviews, and book chapters were hand-searched to identify additional studies. The searchwas not limited by language because numerousstudies have been conducted in Europe, particu-larly in Germany, and reported in German-languagejournals.9 In order to obtain the widest range ofevidence on valerian, included studies were notlimited to randomized clinical trials (RCTs), butonly relevant full reports were evaluated (abstractswere excluded). Additionally, to fully explore theevidence on the sedative effects of valerian,studies of healthy persons without reported sleepdisturbance were included.
Data were extracted onto standardized forms.A quality score based on the likelihood of bias wasgiven to each study using the Jadad scoring system.In this system, studies are scored 0 (poor) to 5(good) based on descriptions of randomization,double-blind methods, and reporting of drop-outs.10 Methodological features were also reviewedusing the criteria of Stevinson and Ernst,4 with theadded criterion that adequate methods of blindingrequired masking of odor as well as appearance.These criteria included reporting of design ele-ments of the study (e.g., randomization andblinding, effect size or power estimates); potentialsources of bias and error (e.g., control of pre-bedtime variables); and measures to mask the

ARTICLE IN PRESS
Valerian as a sleep aid 211
strong, distinctive odor unique to valerian. Studieswere only assigned a point in the Jadad score foradequate description of blinding if both odor andappearance were addressed.
Results
Study characteristics and valerian productsused
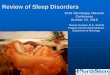
The computerized search yielded 592 article titlesthat were reviewed for relevance (see Fig. 1); 527articles were excluded based on a review of theabstracts and 29 were excluded based on a reviewof the full text. These 556 articles were excludedfor the following reasons: the articles (a) were notclinical studies (418 articles); (b) did not assesssleep as a primary outcome (65); (c) tested multi-ple herbs (other than hops, lemon balm, or passionflower) (6); (d) did not test an oral preparation ofvalerian (2); (e) were pediatric studies (2); (f) werenot related to valerian at all (55); (g) wereabstracts or incomplete reports (6); or (h) used astudy design that did not permit assessment ofvalerian effects (2).
Thirty-six articles describing 37 studies of valer-ian (one article reported two studies)11 for sleep inadults met criteria for inclusion in the review.Seventeen studies were published in German.12–28
The German was translated into English and dataextraction was checked against the articles inthe original language by one of the co-authors(H, Petry), whose first language is German.
There was pronounced heterogeneity of studydesign, especially in regard to: sample inclusion and
Initial search: 592 titles
Excluded: 556 from abstract or title- 527 from full article- 29
Not clinical trial- 418 Not addressing sleep- 65 Unrelated to valerian- 55 Not full report- 6 Multiple herbs- 6 Not oral administration- 2 Excessively biased- 2 Pediatric- 2
Included: 36 (describing 37 studies)
Trials: 28 (describing 29 trials)
Ethanolic- 8 Aqueous- 6 (7 trials) Valepotriate- 5 Combination- 9
Open-label: 8
Figure 1 Search results.
exclusion criteria; duration of treatment; prepara-tion used (valerian species and extraction meth-ods); dose given; dose timing (multiple daily dosesversus bedtime only); and outcomes measured.Of the 37 included studies, 29 were clinical trialsand 8 were open-label studies of clinical use.In the 29 clinical trials (see Table 1), thefollowing preparations were tested: (a) valerianmono-preparations (without other herbs, 20 stu-dies)11,13,17,21,25–27,29–39; (b) valerian with hops(6 studies),15,22,24,40,41 of which one also investi-gated a mono-preparation39; (c) valerian withlemon balm (3 studies)16,23,42; and (d) valerian withboth hops and lemon balm (1 study).43 Eight openlabel trials tested: (a) valerian alone (1 study)44;(b) with hops (2 studies)19,45; (c) with hops andlemon balm (3 studies)14,18,28; and (d) with hops andpassion flower (2 studies).12,20 Open-label trials arediscussed in regard to the safety and tolerability ofthe herb(s) but not for efficacy.
In this review, studies are grouped by extractiontype to allow for comparison of effects amongpreparations that are most likely to contain similarproportions of the various active constituents ofvalerian.
Ethanolic valerian extracts
Eight studies investigated ethanolic-aqueousV. officinalis extracts (see Table 2). All of thesestudies except one34 tested valerian in persons whoreported at least mild sleep disturbance, and moststudies based inclusion on clinical diagnosticcriteria for insomnia. Although some of the studiesreported the proportions of the sample withdifferent types of insomnia symptoms (e.g., sleeponset, sleep maintenance, or both), none ofthe studies analyzed the outcomes based on thespecific insomnia symptom. Compared to theliterature on other types of valerian preparations,studies of ethanolic extracts used the most rigorousstandards for recruiting participants with primaryinsomnia (see Table 1). However, only three studiesreported excluding persons with other primarysleep disturbances (e.g., sleep apnea, periodiclimb movement disorder, restless legs).13,33,34
The commercial preparation of valerian mostcommonly studied is LI 156 (Sedoniums), anethanolic extraction of V. officinalis (70% ethanolused for extraction). All six studies of this producttested 300–600mg prior to bedtime (see Table 2).Only two of these studies measured polysomno-graphic (PSG) sleep outcomes.30,33 In a double-blind randomized crossover trial, Diaper andHindmarch30 compared two doses (300 and

ARTICLE IN PRESS
Table
1Sample
charac
teristicsof
valerian
stud
ies.
Stud
y,ye
arSample
size
Slee
pco
ndition
Age
Female
Exclusions
Other
slee
pdisorder
Med
ical
cond
itions
Psych
iatric
problems
Med
ication
affecting
slee
p
Etha
nolicV.
officina
lisex
tracts
Vorbac
het
al.1
7(199
6)12
1(61va
lerian
,60
place
bo)
Insomnia,
V:47
.2711
V:62
%+
++(nouse
within14
day
s)ICD-10criteria
P:47
.6711
.1P:55
%
Kuhlman
net
al.3
4(199
9)10
2(51va
lerian
,51
place
bo)
Insomnia,
V*:
40.878.7
V:51
%+
++
ICD-10criteria
P*:
42.379.0
P:65
%Don
athet
al.3
3(200
0)16
Insomnia,
All,Med
ian:
49All:75
%+
++
+ICSD
criteria
(ran
ge:22
–55
)(14day
s)Dorn1
3(200
0)75
(39va
lerian
,36
oxazep
am)
Insomnia,
V:50
.6712
.4V:
77%
++
++
ICD-10criteria
O:53
.9712
.0O:61
%(4
wee
ks)
Zieg
leret
al.3
2(200
2)18
6(93va
lerian
,93
oxazep
am)
Insomnia,
V:54
.2712
.3V:
73%
++
+ICD-10criteria
O:50
.6712
.6P:61
%(past3
mon
ths)
(4wee
ks)
Cox
eter
etal.3
1(200
3)21
Diagn
osed
insomnia
All:54
715
All:54
%+
++
Jaco
bset
al.2
9(200
3)39
1(135
valerian
,12
1ka
vaka
va,
135place
bo)
Reporteddifficu
lty
withslee
pon
setor
mainten
ance
within2
wee
ks
V:42
.7710
V:79
%Anx
iety
required,
dep
ression
allowed
+K:41
.1710
K:80
%P:40
.5710
P:88
%
Diaper
andHindmarch
30
(200
4)16
Mildslee
pco
mplaints
All:55
.97
4.7
V:62
%+
P:55
%
Aqu
eous
V.officina
lisex
tracts
Leathw
oodet
al.4
6(198
2);
Leathw
oodan
dCha
uffard
39
(198
2/19
83)
166
Gen
eral
voluntee
rs(noslee
pproblem
required)
NR
NR
D.M. Taibi et al.212

ARTICLE IN PRESS
Leathw
oodet
al.4
6(198
2);
Leathw
oodan
dCha
uffard
39
(198
2/19
83)
10Gen
eral
voluntee
rs(noslee
pproblem
required)
All:29
73.2
All:0%
Kam
m-Koh
let
al.2
1(198
4)78
(39va
lerian
,39
place
bo)
Elder
homeresiden
ts,
beh
avioralslee
pdisturban
cerequired
V:70
.674.4
V:76
%Beh
avioral
disturban
cerequired
+
P:69
.473.9
P:74
%Balderer
andBorbely1
1
(198
5)10
Hea
lthy,no
slee
pdisturban
ceAll:32
.5(ran
ge:
22–44
)All:50
%
Balderer
andBorbely1
1
(198
5)8
Hea
lthy,no
slee
pdisturban
ceAll:22
.6(ran
ge:
21–26
)All:50
%
Leathw
oodan
dCha
uffard
38
(198
5)8
Slee
pon
setproblems
All:45
(SDNR)
All:37
%
Schu
lzet
al.3
7(199
4)14
Elderly,insomnia
All:61
.67
6.5
All:10
0%+
++(14day
s)
High-va
lepo
triate
prep
arations
Jansen
27(197
7)15
0(74va
lerian
,76
place
bo)
Not
spec
ified
,elder
homeresiden
tsV:
78.4
V:61
%(ran
ge62
–89
)P:51
%P:78
.8(67–
89)
Gessner
etal.2
6(198
3)20
(11va
lerian
,9place
bo)
Diagn
osed
slee
pdisturban
ceAll,rang
e:19
–68
All:57
%+
Gessner
andKlasser
25(198
4)11
Slee
pdisturban
cean
dge
neralne
rvou
sco
nditions
All:26
.1(ran
ge:
20–38
)All:45
%+
Herrera-Arellan
oet
al.3
6(200
1)20
Insomnia,
All:45
77.8
All:70
%+
DSM
-III-Rcriteria
Poya
reset
al.3
5(200
2)19
patients,
18co
ntrols
Insomnia,
All:43
.3710
.6All:80
%+
+Re
quired
DSM
-IVcriteria,
chronicBZD
use;
healthyco
ntrols
+BZD
use-
withd
rawn
Com
bina
tion
prep
arations:va
lerian
andho
psMuller-Limmroth
and
Ehrenstein
22(197
7)12
Self-rep
ortedslee
pdisturban
ceAll,rang
e:22
–27
All:50
%
Roden
bec
ket
al.2
4(198
8)15
(8va
lerian
,7place
bo)
Insomnia,
V:45
.4711
.6,
NR
++
ICSD
criteria
P:47
.6712
.5Schm
itzan
dJackel
15(198
8)46
(23va
lerian
,23
bromazep
am)
Insomnia,
All:50
.3713
.6All:80
%+
+DSM
-IVcriteria
Fussel
etal.4
1(200
0)30
Mildto
mod
erate
insomnia
All*:
57.678.1
A:70
%+
+
Morin
etal.4
0(200
5)18
4(59va
lerian
,65
place
bo,
60diphe
nhyd
ramine)
Mildinsomnia,
V:43
.9710
.5V:
59%
++
++
DSM
-IVor
P:45
.2710
.2P:60
%ICSD
criteria
D:43
.879.7
D:60
%
Valerian as a sleep aid 213

ARTICLE IN PRESS
Table
1(con
tinu
ed)
Stud
y,ye
arSample
size
Slee
pco
ndition
Age
Female
Exclusions
Other
slee
pdisorder
Med
ical
cond
itions
Psych
iatric
problems
Med
ication
affecting
slee
p
Com
bina
tion
prep
arations:va
lerian
andlemon
balm
Lind
ahlan
dLind
wall43
(198
9)27
Slee
pdisturban
cean
dfatigu
eAll:54
(ran
ge25
–68
)All:30
%
Dressinget
al.2
3(199
2)20
Not
spec
ified
,he
althy
All:37
.275.9
All:50
%+
+
Dressinget
al.1
6(199
6)49
(25va
lerian
,24
place
bo)
Insomnia,
DSM
-IIIor
ICD-10criteria
V:59
.0(ran
ge31
.2–86
.8)
V:26
%+
++
+
P:54
.2(ran
ge22
.1–81
.4)
P:29
%
Cerny
andSchm
id42(199
9)98
(66va
lerian
,32
place
bo)
Noreportedslee
pproblems
V:33
.4712
.5V:
42%
++
+P:34
.8711
.7P:37
%
*Mea
n7SD
calculated
from
inform
ationgive
nin
thearticle.
NR,no
treported.
Insomniadiag
nostic
guides:ICD,Internationa
lClassifica
tion
ofDisea
ses;
DSM
,Diagn
ostican
dStatistica
lMan
ual;ICSD
,Internationa
lClassifica
tion
ofSlee
pDisorders.
D.M. Taibi et al.214

ARTICLE IN PRESS
Table
2Stud
iesof
valerian
forslee
p.
Stud
y,ye
arSample
with
slee
pdisturban
ce
Stud
ydesign
Interven
tion
Trea
tmen
tduration
Outco
me
mea
sures
Mainva
lerian
slee
pou
tcom
esAdve
rseeffects
Etha
nolicex
tracts
Vorbac
het
al.1
7(199
6)Yes
PDB,RCT
(a)Va
lerian
600mg
28nigh
tsSF-B
Nosign
ifica
ntdifferenc
efrom
place
boAErelatedto
valerian
:he
adac
he(n¼
2),
morning
hang
over
(n¼
1)(b)Place
bo
Kuhlman
net
al.3
4
(199
9)No
PDB,RCT
(a)Va
lerian
600mg
14nigh
tsVIS-M
,VIS-A
Nosign
ifica
ntdifferenc
efrom
place
boAEdifferenc
esbetwee
ntrea
tmen
tsno
tsign
ifica
nt,no
seriou
sAE
(b)Place
bo
Don
athet
al.3
3(200
0)Yes
PDB,RCT,
C/O
(a)Va
lerian
600mg
14nigh
tsPSG
,slee
pdiary,
slee
pque
stionn
aire
(VASrating
s)
Nosign
ifica
ntdifferenc
efrom
place
boAErelatedto
valerian
:he
adac
he(n¼
1),GI
complaints
(n¼
1)(b)Place
bo
Dorn1
3(200
0)Yes
DB,RCT
(a)Va
lerian
600mg
28nigh
tsSF-B
Valerian
versus
baseline:
mSQ
;no
sign
ifica
ntdifferenc
ebetwee
nva
lerian
andox
azep
am
Withd
rawalsrelatedto
trea
tmen
t:va
lerian
(n¼
2),ox
azep
am(n¼
3)
(b)Oxa
zepam
10mg
Zieg
leret
al.3
2(200
2)Yes
DB,RCT
(a)Va
lerian
600mg
42nigh
tsSF-B
Valerian
versus
baseline:
mSQ
;no
sign
ifica
ntdifferenc
ebetwee
nva
lerian
andox
azep
am
AE:
valerian
(n¼
29),
oxazep
am(n¼
36)
(b)Oxa
zepam
10mg
Han
gove
reffects:
valerian
(n¼
2),
oxazep
am(n¼
6)Cox
eter
etal.3
1(200
3)Yes
PDB,n-of-1
design*
(a)Va
lerian
450mg
7nigh
tsSlee
pdiaries
Nosign
ifica
ntdifferenc
efrom
place
boAEdifferenc
esbetwee
ntrea
tmen
tsno
tsign
ifica
nt(b)Place
bo
Jaco
bset
al.2
9(200
3)Yes
PDB,RCT
(a)Va
lerian
,6.4mg
valerenicac
id28
nigh
tsISI
Nosign
ifica
ntdifferenc
efrom
place
boSign
ifica
ntly
grea
ter
inciden
ceof
diarrhe
awithva
lerian
(b)Kav
aka
va,
100mg,
Kav
alac
tone
s(c)Place
bo
Valerian as a sleep aid 215

ARTICLE IN PRESS
Table
2(con
tinu
ed)
Stud
y,ye
arSample
with
slee
pdisturban
ce
Stud
ydesign
Interven
tion
Trea
tmen
tduration
Outco
me
mea
sures
Mainva
lerian
slee
pou
tcom
esAdve
rseeffects
Diaper
and
Hindm
arch
30(200
4)Yes
PDB,RCT,
C/O
(a)Va
lerian
300mg
1nigh
tPSG
,LSEQ
Nosign
ifica
ntdifferenc
efrom
place
boAEpossibly
relatedto
trea
tmen
ts:va
lerian
300mg(n¼
11),
valerian
600mg(n¼
4),place
bo(n¼
8)
(b)Va
lerian
600mg
(c)Place
bo
Aqu
eous
extracts
Leathw
oodet
al.4
6
(198
2);Le
athw
oodan
dCha
uffard
39(198
2/19
83)
No
PC,C/O
(a)Va
lerian
800mg
2nigh
tsPSG
,slee
pque
stionn
aire
Nosign
ifica
ntdifferenc
efrom
place
boNot
men
tion
ed(b)Place
bo
Leathw
oodet
al.4
6
(198
2);Le
athw
oodan
dCha
uffard
39(198
2/19
83)
No
PDB,RCT,
C/O
(a)Va
lerian
400mg
3nigh
tsSQ
andSL
improve
men
trating
s
Valerian
versus
place
bo:
grea
terproportion
sreportedim
prove
dSQ
and
SL
Noresidu
alsedation
(b)Va
lerian
–ho
ps
400mg
(c)Place
boKam
m-Koh
let
al.2
1
(198
4)Yes
PDB,CCT
(a)Va
lerian
90mg
3x/d
14nigh
tsSlee
pque
stionn
aire
Valerian
versus
place
bo:
grea
terproportion
sreportedim
prove
dSL
and
slee
pmainten
ance
Dizzine
ss(4
total):
valerian
(n¼
2),place
bo(n¼
2)(b)Place
bo
(Likertscales)
Balderer
andBorbely1
1
(198
5)No
PDB,CCT,
(a)Va
lerian
450mg
1nigh
tSlee
pdiary,slee
pqua
lity
(VAS)
Valerian
versus
place
bo:
kWASO
andSL,both
doses
Noresidu
alsedation
C/O
(b)Va
lerian
900mg
(c)Place
boBalderer
andBorbely1
1
(198
5)No
PDB,RCT,
C/O
(a)Va
lerian
900mg
1nigh
tPSG
Nosign
ifica
ntdifferenc
efrom
place
boNoresidu
alsedation
(b)Place
bo
Leathw
oodan
dCha
uffard
38(198
5)Yes
PDB,RCT,
C/O
(a)Va
lerian
450mg
4nigh
tsActigraph
y,slee
pque
stionn
aire
Valerian
versus
place
bo:
Sign
ifica
ntly
grea
ter
morning
slee
pnesswith
900mgdose,
noothe
rAE
(b)Va
lerian
900mg
Actigraphy
:k
SL,both
doses
(c)Place
boSR
:Nosign
ifica
ntdifferenc
efrom
place
boSchu
lzet
al.3
7(199
4)Yes
PDB,RCT
(a)Va
lerian
,12
15mgon
nigh
t1,
405mg3x
/dday
s2–
8;
8nigh
tsPSG
,slee
pdiaries,SF-A,SF-
B
Valerian
versus
place
bo:
PSG
:sign
ifica
nceNRSR
:Nosign
ifica
ntdifferenc
efrom
place
bo
Not
men
tion
ed
(b)Place
bo
Valepo
triate
prep
arations
Jansen
27(197
7)No
PDB,RCT
(a)Va
lerian
,10
0mg
valepotriates
3x/d
30nigh
ts4-po
intsymptom
rating
scales
kSlee
pdisturban
ce,
valerian
4place
bo(statistical
testingNR)
NoAEoc
curred
(b)Place
bo
D.M. Taibi et al.216

ARTICLE IN PRESS
Gessner
etal.2
6(198
3)Yes
PDB,CCT,
C/O
,(a)V.
edulis,24
0mg
valepotriates
9nigh
tsVIS-M
,VIS-A,SF-
A,SF-B
Valerian
versus
place
bo:
mSQ
andk
SLk
bad
dream
swith
valerian
.(b)Place
bo
Noothe
rsign
ifica
ntAE
differenc
esbetwee
ntrea
tmen
tsGessner
andKlasser
25
(198
4)Yes
PDB,RCT,
C/O
(a)V.
edulis,60
mg
valepotriates
1nigh
tPSG
,slee
pque
stionn
aires
PSG
:k
Stag
e4with
120mgve
rsus
place
boNoha
ngov
ersymptoms
(b)V.
edulis,12
0mg
valepotriates
SR:Nosign
ifica
ntdifferenc
efrom
place
bo(c)Place
boHerrera-Arellan
oet
al.3
6(200
1)Yes
DB,RCT,
C/O
(a)V.
edulis,45
0mg
1nigh
tPSG
,slee
pine
ssVe
rsus
baseline:
Dyspep
sia(3
total):
(b)V.
officina
lis
450mg
VAS
V.ed
ulis
knu
mbe
rof
awak
enings.
V.ed
ulis
(n¼
1),
V.officina
lis(n¼
2)Nosign
ifica
ntdifferenc
ebetwee
nva
lerian
preparations
Poya
reset
al.3
5(200
2)Yes
PDB,RCT
(a)V.
wallich
ii,
100mg
valepotriates
3x/d
15nigh
tsPSG
,slee
pdiaries,slee
pqua
lity
(VAS)
Valerian
versus
place
bo:
PSG
:k
WASO
,m
SLSR
:m
SQ
AEwithva
lerian
(n¼
3GI
complaints)
(b)Place
bo
Stud
yde
sign
abbrev
iation
s:CCT:
controlled
clinical
trial(non
-ran
dom
ized
);C/O
:crossove
r;DB:dou
ble-blind
(noplace
boco
ndition);PC:place
bo-con
trolled(not
dou
ble-blind
);PDB:
place
bo-con
trolleddou
bleblind
;RCT:
rand
omized
clinical
trial.Outcomemea
sures:
AE,
adve
rseev
ent;
NR,no
treported;
PSG
,polysom
nograp
hy;SF-A,Gortelm
eyer
Schlaffrag
ebog
enA,assesses
slee
pqua
lity
forthepastnigh
t;SF-B,Gortelm
eyer
Schlaffrag
ebog
enB,assesses
slee
pqua
lity
forthetw
owee
ks;SL,slee
platenc
y;SQ
,slee
pqua
lity;SR
,self-rep
ort;
VAS,
visual
analog
scale;
VIS
–M,Visua
lana
logska
la–Morge
n(a
stan
dardized
setof
visual
analog
scales
ofslee
pco
mpletedin
themorning
);WASO
,wak
eafterslee
pon
set.
Valerian as a sleep aid 217

ARTICLE IN PRESS
D.M. Taibi et al.218
600mg) of LI 156 to a placebo after one night in asample of persons with mild sleep complaints. Nosignificant differences were found on PSG orsubjective sleep outcomes (sleep efficiency, sleeplatency, awakenings, sleep stages, and sleepquality ratings). Another double-blind randomizedcrossover study tested 600mg LI 156 for 14 nights inpersons with insomnia.33 In the valerian group,percent slow wave sleep (SWS, NREM Stages 3 and 4which are considered deep sleep) was increasedcompared to baseline. No differences betweenvalerian and placebo were found in other PSGoutcomes or subjective sleep quality ratings.
The other four double-blinded studies of LI 156measured only subjective outcomes. Parallel-grouprandomized controlled trials (RCTs) comparedrepeated dosing of valerian versus placebo inhealthy individuals for 14 days34 or in persons withinsomnia for 28 days.17 Subjective sleep qualityratings improved in the valerian groups of bothstudies, but in neither case was sleep significantlyimproved when compared to placebo. Lack ofsignificance in the healthy sample34 may haveresulted from a ceiling effect. One of thesestudies,34 as well as two other RCTs,13,32 comparedLI 156 (600mg dose) to benzodiazepines (flunitra-zepam and oxazepam). In these studies, theeffectiveness of the benzodiazepines was assumed,and comparable effects of valerian and benzodia-zepines were presumed to confirm the effective-ness of valerian. Kuhlmann et al.34 reportedreduced subjective sleep latency and increasedsleep quality ratings with both valerian andflunitrazepam compared to placebo after a singlenight in a sample of healthy persons, but did notreport the statistical significance of these findings.Two other studies compared valerian and oxazepamfor four weeks13 or six weeks32 in persons withinsomnia. The studies reported significant improve-ment of subjective sleep quality ratings comparedto baseline with both valerian and oxazepam.Improvement did not significantly differ betweenthe treatments, indicating that the effects ofvalerian were equivalent to oxazepam.
Two studies investigated ethanolic valerian ex-tracts other than LI 156. In a double-blind RCT,Jacobs et al.29 compared 28 days of valerianextract (PureWorld Botanicals, 70% ethanolic ex-tract), kava kava extract, or placebo in personswith both sleep disturbance and anxiety. Insomniaseverity index (ISI) scores, subjective sleep latency,and subjective awakenings were reduced with allthree treatments, but the magnitude of improve-ment was greatest in the placebo group and neitherof the herbal treatments differed significantly fromplacebo. Another double-blind study used n-of-one
methods (a within-subject repeated crossover de-sign) to test a high-ethanol (96%) extraction ofvalerian.31 Because this product used an ethanolconcentration over 70% for extraction, the productcontained significant amounts of valepotriates(valtrate) as well as valerenic acid. Each partici-pant was tested for six one-week periods (threevalerian, three placebo) in random order. Treat-ment was considered a success or failure withineach individual based on whether the individualimproved during the weeks of valerian compared tothe weeks of placebo treatment. The analysesshowed valerian to be equivalent to placeboon subjective outcomes of sleep quality, sleeplatency, awakenings, total sleep time, and morningrefreshment.
In sum, ethanolic extracts of V. officinalis,several of which were investigated using rigorousstudy designs, have not been shown to significantlyaffect objective30,33 or subjective17,29,31,33,34 sleepoutcomes in comparison to placebo in subjects withand without insomnia. However, these preparationshave been shown to improve subjective sleepquality ratings in a manner equivalent to benzo-diazepines under the assumption that the benzo-diazepines tested were superior to placebo.13,32
Aqueous valerian extracts
Seven studies (reported in six publications) inves-tigated the effects of aqueous V. officinalis extracts(water alone is used for extraction) on sleep (seeTable 2). These studies varied greatly in methodo-logical quality, and several of the trials did notreport randomization to treatment procedures. Allof these studies reported using a double-blinddesign except for one.39 Four of these studies wereconducted in general volunteers who were notrequired to complain of a sleep disturbance,11,39,46
one in persons with sleep onset difficulties,38 andtwo in elderly persons with sleep disturbance.21,37
None of the studies used insomnia diagnosticcriteria as inclusion criteria, and none reportedexclusion of persons with primary sleep disorders(see Table 1). Only one study excluded medicalconditions that could contribute to sleep distur-bance37 and only two excluded concurrent use ofsleep-altering medications.21,37
Two parallel-group clinical trials investigated acommercially available aqueous valerian extract(Valdisperts) in elderly individuals with insomnia.In a randomized trial, Schulz et al.37 investigated405mg valerian extract or placebo given threetimes a day for eight days to elderly participantswith sleep onset and sleep maintenance problems.

ARTICLE IN PRESS
Valerian as a sleep aid 219
Objective (PSG) and subjective sleep outcomes(sleep efficiency, wake after sleep onset (WASO),sleep quality rating) did not differ significantlybetween valerian and placebo after one dose, butno statistical comparison of valerian and placebo isreported at the end of treatment (after eightnights). Another trial of elderly persons with sleepdisturbances, Kamm-Kohl et al.21 investigated90mg of Valdisperts or placebo three times dailyfor 14 days. When asked whether their sleep onsetand maintenance difficulties improved, signifi-cantly greater proportions of persons on valerianreported that these conditions were ‘‘better’’(versus ‘‘the same or worse’’) after treatment thanthose on placebo.
Several studies investigated a specific aqueousvalerian extract (Dixa S.A., Switzerland) in generalvolunteers (only one of these studies required sleepdisturbance for enrollment).38 An early randomizedcrossover trial by Leathwood and colleagues46
measured subjective sleep in general volunteers(no exclusions noted) with 400mg aqueous valerianextract (Dixa S.A., Switzerland) or placebo takenon two nights each in random order (a 400mgvalerian/hops extract was also tested, discussedlater). A significantly greater proportion of personsrated their sleep quality as ‘‘better than usual’’ andsleep latency as ‘‘shorter than usual’’ when givenvalerian than when given placebo. Improved sleepwas more pronounced in the sub-sample of personsreporting habitually poor sleep. In a double-blindcrossover trial (randomization not reported), Bal-derer and Borbely11 investigated 450 and 900mg ofvalerian extract (Dixa S.A., Switzerland) in 10healthy young persons. One night of valeriansignificantly decreased subjective sleep latencyand WASO but not sleep quality ratings comparedto the placebo. Two studies measured PSG sleepoutcomes. In a small crossover trial, Leathwood andcolleagues39,46 investigated the effects of twonights of valerian extract (400mg, Dixa S.A.,Switzerland) on the sleep of 10 young, healthymen. No significant differences between thevalerian and placebo were found on PSG sleepmeasures (total sleep time, % sleep stages). Inanother crossover trial, Balderer and Borbely11
tested two doses (450 and 900mg) of the sameextract (Dixa S.A., Switzerland) for one night ofeach dose (or placebo) in eight healthy youngpersons. Neither PSG nor subjective sleep outcomes(sleep latency, awakenings, WASO, time in sleepstages) differed significantly between valerianand the placebo. Finally, one study measuredobjective sleep using actigraphs (wrist-worn move-ment detectors that can discriminate waking fromsleep behavior) in addition to subjective outcomes.
In this double-blind crossover trial by Leathwoodand Chauffard38 each of three treatment conditions(450mg valerian, 900mg valerian, Dixa S.A.,Switzerland, or placebo) was given randomly over12 weeknights to individuals with difficulty fallingasleep (recruited from the research staff andfamilies), with the participants undergoing fournights per treatment condition. Both doses sig-nificantly reduced actigraphic sleep latency com-pared to the placebo. Subjective sleep latency andsleep quality ratings did not differ significantlyfrom the placebo. Morning sleepiness was signifi-cantly greater with the 900mg valerian dose thanthe placebo, suggesting dose-dependent effects.
In sum, studies testing the effects of aqueousvalerian extracts produced mixed results. In olderpersons with sleep disturbance, one study reportedthat a significant proportion of the sample reported‘‘better’’ sleep,21 whereas another study did notshow significant effects on either objective orsubjective sleep outcomes.37 Short-term supple-mentation (one to four nights) of valerian was notshown to affect PSG11,39 or subjective sleep out-comes11,38,39 in subjects without known sleepcomplaints, but valerian did reduce subjectivesleep latency and WASO with sleep onset insom-nia.38 The findings of these studies of aqueousvalerian extracts cannot be generalized to personsdiagnosed with insomnia because this type ofproduct has not been rigorously tested in clinicpopulations.
Valepotriate preparations
Five studies investigated valerian extractions stan-dardized on valepotriate content (see Table 2). Thisconstituent is minimally present in the V. officinalisspecies or extractions from this species. However,valepotriates are present in significant levels inother Valeriana species (V. edulis and V. wallichii)and are believed to be largely responsible forpurported clinical effects of preparations fromthese species. The studies of valepotriates variedin the products used, samples studied, and timingof administration (e.g., several times/day and/orat bedtime). Information on valerian extractionmethod was only available from one study.36 Aswith the studies of aqueous extracts, none of thestudies used insomnia diagnostic criteria for inclu-sion (see Table 2). One study excluded subjectsfor primary sleep disorders (other than insomnia),35
two excluded subjects for co-morbid sleepdisturbance,25,35 and three excluded subjects forcurrent use of sleep-altering medications26,35,36
(see Table 1).

ARTICLE IN PRESS
D.M. Taibi et al.220
Three studies investigated extracts of V. edulisspecies. Herrera-Arellano and colleagues36 com-pared two types of valerian extracts, V. edulis(high-valepotriate, 450mg, 62% ethanol extraction)and V. officinalis (high-valerenic acid, 450mg,information on extraction method not available)in a double-blind crossover study of persons withdiagnosed insomnia. There were no significantdifferences between the two species on any PSGoutcome (sleep latency, sleep efficiency, sleepstages), but the overall effects of either prepara-tion are uncertain because the study did notinclude a placebo group. Two of the studies wereplacebo-controlled, double-blind crossover trials(Gessner and Klasser; Gessner et al.)25,26 andinvestigated the effects of V. edulis (HarmonicumMuchs) on sleep in persons with general sleepdisturbance. In one study26 that assessed onlysubjective sleep outcomes, nine nights of valerian(standardized to contain 120mg valepotriates)significantly improved subjective sleep qualityratings and reduced subjective sleep latencycompared to placebo. In the other study, whichassessed the effects of 60 or 120mg valepotriateson PSG outcomes,25 one night of valerian signifi-cantly reduced Stage 4 sleep in comparison toplacebo. Neither dose significantly affected otherPSG outcomes.
Two other studies tested a preparation standar-dized to valepotriate content. One study tested theeffects of a V. wallichii extract (Valmanes) onrebound sleep disturbances in persons with insom-nia following gradual cessation of chronic benzo-diazepine use.35 In this double-blind, placebo-controlled RCT, a 100mg dose of valepotriateswas given three times daily for 15 days. Subjectivesleep quality ratings improved significantly withvalerian compared to the placebo. PSG outcomesshowed reduced WASO. A significant and substantialreduction in sleep latency occurred with placebobut not with valerian. The authors suggested thatthis may have been related to individual differ-ences in withdrawal from benzodiazepines. In aplacebo-controlled, double-blind RCT, geriatricclinic patients were given 100mg valepotriates(species and preparation not reported) three timesdaily for 30 days.27 When asked to rate whethertheir sleep disturbance was better, the same, orworse, both the valepotriate and placebo groupsreported improvement. Improvement was greaterin the valepotriate group, but no statisticalcomparisons were reported.
Overall, the literature on valepotriate prepara-tions provides limited evidence that valepotriatesmay improve sleep, but these studies are highlyvaried. Compared to placebo, studies reported
significantly improved sleep quality ratings inpersons withdrawing from benzodiazepines35 andpersons reporting disturbed sleep.25 One of thesestudies also reported reduced awakening versusbaseline but used no placebo control.36 Thesefindings suggest that valepotriate preparationsmay mildly reduce sleep disturbances. Like aqueousvalerian preparations, high-valepotriate prepara-tions have not been rigorously tested in personsdiagnosed with insomnia and extrapolation fromthe few studies available suggests such efficacywould be limited.
Valerian combination preparations
Many of the valerian products commercially avail-able are combinations with other herbs includinghops, lemon balm, and/or passion flower, all ofwhich purportedly have their own sedating ortranquilizing effects. It is possible that thesecombinations produce synergy and thus are moreeffective than each of these component herbsalone. Controlled studies have investigated onlycombinations of valerian with hops and/or lemonbalm. Most of these studies were in persons withinsomnia15,24,40,41 or those with a general com-plaint of sleep disturbance,22,43 although threestudies recruited healthy persons without requiringsleep disturbance.16,23,42 The specificity of exclu-sion criteria was thorough in some studies, but notin others (see Table 1). Only two of 10 studiesreported screening for primary sleep disordersother than insomnia as well as medical conditionsaffecting sleep, psychiatric problems, and medica-tions affecting sleep.23,40 Most of the other studiesscreened for some but not all of these criteria, buttwo studies did not report screening for any ofthese criteria.
Six studies investigated valerian–hops combina-tions (see Table 3). Three studies investigated theeffects of the valerian–hops combination ZE 91019(Allunas, methanolic-aqueous extract, % alcoholproprietary) on sleep. Two of these studies weredouble-blind, placebo-controlled RCTs that com-pared four weeks of ZE 91019 (500mg valerian/120mg hops24; 374mg valerian/82mg hops)40 toplacebo in persons with insomnia (ICD or DSM-IVcriteria). In these two studies, neither PSG out-comes24,40 nor subjective outcomes (sleep effi-ciency, sleep latency, ISI scores)40 improved or weresubstantially different between valerian–hopsand placebo. In a one-group study of personswith mild to moderate insomnia, Fussel et al.41
reported reduced sleep latency and increasedsleep efficiency measured by PSG with ZE 91019

ARTICLE IN PRESS
Table
3Stud
iesof
valerian
combinationproduc
tsforslee
p.
Stud
y,ye
arSample
with
slee
pdisturban
ce
Stud
ydesign
Interven
tion
Trea
tmen
tduration
Outco
me
mea
sures
Mainslee
pou
tcom
esAdve
rseeffects
Valerian
andHop
sMuller-Limmroth
and
Ehrenstein
22(197
7)Ye
sPDB,CCT,
C/O
,Ex
perim
ental
slee
pdisturban
ceby
trafficno
ise
(a)Va
lerian
–ho
ps24
0mg/
400mg
1nigh
tPSG
Nosign
ifica
ntdifferenc
efrom
place
bo
Not
men
tion
ed
(b)Place
bo
Leathw
oodet
al.4
6(198
2);
Leathw
oodan
dCha
uffard
39
(198
2/19
83)
No
PDB,RCT,
C/O
(a)Va
lerian
400mg
3nigh
tsSlee
pque
stionn
aire
Nosign
ifica
ntdifferenc
ebetwee
nva
lerian
–ho
ps
andplace
bo
Noresidua
lsedation
(b)Va
lerian
–ho
ps40
0mg
(c)Place
bo
Roden
bec
ket
al.2
4(199
8)Ye
sPDB,RCT
(a)Va
lerian
–ho
ps50
0mg/
120mg
28nigh
tsPSG
Nosign
ifica
ntdifferenc
efrom
place
bo
Not
men
tion
ed
(b)Place
bo
Schm
itzan
dJackel
15(199
8)Ye
sDB,RCT
(a)Va
lerian
–ho
ps20
0mg/
45mg
14nigh
tsSF-A,SF-B
Valerian
–ho
psve
rsus
baseline:
mSQ
;no
sign
ifica
ntdifferenc
ebetwee
nva
lerian
and
bromazep
am
Nowithd
rawal
symptoms
(b)Bromazep
am3mg
Stom
achco
mplaint:
valerian
(n¼
1),
bromazep
am(n¼
1)Fu
ssel
etal.4
1(200
0)Ye
sOne
-group
,pre-
post-test
Valerian
–ho
ps50
0mg/
120mg
14nigh
tsPSG
Valerian
–ho
psve
rsus
baseline:
NoAEoc
curred
kSL,k
wak
e,m
SEMorin
etal.4
0(200
5)Ye
sPDB,RCT
(a)Va
lerian
–ho
ps37
4mg/
82mg
28nigh
tsSlee
pdiaries,
slee
pque
stionn
aire
(ISI);
PSG
(n¼
75)
Valerian
hopsve
rsus
diphe
nhyd
ramineor
place
bo:
nosign
ifica
ntdifferenc
e
Noresidua
leffects,
seriou
sAEs,or
rebou
ndinsomnia
(b)Diphe
nhyd
ramine50
mg
(c)Place
bo
Nosign
ifica
ntgrou
pdifferenc
ein
AEs
Valerian
andlemon
balm
Lind
ahlan
dLind
wall43(198
9)Ye
sDB,RCT,
C/O
(a)Va
lerian
–ho
ps–lemon
balm
400mg/
375mg/
160mg
1nigh
tSlee
pqua
lity
(4-
point
scale)
Valerian
400mgve
rsus
4mg:
NoAEoc
curred
(b)Va
lerian
–ho
ps–lemon
balm
4mg/
375mg/
160mg
Greater
proportion
reportedm
SQDressinget
al.2
3(199
2)No
PDB,RCT,
C/O
(a)Va
lerian
–lemon
balm
160mg/
80mg
1nigh
tPSG
Nosign
ifica
ntdifferenc
efrom
place
bo
Norebou
ndeffects
occu
rred
(b)Triazolam
0.12
5mg
(c)Place
bo
Valerian as a sleep aid 221

ARTICLE IN PRESS
Table
3(con
tinu
ed)
Stud
y,ye
arSample
with
slee
pdisturban
ce
Stud
ydesign
Interven
tion
Trea
tmen
tduration
Outco
me
mea
sures
Mainslee
pou
tcom
esAdve
rseeffects
Dressinget
al.1
6(199
6)Ye
sPDB,RCT
(a)Va
lerian
–lemon
balm
320mg/
160mg2x
/d14
nigh
tsVIS-M
,SF-B
Valerian
–lemon
balm
versus
place
bo:
kSL,
mSQ
Noha
ngov
er,rebou
nd,
orwithd
rawals.
AE:
Valerian
/lem
onbalm
(n¼
5),place
bo(n¼
1)(b)place
bo
Cerny
andSchm
id42(199
9)No
PDB,RCT
(a)Va
lerian
–lemon
balm
360mg/
240mg
30nigh
tsSlee
pqua
lity
VAS,
SQim
prove
men
trating
s
Valerian
versus
place
bo:
Noseriou
sAE,
nosign
ifica
ntgrou
pdifferenc
ein
AEs
(b)Place
bo
VAS:
Nosign
ifica
ntdifferenc
e.Agrea
terproportion
reportedSQ
improve
men
t
Stud
yde
sign
abbrev
iation
s:C/O
,crossove
r,DB,dou
ble-blind(noplace
boco
ndition);PDB,place
bo-co
ntrolled
dou
bleblind
;RCT,
rand
omized
clinical
trial.Outcomemea
sures:
AE,
adve
rseev
ent;
NR,no
treported;
PSG
,polysom
nograp
hy;SF-A,Gortelm
eyer
Schlaffrag
ebog
enA,assesses
slee
pqua
lity
forthepastnigh
t;SF-B,Gortelm
eyer
Schlaffrag
ebog
enB,
assesses
slee
pqua
lity
forthetw
owee
ks;SL,slee
platenc
y;SQ
,slee
pqua
lity;SR
,self-rep
ort;
VAS,
visual
analog
scale;
VIS
–M,Visua
lana
logska
la–Morge
n(a
stan
dardized
setof
visual
analog
scales
ofslee
pco
mpletedin
themorning
).
D.M. Taibi et al.222

ARTICLE IN PRESS
Valerian as a sleep aid 223
(500mg valerian/120mg hops) compared to base-line measurements.
Two other studies investigated the valerian–hopscombination Hovas (information on extractionmethod not available).15,46 In the previously de-scribed randomized crossover trial by Leathwoodand Chauffard,46 three random nights of Hovas
(400mg, proportions of valerian/hops not re-ported) did not improve sleep in comparison to aplacebo in healthy persons. In a double-blind RCTofpersons with insomnia, sleep quality ratings im-proved significantly with both Hovas (200mgvalerian/45mg hops) and the benzodiazepine bro-mazepam (3mg).15 The two treatments did notsignificantly differ, although only small improve-ment was seen with either treatment. Finally,in a double-blind controlled clinical trial, Muller-Limmroth and colleagues22 investigated whether ornot a valerian–hops combination (240mg valerian/400mg hops, Seda-Kneipps) would attenuate sleepdisturbances experimentally induced by trafficnoise. No significant differences were found be-tween valerian–hops and placebo on the PSGoutcomes.
Valerian–lemon balm (also called lemon melissa)combinations were investigated in four clinicaltrials; two tested the herbal combination in healthypersons and two recruited persons with sleepdisturbance (see Table 3). In a double-blind RCTof healthy persons, 30 nights of a valerian–lemonbalm combination (360mg valerian, 70% ethanolextraction/240mg lemon balm, 30% methanolextraction, Songha Nights) had no effect on sleepquality ratings on a 0–100 visual analog scale (VAS)compared to a placebo.42 However, a significantlygreater proportion of those on valerian–lemon balmthan those on placebo (33% versus 9%) reportedthat their sleep quality was ‘‘better’’ (versus‘‘unchanged’’ or ‘‘worse’’) even though the VASratings did not reflect this change. Another double-blind study of healthy persons investigated theeffects of one night of the valerian–lemon balmcombination (160mg valerian, 70% ethanol extrac-tion/80mg lemon balm, 30% ethanol extraction;Euvegals).23 In this double-blind crossover study ofhealthy individuals the herbal combination did notimprove PSG-measured sleep efficiency, sleeplatency, or WASO compared to a placebo. Thesame research group conducted a 14-day trial ofEuvegals (320mg valerian, 70% ethanol extrac-tion/160mg lemon balm, 30% ethanol extraction)given twice a day in persons with insomnia. Theherbal combination significantly improved subjec-tive sleep quality ratings and reduced subjectivesleep latency compared to the placebo.16 Finally, ina placebo-controlled, double-blind crossover study
of persons with sleep disturbance, a significantlygreater proportion of participants reported thattheir sleep quality was ‘‘perfect’’ after one night ofa valerian–hops–lemon balm combination (400mgvalerian/375mg hops/160mg lemon balm, infor-mation on extraction method not available; Valeri-ana natts) than a night of hops–lemon balmalone.43
In summary, in subjects with insomnia, placebo-controlled studies of valerian–hops combinationsdid not improve PSG or subjective sleep out-comes,24,40 but a valerian–lemon balm combinationreduced subjective sleep latency and increasedsubjective sleep quality.16 A one-group trialof valerian–hops reported improved sleep com-pared to baseline,41 and another trial ofvalerian–hops reported improvement of sleepquality ratings that was similar to improvementwith a benzodiazepine.15 Neither of the twostudies of valerian–lemon balm in healthy indivi-duals showed significantly improved sleep.16,42
Overall, these findings are similar to results ofstudies of valerian alone. These mixed, butpredominantly negative, findings concerning theeffects of valerian combinations on sleep outcomesindicate that combination products are no moreeffective than valerian alone; that is to say noteffective at all.
Side effects and safety
No serious adverse effects occurred in thesereported clinical trials of valerian (see Tables 2and 3). The number of side effects with ethanolicvalerian extracts did not differ significantly fromplacebo,31,34 and tended to be fewer than benzo-diazepines.13,32 Specific side effects reported withethanolic valerian extracts included headache,gastrointestinal (GI) complaints, morning ‘‘hang-over,’’ diarrhea, drowsiness, exaggerated feeling ofwell-being, mental dullness, difficulty sleeping,depression, irritability, dizziness, feeling remote,nausea, and sweating.17,29,30,32,33 Studies of aqu-eous extracts reported two cases of dizzinesswith valerian21 and one case of nausea possiblyrelated to valerian.46 Additionally, Leathwood andChauffard38 reported evidence of dose-dependenthangover effects, with morning sleepiness ratingssignificantly higher after valerian than placebo forthe 900mg dose but not the 450mg dose. In theclinical trials of valepotriate preparations only fiveparticipants reported adverse effects, and in allcases these were GI (diarrhea, stomach discomfort,bitter taste in mouth).

ARTICLE IN PRESS
D.M. Taibi et al.224
Eight open-label clinical studies with samplesizes ranging from 20 to 830 participants investi-gated the tolerability of valerian or valeriancombination products. In several studies, no ad-verse events occurred,19,20,44 and in another studyonly three minor events occurred.14 When asked torate the tolerability of the herbal products,participants (70–90%) rated them as ‘‘good’’ or‘‘very good’’.12,14,18,20,28
Discussion
Evaluation of the effectiveness of valerian as asleep aid is difficult given the considerable varia-tion among the studies in duration, design, andherbal preparation. Originally, we had intended toperform a meta-analysis of the literature availableon valerian, but concluded that such an analysiswas not appropriate given the variability in theresearch quality. In particular, evidence on valerianfrom both parallel-group and crossover trials shouldnot be combined in the same meta-analysis becauseinclusion of crossover trials does not account forlack of independence of the group data andincreases the risk of Type I error. Other featuresof valerian trials that preclude use of meta-analyticprocedures are use of different types of products(species, extraction methods, and herbal combina-tions) and differing characteristics of the samplesstudied (healthy versus insomnia). There is insuffi-cient data on specific sleep outcomes to conductseparate meta-analyses on the literature dividedinto categories based on product and sample.Therefore, to fully evaluate the current state ofthe evidence of valerian effects on sleep outcomes,we decided that a descriptive synthesis of theliterature with specific attention to product andsample characteristics was most appropriate.
Issues related to dose and treatment durationwere not emphasized in this review because thereare no current standards for an optimal dose orrecommended treatment duration. Given the lackof dose-response studies, it is unclear whether anyof the studies used an optimal dose, although mostwere consistent with expert recommendations.Additionally, it is commonly recommended thatat least two weeks of valerian treatment isnecessary for effects to manifest,8 but thisrecommendation has not been specifically investi-gated. Although a few placebo-controlled studiesof two weeks or longer treatment durationreported significant improvement with valer-ian,16,21,35 a greater number found no significantimprovement.17,24,29,33,34,40,42
Quality of the research evidence
The quality of the studies reviewed was ratedusing the Jadad scoring criteria for potentialsources of bias (higher scores ¼ higher quality)10
(see Table 4). The studies of ethanolic extractswere conducted most recently and were of thehighest quality; most studies had Jadad scoresranging from 3 to 5.13,17,29–32,34 Studies of aqueousextracts and valepotriate-containing extracts weremostly conducted in the 1970s and 1980s, andtended to be of mixed quality; few studies had aJadad score X3.21,36,38,46 The studies of highestquality did not find valerian (ethanolic extracts orvalerian–hops combination) to be significantlysuperior to placebo for improving outcomes ininsomnia.17,29,31,40
In a previous systematic review,4 the authorsevaluated several criteria (e.g., randomization andblinding, power estimates, potential sources ofbias) in addition to the Jadad score that wereimportant to the validity of clinical trials of theeffects of herbs on sleep. None of the studiesreviewed addressed all of the important trial designelements, although the number of elements in-cluded did increase in the more recent studiesexamined. Few of the studies described therandomization procedures or reported data ongroup equivalence, which could bias the findingsif the groups differed on baseline characteristics.Perhaps more problematic was the failure tocalculate sample size, and thus, many studieswere likely underpowered to detect group differ-ences. The majority of studies had samplesizes between 11 and 21 participants, with onlysix studies having moderately large sample sizes(78–391).17,27,29,32,34,46 Nevertheless, the studiesgenerally used statistical methods that were liberalin assigning statistical significance to findings (e.g.,paired tests with no alpha rate correction formultiple testing), which makes the lack of statis-tical significance more compelling evidence againstthe clear effectiveness of valerian as a sleep aid.On the other hand, failure to control pre-bedtimevariables such as caffeine use or exercise may haveallowed these factors to influence sleep outcomes,confounding any potential effects of valerian onsleep.
Of particular methodological concern in thestudies reviewed was the considerable failure toensure that the placebo (or comparison medica-tion) and valerian were adequately masked. Valer-ian has a very distinctive, unpleasant odor. Failureto adequately mask the valerian treatment or‘odorize’ the comparison treatment may increaseexpectations that valerian pills will be effective.

ARTICLE IN PRESS
Valerian as a sleep aid 225
Of the 28 studies that were trials with a comparisongroup, 10 matched treatments on appearance,while seven matched on odor (two described thematching procedures).29,31 Only one study reportedthe success of the employed masking procedure29
(see Table 4). In two recently completed studies bythe authors of this review (C.A. Landis and D.M.Taibi, unpublished), researchers used valerian toconfer the odor of valerian on the placebocapsules. In one study, valerian capsules werestored in proximity to the placebo pills. In theother study, the placebo was stored in plasticcontainers that had been ‘‘odorized’’ by containingactive valerian for a week. Although it is possiblethat these methods may contaminate the placebo,the amount of valerian transferred is likely to beminimal and not clinically effective. In each ofthese studies, participants were not able toidentify which treatment condition they hadreceived, indicating that both masking procedureswere successful.
The specificity of the sample characteristics,including subject inclusion and exclusion criteriawere evaluated (Table 1). Little consideration wasgiven to age and gender, although few studiesspecifically investigated valerian in older adults. Itwas evident that many of the studies did not reportexclusion of potentially confounding variables,including co-morbid insomnia, psychiatric diag-noses, and concurrent use of sleep-altering medi-cations. In particular, a serious omission was thefailure to report exclusion of other sleep disorders(e.g., sleep apnea and restless legs syndrome),even in several of the high-quality studies. Thefindings from studies of ethanolic extracts andvalerian–lemon balm combinations are the mostreliable in relation to controlling for potentialconfounding variables. Finally, none of the studiesof insomnia patients differentiated between typesof insomnia symptoms in the analysis. It is possiblethat valerian products may have differential effi-cacy for sleep initiating versus sleep maintenancesymptoms.
Evaluation of the effects of valerian on sleep
Only a limited number of studies were available oneach type of valerian product. Although some ofthese studies reported improvement over time,often no direct comparisons of valerian and placebogroups were reported.27,37,34 Given that severalstudies of valerian reported improvement of sleepunder the placebo condition (e.g.,17,29,33), im-provement over time in the valerian group is
insufficient to exclude the possibility of placeboeffects or to conclude that the herb is effective.
Valerian effects on subjective sleepoutcomes
The research findings to date do not support theefficacy of valerian or valerian combinations forimproving subjective sleep outcomes. Most of theevidence of improved sleep with valerian prepara-tions is from studies using non-specific outcomesfor clinical trials (i.e. proportion improve-ment)21,38,42,43 or studies in which placebo effectwas not addressed.13,29,32,41 Research evidence ofhigh-quality is available for ethanolic V. officinalisextracts, and the findings do not support theefficacy for the treatment of insomnia. The qualityof research evidence for other valerian products ismixed, but few studies have been conducted withthese products in samples with insomnia. Althoughthere is some evidence that suggests valerian mayimprove sleep outcomes, placebo effects cannot beruled out in many of these trials. Therefore, theevidence is insufficient to recommend clinical useof valerian for treating disturbed sleep.
Recently, Bent and colleagues5 published a meta-analysis of subjective sleep quality and sleeplatency outcomes of valerian treatment, conclud-ing that evidence suggests potential beneficialeffects of valerian on sleep. In this analysis, theauthors did not consider type of valerian product,and they included combination products with asmany as eight other herbs. Two types of sleepquality outcomes have been used in valerianstudies: (1) sleep quality improvement—whetherparticipants rate their sleep as ‘‘improved’’ or ‘‘notimproved’’ or (2) sleep quality ratings—e.g., 0–10numeric scale, 0 ¼ poor, 10 ¼ excellent. Bent andcolleagues conducted their meta-analysis on sleepquality improvement ratings (‘‘improved versus‘‘not improved’’). This analysis favored valerian,but inspection of the studies included revealed apublication bias towards small, positive studies.Additionally, in two of the six studies in which sleepquality improvement favored valerian, sleep qual-ity ratings showed no significant differences be-tween valerian and placebo.17,42 Therefore, theclinical utility of assessing subjective sleep qualityimprovement is questionable. Bent et al. reportedthat results for subjective sleep latency weremixed, and, as discussed in our review, variationin study quality and lack of control for confoundingvariables influenced the outcomes of many of thestudies. Given the limited scope of outcomes andstudies considered in the Bent et al. review, the

ARTICLE IN PRESS
Table
4Qua
lity,metho
dolog
ical
features,an
dsign
ifica
nceof
primaryou
tcom
esof
clinical
trials
ofva
lerian
forslee
p.
Stud
yJadad
Score
Ran
dom
proce
dure
described
Blind
ingof
appea
ranc
edescribed
Blind
ingof
odor
described
Successof
blind
ing
chec
ked
Com
plian
cech
ecke
dSample
size
calculated
Subject
inclusion/
exclusion
criteria
Dropou
tsreported
Con
trol
ofpre-
bed
time
variab
les
Validated
outcom
emea
sures
Intent-to-
trea
tan
alyses
Prim
ary
slee
pou
tcom
essign
ifica
nt
Muller-Limmroth
and
Ehrentstein22
1(+)
Jansen
27
3+
NA*
Leathw
oodan
dCha
uffard,3
9
Leathw
oodet
al.4
6
(lab
)
0(+)
Leathw
oodan
dCha
uffard,3
9
Leathw
oodet
al.4
6
(hom
e)
4+
++
+p
Gessner
etal.2
62
++
(+)
Gessner
and
Klasser
25
2(+)
(+)
Kam
m-Koh
let
al.2
13
++p
Balderer
and
Borbely1
1(hom
e)1
++
(+)
Balderer
and
Borbely1
1(PSG
)2
++
+
Leathw
oodan
dCha
uffard
38
4+
++
+(+)
Lind
ahlan
dLind
wall43
2+
(+)
+p
Dressinget
al.1
62
++
Schu
lzet
al.3
72
++
NA*
Dressinget
al.6
3+
++
++
+Vo
rbac
het
al.1
75
++
(+)
++
++
++
Roden
bec
ket
al.2
42
++
Schm
itzan
dJackel
15
3+
++
+¼
Cerny
andSchm
id42
3+
++
Kuhlman
net
al.3
43
++
++
Don
athet
al.3
32
+(+)
Dorn1
35
++
(+)
++
++¼
Herrera-Arellan
oet
al.3
64
+(+)
++
(+)
Poya
reset
al.3
52
++
+(+)
Zieg
leret
al.3
24
+(+)
++
++
++¼
Cox
eter
etal.3
75
++
++
NA
++
NA
Diaper
and
Hindmarch
30
3+
(+)
++
Jaco
bset
al.2
95
++
++
++
++
++
Morin
etal.4
04
+(+)
++
++
++
+
Item
srelatedto
quality:
Stud
ieslisted
chrono
logica
lly.
+:item
was
adeq
uately
addressed
;(+):
item
was
partially
addressed
;NA:item
was
notap
plica
ble
tothestud
y.Prim
ary
outcom
es(based
onou
tcom
esrepo
rted
inTables
1an
d2):+:
outcom
essign
ifica
nt(versusplace
bo);(+):
only
partof
mainou
tcom
esweresign
ifica
nt;NA*:
statistica
lan
alyses
comparingva
lerian
totheplace
bowereeither
notdon
eor
notreported;
+p:astatistica
llysign
ifica
ntpropo
rtionof
thesample
improve
d,but
thestud
ydid
notco
mparemea
nscores;
+¼:eq
uiva
lenc
eof
valerian
andaben
zodiaze
pine(hyp
othe
siswas
met
ifdifferenc
eswereno
n-sign
ifica
nt).
D.M. Taibi et al.226

ARTICLE IN PRESS
Valerian as a sleep aid 227
preponderance of negative findings was neglected,and the author’s conclusions that valerian, as it hasbeen tested to date, is a promising therapy areunsupported in the broader context of the litera-ture reviewed here.
Valerian effects on objective sleep outcomes
Current evidence suggests that the investigatedvalerian preparations do not significantly affectobjective sleep outcomes, although very fewstudies have actually recorded sleep. Of the studiesadministering V. officinalis mono-preparations,only two of the studies that measured PSG out-comes investigated valerian administration forlonger than three days in persons with sleepdisturbance,33,35 one showed no significant out-comes,33 and the other reported reduced WASO.35
Studies of valerian combinations reporting PSGoutcomes after either one night22,23 or 28 days24,40
found no outcomes significant compared toplacebo. One study of an aqueous valerian extractshowed reduced sleep onset latency by wristactigraphy in persons with sleep onset insomnia.38
However, sleep latency was not longer than 30minat baseline (15min) and on average was reducedonly four to six minutes, providing only weakevidence of valerian sedation. Overall, thesefindings do not support the effectiveness of valerianor valerian combinations for improving objectivesleep outcomes. Additionally, when consideringthat the tested valerian preparations did notclearly show improved subjective sleep ratings,any evidence of improved objective sleep outcomesis of questionable relevance.
Safety of valerian
The studies reviewed support the safety of valer-ian. The most common side effects were mild andtended to be either mild neurological symptoms(dizziness, headache, drowsiness) or gastrointest-inal (GI) symptoms (nausea, diarrhea). Althoughvalerian has been implicated in a few case reportsof transient liver dysfunction,47,48 no hepaticsymptoms or changes in liver function werereported in the research literature reviewed.13,42
Valerian had been shown to cause little to noimpairment of performance, especially in compar-ison to benzodiazepines.30,34,49–51
Concerns have been raised regarding the safetyof ingesting valepotriates. These constituents havebeen shown in vitro to be cytotoxic and to inhibitDNA synthesis.8 A recent in vitro study demon-strated that DNA damage of human epithelial cells
occurred with high doses of valepotriates, but notwith low doses.52 It has been suggested that the GItract is at particularly high risk for adverse effectsof valepotriates because of the chemical degrada-tion of these substances in the stomach.8 While GIsymptoms were reported in the reviewed studies onhigh-valepotriate preparations, these symptomslikely were related to purported muscle-relaxanteffects of valepotriates.8 No report was found inthe literature directly linking valepotriates to theoccurrence of serious adverse events in humans,but caution in the use of these products iswarranted until more is known about potentialadverse effects.
There is little evidence on potential herb–druginteractions of valerian. In vitro studies havedemonstrated mild to moderate inhibition of thedrug-metabolizing enzymes in the small bowel andliver that are involved in first-pass drug metabo-lism.53,54 Although inhibition of these enzymestheoretically increases the risk of excessive levelsof certain medications in the blood, an in vivo studyof humans showed no significant effects of onevalerian preparation on circulating levels of med-ications given to test enzyme inhibition.55 Althoughevidence indicates that valerian is unlikely tosignificantly affect drug metabolism, caution maybe advised with medications that are metabolizedby cytochrome P450 enzyme subtype 3A4, and toa lesser extent subtypes 2C19 and 2D6, if themedications have high toxicity and a narrowtherapeutic range (e.g., digoxin). Additionally,synergistic effects of valerian with medicationsare potentially problematic. In animal studies,valerian had been shown to potentiate barbiturateinduced sleeping time.6 Valerian should not betaken with benzodiazepines and other sedatingsubstances, such as antihistamines and alcohol, dueto the risk of over-sedation.
Conclusion
Although valerian is commonly used in the UnitedStates and Europe as a sleep aid, current evidenceon the efficacy of valerian for improving sleepoutcomes does not support such use. However,valerian is an apparently safe herb, with fewreported side effects. Despite the lack of evidencefor efficacy, these products are unlikely to causeharm other than perhaps delaying individuals fromseeking the effective treatment for insomniasymptoms.
Although current evidence fails to supportefficacy of valerian for relief of insomnia, the

ARTICLE IN PRESS
D.M. Taibi et al.228
widely variable and methodologically mixed natureof the extant literature clearly leaves room forfurther clarification. First, it is important to notethat the source valerian plant material used in moststudies was extracted from dried, rather thanfresh, root and rhizome. The concentration ofcertain constituents of valerian varies betweenfresh and dried products, and study findings ondried root extracts should not be generalized tofresh root preparations. Second, valerian prepara-tions were administered in pill form rather than asa liquid, which is the preferred method recom-mended by herbalists (personal communicationRobin DePasquale, January, 2007). No studies werefound that tested valerian tinctures for sleep;although one tested cognitive impairment with asyrup.50 This is an important distinction becausethe presence and availability of active constituentsvaries between pills and tinctures. Finally, rigorousstudies testing different doses of valerian and typesof valerian products in well-defined samples ofpersons with insomnia are needed. It remainspossible that valerian may be a useful, mildtreatment for sleep disturbance, but currentevidence does not support its use, and research isneeded to determine which products and doses ofvalerian might be efficacious.
Practice points
� Current evidence does not support theefficacy of valerian or valerian combina-tions with other herbs for reducing generalsleep disturbance or insomnia symptoms.� Valerian has been shown to be a safe
product and is unlikely to cause harm inthe majority of patients. Healthcare provi-ders should advise patients of potentialherb–drug interactions (e.g., additive seda-tion, possible alteration of drug metabo-lism).� Caution should be exercised in the use of
valerian by patients who have a history ofliver disease, those at risk for liver dysfunc-tion, and taking other herbs linked to liverdysfunction.
�The most important references are denoted by an asterisk.
Research agenda
� Future studies of valerian should specificallyexclude persons with primary sleep distur-bances other than insomnia (e.g., restlesslegs syndrome, sleep apnea).
� Future studies should use greater specifica-tion of inclusion/exclusion criteria, espe-cially in defining the type of sleepdisturbance in the sample. Study methodsshould also plan for greater control ofpotential sources of bias (see Table 4).� Matching of valerian and placebo odor is
critical to ensure adequate masking and toreduce potential placebo effects.� Evidence on valerian preparations in tinc-
ture form is lacking. Given that this is aformulation preferred by herbalists, re-search on such preparations may providenew information on potential effects ofvalerian.
Acknowledgments
The systematic review and manuscript weresupported by the National Institutes of Health,grant numbers R21-AT-002108, P30-NR04001, andT32-NR07039. The authors thank Robin DiPasquale,N.D., R.H.(AHG) for consulting on this article andCristina Fuller, Ph.D.(c), for assistance with Portu-guese translation.
References
1. Ohayon MM. Epidemiology of insomnia: what we know andwhat we still need to learn. Sleep Med Rev 2002;6(2):97–111.
2. Pearson NJ, Johnson LL, Nahin RL. Insomnia, troublesleeping, and complementary and alternative medicine:Analysis of the 2002 national health interview survey data.Arch Intern Med 2006;166(16):1775–82.
3. Blumenthal M, Ferrier GK, Cavaliere C. Total sales of herbalsupplements in United States show steady growth. Herbal-Gram 2006;71:64–6.
�4. Stevinson C, Ernst E. Valerian for insomnia: a systematicreview of randomized clinical trials. Sleep Med 2000;1(2):91–9.
�5. Bent S, Padula A, Moore D, Patterson M, Mehling W.Valerian for sleep: a systematic review and meta-analysis.Am J Med 2006;119(12):1005–12.
6. Bos R, Woerdenbag HJ, DeSmet PAGM, Scheffer JJ.Valeriana species. In: DeSmet PAGM, Keller K, Hansel R,Chandler RF, editors. Adverse effects of herbal drugs.Berlin: Springer; 1997. p. 165–80.
7. Upton R, Graff A, Williamson E, Bevill A, Ertl F, Reich E,et al. Valerian root, Valeriana officinalis: analytical qualitycontrol, and therapeutic monograph. In: Upton R, editor.American herbal pharmacopoeia and therapeutic compen-dium. Santa Cruz, CA: American Herbal Pharmacopoeia;1999.

ARTICLE IN PRESS
Valerian as a sleep aid 229
�8. Houghton PJ. The scientific basis for the reputed activity ofvalerian. J Pharm Pharmacol 1999;51(5):505–12.
9. Blumenthal M. The complete German Commission EMonographs: therapeutic guide to herbal medicines.Boston, MA: American Botanical Council, IntegrativeMedicine Communications; 1998.
10. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ,Gavaghan DJ, et al. Assessing the quality of reports ofrandomized clinical trials: is blinding necessary? ControlClin Trials 1996;17(1):1–12.
11. Balderer G, Borbely AA. Effect of valerian on human sleep.Psychopharmacology 1985;87(4):406–9.
12. Staiger C, Wegener T. Pflanzliche Dreierkombination beiSchlafstorungen und Unruhezustanden: eine Anwendungs-beobachtung. Z Phytother 2006;27(1):12–5.
13. Dorn M. Wirksameit und Vetraglichkeit von Baldrian versusOxazepam bei nichtorganischen und nichtpsychiatrichenInsomnien: eine randomisierte doppelblinde, klinischeVergleichsstudie. Forsch Komplementarmed Klass Natur-heilkd 2000;7(2):79–84.
14. Volk S, Friede M, Hasenfuss I, Wustenberg P. Phytosedati-vum gegen nervose Unruhezustande und Einschlafstorun-gen: Wirksamkeit und Vetraglichkeit eines pflanzlichenKombinations-praparates aus Baldrianwurzeln, Hopfenzap-fen und Melissenblattern. Z Phytother 1999;20(6):337–44.
15. Schmitz M, Jackel M. Vergleichsstudie zur Untersuchungder Lebensqualitat von Patienten mit exogenen Schlafstor-ungen (vorubergehenden Ein- und Durchschlafstorungen)unter Therapie mit einem Hopfen-Baldrian-Praparat undeinem Benzodiazepin-Praparat. Wien Med Wochenschr1998;148(13):291–8.
16. Dressing H, Kohler S, Muller WE. Verbessering der Schlaf-qualitat mit einem hochdosierten Baldrian-Melisse-Praparat: eine plazebokontrollierte doppelblinde. Psycho-pharmakotherapie 1996;3(3):123–30.
�17. Vorbach EU, Gortelmeyer R, Bruning J. Therapie vonInsomnien: Wirksamkeit und Vetraglichkeit eines Baldrian-praparats. Psychopharmakotherapie 1996;3(3):109–15.
18. Orth-Wagner S, Ressin WJ, Friederich I. Phytosedativumgegen Schlafstorungen: Klinische Wirksamkeit und Vetra-glichkeit eines Phytosedativums mit Auszugen Baldrianwur-zel, Hopfenzapfen und Melissenblattern. Z Phytother1995;16(3):147–56.
19. Schmidt-Voight J. Die Behandlung nervoser Schlafstorungenund innerer unruhe mit einem rein pflanzlichen Sedativum.Therapiewoche 1986;36:663–7.
20. Strosser W, Gladbach B. Pflanzliche Sedativa: alternative inder Therapie leichter Schlafstorungen. Dtsch Apoth Ztg1999;139:50–2.
21. Kamm-Kohl AV, Jansen W, Brockmann P. Moderne Bal-driantherapie gegen nervose Storungen im Senium. MedWelt 1984;35:1450–4.
22. Muller-Limmroth W, Ehrenstein W. Untersuchungen uberdie Wirkung von Seda-Kneipps auf den Schlaf schlafges-torter Menschen: Bedeutung von Seda-Kneipps in derTherapie verschiedener Schlafstorungen. Med Klin 1977;72(25):1119–25.
23. Dressing H, Riemann D, Low H, Schredl M, Reh C, Laux P,et al. Baldrian-Melisse-Kombinationen versus Benzodiade-pin. Bei schlafstorungen gleichwertig? Therapiewoche1992;42(12):726–36.
24. Rodenbeck A, Simen S, Cohrs S, Jordan W, Kinkelbur J,Staedt J, et al. Veranderte Schafstadienstruktur alsHinweis auf die GABAerge Wirking eines Baldrian-Hopfen-Praparates bei Patienten mit psychophysiologischer Insom-nie. Somnologie 1998;2:26–31.
25. Gessner B, Klasser M. Untersuchung der Wirkung vonHarmonicum Muchs auf den Schlaf mit Hilfe polygra-phischer EEG-Aufzeichnungen. EEG EMG Z Elekt ElektVerwandte 1984;15(1):45–51.
26. Gessner B, Klasser M, Volp A. Untersuchung uberdie langzeitwirkung von Harmonicum Muchs auf denschlaf van schlafgestorten personen. Therapiewoche 1983;33(42):5547–58.
27. Jansen W. Double blind trial of a mixture of valerianextract with valepotriates. Therapiewoche 1977;27(14):2779–86.
28. Friede M, Liske E, Woelk H, Wustenberg P. PflanzlicheWirkstoffe gegen Schlafstorungen. Tw Neurologie Psychia-trie 1997;11(10):697–700.
�29. Jacobs BP, Bent S, Tice JA, Blackwell T, Cummings SR. Aninternet-based randomized, placebo-controlled trial ofkava and valerian for anxiety and insomnia. Medicine2005;84(4):197–207.
�30. Diaper A, Hindmarch I. A double-blind, placebo-controlledinvestigation of the effects of two doses of a valerianpreparation on the sleep, cognitive and psychomotorfunction of sleep-disturbed older adults. Phytother Res2004;18(10):831–6.
�31. Coxeter PD, Schluter PJ, Eastwood HL, Nikles CJ, GlasziouPP. Valerian does not appear to reduce symptoms forpatients with chronic insomnia in general practice using aseries of randomised n-of-1 trials. Complement Ther Med2003;11(4):215–22.
�32. Ziegler G, Ploch M, Miettinen-Baumann A, Collet W.Efficacy and tolerability of valerian extract LI 156compared with oxazepam in the treatment of non-organicinsomnia- a randomized, double-blind, comparative clin-ical study. Eur J Med Res 2002;7(11):480–6.
�33. Donath F, Quispe S, Diefenbach K, Maurer A, Fietze I, RootsI. Critical evaluation of the effect of valerian extract onsleep structure and sleep quality. Pharmacopsychiatry2000;33(2):47–53.
34. Kuhlmann J, Berger W, Podzuweit H, Schmidt U. Theinfluence of valerian treatment on ‘reaction time, alert-ness and concentration’ in volunteers. Pharmacopsychiatry1999;32(6):235–41.
35. Poyares DR, Guilleminault C, Ohayon MM, Tufik S. Canvalerian improve the sleep of insomniacs after benzodia-zepine withdrawal. Prog Neuropsychopharmacol Biol Psy-chiatry 2002;26(3):539–45.
36. Herrera-Arellano A, Luna-Villegas G, Cuevas-Uriostegui ML,Alvarez L, Vargas-Pineda G, Zamilpa-Alvarez A, et al.Polysomnographic evaluation of the hypnotic effect ofValeriana edulis standardized extract in patients sufferingfrom insomnia. Planta Med 2001;67(8):695–9.
37. Schulz H, Stolz C, Muller J. The effect of valerian extracton sleep polygraphy in poor sleepers: A pilot study.Pharmacopsychiatry 1994;27(4):147–51.
38. Leathwood PD, Chauffard F. Aqueous extract of valerianreduces latency to fall asleep in man. Planta Med1985;2:144–8.
39. Leathwood PD, Chauffard F. Quantifying the effects of mildsedatives. J Psychiatr Res 1982/83;17(2):115–22.
�40. Morin CM, Koetter U, Bastien C, Ware JC, WootenV. Valerian-hops combination and diphenhydramine fortreating insomnia: a randomized placebo-controlled clin-ical trial. Sleep 2005;28(11):1465–71.
41. Fussel A, Wolf A, Brattstrom A. Effect of a fixed valerian-hop extract combination (Ze 91019) on sleep polygraphy inpatients with non-organic insomnia: a pilot study. Eur JMed Res 2000;5(9):385–90.

ARTICLE IN PRESS
D.M. Taibi et al.230
42. Cerny A, Schmid K. Tolerability and efficacy of valerian/lemon balm in healthy volunteers (a double-blind, placebo-controlled, multicentre study). Fitoterapia 1999;70(3):221–8.
43. Lindahl O, Lindwall L. Double blind study of a valerianpreparation. Pharmacol Biochem Behav 1989;32(4):1065–6.
44. Dominguez RA, Bravo-Valverde RL, Kaplowitz BR, Cott JM.Valerian as a hypnotic for hispanic patients. Cultur DiversEthnic Minor Psychol 2000;6(1):84–92.
45. Notter D, Brattstrom A, Ullrich N. Therapie von Schlafstor-ungen. DAZ 2004;144(14):147–8.
46. Leathwood PD, Chauffard F, Heck E, Munoz-Box R. Aqueousextract of valerian root (Valeriana officinalis L.) improvessleep quality in man. Pharmacol Biocem Behav 1982;17(1):65–71.
47. MacGregor FB, Abernethy VE, Dahabra S, Cobden I, HayesPC. Hepatotoxicity of herbal remedies. BMJ 1989;299(6708):1156–7.
48. Shaw D, Leon C, Kolev S, Murray V. Traditional remediesand food supplements. A 5-year toxicological study(1991–1995). Drug Saf 1997;17(5):342–56.
49. Hallam KT, Olver JS, McGrath C, Norman TR. Comparativecognitive and psychomotor effects of single doses ofValeriana officianalis and triazolam in healthy volunteers.Hum Psychopharmacol 2003;18(8):619–25.
50. Gerhard U, Linnenbrink N, Georghiadou C, HobiV. Vigilanzmindernde Effekte zweier pflanzlicher Schlaf-mittel. Schweiz Rundsch Med Prax 1996;85(15):473–81.
51. Glass JR, Sproule BA, Herrmann N, Streiner D, Busto UE.Acute pharmacological effects of temazepam, diphenhy-dramine, and valerian in healthy elderly subjects. J ClinPsychopharmacol 2003;23(3):260–8.
52. Hui-lian W, Dong-fang Z, Zhao-feng L, Yang L, Qian-rong L,Yu-zhen W. In vitro study on the genotoxicity of dichlor-omethane extracts of valerian (DEV) in human endothelialECV304 cells and the effect of vitamins E and C inattenuating the DEV-induced DNA damages. Toxicol ApplPharmacol 2003;188(1):36–41.
53. Budzinski JW, Foster BC, Vandenhoek S, Arnason JT. An invitro evaluation of human cytochrome P450 3A4 inhibitionby selected commercial herbal extracts and tinctures.Phytomedicine 2000;7(4):273–82.
54. Strandell J, Neil A, Carlin G. An approach to the in vitroevaluation of potential for cytochrome P450 enzymeinhibition from herbals and other natural remedies.Phytomedicine 2004;11(2–3):98–104.
55. Gurley BJ, Gardner SF, Hubbard MA, Williams DK, GentryWB, Khan IA, et al. In vivo effects of goldenseal, kava kava,black cohosh, and valerian on human cytochrome P450 1A2,2D6, 2E1, and 3A4/5 phenotypes. Clin Pharmacol Ther2005;77(5):415–26.
Recommended