Financial Disclosures
•I am a share holder and medical director of Regenerative Sciences, LLC
•I am not being directly compensated for this presentation
Intradiscal Stem cells: Are they an Effective Treatment Technique?
Chris Centeno, M.D.
What autologous biologics can be used in discs?
• Blood Products– PRP
– Platelet lysates
– Cultured serum (IRAP)
– Cultured platelet supernatants
• Stem cells– Bone marrow aspirate concentrate
– Cultured stem cells
At one time or another, we’ve used all of these things in discs…
• Blood Products– PRP
– Platelet lysates
– Cultured serum (IRAP)
– Cultured platelet supernatants
• Stem cells– Bone marrow aspirate concentrate
– Cultured stem cells
How do we currently treat a disc bulge with surgery?
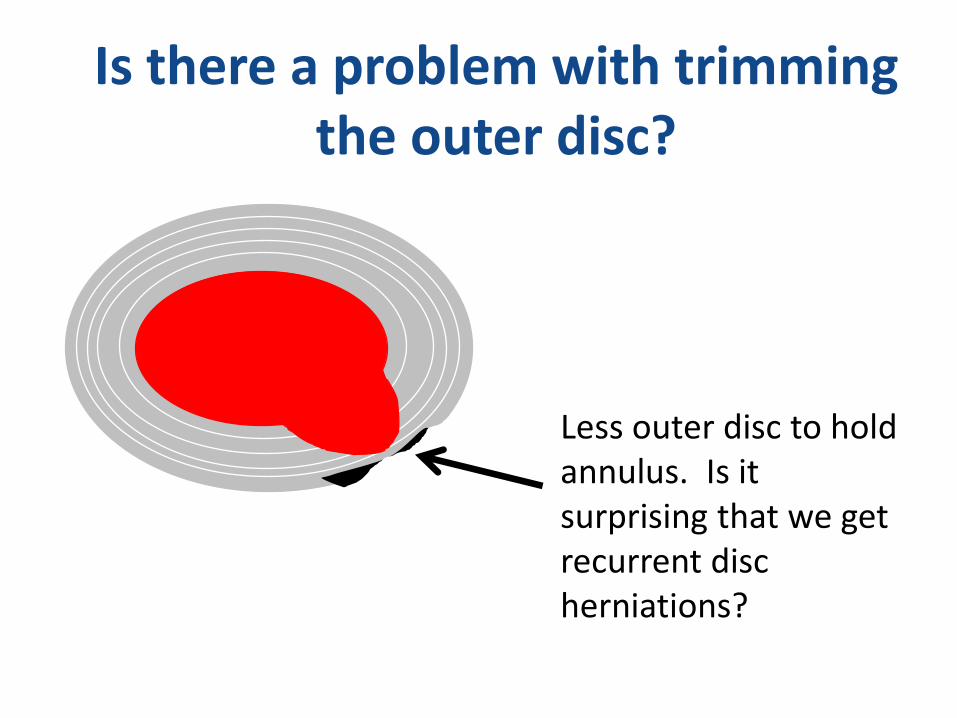
Is there a problem with trimming the outer disc?
Less outer disc to hold annulus. Is it surprising that we get recurrent disc herniations?
What if we could rebuild the torn fibers of the outer disc?
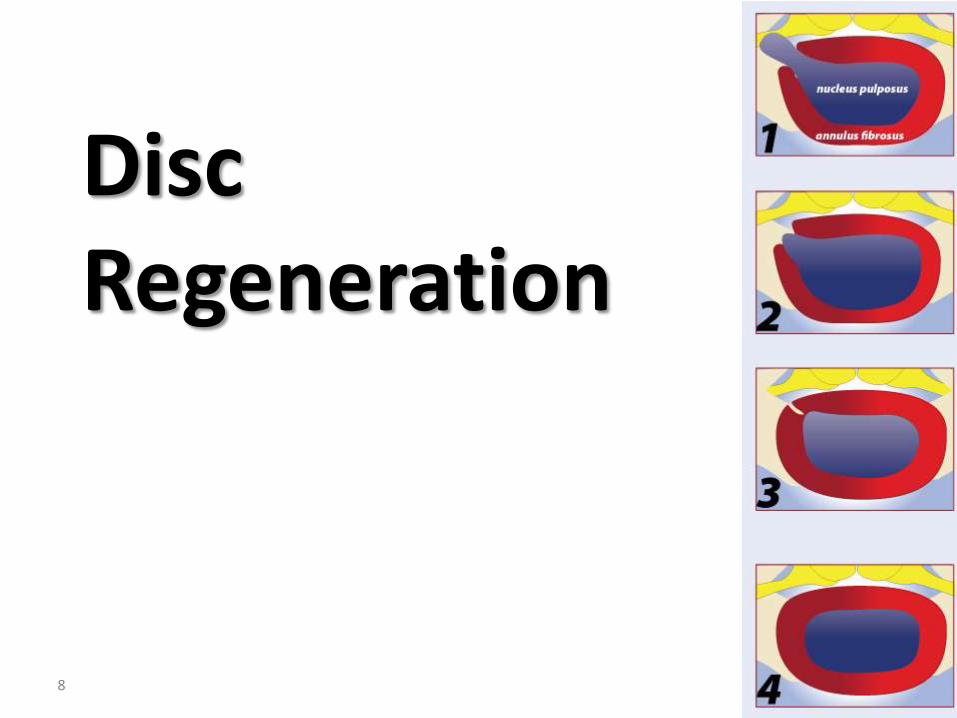
Disc Regeneration
8
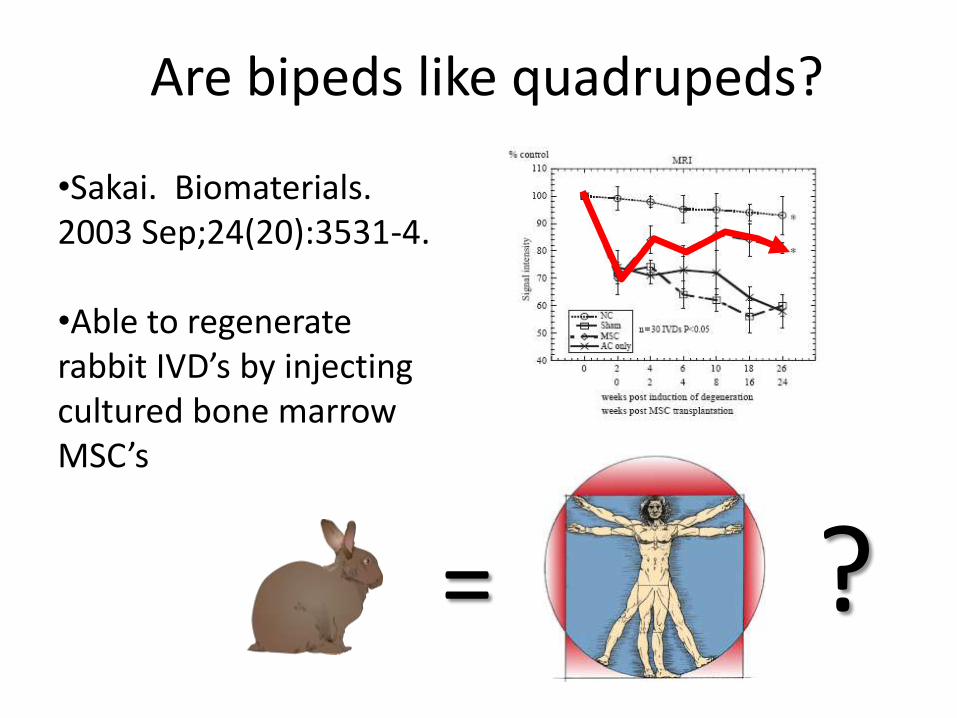
Are bipeds like quadrupeds?
•Sakai. Biomaterials. 2003 Sep;24(20):3531-4.
•Able to regenerate rabbit IVD’s by injecting cultured bone marrow MSC’s
= ?

Our research experience:(pre-post 3.0T MRI with pain functional
ratings)
10
•Injected concentrated bone marrow nucleated cells (BMAC) and PRP into NP-Didn’t work.
•The next step?•Isolate and then culture expand MSC’s.
So how do you isolate and grow mesenchymal stem cells ex-vivo?
Expand them by passaginginto new flasks. They should double every 2 days.
Our research experience:(pre-post 3.0T MRI with pain functional
ratings)
12
•Injected culture expanded MSC’s into NP-Didn’t work.
= ?
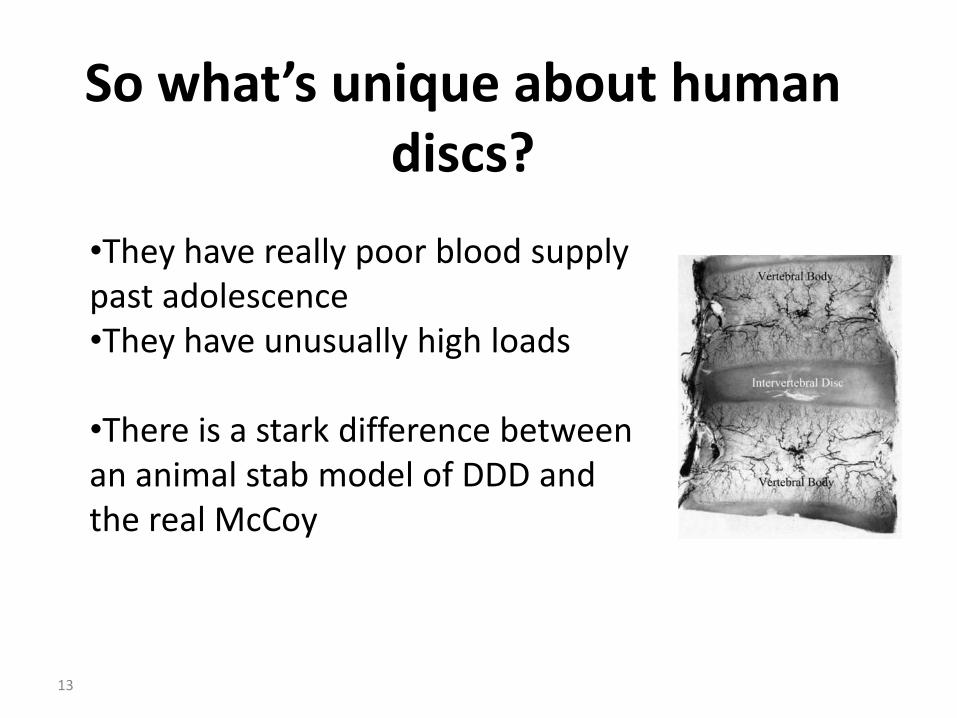
So what’s unique about human discs?
13
•They have really poor blood supply past adolescence•They have unusually high loads
•There is a stark difference between an animal stab model of DDD and the real McCoy
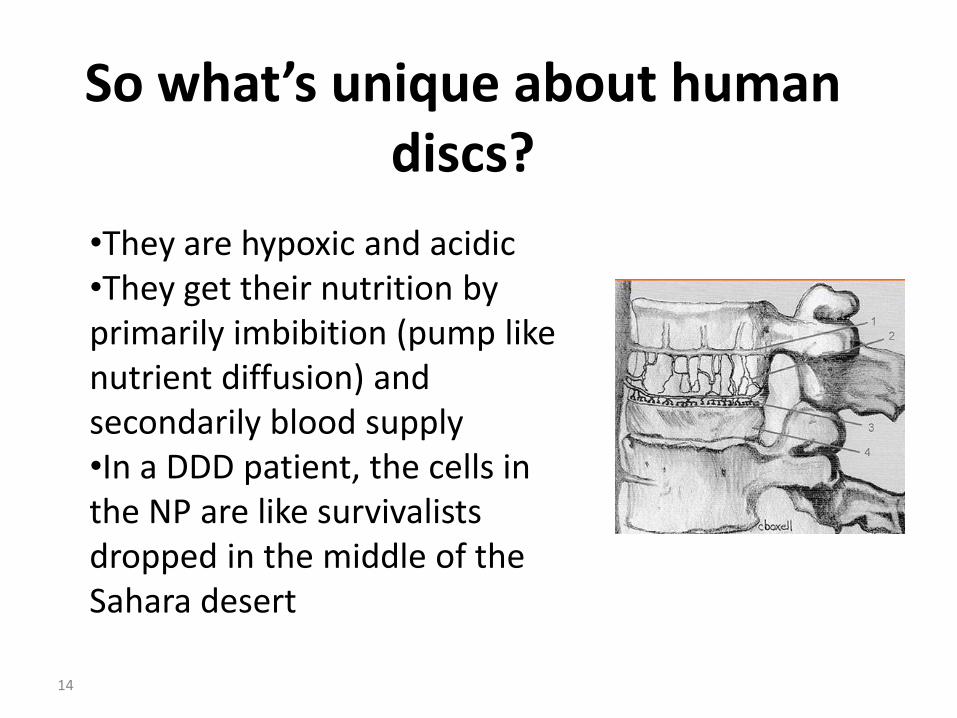
So what’s unique about human discs?
14
•They are hypoxic and acidic•They get their nutrition by primarily imbibition (pump like nutrient diffusion) and secondarily blood supply•In a DDD patient, the cells in the NP are like survivalists dropped in the middle of the Sahara desert
For the last decade, some European researchers have postulated that DDD
and radiculopathy are vascular problems…
15
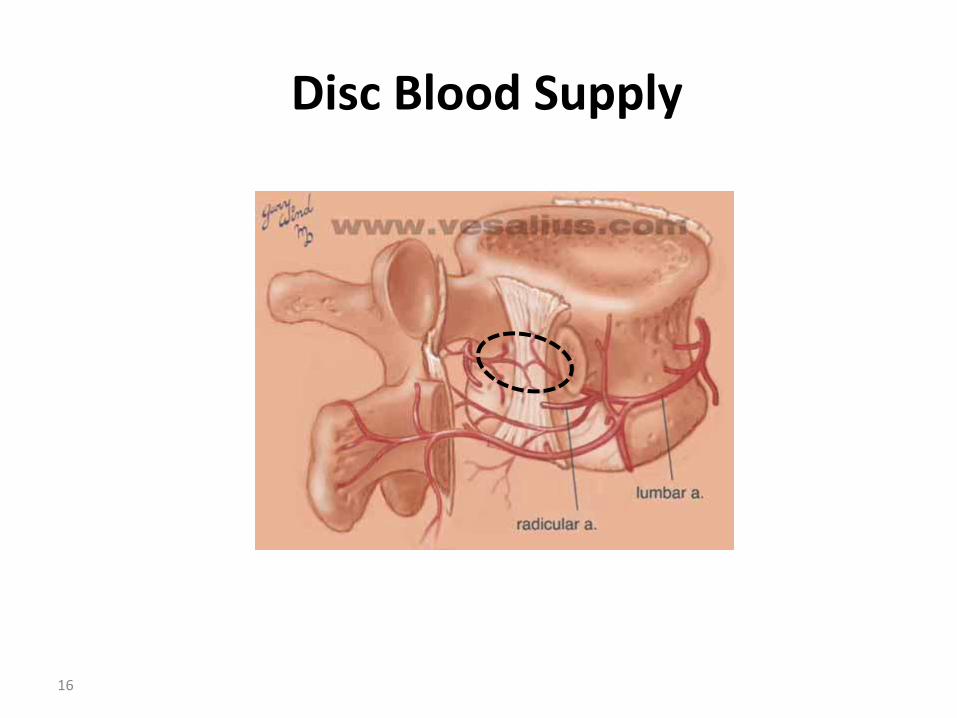
Disc Blood Supply
16
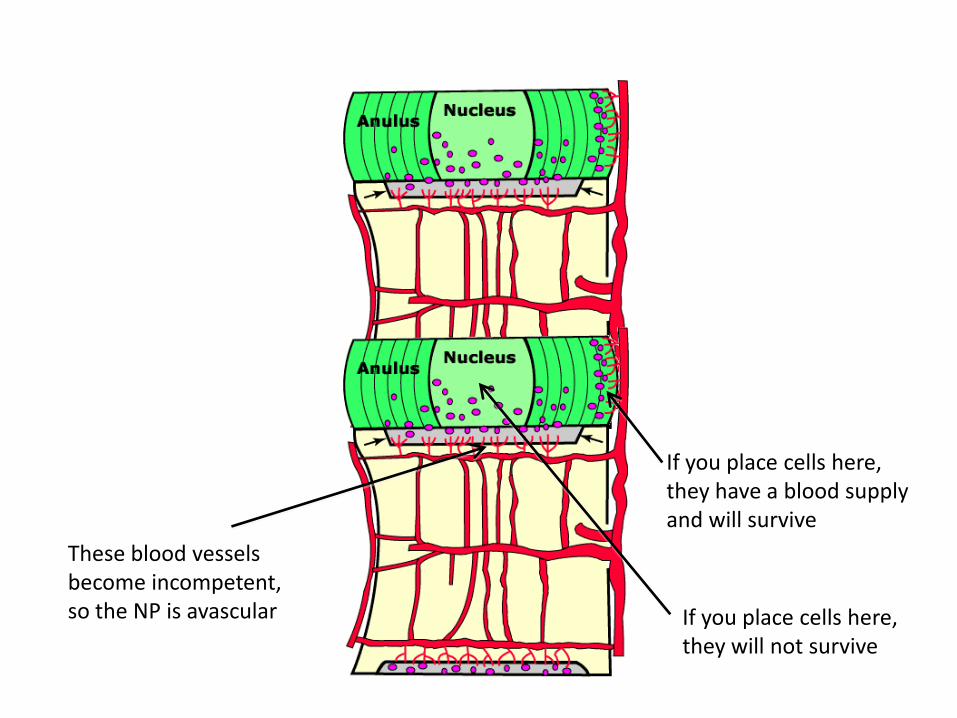
If you place cells here, they have a blood supply and will survive
If you place cells here,they will not survive
These blood vesselsbecome incompetent,so the NP is avascular
18
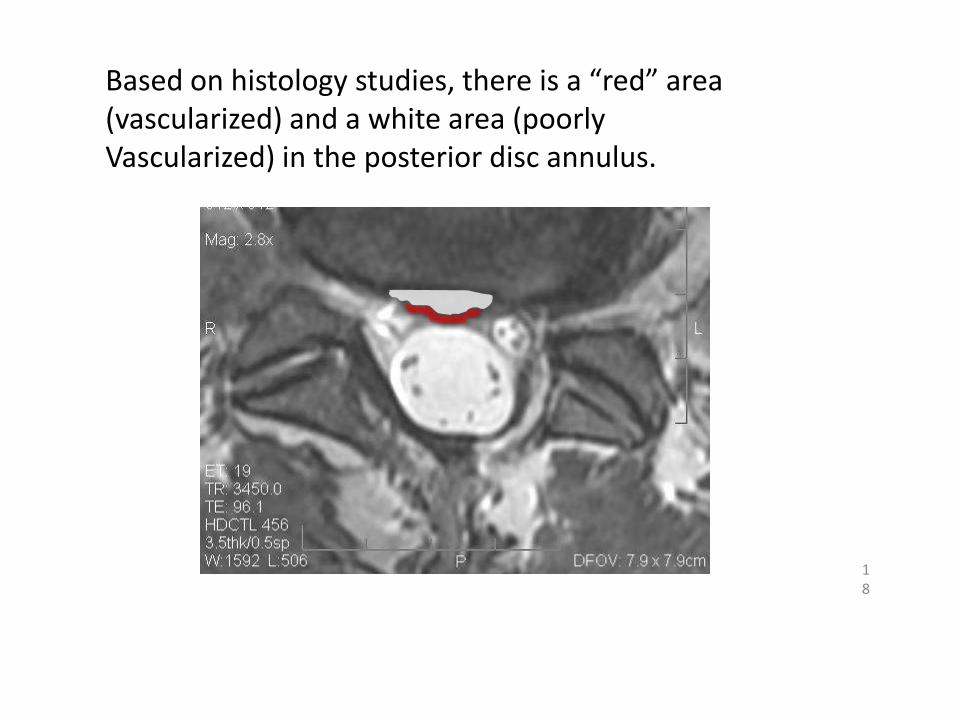
Based on histology studies, there is a “red” area (vascularized) and a white area (poorlyVascularized) in the posterior disc annulus.
The problem is how do you physically get cells to this area via a needle?
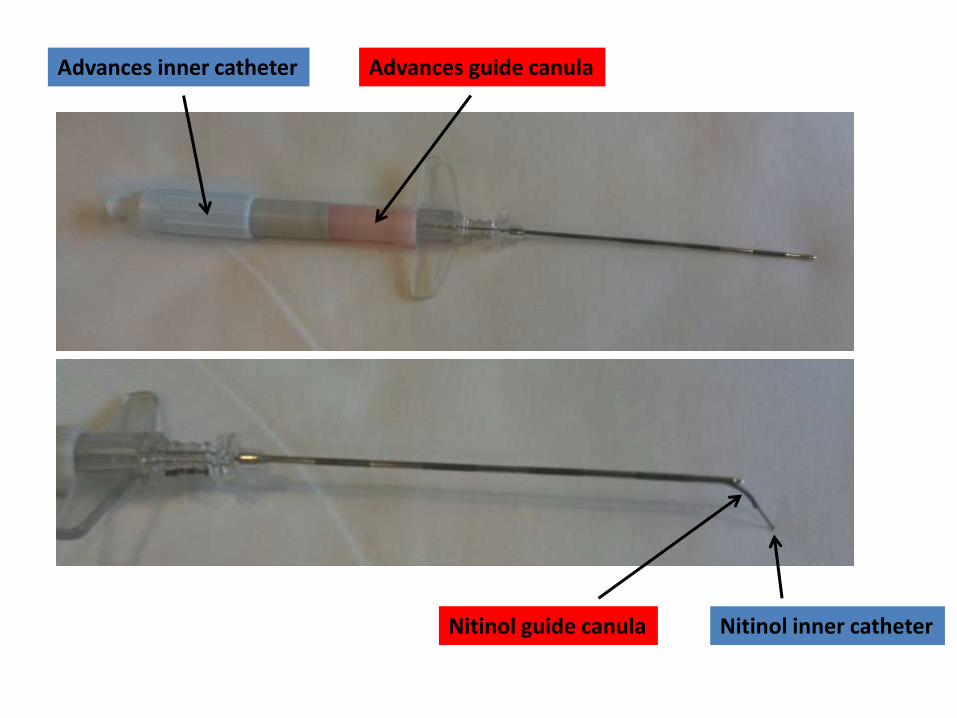
Advances inner catheter Advances guide canula
Nitinol inner catheterNitinol guide canula
What else besides placement can improve cell survival?
21
•Increase vascular supply with vascular growth factors•Condition cells for low oxygen survival while still in culture

The Results in Real Patients (not Rabbits)
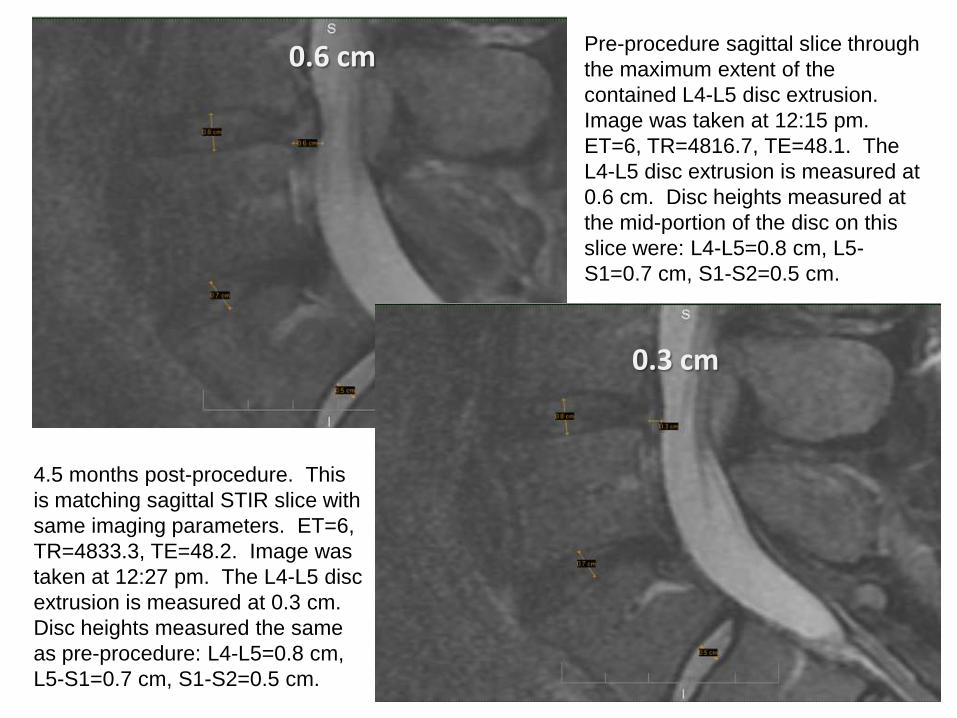
Pre-procedure sagittal slice through
the maximum extent of the
contained L4-L5 disc extrusion.
Image was taken at 12:15 pm.
ET=6, TR=4816.7, TE=48.1. The
L4-L5 disc extrusion is measured at
0.6 cm. Disc heights measured at
the mid-portion of the disc on this
slice were: L4-L5=0.8 cm, L5-
S1=0.7 cm, S1-S2=0.5 cm.
4.5 months post-procedure. This
is matching sagittal STIR slice with
same imaging parameters. ET=6,
TR=4833.3, TE=48.2. Image was
taken at 12:27 pm. The L4-L5 disc
extrusion is measured at 0.3 cm.
Disc heights measured the same
as pre-procedure: L4-L5=0.8 cm,
L5-S1=0.7 cm, S1-S2=0.5 cm.
0.6 cm
0.3 cm
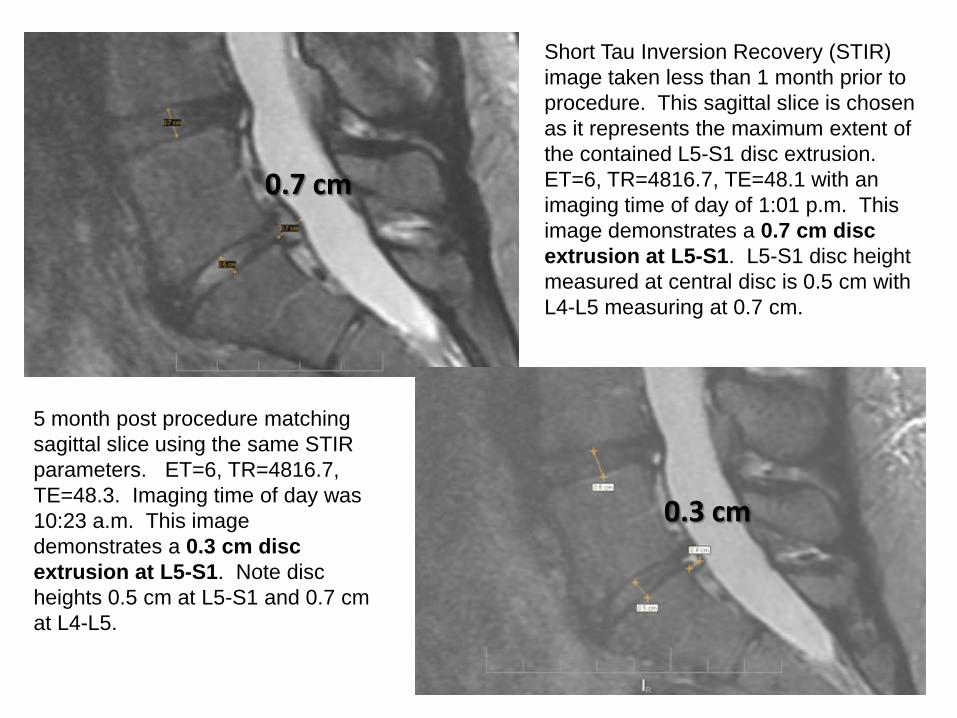
Short Tau Inversion Recovery (STIR)
image taken less than 1 month prior to
procedure. This sagittal slice is chosen
as it represents the maximum extent of
the contained L5-S1 disc extrusion.
ET=6, TR=4816.7, TE=48.1 with an
imaging time of day of 1:01 p.m. This
image demonstrates a 0.7 cm disc
extrusion at L5-S1. L5-S1 disc height
measured at central disc is 0.5 cm with
L4-L5 measuring at 0.7 cm.
5 month post procedure matching
sagittal slice using the same STIR
parameters. ET=6, TR=4816.7,
TE=48.3. Imaging time of day was
10:23 a.m. This image
demonstrates a 0.3 cm disc
extrusion at L5-S1. Note disc
heights 0.5 cm at L5-S1 and 0.7 cm
at L4-L5.
0.7 cm
0.3 cm
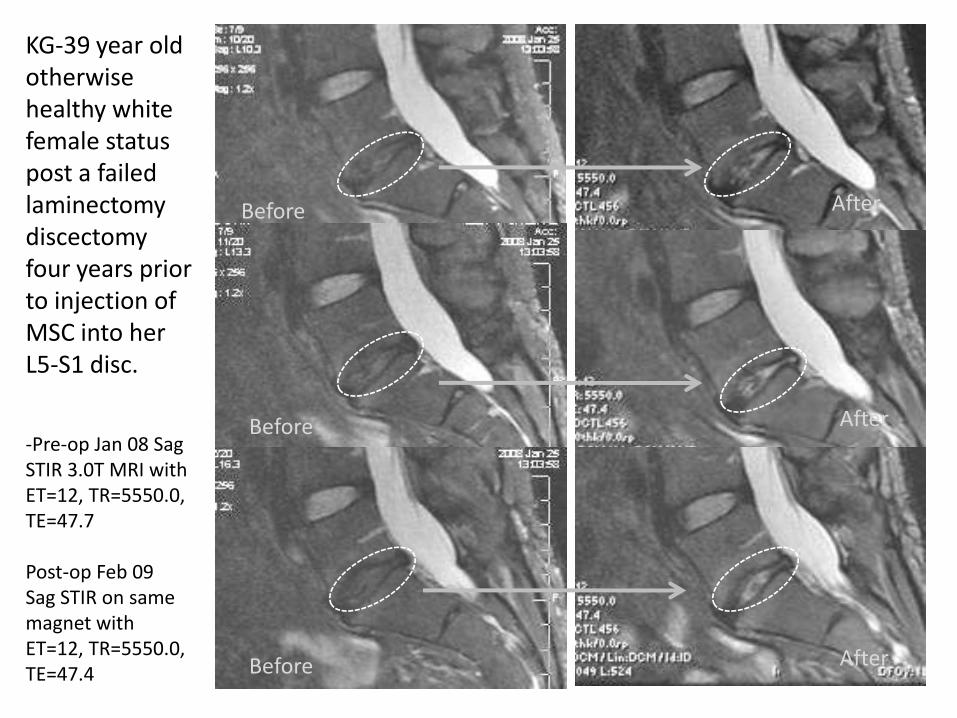
KG-39 year old otherwise healthy white female status post a failed laminectomydiscectomyfour years prior to injection of MSC into her L5-S1 disc.
-Pre-op Jan 08 Sag STIR 3.0T MRI with ET=12, TR=5550.0, TE=47.7
Post-op Feb 09Sag STIR on same magnet with ET=12, TR=5550.0, TE=47.4
Before
Before
Before
After
After
After
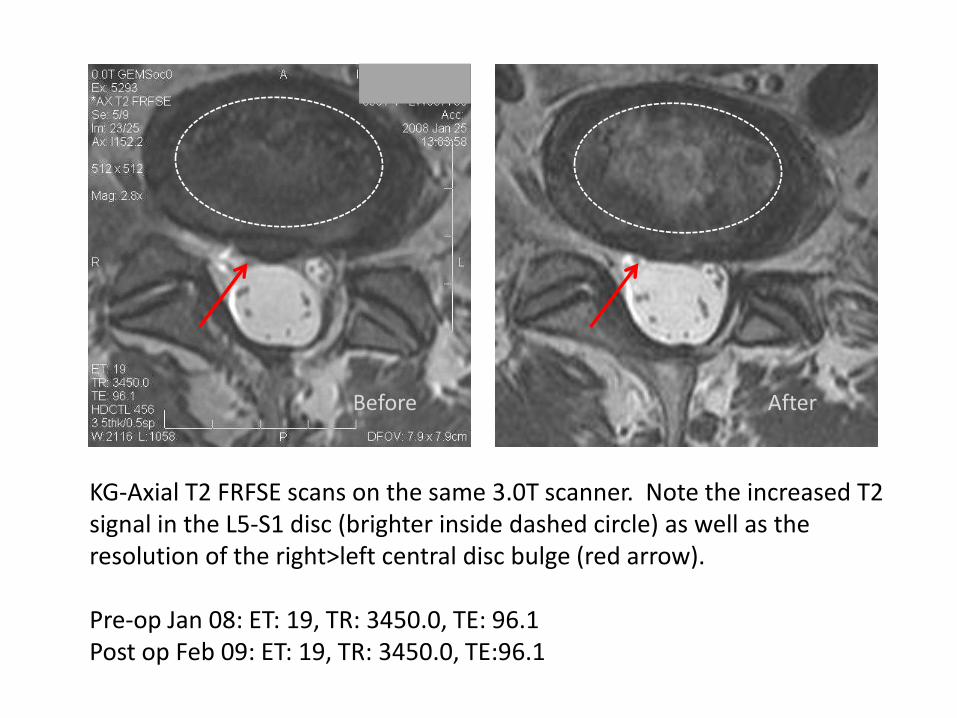
KG-Axial T2 FRFSE scans on the same 3.0T scanner. Note the increased T2 signal in the L5-S1 disc (brighter inside dashed circle) as well as the resolution of the right>left central disc bulge (red arrow).
Pre-op Jan 08: ET: 19, TR: 3450.0, TE: 96.1Post op Feb 09: ET: 19, TR: 3450.0, TE:96.1
Before After
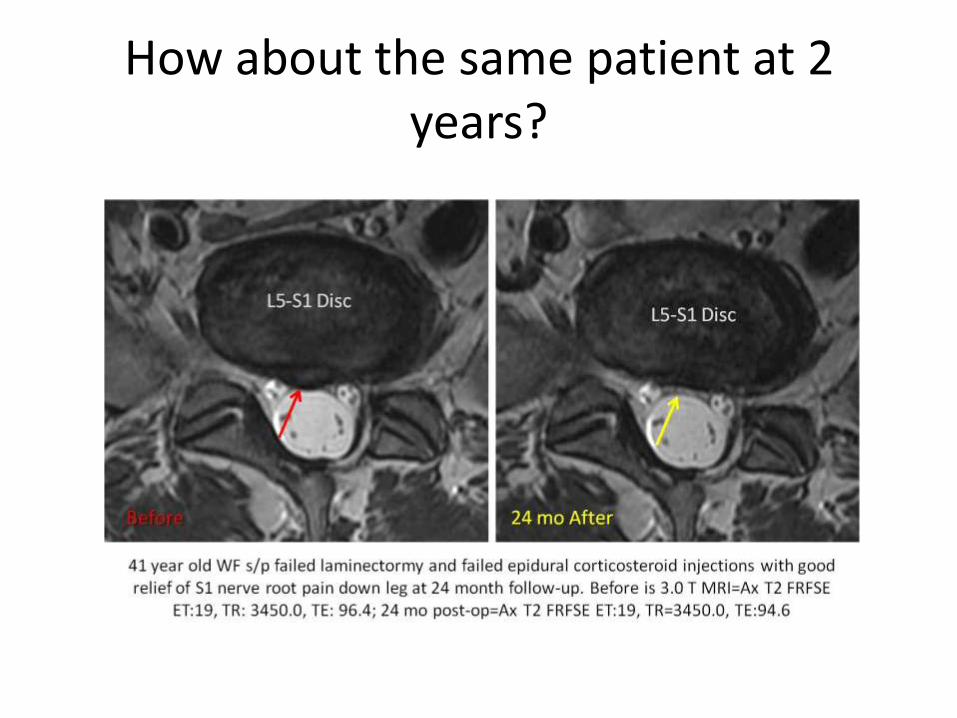
How about the same patient at 2 years?
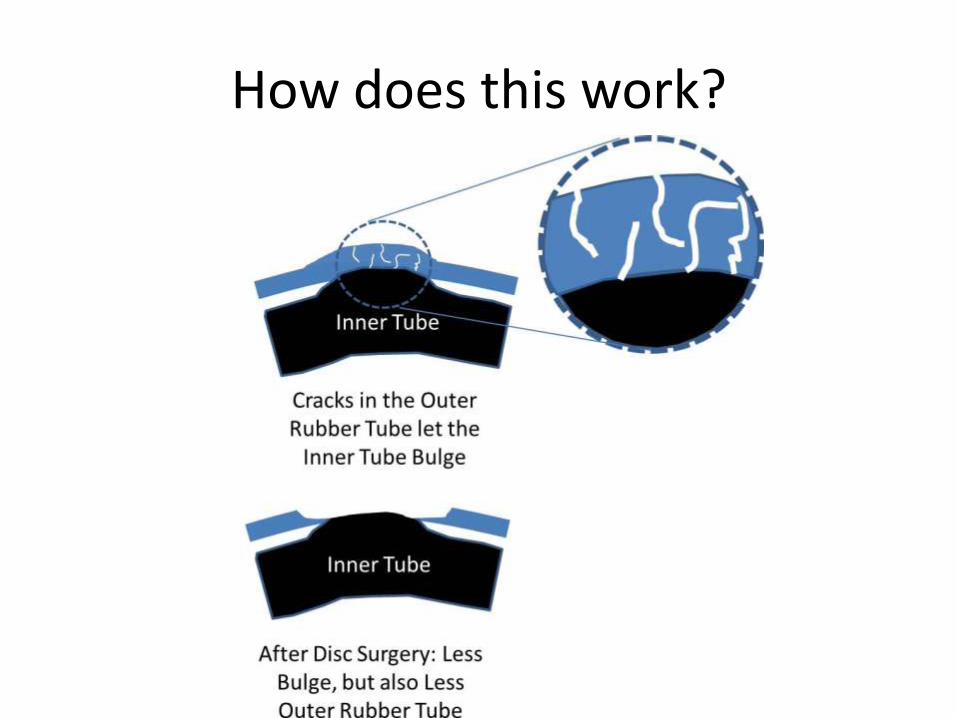
How does this work?
Is there a way to manage radiculopathy and avoid the high dose
steroids?
How about using platelets?
• We have been substituting platelet lysate for corticosteroid in epidurals for about 3 years.
• Our opinion is that it’s as good or better than steroids.
• Tracking two large groups (PL vs. steroids) and should have that data by fall.
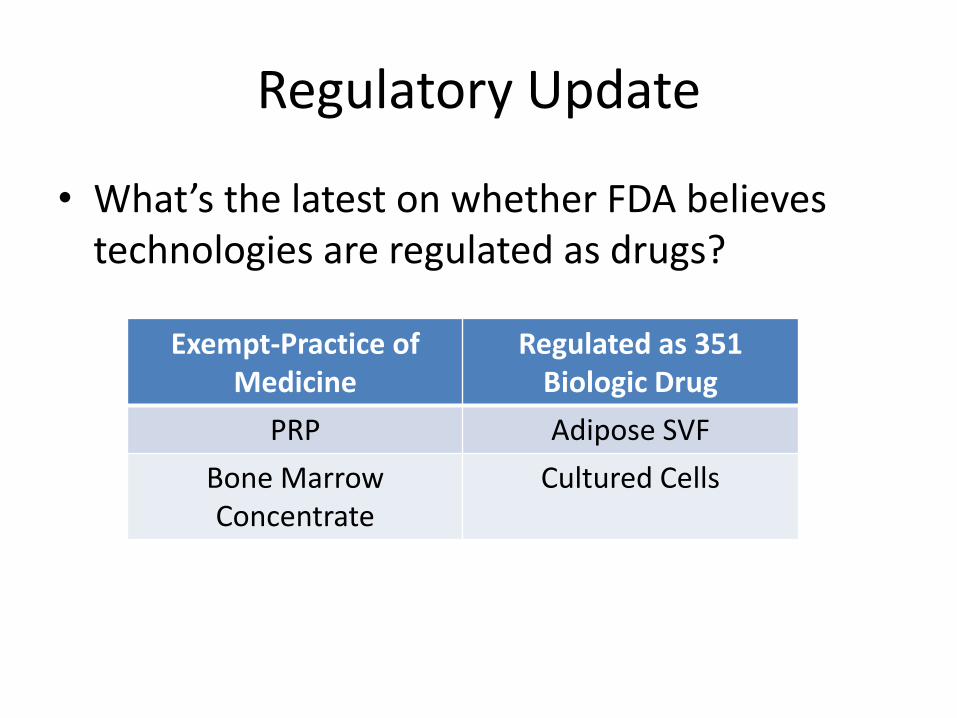
Regulatory Update
• What’s the latest on whether FDA believes technologies are regulated as drugs?
Exempt-Practice of Medicine
Regulated as 351 Biologic Drug
PRP Adipose SVF
Bone MarrowConcentrate
Cultured Cells
New Update: Adipose SVF is a Drug
• FDA Tissue Reference Group has issued at least two letters showing that SVF is a new drug requiring clinical trials
• The TRG has a special taskforce working on how to enforce this new initiative
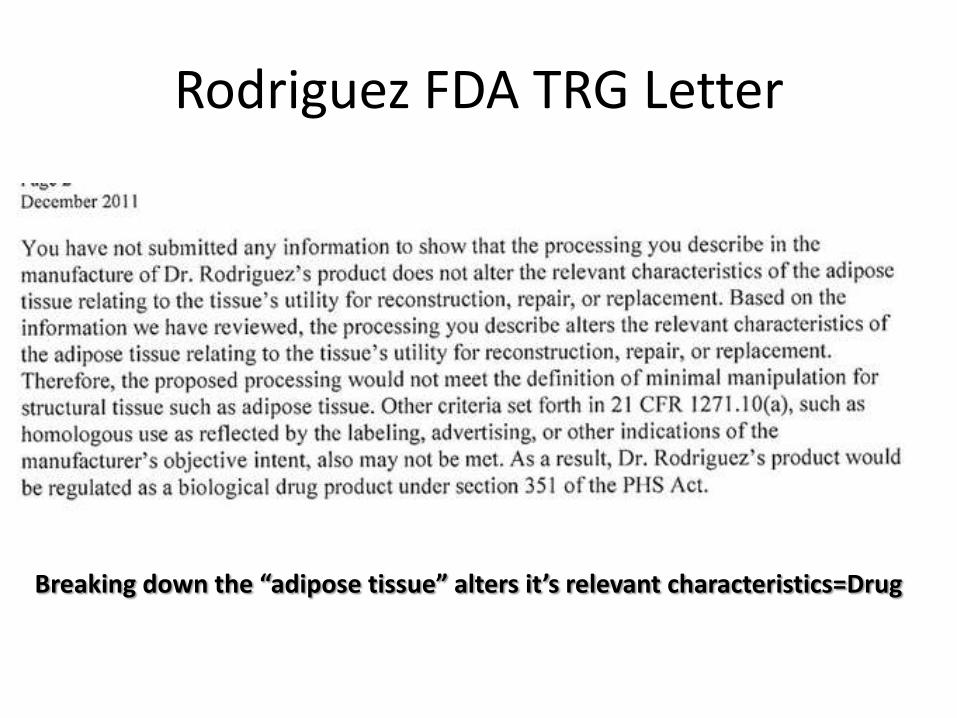
Rodriguez FDA TRG Letter
Breaking down the “adipose tissue” alters it’s relevant characteristics=Drug
Enforcement Actions on SVF
• State of Florida Medical Board/Department of Health revoked the license of a cardiologist infusing IV SVF for pulmonary fibrosis after the patient died-Homicide Investigation in progress
• State of Louisiana Medical Board has disallowed adipose SVF under the practice of medicine
On the flip side of the coin…
• State of Texas Medical Board now allows “non-FDA Approved” stem cells to be used under the practice of medicine as long as:
– The patient is consented as to the investigational nature of the care
– The procedure is approved through an IRB
Summary
• PRP and bone marrow concentrate don’t seem to help discs much
• Routinely cultured stem cells placed into the NP don’t work well either
• Specially cultured and administered stem cells do seem to be capable of resolving disc bulges
• PRP and Bone Marrow Concentrates are being left alone by FDA, adipose SVF is the next big FDA enforcement target
Recommended