8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 1/32
DECUBITUS ULCER
Presenters:
Angod, Lady Aizahlyn I.
Apat, Joselle Janina F.
Araune, Trixie Mariel E.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 2/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 3/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 4/32
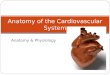
The skin is comprised of three major components:
-Epidermis
-Dermis
-Subcutaneous tissue
Though interrelated, each layer of skin has different structures, cell
types and functions.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 5/32
Definition ´Decubitusµ from the Latin decumbere, ´to lie downµ
Decubitus ulcers, also known as bedsores and pressure sores,
are caused by impaired blood supply and tissue malnutrition
owing to prolonged pressure over skin, soft tissue, muscle, or
bone.
Can occur anywhere on body

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 6/32
Over view It can develop on any part of the body where sustained
pressure and compressive forces are maintained for
a sufficient period of time.
Decubitus ulcers are listed as the direct cause of
death in 7²8% of paraplegics.
Some estimates suggest that 60,000 people die from
decubitus ulcers or their sequelae per year.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 7/32
RISK FACTORS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 8/32
Risk Factors and C au ses The factors causing pressure ulcers are divided into 2
Groups
INTRINSIC - Disease, medication, malnourishment, age,dehydration/fluid status, lack of mobility, incontinence, skincondition, weight.
EXTRINSIC ² External influences which cause skin distortion ²Pressure, Shearing Forces, Friction, Moisture.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 9/32
PressureTissues that are dependent on capillaries are deprived of their
blood supply because of pressure. Eventually the ischaemic
tissues will die.
Shearing ForcesShearing forces will only exist if pressure, usually caused by the persons
own body weight, is also present. Shear forces occur when a part of thebody tries to move but the surface of the skin remains fixed.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 10/32
FrictionFriction forces occur when the shearing force increases sufficiently toovercome the bodies resistance to movement. The movement has anabrasive action
MoistureS
kin should not be left wet as moist skin sticks to material (e.g.bathing, perspiration, incontinence (as urine and feces are acidic,amniotic fluid) as it can become macerated making it more susceptibleto shear and friction.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 11/32
SIGNS AND
SYMPT O MS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 12/32
A bedsore appears first as a reddened area of skin,
which then starts to break down to form an open, raw,oozing wound.
Bedsores occur at areas of abnormal pressure on the
body: In a wheelchair, this is usually the tailbone (coccyx) or
buttocks area, shoulder blades, spine, or backs of thearms or legs.
In a bed, they may occur on the back of the head, ears,shoulder blades, hips, lower back, tailbone, or thebacks or sides of the knees, elbows, ankles, or toes.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 13/32
Bedsores occur in st ag es:
Stage 1 has unbroken, but pink or ashen (in darker skin)
discoloration with perhaps slight itch or tenderness.
Stage 2 has red, swollen skin with a blister or openareas.
Stage 3 has a crater-like ulcer extending deeper into the
skin. Stage 4 extends to deep fat, muscle, or bone and may
have a thick black scab (eschar).

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 14/32
Here are some si g ns to indicate that an infection ha s
developed:
Thick yellow or green pus A bad smell from the sore
Redness or warmth around the sore
Swelling around the sore Tenderness around the sore
Si g ns that the infection may have spread incl ude:
Fever or chills
Mental confusion or difficulty concentrating
Rapid heartbeat
Weakness

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 15/32
DISEASE
PROCESS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 16/32
Individuals sitting/lying in the same
position for long periods of time
(ischemia)
Inadequate blood supply to tissues(ischemia)
Tissue damage and cell death
Bed Sore or decubitus ulcer

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 17/32
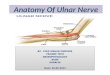
Pressure Ulcer Stag es

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 18/32
Stag e I Pressure Ulcer Skin is intact:
The ulcer appears as a defined area ofpersistent red, blue, or purple hues in lightly
pigmented skin.
In darker skin tones, it may appear withdiscoloration, warmth, edema, induration or
hardness.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 19/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 20/32
Stag e II Pressure Ulcer
Superficial ulceration of the skin:
Partial thickness skin loss involving epidermis,
dermis, or both.
The ulcer is superficial and presents clinically as
an abrasion, blister, or shallow crater.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 21/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 22/32
Stag e III Pressure Ulcer
A deep crater; full thickness loss of skin
tissue:
damage to or necrosis of subcutaneous tissue that mayextend down to, but not through, underlying fascia.
The ulcer presents clinically as a deep crater with orwithout undermining of adjacent tissue.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 23/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 24/32
Stag e IV Pressure Ulcer
Full thickness skin loss:
extensive destruction, tissue necrosis, or damage to
muscle, bone, or supporting structures
(e.g. tendon, joint capsule).
Undermining and sinus tracts also may be present.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 25/32

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 26/32
C O MPLICATI O NS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 27/32
Osteomyelitis
Hypercalcemia Myonecrosis
Necrotizing fasciitis
Amyloidosis
Sepsis
Gangrene Death
Autonomic dysreflexia

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 28/32
DIAGN OSTIC
TESTS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 29/32
How d oes the d oct or diagnose bed sores?
A doctor can make the diagnosis by examining the
patient's skin. Special diagnostic tests areusually unnecessary unless there are symptoms
of infection.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 30/32
W
hen are lab investigati o
ns necessary?
If a patient with bedsores develops symptoms of
infection, then a doctor may order diagnostic tests to
determine whether the infection has invaded the soft
tissues, bones, bloodstream or some other site. These
tests may include a complete blood count, a culture
of the infected bedsore, blood cultures to rule outsepsis, and bone X-rays to look for evidence of
osteomyelitis.

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 31/32
PRE V ENTI O NS

8/8/2019 Anatomy Presfinal
http://slidepdf.com/reader/full/anatomy-presfinal 32/32
Relieving pressure on vulnerable areas of skin
Reducing shear and friction
Inspecting the patient's skin at least once each
day
Minimizing irritation from chemicals
Encouraging the patient to eat well
Encouraging daily exercise Keeping the skin clean and dry
Recommended