Antibiotic Treatment-Resistant Lyme Arthritis
(TRLA)
NIH2/3/04
An Autoimmune Disease?

Clinical Features
Early Lyme Disease
Early Disseminated Lyme Disease
• Neurologic – cranial neuropathy,meningitis, radiculoneuropathy• Joint – Acute, inflammatory largejoint arthritis• Carditis
Late Lyme Disease
• Neurologic – peripheral neuropathy, encephalopathy• Chronic arthritis
Ixodes tick Borrelia burgdorferi(Bb)
Arthritic knee(Single joint)
Erythema migrans
• Erythema migrans (localized and multiple)• Flu-like illness
Acute Inflammatory vs. Chronic Arthritis
• Early attacks - within weeks to a few months after disease onset
• Sudden pain, swelling with massive effusions
• Mostly intermittent
• Remits after a few days/weeks sometimes without antibiotic therapy
• Develops after a prolonged period of latency/minimally symptomatic disease
• Defined as one year or more of persistent joint inflammation, usually the knee
• Does not subside in response to antibiotic therapy
• Correlates with the development of a strong
immune response to OspA (Outer Surface Protein A)
Treatment Resistant Lyme Arthritis(TRLA)

A+/C-A-/C-A-/C+A+/C+
1. unfed tick 3. recently infected host
2. feeding tick, fromgut to salivary gland
Osp Expression during Transmission

Evidence for OspA Upregulation In Vivo
Later in the course of infection, patients develop strong spiking titers of OspA antibodies coinciding with periods of arthritis (Kalish 1995).
Bb transmitted to the host express little or no OspA.
If these responses indicate OspA upregulation, then are inflammatory cues stimulating OspA expression by Bb?

Western Blot Analysis of Osp ExpressionIn vitro vs. In vivo vs. In vivo-Inflamed
Bb, in vitrochamber-grown
Bb, in vivochamber-grown
Flagellin, 41 kD
OspA, 31 kD
OspC, 21 kD
Bb, in vivochamber-grown,zymosan-induced inflammation

Prolonged Bb infection for the development of TRLA
• Antibiotic treatment in the first couple of weeks after exposure eliminates development of TRLA
• Antibiotic treatment later on has no effect
=> Initial exposure to spirochetes required
Autoimmune basis for TRLA
• Synovial samples are PCR-negative for B.burgdorferi DNA after antibiotic treatment1
• Increased frequency of HLA-DR4 alleles: HLA-DRB1*0401, 0404 and 0101, 0102 in the affected population2
1.Carlson et al., Arthritis & Rheumatism 42(12) 19992.Steere et al., New Engl Journal of Med.161 1990

Strong T-cell response to OspA:1. OspA-reactive T-cells in synovial fluid1
2. Human LFA-1 candidate T-cell autoantigen2
Molecular mimicry with OspA?
1.Meyer et al. PNAS 97(21), 20002. Gross et al. Science 281, 1998
A Shift in Paradigm:
1. Linked T-B recognition of autoantigen (GPI) – RA mouse model1. Linked T-B recognition of autoantigen (GPI) – RA mouse model
2. Ectopic germinal centers in RA synovium2. Ectopic germinal centers in RA synovium
Strong B-cell response to OspAStrong B-cell response to OspA
1.Matsumoto et al.Science 286,19992. Kim et al. J Immunol. 162(5), 1999
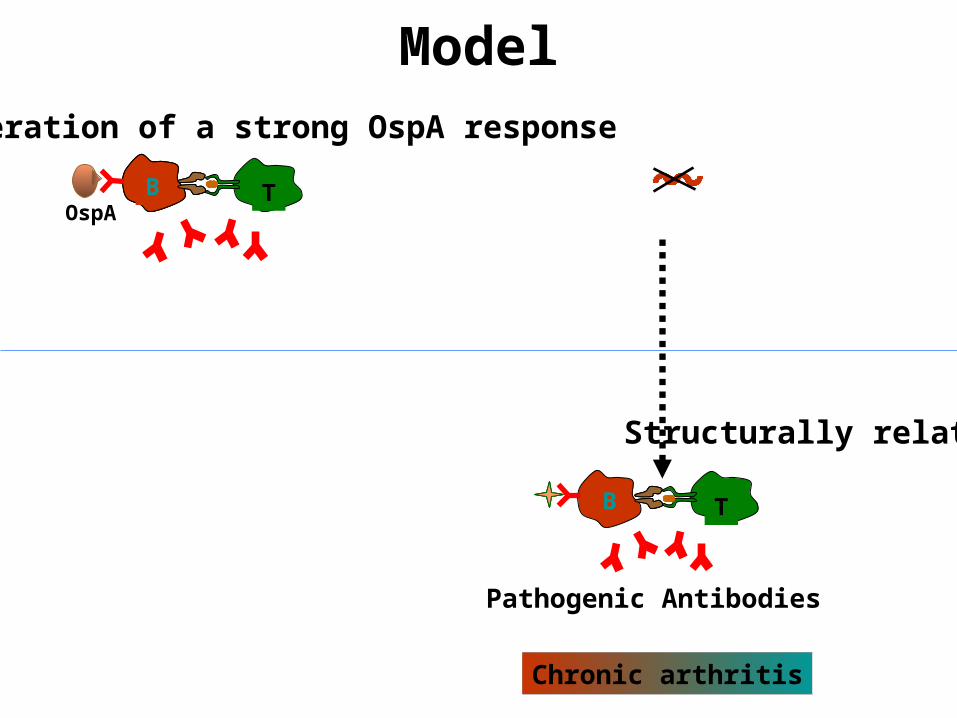
Model
B T
Generation of a strong OspA response
Pathogenic Antibodies
Molecular Mimicry
Structurally related
Chronic arthritis
OspA
B T
Antibiotics

1. Increased Titers of OspA antibodies
• IgG response to OspA develops later in the course of infection
• High titers of OspA antibodies coincide with periods of maximal arthritis
• Mark the transition from episodic to chronic arthritis
• Persist after treatment
2. Germinal centers in inflamed synovium 2222222• Tightly intermixed B-& T-cells
• Follicular dendritic cells
• Activated germinal center B-cells
• Plasma cellsAkin et al., Infection and Immunity, 67(1),1998
Kalish et al., Infection and Immunity 61(7), 1993
Steere et al., Arthritis and Rheumatism, .31 (4), 1988
Antibodies in Lyme ArthritisAntibodies in Lyme Arthritis

Isolation of Ig from single B cells
Stepwise introduction of somatic mutations

Patient ID: DCSample ID: 3-1
Rearranged kappa light chain
QGISSY A T T Y CQQLNSYPPGermline (L8)
QDISSY A ---3---- CQQFNMYPP1
QSISSY N 2
R
T
R CQQFNMYPP
CDR1 CDR2 CDR3
--------- -c-g-t-Germline (L8)
CDR1 CDR2 CDR3
----11---- -t-t-g-1
2
- t - g-
- t - c-
- g- g- t -
- g- a- t -
---- 11 ----- c- g- - a- g- c-
Nucleotide Sequence Alignment
- g- c- c- a- g
- g- c- c- a- t
- a- a- t - g- g - t - t - g-
1
2
Amino Acid Sequence Alignment
18
23
L8
--- 3----
Common CDR3

Patient ID: DCSample ID: 2-1
Rearranged gamma chain
GFTFSSYW Y V I Y M N A E CARGermline (3-7)
CVR1
2 CMR
1CDR 2CDR 3CDR
GFSLSI YW
GFSLSI YW
------ 8------
-- a- t - g- --------- - gc-Germline (3 - 7)
1CDR 2CDR 3CDR
-- t - a- t - ---- 13 ---- - gt -1
2
- t -
- g-
- c- t -
- c- t -
-- t - a- t - ---- 13 ---- - at -- g- - c- t -
Nucleotide Sequence Alignment
---
---
---
Amino Acid Sequence Alignment
2
1
3−7
19
20
------ 8------

Patient ID: DCSample ID: 2-1
Rearranged kappa light chain
QSISSW A S S Q T CQQYNSYS
QSIDIW T T S K S CQHYNRDS2
QSIDIW T T N K S CQHYNRDS3a
Germline (L12)
T T N K S CQHYNRDS3b QSIDIW
QSIDIW T T S Q S CQHYNRDS1
CDR1 CDR2 CDR3
L12
1
2
3a 3b
Amino Acid Sequence Alignment
9
10
11 11

OspA vaccine
Is it a problem?

Protein Sequence DR binding
B.b. B31-OspA 165-173 YVLEGTLTA + 6.5
hLFA-1 L332-340 YVIEGTSKQ + 7.3
B. afzelii OspA 165-173 FTLEGKVAN - 1.3
FTK-OspA 165-173 FTLEGKLTA + 0.2position 1 2 3 4 5 6 7 8 9
Modification of Main OspA T cell Epitope: Minimize Binding to HLA-DRB1*0401

Acknowledgements
Allen C. Steere
B. David Stollar
Jenifer Coburn
Theresa WillettHelena CrowleySrimoyee Ghosh
Recommended