Antithrombotics and Endoscopy: Advice for Endoscopy Nurses from
Cardiogastroenterology Clinic
Neena S. Abraham MD, MSc (EPID), FACG, FASGE, AGAFProfessor of Medicine, Mayo Clinic College of Medicine
Arizona Site Director, Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery
Division of Gastroenterology and Hepatology, Mayo Clinic, Scottsdale, AZDivision of Health Care Policy & Research, Department of Health Sciences
Research, Mayo Clinic, Rochester, MN

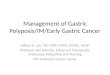
US Population: Age 65+ & Cardiac disease
Administration on Aging- 2012; Heidenreich et al. Circulation 2011.
0
20
40
60
80
100
1900 1920 1940 1960 1980 2000 2011 2020 2040 2060
Mil
lio
ns
By 2030, >40% of US adults will have ≥ 1 form of cardiovascular disease.
*Expected aggressive increase in antiplatelet and anticoagulant use for primary and secondary prevention.

Learning Objectives
1. Understand the GI bleeding risk of patients on antithrombotic regimens Antiplatelets
Anticoagulants
2. Review best-practice recommendations for peri-endoscopic antithrombotic management
ASA + Plavix (DAPT)
Coumadin- when/how/why to hold
Novel Oral Anticoagulants (Pradaxa, Xarelto, Eliquis, Lixiana) and procedure implications

Disclaimers--
THERE ARE NO RECIPES… ONE SIZE DOES NOT FIT ALL…
General Principles to follow for your education
Use Your Resources: a)ANTICOAGULATION Clinic….b)Referring physician/PCP/cardiologist

Low- vs. High-Risk Thromboembolic Conditions
Low-Risk High-RiskUncomplicated or
paroxysmal nonvalvular
atrial fibrillation
Bioprosthetic valve
Mechanical valve in the
aortic position
Deep-vein thrombosis
Atrial fibrillation associated with:Valvular heart diseaseProsthetic valvesActive CHFLVEF <35% History of thromboembolic event
Mechanical valve in any position and
previous thromboembolic event
Non-stented PCI after MI
Anderson et al. Gastrointest Endosc 2009.
Recently (~1 yr) placed coronary stent
Acute coronary syndrome
Prior stent occlusion
HypertensionDiabetes mellitusAge >75 yrs

Endoscopic Bleeding RisksBleeding risk varies with procedure type and presence/absence of
therapeutic interventions.
Becker et al. Am J Gastroenterol 2009; Kwok et al. Am J Gastroenterol 2009; Anderson et al. GIE 2009.
Low Risk (<2% @ 48 hours) High Risk (>2% @ 48 hours)
• Diagnostic + biopsy EGD Double balloon
enteroscopy Colonoscopy
• Biliary/pancreatic stent without sphincterotomy
• ERCP without sphincterotomy• EUS without FNA• Flexible sphincterotomy +
biopsy• Endosonography without FNA• Wireless capsule endoscopy
• Polypectomy: Gastric (7.2%) Duodenal/ampullary
1-3 cm (4.5%) >3 cm (10.3%)
• Endoscopic mucosal resection (22%)• Biliary sphincterotomy (2.0-3.2%)• PEG placement (0.2-2.5%)• Endosonography-guided FNA (0.5-2.9%)• Laser ablation and coagulation (1.1%)• Treatment of varices (2.4-25.4%)

Antiplatelets
Decrease platelet aggregation and inhibit thrombus formation
Aspirin (ASA)
P2Y12 Receptor-Antagonist
Clopidogrel (Plavix)
Prasugrel (Effient)
Ticagrelor (Brilinta)
Mechanism of Action
Irreversible inhibition of COX-1
and COX-2
Irreversible inhibition of
P2Y12 receptor
Irreversible inhibition of
P2Y12
receptor
Reversible inhibition of
P2Y12 receptor
Required time to recover adequate platelet function
7 days 5-7 days 7-9 days 3-5 days

Management of ASA Monotherapy
It is reasonable to perform endoscopic procedures in patients taking ASA.
StudyAntiplatelet
AgentProcedure Case Control
Bleeding Risk
Yousfi et al. 2004
ASA use within 3
days prior
Colonoscopy + polypectomy
40% 33%OR 1.41
(0.68-3.04)
Hussain et al. 2007
ASA or clopidogrel
within 10 days prior
Sphincterotomy 16% 17%OR 0.41
(0.13-1.31)
Becker et al. Am J Gastroenterol 2009.

2012-2013 Indications: Dual Antiplatelet Therapy
Jneid et al. J Am Coll Cardiol 2012; O’Gara et al. Circulation 2013.
ASA indefinitely and clopidogrel or ticagrelor for: Up to 12 months after
bare metal stent (BMS) placement
At least 12 months after drug-eluting stent (DES) placement
Post-StentPost-ACS Up to 12 months following
unstable angina or NSTEMI managed without PCI
At least 14 days (12 months in some) following STEMI
Updated to include ticagrelor and prasugrel.

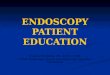
Risk of Clinical Events After Clopidogrel Cessation Among Patients with ACS
Ho et al. JAMA 2008.
0.0%
15.0%
30.0%
45.0%
60.0%
75.0%
PCI-Treated PatientsMedically Treated Patients
Inci
den
ce
of
De
ath
or
MI
0-90d 91-180d 181-270dDays Post-Clopidogrel Cessation
Significantly higher risk of adverse events (~2-fold increase) during first 0-90 days post-ACS with clopidogrel discontinuation

Stent Thrombosis Post-DES: Risk with Antiplatelet Cessation
Eisenberg M et al. Circulation 2009.
ASA and thienopyridine discontinued simultaneously (n=33)
ASA discontinued after thienopyridine previously discontinued (n=15)
Only thienopyridine discontinued; ASA continued (n=94)
0
60
120
Tim
e fr
om
Dru
g
Dis
con
tin
uat
ion
to
T
hro
mb
oti
c E
ven
t
7 days 7 days
122 days
Short-term discontinuation of thienopyridine is safe in patients with DES if ASA therapy maintained
P<0.0001P<0.0001
Patients with Thrombotic Event

ASA After Endoscopic Control of Peptic Ulcer Bleeding
RCT
Hospital-based cohort
Discontinuation of ASA CV patients is associated with increased mortality.
Sung et al. Ann Intern Med 2010. Derogar M et al. Clin Gastroenterol Hepatol 2013.
• Low-dose ASA (n=78) vs. placebo (n=78)
• 30-day recurrent bleeding: 10.3% vs. 5.4% ARR: 4.9%; NNT=20
• 30-day mortality: 1.3% vs. 9.0% ARI: 7.7%; NNH= 13
• N=118 • Discontinued ASA therapy: Mortality and CV event HR 6.3 (1.3-31.3)

Post-Polypectomy Bleeding With and Without Antithrombotic Therapy
Manocha D et al. Am J Med 2012. Singh M et al. Gastrointest Endosc 2010.
0
1
2
3
4
5
6
Overall Immediate(at endoscopy)
Per
cen
t (%
)
Post-Polypectomy Bleeding Type
Delayed(< 4 weeks)
ASA/NSAID (n=502)
No ASA/NSAID (n=672)
Clopidogrel (n=142)
No Clopidogrel (n=1243)
Overall Immediate(at endoscopy)
Delayed(< 4 weeks)
P=NS P=NS
P=NS P=NS
P=NS
P=0.02
100% on ASA
Cessation of ASA/NSAID before
colonoscopy/polypectomy is unnecessary.

Second Generation Thienopyridine Drugs: Rates of Bleeding Events
2nd generation thienopyridine agents
Higher levels of platelet inhibition than clopidogrel higher bleeding risk Most common bleeding location= GI Absolute increase greatest in elderly patients*
Ticagrelor and Prasugrel unaffected by variants of CYP2C19 genotype
Prasugrel unaffected by variants of ABCB1 genotype
Wiviott et al. NEJM 2007
0
0.5
1
1.5
2
2.5
3
3.5
Maj
or
Ble
edin
g (
no
n-C
AB
G)
(%)
2.4%1.8%
2.8%2.2%
Prasugrel Clopidogrel ClopidogrelTicagrelor
HR 1.32 (1.03-1.68) HR 1.19 (1.02-1.38)
TRITON-TIMI 38 Trial PLATO Trial
Bliden KP et al. Am Heart J 2011; Husted S et al. Circ Cardiovasc Qual Outcomes 2012; Cayla G QJM 2012; O’Gara et al. Circulation 2013.
Wallentin et al. N Engl J Med 2009.

Vorapaxar: New PAR-1 Inhibitor
Vorapaxar (Zontivity©)–protease-activated receptor 1 (PAR-1) inhibitor; First-in-class antiplatelet medication
Approved January 2014 and prescribed with DAPT
TRA 20 TIMI-50 trial (N=26,499)
13% reduction of MI, stroke, CV death and revascularization in patients with a previous MI or peripheral artery disease (v. placebo)
Increased moderate or severe bleeding in 4.2% (v. 2.5% placebo); 66% increased risk of bleeding overall
Black Box Warning: contraindicated with history of stroke, TIA and intracranial hemorrhage due to high-risk of bleeding
Bhatt D L et al. Circulation Research. 2014;114:1929-1943

Summary:Peri-Endoscopic Antiplatelet Management
Becker et al. Am J Gastroenterol 2009; Anderson et al. Gastrointest Endosc 2009; Boustiere C et al. Endoscopy 2011; Jneid et al. Circulation 2012; O’Gara Circulation 2013.
1. Avoid stopping all antiplatelets simultaneously.
2. When thienopyridine drugs are discontinued, you must maintain patient on ASA monotherapy.
3. Avoid cessation of thienopyridine drugs (even when ASA is continued) within the first 30 days of PCI and DES or BMS placement.
4. Avoid stopping DAPT in the first 90 days post-ACS.
5. Defer elective endoscopic procedures until patients finishes appropriate course of thienopyridine drug therapy, possibly up to 12 months following PCI and DES placement.
6. Perform elective high-risk endoscopic procedures 5-7 days after clopidogrel cessation, 7-9 days after prasugrel cessation, and 3-5 days after ticagrelor cessation.
7. Resume DAPT once hemostasis is achieved.
8. Continue antiplatelet therapy during elective low-risk endoscopy.

Oral Anticoagulants
Warfarin
Direct Oral Anticoagulants
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)*
Mechanism of Action
Inhibition of Vitamin K-dependent γ-carboxylation
Direct thrombin inhibitor
Direct factor Xa inhibitor
Direct factor Xa inhibitor
Metabolism Liver Renal Renal Renal/Liver
Time to maximum effect
90 d for circulating drug; ~5-7 d for a therapeutic INR
1.25-3 h 2-4 h 1-3 h
Half-life36-42 h for circulating
drug; ~5 d to normalize INR
12-14 h 9-13 h 8-15 h
Excretion 92% renal 80% renal 66% renal ~25% renal

FDA Approves Edoxaban • Approved by FDA January 2015
Oral, reversible Factor Xa inhibitor
62% bioavailable & [T Max]:1-2 Hrs
50% renal excretion
• AFIB Stroke Prevention, DVT/PE
• ENGAGE AF-TIMI 48 Trial warfarin vs. edoxaban (N=21,105)
EDX High Dose: 60 mg/day
EDX Low Dose: 30 mg/day
Both doses non-inferior to warfarin
23% increased GIB risk (High)
33% fewer bleeds overall (Low) Dose reduce with modest renal
impairment, <60 kg, P-glycoprotein inhibitor use
Giugliano et al. NEJM 2013; 369:22

Coumadin– Facts
Discontinue 5 days before procedure
Resume with hemostasis (immediately in most)
Peak onset within 72-96 hours; half-life 20-60 hours; 100% bioavailability
Reversal agents: FFP (fast), Vit K (slow)
High-risk thromboembolic patients
Bridge vs. no bridge?

Bridge Therapy –Who? Thromboembolic Risk Category
Atrial Fibrillation Mechanical Heart Valve
VenousThromboembolism(VTE)
Annual Risk >10% CHADS2* - 5 or 6CVA/TIA w/in 3 mosRheumatic valvular Disease
*CHF, HTN, Age >75, DM, Stroke
Mechanical Mitral ValveCaged-ball or tilting disk aortic valveCVA/TIA w/in 3 mos
VTE within 3 mosHigh-risk thrombophlebitis
Annual risk 5-10% CHADS2 - 3 or 4 Bileaflet Aortic Valve in high-risk patient
VTE 3-12 mos ago
Annual Risk <5% CHADS2 - ≤ 2 No prior CVA/TIA
Bileaflet Aortic Valve in low risk patient
VTE > 12 mos ago
Bridge Therapy organized thru Anticoagulation Clinic

New Data Regarding Bridge Therapy
BRIDGE investigators RCT (2015)
1884 non-valvular atrial fibrillation patients
May not apply to valvular afib, mechanical valves, LVADs, recently diagnosed thromboembolism (<3 months), Afib patients with CHF, post ACS setting etc.
Elective endoscopic and surgical procedures
Randomized to bridging vs. no bridging
Bridging Group (when compared to no bridging)
More major bleeding (3.2% vs. 1.3%)
No difference in thromboembolism risk (0.3% vs, 0.4%)
Douketis et al. NEJM 2015;373:823-833.

Supratherapeutic Warfarin Bleed
Choudari & Palmer. Gut 1994; Wolf A. Am J Gastroenterol 2007.
INR at time of endoscopy is not
predictive of rebleeding
Adjusted OR*: 0.50 (0.21-1.16) *Controlling for age, comorbidity, antiplatelet use, post-
procedure heparin and PPI use, hypotension, ulcer as bleeding source, and active bleeding at endoscopy
Normalizing INR does not reduce rebleeding but
delays endoscopy
• N=102 INR >1.3; Mean INR 1.8 (1.3-2.7)• Rebleeding rate similar with and without reversal agent: 24.7% vs. 30.0% (p=0.54)• Significant delay in endoscopy with normalization of INR: 20.9 h vs. 73.6 h (p<0.0001)• Important stigmata identified in 83% of cases
Endoscopic therapy is very effective– even in patients with moderately elevated INR.

Resuming Warfarin After GI Bleeding (GIB)
Witt DM et al. Arch Intern Med 2012.
Patients with warfarin-associated GIB and indications for continued long-term antithrombotic therapy should resume anticoagulation
within the first week following hemorrhage.
90-Day Thrombosis 90-Day Recurrent GI Bleeding
P=0.002
Warfarin Resumption within 4-7 days
HR: 0.05 (0.01-0.58)
P=0.10
Warfarin Resumption
Within 4-7 days HR: 1.32 (0.50-3.57)
Time in Days Time in Days

Trends in DOAC PrescriptionBarnes et al. Am J Med 2015

Temporary interruption of NOAC prior to endoscopic procedure
Drug (Creatinine Clearance)Last dose prior to low–risk endoscopic procedure *
Last dose prior to high–risk endoscopic procedure **
Dabigatran (>50 mL/min) 1 day 2 days
Dabigatran (31- 50 mL/min) 2 days 4 days
Dabigatran (<30 mL/min) 4 days 6 days
Rivaroxaban/Apixaban/Edoxaban (>50 mL/min)
1 days 2 days
Rivaroxaban/Apixaban/Edoxaban (31 to 50 mL/min)
1-2 days 3-4 days
Rivaroxaban/Apixaban/Edoxaban (< 30 mL/min)
2 days 4 days
* A low-risk procedure has a 48 hour risk of major bleeding of 0% to 2%; a high-risk procedure ** has a 48 hour risk of major bleeding of 2% to 4%

Management of DOAC Bleeding
van Ryan et al. Thromb Heamost 2010.
*Recommendations based on limited nonclinical data ** PCC= prothrombin concentrate complex
Mild Bleeding
Moderate-Severe Bleeding
Life-Threatening Bleeding
Correct hemodynamics to perfuse kidneysBlood-product transfusionEndoscopic evaluation +/- hemodialysis with renal failure Oral charcoal (if ingestion <2h)*; PPI probably helpful if recent ingestion (decreases absorption)
Consider rFVIIa or **PCC Charcoal filtration
Delay next dose Anticoagulant effect dissipates 24 h (with no renal failure)T1/2= 12-17 h
Initial Assessment and Risk Stratification: The ABC’sA= Airway; B= Breathing; C= Circulation

NOAC reversal agents: 2015 or 2016
• Idarucizumab (Praxbind®)•Humanized monoclonal antibody with high affinity for dabigatran; binds free and thrombin-bound dabigatran
• Clinical outcomes (Pollock CV et al. NEJM 2015):
•N=90 bleeding patients on Dabi or with need for surgery.
•2.5 gram bolus IV X 2 normalized dilute thrombin time in 93-98% of patients.
•Cessation of bleeding in 11.4 hours; normal surgical hemostasis in 92%
•Approved 10/16/15 by FDA for “life threatening hemorrhage/need for emergency surgery or procedures”; REVERSE-AD trial ongoing (N=450)

• Andexanet alpha• Phase II study in healthy volunteers
• Decreased anti-Xa activity and plasma concentration of free apixaban
• Future studies required in the setting of major hemorrhage
• Aripazine (PER977)• Synthetic molecule binds to heparin, LMWH and NOACs
in animals
• Whole blood clotting time (in vitro) show reduction of edoxaban effect within 10 minutes of IV infusion (restoration to 10% over baseline)
• Needs human studies and clinical trials
DOAC reversal agents: In Development

My Top 10 Cardiogastroenterology Tips
1. It is safe to perform endoscopy on ASA monotherapy.
2. Avoid stopping thienopyridine in first 90 days post-ACS.
3. Continue ASA therapy when stopping thienopyridine.
4. GIB leading to ACS should be scoped 48-72 h post-ACS. chance of finding high-risk endoscopic stigmata
Leads to faster cardiac catheterization in 43%
5. Endoscopic therapy is effective in patients with moderately elevated INR (< 2.7). No need to normalize INR.

My Top 10 Cardiogastroenterology Tips
6. Warfarin should be resumed within 4-7 days post-GIB.
7. New oral anticoagulants have GIB risk.
8. DAPT + new oral anticoagulants (triple antithrombotic therapy) associated with 3-fold risk of GIB.
9. NOAC-related bleeding Support hemodynamics to promote renal excretion of drug.
10.Elective peri-procedural NOAC management depends on patient’s CrCl: With normal CrCl:
o High-risk endoscopy Hold 2-3 days prior to caseo Low-risk endoscopy Hold 1-2 days prior to case
With impaired CrCL:o High-risk endoscopy Hold 4-6 days prior to caseo Low-risk endoscopy Hold 2-3 days prior to case
Recommended