Genetics in the North East (GeNE) welcomes the opportunity to provide this submission to the Family and Community Development Committee, leading the Victorian Parliamentary Inquiry in Perinatal Services in Victoria. Genetics of the North East is a collaborative network, comprising genetics services at Austin Hospital, the Mercy Hospital for Women and the Northern Hospital. With regard to this inquiry, areas of particular relevance to the GeNE network are the following; (i) ensuring equitable access to prenatal screening and diagnostic genetic services for pregnant women, (ii) ensuring women at increased risk of a pregnancy affected by structural or genetic abnormalities in their fetus have access to comprehensive maternal fetal medicine and genetic services; (iii) ensuring women found to have a pregnancy complicated by a genetic, structural or growth abnormality have access to tertiary diagnostic services, counselling and support for the ongoing management of the pregnancy.
Background
For the 78,000 pregnant women in Victoria every year, the application of fetal ultrasound and genetic screening in obstetrics has revolutionised the management of pregnancy. Routine use of ultrasound in the first half of pregnancy has improved the prediction of adverse obstetric outcomes in later pregnancy, enabled prenatal diagnosis of structural or genetic abnormality and diagnosis of those conditions which may be amenable to in utero therapy. In these latter conditions, the overarching goal of fetal intervention is to improve the health of children by intervening before birth to correct or treat prenatally diagnosed abnormalities.
In tandem with advances in ultrasound and fetal imaging, the last four decades has seen the rapid evolution of prenatal genetic screening. Aneuploidy and genetic screening programmes have advanced rapidly, and have been taken up with enthusiasm by pregnant women and their caregivers. The recent introduction of non‐invasive prenatal testing (NIPT) enables aneuploidy screening of unparalleled sensitivity and specificity, allowing many women to avoid the procedure related miscarriage risks associated with invasive diagnostic testing (amniocentesis and chorionic villous sampling). Unfortunately, this technology comes at a price, creating inequity in access across Victoria.
A high risk result on any genetic screening test commonly leads to invasive testing to confirm the diagnosis. Our capacity to interrogate the fetal genome continues to increase exponentially, and the advances in genomic technology mean the yield of genetic information from prenatal genetic samples is much greater than ever before.
Normal screening generates positive feelings about the pregnancy, but where an increased risk of genetic abnormality is identified, or a fetal abnormality is suspected on prenatal ultrasound, this is extremely stressful. Under these circumstances, women and their families require comprehensive, accurate and timely information about the likely condition.
1

They require prompt and reliable access to confirmatory imaging and genetic testing. Tertiary services are required to not only confirm the nature of the abnormality, but determine the likely aetiology, relevant associations, further investigations required as well as determine implications for the remainder of the pregnancy, labour and delivery, and the short and long term outlook for the baby. This information enables families to make well informed choices regarding the future of the pregnancy. In the face of serious or life threatening abnormalities, some families will make the difficult decision for termination of pregnancy. These women require timely and equitable access to related services, irrespective of their post code of residence. For families with ongoing pregnancies in the setting of a known fetal abnormality, future care planning for the pregnancy includes the need for ongoing maternal and fetal surveillance, and advice regarding the place, mode and timing of delivery, and need for specialist postnatal services.
1. The availability, quality and safety of health services delivering services to women and their babies during the perinatal period
Recommendations:
(i) Genetic screening should be available to all women and couples planning a pregnancy or in the early stages of pregnancy.
Rationale:
Most serious and common genetic conditions affecting a pregnancy arise from families not previously known to be at risk. For this reason, expert advisory groups such as Human Genetics Society of Australasia (HGSA) and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists specifically recommend that screening be offered to women and couples planning a pregnancy and in the early stages of pregnancy1. At present, barriers to pre pregnancy and pregnancy genetic screening include cost, and equity of access2. Health literacy for these conditions is generally low. An appropriately resourced workforce to engage in community and primary health care education is largely lacking, and a systematised approach to genomic health is necessary for these barriers to be addressed and overcome.
(ii) Best available aneuploidy screening should be offered to all Victorian women in early pregnancy.
Rationale:
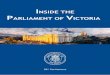
Of the 73,000 births in Victoria every year, nearly 85% of all pregnant women seek genetic screening for aneuploidy, specifically Trisomy 21. The number of prenatal diagnoses of major chromosome abnormalities has risen steadily over the past decades due to high population uptake of screening, improvements in prenatal screening tests and advances in molecular genetics. The number of major chromosome abnormalities detected in Victoria has doubled in the past 20 years (Fig 1). In 2015, a total of 530 chromosome abnormalities were diagnosed by amniocentesis or CVS prior to 25 weeks gestation in Victoria. Of these, 394 were major abnormalities (trisomies, monosomies, triploidy, pathogenic copy number variants (CNVs)). Trisomy 21 comprised the majority (51.8%) of these major abnormalities3.
2

Figure 1: Annual No. of major chromosome abnormalities detected in VIC 1996‐2015
Historically, screening for Trisomy 21 involved second trimester maternal serum screening, evolving to first trimester combined screening and more recently widespread uptake of noninvasive prenatal testing (NIPT). NIPT is the best available screening test for Trisomy 21, substantially reducing false positive rates, unnecessary invasive procedures and procedure related pregnancy losses. State wide data confirms that second trimester screening continues to be widely used in remote areas in Victoria (where there is limited access to high quality ultrasound), first trimester screening in metropolitan and major rural centres, and NIPT in high SES regions, predominantly in metropolitan Melbourne4.
This data clearly demonstrates that universal access and uptake of NIPT is limited by its cost. This is despite several economic modelling studies confirming the cost effectiveness of implementing NIPT, given its improved detection rate, reduced false positive rate and reduced need for ultrasound guided invasive procedures and genomic testing 5. Currently lacking is a framework where there is equitable access to NIPT for Victorian families, either as a primary screening test or as a ‘second tier test’ through an agreed contingent screening model. Victoria is in an excellent position to embed NIPT into public maternity care because it has a local non‐profit laboratory provider of NIPT in the Victorian Clinical Genetics Service. Such an innovative approach would capitalize on Victorian expertise at the Murdoch Children’s Research Institute (MCRI), a world leader in public health genetics research, qualitative studies of genetic screening, and the development of prenatal decision aids. MCRI is uniquely able to develop trustworthy, unbiased educational resources for professionals and the public. This is urgently needed as much of the existing information on NIPT is marketing materials created by commercial companies.
2. The impact that the loss of Commonwealth funding (in particular, the National Perinatal Depression Initiative) will have on Victorian hospitals and medical facilities as well as on the health and wellbeing of Victorian families
Recommendation
For women facing the diagnosis of a suspected or confirmed abnormality in their fetus, they require access to a multidisciplinary team, including perinatal mental health professionals in the perinatal period.
0
50
100
150
200
250
300
350
400
450
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
N
Trisomy 21 Other major chromosomal abnormality
3

Rationale: Comprehensive care in the face of a genetic or structural abnormality requires holistic care for the woman and her family. Discussion within a multidisciplinary team has been shown to improve decision making about management of unborn infants with serious abnormalities. The need for formal perinatal mental health practitioners to be incorporated into such services is highlighted by a recent study involving 1032 expectant mothers carrying fetuses with a confirmed anomaly. This study found that 19.3 % of women and 13.1 % of men reported significant post‐traumatic stress symptoms, and 14 % of men and 23 % of women scored positive for a major depressive disorder6. Pro‐active and pre‐emptive counselling and support for these families is necessary to minimise the impact of fetal abnormality on parents, their other children and their unborn baby.
3. The adequacy of the number, location, distribution, quality and safety of health services capable of dealing with high‐risk and premature births in Victoria
Recommendations:
(i) All Victorian women should have reliable and equitable access to tertiary genetic and maternal fetal medicine services when faced with a suspected diagnosis of genetic or structural abnormality in their fetus.
Rationale: As highlighted previously, the vast majority of pregnant women seek prenatal information regarding their future child. Given that most women who encounter an abnormal genetic diagnosis or structural abnormality during pregnancy were not previously known to be at risk, GeNE and related genetic services require adequate infrastructure and staffing support to ensure all women in Victoria have access to (i) clear and reliable public health messages, (ii) high quality information from primary care providers regarding population screening, (iii) prompt and effective triage of high risk families and results, (iv) tertiary level clinical and diagnostic genetic services in the case of screen positive results, detection of fetal abnormality or pregnancy complication.
A recent Victorian study has demonstrated the importance of providing timely access to accurate information and supportive, non‐judgemental care for women and their partners following prenatal diagnosis of a fetal abnormality7.
Participants identified that the shock of the diagnosis can be lessened when good care is delivered, by provision of:
clear, accurate and respectful communication;
empathic, non‐judgemental, professional support;
timely access to further testing and appointments;
seamless interactions with services and administration;
appropriate choices about invasive testing;
acknowledgment of the enormity and unexpected nature of the diagnosis
This access will be best achieved through well‐resourced clinical networks such as Genetics of the North East (GeNE); ‘hub‐and‐spoke’ models of referral and care between tertiary centres, and their metropolitan, regional, rural and primary care partners.
4

(ii) All Victorian women should have reliable and equitable access to downstream services following a confirmed diagnosis of genetic or structural abnormality in their fetus.
Rationale:
Downstream consequences of screening that will benefit from a co‐ordinated state‐wide strategy include prompt, equitable and reliable access to state of the art diagnostic testing, high quality genetic counselling services, family planning and related services, as well as tertiary obstetric, neonatal and paediatric care. These ‘downstream services’ are crucial when considering building service system capacity
4. The quality, safety and effectiveness of current methods to reduce the incidence of maternal and infant mortality and premature births
Recommendation:
That screening programmes for genetic and structural abnormalities address and prioritise testing strategies which minimise the risk of procedure related pregnancy loss or preterm birth.
Rationale: Prenatal diagnostic tests (amniocentesis or chorionic villous sampling) are associated with procedure related pregnancy loss, and pregnancy complications such as preterm prelabour rupture of membranes and preterm birth. Improved screening tests are able to reduce the rate of invasive procedures with these attendant risks. While prenatal detection of aneuploidy is increasing, invasive testing is decreasing due to improved specificity of Down syndrome screening tests (combined first trimester screening (FTS) had nasal bone assessment included from 2011, and cell‐free DNA based noninvasive prenatal testing became commercially available in 2013) 8. Invasive testing is now at its lowest level in 30 years. Ensuring equitable access to these advanced screening tests for all Victorian women can be expected to further improve the detection rate of aneuploidy while reducing procedure related pregnancy losses and complications.
5. Access to and provision of an appropriately qualified workforce, including midwives, paediatricians, obstetricians, general practitioners, anaesthetists, maternal and child health nurses, mental health practitioners and lactation consultants across Victoria
Recommendation:
That workforce projections also include Genetic Counsellors, Medical Geneticists, Maternal Fetal Medicine and Obstetric Imaging specialists. These practitioners need to be trained and maintained in the workforce to address the current and future prenatal screening requirements of pregnant women and their families.
Rationale: Genetic counselling services have evolved from largely ‘screening support’ to a high acuity services. Genetic counsellors carry much of the load associated with an increasing referral base, increasing number of diagnoses associated with structural abnormalities, high rates of
5

positive results following invasive testing and the high rate of uptake of termination of pregnancy in the face of abnormality. The increase in the number of women receiving a diagnosis of a fetal/chromosome abnormality has important implications for future service provision to ensure that this vulnerable patient group receive appropriate care and psychological support. Supervision and self‐care for genetic counsellors is essential to manage the increasingly demanding nature of the role. Similar demands are made on Medical Geneticists and Maternal Fetal Medicine/ Ultrasound specialists. The risk of ‘burnout’ and loss of workforce is a threat to the maintenance and growth of prenatal diagnosis services. Increased consumer demand in the area of prenatal diagnosis as well as the rapidly evolving science of genomic medicine, means the need for clinical service providers is expanding. It is imperative that primary care providers, obstetricians and midwives are well trained in the area of prenatal genetic screening, and that there are well established links with tertiary services.
6. Disparity in outcomes between rural and regional and metropolitan locations
Recommendation:
That there are clear and well established links between rural, regional, metropolitan and tertiary services to ensure timely and responsive care in the face of suspected structural or genetic fetal abnormality.
Rationale:
For women in regional and rural Victoria, delays in access to prenatal diagnostic services creates additional distress in the face of a suspected structural or genetic abnormality in their fetus. The development of telemedicine services is recommended to enable tertiary genetic and MFM support to be promptly delivered to women in rural areas. Access to family planning and related services is inequitable, with most of this inequity encountered in regional and rural Victoria. All women, irrespective of post code of residence should receive a timely referral, and reliable access to relevant services in the face of genetic or structural abnormality in their fetus.
7. Identification of best practice
Recommendation:
(i) That where there is an established evidence base that advances in genomic testing should be supported and taken up promptly into perinatal services
Rationale:
Prenatal testing: Genomic testing has evolved from basic karyotyping, to the greater resolution obtained with microarray and an attendant increase in diagnostic yield 9. The future holds promise of more and better information from exome sequencing10 Families clearly prioritise the quality and depth of information provided at this time, yet action areas required include (i) a consistent statewide approach to testing algorithms and the applicability of genome wide or targeted sequencing, (ii) a highly skilled and well‐resourced
6

genetic counselling workforce and (iii) close links to research networks that maintain and interrogate large genomic databases in order to maximise the genomic information available and fulfil the potential of this testing to Victorian families.
Post mortem testing: Stillbirth affects 1:130 Victorian families. In a significant number of cases, an underlying cause is never identified. For families who suffer stillbirth or neonatal death, the additional information obtained from genetic sampling after birth can make an immense difference to understanding the reason for the baby’s death, and provide a sign post for future pregnancies of the likelihood of recurrence. As outlined for structural abnormality, priority areas include engagement with stakeholders, providing leadership in the diagnostic testing approach (karyotype, microarray, exome sequencing etc) and facilitating appropriate follow up.
(ii) Regular, accurate, and timely state‐wide reporting of prenatal testing and congenital anomalies are urgently needed to ensure best practice in maternity care and to enable early detection of environmental teratogens.
Rationale:
A review of the Congenital Anomalies Reports from 2007‐09 and 2013‐14 suggests massive underreporting of chromosome anomalies in the 2013‐14 document ‐ about half of the actual prevalence as ascertained through academic sources. Furthermore, prenatal screening for chromosome abnormalities is now fragmented among several commercial and not‐for‐profit providers. There is no systematic oversight of the performance of the various available screening tests (i.e. combined first trimester screening with ultrasound and serum markers, second trimester serum screening, and NIPT). Of particular note, NIPT is provided by both local and international laboratories, with no public reporting of the performance of these test results in our population, despite many thousands of women paying approximately $500 directly out of pocket for these tests each year.
Ascertainment of structural congenital anomalies detected by prenatal ultrasound is also unreliable due to the reliance on voluntary reporting, and the lack of state‐wide data collection on terminations for fetal anomalies prior to 20 weeks gestation across the public and the private sectors. The Australian response to the Zika virus epidemic highlighted the shortcomings of our state birth defects monitoring system, both in the timeliness of reporting (the VIC 2007‐09 Congenital Anomaly Report was only published this year), and its incompleteness due to the reliance on voluntary reporting.
The performance of Victoria’s prenatal screening program cannot be evaluated, and the early detection of an emerging birth defect epidemic will not be possible, unless state‐wide data collection on both structural and genetic anomalies is improved, through mandatory reporting from laboratories, maternity and paediatric services, and linkage between obstetric and newborn datasets.
7

References 1. Joint statement: RANZCOG and HGSA: Prenatal screening and diagnosis of chromosomal and genetic
conditions in the fetus in pregnancy. Accessed 6.9.16 https://www.ranzcog.edu.au/college‐statements‐guidelines.html
2. Massie J, Ioannou L, Delatycki M. Prenatal and preconception population carrier screening for cystic fibrosis in Australia: where are we up to? Aust N Z J Obstet Gynaecol. 2014 Dec;54(6):503‐9
3. Hui L, Hutchinson B, Poulton A, Halliday JL. Population‐based impact of noninvasive prenatal screening (NIPS) on screening and diagnostic testing for fetal aneuploidy. Genet Med. 2017 doi:10.1038/gim.2017.55
4. Hui L, Barclay J, Poulton A, Hutchinson B, Halliday J. Prenatal diagnosis and socioeconomic status in the noninvasive prenatal testing era: a population based study. Submitted, under review BJOG June 2017.
5. RAPID Non invasive prenatal testing (NIPT) evaluation study; a report for the UK National Screening Committee
6. Cole JC, Moldenhauer JS, Berger K, Cary MS, Smith H, Martino V, Rendon N, Howell LJ. Identifying expectant parents at risk for psychological distress in response to a confirmed fetal abnormality. Arch Womens Ment Health. 2016 Jun; 19(3):443‐53.
7. Hodgson J, Pitt P, Metcalfe, et al. Experiences of prenatal diagnosis and decision‐making about termination of pregnancy: A qualitative study. Aust NZ Obstet Gynaecol 2016; 56: 605‐6013.
8. Johnson K, Kelley J, Saxton V, Walker SP, Hui L. Declining invasive prenatal diagnostic procedures: A comparison of tertiary hospital and national data from 2012 to 2015. Aust N Z J Obstet Gynaecol. 2017; 57: 152‐156.
9. Stark Z, Gillam L, Walker SP, McGillivray G. Ethical controversies in prenatal microarray. Curr Opin Obstet Gynecol. 2013 Apr;25(2):133‐7.
10. Pangalos C, Hagnefelt B, Lilakos K, Konialis C First applications of a targeted exome sequencing approach in fetuses with ultrasound abnormalities reveals an important fraction of cases with associated gene defects. PeerJ. 2016 Apr 26;
8
Recommended