Nik Jah1, Pauline Siew Mei Lai1, Chirk Jenn Ng1, Lynne Emmerton2
1Department of Primary Care Medicine, University Malaya Primary Care Research Group (UMPCRG), Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
2 School of Pharmacy, Curtin University, GPO Box U1987, Perth WA 6845, Australia
Barriers and facilitators to community pharmacy management of people with osteoporosis in Malaysia: A qualitative study
1
Introduction
• Osteoporosis has significant impact on healthcare costs and quality of life1
• By the year 2050, almost 50% of hip fractures worldwide will occur in Asia due to an increase of the elderly population2
• Untreated osteoporosis incurs significant costs to primary and secondary care3
1. Cauley JA.(2013) The Journals Of Gerontology, 68(10):1243-51.2. Cooper C, et.al (1992). Osteoporosis International, ;2(6):285-9
3. Harvey N, Dennison E, Cooper C. (2010) Nature reviews Rheumatology, 6(2):99-105.
2
2-3/1/2017
• Community pharmacists can play an important role in providing pharmaceutical care4 (the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s health-related quality of life) for people with osteoporosis5
• However, amongst the models for collaborative disease state management services published internationally, there is sparse evidence regarding the role of community pharmacists in the provision of osteoporosis care.
4. Hepler CD, et.al.(1990) American Journal Hosp Pharm, 47(3):533-43.5. Summers KM, et.al.(2005). Annals of Pharmacotherapy, 39(2):243-8.
3
3-3/1/2017
Objective
• To explore barriers, facilitators and the scope of a hypothetical osteoporosis management service by community pharmacists in Malaysia, informing a vision for developing this service.
4
4-3/1/2017
Methods
• Study design: Qualitative
• Setting : Kuala Lumpur, Malaysia
•Duration: October 2013 to July 2014
55-3/1/2017
Participants
• Included were• Community pharmacists from independent and chain pharmacies
• Working full time (8 hours for 5 days/ week)
• Excluded were locums
• Purposive sampling and the snowballing method was used
• Sample size: estimated 20 participants or until data saturation occurred
6
6-3/1/2017
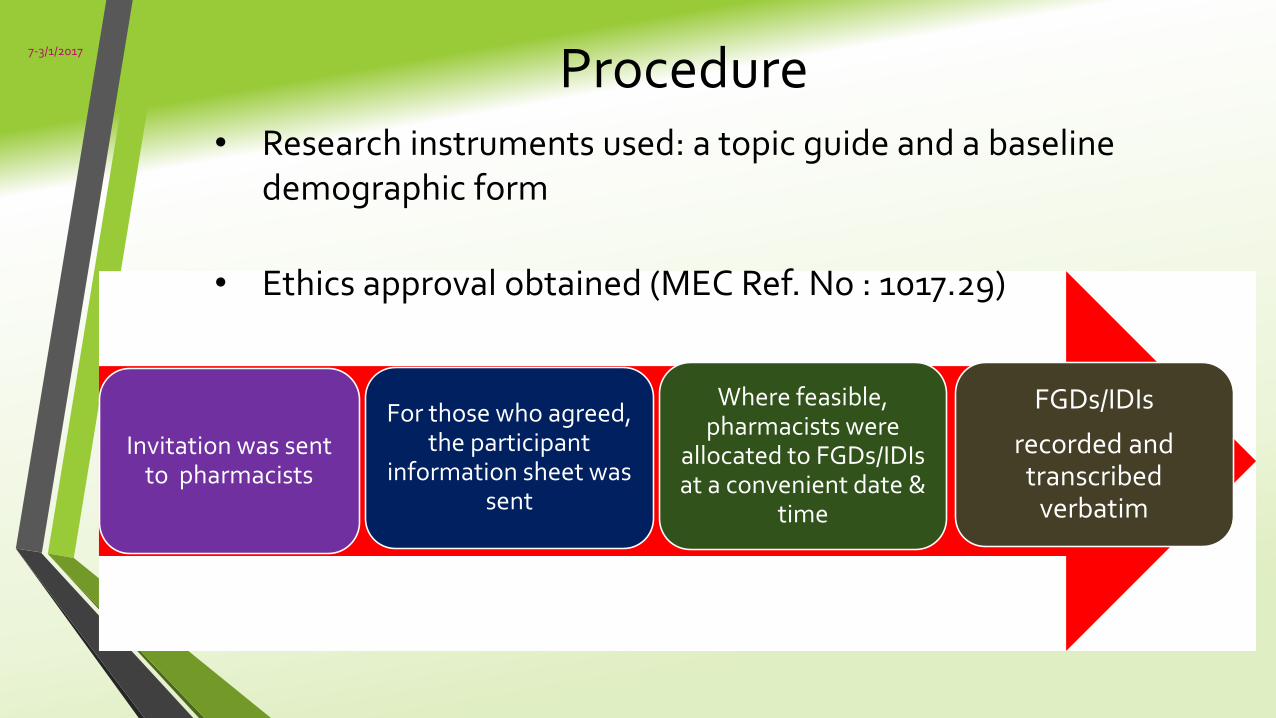
Procedure
Invitation was sent to pharmacists
For those who agreed, the participant
information sheet was sent
Where feasible, pharmacists were
allocated to FGDs/IDIs at a convenient date &
time
FGDs/IDIs
recorded and transcribed
verbatim
• Research instruments used: a topic guide and a baseline demographic form
• Ethics approval obtained (MEC Ref. No : 1017.29)
7
7-3/1/2017
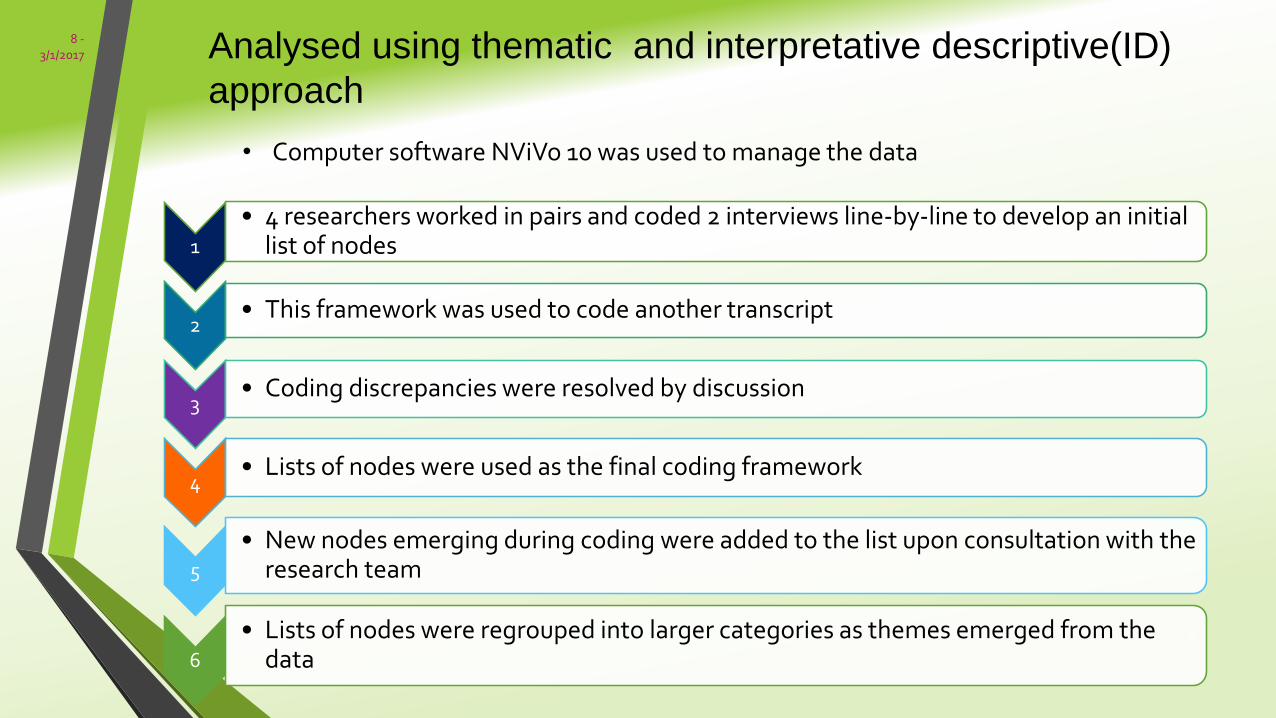
Analysed using thematic and interpretative descriptive(ID)
approach
1
• 4 researchers worked in pairs and coded 2 interviews line-by-line to develop an initial list of nodes
2 • This framework was used to code another transcript
3• Coding discrepancies were resolved by discussion
4• Lists of nodes were used as the final coding framework
5
• New nodes emerging during coding were added to the list upon consultation with the research team
6
• Lists of nodes were regrouped into larger categories as themes emerged from the data
• Computer software NViVo 10 was used to manage the data
8
8 -3/1/2017
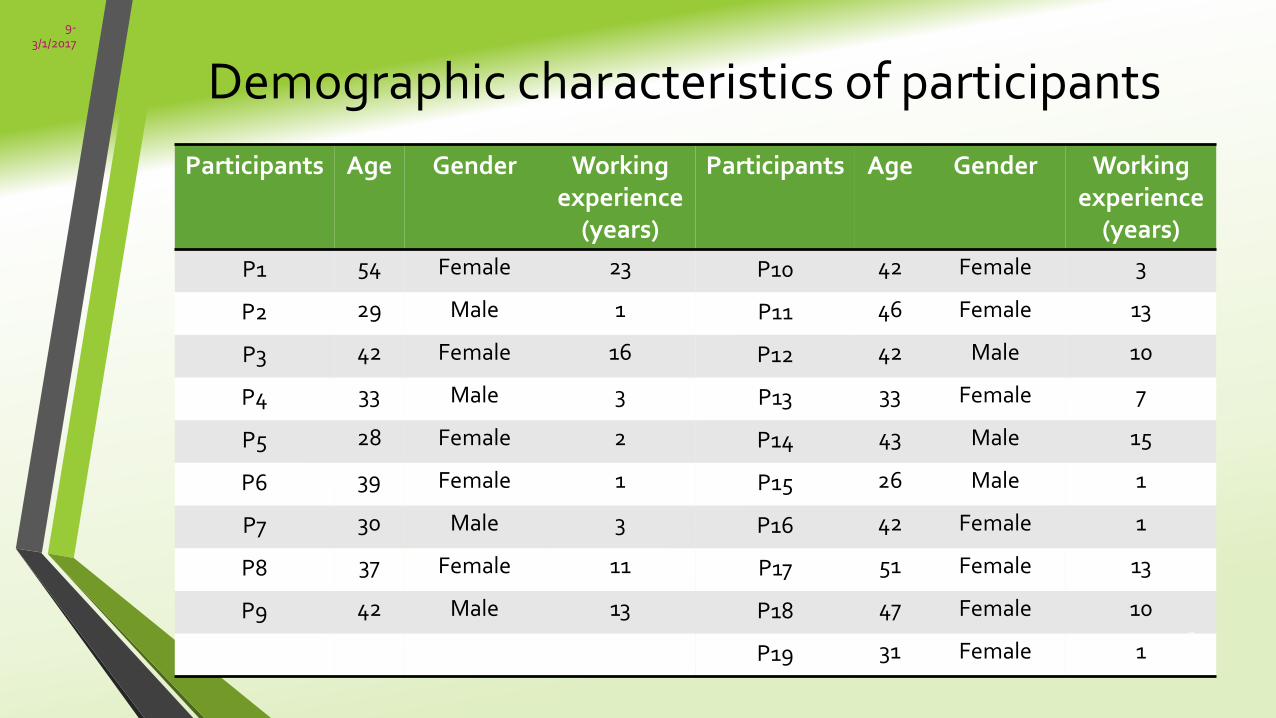
Demographic characteristics of participants
Participants Age Gender Working experience
(years)
Participants Age Gender Workingexperience
(years)
P1 54 Female 23 P10 42 Female 3
P2 29 Male 1 P11 46 Female 13
P3 42 Female 16 P12 42 Male 10
P4 33 Male 3 P13 33 Female 7
P5 28 Female 2 P14 43 Male 15
P6 39 Female 1 P15 26 Male 1
P7 30 Male 3 P16 42 Female 1
P8 37 Female 11 P17 51 Female 13
P9 42 Male 13 P18 47 Female 10
P19 31 Female 19
9-3/1/2017

Results
Description of pharmaceutical care service components
Barriers
Facilitators
10
10-3/1/2017
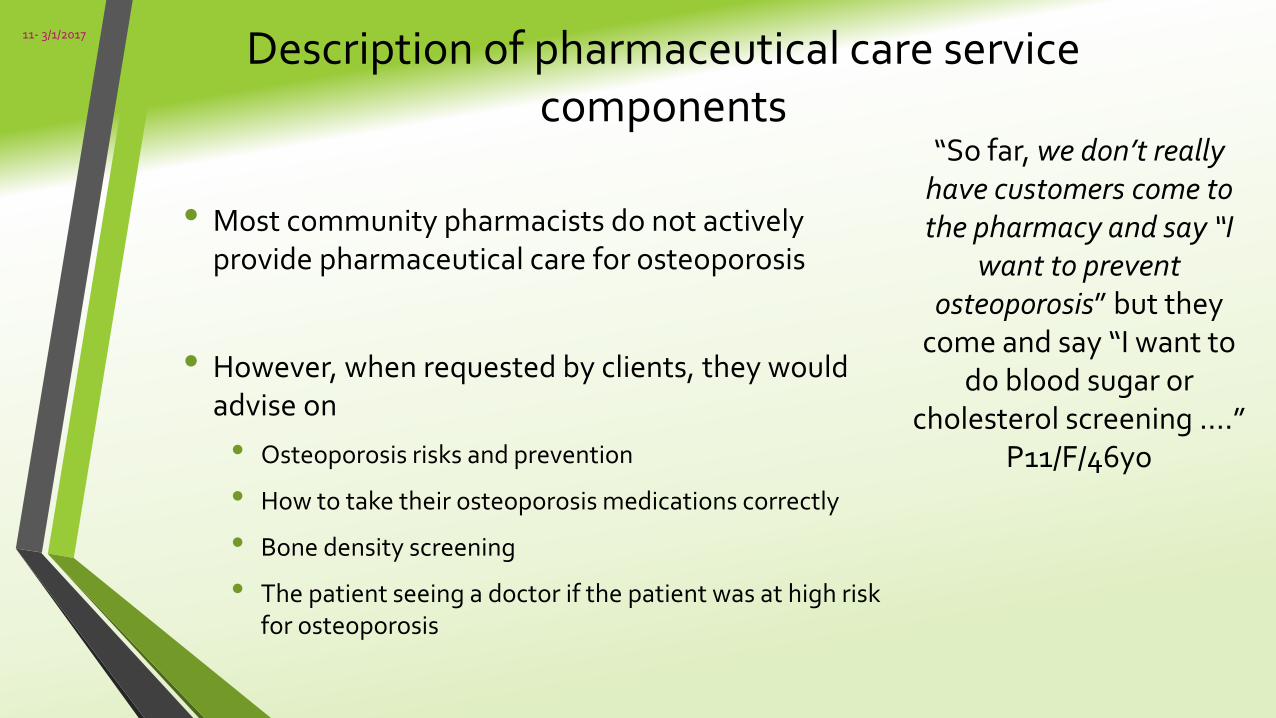
Description of pharmaceutical care service components
• Most community pharmacists do not actively provide pharmaceutical care for osteoporosis
• However, when requested by clients, they would advise on
• Osteoporosis risks and prevention
• How to take their osteoporosis medications correctly
• Bone density screening
• The patient seeing a doctor if the patient was at high risk for osteoporosis
“So far, we don’t really have customers come to the pharmacy and say “I
want to prevent osteoporosis” but they
come and say “I want to do blood sugar or
cholesterol screening ….”P11/F/46yo
11- 3/1/2017
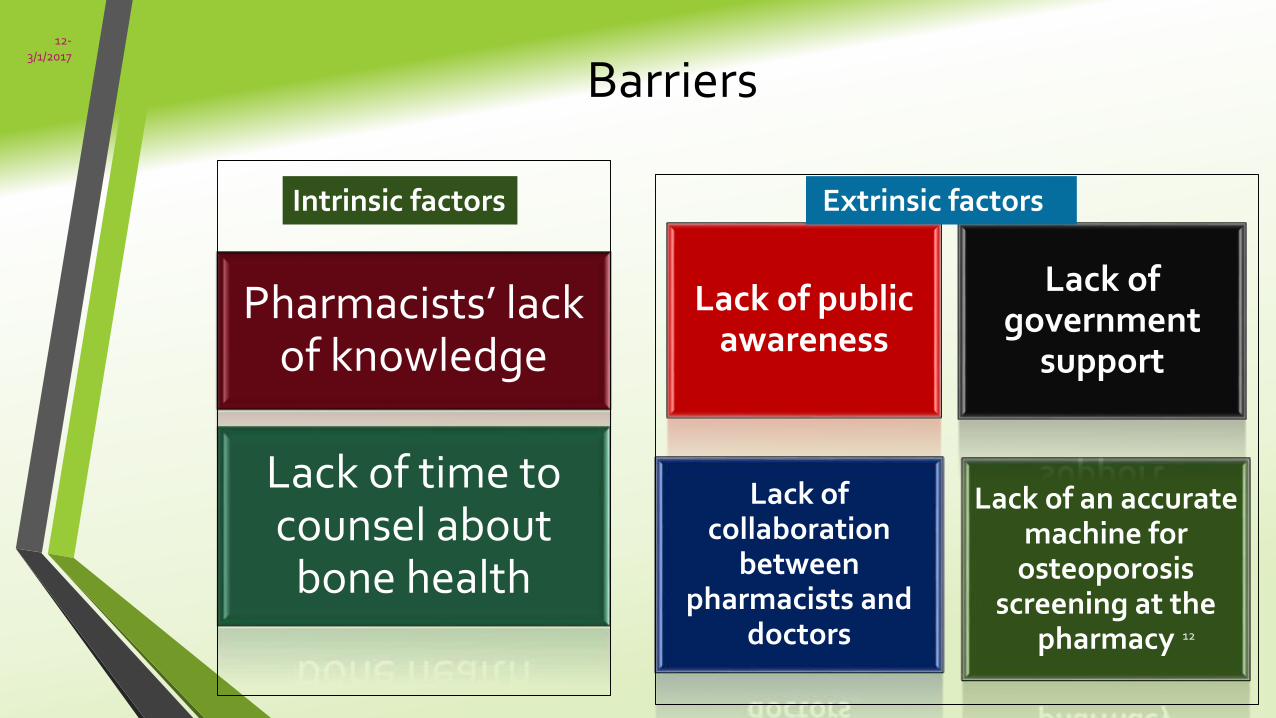
Barriers
Lack of public awareness
Lack of an accurate machine for
osteoporosis screening at the
pharmacy
Lack of collaboration
between pharmacists and
doctors
Lack of government
support
Pharmacists’ lack of knowledge
Lack of time to counsel about
bone health
Extrinsic factorsIntrinsic factors
12
12-3/1/2017
Intrinsic factors
“…I’m not that confident because I do not have a big
picture of what osteoporosis is all about: its treatment,
the apparatus used to screen for Osteoporosis …. So, the management part, I am not
that familiar.”
37yo female
• Lack of knowledge and time
• Not familiar with osteoporosis
• Perceived that osteoporosis is a complicated disease, so they were not confident to advise on osteoporosis
• Felt that the provision of pharmaceutical care in osteoporosis would take a lot of time
• Need to allocated special time to provide pharmaceutical care to osteoporosis patients
13- 3/1/2017
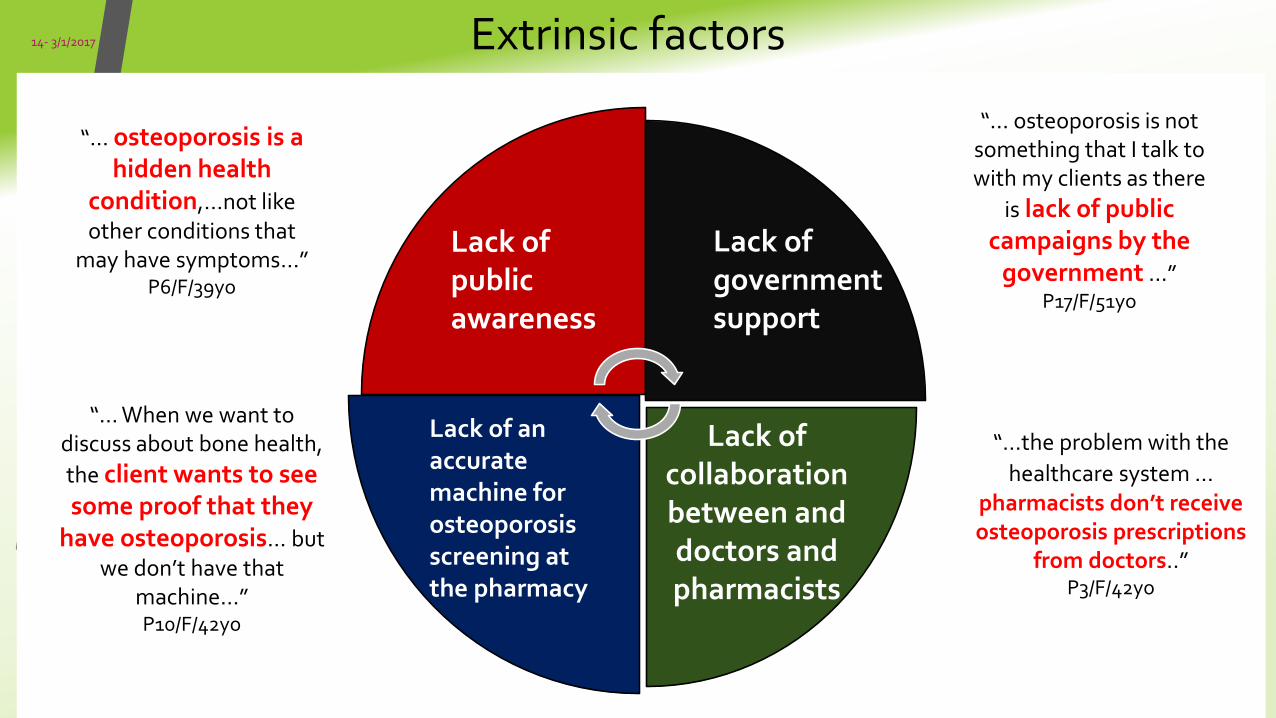
Extrinsic factors
Lack of government support
Lack of collaboration between and doctors and pharmacists
Lack of public awareness
“… When we want to discuss about bone health,
the client wants to see some proof that they
have osteoporosis… but we don’t have that
machine…” P10/F/42yo
“…the problem with the
healthcare system …pharmacists don’t receive osteoporosis prescriptions
from doctors..”P3/F/42yo
“… osteoporosis is not something that I talk to with my clients as there
is lack of public campaigns by the
government …”P17/F/51yo
“… osteoporosis is a hidden health
condition,...not like other conditions that
may have symptoms…”P6/F/39yo
Lack of an accurate machine for osteoporosis screening at the pharmacy
14
14- 3/1/2017
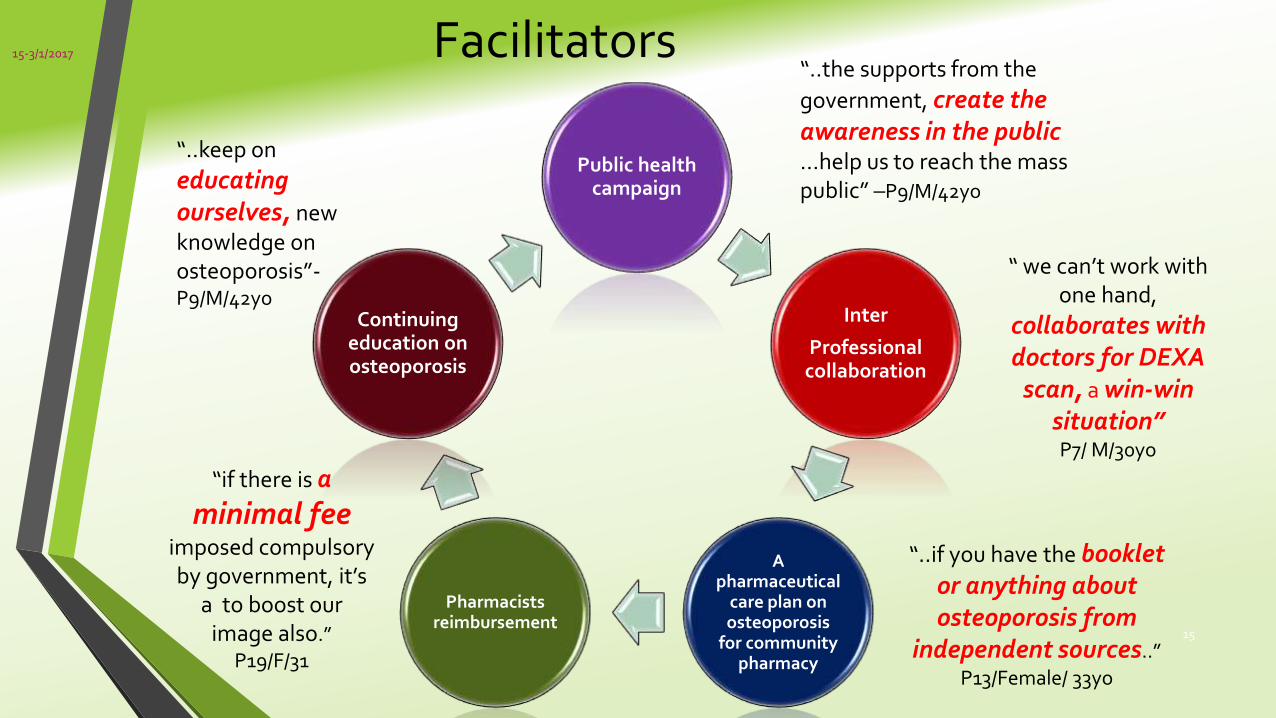
Facilitators
Public health campaign
Inter
Professional collaboration
A pharmaceutical
care plan on osteoporosis
for community pharmacy
Pharmacists reimbursement
Continuing education on osteoporosis
“..keep on
educating ourselves, new knowledge on osteoporosis”-P9/M/42yo
“ we can’t work with one hand,
collaborates with doctors for DEXA
scan, a win-win situation”P7/ M/30yo
“if there is a
minimal feeimposed compulsory by government, it’s
a to boost our image also.”
P19/F/31
“..if you have the booklet or anything about osteoporosis from
independent sources..”
P13/Female/ 33yo
“..the supports from the
government, create the awareness in the public…help us to reach the mass public” –P9/M/42yo
15
15-3/1/2017
Discussion• Findings show that Malaysian community pharmacists’ involvement in the
provision of pharmaceutical care for osteoporosis is minimal.
• Little demand for osteoporosis services from the public
• Deeply rooted in the traditional role of medication dispensing
• Only opportunistic counselling on osteoporosis prevention
( such as risk factors and lifestyle modification) were practiced
• Pharmacists associated clients’ lack of awareness with inadequate public health campaigns. This is surprising when raising public awareness is indeed a role for pharmacists, which may be achieved using posters and health promotion initiatives in-store, and public health messages via the media. 16
16- 3/1/2017
• Previous studies have shown that osteoporosis screening by community pharmacist was well accepted by the public and other health care partners6
• However, osteoporosis screening tools (e.g. heel ultrasound) or stratification algorithm (e.g. fracture risk assessment tool, FRAXTM ) must be based on device-specific cut-offs that are validated in the populations for which they are intended to be used7
• The Osteoporosis Self-Assessment Tool for Asians (OSTA) is a simple and cost-effective risk-screening tool that has been validated for use in the Asian populations8
• Similar to published studies9,10, the adoption of pharmaceutical care elsewhere has been challenged by lack of knowledge, time and incentives, and limited inter-professional collaboration
6. Goode JV, et.al. JAPhA. 2004;44(2):152-60. 7. Thomsen K, et.al. 2015. Osteoporos International 2015.8. Chaiyakunapruk N, et.al.2006.JAPhA. 2006;46(3):391-6.9. Laliberte MC, et.al. 2012. BMC public health.12(1471-2458)10. Wibowo Y, et.al.2010. Rural Remote Health.10(3):1400
17
17-3/1/2017
Limitations
• Small sample of participants may not be generalizable to all community pharmacists, especially those from rural areas
• Commercially-sensitive issues could not be explored in this study, and this is suggested for later research in developing osteoporosis services or proposing a structure for remuneration.
• Participants may have given a socially desirable response to some questions to impress the university-based research team.
18
18- 3/1/2017
Conclusion
• The majority of identified barriers are similar to those reported from other studies of pharmaceutical care implementation
• Although pharmaceutical care services for osteoporosis are underdeveloped in Malaysia, this study suggests general support amongst community pharmacists to meet the needs of the aging Asian population.
• Careful planning, incorporating client needs analysis, and involvement of pharmacy professional bodies and doctors, is indicated in the further development of osteoporosis care services in Malaysian pharmacies.
19
19- 3/1/2017

Acknowledgements
•University of Malaya Postgraduate Research Grant, UMPRG (grant no: PG010-2014A)
• Participants
20
20-3/1/2017
Recommended