Letters to the Editor
Benign panretinal uniform radiallinear-shaped flecks
Our case illustrates a new presentation of benign retina flecks withline-shaped and panretinal, uniform and radial distribution. Com-pared with previous reports of fleck retina disorders, our case doesnot show increased autofluorescence deposits, no delay in darkadaptation, neither significant macular nor nasal disc involvement.1–5
A 51-year-old woman with consanguinous parents was referredfor evaluation of bilateral retinal lesions. On examination, best-corrected visual acuity was 6/7.5 with moderate hyperopic correc-
tion in both eyes. Visual fields were normal. The anterior segmentswere unremarkable.
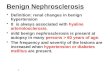
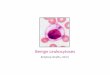
Fundus examination revealed multiple yellow-creamy discreteround and mostly linear-shaped flecks scattered throughout theretina in both eyes with relative sparing of the fovea. The flecksdistributed in a radial pattern centred around the posterior pole(Fig. 1) and were located well posterior to the retinal vasculature.The discs, maculae and retinal vessels appeared unremarkable.Fundus autofluorescence imaging (cSLO, Heidelberg Retina Angio-graph 2; Heidelberg Engineering, Dossenheim, Germany) did notshow hyper- or hypo-fluorescent flecks (Fig. 2a), but multiple dis-crete round lesions above the retinal pigment epithelium wereapparent in the infrared imaging (Fig. 2b). Corresponding spectral
Financial Disclosure: SHT is a fellow of the Burroughs-Wellcome Program in Biomedical Sciences and has been supported by the Bernard Becker-Association
of University Professors in Ophthalmology-Research to Prevent Blindness Award and Foundation Fighting Blindness. Columbia Retinal Phenomics Program is
supported by Dennis W. Jahnigen Award of the American Geriatrics Society, Joel Hoffman Fund, Gale and Richard Siegel Stem Cell Fund, Charles Culpeper
Scholarship, Schneeweiss Stem Cell Fund, Irma T. Hirschl Charitable Trust, and Bernard and Anne Spitzer Stem Cell Fund, Barbara & Donald Jonas Family Fund,
Eye Surgery Fund, and EY018213.
a bFigure 1. A wide-angle montageof the right (a) and left (b) fundidemonstrates multiple yellow-creamdiscrete flecks widely distributed inthe equator and far periphery of theretina. A few flecks are centred inthe posterior pole.
a bFigure 2. (a) Fundus autofluores-cence of the right eye showingabsence of hyper- or hypo-fluorescent flecks; (b) infraredimaging of the right eye showingmultiple discrete round lesions inthe para-foveal area.
Clinical and Experimental Ophthalmology 2008; 36: 891–900doi: 10.1111/j.1442-9071.2009.01906.x
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists

a
c d
b
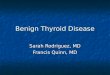
Figure 3. Spectral-domain OCT of the right eye (Optivue). (a) Multiple flecks in the posterior pole (yellow and green arrows represent OCTscans on (b) and (c), respectively, and white square represents longitudinal SLO scan on (d); (b) normal appearing macula; (c) retinal scan nearthe superior temporal vascular arcade showing that flecks are localized across the layers of the RPE complex and photoreceptors inner–outersegment junction, without involving the choroid (arrowheads pointing flecks and open arrowheads pointing shadows from vessels); (d)longitudinal SLO scan from the macula showing multiple flecks at the level of RPE. IS/OS, inner segment/outer segment; OCT, opticalcoherence tomography; ONL, outer nuclear layer; RPE, retinal pigment epithelium; SLO, scanning laser ophthalmoscopy.
a
c d
b
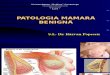
Figure 4. Spectral-domain OCT of the right eye (Cirrus Zeiss). (a) Multiple flecks in the posterior pole (yellow and green arrows representOCT scans on (b) and (c), respectively, and white square represents longitudinal scan on (d); (b) normal appearing macula; (c) retinal scan nearthe superior temporal vascular arcade showing that flecks are localized across the layers of the RPE complex and photoreceptors inner–outersegment junction, without involving the choroid (arrowheads pointing flecks and group of flecks and open arrowheads pointing shadows fromvessels); (d) longitudinal scan from the macula showing a granular aspect on RPE surface. ILM, internal limiting membrane; IS/OS, innersegment/outer segment; OCT, optical coherence tomography; ONL, outer nuclear layer; RPE, retinal pigment epithelium.
892 Letters to the Editor
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists

optical coherence tomography (Optivue SD-OCT, Fremont, CA,and Cirrus, Carl Zeiss Meditec Inc., Dublin, CA, USA) revealedthat these lesions span across the retinal pigment epitheliumcomplex and photoreceptor inner–outer segment junction layers,without involving the choroid (Figs 3,4). To assess retinal function,ISCEV (International Society for Clinical Electrophysiology ofVision) standardized full-field electroretinography were performedfollowing 20 min and overnight dark adaptation. The electroretin-ography traces showed that both scotopic and photopic responseswere symmetric and within normal limits (Fig. 5).
In contrast to previous reports,1–3 the retinal lesions in ourpatient appeared to be significantly smaller, more of a linearshape(s) and uniform in size(s). These lesions were distributed ubiq-uitously in the equator and mid and far periphery of the fundus. Thecentrally located flecks in the posterior pole appeared sparse, small,
round and dot-like. Unfortunately, the patient’s family memberswere not available for eye examination. In contrast to the classicfindings reported by Audo et al.,4 where the retinal flecks demon-strated increased autofluorescence, the fundus imaging of ourpatient did not show any specks of abnormal autofluorescence.Infrared imaging (Fig. 2b) and optical coherence tomography(Figs 3,4) revealed numerous subretinal dot-like lesions, which cor-respond to those observed in funduscopy.
Different types of flecked retinal disorders such as dominantradial drusen, fleck retina of Kandori,1 fundus albipunctatus, retini-tis punctata albescens, fundus flavimaculatus and vitamin A defi-ciency5 may be considered as differential diagnosis. However, thelack of drusen on the nasal side of the optic disc, extension offlecks to peripheral retina, absence of high-density autofluorescentdeposits on scanning laser ophthalmoscopy imaging and presence
Figure 5. Representative photopic and scotopic electroretinogram recordings compared with normal control after 20 min in the right eyeand overnight dark adaptation in the left eye. Full-field electroretinographies were performed with Ganzfeld stimulation on this patient andrevealed normal scotopic and photopic responses.
Letters to the Editor 893
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists

of intact EFEMP1 gene sequence made the diagnosis of dominantradial drusen unlikely. Moreover, normal scotopic electroretinogra-phy response excludes fundus albipunctatus. In addition to clinicalassessment, electrophysiology testing was essential to excludefundus albipunctatus and autofluorescent imaging can be a helpfultool to characterize hyper-autofluorescent deposits observed in dif-ferent variants of benign fleck retina. The normal electrophysiologyand visual field testing, in addition to good visual acuity and lack ofsymptoms justify the condition as benign. Hence, our case representsa different presentation of benign fleck retina,4 with linear-shapedflecks and a panretinal, uniform and radial distribution.
Suzanna Airiani MD,* Wener Cella MD,* Chai Lin ChouMSc, Joaquin Tosi MD and Stephen H Tsang MD PhD
Bernard & Shirlee Brown Glaucoma Laboratory and Edward S.Harkness Eye Institute, College of Physicians and Surgeons,
Columbia University, New York, NY, USAReceived 10 December 2007; accepted 11 November 2008.
REFERENCES
1. Aish SF, Dajani B. Benign familial fleck retina. Br J Ophthalmol1980; 64: 652–9.
2. Isaacs TW, McAllister IL, Wade MS. Benign fleck retina. Br JOphtalmol 1996; 80: 267–8.
3. Dorairaj SK, Murthy KP, Ritch R. Four-generation familialbenign fleck retina. Retin Cases Brief Rep 2007; 1: 25–6.
4. Audo I, Tsang SH, Fu AD, Barnes J, Holder GE, Moore AT.Autofluorescence imaging in a case of benign familial fleckretina. Arch Ophthalmol 2007; 125: 714–15.
5. Elison JR, Friedman AH, Brodie SE. Acquired subretinal fleckssecondary to hypovitaminosis A in a patient with hepatitis C.Doc Ophthalmol 2004; 109: 279–81.
Acute retinal necrosis followingsteroid treatment for unrecognizedRamsay–Hunt syndrome
Acute retinal necrosis (ARN) is a rare viral infection predominantlycaused by varicella zoster and herpes simplex virus type 1 and 2.1
We report a case where ARN developed following steroid mono-therapy initiated for treatment of (unrecognized) Ramsay–Huntsyndrome.
An 81-year-old man presented to the otorhinolaryngologydepartment with sudden onset of complete, left-sided, peripheralseventh nerve palsy, hearing loss and ear pain. He was diagnosedwith a lower motor neuron seventh nerve palsy of unknown cause.Ear vesicles were seen; however, the diagnosis by the otorhino-laryngolist was felt to be uncertain, and he commenced treatmentwith high-dose oral prednisolone (1 mg/kg). No antiviral cover wasstarted. Two weeks later he was referred to the ophthalmologyservice for management of exposure keratopathy.
A temporary tarsorrhaphy was performed, but 9 days later theleft visual acuity decreased to count fingers with a relative afferentpupillary defect. Anterior chamber cells and dense vitritis werepresent, with multifocal areas of patchy peripheral retinal necrosis.
A diagnosis of ARN was made and an anterior chamber tap per-formed, which confirmed varicella zoster as the underlying cause.
The patient was started on intravenous acyclovir improvement,with documented reduction in amount of cellular activity and nofurther progression of the necrotic areas of retina. After 10 days heconverted to oral acyclovir. Oral prednisone was re-started after48 h. Five weeks later the inflammation had reduced but the fundalview was obscured by vitreous debris that reduced vision to handmotions and precluded laser retinopexy. A vitrectomy was per-formed with barrier laser and silicone oil tamponade.
At the 10-day postoperative appointment, a one-millimetrehypopyon was observed. Pseudomonas Aeruginosa was cultured fromthe vitreous aspirate. Despite an intensive antibiotic regime thepatient’s ocular condition deteriorated. A superior corneoscleralmelt developed and progressed to perforation necessitating anevisceration.
Six months later the right eye remains unaffected and he is stillreceiving oral acyclovir prophylaxis.
This patient demonstrates an unusual presentation of ARN,occurring after acute facial nerve palsy. The ear vesicles docu-mented on examination lead us to believe that he had Ramsay–Hunt syndrome, a form of varicella zoster infection involvingcranial nerve VII and, less frequently, V, VI, VIII, IX and X, ratherthan idiopathic facial nerve palsy (Bell’s palsy).2 Bell’s palsy is alsothought to have a viral cause in many cases, with increasing evi-dence for a role of herpes simplex virus in pathogenesis.3
A review of the literature reveals three other reports of ARNfollowing Ramsay–Hunt syndrome. One HIV-positive patient devel-oped bilateral sequential ARN with the first eye being involved at thesame time as the onset of facial nerve palsy.2 Two other cases havebeen reported in HIV-negative individuals.1,4
It can be difficult to differentiate between Bell’s palsy andRamsay–Hunt syndrome, especially in the absence of skin lesions,and careful examination for vesicles within the ear should be part ofany facial nerve evaluation. Although we cannot assume that anti-viral treatment would have prevented the development of ocularinvolvement in our patient, it may potentially have resulted in moresevere disease by lowering the host defences, as immunosuppres-sion is known to increase susceptibility to ARN.1 Temporal associa-tion between herpes zoster dermatitis and development of ARN insome reported cases suggests that haematogenous spread of virus toeye can occur, so it is plausible that early antiviral treatment mayhave reduced viraemia and risk of eye involvement.
Recent studies would support a role for antiviral therapy in themanagement of Bell’s palsy. A prospective, randomized multicentrestudy of 221 patients found that valacyclovir and prednisolonetherapy was more effective than conventional prednisolonetherapy.3 Antiviral treatment is recommended in all patients withherpes zoster, although there are no large-scale randomized controltrials in Ramsay–Hunt syndrome.5
This case presented here illustrates that there may be a risk ofprecipitating ARN when diagnosing and treating an acute lowermotor neuron facial palsy with steroids, as the majority of cases arecaused by herpes viruses.
Joanne L Sims FRANZCO andEhud Zamir MD FRANZCO
Ocular Immunology Service, Royal Victorian Eye and Ear Hospital,Melbourne, Australia
Received 7 July 2008; accepted 5 December 2008
*These authors contributed equally to this report.
894 Letters to the Editor
© 2009 The AuthorsJournal compilation © 2009 Royal Australian and New Zealand College of Ophthalmologists
Recommended