Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Calcium channel blockersCalcium channel blockers
Professor Ian Whyte
Hunter Area Toxicology Service
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Cardiac arrhythmia Cardiac arrhythmia
Primary – quinidine–like drugs, sympathomimetic
drugs, calcium channel blockers, β–blockers, digitalis, chloroquine
Secondary to metabolic/electrolyte abnormalities – salicylates, methanol, ethylene glycol
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Cardiotoxic drugs Cardiotoxic drugs
All patients should have– oxygenation and protection of airway– decontamination of the GIT
atropine pre–medication
– correction of electrolyte abnormalities acid base balance
– cardioversion when appropriate – consultation
PIC 131126
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Cardiac arrest Cardiac arrest
Successful resuscitation has been well documented after 8 hours of CPR
Overdose patients usually have– a reversible cause for their arrest– good general health– novel treatments for arrhythmias– cerebral protection
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Calcium channel blockersCalcium channel blockers
Block calcium channels (L-type) in heart and blood vessels– prolong depolarisation
↑QRS width
– block SA and AV node conduction heart block asystole
– vasodilators– cerebral protection
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Calcium channel blockersCalcium channel blockers
Hypotension– peripheral vasodilatation and myocardial
depression Bradycardia
– AV and SA node block
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case 18 yo female admitted 3 hours after self–
poisoning with– 3.5 g of slow release verapamil (Isoptin SR)– 6 g of paracetamol – 4.5 g of tetracycline– 1 g of pseudoephedrine
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case On arrival in ED
– PR 120, BP 110/80, RR 20, afebrile– drowsy but oriented and cooperative
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
GI decontamination– emesis before arrival– lavaged with return of green tablets– 50 g of charcoal with sorbitol repeated 4 h later
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Investigations– ECG
sinus tachycardia with normal QRS width
– serum paracetamol at 4 h was 38 µmol/l hepatotoxicity > 1300 µmol/l at 4 hours
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
16 hours post overdose– BP fell to 70/40 and then 50/30– PR 50– oxygen saturation dropped to 75 %
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
16 hours post overdose– ECG
absent p waves prominent u waves normal QRS duration and QT interval
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Treatment– IV atropine 0.6 mgs – no response
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Treatment– IV calcium gluconate
6 g over 20 minutes further 6 g over the next hour
– pr 60, sinus rhythm, BP 100/80
– oxygen saturation > 95 %
– infusion of 10% calcium gluconate at 2 G/h for 10 hours
– she was also given 2.5 L IV fluids
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
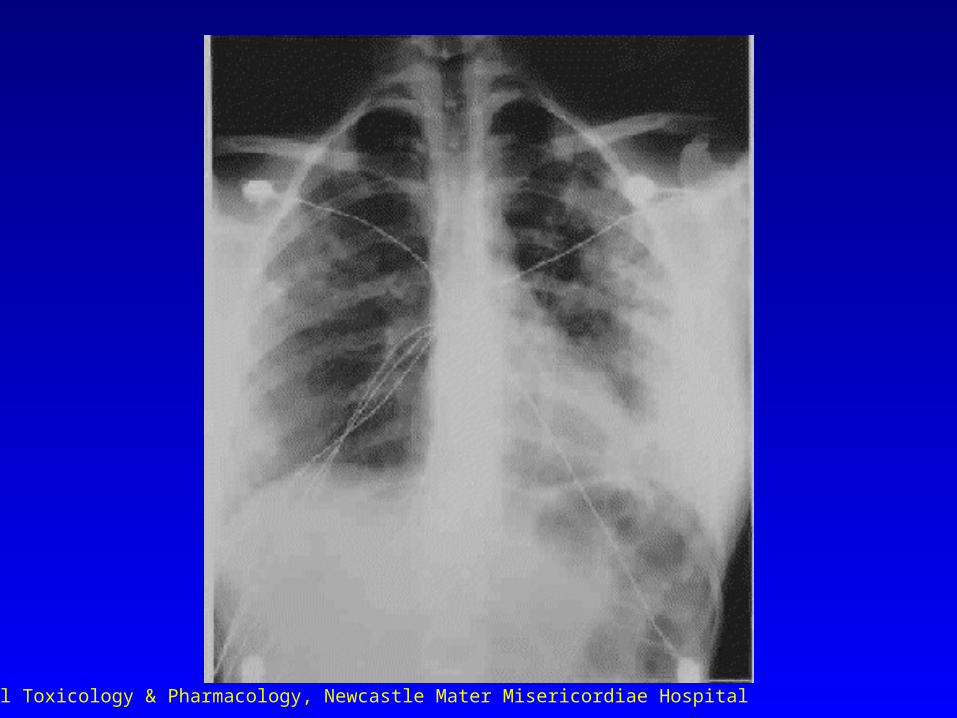
Outcome– non–cardiogenic pulmonary oedema– twenty four hours post admission
largely recovered , sinus rhythm PR 60, BP 115/70
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Outcome– peak serum Ca was 4.8 (2.18–2.47
mmol/l)– serial verapamil levels at 6, 18, 22 and 46
hours were 616, 2374, 2518 and 1006 ng/ml
range during usual therapy– 100–300 ng/ml
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
A thirty one-year-old female is brought to the Emergency Department by relatives
She states that she ingested 25 x 240 mg sustained-release diltiazem tablets approximately one hour earlier as a suicide attempt

Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
The tablets do not belong to her and she has no significant intercurrent illnesses
She appears upset but otherwise well Her pulse is 70/minute, her blood
pressure 125/70 mmHg and her ECG shows normal sinus rhythm
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Outline your initial management
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Despite the relatively benign presentation, this is a life-threatening overdose
Aggressive gastrointestinal decontamination using whole bowel irrigation before clinical effects of poisoning develop
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Give oral polyethylene glycol solution (GoLYTELY) at a rate of 15–20 mL/kg/h
Few patients can drink it this fast so it is best to place a nasogastric tube (premedicate with atropine!)
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Then sit the patient on a commode chair and continue until the rectal effluent looks like the GoLYTELY solution
This may take several hours
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Institute appropriate monitoring This includes establishing IV access,
continuous ECG monitoring and frequent non-invasive blood pressure monitoring
This patient will need a minimum of 16 hours monitoring even if she remains completely asymptomatic
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Admission should be to a monitored bed and personnel should be available who are capable of placing an arterial line, transvenous pacemaker and Swan-Ganz catheter
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Some six hours later, the patient is noted to be drowsy with a pulse rate of 45/minute (first degree heart block) and blood pressure of 80/40 mmHg
How do you respond now?
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB caseCCB case
Despite the excellent decontamination, sufficient drug has been absorbed to result in a toxic syndrome
There is no way of knowing at present how severe it is going to be
Best to assume the worst Management at this point includes
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB treatmentCCB treatment
Normal saline bolus (10–20 mL/kg) Calcium
– 5–10 mL of 10% calcium chloride or 10–20 mL of 10% calcium gluconate over 5 minutes
– repeat every 3–5 minutes up to 3 to 5 doses– if response institute calcium infusion of 1–10 mL/h
of 10% calcium chloride– monitor serum calcium after 30 mL of calcium
chloride or equivalent

Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB treatmentCCB treatment
Glucagon 0.05 mg/kg IV– repeat every 5–10 minutes as needed– if response consider infusion of 0.075–
0.15 mg/kg/h Atropine, isoprenaline and/or pacing
may be tried if associated symptomatic bradycardia
Dopamine infusion if still persistent hypotension
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
CCB treatmentCCB treatment
If no response to the above consider– insulin bolus 1 unit/kg with glucose 25
mL of 50% dextrose IV followed by – insulin infusion of 0.5 units/kg/hr with
50% dextrose infusion at 0.5 g/hr adjusted according to hourly glucose checks
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
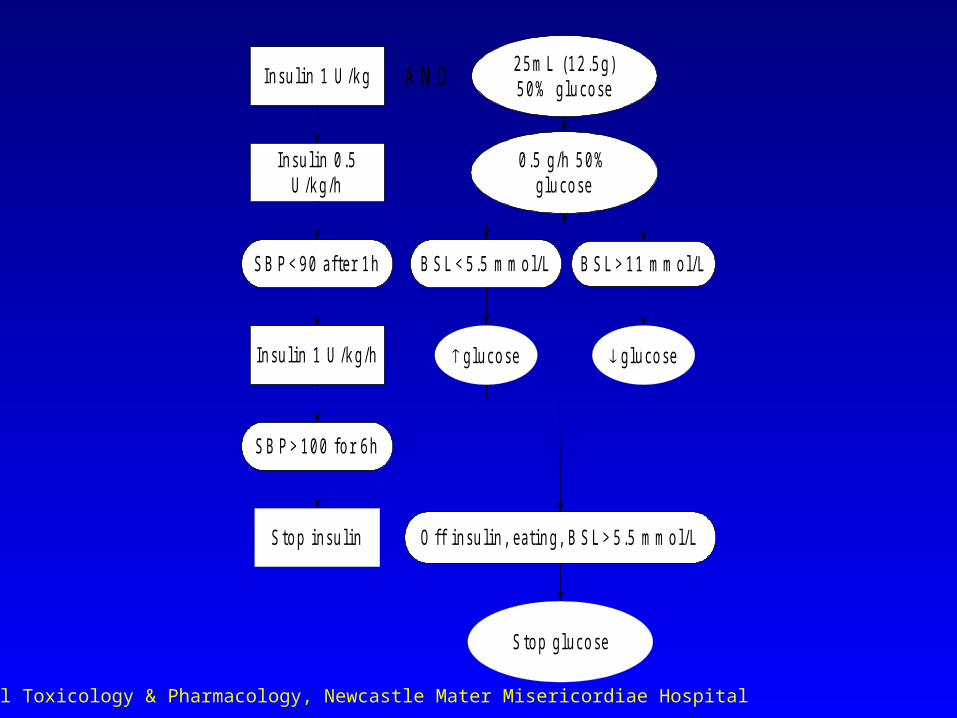
In su l in 1 U /k g
In su l in 0 .5U /k g/h
S B P < 9 0 a fte r 1 h
0 .5 g/h 5 0 %glu co se
2 5 m L (1 2 .5 g)5 0 % glu co se
In su l in 1 U /k g/h
S to p in su lin
S B P > 1 0 0 fo r 6 h
B S L > 1 1 m m o l/LB S L < 5 .5 m m o l/L
O ff in su l in , ea t in g , B S L > 5 .5 m m o l/L
glu co se glu co se
S to p glu co se
A N D
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Cardiopulmonary bypassCardiopulmonary bypass
As a last resort extracorporeal blood pressure support eg cardiopulmonary bypass may be considered
Clinical Toxicology & Pharmacology, Newcastle Mater Misericordiae Hospital
Antidotes: asystole & Antidotes: asystole & bradycardiabradycardia
Atropine everything Bicarbonate tricyclic antidepressants Calcium calcium channel blockers Diazepam chloroquine, organochlorines Epinephrine everything, β–blockers Fab fragments digoxin Glucagon β–blockers, CCBs
Recommended