Hindawi Publishing CorporationCase Reports in UrologyVolume 2013 Article ID 765704 3 pageshttpdxdoiorg1011552013765704
Case ReportIntraperitoneal Urinary Bladder Perforation Observed in aPatient with an Indwelling Urethral Catheter
Soichiro Ogawa Tomonori Date and Osamu Muraki
Department of Urology Fujita General Hospital Kunimi-Town Fukushima 969-1793 Japan
Correspondence should be addressed to Soichiro Ogawa sohfujita-hpjp
Received 28 June 2013 Accepted 4 August 2013
Academic Editors F Ramezanzadeh and F M Solivetti
Copyright copy 2013 Soichiro Ogawa et alThis is an open access article distributed under the Creative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
This report describes a rare case of an 86-year-old man with an indwelling urethral catheter who developed severe abdominal painand was diagnosed with intraperitoneal urinary bladder perforation A home-visiting nurse suspected catheter obstruction andperformed a catheter exchange However bladder irrigation could not subsequently be performed Computed tomography of theabdomen and pelvis after transurethral perfusion of contrast medium demonstrated extravasation of the contrast material into theperitoneal cavity Furthermore the Foley catheter balloon was positioned in the peritoneal cavity through the bladder The patientwas diagnosed with peritonitis due to spontaneous intraperitoneal perforation of the urinary bladder and exploratory laparotomywas performed During exploration a perforated tear at the top of the bladder was discovered where the Foley catheter hadpenetrated the bladder The Foley catheter balloon was floating freely in the peritoneal cavity There was no evidence of pathologiclesions such as cancer or inflammatory mass at the site of the injured peritoneum Successful closure of the damaged peritoneumand bladder was performed Since the proportion of elderly individuals continues to increase in the general Japanese populationthe incidence of the chronic Foley catheterization is expected to increase Therefore clinicians should be aware of this potentialcomplication
1 Introduction
Bladder perforation associated with indwelling urethralcatheter is rare and can be life threatening [1] and long-term use of the urethral catheter can weaken the bladderwall This report describes a rare case of an 86-year-old manwith an indwelling urethral catheter who developed severeabdominal pain and was diagnosed with intraperitonealurinary bladder perforation
2 Case Report
An 86-year-old man was admitted to our hospital withsudden onset of abdominal pain that had persisted for a fewhours He had a past history of two abdominal surgeries at 21years and 4 years earlier for appendectomy and reduction ofbowel torsion respectively He also had a history of cerebralinfarction that occurred more than 20 years prior two brainsurgeries for subdural hematoma removal and neurogenic
bladder that had been managed for more than 4 months witha chronic indwelling urethral catheter
His urethral catheter was exchanged for a new one by ahome-visiting nurse After two days he felt acutely ill withvomiting and a decrease in urine volume A home-visitingnurse suspected catheter obstruction and exchanged theurethral catheter for a new one However bladder irrigationcould not subsequently be performed At the time of hisarrival to our hospital he was conscious and alert witha pulse of 90 bpm a blood pressure of 6925mmHg arespiratory rate of 24min and a temperature of 361∘C Phys-ical examination showed diffuse tenderness coupled withmuscle guarding and rebound pain in the lower abdomenA 16-Fr Foley catheter had been placed Cloudy urine wasobserved in his urinary drainage bag When irrigation wasattempted there was no return Laboratory testing revealedhemoglobin of 138 gdL hematocrit of 401 leukocytecount of 7300mm3 platelet count of 517000mm3 sodiumof 122mEqL potassium of 47mEqL and normal renal
2 Case Reports in Urology
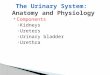
Figure 1 Computed tomography image showing thickening of theurinary bladder wall
Figure 2 Contrast-enhanced computed tomography aftertransurethral perfusion of contrast medium demonstratedextravasation of the contrast material into the peritoneal cavity (998771)In addition the Foley catheter balloon (arrowhead) was locatedwithin the peritoneal cavity through the urinary bladder
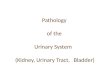
function A contrast-enhanced computed tomography (CT)scan of his abdomen and pelvis after transurethral perfusionof contrast medium showed extravasation of the contrastmaterial into the peritoneal cavity Further the Foley catheterballoon was placed in peritoneal cavity through the urinarybladder (Figures 1 2 and 3) Intraperitoneal free air wasalso observed Based on these CT findings a diagnosis ofperitonitis due to spontaneous intraperitoneal perforation ofthe urinary bladder was made However we could not ruleout bowel perforation at that time Therefore we performedexploratory laparotomy A penicillin-based antibiotic (ampi-cillinsulbactam) was administered
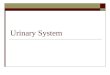
During exploration the peritoneal cavity was found to befilled with a medium amount of opacified fluid A perforatedtear of about 6mm was discovered at the dome of theurinary bladder where the Foley catheter was penetrating thebladder The Foley catheter balloon was floating freely in theperitoneal cavity (Figure 4) The intestines were dilated butno other intraperitoneal injuries were found to explain thefree air There was no evidence of pathologic lesions suchas cancer or inflammatory mass at the site of the injuredperitoneum We concluded that the intraperitoneal air musthave entered through the tear in the urinary bladder Thedamaged portion of the urinary bladder was intraperitoneallyrepaired in a standard two-layer fashion using absorbablesutures (3-0 Polysorb Covidien MA USA) The perfo-rated peritoneum was also closed using 3-0 Polysorb in an
Figure 3 Free intraperitoneal air is identified (arrowhead)
Peritoneal cavity
Figure 4 A perforated tear of about 6mm was discovered at thedome of the urinary bladder (998771) where the Foley catheter waspenetrating The Foley catheter balloon was floating freely in theperitoneal cavity
interrupting suture technique An extraperitoneal suprapubiccystostomy catheter was placed in addition to a urethralcatheter Successful closure was confirmed by the absence ofleakage when filling the bladder to capacityThe surgical fieldwas abundantly washed with saline solution Drainage tubeswere placed in the vesicorectal and Morisonrsquos pouch
Postoperatively the cystostomy drainage catheter wasremoved The patientrsquos recovery was complicated by septicshock decubitus ulcer limb necrosis and pneumonia result-ing in prolonged hospitalization A trial of discontinuation ofthe urethral catheter was unsuccessful The patient was dis-charged 97 days after admission with an indwelling urethralcatheter
3 Discussion
Complications associated with the indwelling urethral cath-eter include bladder stones urinary tract infection bleedingand iatrogenic hypospadias [2] Among these complicationsbladder perforation is rare but can be life threatening similarto other traumatic and iatrogenic injuries [1]
The patient in the present case had a history of cerebralinfarction that occurred more than 20 years earlier and wasgenerally confined to bed because of disuse syndrome Thushe required long-term urethral catheterization
Case Reports in Urology 3
Intraperitoneal perforation of the urinary bladder typ-ically manifests with abdominal pain with guarding dueto peritonitis [3] However a diagnosis of urinary bladderperforation is often difficult because the symptoms arenonspecific and vague [4] Sometimes a discrepancy betweenbladder irrigation and recovery of saline through the Foleycatheter can be suggestive of bladder perforation [3 5] Inthe patientrsquos case bladder irrigationwas unsuccessful leadingus to suspect bladder perforation Of note the patient haddeveloped severe abdominal pain reduction in urine outputand vomiting before a home-visiting nurse replaced theurethral catheter Therefore we suspect that bladder injurylikely occurred before exchange of the urethral catheterHowever the Foley catheter balloon was likely advancedthrough the perforation with exchange of the catheter
Urinary bladder perforation can occur spontaneously inthe setting of a weakened bladder wall Indeed radiationinjury bladder tumors urinary tract infections catheterobstruction and long-term catheterization can damage thebladder and decrease bladder compliance [6] Aging is alsoassociated with increased pressure within the bladder whichcan promote perforation Bladder perforation can also resultfrom trauma to the bladder wall [7] However in thiscase the patient did not experience any bladder trauma Inaddition during the operation there were no gross signsof tumors around the damaged peritoneum and bladderwall Since there was no definite causative factor for thebladder perforation in this case we believe that spontaneousperforation occurred
Bladder perforation was diagnosed by CT in this caseQuagliano et al stated that CT scan is the standard tool forevaluation of abdominal injuries [8] However other studiessuggest that retrograde cystogram is the best method todiagnose bladder injuries [9 10] Appropriately selecting CTscan or cystogram is important in proper diagnosis of bladderinjuries [1]
In general intraperitoneal urinary bladder rupturerequires immediate surgical treatment because it can leadto deadly peritonitis [3] which is less likely to heal withonly catheter drainage [11] Recent studies have describedlaparoscopic repair of intraperitoneal urinary bladder rup-ture Marchand et al stated that laparoscopic repair shouldbe performed only in a stable patient with an isolated bladderrupture or minimal other injuries [10] In the present casewe could not rule out perforation of the digestive tractIn addition the patientrsquos condition was poor Therefore weelected to perform open exploratory surgery
In conclusion this report described a rare case of spon-taneous bladder perforation Since the proportion of elderlyindividuals continues to increase in the general Japanesepopulation the incidence of the chronic Foley catheterizationis expected to increase Therefore clinicians should be awareof this potential complication as well as other indwellingurethral catheter-related complications
References
[1] O Limon E E Unluer F C Unay O Oyar and A SenerldquoAn unusual cause of death spontaneous urinary bladder
perforationrdquoThe American Journal of Emergency Medicine vol30 no 9 pp 3ndash5 2012
[2] I Y Kim S B Lee B K Choi et al ldquoBladder rupture inimmediate postrenal transplant period of uncertain causerdquoExperimental and Clinical Transplantation vol 10 no 2 pp180ndash182 2012
[3] A Tabaru M Endou Y Miura and M Otsuki ldquoGeneralizedperitonitis caused by spontaneous intraperitoneal rupture of theurinary bladderrdquo Internal Medicine vol 35 no 11 pp 880ndash8821996
[4] J G Galbraith J S Butler and G T McGreal ldquoOpioid toxicityas a cause of spontaneous urinary bladder rupturerdquo AmericanJournal of Emergency Medicine vol 29 no 2 pp 239e1ndash239e32011
[5] O A Raheem and Y B Jeong ldquoIntraperitoneally placed Foleycatheter via Verumontanum initially presenting as a bladderrupturerdquo Journal of Korean Medical Science vol 26 no 9 pp1241ndash1243 2011
[6] M A Saleem A M Mahmoud and B R Gopinath ldquoSpon-taneous urinary bladder rupture a rare differential for lowerabdominal pain in a female patientrdquo Singapore Medical Journalvol 50 no 12 pp e410ndashe411 2009
[7] B Kim and M Roberts ldquoLaparoscopic repair of traumaticintraperitoneal bladder rupture case report and review of theliteraturerdquo Canadian Urological Association Journal vol 6 no6 pp e270ndashe273 2012
[8] P V Quagliano S M Delair and A K Malhotra ldquoDiagnosis ofblunt bladder injury a prospective comparative study of com-puted tomography cystography and conventional retrogradecystographyrdquo Journal of Trauma vol 61 no 2 pp 410ndash4212006
[9] W J OrsquoBrien and F C Ryckman ldquoCatheter-induced urinarybladder rupture presenting with pneumoperitoneumrdquo Journalof Pediatric Surgery vol 29 no 10 pp 1397ndash1398 1994
[10] T D Marchand R H Cuadra and D J Ricchiuti ldquoLaparo-scopic repair of a traumatic bladder rupturerdquo Journal of theSociety of Laparoendscopic Surgeons vol 16 no 1 pp 155ndash1582012
[11] S Al-Aghbari A Al-Harthy M Ahmed A Al-Reesi K Al-Wahaibi and H Al-Qadhi ldquoLaparoscopic repair of traumaticIntraperitoneal bladder rupturerdquo SultanQaboosUniversityMed-ical Journal vol 11 no 4 pp 515ndash518 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Urology
Figure 1 Computed tomography image showing thickening of theurinary bladder wall
Figure 2 Contrast-enhanced computed tomography aftertransurethral perfusion of contrast medium demonstratedextravasation of the contrast material into the peritoneal cavity (998771)In addition the Foley catheter balloon (arrowhead) was locatedwithin the peritoneal cavity through the urinary bladder
function A contrast-enhanced computed tomography (CT)scan of his abdomen and pelvis after transurethral perfusionof contrast medium showed extravasation of the contrastmaterial into the peritoneal cavity Further the Foley catheterballoon was placed in peritoneal cavity through the urinarybladder (Figures 1 2 and 3) Intraperitoneal free air wasalso observed Based on these CT findings a diagnosis ofperitonitis due to spontaneous intraperitoneal perforation ofthe urinary bladder was made However we could not ruleout bowel perforation at that time Therefore we performedexploratory laparotomy A penicillin-based antibiotic (ampi-cillinsulbactam) was administered
During exploration the peritoneal cavity was found to befilled with a medium amount of opacified fluid A perforatedtear of about 6mm was discovered at the dome of theurinary bladder where the Foley catheter was penetrating thebladder The Foley catheter balloon was floating freely in theperitoneal cavity (Figure 4) The intestines were dilated butno other intraperitoneal injuries were found to explain thefree air There was no evidence of pathologic lesions suchas cancer or inflammatory mass at the site of the injuredperitoneum We concluded that the intraperitoneal air musthave entered through the tear in the urinary bladder Thedamaged portion of the urinary bladder was intraperitoneallyrepaired in a standard two-layer fashion using absorbablesutures (3-0 Polysorb Covidien MA USA) The perfo-rated peritoneum was also closed using 3-0 Polysorb in an
Figure 3 Free intraperitoneal air is identified (arrowhead)
Peritoneal cavity
Figure 4 A perforated tear of about 6mm was discovered at thedome of the urinary bladder (998771) where the Foley catheter waspenetrating The Foley catheter balloon was floating freely in theperitoneal cavity
interrupting suture technique An extraperitoneal suprapubiccystostomy catheter was placed in addition to a urethralcatheter Successful closure was confirmed by the absence ofleakage when filling the bladder to capacityThe surgical fieldwas abundantly washed with saline solution Drainage tubeswere placed in the vesicorectal and Morisonrsquos pouch
Postoperatively the cystostomy drainage catheter wasremoved The patientrsquos recovery was complicated by septicshock decubitus ulcer limb necrosis and pneumonia result-ing in prolonged hospitalization A trial of discontinuation ofthe urethral catheter was unsuccessful The patient was dis-charged 97 days after admission with an indwelling urethralcatheter
3 Discussion
Complications associated with the indwelling urethral cath-eter include bladder stones urinary tract infection bleedingand iatrogenic hypospadias [2] Among these complicationsbladder perforation is rare but can be life threatening similarto other traumatic and iatrogenic injuries [1]
The patient in the present case had a history of cerebralinfarction that occurred more than 20 years earlier and wasgenerally confined to bed because of disuse syndrome Thushe required long-term urethral catheterization
Case Reports in Urology 3
Intraperitoneal perforation of the urinary bladder typ-ically manifests with abdominal pain with guarding dueto peritonitis [3] However a diagnosis of urinary bladderperforation is often difficult because the symptoms arenonspecific and vague [4] Sometimes a discrepancy betweenbladder irrigation and recovery of saline through the Foleycatheter can be suggestive of bladder perforation [3 5] Inthe patientrsquos case bladder irrigationwas unsuccessful leadingus to suspect bladder perforation Of note the patient haddeveloped severe abdominal pain reduction in urine outputand vomiting before a home-visiting nurse replaced theurethral catheter Therefore we suspect that bladder injurylikely occurred before exchange of the urethral catheterHowever the Foley catheter balloon was likely advancedthrough the perforation with exchange of the catheter
Urinary bladder perforation can occur spontaneously inthe setting of a weakened bladder wall Indeed radiationinjury bladder tumors urinary tract infections catheterobstruction and long-term catheterization can damage thebladder and decrease bladder compliance [6] Aging is alsoassociated with increased pressure within the bladder whichcan promote perforation Bladder perforation can also resultfrom trauma to the bladder wall [7] However in thiscase the patient did not experience any bladder trauma Inaddition during the operation there were no gross signsof tumors around the damaged peritoneum and bladderwall Since there was no definite causative factor for thebladder perforation in this case we believe that spontaneousperforation occurred
Bladder perforation was diagnosed by CT in this caseQuagliano et al stated that CT scan is the standard tool forevaluation of abdominal injuries [8] However other studiessuggest that retrograde cystogram is the best method todiagnose bladder injuries [9 10] Appropriately selecting CTscan or cystogram is important in proper diagnosis of bladderinjuries [1]
In general intraperitoneal urinary bladder rupturerequires immediate surgical treatment because it can leadto deadly peritonitis [3] which is less likely to heal withonly catheter drainage [11] Recent studies have describedlaparoscopic repair of intraperitoneal urinary bladder rup-ture Marchand et al stated that laparoscopic repair shouldbe performed only in a stable patient with an isolated bladderrupture or minimal other injuries [10] In the present casewe could not rule out perforation of the digestive tractIn addition the patientrsquos condition was poor Therefore weelected to perform open exploratory surgery
In conclusion this report described a rare case of spon-taneous bladder perforation Since the proportion of elderlyindividuals continues to increase in the general Japanesepopulation the incidence of the chronic Foley catheterizationis expected to increase Therefore clinicians should be awareof this potential complication as well as other indwellingurethral catheter-related complications
References
[1] O Limon E E Unluer F C Unay O Oyar and A SenerldquoAn unusual cause of death spontaneous urinary bladder
perforationrdquoThe American Journal of Emergency Medicine vol30 no 9 pp 3ndash5 2012
[2] I Y Kim S B Lee B K Choi et al ldquoBladder rupture inimmediate postrenal transplant period of uncertain causerdquoExperimental and Clinical Transplantation vol 10 no 2 pp180ndash182 2012
[3] A Tabaru M Endou Y Miura and M Otsuki ldquoGeneralizedperitonitis caused by spontaneous intraperitoneal rupture of theurinary bladderrdquo Internal Medicine vol 35 no 11 pp 880ndash8821996
[4] J G Galbraith J S Butler and G T McGreal ldquoOpioid toxicityas a cause of spontaneous urinary bladder rupturerdquo AmericanJournal of Emergency Medicine vol 29 no 2 pp 239e1ndash239e32011
[5] O A Raheem and Y B Jeong ldquoIntraperitoneally placed Foleycatheter via Verumontanum initially presenting as a bladderrupturerdquo Journal of Korean Medical Science vol 26 no 9 pp1241ndash1243 2011
[6] M A Saleem A M Mahmoud and B R Gopinath ldquoSpon-taneous urinary bladder rupture a rare differential for lowerabdominal pain in a female patientrdquo Singapore Medical Journalvol 50 no 12 pp e410ndashe411 2009
[7] B Kim and M Roberts ldquoLaparoscopic repair of traumaticintraperitoneal bladder rupture case report and review of theliteraturerdquo Canadian Urological Association Journal vol 6 no6 pp e270ndashe273 2012
[8] P V Quagliano S M Delair and A K Malhotra ldquoDiagnosis ofblunt bladder injury a prospective comparative study of com-puted tomography cystography and conventional retrogradecystographyrdquo Journal of Trauma vol 61 no 2 pp 410ndash4212006
[9] W J OrsquoBrien and F C Ryckman ldquoCatheter-induced urinarybladder rupture presenting with pneumoperitoneumrdquo Journalof Pediatric Surgery vol 29 no 10 pp 1397ndash1398 1994
[10] T D Marchand R H Cuadra and D J Ricchiuti ldquoLaparo-scopic repair of a traumatic bladder rupturerdquo Journal of theSociety of Laparoendscopic Surgeons vol 16 no 1 pp 155ndash1582012
[11] S Al-Aghbari A Al-Harthy M Ahmed A Al-Reesi K Al-Wahaibi and H Al-Qadhi ldquoLaparoscopic repair of traumaticIntraperitoneal bladder rupturerdquo SultanQaboosUniversityMed-ical Journal vol 11 no 4 pp 515ndash518 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Urology 3
Intraperitoneal perforation of the urinary bladder typ-ically manifests with abdominal pain with guarding dueto peritonitis [3] However a diagnosis of urinary bladderperforation is often difficult because the symptoms arenonspecific and vague [4] Sometimes a discrepancy betweenbladder irrigation and recovery of saline through the Foleycatheter can be suggestive of bladder perforation [3 5] Inthe patientrsquos case bladder irrigationwas unsuccessful leadingus to suspect bladder perforation Of note the patient haddeveloped severe abdominal pain reduction in urine outputand vomiting before a home-visiting nurse replaced theurethral catheter Therefore we suspect that bladder injurylikely occurred before exchange of the urethral catheterHowever the Foley catheter balloon was likely advancedthrough the perforation with exchange of the catheter
Urinary bladder perforation can occur spontaneously inthe setting of a weakened bladder wall Indeed radiationinjury bladder tumors urinary tract infections catheterobstruction and long-term catheterization can damage thebladder and decrease bladder compliance [6] Aging is alsoassociated with increased pressure within the bladder whichcan promote perforation Bladder perforation can also resultfrom trauma to the bladder wall [7] However in thiscase the patient did not experience any bladder trauma Inaddition during the operation there were no gross signsof tumors around the damaged peritoneum and bladderwall Since there was no definite causative factor for thebladder perforation in this case we believe that spontaneousperforation occurred
Bladder perforation was diagnosed by CT in this caseQuagliano et al stated that CT scan is the standard tool forevaluation of abdominal injuries [8] However other studiessuggest that retrograde cystogram is the best method todiagnose bladder injuries [9 10] Appropriately selecting CTscan or cystogram is important in proper diagnosis of bladderinjuries [1]
In general intraperitoneal urinary bladder rupturerequires immediate surgical treatment because it can leadto deadly peritonitis [3] which is less likely to heal withonly catheter drainage [11] Recent studies have describedlaparoscopic repair of intraperitoneal urinary bladder rup-ture Marchand et al stated that laparoscopic repair shouldbe performed only in a stable patient with an isolated bladderrupture or minimal other injuries [10] In the present casewe could not rule out perforation of the digestive tractIn addition the patientrsquos condition was poor Therefore weelected to perform open exploratory surgery
In conclusion this report described a rare case of spon-taneous bladder perforation Since the proportion of elderlyindividuals continues to increase in the general Japanesepopulation the incidence of the chronic Foley catheterizationis expected to increase Therefore clinicians should be awareof this potential complication as well as other indwellingurethral catheter-related complications
References
[1] O Limon E E Unluer F C Unay O Oyar and A SenerldquoAn unusual cause of death spontaneous urinary bladder
perforationrdquoThe American Journal of Emergency Medicine vol30 no 9 pp 3ndash5 2012
[2] I Y Kim S B Lee B K Choi et al ldquoBladder rupture inimmediate postrenal transplant period of uncertain causerdquoExperimental and Clinical Transplantation vol 10 no 2 pp180ndash182 2012
[3] A Tabaru M Endou Y Miura and M Otsuki ldquoGeneralizedperitonitis caused by spontaneous intraperitoneal rupture of theurinary bladderrdquo Internal Medicine vol 35 no 11 pp 880ndash8821996
[4] J G Galbraith J S Butler and G T McGreal ldquoOpioid toxicityas a cause of spontaneous urinary bladder rupturerdquo AmericanJournal of Emergency Medicine vol 29 no 2 pp 239e1ndash239e32011
[5] O A Raheem and Y B Jeong ldquoIntraperitoneally placed Foleycatheter via Verumontanum initially presenting as a bladderrupturerdquo Journal of Korean Medical Science vol 26 no 9 pp1241ndash1243 2011
[6] M A Saleem A M Mahmoud and B R Gopinath ldquoSpon-taneous urinary bladder rupture a rare differential for lowerabdominal pain in a female patientrdquo Singapore Medical Journalvol 50 no 12 pp e410ndashe411 2009
[7] B Kim and M Roberts ldquoLaparoscopic repair of traumaticintraperitoneal bladder rupture case report and review of theliteraturerdquo Canadian Urological Association Journal vol 6 no6 pp e270ndashe273 2012
[8] P V Quagliano S M Delair and A K Malhotra ldquoDiagnosis ofblunt bladder injury a prospective comparative study of com-puted tomography cystography and conventional retrogradecystographyrdquo Journal of Trauma vol 61 no 2 pp 410ndash4212006
[9] W J OrsquoBrien and F C Ryckman ldquoCatheter-induced urinarybladder rupture presenting with pneumoperitoneumrdquo Journalof Pediatric Surgery vol 29 no 10 pp 1397ndash1398 1994
[10] T D Marchand R H Cuadra and D J Ricchiuti ldquoLaparo-scopic repair of a traumatic bladder rupturerdquo Journal of theSociety of Laparoendscopic Surgeons vol 16 no 1 pp 155ndash1582012
[11] S Al-Aghbari A Al-Harthy M Ahmed A Al-Reesi K Al-Wahaibi and H Al-Qadhi ldquoLaparoscopic repair of traumaticIntraperitoneal bladder rupturerdquo SultanQaboosUniversityMed-ical Journal vol 11 no 4 pp 515ndash518 2011
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Recommended