
Certain Cardiac Risk Factors Predict Risk FactorInterventions and Influence Communication Between
Physicians and PatientsSamia Mora, MD, Randall S. Stafford, MD, PhD, and Richard C. Pasternak, MD
The low rate of risk factor treatment suggests thatpreventive strategies are not being applied uni-
formly.1–7 Previous data from the 1991 to 1992 Na-tional Ambulatory Medical Care Surveys suggests thatpatterns of cholesterol management may be influencedby nonclinical patient characteristics.8 Identificationof patient characteristics that act as barriers to effec-tive risk factor management may aid in targeting spe-cific patient populations and facilitate the more wide-spread application of prevention measures. In thepresent study, we examined whether certain clinicalconditions can predict which patients get cardiovas-cular risk factor interventions, and we analyzed howphysicians and patients report these interventions in aneffort to understand better how they communicateabout prevention activities.
• • •The study design is a cross-sectional survey of 234
patients and their physicians in an academic cardiol-ogy practice. Three data sources were used to assesspatient experiences during the index visit: (1) reviewof the medical records, (2) a brief telephone interviewwith the patient, and (3) a questionnaire completed bythe physician immediately after the visit.
Outpatients receiving general cardiac care at anurban teaching hospital were systematically selectedfrom a computer-generated schedule over a 6-monthperiod. All patients scheduled for a cardiology fol-low-up or new patient visit were identified through theregistration database. Patients were excluded if theywere seen for a preprocedure or preoperative visit, orif their visit was less than a 3-month follow-up visit.Only 1 visit per patient was analyzed for a total of 234visits. Telephone interviews with patients were con-ducted 3 to 7 days after the office visit.
Twenty-eight physicians, equally divided into car-diology fellows and staff cardiologists, participated inthe study. Physicians were randomly selected for apostvisit questionnaire to be completed at the end oftheir visits. Half the visits had questionnaires andthese were used to assess the cardiac risk factor inter-ventions from the viewpoint of the physicians. Therandomization assessed whether completion of thequestionnaire would change physicians’ behavior dur-ing visits.
Standardized data about patients’ clinical condi-tions, cardiac risk factors, and risk factor interventionsduring visits were extracted from the medical recordnote for the index visit by a trained research assistant.The presence of the following risk factors was as-sessed from the medical record: hypercholesterolemia,diabetes mellitus, obesity, and systemic hypertension.For example, the patient was considered to have hy-percholesterolemia if the physician (either a cardiol-ogy fellow or staff cardiologist) had documented inthe problem list or written text of the index visit thatthe patient had hypercholesterolemia or its synonyms.Blood pressure and cholesterol testing were defined asany mention in the medical record of blood pressureand cholesterol levels measured during the index visit.Cholesterol counseling, dietary assessment, and di-etary counseling were considered to have occurred ifthe record contained any documentation of discussionregarding cholesterol, dietary assessment, or dietaryadvice given during the patient visit. The study wasapproved by the institutional review board of ourinstitution.
Risk factor assessment and intervention rates werecalculated from the medical records. Multiple logisticregression analysis was used to determine predictorsof risk factor services, while adjusting for the follow-ing potentially confounding variables: age, sex, andthe presence of other cardiac risk factors includinghypertension, hypercholesterolemia, diabetes, andobesity. All statistical analyses were performed usingSTATA, 1997.9
Selected patient characteristics are listed in Table1. The mean age of the study population was 66 years(range 27 to 91). Of the 234 patients, 145 (62%) weremen. As documented in the medical records, hyper-cholesterolemia and hypertension were more commoncardiac risk factors than diabetes or obesity. Althoughhalf the physicians were cardiology fellows, they only
From the Department of Medicine, Institute for Health Policy andGeneral Medicine Division, Preventive Cardiology, Cardiology Divi-sion, Massachusetts General Hospital and Harvard Medical School,Boston, Massachusetts. Dr. Pasternak’s address is: Preventive Cardiol-ogy, 852 GRB, Massachusetts General Hospital, 55 Fruit Street,Boston, Massachusetts 02114. E-mail: rpasternak@partners. org.Manuscript received December 20, 1999; revised manuscript re-ceived and accepted April 17, 2000.
TABLE 1 Selected Baseline Patient Characteristics
CharacteristicPatients
(n 5 234)
Age (yrs),50 28 (12%)50–59 37 (16%)60–69 70 (30%).69 98 (42%)
Men 145 (62%)Hypercholesterolemia 68 (29%)Diabetes mellitus 23 (10%)Obesity 16 (7%)Systemic hypertension 70 (30%)
783©2000 by Excerpta Medica, Inc. All rights reserved. 0002-9149/00/$–see front matterThe American Journal of Cardiology Vol. 86 October 1, 2000 PII S0002-9149(00)01082-1
saw a total of 33 patients (14%), whereas the staffcardiologists accounted for the other 201 patient visits(86%).
Risk factor management activities that were eval-uated in the multiple logistic regression model in-cluded blood pressure testing, cholesterol testing, cho-lesterol counseling, diet assessments, and diet coun-seling. Odds ratios (ORs) and their 95% confidenceintervals (CIs) (Table 2) represent the likelihood ofeach risk factor service occurring for patients whohave hypercholesterolemia, hypertension, diabetes, orobesity while controlling for the other potentially con-founding variables.
None of the patient characteristics was a significantpredictor of blood pressure testing. A history of hy-percholesterolemia, however, was a significant predic-tor of cholesterol and dietary services. The likelihoodof undergoing cholesterol testing or counseling inpatients with hypercholesterolemia was 12 timesgreater than in patients who did not have hypercho-lesterolemia (OR for cholesterol testing: 11.8, 95% CI
4.8 to 29.3, p,0.001; OR for cho-lesterol counseling: 12.2, 95% CI 5.2to 28.5, p,0.001).
The presence of hypertension wasa negative predictor for cholesteroland diet interventions. Specifically,diet counseling was reduced with astatistically significant OR of 0.4(95% CI 0.1 to 0.9, p5 0.036.) Incomparison, the presence of diabetesor obesity made dietary servicesmore likely, but not cholesterol test-ing or counseling. Obese patientswere considerably more likely to getdietary assessments (OR 12.4, 95%CI 2.5 to 61.6, p5 0.002) as well as
dietary counseling (OR 10.2, 95% CI 2.8 to 37.7, p,0.001). Similarly, patients with diabetes were 3times more likely to receive diet assessments (OR 2.9,95% CI 1.0 to 8.5, p5 0.045).
Age and gender were not significant predictors forany prevention service. The use of physician question-naires had no influence on risk factor assessment orintervention rates. In addition, there was no differencebetween staff cardiologists and cardiology fellows.
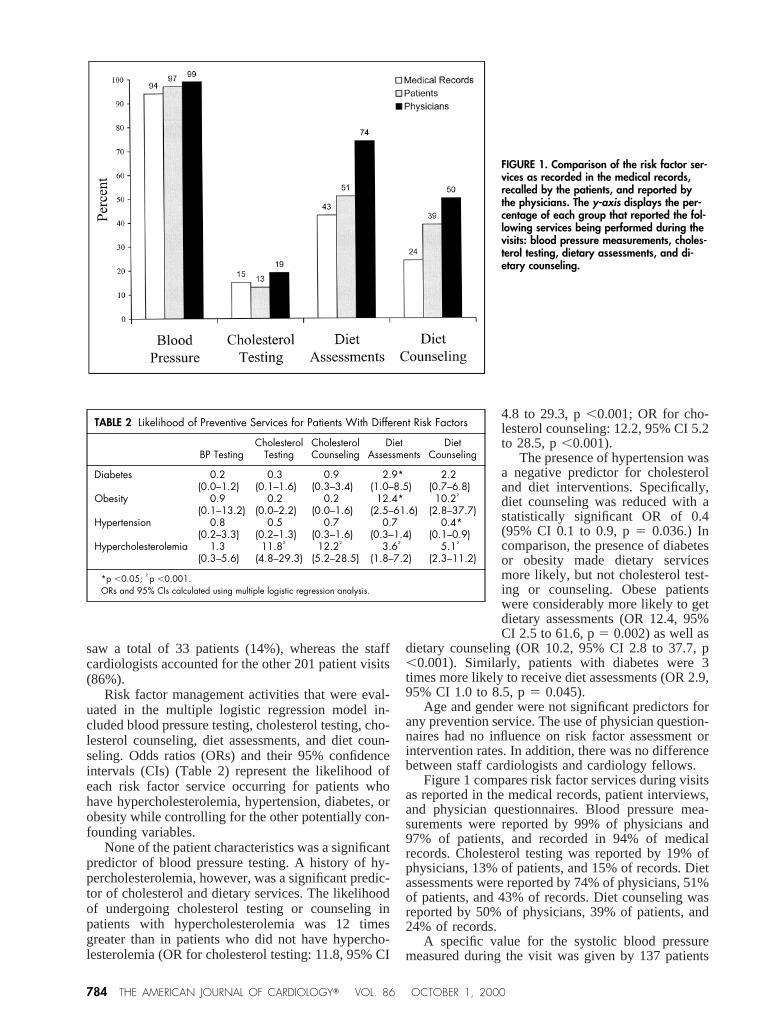
Figure 1 compares risk factor services during visitsas reported in the medical records, patient interviews,and physician questionnaires. Blood pressure mea-surements were reported by 99% of physicians and97% of patients, and recorded in 94% of medicalrecords. Cholesterol testing was reported by 19% ofphysicians, 13% of patients, and 15% of records. Dietassessments were reported by 74% of physicians, 51%of patients, and 43% of records. Diet counseling wasreported by 50% of physicians, 39% of patients, and24% of records.
A specific value for the systolic blood pressuremeasured during the visit was given by 137 patients
FIGURE 1. Comparison of the risk factor ser-vices as recorded in the medical records,recalled by the patients, and reported bythe physicians. The y-axis displays the per-centage of each group that reported the fol-lowing services being performed during thevisits: blood pressure measurements, choles-terol testing, dietary assessments, and di-etary counseling.
TABLE 2 Likelihood of Preventive Services for Patients With Different Risk Factors
BP TestingCholesterol
TestingCholesterolCounseling
DietAssessments
DietCounseling
Diabetes 0.2 0.3 0.9 2.9* 2.2(0.0–1.2) (0.1–1.6) (0.3–3.4) (1.0–8.5) (0.7–6.8)
Obesity 0.9 0.2 0.2 12.4* 10.2†
(0.1–13.2) (0.0–2.2) (0.0–1.6) (2.5–61.6) (2.8–37.7)Hypertension 0.8 0.5 0.7 0.7 0.4*
(0.2–3.3) (0.2–1.3) (0.3–1.6) (0.3–1.4) (0.1–0.9)Hypercholesterolemia 1.3 11.8† 12.2† 3.6† 5.1†
(0.3–5.6) (4.8–29.3) (5.2–28.5) (1.8–7.2) (2.3–11.2)
*p ,0.05; †p ,0.001.ORs and 95% CIs calculated using multiple logistic regression analysis.
784 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 86 OCTOBER 1, 2000

(59%) (correlation coefficient 0.96, p,0.001, meanabsolute difference 1.8, SD 4.6). Similarly, 126 pa-tients (54%) reported their diastolic blood pressure(correlation coefficient 0.91, p,0.001, mean absolutedifference 1.6, SD 3.7).
• • •In this study, we demonstrated that patients with
different cardiovascular risk factors are treated differ-ently with respect to risk factor assessments and ser-vices. The observed higher rate of dietary interven-tions in patients with high cholesterol is consistentwith national guidelines because diet is the preferredinitial approach to treating hypercholesterolemia.10
Dietary prevention services were more likely to occurnot only in patients with hypercholesterolemia, butalso in patients with diabetes and obesity. These prac-tice patterns suggest that physicians are appropriatelyusing dietary services as adjunctive management forpatients with these risk factors.
Several findings in our study were unexpected.First, we found that patients with hypertension re-ceived less dietary counseling and had a nonsignifi-cant trend toward less dietary assessments and choles-terol services. Second, we found a lack of associationbetween cholesterol services and the presence of therisk factors diabetes, hypertension, and obesity.
To determine whether these differences in riskmanagement activities reflected physician reportingbehavior, we analyzed the reporting of preventiveservices in the medical records compared with patientand physician reports. As expected, physiciansshowed a trend toward reporting more services com-pared with what they documented in the medicalrecords or what patients reported (Figure 1), a phe-nomenon that is consistent with previous studies.11–16
A 1996 British Cardiac Society study found that therecording of coronary risk factors in patients’ recordswas often incomplete and that it varied by risk fac-tor.17 Our findings confirm that patient-physician-medical record agreement was not consistent.
In conclusion, hypercholesterolemia was foundto be a strong predictor of dietary and cholesterolservices, whereas obesity and diabetes mellituswere predictors only of dietary services, and, sur-prisingly, hypertension appeared to be negativelyassociated with risk factor services. These resultssuggest that different risk factors influence com-munication as well as performance of preventive
services, and that physicians are underestimatingthe importance of treating multiple risk factorssimultaneously. To close the gap between physicianknowledge and patient treatment, our findings sug-gest that the delivery of preventive services may beimproved if physicians were more aware of thesynergistic nature of cardiovascular risk factors.
Acknowledgment: We wish to thank Theresa Bishopand Robin E. Chaput for their help with the adminis-trative and data collection aspects of this study.
1. National Cholesterol Education Program. Summary of the second report of theNational Cholesterol Education Program (NCEP). Expert Panel on Detection,Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult TreatmentPanel II).JAMA 1993;269:3015–3023.2. Joint National Committee on Prevention, Detection, Evaluation, and Treatmentof High Blood Pressure. The sixth report of the Joint National Committee onprevention, detection, evaluation, and treatment of high blood pressure.ArchIntern Med1997;157:2413–2446.3. Roberts WC. Getting cardiologists interested in lipids.Am J Cardiol1993;72:744–745.4. Cohen MV, Byrne MJ, Levine B, Gutowski T, Adelson R. Low rate oftreatment of hypercholesterolemia by cardiologists in patients with suspected andproven coronary artery disease.Circulation 1991;83:1294–1304.5. Giles WH, Anda RF, Jones DH, Serdula MK, Merritt RK, DeStefano F. Recenttrends in the identification and treatment of high blood cholesterol by physicians:progress and missed opportunities.JAMA 1993;269:1133–1138.6. Hennekens CH. Increasing burden of cardiovascular disease.Circulation1998;97:1095–1102.7. Pasternak RC, Grundy SM, Levy D, Thompson PD. 27th Bethesda Confer-ence: matching the intensity of risk factor management with the hazard forcoronary disease events. Task Force 3. Spectrum of risk factors for coronary heartdisease.J Am Coll Cardiol1996;27:978–990.8. Stafford RS, Blumenthal D, Pasternak RC. Variations in cholesterol manage-ment practices of U.S. physicians.J Am Coll Cardiol1997;29:139–146.9. STATA Reference Manual, Release 5. College Station, TX: Stata Press, 1997.10. Chait A, Brunzell JD, Denke MA, Eisenberg D, Ernst ND, Franklin FA Jr,Ginsberg H, Kotchen TA, Kuller L, Mullis RM. Special report: rationale of thediet-heart statement of the American Heart Association. Report of the NutritionCommittee.Circulation 1993;88:3008–3029.11. Bostick RM, Luepker RV, Kofron PM, Pirie PL. Changes in physicianpractice for the prevention of cardiovascular disease.Arch Intern Med1991;151:478–484.12. Starfield B. Concord, discord, and primary care.Mayo Clin Proc1996;71:1209–1210.13. Starfield B, Wray C, Hess K, Gross R, Birk PS, D’Lugoff BC. The influenceof patient-practitioner agreement on outcome of care.Am J Public Health1981;71:127–131.14. Scheitel SM, Boland BJ, Wollan PC, Silverstein MD. Patient-physicianagreement about medical diagnoses and cardiovascular risk factors in the ambu-latory general medical examination.Mayo Clin Proc1996;71:1131–1137.15. Vivier PM, Dietrich AJ, Witters LA. Management of elevated cholesterollevels by New Hampshire primary care physicians.J Fam Pract1988;27:167–172.16. Caggiula AW, Watson JE, Milas NC, Olson MB, Kuller LH, Orchard TJ.Evaluating the efficacy of the National Cholesterol Education Program AdultTreatment Guidelines: cholesterol lowering intervention program.Prev Med1995;24:485–491.17. ASPIRE Steering Group. A British Cardiac Society survey of the potential forthe secondary prevention of coronary disease: ASPIRE (Action on SecondaryPrevention through Intervention to Reduce Events).Heart 1996;75:334–342.
BRIEF REPORTS 785
Recommended

















