
CHALLENGES IN STUDIES OF AGEING AND ORAL HEALTH
Prof. Dr. Jacques Vanobbergen, 9th of June 2017
DEPARTMENT COMMUNITY DENTISTRY AND ORAL PUBLIC HEALTH
RESEARCH GROUP GERODONTOLOGY
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
CONTENT
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
CONTENT
• Some
interesting
results of
recent studies.
• Looking for
some
evidence?
CONTENT
• What do we have?
• What are the
methodological
challenges?
• What do we need?
• Discussion
section of
reports
• Published in
the last 10
years
• Weaknesses
and limitations
of reported
studies
• Searching until
saturation
• Priorities for
further reserach

INTRODUCTION
• Focus:
• Challenges in studies of ageing related to
oral public health
Joint EFP/ORCA workshop on the bounderies between
caries and periodontal diseases.
Group 4: .. In the ageing population
November 2016
Parador De La Granja - Spain
INTRODUCTION
• Focus:
• Challenges in studies of ageing related to
oral public health
Joint EFP/ORCA workshop on the bounderies between
caries and periodontal diseases.
Group 4: .. In the ageing population
Parador De La Granja - Spain
Demographic changes drive the need to learn more
about the burden of oral diseases (in particular
caries and periodontal diseases) in older populations.
More research is needed to provide the foundation for
better prevention and management of these
diseases in older populations.
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B, Preshaw PM, Pretty I, Renvert S,
Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental caries and periodontal diseases in the ageing population: call to
action to protect and enhance oral health and well-being as an essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA
workshop on the boundaries be. Journal of Clinical Periodontology 44, S135–S144 (2017).
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Damage due to both periodontitis and caries is largely
irreversible and therefore cumulative over the lifetime
• with age the exposure to risk factors for both
periodontitis and caries changes
disease experience is certainly increasing with
age, but not necessarily due to age
• Lopez, R., Smith, P. C., Gostemeyer, wendicke, F. (2017) Aging, dental caries and periodontal diseases. Journal of
Clinical Periodontology 44:S18, 145–152.
• Tonetti, M. S. et al. Dental caries and periodontal diseases in the ageing population: call to action to protect and
enhance oral health and well-being as an essential component of healthy ageing - Consensus report of group 4 of
the joint EFP/ORCA workshop on the boundaries be. Journal of Clinical Periodontology 44, S135–S144 (2017).
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
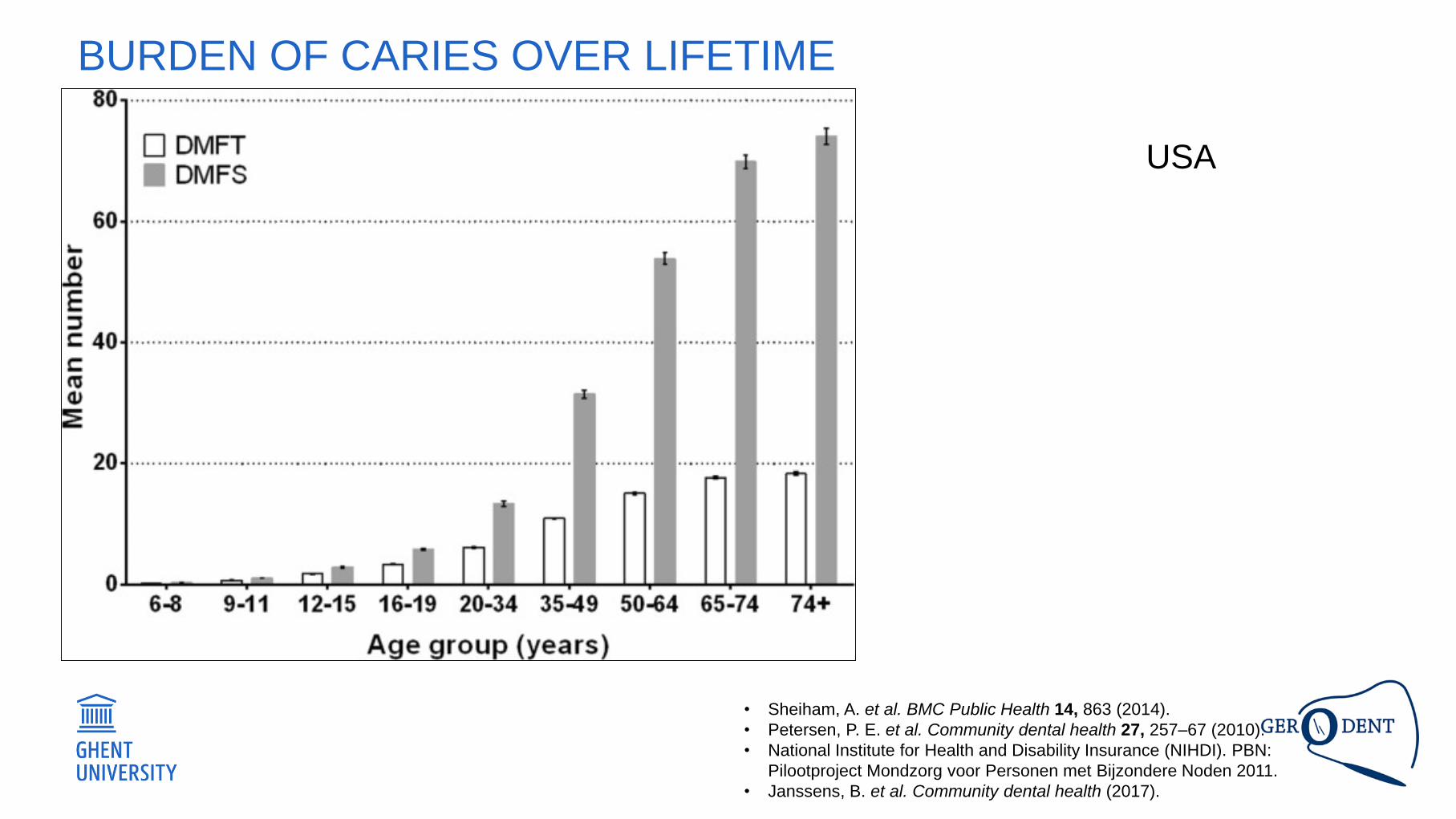
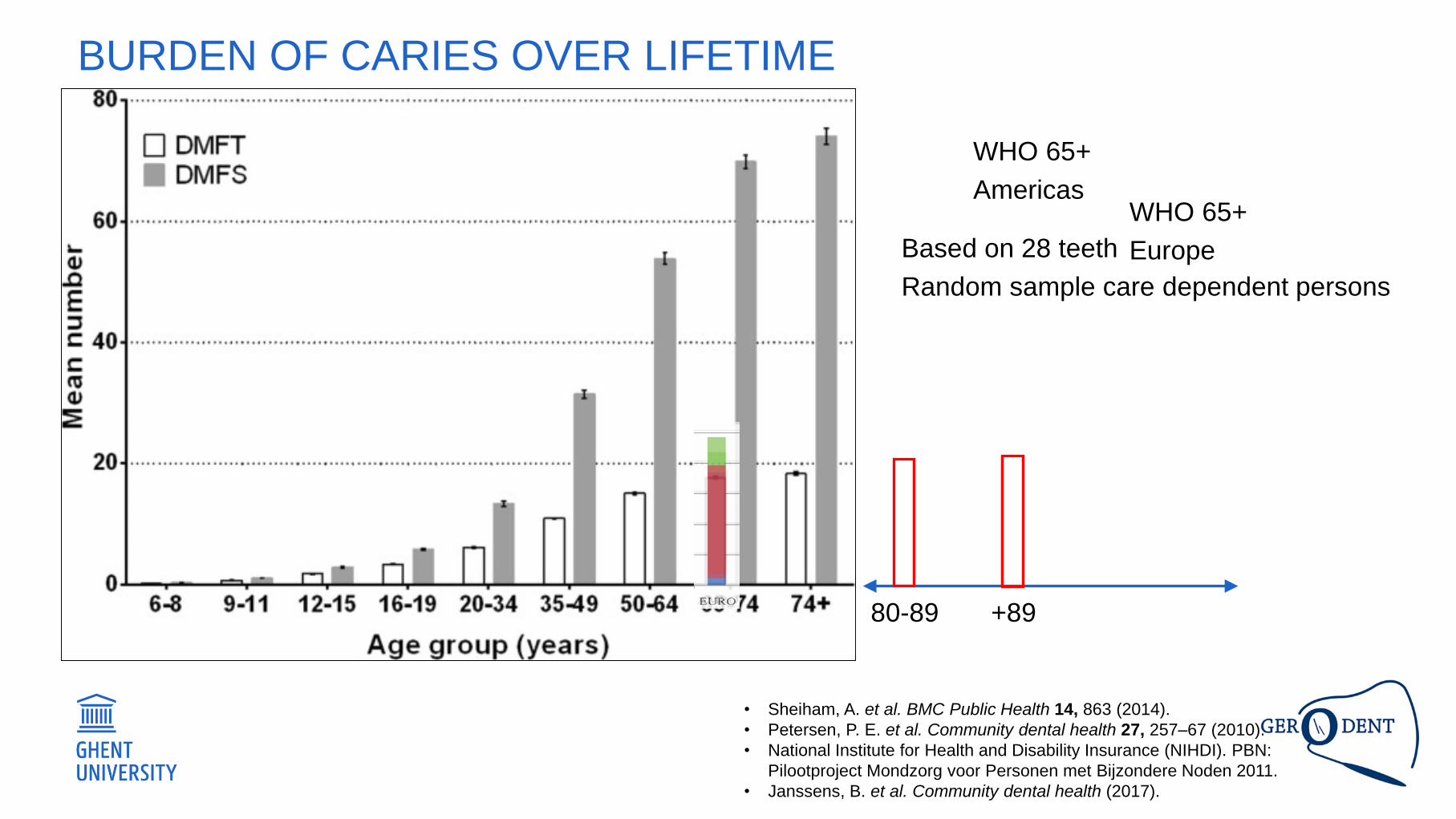
BURDEN OF CARIES OVER LIFETIME
• Sheiham, A. et al. BMC Public Health 14, 863 (2014).
• Petersen, P. E. et al. Community dental health 27, 257–67 (2010).
• National Institute for Health and Disability Insurance (NIHDI). PBN:
Pilootproject Mondzorg voor Personen met Bijzondere Noden 2011.
• Janssens, B. et al. Community dental health (2017).
USA
BURDEN OF CARIES OVER LIFETIME
• Sheiham, A. et al. BMC Public Health 14, 863 (2014).
• Petersen, P. E. et al. Community dental health 27, 257–67 (2010).
• National Institute for Health and Disability Insurance (NIHDI). PBN:
Pilootproject Mondzorg voor Personen met Bijzondere Noden 2011.
• Janssens, B. et al. Community dental health (2017).
80-89 +89
Based on 28 teeth
Random sample care dependent persons
WHO 65+
AmericasWHO 65+
Europe
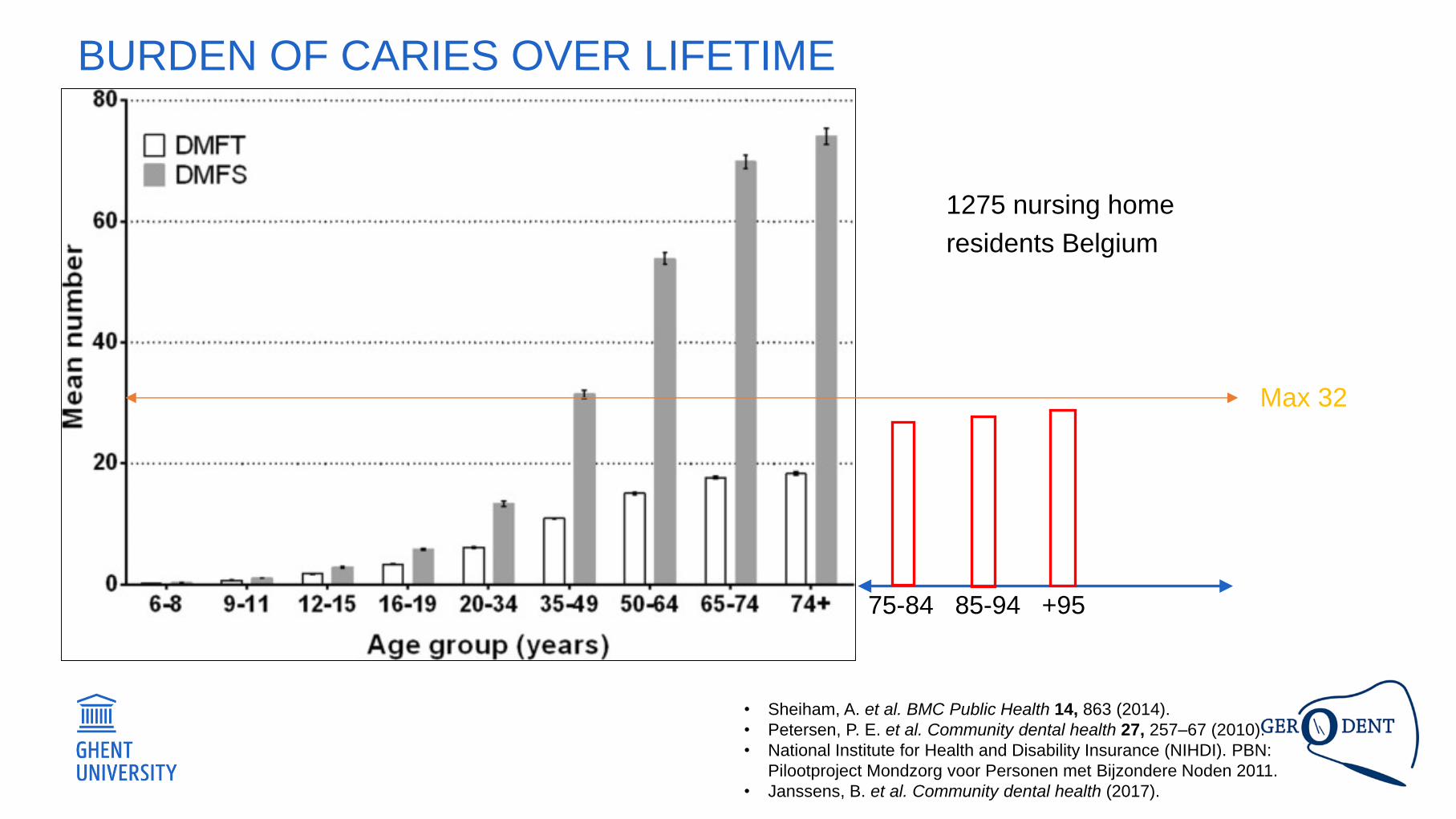
BURDEN OF CARIES OVER LIFETIME
• Sheiham, A. et al. BMC Public Health 14, 863 (2014).
• Petersen, P. E. et al. Community dental health 27, 257–67 (2010).
• National Institute for Health and Disability Insurance (NIHDI). PBN:
Pilootproject Mondzorg voor Personen met Bijzondere Noden 2011.
• Janssens, B. et al. Community dental health (2017).
Max 32
75-84 85-94 +95
1275 nursing home
residents Belgium
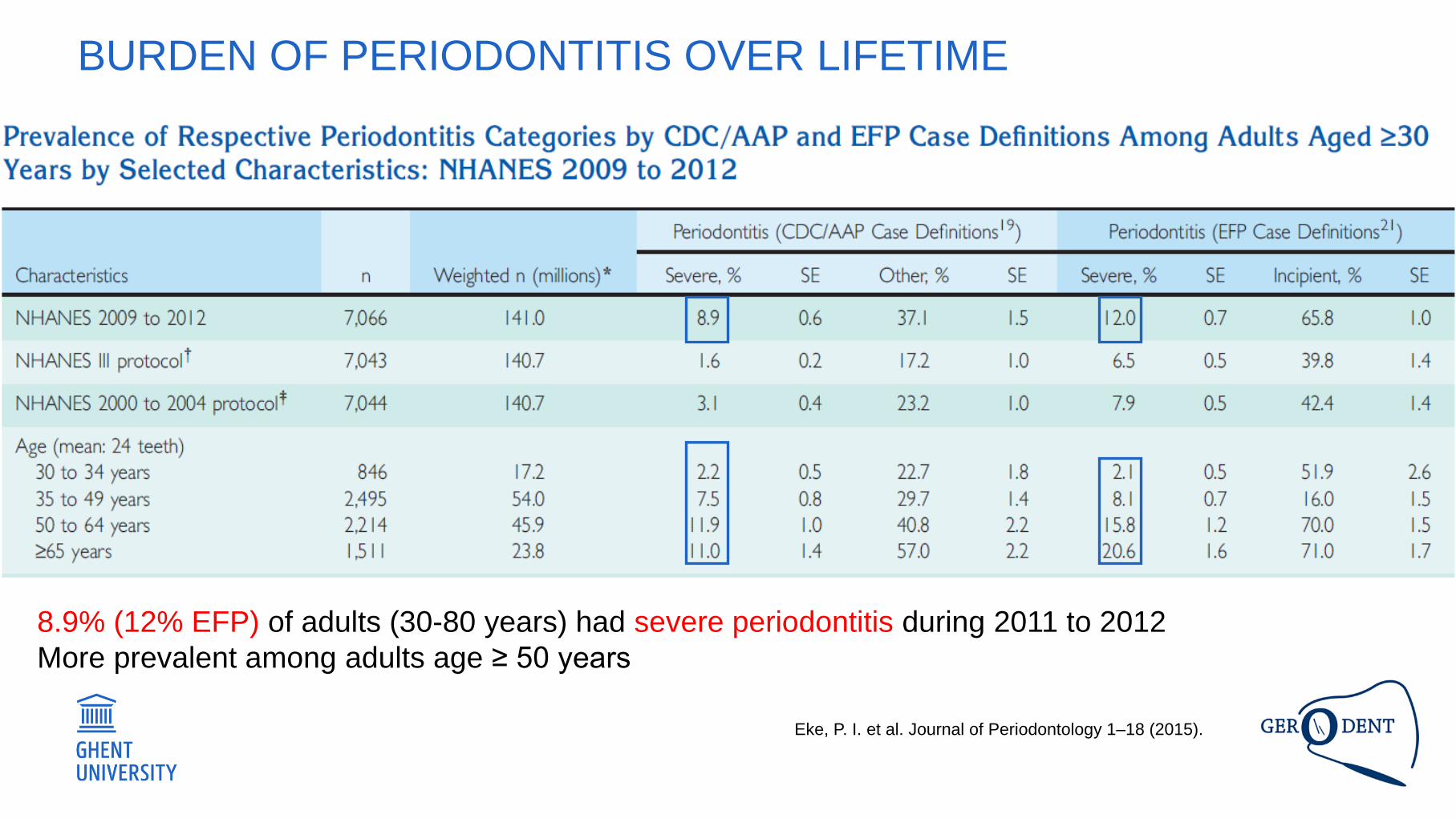
BURDEN OF PERIODONTITIS OVER LIFETIME
Eke, P. I. et al. Journal of Periodontology 1–18 (2015).
8.9% (12% EFP) of adults (30-80 years) had severe periodontitis during 2011 to 2012
More prevalent among adults age ≥ 50 years
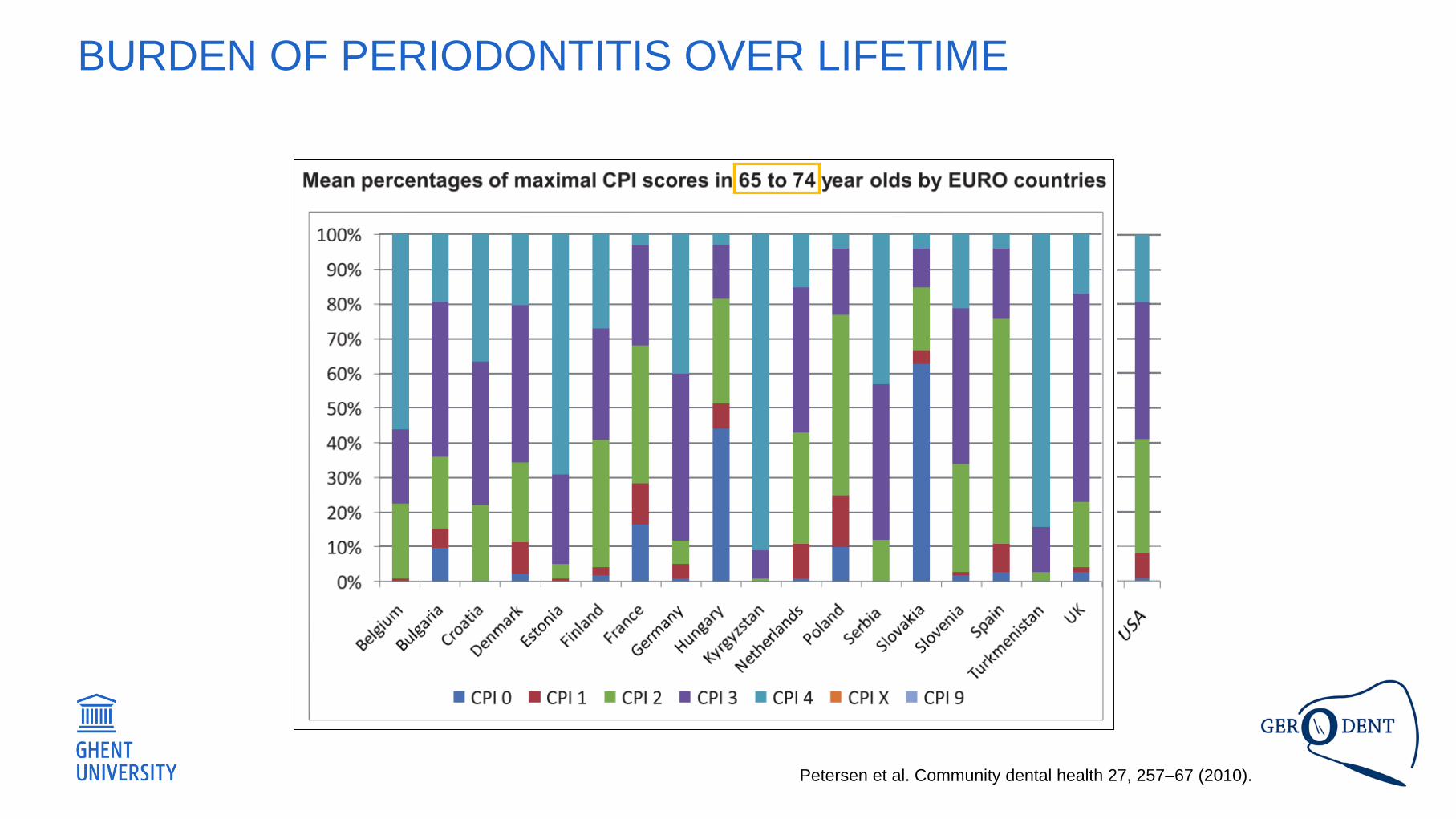
Petersen et al. Community dental health 27, 257–67 (2010).
BURDEN OF PERIODONTITIS OVER LIFETIME
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Selection bias
• Low response rates
• Exclusion of subjects
• Drop outs
• Survivor effect
• Information bias
• Examiner reliability
• Validity: Standardisation and comparability
• Difficulties in doing examination
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Selection bias
• Low response rates (informed consent)
• Exclusion of subjects
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Difficulties in obtaining informed consent
• Exclusion of subjects with cognitive
impairment
• Not sampling institutionalised persons• Chalmers, J.M., et al. Caries experience in existing and new nursing home residents in Adelaide,
Australia. Gerodontology (2002) 19, 30–40.
• Eke, P. I. et al. Journal of Periodontology 1–18 (2015).
• Heegaard, K.M., Holm-Pedersen, P., Bardow, A., Hvidtfeldt, U.A., Grøbæk, M., and Avlund, K. The
Copenhagen Oral Health Senior Cohort: Design, population and dental health. Gerodontology (2015)
28, 165–176.
• Selection bias
• Drop outs
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• More pronounced in elderly population groups
because of worsening health or death.
• High dropout (70 years –>85 years) because
of mortality or morbidity
• 17% to 43% of baseline subjects were
deceased at one year follow up.
• Chalmers, J.M., et al. Caries experience in existing and new nursing home residents in Adelaide, Australia. Gerodontology (2002) 19, 30–40.
• Krustrup, U., et al. The overtime effect of social position on dental caries experience in a group of old-aged Danes born in 1914. Journal of
Public Health Dentistry . (2008) 68, 46–52.
• VdPutten GJ, et al. Effectiveness of supervised implementation of an oral health care guideline in care homes: a single-blinded cluster
randomised controlled trial. Clin Oral Inv (2013) 17:1143-1153
• Hoeksema, A.R., Peters, L.L., Raghoebar, G.M. et al. Oral health status and need for oral care of care-dependent indwelling elderly: from
admission to death Clin Oral Invest (2016).
• Selection bias
• Drop outs
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• In most cases there is no information about
non-responding care-homes and residents
• Difficulties in responder-non-responder
analyses
• Replaced by healthier counterparts
• Hirotomi, T., Kocher, T., Yoshihara, A., Biffar, R., Micheelis, W., Hoffmann, T., Miyazaki, H., and Holtfreter, B. Comparison of periodontal
conditions among three elderly populations in Japan and Germany. Journal of Clinical Periodontology (2014) 41, 633–642.
• Karki, A.J., Monaghan, N., and Morgan, M. Oral health status of older people living in care homes in Wales. British Dental Journal (2015) 219,
331–334.
• Heegaard, K.M., Holm-Pedersen, P., Bardow, A., Hvidtfeldt, U.A., Grøbæk, M., and Avlund, K. The Copenhagen Oral Health Senior Cohort:
Design, population and dental health. Gerodontology (2015) 28, 165–176.
• Selection bias
• Survivor effect
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Premature death because of poor oral health: survivors are the
sample
• Healthy elderly people probably overrepresented in surveys
• Remaining teeth are ‘survivors’ without fillings, carious lesions or
periodontal disease.
• ‘Biological elite’ remains • Vilstrup, L., Holm-Pedersen, P., Mortensen, E. L., & Avlund, K. Dental status and dental caries in 85-year-old Danes. Gerodontology, (2007) 24(1), 3–
13.
• Krustrup, U., et al. The overtime effect of social position on dental caries experience in a group of old-aged Danes born in 1914. Journal of Public
Health Dentistry . (2008) 68, 46–52.
• Holmén, A., et al. Oral status in home-dwelling elderly dependent on moderate or substantial supportive care for daily living: Prevalence of edentulous
subjects, caries and periodontal disease. Gerodontology )2012).
• Hirotomi, T., Kocher, T., Yoshihara, A., Biffar, R., Micheelis, W., Hoffmann, T., Miyazaki, H., and Holtfreter, B. Comparison of periodontal conditions
among three elderly populations in Japan and Germany. Journal of Clinical Periodontology (2014) 41, 633–642.
• Karki, A.J., Monaghan, N., and Morgan, M. Oral health status of older people living in care homes in Wales. British Dental Journal (2015) 219, 331–
334.
• Information bias
• Examiner reliability
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Lack of calibration, sometimes because of frailty of
the patients
• Use of own dentist (trust and more informed consent)
• Intra-examiner agreement was not recorded due to
high age and length of examination
• Vilstrup, L., Holm-Pedersen, P., Mortensen, E. L., & Avlund, K. Dental status and dental caries in 85-year-old Danes. Gerodontology, (2007)
24(1), 3–13.
• Gerritsen, P.F.M., Cune, M.S., Van Der Bilt, A., and De Putter, C. Dental treatment needs in Dutch nursing homes offering integrated dental
care. Special Care in Dentistry (2011) 31, 95–101
• Karki, A.J., Monaghan, N., and Morgan, M. Oral health status of older people living in care homes in Wales. British Dental Journal (2015) 219,
331–334.
• Information bias
• Validity and comparability: Standardisation
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Validity in one age group does not always mean
validity in an other age group
• Internal validity versus external validity
• Comparability of indices (CDC/AAP ~ EFP)
• DMFT not be the best indicator of dental caries
among the elderly
• Use of different periodontal probes.
• Moreira, R.D.S., Nico, L.S., and Tomita, N.E. Oral health conditions among the elderly in Southeastern São Paulo State. Journal of Applied Oral
Science (2009)17, 170–178.
• Hirotomi, T., Kocher, T., Yoshihara, A., Biffar, R., Micheelis, W., Hoffmann, T., Miyazaki, H., and Holtfreter, B. Comparison of periodontal conditions
among three elderly populations in Japan and Germany. Journal of Clinical Periodontology (2014) 41, 633–642.
• Eke, P. I. et al. Journal of Periodontology 1–18 (2015).
• Information bias
• Difficulties in doing examination
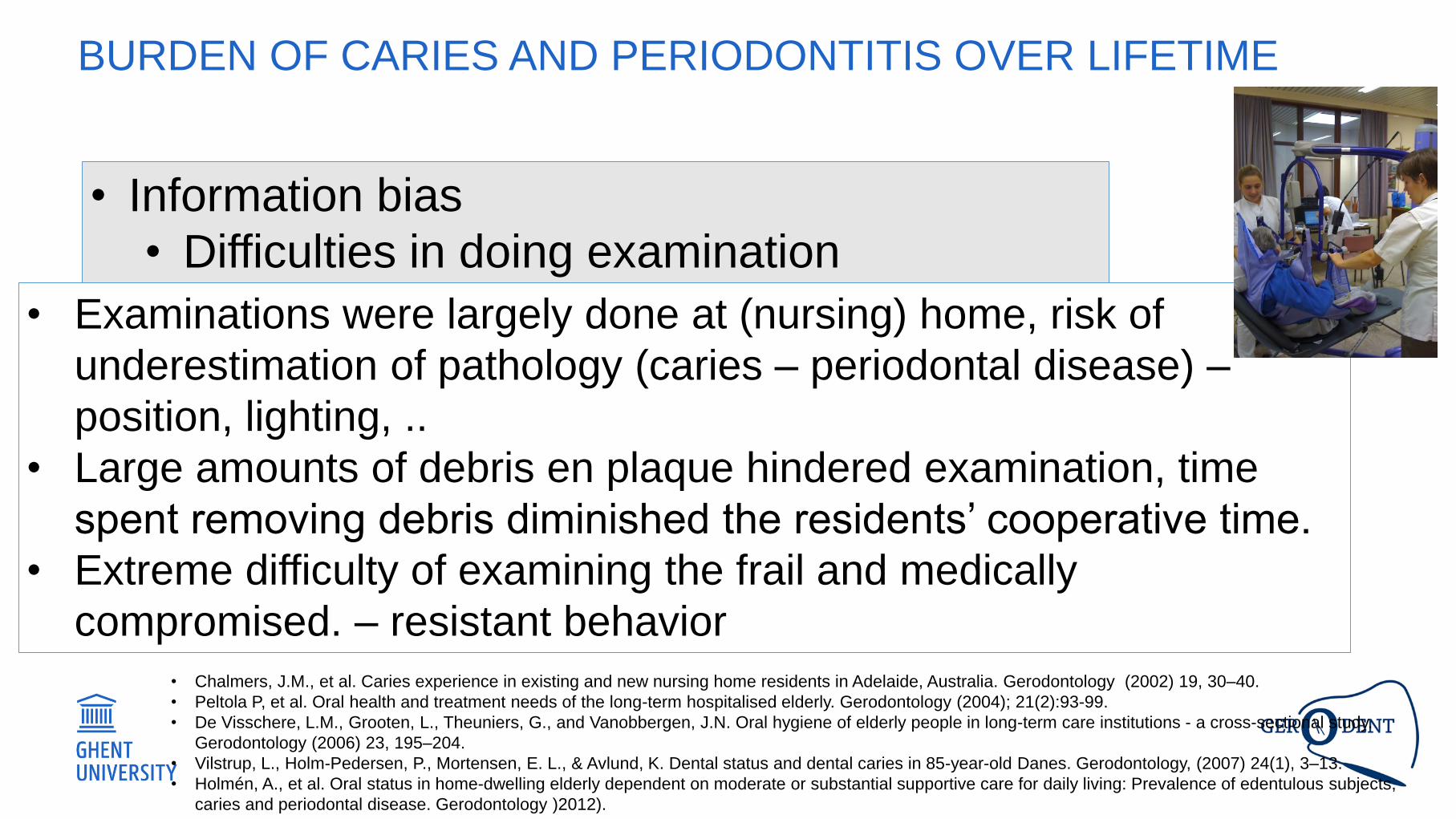
BURDEN OF CARIES AND PERIODONTITIS OVER LIFETIME
• Examinations were largely done at (nursing) home, risk of
underestimation of pathology (caries – periodontal disease) –
position, lighting, ..
• Large amounts of debris en plaque hindered examination, time
spent removing debris diminished the residents’ cooperative time.
• Extreme difficulty of examining the frail and medically
compromised. – resistant behavior
• Chalmers, J.M., et al. Caries experience in existing and new nursing home residents in Adelaide, Australia. Gerodontology (2002) 19, 30–40.
• Peltola P, et al. Oral health and treatment needs of the long-term hospitalised elderly. Gerodontology (2004); 21(2):93-99.
• De Visschere, L.M., Grooten, L., Theuniers, G., and Vanobbergen, J.N. Oral hygiene of elderly people in long-term care institutions - a cross-sectional study.
Gerodontology (2006) 23, 195–204.
• Vilstrup, L., Holm-Pedersen, P., Mortensen, E. L., & Avlund, K. Dental status and dental caries in 85-year-old Danes. Gerodontology, (2007) 24(1), 3–13.
• Holmén, A., et al. Oral status in home-dwelling elderly dependent on moderate or substantial supportive care for daily living: Prevalence of edentulous subjects,
caries and periodontal disease. Gerodontology )2012).
Morley, J. E. European Geriatric Medicine 7, 285–288 (2016).
Also in dentistry!!!
PREVENTION
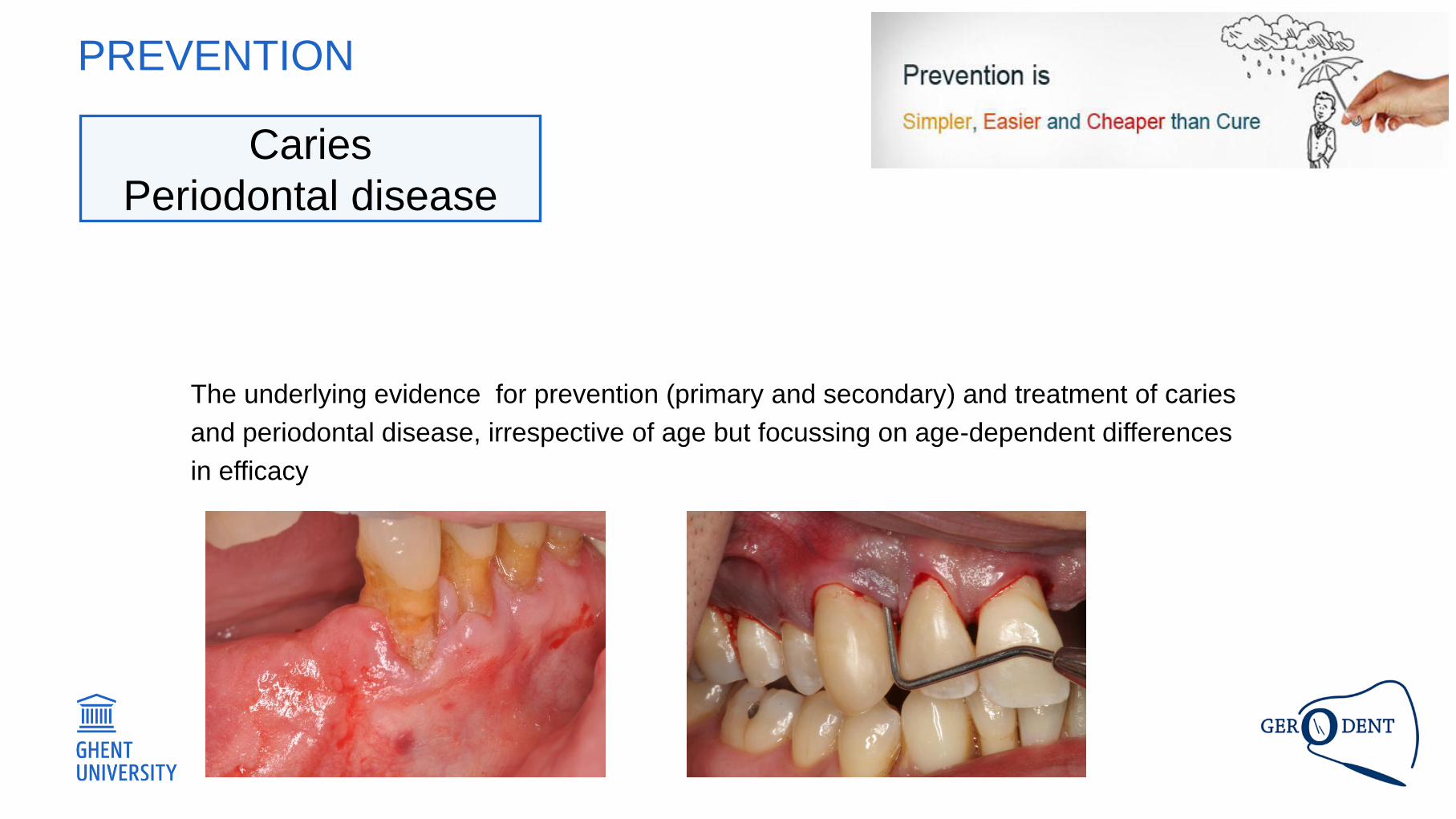
Caries
Periodontal disease
PREVENTION
The underlying evidence for prevention (primary and secondary) and treatment of caries
and periodontal disease, irrespective of age but focussing on age-dependent differences
in efficacy
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
PREVENTION
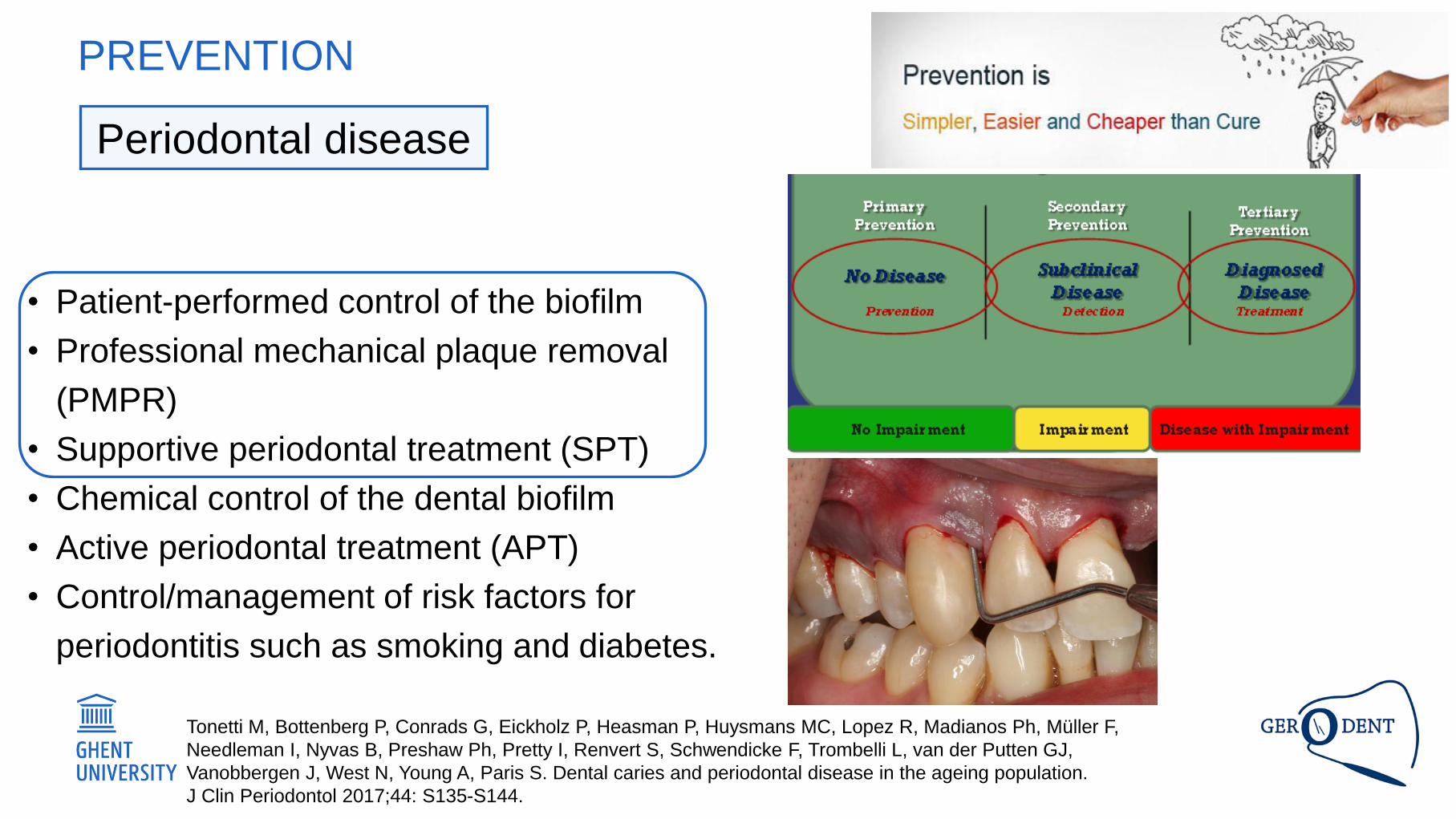
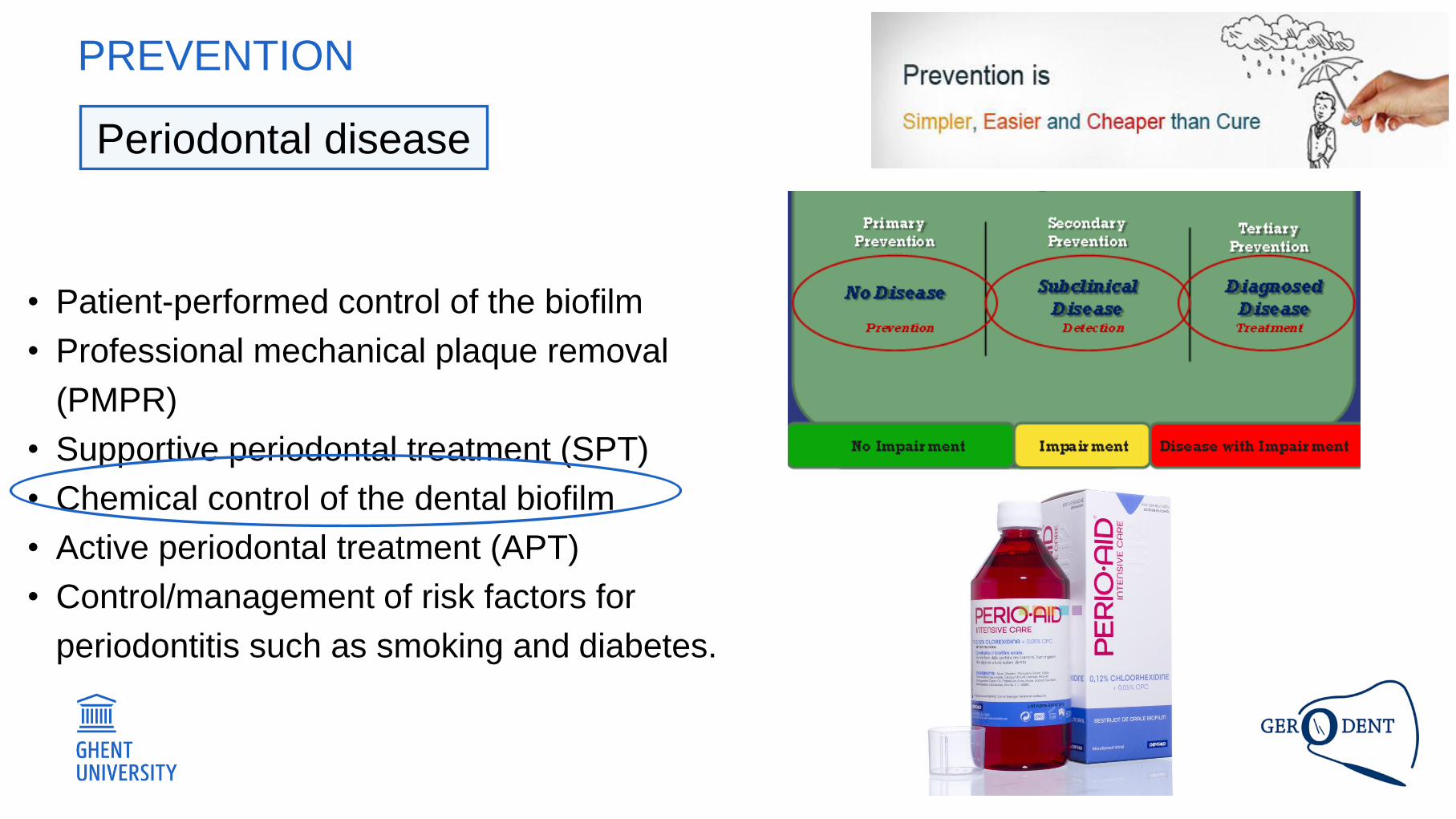
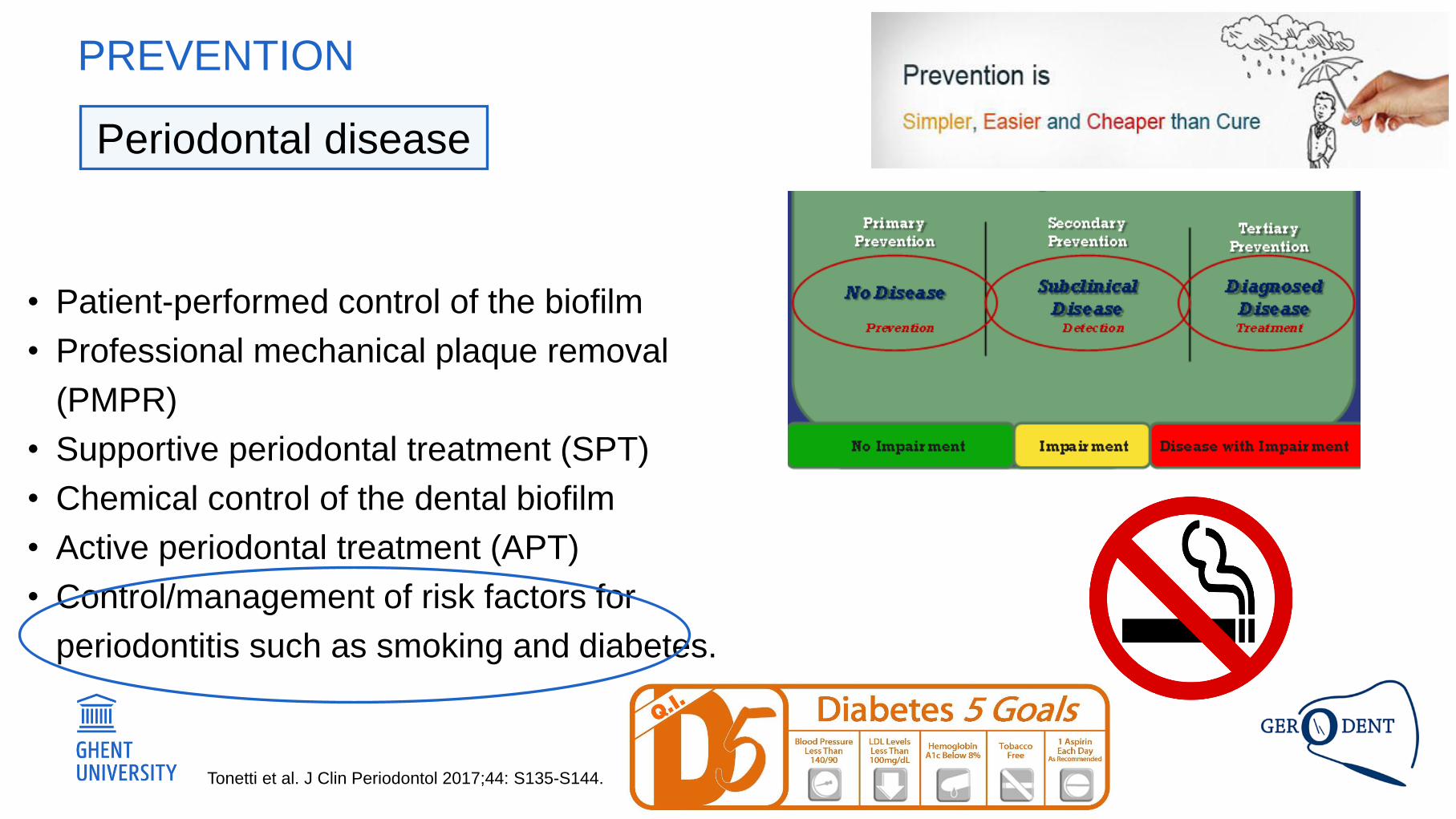
Periodontal disease
PREVENTION
• Patient-performed control of the biofilm
• Professional mechanical plaque removal
(PMPR)
• Supportive periodontal treatment (SPT)
• Chemical control of the dental biofilm
• Active periodontal treatment (APT)
• Control/management of risk factors for
periodontitis such as smoking and diabetes.
Tonetti M, Bottenberg P, Conrads G, Eickholz P, Heasman P, Huysmans MC, Lopez R, Madianos Ph, Müller F,
Needleman I, Nyvas B, Preshaw Ph, Pretty I, Renvert S, Schwendicke F, Trombelli L, van der Putten GJ,
Vanobbergen J, West N, Young A, Paris S. Dental caries and periodontal disease in the ageing population.
J Clin Periodontol 2017;44: S135-S144.
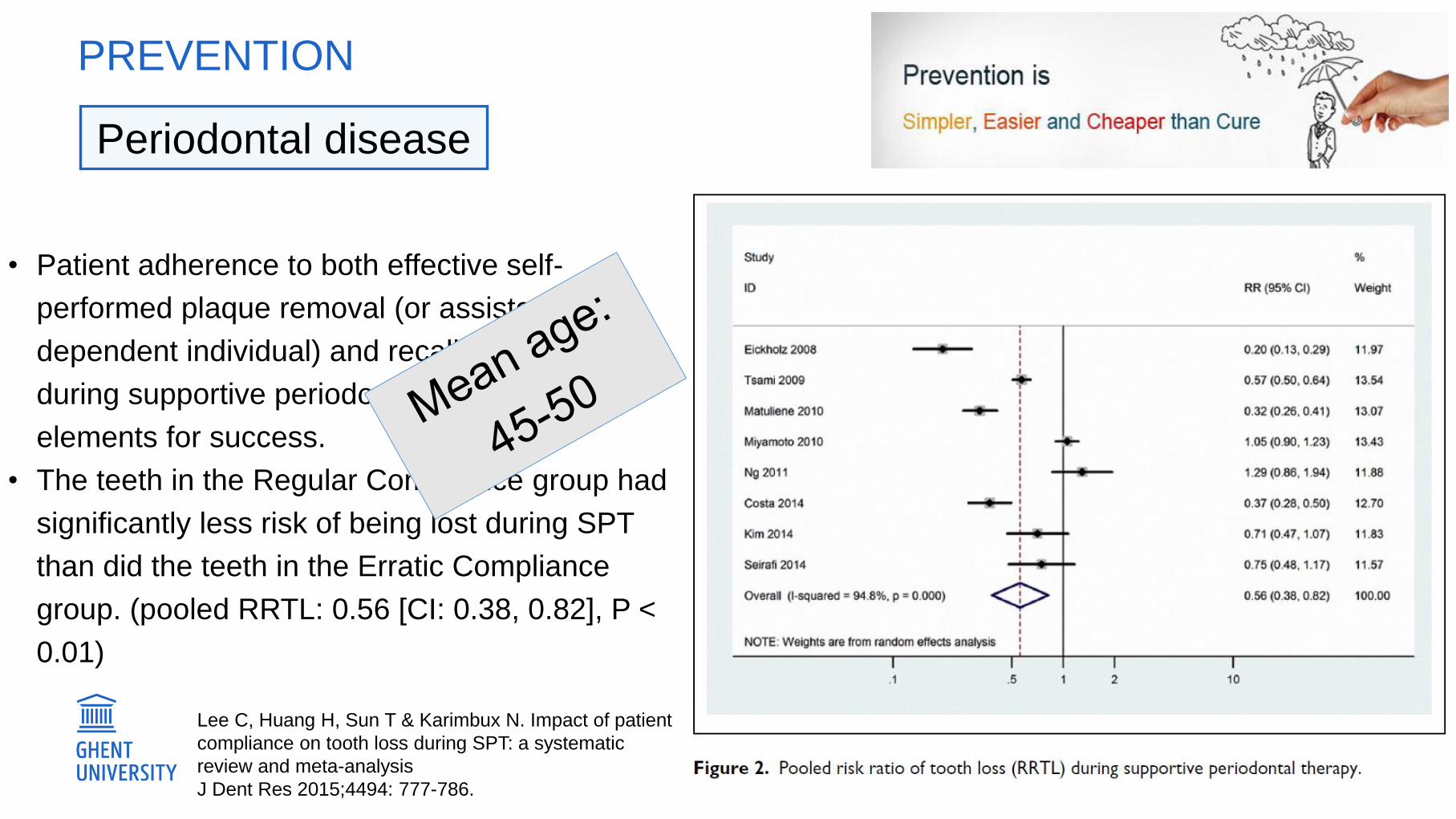
PREVENTION
• Patient adherence to both effective self-
performed plaque removal (or assisted in the
dependent individual) and recall attendance
during supportive periodontal therapy are key
elements for success.
• The teeth in the Regular Compliance group had
significantly less risk of being lost during SPT
than did the teeth in the Erratic Compliance
group. (pooled RRTL: 0.56 [CI: 0.38, 0.82], P <
0.01)
Lee C, Huang H, Sun T & Karimbux N. Impact of patient
compliance on tooth loss during SPT: a systematic
review and meta-analysis
J Dent Res 2015;4494: 777-786.
Periodontal disease
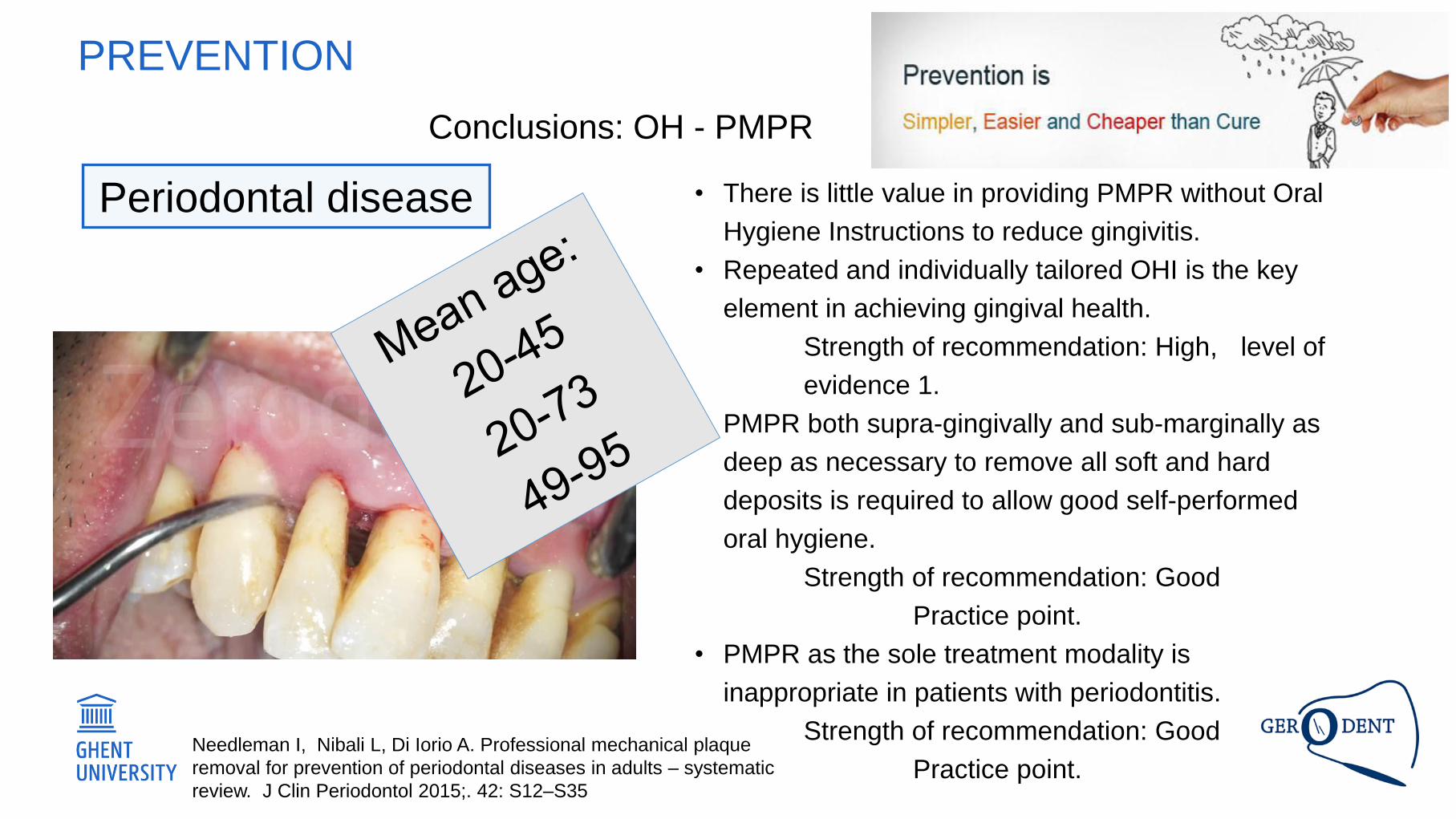
PREVENTION
• There is little value in providing PMPR without Oral
Hygiene Instructions to reduce gingivitis.
• Repeated and individually tailored OHI is the key
element in achieving gingival health.
Strength of recommendation: High, level of
evidence 1.
• PMPR both supra-gingivally and sub-marginally as
deep as necessary to remove all soft and hard
deposits is required to allow good self-performed
oral hygiene.
Strength of recommendation: Good
Practice point.
• PMPR as the sole treatment modality is
inappropriate in patients with periodontitis.
Strength of recommendation: Good
Practice point.Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque
removal for prevention of periodontal diseases in adults – systematic
review. J Clin Periodontol 2015;. 42: S12–S35
Conclusions: OH - PMPR
Periodontal disease
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
PREVENTION
• Selection bias
• Dropout is always a concern!
• Exclusion of subjects (frail elderly – dementia)
• Very few studies
• More inclusive regarding the quality criteria
• Precision of the estimate (95% CI)
• Comparability
• study designs
• Age groups
PREVENTION
• Lee C, Huang H, Sun T & Karimbux N. Impact of patient compliance on tooth loss during SPT: a systematic
review and meta-analysis. J Dent Res 2015;4494: 777-786.
• Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque removal for prevention of periodontal
diseases in adults – systematic review. J Clin Periodontol 2015;. 42: S12–S35
• Information bias
• Calibration of the examiners
• Blinding
• Examiner blinding
• Patient blinding
• Assessment of the compliance
• Difficulties to include all confounders
• E.g. motivation of patient / clinician who provides OHI
PREVENTION
• Lee C, Huang H, Sun T & Karimbux N. Impact of patient compliance on tooth loss during SPT: a systematic
review and meta-analysis. J Dent Res 2015;4494: 777-786.
• Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque removal for prevention of periodontal
diseases in adults – systematic review. J Clin Periodontol 2015;. 42: S12–S35
PREVENTION
• Patient-performed control of the biofilm
• Professional mechanical plaque removal
(PMPR)
• Supportive periodontal treatment (SPT)
• Chemical control of the dental biofilm
• Active periodontal treatment (APT)
• Control/management of risk factors for
periodontitis such as smoking and diabetes.
Periodontal disease
PREVENTION
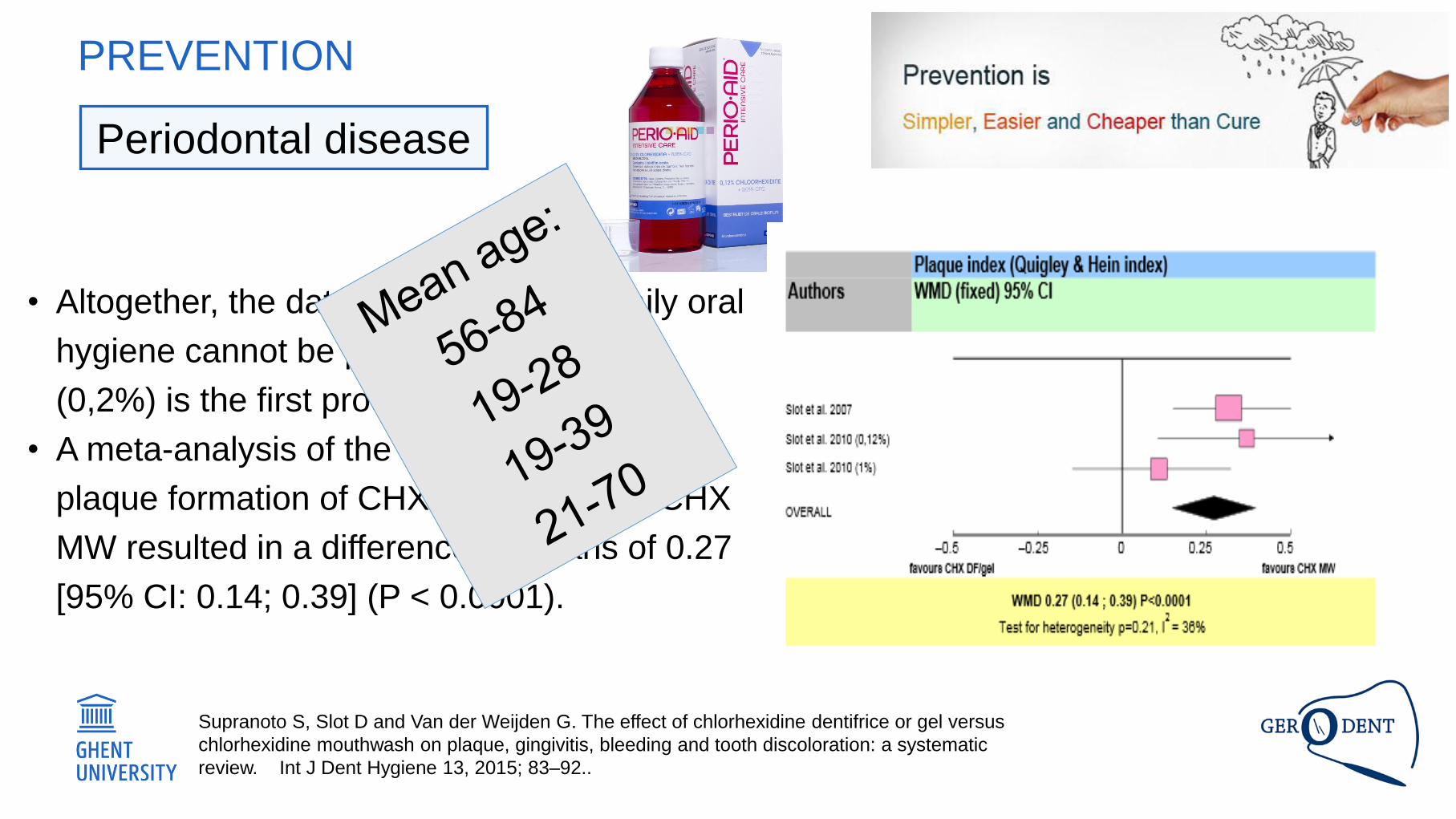
• Altogether, the data show that when daily oral
hygiene cannot be performed, CHX MW
(0,2%) is the first product of choice.
• A meta-analysis of the effect on ‘de novo’
plaque formation of CHX DF/gel versus CHX
MW resulted in a difference in means of 0.27
[95% CI: 0.14; 0.39] (P < 0.0001).
Supranoto S, Slot D and Van der Weijden G. The effect of chlorhexidine dentifrice or gel versus
chlorhexidine mouthwash on plaque, gingivitis, bleeding and tooth discoloration: a systematic
review. Int J Dent Hygiene 13, 2015; 83–92..
Periodontal disease
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
PREVENTION – CHEMICAL CONTROL OF THE BIOFILM
• Selection bias
• Wide spread of age groups
• Only three studies could be included
• Information bias
• Low to moderate risk of bias
• Patient blinding not feasible
• Assessment of compliance?
PREVENTION – CHEMICAL CONTROL OF THE BIOFILM
Supranoto S, Slot D and Van der Weijden G. The effect of chlorhexidine dentifrice or gel versus
chlorhexidine mouthwash on plaque, gingivitis, bleeding and tooth discoloration: a systematic
review. Int J Dent Hygiene 13, 2015; 83–92..
PREVENTION
• Patient-performed control of the biofilm
• Professional mechanical plaque removal
(PMPR)
• Supportive periodontal treatment (SPT)
• Chemical control of the dental biofilm
• Active periodontal treatment (APT)
• Control/management of risk factors for
periodontitis such as smoking and diabetes.
Tonetti et al. J Clin Periodontol 2017;44: S135-S144.
Periodontal disease
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
PREVENTION
PREVENTION
• Caries management (continuum of
preventive and treatment strategies)
• Primary prevention: caries onset
prevention
• Secondary prevention: arrest of
caries lesions
Rich history of
RCT’s and
Cochrane Reviews
involving
adolescents and
younger children
Caries
Tonetti M, Bottenberg P, Conrads G, Eickholz P, Heasman P, Huysmans MC, Lopez R, Madianos Ph, Müller F,
Needleman I, Nyvas B, Preshaw Ph, Pretty I, Renvert S, Schwendicke F, Trombelli L, van der Putten GJ,
Vanobbergen J, West N, Young A, Paris S. Dental caries and periodontal disease in the ageing population.
J Clin Periodontol 2017;44: S135-S144.
PREVENTION
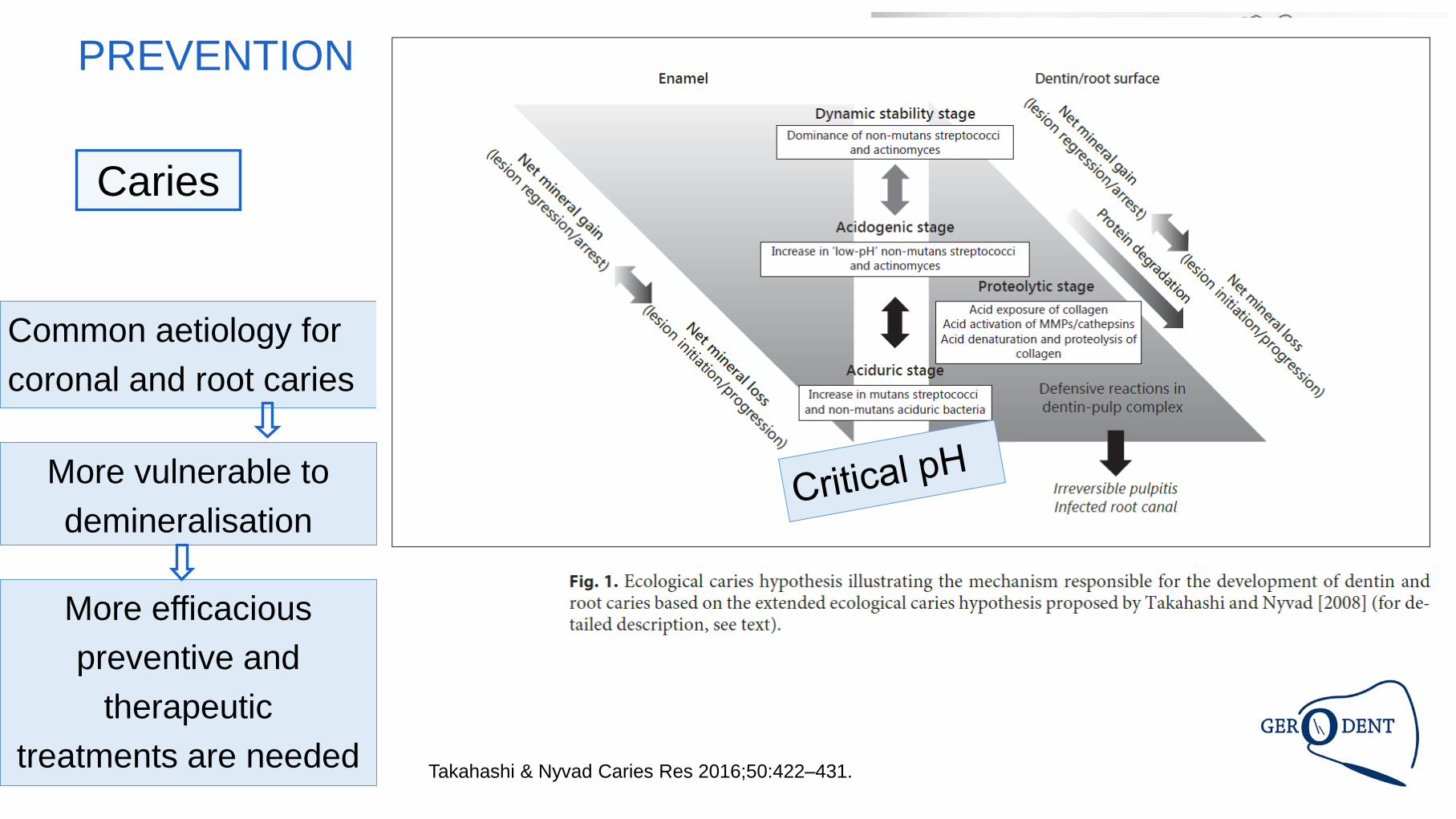
Takahashi & Nyvad Caries Res 2016;50:422–431.
Common aetiology for
coronal and root caries
More vulnerable to
demineralisation
More efficacious
preventive and
therapeutic
treatments are needed
Caries
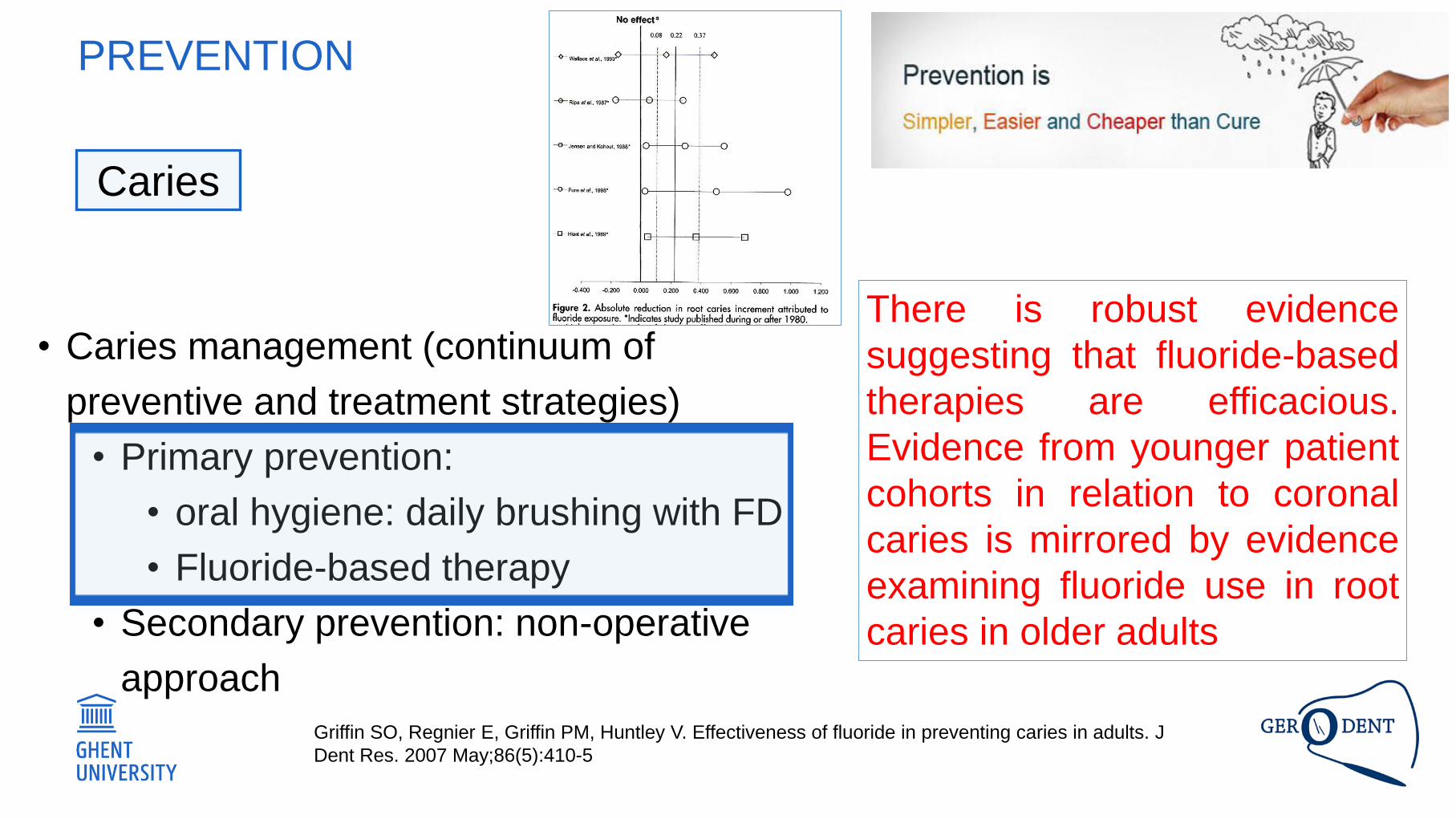
PREVENTION
• Caries management (continuum of
preventive and treatment strategies)
• Primary prevention:
• oral hygiene: daily brushing with FD
• Fluoride-based therapy
• Secondary prevention: non-operative
approach
There is robust evidence
suggesting that fluoride-based
therapies are efficacious.
Evidence from younger patient
cohorts in relation to coronal
caries is mirrored by evidence
examining fluoride use in root
caries in older adults
Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J
Dent Res. 2007 May;86(5):410-5
Caries
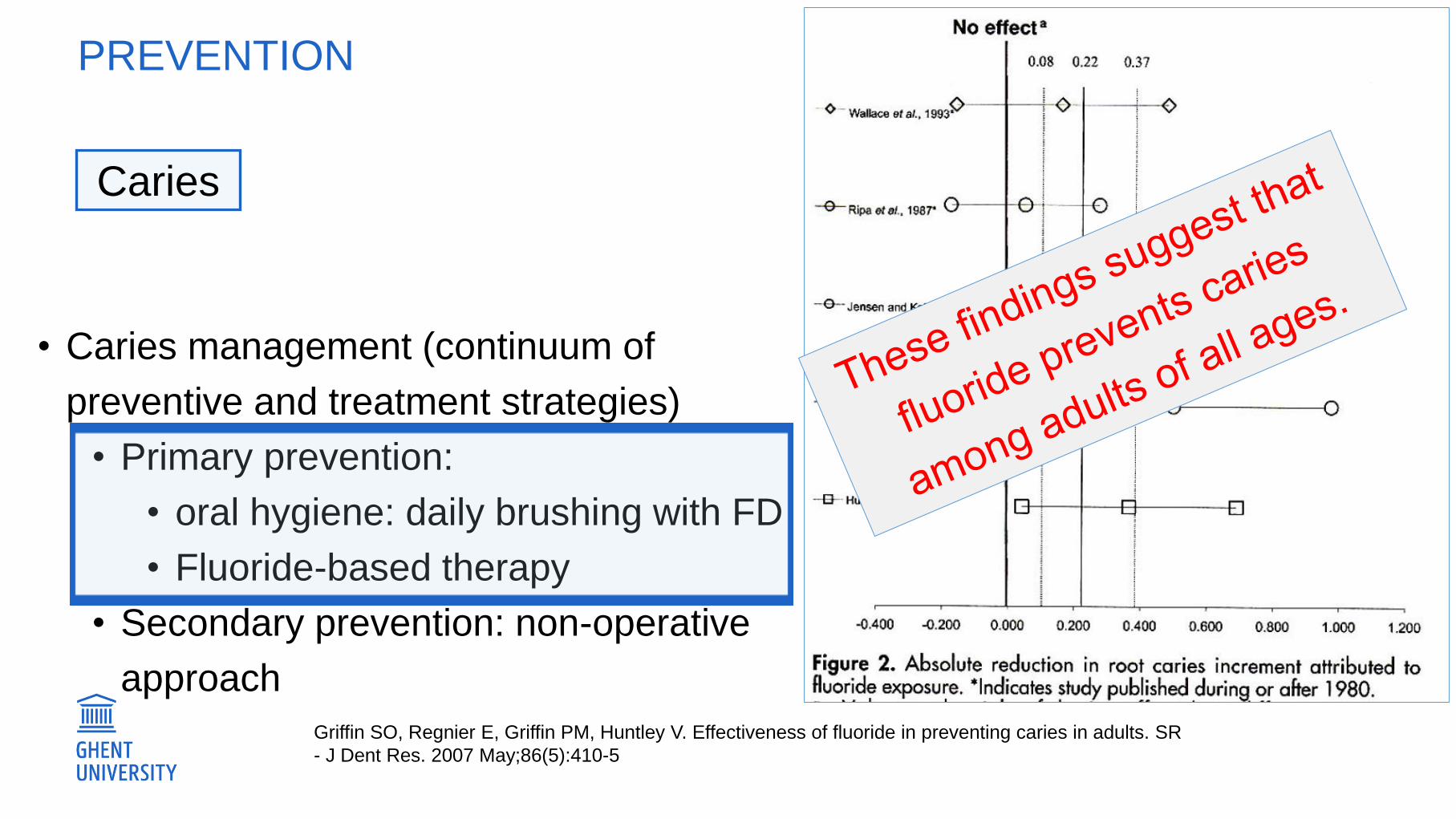
PREVENTION
• Caries management (continuum of
preventive and treatment strategies)
• Primary prevention:
• oral hygiene: daily brushing with FD
• Fluoride-based therapy
• Secondary prevention: non-operative
approach
There is robust evidence
suggesting that fluoride-based
therapies are efficacious.
Evidence from younger patient
cohorts in relation to coronal
caries is mirrored by evidence
examining fluoride use in root
caries in older adults
Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. SR
- J Dent Res. 2007 May;86(5):410-5
Caries
PREVENTION
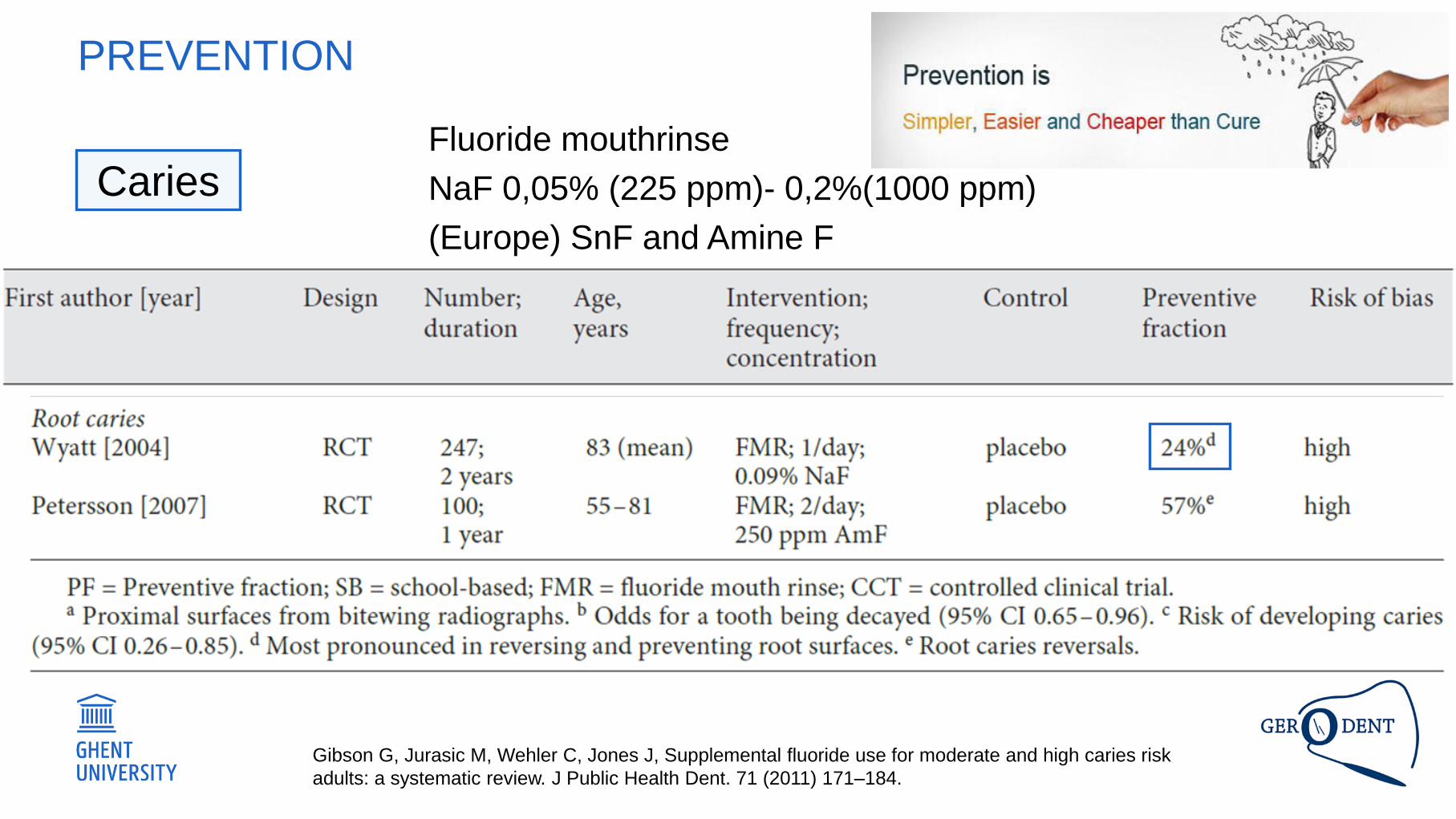
Gibson G, Jurasic M, Wehler C, Jones J, Supplemental fluoride use for moderate and high caries risk
adults: a systematic review. J Public Health Dent. 71 (2011) 171–184.
Fluoride mouthrinse
NaF 0,05% (225 ppm)- 0,2%(1000 ppm)
(Europe) SnF and Amine F
Caries
PREVENTION
• Caries management (continuum of
preventive and treatment strategies)
• Primary prevention:
• oral hygiene: daily brushing with FD
• Fluoride-based therapy
• Secondary prevention: non-operative
approach
boosting fluoride
concentrations for
improved control of root caries
in a non-operative approach
Caries
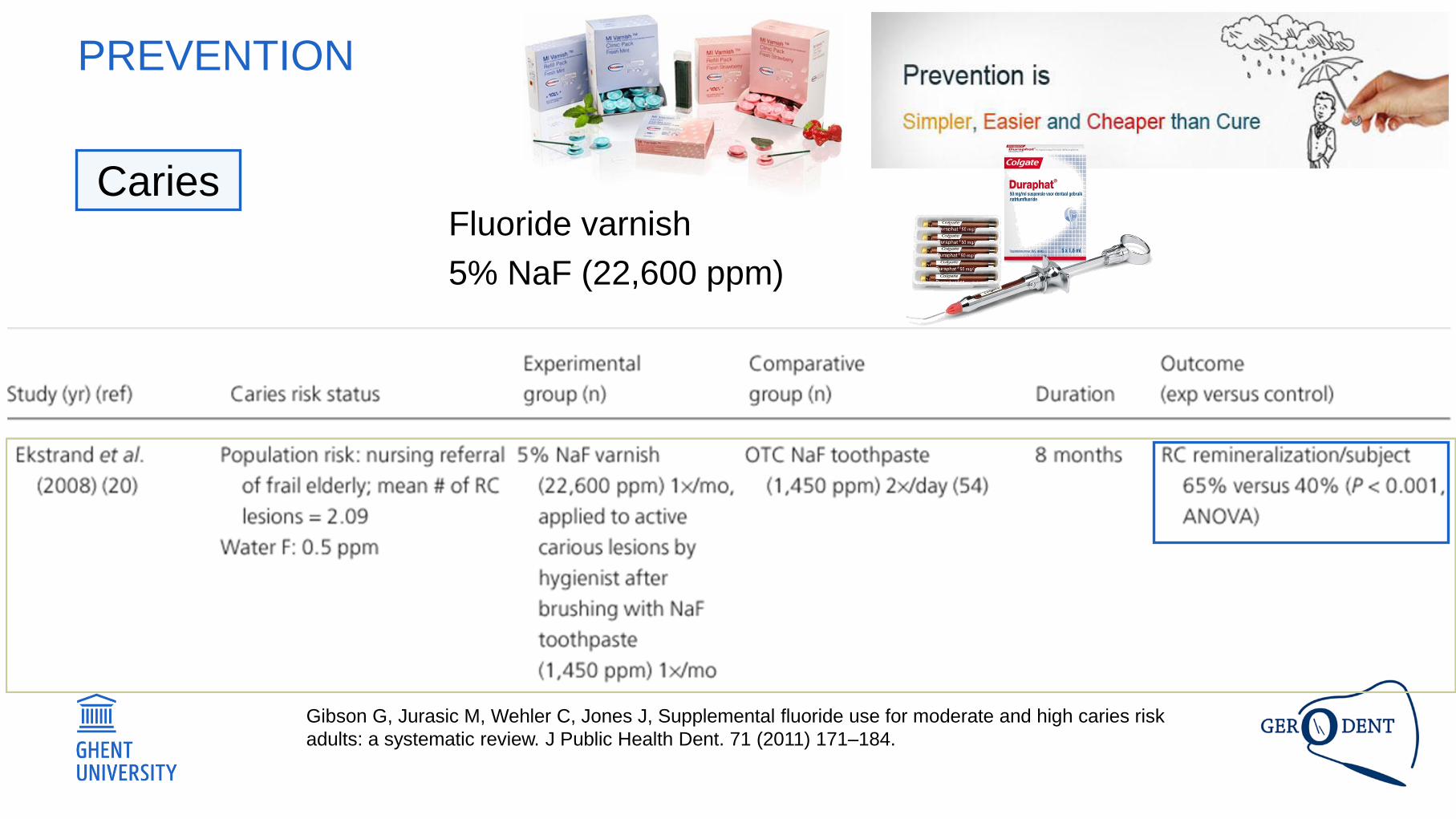
PREVENTION
Gibson G, Jurasic M, Wehler C, Jones J, Supplemental fluoride use for moderate and high caries risk
adults: a systematic review. J Public Health Dent. 71 (2011) 171–184.
Fluoride varnish
5% NaF (22,600 ppm)
Caries
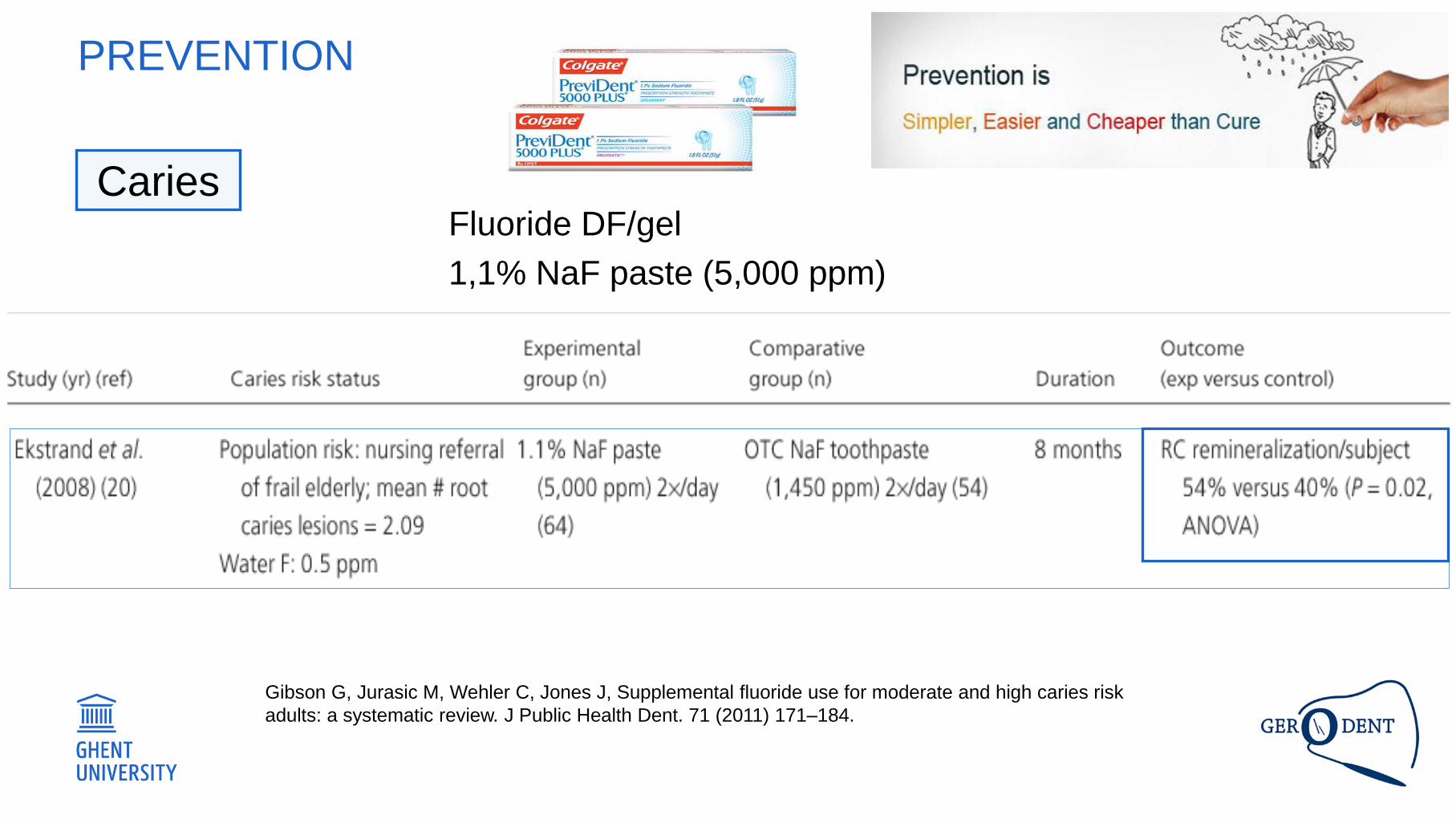
PREVENTION
Gibson G, Jurasic M, Wehler C, Jones J, Supplemental fluoride use for moderate and high caries risk
adults: a systematic review. J Public Health Dent. 71 (2011) 171–184.
Fluoride DF/gel
1,1% NaF paste (5,000 ppm)
Caries
PREVENTION
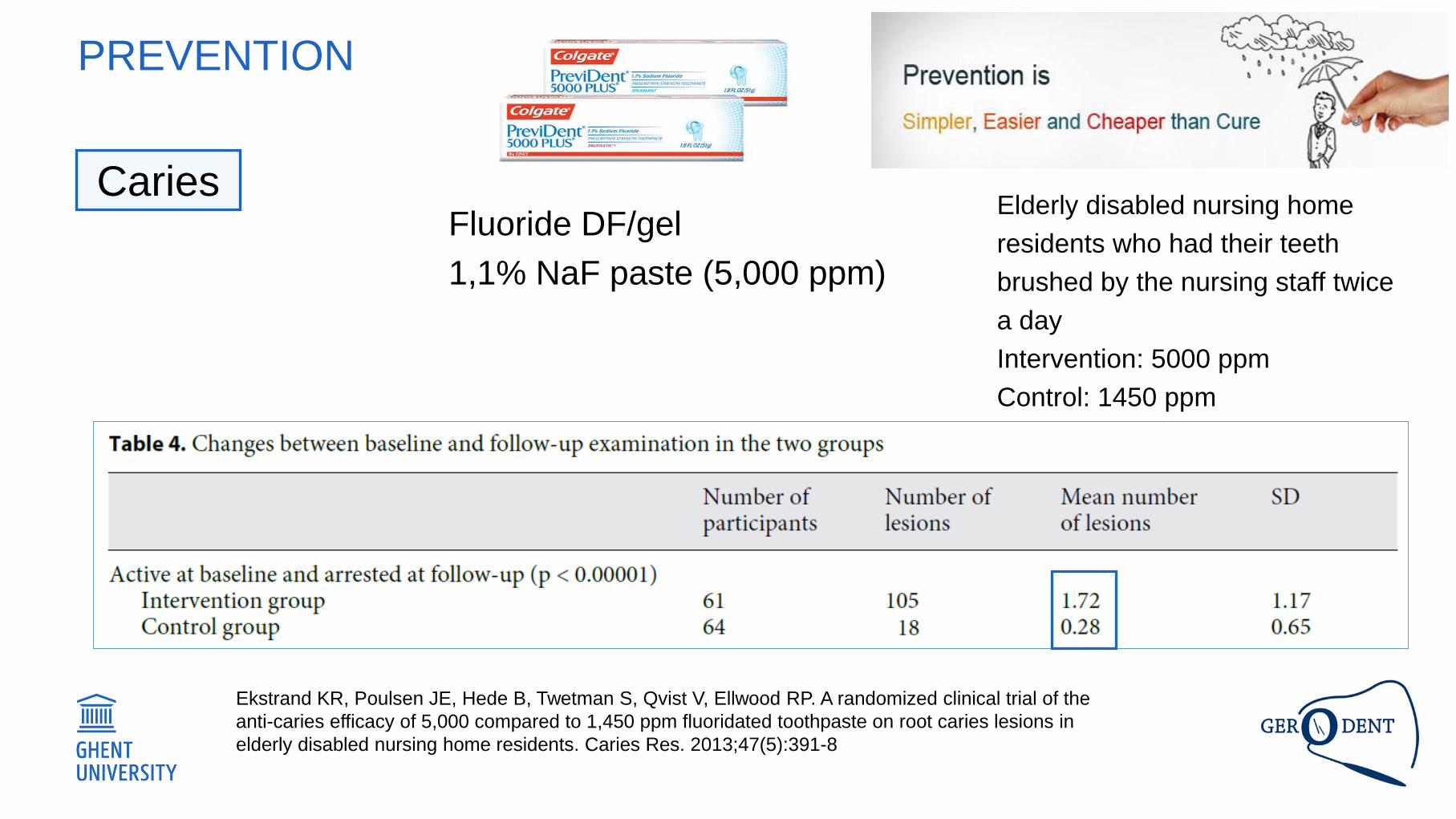
Fluoride DF/gel
1,1% NaF paste (5,000 ppm)
Ekstrand KR, Poulsen JE, Hede B, Twetman S, Qvist V, Ellwood RP. A randomized clinical trial of the
anti-caries efficacy of 5,000 compared to 1,450 ppm fluoridated toothpaste on root caries lesions in
elderly disabled nursing home residents. Caries Res. 2013;47(5):391-8
Elderly disabled nursing home
residents who had their teeth
brushed by the nursing staff twice
a day
Intervention: 5000 ppm
Control: 1450 ppm
Caries
PREVENTION
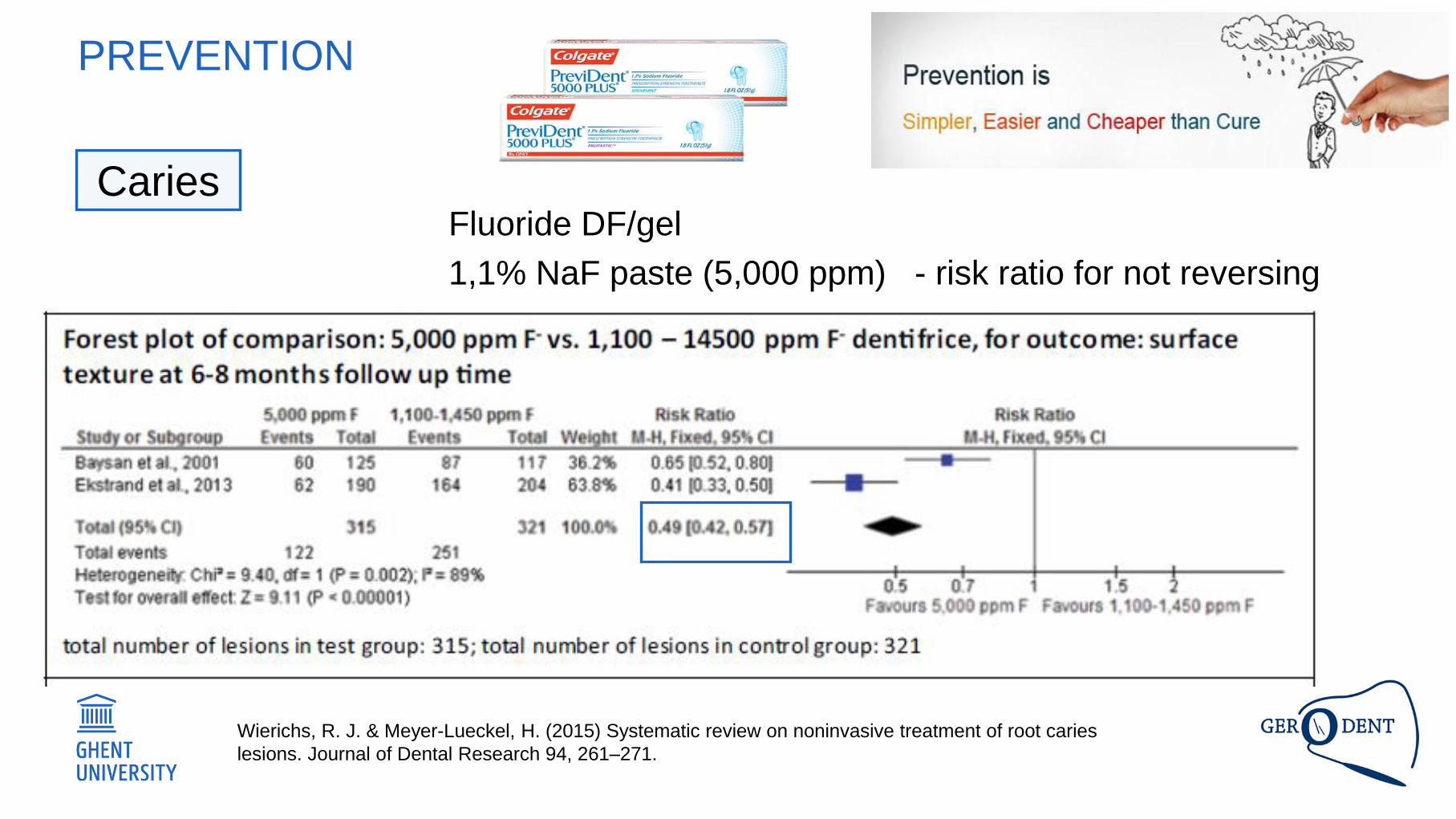
Fluoride DF/gel
1,1% NaF paste (5,000 ppm) - risk ratio for not reversing
Wierichs, R. J. & Meyer-Lueckel, H. (2015) Systematic review on noninvasive treatment of root caries
lesions. Journal of Dental Research 94, 261–271.
Caries
PREVENTION
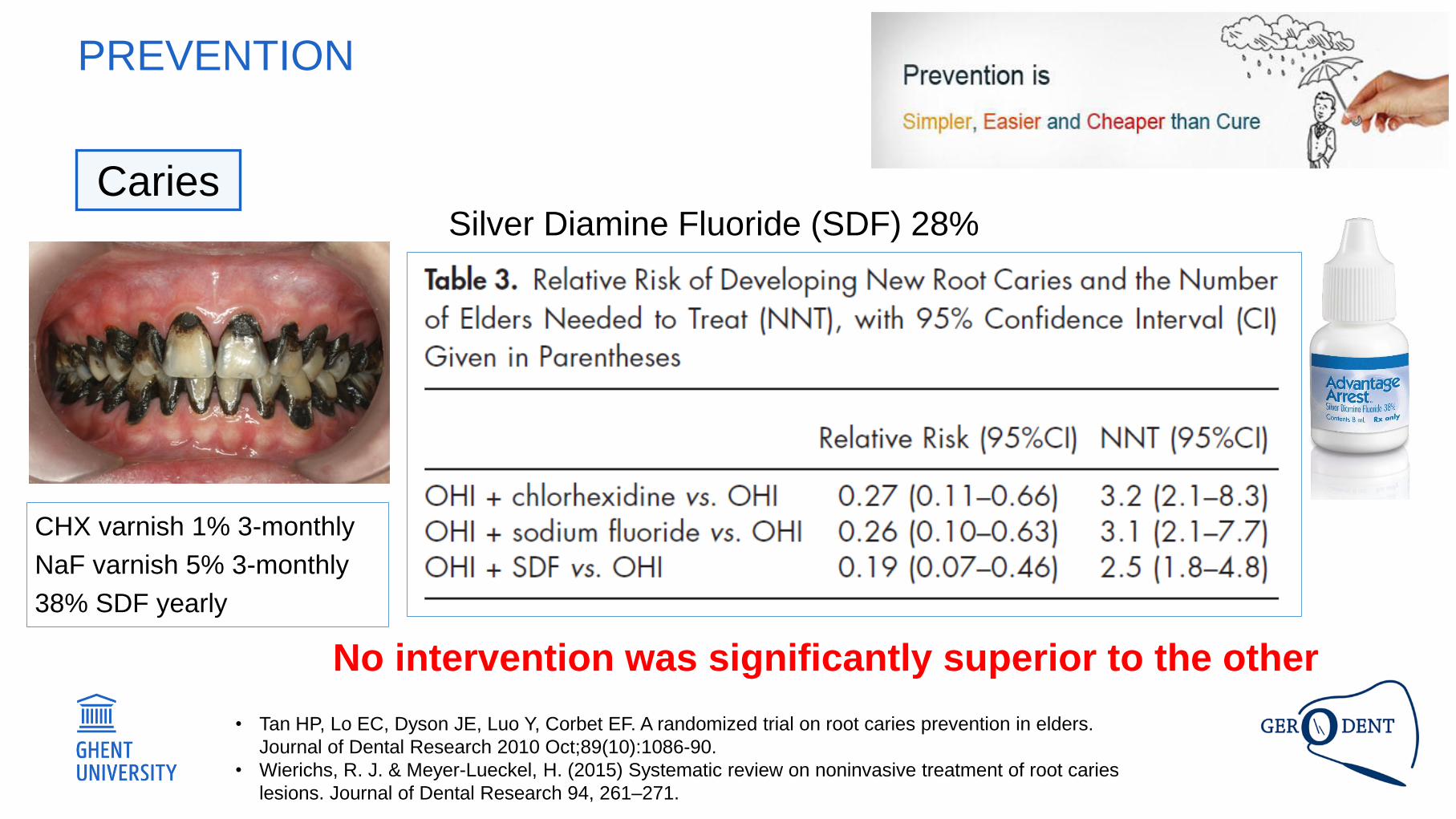
Silver Diamine Fluoride (SDF) 28%
• Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders.
Journal of Dental Research 2010 Oct;89(10):1086-90.
• Wierichs, R. J. & Meyer-Lueckel, H. (2015) Systematic review on noninvasive treatment of root caries
lesions. Journal of Dental Research 94, 261–271.
CHX varnish 1% 3-monthly
NaF varnish 5% 3-monthly
38% SDF yearly
No intervention was significantly superior to the other
Caries
PREVENTION
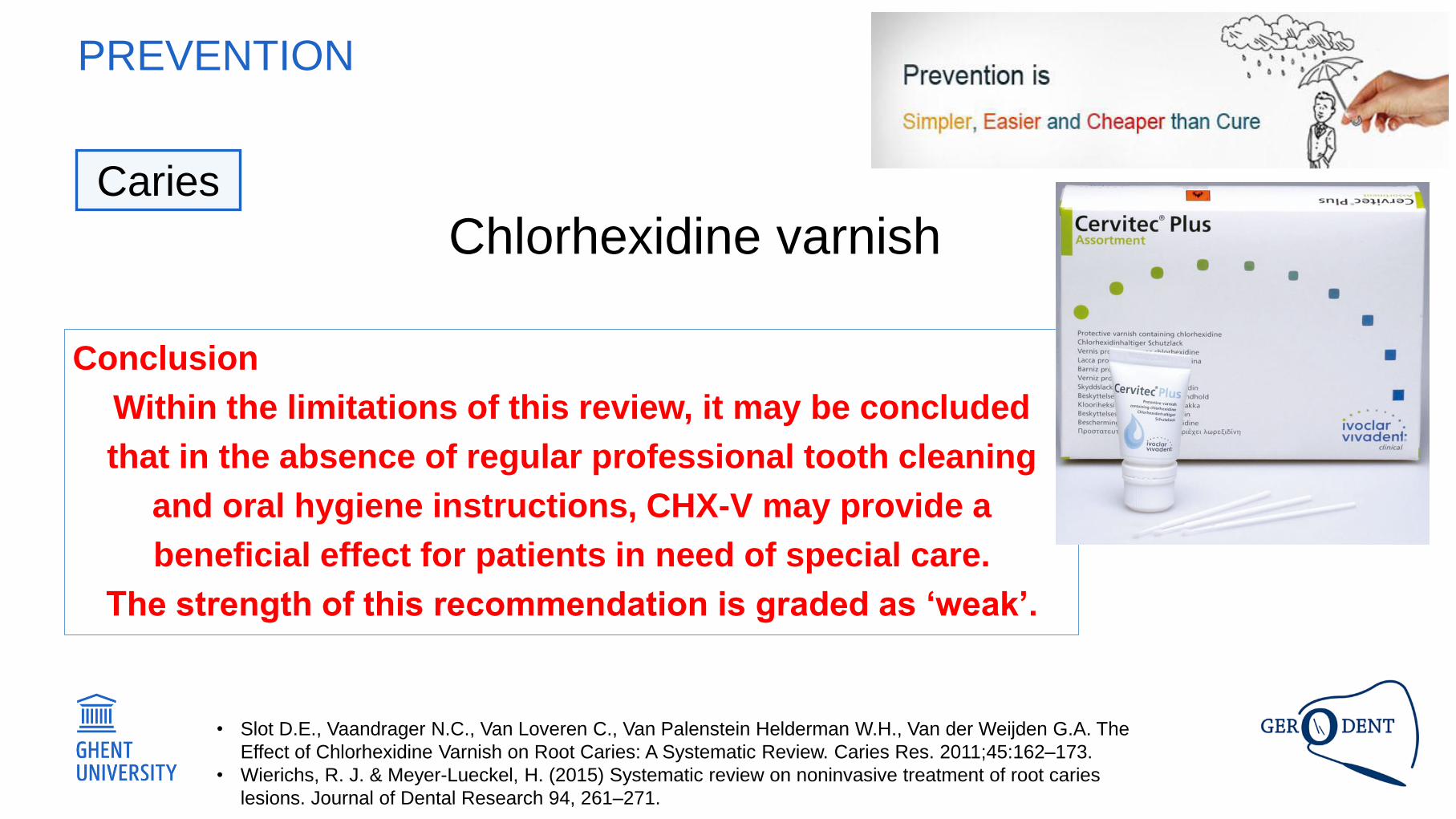
Chlorhexidine varnish
• Slot D.E., Vaandrager N.C., Van Loveren C., Van Palenstein Helderman W.H., Van der Weijden G.A. The
Effect of Chlorhexidine Varnish on Root Caries: A Systematic Review. Caries Res. 2011;45:162–173.
• Wierichs, R. J. & Meyer-Lueckel, H. (2015) Systematic review on noninvasive treatment of root caries
lesions. Journal of Dental Research 94, 261–271.
Conclusion
Within the limitations of this review, it may be concluded
that in the absence of regular professional tooth cleaning
and oral hygiene instructions, CHX-V may provide a
beneficial effect for patients in need of special care.
The strength of this recommendation is graded as ‘weak’.
Caries
PREVENTION
Conclusion
Heasman PA, Ritchie M, Asuni A, Gavillet E, Simonsen JL, Nyvad B. Gingival recession and root caries
in the ageing population: a critical evaluation of treatments. J Clin Periodontol. 2017 Mar;44 Suppl
18:S178-S193.
• Root caries lesion development can be controlled at the population level by brushing the teeth
twice a day with conventional fluoride toothpaste (1000-1500 ppm F).
• Active root caries lesions can be converted into inactive lesions by twice daily brushing with
conventional fluoride toothpaste (1000-1500 ppm F), combined with professional applications of
5% NaF varnish or 2% NaF solution 3-4 times a year.
• Alternatively, lesion arrest might be obtained by brushing lesions twice a day with high-F
toothpaste (5000 ppm F).
• Fluoride interventions should be combined with meticulous dental hygiene and sugar control to
optimize the caries-controlling effect.
• Daily use of a fluoridated mouth-rinse may help in controlling root caries lesion development in
the elderly medically compromised patient.
• Chlorhexidine has no additional effect in combination with regular use of fluoride.
Caries
• Introduction - focus
• Burden of caries and periodontal disease over
lifetime
• Assess the evidence for age-adequate
effective strategies to prevent and treat caries
and periodontal disease.
PREVENTION
• Drop out (70 years -> 85 years (mortality/morbidity)
• Case definition (e.g. activity of RCL)
• Paucity and poverty of evidence
• Quantity and quality of studies on fluoride
effectiveness among adults!
• Poor compliance (difficult to control and measure)
• Patient/examiner blinding is limited
• Follow-up times rather short
PREVENTION
• Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007 May;86(5):410-5
• Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders. Journal of Dental Research 2010
Oct;89(10):1086-90.
• Gibson G, Jurasic M, Wehler C, Jones J, Supplemental fluoride use for moderate and high caries risk
• adults: a systematic review. J Public Health Dent. 71 (2011) 171–184.
• Ekstrand KR, Poulsen JE, Hede B, Twetman S, Qvist V, Ellwood RP. A randomized clinical trial of the anti-caries efficacy of 5,000 compared to
1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013;47(5):391-8
• Wierichs, R. J. & Meyer-Lueckel, H. (2015) Systematic review on noninvasive treatment of root caries lesions. Journal of Dental Research 94,
261–271.
• Drop out (70 years -> 85 years (mortality/morbidity)
• Case definition (e.g. activity of RCL)
• Paucity and poverty of evidence
• Quantity and quality of studies on fluoride
effectiveness among adults!
• Poor compliance
• Patient/examiner blinding is limited
• Follow-up times rather short
PREVENTION
• Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007 May;86(5):410-5
• Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders. Journal of Dental Research 2010
Oct;89(10):1086-90.
• Gibson G, Jurasic M, Wehler C, Jones J, Supplemental fluoride use for moderate and high caries risk
• adults: a systematic review. J Public Health Dent. 71 (2011) 171–184.
• Ekstrand KR, Poulsen JE, Hede B, Twetman S, Qvist V, Ellwood RP. A randomized clinical trial of the anti-caries efficacy of 5,000 compared to
1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013;47(5):391-8
• Wierichs, R. J. & Meyer-Lueckel, H. (2015) Systematic review on noninvasive treatment of root caries lesions. Journal of Dental Research 94,
261–271.
RECOMMENDATIONS (RANDOM ORDER)
• Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007 May;86(5):410-5
• Ferreira, R.C., De Magalhães, C.S., and Moreira, A.N. Tooth loss, denture wearing and associated factors among an elderly institutionalised
Brazilian population. Gerodontology (2008). 25, 168–178.
• Eke, P. I. et al. Journal of Periodontology 1–18 (2015).
• Heegaard, K.M., Holm-Pedersen, P., Bardow, A., Hvidtfeldt, U.A., Grøbæk, M., and Avlund, K. The Copenhagen Oral Health Senior Cohort:
Design, population and dental health. Gerodontology (2015) 28, 165–176.
• Assessment methods need to be converged, a gold
standard for periodontal recording is necessary.
• Qualitative research methods can be appropriate to
understand some complex relationships.
• Full mobile equipment will be useful.
• Using the shortest study duration reduces sample
bias
RECOMMENDATIONS (RANDOM ORDER)
• Chalmers, J.M., et al. Caries experience in existing and new nursing home residents in Adelaide, Australia. Gerodontology (2002) 19, 30–40.
• Palmer RF, Royall DR. Missing data? Plan on it! J Am Geriatric Soc (2010) 58:S343-S348.
• Previous studies can be useful to improve sampling
strategies.
• Recently evolved, statistically sound alternatives to
eliminating cases with missing data are now
accepted as state of the art.
• Full information likelihood procedure
• Multiple imputation methods
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B,
Preshaw PM, Pretty I, Renvert S, Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental
caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an
essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries be.
Journal of Clinical Periodontology 44, S135–S144 (2017).
FUTURE RESEARCH
There is an urgent need for epidemiological
surveillance of caries, periodontal diseases,
tooth loss and oral health-related quality of
life in older populations.
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B,
Preshaw PM, Pretty I, Renvert S, Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental
caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an
essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries be.
Journal of Clinical Periodontology 44, S135–S144 (2017).
FUTURE RESEARCH
There is an urgent need for epidemiological
surveillance of caries, periodontal diseases,
tooth loss and oral health-related quality of
life in older populations.
National oral health surveys need to include
representative samples of 65- to 74-year-olds and 75+
year-olds, including the very old (85 years and older)
and frail and/or care dependent elders, and older
people with multimorbidity and polypharmacy (e.g. by
oversampling).
Reporting of surveys need to follow standardized
formats in order to allow comparisons and data
synthesis.
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B,
Preshaw PM, Pretty I, Renvert S, Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental
caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an
essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries be.
Journal of Clinical Periodontology 44, S135–S144 (2017).
FUTURE RESEARCH
There is an urgent need for epidemiological
surveillance of caries, periodontal diseases,
tooth loss and oral health-related quality of
life in older populations.
Epidemiological evaluations in older populations
should include oral hygiene levels, tooth loss,
attachment level, pocket probing depths and
inflammation (bleeding on probing) as well as the
presence and number of coronal and root caries
lesions, their severity and activity.
Quality-of-life measures, salivary secretion rates and
(medical) risk factors should also be assessed.
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B,
Preshaw PM, Pretty I, Renvert S, Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental
caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an
essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries be.
Journal of Clinical Periodontology 44, S135–S144 (2017).
FUTURE RESEARCH
Priorities should be placed on how preventive
and therapeutic regimens may preserve oral
health, quality of life and nutrition into older
age as comorbidities present unique
challenge to the delivery of intrinsically
efficacious and effective strategies.
• Tonetti, M. S., Bottenberg P, Conrads G, Eickholz P, Heasman P, Lopez R, Madianos P, Müller F, Needleman I, Nyvad B,
Preshaw PM, Pretty I, Renvert S, Schwendicke F, Trombelli L, vd Putten GJ, Vanobbergen J, West N, Young A, Paris S. Dental
caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an
essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries be.
Journal of Clinical Periodontology 44, S135–S144 (2017).
FUTURE RESEARCH
Priorities should be placed on how preventive
and therapeutic regimens may preserve oral
health, quality of life and nutrition into older
age as comorbidities present unique
challenge to the delivery of intrinsically
efficacious and effective strategies.
To understand disease progression with age,
future long-term longitudinal studies recording
the disease extent and severity of both caries
and periodontitis in these age groups, as well as
a comprehensive set of preventive strategies,
are warranted.
ACKNOWLEDGMENT
• A valuable input from
Drs Barbara Janssens
Lynn Janssens
Ellen Palmers
!!
!

Prof. Dr. Jacques Vanobbergen
community dentistry and oral public health
E
www.ugent.be
www.gerodent.be
Ghent University
@ugent
Ghent University
thank you for your attention
Recommended

















